Embed Size (px)
Citation preview

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 1/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 2/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 3/338
Although great care has been taken to provide accurate and current information, neither the author(s)
nor the publisher, nor anyone else associated with this publication, shall be liable for any loss,
damage, or liability directly or indirectly caused or alleged to be caused by this book. The material
contained herein is not intended to provide specific advice or recommendations for any specific
situation.
Trademark notice: Product or corporate names may be trademarks or registered trademarks and are
used only for identification and explanation without intent to infringe.
Library of Congress Cataloging-in-Publication Data
A catalog record for this book is available from the Library of Congress.
ISBN: 0–8247–4107–2
This book is printed on acid-free paper.
Headquarters
Marcel Dekker, Inc.
270 Madison Avenue, New York, NY 10016, U.S.A.
tel: 212–696–9000; fax: 212–685–4540
Distribution and Customer Service
Marcel Dekker, Inc.
Cimarron Road, Monticello, New York 12701, U.S.A.
tel: 800–228–1160; fax: 845–796–1772
Eastern Hemisphere DistributionMarcel Dekker AG
Hutgasse 4, Postfach 812, CH–4001 Basel, Switzerland
tel: 41–61–260–6300; fax: 41–61–260–6333
World Wide Web
http://www.dekker.com
The publisher offers discounts on this book when ordered in bulk quantities. For more information,
write to Special Sales/Professional Marketing at the headquarters address above.
Copyright 2003 by Marcel Dekker, Inc. All Rights Reserved.
Neither this book nor any part may be reproduced or transmitted in any form or by any means,
electronic or mechanical, including photocopying, microfilming, and recording, or by any informa-tion storage and retrieval system, without permission in writing from the publisher.
Current printing (last digit):
10 9 8 7 6 5 4 3 2 1
PRINTED IN THE UNITED STATES OF AMERICA

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 4/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 5/338
Preface
Heil dir, Sonne!
Heil dir, Licht!
With the explosion of refractive surgical technologies and techniques we have wit-
nessed increased success in the treatment of hyperopia, but we still stand restrained in our
ability to free our patients from presbyopic spectacles. We eagerly await the momentof overcoming the seemingly insurmountable obstacles of presbyopic correction to echo
Brunhilde’s greetings of the sun and of the light in the third act of Wagner’s opera Siegfried ,
at the time of her resurrection after decades of slumber:
Long was my sleep.
Who is the hero who awakened me?
Siegfried forged “Nothung,” the famous sword that could be forged only by a man
who did not know fear, and used it to slay the dragon Fafner (and recover the magical
Ring and Tarnhelm). He defied the gods and entered Loge’s impenetrable circle of flames
to rescue the sleeping Brunhilde.
We are on the verge of facing a similar success story in refractive surgery. Many
unsung heroes are paving the way for the next discovery that will change the way we
treat hyperopia and revolutionize the surgical correction of presbyopia. The wide rangeof investigations covered in this book indicates that it will not be long before we will be
able to fulfill our quest to conquer these two frontiers in refractive surgery.
This book is the second of a series of books dedicated to refractive surgery published
by Marcel Dekker, Inc. The focus of the first volume in this series was LASIK fundamen-
tals, surgical techniques, and complications, a topic that has received a lot of coverage in
both the peer- and non-peer-reviewed literature. For this book, we asked Drs. Tsubota
iii

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 6/338
iv Preface
and Boxer Wachler to edit the manuscripts, and they have worked diligently with the
contributors to ensure maximal coverage and minimal redundancy.
It may come as no surprise to the reader that the methods of treatment of hyperopia
and presbyopia are grouped in a single refractive surgical textbook. The classical teachings
of physiological optics separate these two areas, but many of the surgical techniques
employed for the correction of hyperopia may have applications for presbyopia.
The introductory section is written by experts in the fields of basic optics, mecha-
nisms of accommodation, aging of the lens, and contact lens basics. Among topics dis-
cussed in the section on hyperopia are LASIK and PRK for hyperopia and hyperopic
astigmatism, laser thermokeratoplasty, conductive keratoplasty, hyperopic intracorneal
segments, phakic IOLs. The section on presbyopia includes discussions of monovision
refractive surgery, multifocal corneal approach, scleral relaxation, scleral expansion bands,
multifocal IOLs, refractive lens exchange with a multifocal intraocular lens, Phaco-Erstaz,
and accommodating and adjustable IOLs. The topographical changes, corneal surface
profiles, wavefront contrast sensitivity changes, and wound healing after hyperopic surgery
are discussed in a separate section with special emphasis on clinical applications. Thecontributors draw on first-hand experiences with the aim of providing an engaging book
covering these important topics.
We are indebted to the coeditors, students, residents, and colleagues who have made
valuable contributions to this book. We are grateful for their effort in integrating the
sometimes limited information in peer-reviewed literature with the knowledge derived
from their clinical experiences and interactions with colleagues. We hope that this provides
a text that is both clinically relevant and as evidence-based as possible.
We thank Dr. Geoffrey Greenwood and Elizabeth Curione of Marcel Dekker, Inc.,
for their commitment to this project. Special thanks go to Leona Greenhill, for her editorial
assistance, and to Rhonda Harris, who managed this project with care and precision. Her
attention to detail and her dedication have enabled us to work coherently in the face of
adversity.
We take the opportunity to acknowledge the pioneering surgeons and researchersin the field of refractive surgery. Their work and vision have provided the basis not only
for current advances in hyperopia and presbyopia that we can offer to our patients, but
also for future advances to be made by the next generation of thoughtful contributors to
this important field.
Dimitri T. Azar
Douglas D. Koch

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 7/338
Contents
Preface iii
Contributors ix
1. Introduction 1Kazuo Tsubota
2. Basic Optics of Hyperopia and Presbyopia 17
Michael K. Smolek and Stephen D. Klyce
3. The Helmholtz Mechanism of Accommodation 27
Adrian Glasser
4. S chachar’s Theory of the Mechanisms of Accommodation 47
Jay S. Pepose and Moonyoung S. Chung
5. Aging and the Crystalline Lens: Review of Recent Literature (1998–2001) 55
Leo T. Chylack, Jr.
6. Hyperopia 63
Ivo John Dualan and Penny A. Asbell
v

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 8/338
vi Contents
7. Surgical Treatment Options for Hyperopia and Hyperopic Astigmatism 69
Paolo Vinciguerra and Fabrizio I. Camesasca
8. Laser Thermokeratoplasty and Wavefront-Guided LTK 83
Shahzad I. Mian and Dimitri T. Azar
9. Conductive Keratoplasty for the Correction of Low to Moderate Hyperopia 95
Marguerite B. McDonald, Jonathan Davidorf, Robert K. Maloney,
Edward E. Manche, Peter Hersh, and George M. Salib
10. Intracorneal Segments for Hyperopia 107
Laura Gomez and Arturo S. Chayet
11. Anterior Chamber Phakic Intraocular Lenses in Hyperopia 115
Georges Baı koff
12. Hyperopic Phakic Intraocular Lenses 119
Thanh Hoang-Xuan and Franc ¸ois Malecaze
13. Hyperopia and Presbyopia: Topographical Changes 129
Stephen D. Klyce, Michael K. Smolek, Michael J. Endl, Vasavi Malineni,
Michael S. Insler, and Marguerite B. McDonald
14. Corneal Surface Profile After Hyperopia Surgery 141
Damien Gatinel
15. Wavefront Changes After Hyperopia Surgery 151
Maria Regina Chalita and Ronald R. Krueger
16. Contrast Sensitivity Changers After Hyperopia Surgery 163
Lavinia C. Coban-Steflea, Tommy S. Korn, and Brian S. Boxer Wachler
17. Wound Healing After Hyperopic Corneal Surgery: Why There Is Greater
Regression in the Treatment of Hyperopia 173
Renato Ambrosio, Jr., and Steven E. Wilson
18. Monovision Refractive Surgery for Presbyopia 189
Dimitri T. Azar, Margaret Chang, Carolyn E. Kloek, Samiah Zafar,
Kimberly Sippel, and Sandeep Jain
19. Multifocal Corneal Approach to Treat Presbyopia 201
Janie Ho and Dimitri T. Azar
20. Scleral Relaxation to Treat Presbyopia 209
Hideharu Fukasaku
21. The Scleral Expansion Procedure 219
Chris B. Phillips and Richard W. Yee

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 9/338
viiContents
22. Multifocal IOLs for Presbyopia 237
Hiroko Bissen-Miyajima
23. Refractive Lens Exchange with a Multifocal Intraocular Lens 249
I. Howard Fine, Richard S. Hoffman, and Mark Packer
24. The Limits of Simultaneous Ametropia Correction in Phaco-Ersatz 259
Arthur Ho, Fabrice Manns, Viviana Fernandez, Paul Erikson, and
Jean-Marie Parel
25. Accommodating and Adjustable IOLs 279
Sandeep Jain, Dimitri T. Azar, and Rasik B. Vajpayee
26. Accommodative Amplitude Measurements After Surgery for Presbyopia 287
David L. Guyton
27. Complications of Hyperopia and Presbyopia Surgery 291
Liane Clamen Glazer and Dimitri T. Azar
28. Future Developments 315
Brian S. Boxer Wachler
Index 319

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 10/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 11/338
Contributors
Renato Ambrosio, Jr., M.D. Department of Ophthalmology, University of Washington,
Seattle, Washington, U.S.A., University of Sao Paolo, Sao Paolo, and Department of
Cornea and Refractive Surgery, Clinica e Microcirurgia Oftalmologica Renato Ambrosio,
Rio de Janeiro, Brazil
Penny A. Asbell, M.D. Mount Sinai Medical Center, New York, New York, U.S.A.
Dimitri T. Azar, M.D. Corneal and Refractive Surgery Services, Massachusetts Eye
and Ear Infirmary, Schepens Eye Research Institute, and Harvard Medical School, Boston,
Massachusetts, U.S.A.
Georges Baı ¨koff, M.D. Clinique Montecelli, Marseille, France
Hiroko Bissen-Miyajima, M.D., Ph.D. Department of Ophthalmology, Tokyo Dental
College, Suidobash Hospital, Tokyo, Japan
Brian S. Boxer Wachler, M.D. Boxer Wachler Vision Institute, Beverly Hills, Califor-
nia, U.S.A.
Fabrizio I. Camesasca, M.D. Department of Ophthalmology, Istituto Clinico Humani-
tas, Milan, Italy
Maria Regina Chalita, M.D. Department of Refractive Surgery, Cole Eye Institute,
Cleveland Clinic Foundation, Cleveland, Ohio, U.S.A.
ix

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 12/338
x Contributors
Margaret Chang, M.S. Corneal and Refractive Surgery Services, Massachusetts Eye
and Ear Infirmary, Schepens Eye Research Institute, and Harvard Medical School, Boston,
Massachusetts, U.S.A.
Arturo S. Chayet, M.D. Codet Aris Vision Institute, Tijuana, B.C., Mexico
Moonyoung S. Chung, M.D. Pepose Vision Institute, Chesterfield, Missouri, U.S.A.
Leo T. Chylack, Jr., M.D. Department of Ophthalmology, Harvard Medical School and
Center for Ophthalmic Research, Brigham and Women’s Hospital, Boston, Massachusetts,
U.S.A.
Lavinia C. Coban-Steflea, M.D. Department of Ophthalmology, Bucharest University
Hospital, and Carol Davila University of Medicine and Pharmacy, Bucharest, Romania
Jonathan Davidorf, M.D. Davidorf Eye Group, West Hills, and Maloney Vision Insti-tute, Los Angeles, California, U.S.A.
Ivo John Dualan, M.D. Mount Sinai Medical Center, New York, New York, U.S.A.
Michael J. Endl, M.D. Department of Ophthalmology, Louisiana State University
Health Sciences Center, New Orleans, Louisiana, U.S.A.
Paul Erickson, O.D., Ph.D. Cooperative Research Centre for Eye Research and Tech-
nology, The University of New South Wales, Sydney, New South Wales, Australia
Viviana Fernandez, M.D. Ophthalmic Biophysics Center, Bascom Palmer Eye Institute,
University of Miami Medical School, Miami, Florida, U.S.A.
I. Howard Fine, M.D. Department of Ophthalmology, Casey Eye Institute, Oregon
Health and Science University, Portland, Oregon, U.S.A.
Hideharu Fukasaku, M.D. Fukasaku Eye Centre, Yokohama, Japan
Damien Gatinel, M.D. Fondation Ophthalomogique Adolphe de Rothschild and Bichat
Claude Bernard Hospital, Paris, France
Adrian Glasser, Ph.D. College of Optometry, University of Houston, Houston, Texas,
U.S.A.
Liane Clamen Glazer, M.D. Massachusetts Eye and Ear Infirmary, Schepens Eye Re-search Institute, and Harvard Medical School, Boston, Massachusetts, U.S.A.
Laura Gomez, M.D. Codet Aris Vision Institute, Tijuana, B.C., Mexico
David L. Guyton, M.D. Department of Ophthalmology, The Wilmer Institute, The Johns
Hopkins University School of Medicine, Baltimore, Maryland, U.S.A.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 13/338
xiContributors
Peter Hersh, M.D. Cornea and Laser Vision Center, Teaneck, New Jersey, U.S.A.
Arthur Ho, M.Optom., Ph.D. Cooperative Research Centre for Eye Research and Tech-
nology, The University of New South Wales, Sydney, New South Wales, Australia
Janie Ho, M.D. Department of Ophthalmology, University of California at San Fran-
cisco, San Francisco, California, U.S.A.
Thanh Hoang-Xuan, M.D. Fondation Ophthalomogique Adolphe de Rothschild and
Paris University, Paris, France
Richard S. Hoffman, M.D. Department of Ophthalmology, Casey Eye Institute, Oregon
Health and Science University, Portland, Oregon, U.S.A.
Michael S. Insler, M.D. Department of Ophthalmology, Louisiana State University
Health Sciences Center, New Orleans, Louisiana, U.S.A.
Sandeep Jain, M.D. Corneal and Refractive Surgery Service, Massachusetts Eye and
Ear Infirmary, Schepens Eye Research Institute, and Harvard Medical Schoool, Boston,
Massachusetts, U.S.A.
Carolyn E. Kloek, B.A. Corneal and Refractive Surgery Service, Massachusetts Eye
and Ear Infirmary, Schepens Eye Research Institute, and Harvard Medical School, Boston,
Massachusetts, U.S.A.
Stephen D. Klyce, Ph.D. Department of Ophthalmology, Louisiana State University
Health Sciences Center, New Orleans, Louisiana, U.S.A.
Tommy S. Korn, M.D. University of California–San Diego, and Sharp Rees-Stealy
Medical Group, San Diego, California, U.S.A.
Ronald R. Krueger, M.D. Department of Refractive Surgery, Cole Eye Institute, Cleve-
land Clinic Foundation, Cleveland, Ohio, U.S.A.
Francois Malecaze, M.D. Hopital Purpan, Toulouse, France
Vasavi Malineni, M.D. Department of Ophthalmology, Louisiana State University
Health Sciences Center, New Orleans, Louisiana, U.S.A.
Robert K. Maloney, M.D. Maloney Vision Institute, Los Angeles, California, U.S.A.
Edward E. Manche, M.D. Stanford University School of Medicine, Palo Alto, Califor-
nia, U.S.A.
Fabrice Manns, Ph.D. Ophthalmic Biophysics Center, Bascom Palmer Eye Institute,
University of Miami Medical School, Miami, and Department of Biomedical Engineering,
University of Miami College of Engineering, Coral Gables, Florida, U.S.A.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 14/338
xii Contributors
Marguerite B. McDonald, M.D. Department of Ophthalmology, Louisiana State Uni-
versity Health Sciences Center, New Orleans, Louisiana, U.S.A.
Shahzad I. Mian, M.D. Corneal and Refractive Surgery Service, Massachusetts Eye
and Ear Infirmary, Schepens Eye Research Institute, and Harvard Medical School, Boston,
Massachusetts, U.S.A.
Mark Packer, M.D. Department of Ophthalmology, Casey Eye Institute, Oregon Health
and Science University, Portland, Oregon, U.S.A.
Jean-Marie Parel, Ph.D. Ophthalmic Biophysics Center, Bascom Palmer Eye Institute,
University of Miami Medical School, Miami, Department of Biomedical Engineering,
University of Miami College of Engineering, Coral Gables, Florida, U.S.A., and University
of Liege, CHU Sart-Tilman, Liege, Belgium
Jay S. Pepose, M.D., Ph.D. Department of Ophthalmology and Visual Sciences, Wash-
ington University School of Medicine, St. Louis, and Pepose Vision Institute, Chesterfield,
Missouri, U.S.A.
Chris B. Phillips, M.D. Department of Ophthalmology, Hermann Eye Center and Uni-
versity of Texas Health Science Center at Houston Medical School, Houston, Texas,
U.S.A.
George M. Salib, M.S., M.D. Department of Ophthalmology, Tulane University School
of Medicine, New Orleans, Louisiana, U.S.A.
Kimberly Sippel, M.D. Massachusetts Eye and Ear Infirmary, Schepens Eye ResearchInstitute, and Harvard Medical School, Boston, Massachusetts, U.S.A.
Michael K. Smolek, Ph.D. Department of Ophthalmology, Louisiana State University
Health Sciences Center, New Orleans, Louisiana, U.S.A.
Kazuo Tsubota, M.D. Department of Ophthalmology, Tokyo Dental College, Ichikawa
City, Chiba, Japan
Rasik B. Vajpayee, M.D. Corneal and Refractive Surgery Service, Massachusetts Eye
and Ear Infirmary, Schepens Eye Research Institute, and Harvard Medical School, Boston,
Massachusetts, U.S.A.
Paolo Vinciguerra, M.D. Department of Ophthalmology, Istituto Clinico Humanitas,
Milan, Italy
Steven E. Wilson, M.D. Department of Ophthalmology, University of Washington, Se-
attle, Washington, U.S.A.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 15/338
xiiiContributors
Richard W. Yee, M.D. Department of Ophthalmology, Hermann Eye Center and Uni-
versity of Texas Health Science Center at Houston Medical School, Houston, Texas,
U.S.A.
Samiah Zafar, M.B.B.S. Corneal and Refractive Surgery Service, Massachusetts Eye
and Ear Infirmary, Schepens Eye Research Institute, and Harvard Medical School, Boston,
Massachusetts, U.S.A.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 16/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 17/338
1
Introduction
KAZUO TSUBOTA
Tokyo Dental College, Ichikawa City, Chiba, Japan
SUMMARY
A new era of refractive surgery is on the horizon in the field of hyperopia and presbyopia
correction. Corneal intervention, corneal implants, corneal rings, intraocular lenses, and
scleral intervention are the major treatment strategies. Although this field is new and some
of the novel surgeries may not endure into the future, this book covers all of the clinical
and basic research activities available as of the year 2003.
A. OVERVIEW
Refractive surgery is currently evolving toward a new stage. Although high myopia and
irregular astigmatism cannot be corrected fully, laser-assisted in situ keratomileusis
(LASIK) for myopia and myopic astigmatism has already become an established technol-
ogy, with millions of patients benefiting from LASIK every year all over the world. The
next challenge will be the correction of hyperopia and presbyopia. In most advanced
countries, life spans have been increasing annually and have now passed the 80-year mark.
Baby boomers in the United States, Japan, Europe, and other countries are getting older,
with an expected mean age of 50 to 60 years by the year 2005. Although the ratio of hyperopia cases is lower at younger ages, hyperopia becomes increasingly significant in
the later stages of life. It has been estimated that around 20% of the U.S. population are
hyperopic at the age of 40, and the rate is above 60% at age 65. Even in Japan, where
myopia is the dominant refractive error, the ratio increases from 15% at age 40 to 30%
at age 65. People may develop cataracts, possibly indicating phacoemulsification and
intraocular lens implantation, but the majority of the elderly still do not have cataract
1

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 18/338
2 Tsubota
Table 1 Medical and Surgical Correction of Hyperopia
Medical correction Surgical correction
Glasses
Contact lenses
Photorefractive keratectomy (PRK) or laser-
assisted in situ keratomileusis (LASIK)
Phakic intraocular lenses (IOLs)
Clear lens extraction with IOLs
Laser thermal keratoplasty (LTK)
Conductive keratoplasty (CK)
Diode laser keratoplasty
Corneal implant
Intracorneal ring (ICR) modification
surgery. It is well known that nearly everyone develops presbyopia with age. Thus, in anaging society, correction of hyperopiaandpresbyopia is anticipated to becomemore impor-
tant than it currently is.
This book covers the current medical and surgical treatments for the correction of
hyperopia and presbyopia. An effort is also made to cover new technologies, although
these are still preliminary and controversial. In this sense, this is no ordinary textbook
based only on authority and established principles. Rather, it is a new comprehensive
information book introducing current technology and developmental trials. The emerging
innovation of thermal or conductive keratoplasty as well as corneal implants for
hyperopic correction now provide exciting potential. Furthermore, the new Schachar
theory of presbyopia is now attracting attention as a strategy for the treatment of
presbyopia. Scleral relaxation, using a diamond knife or laser, and scleral expansion
rings are also potential technologies. All of the established as well as the new medical
and surgical treatments are described in this book, with the relevant theoretical back-
grounds, clinical results, and possible complications indicated (Tables 1 and 2, Figs.
1 and 2).
Table 2 Medical and Surgical Correction of Presbyopia
Medical correction Surgical correction
Key: HCL, hard contact lens; SCL, soft contact lens; LASIK, laser-assisted in situ
keratomileusis; IOL, intraocular lens.
Bifocal and multifocal glasses
Bifocal and multifocal HCL
Bifocal and multifocal SCL
Bifocal disposable SCL
Monovision by LASIK
Multifocal LASIK
IOL with multifocal
Hinged IOLScleral expansion ring
Scleral incision
Scleral relaxation by laser
Small-diameter corneal lens

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 19/338
3Introduction
Figure 1 Surgical correction of hyperopia.
Figure 2 Surgical correction of presbyopia.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 20/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 21/338
5Introduction
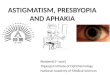
Figure 4 Photograph of epikeratophakia. Note the corneal lens on the top of the cornea.
technique was abandoned. Predictability was not adequate, such that the procedure did not
gain popularity. In the specific situation of postoperative hyperopia after radial keratotomy,
suturing of the corneal incision is useful for the correction of hyperopia up to 2 diopters. It
is believed to stabilize refractive status, thus minimizing corneal shape fluctuation (13,14).
Automated lamellar keratoplasty is another method for the correction of hyperopia.
Historically, the idea for this also came from keratomileusis. Steepening of the central
cornea was observed to occur with lamellar keratotomy alone. Recently, ectasia of the
cornea after myopic LASIK has become a major long-term safety concern. Progressive
ectasia in a significant percentage of eyes, another major concern, also renders this tech-
nique unattractive. When the cut is deep, more ectasia unavoidably occurs with this proce-dure. The amount of ectasia depends on the optical zone. When the optical zone is small,
the curvature is relatively high. When the optical zone is large, the curvature is low. The
nomogram was developed on the basis of this observation (15,16). When the optical zone
is 6.6 mm, the correction is 1.0 D; whereas the correction is 6.5 D with an optical zone
of 5.0 mm. The cut should be deep—e.g., 65%. The initial results were promising, but
the nomogram is not always predictable. With the development of hyperopic LASIK, use
of this procedure is now limited (17).
The mechanical corneal contouring device invented by Eiferman and Nordquist is
another means of correcting hyperopia (18). The principle is based on the observation that
when the peripheral cornea is flattened, the central optical power is increased. The instru-
ment consists of a vacuum chamber and steel blades positioned at orthogonal angles. When
a Teflon stopper is added to the blade and the stopper pressed down on the eye, the
peripheral cornea bulges, such that the blades can remove more tissue in the peripherythan at the central cornea. The clinical results remain unknown.
C. CURRENT SURGICAL CORRECTION OF HYPEROPIA
Photorefractive keratectomy (PRK) for hyperopia is useful for the correction of hyperopia
up to 3.0 to 4.0 D; however, healing of the corneal epithelium has effects on the final

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 22/338
6 Tsubota
result, such as regression and/or haze (19–23). Predictability is still poor for moderate to
high myopia. LASIK, which was originally developed for the correction of myopia
(24–26), is considered theoretically to be more advantageous for the correction of hyper-
opia because it is possible to ablate the corneal midperiphery by stromal photorefractive
ablation and to prevent strong epithelial regression with an overlying flap (27– 29). With
the expansion of optical zone treatment, LASIK has now become an acceptable treatment
for hyperopia of up to 5 D (30–36). This method is fully discussed in Chapters 7, 13–15.
The Phakic IOL has also been used for the correction of hyperopia as well as for
aphakia and high myopia (37–40). The use of posterior chamber phakic IOL, such as the
Staar Collamer implantable contact lens (Staar Surgical, AG, Nidau, Switzerland) appears
to be promising, although there is a risk of cataract formation. The recent development
of very light floating lenses, such as the Medennium (Ciba Vision, Duluth, GA), may be
another innovation. The lens is very light, almost floating, and does not touch the patient’s
own lens. Iris-claw lenses in phakic eyes, to correct hyperopia, are also promising (Fig.
5), despite the risks of glaucoma and corneal degeneration. Very thin anterior chamber
phakic IOLs, angle support lenses such as Nuvita (Bausch & Lomb Surgical, Rochester,NY), and new foldable lenses designed by Baıkoff (fully discussed in Chapter 11) are
other promising technologies. These are discussed in detail in Chapters 11 and 12. Clear
lens extraction can produce cystoid macular edema and retinal detachment and is less
accurate and predictable for hyperopia below 3.0 D (41,42).
Reshaping the corneal curvature by heating of the peripheral cornea is another major
approach for hyperopic correction. Currently, there are three ways to do this. One is laser
thermal keratoplasty (LTK) (43–46). This employs a holmium laser technique, called the
Sunrise LTK Procedure (Sunrise Technologies International, Inc. Fremont, CA), to heat
the corneal collagen in several spots in the periphery. The resulting thermal contraction
steepens the central corneal curvature, thus correcting hyperopia. This procedure has re-
ceived approval from the U.S. Food and Drug Administration (FDA). The treatment range
will be up to 2.5 D. The second method is conductive keratoplasty (CK) (Refractec, Inc,
Figure 5 Artisan hyperopia 5 mm, phakic intraocular lens (IOL) for the correction of hyperopia.
(Figure provided courtesy of OPHTEC BV, Groningen, The Netherlands.)

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 23/338
7Introduction
Figure 6 Conductive keratoplasty for the correction of hyperopia. (Figure provided courtesy of Refractec, Inc., Irvine, CA, USA.)
Irvine, CA) (Fig. 6). This method uses a radiofrequency generator as the energy source
instead of a holmium:YAG laser. The energy is delivered through a microtip inserted deep
into the stroma. The procedure is considered to minimize regression relative to LTK
because the energy is applied deep in the cornea, thereby creating an affected spot that is
uniform in depth. The CK was approved by the FDA in April 2002. Diode laser treatment
is a third approach (47–49). This procedure uses a 1.8-U diode laser as an energy source
(Rodenstock, Munich, Germany). The application is similar to CK in that the probe is in
contact with the peripheral cornea. The diode laser has not yet obtained FDA approval.
All three technologies are described in detail in Chapters 8 and 9.The ICS (Intrastromal Corneal Segments) or “Hyperopia Segments” is a variation
of the INTACS Prescription Inserts (Addition Technology, Inc., Fremont, CA) under
investigation in the United States, Europe, Brazil, Mexico, Singapore, and the U.K. While
INTACS inserts correct for myopia by flattening the central portion of the cornea, the
ICS is designed to correct hyperopia by steepening the anterior corneal curvature by the
insertion of the ring materials at the limbal area, instead of inserting at the 7-mm central
zone as for myopic correction. The ICS may also be used for hyperopia concurrent with
astigmatism or hyperopic astigmatism. Clinical investigations have been initiated in both
Mexico and Europe for the treatment of hyperopia using the ICS clinical product. The
results are most encouraging, with stability achieved around the Month 3 exam and hyper-
opic corrections of up to 4.63 D (based MRSE) at Month 6 (n 43) and slightly less than
3.0 diopters of hyperopic correction (2.75 D) at the Month 12 exam. Manifest Refraction
stability is demonstrated through the Month 12 time point. Clinical trials in Europe areongoing.
Corneal implants have long been an attractive idea, but lack of suitable materials has
inhibited the development of this technology. New materials have again made it attractive.
Historically, Barraquer, who inserted glass materials into the corneal stroma in animals,
developed the intracorneal technique. There was always a loss of transparency, with vascu-
larization and extrusion of lenses. It was not known at that time that nutrients such as

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 24/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 25/338
9Introduction
request to move into Phase II of the clinical protocol. As of November 2002, Anamed is
awaiting FDA approval to begin Phase II. This is considered to be a promising technology.
However, the long-term complications—such as corneal stromal and epithelial thinning
as well as endothelial change—must be evaluated in terms of safety.
D. CURRENT MEDICAL AND SURGICAL CORRECTION OF
PRESBYOPIA
The major means of correction are simple glasses or simple contact lenses (55). The
development of bifocal glasses provided the first convenience, allowing the use of only
one pair of glasses throughout the day. Bifocal contact lenses are another popular method
for the correction of presbyopia (56). According to the 1999 contact lens spectrum reader
profile survey, 21.5% were fit with monovision, 9% with soft multifocals, 3% with rigid
gas permeable (RGP) multifocals, and 5% with single-vision contact lenses and reading
glasses. The remainder had spectacles only. A major disadvantage of this method is com-
promised visual quality (57). Success depends on the patient having a realistic expectation.Monovision contact lenses are also used (58,59). The increasing prevalence of dry eye in
the elderly might be an obstacle to the application of this technique for many patients.
Since the introduction of disposable bifocal contact lenses (Vistakon’s Acuvue Contact
Lenses, Jacksonville, FL) in 1999 (60), use of bifocal contact lenses for the correction of
presbyopia has been increasing. With further development of materials and designs from
companies such as Ciba Vision and Bausch & Lomb, Inc., bifocal contact lenses have
apparently become the major corrective method for presbyopia.
The intraocular lens with multifocal optics is another method for correcting presby-
opia. This method is based on a theory termed “the simultaneous vision principle,” whereby
separate images of near and distant objects are formed and, if the power difference between
the two optical systems is more than 3.0 D, the images are dissimilar enough for the brain
to interpret them as separate. The brain therefore selects the highly focused image and
suppresses the other. This IOL can be achieved with two distinct optical elements (bifocalIOL) (61) or by means of diffractive optics (62), in which concentric diffractive zones
are applied to the posterior surface of the implant in order to focus light from near objects.
Both types of IOLs require central fixation and are relatively successful in younger patients.
Monovision intraocular lenses are also the choice for presbyopic correction (61).
The IOL with real accommodative power has long been studied by Japanese and
other researchers. The gel technology reached a certain level, using monkey eyes, in which
the lens capsule was filled with soft gel. However, clinical application has not yet begun.
Recently, a hinged haptic accommodative lens was developed and has attracted considera-
ble attention. The proper functioning of the lens is dependent on movement of the remain-
ing lens capsule, contracted by the ciliary muscle. When the lens capsule expands, the
lens changes position and focuses. There are now several companies working on this
technology (Fig. 8).
Like the multifocal intraocular lens, LASIK can also offer the multifocal effect bymeans of changing the corneal shape. It was first observed that regional variation in corneal
curvature in the eyes of patients 45 years of age or older sometimes provides good near
vision without correction (63). The regional variation in corneal power apparently ex-
plained how the multifocal lens effect could be achieved. Thus, intentional multifocal
LASIK is a potential technology, which is still under investigation (64). Another practical
method is monovision LASIK. Monovision is defined as providing optical correction of

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 26/338
10 Tsubota
Figure 8 Finite-element computer simulation of accommodative intraocular lens (IOL), a flexible
micro-opticwith accommodative features. (Figure provided courtesy of Human Optics AG,Erlangen,
Germany.)
one eye for distance vision and of the other eye for near vision. This is usually achieved
with contact lenses or intraocular lenses after cataract extraction, but can be achieved by
LASIK as well (65). The ideal diopter difference necessary for both distant and near vision
has not yet been determined. Since most patients with presbyopia undergoing LASIK still
have some accommodative ability, there are several components that should be evaluatedand determined for mass application of LASIK monovision. This is fully discussed by
Azar in Chapter 18.
The concept of anterior ciliary sclerotomy (ACS) is a new challenge in the treatment
of presbyopia (66). This surgery is based on the theory that the lens is ectodermal in origin
and constantly grows throughout life, gradually filling the eye and leaving no space for
accommodation (67,68). Loss of lens elasticity might contribute to the mechanism of
presbyopia, and this theory raises the possibility that reduced space is the cause of the
reduced accommodative power of the lens. Thus, somehow expanding the globe by ciliary
sclerotomy can provide space for the ciliary body and lens for accommodation. Along
this line, the original anterior sclerotomy as well as Fukasaku incisional surgeries have
been developed (69). Since there is regression of the results due to wound healing, Fuka-
saku recently developed a method of inserting silicon plugs for the maintenance of the
incision (69). Furthermore, the erbium:YAG laser has also been applied to making a widescleral incision that may not heal quickly, thus maintaining the effect (Figs. 9 and 10). I
have personal experience of two patients who had previously undergone LASIK. Both
were Japanese males, aged 58 and 48 years. Both had 1.0 far vision without correction
and near vision of 0.3 without correction, and both were having difficulty with reading.
I applied the laser to a limbal-scleral area 4.0 mm in length. A total of 8 lasers were
applied in a radial configuration. One day after surgery, both patients had 0.6 to 0.7 near

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 27/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 28/338
12 Tsubota
Figure 10 Slit-lamp view of the sclera incision by Erbium:YAG. The arrow indicates the incisionfully covered by the conjunctiva.
vision without correction, reporting that they could read the newspaper without glasses.
The technique must be evaluated in regard to long-term safety and efficacy, but the results
appear to be promising. Recently, Schachar et al. proposed a new surgical treatment using
a scleral expansion ring based on the same theory (Fig. 11) (67). Since several negative
reports have been published on this theory and surgery (70,71), this area is discussed in
Chapters 3, 20, and 21.
Figure 11 Slit-lamp view of the Schachar scleral band. Note that the scleral band is visible and
slightly elevated.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 29/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 30/338
14 Tsubota
26. Pallikaris IG, Papatzanaki ME, Stathi EZ, Frenschock O, Georgiadis A. Laser in situ keratomi-
leusis. Lasers Surg Med 1990; 10:463–468.
27. Ditzen K, Huschka H, Pieger S. Laser in situ keratomileusis for hyperopia. J Cataract Refract
Surg 1998; 24:42–47.
28. Argento CJ, Cosentino MJ. Laser in situ keratomileusis for hyperopia. J Cataract Refract Surg
1998; 24:1050–1058.
29. Knorz MC, Lierman A, Jendritza B, Hugger P. LASIK for hyperopia and hyperopic astigma-
tism—results of a pilot study. Semin Ophthalmol 1998; 13:83–87.
30. Zadok D, Maskaleris G, Montes M, Shah S, Garcia V, Chayet A. Hyperopic laser in situ
keratomileusis with the Nidek EC–5000 excimer laser. Ophthalmology 2000; 107:1132–1137.
31. Argento CJ, Cosentino MJ. Comparison of optical zones in hyperopic laser in situ keratomi-
leusis: 5.9 mm versus smaller optical zones. J Cataract Refract Surg 2000; 26:1137–1146.
32. Buzard KA, Fundingsland BR. Excimer laser assisted in situ keratomileusis for hyperopia. J
Cataract Refract Surg 1999; 25:197–204.
33. Williams DK. One-year results of laser vision correction for low to moderate hyperopia.
Ophthalmology 2000; 107:72–75.
34. Esquenazi S, Mendoza A. Two-year follow-up of laser in situ keratomileusis for hyperopia.J Refract Surg 1999; 15:648–652.
35. O’BrartDP, Stephenson CG,Baldwin H, Ilari L, Marshall J. Hyperopic photorefractive keratec-
tomy with the erodible mask and axicon system: two year follow-up. J Cataract Refract Surg
2000; 26:524–535.
36. Lindstrom RL, Linebarger EJ, Hardten DR, Houtman DM, Samuelson TW. Early results of
hyperopic and astigmatic laser in situ keratomileusis in eyes with secondary hyperopia. Oph-
thalmology 2000; 107:1858–1863; discussion 1863.
37. Davidorf JM, Zaldivar R, Oscherow S. Posterior chamber phakic intraocular lens for hyperopia
of 4 to 11 diopters. J Refract Surg 1998; 14:306–311.
38. Rosen E, Gore C. Staar Collamer posterior chamber phakic intraocular lens to correct myopia
and hyperopia. J Cataract Refract Surg 1998; 24:596–606.
39. Sabbagh LB. Phakic IOLs revisited; the current FDA trials. J Refract Surg 2000; 6:664–667.
40. Vetrugno M, Cardascia N, Cardia L. Anterior chamber depth measured by two methods in
myopic and hyperopic phakic IOL implant. Br J Ophthalmol 2000; 84:1113–1116.41. De Smedt SK, Vrijghem JC. Clear lens extraction to correct hyperopia in presbyopic eyes
with or without arcuate keratotomy for pre-existing astigmatism. Bull Soc Belge Ophtalmol
2000; 277:43–51.
42. Lyle WA, Jin GJ. Clear lens extraction to correct hyperopia. J Cataract Refract Surg 1997;
23:1051–1056.
43. Koch DD, Kohnen T, Anderson JA, Binder PS, Moore MN, Menefee RF, Valderamma GL,
Berry MJ. Histologic changes and wound healing response following 10-pulse noncontact
holmium:YAG laser thermal keratoplasty. J Refract Surg 1996; 12:623–634.
44. Koch DD, Kohnen T, McDonnell PJ, Menefee RF, Berry MJ. Hyperopia correction by noncon-
tact holmium:YAG laser thermal keratoplasty. United States phase IIA clinical study with a
1-year follow-up. Ophthalmology 1996; 103:1525–1535; discussion 1536.
45. Alio JL, Ismail MM, Sanchez Pego JL. Correction of hyperopia with non-contact Ho:YAG
laser thermal keratoplasty. J Refract Surg 1997; 13:17–22.
46. Eggink CA, Meurs P, Bardak Y, Deutman AF. Holmium laser thermal keratoplasty for hyper-
opia and astigmatism after photorefractive keratectomy. J Refract Surg 2000; 16:317–322.
47. Brinkmann R, Koop N, Geerling G, Kampmeier J, Borcherding S, Kamm K, Birngruber R.
Diode laser thermokeratoplasty: application strategy and dosimetry. J Cataract Refract Surg
1998; 24:1195–1207.
48. Geerling G, Koop N, Tungler A, Brinkmann R, Wirbelauer C, Birngruber R, Laqua H. Diode
laser thermokeratoplasty. Initial clinical experiences. Ophthalmologe 1999; 96:306–311.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 31/338
15Introduction
49. Geerling G, Koop N, Brinkmann R, Tunglar A, Wirbelauer C, Birngruber R, Laqua H. Continu-
ous-wave diode laser thermokeratoplasty: first clinical experience in blind human eyes. J
Cataract Refract Surg 1999; 25:32–40.
50. Schanzlin DJ. Studies of intrastromal corneal ring segments for the correction of low to moder-ate myopic refractive errors. Trans Am Ophthalmol Soc 1999; 97:815–890.
51. Cochener B, Savary-LeFloch G, Colin J. Effect of intrastromal corneal ring segment shift on
clinical outcome: one year results for low myopia. J Cataract Refract Surg 2000; 26:978–986.
52. Asbell PA, Ucakhan OO, Durrie DS, Lindstrom RL. Adjustability of refractive effect for
corneal ring segments. J Refract Surg 1999; 5:627–631.
53. Lindstrom R. Small diameter intracorneal inlay lens for the correction of presbyopia. In: Sher
N, ed. Surgery for Hyperopia and Presbyopia. Baltimore: Williams & Wilkins. 1997:195–199.
54. Keates RH, Martines E, Tennen DG, Teich C. Small-diameter corneal inlay in presbyopic or
pseudophakic patients. J Cataract Refract Surg 1995; 21:519–521.
55. Fonda G. Presbyopia corrected with single vision spectacles or corneal lenses in preference
to bifocal corneal lenses. Trans Ophthalmol Soc Aust 1966; 25:78–80.
56. Back A, Grant T, Hine N. Comparative visual performance of three presbyopic contact lens
corrections. Optom Vis Sci 1992; 69:474–480.
57. Atwood JD. Presbyopic contact lenses. Curr Opin Ophthalmol 2000; 11:296–298.58. Westin E, Wick B, Harrist RB. Factors influencing success of monovision contact lens fitting:
survey of contact lens diplomates. Optometry 2000; 71:757–763.
59. Josephson JE, Caffery BE. Monovision vs aspheric bifocal contact lenses: a crossover study.
J Am Optom Assoc 1987; 58:652–654.
60. Key JE, Yee JL. Prospective clinical evaluation of the Acuvue Bifocal contact lens. Clao J
1999; 25:218–221.
61. Chateau N, Baude D. Simulated in situ optical performance of bifocal contact lenses. Optom
Vis Sci 1997; 74:532–539.
62. Gray PJ, Lyall MG. Diffractive multifocal intraocular lens implants for unilateral cataracts in
prepresbyopic patients. Br J Ophthalmol 1992; 76:336–337.
63. Moreira H, Garbus JJ, Fasano A, Lee M, Clapham TN, McDonnell PJ. Multifocal corneal
topographic changes with excimer laser photorefractive keratectomy. Arch Ophthalmol 1992;
110:994–999.
64. Anschutz T. Presbyopic PRK. In: Sher N, ed. Surgeryfor Hyperopia and Presbyopia. Baltimore:
Williams & Wilkins, 1997:63–77.
65. Hom MM. Monovision and LASIK. J Am Optom Assoc 1999; 70:117–122.
66. Thornton S. Anterior ciliary sclerotomy (ACS), a procedure to reverse presbyopia. In: Sher
N, ed. Surgery for Hyperopia and Presbyopia. Baltimore: Williams & Wilkins, 1997:33–36.
67. Schachar RA. Cause and treatment of presbyopia with a method for increasing the amplitude
of accommodation. Ann Ophthalmol 1992; 24:445–447, 452.
68. Schachar RA. Pathophysiology of accommodation and presbyopia. Understanding the clinical
implications. J Fla Med Assoc 1994; 81:268–271.
69. Fukasaku H, Marron JA. Anterior ciliary sclerotomy with silicone expansion plug implantation:
effect on presbyopia and intraocular pressure. Int Ophthalmol Clin 2001; 41:133–141.
70. Glasser A, Kaufman P. The mechanism of accommodation in primates. Ophthalmology 1999;
106:863–872.
71. Mathews S. Scleral expansion surgery does not restore accommodation in human presbyopia.
Ophthalmology 1999; 106:873–877.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 32/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 33/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 34/338
18 Smolek and Klyce
For the emmetrope, the far point is located at optical infinity, and no power correction
is needed to image a distant target onto the retina (Fig. 1). In myopia, the far point lies
close to and a finite distance in front of the eye, so that light from the far point target
enters the eye with a certain amount of negative vergence. The amount of negative vergence
cancels the excess power inherent within the myopic eye, and the light comes to a focus
at the retina. The specific location of the far point for the “nearsighted” myope depends
on the level of myopic error; the higher the error, the nearer the far point will be to the
eye. In order for the myope to clearly see a target located at optical infinity, negative
power must be added to reduce the vergence of the distant light to a negative amount
before it enters the eye; otherwise the excessive power of the eye’s optics must be reduced,
as through flattening of the cornea by laser surgery. Myopic error is always expressed
with a negative sign indicative of the negative power that must be added to achieve
correction for viewing distant targets.
In hyperopia, the far point is commonly said to exist “beyond infinity,” because
only converging rays can be brought to a focus onto the retina in the uncorrected hyperope
(Fig. 1). Actually, it is more accurate to say that the far point of the hyperope is a virtualobject that is located a finite distance behind the retina. The far point of the hyperope can
be found by noting the location where the converging rays entering the eye would come
to a focus if the eye were not present to intercept the light.
Because hyperopic eyes have insufficient plus power to see targets clearly at infinity,
positive vergence must be added to the light entering the eye and the refraction is signified
by a plus sign. Plus power can be added to the light entering the eye or the eye itself can
be made to have relatively more power by making the cornea steeper through laser surgery.
However, many young to middle-aged hyperopes can fully correct their distance vision
error by adding enough plus power through accommodation to shift the far point to infinity.
This ability to self-correct their refractive error gives these hyperopes a distinct advantage
over myopes, who cannot “disaccommodate” to move the far point away from the eye.
It also explains why these hyperopes can be considered to be farsighted, because they in
fact become self-corrected for far vision. Unfortunately, as hyperopes age, the ability to
Figure 1 Far point location specified for three refractive states. R is the location of the far point,
defined as the most remote distance at which the unaccommodated eye can see clearly. R’ is the
conjugate focus of the far point, which is always located at the retina. D refers to the vergence
power entering the eye to bring light to a focus on the retina: zero for emmetropia, negative for
myopia, and positive for hyperopia.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 35/338
19Basic Optics of Hyperopia and Presbyopia
Figure 2 Graphic representation of the decline in accommodative amplitude with age (2).
accommodate diminishes (Fig. 2); thus they lose their ability to see clearly at any distance,
while older myopes still retain at least a portion of their ability to see clearly at some
distance.
C. ACCOMMODATION FOR NEAR VISION
The closer an object is to the cornea, the greater the divergence of light entering the eye
and the greater the need for more plus power to make the near object conjugate with the
retina. In youth, accommodation allows viewing at a variety of distances from infinity tovery near targets. As a person ages, however, the accommodative ability decreases, and
the near point moves away from the eye. Because uncorrected hyperopes often use a
portion of their accommodative ability to correct their refractive error for distance, the
near point is located farther from the eye; therefore hyperopes often experience near vision
problems at an earlier age than myopes or emmetropes. It should be noted that some
myopes may not experience any near vision problems in the uncorrected state if their
refractive error maintains a clear image within a comfortable working distance that is
neither too close nor too far from their eyes.
It is important to appreciate that there is a limited and diminishing amount of accom-
modation available at any given age and that the amount available depends in part on
whether accommodation is being used to correct for a hyperopic error. This amount of
accommodation in play is specified by the amplitude of accommodation, which is defined
as the vergence difference between the far point and the near point. The relationshipbetween age and accommodative amplitude was established by Donders (1) and later
refined by Duane (2), who presented what has since become the classic representation of
accommodative amplitude as a function of age (Fig. 2). Duane’s data show that accommo-
dation begins to decrease in early adulthood, well before the decline is noticed during
the performance of near vision tasks, such as reading. For adolescents, accommodative
amplitude is approximately 14 D, which corresponds to a near point of approximately 7

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 36/338
20 Smolek and Klyce
cm for an emmetrope. By age 45, this accommodative amplitude drops, due to changes
in the accommodative apparatus controlling the crystalline lens power, to about 4 D and
results in at best a 25-cm near point distance for that same emmetrope. Normal reading
distance is considered to be around 15 in. or 37 cm, which is still within the range of a
person in his or her mid- to late forties. However, it must be remembered that a continuous
and excessive need to accommodate can be tiring and uncomfortable, so the decline in
accommodative amplitude will be noticed by many subjects who are only in their mid-
forties and who still have a fair amount of accommodative amplitude in reserve.
If the eye has insufficient accommodative amplitude, which normally occurs with
advancing age and requires a plus lens addition for comfortable near vision, the condition is
called presbyopia. There are no specific values that define the absolute onset of presbyopia,
because its effects are dependent on a number of factors including the refractive error,
age, amplitude of accommodation, and the near vision tasks and lifestyle of a particular
patient. Because using accommodation to correct for distance vision is often tiring in itself,
the hyperope will be more likely to complain of tired eyes, eyestrain, and diplopia, and
may do so at an earlier age. Children do not normally experience vision problemsfrom mild amounts of hyperopia because their accommodative reserve is large. However,
those with moderate to high levels of hyperopia may experience visual problems
ranging from mild eyestrain and headaches after near work to more severe problems
such as strabismus and amblyopia (3). Some of these complaints are associated specifi-
cally with the ability of the two eyes to fuse images binocularly, because the accommoda-
tive process is neurologically tied to the convergence of the eyes.
There is a clinical distinction made between accommodative amplitude, which is
the optical difference between the near and far point measured in diopters, and the range
of accommodation, which is the linear difference between the far point and the near point
in terms of physical distance. In the uncorrected myope, the far point may be located very
close to the eye. The myope’s range of accommodation is thus very limited, whereas
prepresbyopic low hyperopes may have a range that allows vision to infinity, just as in
emmetropia (Fig. 3).
D. MANIFEST VERSUS LATENT HYPEROPIA
The refractive state of the eye is measured at rest with respect to the far point, but achieving
a totally unaccommodated state can be problematic, especially in the uncorrected hyperope
who uses accommodation to self-correct for distance vision. Consequently, refractions are
separated into two basic types—manifest and latent refractions—which can give different
refraction values for the same eye. A manifest refraction is the obvious, nonhidden part
of the refraction that is based on the elimination of any natural stimulus to accommodate.
Generally this is best accomplished by providing additional positive vergence of a known
amount to the incoming light to the extent that the eye is made artificially myopic. The
process is referred to as fogging. The far point thus moves to a finite distance in front of
the eye, which in itself is beneficial with respect to interacting with and measuring thelocation of the far point. Of course, once the myopia-shifted far point is measured, the
added vergence power is subtracted to provide the true far point location.
While fogging a patient removes the manifest portion of the total accommodation
that may be in play, it does not necessarily remove the latent or hidden portion of accommo-
dation that may still exist. Latent accommodation is that part which cannot be relaxed due
to excessive, spastic tonicity of the ciliary apparatus controlling accommodation. Self-

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 37/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 38/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 39/338
23Basic Optics of Hyperopia and Presbyopia
D hyperope wearing glasses who has successful refractive surgery is expected to lose two
to four letters of acuity as a result of moving the correction to the cornea, depending on
the exact distance of the spectacle plane from the cornea (Table 1).
F. HYPEROPIA AND BIOMETRIC CHANGES DURING LIFE
Based on spherical equivalent data obtained during cycloplegic refractions, the average
eye is hyperopic through most of life (Fig. 4). The average refraction is approximately
2.25 D at birth and reaches a hyperopic peak around 8 years of age, after which the
refraction becomes increasingly less hyperopic during adolescence and comes close to
being emmetropic during early adulthood (5). In the Beaver Dam Eye Study of adults,
hyperopia was more prevalent than myopia in age-matched subjects (49 vs 26.2%, respec-
tively, p 0.0001) (6). Hyperopia increases in later adulthood from 22.1% between ages
43 and 54 to 68.5% at age 75 and above; however, Slataper noted that the refraction
tends to drift back toward myopia with very advanced age (5). The hyperopic shift
for older adults between the ages of 45 and 65 has been attributed to reductions inthe axial length of the eye and changes in the focal power of the lens (7). The cause
of the myopic drift in advanced age may be attributed to a shrinking radius of
curvature of the cornea, which leads to a higher corneal power (8). This effect occurs
predominantly in females (9).
Passive growth of the eye during childhood tends to be a correlated, uniform expan-
sion of ocular dimensions (7,10). By “correlated” we mean that as eye growth causes the
retina to recede from the optical elements of the eye, we also see changes in the lens and
cornea that ideally allow emmetropia to be achieved if the eye is hyperopic or retained
if the eye is already emmetropic. Furthermore, it must be remembered that as axial length
increases, there is a reduction in the vergence power required to focus an image on the
Figure 4 Graph based on Slataper’s data (5) of average refractive error during life. Note that the
error tends to be hyperopic throughout life and relatively stable from young adulthood to middle
age. N 34,570 eyes assessed by cycloplegic refractions.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 40/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 41/338
25Basic Optics of Hyperopia and Presbyopia
error and the axial length of the globe (r 2 0.611, p 0.0001) (14). There was also a
weak but significant correlation between mean corneal radius and mean refractive error
(r2 0.128, p 0.009). Grosvenor also found that hyperopic eyes were smaller and
tended to have flatter corneas than emmetropic eyes (15).
G. OPTICS OF THE CRYSTALLINE LENS
The lens has an average index of refraction that higher than the index of corneal stroma
(1.427 vs. 1.376) (16). However, the contribution of the lens to the total power of the eye
is about half that of the anterior corneal surface, because the lens is surrounded by fluid
with an index near 1.336, whereas the cornea is exposed to air with an index of 1.0, which
greatly increases its refractivity. While a single index of refraction of the lens is useful
for simple calculations, in reality, the lens cannot be defined by a single value. Mapping
the gradient index of the lens has proved difficult. Simple models using concentric shells
of varying index gradients do not yield accurate ray-tracing results, and the models do
not agree with refractive index measurements made by tissue probes (17). It is interestingto find that significant levels of transient hyperopia have been attributed entirely to changes
in the refractive index of the lens. Saito and coworkers noted hyperopia peaking between
1 to 2 weeks after abrupt decreases in plasma glucose and attributed this effect to water
influx into the lens (18). Okamoto et al. also noted hyperopia after treatment forhyperglyce-
mia and found no changes in lens thickness or anterior chamber depth, thus implicating
a change entirely due to the refractive index of the lens (19).
Although the lens is the primary component associated with accommodation for near
vision, the contribution of depth of focus of the eye should not be discounted, particularly in
presbyopic eyes. Brighter viewing conditions or the use of miotics that constrict the pupil
increase the depth of focus and help to extend the effective range of accommodation.
H. OPTICAL ABERRATIONS
The shape of the gradient index profile across the lens as well as shape changes due to
accommodation alter not only effective power but also the spherical aberration of the eye
(20). By accommodating to approximately 3 D (a 33-cm viewing distance), the negative
spherical aberration of the lens corrects for much of the positive spherical aberration
induced by the cornea (21). Further accommodation tends to give the eye an overall
negative spherical aberration, but the exact amount varies among individuals (22). In
general, near accommodation tends to increase the monochromatic wavefront aberrations
of the eye (23). Fourth-order aberrations can either increase or decrease with increasing
accommodation, but higher-order aberrations tend to increase (22). It has been suggested
that there is no correlation between the change in aberration during accommodation and
the total amount of aberration for the relaxed eye (22). It can be concluded that any
clarity of vision provided by refractive surgery must diminish by a measurable extent with
accommodation, but certainly more work needs to be done to ascertain the significanceof aberration change on visual performance.
REFERENCES
1. Donders FC. On the Anomalies of Accommodation and Refraction of the Eye. London, 1864.
2. Duane A. Normal values of accommodation at all ages. JAMA 1912; 59:1010– 1013.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 42/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 43/338
3
The Helmholtz Mechanism of
Accommodation
ADRIAN GLASSER
College of Optometry, University of Houston, Houston, Texas, U.S.A.
“There is no other portion of physiological optics where one finds so many differing and
contradictory ideas as concerns the accommodation of the eye, where only . . . in the most
recent time have we actually made observations where previously everything was left to the
play of hypotheses.”
H. Von Helmholtz (1909)
A. INTRODUCTION
In 1853 Hermann von Helmholtz described the mechanism of accommodation of the
human eye. This was not the first description of how the human eye accommodates. Many
descriptions of and much research on accommodation preceded the work of Helmholtz
(1), yet the accommodative mechanism of the human eye is still generally referred to as
the “classic Helmholtz accommodative mechanism.” Helmholtz succeeded where others
had failed at providing a comprehensive and consistent explanation of how accommodation
occurs. It was comprehensive in that he described the functions of all of the major elements
of the accommodative apparatus, and it was consistent in that it required no significant
modifications of what was known with certainty at the time regarding how accommodation
occurs.
B. THE ANATOMY OF THE ACCOMMODATIVE APPARATUS
In order to understand how accommodation occurs, it is necessary to have a clear under-
standing of the accommodative apparatus and the relationships of the accommodative
structures to each other. While in recent years there has been some limited debate over
27

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 44/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 45/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 46/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 47/338
31The Helmholtz Mechanism of Accommodation
change of accommodation and is readily measured. The cornea, the anterior and posterior
lens surfaces, and the lens gradient refractive index provide optical refractive power to
the eye. In the unaccommodated, emmetropic eye, the optical refracting power allows the
image of a distant object to be focused on the retina. In this case, parallel rays of light
from the distant object enter the eye and become convergent to focus the image on the
retina. A near object, closer to the eye than optical infinity, however, has diverging light
rays entering the cornea. In order for the divergent rays to be drawn to a focus on the retina,
the optical power of the eye must increase. During accommodation, this is accomplished
primarily by an increase in curvature of the anterior and posterior lens surfaces. In addition,
lens thickness increases and anterior chamber depth and, to a lesser degree, vitreous cham-
ber depth decreases during accommodation. All these changes contribute to an increase
in optical refracting power. If the optical power or the refraction of a young eye is measured
with an objective refractometer during accommodation, it is clear that the optical power
increases, resulting in a myopic shift in the refraction.
2. Depth of FieldThe accommodative triad describes the neuronally coupled accommodation, convergence,
and pupil constriction that occur with an accommodative effort. Both accommodation and
pupil constriction contribute to near visual acuity. Depth of field is the distance an object
can be moved in object space without appreciably altering image focus or, in the case of
the eye, without appreciably altering the eye’s visual acuity. This plays an important role
in the perception of a sharply focused image on the retina. An eye with a large pupil
diameter has a small depth of field. This means that the eye can detect a change in focus
of the retinal image with small movements of the object toward or away from the eye.
An eye with a small pupil diameter has a large depth of field. In this case, the object can
be moved a greater distance toward or away from the eye without appreciably altering
the retinal image focus. The pupillary constriction that occurs with accommodation results
in an increased depth of field, which also contributes to maintaining a clear image of a
near object on the retina. Pupillary constriction can also occur without accommodation,
as with increased illumination. This too improves depth of field and hence near reading
ability, but without accommodation. Pupillary constriction and increased depth of field
are important for improving near reading ability but are very different from the refractive
change that accompanies accommodation.
3. Aberrations of the Eye
The imperfect optics of the eye mean that the eye suffers from optical aberrations. The
low-order aberrations, such as defocus and astigmatism, can be corrected with optical
prescriptions, but higher-order aberrations cannot. These higher-order aberrations include
spherical aberration and coma, for example. While the presence of aberrations in the eye
reduces retinal image quality, they also have important implications for accommodation.
Ocular aberrations result in decreased retinal image quality and contribute to a larger depthof field of the eye due to its inability to detect small changes in image focus as an object
is moved closer or further from the optimal point of focus. Before the accommodative
mechanism was fully understood, Sturm (2) proposed that astigmatism could explain how
the eye could see at different distances. An optical system with astigmatism has two line
foci at orthogonal meridians separated by a distance called the interval of Sturm. No
perfect image focus is attained anywhere between the two line foci, so if an object is

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 48/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 49/338
33The Helmholtz Mechanism of Accommodation
zonular fibers at the lens equator pull and hold the lens in a flattened and unaccommodated
state. The zonular fibers extend from the ciliary processes to their insertion on the lens
capsule at the lens equatorial region. When the ciliary muscle contracts with an accom-
modative effort, it undergoes a forward redistribution of its center of mass (Fig. 3).
This moves the anterior-inward apex of the ciliary body toward the lens equator to
release the resting zonular tension. When the zonular tension is released, the elastic
lens capsule molds the lens to decrease equatorial diameter, increase thickness, and
allow the lens anterior and posterior surfaces to undergo an increase in curvature (Fig. 3).
H. TSCHERNING’S THEORY OF ACCOMMODATION
Tscherning (28) challenged the Helmholtz theory of accommodation, believing that with
accommodation there is an increase in traction of the zonular fibers at the lens equator
and that the curvatures of the central lens increase while those at the periphery flatten on
account of the greater resistance and steeper curvatures of the lens nucleus (Fig. 4). In
other words, with a traction of the zonular fibers, the softer cortex is molded aroundthe harder nucleus, so that the central lens surface curvatures more closely resemble
the steeper central curvatures of the lens nuclear surface. Tscherning also believed
that the vitreous provided a force on the lens posterior surface to aid in the accom-
modative mechanism. Tschering’s accommodative mechanism required no significant
modification of the anatomy of the accommodative apparatus as Helmholtz had de-
scribed it.
Figure 4 Tscherning (Ref. 28.) proposed an alternative mechanism of lenticular accommodation.
(A) The unaccommodated lens is shown as a solid line with the accommodated lens superimposed
as a dashed line. Tscherning believed that the accommodative change in the form of the lens occurred
as a consequence of an increase in traction of the zonular fibers at the lens equator. Thus, as depictedby Tscherning, the unaccommodated lens has a larger diameter, but the lens undergoes no change
in axial thickness. The anterior surface of the lens is to the left. (B) Tscherning believed this change
in form of the lens occurred as a consequence of the relatively softer cortex being molded around
the relatively hardened nucleus. He believed the surfaces of the nucleus to be more steeply curved
than the surfaces of the lens. With an increase in traction of the zonular fibers at the lens equator
the peripheral lens surfaces are flattened while at the middle of the lens the curvatures increase.
The cornea and anterior lens surface are on the left of the diagram. (From Ref. 28.)

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 50/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 51/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 52/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 53/338
37The Helmholtz Mechanism of Accommodation
Figure 6 Recent experiments on iridectomized rhesus monkeys using Edinger-Westphal stimu-
lated accommodation are in agreement with the Helmholtz accommodative mechanism (42). (A) A
gonioscopy lens placed on the temporal cornea allows visualization of the ciliary processes and lens
equator. (B) The movements of these structures can be observed during accommodation. (C) The
subtracted image pair shows that the eye remains relatively stable during accommodation, but thereis a pronounced movement of the ciliary processes and lens equator away from the sclera with
accommodation. (D) The ciliary muscle and lens equator can be observed with ultrasound biomicros-
copy (UBM). (E) The apex of the ciliary muscle and the lens equator move away from the sclera
during accommodation. (F) The subtracted image pair shows that while the eye is relatively stable,
the ciliary muscle and lens equator move away from the sclera during accommodation. (G) The
entire equatorial diameter of the lens can be seen when a Goldman lens is placed on the cornea.
(H) With accommodation, there is a concentric decrease in equatorial diameter of the crystalline
lens and an inward movement of the ciliary processes. (I) The subtracted image pair shows that the
eye remains relatively stable relative to the pronounced accommodative movements that are ob-
served. Each of the movements observed are in accordance with the Helmholtz accommodative
mechanism and opposite to those proposed by Schachar. The accommodative movements observed,
such as a concentric decrease in lens diameter (G–I), cannot be explained by eye movements. (From
Ref. 42.)

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 54/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 55/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 56/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 57/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 58/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 59/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 60/338
44 Glasser
R. DOES SCLERAL EXPANSION SURGERY RESTORE
ACCOMMODATION?
Regardless of the accommodative mechanism or the causes of presbyopia, it is theoreticallypossible that scleral expansion surgery may restore accommodation through some un-
known mechanism. However, the only published objective measurements of accommoda-
tion in patients with postoperative scleral expansion show that no accommodation is re-
stored (45). Subjective tests suggest that near reading distance may be temporarily
improved following scleral expansion (44). It is not clear why this would occur. The push-
up or near reading test that is typically used to assess accommodation postoperatively is
inappropriate to determine if accommodation occurs. The push-up test does not unequivo-
cally measure accommodation and is subject to errors due to depth of focus of the eye
and ocular aberrations. By definition, accommodation is a dioptric change in optical power
of the eye. If accommodation occurs, this can be measured with objective instrumentation
designed to measure the optical power of the eye. Unilateral scleral expansion surgery
reportedly improves near vision bilaterally. A physiological explanation for this is unlikely,
but it may reflect the inadequacy of subjective accommodation testing. It is possible, forexample, that scleral expansion surgery may inadvertently introduce corneal or lenticular
aberrations or some degree of multifocality to the eye. While this may prove beneficial
to provide some degree of functional near vision, it is clearly not accommodation. Schachar
has suggested that this is not the cause of the improved near vision, since keratometry is
unaltered by scleral expansion (24). However, this does not address the possibility of
aberrations in the lens. In addition to instrumentation available to measure accommodation
objectively, excellent wavefront technology exists to objectively measure the aberrations
of the eye. These measurements should be made pre- and postoperatively, in conjunction
with objective and appropriate measurements of accommodation to demonstrate if there
are any benefits to scleral expansion.
REFERENCES
1. von Helmholz H. Ueber die Accommodation des Auges. Arch Ophthalmol 1853; 1:1–74.
2. von Helmholz HH. Handbuch der Physiologishen Optik. In: Southall JPC, trans. Helmholtz’s
Treatise on Physiological Optics. New York: Dover, 1962:143–172.
3. Tamm ER, Lutjen-Drecoll E. Ciliary body. Micro Res Tech 1996; 33:390–439.
4. Brucke E. Ueber den Musculus Cramptonianus und den Spannmuskel der Choroidea. Arch
Anat, Physiol Wissenschaft Med 1846; 1:370.
5. Muller H. Uber einen ringformigen Muskel am Ciliarmuskel des Menschen und uber den
Mechanismus der Akkommodation. Graefes Arch Ophthalmol 1858; 3:1.
6. Rohen JW. Scanning electron microscopic studies of the zonular apparatus in human and
monkey eyes, Invest Ophthalmol Vis Sci 1979; 18:133–144.
7. Glasser A, Croft MA, Brumback L, Kaufman PL. Ultrasound biomicroscopy of the aging
rhesus monkey ciliary region. Optom Vis Sci 2001; 78(6):417–424.
8. Farnsworth PN, Burke P. Three-dimensional architecture of the suspensory apparatus of theaging lens of the rhesus monkey. Exp Eye Res 1977; 25:563–576.
9. Schachar RA. Zonular function: a new hypothesis with clinical implications. Arch Ophthalmol
1994; 26:36–38.
10. McCulloch C. The zonule of Zinn: its origin, course, and insertion, and its relation to neighbor-
ing structures. Trans Am Ophthalmol Soc 1954; 52:525–585.
11. Glasser A, Campbell MCW. Presbyopia and the optical changes in the human crystalline lens
with age. Vision Res 1998; 38:209–229.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 61/338
45The Helmholtz Mechanism of Accommodation
12. Paterson CA, Delamere NA. The Lens. In: WM Hart, ed. Adler’s Physiology of the Eye, 9th
ed. St. Louis: Mosby 1992:348–390.
13. Fincham EF. The mechanism of accommodation. Br J Ophthalmol Monogr VIII. 1937:7–80.
14. Scammon R, Hesdorffer M. Growth in mass and volume of the human lens in postnatal life.
Arch Ophthalmol 1937; 17:104–112.
15. Weale RA. The Lens. In: The Aging Eye. New York: Harper & Row, 1963:69–102.
16. Glasser A, Campbell MCW. Biometric, optical and physical changes in the isolated human
crystalline lens with age in relation to presbyopia. Vision Res 1999; 39:1991–2015.
17. Weekers R, Delmarcelle Y, Luyckx-Bacus J. Biometrics of the crystalline lens. In: J Bellows
J, ed. Cataract and Abnormalties of the Lens. Grune & Stratton, 1975:134–147.
18. Koretz JF, Cook CA, Kaufman PL. Accommodation and presbyopia in the human eye. Changes
in the anterior segment and crystalline lens with focus. Invest Ophthalmol Vis Sci 1997; 38:
569–578.
19. Dubbelman M, Van der Heijde GL, Weeber HA. The thickness of the aging human lens
obtained from corrected Scheimpflug images. Optom Vis Sci 2001; 78:411–416.
20. Dubbelman M, Van Der Heijde GL. The shape of the aging human lens: curvature, equivalent
refractive index and the lens paradox. Vision Res 2001; 41:1867–1877.21. Brown N. The change in lens curvature with age. Exp Eye Res 1974; 19:175–183.
22. Smith P. Diseases of the crystalline lens and capsule: on the growth of the crystalline lens.
Trans Ophthalmol Soc U K 1883; 3:79–102.
23. Rafferty NS. Lens morphology. In: Maisel H, ed. The Ocular Lens Structure, Function, and
Pathology. New York: Marcel Dekker, 1985:1–60.
24. Schachar RA. Cause and treatment of presbyopia with a method for increasing the amplitude
of accommodation. Ann Ophthalmol 1992; 24:445–452.
25. Schachar RA. Pathophysiology of accommodation and presbyopia: understanding the clinical
implications. J Fla Med Assoc 1994; 81:268–271.
26. Strenk SA, Semmlow JL, Strenk LM, Munoz P, Gronlund-Jacob J, DeMarco KJ. Age-related
changes in human ciliary muscle and lens: a magnetic resonance imaging study. Invest Ophthal-
mol Vis Sci 1999; 40:1162–1169.
27. Keeney AH, Hagman RE, Fratello CJ. Dictionary of Ophthalmic Optics. Boston: Butterworth-
Heinemann, 1995:4.28. Tscherning M. Physiologic Optics, 4th ed. Philadelphia: The Keystone Press, 1924:192–228.
29. Cramer A. Het accommodatievermogen der oogen, physiologisch toegelicht. Natuurkundige
Verhandelingen vande Hollandsche Maatschappij der Wetenschappen te Haarlem 1853; 1:
139-Haarlem: De Erven Loosjes.
30. Guthoff R, Ludwig K. The Accommodative ability of the eyes. In: Current Aspects of Human
Accommodation. Heidelberg: Kaden Verlag, 2001:171–200.
31. Graefe A. Fall von acquirirter Aniridie als Beitrag zur Accommodattionslehre. Arch Ophthal-
mol 1861; 7:150–161.
32. Young T. On the mechanism of the eye. Phil Trans R Soc Lond 1801; 91:23–88.
33. Schachar RA, Cudmore DP, Black TD. Experimental support for Schachar’s hypothesis of
accommodation. Arch Ophthalmol 1993; 25:404–409.
34. Samuelson D. A reevaluation of the comparative anatomy of the eutherian iridocorneal angle
and associated ciliary body musculature. Vet Comp Ophthalmol 1996; 6:153–172.
35. Koretz JF, Kaufman PL, Neider MW, Goeckner PA. Accommodation and presbyopia in the
human eye—aging of the anterior segment. Vision Res 1989; 29:1685–1692.
36. Beers APA, Van Der Heijde GL. In vivo determination of the biomechanical properties of the
component elements of the accommodative mechanism. Vision Res 1994; 34:2897–2905.
37. Schachar RA, Cudmore DP, Black TD, Wyant JC, Shuang VW, Huang T, Mckinney RT,
Rolland JP. Paradoxical optical power increases of a deformable lens by equatorial stretching.
Ann Ophthalmol 1998; 30:10–18.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 62/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 63/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 64/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 65/338
49Schachar’s Theory of Accommodation
apply to the lens equator decreases linearly with age, resulting in a linear decrease in the
amplitude of accommodation (i.e., presbyopia).
1. Schachar’s Supporting Data
Schachar first showed experimental support of his theory by progressively stretching the
sclerae and ciliary bodies of bovine eyes and then measuring the change in focal length
and equatorial diameter of the lens. All eyes showed a decrease in focal length and therefore
an increase in the optical power as well as an increase in equatorial diameter (3). Schachar
(4) has also constructed a physical model of the variable-focus lens using a gelatin-filled
balloon that can change optical power to 10 D, simulating an aspect of his theory of
accommodation. Profile photographs were taken of a gelatin-filled balloon relaxed and
stretched at the equator. He was able to prove, both with the photographs and mathemati-
cally, that with equatorial stretching, the central anterior lens becomes steeper, the periph-
eral anterior lens becomes flatter, and there is no change in the posterior radius of curvature.
Schachar (5) used a vertical scanning interference microscope to measure the mean radiusof curvature of both anterior and posterior surfaces of constant-volume, deformable, water-
filled lenses prior to and during stepwise equatorial stretching. Central steepening and
peripheral flattening of the lens was again demonstrated.
In another study, high-frequency, high-resolution anterior segment ultrasound biomi-
croscopy was used to measure in vivo changes occurring at the lens equator in 12 young
human subjects during pharmacologically controlled accommodation (6). The patients
ranged in age from 20 to 34 years with a mean age of 26 years and a standard deviation
of 5 years. The patients had a correctable visual acuity of 20/20 and accommodative mean
amplitude of 9.5 D. One drop of 1% tropicamide was placed in the right eye. The pupil
and the near point without correction were measured 25 min later using four-point print.
Ultrasound biomicroscopy (UBM) was performed using the Humphrey Instruments biomi-
croscope to image the lens equator in the unaccommodated state. A video recording was
made of the UBM images. Later, one drop of 2% pilocarpine was administered in theright eye, and 1 h later the pupil and the near point without correction were measured.
Ultrasound biomicroscopy was then performed, after which a video recording was made
of the UBM images. The induced accommodation was the difference between the near
point measurements after pilocarpine and tropicamide.
A frame-by-frame comparison was made between the two videos for each patient,
using a video mixer and computer subtraction techniques. Over 20,000 images of each of
the 12 subjects were compared. Separate and different images of the same patient in the
unaccommodated and the accommodated states were superimposed. The cornea and sclera
were used as positional references, which provided a reliable method to avoid errors that
accompany misalignment and rotation, since the cornea and sclera do not change position
during accommodation. In this study it was demonstrated that, during accommodation,
the lens equator moves toward the sclera. The mean displacement of the lens equator
toward the sclera was 6.8 1 m for each diopter of increase in accommodation (6). Thisconfirmed predictions of previous mathematical and physical models (4,7,8) and was
consistent with the increase in the optical power of the bovine lens with equatorially
stretching that occurred in Schachar’s previous study (3).
Schachar and his colleagues mathematically modeled the human crystalline lens to
approximate both the Schachar and the Helmholtz theories of accommodation (9). They
used nonlinear finite-element analysis that included the material properties and proper

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 66/338
50 Pepose and Chung
boundary conditions approximating the human crystalline lens. They used ANSYS 5.6, a
general-purpose, nonlinear, finite-element computer program to perform their analysis.
They calculated the amount of force necessary to produce a given amount of equatorial
displacement. The thick-lens formula was used to establish the optical power of the crystal-
line lens. Then the longitudinal spherical aberration of various levels of crystalline lens
accommodation was investigated using Zemax EE, an optical computer program.
The results of nonlinear finite-element analysis by Schachar et al. demonstrated that
only the tension produced solely by the equatorial zonules was able to produce the known
properties of the accommodative process, which include an increase in central optical
power, and also accounts for the physiological force limitations of the ciliary muscle.
They also demonstrated that the increase in equatorial diameter associated with the tension
produced by the equatorial zonules was consistent with the ultrasound biomicroscopy
measurements showing that the lens equator moves toward the sclera during pharmacologi-
cally controlled accommodation. The analysis demonstrated that when the anterior and
posterior zonules or all three sets of zonules totally relax, the central optical power of the
crystalline lens would decrease, not increase. These results contradict Helmholtz’s theoryof accommodation.
2. Clinical and Experimental Data Supporting Helmholtz’s Theory
Schachar’s hypothesis of accommodation has recently been challenged. Glasser and Camp-
bell (11,12) isolated human lenses from 27 human eyes aged 10 to 87 years. An in vitro
scanning laser technique was used to measure the focal length and spherical aberration
of the lenses as the lenses were exposed to increasing and decreasing radial stretching
forces through the ciliary body–zonular complex. They demonstrated that for the three
youngest lenses (11,31, and 39 year old), the focal length did change with stretch. On the
other hand, the older lenses, 54 and the 87 years old, demonstrated no change in focal
length over the extent of stretch applied. These results contradict Schachar’s hypothesis
of accommodation, which maintains that the lens remain malleable even with increasingage. In a different investigation by Glasser and Campbell (12,13), another group of 19
lenses 5 to 96 years of age were studied. In this group, which included older lenses with
signs of early cataract, the focal length increased up to approximately age 65, but then
their focal length decreased. Both studies demonstrated that over the years when accommo-
dation is gradually lost due to presbyopia, the focal length of the unstretched lenses gradu-
ally increased linearly, supporting a lens/capsule compliance and elasticity-based theory
of presbyopia.
Glasser and Kaufman (14) studied the accommodative mechanism in six cynomolgus
monkeys (10 to 13 year old) and eight rhesus monkeys (6 to 17 years old) with stimulated
accommodative amplitudes ranging from 7 and 18 D. The monkeys had complete bilateral
iridectomies. Stimulating electrodes surgically implanted in the Edinger-Westphal nucleus
were used to induce varying amplitudes of accommodation. Accommodation was also
induced and reversed in several other cynomolgus and rhesus monkeys. Carbachol chlorideiontophoresis, topical pilocarpine hydrochloride, and systemic pilocarpine hydrochloride
were the agents used to stimulate accommodation, and topical and systemic atropine sulfate
was used to reverse the accommodation.
Goniovideography of the iridectomized eyes was performed, demonstrating the tips
of the ciliary processes, the anterior zonular fibers, and the lens equator. Ultrasound biomi-
croscopy was also performed using the Humphrey Instruments biomicroscope. Gonioscopy

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 67/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 68/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 69/338
53Schachar’s Theory of Accommodation
operated in a darkened room, does not offer the usual accommodative stimulus but relies
purely on defocus. The instrument, which requires the subject to use a bite plate for
stability and alignment, generally takes practice to obtain reliable data, and it was unclear
if this level of training and reproducibility was achieved. Glasser and colleagues (12) have
speculated that the possible restoration of near vision via scleral expansion could function
via nonaccommodative mechanisms, such as inducing multifocality of the crystalline lens.
A number of patients in the phase I clinical trial of scleral expansion in the United States
are now undergoing wavefront analysis to provide an objective measurement and assess
mechanisms that may underlie improvement in near vision after this procedure.
B. CONCLUSION
There are few subjects in ophthalmology capable of generating as much lively debate as
that of accommodation and presbyopia. The processes of accommodation and disaccom-
modation are complex, to say the least, and involve changes in muscular, lenticular, and
extralenticular components. At some time, almost every one of these components has beenproposed as a factor in the development of presbyopia.
We have tried in this chapter to present a balanced view of Schachar’s versus Helm-
holtz’s theory of accommodation, along with experimental evidence and arguments that
have been espoused by proponents of both sides. In a number of key respects, the proposed
mechanisms are antithetical. The universal nature of presbyopia and the intense interest
in its reversal justifies further research in this area to elucidate its pathophysiology.
ACKNOWLEDGMENT
Supported by the Midwest Corneal Research Foundation, Inc.
REFERENCES
1. Koretz JF. Accommodation and Presbyopia. In: Albert DM, Jakobiec FA, eds. Principles and
Practice of Ophthalmology: Basic Sciences. Philadelphia: Saunders, 1994:270–282.
2. Schachar RA. Is Helmholtz’s theory of accommodation correct? Ann Ophthalmol 1999; 31(1):
10–17.
3. Schachar RA, Cudmore DP, Black TD. Experimental support for Schachar’s hypothesis of
accommodation. Ann Ophthalmol 1993; 25:404–409.
4. Schachar RA, Cudmore DP, Black TD. A revolutionary variable focus lens. Ann Ophthalmol
1996; 28:11–18.
5. Schachar RA, Cudmore DP, Black TD, Wyant JC, Shung VW, Huang T, Mckinney RT,
Rolland JP. Paradoxical optical power increase of a deformable lens by equatorial stretching.
Ann Ophthalmol 1998; 30(1):10–18.
6. Schachar RA, Tello C, Cudmore DP, Liebmann JM, Black TD, Ritch R. In vivo increase of the human lens equatorial diameter during accommodation. Am J Physiol (United States) 1996;
271(3 pt 2): R670–R676.
7. Schachar RA, Cudmore DP, Torti R, Black TD, Huang T. A physical model demonstrating
Schachar’s hypothesis of accommodation. Ann Ophthalmol 1994; 26:4–9.
8. Schachar RA, Huang T, Huang X. Mathematical proof of Schachar’s hypothesis of accommo-
dation. Ann Ophthalmol 1993; 25:59.
9. Schachar RA, Bax AJ. Mechanism of accommodation. Int Ophthalmol Clin 2001; 41(2):17–32.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 70/338
54 Pepose and Chung
10. Mathews S. Scleral expansion surgery does not restore accommodation in human presbyopia.
Ophthalmology 1999; 106:873– 877.
11. Glasser A, Campbell MCW. Presbyopia and the optical changes in the human crystalline lens
with age. Vis Res 1998; 38:209–229.12. Glasser A, Croft MA, Kaufman PL. Aging of the human crystalline lens and presbyopia. Int
Ophthalmol Clin 2001; 41(2):1–15.
13. Glasser A, Campbell MCW. Biometric, optical and physical changes in the isolated human
crystalline lens with age in relation to presbyopia. Vis Res 1999; 39:1991.
14. Glasser A, Kaufman PL. The mechanism of accommodation in primates. Opthalmology 1999;
106(5):863–872.
15. Schachar RA. Presbyopia: Cause and Treatment. In: Schachar RA, Roy FH eds. Presbyopia:
Cause and Treatment. The Hague, The Netherlands: Kugler, 2001:1–20.
16. Wilson RS. Does the lens diameter increase or decrease during accommodation? Human ac-
commodation studies: a new technique using infrared retro-illumination video photography
and pixel unit measurements. Trans Am Ophthalmol Soc 1997; 95:261–270.
17. Wilson RS, Merlin LM. Infrared video photographic analysis of human accommodation. Invest
Ophthalmol Vis Sci 1997; 38(suppl):S986.
18. Wilson RS, Merlin LM. Infrared video photographic analysis of the lens-zonular-ciliary spacein human accommodation. Invest Ophthalmol Vis Sci 1998; 39(suppl):S312.
19. Strenk SA, Semmlow JL, Strenk LM, Munoz P, Gronlund-Jacob J, DeMarco JK. Age-related
changes in human ciliary muscle and lens: a magneticresonance imaging study. Invest Ophthal-
mol Vis Sci 1999; 40(6):1162–1169.
20. Yang GS, Yee RW, Cross WD, Chuang AZ, Ruis RS. Scleral expansion: a new surgical
technique to correct presbyopia. Invest Ophthalmol Vis Sci 1997; 38(suppl):S497.
21. Smith P. Disease of the crystalline lens and capsule: on the growth of the crystalline lens.
Trans Ophthalmol Soc UK 1883; 3:79.
22. Schachar RA. Cause and treatment of presbyopia with a method for increasing the amplitude
of accommodation. Ann Ophthalmol 1992; 24:445–452.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 71/338
5
Aging and the Crystalline Lens
Review of Recent Literature (1998–2001)
LEO T. CHYLACK, JR.
Harvard Medical School and Brigham and Women’s Hospital,
Boston, Massachusetts, U.S.A.
This chapter on aging and the crystalline lens is based on a review of the literature between
1998 and 2001. Due to the limits on the length of this chapter and the numerous recent
publications in this field, I have not been able to cite many important earlier works. I
extend my apologies to the authors of these works.
Bron et al. (1) published an excellent general summary of the aging lens in 2000.
The avascular lens grows throughout life. Being enclosed by a capsule and lacking a
means of shedding cells, the lens is an excellent organ in which to study aging. There are
changes in lens size, shape, and mass throughout life that occur at different rates. The
sagittal diameter of the lens is approximately constant at 9.0 mm., but the anteroposterior
distance varies from 2.5 to 3.5 mm. These dimensions may increase in the mature/hyperma-
ture cataract. In spite of decreases with age in the radius of the anterior surface of the
lens and changes in the points of zonular insertion, the clear lens retains its ability to focus
an image clearly on the retina. Although the central epithelial cells divide rarely, they
survive throughout life. The germinative epithelial cells are actively dividing cells, and
the equatorial epithelial cells undergo terminal differentiation. As lens fibers form, they
lose their nuclei and other intracellular organelles; in the deeper cortex, fiber cells areessentially organelle-free. The slightly tortuous course of the long fiber cells as they arch
over the equator and meet near the opposite pole to form sutures has been illustrated in
elegant studies by Kuszak et al. (2–4). The complexity of these sutures increases with
age and may account for the increased light scattering in the zones of disjunction seen
biomicroscopically. Lens protein synthesis in the epithelium and superficial cortex contin-
ues throughout life, but these proteins undergo several posttranslational changes, among
55

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 72/338
56 Chylack
which are chemical and photochemical oxidation, glycation, and racemization. Antioxidant
defense mechanisms may ameliorate some of these posttranslational changes. Also, with
increasing age monomeric proteins associate in covalently bound aggregates to form high-
molecular-weight aggregates whose hydrodynamic radii approach in size the wavelengths
of visible light. As size increases, light scattering also increases to the point of lens opacifi-
cation and frank cataract. Changes with age in protein conformation and phospholipid
composition of fiber membranes increase nuclear rigidity and contribute to presbyopia.
This chapter considers many of these changes in more detail.
In the past 15 years, epidemiological research on age-related cataracts (ARCs) has
revealed risk factors that pertain to behavior (e.g., diet, smoking, lifestyle, drug use) and
suggested that ARC may be a preventable disease (5,6). This is most encouraging, for
each year increasing percentages of public and private health care budgets are used to
provide surgical care for ARC.
A. AGING AND CHANGES IN LENS SIZE AND SHAPE
Several authors (7–12) have documented the growth of the lens throughout life. Koretz
et al. analyzed (24) Scheimpflug photographs of the unaccommodated lens in 100 subjects
from 18 to 70 years of age to determine the regions that changed with time. With Scheimp-
flug optics the lens image is in focus from the anterior to posterior pole. The geometric
distortion of Scheimpflug images can be corrected (14), so that accuratemeasures of the
lens can be obtained. Koretz et al. measured the lens with Hough transforms and other
image analysis methods. The radii of the anterior and posterior surfaces of the whole lens
decrease, but the volume increases with increasing age. In contrast, neither the shape nor
the volume of the nucleus changes with age. The central clear zone and center of mass
of the nucleus move anteriorly with age. The correlation between lens shape and location
(relative to the cornea) is very high, confirming earlier results. Also, the anterior movement
of the lens with age increases the likelihood of phakic IOL–lenticular touch and complica-
tions.Another study (15) explored the relationship of accommodative convergence per
unit of accommodative response (AC/A ratio), refractive error, and age to determine if
the AC/A ratio was a risk factor for myopia. A high AC/A ratio was associated with—and
a risk factor for—rapid onset of myopia. A higher AC/A ratio, associated with a flatter
crystalline lens, increased the effort to accommodate, or “pseudocycloplegia.” Accommo-
dative deficits in myopia may be the functional consequence of myopic enlargement of
the eye. This enlargement was documented in a study (16) of changes in biometric measure-
ments and refractive errors over a 3-year period in eyes of university students. After 3
years, the mean change in refractive error (in OD) was 0.52 / 0.45D ( p Ͻ 0.05).
The mean lens thickness increased by 0.07 / 0.10 mm ( p Ͻ 0.05), and the mean
elongation of the vitreous chamber was 0.27 / 0.30 mm ( p Ͻ 0.05). Regardless of
the original refractive error, the change in refractive error over the 3-year period was
toward myopia. There were no statistically significant changes in the curvature of thecornea or depth of the anterior chamber. The authors concluded that the myopic shift was
due to an elongation of the vitreous chamber.
In a study of 1-year-old chickens (17), form deprivation vision such as is obtained
through translucent glass or eyelids that have been sutured closed, even in fully grown
birds, was associated with a myopic shift that was similar but not as large as that in
neonatal chicks. The decreases in retinal dopamine seen in neonatal chicks were also seen

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 73/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 74/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 75/338
59Aging and the Crystalline Lens
with age. The low ratio of GSH/P-SH and the relatively inactive GSH-redox cycle in the
nucleus make the nucleus more susceptible to oxidative stress than the cortex. That, indeed,
this is the case has been demonstrated in animal models with hyperbaric oxygen (32),
UVA irradiation (33,34), and the glutathione peroxidase knockout mouse (35–37). With
increased oxidative stress in nuclei of lenses in these animal models, there is an increase
in protein disulfides and light scattering. Also with reduced activity of the GSH-redox
cycle, there is damage to Na , K -ATPase (an enzyme involved with many of the active
transport mechanisms in LECs), to cytoskeletal proteins, and to membrane proteins in-
volved in regulating membrane permeability. An excellent review of these topics has
recently been published (38).
As oxidative stress increases and the size of the GSH pool decreases, some proteins
thiols (P-SH) are converted to protein-thiol mixed disulfides (29), either protein-S-S-
glutathione (PSSG) or protein-S-S-cysteine (PSSC). The formation of PSSG precedes the
formation of PSSP (29) and increases insolubilization of lens proteins. Lou et al. (29)
discovered that the early oxidative damage could be reversed if the oxidant was removed
in time. This reversal is mediated by the enzyme thiol transferase (TTase), recently foundin the lens. Lou et al. showed that recombinant TTase, although requiring GSH for activity,
was much more efficient in dethiolating lens proteins than GSH alone. TTase favored
PSSG over PSSC and gamma-crystallin-S-S-G over alpha-crystallin-S-S-G. TTase was
also remarkably resistant to oxidation. The TTase dethiolase activity reactivates enzymes
deactivated by S-thiolation. It is this ability to regulate and repair SH-dependent enzymes
that suggests that TTase plays an important role in ARC formation.
In a study (39) of ascorbate oxidation and advanced glycation in the lens, the major
advanced glycation end product (AGE), N (epsilon)-carboxymethyl-L-lysine (CML), was
found to have an EDTA-like (chelator) structure that might bind copper. Ascorbylation
led to increased CML formation, copper binding, and free radical formation in the lens.
These results suggested that there is a vicious cycle in the lens between AGE formation,
lipoxidation, metal binding, and oxidative damage. It is possible that chelators may play
a role in the therapy of ARC.In another interesting study of the possible value of antioxidants in the treatment of
ARC (40), it was shown that chronic administration of vitamin E, but not of sodium
ascorbate, restored the age-associated decrease in GSH content in rat lenses to levels
comparable to those in younger rats. The age-associated decrease in lenticular glutathione
peroxidase, glutathione reductase, and glucose-6-phosphate dehydrogenase was not re-
versed by chronic administration of either vitamin E or sodium ascorbate (40).
In addition to the age-associated change in lens proteins, there are age-associated
changes in lens lipids. The percentage of sphingolipid nearly doubles with age, and there
is also an increase in hydrocarbon chain saturation with age. These increases were much
greater in the deeper layers of the lens (41). These data support the idea that the degree
of lipid hydrocarbon order is determined by the amount of lipid saturation, and this, in
turn, is regulated by the content of saturated sphingolipid. Hyperbaric oxygen treatment
increases the lipid disorder in the nucleus and the levels of lipid hydroxyl, hydroperoxyl,and aldehydes. The transparency of the nucleus is also reduced as these lipid oxidation
products accumulate in the lens.
The Roche European-American Cataract Trial (REACT) (42,43), the first prospec-
tive, randomized, placebo-controlled clinical trial of oral vitamins E and C, and beta-
carotene suggested that antioxidant treatment might slow the progression of ARC. A small
but statistically significant deceleration of ARC was found after 3 years of treatment in

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 76/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 77/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 78/338
62 Chylack
40. Campisi A, Di Giacomo C, Russo A, Sorrenti V, Vanella G, Acquaviva R, Li Volti G, Vanella
A. Antioxidant systems in rat lens as a function of age: effect of chronic administration of
vitamin E and ascorbate. Aging (Milano) 1999; 11:39–43.
41. Borchman D, Giblin FJ, Leverenz VR, Reddy VN, Lin LR, Yappert MC, Tang D, Li L. Impactof aging and hyperbaric oxygen in vivo on guinea pig lens lipids and nuclear light scatter.
Invest Ophthalmol Vis Sci 2000; 41:3061–3073.
42. Chylack Jr LT, Wolfe JK, Friend J, Tung W, Singer DM, Brown NP, Hurst MA, Kopcke W,
Schalch W. Validation of methods for the assessment of cataract progression in the Roche
European-American Anticataract Trial (REACT). Ophthalm Epidemiol 1995; 2:59– 75.
43. Chylack Jr LT, Phelps-Brown N, Bron A, Hurst M, Kopcke W, Thien U, Schalch W, the
REACT Group. The Roche European American Cataract Trial (REACT): a randomized clinical
trial to investigate the efficacy of an oral antioxidant micronutrient mixture to slow progression
of age-related cataract. Ophthalm Epidemiol 2002; 9:49–80.
44. Hanssen E, Franc S, Garrone R. Fibrillin-rich microfibrils: structural modifications during
ageing in normal human zonule. J Submicrosc Cytol Pathol 1998; 30:365–369.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 79/338
6
Hyperopia
IVO JOHN DUALAN and PENNY A. ASBELL
Mount Sinai Medical Center, New York, New York, U.S.A.
A. CONTACT LENS VS REFRACTIVE SURGERY
1. History of Contact Lens
Why would anyone choose contact lenses over refractive surgery? Contact lenses have
been around for decades and are therefore true, tried, and tested. Surgical procedures, on
the other hand, are still considered innovative, and no long-term follow-up data are yet
available. Contact lenses were first described and used well over a century ago but came
into popular use after World War II, where the first hard contact lenses, made of polymeth-
ylmethacrylate (PMMA), were introduced. In the 1960s the advent of soft lens materials
made of hydroxy-ethyl methacrylate (HEMA) led to the widespread use of contact lenses
in the United States. In the 1970s rigid gas-permeable lenses were introduced, and in the
1980s astigmatic and presbyopic connecting lenses became available. Flexibility of lens
use increased with the introduction of extended-wear contact lenses in the 1980s and
disposable lenses that can be replaced weekly, monthly, and even daily. The last decade has
seen advances in contact lenses for correcting presbyopia, including bifocal and multifocal
contact lenses.
2. Market Information
Currently, it is estimated in the United States that over 30 million people use contactlenses. Some 80% are using soft lenses and approximately 20% are using rigid gas-permea-
ble lenses.
Contact lenses offer individuals a readily available method of correcting refractive
errors that can be personalized to their individual needs. Excellent visual acuity is routinely
attained with contact lenses; 100% likely see 20/40 or better and well over 95% achieve
20/20 or better, though visual “results” with contact lenses are rarely reported. Contact
63

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 80/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 81/338
65Hyperopia
1. Advantages of Soft Contact Lenses
Immediate comfort is clearly the advantage of these lenses. Soft contact lenses are generally
large in diameter and extend beyond the cornea and limbus and fit under the upper lidmargin. Though there is slight movement with each blink because of the size of the lens
and the flexibility of the material, little sensation is associated with soft contact lens use.
Adaptation to soft contact lenses is rapid and patients can begin enjoying quality vision
almost from the moment the lenses are placed.
Key advantages of soft contact lens use are
Adaptation
Comfort
High-quality visual acuity
Ability to use on an intermittent basis
Ease of fitting
Ease of contact lens care
Correction of a wide range of refractive errors
Soft contact lenses can usually be fitted in one visit, with a brief follow-up to ensure
that they continue to provide excellent comfort and vision. Few unscheduled visits are
required, and patients typically return every 6 to 12 months for a follow-up that includes
evaluation for other ocular diseases, such as glaucoma and to ensure the general ocular
health as well continued proper use of the contact lenses.
2. Disadvantages of Soft Contact Lenses
Unlike myopes, hyperopes may have difficulties with visualization of contact lenses during
handling, since these patients do not have any near point in focus. Deposits can develop
on the lenses, which can interfere with comfort and vision. Patients who may be exposed
to environmental hazards such as volatile chemicals and those who have poor or inadequate
tear film are presently not good candidates for the use of soft contact lenses.
3. Lens Selection
There are a variety of things to be considered in picking a soft contact lens for a particular
patient. Most soft lenses come in predetermined parameters from the manufacturer, though
some can be custom-ordered for a particular prescription, such as lenses for patients with
high astigmatism. Soft contact lenses vary in water content: low range (30 to 45% water),
medium content (40 to 58% water), and high content (60 to 80% water). The amount of
water is a factor in the oxygen permeability of the lens and also influences comfort and
ease of handling. Contact lens parameters include the base curve of the central optic zone
and the diameter of the lens. Typically, a trial lens will be placed to evaluate the fit and
determine the refractive correction needed to account for the reduced vertex distance and
residual astigmatism. Many manufacturers supply practitioners with trial lenses that canthen be dispensed on the initial visit. Replacement lenses can then be sent directly to the
patient’s home or work for added convenience.
Another key consideration in fitting a soft lens is the wear schedule. For patients
who might need intermittent correction, as for social events or sports, one-day disposable
lenses may very well be suitable. Other patients do well with daily-wear disposable lenses
that are replaced weekly or biweekly. Soft lenses can also be used on a flexible replacement

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 82/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 83/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 84/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 85/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 86/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 87/338
71Surgical Treatment Options
Figure 3 Importance of corneal diameter in hyperopic refractive surgery.
Also, hyperopic ablation generates a negative longitudinal spherical aberration with worse
vision quality, due to the fact that para-axial light rays will pass through the first curvatureflexus, which imparts a hyperopic shift (Figs 4 and 5).
However, it is important to remember that these problems are sometimes reduced
by the anatomical characteristics of hyperopic eyes. Generally speaking, the size of the
optical zone is less important for a hyperopic patient than for a myopic one. The hyperopic
eye features smaller axial length, anterior chamber, and corneal diameter. Given the same
ablation diameter, an eye with a shallow anterior chamber will enjoy a larger optical zone
than one with a deep chamber (Fig. 6), and will have a larger percentage of corneal surface
involved by the treatment. Moreover, the two transition zones mentioned above will lie
peripherally, positioned in a corneal area with lesser curvature and lesser influence on
refraction. In a hyperopic eye with a shallow anterior chamber, the treatment results will
be less influenced by pupil diameter: even an optical zone of small size may cover the
pupillary area sufficiently, since the treated corneal arc will be closer to the pupillary area
and thus able to cover the pupil halos during mydriasis (Fig. 6). What is really important
is that the optical zone be truly homogeneous.
Figure 4 Myopic ablation. With a wide ablation area, the optical zone is wide and uniform,
without aberrations induced on para-axial rays.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 88/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 89/338
73Surgical Treatment Options
the way the cornea changes from a flatter periphery to a more curved central
portion. Eccentricity values (e values) are positive when the cornea is prolate,
negative when it is oblate. Normal eccentricity values range between 0.5 and
0.6 (normally prolate cornea, curved in the center, flat in the periphery). A
hyperopic treatment increases the e value; Figures 7 through 11 show cases
with progressively higher e values, approaching a keratoconus-like situation.
Central keratoconus, featuring a high eccentricity, with e values of 1.5 or
more, amplifies the physiological situation of transition from a curved central
cornea to a flat periphery. On the contrary, a myopic treatment induces negative
eccentricity, inverting the normal morphology.
2. Longitudinal spherical aberration (LSA). LSA expresses the aberration induced
by corneal multifocality. It is a measure of spherical aberration; its increase
indicates a decrease in contrast sensitivity.
3. Root mean square (RMS). RMS is a measure of the irregularity of curvature,
expressing the amount of deviation from a regular corneal curvature.
4. Surface asymmetry index (SAI). SAI is a measure of corneal symmetry in thepupillary area. Its increase leads to an increase in coma.
In the past, it was generally thought that excessively high corneal curvature values
would lead to a keratoconus-like situation. From our studies, it appears that an important
factor for this complication is the corneal curvature gradient (eccentricity). Interestingly,
Figure 7 through 11 Eyes with progressively higher e values, approaching a keratoconus-like
situation.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 90/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 91/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 92/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 93/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 94/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 95/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 96/338
85Laser Thermokeratoplasty
3. Keratocyte response. Keratocyte injury occurs when stromal collagen is heated
to 79ЊC, which induces wound healing, including extracellular matrix remodel-
ing and keratocyte activation (27). These changes contribute to postoperative
regression of induced refractive effect.
4. Stability of corneal collagen. Normal replacement of treated collagen by newly
synthesized collagen may also contribute to regression of refractive effect. Colla-
gen turnover in the cornea is very slow, with a half-life of 10 years; the stability
of corneal collagen after LTK is unknown (28,29).
C. CONTACT AND NONCONTACT LTK
The Ho:YAG laser delivery system can be used with a contact probe (Summit Technology,
Waltham, MA, and Technomed, Baesweiler, Germany) or a noncontact device (Sunrise
Technologies, Fremont, CA) (22,30). The contact probe allows for sequential delivery of
laser pulses into premarked spots using a fiberoptic handpiece brought into direct contact
with the cornea. The spot size is variable and dependent on the diameter of the fiberoptic handpiece (Summit Technology, Waltham, MA, 0.7 mm; Technomed, Baesweiler,
Germany, 0.55 mm). Depending on the degree of hyperopia, rings of eight spots are applied
with a treatment zone of 6.5 and 9.0 mm, 7.0 and 9.0 mm, and 7.5 mm with the Summit
Ho:YAG LTK and 6, 7, or 8 mm with the Technomed Ho :YAG LTK.
The noncontact Ho:YAG laser device allows for simultaneous delivery of eight laser
pulses using a slit-lamp, with a fixed spot size of 0.60 mm. One, two or three radial or
staggered concentric octagonal rings are placed at 6-to 8-mm ring diameters. This technol-
ogy can be coupled with real-time wavefront measurements to minimize the unpredictabil-
ity of the surgery.
D. PATIENT SELECTION
The noncontact Ho:YAG laser (Hyperion, Sunrise Technologies, Freemont, CA) was ap-proved by the U.S. Food and Drug Administration (FDA) in June 2000 for the temporary
reduction of hyperopia in patients with the following indications:
1. Age Ն 40 years
2. Manifest refraction spherical equivalent of 0.75 to 2.5 diopters
3. Cylindrical correction Յ 0.75 diopters
4. Stable refraction 6 months prior to the procedure
LTK is contraindicated in patients:
1. During pregnancy or while nursing
2. With keratoconus
3. With clinically significant corneal dystrophy or scarring in the 6-or 7-mm central
zone4. With a history of herpetic keratitis
5. With an autoimmune disease, collagen vascular disease, clinically significant
atopic syndrome, insulin-dependent diabetes or an immunocompromised state
Patient evaluation includes visual assessment with both uncorrected and best-cor-
rected visual acuity with cycloplegic refraction. Intraocular pressure should be measured
to exclude narrow-angle glaucoma in hyperopic patients. A poor LTK effect is observed in
patients with high intraocular pressure (31). Corneal topography is performed to determine

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 97/338
86 Mian and Azar
presence of irregular astigmatism. Pachymetry is helpful, because thinner corneas have
greater effect with LTK. Systemic anti-inflammatory medications should be avoided 2
months preoperatively and 3 months postoperatively due to their contribution to regression
of refractive effect. Wavefront-guided LTK studies are underway, but have not been ap-
proved as of yet by the FDA.
E. SURGICAL PROCEDURE
1. Contact LTK
With the contact Ho:YAG laser (Summit Technology, Waltham, MA, and Technomed,
Baesweiler, Germany), energy is delivered through a quartz fiberoptic probe handpiece
and focused by a disposable tip at the corneal surface with a cone angle of 120 Њ (32).
Preoperatively, patients are given topical tetracaine anesthesia and the pupil is constricted
with 1% pilocarpine. The optical zone center is located using coaxial fixation and marked
over the center of the pupil. Probe placement is guided by using a specially designed
marker with radial and arcuate marks. The probe tip is applied perpendicular to the cornealsurface at the intersection of the radial and arcuate marks. The laser energy is set at 19
mJ per pulse for 25 pulses, pulse duration of 300 ms, with a repetition rate of 15 Hz. The
patients receive either 8 or 16 spots at variable optical zones. Loose epithelium is debrided
with a weck-cell sponge from the treatment areas after and the eye is patched after adminis-
tering antibiotic/steroid ointment. Postoperatively, patients receive tobramycin 0.3% /dexa-
methazone 0.1% ointment five times daily until re-epithelialization.
2. Noncontact LTK
The noncontact Ho:YAG laser (Hyperion, Sunrise Technologies, Fremont, CA) is a solid-
state, pulsed laser connected to a slit-lamp delivery system (Nikon) capable of projecting
eight uniform beams in an octagonal ring (33). Each beam has an individual shutter with
adjustable optical zone diameters, allowing for different treatment patterns. The laser
energy is set from 21 to 25 mJ per pulse for 5 to 10 pulses with a repetition rate of 5 Hzapplied over several seconds. Two HeNe laser beams are used for alignment, centration,
and coaxial focusing. Preoperatively, topical anesthetic drops (0.5% proparacaine solution)
are administered, starting 20 min before treatment, for a total of four drops. A lid speculum
is inserted to allow the eyelids to be held open for 3 min before laser application to dry
the tear film. This helps standardize the effects of epithelial swelling and corneal hydration
on delivery of laser energy to the corneal stroma. The patient is instructed to fixate on a
flickering red light during laser application. The ring diameter and number of rings applied
depends on the desired correction. Postoperatively, patients are given 0.3% tobramycin
and diclofenac sodium drops four times daily until the epithelium is healed. Patients may
also take acetaminophen or acetaminophen with codeine for pain management. In real-
time wavefront-guided LTK, the energy per pulse can be adjusted to improve the surgical
outcomes.
F. VISUAL OUTCOMES
1. Contact LTK
The safety of contact Ho:YAG LTK was initially established in 33 human cadaver and 4
blind human eyes (21). Sixteen coagulations on two concentric rings, with diameters of
6 and 9 mm, were applied. This resulted in central corneal steepening with a refractive

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 98/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 99/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 100/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 101/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 102/338
91Laser Thermokeratoplasty
tive uncorrected visual acuity. There was a mean increase of 4.60 1.20 D in central
keratometric power. Contact Ho:YAG LTK was also evaluated for correction of hyperopia
and astigmatism after PRK. Eggink et al. reported limited efficacy and predictability in
16 eyes treated with contact Ho:YAG LTK (55). However, there were no sight-threatening
complications. Goggin and Lavery reported treatment of 11 eyes with mean preoperative
spherical equivalent of 2.06 1.02 D and postoperatively to 0.511 0.55 D after
1-year follow-up. (56) a total of 91% were 20/40 or better and 82% were within 1.00
D of the target spherical equivalent.
4. LTK for LASIK-Induced Hyperopia
LASIK is a safe and effective technique for correction of moderate to high myopia. How-
ever, 2 to 8% of patients may have significant overcorrection (57). The efficacy and safety
of noncontact Ho:YAG LTK for correction of hyperopia after LASIK was evaluated in
13 eyes (58). After 18 months of follow-up, the mean cycloplegic refraction changed from
4.6 1.4 D ( 2.50 to 7.25 D) to 0.76 0.11 D. All of the patients were within
1.50 D of emmetropia, and no patient lost lines of best-corrected visual acuity.
G. COMPLICATIONS
Mild pain, tearing, photophobia, and foreign-body sensation have been reported 1 to 3 days
after surgery.(21,39,42,46,50) These complications were related to laser-induced epithelial
injury, which resolved within 3 days in most patients. Opacities in each treatment spot
decreased over time, becoming undetectable in most patients in room light; however, the
opacities were observed with slit-lamp biomicroscopy even after 2 years (42). Astigmatism
has been shown to be induced by Ho:YAG LTK, especially with the smaller treatment
diameters (32,42,50). No significant changes in endothelial cell density occurred up to 12
months postoperatively (33,44). There was no significant loss of contrast sensitivity and
no change in glare test measurements (33,46,50).
H. CONTINUOUS-WAVE DIODE LTK
Compared to pulsed Ho:YAG lasers, diode lasers provide continuous heat to the target
tissue with more uniform stromal heating. This potentially allows for higher and more
stable refractive correction. Wavelength settings of 1.854, 1.870, 1.885, and 2.1 m have
been studied (59–63). The shorter wavelengths achieve greater corneal depth, with a
wavelength of 1.854 m causing extensive local endothelial damage (0.8 to 1.2 mm in
diameter) (61,62). A wavelength of 1.885 m has a penetration depth of 380m, compara-
ble to the absorption of the Ho:YAG laser emitting at 2.07-m wavelength. Continuous-
wave diode LTK has been tested in eight blind human eyes (63). A wavelength of 1.854
or 1.870 m with 100 to 150 mW power was applied for 10 s. The radiation was focused
into the corneal stroma between 400 and 600 m or 1000 m with one or two eight-spotrings. The refractive change increased with higher laser power and smaller ring diameters.
Two rings provided higher and more stable refractive effect of up to 5.66 D. The
refractive effect stabilized between 3 and 6 months. Greater endothelial damage was noted
with a wavelength of 1.854 m.
Ho:YAG LTK offers an alternative treatment for the correction of hyperopia up to
2.50 D. There is an initial overcorrection followed by regression, dependent on age and

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 103/338
92 Mian and Azar
corneal thickness. Clinical studies have established the safety and efficacy of Ho:YAG
LTK up to 2 years after treatment. LTK may also be used to treat PRK and LASIK-
induced hyperopia. Diode lasers may help further improve stability of refractive effect
with LTK. Wavefront-guided LTK may further improve the predictability of this procedure
and allow for predictable outcomes even for retreatments of initial undercorrections.
REFERENCES
1. Lans LJ. Experimentelle Untersuchungen uber Entstehung von Astigmatismus durch nicht-
perforirende Corneawunden. Graefes Arch Ophthalmol 1898; 45:117–152.
2. Terrien F. Dystrophie marginale symmetrique des deux cornees avec astigmatisme regulier
consecutif et guerison par la cauterisation ignee. Arch Ophthalmol (Paris) 1900; 20:12–21.
3. Wray C. Case of 6 D of hypermetropic astigmatism cured by the cautery. Trans Ophthalmol
Soc UK 1914; 34:109–110.
4. Gassett AR, Shaw EL, Kaufman HE, Itoi M, Sakimoto T, Ishii Y. Thermokeratoplasty. Trans
Am Acad Ophthalmol Otolaryngol 1973; 77:OP–441–OP–454.
5. Shaw EL, Gassett AR. Thermokeratoplasty (TKP) temperature profile. Invest Ophthalmol Vis
Sci 1974; 13:181–186.
6. Keates RH, Dingle J. Thermokeratoplasty for keratoconus. Ophthalm Surg 1975; 6:89–92.
7. Fogle JA, Kenyon KR, Stark WJ. Damage to epithelial basement membrane by thermokera-
toplasty. Am J Ophthalmol 1977; 83:392–401.
8. Aquavella JV, Smith RS, Shaw EL. Alterations in corneal morphology following thermokera-
toplasty. Arch Ophthalmol 1976; 94:2082– 2085.
9. Arensten JJ, Rodrigues MM, Laibson PR. Histopathologic changes after thermokeratoplasty
for keratoconus. Invest Ophthalmol Vis Sci 1977; 16:32–38.
10. Itoi M. Computer phtokeratometry changes following thermokeratoplasty. In: Schachar RA,
LevyNS, Schachar L, eds. Refractive Modulation of the Cornea. Denison, TX: LAL Publishers,
1981:61–69.
11. Rowsey JJ, Doss JD. Preliminary report of Los Alamos Keratoplasty techniques. Ophthalmol-
ogy 1981; 88:755–760.12. Neumann AC, Fyodorov S, Sanders DR. Radial thermokeratoplasty for the correction of hyper-
opia. J Refract Corneal Surg 1990; 6:404–412.
13. Neumann AC, Sanders D, Raanan M, DeLuca M. Hyperopic thermokeratoplasty: clinical
evaluation. J Cataract Refract Surg 1991; 17:830–838.
14. Neumann AC. Thermokeratoplasty for hyperopia. Ophthalmol Clin North Am 1992; 5:
753–772.
15. Feldman ST, Ellis W, Frucht-Perry J, Chayet A, Brown SI. Regression of effect following
radial thermokeratoplasty in humans. J Refract Corneal Surg 1989; 5:288–291.
16. Beckman H, Fuller TA, Boyman R, Mandell G, Nathan LE Jr. Carbon dioxide laser surgery
of the eye and adnexa. Ophthalmology 1980; 87:990–1000.
17. Peyman GA, Larson B, Raichand M, Andrews AH. Modification of rabbit corneal curvature
with use of carbon dioxide laser burns. Ophthalm Surg 1980; 11:325–329.
18. Kanoda AN, Sorokin AS. Laser correction of hypermetropic refraction. In: Fyodorov SN, ed.
Microsurgery of the Eye: Main Aspects. Moscow: MIR Publishers, 1987:147–154.19. Horn G, Spears KG, Lopez O, Lewicky A, Yang XY, Riaz M, Wang R, Silva D, Serafin J.
New refractive method for laser thermal keratoplasty with the Co:MgF2 laser. J Cataract Refract
Surg 1990; 16:611–616.
20. Koch DD, Padrick TD, Menefee RL. Laser phtothermal keratoplasty: nonhuman primate re-
sults. Invest Ophthalmol Vis Sci 1992; 33(suppl):768.
21. Seiler T, Matallana M, Bende T. Laser themokeratoplasty by means of a pulsed holmium:YAG
laser for hyperopic correction. J Refract Corneal Surg 1990; 6:335–339.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 104/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 105/338
94 Mian and Azar
45. Koch DD, Kohnen T, Anderson JA, Binder PS, Moore MN, Menefee RF, AAS, Valderamma
GL, Berry MJ. Histologic changes and wound healing response following 10-pulse noncontact
holmium:YAG laser thermal keratoplasty. J Refract Surg 1996; 12:623–634.
46. Kohnen T, Villarreal V, R, MenefeeR, Berry M, Koch DD.Hyperopia correction by noncontactholmium:YAG laser thermal keratoplasty: five-pulse treatments with 1 year follow-up. Graefes
Arch Clin Exp Ophthalmol 1997; 235:702–708.
47. Alio JL, Ismail MM, Sanchez Pego JL. Correction of hyperopia with non-contact Ho:YAG
laser thermal keratoplasty. J Refract Surg 1997; 13(1):17–22.
48. Gezer A. The role of patient’s age in regression of holmium:YAG thermokeratoplasty-induced
correction of hyperopia. Eur J Ophthalmol 1997; 7(2):139–143.
49. Nano HD, Muzzin S. Noncontact holmium:YAG laser thermal keratoplasty for hyperopia. J
Cataract Refract Surg 1998; 24:751–757.
50. Aker AB, Brown DC. Hyperion laser thermokeratoplasty for hyperopia. Int Ophthalmol Clin
2000; 40(3):165–181.
51. Portellinha W, Nakano K, Oliveira M, Simoceli R. Laser in situ keratomileusis for hyperopia
after thermal keratoplasty. J Refract Surg 1999; 15(2 suppl):S218–S220.
52. Attia W, Perez-Santonja JJ, Alio JL. Laser in situ keratomileusis for recurrent hyperopia
following laser thermal keratoplasty. J Refract Surg 2000; 16:163–169.53. Pop M. Laser thermal keratoplasty for the treatment of photorefractive keratectomy overcorrec-
tions: a 1-year follow-up. Ophthalmology 1998; 105(5):926–931.
54. Alio JL, Ismail MM, Artola A, Perez-Santonja JJ. Correction of hyperopia induced by photore-
fractive keratectomy using non-contact Ho:YAG laser thermal keratoplasty. J Refract Surg
1997; 13:13–16.
55. Eggink CA, Meurs P, Bardak Y, Deutman AF. Holmium laser thermal keratoplasty for hyper-
opia and astigmatism after photorefractive keratectomy. J Refract Surg 2000; 16:317–322.
56. Goggin M, Lavery F. Holmium laser thermokeratoplasty for the reversal of hyperopia after
myopic photorefractive keratectomy. Br J Ophthalmol 1997; 81:541–543.
57. Perez-Santonja JJ, Bellot J, Claramonte P, Ismail MM, Alio JL. Laser-in-situ keratomileusis
to correct high myopia. J Cataract Refract Surg 1997; 23:372–385.
58. Ismail MM, Alio JL, Perez-Santonja JJ. Noncontact thermokeratoplasty to correct hyperopia
induced by laser-in-situ keratomileusis. J Cataract Refract Surg 1998; 24:1191–1194.
59. Bende T, Jean B, Oltrup T. Laser thermal keratoplasty using a continuous wave diode laser.
J Refract Surg 1999; 15:154–158.
60. Brinkmann R, Koop N, Geerling G, Kampmeier J, Borcherding S, Kamm K, Birngruber R.
Diode laser thermokeratoplasty: application strategy and dosimetry. J Cataract Refract Surg
1998; 24(9):1195–1207.
61. Koop N, Wirbelauer C, Tungler A, Geerling G, Bastian GO, Brinkmann R. Thermal damage
to the corneal endothelium in diode laser thermokeratoplasty. Ophthalmologe 1999; 96(6):
392–397.
62. Wirbelauer C, Koop N, Tungler A, Geerling G, Birngruber R, Laqua H, Brinkmann R. Corneal
endothelial cell damage after experimental diode laser thermal keratoplasty. J Refract Surg
2000; 16:323–329.
63. Geerling G, Koop N, Brinkmann R, Tungler A, Cand med.m, Wirbelauer C, Birngruber R,
Laqua H. Continuous-wave diode laser thermokeratoplasty: first clinical experience in blind
human eyes. J Cataract Refract Surg 1999; 25:32–40.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 106/338
9
Conductive Keratoplasty for theCorrection of Low to Moderate
Hyperopia
MARGUERITE B. McDONALD
Louisiana State University Health Sciences Center, New Orleans, Louisiana, U.S.A.
JONATHAN DAVIDORF
Davidorf Eye Group, West Hills, and Maloney Vision Institute, Los Angeles,
California, U.S.A.
ROBERT K. MALONEY
Maloney Vision Institute, Los Angeles, California, U.S.A.
EDWARD E. MANCHE
Stanford University School of Medicine, Palo Alto, California, U.S.A.
PETER HERSH
Cornea and Laser Vision Center, Teaneck, New Jersey, U.S.A.
GEORGE M. SALIB
Tulane University School of Medicine, New Orleans, Louisiana, U.S.A.
A. HYPEROPIA CORRECTION BY CONDUCTIVE KERATOPLASTY
1. Thermokeratoplasty Procedures
Surgical correction of hyperopia has been a greater challenge to ophthalmology than the
correction of myopia. Attempts to steepen the central cornea by non-ablative methods,
such as thermal keratoplasty, date back to the rabbit studies by Lans in the nineteenth
century. During the 1980s, hot-wire thermokeratoplasty, a technique developed in the
95

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 107/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 108/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 109/338
98 McDonald et al.
discontinued for at least 3 weeks and soft lenses for at least 2 weeks prior to the preoperative
evaluation. Wearers of hard contact lenses should have two central keratometry readings
and two manifest refractions taken at least 1 week apart. The manifest refraction measure-
ments must not differ from the earlier measurements by more than 0.50 D in either merid-
ian. Keratometry mires must be regular.
b. Unsuitable Patients
Patients with a peripheral pachymetry reading at the 6-mm optical zone of less than 560
m are not suitable for treatment with the Viewpoint CK System. Also unsuitable are
those who have had strabismus surgery; have anterior segment pathology; have residual,
recurrent, active ocular or uncontrolled eyelid disease or any corneal abnormality; or have
signs of progressive or unstable hyperopia. Other relative contraindications are a history
of herpes zoster keratitis, herpes simplex keratitis, glaucoma, a history of steroid-respon-
sive rise in intraocular pressure (IOP), a preoperative IOP Ͼ21 mmHg, or narrow angles.
Patients with diabetes, diagnosed autoimmune disease, connective tissue disease, an immu-
nocompromised state, current treatment with chronic systemic corticosteroid or other im-munosuppressive therapy that may affect wound healing; a history of keloid formation;
intractable keratoconjunctivitis sicca; or pregnancy are also contraindicated to receive the
CK treatment.
3. Examinations
Preoperative examinations should include a manifest and cycloplegic refraction, an uncor-
rected and best spectacle-corrected visual acuity (distance and near), a slit-lamp and fun-
doscopic examination, applanation tonometry, central keratometry, ultrasonic pachymetry,
and computed corneal topography.
4. Performing the CK Procedure
Correct the patient’s full cycloplegic spectacle refraction. Administer one drop of topicalanesthetic three times at 5-min intervals and monitor the patient for degree of anesthesia.
Do not use pilocarpine. Insert the CK lid speculum to provide corneal exposure and act
as an electrical return path. Do not use a lid drape, for it may prevent direct contact of
the lid speculum and eyelid, which would disrupt the electrical current return path. Tape
the fellow eye closed. Position the operating microscope or slit-lamp biomicroscope over
or in front of the eye to be treated.
Mark the cornea with the CK marker, and remind the patient to fixate on the light
from the microscope. Dampen the CK marker with gentian violet or rose bengal stain.
Center the marker’s cross hairs over the center of the pupil and apply light pressure on
the marker to make a circular mark with eight intersections on the cornea. If using gentian
violet, irrigate with balanced salt solution to remove excess ink. Dry the surface of the
cornea thoroughly with a fiber-free sponge to avoid dissipation of applied energy by a
wet surface.Set the appropriate treatment parameters on the console according to the nomogram
(Table 1). The default setting for treatment is 350 kHz, 60% power (0.6 W) for 0.6 s.
Inspect the Keratoplast tip under the microscope to ensure it is not damaged or bent prior
to application. When treating 0.75 to 0.875 D of hyperopia (eight spots), treat only at the
7-mm optical zone, beginning treatment at the 12 o’clock position and continuing in the
sequence shown in Figure 3. When treating higher levels of hyperopia, follow the nomo-

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 110/338
99Conductive Keratoplasty
Table 1 Conductive Keratoplasty Nomogram
Diopters to be Number of
corrected CK treatment spots
ϩ0.75 D to ϩ0.875 D 8
ϩ1.00 D to ϩ1.625 D 16
ϩ1.75 D to ϩ2.25 D 24
ϩ2.375 D to ϩ3.00 D 32
CK—Conductive Keratoplasty
gram and application sequence. For example, for treating 1.00 to 1.625 D of hyperopia,
apply a total of 16 spots: 8 spots at the 6-mm optical zone and 8 at the 7-mm optical
zone. Begin application at each of these optical zones at the 12 o’clock position and
continue in sequence until the full circle of spots has been completed. For treating 1.75
to 2.25 D, apply treatment at the 6-, 7-, and 8-mm optical zones for a total of 24 spots.
For treating 2.375 D to 3.00 D, apply treatment to the 6-, 7-, and 8-mm optical zones and
then to each of the eight sectors between the previously treated spots at the 7-mm optical
zone for a total of 32 spots.
To treat each spot, place the tip of the delivery probe at the treatment mark on the
cornea, perpendicular to the corneal surface. Apply light pressure until the tip penetrates
the cornea down to the insulator stop. Depress the foot pedal to apply the radio frequency
energy. A tone will sound as the energy is applied. At each treatment spot, keep the tip
in place until the preprogrammed treatment time has been completed (the tone stops).
Clean the tip with a fiber-free sponge after each treatment spot to remove any tissue debris,
Figure 3 Number, location, and sequence of treatment spots. (Courtesy of Refractec, Inc., Irvine,
CA.)

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 111/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 112/338
101Conductive Keratoplasty
Figure 4 Postoperative UCVA over time.
2. Results
a. Efficacy
Twelve months postoperatively, UCVA was 20/20 or better in 53/96 (55%), 20/25 or
better in 73/96 (76%), and 20/40 or better in 87/96 (91%) of the eyes (Fig. 4). Near UCVA
increased an average of six Jaeger lines. Mean MRSE values showed 53/96 (55%) within
0.50 D of intended correction, 87/96 (91%) within 1.00 D, and 94/96 (98%) within
2.00 D (Fig. 5). A summary of the efficacy results with conductive keratoplasty is
shown in Table 3.
Table 3 Summary of Efficacy Results with Conductive Keratoplasty Compared with FDA
Guidelines for Refractive Procedures
FDA 6 Months 9 Months 12 Months
guideline (Nϭ348) (Nϭ276) (Nϭ96)
UCVA Ն 20/20 50% 46% 48% 55%
UCVA Ն 20/25 Not stipulated 65% 72% 76%
UCVA Ն 20/40 85% 90% 92% 91%MRSE Ϯ 0.50 D 50% 60% 66% 55%
MRSE Ϯ 1.00 D 75% 88% 88% 91%
MRSEϮ 2.00 D Not stipulated 99% 99% 98%
FDAϭ Food and Drug Administration
UCVA ϭ Uncorrected Visual Acuity
MRSE ϭManifest Refractive Spherical Equivalent

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 113/338
102 McDonald et al.
Figure 5 Accuracy of achieved MRSE.
b. Corneal Topography
Corneal topography of a typical eye with an MRSE of 3.25 D and UCVA of 20/125
preoperatively shows central steepening postoperatively surrounded by a midperipheral
flattening (Fig. 6). Twelve months postoperatively, this eye had an MRSE of 0.25 D
and UCVA of 20/20.
Figure 6 Conductive keratoplasty case study. Corneal topography of a typical eye with an MRSE
of 3.25 preoperatively D and UCVA of 20/125 preoperatively shows post-CK central steepening
surrounded by a midperipheral flattening. Twelve months postoperatively, this eye had an MRSE
of 0.25 D and UCVA of 20/20.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 114/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 115/338
104 McDonald et al.
Figure 8 Slit-lamp view of treatment spot 1 h after CK showing bands of striae between spots.
The surface leukomas are small because all of the energy is delivered within the stroma. (Courtesy
of Refractec, Inc., Irvine, CA.)
d. Slit Lamp
One hour after treatment, the opacities at each treatment spot were visible by slit lamp as
small surface leukomas, with a band of striae connecting the treatment spots (Fig. 8).
These leukomas are small because CK delivers energy deep into the stroma rather than
on the surface. The striae between treatment zones remain visible at 3, 6, and 12 months,
as reported by the United States CK clinical trial investigators, and suggest that the effect
of treatment on the stroma is long-lasting.
e. Safety
No eye had lost two or more lines of BSCVA and no eye had BSCVA worse than 20/40
at 12 months (Table 5). A total of 1/127 (1%) of eyes had an increase of Ͼ2.00 D of
Table 5 Summary of Safety Results with Conductive Keratoplasty
Postoperative visit
1 Month 3 Months 6 Months 9 Months 12 Months
(Nϭ390) (Nϭ390) (Nϭ384) (Nϭ218) (Nϭ79)
2 Lines loss of BSCVA 6% 5% 4% 2% 0%
Ͼ2 Lines loss of BSCVA 2% 1% 1% Ͻ1% 0%BSCVA Worse than 20/40 0% 0% 0% 0% 0%
Increase 2.00 D Cylinder 3% 2% 1% 0% 0%
IncreaseϾ 2.00 D Cylinder 3% 2% 1% Ͻ1% 1%
BSCVAϽ20/25 if better 4% 2% 1% 1% 0%
than 20/20 Pre-op
BSCVA—Best Spectacle-Corrected Visual Acuity

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 116/338
105Conductive Keratoplasty
cylinder at 12 months and 0/127 had an increase of 2.00 D. Seventy five percent had no
change (within 0.50 D) in cylinder. No eye with BSCVA of 20/20 or better preopera-
tively was worse than 20/25 postoperatively. No intraoperative complications or adverse
events occurred during the surgeries, and there were no treatment-related adverse events.
D. CONCLUSION
The 12-month results in the ongoing 2-year prospective clinical study of the CK technique
for correcting low to moderate spherical hyperopia are encouraging. Postoperative visual
acuity and predictability of refraction were excellent and are comparable to or better than
results obtained with PRK or LASIK for low hyperopia (17–34). The CK refractive effect
appears to stabilize by 6 months, surpassing the early studies of refractive stability results
seen following the noncontact LTK method (11–16). However, recent LTK postmarketing
approval data from phase 3 FDA clinical trials shows that LTK is stable after 3 months.
Availability of the 2-year results will confirm the efficacy, predictability, and safety
of results seen with CK at 1 year and provide validation of this nonlaser option for thetreatment of low to moderate hyperopia.
REFERENCES
1. Fogle JA, Kenyon KR, Stark WJ. Damage to the epithelial basement membrane by thermokera-
toplasty. Am J Ophthalmol 1977; 83:392–401.
2. Neumann A, Sanders D, Raanan M, DeLuca M. Hyperopic thermokeratoplasty: clinical evalua-
tion. J Cataract Refract Surg 1991; 17:830–838.
3. Feldman S, Ellis W, Frucht-Pery J, Chayet A, Brown S. Regression of effect following radial
thermokeratoplasty in humans. J Refract Surg 1995; 18:288–291.
4. CharpentierD, Nguyen-Khoa J, Duplessix M, Colin J, Denis P. Intrastromal thermokeratoplasty
for correction of spherical hyperopia: a 1-year prospective study. J Fr Ophthalmol 1995; 18:
200–206.5. McDonnell PJ. Radial thermokeratoplasty for hyperopia: I. The need for prompt investigation.
Refract Corneal Surg 1989; 5:50–52.
6. Durrie DS, Schumer JD, Cavanaugh TB. Holmium:YAG laser thermokeratoplasty for hyper-
opia. J Refract Corneal Surg 1994; 10:S277–S280.
7. Eggink CA, Bardak Y, Cuypers MHM, Deutman AF. Treatment of hyperopia with contact
Ho:YAG laser thermal keratoplasty. J Refract Surg 1999; 15:16–22.
8. Eggink CA, Meurs P, Bardak Y, Deutman AF. Holmium laser thermal keratoplasty for hyper-
opia and astigmatism after photorefractive keratectomy. J Refract Surg 2000; 16:317–322.
9. Koch DD, Kohnen T, McDonnell PJ, Menefee RF, Berry MJ. Hyperopia correction by non-
contact holmium:YAG laser thermokeratoplasty; United States phase IIA clinical study with
a 1-year follow-up. Ophthalmology 1996; 103:1525–1536.
10. Koch DD, Kohnen T, Anderson JA, Binder PS, Moore MN, Menefee RF, Valderamma GL,
Berry MJ. Histologic changes and wound healing response following 10-pulse noncontact
holium: YAG laser thermal keratoplasty. J Refract Surg 1996; 12:623–634.11. Koch DD, Abarca A, Villarreal R, Menefee R, Kohnen T, Vassiliadis A, Berry M. Hyperopia
correction by non-contact holmium: YAG laser thermokeratoplasty: clinical study with two-
year follow-up. Ophthalmology 1996; 103:731–740.
12. Koch D, Kohnen T, McDonnell P, Menefee R, Berry M. Hyperopia correction by noncontact
holmium: YAG laser thermal keratoplasty. Ophthalmology 1997; 104:1938–1947.
13. Nano HD, Muzzin S. Noncontact holmium:YAG laser thermal keratoplasty for hyperopia. J
Cataract Refract Surg 1998; 24:751–757.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 117/338
106 McDonald et al.
14. Koch DD, Kohnen T, McDonnell PJ, Menefee R, Berry M. Hyperopia correction by noncontact
holmium:YAG laser thermal keratoplasty: United States phase IIA clinical study with a 2-
year follow-up. Ophthalmology 1997; 104:1938–1947.
15. Alio JL, Ismail MM, Sanchez Pego JL. Correction of hyperopia with non-contact Ho:YAGlaser thermal keratoplasty. J Refract Surg 1997; 13:17–22.
16. Alio JL, Ismail MM, Artola A, Perez-Santonja JJ. Correction of hyperopia induced by photore-
fractive keratectomy using non-contact Ho:YAG laser thermal keratoplasty. J Refract Surg
1997; 13:13–16.
17. Pop M. Laser thermal keratoplasty for the treatment of photorefractive keratectomy overcorrec-
tions: A 1-year follow-up. Ophthalmology 1998; 105:926–931.
18. Ismail MM, Alio JL, Perez-Santonja JJ. Noncontact thermokeratoplasty to correct hyperopia
induced by laser in situ keratomileusis. J Cataract Refract Surg 1998; 24:1191–1194.
19. Bende T, Jean B, Oltrup T. Laser thermal keratoplasty using a continuous wave diode laser.
J Refract Surg 1999; 15:154–158.
20. Geerling G, Koop N, Brinkmann R, Tungler A, Wirbelauer C, Birngruber R, Laqua H. Continu-
ous-wave diode laser thermokeratoplasty in blind human eyes. J Refract Surg 1999; 25:32–40.
21. Mendez A, Mendez Noble A. Conductive keratoplasty for the correction of hyperopia. In:
Sher NA, ed. Surgery for Hyperopia and Presbyopia. Williams & Wilkins; 1997:163–171.22. Jackson WB, Mintsioulis G, Agapitos PJ, Casson EJ. Excimer laser photorefractive keratec-
tomy for low hyperopia: safety and efficacy. J Cataract Refract Surg 1997; 23:480–487.
23. Daya SM, Tappouni FR, Habib NE. Photorefractive keratectomy for hyperopia. Six month
results in 45 eyes. Ophthalmology 1997; 104:1952–1958.
24. Vinciguerra P, Epstein D, Radice P, Azzolini M. Long-term results of photorefractive keratec-
tomy for hyperopia and hyperopic astigmatism. J Refract Surg 1998; 14:S183-S185.
25. Pietila J, Makinen P, Pajari S, Uusitalo H. Excimer laser photorefractive keratectomy for
hyperopia. J Refract Surg 1997; 13:504–510.
26. O’Brart DP, Stephenson CG, Oliver K, Marshall J. Excimer laser photorefractive keratectomy
for the correction of hyperopia using an erodible mask and axicon system. Ophthalmology
1997; 104:1959–1970.
27. Dausch D, Klein R, Schroder E. Excimer laser photorefractive keratectomy for hyperopia. J
Refract Surg 1993; 9:20–28.
28. Davidorf DM, Eghbali F, Onclinx T, Maloney RF. Effect of varying the optical zone diameter
on the results of hyperopic laser in situ keratomileusis. Ophthalmology 2001; 108:1266–1268.
29. Argento CJ, Cosentino MJ. Laser in situ keratomileusis for hyperopia. J Cataract Refract Surg
1998; 24:1050–1058.
30. Ditzen K, Huschka H, Pieger S. Laser in situ keratomileusis for hyperopia. J Cataract Refract
Surg 1998; 24:42–47.
31. Esquenazi S, Mendoza A. Two-year follow-up of laser in situ keratomileusis for hyperopia.
J Refract Surg 1999; 15:648–652.
32. Goker S, Er H, Kahvecioglu C. Laser in situ keratomileusis to correct hyperopia from 4.25
to 8.0 D. J Refract Surg 1998; 14:26–30.
33. Rashad KM. Laser in situ keratomileusis for the correction of hyperopia from 1.25 to 5.00
diopters with the Keracor 117C laser. J Refract Surg 2001; 17:123–128.
34. Tabbara KF, El-Sheikh HF, Islam SM. Laser in situ keratomileusis for the correction of hyper-
opia from 0.50 to 11.50 diopters with the Technolas Keracor 117C laser. J Refract Surg
2001; 17:113–122.
35. Goth P, Stern R. Conductive Keratoplasty, Principles and Technology, presented at the Ameri-
can Society for Cataract and Refractive Surgery, Boston, April, 2000.
36. Data on File, Refractec, Inc.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 118/338
10
Intracorneal Segments for Hyperopia
LAURA GOMEZ and ARTURO S. CHAYET
Codet Aris Vision Institute, Tijuana, B.C., Mexico
A. BACKGROUND
The intracorneal segments (ICS) for hyperopia reshape the anterior surface of the cornea
without permanently changing the structure or function of the natural eye and are intended
to be an alternative to eyeglasses, contact lenses, or irreversible refractive surgery proce-
dures for hyperopic patients. The radially placed segments create a flattening of the periph-
eral cornea by shortening the chord length tangential to the limbus. This peripheral flatten-ing causes the central cornea to steepen and the corneal radius to decrease, thus correcting
for hyperopia (Fig. 1). Implantation of the segments does not involve the central cornea
and no tissue is removed. In addition, the cornea maintains its asphericity and normal
prolate shape when the segments are implanted—an advantage also reported for the intra-
stromal corneal ring segments for myopia (Intacs) (1,2).
The ICS for hyperopia are designed to be permanent; however, they can be removed
if desired. The ICS were conceptualized and developed by Steven M.Verity and David
Schanzlin. They initiated these studies in cadaver eyes using wires as the implantable
intracorneal devices.
The ICS for hyperopia were manufactured by Kera Vision, a vision correction com-
pany, founded in 1986 with the purpose of giving people clear vision without using correc-
tive lenses or undergoing surgeries that cut or remove tissue from the central optical zone
of the cornea. The company filed for bankruptcy in 2001, and these segments are currentlynot produced. However, the segments have been licensed to another entity, which may
produce them in the future.
The ICS are inserted radially between the layers of the corneal stroma through six
or eight small incisions made in the periphery of the cornea. When surgically placed at
approximately two-thirds depth into the corneal stroma, these segments reshape the anterior
corneal curvature, steepening the central cornea and thereby correcting for hyperopia (Fig.
107

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 119/338
108 Gomez and Chayet
Figure 1 Diagram showing how the intrecorneal segments (ICS) work. The six radially placed
segments create a flattening of the peripheral cornea by shortening the chord length between each
segment in the direction of the arrows. This peripheral flattening causes the central cornea to steepen,
correcting for hyperopia
2). The degree of corneal steepening achieved using the ICS is directly related to the
thickness of the ICS product implanted.
The segments are made of polymethylmethacrylate (PMMA) and vary in length
from 1.5 to 2.0 mm. Each segment has a hexagonal cross section and is tapered along the
internal side to facilitate implantation. The ICS thicknesses that we tested were 0.35, 0.40,and 0.45 mm. The width of the segments was 0.5 or 0.8 mm. The 1.8 mm length with
0.8 mm width has been the most used.
Figure 2 A 42-year-old woman with six ICS in place 18 months postoperatively.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 120/338
109Intracorneal Segments for Hyperopia
Most of the initial ICS surgeries worldwide in human eyes were performed by the
authors (AC and LG) in Tijuana, Mexico. A small European trial was started. In the United
States, there is no experience with this technique in human eyes.
B. INDICATIONS/CONTRAINDICATIONS
The intracorneal segments for hyperopia are intended for the correction of low hyperopia
with a cylinder less than or equal to 0.75 D. Our experience included patients with a
cycloplegic spherical equivalent refraction between 1.00 to 5.00 D; however, we
found that this technique did not correct hyperopias greater than 2.0 D. Patients should
have a documented stability of their refraction as demonstrated by a change of less than
or equal to 0.50 D in spherical and cylindrical components of the manifest refraction for
the prior 6 months.
The ICS are contraindicated in
Pregnant or nursing womenPatients with signs of keratoconus
Patients with clinically significant corneal dystrophy or scarring in the 6- or 7-mm
central zone
Patients with a history of herpetic keratitis
Patients with an autoimmune disease, collagen vascular disease, clinically significant
atopic syndrome, insulin-dependent diabetes or an immunocompromised state
C. PREOPERATIVE PREPARATION
A complete ocular exam of both eyes should be performed. This includes visual acuity
testing with and without correction using standardized ETDRS (Early Treatment Diabetic
Retinopathy Study) visual acuity charts, slit-lamp examination, corneal topography, kera-
tometry, manifest and cycloplegic refractions, tonometry, and ultrasound pachymetry of
the central and peripheral cornea and funduscopy.
D. SURGICAL TECHNIQUE
The operative eye was prepared with povidone-iodine 10% solution and the eyelid margins
and cilia were draped to fully isolate the surgical field. Topical anesthesia was achieved
using two drops of 0.5% tetracaine hydrochloride. A Barraquer wire speculum was placed
to hold the lids apart. One eye was treated at a time.
The surgical procedure started with the identification of the geometric center of the
cornea using a blunt Sinskey hook. A preinked marker was centered on the cornea to
provide a visual guide for the placement of the six circumferential incisions and the
placement of each segment at a 6.0-mm optical zone. Corneal pachymetry (DHG Technol-ogy, Exton, PA) was performed over the site of each incision. A 15-degree diamond knife
(KMI, Philadelphia, PA) was used to make a 1.0-mm incision at a depth of 67% of the
pachymetry reading along the peripheral corneal marks. A modified Suarez spreader was
used to begin a lamellar corneal dissection at the base of each incision. Specially designed
instruments (KeraVision, Fremont, CA) were used to create an intrastromal pocket toward
the previously marked 6-mm optical zone. It is very important to make sure that the tunnels

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 121/338
110 Gomez and Chayet
are made at approximately two-thirds of the corneal depth, otherwise the segments are
placed too superficially; this may lead to extrusion of the segments or undercorrection.
Each segment is then manually inserted into each tunnel with the use of specially
designed forceps (Kera Vision, Fremont, CA). All ICS were supplied sterile. The ICS
were sterilized with ethylene oxide (EtO) and subjected to aeration to remove residual
EtO. The segments should be introduced far enough that they are left at the 6.0-mm optical
zone. Leaving them too close to the limbus increases the possibility of neovascularization.
The 1.8-mm segments are easier to insert, as they are shorter. There is generally no need
to suture the incisions. In our hands the surgical procedure takes 15 to 17 min in all.
E. POSTOPERATIVE CARE
After the procedure is completed, topical gentamicin 0.3% eyedrops and topical diclofenac
0.1% are instilled into the eye before removal of the speculum. The patient is then dis-
charged wearing a protective eye shield. No patch is necessary. The postoperative manage-
ment for ICS placement is similar to that for Intacs (3).Patients are instructed to apply 0.3% tobramycin and 0.1% dexamethasone four
times daily for 1 week. Artificial tears are used as needed. Patients should be examined
the day after the procedure for wound revision. The incision sites will show a linear
fluorescein staining for 3 to 5 days. By the first postoperative week most of the staining, is
resolved. Each subsequent postoperative visit should include a manifest and a cycloplegic
refraction with and without correction visual acuity testing, slit-lamp examination, tonome-
try, keratometry, and topography examination.
After 3 months of follow-up on the operative eye and if refractive stability is
achieved, the patient’s contralateral eye can be surgically corrected.
F. VISUAL OUTCOMES
We have performed over 50 ICS implantations in men and women under 58 years of age.We have implanted all the types of segments manufactured to date: the 2.0-, 1.8- and 1.5-
mm segments and a variety of thinner segments. The hyperopias we have treated have
not exceeded the manifest refraction spherical equivalent (SE) of 2.75 and cycloplegic
refraction SE of 4.5 D.
Visual recovery after the ICS procedure was not as rapid as after Intacs (4). Patients
experienced blurry vision for distance but were able to read without glasses after a week.
Near (uncorrected visual acuity) (UCVA) was better than distance UCVA because there
was an initial overcorrection.
Improvement in UCVA occurred earlier with the 1.8-mm segments than with the
others. Some 71% of the patients achieved 20/20 or better UCVA 2 weeks after the surgery
compared with 27% in the 2.0-mm segment group. Ghost images and halos were a frequent
complaint in this first postoperative period. Visual acuities continued to improve over the
following weeks; by the first month, 76% of the patients were 20/20 or better in the 1.8-mm segments and 64% in the 2.0-mm group. The visual acuity and visual recovery were
similar to those reported for other keratorefractive procedures, and the results remained
constant at 18 months (5,6).
The procedure has not been associated with loss of best spectacle-corrected visual
acuity (BSCVA), demonstrating the safety of the procedure. Moreover, no patient had a
BSCVA less than 20/20. This can be attributed to the fact that the central cornea is not

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 122/338
111Intracorneal Segments for Hyperopia
Figure 3 Corneal topographies of the right and left corneas showing the central steepening of the cornea produced by the ICS.
touched during the procedure. Some 25% of the patients in the 2.0-mm group and 35%
of the patients in the 1.8-mm group experienced a gain of one line of BSCVA at 18
months. This advantage is due to the preservation of the corneal positive asphericity with
this procedure.
Refractive stability was achieved later than in the Intacs for myopia (4). After the
initial overcorrection, stability is obtained by the third month postoperatively. Corneal
topographies showed the central steepening of the cornea with an optical zone between
5 and 6 mm in diameter (Fig. 3). Continuing follow-up however, has demonstrated that
there is no long-term stability of the correction and visual outcome achieved. We followedthese patients for over 3 years and found that there is progressive hyperopic drift with
time, which is observed after the second year. This finding is similar to that observed with
laser thermokeratoplasty, where one sees a good initial correction but loss of effect with
time (7). With the ICS, only 60% of the initial manifest refraction correction and 46% of the
cycloplegic refraction is maintained after 3 years. Eyes with higher corrections (hyperopias
greater than 2.0 D) show a greater tendency to lose correction with time. The average
amount of hyperopic drift is 0.9 D, ranging from 0.5 to 1.75 D. Although the amount of
loss of correction has been small, considering that the attempted correction was 2.0 D,
this change is significant for these patients. Similarly, by 3 years, only 9% of the patients
have an UCVA of 20/15 or better.
G. COMPLICATIONSMost of the complications we encountered were related to the fact that the surgical tech-
nique is mostly manual. Among the single segment complications we encountered, the
presence of neovascularization was the most common. Segments placed too peripherally
and close to the limbus will predispose for growth of neovessels surrounding the segments.
These neovessels can grow deeply in the stromal tunnel and will eventually surround the
segment. We encountered this complication in 19% of the patients. In our experience,

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 123/338
112 Gomez and Chayet
topical steroids did not stop the growth of the vessel at any time during the active growth
stage. We recommend removal of the affected segment, especially if the patient is symp-
tomatic. Coagulation of the vessel with argon laser might stop the vessel growth. However,
typically such vessels recanalize; therefore we do not recommend intervention with laser.
A shallow placement of the segments will produce superficialization of the segments
with time, superficial punctate keratitis, and thinning of the overlaying cornea. Spontaneous
extrusion of a single segment is a rare complication that is related to shallow implantation
of the segment. Epithelial ingrowth can occur around the segment and is surgically induced.
We have found that by avoiding corneal de-epithelization during the procedure and by
dissecting each tunnel as tightly as possible, this complication is almost completely elimi-
nated. When these complications occur, the segments can be removed and subsequently
reinserted. In our experience, most single segments can be successfully reinserted without
complications or loss of preoperative BCVA. In the case of the shallow segments, a deeper
tunnel can be dissected and the segments reinserted more deeply at the same surgical
sitting as the explantation. In the presence of neovascularization, it is recommended to
wait until the vessels have regressed and then to proceed with reinsertion of the segment.With experience, we have found that these types of complications are significantly reduced,
which tells us that there is a learning curve with this technique.
Some complications are related to the presence of the segments per se. These were
white, chalky crystalline lamellar deposits that developed only in the inner most third of
the segments (Fig. 4). The lamellar deposits present around the segments are similar to
those reported adjacent to hydrogel corneal inlays (8,9) and in some patients after Intacs
(10). These deposits are presumably caused by separation of the corneal lamellae. Lamellar
deposits were seen in 80% of the eyes. Half of them were fully confluent, and no iris
detail could be seen. They started to appear between 2 to 3 months after the procedure
and peaked at 9 months. Only rarely were they noticeable to the patient. However, in one
case, they were so severe and esthetically visible, that all the segments had to be explanted.
After explantation, the deposits tend to disappear. In our experience, if the segment is not
removed, the deposits do not recede, as it appears to be the case with Intacs (3). Theygenerally do not produce visual symptoms. Other causes for removal of all segments in
Figure 4 White, chalky lamellar deposits typically seen in the inner portion of the segments.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 124/338
113Intracorneal Segments for Hyperopia
one eye are varied. Undercorrection and patient dissatisfaction with the refractive result,
usually due to induced irregular astigmatism, are among the most common causes.
Removal of the intracorneal segments is performed under topical anesthesia (tetra-
caine 0.5%) after sterilization of the eye with topical povidone-iodine solution. The patient
is prepared and draped in the same fashion as in the original surgery. A speculum is
inserted to hold the eyelids apart. The incision is reopened with a diamond blade, as this
allows minimally traumatic reopening of the incision. In our experience, attempts at blunt
dissection with instruments like a Sinskey hook are more traumatic than reopening with
a sharp blade. After the incision is opened, the tunnel is approached with a corneal spreader
spatula designed for this purpose. The spatula is used to reopen the tunnel and loosen
each segment within the tunnel. Subsequently, two small hooks are used to slide the
segments into the corneal tunnel and bring them through the incision. There is no position-
ing hole at the tip of the segments to engage each segment and facilitate its removal. Care
is taken to do this in a minimally traumatic manner.
The explantation of the ICS for hyperopia is not an easy procedure, unlike the
explantation of the Intacs for myopia (4,11). The exceptions are when single segmentsare explanted in the presence of neovascularization. These segments are usually loose,
close to the limbus, and easy to remove. When the segments are inserted close to the 6.0-
mm optical zone, they are harder to loosen, and no instruments are available to grasp the
segment and pull it out through the tunnel and out of the incision. Potential problems can
also be encountered when there have been difficulties with wound healing.
Postoperative care after total explantation of the ICS for hyperopia is moderately
painful; patients usually require systemic analgesia and topical anti-inflammatory drops.
Reversibility of the refractive effect, as demonstrated with the return of BSCVA and
manifest refraction to preoperative levels, is on average achieved at 3 months after the
explantation, rarely before. Removal of these segments can be followed, if desired, by a
safe and effective Lasik or PRK for low to moderate myopia.
This procedure is not intended to produce astigmatism; however, we induced 1D or
more of astigmatism in 23% of our cases. All segments should be placed symmetricallyand at the same depth in order to avoid this complication.
Rarely, patients have reported occasional pain without apparent cause or an unex-
plained photophobia. We have not seen cases of glare or halos 6 months after the surgery
and beyond.
H. SUMMARY
The ICS procedure reduces low hyperopic errors without astigmatism while sparing the
visual axis. They work better for patients with hyperopias of less than 2.0 D. As opposed
to laser thermokeratoplasty and conductive keratoplasty, the ICS procedure offers the
benefit of reversibility and preservation of the positive corneal asphericity. The procedure
is safe and there has been no loss of BSCVA in any treated patient so far. The effect of
ICS implantation appears to stabilize after the first 3 months and is maintained for 18 to24 months after the procedure. However, after the second year there is a progressive
loss of correction, which leads us to question the benefit of performing this procedure.
Complications with ICS implantation are mostly related to the surgical technique, which
is manual.
In general, removal of these segments can be followed by a safe and effective
segment reinsertion or, if preferred, LASIK or PRK for low to moderate myopia.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 125/338
114 Gomez and Chayet
REFERENCES
1. Nose W, Neves RA, Burris TE. The intrastromal corneal ring: 12-month sighted myopic eyes.
J Refract Surg 1996; 12:20–28.2. Holmes-Higgin DK, Baker PC, Burris TE, Silvestrini TA. Characterization of the aspheric
corneal surface with the intrastromal corneal ring segments. J Refract Surg 1999; 15:520–528.
3. Asbell PA. Intrastromal corneal ring. In: Kaufman HE, Barron BA, McDonald M, eds. Cornea,
2nd ed. Boston: Butterworth-Heinemann, 1997: 1037–1044.
4. Gomez L, Chayet A. Laser in situ Keratomileusis results after intrastromal corneal ring seg-
ments (intacs). 2001; 108:1738–1743.
5. Anschutz T. Laser correction of hyperopia and presbyopia. Int Ophthalmol Clin 1994; 34:
107–137.
6. Jackson WB, Casson E, Hodge WG, Mintsioulis G, Agapitos PJ. Laser vision correction for
low hyperopia. Ophthalmology 1998; 105:1727–1737.
7. Koch DD, Berry MJ, Vassiliadis A. Noncontact holmium: YAG laser thermal keratoplasty.
In: Salz JJ, ed. Corneal Laser Surgery. St Louis: Mosby, 1995:247–254.
8. McCarey B, Andrews D. Refractive keratoplasty with intrastromal hydrogel lenticular implants.
Invest Ophthalmol Vis Sci 1981; 21:107–115.9. Gomez ML, Barraquer JI. Permalens hydrogel intracorneal lenses for spherical ametropia. J
Refract Surg 1997; 13:342–348.
10. Reinstein DZ, Srivannaboon S, Holland SP. Epithelial and stromal changes induced by Intacs
examined by three-dimensional very high-frequency digital ultrasound. J Refract Surg 2001;
17(3):310–318.
11. Asbell PA, Ucakgan O, Odrich M. Photorefractive keratectomy after intrastromal corneal ring
segment explantation. Am J Ophthalmol 1999; 128(suppl 6):755–756.
12. Koch DD, Kohnen T, McDonnell PJ, Menefee R, Berry M. Hyperopia correction by noncontact
holmium: YAG laser thermal keratoplasty: US phase IIA clinical study with 2-year follow-
up. Ophthalmology 1997; 104(suppl 11):1938–1947.
13. BrinkmannR, Radt B,Flamm C, KampmeierJ, Koop N,Birngruber R.Influence oftemperature
and time on thermally induced forces in corneal collagen and the effect on laser thermokera-
toplasty. J Cataract Refract Surg 1995; 26:744–754.
14. Asbell PA, Maloney RK, Davidorf J, Hersh P., McDonald M, Manche E. Conductive Kera-toplasty Study Group. Conductive keratoplasty for the correction of hyperopia. Trans Am
Ophthalmol Soc 2001; 99:79–84, discussion 84–87.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 126/338
11
Anterior Chamber Phakic IntraocularLenses in Hyperopia
GEORGES BAIKOFF
Clinique Montecelli, Marseille, France
INTRODUCTION: BACKGROUND
Nowadays, several methods of surgery may be applied to treat myopia. These methods
may be combined to achieve the surgical goal. While photorefractive keratectomy (PRK),
laser assisted in situ keratomileusis (LASIK) and intracorneal rings (ICR), may be usedto treat low myopia, LASIK is the method of choice for up to 10 diopters. Higher levels
of myopia may require phakic intraocular lenses (IOLs) or even clear lens extraction.
However, treatment of the most common cause of ammetropia, presbyopia, is still under
investigation. Several techniques have been assessed including presbyopic LASIK, intra-
corneal inlays, clear lens extraction followed by multifocal IOL implantation, scleral rings
and recently phakic presbyopic IOLs. Among these techniques, additive surgeries benefit
adjustibility, adaptibility, and reversibility. This is why we have been investigating the
design of phakic multifocal IOLs for the past 18 months.
A. ANTERIOR CHAMBER PHAKIC IOLS
Phakic intraocular lenses may be divided in 3 main categories:
Posterior chamber IOLs
Anterior chamber IOLs with iris fixation
Anterior chamber IOLs with angle fixation
Since 1986 we have been designing anterior chamber lenses with angle fixation (ZB,
ZB5M, NUVITA, GBR, VIVARTE), we now aim to apply the multifocal concept to the
most recent generation lenses.
115

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 127/338
116 Baıkoff
We decided on foldable anterior chamber lens that may be inserted using a 3.2 mm
incision. A 2 piece implant has been designed: the haptics with PMMA properties have
a “2” shape that ends with three footplates fixated in the angle. A very soft optic, in
hydrophilic acrylic, binds tangentially to the haptics. This design allows maintaining a
stable anterior chamber as well as a gentle fixation in the angle (with the hydrophilic
acrylic footplates).
The len’s profile is equivalent to that of the NUVITA. Indeed, prospective and
retrospective studies demonstrated the short and long term safety of the ZB5M and the
NUVITA on the endothelium. The only problem detected with these lenses was cosmetic:
moderate pupil deformations (that may give a cat’s eye aspect) have been rarely reported
(less than 5% of the cases).
In order to reduce the risk of pupil ovalization, a special interest has been held on
a precise measurement of the anterior chamber. The measurement from sclera to sclera
using a caliper is indeed inaccurate. It is the reason we developed an objective technique
based on the retro-illumination of the anterior segment. This method allows precise and
accurate assessment of the angle-to-angle inner diameter of the anterior chamber andtherefore to exactly adjust the size of the implant. Additionally, a plastic stick has been
designed to confirm this measurement preoperatively.
B. FOLDING OF THE OPTIC
The optic was initially folded in two; the aperture was then either anterior (with a risk of
endothelial touch) or posterior (with a risk of iris contact). It was therefore necessary to
expand significantly the anterior chamber with healon. A special folding device is now
available to overcome this problem.
Indeed, an “N shaped” folding system has been designed to allow an aperture of
the implant parallel to the iris plan. The first model of presbyopic implant favors far vision
in the center of the optic, while the middle and the peripheral parts allow near and far vision
respectively. Many other possibilities may be evaluated throughout the future clinical trials.
C. INDICATIONS AND CONTRAINDICATIONS
The current indication includes presbyopic patients with emmetropia and without astigma-
tism. It is known that pseudophakic emmetropic patients without astigmatism implanted
with multifocal lenses have a success rate of 70%; which means that they do not wear
glasses for either near or far vision. If either an ametropia or an astigmatism exists, this
success rate falls down to 30%. Accordingly, in the first set of investigation, the implanta-
tion of presbyopic intraocular lenses is only proposed to emmetropic and stigmatic patients
in order to obtain optimal results. However, it may be possible in the near future to develop
implants with spherical power to treat low myopia or hyperopia. The only method currently
available to treat an associated astigmatism is to perform LASIK.
CONTRAINDICATIONS
Contraindications are those of anterior chamber implant surgery, including the need to
respect a 3 mm anterior chamber depth, an endothelial cell count over 2500 cells per
mm2, and the absence of other disorders of the anterior chamber (cataract, uveitis, corneal
dystrophy, glaucoma, etc.).

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 128/338
117Anterior Chamber Phakic IOL in Hyperopia
D. PREOPERATIVE MANAGEMENT
Preoperative management is generally easy. The eye to be treated, obviously lacking any
signs of conjunctival or corneal infection, must be in therapeutic myosis.
E. SURGICAL TECHNIQUE
The first patients have been operated under general or loco-regional anesthesia. In the
future topical anesthesia may be used. A 3.2 mm surgical incision, using a pre-calibrated
phako knife is first performed.
The incision, performed in an auto-sealed fashion, may be placed at 12 o’clock
while one or two lateral paracenthesis may be performed to help the manipulations. The
anterior chamber is then deepened using viscous material to:
1. Protect the endothelium
2. Enhance the volume of the anterior chamber to facilitate the lens aperture with-
out any danger for either endothelium or iris.The implant removed from its container is then placed on the folder. Once folded in N,
the implant is held with a special forceps that will allow the anterior chamber followed
by the rest of the inferior handle. The haptic may be easily folded to pass through the 3.2
mm incision. Subsequently, the optic is introduced in the anterior chamber and the inferior
footplates are directed towards the opposite angle. Once the optic is entirely introduced,
the superior blocks the implant and the inserting forceps is removed. The optic gently
opens in the anterior chamber parallel to the iris. The last manipulation of the insertion
is to place the trailing haptic in the anterior segment using either a forceps or a Leister
hook. Gonioscopy is performed to check the correct location of the handles, then viscous
is removed.
F. VISUAL OUTCOMES/COMPARISON OF RESULTS
As of today, 6 eyes of 5 patients benefited the implantation with more than 1 year follow
up (thanks to professor Eva VOLKOVA in BRNO, Czech Republic). As the first implanted
lenses were prototypes, the correct sizes were not available for all the treated eyes. Two
have been removed due to an oversizing, the 4 remnants are still in place. No anatomical
complications have been detected on these eyes and visual outcome is excellent. Three
eyes recovered 20/20 and the other 20/25 without additional correction in the 1st day
postoperatively. No complications could be observed on this first series.
G. SUMMARY
Presbyopic phakic IOLs implantation is an emergent technique that will become more and
more important in the future due to its simplicity. The benefit of a foldable implant is tobe inserted with a small auto sealed incision without induced astigmatism. The technique
has been simplified since the beginning and it will soon be feasible under topical anesthesia.
The major interest of this technique is to adjust the power of the addition to the
patient’s presbyopia and to be reversible in case of unfavorable outcome. Multicentric
studies must be performed to better assess the quality of the optic.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 129/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 130/338
12
Hyperopic Phakic Intraocular Lenses
THANH HOANG-XUAN
Fondation Ophthalomogique Adolphe de Rothschild and Paris University, Paris, France
FRANCOIS MALECAZE
Hopital Purpan, Toulouse, France
A. BACKGROUND
The use of phakic intraocular lenses (IOLs) in refractive surgery started in the 1950s and
was initially aimed only at correcting high myopia (1). It is now also indicated in moderate
myopia, particularly when photorefractive keratectomy (PRK) and laser-assisted in situ
keratomileusis (LASIK) are contraindicated. Surgical correction of hyperopia is more
recent. Hexagonal keratotomy (2), epikeratoplasty (3) and automated lamellar keratoplasty
(4) are no longer used, and holmium: YAG laser thermokeratoplasty (5), conductive kera-
toplasty (16), PRK, and LASIK are only effective in low hyperopia ( 4 D or less) (6,7).
The only surgical procedures to correct high hyperopia are phakic IOL implantation and
clear lens extraction associated with one- or two-(piggyback) posterior chamber (PC) IOL
implantation. Disadvantages of clear lens extraction associated with PC IOL implantation
include loss of accomodation, difficulties with IOL power calculation, and irreversibility
(8,9). Only the iris-fixed and PC phakic IOLs can be used to correct hyperopia. Angle-
supported phakic IOLs are contraindicated in hyperopic patients because they often have
or will have narrow angles. The literature on correction of hyperopia using phakic IOLs
is scant, since this surgical procedure is is relatively new for this indication. Only five
reports have been published: one on the Artisan iris-claw lens (10) and four on PC phakic
IOL (11–14).
B. PHAKIC IOL TYPES
1. Iris-Fixed Phakic IOL (Artisan)
The Artisan hyperopia lens is a biconvex lens manufactured by Ophtec. It is fixed to the
iris at its midperiphery, which is immobile, by enclavation of a fold of anterior iridal
119

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 131/338
120 Hoang-Xuan and Malecaze
Figure 1 Hyperopic Artisan phakic intraocular lens. (Courtesy of Ophtec, Groningen, the Nether-
lands.)
tissue into the two diametrically opposed “claws” of the lens. It is a one-piece, UV-
absorbing, polymethylmethacrylate lens with an overall length 8.5 mm (IOLs 7.5 mm
long may also be available) and a diameter of the optical part of 5.0 mm. Its power range
is 1.0 to 12.0 D with a 0.5–increment increase (Figs. 1 and 2).
2. Posterior Chamber Phakic IOL
The only marketed hyperopia PC phakic IOL is the STAAR Collamer intraocular lens,also called an implantable contact lens (ICL) and manufactured by STAAR Surgical. It
is made of a flexible hydrophilic collagen copolymer, a compound combining HEMA and
porcine collagen (less than 0.1%). Its refractive index is 1.45 at 35ЊC. It is available with
lengths of 11.0 to 13 mm. The diameter of the optical zone is 5.5 mm, and the dioptric
power ranges from 3 to 17 D (Fig. 3).
C. INDICATIONS/CONTRAINDICATIONS
The best indications are hyperopes of 4 D or more who do not tolerate contact lens, cannot
wear spectacle correction for occupational or psychological reasons, and cannot or do not
want to undergo alternative refractive procedures. Candidates are often middle-aged or
older patients whose visual discomfort is increased by presbyopia. Hyperopes also experi-
ence more difficulties in inserting their contact lenses.
Contraindications include
One-eyed patients
Unstable refraction
History of ocular disease, including glaucoma, cataract, uveitis, and progressive and/
or severe retinal/choroidal disease

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 132/338
121Hyperopic Phakic Intraocular Lenses
Figure 2 Hyperopic Artisan phakic intraocular lens. (Courtesy of Ophtec, Groningen, the Nether-
lands.)
Figure 3 Hyperopic Artisan phakic intraocular lens.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 133/338
122 Hoang-Xuan and Malecaze
History of connective tissue disease
Corneal endothelial disease and/or endothelial cellular density less than 2000 mm2
Central anterior chamber depth less than 3.0 mm for the Artisan iris-claw lens, and
2.8 mm for the ICL STAAR lens
Pupil larger than 6.0 mm in scotopic luminance
Patients who will obviously not be compliant for lifelong ophthalmological follow-
up
D. PREOPERATIVE PREPARATION
1. IOL Power Calculation
The Artisan iris-claw lens dioptric power is calculated on the basis of the curvature of
the cornea (K), the anterior chamber depth, and the spectacle correction by applying the
van der Heijde formula (15). It is approximatively the same as the power of the spectacles
at a vertex distance of 12 mm.
The STAAR Collamer’s IOL dioptric power is determined using Feingold’s formula
(proprietary) that utilizes the refraction, keratometric power, corneal thickness, and anterior
chamber depth. The IOL length is the horizontal limbal white-to-white measurement 0.5
mm (not well defined).
2. Anesthesia
Most patients are operated on on an outpatient basis. The anesthesia methods are based
on patient and surgeon preferences: general anesthesia or peribulbar injection. Topical
anesthesia can be applied for STAAR Collamer lens implantation but not for Artisan iris-
claw lens surgery, for which full akinesia and analgesia are required.
3. Pupil Size
Artisan iris-claw lens implantation requires preoperative miosis to protect the natural lens
during the insertion and fixation of the IOL. A constricted pupil also facilitates proper
centration of the lens. For this purpose, two argon laser marks can be made on the iris at
diametrically opposite sites to facilitate proper centration of the IOL during the surgery,
contrary to STAAR Collamer phakic lens implantation, which requires full pupillary dila-
tion.
4. Prevention of Pupil Block
A perioperative peripheral surgical iridotomy is performed during the Artisan iris-claw
lens implantation procedure, rather than preoperative laser iridotomies. Two generous
peripheral laser iridotomies separated by 80 degrees are required before implantation of
the STAAR Collamer phakic lens.
E. SURGICAL TECHNIQUE
1. Artisan Iris-Claw Lens
Two side port incisions and a 5.2-mm (superior or temporal) clear corneal or (superior)
scleral tunnel incision are made. High-viscosity sodium hyaluronate is injected, and the

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 134/338
123Hyperopic Phakic Intraocular Lenses
Figure 4 ICL hyperopic phakic intraocular lens.
phakic IOL is introduced with a specially designed fixation forceps into the anterior cham-
ber through its smaller diameter. It is then rotated 90 degrees, its long axis becoming
parallel to the incision.
Most surgeons use specially designed iris entrapment needles introduced through
the side port incisions to enclavate the iris folds into the lens claws (Figs. 4 and 5).Intraocular acetylcholine chloride can be added if miosis is not sufficient. Accurate centra-
Figure 5 ICL phakic intraocular lens.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 135/338
124 Hoang-Xuan and Malecaze
Figure 6 Trapping of an iris fold between the claws of a hyperopic Artisan phakic intraocular
lens using an enclavation needle.
tion and fixation of the IOL is crucial to prevent postoperative glare or halos. A 1-mm
fold of midperipheral iris tissue is created under the claw using the iris entrapment needle;
a gentle pressure of the claw over the fold entraps it. The peripheral iridotomy is then
performed, the viscoelastic substance removed, and the wound tightly closed with 10–0
nylon sutures.
Postoperative care consists of steroidal and antibiotic eyedrops for 2 weeks and a
regular follow-up, particularly long-term evaluation of the corneal endothelium’s density
using specular microscopy. Patients also must be instructed not to rub their eyes after
surgery.
Figure 7 Introduction of an ICL hyperopic phakic intraocular lens into the eye using an injector.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 136/338
125Hyperopic Phakic Intraocular Lenses
Figure 8 Positioning of the haptic of the ICL phakic intraocular lens into the sulcus using a
tucker.
2. STAAR Collamer Phakic IOL
A side port incision is performed and viscoelastic material is injected. The foldable implant
is inserted through a 3.2-mm clear corneal beveled incision on the steepest axis, either
with an injector (Fig. 6) or MacPherson forceps. Care must be taken to orient the lens
properly while it unfolds and to avoid any central touch of IOL with the natural lens. The
optic disk is centered, and gentle downward pressure using a specially designed instrument
makes it possible to place each footplate one after the other behind the iris (Figs. 7 and
8). Then, the viscoelastic material is removed and acetylcholine chloride is injected into
the anterior chamber. Postoperative care consists of steroidal and antibiotic eyedrops for
1 to 2 weeks.
F. VISUAL OUTCOMES/COMPARISON OF RESULTS (Tables 1 and 2)
1. Artisan Iris-Claw Lens
Fechner et al. (10) published in 1998 the only study on hyperopic correction using the
iris-claw phakic lens. A total of 67 hyperopes were divided into three groups: 6.0 to
8.9 D (group 1), 9.0 to 11.9 D (group 2), and more than 12.0 D (group 3). In
all groups, the standard deviation between intended and final postoperative uncorrected
visual acuities was less than 2.80 D. The refractive results were stable at a follow-up of
4 months, and there was no loss of the mean best corrected postoperative best-correctedvisual acuity (BCVA). We implanted nine hyperopic patients, 4.4 to 8.1 D, with a
mean follow-up of 12 months (personal communication). Postoperative spherical equiva-
lent (SE) ranged from 0.75 to 0.75 D; 100% and 66.7% of eyes were within 1.00
and 0.50 D of emmetropia, respectively. Because of the loss of magnification, 78% of
patients demonstrated a loss in postoperative spectacle BCVA compared to the preopera-
tive spectacle BCVA.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 137/338
126 Hoang-Xuan and Malecaze
T a b l e 1
V i s u a l a n d
R e f r a c t i v e O u t c o m e s
R e f r a c t i v e
R e f r a c t i v e
U n c o r r e c t e d
U n c o r r e c t e d
o u t c o m e
o u t c o m e
V A p o s t o p
V A
p o s t o p
P h a k i c I O L
N o . o f
F o l l o w - u p
E S
( D )
E S ( D )
( D ) Ϯ
0 . 5 0
( D ) Ϯ
1 . 0 0
2 0 / 4 0 o r b e t t e r
2 0 / 2
0 o r b e t t e r
t y p e
A u t h o
r s
e y e s
( m o n t h s )
p r
e o p
p o s t o p
( % e y e s )
( % e y e s )
( % e y e s )
( % e y e s )
A r t i s a n
F e c h n e r ( 1 0 )
6 7
7 8 . 1
ϩ 6 t o ϩ
1 8
Ϫ 5 t o ϩ
3 . 5
( 1 9 9 8
)
( 1 2 t o 1 2 0 )
( ϩ 9 . 9 8 Ϯ
2 . 6 )
( ϩ 0 . 0 7 Ϯ
2 . 0 3 )
A r t i s a n
H o a n g - X u a n a n d
9
1 2
ϩ 4 . 4 0 t o ϩ
l 8 . 1 2
Ϫ 0 . 7 5 t o ϩ
0 . 7 5
6 6 . 7
1 0 0
6 7
1 1
M a l e c a z e ( 2 0 0 1 )
( u n p u b l i s h e
d d a t a )
ϩ 6 . 6 1
Ϯ
0 . 3 5
Ϫ 0 . 0 8 Ϯ
0 . 7 1
S T A A R
R o s e n ( 1 1 )
9
3
ϩ 2 . 2 5 t o ϩ
5 . 6 2
Ϫ 0 . 1 2 t o ϩ
0 . 5 0
8 8 . 8
8 9
4 4
( 1 9 9 8
)
S T A A R
D a v i d o r f
( 1 2 )
2 4
8 . 4
ϩ 3 . 7 5 t o ϩ
1 0 . 5 0
Ϫ 3 . 8 8 t o ϩ
1 . 2 5
5 8
7 9
6 3
8
( 1 9 9 9
)
( 1 t o 1 8 )
( ϩ 6 . 5 1
Ϯ
2 . 0 8 )
( Ϫ 0 . 3 9 Ϯ
1 . 2 9 )
S T A A R
P e s a n d o
( 1 3 )
1 5
1 2
ϩ 4 . 7 5 t o ϩ
1 1 . 7 5
Ϫ 1 . 0 0 t o ϩ
1 . 5 0
6 9 . 2 5
9 2 . 3
4 6 . 1 5
0
( 1 9 9 9
)
( 6 t o 1 8 )
( ϩ 7 . 7 7
Ϯ
2 . 0 8 )
( ϩ
0 . 0 2 Ϯ
0 . 6 4 )
S T A A R
S a n d e r s ( 1 4 )
1 0
6
ϩ
2 . 5 0 t o ϩ
1 0 . 8 8
Ϫ 0 . 5 0 t o ϩ
1 . 5 0
8 0
9 0
1 0 0
7 0
( 1 9 9 9
)
( ϩ
6 . 2 3 )
( ϩ
0 . 2 0 Ϯ
0 . 6 1 )

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 138/338
127Hyperopic Phakic Intraocular Lenses
Table 2 Safety of Hyperopic Phakic Intraocular Lenses
Loss of Unchanged Gain of
Phakic IOL BSCVA BSCVA BSCVAtype Authors (% eyes) (% eyes) (% eyes) Complications
Artisan
Artisan
STAAR
STAAR
STAAR
STAAR
22.2 (1 line)
55.5 (Ͼ2 lines)
25 (1 line)
4 (Ͼ
2 lines)
7.69
0
0
44.4
33
76.92
Fechner (10) (1998)
Hoang-Xuan and
Malecaze (2001)
(unpublished data)
Rosen (11) (1998)
Davidorf (12) (1999)
Pesando (13) (1999)
Sanders (14) (1999)
22.2 (1 line)
22.2 (1 line)
22.2 (2 lines)
29 (1 line)
4 (2 lines)4 (Ͼ2 lines)
15.38
2 (3 lines)
One glaucoma and
corneal edema
(in two eyes of
same patient)
None
Three pupillary
block glaucomas
Two pupillary
block glaucomas
One lens opacity
None
2. STAAR Collamer Phakic IOL
Four studies on hyperopic correction using the STAAR Collamer phakic lens have been
published (11–14).
These studies included 9, 24, 15, and 10 hyperopes respectively, the latter study(14) being a phase I clinical trial sponsored by the U.S. Food and Drug Administration.
In total, 58 patients underwent STAAR Collamer phakic IOL implantation.
Cumulative data show that preoperative SE ranged from 2.25 to 11.75 D. Mean
follow-up ranged from 3 to 12 months. Postoperative SE ranged from 3.88 to 1.50
D; 58 to 80% of eyes were within 0.50 D of emmetropia and 79 to 92.3% of eyes were
within 1.00 D of emmetropia. In Rosen’s study (11), the efficacy index was 0.98, which
was superior to the index for myopic patients implanted with the same type of phakic IOL
in series published by the same authors. Davidorf et al. (12) also compared their results
favorably to the predictability in their series of high myopic eyes.
Seven of 24 eyes (29%) (12) and one of 15 eyes (7.69%) (13) lost one or more lines
of postoperative BCVA. Conversely, only 8% of hyperopic eyes operated on by Davidorf et
al (12) demonstrated a gain in postoperative spectacle BCVA compared to the preoperative
spectacle BCVA. This is explained by the loss of magnification induced by the surgery.
G. COMPLICATIONS
In Fechner’s series of the artisan lens, one patient had glaucoma and corneal edema in
both eyes (10). In our study, no complications occurred and no change in endothelial cell
density was noted after a follow-up of 1 year (personal communication).

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 139/338
128 Hoang-Xuan and Malecaze
For the ICL, postoperative pupillary block glaucoma occurred in 3 of 24 eyes and
in 2 of the 15 eyes in the series of Davidorf et al. (12) and Pesando et al. (13), respectively.
This complication was due to iridotomies that were too small.
H. SUMMARY
Two types of phakic IOLs are available to correct hyperopia: the Artisan iris-claw lens
and the STAAR Collamer PC IOL. These represent the only surgical refractive procedures
capable of correcting hyperopia of 4 D or more. There have been very few publications,
but the results are encouraging. The predictibility, efficacy, stability, and safety of these
procedures are excellent, as well as the quality of the resultant vision. The time of recovery
is short and the surgeries are reversible. Long-term follow-up is, however, mandatory with
respect to delayed complication such as iris atrophy at the fixation sites and progressive
endothelial cell loss (iris-claw lens), and cataract and pigmentary dispersion (PC phakic
lens).
REFERENCES
1. Strampelli B. Sopportabilita di lenti acriliche in camera anteriore nella afachia o nei vizi di
refrazione. Ann Ottamol Clin Oculist Parma 1954; 80:75–82.
2. Basuk WL, Zisman M, Waring III GO, Wilson LA, Binder PS, Thompson KP, Grossniklaus
HE, Stulting RD. Complications of hexagonal keratotomy. Am J Ophthalmol 1994; 117:37–49.
3. Ehrlich MI, Nordan LT. Epikeratophakia for the treatment of hyperopia. J Cataract Refract
Surg 1989; 15:661–666.
4. Lyle WA, Jin GJC. Hyperopic automated lamellar keratoplasty: complications and visual
results. Arch Ophthalmol 1998; 116:425–428.
5. Koch DD, Kohnen T, McDonnell PJ, Menefee RF, Berry MJ. Hyperopia correction by noncon-
tact holmium:YAG laser thermal keratoplasty; United States phase IIA clinical study with a
1-year follow-up. Ophthalmology 1996; 103:1525–1536.
6. Jackson WB, Casson E, Hodge WG, Mintsioulis G, Agapitos PJ. Laser vision correction for
low hyperopia. An 18-month assessment of safety and efficacy. Ophthalmology 1998; 105:1727–1738.
7. Arbelaez MC, Knorz MC. Laser in situ keratomileusis for hyperopia and hyperopic astigma-
tism. J Refract Surg 1999; 15:406–414.
8. Kolahdouz-Isfahani AH, Rostamian K, Wallace D, Salz JJ. Clear lens extraction with intraocu-
lar lens implantation for hyperopia. J Refract Surg 1999; 15:316–323.
9. Holladay JT, Gills JP, Leidlein J, Cherchio M. Achieving emmetropia in extremely short
eyes with two piggyback posterior chamber intraocular lenses. Ophthalmology 1996; 103:
1118–1123.
10. Fechner PU, Singh D, Wulff K. Iris-claw lens in phakic eyes to correct hyperopia: preliminary
study. J Cataract Refract Surg 1998; 24:48–56.
11. Rosen E, Gore C. Staar Collamer posterior chamber intraocular lens to correct myopia and
hyperopia. J Cataract Refract Surg 1998; 24:596–606.
12. Davidorf JM, Zaldivar R, Oscherow S. Posterior chamber phakic intraocular lens for hyperopia
of 4 to 11 diopters. J Refract Surg 1998; 14:306–311.13. Pesando PM, Ghiringhello MP, Tagliavacche P. Posterior chamber Collamer phakic intraocular
lens for myopia and hyperopia. J Refract Surg 1999; 15:415–423.
14. Sanders DR, Martin RG, Brown DC, Shepherd J, Deitz MR, deLuca MC. Posterior chamber
phakic intraocular lens for hyperopia. J Refract Surg 1999; 15:309–315.
15. van der Heijde GL, Fechner PU, Worst JGF. Optische Konsequenzen der Implantation einer
negativen Intraokularlinse bei myopen Patienten. Klin Mbl Augenheilk 1988; 193:99–102.
16. McDonald MB, et al. Ophthalmology 2002; 109:1978–1989.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 140/338
13
Hyperopia and Presbyopia
Topographical Changes
STEPHEN D. KLYCE, MICHAEL K. SMOLEK, MICHAEL J. ENDL, VASAVIMALINENI, MICHAEL S. INSLER, and MARGUERITE B. McDONALD
Louisiana State University Health Sciences Center, New Orleans, Louisiana, U.S.A.
A. INTRODUCTION
Techniques for refractive surgery have made tremendous strides since the pioneering work
of Jose Barraquer and theintroduction of radialkeratotomy in the late 1970s (1). Traditionaloutcome measures for the efficacy of specific refractive surgeries are primarily uncorrected
and best-corrected visual acuities and cycloplegic and manifest refractions. Corneal topog-
raphy analysis has not been considered a primary outcome measure for clinical trials in
the United States—this despite the fact that corneal topography is now the standard of
care for preoperative screening of refractive surgical candidates and analysis of postopera-
tive results and is a mainstay of anterior segment practice. Direct analysis by corneal
topography has clearly shown the causes of visual loss after eventful refractive surgery.
The best examples include the formation of central islands and peninsulas after surface
ablation with the excimer laser (2) and induced generalized irregular astigmatism after
automated lamellar keratectomy (3). In this chapter, the topographic characteristics of the
presbyope and the current modalities for the correction of hyperopia are reviewed.
B. KERATOFRACTIVE PROCEDURES FOR
HYPEROPIA—TOPOGRAPHICAL CORRELATES
Kohnen et al. (4) used computed videokeratography to demonstrate peripheral corneal
flattening and central corneal steepening following noncontact Ho:YAG laser thermal
keratoplasty (LTK) for the correction of hyperopia. Greater changes in corneal curva-
129

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 141/338
130 Klyce et al.
ture and smaller amounts of topographical regression were noted when a two-ring laser
treatment pattern was applied. When the topography was analyzed, several forms of in-
duced astigmatism were observed: bowtie (both symmetrical and asymmetrical), irregu-
larly irregular, and semicircular patterns. Only one eye in the entire study group was
observed to have a homogeneous pattern. At present, noncontact LTK appears to be most
promising for low hyperopia up to approximately 2 D. Regression of the effect appears
to limit the procedure’s usefulness for refractive errors higher than 2 D. Furthermore,
factors such as younger age (less than age 30) and increased preoperative corneal thickness
may also contribute to faster rates of regression (5).
Early hyperopic photorefractive keratoplasty (H-PRK) ablations consisted of small
optical zones (approximately 4.0 mm) with small transition zones, creating an overall
treatment zone diameter of 7 to 8 mm. Small optical zones increase the patient’s sensitivity
to small decentrations. Likewise, small transition zones produce abrupt topographical and
refractive changes between treated and untreated tissue. This “lack of smoothness” pro-
motes more aggressive stromal and epithelial regeneration and thus refractive regression
(6). It should also be noted that in myopic PRK, significant decrements in the characterand magnitude of corneal optical aberrations have been found with larger optical and
transition zones. Larger optical and transition zones result in a more natural physiological
pattern of measured aberrations in myopic PRK (6), and a similar result would be expected
in approaches to correct hyperopia. These considerations have led to larger optical zones
of 6.0 mm, with overall hyperopic ablations now reaching 9.0 mm.
With these considerations, induced aberrations after H-PRK have been carefully
evaluated (7). Corneal topography after H-PRK showed a change from positive to negative
spherical aberration on the order of 3 D. It is known that the positive spherical aberration
of the cornea and the spherical aberration of the crystalline lens act in concert to decrease
the overall aberrations of the eye. However, if hyperopic procedures over correct for
corneal spherical aberration, a negative impact on visual function is expected. This effect
can be seen in Figure 1.
Even with larger ablation sizes, difficulties remain. By the nature of the procedure,
the functional optical zone becomes smaller as the attempted correction increases in size.
This is undoubtedly one of the most significant factors contributing to the poor success
rate of both H-PRK and hyperopic laser assisted in situ keratomileusis (H-LASIK) for the
correction of 5.00 D or greater. Moreover, Choi et al. (8a) report an increased risk of
irregular astigmatism based on topographic analyses when corrections above this level
are attempted. The comfort level in this respect seems to be surgeon-related; therefore
some surgeons limit attempted corrections to 4.0 D or less.
In reference to H-LASIK, a 9.0-mm ablation size requires the creation of a 9.5-mm
flap. Although modern microkeratomes may provide for this flap size, some patients with
small eyes or thin corneas are unsuitable candidates for this treatment. Larger flap diame-
ters and larger amounts of correction increase the chances of striae formation, which can
translate to irregular astigmatism on corneal topography.H-LASIK is gaining widespread use as a procedure to correct primary hyperopia as
well as to modify consecutive hyperopia after overcorrection from LASIK for myopia; it
is said to be safe and effective (8). Two typical case reports are given below to illustrate
the topography obtained. Each patient underwent hyperopic LASIK with the VISX, Inc.,
Star Excimer Laser System. The diameter of the optical zone was 5.00 mm, with a total
treatment zone of 9.00 mm OU.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 142/338
131Changes in Hyperopia and Presbyopia
Figure 1 H-LASIK effect on corneal topography and total eye aberration measured with NIDEK
OPD-Scan. (1) (top left panel) standard corneal topography showing off-center treatment; (2) skias-
copic (pointwise refraction) map: in the postoperative period, corneal aberrations for this eye account
for the bulk of the total ocular aberrations; (3) placido image; (4) wavefront map showing induction
of excess negative spherical aberration and coma.
Case 1. A 66-year-old woman with no prior history of ocular surgery underwent H-LASIK
for a refractionof 0.75 1.00 170 ODand 0.25 1.25 180 OS.Her bestspectacle-
corrected visual acvity (BSCVA) was 20/20 ( 2) OU.The patient requested refractive surgery
for monovision. Her preoperative K-readings were 44.3/44.5 at 118 OD and 44.4/44.8 at 163
OS. The laser was programmed to correct OD for 1.00 1.25 170 and OS for 2.50
1.50 180. The total ablation depth was 20m OD and 38 m OS. Optical zone diameterwas 5.00 mm. Her visual acuity without correction on postoperative day 1 was 20/200 OD
and 20/80 OS. Two weeks postoperatively, her visual acuity without correction was 20/70
( 1) OD and 20/200 OS and her BSCVA was 20/25 OD and 20/40 OS. The manifest
refraction was 0.75 1.00 050 OD and 2.50 0.75 055 OS. At 4 weeks
postoperatively, her visual acuity without correction was 20/30 ( 2) OD and 20/25 ( 2)
OS. Her refraction at this t ime was 0.75 0.75 055 OD and 1.50 0.75 165
OS, with BSCVA being 20/25 OD and 20/25 ( 2) OS. Postoperative corneal topography

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 143/338
132 Klyce et al.
A
B
Figure 2 H-LASIK 1-month postoperative topography for 66-year-old requesting monovision.
(A) OD; attempted correction: 1.00 1.25 170. (B) OS; attempted correction: 2.50 1.50
180.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 144/338
133Changes in Hyperopia and Presbyopia
showed the extent of induced cylinder, revealed a steepening of the central 5 mm of the
cornea, and produced simulated keratometry readings (SimKs) of 46.13/44.17 at 96 with a
potential visual acuity (PVA) of 20/25 to 20/30 OD and 47.41/46.68 at 94 with a PVA of
20/20 to 20/30 OS (Figure 2).
Case 2. A 26-year-old woman presented for refractive surgery evaluation. She had a refractive
error of 4.75 0.50 083 OD and 5.25 0.75 095 OS. Her BSCVA was 20/25
OU. Her keratometry readings were 44.1/45.6 at 091 OD and 44.1/46.0 at 099 OS. The desired
correction for the right eye was 6.00 0.50 083 and for the left eye was 6.00
0.50 105. Total ablation depth was 65 m OU. Optical zone diameter was 5.00 mm. On
postoperative day 1 her uncorrected visual acuity was 20/30 OD and 20/40 OS. Six months
postoperatively, BSCVA was 20/25 ( 1) OD with no improvement with manifest refraction.
BSCVA OS was 20/25 ( 1) with a manifest refraction of 1.00 0.75 165. There was
some evidence of regression OS. Postoperative keratometry readings were 48.70/49.18 at 058
OD and 47.24/48.07 at 051 OS (Figure 3).
Hence, H-LASIK seems a good choice of procedures at least for the temporary
correction of hyperopia. Long-term stability will need to be demonstrated for this approach,
as for others discussed in this chapter.
Conductive keratoplasty (CK) is being developed as an alternative procedure for
treating hyperopia. It is argued that if the collagen is heated to a carefully controlled
critical temperature, the shrinkage and changes in corneal shape might be more permanent.
Figure 3 Six-month postoperative corneal topography of H-LASIK patient showing good centra-
tion OU. (Central green irregularities OS are temporary, from tear film breakup.)

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 145/338
134 Klyce et al.
Figure 4 Preoperative and postoperative topographies after CK. Note large uniform area of in-
creased power.
Conductive keratoplasty uses radiofrequency energy to generate heat in the corneal periph-
ery. As with LTK, the shrinkage of the collagen occurs from the production of a ring
pattern of treatment spots around the corneal periphery. This shrinkage creates a purse-
string effect to steepen the central cornea. One of the immediately appreciated benefits
of CK over H-LASIK is the larger functional optical zone (Figure 4).
C. MULTIFOCAL EFFECTS
As the number of patients undergoing refractive surgery expands, the curious phenomenon
of presbyopic patients presenting with functional near and far vision after refractive surgery
is being more frequently reported for both myopic and hyperopic corrections. Described
as a “multifocal” effect, this side effect of the surgery deserves scrutiny.
It was Benjamin Franklin who conceived the first bifocal spectacle in 1874, initiatingwhat is perceived to be a sequence of developments (Figure 5). Deliberate multifocality
was introduced to the contact lens field prior to 1967 (9) and to the intraocular lens
(IOL) arena before 1987 (10). While early models of IOLs and contact lenses exhibited
pronounced aberrations that reduced contrast sensitivity, current renditions have enjoyed
a measure of patient acceptance, at least with contact lenses. Unintentional iatrogenic
multifocality was first identified with corneal topography in 11 eyes after radial kerato-

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 146/338
135Changes in Hyperopia and Presbyopia
Figure 5 Historical use of multifocality in vision correction: Ben Franklin’s bifocal spectacles,
bifocal contact lenses, bifocal IOLs, multifocality in radial keratotomy (11) and in photorefractive
keratectomy for myopia (13).
tomy, and although the possibility of complications from degradation of contrast sensitivity
as well as monocular diplopia was anticipated, no patient complaints of this type were in
fact reported (11). However, shortly after this report, additional analysis showed that
certain patients with the multifocal effect after radial keratotomy could experience visually
debilitating irregular astigmatism. This should be considered a complication of surgery
(12). Multifocal effects have also been found following PRK (13) for myopia and contrib-
ute to a form of artificial accommodation in pseudophakic eyes (14).
It is well known that patients with an extreme amount of irregular corneal astigma-
tism often refract over a large range of powers. This is the basis for the so-called multifocal
effect; in spectacles, distinctly separate areas of the lens are prepared with different specific
powers, whereas the power distributions of the multifocal cornea are more continuously
graded and are analogous to gradations of refractive powers of the Varilux contact lens
system. It might therefore be more accurate to describe the multifocal property as one of varifocality.
A topographical multifocal effect can be assessed by direct examination of the distri-
bution of corneal powers over the entrance pupil. The standard statistical metric for measur-
ing the width of such distributions is the coefficient of variation; hence, an appropriate
topographic definition of corneal multifocality is the coefficient of variation of corneal
power (CVP) (15). The increase in the range or width of the distribution of central corneal

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 147/338
136 Klyce et al.
Figure 6 Corneal power distribution in the central 3 mm before and after conductive keratoplasty.
Note the broader distribution of corneal powers after surgery, which will enhance the multifocaleffect. This is an analysis of the topography shown in Figure 3.
powers is illustrated in Figure 6. It can be noted that the power distribution is broad and
without distinct peaks; hence the appellation varifocal. Conversely, Benjamin Franklin’s
bifocals would produce a bimodal distribution: two peaks whose widths directly relate to
the precision of manufacture.
Despite the promising aspects of artificially inducing accommodation with controlled
corneal multifocality, significant levels of uncontrolled multifocality can lead to a reduction
Figure 7 The effect of irregular astigmatism on vision can be simulated by placing the measured
surface into a model eye and doing ray tracing. CTView V3.12 (Sarver and Associates, Merritt
Island, FL) was used for this calculation.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 148/338
137Changes in Hyperopia and Presbyopia
Figure 8 After correction for distance vision with conductive keratoplasty for hyperopia, uncor-
rected near vision (UNVA N) also improves (p Ͻ 0.001). (Data courtesy of Refractec, Inc., lrvine,
CA).
in contrast sensitivity and symptomatic vision. The effect of varifocality in corneal surgery
can be evaluated mathematically by fitting the surface with Zernike polynomials and
calculating from this the modulation transfer function. This will give the global optical
characteristics of the corneal surface and allow the simulation of multifocal effects on
vision, as shown in Figure 7.
With hyperopic keratorefractive surgery, there is another effect that comes into play
under the guise of multifocality. In one cohort of patients undergoing the conductive
keratoplasty procedure for the correction of low hyperopia, postoperative near vision either
remained constant or was enhanced at 1 month for every eye in the study (Figure 8). The
average improvement was statistically significant ( p Ͻ 0.001). This is a striking effect
that generally contrasts with myopic keratorefractive surgeries, where functional nearvision typically worsens in the presbyopic patient population (16). This effect can be
explained. Presbyopes who are mildly myopic often have excellent near vision without
correction. With keratorefractive surgery, near vision is sacrificed for improved distance
vision. On the other hand, presbyopic hyperopes have very poor uncorrected near vision,
and when keratorefractive surgery is used to correct their distance vision, this brings their
near focal point closer to the eye and improves vision at the near reading distances.
Multifocality and better than expected near vision after keratorefractive surgery for
the correction of hyperopia are due to a combination of factors. Focus over a range of
distances is made possible by the varifocal nature of some postoperative corneal topo-
graphies. Residual accommodation in younger patients can enable uncorrected near vision.
Use of the pinhole effect and bright illumination make a contribution as well. Finally,
improvements in uncorrected near vision can be expected after hyperopic corrections
because the near focal plane is brought closer to the eye, whereas with myopic corrections,it is moved further away.
D. DIAGNOSTIC IMPLICATIONS
Several approaches have been developed to provide for the automatic interpretation of
corneal topography (17). Among these, neural networks appear to have the greatest poten-

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 149/338
138 Klyce et al.
tial for success (18–20). A principal consideration in developing a strategy for the training
of such a network is data collection. Generally, 20 to 30 examples of each class of corneal
topography are collected to provide a broad range of “experience” for the neural network.
In this way the network can “learn” the hallmarks of each corneal condition and then be
able to classify new corneal maps accordingly. With the widespread success of refractive
surgery, there is concern that donor corneas for transplantation might be compromised by
previous surgery. As a result, a class of corneas was developed that are referred to as
having “myopic refractive correction.” There appear to be no consistent features among
the various myopic refractive corrections that persist to allow differentiation between the
various types. This even includes radial keratotomy, because the lower power over the
incision sites tends to be erased with time. Fortunately, no other corneal condition or
disorder is known that has the principal feature of uniform central corneal flattening. With
hyperopia, central corneal steepening is the principal characterizing feature, and again,
differentiation among the several corneal surgical approaches may not be possible. How-
ever, the central corneal steepening after hyperopic correction, unlike correction for my-
opia, outwardly mimics the characteristics of keratoconus, with a centralized cone (Figure9). This may confound the clinician, as well as the automated classification algorithms
that detect keratoconus. Patient history and corneal pachymetry may be required for differ-
entiation between hyperopia-corrected corneas and keratoconus unless some distinguishing
topographical metric is found.
Figure9 Postoperative topography of H-LASIK. Note the fairly typical appearance of keratoconus
as a consequence of the surgery. Corneal topography classification programs will need to be retrained
to determine whether it is possible to automatically differentiate H-LASIK from keratoconus.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 150/338
139Changes in Hyperopia and Presbyopia
E. SUMMARY
Corneal topographic analysis is helpful in elucidating the strengths and weaknesses of
refractive surgical procedures, and surgery for hyperopia is no exception. Centration iscritical, and a large treatment zone size is technically difficult to achieve. A hyperopic
procedure’s stability can be objectively and precisely measured with corneal topography.
However, the results of stability measurements may be confounded by the fact that people
in this age group (50–65 years) are undergoing progressive hyperopia naturally; this must
be taken into account. Several factors, including varifocality of corneal topography, con-
tribute to better than expected near visual function after the surgery. With advancing age,
qualities of the tear film diminish, and this leads to fine surface irregularities, while the
induction of coma results from global asymmetrical changes in shape.
REFERENCES
1. Waring GO. Refractive Keratotomy for Myopia and Astigmatism, St Louis: Mosby, 1992.
2. Lin DT, Sutton HF, Berman M. Corneal topography following excimer photorefractive keratec-
tomy for myopia. J Cataract Refract Surg 1993; 19(suppl):149.
3. Klyce SD, Martinez CE. Corneal topography. In: Albert DM, Jakobiec F, eds. Principles and
Practice of Ophthalmology. Philadelphia: Saunders, 2000: 668–694.
4. Kohnen T, Husain SE, Koch DD. Corneal topographical changes after noncontact holmium:
YAG laser thermal keratoplasty to correct hyperopia. J Cataract Refract Surg 1995; 22:
427–435.
5. Alio JL, Ismail MM, Pego JLS. Correction of hyperopia with noncontact Ho:YAG laser thermal
keratoplasty. J Refract Surg 1997; 13:17–22.
6. Endl MJ, Martınez CE, Klyce SD, McDonald MB, Coorpender SJ, Applegate RA, Howland
HC. Effect of larger ablation zone and transition zone on corneal optical aberrations after
PRK. Arch Ophthalmol 2001; 119:1159–1164.
7. Oliver EM, O’Brart DPS, Stephenson CG, Applegate RA, Tomlinson A, Marshall J. Anterior
corneal optical aberrations induced by photorefractive keratectomy for hyperopia. J RefractSurg 2001; 17:406–413.
8. Ziff SL. Multifocal contact lenses. Am J Optom Arch Am Acad Optom 1967; 44:222–225.
8a. Choi RY, Wilson SE. Hyperopic laser in situ keratomileusis: primary and secondary treatments
are safe and effective. Cornea 2001; 20:388–393.
9. Keates RH, Pearce JL, Schneider RT. Clinical results of the multifocal lens. J Cataract Refract
Surg 1987; 13:557–560.
10. Werblin TP, Klyce SD. Epikeratophakia: the surgical correction of aphakia: I. Lathing of
corneal tissue, Curr Eye Res 1981; 1:123–129.
11. McDonnell PJ, Garbus J, Lopez PF. Topographic analysis and visual acuity after radial kerato-
tomy. Am J Ophthalmol 1988; 106:692–695.
12. Maguire LJ, Bourne WM. A multifocal lens effect as a complication of radial keratotomy.
Refract Corneal Surg 1989; 5:394–399.
13. Scher K, Hersh PS. Disparity between refractive error and visual acuity after photorefractive
keratectomy: multifocal corneal effects. J Cataract Refract Surg 1997; 23:1029–1033.14. Fukuyama M, Oshika T, Amano S, Yoshitomi F. Relationship between apparent accommoda-
tion and corneal multifocality in pseudophakic eyes. Ophthalmology 1999; 106:1178–1181.
15. Martinez CE, Klyce SD, Waring III GO, El Maghraby A. The topography of LASIK. In:
Pallikaris IG, Siganos DS, eds. LASIK. Thorofare, NJ: Slack, 1997:339–357.
16. Wright KW, Guemes A, Kapadia MS, Wilson SE. Binocular function and patient satisfaction
after monovision induced by myopic photorefractive keratectomy. J Cataract Refract Surg
1999; 25:177–182.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 151/338
140 Klyce et al.
17. Maeda N, Klyce SD, Smolek MK, Thompson HW. Automated keratoconus screening with
corneal topography analysis. Invest Ophthalmol Vis Sci 1994; 35:2749–2757.
18. Maeda N, Klyce SD, Smolek MK. Application of neural networks to the classification of
corneal topography: preliminary demonstration. Invest Ophthalmol Vis Sci 1995; 36:1327–1335.
19. Maeda N, Klyce SD, Smolek MK. Comparison of methods for detecting keratoconus using
videokeratography. Arch Ophthalmol 1995; 113:870–874.
20. Smolek MK, Klyce SD. Current keratoconus detection methods compared with a neural net-
work approach. Invest Ophthalmol Vis Sci 1997; 38:2290–2299.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 152/338
14
Corneal Surface Profile AfterHyperopia Surgery
DAMIEN GATINEL
Fondation Ophthalomogique Adolphe de Rothschild and Bichat Claude Bernard
Hospital, Paris, France
The desired change in corneal curvature to correct for hyperopia with current excimer
laser systems is based on principles of geometric optics and the precise interaction of the
excimer radiation with the corneal tissue. In comparison to myopic correction in which
the goal is to flatten the central cornea, in hyperopia the central corneal area must besteepened to increase its optical power. This central steepening makes the planned correc-
tion of the hyperopic eye more difficult because the steepened central corneal portion has
to join the peripheral unablated area of lower curvaturevia a transition area. These represent
the important special features of the correction of hyperopic errors, which are emphasized
in this chapter.
A. CORRECTION OF PURE SPHERICAL HYPEROPIC ERRORS
The profile of ablation to correct for spherical hyperopia is radially symmetrical and
predominates in the periphery in an annular fashion. A subtraction shape model based on
geometric optics allowed Munnerlyn et al., in 1988, to announce the principles of laser-
guided photoablation in the central corneal area (effective optical zone) (1). The modifica-
tions of the corneal profile are analyzed separately below for the optical zone and for the
transition zone.
1. Optical Zone Design
Conforming to the pioneering work of Munnerlyn et al., the change in paraxial corneal
power can be predicted by considering the initial unablated and the final ablated corneal
141

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 153/338
142 Gatinel
Figure 1 Schematic representation of the lenticule ablated for the correction of spherical hyper-
opia. The profile of ablation is outlined along two perpendicular meridians (green). The thickness
of the lenticule is maximal at its edges and null at its center.
surface as two spherical surfaces with a single but different radius of curvature. The
removal of tissue is equivalent to adding a thin lens of equal but opposite power. This
permits the calculation of the ablation profile over theoptical zone for a spherical hyperopic
error (see Appendix 1).
To generate a three-dimensional graphic representation of the theoretical shapes of
the lenticules ablated during laser-assisted in situ keratomileusis (LASIK) of similar
amounts of spherical and cylindrical ablation, we used a digital modeling software that
allow to visualize the results of Boolean operation on orientated three-dimensional surfaces
(see Appendix 2).
The difference between each of the radii of curvature was exaggerated as compared
to the surgical range so as to facilitate the spatial visualization of the contour features of
the generated lenticules.
Spherical hyperopic ablation results in the ablation of a concave lenticule within
the optical zone, which is represented on Figure 1. Its thickness is null in the center and
increases progressively toward the periphery, where it reaches its maximum at the edge
of the optical zone. In first-order approximation, the maximum thickness of the edge of
the ablated lenticule over the optical zone is proportional to the magnitude of the hyperopic
treatment and to the square of the chosen optical zone diameter. The volume of tissue
ablation needed to steepen the cornea is thus delimited by the initial anterior surface and
the final postoperative steeper spherical surface over a circular optical zone.
2. Transition Zone Design
For necessary geometric feature, Any cornea that has had tissue removed centrally tosteepen its curvature (optical zone) while leaving the periphery untouched must undergo
an additional ablation to sculpt a smooth blending zone (transition zone).
This flatter area, commonly referred to as the transition zone, thus represents a
constant feature that ideally would have no undesirable optical effects and would ensure
the stability of the induced refractive changes in the optical zone by limiting unwanted
biological and biomechanical changes.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 154/338
143Corneal Surface After Hyperopia Surgery
When we address theoretical considerations on the different approaches to blend a
steepened optical zone to the untouched peripheral cornea, some constraints had be taken
into consideration (2). Should this be done by a noncontinuous constant curvature profile,
avoiding the induction of a continuous negative curvature, or by minimizing the slope of
the transition zone with a continuous change in its curvature but inducing negative curva-
ture (Fig. 2)? Because the patterns of ablation for the hyperopic transition zone are proprie-
tary, it is difficult to find confirmations of the use and interest of any of the transition
zone profile design characteristics. It seems, however, reasonable to postulate that any
profile of ablation should be “smooth” in a mathematical sense—i.e., avoiding local dis-
continuities to prevent epithelial hyperplasia. A continuous profile of ablation with a very
gradual change in its curvature seems a better option to correct for hyperopia while limiting
regression. This pattern implies the need of two points of inflexion (inversion of the sign
of the local curvature) to prevent the occurrence of discontinuities (Fig. 2).
Some publications have emphasized on the need for a large transition zone outer
diameter in order to improve biological tolerance and minimize regression (3–5). Con-
versely, enlarging the optical zone diameter, although desirable to preserve the quality of vision and reduce the risk of decentration, represents a limiting factor, since the depth per
diopter at the edge of the optical zone will increase with the square of the optical zone
diameter. This could account for the low success rate observed for corrections over 5 or
6 D of hyperopia. The determination of the diameter of the ablation zone should logically
Figure 2 Profile of ablation for the spherical hyperopic error. O, ablation center; OZ, optical
zone; TZ, transitionzone; dotted black line, preoperative corneal profile; fullblack line, postoperative
corneal profile; blue line, postoperative profile over the transition zone with no local curvature
discontinuities but negative slope between the points of inflexion T and N; red line, postoperative
transitional profile having a constant positive slope, but with a noncontinuous junction with the
edge of the optical zone.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 155/338
144 Gatinel
depend on the diameter of the optical zone. For example, a planned optical zone of 6.0
mm would require an ablation zone of 8.5 to 9.0 mm. Otherwise, effective optical zone
diameters might be diminished by epithelial filling of the peripheral ring of ablation in
case of high-magnitude of treatment. In LASIK, the corneal flap covering of the ablation
zone minimizes the epithelial healing response (6). This might account for the better
reported results of this technique over photorefractive keratectomy (PRK).
Because the total ablation zone diameter is equal to the outer diameter of the transi-
tion zone, it is mandatory to obtain large flap sizes for hyperopic LASIK procedures (7).
B. CORRECTION OF PURE CYLINDRICAL HYPEROPIC ERRORS
1. Optical Zone Design
The principles of the Munnerlyn pattern can be extended to the correction of astigmatism
by taking into consideration the meridional variations in corneal apical power. In the case
of pure hyperopic astigmatism, a “cylindrical profile of ablation” can be generated, whichaims to selectively steepen the initial flatter principal meridian. This pattern has no center
but there is axis symmetry along each of the principal meridians. A three-dimensional
representation of the etched corneal lenticule for such correction over a circular optical
zone is depicted in Figure 3. The depth of ablation is maximal at the edge of the optical
zone along the flat meridian, while the steep meridian is untreated by the laser.
2. Transition Zone Design
The shape of the transition zone is dictated by the features of the optical zone. As for the
optical zone, the central symmetry is broken. The step in tissue height is maximal at the
boundary of the optical zone along the flat meridian. This discontinuity then tapers slowly
and becomes null along the untreated steep meridian. To alleviate this variation, the diame-
ter of the transition zone should be longer along the flat meridian and minimal (equal to
Figure 3 Schematic representation of the lenticule corresponding to the correction of a pure
hyperopic astigmatism. Its thickness is null along the steep meridian (S) and maximal in the periphery
along the flat meridian (F). The profile of ablation along the flat meridian is underlined in green.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 156/338
145Corneal Surface After Hyperopia Surgery
A
B
Figure 4 (A) Schematic representation of the lenticule corresponding to the correction of a pure
hyperopic astigmatism with the transition zone. The ablation along the flat meridian is highlightedin green. (B) Representation of the volume of the transition zone alone. Its outer perimeter is
elliptical, since the groove to blend reaches its maximum depth over the flat axis.
that of the optical zone) and minimal along the steep meridian while having a constant
slope over the optical zone. The shape of the outer limit of the transition zone is thus
elliptical (Fig. 4A and B). This might be clinically relevant in optimizing the position of
the hinge in LASIK procedures by placing it perpendicular to the flat meridian.
C. CORRECTION OF COMPOUND CYLINDRICAL HYPEROPIC
ERRORSThe refraction as commonly done clinically is an arc-based mathematical expression lim-
ited to the principal major and minor axes, and any compound hyperopic astigmatic refrac-
tive error can be expressed by different equivalent expressions. Thus, different sequential
treatment strategies for the correction of compound hyperopic astigmatism have been
proposed: they all consist in the combination of spherical and cylindrical treatments of
equal or opposite signs.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 157/338
146 Gatinel
1. The positive-cylinder approach (ablating the cylinder along the flattest meridian
and then treating the residual spherical component)
2. The negative-cylinder approach (ablating the cylinder along the steepest merid-
ian and then treating the residual spherical component)
3. The cross-cylinder approach (ablating half of the power of the cylinder along
the steepest meridian and the remaining half along the flattest meridian before
the residual spherical equivalent is treated)
Even if the optical result may be the same, these strategies may result in different
amount and depths of tissue ablation. The increasing number of reports of corneal ectasia
following LASIK suggests that the strategies that remove less of the corneal tissue should
be preferred for the treatment of any compound astigmatism. Recently Azar et al. compared
the theoretical ablation profiles and depths of tissue removal in the treatment of compound
hyperopic astigmatism and of mixed astigmatism (8). They found that strategies combining
the use of hyperopic spherical and myopic cylindrical corrections incur the greatest amount
of corneal tissue ablation.
Three-dimensional drawings were generated to depict the theoretical shapes of the
volumes of corneal tissue ablated to treat similar amounts of compound astigmatic hyper-
opic errors (Fig. 5A–C). These images can be interpreted more easily and quickly than
abstract mathematical functions. The shapes and volumes of the corresponding lenticules
can be analyzed for different strategies of ablation, and this makes if possible to estimate
the theoretical differences in the amount of ablated corneal volume.
In compound hyperopic astigmatism, all the corneal meridians have excessive flat-
tening. The negative cylinder and the cross cylinder approaches both imply an additional
flattening that will cause redundant ablation by necessary additional positive spherical
treatment.
Figure 5 Schematic representation of the lenticules ablated for the correction of compound hyper-
opic astigmatism for three different strategies to treat the same refraction: 3 ( 2 0 degrees).
The optical zone diameter is identical for each of the depicted strategies. (A) Positive-cylinder
approach. The positive cylinder (2 0 degrees) ablated lenticule is represented above, with its
section along the flat axis outlined in light green. The spherical ablated lenticule ( 3) is represented
below, with two meridian outlined in dark green.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 158/338
147Corneal Surface After Hyperopia Surgery
Figure 5 Continued. (B) Cross-cylinder approach. The astigmatic component is split in two parts:
( 1 0 degrees) and ( 1 90 degrees). The corresponding lenticules are represented (the
profile of ablation along the principal meridians are outlined in red and light green for the negativeand positive cylinders, respectively). The remaining spherical equivalent ( 4) is then treated by
the ablation of a positive spherical lenticule (two perpendicular meridian outlined in dark green).
(C) Negative-cylinder approach. The refraction is treated as: ( 2 90 degrees) 5. The lenticules
corresponding to the negative-cylindrical and the positive-spherical treatments are shown with their
meridian outlined in red and dark green, respectively. The positive-cylinder approach minimizes
the volume of ablation and induces no ablation at the center of the optical zone. The cross-cylinder
approach induces an additional volume of ablation compared to the positive-cylinder approach. The
negative-cylinder approach induces the maximum volume of ablated tissue.
D. CUSTOMIZED ABLATION
In the preceding text, we have studied the changes in corneal profile induced by thecorrection of simple spherocylindrical errors. Customized ablations aim to correct both
the spherocylindrical error and the higher-order aberrations based on the collection of
wavefront or corneal topography data. This induces variations of the amount of tissue
removed at specific locations, and the ablation profile thus specified will have specific
features. For example, taking into account the corneal apical radius asphericity will induce
variations in the ablation depth. This might, however, not alter the “global pattern” of the

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 159/338
148 Gatinel
ablation profile for patients with hyperopic errors but rather induce radially asymmetrical
variations in the peripheral “step” at the edge of the optical zone. The transition zone
pattern will have to take this variability in account and its optimized slope will have to
be determined to ensure the stability of the induced changes over the optical zone.
E. CONCLUSION
For several reasons, the correction of hyperopia with PRK or LASIK is more difficult
than for myopia. The patterns of the profiles of ablation to steepen the cornea might
account for the limited success in excimer laser surgery for hyperopia. Refinements based
on simple geometrical considerations and the incorporation of customized data might
improve the results of such surgery.
APPENDIX 1
To correct for a spherical hyperopic error, Munnerlyn et al., by considering the initialunablated and the final ablated corneal surface as two spherical surfaces with a single but
different radius of curvature (Fig. 6), proposed the following formula for the ablation
profile over the optical zone:
t ( y) R2 R1 R21 y2 R2
2 y2
where t( y) expresses the depth of tissue removal as a function of the distance y from the
center of an optical zone diameter of S when R1 and R2 are the initial and final corneal
anterior radii of curvature, respectively. The power of the removed lenticule (D) corre-
sponds to the intended refractive change and is related to R1, R2, and the index of refraction
(n) as follows:
Figure 6 Schematic representation of the profile of ablation for spherical hyperopia along a
corneal meridian. Both initial and final surfaces are assumed to be spherical of radius R1 and R2
respectively. The gray portion corresponds to the material to be removed to steepen the anterior
part of the cornea over an optical zone diameter of S mm.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 160/338
149Corneal Surface After Hyperopia Surgery
D (n 1) 1
R2
1
R1
where R2 Ͻ R1 for hyperopic ablationsThe maximal depth occurs at the edge of the optical zone of diameter S and is equal
to:
t (S /2) R2 R1 R21 (S /2)2 R222 (S /2)2
APPENDIX 2
To generate a conceptual graphic representation of theoretical shapes of the lenticules
ablated during LASIK treatments of similar amounts of spherical and cylindrical treatment,
we used a digital modeling software that makes it possible to visualize the results of
Boolean operation on orientated three-dimensional surfaces (Bryce 3D, Metacreation Corp.
Dublin, Ireland). Using these Boolean operations (subtraction of one object from another)
on geometrical primitives such as spheres, cylinders, or toroidal ellipsoids, three-dimen-sional representations of the theoretical ablated volumes were generated (Fig. 7).
The optical zone was circular and the final corneal surface was spherical in all
cases. For spherical corrections, the initial and final corneal surfaces were modeled as two
sphericalsurfaces of different radii of curvature(the latterbeing flatter for myopic spherical
corrections and steeper for hyperopic correction). For pure cylindrical corrections, the
initial corneal surface was modeled as a spherocylinder with two major apical radii of
curvature along the principal meridians, the final surface being spherical. In cases of
myopic cylindrical correction, one of the principal radii of curvature of the initial surface
was shorter, the other being equal to that of the final corneal surface. In the case of
hyperopic cylindrical corrections, one of the principal radii of curvature of the initial
surface was longer, the other being equal to that of the final corneal surface. The three-
Figure 7 Model of the ablated lenticule for the correction of pure hyperopic astigmatism. This
volume is generated by boolean operation on primitive figures such as sphere, ellipsoid, cylinder,
in accordance with assumptions regarding subtraction shape models.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 161/338
150 Gatinel
dimensional representation of a lenticule was obtained by first subtracting the volume of
the primitive modeling of the final theoretical corneal surface from the primitive volume
modeling of the initial corneal surface. These primitives were aligned and centered on the
Z axis. The ablated lenticule for the correction of pure cylindrical myopic astigmatism
was generated by adjusting the distance between the apex of each surface so that they
would intersect along the steep meridian within a predetermined circular optical zone.
The difference between each of the radii of curvature was exaggerated as compared to
the clinical and surgical range to facilitate the spatial visualization of the contour features
of the generated lenticules. However, in comparing different strategies, the initial and final
surfaces were identical and were rescaled to the same ratio for purposes of comparison.
This made it possible to estimate the theoretical differences in the amount of ablated
corneal volume by the different available strategies that combine the ablation of these
elementary lenticules to correct for a given compound hyperopic astigmatic refractive
error.
The transition zone was modeled as a spherical (constant positive curvature) surface
encompassing the circular inferior edge of the ablated lenticule and joining the peripheralunablated cornea.
To facilitate the visualization and the distinction of the shapes of the ablated lenti-
cules, cross-sectional color outlines were added along the principal meridians.
REFERENCES
1. Munnerlyn C, Koons S, Marshall J. Photorefractive keratectomy: a technique for laser refractive
surgery. J Cataract Refract Surg 1988; 14:46–52.
2. Dierick HG, Missoten L. Corneal ablation profiles for correction of hyperopia with the excimer
laser. J Refract Surg, 1996; 12:767–773.
3. Chayet AS, Assil KK, Montes M, Castellanos A. Laser in situ keratomileusis for hyperopia:
new software. J Refract Surg 1997; 13(suppl):S434–S435.
4. Arbelaez MC, Knorz MC. Laser in situ keratomileusis for hyperopia and hyperopic astigmatism.
J Refract Surg 1999; 15:406–414.
5. Ditzen K, Huschka H, Pieger S. Laser in situ keratomileusis for hyperopia. J Cataract Refract
Surg 1998; 24:42–47.
6. Pallikaris IG, Siganos DS. Excimer laser in situ keratomileusis and photorefractive keratectomy
for correction of high myopia. J Refract Corneal Surg 1994; 10:498–510.
7. Rashad KM. Laser in situ keratomileusis for the correction of hyperopia from 1.25 to 5.00
diopters with the Technolas Keracor 117C laser. J Refract Surg 2001; 17:113–122.
8. Azar DT, Primack JD. Theoretical analysis of ablation depths and profiles in laser in situ
keratomileusis for compound hyperopic and mixed astigmatism. J Cataract Refract Surg 2000;
26(8):1123–1136.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 162/338
15
Wavefront Changes After HyperopiaSurgery
MARIA REGINA CHALITA and RONALD R. KRUEGER
Cole Eye Institute, Cleveland Clinic Foundation, Cleveland, Ohio, U.S.A.
A. BASIS OF WAVEFRONT ANALYSIS
1. Definition of Wavefront and Aberrations
In physical optics, light is considered as a wave, and the light wave spreads in all directions
as a spherical wave. The wavefront is the shape of light waves that are all in phase (1). Theideal eye, defined as an emmetropic eye without any aberrations, has a perfect wavefront,
described as a plane perpendicular to the line of sight (Fig. 1) (2). For real eyes, wavefronts
that converge toward the retina are not spherical, so perfect imaging never occurs.
Wavefront aberration is defined as the difference between the actual wavefront and
the ideal wavefront in the plane of the eye’s exit pupil (Fig. 2) (3).
Ocular aberrations are not constant during life (4); they increase with age (5) and
may change during accommodation (6,7). In optics, aberrations are classified in two differ-
ent types: monochromatic and chromatic (8).
2. Monochromatic Aberrations
Monochromatic aberrations involve specific wavelengths of visible light and can be subdi-
vided into defocus (spherical refractive error), astigmatism (cylindrical refractive error),coma, spherical aberration, and other terms of higher-order aberrations. Defocus and astig-
matism are considered low-order aberrations and can be corrected with glasses, contact
lenses, or refractive surgery (9). They correspond to approximately 85% of the average
wavefront error. Coma, spherical aberrations, and others are high-order aberrations (refrac-
tive distortions, that limit the vision of healthy eyes to less than the retinal limits) and
cannot be corrected with spherocylinder lens or with standard refractive surgery (10).
151

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 163/338
152 Chalita and Krueger
Figure 1 The Shack-Hartmann wavefront sensor forms a regular lattice of image points for a
perfect plane wave front of light.
They are responsible for approximately 15% of the average wavefront error. For coma,
the wavefront is asymmetrical about the perfectly spherical wavefront, producing a comet-
shaped pattern on the emmetropic plane. For spherical aberration, the converging wave-
front looks spherical near the center of the pupil but changes its curvature toward the edge
of the pupil. This aberration gives a continuum of foci and results in point images with
halos. Other terms of higher order aberrations are a group of all other deviations of the
converging wavefront from perfect sphericity.
3. Chromatic Aberrations
Chromatic aberrations are errors that result of dispersion in optical elements of the eye.
Refractive surgery techniques cannot correct chromatic aberration, since this error is inher-
ent to the properties of the ocular materials and not to the shape of the ocular components(11).
Figure 2 The Shack-Hartmann wavefront sensor forms an irregular lattice of image points for
an aberrated wavefront of light.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 164/338
153Wavefront Changes After Hyperopia Surgery
Figure 3 Three-dimensional pictorial directory of Zernike modes 0 to 20.
Aberrations are also classified in terms of orders using Zernike polynomials (12).
The wavefront error (difference in shape between the aberrated wavefront and the ideal
wavefront) for myopia, hyperopia, and astigmatism is well represented by a polynomial
of second order. These aberrations are therefore called second-order aberrations. Following
the same principle, coma is a third-order aberration and spherical aberration a fourth-order
aberration (Fig. 3).
Laser surgery [photorefractive keratectomy (PRK) and laser-assisted in situ keratom-
ileusis (LASIK)] increases high-order optical aberrations in human eyes, especially spheri-
cal aberration and coma (13,14). This increase in high-order optical aberrations after cor-
neal laser surgery is correlated with a significant decrease in quality of vision, especially
under scotopic conditions (15).
4. Detection of Wave Aberration: History of Shack-Hartmann
Most of the methods of wave aberration detection and reconstruction have been based on
ray tracing. These methods were first described in1900 by Hartmann. About 5 years earlier,
Tscherning constructed an aberroscope: a grid superimposed on a 5-D spherical lens wherea subject could see a shadow image of the grid on the retina. From the distortions of the
grid, one could infer the aberrations of the eye. Over 70 years later, Howland invented
the crossed cylinder aberroscope. Instead of using a spherical lens, he used a crossed
cylinder lens of 5 D with the negative axis at 45 degrees (16,17).
In 1961, Smirnov developed another method where a grid is viewed by the entire
aperture of the eye minus a single central intersection, which is viewed through a small

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 165/338
154 Chalita and Krueger
aperture made to scan the entire pupil sequentially. In 1998, Webb and coauthors made
a modern implementation of Smirnov’s method that computes the wave aberration and
reduces it to Zernike polynomials.
Last, the Shack-Hartmann sensor was developed in 1970 by Shack in order to im-
prove the images of satellites taken from earth. The first practical application was in 1984
by Wilson to test large telescopes. In 1989, Bille was the first to publish using the Shack-
Hartmann in ophthalmology to measure the profile of the cornea and in 1997 he became
the first to project a source onto the retina and use the Shack-Hartmann sensor to measure
aberrations of the eye. In the same year, Williams became the first to use the Shack-
Hartmann sensor with adaptative optics to measure and correct aberrations of the eye (18).
5. Principles of Shack-Hartmann
The Shack-Hartmann aberrometer has an objective lens that is actually an array of tiny
lenses. With this kind of lens the reflected light is broken into many individual beams,
thereby producing multiple images of the same retinal spot of light. For a perfect eye, the
reflected plane wave will be focused into a perfect lattice of point images, each image
falling on the optical axis of the corresponding lenslet. By contrast, the aberrated eye
reflects a distorted wavefront. By measuring the displacement of each spot from its corre-
sponding lenslet axis, we can deduce the slope of the aberrated wavefront when it entered
the corresponding lenslet. The wavefront should be analyzed as soon as it passes through
the eye’s pupil (19,20).
B. WAVEFRONT OF HYPEROPIC TREATMENT
1. Profile of Hyperopic Correction
In 1988 Munnerlyn and coworkers described the equations that served as a starting point
for developing current ablation algorithms. For a hyperopic ablation, the preoperative
cornea is modeled as a sphere of lesser curvature than the desired postoperative cornea,which is also modeled as a sphere. Tissue is removed from the peripheral area, flattening
this region and producing increased postoperative corneal curvature as a final result. This
concept is referred to as the shape-subtraction model of refractive surgery; it permeates
current thinking in refractive surgery and forms the basis for both topography and wave-
front-guided procedures (21).
2. Wavefront Measurements and Aberration Changes Before andAfter Conventional Hyperopic LASIK
In our service, we use the Alcon LADARWave Device (Orlando, FL) to study visual
aberrations. The LADARWave Device makes detailed measurements of the aberrations
present using the Shack-Hartmann principles. We can measure defocus, astigmatism, and
higher-order aberration that can be decomposed into coma, spherical aberrations, and otherterms of higher order aberrations (Fig. 4).
If we imagine a normal cornea with its normal prolate shape without any kind of
surgery done, we will find higher-order aberrations but in low amounts. The pattern of
each higher-order aberration is well defined: coma has a comet-shaped pattern with an
elevated area (semicircle of hyperopia) just next to a depressed area (semicircle of myopia)
in the same meridian (Fig. 5). Spherical aberration has a central elevated area (focus of

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 166/338
155Wavefront Changes After Hyperopia Surgery
Figure 4 LADARWave image showing the total wavefront pattern of a patient with hyperopic
LASIK to achieve monovision.
Figure 5 Coma pattern in a normal eye (LADARWave).

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 167/338
156 Chalita and Krueger
Figure 6 Spherical aberration pattern in a normal eye (LADARWave).
hyperopia) surrounded by a depressed circle (annulus of myopia) and with normalization
in the far periphery (resembling a flat sombrero) (Fig. 6).
Other terms such as trefoil, quadrafoil, and secondary astigmatism generally have
lower values (Fig. 7A and B).
Patients that underwent hyperopic treatments have an accentuated prolate corneal
pattern (Fig. 8) (22,23).
When we analyze the spherical aberration pattern of these eyes, we can notice a
decrease in the magnitude of spherical aberration and an inversion in the shape pattern.
This is because the waves that come from the peripheral ablated zone converge less, so
this area looks like a peripheral elevated red ring (annulus of relative hyperopia) and the
central rays converge more, giving a central depressed area (focus of relative myopia).
We call this pattern a flipped over sombrero hat, which is the opposite pattern of myopic
treated eyes (Fig. 9).
C. COMPARISON OF HYPEROPIC VERSUS MYOPIC TREATMENTWAVEFRONT
1. Profile of Myopic CorrectionAs described by Munnerlyn in 1988, for a myopic ablation, the preoperative cornea is
modeled as a sphere of greater curvature than the desired postoperative cornea, which is
also modeled as a sphere within the treated zone. The apex of the desired postoperative
cornea is displaced from the preoperative cornea by the maximal ablation depth, which
is determined by the ablation zone size. The intervening tissue is simply removed or
“subtracted” to produce the final result.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 168/338
157Wavefront Changes After Hyperopia Surgery
A
B
Figure 7 (A) Trefoil pattern. (B) Quadrafoil pattern.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 169/338
158 Chalita and Krueger
Figure 8 LADARWave image showing defocus, astigmatism, and higher-order aberrations of a
hyperopic patient.
Figure 9 Spherical aberration after hyperopic treatment showing negative asphericity, as repre-
sented by a flipped over sombrero.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 170/338
159Wavefront Changes After Hyperopia Surgery
Figure 10 LADARWave device showing defocus, astigmatism, and higher-order aberrations in
a myopic patient.
Patients who have undergone myopic treatments have an oblate corneal pattern (Fig.
10) (24). The wavefront pattern shows a flattening or concavity to the otherwise bowl-shaped wavefront of myopia.
Analyzing the wavefront of these myopic treatments, we notice that the spherical
aberration increases in number and size, with the depressed and elevated areas being
accentuated. We describe this kind of pattern as a sombrero hat (Fig. 11).
2. Comparison of Aberration Changes in Hyperopia Versus Myopia
In a study of 113 candidates for LASIK surgery, analyzing all aberrations, defocus and
astigmatism were dominant. When analyzing only higher-order terms, coma and spherical
aberrations were the most significant.
Another study described the pre-and postwavefront measurements of patients sub-
mitted to LASIK for myopia or hyperopia and myopic PRK. It was found that, for LASIK,
postoperative total error was significantly smaller for myopes than hyperopes ( p Ͻ 0.05).Both myopic and hyperopic LASIK patients exhibit modest regression in defocus. In
analyzing higher-order aberrations, it was noticed that spherical aberration decreased in
hyperopic treatments and increased in myopic corrections. All other higher-order terms
increased after either type of correction. In the postoperative interval, coma was the most
dynamic higher-order aberration, with an overall decrease over time until 6-months postop-
eratively.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 171/338
160 Chalita and Krueger
Figure 11 Spherical aberration after myopic treatment showing increased positive asphericity,
as represented by a sombrero hat.
REFERENCES
1. Applegate RA, Thibos LN, Hilmantel G. Optics of aberroscopy and super vision. J CataractRefract Surg 2001; 27:1093–1107.
2. Maeda N. Wavefront technology in ophthalmology. Curr Opin Ophthalmol 2001; 12:294–299.
3. Huang D. Physics of customized corneal ablation. In: MacRae SM, Krueger RR, Applegate
RA, eds. Customized Corneal Ablation: The Quest for Supervision. Thorofare NJ: Slack, 2001:
51–62.
4. Mrochen M, Kaemmerer M, Seiler T. Wavefront-guided laser in situ keratomileusis: early
results in three eyes. J Refract Surg 2000; 16:116–121.
5. Kaemmerer M, Mrochen M, Mierdel P, Krinke HE, Seiler T. Clinical experience with the
Tscherning aberrometer. J Refract Surg 2000; 16:S584–S587.
6. Krueger RR, Mrochen M, Kaemmerer M, Seiler T. Understanding refraction and accommoda-
tion through “retinal imaging” aberrometry. Ophthalmology 2001; 108:674–678.
7. Artal P. Understanding aberrations by using double-pass techniques. J Refract Surg 2000; 16:
S560–S562.
8. Schwiegerling J. Theoretical limits to visual performance. Surv Ophthalmol 2000; 45(2):139–146.
9. Applegate RA. Limits to vision: Can we do better than nature? J Refract Surg 2000; 16:
S547–S551.
10. Williams D, Yoon GY, Porter J, Guirao A, Hofer H, Cox I. Visual benefit of correcting higher
order aberrations of the eye. J Refract Surg 2000; 16:S554–S559.
11. Thibos LN. The prospects for perfect vision. J Refract Surg 2000; 16:S540–S546.
12. Thibos L. Wavefront data reporting and terminology. J Refract Surg 2001; 17:S578–S583.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 172/338
161Wavefront Changes After Hyperopia Surgery
13. Oshika T, Klyce SD, Applegate RA, Howland HC, Danasoury MAE. Comparison of corneal
wavefront aberrations after photorefractive keratectomy and laser in situ keratomileusis. Am
J Ophthalmol 1999; 127:1–7.
14. Mrochen M, Kaemmerer M, Mierdel P, Seiler T. Increased higher-order optical aberrationsafter laser refractive surgery. A problem of subclinical decentration. J Cataract Refract Surg
2001; 27:362–369.
15. Mrochen M, KaemmererM, Seiler T. Clinical resultsof wavefront-guided laser in situ keratom-
ileusis 3 months after surgery. J Cataract Refract Surg 2001; 27:201–207.
16. Howland HC. The history and methods of ophthalmic wavefront sensing. J Refract Surg 2000;
16:S552–S553.
17. Mrochen M, Kaemmerer M, Mierdel P, Krinke HE, Seiler T. Principles of Tscherning aber-
rometry. J Refract Surg 2000; 16:S570–S571.
18. Platt BC, Shack R. History and principles of Shack-Hartmann wavefront sensing. J Refract
Surg 2001; 17:S573–S577.
19. Krueger RR. Technology requirements for Summit-Autonomus CustomCornea. J Refract Surg
2000; 16:S592–S601.
20. Thibos L. Principles of Shack-Hartmann aberrometry. J Refract Surg 2000; 16:S563–S565.
21. Roberts C, Dupps Jr WJ. Corneal biomechanics and their role in corneal ablative procedures.In: MacRae SM, Krueger RR, Applegate RA eds. Customized Corneal Ablation: The Quest
for Supervision. Thorofare, NJ: Slack, 2001:109–131.
22. Argento CJ, Consentino MJ. Laser in situ keratomileusis for hyperopia. J Cataract Refract
Surg 1998; 24:1050–1058.
23. McDonald M. Summit—Autonomus CustomCornea Laser in situ keratomileusis outcomes. J
J Refract Surg 2000; 16:S617–S618.
24. Pettit GH, Campin J, Liedel K, Housand B. Clinical experience with the CustomCornea mea-
surement device. J Refract Surg 2000; 16:S581–S583.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 173/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 174/338
16
Contrast Sensitivity Changes AfterHyperopia Surgery
LAVINIA C. COBAN-STEFLEA
Bucharest University Hospital and Carol Davila University of Medicine and
Pharmacy, Bucharest, Romania
TOMMY S. KORN
University of California–San Diego and Rees-Stealy Medical Group, San Diego,
California, U.S.A.
BRIAN S. BOXER WACHLER
Boxer Wachler Vision Institute, Beverly Hills, California, U.S.A.
A. INTRODUCTION
Understanding the importance of contrast sensitivity can be easier if we emphasize its
relationship to spatial vision, which is the core of the visual perception (1). Spatial fre-
quency theory of image processing is based on spatially extended patterns called sinusoidal
gratings, which are characterized by four parameters: spatial frequency, orientation, ampli-
tude, and phase. The contrast sensitivity function is a measure of the observer’s sensitivity
to gratings at different frequencies and is determined by the lowest contrast at which the
sinusoidal gratings can still be detected (2). Over 200 years ago, contrast sensitivity began
to be acknowledged as a clinical tool for doctors in studying visual disorders (3). In
1760 Bouguer defined and gave a value to the term light-difference threshold , the first
denomination of contrast threshold. Since then other researchers have made a great numberof contributions to this field: Bjerrum (1884) with letter charts, the first low-contrast letter
acuity tests, and Young (1918) with the ink spot test, an easy method to measure the light-
difference threshold. More recently Schade (1956) applied his knowledge of television
technology to contrast sensitivity testing. The work of Campbell and Green contributed
to a better understanding of the optical and neural mechanism of contrast sensitivity testing
and inspired further studies regarding alterations of contrast sensitivity in ocular diseases.
163

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 175/338
164 Coban-Steflea et al.
Correction of hyperopia has been a constant concern of ophthalmologists over the
past decades. Some of the surgical procedures that have been developed—hexagonal
keratotomy (4,5), keratophakia, keratomileusis, and epikeratophakia (6–9)—have been
abandoned because of limited applicability or side effects. Among current corrective proce-
dures undoubtedly laser-assisted in situ Keratomileusis (LASIK) and Ho:YAG laser ther-
mal keratoplasty (LTK) are the most widespread. Recently published clinical results em-
phasize the fact that LASIK is a procedure with good predictability, stability, efficacy,
and safety for the correction of low to moderate spherical hyperopia (10). Long-term
predictability with occurrence of undercorrection is influenced by the preoperative kerato-
metric values and ablation zone diameter (11). Other studies point out the importance of
corneal thickness and width of the flap for LASIK feasibility (12). The effectiveness of
LASIK for severe hyperopia and hyperopic astigmatism is reduced (13,14). For treatments
over 5.00 D, the incidence of loss of best-corrected visual acuity was increased. Current
nomograms require the cut of a larger flap in order to enlarge the ablation zone and to
decrease the risk of halos, glare, and night vision difficulties for patients with high hyper-
opia and astigmatism (15). A lower predictability for astigmatic corrections was alsoreported after LASIK for myopia (16) in spite of in situ axis alignment (17,18). Encourag-
ing results have been reported with respect to the safety, predictability, and stability of
LASIK correction, for small degrees of hyperopia that were secondary to previous radial
keratotomy (RK), and for automated lamellar keratoplasty (ALK) (19). The degree of
regression after H-LASIK was reported to be higher relative to myopic corrections but
lower, even in high hyperopia, than with the PRK procedure (20). Flap irregularities,
epithelium, infection, or nonspecific inflammation at the flap interface have been reported
complications of the LASIK procedure (21). Loss of vision can occur in cases of button-
holes, free cap, or amputation of the flap (22).
Correction of hyperopia and astigmatism by thermal keratoplasty was reported more
than 100 years ago (23–25). The actual mechanism by which this procedure alters the
anterior corneal curvature has been clarified with the discovery of shrinkage temperature
of corneal collagen by Stringer and Parr (26). In 1970s and 1980s, keratoconus was thefocus of theromokeratoplasty technology. A number of clinical studies done have evaluated
thermal keratoplasty potential to replace penetrating keratoplasty in keratoconus treatment
(27–30). In spite of the fact that initial flattening of the cone followed the procedure,
regression occurred within a few weeks postoperatively. It was not uncommon for these
keratoconus treatments to be accompanied by complications such as corneal scarring,
vascularization, and bullous keratopathy. Additionally, poor predictability and stability
contributed to the withdrawing of the procedure from clinical use for keratoconus.
A more recent approach to thermal keratoplasty is credited to Fyodorov, who devel-
oped a technique, using controlled thermal burns of corneal stroma with a retractable probe
tipheated to 600ЊC and applied in a radial pattern. The procedure was eventually abandoned
because of the high incidence of postoperative regression (31). In spite of repeated chal-
lenges to achieve predictable and stable refractive outcomes, researchers did not give up
on probe technology but took another avenue, which was the use of lasers to delivercontrollable amounts of energy to the stroma.
Lasers such as continuous CO2 and cobalt magnesium fluoride have been used in
experimental studies on rabbit corneas, with transient results (32,33). Reports of clinical
studies that used the erbium:glass laser (34) have shown good results for hyperopia higher
than 3.00 D. Over the past decade, ophthalmologists in the United States have directed
their work at evaluating two Ho:YAG laser systems: the noncontact system (Sunrise Tech-

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 176/338
165Changes After Hyperopia Surgery
nologies, Fremont, CA) and the contact system (Summit Technologies, Waltham, MA).
The Sunrise Ho:YAG is a pulsed laser that emits laser light at a wavelength of 2.13 m.
Other technical characteristics include pulse repetition frequency of 5 Hz and pulse energy
in the range of 226 to 258 in correlation with the amount of refractive correction required.
The energy is applied to the cornea in a noncontact mode through a fiberoptic slit-lamp
system; the treatment pattern is represented by rings of spots concentric to the pupil (35).
Sand, who was granted a patent for performing infrared LTK, was an important contributor
to the development of this technology. Initial in vitro investigations have been made on
swine and human cadaver eyes (36,37) in an attempt to establish a treatment protocol.
Further studies done on human poorly sighted eyes showed a mean change in corneal
curvature of 1.10 D followed by some amounts of regression (38). Results of clinical trials
done outside the United States, which used the eight-spot treatment pattern applied at
different diameters (6, 7, or 8 mm), had shown that the procedure works best up to 3.00
D. They also proposed a treatment algorithm adjusted to variables such as age and central
corneal thickness (39). Other studies have demonstrated that the amount of refractive
change is increased when a two-ring treatment is applied at the 6- and 7-mm center linein a radial instead of a staggered pattern (40,41). The U.S. phase III study protocol has
defined the efficacy criteria for the LTK procedure as improvement in distance UCVA
and reduction in hyperopia manifest refraction spherical equvalent (MRSE) Ͼ 0.5 D.
Evaluation at 2 years showed that 69.4% of patients had more than two lines of improve-
ment in distance uncontrolled visual acuity (UCVA) and no eyes had lost more than two
lines of best spectacle corrected visual acuity (BSCDVA) (35).
B. CONTRAST SENSITIVITY IN LASIK AND LTK
In understanding the outcomes of contrast sensitivity, we conducted a study to evaluate
the quality of vision through its changes in LASIK and noncontact Ho:YAG LTK for the
correction of low to moderate spherical hyperopia. We analyzed the results of two groups
of patients who had LASIK and LTK, respectively, as primary procedures. There was nohistory of ocular diseases or surgery. We compared best-corrected contrast sensitivity
values preoperatively and at 3 months postoperatively. Contrast sensitivity was measured
with the self-calibrated, internally luminated CSV-1000E Vector Vision (Dayton, OH) at
12 cycles per degree (cpd) spatial frequency. The patient was instructed to identify whether
the bars were in the top circle, bottom circle, or neither. The last correct identification
has been taken as the contrast sensitivity. On the contrast sensitivity chart the numbers
represent normalized ratios where values greater than 1.0 correspond to percent contrasts
sensitivity above the population average and values below 1.0 represent percent of the
average contrast sensitivity below the population average (42). Visual acuity was measured
with the Vector Vision acuity chart using a scoring method of the U.S. Food and Drug
Administration for refractive surgery clinical trials (43). All visual function tests were
done with best spectacle-corrected visual acuity.
Data were analyzed with the StatView (SAS Institute Inc., Cary, NC) statisticalpackage. Visual acuity data were analyzed in logMAR values. Normalized contrast sensi-
tivity values were converted to log values and used for statistical analysis.
The LASIK study group comprised 94 eyes of 49 patients, 21 men and 28 women.
Mean patient age was 59.67 years 7.95 SD, range 44 to 78 years. Preoperatively, mean
deviation from target manifest refraction was 2.4 D 1.2 D, SD, (range 0.37 to
5.60 D). LASIK procedures were performed by the same surgeon (B.B.W.) using the

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 177/338
166 Coban-Steflea et al.
Table 1 H-LASIK Group—Preoperative and Postoperative Log Contrast Sensitivity Values and
Best Spectacle-Corrected LogMAR Visual Acuity Values
Mean Standard deviation Minimum Maximum
Preop log CS 1.30 0.22 0.61 1.69
Postop log CS 1.23 0.27 0.61 1.54
Preop logMAR VA Ϫ0.01 0.08 Ϫ0.20 0.20
Postop logMAR VA 0.02 0.10 Ϫ0.20 0.50
Moria LSK (Doylestown, PA) microkeratome and the Summit Apex Plus Laser (Summit
Technology Inc., Waltham, MA); the treatment zone was centered on the pupil. Results
have shown a mean postoperative deviation from target manifest refraction of 0.09 D
0.88 D, SD, (range 2.25 to 2.00 D) at 3 months. Table 1 shows the mean preopera-tive and postoperative log contrast sensitivity values, standard deviations, and maximum
and minimum values. At 3 months postoperatively the mean log contrast sensitivity value
was not statistically significantlydifferent compared to preoperative levels ( p 0.18). The
mean best spectacle-corrected logMAR visual acuity value at 3 months was statistically
significantly worse relative to preoperative value ( p 0.008). However, the change was
not clinically significant, as the logMAR conversion was a loss of 1.5 letters on the acuity
chart. There was a statistically significant correlation between achieved refraction and
changes in log contrast sensitivity values ( p 0.006) (Fig. 1) (r 0.29, p 0.006).
This indicated that higher amounts of hyperopic correction were associated with greater
loss of best-corrected contrast sensitivity. No statistically significant correlation was ob-
Figure 1 Correlation between changes in log contrast sensitivity values and achieved refraction
in the H-LASIK group.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 178/338
167Changes After Hyperopia Surgery
Figure 2 Correlation between changes in best spectacle-corrected logMAR visual acuity values
and achieved refraction in the H-LASIK group.
servedbetween achieved refractionandchanges in best spectacle-corrected logMARvisual
acuity (r 0.05, p 0.58)(Fig. 2).
The LTK study group comprised 55 eyes of 35 patients, 16 males and 19 females.
Mean patient age was 57.61 years 7.35, SD, with a range of 39 to 71 years; mean
deviation from target manifest refraction of treated eyes was 1.5 D 0.59 D, SD, range
0 to 3.00 D. Noncontact Ho:YAG LTK treatments were performed by the same surgeon
(B.B.W.) using the Sunrise Hyperion Holmium Laser Corneal Shaping System (Sunrise
Technologies Inc., Fremont, CA). The treatment was centered on the corneal purkinje
image of the patient fixation light. The light reflex closely approximates the visual axis.Therefore, in cases of positive angle kappa, the treatment was not centered on the pupil.
Laser parameters included wavelength, 2.13 m; pulse duration, 250 s; pulse repetition
frequency, 5 Hz; pulse energy, adjustable from 226 to 258 mJ/pulse. In the current study
we used a two concentric radial 8-spot ring treatment pattern centered around the fixation
light reflex on the cornea. Postoperatively, results showed a mean deviation from target
manifest refraction of 0.36 D 0.84 D, SD, range 3.50 to 1.25 D. Mean log
contrast sensitivity value was not statistically significantly decreased ( p 0.07) (Table
2) and mean best spectacle-corrected logMAR visual acuity value was statistically signifi-
Table 2 LTK Group—Preoperative and Postoperative Log Contrast Sensitivity Values and Best
Spectacle-Corrected LogMAR Visual Acuity Values
Mean Standard deviation Minimum Maximum
Preop log CS 1.28 0.24 0.61 1.69
Postop log CS 1.19 0.29 0 1.84
Preop logMAR VA Ϫ0.01 0.08 Ϫ0.2 0.2
Postop logMAR VA 0.04 0.11 Ϫ0.1 0.6

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 179/338
168 Coban-Steflea et al.
Figure 3 Correlation between changes in log contrast sensitivity values and achieved refraction
in the LTK group.
cantly worse ( p 0.0067) relative to preoperative values. The change in acuity was not
clinically significant as the change represented approximately four letters on the acuity
chart. No statistically significant correlation ( R 0.16, p 0.25) was found between
achieved refraction and changes in log contrast sensitivity values (Fig. 3). Figure 4 shows
the lack of correlation between achieved refraction and best-spectacle corrected logMAR
visual acuity values (r 0.15, p 0.26).
Figure 4 Correlation between changes in best spectacle-corrected logMAR visual acuity values
and achieved refraction in the LTK group.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 180/338
169Changes After Hyperopia Surgery
C. DISCUSSION
As new surgical procedures are added to the refractive surgery armamentarium, assessing
visual outcome becomes more difficult. Information regarding postoperative visual acuityand refractive changes is no longer satisfactory to evaluate the quality of the image
projected on the retina (44). Contrast sensitivity, as a functional method, has been shown
to be directly affected by the distorted image following excimer laser surgery (45). Using
digitized retroillumination, Vinciguerra has shown that corneal distortion arising from
prominent flap striae may be overlooked by the customary slit-lamp examination (46).
Our results have shown a slight decrease in contrast sensitivity at 12 cpd spatial frequency
postoperatively after LASIK procedure. However the difference was not statistically signif-
icantly different ( p 0.18). Previous literature data that have demonstrated that spatial
frequency of 12 cpd is mostly affected by degradation in optics, such as aberration or blur
(47). Other studies reported a loss of contrast sensitivity at 12 months after LASIK of up
to one line for low hyperopia and of more than two lines for high hyperopia with no
statistical significance (13). An interesting finding in the LASIK group was the significant
correlation between achieved refraction and change in contrast sensitivity, demonstratingthat larger amounts of correction are accompanied by larger loss of contrast sensitivity.
This indicates that with the Summit Apex Plus laser used for LASIK and centered on the
pupil, higher degrees of hyperopic treatment as associated with a higher risk of loss of
best-corrected contrast sensitivity.
Contrast sensitivity showed little change after the LTK procedure. The minimal
decrease observed was not statistically significant ( p 0.07). Furthermore, contrast sensi-
tivity changes showed no correlation with the amount of spherical correction attempted.
Clinical trials at 1 and 2 years after LTK reported that mean contrast sensitivity increased
at all follow-up visits for the two-ring treatment group at Regan charts (40,48). Postopera-
tively visual acuity did not vary significantly ( p 0.0067) and was not influenced by
the amount of correction, although the amount of hyperopia corrected in the LTK group
was less than that corrected in the LASIK group.
We conclude that measuring contrast sensitivity after refractive surgical procedures
should be encouraged and further developed in order to assess the limits of safety for
given procedures and devices used for such procedures. Studies should be directed at
identifying laser characteristics and treatment patterns that are able to optimize the optical
system of the eye, thus increasing safety.
REFERENCES
1. Palmer SE. Vision Science— Photons to Phenomenology. Cambridge, MA: MIT Press, 1999:
146–198.
2. Blakemore C, Campbell FW. Onthe existence of neurons in thehuman visual system selectively
responsive to the orientation and size of retinal images. J Physiol 1969; 203:237–260.
3. Shapley R, Man-Kit Lam D. Contrast Sensitivity: Proceedings of the Retina Research Founda-tion Symposia. Vol. 5. Cambridge, MA: MIT Press, 1993: 253–266.
4. Werblin TP. Hexagonal keratotomy. Should we still be trying? J Refract Surg 1996; 12:
613–620.
5. Grandon SC, Sanders DR, Anello RD, Jacobs D, Biscaro M. Clinical evaluation of hexagonal
keratotomy for the treatment of primary hyperopia. J Cataract Refract Surg 1995; 21:140–149.
6. Swinger CA, Barraquer JI. Keratophakia and keratomileusis—clinical results. Ophthalmology
1981; 88:709–715.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 181/338
170 Coban-Steflea et al.
7. Barraquer JI. Keratomileusis. Int Surg 1967; 48:103–117.
8. Morgan KS, Stephenson GS, McDonald MB, Kaufman HE. Epikeratophakia in children. Oph-
thalmology 1984; 91:780–784.
9. Anshutz T. Laser correction of hyperopia and presbyopia. In: ed. International OphthalmologyClinics. Refractive Surgery. Boston: Little, Brown, 1994:107–137.
10. Boxer Wachler BS, O’Brien TP, Tauber S. Vision Correction—Seeing the Future. Current
Laser Refractive and Surgical Alternatives for the Correction of Hyperopia. Oxford Institute
for Continuing Education, 2000:3–5.
11. Esquenazi S, Mendoza A. Two-year follow-up of laser in situ keratomileusis. J Refract Surg
1999; 15:648–652.
12. Rosa JL, Febbraro DS. Laser in situ keratomileusis for hyperopia. J Refract Surg 1999; 5(2
suppl):S212–S215.
13. Arbelaez MC, Knorz MC. Laser in situ keratomileusis for hyperopia and hyperopic astigma-
tism. J Refract Surg 1999; 15:406–414.
14. Barraquer C, Gutierrez AM. Results of laser in situ keratomileusis in hyperopic compound
astigmatism. J Cataract Refract Surg 1999; 25:1198–1204.
15. Lipner M. Distant visions: how practitioners outside the United States are treating hyperopia.
Eye World 1999; 4:17–18.
16. Knorz MC, Wiesinger B, Liebermann A, Seiberth V, Liesenhoff H. Laser in situ keratomileusis
for moderate and high myopia and myopic astigmatism. Ophthalmology 1998; 105:932–940.
17. Stevens JD. Astigmatic excimer laser treatment: theoretical effects of axis misalignment. Eur
J Implant Ref Surg 1994; 6:310–318.
18. Vajpayee RB, McCarthy CA, Taylor HR. Evaluation of axis alignment system for correction
of myopic astigmatism with the excimer laser. J Cataract Refract Surg 1998; 24:911–916.
19. Buzard KA, Fundingsland BR. Excimer laser assisted in situ keratomileusis for hyperopia. J
Cataract Refract Surg 1999; 25:197–204.
20. Reviglio VE, Luna JD, Rodriguez ML, Garcia FE, Juarez CP. Laser in situ keratomileusis
using the LaserSight 200 laser: results of 950 consecutive cases. J Cataract Refract Surg 1999;
25:1062–1068.
21. Wilson SE. LASIK: management of common complications (review). Cornea 1998; 17:
459–467.
22. Farah SG, Azar DT, Gurdal C, Wong J. Laser in situ keratomileusis: literature review of a
developing technique (review). J Cataract Refract Surg 1998; 24:989–1006.
23. Lans LJ. Experimentelle Untersuchungen uber die Entstehung von Astigmatismus durch nicht-
perforierende Corneawunden. Graefes Arch Clin Exp Ophthalmol 1898; 45:117–152.
24. Wray C. Case of 6 D of hypermetropic astigmatism cured by the cautery. Trans Ophthalmol
Soc UK 1914; 34:109–110.
25. O’Connor R. Corneal cautery for high myopic astigmatism. Am J Ophthalmol 1933; 16:337.
26. Striger H, Parr J. Shrinkage temperature of eye collagen. Nature 1964; 204:1307.
27. Gasset AR. Thermokeratoplasty in the treatment of keratoconus. Am J Ophthalmol 1975; 79:
226–232.
28. Aquavella JV, Buxton JN, Shaw EL. Thermokeratoplasty in the treatment of persistent corneal
hydrops. Arch Ophthalmol 1977; 95:81–84.
29. Itoi M. Computer photokeratometry changes following thermokeratoplasty. In: Schachar RA,
Levy NS, Schachar L, eds. Refractive Modulation of the Cornea. Denison, TX LAL Publishers,1981.
30. Rowsey JJ, Doss JD. Preliminary report of Los Alamos keratoplasty techniques. Ophthalmol-
ogy 1981; 88:755–760.
31. Caster AI. The Fyodorov technique of hyperopia correction by thermal coagulation: a prelimi-
nary report. J Refract Surg 1988; 4:105–108.
32. Peyman GA, Larson B, Raichand M, Andrews AH. Modification of rabbit corneal curvature
with use of carbon dioxide laser burns. Ophthalmic Surg 1980; 11:325–329.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 182/338
171Changes After Hyperopia Surgery
33. Horn G, Spears KG, Lopez O, Lewicky A, Yang X, Riaz M, Wang R, Silva D, Serafin J.
New refractive method for laser thermal keratoplasty with the Co: MgF2 laser. J Cataract
Refract Surg 1990; 16:611–616.
34. Kanoda AN, Sorokin AS. Laser correction of hypermetropic refraction. In: Fyodorov SN, ed.Microsurgery of the Eye: Main Aspects. Moscow: MIR Publishers, 1987:147–154.
35. Aker AB, Boxer Wachler BS, Brown DC. Vision Correction—Seeing the Future. Noncontact
Holmium:YAG Laser Thermal Keratoplasty for the Treatment of Hyperopia. Oxford Institute
for Continuing Education, 2000:3–5.
36. Koch DD, Berry MJ, Vassiliadis AJ, Abarca AA, Villarreal R, Haft EA. Noncontact holmium:
YAG laser thermal keratoplasy. In: Salz JJ, ed. Corneal Laser Surgery. Philadelphia: Mosby,
1995:247–254.
37. Moreira H, Campos M, Sawusch MR, McDonnell JM, Sand B, McDonnell PJ. Holmium laser
thermokeratoplasty. Ophthalmology 1993; 100:752–761.
38. Ariayasu RG, Sand B, Menefee R, Hennings D, Rose C, Berry M, Garbus JJ, McDonnell PJ.
Holmium laser thermal keratoplasty of 10 poorly sighted eyes. Refract Surg 1995; 11:358–365.
39. Alio JL, Ismail MM, Sanchez Pego JL. Correction of hyperopia with noncontact Ho:YAG
laser thermal keratoplasty. J Refract Surg 1997; 13:17–22.
40. Koch DD, Kohnen T, McDonnell PJ, Menefee RF, Berry MJ. Hyperopia correction by noncon-tact holmium:YAG laser thermal keratoplasty. US phase IIA clinical study with a 1-year
follow-up. Ophthalmology 1996; 103:1525–1536.
41. Vinciguerra P, Kohnen T, Azzolini M, Radice P, Epstein D, Koch DD. Radial and staggered
patterns to correct hyperopia using noncontact holmium:YAG laser thermal keratoplasty. J
Cataract Refract Surg 1998; 24:21–30.
42. Boxer Wachler BS, Kruger RR. Normalized contrast sensitivity: a new notation for mainstream
contrast sensitivity testing in refractive surgery. Invest Ophthalmol Vis Sci 1997; 38:530.
43. Boxer Wachler BS, Durrie DS, Assil KK, Kruger RR. Role of clearance and treatment zones
in contrast sensitivity: significance in refractive surgery. J Cataract Refract Surg 1999; 25:
16–23.
44. Pallikaris IG. Quality of vision in refractive surgery. J Refract Surg 1998; 14:551–557.
45. Boxer Wachler BS, Frankel RA, Kruger RR, Durrie DS, Assil KK. Contrast sensitivity and
patient satisfaction following photorefractive keratectomy and radial keratotomy. Invest Oph-
thalmol Vis Sci 1996; 37(suppl):S19.
46. Vinciguerra P, Azzollini M, Radice P. A new corneal analysis after excimer laser ablation:
digitized retroillumination. In: Pallikaris IG, Siganos DS, eds. LASIK. Thorofare, NJ: Slack,
1997:331–337.
47. Campbell FW, Green DS. Optical and retinal factors affecting visual resolution. J Physiol
1965; 181:576–593.
48. Koch D, Abarca A, Villarreal R, Menefee R, Kohnen T, Vassiliadis A, Berry M. Hyperopia
correction by noncontact holmium:YAG laser thermal keratoplasty. Clinical study with two-
year follow-up. Ophthalmology 1996; 103:731–740.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 183/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 184/338
17
Wound Healing After HyperopicCorneal Surgery
Why There Is Greater Regression in theTreatment of Hyperopia
RENATO AMBRO SIO, JR.
University of Washington, Seattle, Washington, U.S.A., University of Sa o Paolo,
Sa o Paolo, and Clınica e Microcirurgia Oftalmologica Renato Ambrosio, Rio de
Janeiro, Brazil
STEVEN E. WILSON
University of Washington, Seattle, Washington, U.S.A.
A. INTRODUCTION
Biological diversity in the corneal wound-healing response is a major factor in the out-
comes of all keratorefractive surgical procedures (1,2). It is one of the most important
determinants for overcorrection, undercorrection, and other complications, such as haze
(3) and irregular astigmatism, which occur with laser-assisted in situ keratotomileusis
(LASIK) and photorefractive keratectomy (PRK) in the treatment of myopia (4,5), hyper-
opia (6,7), or astigmatism (8,9).
This response is very similar in different species, facilitating the creation of animal
models for better characterization of the wound-healing response. There are quantitative
and qualitative variations in specific processes that comprise the cascade. There is also
variability depending on the inciting injury within a species. For example, thermal, inci-sional, lamellar, and surface scrape injuries are followed by wound-healing responses that
are similar in some respects but different in others.
Corneal wound healing following correction of hyperopia may be more complex
than that associated with corrections of myopia (10). Steepening of the central cornea is
required for hyperopic treatments. This leads to the creation of a corneal contour with a
steeper central area and a flatter paracentral area.
173

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 185/338
174 Ambrosio and Wilson
Refractive regression is defined as a gradual, partial, or total loss of the initial
correction. It limits the predictability of all refractive surgery procedures performed on
the cornea. It has been hypothesized that changes occurring as a result of corneal wound
healing lead to addition of new tissue. Epithelial hyperplasia and stromal remodeling are
the two mechanisms that are thought to underlie this phenomenon (3,11,12).
1. Keratocytes Disappear in Response to Epithelial
Injury—Keratocyte Apoptosis
One of the earliest observations that debunked the prior dogma regarding the quiescence
of keratocytes was detection of disappearance of superficial keratocytes following corneal
epithelial scrape injury. This observation was made first by Dohlman and coworkers in
1968 (16). Studies by later investigators confirmed that keratocytes in the anterior stroma
disappear following corneal epithelial scrape injury (17–20) as well as thermokeratoplasty
(21). The mechanism of disappearance of the keratocytes was not elucidated in these
studies. The authors of these studies suggested that the disappearance of the keratocyteswas attributable to several factors, such as osmotic changes from the loss of epithelium,
exposure to the atmosphere, or even artifact.
In 1996, Wilson and coworkers (20) first demonstrated that the early disappearance
of keratocytes that follows epithelial injury is mediated by apoptosis (13–15,22–29). Cell
shrinkage, blebbing with formation of membrane bound bodies, condensation, fragmenta-
tion of the chromatin, and DNA fragmentation consistent with apoptosis were detected
in anterior stromal keratocytes after epithelial scrape wounds by transmission electron
microscopy. Nuclear DNA fragmentation was confirmed by the TUNEL assay for 3′-
hydroxyl DNA ends.
Apoptosis is a programmed form of cell death that occurs without the release of
lysosomal enzymes or other intracellular components that could damage the surrounding
tissue or cells. Uncontrolled release of cellular contents is characteristic of necrotic cell
death (26). Studies have suggested that apoptosis is mediated by cytokines released from
the injured epithelium, such as interleukin 1 (IL-1) (22), the Fas/Fas ligand system (27),
bone morphogenic proteins (BMP) 2 and 4 (28), or tumor necrosis factor (TNF) alpha
(29).
Virtually any type of epithelial injury induces keratocyte apoptosis. These include
mechanical scrapes (22–25), corneal surgical procedures like PRK and LASIK (24), herpes
simplex keratitis (14), incisions (25), and even a plastic ring pressed firmly against the
epithelial surface (24).
Keratocytes undergo apoptosis after epithelial injury to a depth of one-third to one-
half the stromal thickness, depending on the species and the type of injury. Cellular pro-
cesses, known as gap junctions, connect keratocytes in the unwounded cornea to form a
syncytium (31,32). It is possible that signals transmitted by cytokines to the most superficial
keratocytes are relayed to deeper keratocytes via these intercellular communication chan-nels. Alternatively, the proapoptotic cytokines may penetrate into the stroma after injury.
The keratocyte apoptosis response in the stroma varies with the type of corneal
epithelial injury (25). Thus, injuries such as scraping of the epithelium (25) or viral infec-
tion of the epithelium (14) triggers keratocyte apoptosis in the superficial stroma. A lamel-
lar cut across the cornea produced by a microkeratome also induces keratocyte apoptosis.
This can be detected at the site of epithelial injury and along the lamellar interface (Figure

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 186/338
175Wound Healing After Corneal Surgery
Figure 1 (A) Apoptosis detected along the lamellar interface by TUNEL assay in rabbit eye that
had LASIK and (B) on the surface in rabbit eye that had PRK.
1). Localization of keratocyte apoptosis in LASIK is thought to be attributable to trackingof epithelial material, including proapoptotic cytokines, into the interface by the microkera-
tome blade (22–25). Alternatively, cytokines from the injured peripheral epithelium could
diffuse along the lamellar interface and into the central stroma (22–25).
Apoptosis has also been correlated with severe complications. Meitz et al. (33)
reported a severe case of acute corneal necrosis following PRK for hyperopia that required
penetrating keratoplasty. Histopathological studies of the excised tissue were negative for
micro-organisms. Utilizing light microscopy, an anterior zone of corneal necrosis was
found to be present, with a moderate amount of acute inflammation at the interface between
necrotic and viable corneal stroma; in addition, keratocytes with typical features of
apoptosis were detected by TUNEL assay and electron microscopy (Figure 2).
2. Keratocyte Proliferation and Migration: Myofibroblasts
After the loss of keratocytes caused by apoptosis within the first few hours of corneal
epithelial injury, there will be an area of stroma devoid of keratocytes. Zieske and cowork-
ers (34) demonstrated that remaining keratocytes in the posterior and peripheral cornea
begin to undergo mitosis about 12 to 24 hours after the injury (34). Keratocyte mitosis
can be detected using bromodeoxyuridine incorporation or immunocytochemical staining
for a mitosis-specific antigen called Ki-67 (34).

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 187/338
176 Ambrosio and Wilson
Figure 2 Transmission electron microscopy (TEM) of rabbit cornea, 24 hours after Hi PRK
( 9.0D): Keratocyte apoptosis and a PMN.
The cell types derived from the keratocytes that undergo mitosis following corneal
epithelial injury remain to be completely characterized. Studies have suggested that myofi-
broblasts are an important cell type generated following injury (38–41). These studies,
however, are primarily in vitro tissue culture-based investigations. Little information is
available regarding the fate of the cells that undergo mitosis following PRK (41). Nothing
has been reported about the status of these cells following LASIK.
3. Resolution of The Wound-Healing Response—Return to“Normalcy”
In the months following injury to the cornea, the wound-healing response is completed
and there is a return to normal morphology and function. This process is associated with
elimination of some of the cells associated with wound healing and remodeling of disor-
dered collagen that was produced by myofibroblasts or keratocytes during the wound-
healing process (54–55). This process begins within a few weeks after injury and can
continue for years following severe injury.
The corneal epithelium may undergo hyperplasia following corneal injury (1,56)
as well as refractive surgery (11,12,21,57–59) as a part of the wound-healing response.
Hyperplasia may vary between individuals, the eyes of a single individual, and with differ-
ent types and levels of refractive correction. This is thought to be an important mechanism
for regression of many keratorefractive procedures (1,12,56–59). There may be a return
to a normal epithelial thickness over a period of months to years, and this may result in
instability of the refractive effect of PRK or LASIK. The regulatory mechanisms thatmodulate this return to normal corneal epithelial morphology have not been characterized.
B. CONSIDERATIONS ON HYPEROPIC CORRECTIONS: WHY ARETHEY DIFFERENT FROM MYOPIC CORRECTIONS?
The surgical correction of hyperopia remains challenging, especially for corrections greater
than 4 to 5 D. While corneal surgery for myopia requires flattening the cornea with an

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 188/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 189/338
178 Ambrosio and Wilson
there was better predictability and stability than with an ablation zone of 5.5 9.0 mm
(70). One possible explanation for this observation is that the corneal flap size may have
been smaller than the periphery of the hyperopic treatment. In such settings, a smaller
ablation zone may be preferable.
Excimer laser surgery for hyperopia may induce more astigmatism than for myopia.
Significant change in the astigmatism power and axis was noted 3 months following
hyperopic spherical LASIK in a two-step approach for treating hyperopic or mixed astig-
matism (71). This could be related to centration issues in the treatment of hyperopia relative
to myopia.
Attempts to shrink the peripheral corneal collagen with thermal energy (thermokera-
toplasty) were first reported by Lans over a century ago (72). Central steepening of the
cornea is achieved by thermal shrinkage of the midperipheral corneal tissue. The use of
different types of lasers and radiofrequency energy in the corneal stroma to shrink the
collagen lamellae is an active topic of study and is discussed elsewhere in this book.
Recent reports have shown that these procedures may be effective in correcting low hyper-
opia, although corrections were subject to regression (73). Age-dependent corneal factorswere shown to influence the effectiveness of thermal energy on stromal collagen and
regression (74). Stability following thermokeratoplasty may be related to the type of lesion
produced. A perfect thermal lesion, delivered at the perfect depth, with a perfect geometry,
and for the perfect length of time would cause a permanent change in the collagen fibers
in the cornea, so that regression would be less likely to occur. It remains to be seen whether
such a “perfect thermal lesion” that is permanent can be created or whether ever-vigilant
keratocytes will eventually detect these anomalies in the collagen fibers and repair them.
Corneal iron pigmentation lines or rings can be observed after hyperopic corneal
surgery (75–78). Corneal iron deposition has been seen in the normal cornea with aging
(Hudson-Stahli line) and in pathological corneal conditions such as keratoconus (Fleischer
ring), pterygia (Stocker-Busacca line), and filtering blebs (Ferry’s line). Stellate iron lines
were also described after radial keratotomy (79) and in cases of central island (80). The
most likely explanation for the formation of such lines is that the iron is derived from thetear film and deposited in the corneal epithelium in those areas where there is tear pooling.
Since keratorefractive procedure for hyperopia sculpts the cornea to resemble a convex
lens, a furrow-like ring zone in the corneal periphery is produced. This can be observed
when looking at the corneal elevation map after H-LASIK. (Figure 4). Tear pooling occurs
and subsequently triggers iron deposition. It may also prolong the exposure time to tear
film cytokines (81,82) causing epithelial hyperplasia in this midtransition zone (junction
of the optical and ablated zones) (11).
C. MECHANISMS OS REGRESSION
A complete understanding of the mechanisms underlying regression after keratorefractive
surgery in vivo require the study of the wound-healing response and factors related to
biomechanics. A thorough understanding of corneal microstructure can now be obtainedusing new methods. High-frequency (50-MHz) ultrasound biomicroscopy (UBM and
VHF) (83–86) (Figure 5) and optical coherence tomography (OCT) (87–89) are two
promising technologies that have the capacity to measure the thickness of each layer within
the cornea. These measurements could help us to distinguish between epithelial hyperplasia
and stromal remodeling as the cause of the refractive regression in individual eyes. Confo-
cal microscopy allows for optical sectioning through intact living cornea, obtaining images

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 190/338
179Wound Healing After Corneal Surgery
Figure 4 Elevation map before and after hyperopic LASIK.
of the cornea at its cellular level in four dimensions ( x , y, z, and t -time) (3,10,90,91). It
has been difficult, however, to obtain reliable measurements of epithelial thickness using
this technology. Slit-based videokeratography instruments like the Orbscan (Bausch &
Lomb, Orbtek, Inc., Salt Lake City, UT) may be useful for assessing pachymetric values
through the entire cornea as well as for measuring posterior curvature (92,93). However,
uncertainty regarding the meaning of values derived from the posterior surface of the
cornea is a limiting factor. Studies have shown that corneal thickness measurements are
inaccurate with this instrument (94,95). At the present time, therefore, it appears that
high-frequency ultrasound or OCT provides the best opportunity for monitoring epithelial
thickness following refractive surgery procedures. Studies are in progress using thesemethods.
Animal model studies have been performed to characterize corneal wound healing
following surgery for hyperopia (11,21,96–99). It is important to recognize the possible
limitations of the rabbit model in assessing the nature of the wound-healing response in
humans. Wound healing is thought to be more vigorous in rabbits, and qualitative as well
as quantitative differences may exist. It is feasible to perform studies in patients who

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 191/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 192/338
181Wound Healing After Corneal Surgery
mal regrowth should help to increase our understanding of regression associated with the
laser correction of hyperopia.
Other sources of regression may be a greater than average wound-healing response
in individual patients or variations in surgery that promote increased healing. For example,
a thin flap may be associated with regression, since the stromal wound-healing response
and epithelium-modulating modulating growth factor production are more likely to be in
proximity to the epithelium (13). This is probably a major factor promoting epithelial
hyperplasia. Other factors such as epithelial defects produced by the microkeratome and
diffuse interface keratitis may also be associated with a stronger wound-healing response
and therefore regression. The rate of enhancement in a recent series was significantly
higher (53 versus 16%; p 0.02) following DLK than for eyes that did not have DLK
(Wilson and Ambrosio, unpublished data, 2001). Since the treatment for hyperopia is
typically performed in the periphery of the cornea, closer to the limbus, it is likely that a
stronger inflammatory reaction will follow those surgeries. A study involving an animal
model comparing hyperopic and myopic PRK, using specific antibodies for inflammatory
cells as well as cytokines, might be helpful for elucidating this hypothesis.The higher the level of correction attempted for hyperopia, the more likely regression
due to wound healing will occur. In our experience with hyperopic LASIK and PRK,
regression is most common in eyes where the attempted correction is over 4 to 5 D.
Intraocular pressure could be a factor in the regression of hyperopic LASIK in some
cases with high-pressure increases. A case of acute angle-closure glaucoma was reported
by Paciuc et al. 1 year after hyperopic LASIK (100). The glaucoma attack was treated
with laser peripheral iridotomy and a prophylactic iridotomy was performed in the fellow
eye. Corneal topography was performed 2, 5, and 18 weeks after the acute episode and
a myopic shift occurred in the eye that had angle closure. This resolved over 3 months.
It is important to consider that the eye blinks over 10,000 times per day (101) at lid
velocities up to 30 cm/s (102). Each blink has enough force to raise intraocular pressure
10 to 70 mmHg (103).
Koch and coworkers (21) studied Ho:YAG LTK on three human corneas 1 day
before their removal at penetrating keratoplasty in patients with corneal edema secondary
to Fuchs endothelial dystrophy (without bullous epithelial changes) and on six New
Zealand white rabbit corneas followed for up to 3 months. The pulse radiant energy level
was noted to be proportional to the acute tissue injury. In human corneas, changes in the
irradiated zones included epithelial cell injury and death, loss of fine filamentous structure
in Bowman’s layer, disruption of stromal lamellae, and keratocyte injury and death. A
cone-shaped zone of increased stromal hematoxylin uptake extending posteriorly for 90%
of stromal thickness was noted in the treatment areas. Special immunohistochemical stains
to detect apoptosis were not used, although transmission electron microscopy findings
suggested that they might play a role. In the rabbit corneas, similar acute changes were
noted. By 3 weeks, epithelial hyperplasia and stromal contraction were present. Wound
healing in the rabbits included repair of the epithelial attachment complex, keratocyteactivation, synthesis of type I collagen, and partial restoration of stromal keratin sulfate
and type VI collagen. There was also a marked endothelial proliferative response in the
rabbit corneas. Attempted corrections with LTK of greater than 2 D are associated with
significant regression. This is likely related to stromal remodeling, with the keratocytes
functioning to repair the altered collagen over time.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 193/338
182 Ambrosio and Wilson
D. FUTURE DIRECTIONS AND CONCLUSIONS
The ability to modulate corneal wound healing to achieve better clinical outcomes would
be beneficial to extend the efficacy and safety of keratorefractive corrections of hyperopia.Apoptosis is the first detected event in the complex cascade of the corneal wound healing.
Differences in this initiator and subsequent events in healing between eyes likely is a
major determinant of variation between eyes following laser correction for hyperopia.
Development of methods to control this first event may be useful for normalizing the
response between patients.
A better understanding of the mechanisms associated with regression, especially
differentiating between the key determinants epithelial hyperplasia and stromal remodel-
ing, would provide specific strategies to improve stability.
Corneal implants and inlays may become an option for hyperopic treatment in the
future. New alloplastic materials with acceptable permeability for corneal tissue, with
refractive indices and clarity equal to those of the cornea, may provide a reversible refrac-
tive procedure for hyperopia. Intracorneal lenses with higher refractive indexes than the
cornea and therefore intrinsic refractive power would not rely on changing the cornea’sshape. They could attenuate epithelial hyperplasia as a factor in regression.
Corneal surgery for hyperopia has lagged behind that of myopia primarily due to
issues related to efficacy, stability, and safety. Several procedures were abandoned during
the past decade. Understanding and respecting the limits of the available procedures is
key for achieving success with hyperopic patients. Intraocular procedures for hyperopia,
such as phakic intraocular lenses and clear lens extraction, may have an important role
in treating this group of patients if safety can be improved.
ACKNOWLEDGMENTS
Supported in part by an unrestricted grant from Research to Prevent Blindness, New York,
N.Y., and U.S. Public Health Service grant EY 10056 and EYO1730 from the NationalEye Institute, National Institutes of Health, Bethesda, Maryland.
PROPRIETARY INTEREST STATEMENT
The authors have no proprietary or financial interest in relation to this manuscript.
REFERENCES
1. Wilson SE, Mohan RR, Hong JW, Lee JS, Choi R, Mohan RR. The wound healing response
after laser in situ keratomileusis and photorefractive keratectomy: elusive control of biological
variability and effect on custom laser vision correction. Arch Ophthalmol 2001; 119:889–896.
2. Wilson SE, Mohan RR, Mohan RR, Ambrosio R Jr, Hong J, Lee J. The corneal woundhealing response: cytokine-mediated interaction of the epithelium, stroma, and inflammatory
cells. Prog Ret Eye Res. 2001 9; 20(5):625–637.
3. Moller-Pedersen T, Cavanagh HD, Petroll WM, Jester JV. Stromal wound healing explains
refractive instability and haze development after photorefractive keratectomy: a 1-year confo-
cal microscopic study. Ophthalmology 2000; 107:1235–1245.
4. Kim JH, Kim MS, Hahn TW, Lee YC, Sah WJ, Park CK. Five year results of photorefractive
keratectomy for myopia. J Cataract Refract Surg 1997; 23:731–735.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 194/338
183Wound Healing After Corneal Surgery
5. Shah SS,Kapadia MS,Meisler DM,WilsonSE. Photorefractive keratectomy using the summit
SVS Apex laser with or without astigmatic keratotomy. Cornea 1998; 17:508–516.
6. Esquenazi S, Mendoza A. Two-year follow-up of laser in situ keratomileusis for hyperopia.
J Refract Surg 1999; 15:648–652.7. Zadok D, Maskaleris G, Montes M, Shah S, Garcia V, Chayet A. Hyperopic laser in situ
keratomileusis with the Nidek EC–5000 excimer laser. Ophthalmology 2000; 107:
1132–1137.
8. Hersh PS, Abbassi R. Surgically induced astigmatism after photorefractive keratectomy and
laser in situ keratomileusis. Summit PRK-LASIK Study Group. J Cataract Refract Surg 1999;
25:389–398.
9. KapadiaMS, Krishna R, Shah S, Wilson SE.Surgicallyinduced astigmatism after photorefrac-
tive keratectomy with the excimer laser. Cornea 2000; 19:174–179.
10. Vesaluoma MH, Petroll WM, Perez-Santonja JJ, Valle TU, Alio JL, Tervo TM. Laser in situ
keratomileusis flap margin: wound healing and complications imaged by in vivo confocal
microscopy. Am J Ophthalmol 2000; 130:564–573.
11. Dierick HG, Van Mellaert CE, Missotten L. Histology of rabbit corneas after 10-diopter
photorefractive keratectomy for hyperopia. J Refract Surg 1999; 15:459–468.
12. Lohmann CP, Guell JL. Regression after LASIK for the treatment of myopia: the role of the
corneal epithelium. Semin Ophthalmol 1998; 13:79–82.
13. Wilson SE, Mohan RR, Mohan RR, Ambrosio Jr R, Hong J-W, Lee J-S. The corneal wound
healing response: Cytokine-mediated interaction of the epithelium, stroma, and inflammatory
cells. Prog Ret Eye Res 2001; 20:625–637.
14. Wilson SE, Pedroza L, Beuerman R, Hill JM. Herpes simplex virus type–1 infection of
corneal epithelial cells induces apoptosis of the underlying keratocytes. Exp Eye Res 1997;
64:775–779.
15. Wilson SE. Role of apoptosis in wound healing in the cornea. Cornea 2000; 19(suppl):
S7–S12.
16. Dohlman CH, Gasset AR, Rose J. The effect of the absence of corneal epithelium or endothe-
lium on stromal keratocytes. Invest Ophthalmol Vis Sci 1968; 7:520–534.
17. Nakayasu K. Stromal changes following removal of epithelium in rat cornea.Jpn J Ophthalmol
1988; 32:113–125.
18. Campos M, Szerenyi K, Lee M, McDonnell JM, McDonnell PJ. Keratocyte loss after corneal
deepithelialization in primates and rabbits. Arch Ophthalmol. 1994; 112:254–260.
19. Szerenyi KD, Wang X, Gabrielian K, McDonnell PJ. Keratocyte loss and repopulation of
anterior corneal stroma after de-epithelialization. Arch Ophthalmol 1994; 112:973–976.
20. Polack FM. Keratocyte loss after corneal deepithelialization in primates and rabbits. Arch
Ophthalmol 1994; 112:1509.
21. Koch DD, Kohnen T, Anderson JA, Binder PS, Moore MN, Menefee RF, Valderamma GL,
Berry MJ. Histologic changes and wound healing response following 10-pulse noncontact
holmium: YAG laser thermal keratoplasty. J Refract Surg 1996; 12:623–634.
22. Wilson SE, He Y-G, Weng J, Li Q, Vital M, Chwang EL. Epithelial injury induces keratocyte
apoptosis: hypothesized role for the interleukin–1 system in the modulation of corneal tissue
organization. Exp Eye Res 1996; 62:325–338.
23. Wilson SE. Molecular cell biology for the refractive corneal surgeon: programmed cell death
and wound healing. J Refract Surg 1997; 13:171–175.24. Wilson SE. Keratocyte apoptosis in refractive surgery: Everett Kinsey Lecture. CLAO J 1998;
24:181–185.
25. Helena MC, Baerveldt F, Kim W-J, Wilson SE. Keratocyte apoptosis after corneal surgery.
Invest Ophthalmol Vis Sci 1998; 39:276–283.
26. Kim WJ, Mohan RR, Mohan RR, Wilson SE. Caspase inhibitor z-VAD-FMK inhibits kerato-
cyte apoptosis, but promotes keratocyte necrosis, after corneal epithelial scrape. Exp Eye Res
2000; 71:225–232.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 195/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 196/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 197/338
186 Ambrosio and Wilson
68. Argento CJ, Cosentino MJ. Comparison of optical zones in hyperopic laser in situ keratomi-
leusis: 5.9 mm versus smaller optical zones. J Cataract Refract Surg 2000; 26:1137–1146.
69. Davidorf JM, Eghbali F, Onclinx T, Maloney RK. Effect of varying the optical zone diameter
on the results of hyperopic laser in situ keratomileusis. Ophthalmology 2001; 108:1261–1265.70. Aron-Rosa DS, Febbraro JL. Laser in situ keratomileusis for hyperopia. J Refract Surg 1999;
15(suppl):S212–S215.
71. Ambrosio R Jr, Wilson SE. Two step LASIK for hyperopic or mixed astigmatism with the
VisX S2 laser. Invest Ophthalmol Vis Sci (Suppl) 2001; 42:S7224.
72. Lans U. Experimentelle Utersuchungen uber die Entstehung von Astigmatismus durch nicht-
perforierende Corneawunden. Graefes Arch Clin Exp Ophthalmol 1898; 45:117.
73. Vinciguerra P, Kohnen T, Azzolini M, Radice P, Epstein D, Koch DD. Radial and staggered
treatment patterns to correct hyperopia using noncontact holmium:YAG laser thermal kera-
toplasty. J Cataract Refract Surg 1998; 24:21–30.
74. Gezer A. The role of patient’s age in regression of holmium: YAG thermokeratoplasty–in-
duced correction of hyperopia. Eur J Ophthalmol 1997; 7(2):139–143.
75. Bilgihan K, Akata F, Gurelik G, Adiguzel U, Akpinar M, Hasanreisoglu B. Corneal iron ring
after hyperopic photorefractive keratectomy. J Cataract Refract Surg 1999; 25:685–687.
76. Ozdamar A, Aras C, Sener B, Karacorlu M. Corneal iron ring after hyperopic laser-assisted
in situ keratomileusis. Cornea 1999; 18:243–245.
77. Molina CA, Agudelo LM. Corneal iron pigmentation after LASIK for hyperopia (letter). J
Refract Surg 2000; 16:755–756.
78. Probst LE, Almasswary MA, Bell J. Pseudo-Fleischer ring after hyperopic laser in situ kera-
tomileusis. J Cataract Refract Surg 1999; 25:868–870.
79. Steinberg EB, Wilson LA, Waring III GO, Lynn MJ, Coles WH. Stellate iron lines in the
corneal epithelium after radial keratotomy. Am J Ophthalmol 1984; 98:416–421.
80. Krueger RR, Tersi I, Seiler T. Corneal iron line associated with steep central islands after
photorefractive keratectomy. J Refract Surg 1997; 13(4):401–403.
81. Tervo T, Vesaluoma M, Bennett GL, Schwall R, Helena M, Liang Q, Wilson SE. Tear
hepatocyte growth factor (HGF) availability increases markedly after excimer laser surface
ablation. Exp Eye Res 1997; 64:501–504.
82. Wilson SE, Li Q, Mohan RR, Tervo T, Vesaluoma M, Bennett GL, Schwall R, Tabor K,
Kim J, Hargrave S, Cuevas KH. Lacrimal gland growth factors and receptors: lacrimal fibro-
blastic cells are a source of tear HGF. Adv Exp Med Biol 1998; 438:625–628.
83. McWhae J, Willerscheidt A, Gimbel H, Freese M. Ultrasound biomicroscopy in refractive
surgery. J Cataract Refract Surg 1994; 20:493–497.
84. Reinstein DZ, Silverman RH, Sutton HF, Coleman DJ. Very high-frequency ultrasound cor-
neal analysis identifies anatomic correlates of optical complications of lamellar refractive
surgery: anatomic diagnosis in lamellar surgery. Ophthalmology 1999; 106:474–482.
85. Holland SP, Srivannaboon S, Reinstein DZ. Avoiding serious corneal complications of laser
assisted in situ keratomileusis and photorefractive keratectomy. Ophthalmology 2000; 107:
640–652.
86. Reinstein DZ, Silverman RH, Raevsky T, Simoni GJ, Lloyd HO, Najafi DJ, Rondeau, MJ
Coleman DJ. Arc-scanning very high-frequency digital ultrasound for 3D pachymetric map-
ping of the corneal epithelium and stroma in laser in situ keratomileusis. J Refract Surg 2000;
16:414–430.87. Maldonado MJ, Ruiz-Oblitas L, Munuera JM, Aliseda D, Garcia-Layana A, Moreno-Mon-
tanes J. Optical coherence tomography evaluation of the corneal cap and stromal bed features
after laser in situ keratomileusis for high myopia and astigmatism. Ophthalmology 2000;
107:81–87; discussion 88.
88. Ustundag C, Bahcecioglu H, Ozdamar A, Aras C, Yildirim R, Ozkan S. Optical coherence
tomography for evaluation of anatomical changes in the cornea after laser in situ keratomi-
leusis. J Cataract Refract Surg 2000; 26:1458–1462.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 198/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 199/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 200/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 201/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 202/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 203/338
192 Azar et al.
0.68 D; strict monovision patients, 1.52 D (PϽ .001). Twenty-nine (78.4%) minimonovi-
sion patients and 49 (81.7%) strict monovision patients were satisfied with visual outcome
after LASIK. The difference in satisfaction between the two groups was not statistically
significant. Only three patients in our entire study were monovision failures requiring
retreatment; all had strict monovision before retreatment. One was dissatisfied with dis-
tance vision, and two complained of imbalance.
Other studies have examined monovision success rates after refractive surgery. In
42 presbyopic myopic patients with monovision induced by refractive surgery, Jain and
associates found a monovision success rate of 88% (1). One case report examined an
aircraft pilot who underwent PRK with intentional undercorrection of the dominant eye.
Postoperatively, the patient noted no deleterious visual effects and was still able to pilot
an aircraft (8).
Wright and colleagues studied binocular function and patient satisfaction in 21 pres-
byopic myopic patients between the ages of 37 and 53 in whom monovision induced
by refractive surgery (9). Sixteen emmetropic patients served as a control group. In the
monovision group, 20 patients (95.2%
) had binocular visual acuity of 20/25 or better. Nopatient in the monovision group used reading glasses postoperatively, whereas 4 of 16
patients (25%) in the control group used such glasses. Stereoacuity was slightly lower in
the monovision group but not statistically significantly so. Patient satisfaction was very
high in the monovision group.
Anecdotal evidence indicates that refractive surgery patients are often able to read
better than their refractive error would suggest; for example, a 50-year-old myope corrected
to plano in one eye and 0.75 D in the other may still able read fine print. This phenome-
non has been attributed to the creation of a multifocal corneal topography after refractive
surgery (10,11). Therefore, a smaller degree of anisometropia may be required to obtain
adequate visual function for near and distance for refractive surgery monovision patients.
This would serve to preserve binocular visual function and increase monovision success
rates compared to monovision contact lens users.
F. PREOPERATIVE COUNSELING
All patients who opt for monovision should be informed of the adverse effect monovision
may have on some visual function parameters (2,3). Specifically, they need to be informed
of the risks of reduced binocular visual acuity, stereoacuity, and contrast sensitivity. In
addition, they need to be made aware of the risk of distance and near ghosting as a result
of incomplete blur suppression. Blur suppression appears to be particularly problematic
under night driving conditions because, as mentioned earlier, interocular blur suppression
becomes less effective under dim illumination conditions (2,3). Therefore, patients must
be advised of the need for distance glasses when driving. Liability is an important consider-
ation when selecting a refractive patient for monovision (3,12). Therefore, discussions of
the risks and benefits associated with monovision need to be carefully documented in a
patient’s chart.It is important to ascertain the personal preference of the patient. Some patients
(particularly those who are active in sports) wish to have the most optimal distance vision
possible and are willing to tolerate difficulties with near vision and associated need for
reading glasses in order to achieve this. These patients should be fully corrected for distance
vision in both eyes. Other patients (particularly those who do a lot of reading or other
fine near work) may be willing to tolerate mildly decreased binocular distance vision in

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 204/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 205/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 206/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 207/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 208/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 209/338
198 Azar et al.
between the average age of successful versus unsuccessful monovision patients but failed
to find any statistically significant difference in age between the two groups (5,31).
N. CONCLUSIONS
Monovision has been evaluated extensively in contact lens users, but few studies comment
on its success in refractive surgery. Furthermore, the impact of the magnitude of anisome-
tropia created in monovision patients has not been fully characterized. We have introduced
a new term, minimonovision, to characterize monovision patients with a lesser degree of
near vision correction than full monovision (7). The inclusion criteria for strict monovision
and minimonovision are mutually exclusive. We found that strict monovision and minimo-
novision groups had comparable satisfaction rates. We also found that crossed monovision
patients overall were as satisfied as uncrossed monovision patients, and that within the
minimonovision and monovision subgroups, crossed monovision did not affect satisfac-
tion. The rate of satisfaction for monovision after LASIK was similar to the rate in contact
lens wearers.Monovision is associated with some compromises of visual function, the extent of
which depend on the particular individual and the requirements imposed by different
viewing conditions. However, for those refractive surgery patients willing and able to
adapt, these compromises constitute reasonable a trade-off for reducing dependence on
near-vision correction.
Refractive surgery may be used to take advantage of the monovision option in
presbyopic refractive surgery patients. However, this option should be pursued only after
careful preoperative screening and counseling of the patient. Creating a monovision situa-
tion with refractive surgery constitutes a practical alternative to other surgical treatment
modalities for presbyopia, such as scleral expansion/relaxation and multifocal corneal
treatment.
REFERENCES
1. Jain S, Ou R, Azar DT.Monovision outcomes in presbyopic individuals after refractive surgery.
Ophthalmology 2001; 108:1430–1433.
2. Jain S, Arora I, Azar DT. Success of monovision in presbyopes: review of the literature and
potential applications to refractive surgery. Surv Ophthalmol 1996; 40:491–499.
3. Sippel KC, Jain S, Azar DT. Monovision achieved with excimer laser refractive surgery. Int
Ophthalmol Clin 2001; 41:91–101.
4. Schor C, Erickson P. Patterns of binocular suppression and accommodation in monovision.
Am J Optom Physiol Opt 1988; 65:853–861.
5. Schor C, Landsman L, Erickson P. Ocular dominance and the interocular suppression of blur
in monovision. Am J Optom Physiol Opt 1987; 64:723–730.
6. Fonda G. Presbyopia corrected with single vision spectacles or corneal lenses in preference
to bifocal corneal lenses. Trans Ophthalmol Soc Aust 1966; 25:78–80.7. Chang MA, Kloek CE, Zafar S, Jain S, Azar DT. Analysis of strict monovision and mini-
monovision LASIK surgery in presbyopes. Arch Ophthalmol 2002. Submitted.
8. Maguen E, Nesburn AB, Salz JJ. Bilateral photorefractive keratectomy with intentional unilat-
eral undercorrection in an aircraft pilot. J Cataract Refract Surg 1997; 23:294–296.
9. Wright KW, Guemes A, Kapadia MS, Wilson SE. Binocular function and patient satisfaction
after monovision induced by myopic photorefractive keratectomy. J Cataract Refract Surg
1999; 25:177–182.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 210/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 211/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 212/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 213/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 214/338
203Multifocal Corneal Ablations
Figure 1 Multifocal myopia-presbyopia PRK. Left, central near zone; right, sectoral near zone.
(Adapted from Ref. 4.)
In 1998, Vinciguerra et al. published their study involving zonal PRK for treating
presbyopia. The group used a 193-nm Aesculap-Meditec Mel 60 excimer laser with a
mask consisting of a mobile diaphragm formed by a blunt concave blade and a blunt
convex blade (6). An inferior semilunar region was ablated for a presbyopic correction
of 3.00 D. Within this region, the depth of cut was progressively reduced from the corneal
center to periphery as the blades of the diaphragm progressively closed upon each other.
Figure 2 Multifocal hyperopic-presbyopic PRK. (Adapted from Ref. 4.)

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 215/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 216/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 217/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 218/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 219/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 220/338
20
Scleral Relaxation to Treat Presbyopia
HIDEHARU FUKASAKU
Fukasaku Eye Centre, Yokohama, Japan
A. INTRODUCTION
Accommodation has until recently been explained by the Helmholtz hypothesis. This
hypothesis holds that passive anteroposterior thickening of the lens and relative curvature
changes in the anterior and posterior lens surfaces result from zonular relaxation with
ciliary muscle contraction (Fig. 1). Presbyopia is likewise described as the loss of accom-
modation due to decreasing elasticity of the lens fibers and capsule (1,2). Recent work
(3,4) suggests a very different model of accommodation. Morphological changes in the
lens with accommodative effort are seen as the result of active rather than passive interac-
tions. The three components of the ciliary body—the longitudinal, radial and circular
fibers—act in concert to increase tension in the equatorial zonules while decreasing tension
in the anterior and posterior zonules. The result is an active elongation of the lens diameter
with peripheral thinning and central thickening due to dynamic internal volume changes
(Fig. 2). The net result is increased plus refracting power of the eye.
The important difference between the Helmholtz model and the Schachar model is
that the latter suggests a more active interaction between the ciliary muscle and the lens/
zonule complex, positing an interaction in which active effort by the ciliary muscle leads
not only to passive relaxation of the lens/zonule complex but also a more complicated
active differential response of different zonular types resulting in morphological changesin the lens.
If this recent model of accommodation is correct, then presbyopia may not be ex-
plained by simple sclerosis of the lens fibers and capsule as previously understood. Rather,
the decline in accommodative power of the eye may be due to the inability of the lens
equator to expand into the posterior chamber. Thornton (5) has described this as “a crowd-
ing” of the lens in the posterior chamber as the lens grows.
209

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 221/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 222/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 223/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 224/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 225/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 226/338
215Scleral Relaxation to Treat Presbyopia
surprising. The effect depends on expansion of the scleral circumference overlying the
ciliary body. As the incisions heal, there is wound closure and a reduction in scleral
circumference back to near preoperative levels. The addition of silicone plugs in ACS-SEP
effectively blocked this wound closure and maintained the gained scleral circumferential
expansion and hence the gain in accommodative amplitude. The fact that the initial gain
in accommodative amplitude with ACS-SEP was actually slightly less than either our initial
ACS technique or our enhanced ACS technique using spreading dissection is probably due
the effect of the sutures holding the SEP in place tending to close the wound initially.
We are now careful not to place any unnecessary tension on these sutures. In addition,
we are now using 11–0 Merceline, which should induce less tension and last longer than
nylon.
D. ANTERIOR CILIARY SCLEROTOMY AND INTRAOCULAR
PRESSURE
We noted also that in addition to increasing the amplitude of accommodation, ACS-SEPwas also associated with a dramatic drop in intraocular pressure (IOP) (Fig. 9). Simple
ACS and ACS enhanced by spreading dissection, in contrast, caused only a minimal drop
in IOP that was lost fairly rapidly. The explanation probably lies in the depth and perma-
nence of the radial incisions. Simple ACS is a shallower incision. No attempt is made to
complete a full-thickness sclerotomy. ACS enhanced by spreading dissection, on the other
hand, ensures a full-thickness sclerotomy by use of the Fukasaku forceps to dissect down
Figure 9 Intraocular pressure.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 227/338
216 Fukasaku
to the uveal plane. This exposes the subscleral space, which is normally an anatomical
potential space due to the differential embryological development of the scleral and uveal
coats. With dissection, it is possible to create a limited, localized ciliochoroidal detachment
that increases the uveoscleral outflow of aqueous. Traumatic cyclodialysis and surgical
ciliochoroidal detachments are known to dramatically increase uveoscleral outflow and
can cause hypotony (7,8). There is no evidence of wound leakage per se, as there is no
filtering bleb or Seidel’s sign when fluorescein is applied to the conjunctiva overlying the
wound.
The loss of IOP-lowering effect with ACS enhanced by scleral spreading over a
matter of several months probably reflects closure of the incision and hence closure of
the ciliochoroidal detachment with a decrease in uveoscleral outflow. ACS-SEP, on the
other hand, shows negligible loss in IOP-lowering effect over many months. This probably
represents continued maintenance of the incision separation with the silicone plug and
continued ciliochoroidal detachment with ongoing increased uveoscleral outflow.
We have been very satisfied with ACS-SEP and its ability to provide a stable increase
in accommodative amplitude. Patients likewise have been extremely pleased with theresults. They report that they are now able to attend to the activities of daily living much
better, such as reading newspapers and product labels. This despite the modest measured
increase in accommodative amplitude of only 1.5 D. We expect that patient satisfaction
will increase further with correction of the fellow eye.
E. FUTURE DIRECTIONS
Future planned improvements include replacing the criss-cross 10 –0 nylon suture with a
11–0 Merceline horizontal mattress suture. We expect that we will be better able to lover
the profile of the suture knot to avoid potential conjunctival irritation or erosion and
achieve longer suture life. We have also redesigned the expansion plug to be broader at
the base (more trapezoidal on end view) to limit forces that might extrude the plug. We
are also creating preformed holes in the plug to avoid the time-consuming and difficulttask of driving the small cutting needle of 10–0 or 11–0 suture.
The dramatic and sustained drop in IOP with ACS-SEP suggests a possible role for
this procedure in the treatment of glaucoma. The advantage of ACS-SEP in this role is
that it seems to affect uveoscleral outflow. Uveoscleral outflow can account for up to 40%
of total aqueous outflow (9,10). Thus, unlike beta blockers, which have little effect on
IOP during sleep, stimulation of uveoscleral outflow should help to protect the patient
both day and night. Thus far, IOP reduction has been a serendipitous finding in ACS-SEP
in which we implant expansion plugs in each of the four oblique quadrants. The next
logical step will be to attempt to titrate IOP reduction by varying the number of plugs or
perhaps the size of the plugs. Again, this study is under way at our facility.
We believe that ACS-SEP is a valuable procedure in the treatment of presbyopia—a
procedure that is safe, effective, and well accepted by patients. Likewise, ACS-SEP prom-
ises to become another treatment modality for glaucoma, and we are working on improvingits predictability.
REFERENCES
1. von Helmholtz HL. Physiological Optics. New York: Dover Press, 1962: 143–172,375–415.
2. Fincham EF. The mechanism of accommodation. Br J Ophthalmol 1937; 8(suppl):5–80.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 228/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 229/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 230/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 231/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 232/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 233/338
222 Phillips and Yee
T a b l e 1
S u m m a r y o
f P r i m a r y O u t c o m e V a r i a b l e s a t E a c h F o l l o w - u p P e r i o d ( M e a n Ϯ S D )
O p e r a t e d e y e
N o n o p e r a t e d e y e
V a r i a b l e
P r e o p
( n ϭ 6 )
1 m o n t h ( n ϭ 6 )
3 m o n t h s ( n ϭ
6 )
6 m o n t h s ( n ϭ 3 )
P r e o p ( n ϭ 6 )
1 m o n t h ( n ϭ 6 )
3 m o n t h s ( n ϭ 6 )
6 m o n
t h s ( n ϭ 3 )
N P A ( c m )
6 9 Ϯ
1 . 6
7
2 0 . 8
3 Ϯ 5 . 1
9
2 0 . 8
3 Ϯ 6 . 3 1
a
2 4 . 6
7 Ϯ 5 . 6
9 a
6 9 Ϯ 1 . 2
6
4 0 . 1
7 Ϯ 2 8 . 5
8
2 7 . 5 Ϯ 6 . 1
2 a
3 2 Ϯ 2 . 6
5 a
S E b ( d i o p t e r s )
1 . 2 Ϯ 1 . 3
3
0 . 8
1 Ϯ 1 . 1
3
1 . 1
3 Ϯ 1 . 2
0 . 7
5 Ϯ 0 . 5
1 . 0
8 Ϯ 1 . 1
5
1 . 1
7 Ϯ 1 . 1
8
1 . 0
6 Ϯ 1 . 1
0
0 . 5
Ϯ 0 . 2
2
C y l i n d e r
0 . 4 2 Ϯ 0 . 5
2
0 . 6
3 Ϯ 0 . 4
4
0 . 5
8 Ϯ 0 . 5
0 Ϯ 0
0 . 5 Ϯ 0 . 5
2
0 . 5
8 Ϯ 0 . 5
6
0 . 6
3 Ϯ 0 . 5
2
0 . 5
Ϯ 0 . 2
5
D i s t a n c e V A c
Ϫ 0 . 3
3 Ϯ 0 . 5
Ϫ 0 . 1
1 Ϯ 0 . 1
6
Ϫ 0 . 1
4 Ϯ 0 . 1 9
Ϫ 0 . 0
6 Ϯ 0 . 1
Ϫ 0 . 3
3 Ϯ 0 . 5
Ϫ 0 . 1
1 Ϯ 0 . 2
2
Ϫ 0 . 1
2 Ϯ 0 . 2
4
Ϫ 0 . 0 3 Ϯ 0 . 0
6
2 0 / 4 3
2 0 / 2 6
2 0 / 2 8
2 0 / 2 3
2 0 / 4 3
2 0 / 2 6
2 0 / 2 6
2
0 / 2 1
N e a r V A
Ϫ 0 . 8 5 Ϯ 0 . 1
6
Ϫ 0 . 0
3 Ϯ 0 . 0
7 a
Ϫ 0 . 0
6 Ϯ 0 . 0 7
a
Ϫ 0 . 0
3 Ϯ 0 . 0
6 a
Ϫ 0 . 8
5 Ϯ 0 . 1
6
Ϫ 0 . 4
7 Ϯ 0 . 4
5
Ϫ 0 . 1
2 Ϯ 0 . 2
1 a
Ϫ 0 . 0
6 Ϯ 0 . 1
0 a
2 0
/ 1 4 2
2 0 / 2 1
2 0 / 2 3
2 0 / 2 1
2 0 / 1 4 2
2 0 / 5 9
2 0 / 2 6
2
0 / 2 3
B l u r p o i n t
Ϫ 0 . 6 3 Ϯ 0 . 1
4
Ϫ 1 . 9
5 Ϯ 1 . 0
5
Ϫ 2 . 6
7 Ϯ 2 . 6 3
Ϫ 0 . 6
7 Ϯ 1 . 6
6
Ϫ 0 . 5
4 Ϯ 0 . 2
5
Ϫ 1 . 6
5 Ϯ 0 . 4
9 a
Ϫ 1 . 5
4 Ϯ 0 . 3
7 a
Ϫ 0 . 3 3 Ϯ 1 . 6
1
I O P
1 7 . 2
Ϯ 2 . 7
1 6 . 2 Ϯ 0 . 8
4
1 3 . 6 Ϯ 1 . 1 4
1 4 Ϯ 1 . 7
3
1 7 . 3 Ϯ 2 . 0
1 6 . 4 Ϯ 1 . 5
1 7 . 1 Ϯ 1 . 8
1 5 . 8 Ϯ 0 . 7
6
a S i g n i f i c a n t d i f f e r e n c e b
e t w e e n t h e p r e o p a n d t h e f o l l o w - u p m e a s u r e m e n t s u s i n g p a i r e d t - t e s t ( p Յ
0 . 0
5 ) .
b S E ϭ s p h e r i c a l e q u i v a l e n t .
c B o t h d i s t a n c e a n d n e a r v i s i o n a r e c o m p u t e d b a s e d o n l o g 1 0 s c a l e .
T h e n
u m b e r s b e l o w t h e s e n u m b e r s i n d i c a t e t h e e q u i v a l e n t s n e l l e n r e f r a c t i o n .

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 234/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 235/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 236/338
225The Scleral Expansion Procedure
Figure 6 Marking the limbus with the quadrant marker.
Mark the 12 o’clock position at the slit lamp. This is an important reference mark
to be used later for proper segment placement away from the area of ciliary arteries. If
this reference mark is not made, cyclotorsion of the eye can occur when the patient lies
down for the procedure. This will increase the risk of anterior ischemic syndrome from
malpositioned segments. After the patient is taken to the operating room, the 12 o’clock
meridian is used to align the quadrant marker in order to mark the location of the scleral
expansion segments (Fig. 6.).
D. ANESTHESIA
A small amount of subconjunctival anesthesia is injected at the 12:00 and 6:00 o’clock
meridians to elevate the conjunctiva and produce a surgical plane for dissection. Retrobul-
bar and peribulbar anesthesia is generally avoided because the pupil dilates and the eye
may become soft, making it more difficult to construct the scleral belt loops. Additionally,
a dilated pupil precludes evaluation of iris sphincter function, which is necessary to assess
anterior segment circulation.
E. CONJUNCTIVAL DISSECTION
A 4 to 5-mm vertical incision is placed perpendicular to the limbus at the 12 and 6 o’clock meridians. These incisions are extended circumferentially at the limbus approximately 1
mm past the oblique quadrant marks. The conjunctiva from 7:30 to 10:30 o’clock and
from 2:30 to 4:30 o’clock is left intact to avoid postoperative redness in the palpebral
opening. The flap is dissected approximately 5 mm posterior to the limbus, leaving no
Tenon’s capsule in the area where the scleral expansion segments will be placed. As little
cautery as possible should be used so as to preserve the structural integrity of the sclera.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 237/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 238/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 239/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 240/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 241/338
230 Phillips and Yee
Figure 14 (A and B) The dimensions of the segment.
sometimes necessary to pass the segment upside down and then rotate the segment intoplace using the injector and heavy needle holder. Rotation of the segment will stretch the
belt loop, but a slightly stretched belt loop will produce a greater effect than a thin belt
loop. If it is still not possible to pass the segment, the segment may be getting caught in
a blind pocket. Reapply the scleral fixator at the opposite end of the tunnel and try passing
the segment in reverse by beginning at the exit side of the scleral belt loop.
If the patient suddenly moves or complains of eye pain, immediately stop advancing
the segment. This may indicate that the vitreous, subchoroidal space, or ciliary body has
been entered. This can be confirmed by the presence of vitreous or fluid containing black
pigment exiting one or both ends of the scleral belt loop. At this point, the segment should
be removed and the eye examined. If the surgeon feels it is safe, it may still be possible
to pass the segment upside down from the other direction.
If the scleral belt loop is torn or severed, remove the segment and close the sclera.
The operation may be completed after the sclera is healed in 2 or 3 months.
Figure 15 Placement of the segment.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 242/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 243/338
232 Phillips and Yee
far rather than far to near. Patients should hold an eye chart 4 in. (10 cm) from their eye
and look at the smallest line they can see. Patients are then asked to concentrate until they
can see any letter on the next smaller line. Next they should hold fixation on the letter
on the smaller line and slowly move it away from the eye until it is at full arm’s length.
The eye chart can then be brought slowly back toward the eye while continuously holding
fixation on the smaller line until the eye chart is back at 10 cm from the eye. Once they
can read all the letters on that smaller line, have them move to the next smaller line and
again move the eye chart to arm’s length while maintaining fixation on the smaller line,
and so on. Patients should repeat this exercise as frequently as possible, but for at least
10 repetitions, four times a day, each time trying to fixate on a smaller line beginning at
the close distance of 10 cm from the eye. It is much better to do frequent exercise sessions
throughout the day than one long session. Following the exercises, patients will notice
that they can read better. Patients will usually experience ciliary pain during the exercises
for the first 2 weeks after surgery. The patients can be told that this pain is a good sign
and that the exercise is strengthening their ciliary muscles. Patients should avoid the use
of a near vision optical aid during their daily reading tasks. Additionally, patients shouldsquint as little as possible during the eye exercise; if they initially have difficulty perform-
ing their daily reading tasks, encourage them to use a bright light or, only if absolutely
necessary, to squint in order to avoid the use of a near optical aid. As they continue the
eye exercise, the requirement to squint or use a bright light during their daily reading
tasks will decrease.
L. COMPLICATIONS
Only one case of AIS has been reported using the latest 5.5-mm scleral expansion segments
(23). This complication may have resulted from improper positioning of the segments
(23). One case of endophthalmitis has also been reported (23). This case was thought to
result from a break in sterile technique (23). Additionally, one case of scleral thinningsimilar to that observed with scleral buckles has been reported and may have been a result
of scleral expansion (24). To date, no cases of malignant glaucoma have been reported
using the new scleral expansion segments. Theoretically, this is a possibility, as the seg-
ments may increase posterior pressure, blocking outflow and resulting in aqueous misdirec-
tion. Intravenous manitol is given to dehydrate the vitreous decreasing the likelihood of this
complication. Other minor complications include conjunctival hyperemia, subconjunctival
hemorrhage, transient ptosis, rotation or subluxation, of the scleral expansion segments,
photophobia due to tear film instability, conjunctival erosion, accommodative fatigue,
temporary keratoconjunctivitis, swollen or irregular conjunctiva, and astigmatism, which
may last for 2 to 3 months and but subsides with intense treatment with artificial tears.
M. CLINICAL RESULTS
Increases in accommodation after this technique have ranged from 1.00 to 10.00 D (13).
Two different studies (20) of 29 and 7 patients have reported an increased range of accom-
modation in all patients, with an average of 3.02 and 3.13 D respectively. Similar to our
findings, an increased range of near vision was also noted in the unoperated eye. This
increase approached 20 to 50% of the increase measured in the operated eye.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 244/338
233The Scleral Expansion Procedure
N. SCLERAL EXPANSION AND OTHER REFRACTIVE PROCEDURES
Scleral expansion has been successfully performed after LASIK, PRK, and RK. With
regard to LASIK, however, it is easier to perform LASIK before scleral expansion dueto difficulties that may be encountered while applying the suction ring. Scleral expansion
has been performed as early as 6 weeks post-LASIK. Obviously, PRK and laser epithelial
keratomileusis (LASEK) are good alternatives for patients who have had previous scleral
expansion procedures.
O. OTHER SCLERAL EXPANSION PROCEDURES
Several other methods have been used to expand the sclera. Some surgeons have made
simple scleral incisions with a diamond knife to expand the sclera. The scleral incisions
are limited to an accommodative range of only about 1.50 D, and, as the incisions heal,
the effect declines (R. Schachar, personal communication, 2001). In order to prevent the
incisions from healing, Fukasaku has inserted silicone plugs into the scleral incisions (24a).
The infrared laser has also been used to make deep scleral incisions (25). The average
correction is also limited to an accommodative range of about 1.50 D and will likely
regress with time (R. Schachar, personal communication, 2001). In contrast to the above,
Lin has described no regression after scleral expansion using infrared laser (J. Lin, personal
communication, 2001). A major concern with the infrared laser is that it can coagulate
blood vessels and lead to anterior segment ischemia. There have been two phthisical eyes
as a result of making scleral incisions with the infrared laser for the treatment of presbyopia
(R. Schachar, personal communication, 2001). Last, as a result of the deeper tissue ablation,
the potential for rupture after blunt trauma is also a concern.
P. SCLERAL EXPANSION AND GLAUCOMA
While chronic open-angle glaucoma is a genetic disease, predisposed patients may benefitfrom scleral expansion due to anatomical modifications produced by the procedures in
the ciliary muscle and trabecular meshwork (26,27). International clinical trials evaluating
scleral expansion for the treatment of ocular hypertension and primary open-angle glau-
coma in Canada and Mexico have demonstrated excellent preliminary results (27,28). The
median decrease in IOP after scleral expansion was 7 mmHg, and the postoperative de-
crease in IOP appears to be equivalent to the IOP-lowering effect of the preop, physician-
prescribed topical glaucoma medications (27).
Q. SUMMARY
Scleral expansion is a new procedure designed to treat presbyopia surgically. While the
theory on which it is based continues to be a subject of intense debate, it must be noted
that patients report an improved ability to read at near after scleral expansion. Given theimmense impact of presbyopia, surgical reversal of presbyopia will likely continue to be
an area of significant interest. In addition, scleral expansion may offer a new modality
for the treatment and prevention of ocular hypertension and primary open-angle glaucoma.
If scleral expansion is found to effectively decrease IOP, the adverse reactions and systemic
side effects commonly observed with glaucoma medications could be avoided and potential
surgical filtering and shunt procedures could be delayed or eliminated.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 245/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 246/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 247/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 248/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 249/338
238 Bissen-Miyajima
was dependent on pupil size and sometimes inferior to that with monofocal IOLs. Another
concern is the loss of contrast sensitivity. Because of these unpleasant drawbacks, many
surgeons went back to implanting conventional monofocal IOLs. The results of recent
multifocal IOLs are more promising and the interest in this type of IOL has increased
again.
B. THEORETICAL BENEFITS AND CAVEATS
Before describing theoretical benefits and caveats, one should understand the different
designs of IOL.
1. Different Types of Multifocal IOLs
a. Refractive Type
The initial refractive type was two zones with a central 2-mm button for near, and this
IOL was called “bull’s eye” (Fig. 1A). The center part had additional 4 D, which wouldbe equivalent to 2.5 D in spectacles. If the pupil size was too small, the patient had
insufficient visual acuity and this lens was abandoned. Then other types of refractive IOLs
were introduced (Fig. 1B and C). Some are far-dominant and others are near-dominant.
Recently, the zonal progressive type of AMO ARRAY (Fig. 1D) became a standard
multifocal IOL in several countries. The center part is for far vision and patients usually
get good distance visual acuity (VA).
b. Diffractive Type
Another type is the diffractive type, which is not affected by pupil size. This IOL has a
0.6-mm central zone and some 30 annular diffracting zones on its posterior surface (Fig.
1E). The light can be diffracted toward two foci; 41% for near and 41% for distance.
Thus, 18% of the light would be lost, and the loss of contrast sensitivity became the
biggest concern.
2. Theoretical Benefit
a. Less Dependence on Spectacles
Theoretical benefits of multifocal IOLs are based on their depth of focus. Figure 2 shows
the results of distance visual acuity with defocus of the patient from emmetropia following
AMO ARRAY. There are two spikes, which means that the patient can focus both far
and near. Another interesting thing about this particular IOL is that the valley between
two spikes is not deep and patients have a chance to see things at middle distance. Thus,
the potential of not depending on spectacles is high.
3. Theoretical Caveat
a. Decreased Contrast Sensitivity
The caveat of multifocal IOLs in general is the loss of contrast sensitivity due to their
design. By in a randomized study of multifocal IOLs, a significant decrease of visual
acuity was reported at 11% contrast with multifocal IOLs compared to the monofocal
IOLs (1). Although this problem can be detected by examination of contrast visual acuity,
most patients do not have the problem in daily life.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 250/338
239Multifocal IOLs for Presbyopia
Figure 1 (A) IOLAB two-zone refractive type with a central 2-mm button for near. (B) IOPTEX.
(C) Pharmacia. (D) AMO ARRAY. (E) Diffractive IOL (3M). This IOL has a 0.6-mm central zone
and some 30 annular diffracting zones on its back surface.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 251/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 252/338
241Multifocal IOLs for Presbyopia
able 1 Exclusion Criteria
Patient with multifocal IOL in the fellow eye
Uncontrolled glaucomaProgressive diabetic retinopathy
orneal lesions that may affect visual acuity
ther complications that may affect visual acuity
Preoperative astigmatism greater than 1.5 D
Frequent driving or operation of dangerous machinery at night
2. Expectation of the Patient
The patient who is highly motivated is often a good candidate. The increased number of
refractive surgeries has proved that many patients long for life without spectacles and
contact lenses. Younger patients underage 45 are also candidates, since the most undesira-ble complication following cataract surgery at this age is the loss of accommodation.
Despite their perfect vision at far, they may suffer from the new experience of not being
able to read without spectacles.
3. Occupation
Individuals with occupations that require good far and near vision in which the use of
spectacles or contact lenses might be dangerous represent another good candidate group.
D. PREFERRED SURGICAL TECHNIQUES
The preferred surgical techniques should provide predictability of postoperative refraction
and stability of IOL position. For this purpose, small incision and continuous curvilinear
capsulorhexis (CCC) are recommended.
1. Incision
It is well known that surgically induced astigmatism has recently been diminished by the
use of small-incision cataract surgery. For this purpose, a foldable multifocal IOL is
preferable. Also, a self-sealing incision should be made so as to avoid suture-induced
astigmatisms.
2. IOL Position
Capsular bag implantation of IOLs provides a stable position. IOL tilt or decentration
causes severe complications with multifocal IOLs due to their design. Thus, CCC should
be completed. If the IOL haptics position is unclear, which may cause unpleasant phenom-ena such as glare and halo, one should try to implant the IOL symmetrically, either both
haptics in the capsular bag or in the sulcus.
3. Posterior CCC
Near vision can easily be decreased by the posterior capsular opacity with multifocal IOLs.
In other words, the rate of neodymium:YAG capsulotomy is higher than that of monofocal

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 253/338
242 Bissen-Miyajima
Table 2 Visual Acuities with Different Multifocal IOLs
Lindstrom Usui and Negishi and
(1993) associates (1992) associates (1997)
IOL
Type of IOL
Uncorrected distance
VA
Corrected distance VA
Uncorrected near VA
J1-J3
Distance-corrected near
VA J1-J3
Best-corrected near VA
J1-J3
3M
Diffractive
20/40 or better 53.1%
20/25 or better 84.9%
82%
92%
97%
AMO Array
Refractive
20/40 or better 90.3%
20/25 or better 100%
62.1%
62.1%
97%
Ioptex
Refractive
Not described
20/40 or better
94.9%
45.6%
60.4%
94.1%
IOLs. If the opacity or the fibrosis of the posterior capsule is obvious and cannot be
polished during surgery, one may perform posterior CCC. Especially when we implant
multifocal IOLs in younger patients, we should consider performing posterior CCC, since
a neodymium:YAG capsulotomy may be necessary earlier.
a. Clinical Results
There have been many reports on the results of multifocal IOLs following cataract extrac-
tion. The reports on multifocal IOL with clear lensectomy are limited. The desirable results
with cataract patients persuade clear lensectomy for the patient who would like to have
refractive surgery, including the correction of presbyopia.
b. Visual Acuity (VA)
Table 2 shows the reported results of several multifocal IOLs (2). The time-lapse changes
of the mean postoperative VA in a Japanese clinical study are shown in Table 3. The
average distance uncorrected VA was 20/25, best corrected VA was better than 20/20.
For near, uncorrected VA was 0.39, withdistance correction, it was 0.43; andbest corrected
Table 3 Time Lapse Changes of the Average VA
Observation
Pre-op 1 day 1 week 1 month 3 months 6 months 1 year
Uncorrected distance VA 0.13 0.63 0.73 0.74 0.69 0.73 0.78
Corrected distance VA 0.23 0.90 1.06 1.08 1.07 1.05 1.12
Uncorrected near VA 0.13 0.29 0.34 0.36 0.40 0.41 0.39
Distance-corrected near VA 0.13 0.30 0.36 0.38 0.39 0.40 0.43
Best corrected near VA 0.20 0.56 0.74 0.73 0.72 0.72 0.77

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 254/338
243Multifocal IOLs for Presbyopia
VA was 0.77. The VA at the 1 week postoperative visit was as good as the one at 1 year.
We can expect early visual recovery with this type of IOL.
c. Contrast Sensitivity
The loss of contrast sensitivity with multifocal IOLs is accepted as a drawback of this
design. Despite previous reports, our results are encouraging. The mean contrast sensitivity
at 1 year after the operation was above the lowest of normal range (Fig. 3). Contrast VA
with variable-contrast charts (VCVAC) showed that the contrast VA of the eye with a
multifocal IOL in 15 and 2.5% contrast was comparable to that with a monofocal IOL
(Fig. 4).
d. Halo and Glare
Halo and glare are also of concern following multifocal IOL surgery. One year after the
operation, patients were asked about halo and confirmed its intensity. At each final follow-
up observation, 22.4% complained mild or moderate halo, which was only a transient
symptom in every case against sun in daytime and/or light sources at night. This was notexperienced to the extent of causing problems in daily life. Glare values were measured
by Miller-Nadler Glaretester and percent glare was 5.6. No percent glare decrease was
observed, potentially generating clinical problems.
e. Spectacle Usage
It is not easy to analyze spectacle usage, since some patients use spectacles most of the
time and the others use them only when necessary. Approximately 60% were able to
function comfortably without spectacles. Figure 5 shows the changes of using spectacles
by the follow-up time. Until 1 month after operation, most patients were not using specta-
Figure 3 Contrast sensitivity. The mean contrast sensitivity after the operation was above the
lowest of normal range.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 255/338
244 Bissen-Miyajima
Figure 4 Contrast visual acuity. Contrast VA of the eye with multifocal IOL (array) in 15 and
2.5% contrast was comparable to that with monofocal IOL.
Figure 5 Changes of using spectacles.
Figure 6 Patient’s satisfaction.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 256/338
245Multifocal IOLs for Presbyopia
Figure 7 Vision simulation system.
cles. Once they get used to read with reading glasses, some prefer the clear letters using
the zone for far with additional correction with spectacles. That is why the rate for spectacle
usage increases after 3 months or 1 year.
e. Patient’s Satisfaction (Questionnaire)
It is important that patients be satisfied with the results (Fig. 6). Especially if clear lens
extraction has been performed, patients expect better reading ability.
f. Patient’s View with Model Eye
a. Vision Simulation System
The concern of implanting multifocal IOL is that the surgeon or patient cannot estimate
the view after the surgery. Because of this, it takes a long time to explain to the patient
about the results of multifocal IOL. The image through multifocal implantation was
recorded using the vision simulation system developed by Ohnuma (Fig. 7) (3).b. Patient’s View
Using photos taken by the vision simulation system, the view of the patient was examined.
First, the view was seen by each eye while the fellow eye was covered. Then the view
was compared with each eye. The photo which was most similar to the view with multifocal
IOL was chosen.
The results are shown in Figure 8. During the day, the vision is clearer than that
with a multifocal IOL and closer to the view with a monofocal IOL. However, for near
vision, the photo taken by the model eye was similar to the real view with a multifocal
IOL.
E. COMPLICATIONS AND MANAGEMENT
1. IOL Power Miscalculation
When the biometry was not perfect and the patient ends up with myopia or hyperopia, he
or she may not receive the advantage of multifocal IOL. It is known that this type of
multifocal IOL should be emmetropic to slightly hyperopic (Fig. 9A). If the postoperative
refraction is more than 0.5 D, the blur circles become larger at distance and near compared
to emmetropia (Fig. 9B)). This will cause potential halos at night. If the postoperative

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 257/338
246 Bissen-Miyajima
Figure 8 Patient’s view. (A) Clinic at day. (B) Clinic at night. (C) Clock.
refraction is hyperopic, halo at night should be minimal (Fig. 9C). Thus, postoperative
refraction is an important factor. IOL exchange or piggyback implantation should beconsidered if the patient suffers halo at night or strongly wishes better distance and near
vision.
2. IOL Decentration
With the introduction of CCC, clinically obvious decentration of IOL became rare. How-
ever, when it occurs, it may cause visual disturbance. Mostly, these are caused by asymmet-

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 258/338
247Multifocal IOLs for Presbyopia
Figure 9 Refractive error and blur circles. (A) Emmetropic to slightly hyperopic (plano to 0.5
D). (B) Myopic refraction (Ͼ 0.5). (C) Hyperopic refraction (Ͼ 0.5 D).
rical fixation of the IOL. Surgical replacement of the IOL should be considered. If thereplacement is not possible due to the defect of posterior capsule, one may consider
exchanging the IOL to monofocal IOL.
3. Halo and Glare Vision
Complications are mainly related to IOL design. Most common complaints are halo and
glare at night. These are usually relieved by time. From our questionnaire, some patients

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 259/338
248 Bissen-Miyajima
have reported being bothered with halo and glare while they were driving at night. How-
ever, the readability of traffic signs is about the same as with monofocal IOLs.
4. Insufficient Near Vision
This is caused by incorrect IOL power calculation, small pupil diameter, or opacity in the
path from cornea to retina. The former two reasons are most common. If the incorrect
IOL power is the main reason, one may consider IOL exchange or piggyback implantation.
If the pupil diameter is smaller than the near zone, the patient will not get the advantage
of near addition.
F. CONCLUSIONS
Treating presbyopia is still a challenge. However, we already have clinical data of im-
planting multifocal IOLs for cataract patients. At this time, if the patient will need cataract
surgery sooner or later, multifocal IOL is a rather safe way to treat presbyopia. On the
other hand, for the patient with a clear lens, this may be a decision to be made by thesurgeon. The surgeon must be confident in his or her biometry and surgical technique. If
the patient understands the risk of removing the lens and implanting an IOL, a multifocal
IOL should always be considered as the best choice for the treatment of presbyopia.
REFERENCES
1. Steinert RF, Post CT Jr, Brint SF, Fritch CD, Hall DL, Wilder LW, Fine IH, Lichtenstein SB,
Masket S, Casebeer C. A prospective, randomized, double-masked comparison of a zonal-
progressive multifocal intraocular lens and a monofocal intraocular lens. Ophthalmology 1992;
99:853–860.
2. Negishi K, Bissen-Miyajima H, Kato K, Kurosaka D, Nagamoto T. Evaluation of a zonal-
progressive multifocal intraocular lens. Am J Ophthalmol 1997; 124:321–330.
3. Ohnuma K. Image focused by a multi-focal intraocular lens and its estimation. J Eye 2001; 18:395–400.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 260/338
23
Refractive Lens Exchange with aMultifocal Intraocular Lens
I. HOWARD FINE, RICHARD S. HOFFMAN, and MARK PACKER
Casey Eye Institute, Oregon Health and Science University,
Portland, Oregon, U.S.A.
A. INTRODUCTION
The options for treating the refractive surgery patient are greater now than at any time in
ophthalmic history. Excimer laser refractive surgery is growing in popularity throughoutthe world, but it has its limitations. Patients with extreme degrees of myopia and hyperopia
are poor candidates for corneal refractive surgery, and presbyopic patients must rely on
reading glasses or monovision in order to obtain the full range of visual function. These
limitations in laser refractive surgery have led to a resurgence of intraocular modalities
for the correction of refractive errors.
B. MULTIFOCAL LENSES
Perhaps the greatest catalyst for the resurgence of refractive lens exchange has been the
development of multifocal lens technology. High hyperopes, presbyopes, and patients with
borderline cataracts who have presented for refractive surgery have been ideal candidates
for this new technology.
Multifocal intraocular lens (IOL) technology offers patients substantial benefits. Theelimination of a presbyopic condition and restoration of normal vision by simulating
accommodation greatly enhances the quality of life for most patients. The only multifocal
IOL available for general use in the U.S. is the Array (Advanced Medical Optics; Irvine,
CA). The advantages of astigmatically neutral clear corneal incisions have allowed for
increased utilization of multifocal technology in both cataract and refractive lens exchange
surgery.
249

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 261/338
250 Fine et al.
Figure 1 The AMO Array foldable silicone multifocal intraocular lens.
C. LENS DESIGN
The principle of any multifocal design is to create multiple image points behind the lens.
The goal of these lenses is to enable less reduction in visual acuity for a given amount
of defocus by improving the depth of field. The Array is a zonal progressive intraocular
lens with five concentric zones on the anterior surface (Fig. 1). Zones 1, 3, and 5 are
distance dominant zones while zones 2 and 4 are near dominant. The lens has an aspherical
component and thus each zone repeats the entire refractive sequence corresponding to
distance, intermediate, and near foci. This results in vision over a range of distances. The
lens uses 100% of the incoming available light and is weighted for optimum light distribu-
tion. With typical pupil sizes, approximately half of the light is distributed for distance,
one-third for near vision, and the remainder for intermediate vision. The lens utilizes
continuous surface construction and consequently there is no loss of light through defrac-
tion and no degradation of image quality as a result of surface discontinuities. The lens
has a foldable silicone optic that is 6.0 mm in diameter, with haptics made of polymethyl-
methacrylate and a haptic diameter of 13 mm. The lens can be inserted through a clear
corneal or scleral tunnel incision that is 2.8 mm wide, utilizing the Unfolder injector
system (Advanced Medical Optics; Irvine, CA).
D. CLINICAL RESULTS
The efficacy of multifocal technology has been documented in many clinical studies. Earlystudies of the one-piece Array documented a larger percentage of patients who were able
to read J2 print after undergoing multifocal lens implantation compared to patients with
monofocal implants (13–15). Similar results have been documented for the foldable Array
(16). Clinical trials comparing multifocal to monofocal lens implantation in the same
patient also revealed improved intermediate and near vision in the multifocal eye versus
the monofocal eye (17,18).

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 262/338
251Refractive Lens Exchange
Many studies have evaluated both the objective and subjective qualities of contrast
sensitivity, stereoacuity, glare disability, and photic phenomena following implantation of
multifocal IOLs. Refractive multifocal IOLs, such as the Array, were found to be superior
to diffractive multifocal IOLs by demonstrating better contrast sensitivity and less glare
disability (19). The Array does produce a small amount of contrast sensitivity loss equiva-
lent to the loss of one line of visual acuity at the 11% contrast level using Regan contrast
sensitivity charts (14). This loss of contrast sensitivity at low levels is only present when
the Array is placed monocularly; it has not been demonstrated with bilateral placement
and binocular testing (20). In addition to relatively normal contrast sensitivity, good ran-
dom-dot stereopsis and less distance and near aniseikonia were present in bilateral versus
unilateral implants (21).
One of the potential drawbacks of the Array lens has been the potential for an
appreciation of halos around point sources of light at night in the early weeks and months
following surgery (22). Most patients will learn to disregard these halos with time, and
bilateral implantation appears to improve these subjective symptoms. Concerns about the
visual function of patients at night have been allayed by a driving simulation study inwhich bilateral Array multifocal patients performed only slightly worse than patients with
bilateral monofocal IOLs. The results indicated no consistent difference in driving perfor-
mance and safety between the two groups (23). In a study by Javitt et al., 41% percent
of bilateral Array subjects were found never to require spectacles, compared to 11.7% of
monofocal controls. Overall, subjects with bilateral Array IOLs reported better overall
vision, less limitation in visual function, and less use of spectacles than monofocal controls
(24).
A small recent study reviewed the clinical results of bilaterally implanted Array
multifocal lens implants in refractive lens exchange patients (25). A total of 68 eyes
were evaluated, comprising 32 bilateral and 4 unilateral Array implantations. Of patients
undergoing bilateral refractive lens exchange, 100% achieved binocular visual acuity of
20/40 and J5 or better measured 1 to 3 months postoperatively. Over 90% achieved uncor-
rected binocular visual acuity of 20/30 and J4 or better, and nearly 60% achieved uncor-rected binocular visual acuity of 20/25 and J3 or better (Fig. 2). This study included patients
Figure 2 Clinical results of bilateral Array implantation following refractive lens exchange.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 263/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 264/338
253Refractive Lens Exchange
monofocal patients with concurrent eye disease such as macular degeneration, glaucoma,
and diabetic retinopathy (26).
Utilization of these lenses in patients who complain excessively, are highly introspec-
tive and fussy, or obsess over body image and symptoms should be avoided. In addition,
conservative use of this lens is recommended in evaluating patients whose occupations
involve frequent night driving or that place high demands on vision and near work, such
as engineering and architecture. Such patients must demonstrate a strong desire for relative
spectacle independence in order to be considered for a refractive lens exchange with Array
implantation.
In our practice, patient selection has been reduced to a very rapid process. Once
someone has been determined to be a candidate for refractive lens exchange, he or she is
asked two questions: the first is “If an implant could be placed in your eye that would
allow you to see both distance and near without glasses under most circumstances, would
that be an advantage?” Patients are then asked: “If the lens is associated with halos around
lights at night, would it still be an advantage?” If they do not think they would be bothered
by these symptoms, they receive a multifocal IOL. If concern over halos or night drivingis strong, these patients may receive monofocal lenses with appropriate informed consent
regarding loss of accommodation and the need for reading glasses or consideration of a
different refractive surgical procedure.
Prior to receiving an Array, all candidates should be informed of the lens statistics
to ensure that they understand that spectacle independence is not guaranteed. Approxi-
mately 41% of the patients who are implanted with bilateral Array IOLs will never need
to wear glasses, 50% wear glasses on a limited basis as for driving at night or during
prolonged reading, 12%will always need to wear glasses for near work, and approximately
8% will need to wear spectacles on a full-time basis for distance and near correction (23).
In addition, 15% of patients were found to have difficulty with halos at night and 11%
had difficulty with glare, compared to 6% and 1% respectively of monofocal patients.
F. PREOPERATIVE MEASUREMENTS
The most important assessment of successful multifocal lens use other then patient selec-
tion involves precise preoperative measurements of axial length in addition to accurate
lens power calculations. There are some practitioners who feel that immersion biometry
is necessary for accurate axial length determination. However, applanation techniques in
combination with the Holladay 2 formula yield accurate and consistent results with greater
patient convenience and less technician time. A newer device now available, the Zeiss
IOLMaster, is a combined biometry instrument for noncontact optical measurements of
axial length, corneal curvature, and anterior chamber depth that yields extremely accurate
and efficient measurements with minimal patient inconvenience. The axial length measure-
ment is based on an interference-optical method termed partial coherence interferometry
and measurements are claimed to be compatible with acoustic immersion measurementsand accurate to within 30 m. The Quantel Axis II immersion biometry unit is also a
convenient and accurate device for axial length measurements. The device yields quick
and precise axial length measurements using immersion biometry without requiring the
patient to be placed in the supine position. Regardless of the technique being used to
measure axial length, it is important that the surgeon use biometry that he or she feels
yields the most consistent and accurate results.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 265/338
254 Fine et al.
When determining lens power calculations, the Holladay 2 formula takes into ac-
count disparities in anterior segment and axial lengths by adding the white-to-white corneal
diameter and lens thickness into the formula. Addition of these variables helps predict the
exact position of the IOL in the eye and has improved refractive predictability. The SRK
T and the SRK II formulas can be used as a final check in the lens power assessment;
for eyes with less than 22 mm in axial length, the Hoffer Q formula should be utilized
for comparative purposes.
G. SURGICAL TECHNIQUE
The multifocal Array works best when the final postop refraction has less than 1 D of
astigmatism. It is thus very important that incision construction be appropriate with respect
to size and location. A clear corneal incision at the temporal periphery that is 3 mm or
less in width and 2 mm long is highly recommended (29). Each surgeon should be aware
of his or her usual amount of surgically induced astigmatism by vector analysis.
In preparation for phacoemulsification, the capsulorhexis must be round in shapeand sized so that there is a small margin of anterior capsule overlapping the optic circumfer-
entially (Fig. 4). This is important in order to guarantee in-the-bag placement of the IOL
and prevent anterior/posterior alterations in location that would affect the final refractive
status.
Minimally invasive surgery is very important. Techniques that produce effective
phacoemulsification times of less than 20 s and average phacoemulsification powers of
10% or less are highly advantageous and can best be achieved with power modulations
(burst mode or two pulses per second) rather than continuous phacoemulsification modes
(33,34). The Array is inserted most easily by means of the Unfolder injector system.
Complete removal of all viscoelastic from the anterior chamber and behind the lens will
reduce the incidence of postoperative pressure spikes and myopic shift from capsular block
syndrome.
Figure 4 The Array multifocal intraocular lens in situ. Note the capsulorhexis overlapping the
edge of the lens optic.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 266/338
255Refractive Lens Exchange
H. COMPLICATIONS MANAGEMENT
When intraoperative complications develop, they must be handled precisely and appropri-
ately. In situations in which the first eye has already had an Array implanted, managementof complications must be directed toward finding any possible way of implanting an
Array in the second eye. Under most circumstances, capsular rupture will still allow for
implantation of an Array as long as there is an intact capsulorhexis. Under these circum-
stances, the lens haptics are implanted in the sulcus and the optic is prolapsed posteriorly
through the anterior capsulorhexis.
It is important to avoid trauma to the iris since pupillary size and shape may affect
the visual function of a multifocal IOL postoperatively. If the pupil is less than 2.5 mm,
there may be an impairment of near visual acuity due to the location of the rings serving
near visual acuity. For patients with small postoperative pupil diameters affecting near
vision, a mydriatic pupilloplasty can be performed successfully with the Argon laser (35).
Enlargement of the pupil will expose the near dominant rings of the multifocal IOL and
restore near vision in most patients.
I. TARGETING EMMETROPIA
The most important skill to master in the refractive lens exchange patient is the ultimate
achievement of emmetropia. Emmetropia can be achieved successfully with accurate intra-
ocular lens power calculations and adjunctive modalities for eliminating astigmatism. With
the trend toward smaller astigmatically neutral clear corneal incisions, it is now possible
to address pre-existing astigmatism more accurately at the time of lens surgery. The popu-
larization of limbal relaxing incisions by Gills and Nichamin has added a useful means
of reducing up to 3.50 diopters of pre-existing astigmatism by placing paired 600-m-
deep incisions at the limbus in the steep meridian. When against-the-rule astigmatism is
present, the temporal groove of the paired limbal relaxing incisions can be utilized as the
site of entry for the clear corneal incision. This is a simple and practical approach forreducing pre-existing astigmatism at the time of surgery, and since the coupling of these
incisions is one to one, no alteration in the calculated lens power is needed.
J. REFRACTIVE SURPRISE
On occasion, surgeons may be presented with an unexpected refractive surprise following
surgery. These miscalculations in lens power can be disappointing to both the surgeon
and patient, but happily the means for correcting these refractive errors are increasing.
When there is a gross error in the lens inserted, the best approach is to perform a lens
exchange as soon as possible. When smaller errors are encountered or lens exchange is
felt to be unsafe, various adjunctive procedures are available to address these refractive
surprises.
One of the simplest techniques to address residual myopia following surgery is atwo-, three-, or four-cut radial keratotomy (RK) with a large optical zone. RK is still a
relatively safe procedure with little likelihood for significant hyperopic shift with conserva-
tive incision and optical zone placement. When residual hyperopia is present following
cataract surgery, conductive keratoplasty (Refractec) is an option for reducing hyperopia
and appears to work best in older patients and in patients with 1 to 2 D of refractive error.
Another option for reducing 0.5 to 1.0 D of hyperopia involves rotating the IOL out of

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 267/338
256 Fine et al.
the capsular bag and placing it in the ciliary sulcus to increase the functional power of
the lens. LASIK can also be performed to eliminate myopia, hyperopia, or astigmatism
following surgery complicated by unexpected refractive results.
An interesting and simple intraocular approach to the postoperative refractive sur-
prise involves the use of intraocular lenses placed in the sulcus over the primary IOL in
a piggyback fashion. Staar Surgical now produces the AQ5010V foldable silicone IOL
that is useful for sulcus placement as a secondary piggyback lens. The Staar AQ5010V
has an overall length of 14.0 mm and is available in powers between 4.0 to 4.0 D
in whole-diopter powers. Useful for smaller eyes with larger hyperopic postoperative errors
is the Staar AQ2010V, which is 13.5 mm in overall length and is available in powers
between 5.0 to 9.0 diopters in whole-diopter steps. This approach is especially useful
when expensive refractive lasers are not available or when corneal surgery is not feasible.
K. POSTOPERATIVE COURSE
If glasses are required after surgery in a patient implanted with a multifocal IOL, thespherical correction should be determined by overplusing the patient to a slight blur and
gradually reducing the power until the best acuity is reached. Patients are able to focus
through the near portions of their IOL; thus it is possible to overminus a patient if care
is not taken to push the plus power. When using this defocusing technique, it is critical
to stop as soon as distance acuity is maximized to avoid overminusing the patient. The
cylinder power should be the smallest amount that provides the best acuity. If add power
is necessary, the full add power for the required working distance should be prescribed.
If patients are unduly bothered by photic phenomena such as halos and glare, these
symptoms can be alleviated by various techniques. Weak pilocarpine at a concentration
of 1/8% or weaker will constrict the pupil to a diameter that will usually lessen the severity
of halos without significantly affecting near visual acuity. Similarly, brimonidine tartrate
ophthalmic solution 0.2% (Alphagan) has been shown to reduce pupil size under scotopic
conditions (36) and can also be administered in an attempt to reduce halo and glare
symptoms. Another approach involves the use of overminused spectacles in order to push
the secondary focal point behind the retina and thus lessen the effect of image blur from
multiple images in front of the retina. Polarized lenses have also been found to be helpful
in reducing photic phenomena. Perhaps the most important technique is the implantation
of bilateral Array lenses as close in time as possible in order to give patients the ability
to use the lenses together, which appears to allow for improved binocular distance and
near vision compared to monocular acuity. Finally, most patients report that halos improve
or disappear with the passage of several weeks to months.
L. FINAL COMMENTS
As this procedure becomes more popular, it will create a win-win situation for all involved.First, patients can enjoy a predictable refractive procedure with rapid recovery that can
address all types and severities of refractive errors in addition to addressing presbyopia with
multifocal or accommodative lens technology. Second, surgeons can offer these procedures
without the intrusion of private or government insurance and establish a less disruptive
relationship with their patients. Finally, government can enjoy the decreased financial
burden from the expenses of cataract surgery for the ever-increasing ranks of aging baby

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 268/338
257Refractive Lens Exchange
boomers as more and more of these patients opt for lens exchanges to address their refrac-
tive surgery goals, ultimately reaching Medicare coverage as pseudophakes.
Successful integration of refractive lens exchanges into the general ophthalmolo-
gist’s practice is fairly straightforward, since most surgeons are currently performing small-
incision cataract surgery for their cataract patients. Essentially, the same procedure is
performed for a refractive lens exchange, differing only in removal of a relatively clear
crystalline lens and simple adjunctive techniques for reducing corneal astigmatism. Al-
though any style of foldable IOL can be used for lens exchanges, multifocal IOLs currently
offer the best option for addressing both the elimination of refractive errors and presbyopia.
Refractive lens exchange with multifocal lens technology is not for every patient consider-
ing refractive surgery but does offer substantial benefits, especially in high hyperopes,
presbyopes, and patients with borderline or soon to be clinically significant cataracts who
are requesting refractive surgery. Appropriate patient screening, accurate biometry and
lens power calculations, and meticulous surgical technique will allow surgeons to maxi-
mize their success with this procedure.
REFERENCES
1. Colin J, Robinet A. Clear lensectomy and implantationof low-power posterior chamber intraoc-
ular lens for the correction of high myopia. Ophthalmology 1994; 101:107–112.
2. Siganos DS, Pallikaris IG. Clear lensectomy and intraocular lens implantation for hyperopia
from 7 to 14 diopters. J Refract Surg 1998; 14:105–113.
3. Pucci V, Morselli S, Romanelli F, Pignatto S, ScandellariF, BellucciR. Clear lens phacoemulsi-
fication for correction of high myopia. J Cataract Refract Surg 2001; 27:896–900.
4. Ge J, Arellano A, Salz J. Surgical correction of hyperopia: clear lens extraction and laser
correction. Ophthalmol Clin North Am 2001; 14:301–313.
5. Fine IH, Hoffman RS, Packer P. Clear-lens extraction with multifocal lens implantation. Int
Ophthalmol Clin 2001; 41:113–121.
6. Pop M, Payette Y, Amyot M. Clear lens extraction with intraocular lens followed by photore-fractive keratectomy or laser in situ keratomileusis. Ophthalmology 2000; 107:1776–1781.
7. Kolahdouz-Isfahani AH, Rostamian K, Wallace D, Salz JJ. Clear lens extraction with intraocu-
lar lens implantation for hyperopia. J Refract Surg 1999; 15:316–323.
8. Jimenez-Alfaro I, Miguelez S, Bueno JL, Puy P. Clear lens extraction and implantation of
negative-power posterior chamber intraocular lenses to correct extreme myopia. J Cataract
Refract Surg 1998; 24:1310–1316.
9. Lyle WA, Jin GJ. Clear lens extraction to correct hyperopia. J Cataract Refract Surg 1997;
23:1051–1056.
10. Lee KH, Lee JH. Long-term results of clear lens extraction for severe myopia. J Cataract
Refract Surg 1996; 22:1411–1415.
11. Gris O, Guell JL, Manero F, Muller A. Clear lens extraction to correct high myopia. J Cataract
Refract Surg 1996; 22:686–689.
12. Lyle WA, Jin GJ. Clear lens extraction for the correction of high refractive error. J Cataract
Refract Surg 1994; 20:273–276.13. Percival SPB, Setty SS. Prospectively randomized trial comparing the pseudoaccommodation
of the AMO Array multifocal lens and a monofocal lens. J Cataract Refract Surg 1993; 19:
26–31.
14. Steinert RF, Post CT, Brint SF, Fritch CD, Hall DL, Wilder LW, Fine IH, Lichtenstein SB,
Masket S, Casebeer C. A progressive, randomized, double-masked comparison of a zonal-
progressive multifocal intraocular lens and a monofocal intraocular lens. Ophthalmology 1992;
99:853–861.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 269/338
258 Fine et al.
15. Negishi K, Nagamoto T, Hara E, Kurosaka D, Bissen-Miyajima H. Clinical evaluation of a
five-zone refractive multifocal intraocular lens. J Cataract Refract Surg 1996; 22:110–115.
16. Brydon KW, Tokarewicz AC, Nichols BD. AMO Array multifocal lens versus monofocal
correction in cataract surgery. J Cataract Refract Surg 2000; 26:96–100.17. Vaquero-Ruano M, Encinas JL, Millan I, Hijos M, Cajigal C. AMO Array multifocal versus
monofocal intraocular lenses: Long-term follow-up. J Cataract Refract Surg 1998; 24:118–123.
18. Steinert RF, Aker BL, Trentacost DJ, Smith PJ, Tarantino N. A prospective study of the AMO
Array zonal-progressive multifocal silicone intraocular lens and a monofocal intraocular lens.
Ophthalmology 1999; 106:1243–1255.
19. Pieh S, Weghaupt H, Skorpik C. Contrast sensitivity and glare disability with diffractive and
refractive multifocal intraocular lenses. J Cataract Refract Surg 1998; 24:659–662.
20. Arens B, Freudenthaler N, Quentin CD. Binocular function after bilateral implantation of
monofocal and refractive multifocal intraocular lenses. J Cataract Refract Surg 1999; 25:
399–404.
21. Haring G, Gronemeyer A, Hedderich J, de Decker W. Stereoacuity and aniseikonia after
unilateral and bilateral implantation of the Array refractive multifocal intraocular lens. J Cata-
ract Refract Surg 1999; 25:1151–1156.
22. Dick HB, Krummenauer F, Schwenn O, Krist R, Pfeiffer N. Objective and subjective evaluationof photic phenomena after monofocal and multifocal intraocular lensimplantation.Ophthalmol-
ogy 1999; 106:1878–1886.
23. Featherstone KA, Bloomfield JR, Lang AJ, Miller-Meeks MJ, Woodworth G, Steinert RF.
Driving simulation study: bilateral Array multifocal versus bilateral AMO monofocal intraocu-
lar lenses. J Cataract Refract Surg 1999; 25:1254–1262.
24. Javitt JC, Wang F, Trentacost DJ, Rowe M, Tarantino N. Outcomes of cataract extraction with
multifocal intraocular lens implantation—Functional status and quality of life. Ophthalmology
1997; 104:589–599.
25. Packer M, Fine IH, Hoffman RS. Refractive lens exchange with the Array multifocal lens. J
Cataract Refract Surg. 2002; 28:421–424.
26. Kamath GG, Prasas S, Danson A, Phillips RP. Visual outcome with the Array multifocal
intraocular lens in patients with concurrent eye disease. J Cataract Refract Surg 2000; 26:
576–581.
27. Rodriguez A, Gutierrez E, Alvira G. Complications of clear lens extraction in axial myopia.Arch Ophthalmol 1987; 105:1522–1523.
28. Ripandelli G, Billi B, Fedeli R, Stirpe M. Retinal detachment after clear lens extraction in 41
eyes with axial myopia. Retina 1996; 16:3–6.
29. Fine IH. Corneal tunnel incision with a temporal approach. In: Fine IH, Fichman RA, Grabow
HB, eds. Clear-Corneal Cataract Surgery & Topical Anesthesia. Thorofare, NJ: Slack, 1993:
5–26.
30. Gills JP, Gayton JL. Reducing pre-existing astigmatism. In: JP Gills, Cataract Surgery: The
State of the Art. Thorofare, NJ: Slack, 1998:53–66.
31. Nichamin L. Refining astigmatic keratotomy during cataract surgery. Ocular Surgery News,
April 15, 1993.
32. Fine IH. Cortical cleaving hydrodissection. J Cataract Refract Surg 1992; 18:508–512.
33. Fine IH. The choo-choo chop and flip phacoemulsification technique. Oper Tech Cataract
Refract Surg 1998; 1,2:61–65.
34. Fine IH, Packer M, Hoffman RS. “The use of power modulations in phacoemulsification:Choo choo chop and flip phacoemulsification.” J Cataract Refract Surg 2001; 27:188–197.
35. Thomas JV. Pupilloplasty and photomydriasis. In: Belcher CD, Thomas JV, Simmons RJ, eds.
Photocoagulation in Glaucoma and Anterior Segment Disease. Baltimore: Williams & Wilkins
1984; 150–157.
36. McDonald JE, El-Moatassem Kotb AM, Decker BB. Effect of brimonidine tartrate ophthalmic
solution 0.2% on pupil size in normal eyes under different luminance conditions. J Cataract
Refract Surg 2001; 27:560–564.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 270/338
24
The Limits of Simultaneous AmetropiaCorrection in Phaco-Ersatz
ARTHUR HO and PAUL ERICKSON
The Cooperative Research Centre for Eye Research and Technology, The University
of New South Wales, Sydney New South Wales, Australia
FABRICE MANNS
Bascom Palmer Eye Institute, University of Miami Medical School, Miami, and
University of Miami College of Engineering, Coral Gables, Florida, U.S.A.
VIVIANA FERNANDEZ
Bascom Palmer Eye Institute, University of Miami Medical School, Miami, Florida,
U.S.A.
JEAN-MARIE PAREL
Bascom Palmer Eye Institute, University of Miami Medical School, Miami,
University of Miami College of Engineering, Coral Gables, Florida, U.S.A., and University of Liege, CHU Sart-Tilman Liege, Belgium
A. INTRODUCTION
To the eye-care practitioner, the importance of presbyopia as a major concern need not
be emphasized. Currently, in the United States alone, 35% of the population of 278 million
(1) is presbyopic and therefore requires some form of optical aid for near vision. Further,
the number of presbyopes is increasing. Statistics from the U.S. Census Bureau predictthat over the next decade, the number of people over 45 years of age will increase by
approximately 21 million, but the population under 45 years will remain relatively un-
changed.* This trend foran increasing representation of the over-45 agegroupin thepopula-
* U.S. Census Bureau, International Database, May, 2000. The projected population of the United States in the
year 2010 is 300 million, on increase of 22 million from the figure for year 2001. Of this increase, the (presbyopic)
age group above 45 years age will account for approximately 21 million (1).259

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 271/338
260 Ho et al.
tion is occurring throughout the developed countries. Therefore, increasing emphasis will
be placed on the provision of near vision aids to this sector of the world’s population.
1. Background to Presbyopia Restoration
Unfortunately, currently available devices for near vision assistance—which we may call
the “conventional” presbyopia options—suffer from a number of optical and practical
disadvantages. Devices such as bifocal spectacles, diffractive intraocular lenses (IOLs),
and monovision compromise the position of gaze, field of view, image contrast, or stereop-
sis because of the method by which they provide near focusing power. More critically,
these conventional options do not recreate the continuous focusing ability of the natural
young eye. Of the conventional options available, the progressive aspheric spectacle lens
(PAL) most closely approaches the ideal of providing continuous near focal distance.
However, the continuous focus facility of PALs compromises the position of gaze and
field of view within which the required power may be used and introduces often significant
optical distortions due to the need to employ sophisticated aspheric surfaces in the design
(2,3).
Clearly, none of the conventional options can provide a continuous near focus, full
aperture, and field optical system for the presbyope.
Given the deficiencies of the conventional options, many workers have been engaged
in the development of strategies seeking to truly restore accommodative function to the
presbyopic eye (4–8).
2. Phaco-Ersatz
The strategy of Phaco-Ersatz (4,7,9–11) is to restore accommodation to the presbyopic
eye. In this method (Fig. 1), the contents of the presbyopic crystalline lens is extracted
Figure 1 The procedure of Phaco-Ersatz for restoring accommodation. (A) A corneal incision is
made followed by a very small diameter (ϳ1 mm) capsulorhexis. The lens nucleus, cortex, and
epithelial cells are extracted through the minicapsulorhexis, leaving an intact lens capsule (B). Using
a fine cannula, a polymer gel with the appropriate properties is injected into the lens capsule (C),
reproducing a soft, flexible de novo lens (D). The two controllable variables in this approach, which
forms the basis of the strategies discussed in this chapter, are the refractive index of the polymer
gel and the refilled volume of the de novo lens.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 272/338
261Phaco-Ersatz
through a small (around 1 mm in diameter) capsulorhexis and is replaced with a soft
polymer gel that is injected into the intact lens capsule. Accommodation is restored by
replacing the hardened lens with a polymer gel that recreates the flexibility of the young
lens.
Phaco-Ersatz can restore up to 4 D of accommodation in the senile nonhuman primate
when a silicone gel is used as the lens refillant (9,10). The most recent developments have
refined Phaco-Ersatz by using more sophisticated polymer gels that do not leak out of the
capsule and by improving the delivery of the surgery (11–14).
Modern Phaco-Ersatz has reached a sufficiently advanced stage that our attention
may now be extended to address other patient-related issues. Certainly with the Phaco-
Ersatz method, it is possible for the patient to employ any of the conventional options for
correcting static refractive error such as spectacles and contact lenses. However, patients
strongly prefer to avoid any form of ophthalmic appliance. This is evident by the increasing
development in and popularity of refractive surgery. Hence, an ability to simultaneously
correct refractive error while restoring accommodation would significantly enhance the
attractiveness and acceptability of any such procedure for presbyopia correction.
3. Simultaneous Correction of Ametropia
Surgical vision correction options such as radial keratotomy (RK), photo-refractive kera-
tectomy (PRK), laser-assisted in situ keratomileusis (LASIK), keratoprostheses (e.g., cor-
neal inlays) and phakic IOLs may also be used with Phaco-Ersatz. Together, these would
restore accommodation as well as correct the ametropic patient.
However, there are advantages in providing a Phaco-Ersatz procedure that can, by
itself, simultaneously correct ametropia. For example, there would be reduced risk because
only one instead of two surgical procedures is required. Further, the disadvantages [e.g.,
postsurgical corneal haze and discomfort in PRK and LASIK (15,16)] of some of the
aforementioned vision correction options may be obviated.
The purpose of this chapter is to investigate the feasibility of strategies intrinsic to
the Phaco-Ersatz procedure that could simultaneously correct ametropia while restoring
accommodation.
4. Two Intrinsic Approaches
As the Phaco-Ersatz procedure can principally modify the crystalline lens physical param-
eters, we are limited to two intrinsic strategies by which ametropia may be corrected
simultaneously:
1. controlling the refractive index of the refillant
2. controlling the refilled volume of the de novo lens
The first strategy relies on controlling the power of the de novo lens by increasing
or decreasing the refractive index of the polymer gel used for refilling. Assuming that the
other properties such as curvature and thickness are not altered, this strategy is conceptuallyrelatively straightforward. Using a polymer gel with a lower refractive index would reduce
the power of the crystalline lens, thereby reducing the power of the total eye. This could
be used to correct myopia. Conversely, polymer gel with a higher refractive index would
increase the power of the eye and be useful for correcting hypermetropia.
The implementation of this first strategy requires polymer gels with a range of
refractive indices to be synthesised and made available for Phaco-Ersatz. During the opera-

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 273/338
262 Ho et al.
tion, the surgeon would choose a polymer gel with an appropriate refractive index for the
correction of the patient’s particular amount of ametropia.
The second strategy involves altering the volume of the de novo lens with a view
to altering the anterior and posterior curvatures and thickness. By doing so, the power of
the crystalline lens and hence the total power of the eye can also be altered.
This second strategy can be implemented in two ways. Firstly the refractive error
of the patient could be measured prior to operation and the appropriate volume for refilling
calculated and used. Alternatively, an in-line refractometer could be used to monitor the
refractive state of the eye during refilling to provide an endpoint indication to the surgeon
when the correct volume has been reached.
Given the simplicity of these strategies, their applicability and feasibility is worthy
of evaluation.
While the concepts relating to these two strategies are relatively simple, there are
numerous difficulties that render the evaluation of the feasibility of these strategies imprac-
tical by physical in-surgery means. For instance, in order to evaluate the feasibility of
controlling refractive index of the refillant, a range of polymers would need to be synthe-sized first. Even then, extraneous factors, such as the mechanical properties of the range
of polymer gels, would need to be controlled in order to return valid results.
With these constraints, analyses by theoretical modeling provide a good, workable,
first approximation as an alternative to evaluation of the feasibility of these strategies. In
the remainder of this chapter, we endeavor to evaluate, by computer-assisted modeling,
the feasibility of controlling refractive index and controlling refilled volume as strategies
for the simultaneous correction of ametropia with Phaco-Ersatz.
5. Controlling Refractive Index
As mentioned, this strategy involves the management of the refractive status (or “error”)
of the eye through controlling the power of the de novo lens by controlling its refractive
index. A hint as to the feasibility of this strategy came from early studies in lens refilling
that coincidentally made use of materials of a low refractive index. In those studies, the
eye with de novo lenses with low refractive index were found to be hypermetropic (17).
However, altering the refractive index of the lens has an accompanying effect on
the amplitude of accommodation. Hence, while ametropia may be correctable by control-
ling the refractive index of the refillant, it is equally important to ensure that the resultant
amplitude of accommodation is sufficient for near work. Therefore, any analysis of the
feasibility of this strategy must take into account the range of ametropia that is correctable
as well as the impact on the amplitude of accommodation.
We reported on such a study (18) in which the feasibility of simultaneous correction
of ametropia with Phaco-Ersatz through controlling the refractive index of the polymer
gel was analyzed by theoretical modeling (Fig. 3).
We analyzed a paraxial [Gullstrand no 1 Schematic Eye (19)] and a finite asphericeye [Navarro aspheric model eye (20)] using paraxial optical equations and computer-
assisted optical ray tracing (Zemax version 9, Focus Software Incorporated, AZ) respec-
tively. Both refractive and axial refractive ametropia were analyzed. In each case, the
refractive index of the gel varied between 1.34 and 1.49. A backward ray trace (from
retina to air) was conducted to find the corresponding far point of the eye. The accommoda-
tion state of the model eye was then set to a nominal value of 10 D and the backward ray

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 274/338
263Phaco-Ersatz
trace repeated to find the near point. The amount of correctable ametropia was obtained
from the first ray trace. The difference in results between the second and first ray trace
yields the associated amplitude of accommodation.
B. RESULTS
1. Refractive Error Correction
Using the Gullstrand model eye and a refractive index range of 1.34 to 1.49 for the refillant,
the range of correctable refractive ametropia is between 11.0 D and 14.6 D, and
12.6 D and 12.4 D for refractive and axial ametropia, respectively (Fig. 2). For the
Navarro eye, this range is between 12.4 D and 12.2 D, and 14.6 D and 10.9 D
for refractive and axial ametropia, respectively.
2. Amplitude of Accommodation
When the refractive index of the refillant ranges from 1.34 to 1.49, the amplitude of
accommodation ranges from near zero to 14.6 D and 13.4 D for refractive and axial
Figure2 Refractive and axial ametropia correctable by varying the refractive index of the polymer
gel in Phaco-Ersatz for two model eyes. Interpolation of the Gullstrand results indicates that the
lens cortex and nucleus may be replaced by an equivalent single uniform refractive index of 1.409
to achieve emmetropia. (From Ref. 18.)

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 275/338
264 Ho et al.
hypermetropia, respectively, with the Gullstrand eye model, and to 9.7 D and 8.9 D for
refractive and axial hypermetropia, respectively, with the Navarro model. The nominal
state of accommodation was equivalent to 10 D in all cases.
3. Discussion
It should be noted that the reported theoretical analysis (18) is based on a key assumption
that the shape of the refilled lens does not differ significantly from the original natural
lens. This assumption is probably reasonable given that the shape of the young lens is
determined largely by the properties of the capsule (21,22). Thus, provided the mechanical
properties of the polymer gel refillant closely mimic those of the young natural lens, large
departures from the natural shape are presumed to be unlikely (Fig. 3).
The implications of controlling the refractive index of the refillant on correction of
ametropia and amplitude of accommodation is shown by combining the data from Figs.
2 and 3 (Fig. 4). The amplitude of accommodation progressively decreases as we attempt
to correct higher amounts of myopia. In the limiting case, the correction of a 12 Dmyope would result in virtually no accommodation being available. At this point, the
refractive index of the refillant is almost identical to that of the surrounding ocular media
and hence, the de novo lens has near zero power and consequently is also incapable of
providing accommodative power.
Figure 3 Amplitude of accommodation resulting from varying the refractive index of the polymer
gel in Phaco-Ersatz for two model eyes and ametropia types. (From Ref. 18.)

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 276/338
265Phaco-Ersatz
Figure 4 Relationship between the amplitude of accommodation and the amount of ametropia
that was correctable for two model eyes and ametropia types. (From Ref. 40.)
A practical limit to the range of ametropia that is correctable may be derived by
assuming a required minimum amplitude for accommodation. For example, if a standardnear work distance of 40 cm is adopted and assuming that an additional 50% of accommo-
dative amplitude is required in reserve at all times for comfortable, prolonged reading
(23), we set the acceptable minimum amplitude of accommodation at around 5 D. With
this value, Figure 4 indicates that, for the Gullstrand model eye, myopia greater than 2.5
D should not be corrected by reducing the refractive index of the refillant. According to the
Navarro model, no corrections for myopia are acceptable with the assumed requirements.
In addition to the limitation on myopic corrections, the following practical issues may
also impact the feasibility of this strategy. These issues are as follows:
The need for a series of polymer gels with a large range of refractive indexes to be
available for Phaco-Ersatz. The synthesis of such a range of polymers with similar
mechanical properties and biocompatibility factors poses a daunting technical
challenge to polymer developers.The accuracy required for correction of ametropia to an accuracy of 0.125 D
would require the refractive index to be controlled to an accuracy of 0.0008.
This accuracy needs to be maintained over its working life despite potential
changes in hydration and fouling.
Correction of ametropia with this strategy is limited to spherical refractive errors.
Astigmatic correction is not feasible.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 277/338
266 Ho et al.
Figure 5 Geometrical definitions of the two models for under- and overfilling of the crystalline
lens. (A) Model 1 describes the “spherization” model. The “normal” lens is defined by an ellipsoid
of revolution with major and minor axes a and b (see Table 1). When the lens is under- or overfilled,
its major and minor axes are defined by a′ and b′. A scaling factor is used to determine a′ and b′
from a and b [Eq. (2a) and (2b)]. With this set of equations for defining a ′ and b′, the effect is that
as the lens volume changes, there is a more rapid accompanying change in the curvature of the
anterior than the posterior lens surface. (B) Model 2 describes the “proportional expansion” model.
In this model, a′ and b′ are set by a scaling factor according to Eqs. (3a) to (3c). This model provides
for a more rapid accompanying change in the posterior curvature of the lens surface as lens volume
changes. Note that the scaling factor [s in Eqs. (2a), (2b), (3b), and (3c)] is used only as a parameter
for computation. The relationship between this scaling factor and lens volume is different for the
two models.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 278/338
267Phaco-Ersatz
Figure 6 The relationship between the equivalent power of the crystalline lens and its thickness,
with lens volume according to Models 1 and 2.
Correction of anisometropia is also not feasible, as such an attempt would result in
anisoaccommodation. Further, the result at near is an induced anisometropia of
the opposite sign to the original state of anisometropia.
A further issue relates to ocular aberrations. There is evidence (24–26) that the
spherical aberration of the eye changes over the range of accommodation (Figure 5). It
has been postulated that this change in spherical aberration with accommodation is an
effect of the refractive index gradient of the crystalline lens (27) (Fig. 6). When this
gradient is replaced by a uniform refractive index, ocular aberration during near work
with the de novo lens would differ from the natural lens and may affect near visual
performance (Fig. 7). Conversely, the greater positive aberration might increase depth of
focus and reduce the accommodative demand and, more significantly, permit greater toler-
ance in the accuracy of ametropia correction.
While a number of limitations have been presented above with respect to the strategy
under discussion, it should be noted that a few of these (e.g., requirement of accuracy of
refractive index) apply not just to controlling refractive index within Phaco-Ersatz but
also to any nonaccommodating polymer-based intracapsular ametropia correction devices(e.g., injectable IOLs) as well (Fig. 8).
4. Summary
While conceptually attractive, it is clear from the foregoing findings and the number of
potential implementation difficulties that significant challenges will face any attempt to
introduce this strategy as a method for correcting ametropia within Phaco-Ersatz.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 279/338
268 Ho et al.
Figure 7 Refractive and axial ametropia correctable by controlling the refilled volumed of the
crystalline lens in Phaco-Ersatz according to models 1 and 2 using the modified Navarro eye.
Figure 8 Axial positions of the anterior cornea, anterior and posterior crystalline lens surfaces
and the lens equator and retina as a function of lens volume for refractive and axial ametropia within
models 1 and2. The anterior cornea is located at the x 0 axial position. Note the extreme shallowness
of the anterior chamber and great lens thickness associated with the correction of high amounts of
hypermetropia.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 280/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 281/338
270 Ho et al.
Table 1 The Prescription of the Modified Navarro Eye for Modeling the Relationship Between
Refilled Lens Volume and Ametropia Correction
Surface Radius Thickness Index Diameter Q
Cornea anterior 7.72 0.55 1.376 – Ϫ0.26
Cornea posterior 6.50 3.05 1.3374 – 0.00
Lens anterior 10.20 1.898 1.42 – 4.3740
Lens equator – 3.227 1.42 8.8 –
Lens posterior Ϫ6.00 15.672 1.336 – 0.8595
tion to the anatomical and geometrical parameters of the crystalline lens. This lens model
was based on combining two half-ellipsoids of revolution, as employed by past workers
(27,32). The anterior and posterior radii of curvature of the lens were the same as thoseof the Navarro eye. By setting the length of the major axes (perpendicular to the optical
axis) of the half-ellipsoids to be identical, the continuity of the lens surface at the equator
was ensured. We chose 200 L as a reasonable nominal initial volume of the model lens
to simulate the natural human lens (33).
Given the assumed curvatures, equatorial diameter, and lens volume, the asphericity
and half-thickness of each half-ellipsoid were calculated employing equations relating to
the apical radius of curvature and shape factors of conic sections (34).
Finally, the model eye was “emmetropized” by adjusting the vitreous chamber depth
(distance between posterior lens surface and retina).
The resultant prescription of the modified Navarro model eye for analysis of control-
ling refilled lens volume is given in Table 1. The volume of this lens model is 208 L.
The equatorial diameter of 8.8 mm is slightly less while the thickness of 5.12 mm
is slightly greater than the respective parameters for the typical adult lens (28). However,this was necessitated by a compromise in providing reasonable optical and geometrical
properties to the model.
c. Refilling Model
No information is available in the literature about the quantitative relationship between
lens curvatures and lens volume. Hence, a validated model of the change in lens curvature
with refilling is not possible at this stage. In view of this paucity of information, we
developed two simple but plausible mathematical models for lens refilling. These were:
1. Model 1: “spherization”
2. Model 2: proportional expansion
These two models (Fig. 5) provide contrasting relationships between lens thicknessand curvature with increasing lens volume during refill. In general, Model 1 predicts that
the anterior curvature and half-thickness of the lens will change more quickly than the
posterior curvature and half-thickness as the lens refills during Phaco-Ersatz, while Model
2 predicts the converse. The intention of testing two such disparate models is to provide
a “bracketing” of the results, such that the actual life situation might lie somewhere in
between.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 282/338
271Phaco-Ersatz
Model 1: “Spherization.”
This model assumes that as the lens is filled and then overfilled; it converges toward a
sphere (i.e., the length of the major and minor axes at the endpoint of filling is the same).Hence, the posterior and anterior curvatures would converge with overfilling. Given that
the anterior radius of curvature is greater at the “normal” volume, this model predicts that
with overfilling, the anterior curvature would change more rapidly than the posterior
curvature. We assumed that the lens equator expands slightly with overfilling.
Model 1 is represented mathematically as follows (Fig. 5). The anterior and posterior
half-lenses are represented by half-ellipsoids of revolution such that their two-dimensional
cross sections may be described by
x 2
a2
y2
b2 1 (1)
where x is the distance along the optical axis
y is the distance across the optical axisa is the half-length of the minor axis representing the half-thickness of the lens-half
at normal volume
b is the half-length of the major axis representing the half-diameter of the lens at
its equator at normal volume
Lens refilling according to Model 1 follows the relationship of
a′ s (be a) a (2a)
b′ s (be b) b (2b)
where a′ is the half-thickness of the over-or underfilled half-lens.
b is the half-diameter of the over-or underfilled lens.
be is the radius of the endpoint sphere towards which the shape of an overfilled lenswill converge.
s is a scaling factor defining the amount of over-or underfilling (s 0 is normal
volume of filling, s Ͼ 0 is overfilling, and s Ͻ 0 is underfilling).
Model 2: “Proportional Expansion.”
Model 2 assumes that as the lens is filled and then overfilled, the posterior and anterior
half-ellipsoids increase in axial dimensions (i.e., the length of the minor axis) in the same
ratio. In contrast to Model 1, the posterior curvature in Model 2 would increase more
rapidly than the anterior curvature as the lens overfills. As in Model 1, we assumed that
the lens equator expands slightly with overfilling.
Model 2 is represented mathematically as follows (Fig. 5):
The anterior and posterior half-lenses are again represented by half-ellipsoids of
revolution according to Eq (1). During lens refilling, Model 2 defines the following changesin lens shape:
a′a (a′p aa)/ ap (3a)
a′p s (be ap) ap (3b)
b′ s (be b) b (3c)
where nomenclatures are as for the previous equations and subscript a values pertaining

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 283/338
272 Ho et al.
to the anterior half-lens; subscript p values for the posterior half-lens. For both models,
we assumed be to be 4.9 mm.
5. COMPUTATION AND ANALYSES
a. Calculation of Volume of Over-Underfilling
For a lens constructed of two half-ellipsoids of revolution, the volume V can be calculated
as
V 2
3 b
2 (aa ap) (4)
From Eqs. (1) through (4) and assigning various values for scaling factor s, we can calculate
the volume of the de novo lens at various amounts of filling.
b. Calculation of Lens Power
The central radius of curvature r of an ellipse is given by (34)
r a
b2 (5a)
and its thickness (34) d by:
d aa ap (5b)
From Eqs. (1) through (3) and (5a) and (5b), the assigned refractive indices, and assigning
various values for the scaling factor s, the power of the de novo lens can be calculated
at various amounts of filling.
c. Modeling Correctable Ametropia
Armed with the calculated lens curvatures and thicknesses at different levels of lens refill-
ing, it is now possible to calculate the associated amount of ametropia that is correctable
within the two models using the modified Navarro eye model.
One final variable had to be fixed—that of the position of the lens at different
levels of filling. Because of the enormous complexity of the interactions between capsular
tension, lens volume, vitreous influence, zonular tension and iris influence as well as the
lack of precise, quantitative information in many of these factors, we assumed a simplified
model in which the equatorial plane of the lens remains fixed in the axial ( x ) direction at
all levels of filling. Under this assumption, the anterior and posterior lens surfaces would
bulge forward and backward, respectively, by an amount equal to the change in the length
of the minor axes of the respective half-ellipsoids.
The amount of ametropia correctable was computed in two ways—assuming refrac-
tive ametropia and assuming axial ametropia.
Paraxial optical equations were used in all calculations. Dioptric values of ametropia
were referred to the plane of the cornea on the model eye.
6. Results
Figure 6 shows the relationship between the volume of lens refilled (expressed as a percent-
age of a lens with normal volume) and equivalent refractive power and thickness of the
resultant lens. The resultant lens thicknesses are not greatly different for Models 1 and 2.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 284/338
273Phaco-Ersatz
The refractive power of the refilled lens varied slightly more with change in refilled volume
for Model 1 than for Model 2. This suggests that should lens refilling follow the shape
and thickness changes predicted by Model 1, a greater amount of ametropia may be
correctable.
From the results shown in Fig. 6, the overall power of the eye with a refilled lens,
and hence the amount of ametropia correctable, was computed. This is shown in Fig. 7,
which plots the amount of ametropia that is correctable under Models 1 and 2 for both
axial and refractive ametropia. The maximum ametropia that is correctable occurs using
Model 1 with axial ametropia (approximately 4 D). The minimum ametropia that is
correctable occurs using Model 2 with axial ametropia.
7. Discussion
a. Eye Model
As noted, the geometrical dimensions of the lens model deviated from typical adult human
lenses in that the equatorial diameter was slightly less and the thickness slightly higher.This compromise was necessary to enable simple ellipsoids of revolutions to be used to
construct a model lens while maintaining reasonable values for the optics and geometrical
parameters. A more mathematically sophisticated approach (35) has been developed to
provide an anatomically precise representation of the adult human lens. However, that
model employed a pair of parametric functions within a system of polar coordinates to
describe the lens. Given the parametric nature of the model description, there is no direct
method by which changes in volume and curvature may be modeled without a high level
of mathematical complexity. Hence for convenience, we adopted the half-ellipsoids of
revolution (27,32).
The assumed endpoint diameter of the lens was 8.9 mm, which represents a 0.1-
mm increase in the diameter of a lens when overfilled to 200% (double the volume).
Should this prove to be an overestimation, there would be an increase in the amount of
ametropia that is correctable with controlled lens refilling due to the expected increase incurvatures.
This model is able to estimate only the amount of ametropia that is correctable by
controlling the refilled volume of a lens with Phaco-Ersatz. Due to a number of limitations
relating to quantitative understanding of the influence of lens volume on lens shape during
accommodation, it is not yet possible to study the effect of over- or underfilling on the
amplitude of accommodation, as has been done for the refractive index strategy.
Hence, there may be detrimental effects on the amplitude of accommodation in the
application of this strategy, which are yet to be determined.
The critical assumption in our lens model is that the lens capsule has a negligible
effect on the change in curvature and thickness during refilling. Intuitively, this would
not be the case, given that there is a difference in thickness between the anterior and
posterior capsules (21,36,37), which would influence lens shape and thickness during
refilling. However, we have introduced two contrasting models for refilling with the inten-tion that the actual lens response would lie somewhere within this “bracketing.” We be-
lieve, therefore, that the robustness of the predictions within our model should be reasona-
ble, especially considering that the two contrasting refilling models returned similar
predictions.
Finally, there are effects on aberrations that have not been considered. First, the
gradient index of the natural lens has been eliminated by Phaco-Ersatz. This would alter

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 285/338
274 Ho et al.
the aberration state of the eye at both distance and, as discussed, more critically at near.
Further, as the lens shape changes, it is highly likely that its surface asphericity would also
change, thereby altering the aberrations at different refill volumes. These considerations are
beyond the scope of the current model but merit further investigation.
b. Correction of Ametropia
If we accept the above assumptions and exceptions discussed, then our theoretical analysis
with the eye model predicts the following:
Even at the highest estimate predicted, the amount of ametropia that is correctable
is too low to be practical (Model 1 and axial ametropia). Therefore controlling
the refilled volume alone during Phaco-Ersatz for correcting ametropia is insuffi-
cient to correct any other than low degrees of ametropia.
The reciprocal of the average slope of the four curves in Fig. 7 indicates that in
order to correct ametropia with an accuracy of 0.125 D, percentage refilling
would have to be controlled to an accuracy of 2.3%. This equates to an approxi-mate accuracy in volume of 5 L. This may pose a technical and surgical
challenge.
c. Issues of Implementation
There are also issues of implementation relating to this strategy.
Figure 8 shows the predicted positions of the lens surfaces and retina with changes
in refilled lens volume assuming a fixed position for the equatorial plane. Over the range
of under-to overfilling analyzed (50 to 150%), the lens thickness changes from approxi-
mately 3.5 mm to approximately 8 mm. Even ignoring the effect of the iris and vitreous,
it is certain that such a range would impose impractical values to the resultant anterior
chamber depth. In particular, correction of medium to high hypermetropia would result
in dangerously shallow anterior chambers.In addition to considerations of anterior chamber depth, there are other practical
limits to the amount of over-and underfilling that can be achieved. The minimum amount
of underfilling is set by the lowest volume that can still produce an undistorted, optically
useful de novo lens. Below this limit, prism due to sagging, and distortions due to rippling,
warping, or waviness as a result of a lack of sufficient capsule tension may degrade vision
below acceptable limits.
There is also an upper limit on the amount of overfilling. Beyond this limit, given
the finite breaking strain of the capsule (38,39), rupture of the capsule would occur.
While reliable data on the limits of optical imperfection with excessive underfilling
and capsule rupture with excessive overfilling do not exist, a reasonable estimation may
be assumed on these lower and upper limits. Experience in our laboratories, which has
been conducting surgical trials of Phaco-Ersatz, suggests that a “safe” limit for over- and
underfilling may be 20% of the normal volume. Referring back to Fig. 7, introductionof this limit to the volume of refilling predicts that the range of ametropia that is correctable
is significantly reduced to approximately 2 D. This is probably not a viable range for
useful correction of ametropia.
In addition to the above, other implementation issues relevant to the first strategy
as listed in the previous section also apply. These include a limitation in the range of
correction to spherical (nonastigmatic) refractive errors.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 286/338
275Phaco-Ersatz
8. Summary
Due to the complexity of the interplay between physiology, mechanics, and optics, we
have been able to test only a simplified model of controlled refilling. However, even thisfirst approximation suggests that the range of corrections achievable within this strategy
would be small because of the limitations of lens thickness as well as implementation
difficulties.
9. Conclusions
In this chapter, we have analyzed, using theoretical modeling, the feasibility of two strate-
gies that are intrinsic to Phaco-Ersatz for simultaneous correction of ametropia. It appears
from the results and consideration of implementation issues that neither strategy on its
own is sufficient or feasible for simultaneous correction of ametropia within Phaco-Ersatz.
We have not investigated the feasibility of a combination of the two strategies.
However, in view of the above discussions, it may be expected that those combinations
would also lack sufficient range and accuracy for applicability.
We therefore conclude, even in the absence of physical experimental results, that
simultaneous correction using these two intrinsic strategies would be unattractive and
probably not feasible.
However, predictions from models are only as reliable as the assumptions made and
the values for parameters assumed. We recognize that there are potential shortcomings in
our theoretical analyses, which warrant further research. In particular, the lack of reliable,
quantitative knowledge of relationships such as lens shape and thickness with different
level of refilling—as well as the effect of the capsule thickness, vitreous, and iris on lens
shape and position—merits study as well in order to refine our models. A number of
studies are under way in our laboratories seeking to address such issues (13,30,31). We
believe that researchers in this area should persist in their efforts to understand those
relationships.
REFERENCES
1. US Census Bureau International Program Center. International Database (IDB). update May
2000.
2. Simonet P, Papineau Y, LaPointe R. Peripheral power variations in progressive addition lenses.
Am J Optom Physiol Opt 1986; 63(11):873–880.
3. Sullivan C, Fowler C. Progressive addition and variable focus lenses: a review. Ophthalm
Physiol Opt 1988; 8:402–414.
4. Parel J-M, Gelender H, Trefers W, Norton E. Phaco-Ersatz: cataract surgery designed to
preserve accommodation. Graefes Arch Clin Exp Ophthalmol 1986; 224(2):165–173.
5. Nishi O, Hara T, Hara T, Hayashi F, Sakka Y, Iwata S. Further development of experimental
techniques for refilling the lens of animal eyes with a balloon. J Cataract Refract Surg 1989;15:584–588.
6. Hara T, Hara T, Yasuda A, Yamada Y. Accommodative intraocular lens with spring action:
Part 1. Design and placement in an excised animal eye. Ophthalm Surg 1990; 21:128–133.
7. Parel JM. Phaco-Ersatz 2001: cataract surgery designed to preserve and restore accommodation.
An Inst Barraquer 1991; 22:1–20.
8. Hettlich HJ, Asiyo-Vogel M. Experiments with balloon implantation into the capsular bag as
an accommodative IOL. Ophthalmologe 1996; 93:73–75.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 287/338
276 Ho et al.
9. Haefliger E, Parel J-M, Fantes F, Norton E, Anderson D, Forster R, Hernandez E, Feuer WJ.
Accommodation of an endocapsular silicone lens (Phaco-Ersatz) in the nonhuman primate.
Ophthalmology 1987; 94(4):471–477.
10. Haefliger E, Parel J-M. Accommodation of an endocapsular silicone lens (Phaco-Ersatz) inthe aging rhesus monkey. J Refract Corneal Surg 1994; 10(5):550–555.
11. Parel J-M, Holden B. Accommodating intraocular lenses and lens refilling to restore accommo-
dation (restoring accommodation). In: Azar D, ed. Intraocular Lenses in Cataract and Refractive
Surgery. Philadelphia: Saunders, 2001.
12. Parel JM, Simon G. Phaco-Ersatz 2001: update. Ann Inst Barraquer 1995; 25:143–151.
13. Tahi H, Fantes F, Hamaoui M, Parel J-M. Small peripheral anterior continuous curvilinear
capsulorhexis. J Cataract Refract Surg 1999; 25:744–747.
14. Tahi H, Chapon P, Parel JM, inventors; CRCERT, assignee. Mini capsulorhexis valve (MCV)
for crystalline lens refilling and posterior capsule opacification (PCO) prevention procedures.
United States patent US60/121,179 (US Patent Appl, 2000). PCT/US00/04339 (International
Appl 2000).
15. Wilson S. LASIK: management of common complications. Laser in situ keratomileusis. Cornea
1999; 17(5):459–467.
16. Price F, Jr, Belin M, Nordan L, McDonnell P, Pop M. Epithelial haze, punctate keratopathy
and induced hyperopia after photorefractive keratectomy for myopia. J Refract Surg 1999;
15(3):384–387.
17. Kessler J. Refilling the rabbit lens. Further experiments. Arch Ophthalmol 1966; 76(4):
596–598.
18. Ho A, Erickson P, Manns F, Pham T, Parel J-M. Theoretical analysis of accommodation
amplitude and ametropia correction by varying refractive index in Phaco-Ersatz. Optom Vis
Sci 2001; 78(6):1.
19. Gullstrand A. Appendix II: Procedure of rays in the eye. Imagery—laws of the first order. In:
Southall J, ed. Helmholtz’s Treatise on Physiological Optics. 3rd ed. Optical Society of Amer-
ica, 1909.
20. Navarro R, Santamaria J, Bescos J. Accommodation-dependent model of the human eye with
aspherics. J Opt Soc Am A 1985; 2(8):1273–1281.
21. Fincham E. The mechanism of accommodation. Br J Ophthalmol 1937; Monograph Suppl
VIII:5–80.
22. Nishi O, Nishi K, Mano C, Ichihara M, Honda T. Controlling the capsular shape in lens
refilling. Arch Ophthalmol 1997; 115:507–510.
23. Borish IM. Clinical Refraction, 3rd ed. Chicago: Professional Press, 1970.
24. Atchison D, Smith G. Continuous gradient index and shell models of human lens. Vis Res
1995; 35(18):2529–2538.
25. He J, Burns S, Marcos S. Monochromatic aberrations in the accommodated human eye. Vis
Res 2000; 40:41–48.
26. Gray G, Campin J, Liedel K, Pettit G. Use of wavefront technology for measuring accommoda-
tion and corresponding changes in higher order aberrations. Invest Ophthalmol Vis Sci 2001;
42(4):S26.
27. Smith G, Pierscionek B, Atchison D. The optical modelling of the human lens. Ophthalm
Physiol Opt 1991; 11:359–369.
28. Howcroft M, Parker J. Aspheric curvatures for the human lens. Vis Res 1977; 17:1217–1223.29. Glasser A, Campbell M. Biometric, optical and physical changes in the isolated human crystal-
line lens with age in relation to presbyopia. Vis Res 1999; 39:1991–2015.
30. Hamaoui M, Manns F, Ho A, Parel J-M. Topographical analysis of ex-vivo human crystalline
lens. Invest Ophthalmol Vis Sci 2000; 41(4):S428.
31. Fernandez V, Manns F, Zipper S, Sandadi S, Minhaj A, Ho A, et al. Topography of anterior
and posterior crystalline lens surfaces of human eye-bank eyes. Invest Ophthalmol Vis Sci
2001; 42(4):S880.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 288/338
277Phaco-Ersatz
32. Popiolek-Masajada A. Numerical study of the influence of the shell structure of the crystalline
lens on the refractive properties of the human eye. Ophthalm Physiol Opt 1999; 19(1):41–49.
33. Koretz J, Cook C, Kaufman P. Aging of the human lens: changes in lens shape at zero-diopter
accommodation. J Opt Soc Am A 2001; 18(2):265–272.34. Burek H, Douthwaite W. Axial-radial interconversion. J Br Contact Lens Assoc 1993; 16(1):
5–13.
35. Kasprzak H. New approximation for the whole profile of the human crystalline lens. Ophthalm
Physiol Opt 2000; 20(1):31–43.
36. Salzmann M. Anatomy and Histology of the Human Eyeball in the Normal State: Its Develop-
ment and Senescence. Chicago: University of Chicago Press; 1912.
37. Tahi H, Hamaoui M, Parel J-M. Human lens-capsule thickness: correlation with lens shape
during accommodation and practical consequence for cataract surgery designed to restore
accommodation. Invest Ophthalmol Vis Sci 1999; 40:S887.
38. Krag S, Andreassen T, Olsen T. Elastic Properties of the lens capsule in relation to accommoda-
tion and presbyopia. Invest Ophthalmol Vis Sci 1996; 37(3):S163.
39. Krag S. Biomechanical measurements of the lens capsule. Acta Ophthalmol Scand 1999; 77(3):
364.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 289/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 290/338
25
Accommodating and Adjustable IOLs
SANDEEP JAIN, DIMITRI T. AZAR, and RASIK B. VAJPAYEE
Corneal and Refractive Surgery Service, Massachusetts Eye and Ear Infirmary,
Schepens Eye Research Institute, and Harvard Medical School, Boston, Massachusetts, U.S.A.
A. INTRODUCTION
This chapter focuses on recent developments of accommodating and adjustable intraocular
lenses (IOLs). The former group of lenses is aimed at compensating for the loss of lens
accommodation after cataract surgery, whereas the latter group aims to minimize andcompensate for the unpredictability of refractive outcomes after cataract surgery (1).
B. ACCOMMODATING IOLs
Following cataract surgery, some accommodative functions of the ciliary muscle are re-
tained. Several ophthalmic research groups have developed aphakic IOLs that can to
provide some accommodation based on the maintenance of the accommodative function
of the ciliary muscle. The AT45 (C&C Vision, Aliso Viejo, CA) IOL was designed by
Stuart Cumming, M.D., of Aliso Viejo (1). Khalil Hanna designed the Human Optics
accommodating IOL; these lenses are placed in the capsular bag and are designed to
change position once the accommodative stimulus induces ciliary muscle contraction. The
success of these lenses depends on their ability to achieve high fidelity in transmitting the
accommodative stimulus to the lens capsule after cataract surgery. Clinical studies with
these lenses are under way, and preliminary studies are encouraging (2).
1. Description of Accommodating IOLs
The accommodating AT45 lens is a conventional posterior chamber silicone lens. Its optic
measures 4.5 mm in diameter. It does not have conventional plate or loop haptics but has
279

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 291/338
280 Azar et al.
Figure 1 New intraocular lenses from C&C are designed to move forward into the anterior
chamber to accommodate much like the natural lens. (Courtesy of C&C Vision).
two flexible arms located 180 degrees apart (Fig. 1). These flexible arms allow the lens
to move forward and backward in the posterior chamber on constriction and relaxation
of the ciliary muscle. At the end of each arm is a T-shaped polyamide haptic that follows
the curve of the capsular bag after implantation and maintains centration and stability by
resting in the capsular bag. The HumanOptics designs had a modified steering wheel
appearance which has been modified to allow greater accomodation.
C. MULTICOMPONENT IOLs
Since the advent of refractive surgery, we have been able to correct ametropia to what is
achievable with spectacle and contact lens corrections. This has been especially applicable
to the calculation of intraocular lens power if cataracts occur after refractive surgery.Several formulas have been used to improve the predictability of IOL calculations after
Figure 2 Intraocular lens from HumanOptics designed to move forward into the anterior chamber
to accommodate, much like the natural lens. (Courtesy of HumanOptics).

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 292/338
281Accommodating and Adjustable IOLs
refractive surgery, but surprises are occasionally encountered. Patients who have had re-
fractive surgery and subsequent cataract surgery demonstrate surprising hyperopic errors
in IOL power determination. The ability to correct hyperopic surprises after cataract sur-
gery in patients who have undergone previous refractive surgery would be desirable in
the group of patients who are accustomed to spectacle-free vision (4). The use of adjustable
or multicomponent intraocular lenses is a new concept that allows fine tuning of an already
fairly accurate refractive procedure (Fig. 2).
1. Description of Multicomponent IOLs
The multicomponent intraocular lens is a three-component lens consisting of a base lens
and two additional refractive attachments. The base lens has a planoconvex optical, and
the overall mechanical design of the lens is similar to that of currently used posterior
chamber lenses. The lens is made of polymethylmethacrylate (PMMA) and consists of
one piece, with a diameter of 6.0 mm and an optical aperture of 5.5 mm. The basic lens
looks much like a conventional posterior chamber IOL (PCIOL). The base lens has two
machined slots whose thickness is approximately 1.2 mm. These slots accept the cap lensand hold the assembly together. The base lens is placed into the posterior capsular bag
permanently heals there (Fig. 3). After its implantation, it acts as a platform for the other
two detachable refractive elements (3).
Attached to the base lens are two additional refractive elements. The middle lens,
or sandwich lens, carries the astigmatic (4.00-D sphere and 0.00 to 4.00-D diopter cylinder
Figure 3 Multicomponent IOL. (From Werblin TP. Multicomponent intraocular lens. J Refract
Surg. 1996 S :187–189, with permission).

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 293/338
282 Azar et al.
in 0.25-D increments) correction. This PMMA or silicone lens has an optical aperture of
5.5 mm. The other refractive attachment is a cap lens that has additional refractive power.
This lens may be either monofocal or multifocal. This PMMA planoconvex lens has an
optical clear aperture of 5.5 mm. It has a tab and two small haptics that, during the
assembly, are set into slots in the base lens using a specially modified forceps.
The total central thickness of a multicomponent intraocular lens is 1.88 mm for a
28.00-D lens. This is only slightly thicker than a standard silicone IOL of 20.00 D.
D. LIGHT-ADJUSTED IOL
This lens is also designed to help patients with cataracts who have previously undergone
corneal refractive procedures, in which it is difficult to measure corneal curvature accu-
rately for appropriate IOL calculations.
Calhoun Vision has developed this lens, which may allow for noninvasive adjustment
and correction of residual postimplantation refractive errors following cataract surgery by
applying near-ultraviolet light to the IOL (4). The refractive power of an IOL—composedof a cross-linked silicone polymer matrix, a guest macromer, and a photoinitiator—can
be adjusted. The application of the appropriate wavelength of light onto the central optical
portion of the light-adjusted lens (LAL) polymerizes the macromer in the exposed region,
thereby producing a difference in the chemical potential between the irradiated and nonirra-
diated regions. To re-establish thermodynamic equilibrium, unreacted macromer and pho-
toinitiator diffuse into the irradiated region. As a consequence of the diffusion process and
material properties of the host silicone matrix, the LAL will swell, producing a concomitant
decrease in the radius of curvature of the lens and a corresponding hyperopic shift in the
refractive power of the lens (Fig. 4).
The process may be repeated if the surgeon wants further refractive change in the
lens. The surgeon may then irradiate the entire lens, consuming the remaining, unreacted
Figure4 Cartoon schematic illustrating the proposed mechanism of swelling. (a) Selective irradia-
tion of the central zone of IOL polymerizes macromer, creating a chemical potential between the
irradiated and nonirradiated regions; (b) to reestablish equilibrium, excess macromer diffuses into
the irradiated region causing swelling; and (c) irradiation of the entire IOL “locks” the macromer
and the shape change.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 294/338
283Accommodating and Adjustable IOLs
macromer and photoinitiator. This action effectively locks in the refractive power of the
lens (4).
The surgeon may induce a myopic change by irradiating the edges of the LAL to
effectively drive macromer and photoinitiator out of the lens central region, thereby in-
creasing the radius of curvature and decreasing the power.
One concern with the LAL is that after irradiation, the lens may not necessarily
maintain a resolution efficiency acceptable to the patient. However, preliminary data show
that this light-adjustable silicone IOL materials may provide a means to precisely and
noninvasively adjust IOL power postop, after the refractive status of the eye has stabilized.
E. RESULTS OF ACCOMMODATING AND MULTIFOCAL IOLIMPLANTATION
Calhoun’s adjustable silicone formulations may become a platform technology useful
in both pseudophakic and phakic IOLs. As additional IOLs are developed, such as the
accommodating IOLs of C&C Vision and Human Optics (Erlangen, Germany), the abilityto overcome imprecision in IOL power calculation by postoperative light adjustment has
the potential to add value to these and other novel IOL designs (1–4).
The accommodating IOL is implanted after conventional phacoemulsification sur-
gery through a 3- or 5-mm incision. The AT45 lens is maximally positioned against the
vitreous face and sealed in place with 3 weeks of atropine treatment posoperatively. At
the base of the arms of lens are hinges that allow the lens to move forward, based on
ciliary contraction and pressure from vitreous. Any forward movement of the lens allows
for near vision, simulating natural accommodation (1,2).
The early results of a phase 1 clinical trial show the lens to be safe, complication-
free, and well tolerated. The lens appeared to provide some accommodation. The lens is
still in the evaluation stage and further clinical trials are in progress (2).
The multicomponent lens is still in the process of development, and results of clinical
trials are awaited. The multicomponent lens has been used in a cat model; at 6-monthfollow-up, it was well tolerated.
Werblin has developed a hypothetical human surgical procedure that is analogous
to routine phacoemulsification surgery with implantation of a PCIOL through a 7.00-
mm incision (Fig. 3) (3). Once the base lens is implanted, the cap-and-lens assembly is
intraoperatively affixed by the surgeon to the base lens. The sandwich lens is oriented
at the appropriate astigmatic axis, based on the preoperative assessment of anticipated
postoperative astigmatism.
Once refractive stability is achieved, the patient’s refractive status is evaluated and
the refractive attachments can be removed or changed, depending on the amplitude and
type of residual refractive error or, in case of a multifocal attachment, if the patient is not
satisfied with the quality of vision. Such change or removal involves a second operative
procedure consisting of opening the original wound, detaching the cap-and-sandwich lens
component, and replacing it with new attachments (1,3).In contrast to accommodating and adjustable IOLs, several clinical studies have
evaluated the feasibility and efficacy of multifocal IOLs (1,5–15).
In a prospective study, Vaquero et al. compared the results of implanting the AMO
array multifocal lenses with implanting a monofocal lens (5). Although distance acuity
and contrast sensitivity were similar in both groups, patients with the multifocal lens had
significantly better near acuity. In a prospective, double-masked, comparative clinical trial,

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 295/338
284 Azar et al.
Steinert et al. reported that significantly less correction was required in the multifocal
group than the monofocal group. However, patients in the multifocal group sustained a
small loss of contrast sensitivity (6).
Holladay et al. have evaluated the optical performances of several multifocal lenses
using laboratory and photographic studies (7). They found a two- to threefold increase in
depth of field for all multifocals but also showed a 50% reduction in contrast in retinal
image and a one-line drop in best corrected acuity. Percival and Setty conducted several
clinical trials of multifocal lenses and found them to provide better simultaneous distance
and near acuities in a significantly higher number of patients (8). Bleckman and coauthors
found multifocal progressive IOLs to provide adequate visual performance at various
distances but only in optimal light conditions (9).
In a small-sample retrospective study, Negishi et al. demonstrated that eyes im-
planted with the five-zone refractive multifocal lenses showed better near visual acuity
than control eyes and that the results compared favorably in other aspects of visual function
(10). In a clinical trial, Wille reported a better performance of monofocal lenses for distance
vision when compared to multifocal lenses (11). The mean postoperative acuity was 0.5line higher in the monofocal than in the multifocal group.
After testing contrast sensitivity and glare in patients implanted with diffractive
multifocal IOLs, Winther-Nielsen and coworkers concluded that the most significant loss
of contrast sensitivity is found with central glare under twilight conditions (12).
In a comparative study of monofocal versus multifocal lenses, Vaqero-Ruano, et al.
reported a wider depth of focus and significantly better near vision without addition in
patients with multifocal lenses (13). The contrast sensitivity results at 96 and 50% were
similar. Walkow et al. prospectively evaluated a diffractive versus a refractive multifocal
IOL and found similar and satisfactory functional results with both except that near uncor-
rected vision was significantly better with the diffractive lens (14).
In a case control study, Javitt et al. measured functional status and quality of life
after bilateral implantation of multifocal versus a monofocal IOLs (15). The subjects with
bilateral multifocal IOLs reported better overall vision, less limitation in visual function,
and less spectacle usage than the control subjects with monofocal lenses. The difference
was most significant in ratings of near vision without spectacles.
H. CONCLUSIONS
Based on the relatively high success rate of multifocal IOLs, it is likely that several design
adjustments may need to be incorporated into accommodating and adjustable IOLs before
their use becomes commonplace. It is also likely that several of these technological ad-
vances may have to be combined in order to provide increased predictability for distance
acuity without correction after cataract surgery as well as excellent near visual acuity. The
multifocal IOLs’ ability to provide good distance and near visual acuity is not withoutvisually disturbing loss of contrast sensitivity. Similarly, the success of monovision refrac-
tive surgery does not exceed the 80% mark in most studies (16–19). Accordingly there
will be ample room for innovation in technology and surgical technique to provide excellent
uncorrected distance and near acuities without optical aberrations. The successful prelimi-
nary results of accommodatingand adjustable IOLs will provide the incentive for continued
efforts and developments in this exciting field of research.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 296/338
285Accommodating and Adjustable IOLs
REFERENCES
1. Vajpayee RB, Jain S, Azar DT. Astigmatic intraocular lenses, multifocal intraocular lenses,
and other specialized intraocular lenses. In: Azar DT, ed. Intraocular Lenses in Cataract andRefractive Surgery. Philadelphia: Saunders, 2001: 299– 306.
2. New IOL restored some accommodation in trial. Ocul Surg News. 1999.
3. Werblin TP. Multicomponent intraocualar lens. J Refract Surg 1996; 12:187–189.
4. Schwiegerling JT, Schwartz DM, Sandstedt CA, Jethmalani J. Light-adjustable intraocular
lenses: finessing the outcome. Rev Refract Surg 2002: 23–25.
5. Vaquero M, Encinas JL, Jimenez F. Visual function with monofocal versus multifocal IOLs.
J Cataract Refract Surg 1996; 22:1222–1225.
6. Steinert RF, Post CT Jr, Brint SF, Fritch CD, Hall DL, Wilder LW, Fine IH, Lichtenstein SB,
Masket S, Casebeer C. A prospective, randomized, double-masked comparison of a
zonal—progressive multifocal intraocular lens and a monofocal intraocular lens. Ophthalmol-
ogy 1992; 99:853–861.
7. Holladay JT, van Dijk H, Lang A, Portney V, Willis TR, Sun R, Oksman HC. Optical perfor-
mance of multifocal intraocular lenses. J Cataract Refract Surg 1990; 16:413–422.
8. Percival SPB, Setty SS. Prospectively randomized trial comparing the pseudoaccommodationof the AMO ARRAY multifocal lens and a monofocal lens. J Cataract Refract Surg 1993; 19:
26–31.
9. Bleckmann H, Schmidt O, Sunde T, Kaluzny J. Visual results of progressive multifocal poste-
rior chamber intraocular lens implantation. J Cataract Refract Surg 1996; 22:1102–1107.
10. Negishi K, Nagamoto T, Hara E, Kurosaka D, Bissen-Miyajima H. Clinical evaluation of a
five-zone refractive multifocal intraocular lens. J Cataract Refract Surg 1996; 22:110–115.
11. Wille H. Distance visual acuity with diffractive multifocal and monofocal intraocular lenses.
J Cataract Refract Surg 1993; 19:251–253.
12. Winther-Nielsen A, Corydon L, Olsen T. Contrast sensitivity and glare in patients with a
diffractive multifocal intraocular lens. J Cataract Refract Surg 1993; 19:254–257.
13. Vaquero-Ruano M, Encinas JL, Millan I, Hijos M, Cajigal C. AMO Array multifocal versus
monofocal intraocular lenses: long-term follow-up. J Cataract Refract Surg 1998; 24:118–123.
14. Walkow T, Liekfeld A, Anders N, Pham DT, Hartmann C, Wollensak J. A Prospective evalua-
tion of a diffractive versus a refractive designed multifocal intraocular lens. Ophthalmology1997; 104:1380–1386.
15. Javitt JC, Wang F, Trentacost DJ, Rowe M, Tarantino N. Outcomes of cataract extraction with
multifocal intraocular lens implantation. Functional status and quality of life. Ophthalmology
1997; 104:589–599.
16. Jain S, Azar DT. Eye infections after refractive keratotomy. J Refract Surg 1996; 12(1):
148–155.
17. Jain S, Arora I, Azar DT. Success of monovision presbyopes: review of the literature and
potential applications to refractive surgery. Surv Ophthalmol 1996; 40(6):491–499.
18. Sippel KC, Jain S, Azar DT. Monovision achieved with excimer laser refractive surgery. Int
Ophthalmol Clin 2001; 41(2):91–101.
19. Chang MA, Kloek CE, Zafar S,JainS, Azar DT. Analysis ofstrict monovisionand minimonovi-
sion LASIK surgery in presbyopes. Arch Ophthalmol. Submitted.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 297/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 298/338
26
Accommodative AmplitudeMeasurements After Surgery for
Presbyopia
DAVID L. GUYTON
The Wilmer Institute, The Johns Hopkins University School of Medicine, Baltimore,
Maryland, U.S.A.
A. INTRODUCTION
Several years ago in Houston, Texas, through the courtesy of Dr. Richard Yee, I had the
opportunity to examine and refract two patients after surgery for presbyopia. My observa-tions were not only surprising but also instructive. The surgery had been successful, but
by a different mechanism from that proposed. The answer was in the retinoscopic reflex.
Both patients had undergone Schachar’s scleral band procedures for presbyopia 2
to 3 months before. Both had experienced a beneficial optical effect, and both showed
similar retinoscopic reflexes. The one with the more “complete” effect had the more
striking reflexes. This patient was 56 years old. She had previously been essentially em-
metropic bilaterally and had depended on reading glasses for near vision. She now went
without glasses entirely, with 20/20 uncorrected visual acuity at both distance and near.
She was ecstatic with the result. She had been invited to the clinic for me to examine just
prior to having the scleral bands removed because of erosion through the conjunctiva.
After confirming the distance and near 20/20 uncorrected visual acuity in each
eye, I proceeded with the distance refraction. The retinoscopic reflex was confusing, but
subjective refraction showed only small astigmatic corrections. With these minor correc-tions in place, I placed a small visual acuity chart beneath the peephole of my retinoscope
and asked her to look from distance to near as I observed the retinoscopic reflexes.
B. DYNAMIC RETINOSCOPY
The technique I was using is a form of dynamic retinoscopy first described by Edward
Jackson in 1895 (1). It is a marvelous method to assess the speed and completeness of
287

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 299/338
288 Guyton
Figure 1 Dynamic retinoscopy without lenses. The patient (A), wearing refractive correction if
any, looks alternately between a distant target and a near accommodative target that the examiner
holds just beneath the retinoscope peephole (B). Accommodation is observed objectively by neutrali-
zation of the “with” retinoscopic reflex when the patient accommodates to the plane of the near
target.
accommodation, a method well described in the literature (2–4) (see Fig. 1) but not familiar
to most ophthalmologists. The typical appearance is strong “with” movement with the
patient looking past the edge of the retinoscope at the distance fixation target. As attentionis shifted to the accommodative target just beneath the peephole of the retinoscope and
as the eyes accommodate to this distance, the retinoscopic reflex broadens to neutralization
over about 1/2 s. In other words, the pupil fills with light, and neither “with” nor “against”
movement is visible. This striking change in the retinoscopic reflex can be observed
repeatedly as the patient is instructed to look back and forth between distance and near.
The speed, completeness, and stability of accommodation can thus be observed objectively.
Residual astigmatism is easily detected, and when the procedure is performed under binoc-
ular conditions, anisometropia is evident by unequal neutralization of the two reflexes.
To my surprise, my “rejuvenated” presbyope showed absolutely no perceptible
change in the retinoscopic reflexes when looking from distance to near, and yet she could
easily read the smallest letters on the near acuity chart. The clue to this total lack of
objective accommodation, even though subjective accommodation appeared restored, was
the shape of the retinoscopic reflexes.
C. RETINOSCOPIC REFLEXES
The streak retinoscope gives a linear reflex in eyes with regular spherical or astigmatic
refractive error. In other words, the streak is the same width everywhere along its length.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 300/338
289Accommodative Amplitude Measurements
Figure 2 The retinoscopic reflex seen with (A) the eye focused well beyond the retinoscope; (B)
the eye focused just beyond the retinoscope; (C) a multifocal crystalline lens focused for distance
in the center of the pupil and for near in the periphery of the pupil.
Typical reflexes are illustrated in Figure 2A, which shows the eye focused well beyond
the retinoscope. Figure 2B shows the eye focused just beyond the retinoscope. If the eye
were focused exactly in the plane of the retinoscope peephole, the red retinoscopic reflex
would totally fill the pupil.
D. MULTIFOCAL CRYSTALLINE LENS
My patient’s reflexes correlated with neither Figure 2A nor Figure 2B but rather with
Figure 2C. The streak was narrow in the center and broad at the top and bottom, in an
hourglass shape. This shape persisted as the streak was rotated from one meridian to the
next. Clearly the eye was focused for distance in the center of the pupil and for near in
its periphery. A multifocal crystalline lens appeared to have been created by the procedure.
(This appearance changed little as the retinoscope was moved off axis, indicating that the
multifocal effect was in the crystalline lens, not in the cornea.)
E. INCREASED DEPTH OF FOCUS
It now became clear how this presbyopic patient was able to see clearly at both distances.She had been given multifocal crystalline lenses by the surgery. Because the retinoscopic
reflex had not changed from distance fixation to near fixation, no true accommodation
was occurring. The new multifocal effect simply created a huge depth of focus that enabled
both distance and near vision without any active accommodation.
By adding plus lenses to neutralize the centerof the retinoscopicreflex, I observed the
peripheral portion of the reflex to move strongly “against,” confirming that the periphery of
the pupil was myopic with respect to the center. This type of refractive aberration is called
“positive” spherical aberration, most commonly occurring naturally in young children.
When it occurs naturally, however, the zones in the center and periphery are more clearly
defined, with linear streak reflexes in each zone. In my “rejuvenated” presbyope, the
transition from the emmetropic central zone to the myopic peripheral zone appeared more
continuous, resulting in the hourglass-shaped reflex.
F. TRADITIONAL TECHNIQUES FOR MEASURING
ACCOMMODATION
I have not yet had the opportunity to confirm this retinoscopic appearance in other patients
after surgery for presbyopia. If indeed this finding is routinely present, then traditional
methods for measuring accommodation are not applicable to these patients.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 301/338
290 Guyton
Donders’s push-up method of measuring accommodative amplitude becomes instead
a method of measuring the effective depth of focus of the eye, with any contribution due
to true accommodation being impossible to distinguish. Similarly, adding minus lenses
until blur occurs is simply a measure of depth of focus, not of accommodation.
Infrared objective optometers have been used in attempts to measure accommodation
after surgery for presbyopia, but without success (5). Caution must be observed in using
these instruments, however, because some of them use only small portions of the pupil
for the refractive measurement, and small changes in alignment can yield variable results
in the presence of irregular or multifocal optics.
G. WAVEFRONT ANALYSIS
Wavefront analysis methods of measuring the refractive state across the pupil will be able
to determine the refractive state of the multifocal zones in the altered crystalline lenses
observed by retinoscopy. These new methods will also be able to detect whether or not
any true optical changes occur with attempted accommodation (6). To my knowledge,these instruments have not yet been used to measure accommodation after surgery for
presbyopia. I look forward to the results.
H. CONCLUSION
Whatever the mechanism of refractive change produced by surgical procedures for presby-
opia, there is no question that a close focus can be created under certain conditions.
Whether these beneficial effects will prove to be reproducible and stable and whether they
will provide acceptable visual acuity and contrast remains to be seen.
REFERENCES
1. Jackson E. Skiascopy and Its Practical Application to the Study of Refraction. Philadelphia:Edwards and Docker Co., 1895:86–88.
2. Guyton DL, O’Connor GM. Dynamic retinoscopy. Curr Opin Ophthalmol 1991; 2:78–80.
3. Rutstein RP, Fuhr PD, Swiatocha J. Comparing the amplitude of accommodation determined
objectively and subjectively. Optom Vis Sci 1993; 70:496–500.
4. Rosenfield M, Portello JK, Blustein GH, Jang C. Comparison of clinical techniques to assess
the near accommodative response. Optom Vis Sci 1996; 73:382–388.
5. Mathews S. Scleral expansion surgery does not restore accommodation in human presbyopia.
Ophthalmology 1999; 106:873– 877.
6. Gray GP, Campin JA, Pettit GH, Liedel KK. Use of wavefront technology for measuring
accommodation and corresponding changes in higher order aberrations (abstr). Invest Ophthal-
mol Vis Sci 2001; 42:S26.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 302/338
27
Complications of Hyperopia andPresbyopia Surgery
LIANE CLAMEN GLAZER and DIMITRI T. AZAR
Corneal and Refractive Surgery Service, Massachusetts Eye and Ear Infirmary,
Schepens Eye Research Institute, and Harvard Medical School, Boston,
Massachusetts, U.S.A.
A. BACKGROUND
Planning refractive surgery for a myope is like being an experienced golfer with manyclubs to choose from and a good understanding of the potentials and the limitations of
each club. Choosing a procedure for hyperopic refractive surgery, on the other hand, is
more like being a novice golfer, still not quite sure which clubs are useful and which are
optimal under different circumstances. Indeed, there is still no consensus as to the best
methods for the surgical treatment of hyperopia. As one compares the treatment options
that are currently available, a solid understanding of the potential complications of each
refractive procedure will help one choose the most appropriate procedure for each patient.
There are a number of reasons why refractive surgery for hyperopia has not been
as popular as surgery to correct myopia. First, while hyperopia affects approximately
40% of the adult population, it is less visually significant than myopia (1). For example,
approximately 80% of adult hyperopes require corrections of only 3.0 D or less (2).
Accommodation may produce enough additional plus power to focus parallel rays of
light on the retina. Thus, young hyperopes can often compensate and see well until theiraccommodative power weakens and they start experiencing manifest hyperopia in their
mid-to late 30s. It follows that the average age of people seeking hyperopic correction is
approximately 48 years, much higher than those seeking myopic correction (3–5). These
older patients are more likely to suffer from presbyopia, dry eyes, glaucoma, and cataracts.
Finally, hyperopic refractive surgery is more challenging than myopic surgery because it
is more difficult to permanently steepen the central cornea than to flatten it.
291

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 303/338
292 Glazer and Azar
Complications plagued early attempts at hyperopic refractive surgery. The first at-
tempts at hyperopic correction using hexagonal keratotomy, automated lamellar kera-
toplasty, contact laser thermal keratoplasty (LTK), epikeratophakia, and keratophakia often
created more problems than they solved: irregular astigmatism, corneal ectasia, unpredicta-
ble results, or regression frequently occurred. Therefore, these methods of correcting hyper-
opia have been abandoned. In the evolution of hyperopic refractive surgery, the fittest
procedures have proven to be PRK, LASIK, noncontact LTK, phakic intraocular lens
(IOL) implantation, and clear lens extraction with IOL implantation. Of course, even these
procedures can occasionally cause complications.
B. COMPLICATIONS OF PRK AND LASIK
Excimer lasers are used for both photorefractive keratectomy (PRK) and laser-assisted in
situ keratomileusis (LASIK). When using a laser to achieve correction of hyperopia, the
surgeon creates peripheral annular ablation around the central optical zone to produce
central steepening. This requires excimer lasers with larger ablation diameters than thoseused to correct for myopia. In addition, more tissue must be removed per diopter of
correction for hyperopic versus myopic LASIK or PRK.
1. Hyperopic-Photorefractive Keratectomy (H-PRK)
PRK was introduced as a method for correcting refractive errors in 1983 (6–7). However,
PRK for hyperopia (H-PRK) is still fairly uncommon and certainly much less common
than PRK for myopia. A hyperopic ablation takes approximately three times longer to
perform than a myopic ablation of similar magnitude. It simply takes longer to create a
peripheral ablation zone that will steepen the central cornea than it does to create a central
ablation area that flattens the central cornea (Fig. 1). The time involved increases the
likelihood of dehydration and decentration (8). Decentration may cause irregular astigma-
tism and loss of best corrected visual acuity (BCVA). In addition, regression of effect is
more likely to occur after H-PRK than after a PRK procedure for myopia. Finally, while
the U.S. Food and Drug Administration (FDA) has approved PRK for the correction of
hyperopia of up to 6.00 D with less than 1.00 D of astigmatism, steepening a cornea
above 4.00 D becomes increasingly difficult: smaller optical zones and greater sensitivity
Figure 1. Hyperopic ablation profile of the VISX STAR Laser. This example of a hyperopic
ablation profile demonstrates the large peripheral ablation zone necessary for H-PRK. (From Ref.
4.)

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 304/338
293Complications of Refractive Surgery
to decentration are evident in higher hyperopic corrections. There are other potential com-
plications of H-PRK (Table 1). For example, PRK produces large (9.5-mm) epithelial
defects, leading to prolonged healing time, and an increased risk of infection while the
cornea is healing. Recurrent corneal erosions are a bothersome potential complication of
PRK. Haze and scar formation may also occur. Postoperative glare may be a nuisance,
particularly for patients with larger pupils.
Table 1 Complications of PRK for Correction of Spherical Primary Hyperopia
Mean Loss of best
No. of follow-up Technique and corrected visual
Study Year eyes (months) microkeratome used Complications acuity (BCVA)
O’Brart (12)
Daya (3)
Jackson (4)
Williams (5)
El-Agha (9)
Haw (10)
1997
1997
1998
2000
2000
2000
43
25
65
41
22
18
6
6
14
12
12
24
Summit Apex Plus
Laser, combining
an erodible mask
and an Axiconsystem
9.5-mm peripheral
zone/6.5-mm
optical zone
Chiron Keracor 116
Excimer Laser
8.5-mm peripheral
zone/5.0-mm
optical zone
VISX Star Excimer
Laser
9.0-mm peripheral
zone/ 5.0-mm
optical zone
VISX Star Excimer
Laser
9.0-mm peripheral
zone/ 5.0-mm
optical zone
VISX Star S2
Excimer Laser
8.8- to 9.0-mm
ablation
diameter/5.0-mm
optical zone
Summit Apex PlusExcimer Laser,
Combining an
Erodible mask and
an Axicon system
9.4-mm peripheral
zone/6.5-mm
optical zone
• 21% subepithelial
haze
• 2.3% recurrent
corneal erosions• 5% irregular
epithelial healing
• 2.3% astigmatic
change
• Յ4.4% halos
• Յ6.7% glare
(Note: Complication
rates combine PRK
patients with PARK
patients.)
• 15.4% filaments in
the eyes
• 21.5% epithelial
erosions
• 23% epithelial ridgeat the site of
epithelial closure
• Յ21% haze
(Note: Complication
rates combine
primary PRK and
secondary PRK
patients.)
• 4.5% transient
peripheral haze in
the ablation zone
• 78% midperipheralstromal haze, sparing
the optical zone
• 23% lost 1 line
• 5% lost 2 lines
• 6.7% lost 2
lines
• 31% lost 1 line
at 6 months
• 2% lost 2 lines
at 6 months
• 29% lost 1 lineat 18 months
• No long-term
loss of BCVA
• 13.6% lost 1
line
• 9.0% lost 2
lines
• 5.5% lost 2 ormore lines
under glare
conditions

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 305/338
294 Glazer and Azar
a. Ablation Zone Decentration
A hyperopic correction, which produces a steepening of the central cornea, is less forgiving
of decentration. And yet centration is more difficult during hyperopic corrective surgerybecause hyperopic eyes tend to be smaller, with smaller corneas, and because the ablation
zone must be large. In addition, H-PRK takes up to three times longer than a comparable
myopic PRK procedure; thus the risk of decentration is higher. Decentration is the H-
PRK complication that is most likely to cause loss of BCVA or irregular astigmatism.
Decentration, with either H-PRK or H-LASIK, may occur either due to a decentered
treatment throughout the ablation (shift) or due to intraoperative drift. Shift can be second-
ary to poor patient fixation or to the surgeon’s error. Drift occurs secondary to involuntary
intraoperative eye movement or to a surgeon’s attempt to correct apparent decentration
during treatment.
Decentration is difficult to treat. Theoretically, one can lift the flap and retreat the
patient with decentration of the treatment in the opposite direction to the previous ablation.
An alternative solution is to use miotics to constrict the pupillary axis and to minimize
optical aberrations. Finally, a hard contact lens may neutralize optical aberrations resultingfrom irregular astigmatism (13).
Techniques to avoid decentration include (1) the creation of larger optical (5-mm)
and ablation (9.0–9.5 mm) zones, (2) the use of faster laser pulses to decrease the ablation
time, and (3) more sophisticated eye-tracking devices. Finally, performing the ablation
under the lowest illumination possible can improve patient fixation.
b. Regression
Regression of effect after H-PRK remains one of the limitations of this procedure. It has
been observed that “aggressive healers,” patients with severe corneal haze and marked
scarring in the region of ablation, had significant regression of their refractive correction.
This observation supports the theory that the mechanisms associated with regression are
the subepithelial deposition of collagen and glycosaminoglycans which occurs duringwound healing and produces a filling in of the ablation and loss of effect (12,14–15).
Some ophthalmologistshave given topical corticosteroids after PRK in an attempt to inhibit
regression. Studies consistently show that while topical corticosteroids (fluorometholone or
dexamethasone) inhibit some regression when used during the first 3 to 6 postoperative
months, this effect is negated approximately 3 months after cessation of steroids (4,14–17).
The development of new strategies to reduce aggressive wound healing and haze after
PRK may prevent post-PRK regression.
c. Haze
One potential post-PRK complication is the development of haze. Fortunately, haze is
less of an issue with H-PRK than it is for myopic PRK. This is because the stromal haze
is most dense at the border of the ablated zone, which is in the peripheral (rather than
central) cornea of eyes treated for hyperopia (Fig. 2). Nevertheless, haze can contributeto regression of effect, as mentioned above. Therefore, it is best to try to prevent haze
formation. Risk factors for haze include small ablation diameters with steep transition
zones, UV exposure, acute systemic viral illness, and ocular surface disorders such as dry
eyes (18–20).
Haze may be prevented by maintaining a good tear film layer with nonpreserved
tears or punctal plugs if necessary. One can encourage patients to decrease exposure to

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 306/338
295Complications of Refractive Surgery
Figure 2 Midperipheral ring of corneal haze, characteristic of the haze seen after PRK for hyper-
opia. (From Ref. 10.)
UV radiation by using sunglasses and a hat for 1 year after PRK is performed. Some
authors suggest preventing formation of the corneal haze with a single intraoperative
treatment of mitomycin C to suppress proliferation of keratocytes. Studies in rabbits have
proven this to be very effective (21). A less aggressive approach is to wait and see if haze
occurs and then to apply mitomycin C to treat corneal haze and reduce the regression that
often accompanies the haze (22). One can treat stromal haze that persists beyond 6 months
with excimer laser retreatment or a transepithelial PRK followed by PRK retreatment.
2. Hyperopic-Laser in situ Keratomileusis (H-LASIK)
Although early trials of hyperopic LASIK (H-LASIK) reported unsatisfactory results with
a high rate of BCVA loss and significant regression, H-LASIK is now supplanting H-
PRK as the refractive procedure of choice for hyperopia (23,24). H-LASIK is associated
with a faster recovery time with less postoperative pain than H-PRK. Initially, H-LASIK
was limited by small outer-zone ablations: microkeratomes that could create only small
flaps as well as unrefined excimer laser algorithms contributed to the poor results of early
H-LASIK. With the development of keratomes that are able to create 9.5-mm rather than
the older 8.5-mm flaps, H-LASIK has become safer. In addition, better algorithms and
nomograms are being developed as we accrue more experience with H-LASIK.
Limitations of LASIK for the treatment of hyperopia include problems with predicta-
bility, regression, and difficulty treating hyperopia greater than 4 D. Complications of
H-LASIK can be divided into three groups. First are the complications specific to thesurgical correction of hyperopia itself. As discussed above, these include the older age of
the patients and the length of time of the procedure. Second, there may be intraoperative
complications, including flap complications and ablation-related complications. Finally,
postoperative complications include infection, flap complications, striae, diffuse lamellar
keratitis, epithelial ingrowth, decentration, corneal ectasia, and, rarely, retinal complica-
tions (Table 2).

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 307/338
296 Glazer and Azar
Table 2 Complications of LASIK for Correction of Spherical Primary Hyperopia
Mean Loss of best
No. of follow-up Technique and corrected visualStudy Year eyes (months) microkeratome used Complications acuity (BCVA)
(continued )
Suarez (25)
Ditzen (26)
Goker (27)
Knorz (28)
Esqucnazi (29)
Lindstrom (30)
1996
1998
1998
1998
1999
1999
154
43
54
23
100
46
3
12
19
12
12
6
Coherent/Schwind
Keratom II
Excimer Laser
Automated Corneal
Shaper
8.5-mm flap diameter
MEL 60 Excimer
Laser
Automated Corneal
Shaper
8.5-mm flap diameter
Keracor 116 Excimer
Laser
Automated Corneal
Shaper
8.5-mm flap diameter
Keracor 117 Excimer
Laser
Automated Corneal
Shaper
8.5-mm flap diameter
Keracor 117CT
Excimer Laser
Automated Corneal
Shaper
8.5-mm flap diameter
VISX STAR S2
Excimer Laser
Hansatome
9.5-mm flap diameter
• 1.3% corneal ectasia
• Epithelial invasion of
the interface
• Traumatic flap
displacement
• Bilateral haze
• 15% epithelial
ingrowth
• 2.3% haze
• 7.5% scars
• 4.7% vertical
decentration
• 2.3% central island
• 4.7% free cap• 11.6% flap
dislocation
• 11.6% flap folds
• 31.4% epithelial
ingrowth
• 13%
regressed/under-
corrected
• 9.3% glare at 9
months
• 3.7% transient
diplopia that resolved
entirely
• 1.8% irregular flap
cut• 1.8% decentration
• 3.7% irregular
astigmatism
• No significant
complications noted
• 6% epithelial
ingrowth into the
interface
• 4% scars on nasal
side
• 2% ablationdecentration
• 2% transient diplopia
• 5% flap folds
• 6.5% transient
epithelial defect
• 4.3% diffuse lamellar
keratitis
• 2% lost 1 line
• 1.3% lost 2
lines
• 9% lost 1 line
• 4.7% lost 3
lines
• 5.6% lost 2
lines
• 63% of low
hyperopes lost
1 line
• 50% of high
hyperopes lost
1 line
• 6% lost 1 line
at 1 year
follow-up
• 6% lost 2 lines
at 1 year
follow-up• 5% lost 2 lines
at 2 year
follow-up
• 11% lost 1 line
• 2.2% lost 2
lines

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 308/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 309/338
298 Glazer and Azar
or misalignment, which may lead to irregular astigmatism. When pannus exists, a large
flap may cause bleeding, which must be cleared from the bed prior to ablation.
Appropriate preoperative examinations can help one identify and discourage patients
at greater risk for flap complications. Preplaced surgical landmarks that straddle the flap
edge will help with accurate repositioning of the flap in the operative and postoperative
period. In addition, the newer microkeratomesand suction rings create fewer flap complica-
tions.
b. Epithelial Ingrowth
To achieve successful H-LASIK results, the diameter of the corneal flap must be large
enough. Epithelial ingrowth can result from laser energy to the periphery of the flap, or
it may occur secondary to wound edge instability with migration of epithelial cells under
the flap (Fig. 3). Epithelial ingrowth can progress to involve the visual axis, creating
irregular astigmatism and even melting of the overlying flap (13,36).
If epithelial cells under the flap progress toward the visual axis or induce stromal
melting, the flap should be lifted, the stromal bed and flap undersurface should be thor-oughly irrigated and scraped, and the flap should then be repositioned (37).
With larger flaps of 9 to 10 mm, the risk of epithelial ingrowth is greatly reduced,
most likely because this avoids ablation of epithelium beyond the edge of the flap (38).
Other measures one may take to prevent epithelial ingrowth include using dedicated instru-
ments exclusively for interface manipulation, so that these instruments do not come in
contact with the surrounding epithelium. Also, one should be careful to avoid flap folds,
as these may provide a conduit for cell infiltration (13).
c. Decentration
Decentration or small optical zones may lead to irregular astigmatism, causing loss of
BCVA, glare, monocular diplopia or halos, and halo effects. The same principles of de-
centration described above for PRK apply here. For example, whether with PRK or LASIK,
a larger optical zone is more forgiving of a slight decentration. More sophisticated LASIK
ablation profiles may also diminish the risk of decentration: a more gradual transition
zone between ablated and unablated tissue helps minimize epithelial and stromal regenera-
tion, with its subsequent regression.
Figure 3 Epithelial ingrowth after LASIK. (A) Stable epithelial ingrowth at the LASIK interface.
(B) Retroillumination used to view the same area of epithelial ingrowth. (From Ref. 13.)

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 310/338
299Complications of Refractive Surgery
Figure 4 Diffuse lamellar keratitis following LASIK. (A) Diffuse lamellar keratitis 2 days after
LASIK. (B) Diffuse lamellar keratitis, 5 days after LASIK, with central coalescence, scarring, and
stromal melt. (From Ref. 13.)
d. Diffuse Lamellar Keratitis
Although diffuse lamellar keratitis (DLK) is a recently described syndrome, not yet docu-
mented after H-LASIK, it has been reported in approximately 0.2 to 3.2% of cases of
myopic LASIK (13,39–42). DLK is characterized by a proliferation of inflammatory cells
at the LASIK interface (Fig. 4). It can lead to loss of BCVA due to irregular astigmatism
and may also cause stromal corneal melting with induced hyperopia or hyperopic astigma-
tism.
The cause of DLK is still unclear; thus, prevention remains a challenge. When
present, however, DLK must be treated immediately with hourly topical prednisolone
actate 1% and broad-spectrum topical antibiotic coverage. It has been observed that if the
DLK is not resolved by the fifth postoperative day, there is typically central coalescence
of the inflammatory cells, which may lead to central stromal melting and scarring. Thus,if inflammation progresses despite the steroid/antibiotic treatment, the flap should be lifted,
scraped, and irrigated by the fourth postoperative day at the latest (13). The use of topical
intrastromal steroid during LASIK has been proposed as a way of reducing the incidence
and severity of DLK (43).
e. Late Flap Dislocation
One rare, potential H-LASIK complication is traumatic flap dislocation, occasionally seen
months or years after LASIK (44,45). One might expect a slightly greater risk of flap
dislocation in H-LASIK because the flap tends to be wider than that created for myopic
LASIK. For this reason, it would be wise to avoid performing H-LASIK on high-risk
patients, such as boxers. One should also encourage patients to wear safety glasses when
engaging in high-risk sports activities after H-LASIK.
f. Corneal Ectasia
Corneal ectasia is a rare complication. For example, in one of the largest studies of H-
LASIK, Suarez et al. performed LASIK on 154 eyes of patients with simple hyperopia
of between 1.00 and 8.50 D with astigmatism of less than 0.75 D. Suarez et al. had
only two cases of postoperative corneal ectasia, both occurring in patients with high levels
of hyperopia. Keratectasia is most likely due to the mechanical uncoupling of the posterior

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 311/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 312/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 313/338
302 Glazer and Azar
Table 3 Complications of Noncontact LTK for Correction of Spherical, Primary Hyperopia
Mean Loss of best
No. of follow-up Technique corrected visualStudy Year eyes (months) used Complications acuity (BCVA)
Koch (56)
Koch (55)
Alio (57)
Nano (58)
Vinciguerra (59)
1996
1997
1997
1998
1998
17
28
57
182
16
24
24
15
12
12
Sunrise
Technologies
delivery system
1 ring of 8 spots
per ring
Sunrise
Technologies
delivery system
1–2 rings of 8
spots per ring
Sunrise
Technologies
delivery system
2–3 rings of 8spots per ring
Sunrise
Technologies
delivery system
1–3 rings of 8
spots per ring
Sunrise
Technologies
delivery system
3 rings of 8 spots
per ring
• 27% had 0.5 to 1.0
D of induced
astigmatism
• 27% regression
• 29% regression in
the 1-ring group
• 31.5% had total
regression
• 45% regression
• 0.55% decentered
treatment ring
• 0.55% with 1 D of
induced astigmatism
• 25% complained of
halos or ghost
images at 12-month
follow-up
• 6% lost 2 lines
of BCVA
• 7% lost 1 line
of spectacle-
corrected near
visual acuity
• No loss of
BCVA
• No loss of
BCVA
• No loss of
BCVA
3 months, but only 50.8% maintained this level at 15 months. In fact, by 15 months, only
57.8% were within 1.00 D of the intended refraction (57). In addition to regression of
effect, astigmatism may occur as a result of noncontact LTK.
3. Etiology of Regression
Some researchers feel that regression is inherent to the current technique for LTK. The
Ho:YAG LTK technique delivers pulses of energy to the cornea. The pulses themselves
may trigger a mixed shrinkage/relaxation pattern. For example, if the energy pulses are
too low, an insufficient amount of collagen shrinkage is achieved, and the initial refractive
change may gradually be lost. On the other hand, if the laser heats the collagen fibrils to
65 to 70ЊC, collagen relaxation occurs.
Regression after noncontact LTK is more common in younger patients and patientswith thicker central corneas (57). Regression may be due to the elasticity of Bowman’s
membrane and stromal collagen in younger patients, which causes the cornea to return to
its previous shape. Similarly, thicker corneas may be more likely to resume their previous
configuration. At least in rabbit models, noncontact LTK provokes procollagen synthesis
by fibroblastic keratocytes, causing stromal remodeling which can produce irregularities
in the anterior corneal surface leading to epithelial hyperplasia. This in turn, results in an

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 314/338
303Complications of Refractive Surgery
altered corneal curvature (60). While the precise wound healing response to noncontact
LTK in humans is not known, it is possible that both regression and astigmatism may
result from a similar response.
4. Prevention
Investigators are speaking optimistically about a new continuous-wave diode laser that
can change the shape of the cornea without the peaks and troughs of the pulsed Ho:YAG
laser (61,62). The continuous-wave diode laser is expected to avoid tissue overheating,
thereby improving long-term refractive stability. In addition, FDA trials are under way
on a device that uses radiofrequency energy to the peripheral cornea; this may produce
more controlled shrinkage of collagen lamellae (63).
5. Conclusion
One point to remember is that while regression and, less frequently, astigmatism mayresult from noncontact LTK, it is rare for patients to lose even one line of BCVA. No
eyes have been reported to have lost two or more lines of BCVA from noncontact LTK
(55–58). For risk-averse low hyperopes ( 0.75 to 2.50 D), noncontact LTK is a proce-
dure to consider because it causes very few BCVA-threatening complications.
D. COMPLICATIONS OF PHAKIC INTRAOCULAR LENSES ANDCLEAR LENS EXTRACTIONS WITH INTRAOCULAR LENSIMPLANTS
1. Background
While most types of refractive surgeries alter the cornea, the refractive power of the eyecan also be changed by implanting an intraocular lens (IOL) with or without extraction
of the crystalline lens. Barraquer implanted the first phakic intraocular lens in the 1950s
(64). Unfortunately, many of these anterior chamber lenses were poorly finished and had
sharp edges. After Barraquer had implanted almost 500 lenses, significant complications
such as corneal edema occurred, and over 300 of the lenses had to be removed (65). After
this experience, interest in phakic IOLs waned until labs were better able to guarantee the
quality of IOLs.
Intraocular lenses being made today are of much better quality than those used in
the 1950s. A recent study used a scanning electron microscope to analyze the surface
quality of new-generation phakic IOLs; the study showed that these lenses did not have
any defects that would contraindicate their use as phakic IOLs (66). This study examined
the three major types of lenses currently used as phakic IOLs: anterior chamber lenses
(currently used only in myopic eyes), iris-fixated anterior chamber lenses, and posteriorchamber lenses.
2. Complications
Even when perfectly constructed IOLs with smooth surfaces are placed, there is still a
risk of progressive corneal endothelial cell loss secondary to phakic IOLs (67–71). Other

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 315/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 316/338
305Complications of Refractive Surgery
Figure 6 The STAAR Collamer posterior chamber phakic intraocular lens implant. (From Ref.
79.)
an anterior subcapsular cataract developing immediately after surgery in one eye (6.7%),
causing a loss of two lines of BCVA (79).
Because hyperopic eyes tend to be shorter, they are more prone to pupillary block
after implantation of posterior chamber lenses. One study using the Staar Collamer Im-
plantable Contact Lens (ICL) reported 2 of 15 eyes (13%) developing a severe pupillary
block despite two iridotomies that had been performed 2 weeks prior to surgery. The
increased intraocular pressures due to the pupillary block necessitated removal of the
implants (79). Another study of the Staar ICL reported a 12.5% incidence of postoperative
pupillary block. In addition, IOL decentration of more than 1 mm occurred in 2 of the 24
eyes (76).
Sight-threatening complications such as endophthalmitis have been reported to occur
in phakic IOL procedures for myopia and could theoretically occur for hyperopic phakic
IOL implantation procedures as well (75). Occasionally, silicone plate phakic intraocular
lenses need to be removed due to incorrect sizing of the lens and poor fixation within the
sulcus (82). Retinal detachments after phakic IOL implantation have been reported in
4.8% of myopic eyes (74). This complication has not yet been reported in hyperopic eyes.
Iris-fixated phakic IOLs for the correction of high hyperopia can be associated with
serious complications such as corneal decompensation and glaucoma (Fig. 7) (78). Other
risks include cataract formation and glaucoma (pupillary block glaucoma, pigmentary
glaucoma, narrow-angle glaucoma, and malignant glaucoma) (76). Peripheral iridotomies
can treat or prevent pupillary-block glaucoma. Shallow anterior chambers should be a
contraindication to performing an ICL because of the risk of narrow-angle glaucoma. Lensdecentration may also occur.
3. Clear Lens Extraction with IOL Implantation
Clear lens extraction (CLE) with IOL placement has been studied as a surgical correction
of hyperopia. Some of the disadvantages associated with this procedure as a treatment for
myopia are not as a relevant when it is considered as a hyperopic treatment. For example,

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 317/338
306 Glazer and Azar
Figure 7 The Fechner iris-claw intraocular lens implant. (From Ref. 78.)
myopes are more prone to retinal detachments (RDs). But the increased risk of an RD
after clear lens extraction surgery is less relevant in hyperopes. In addition, the loss of
accomodation that accompanies removal of the crystalline lens is a moot point in the high
hyperope, who can see neither at distance nor at near without correction. One problem of
CLE with IOL placement encountered with hyperopes, which is not relevant in myopes, is
the potential need to implant more than one IOL (piggyback IOLs) to correct for hyperopia.Several recent studies on clear lens extraction for hyperopia demonstrate that this
is a safe and effective procedure. Kolahdouz-Isfahani performed clear lens extraction on
18 eyes. Two eyes lost two lines of BCVA, but no reason for the loss of BCVA was
found after a complete ocular examination was performed. Complications included one
case of postcapsular opacification requiring one YAG capsulotomy, one case of a lens
dislocation requiring an IOL exchange, and one case of malignant glaucoma (83). Another
study of 35 eyes reported that no eyes lost BCVA postoperatively. Additional procedures
consisted of one IOL exchange and one PRK for overcorrection, both due to IOL miscalcu-
lations. Posterior capsular opacification developed in 19 eyes (54.2%), requiring 19 YAG
capsulotomies (84). One study of 20 eyes that underwent clear lens extraction and IOL
implantation reported no complications; there was no loss of BCVA and no need for
further procedures. The authors did find, however, that the procedure was less accurate
and less predictable for less than 3.00 D of hyperopia (85).Pop et al. performed CLE with IOLs followed by PRK or LASIK. The only post-
CLE complication in this study was interlenticular opacification (ILO), which occurred
in 14 eyes that had piggyback polyacrylic lenses. Of the initial 65 eyes in the study, 40
eyes received two IOLs (piggyback IOLs) because the lens power needed was higher than
30 D. Thus, 35% of all the piggybacks developed interlenticular opacification. There were
no other reported complications from the CLE surgery (86).

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 318/338
307Complications of Refractive Surgery
Other potential risks of clear lens extraction surgery with IOL implants include the
risks associated with any cataract surgery, such as hemorrhage, retinal detachment, cystoid
macular edema, and endophthalmitis. Approximately 10% of high hyperopes have axial
lengths of less than 21 mm, predisposing them to choroidal effusions.
4. Prevention
As with any type of surgery, many surgical complications of phakic IOL surgery or CLE/
IOL surgery decrease with surgeon experience. Visual complications such as halo and
glare are significantly reduced with increased optic size from 5.0 to 6.0 mm.
When iris-claw lenses are used, the risk of corneal decompensation can be decreased
by using adequate viscoelastic during surgery, so that the IOL does not touch the cornea;
ensuring sufficient anterior chamber depth; and providing long-term monitoring of the
corneal endothelium (78).
Glaucoma is always a potential problem associated with IOL implantation in small,
hyperopic eyes. During clear lens extraction with IOL implantation, peripheral iridectomies
should be performed in eyes with corneal diameters of 11.0 mm or less or axial lengths
of 20 mm or less. Peripheral iridotomies should be performed prior to the implantation
of phakic IOLs.
5. Conclusion
While many daunting complications may occur secondary to phakic IOL implantation or
CLE/IOL implantation, there are certainly many advantages to treatment of hyperopia
with either of these techniques. First, IOL implantation is the only refractive procedure
that can correct higher degrees of hyperopia. Second, it uses skills that physicians who
perform cataract surgery have honed and polished. Finally, it does not require expensive
equipment, such as lasers. Hopefully, more long-term data will be available in the future
to help decrease the rate of potential complications associated with phakic IOL surgery.
E. COMPLICATIONS OF INTRACORNEAL SEGMENTS AND LENSES
1. Background
Intacs, the intrastromal corneal ring segment (ICRS), consists of two 160-degree poly-
methyl methacrylate (PMMA) segments placed in two pockets of the peripheral stroma
(Fig. 8). The procedure is unique in that it retains the potential to be adjusted or reversed.
Figure 8 The Intrastromal corneal ring. (From Ref. 91.)

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 319/338
308 Glazer and Azar
In April 1999, the FDA approved Intacs for myopic correction of 1.00 to 3.00
D with 1.00 D or less of astigmatism. Intacs can also be used to create central corneal
steepening to correct for hyperopia. Studies are currently investigating the use of small
linear segments placed in the peripheral cornea to create shortening of the peripheral length
of the corneal arc, with subsequent central corneal steepening. By altering the thickness
of the insert, one can titrate the refractive effect.
Although there have been no published studies on Intacs for hyperopia, clinical trials
are currently under way in Germany and Spain. These trials have produced promising
preliminary results: study 1 enrolled 19 patients, and at 1 year 95% (18 of 19) achieved
an UCVA of 20/40 or better. Of note, an induced astigmatism of 1.00 D or greater was
seen in 32% (6 of 19) of the cases. Eleven patients were enrolled in study 2, with 6
months of follow-up. Ten of the 11 eyes (91%) were 20/40 or better, and 4 eyes (36%)
experienced an induced astigmatism of 1.00 D or more. Finally, study 3 enrolled 9
patients with 6 months follow up. All patients had an UCVA of 20/40 or better; only 1
patient had an induced astigmatism equal to or greater than 1.00 D (87).
2. Complications
Published studies of Intacs today are for the correction of myopia. However, the complica-
tions of Intacs would be similar whether the segments were placed for the correction of
myopia or for hyperopia. In the FDA phase II and III studies, the incidence of adverse
events was 2% of the 452 eyes enrolled. Complications of the ICRS procedure include
accidental perforation into the anterior chamber (2 eyes), surface perforation of the epithe-
lium anteriorly (3 eyes), significant decentration of the rings requiring removal or reposi-
tioning (5 eyes), and infectious keratitis (1 eye). All eyes in the group of patients with
complications returned to preoperative BCVA by their 6-month follow-up appointment
(88).
Schanzlin reported no serious complications in the 125 eyes that received ICRS in
his study. Minor postoperative problems included one case of transient conjunctivitis,
three cases of filamentary keratitis, and one case of transient iritis. One patient, whoseincision had gone into a region of superior pannus, developed deep stromal blood vessels.
At 12 months follow-up, four patients had a two-line loss of BCVA, from 20/12.5 to 20/
20. All four of these patients had a substantial improvement in their UCVA (89).
Postoperative astigmatism is clearly a significant potential problem, with 20 of 102
patients in one group experiencing post-ICR astigmatism of 1.0 D or more at 3 months
follow-up. Various theories exist as to the cause of the astigmatism; it may be related to
suture tightness (90). Induced astigmatism may also result from postoperative movement
of the intracorneal ring segments. Finally, Intacs-induced astigmatism can result from
irregular stromal and epithelial thickening between the Intacs rings (91).
Reports describe one patient with persistent focal edema due to a small Descemet’s
tear from a lamellar dissection that was too deep. Although the edema necessitated ICR
removal, the patient’s BCVA was 20/20 at exit from the study. One of 102 patients incurred
an intraoperative perforation of Descemet’s membrane, requiring an ICRS explantation(90). Channel deposits associated with Intacs are occasionally seen but are not associated
with impaired visual acuity (88,89).
3. Prevention
One can attempt to prevent postimplant complications through meticulous attention to
positioning, proper incision depth and pocketing, and sterile technique. In addition, proper

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 320/338
309Complications of Refractive Surgery
attention to wound architecture along with adequate closure and tissue approximation with
suturing can minimize the frequency of wound-related complications such as wound gape
and epithelial cysts. One can prevent corneal neovascularization status post-ICRS by avoid-
ing incisions that make contact with pannus or a limbal blood vessel and by warning
against eye rubbing so as to prevent wound dehiscence.
4. Conclusion
Intacs may prove to be a valuable tool for the correction of hyperopia. Advantages over
procedures such as LASIK and PRK include the fact that the Intacs insert is placed in the
peripheral cornea and the central cornea is never violated during the surgical procedure.
In addition, the Intacs devices can easily be removed if necessary. Finally, the refractive
effect can be adjusted by replacement of any of the implanted radial segments. The compli-
cation of induced astigmatism may become less of an issue as more Intacs devices are
implanted: the cause of induced astigmatism may become better understood and thus better
prevented. In addition, surgical technique will be improved as more of these surgeries areperformed.
F. CONCLUSION
Clearly, since hyperopic refractive surgery is entirely elective, the surgeon must have a
thorough understanding of any potential complications of each type of procedure. The
risk/benefit balance is tipping in favor of H-PRK, H-LASIK, or noncontact LTK for low
to moderate hyperopes and toward intraocular lens implantation with or without clear lens
extraction for moderate to high hyperopes. The use of ICRS for hyperopia may be useful
for low to moderate hyperopes; however, long-term results of current studies have yet to
be reported.
Thorough preoperative evaluations and preventive techniques such as those de-
scribed above can help to avoid complications. However, even with the most prepared
surgeon and in the best of hands, complications may occur. Thus, it is essential to provide
patients with a clear understanding of the potential risks of a procedure before proceeding.
REFERENCES
1. Sorsby A. Biology of the eyes as an optical system. In: Duane TD, Jaeger EA, eds. Clinical
Ophthalmology. Philadelphia: Lippincott, 1988:1394–1414.
2. Leibowitz HM, Krueger DE, Maunder LR, Milton RC, Kini MM, Kahn HA, Nickerson RJ,
Pool J, Colton TL, Ganley JP, Loewenstein JI, Dawber TR. The Framingham Eye Study
Monograph. VIII. Visual acuity. Surv Ophthalmol 1980; 24(suppl):472–479.
3. Daya SM, Tappouni FR, Habib NE. Photorefractive keratectomy for hyperopia: six-month
results in 45 eyes. Ophthalmology 1997; 104:1952–1958.4. Jackson WB, Casson E, Hodge WG, Mintsioulis G, Agapitos PJ. Laser vision correction for
low hyperopia. An 18-month assessment of safety and efficacy. Ophthalmology 1998; 105:
1727–1738.
5. Williams DK. One year results of laser vision correction for low to moderate hyperopia.
Ophthalmology 2000; 107:72–75.
6. Marshall J, Trokel S, Rothery S, Schubert H. An ultrastructural study of corneal incisions
induced by an excimer laser at 193 nm. Ophthalmology 1985; 92:749–758.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 321/338
310 Glazer and Azar
7. Marshall J, Trokel S, Rothery S, Krueger RR. Long-term healing of the central cornea after
photorefractive keratectomy using an excimer laser. Ophthalmology 1988; 95:1411–1421.
8. Isfahani AH, Pangilinan R, Shah S. Surgical correction of hyperopia. Ophthalmol Clin North
Am 1997; 9(part 4):599–615.9. El-Agha MSH, Johnston EW, Bowman RW, Cavanagh HD, McCulley JP. Excimer laser
treatment of spherical hyperopia: PRK or LASIK? Trans Am Ophthalmol Soc. 2000; 98:
59–65.
10. Haw WW, Manch EE. Prospective study of photorefractive keratectomy for hyperopia using
an axicon lens and erodible mask. J Refract Surg 2000; 16:724–730.
11. Pacella E, Abdolrahimzadeh S, Balacco Gabrieli C. Excimer laser photorefractive keratectomy
for hyperopia. Ophthalm Surg Lasers 2001; 32:30–34.
12. O’Brart DP, Stephenson CG, Oliver K, Marshall J. Excimer laser photorefractive keratectomy
for the correction of hyperopia using an erodible mask and axicon system. Ophthalmology
1997; 104:1959–1970.
13. Melki SA, Azar DT. LASIK complications: etiology, management, and prevention. Surv Oph-
thalmol 2001; 46:95–116.
14. Gartry DS, Kerr-Muir MG, Lohmann CP, Marshall J. The effect of topical corticosteroids on
refractive outcome and corneal haze after photorefractive keratectomy. Arch Ophthalmol 1992;
110:944–952.
15. O’Brart DP, Lohmann CP, Klonos G, Corbett MC, Pollock WS, Kerr-Muir MG, Marshall J.
The effects of topical corticosteroids and plasmin inhibitors on refractive outcome, haze and
visual performance after excimer laser photorefractive keratectomy: a prospective, randomised,
observer-masked study. Ophthalmology 1994; 101:1565X74.
16. Gartry DS, Kerr Muir MG, Marshall J. The effect of topical corticosteroids on refraction and
corneal haze following excimer laser treatment of myopia: an update. A prospective, random-
ized, double-masked study. Eye 1993; 7:584–590.
17. Fagerholm P, Hamberg-Nystrom H, Tengroth B, Epstein D. Effect of postoperative steroids
on the refractive outcome of photorefractive keratectomy for myopia with the Summit excimer
laser. J Cataract Refract Surg 1994; 20(suppl):212–215.
18. Stojanovic A, Nitter TA. Correlation between ultraviolet radiation level and the incidence of
late-onset corneal haze after photorefractive keratectomy. J Cataract Refract Surg 2001; 27(3):
404–410.
19. Corbett MC, O’Brart DP, Warburton FG, Marshall J. Biologic and environmental risk factors
for regression after photorefractive keratectomy. Ophthalmology 1996; 103:1381–1391.
20. Siganos DS, Katsanevaki VJ, Pallikaris IG. Correlation of subepithelial haze and refractive
regression 1 month after photorefractive keratectomy for myopia. J Refract Surg 1999;
15 8–342.
21. Xu H, Shuangzhen L, Xia A, Huang P, Wang P, Wu X. Mitomycin C reduces haze formation
in rabbits after excimer laser photorefractive keratectomy. J Refract Surg 2001; 17:342–349.
22. Majmudar PA, Forstot SL, Dennis RF, Nirankari VS, Damiano RE, Brenart R, Epstein RJ.
Topical mitomycin-C for subepithelial fibrosis after refractive corneal surgery. Ophthalmology
2000; 107(1):89–94.
23. Ojeimi G, Waked N. Laser in situ keratomileusis for hyperopia. J Cataract Refract Surg 1997;
13(suppl):432–433.
24. Sinan G, Hamdi E, Cegmi K. Laser in situ keratomileusis to correct Hyperopia from 4.25to 8.00 diopters. J Cataract Refract Surg 1998; 14:105.
25. Suarez E, Torres F, Duplessie M. LASIK for correction of hyperopia and hyperopia with
astigmatism. Int Ophthalmol Clin 1996; 36(4):65–72.
26. Ditzen K, Huschka H, Pieger S. Laser in situ keratomileusis for hyperopia. J Cataract Refract
Surg 1998; 24:43–47.
27. Goker S, Er H, Kahvecioglu C. Laser in situ keratomileusis to correct hyperopia from 4.25
to 8.00 diopters. J Refract Surg 1998; 14:26–30.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 322/338
311Complications of Refractive Surgery
28. Knorz MC, Liermann A, Jendritza B, Hugger P. LASIK for hyperopia and hyperopic astigma-
tism—results of a pilot study. Semin Ophthalmol 1998; 13(2):83–87.
29. Esquenazi S, Mendoza A. Two year follow-up of last in situ keratomileusis for hyperopia. J
Refract Surg 1999; 15:648–652.30. Lindstrom RL, Hardten DR, Houtman DM, Witte B, Preschel N, Chu YR, Samuelson TW,
Linebarger EJ. Six-month results of hyperopic and astigmatic LASIK in eyes with primary
and secondary hyperopia. Trans Am Ophthalmol Soc 1999; 97:241–260.
31. Arbelaez MC, Knorz MC. Laser in situ keratomileusis for hyperopia and hyperopic astigma-
tism. J Refract Surg 1999; 15:406–414.
32. Zadok D, Maskaleris G, Montes M, Shah S, Garcia V, Chayet A. Hyperopic laser in situ
keratomileusis with the Nidek EC–5000 excimer laser. Ophthalmology 2000; 107(6):
1132–1137.
33. Reviglio VE, Bossana EL, Luna JD, Muino JC, Juarez CP. Laser in situ keratomileusis for
myopia and hyperopia using the Lasersight 200 laser in 300 consecutive eyes. J Refract Surg
2000; 16(6):716–723.
34. Argento CJ, Cosentino MJ. Comparison of optical zones in hyperopic laser in situ keratomi-
leusis: 5.9 mm versus smaller optical zones. J Cataract Refract Surg 2000; 26(8):1137–1146.
35. Choi RY, Wilson SE. Hyperopic laser in situ keratomileusis: primary and secondary treatments
are safe and effective. Cornea 2001; 20(4):388–393.
36. Castillo A, Diaz-Valle D, Gutierrez AR, Toledano N, Romero F. Peripheral melt of flap after
laser in situ keratomileusis. J Refract Surg 1998; 14:61–63.
37. Walker MB, Wilson SE. Incidence and prevention of epithelial growth within the interface
after laser in situ keratomileusis. Cornea 2000; 19:170–173.
38. O’Brart DP. The status of hyperopic laser in situ keratomileusis. Curr Opin Ophthalmol 1999;
10:247–252.
39. Lin RT, Maloney RK. Flap complications associated with lamellar refractive surgery. Am J
Ophthalmol 1999; 127:129–136.
40. Linebarger EJ, Hardten DR, Lindstrom RL. Diffuse lamellar keratitis: diagnosis and manage-
ment. J Cataract Refract Surg 2000; 26:1072–1077.
41. Smith RJ, Maloney RK. Diffuse lamellar keratitis. A new syndrome in lamellar refractive
surgery. Ophthalmology 1998; 105:1721–1726.
42. Stulting RD, Carr JD, Thompson KP, Waring III GO, Wiley WM, Walker JG. Complications
of laser in situ keratomileusis for the correction of myopia. Ophthalmology 1999; 106:13–20.
43. Peters NT, Lingua RW, Kim CH. Topical intrastromal steroidduring laser in situ keratomileusis
to retard interface keratitis. J Cataract Refract Surg 1999; 25:1437–1440.
44. Lemley HL, Chodosh J, Wold TC, Bogie CP, Hawkins TC. Partial dislocation of laser in situ
keratomileusis flap by air bag injury. J Refract Surg 2000; 16:373–374.
45. Geggel HS, Coday MP. Late-onset traumatic laser in situ keratomileusis flap dehiscence. Am
J Ophthalmol 2001; 131(4):505–506.
46. Vinciguerra P, Camesasca FI. Prevention of corneal ectasia in laser in situ keratomileusis. J
Refract Surg 2001; 17(suppl):S187–S189.
47. Lans LJ. Experimentelle Untersuchungen uber Entstehung von Astigmatismus durch nichtperf-
oririende Corneawunden. Arch Ophthalmol 1898; 45:117–152.
48. Stringer H, Parr J. Shrinkage temperature of eye collagen. Nature 1964; 204:1307.
49. Neumann AC, Sanders D, Raanan M, DeLuca M. Hyperopic thermokeratoplasty: clinicalevaluation. J Cataract Refract Surg 1991; 17:830–838.
50. Seiler T, Matallana M, Bende T. Laser thermokeratoplasty by means of a pulsed holmium:
YAG laser for hyperopic correction. Refract Corneal Surg 1990; 6:335–339.
51. Allain JC, Lous LE, Cohen-Solal: Isometric tensions developed during the hydrothermal swell-
ing of rat skin. Connect Tissue Res 1980; 7:127–133.
52. Durrie DS, Schumer DJ, Cavanough TB. Holmium:YAG laser thermokeratoplasty for hyper-
opia. J Refract Corneal Surg 1994; 10:S277–S280.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 323/338
312 Glazer and Azar
53. Goggin M, Lavery F. Holmium laser thermokeratoplasty for reversal of hyperopia after myopic
photorefractive keratectomy. Br J Ophthalmol 1997; 81:541–543.
54. Tutton MK, Cherry PKM. Holmium:YAG laser thermokeratoplasty to correct hyperopia: two
years follow-up. Ophthalmic Surg Lasers 1996; 27(5 suppl):S521–S524.55. Koch DD, Kohnen T, McDonnell PJ, Menefee R, Berry M. Hyperopia correction by noncontact
holmium:YAG laser thermal keratoplasty: U.S. Phase IIA clinical study with 2-year follow-
up. Ophthalmology 1997; 104:1938–1947.
56. Koch DD, Abarca A, Villarreal R, Menefee R, Kohnen T, Vassiliadids A, Berry M. Hyperopia
correction by noncontact holmium:YAG laser thermal keratoplasty: clinical study with 2-year
follow-up. Ophthalmology 1996; 103:731– 740.
57. Alio JL, Ismail MM, Sanchez Pego JL. Correction of hyperopia with non-contact Ho: AG
laser thermal keratoplasty. J Refract Surg 1997; 13:17–22.
58. Nano HD, Muzzin S. Noncontact holmium:YAG laser thermal keratoplasty for hyperopia. J
Cataract Refract Surg 1998; 24:751–757.
59. Vinciguerra P, Kohnen T, Azzolini M, Radice P, Epstein D, Koch DD. Radial and staggered
treatment patterns to correct hyperopia using noncontact holmium:YAG laser thermal kera-
toplasty. J Cataract Refract Surg 1998; 24:21–30.
60. Koch DD, Kohnen T, Anderson JA, Binder PS, Moore MN, Menefee RF, Valderamma GL,
Berry MJ. Histologic changes and wound healing response following 10-pulse noncontact
holmium:YAG laser thermal keratoplasty. J Refract Surg 1996; 12:623–634.
61. Bende T, Jean B, Oltrup T. Laser thermal keratoplasty using a continuous wave diode laser.
J Refract Surg 1999; 15:154–158.
62. Geerling G, Koop N, Brinkman R, Tungler A, Wirbelauer C, Birngruber R, Laqua H. Continu-
ous-wave diode laser thermal keratoplasty: first clinical experience in blind human eyes. J
Cataract Refract Surg 1999; 25:32–40.
63. Sher NA. Hyperopic refractive surgery. Curr Opin Ophthalmol 2001; 12:304–308.
64. Barraquer J. Anterior chamber plastic lenses. Results of and conclusions from five years of
experience. Trans Ophthalmol Soc UK 1959; 79:393–424.
65. Drews RC. The Barraquer experience with intraocular lenses, 20 years later. Ophthalmology
1982; 89:386–393.
66. Kohnen T, Baumeister M, Magdowski G. Scanning electron microscopic characteristics of
phakic intraocular lenses. Ophthalmology 2000; 107:934–939.
67. Landesz M, Worst JGR, van Rij G. Long-term results of correction of high myopia with an
iris claw phakic intraocular lens. J Refract Surg 2000; 16:310–316.
68. Mimouni F, Colin J, Koffi V, Bonnet P. Damage to the corneal endothelium from anterior
chamber intraocular lenses in phakic myopic eyes. Refract Corneal Surg 1991; 7:277–281.
69. Saragoussi JJ, Cotinat J, Renard G, Savoldelli M, Abenhaim A, Pouliquen Y. Damage to the
corneal endothelium by minus power anterior chamber intraocular lenses. Refract Corneal
Surg 1991; 7:282–285.
70. Perez-Santonja JJ, Iradier MT, Sanz-Iglesias L, Serrano JM, Zato MA. Endothelial changes
in phakic eyes with anterior chamber intraocular lenses to correct high myopia. J Cataract
Refract Surg 1996; 22:1017–1022.
71. Menezo JL, Cisneros AL, Rodriguez-Salvador V. Endothelial study of iris-claw phakic lens:
four-year follow-up. J Cataract Refract Surg 1998; 24:1039–1049.
72. Trindade F, Pereira F. Cataract formation after posterior chamber phakic intraocular lensimplantation. J Cataract Refract Surg 1998; 24:1661–1663.
73. Brauweiler PH, Wehler T, Busin M. High incidence of cataract formation after implantation
of a silicone posterior chamber lens in phakic, highly myopic eyes. Ophthalmology 1999; 106:
1651–1655.
74. Ruiz-Moreno JM, Alio JL, Perez-Santonja JJ, de la Hoz F. Retinal detachment in phakic eyes
with anterior chamber intraocular lenses to correct severe myopia. Am J Ophthalmol 1999;
127:270–275.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 324/338
313Complications of Refractive Surgery
75. Perez-Santonja JJ, Ruiz-Moreno JM, de la Hoz F, Giner-Gorriti C, Alio JL. Endophthalmitis
after phakic intraocular lens implantation to correct high myopia. J Cataract Refract Surg 1999;
25:1295–1298.
76. Davidorf JM, Zaldivar R, Oscherow S. Posterior chamber phakic intraocular lens for hyperopiaof 4 to 11 diopters. J Refract Surg 1998; 14:3.
77. Rosen E, Gore C. Staar Collamer posterior chamber phakic intraocular lens to correct myopia
and hyperopia. J Cataract Refract Surg 1998; 24:596–606.
78. Fechner PU, Singh D, Wulff K. Iris-Claw lens in phakic eyes to correct hyperopia: preliminary
study. J Cataract Refract Surg 1998; 24:48.
79. Pesando PM, Ghiringhello MP, Tagliavacche P. Posterior chamber collamer phakic intraocular
lens for myopia and hyperopia. J Refract Surg 1999; 15:415–423.
80. Sanders DR, Martin RG, Brown DC, Shepherd J, Deitz MR, De Luca M. Posterior chamber
phakic intraocular lens for hyperopia. J Refract Surg 1999; 15:309–315.
81. Pershin KB, Pashinova NF. Refractive Surgery of Hyperopia. J Refract Surg 2000; 16(suppl):
S242-S246.
82. Zaldivar R, Oscherow S, Giselle R. The STAAR Posterior Chamber Phakic Intraocular Lens.
Int Ophthalmol Clin 2000; 40:237–244.
83. Visessook N, Peng Q, Apple DJ, Gerl R, Schmickler S, Schoderbek RJ Jr, Guindi A. Pathologi-cal examination of an explanted phakic posterior chamber intraocular lens. J Cataract Refract
Surg 1999; 25:216–222.
84. Kolahdouz-Isfahani AH, Rostamian K, Wallace D, Salz JJ. Clear lens extraction with intraocu-
lar lens implantation for hyperopia. J Cataract Refract Surg 1999; 15(3):316–323.
85. Siganos DS, Pallikaris IG. Clear lensectomy and intraocular lens implantation for hyperopia
from 7 to 14 diopters. J Cataract Refract Surg 1998; 14:105–113.
86. Lyle WA, Jin GJ. Clear lens extraction to correct hyperopia. J Cataract Refract Surg 1997;
23(7):1051–1056.
87. Pop M, Payette Y, Amyot M. Clear lens extraction with intraocular lens followed by photore-
fractive keratectomy or laser in situ keratomileusis. Ophthalmology 2001; 108(1):104–111.
88. Verity SM. Intacs for myopia and hyperopia. Refractive Surgery 2001, American Academy
of Ophthalmology Annual Meeting, New Orleans, 2001, pp 83–87.
89. Linebarger EJ, Song D, Ruckhofer J, Schanzlin DJ. Intacs: the Intrastromal Corneal Ring. Int
Ophthalmol Clin 2000; 40:199–208.
90. Schanzlin DJ. Studies of Intrastromal Corneal Ring Segments for the correction of low to
moderate myopic refractive errors. Trans Am Ophthalmol Soc 1999; 97:815–890.
91. Burris TE. Intrastromal corneal ring technology: results and indications. Curr Opin Ophthalmol
1998; 9:9–14.
92. Reinstein DZ, Srivannaboon S, Holland SP. Epithelial and stromal changes induced by Intacs
examined by three-dimensional very high frequency digital ultrasound. J Refract Surg 2001;
17:310–318.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 325/338

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 326/338
28
Future Developments
BRIAN S. BOXER WACHLER
Boxer Wachler Vision Institute, Beverly Hills, California, U.S.A.
Presently, there are several viable treatments for the correction of hyperopia and presby-
opia. In order to broaden the scope of patient acceptance, current and investigative tech-
niques will continue to develop in the future as the clinicians and researchers strive for
greater efficacy, safety, and visual quality. Each area within refractive surgery will bring
improvements specific unto itself.
A. HYPEROPIA
1. LASIK and PRK
Hyperopic laser-assisted in situ keratomileusis (LASIK) and photorefractive keratectomy
(PRK) have the advantage of directly reshaping the cornea with high safety in low to
moderate degrees of correction. There is growing interest in where hyperopic ablations
should be centered on the eye. Conventional teaching is to center treatments on the pupil-
lary center. This paradigm has developed from a 1987 article by Uozoto and Guyton (1)
that demonstrated, through mathematical analysis, the rationale for pupil centration of
refractive procedures. An opposing article by Pande and Hillman(2) used another set of
analyses to show that the corneal sighted light reflex (which best approximates the visual
axis of the eye) is the best location for centering refractive procedures. Positive angle
kappa (corneal sighted light reflex located nasal to pupilary center) is not nearly as commonin myopes as it is in hyperopes(3). Therefore, since the excimer was used initially for
myopia, the potential for decentered ablations due to pupilary centration was low. I believe
that the combination of delayed hyperopic excimer capability and the lower number of
such patients undergoing treatments has obscured the issue that hyperopic ablations and
perhaps myopic ablations as well may be better centered on the corneal sighted light reflex.
Over 2 years ago, I began to question the recommendation of the Uozoto and Guyton
315

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 327/338
316 Boxer Wachler
Figure 1 Decentration of the treatment zone is seen in the right eye compared to the left eye in
the hyperopic patient will bilateral angle kappa. The laser ablation was centered on the pupil in the
right eye and on the coaxially sighted corneal light reflex in the left eye.
article after noting the decentrations of hyperopic LASIK was not uncommon in my
practice. In one hyperopic patient with angle kappa, I centered the hyperopic treatment
on the pupil on the first eye; on the second eye, the treatment was centered on the cornealsighted light reflex(4). The postoperative topographies demonstrate decentration of the
treatment in the eye where the laser was centered on the pupil, while the fellow eye showed
a centered ablation (Fig. 1). This area will undergo further study, evaluating not only
topography but also visual acuity, contrast sensitivity, and higher-order aberrations.
The dioptric limits of hyperopic excimer correction are not entirely clear. Therefore,
there will be better definitions of the limitations of hyperopic ablations, which may be
defined by acceptable degrees of induced higher-order aberrations. The pupil is the guard-
ian of the aberrations of the eye. Based on individual pupil-dependent aberrations, future
studies will likely determine the limits of hyperopic treatments.
In myopic LASIK, the flap itself has been shown to be a source of higher-order
aberrations, specifically spherical aberrations(5). In hyperopic LASIK, it is unknown what
role flap-induced aberrations play. We can expect to see such evaluations in the future
for hyperopic LASIK compared to hyperopic PRK.
2. Thermokeratoplasty
Laser thermokeratoplasty (LTK)has the advantage of being very safe due to its noncontact
modality, which also avoids surgery in the central cornea. As an indirectly acting proce-
dure, one of its limitation is that the variable corneal steepening may occur with the same

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 328/338
317Future Developments
degree of treatment, also that some eyes have more instability of the effect than others.
The future of LTK lies in the ability to perform intraoperative, real-time refractive monitor-
ing using wavefront analysis during the treatment. This may allow the surgeon to stop
the treatment when the desired refractive effect is achieved, making the treatment indepen-
dent of corneal physiology, dehydration, stiffness, and surgeon technique. Preliminary
results of lower-energy treatments hold promise for more stable postoperative effects.
Like LTK, conductive keratoplasty (CK) offer the advantage of avoiding the central
cornea. CK will be evaluated for additional uses, as for astigmatism, by steepening the
flat axis (opposite to astigmatic keratotomy, whereby the steep axis is flattened). The
ability of the probe to be used selectively may make this device useful for treating irregular
astigmatism, as in keratoconus. Focal heat treatments of keratoconus have been evaluated
in the past, but the controlled temperature gradient of CK may lead to more stability than
previous probe technologies.
3. Intraocular Lenses
Phakic intraocular lenses offer the advantage of high-quality of vision in higher corrections
as well as being removable. Phakic lenses will continue to undergo safety evaluation with
longer-term follow-up. Such lenses have the ability to treat higher degrees of hyperopia
than excimer lasers. Wavefront analysis will help determine the optical advantages of
phakic implants compared to excimer laser treatments. Adjustability of lens power may
be achieved in the future through exchangeable optic with a haptic carrier or thoroughly
laser adjustments of the optic postimplantation.
B. PRESBYOPIA
1. Scleral Expanding Bands
Scleral expansion surgery, although not without controversy, has been slowly gaining
credibility. The data from international and preliminary U.S. Food and Drug Administra-
tion clinical trial results demonstrate improved reading ability postoperatively. As a result,
there will be greater attention paid to refining this technique and improving accommodative
predictability. Ultrasound will be used to elucidate the relationship to segment positioning
relative to zonules and lens capsule and how this affects postoperative accommodative
amplitudes. Surgical intrumentation will improve, thus decreasing the duration of what is
now an approximately 45-min procedure. The new device, called the “Focal One,” is an
automated blade that creates the belt loops and has already improved efficiency in perform-
ing the procedure.
2. Multifocal LASIK and Intraocular Lenses
Presbyopic LASIK has the advantage of improving near vision in carefully selected pa-
tients. Wavefront analysis will be an important adjunct to help elucidate the acceptable
induced aberrations that maximize near vision without compromising quality of vision.
Some monofocal intraocular lenses made with wavefront optic profiles have been reported
to improve near vision with distance as well. Accomodating endocapsular intraocular
lenses will continue to be evaluated for longer-term safety and efficacy.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 329/338
318 Boxer Wachler
C. Conclusions
We are beginning a new era as refractive surgery now embraces the challenge of correcting
presbyopia. Through the creativity and determination of many ophthalmic care providersand investigators, greater numbers of patients are experiencing the increased freedom that
comes with treating hyperopia and presbyopia. The future is very bright for the surgical
correction of hyperopia and presbyopia.
References
1. Uuzoto H, Guyton DL. Centering corneal surgical procedures. Am J Ophthalmol 1987; 103:
264–275.
2. Pande M, Hillman JS. Optical zone centration in keratorefractive surgery. Entrance pupil center,
visual axis, coaxially sighted corneal reflex, or geometric corneal center? Ophthalmology 1993;
100:1230–1237.
3. Burian HM. The sensorial retinal relationships in comitant strabismus. Arch Ophthalmol 1947;
37:336–340.4. Korn T, Chandra N, Boxer Wachler BS. Visual outcomes of hyperopic LASIK: centration based
on pupil center versus visual axis. American Society of Cataract and Refractive Surgery Annual
Meeting, April 2001.
5. Roberts C. Flap-induced spherical aberrations. Videorefractiva Italy Ophthalmology Congress.
February 2001.

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 330/338
Accommodative mechanism, debate, 34
Accommodative tone, 211
Accommodative triad, 31
ACS (See Anterior ciliary sclerotomy (ACS))
ACS-SEP, 214
Age-related cataract (ARC), 58
Aging
crystalline lens, 55–63
size and shape, 56–57
oxidative stress, 58–59
presbyopia, 57–58
refractive error, 57
zonule, 60
AIS, 223–224, 232
ALK, 5, 164
Alternating-vision bifocal contact lenses, 68
American Optical vectographic test, 195
Ametropia
correctable modeling, 272
correction, 261
simultaneous within Phaco-Ersatz, 269
AMO ARRAY, 238, 239
foldable silicone multifocal intraocular
lens, 250
Amplitude of accommodation, 19
simultaneous ametropia correction
Phaco-Ersatz, 263 –264
Index
Aberrations
defined, 151
hyperopia vs. myopia, 159
Ablation zone decentration, 294
Accommodating and adjustable intraocular
lens (IOL), 279–285
results, 283–284
Accommodation
defined, 30–31
Fincham, 40–42
Gullstrand, 39– 40
Helmholtz description, 32–33
measurement, 36–38
near vision, 19–20
optical changes, 30–32
scleral expansion surgery, 44
Accommodative amplitude, 20, 213
after surgery for presbyopia, 287–290
dynamic retinoscopy, 287– 288
increased depth of focus, 289
measuring accommodation, 289– 290
multifocal crystalline lens, 289
retinoscopic reflexes, 288–289
wavefront analysis, 290
Accommodative apparatus, anatomy, 27– 28
Accommodative intraocular lens (IOL)
finite-element computer simulation, 10
319

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 331/338
Anesthesia, hyperopic phakic intraocular
lenses, 122
Anisometropic blur-suppression test, 195
Anterior chamber phakic intraocular lenshyperopia, 115– 117
contraindications, 116
indications, 116
optic folding, 116
preoperative management, 117
visual outcomes, 117
Anterior ciliary sclerotomy (ACS), 9–10,
211, 212–214
enhanced, 213
future directions, 216
interocular pressure, 215–216
Anterior ciliary sclerotomy with implantation
of scleral expansion plugs (ACS-
SEP), 214Anterior ischemic syndrome (AIS), 223–224,
232
Antibiotics, hyperopic phakic intraocular
lenses, 124
Aphakic epikaratophakia, 130
Apoptosis, keratocytes, 174– 176
ARC, 58
Array implantation, 251
Array lens, 251
Array multifocal intraocular lens in situ, 254
Artisan hyperopia, 6
Artisan hyperopia lens, 119–120, 121
Artisan iris-claw lens, 125
hyperopic phakic intraocular lenses,122–125
Artisan phakic intraocular lens (IOL)
hyperopia, 124
Astigmatism, 67, 159, 178
hyperopic, 80–82
cross-cylinder technique, 80–82
treatment, 82
irregular, 136
rigid gas permeable lens, 67
thermal keratoplasty, 164
Automated lamellar keratoplasty (ALK), 5,
164
Axis variation, 82
Badal optical system, 52
Baikoff foldable contact lenses, 6
Barraquer cryolathe, 4
Beaver Dam Eye Study, 23
Best spectacle-corrected visual acuity
(BSCVA), 110
Bifocal contact lens, presbyopia, 9, 68
320 Index
Bifocal spectacle, first, 134
Binocular depth of focus, 196–197
Binocular inhibition, 196
Binocular summation, 196Binocular visual acuity, 196
Blur circles, 247
BMP, 174
Bone morphogenic proteins (BMP), 174
Brucke’s muscle, 28
BSCVA, 110
Calibrated marker, 227
Capsulorhexis, 254
Carbon dioxide laser, 84
Cataracts
age-related, 58
oxidative stress, 58–59
presbyopia multifocal IOLs, 240–241refractive surgery, 237
Central corneal power, 136–137
Chromatic aberrations, 152– 153
Ciliary muscle, 28–29, 35
magnetic resonance imaging, 51
CK (See Conductive keratoplasty (CK))
CK Keratoplast tip, 96
Clear lens extraction (CLE), with IOL
placement, 305–307
Cobalt magnesium fluoride laser, 164
Coma pattern, 155
Compound cylindrical hyperopic errors,
correction, 145 –146
Computed videokeratography (CVK), 129Conductive keratoplasty (CK), 133 –134
device, 97
examinations, 98
hyperopia, 7, 95–105
thermokeratoplasty procedures, 95–96
mechanism, 96–97
patient selection, 97–98
performing, 98–100
postoperative care, 100
procedure, 97–98
radiofrequency-based, 96
for reducing hyperopia, 255
United States multicenter clinical trial,
100–105
corneal topography, 102
efficacy, 101
patients and methods, 100
results, 101–105
safety, 104–105
slit lamp, 104
stability, 103

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 332/338
thermal keratoplasty, slit-lamp photograph,
301
topography, 77, 137conductive keratoplasty, 102
H-LASIK, 131
wound healing
animal studies, 179–180
future directions, 182
Corneal collagen, peripheral
thermokeratoplasty, 178
Corneal surgery, hyperopia wound healing,
173–183
Correction profile, hyperopia, 154
Criss-cross nylon suture, 216
Cross-cylinder technique, hyperopic
astigmatism, 80–82
Crossed monovision, 194
Crystalline lens
aging, 55–63
anatomy, 29
magnetic resonance imaging, 51
optics, 25
size and shape, aging, 56–57
CSV–1000E Vector Vision, 165
Customized ablation, 147–148
CVK, 129
Decentration, 82, 298, 316
ablation zone, 294
corneal curvature, 78Defocus, 159
Defocus curve, 240
Deformable lens, equatorial stretch, 48
Diamond blade, 227
Diffractive multifocal intraocular lens (IOL),
238
Diffuse lamellar keratitis, 299
Dilated pupil, 231
Diode laser treatment, hyperopia, 7
Early hyperopic-photorefractive keratectomy
(H-PRK) ablation, 130
Eccentricity, 73
Edinger-Westphal stimulated
accommodation, 37
Elevation map, hyperopic LASIK, 179
Emmetrope, 18
Encircling band, 220, 221
Enhanced anterior ciliary sclerotomy (ACS),
213
[Cornea]Conjunctival closure, scleral expansion
procedures, 231
Contact holmium:yttrium-aluminum-garnet
laser (Ho:YAG) laser thermalkeratoplasty (LTK), safety, 86–87
Contact laser thermal keratoplasty (LTK), 85,
86
visual outcome, 86–87
Contact lens
Baikoff foldable, 6
bifocal, presbyopia, 9, 68
history, 63
living, 4
market information, 63–64
multifocal, 38, 68
vs. refractive surgery, 63–64
rigid gas permeable, 66–67
advantages, 66
disadvantages, 66
selection, 66–67
soft, 64–65
advantages, 65
astigmatism, 67
disadvantages, 65
selection, 65–66
Staar Collamer implantable, 6
Varilux, 135
Continuous carbon dioxide laser, 164
Continuous-wave diode LTK, 91–92
Contrast sensitivity, 196
LTK, 165–168
Contrast sensitivity changes after
hyperopia surgery, 163 –169
Conventional hyperopic LASIK
wavefront measurements and aberration
changes, 154–156
Cornea
cautery, 83
collagen stability, laser thermal
keratoplasty, 85
curvature, decentration, 78
curvature gradient, 73, 79–80
eccentricity, 72–73
ectasia, 299–300
folds, 231
haze, 295
image, ultrasound biomicroscopy, 180
implants, 7
pachymetry, 109
pigmentation lines, 178
surface profile, after hyperopia surgery,
141–150
321Index

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 333/338
Epikeratophakia, 4, 5
Epithelium
hyperplasia, 177, 180
ingrowth, 298measurement, 178– 179
Equatorial stretch, deformable lens, 48
Erbium:glass laser, 164
Erbium:yttrium-aluminum-garnet (YAG)
laser, 10
sclera incision, slit-lamp, 12
Excimer laser surgery, hyperopia, 178
Expansion band, 221, 223
Eye
aberrations, 31– 32
exercises, scleral expansion procedures,
231–232
increase optical power, 30–31
models, 269–275
implementation issues, 274
predictions using, 274
pros and cons, 273–274
requirements, 269
Far point, 17–18
Fechner iris-claw intraocular lens implant,
306
Fenestrated intracorneal polysulfone lenses, 7
Ferry’s line, 178
Field depth, 31
Fincham, accommodation, 40– 42
Finite aspheric eye, 262Finite-element computer simulation
accommodative intraocular lens, 10
Flap complications, 297–298
Fleischer ring, 178
Fogging, 20
Glass lens, 7
Glaucoma, scleral expansion, 233
Glutathione (GSH), 58
Goldman lens, 42
Goniovideography
iridectomized eyes, 50
GSH, 58
Gullstrand, accommodation, 39– 40
Haze, 294–295
Helmholtz mechanism of accommodation,
27–44, 220
Helmholtz model, 209, 210
Hexagonal keratotomy, 4
322 Index
H-LASIK, 295–300
case study, 131–135
corneal topography, 131
elevation map, 179log contrast sensitivity values, 166
postoperative topography, 132, 133, 138
refraction, 166, 167
regression, 181
Holmium:yttrium-aluminum-garnet laser (Ho:
YAG) laser, 85
pulsed, 84
Holmium:yttrium-aluminum-garnet laser (Ho:
YAG) laser thermal keratoplasty
(LTK), 96, 129, 164
H-PRK, 292–294
regression, 181
Hudson-Stahli line, 178
HumanOptics, 280
Humphrey Instruments biomicroscope, 49,
50
Hyperbaric oxygen, 59
Hyperion noncontact laser thermal
keratoplasty, 97
Hyperopia, 2, 63–68
ablation, 69–80
keratorefractive indexes, 72–77
anterior chamber phakic intraocular lens,
115–117
Artisan phakic IOL, 124
astigmatism, 80–82
cross-cylinder technique, 80–82
treatment complications, 82
conductive keratoplasty, 7, 95–105
thermokeratoplasty procedures, 95–96
corneal surgery wound healing, 173–183
correction
history, 4–5
vs. myopic corrections, 176–179
profile, 154
excimer laser surgery, 178
future developments, 315– 317
intracorneal lens, 8
intracorneal segments, 107 –113
keratofractive procedures, topographical
correlates, 129 –135
manifest vs. latent, 20
vs. myopia, aberration, 159
optics, 17–26
phakic intraocular lenses, 119–128
refractive surgery, 71
classification, 177
spherical aberration, 158

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 334/338
hyperopia anterior chamber phakic,
115–117
contraindications, 116indications, 116
optic folding, 116
preoperative management, 117
visual outcomes, 117
hyperopic Artisan phakic, 124
iris-fixed phakic, 119–120
light-adjusted, 282–283
multicomponent, 280– 282
multifocal
decreased contrast sensitivity, 238
glare and halo, 240
impression, 237 –238
incorrect power, 240
types, 238
phakic (See Phakic intraocular lens)
posterior chamber phakic, 6
power calculation, hyperopic phakic
intraocular lenses, 122
refractive multifocal, 238
STAAR Collamer phakic, hyperopic
phakic intraocular lenses, 125, 127
Intraocular pressure, 215
Intrastromal corneal ring, 307
IOL (See Intraocular lens (IOL))
Iridectomized eyes, goniovideography, 50
Iridotomy, laser peripheral, 181
Iris-claw lens (ICL)
Artisan, 122–125, 125
Fechner implant, 306
hyperopic phakic intraocular lens,
122–125
Iris-fixed phakic intraocular lens, 119–120
Irregular astigmatism, 136 –137
Keratoconus, 178
Keratocytes
apoptosis, 174–176
laser thermal keratoplasty, 85
proliferation and migration, 175–176
Keratophakia, 4
Keratoplasty
automated lamellar, 5, 164
thermal (See Thermal keratoplasty)
Keratorefractive indexes, hyperopic ablation,
72–77
Keratoscopy, 76
Kera Vision, 107
Ki–67, 175
[Intraocular lens]
surgery, 3, 69–70
complications, 291– 309
contrast sensitivity changes after,
163–169
corneal surface profile, 141–150
wavefront changes, 151–159
thermal keratoplasty, 164
treatment complications, 78– 80
treatment wavefront, 154– 156
vs. myopic, 156–159
Hyperopic-laser in situ keratomileusis. see
H-LASIK
Hyperopic LASIK. (See H-LASIK)
Hyperopic-photorefractive keratectomy (H-
PRK), 292–294
regression, 181
ICL (See Iris-claw lens (ICL))
ICR myopia, 7
ICS (See Intracorneal segments (ICS))
Ideal monovision result, 190
IL–1, 174
Infrared videophotography, 51
Injector, 124
Interleukin 1 (IL–1), 174
Interocular blur suppression, 195
Interocular pressure, ciliary sclerotomy,
215–216
Interval of Strum, 31–32
Intracorneal lens, hyperopia, 8Intracorneal ring (ICR), myopia, 7
Intracorneal segments (ICS)
central steepening, 111
complications, 307– 309
hyperopia, 107 –113
complications, 111– 113
contraindications, 109
indications, 109
postoperative care, 110
preoperative preparation, 109
surgical technique, 109
visual outcomes, 110–111
postoperative, 108
Intraocular lens (IOL)
accommodating and adjustable results,
283–284
accommodative finite-element computer
simulation, 10
diffractive multifocal, 238
future developments, 317
[Hyperopia]
323Index

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 335/338
LADARWave
device, 159
image, 155, 156, 158
Lamella diamond blade, 228
Lamellar deposits, 112
Lamellar flap, 4
Lamellar keratitis, diffuse, 299
Laser-assisted in situ keratomileusis
(LASIK), 1, 6, 90, 96, 261
complications, 292 –298
contrast sensitivity, 165–168
future developments, 315 –316
induced hyperopia, LTK, 91
multifocal, future developments, 317
Laser peripheral iridotomy, 181
Laser scleral relaxation, 11
Laser thermal keratoplasty (LTK), 6, 83–92complications, 91
contact, 85–88, 86
visual outcome, 86–87
contact and noncontact, 85
contact Ho:YAG, safety, 86–87
continuous-wave diode, 91– 92
contraindications, 85–86
contrast sensitivity, 165–168
corneal collagen stability, 85
history, 83–84
holmium:YAG, 129, 164
Ho:YAG, 129
Hyperion noncontact, 97
keratocyte response, 85LASIK-induced hyperopia, 91
log contrast sensitivity values, 167
mechanism, 84–85
noncontact, 85, 86
complications, 300 –303
visual outcome, 87–88
noncontact Ho:YAG, safety, 87
patient selection, 85–86
PRK-induced hyperopia, 90 –91
refraction, 168
Sunrise Procedure, 6
surgical procedure, 86
technique, Hyperion noncontact, 97
temperature, 84
tissue elasticity, 84–85
visual outcomes, 86–87
YAG, 96
LASIK. (See Laser-assisted in situ
keratomileusis (LASIK))
Late flap dislocation, 299
324 Index
Lens
capsule, 30
crowding, 211
opacification, oxidative stress, 58– 59origin, 210
proteins, 59
Lenticule, schematic representation, 144–147
Lenticule ablation, 142
model, 149
Light-adjusted intraocular lens (IOL),
282–283
Light-difference threshold, 163
Limbus, marking, 225, 226
Living contact lens, 4
Longitudinal spherical aberration (LSA), 73
LTK (See Laser thermal keratoplasty (LTK))
Magnetic resonance imaging (MRI)
ciliary muscle, 51
crystalline lens, 51
Magnification, visual acuity, 22–23
Medennium, 6
Merceline horizontal mattress suture, 216
Miller-Nadler Glaretester, 243
Minimally invasive surgery, 254
Monochromatic aberrations defined, 151– 152
Monovision
after refractive surgery satisfaction,
191–192
defined, 9
factors influencing, 197– 198
failures, 195
presbyopia, 67– 68
success rates after contact lenses, 190
task performance, 197
visual performance, 195–196
Monovision refractive surgery
outcomes, 190
presbyopia, 189 –198
preoperative counseling, 192 –193
Monovision trial, 193
Moria LSK microkeratome, 166
MRI
ciliary muscle, 51
crystalline lens, 51
Multicomponent intraocular lens, 280– 282
Multifocal contact lenses, 38, 68
Multifocal effects, 134–136
historical, 134 –136
Multifocal hyperopic-presbyopic
photorefractive keratectomy (PRK),
203

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 336/338
Navarro aspheric eye, 269–270
Near point, 17–18
Near reading test, 44
Near vision accommodation, 19–20Neural networks, 137–138
Noncontact holmium:yttrium-aluminum-
garnet laser thermal keratoplasty
safety, 87
Noncontact laser thermal keratoplasty, 85, 86
complications, 300 –303
visual outcome, 87–88
Nonsteroidal anti-inflammatory drugs
(NSAID), 224
Non-wave diode laser thermal keratoplasty
(LTK), 96
Ocular aberrations, 31–32
Optical zone design, 141–142, 144
Ora serrata, 29
Oxidative stress
cataracts, 58–59
lens opacification, 58–59
Papillary constriction, 31
Paraxial eye, 262
Pars plana, 29
Pars plicata, 29
Perfect thermal lesion, 178
Peripheral corneal collagen
thermokeratoplasty, 178
Peripheral vision, 196
Phacoemulsification, 254
Phaco-Ersatz, 260 –261simultaneous ametropia correction,
259–274
Phakic intraocular lens, 6
in and CLE with IOL implants,
complications, 303 –307
hyperopia, 119– 128
complications, 127 –128
contraindications, 120–122
indications, 120– 122
posterior chamber phakic IOL, 120
preoperative preparation, 122
STAAR Collamer phakic IOL, 125, 127
surgical technique, 122–125
visual outcomes, 125–128
types, 119–120Phorias, 197
Photic phenomena, 256
Photorefractive keratectomy (PRK), 5, 90,
202, 261
complications, 292 –298
future developments, 315 –316
induced hyperopia, LTK, 90–91
Multifocal intraocular lens
refractive lens exchange, 249–258
Multifocal intraocular lens (IOL), 249
decreased contrast sensitivity, 238design, 250
glare and halo, 240
impression, 237 –238
incorrect power, 240
presbyopia, 237– 248
clinical results, 242
complications, 245– 248
contraindications, 240–241
contrast sensitivity, 243
contrast visual acuity, 244
exclusion criteria, 241
halo and glare, 243, 247–248
incision, 241
indications, 240 –241insufficient near vision, 248
IOL decentration, 246–247
IOL position, 241
IOL power miscalculation, 245–246
occupation, 241
patient expectations, 241
patient satisfaction, 244, 245
patient view with model eye, 245
posterior CCC, 241–242
preferred surgical techniques, 241– 245
spectacle usage, 243–244
theoretical benefits, 238 –240
theoretical caveat, 238–240
vision simulation system, 245
visual acuity, 242–243types, 238
Multifocal laser-assisted in situ
keratomileusis, future developments,
317
Multifocal myopia-presbyopia
photorefractive keratectomy, 203
Multifocal presbyopic photorefractive
keratectomy videokeratography, 205
Musculus crystallinus, 39
Mylar balloon, 48
Myofibroblasts, 175–176
Myopia
ablation, 71
correctionvs. hyperopic corrections, 176– 179
profile, 156–159
error, 18
vs. hyperopia aberration, 159
intracorneal ring, 7
refractive correction, 138
spherical aberration, 160
325Index

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 337/338
Pilocarpine, 38, 256
Plastic polymethylmethacrylate band, 220
Polymethylmethacrylate (PMMA) lenses, 202
Posterior chamber phakic intraocular lens, 6Postoperative pupil check, scleral expansion
procedures, 231
Presbyopia, 2, 67–68, 219
accommodative amplitude measurements
after, 287–290
aging, 57–58
amplitude of accommodation, 20
bifocal contact lens, 9, 68
correction, 8–9
future developments, 317 –318
keratofractive procedures, topographical
correlates, 129–135
monovision, 67–68
monovision refractive surgery, 189– 198eye determination for distance, 193–194
preoperative counseling, 192–193
multifocal corneal approach, 201–208
historical and experimental, 201–202
results, 204–207
techniques, 202 –204
multifocal intraocular lens, 237–248
optics, 17–26
restoration, background, 260
scleral relaxation, 209–214
surgery, 3
complications, 291 –309
Presbyopic photorefractive keratectomy, 204
PRK (See Photorefractive keratectomy(PRK))
Progressive aspheric spectacle lens (PAL),
260
Proportional expansion, refilling model,
271–272
Pseudocycloplegia, 56
Pterygia, 178
Pulsed holmium:yttrium-aluminum-garnet
laser, 84
Pupil block hyperopic phakic intraocular
lenses, 122
Pupil check, postoperative scleral expansion
procedures, 231
Pupillary constriction, 31
Pupil size, hyperopic phakic intraocular
lenses, 122
Pure cylindrical hyperopic errors, correction,
144–145
Pure spherical hyperopic errors, correction,
141–144
Push-up test, 38, 44
326 Index
Quadrafoil pattern, 157
Quantel Axis II immersion biometry unit,
253
Radial keratotomy (RK), 219–220, 255, 261
Radial thermokeratoplasty, 84
Radiofrequency-based conductive
keratoplasty, 96
Radiofrequency energy, 83
Range of accommodation, 20–21
REACT, 59
Refilling model, 270–272
proportional expansion, 271–272
spherization, 271
Refractec, for reducing hyperopia, 255
Refractive error, 247
aging, 57
contact lens vs. refractive surgery, 64simultaneous ametropia correction, Phaco-
Ersatz, 263
Refractive index, 262–263
Refractive lens exchange
scattergram, 252
with multifocal intraocular lens, 249–258
clinical results, 250–252
complications, 255
patient selection, 252–253
postoperative course, 256
preoperative measurements, 253 –254
refractive surprise, 255– 256
surgical technique, 254
targeting emmetropia, 255Refractive procedures, 233
Refractive surgery
cataract surgery, 237
vs. contact lens, 63–64
monovision, satisfaction, 191 –192
Regression, 294, 302–303
H-LASIK, 181
H-PRK, 181
mechanisms, 178– 182
Retinoscopic reflex, 287, 289
Retreatments, 80
Rigid gas permeable (RGP) lens, 66–67
advantages, 66
astigmatism, 67
disadvantages, 66
selection, 66–67
RK, 219–220, 255, 261
RMS, 73
Roche European-American Cataract Trial
(REACT), 59
Root mean square (RMS), 73

7/29/2019 Hyperopia and Presbyopia
http://slidepdf.com/reader/full/hyperopia-and-presbyopia 338/338
Snellen letters, 22
Snellen visual acuity, 22
Soft contact lens, 64–65
advantages, 65astigmatism, 67
disadvantages, 65
selection, 65–66
Soft toric lenses, 67
Spectacle, bifocal, first, 134
Spherical hyperopia, ablation, 148
Spherical hyperopic error ablation, 143
Spherization, refilling model, 271
Sphingolipid, 59
Spreading dissection, 213
Square diamond blade, 227
Staar Collamer implantable contact lens, 6
Staar Collamer phakic intraocular lens
hyperopic phakic intraocular lenses, 125,
127
Staar Collamer posterior chamber phakic
intraocular lens implant, 305
Star Excimer Laser system, 130
StatView, 165
Stellate iron lines, 178
Stereoacuity, 196
Steroids, hyperopic phakic intraocular lenses,
124
Stocker-Busacca line, 178
Suarez spreader, 109
Summit Apex Plus Laser, 166
Sunrise Ho:YAG laser, 164
Sunrise LTK Procedure, 6
Surface asymmetry index (SAI), 73
Swan-Jacob gonioscopy, 42
Temperature, laser thermal keratoplasty, 84
Thermal keratoplasty, 83
astigmatism, 164
cornea, slit-lamp photograph, 301
future developments, 316 –317
hyperopia, 164
peripheral corneal collagen, 178
radial, 84
Thermal lesion, perfect, 178
Thornton Triple Edge diamond knife, 212
Tissue elasticity, laser thermal keratoplasty,
84–85
TNF alpha, 174
Transition zone
design, 142–145
lack, 79
Trefoil pattern, 157
SAI, 73
Scarring, middle periphery, 79
Schachar model, 209
Schachar’s scleral band procedures, 287Schachar’s theory of accommodation, 34,
47–53, 220
challenged, 50
evidence against, 42–43
Schachar theory of presbyopia, 2
evidenced against, 43
Scheimpflug optics, 56
Sclera
origin, 210
slit-lamp erbium:YAG, 12
Scleral belt loops, 228, 229
dissect, 227–229
scleral expansion procedures, 226
Scleral expanding bands
future developments, 317
Scleral expansion, 219–233
anesthesia, 225
clinical results, 232
complications, 232
conjunctival closure, 231
conjunctival dissection, 225–226
current method, 224–225
early procedures, 219–220
eye exercises, 231–232
glaucoma, 233
patient selection, 223
postoperative pupil check, 231
scleral belt loops, 226
scleral expansion segments, 229 –230
Scleral expansion segments, 229–230
dimensions, 230
placement, 230
Scleral expansion surgery
accommodation, 44
Scleral relaxation, 2
presbyopia, 209– 214
Shack-Hartmann wavefront sensor, 152
history, 153–154
principles, 154
Sighting preference, 197
Silicone expansion plugs, 214
Simultaneous ametropia correction
Phaco-Ersatz, 259– 270
results, 263–267
Simultaneous vision principle, 9
Sinskey hook, 109
Slab off, 67
Slit-lamp, sclera incision, erbium:YAG, 12
327Index