Embed Size (px)
Citation preview

Doctrine forHealth Services Support
in Joint Operations
Joint Pub 4-02
26 April 1995

PREFACE
i
1. Scope
This publication delineates requirementsand considerations for the health servicesupport (HSS) system as well as HSSaspects of joint planning, special operations,and military operations other than war. Italso addresses the medical threat and theneed for medical intelligence.
2. Purpose
This publication has been prepared underthe direction of the Chairman of the JointChiefs of Staff. It sets forth doctrine togovern the joint activities and performanceof the Armed Forces of the United States injoint operations as well as the doctrinal basisfor US military involvement inmultinational and interagency operations.It provides military guidance for theexercise of authority by combatantcommanders and other joint forcecommanders and prescribes doctrine forjoint operations and training. It providesmilitary guidance for use by the ArmedForces in preparing their appropriate plans.It is not the intent of this publication torestrict the authority of the joint forcecommander (JFC) from organizing the forceand executing the mission in a manner theJFC deems most appropriate to ensure unityof effort in the accomplishment of theoverall mission.
3. Application
a. Doctrine and guidance established inthis publication apply to the commandersof combatant commands, subunifiedcommands, joint task forces, andsubordinate components of thesecommands. These principles and guidancealso may apply when significant forces ofone Service are attached to forces of anotherService or when significant forces of oneService support forces of another Service.
b. The guidance in this publication isauthoritative; as such, this doctrine will befollowed except when, in the judgment ofthe commander, exceptional circumstancesdictate otherwise. If conflicts arise betweenthe contents of this publication and thecontents of Service publications, thispublication will take precedence for theactivities of joint forces unless the Chairmanof the Joint Chiefs of Staff, normally incoordination with other members of theJoint Chiefs of Staff, has provided morecurrent and specific guidance.Commanders of forces operating as part ofa multinational (alliance or coalition)military command should followmultinational doctrine and guidance ratifiedby the United States. For doctrine andprocedures not ratified by the United States,commanders should evaluate and follow themultinational command’s doctrine andprocedures, where applicable.
For the Chairman of the Joint Chiefs of Staff:
T.R. PATRICK Colonel, USA Secretary, Joint Staff

i i
Preface
Joint Pub 4-02
Intentionally Blank

TABLE OF CONTENTS
iii
PAGE
EXECUTIVE SUMMARY ........................................................................................... v
CHAPTER ITHE HEALTH SERVICE SUPPORT SYSTEM
• Mission ................................................................................................................. I-1• Conserving the Fighting Strength ........................................................................ I-1• Echelons of Care .................................................................................................. I-1• Patient Evacuation ................................................................................................ I-4• HSS Principles...................................................................................................... I-5• Relationships and Responsibilities for Joint HSS ............................................... I-6
CHAPTER IIJOINT HEALTH SERVICE SUPPORT PLANNING
• The Joint Operation Planning Process ............................................................... II-1• Health Service Support Planning Considerations .............................................. II-1• HSS Estimate of the Situation............................................................................ II-5• HSS Planning Factors ........................................................................................ II-6• HSS Policies and Procedures ............................................................................. II-7• Special HSS Planning Considerations ............................................................... II-8• HSS for the Return of US Prisoners of War ...................................................... II-9• HSS for EPWs .................................................................................................... II-9• Command, Control, Communications, and Computer Systems ...................... II-10• Dental Services Support .................................................................................... II-11
CHAPTER IIIHEALTH SERVICE SUPPORT IN SPECIAL OPERATIONS
• General .............................................................................................................. III-1• Organic HSS Capability .................................................................................... III-1• SOF Medical Support Planning ........................................................................ III-3
CHAPTER IVHEALTH SERVICE SUPPORT IN MILITARY OPERATIONS OTHER THAN WAR
• General .............................................................................................................. IV-1• Humanitarian and Civic Assistance, Humanitarian Assistance, and Domestic Support Programs ................................................................... IV-4• Other HA ........................................................................................................... IV-6• HSS Aspects of Combatting Terrorism............................................................. IV-6• Disaster Relief Assistance ................................................................................. IV-6• The AE Role ...................................................................................................... IV-7

iv
Table of Contents
Joint Pub 4-02
APPENDIX
A Medical Threat ................................................................................................. A-1B Medical Intelligence ........................................................................................ B-1C References ........................................................................................................ C-1D Administrative Instructions ............................................................................. D-1
GLOSSARY
Part I—Abbreviations and Acronyms ................................................................. GL-1Part II—Terms and Definitions ........................................................................... GL-3
FIGURE
I-1 Echelons of Care and DOD Theater Combat Medical System ..................... I-2I-2 Health Service Support Principles ................................................................ I-6I-3 Responsibilities for Joint HSS ...................................................................... I-7I-4 Armed Forces Blood Distribution System ................................................. I-10II-1 PMI Medical Equipment Flow .................................................................... II-4II-2 HSS Planning Factors ................................................................................. II-7II-3 Support Requirements for Combat Search and Rescue Operations ........... II-9II-4 Levels of Dental Care ................................................................................ II-11III-1 Challenges of SOF Medical Support ......................................................... III-4IV-1 Humanitarian and Civic Assistance (HCA) Program Overview ............... IV-4IV-2 Assessment Factors in Assistance Programs ............................................. IV-5IV-3 Disaster Relief Assistance ......................................................................... IV-7

v
EXECUTIVE SUMMARYCOMMANDER'S OVERVIEW
•
•
•
•
•
Discusses the Health Service Support (HSS) Mission andObjectives in Joint Operations
Covers Planning and Coordination for HSS Services
Provides Special Planning Considerations for UniqueOperations
Discusses Requirements for HSS in Special Operations
Covers HSS in Military Operations Other Than War
Health Service Support Mission and Objectives
The health service support (HSS) mission in jointoperations is to minimize the effects of wounds, injuries,and disease on unit effectiveness, readiness, and morale.This mission is accomplished by a proactive preventivemedicine program and a phased health care system(echelons of care) that extends from actions taken at thepoint of wounding, injury, or illness to evacuation from atheater for treatment at a hospital in the continental UnitedStates (CONUS). The primary objective of HSS is toconserve the commander’s fighting strength of land, sea,air, and special operations forces. HSS in joint operationsrequires continuous planning, coordination, and training toensure a prompt, effective, and unified health care effort.
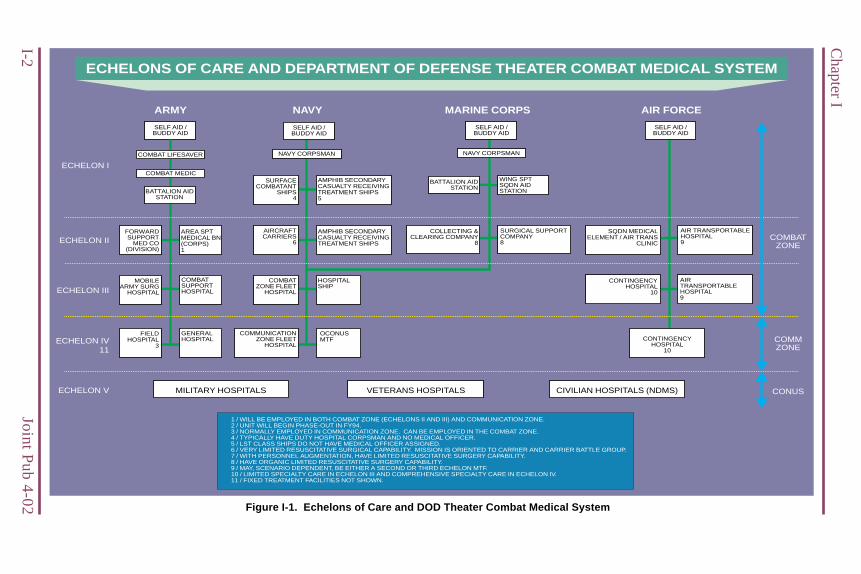
Echelon I. Care is rendered at the unit level and includesself aid and buddy aid, examination, and emergencylifesaving measures.
Echelon II. Care is administered at an HSS organizationby a team of physicians or physician assistants, supportedby appropriate medical technical or nursing staff.
Echelons of Health Care
Effective health servicesupport (HSS) enhancesthe combat strength ofthe joint force.
Five echelons of caremake up the HSS system.

vi
Executive Summary
Joint Pub 4-02
Each Service componenthas an HSS system thatencompasses six healthcare principles.
Operational plannersmust select the best ormost appropriate meansof performing a jointforce mission.
Echelon III. Care administered requires clinicalcapabilities normally found in a medical treatment facility(MTF).
Echelon IV. Care provided is not only a surgical capabilityas provided in Echelon III, but also further definitive therapyfor patients in the recovery phase.
Echelon V. Care is convalescent, restorative, andrehabilitative and is normally provided by military,Department of Veterans Affairs, or civilian hospitals inCONUS.
Conformity. Integration and compliance with thecommander’s plan.
Proximity. Provide HSS as close to combat operationsas the tactical situation permits.
Flexibility. Shift HSS resources to meet changingrequirements.
Mobility. Anticipate requirements for rapid movementof HSS units to support combat forces during operations.
Continuity. Provide optimum, uninterrupted care andtreatment to the wounded, injured, and sick.
Coordination. Ensure that HSS resources in short supplyare efficiently employed and used to effectively supportthe planned operation.
Timely, effective planning and coordination are essentialto ensure adequate and sustainable HSS in a theater.Proper planning permits a systematic examination of allfactors in a projected operation and ensures interoperabilitywith the campaign or operation plan. Organization ofthe HSS system is determined largely by the joint force’smission, the medical threat, medical intelligence, the theaterevacuation policy, and hospitalization and evacuationrequirements.
Health Care Principles
Operational Planning and Coordination

vii
Executive Summary
The geographiccombatant commanderhas overall responsibilityfor health care within thetheater.
Patient evacuationrequires detailedplanning for successfulexecution.
The HSS estimate’spurpose is to provide ananalysis of HSSinformation.
Special HSS planningconsiderations arenecessary for uniqueoperations and situations.
Geographic combatant commanders are responsible forcoordinating and integrating HSS within their theaters.A joint force surgeon (JFS) should be appointed for eachcombatant command, subunified command, and joint taskforce. JFSs need to assess component command HSSrequirements and capabilities, both quantitatively andqualitatively, and provide guidance to enhance theeffectiveness of HSS through shared use of assets. Themovement of casualties to or between MTFs within thecombat zone or forward of corps level is a Servicecomponent responsibility. Distribution of respectivecomponent HSS capabilities, as directed by the geographiccombatant commander, will aid in ensuring efficient use oflimited HSS resources, particularly assets and beds.
Timely patient evacuation plays an important role in thedesign of the treatment sequence from front to rear. Whenthe echelons of HSS become more sophisticated, the meansof patient evacuation also become more sophisticated.Patient evacuation involves route planning, movementcontrol, and the locating of evacuation facilities. A majorfactor in the evacuation of patients through the five echelonsof medical care is that specific medical equipment anddurable supplies designated as patient movement itemsmust be available to support the patient during theevacuation.
The HSS estimate provides an analysis of HSS informationpertaining to enemy intentions, allied or coalitionpartner’s capabilities, limitations, courses of action, andpotential HSS consequences associated with acontemplated operation. The HSS estimate will includeall HSS facts, assumptions, and deductions that can affectthe operation. Based upon the HSS estimate of the situation,the JFS, in coordination with the component commandsurgeons, must plan for medical policies and proceduresthat can be best adapted to the joint operation.
Amphibious Task Force. Amphibious task force medicalplanning responsibilities are closely related to those of thelanding force; their facilities are mutually supporting.Detailed, coordinated, and parallel planning is requiredbetween the commanders, amphibious task force, andlanding force.
Special Health Service Support Planning Considerations

viii
Executive Summary
Joint Pub 4-02
HSS functions dependupon responsivecommand, control,communications, andcomputer systems.
The HSS dental service isa major contributor tomaintaining unit fightingstrength.
Combat Search and Rescue (CSAR). The HSScapabilities of CSAR units vary from component tocomponent, but are generally limited. Certain componentCSAR units are dedicated to CSAR operations while othersperform CSAR as a secondary mission. Although CSARunits require HSS similar to other units, supportedgeographic combatant commanders must establish a flexibleHSS system to meet the demands of CSAR operations.
The Return of US Prisoners of War (POWs). Thegeographic combatant commander establishes a theaterprotocol on the proper handling and provision of HSS forreturn of US POWs. HSS will be administered within areasonably short period upon return to friendly forces,treatment assessments will be established, and operationalspecialty medical support will be provided immediately.
Enemy Prisoners of War (EPWs). In consonance withprovisions outlined in the Geneva Conventions, patientswho are EPWs are afforded the same level of HSS andmedical care as patients of the detaining power. Seriouslywounded, injured, or sick EPWs will be evacuated throughmedical channels, but will be segregated from US and alliedpatients. The joint force commander must ensureappropriate security is provided to guard the EPWs.
Effective command, control, communications, andcomputer (C4) systems are vital to successful HSS injoint operations. Early identification of a theater’s C4system requirements for HSS connectivity is essential. HSSsystem management information systems support theinformation management requirements of HSS units acrossthe range of military operations. Records and reports arerequired to pass information and assist in the evaluation ofpolicies and procedures.
Joint operation planning must include consideration of thevarious roles of dental services. The planning processincludes an evaluation of the size and anticipated durationof the operation, along with the levels of dental care requiredthroughout the operation. The four levels of dental careare: Emergency Dental Care, Sustaining Dental Care,Maintaining Dental Care, and Comprehensive Care.
Command, Control, Communications, and Computer Systems
Dental Services

ix
Executive Summary
The nature of special operations requires that units be small,highly skilled, self-contained teams that can be easilyinserted and extracted by air, sea, and land delivery methods.Medical support of special operations units ischaracterized by an austere structure and a limitednumber of medical personnel. The nature of specialoperations forces (SOF) missions requires that SOF medicalpersonnel possess a variety of enhanced medical skills thatenable them to operate under a multiplicity ofcircumstances. Special operations medical supportplanning must provide integrated, augmentedconventional support into the concept of the specialoperating mission without compromising the objectives.The planning must also articulate the unique aspects of theoperation that will complicate the delivery of HSS servicessupport by conventional units.
Military operations other than war are usually jointoperations, often performed in concert with othergovernment agencies, nongovernmental organizations, andprivate volunteer organizations. HSS policies duringmilitary operations for operations other than war maybe substantially different from the policies associatedwith a general war. HSS operations conducted to enhancethe stability of a host-nation government must be well-coordinated with all concerned agencies and integrated intothe respective US Embassy plan. Independent, unplannedmedical civic action programs should not be undertaken.
Humanitarian and civic assistance (HCA) programs operatein conjunction with US military operations or exercises.HCAs serve the local populace by furnishing assistance thatthe local government is not capable of providing. HSS isoften provided within a larger military involvement. Asignificant number of humanitarian assistance programsinvolve disaster relief operations. The military can provideassistance to help ease the effects of natural disasters andmanmade events.
Special operations forceshave unique requirementsfor medical support.
Military operations otherthan war encompass awide range of activities.
Humanitarian and civicassistance activities aredesigned to provideassistance to the host-nation populace.
Special Operations
Military Operations Other Than War

x
Executive Summary
Joint Pub 4-02
HSS attempts to provide prompt, effective, and unifiedhealth care services to enhance the combat fighting abilityof joint forces. HSS in joint operations requires continuousplanning, coordination, and training. HSS is a phased healthcare system that is based on five echelons of care.
CONCLUSION

CHAPTER ITHE HEALTH SERVICE SUPPORT SYSTEM
I-1
1. Mission
The Health Service Support (HSS)mission in joint operations is to minimizethe effects of wounds, injuries, anddisease on unit effectiveness, readiness,and morale. This mission is accomplishedby a proactive preventive medicine(PVNTMED) program and a phasedhealth care system (echelons of care) thatextends from actions taken at the point ofwounding, injury, or illness to evacuationfrom a theater for treatment at a hospital inthe continental United States (CONUS).One measure of this system’s effectivenessis its ability to save life and limb, to reducethe disease and nonbattle injury rate, andto return patients to duty quickly and as farforward in the theater as possible. Anothermeasure is the system’s ability to evacuatepatients to the Communications Zone or outof the theater as appropriate, within theoperational evacuation policy, with aminimum delay.
2. Conserving the FightingStrength
a. The primary objective of HSS is toconserve the commander’s fightingstrength of land, sea, air, and specialoperations forces. In joint operations, thisobjective is most effectively achievedthrough optimum use and integration ofavailable component command HSS assets.
b. Effective HSS enhances the combatstrength of the joint force by maintainingphysically and emotionally fit personneland by treating the wounded, injured, orsick to promote their survival, recovery, and
rapid return to duty (RTD). By applyingthe HSS principles and using the echelonsof care discussed in this chapter,commanders can retain acclimated andexperienced personnel, thus minimizingthe requirements for replacements, patientevacuation, and additional logistic support.
c. At their inception, the principles ofHSS and echelons of care did notspecifically address joint or multinationaloperations; however, their implementationis common among Service componentsand applies to HSS planning and executionby joint force commanders (JFCs). HSS injoint operations requires continuousplanning, coordination, and training toensure a prompt , effective, and unifiedhealth care effort.
3. Echelons of Care
Five echelons of care make up the HSSsystem, extending from the point ofwounding, injury, or illness (Figure I-1).Each succeeding echelon possesses thesame treatment capabilities as thoseechelons forward and adds a newtreatment capability.
a. Echelon I. Care is rendered at the unitlevel and includes self aid and buddy aid,examination, and emergency lifesavingmeasures such as maintenance of airway,control of bleeding, prevention and controlof shock, and prevention of further injuryby trained personnel. This echelon mayinclude an aid station that has physiciansor physician assistants. Treatment at theaid station includes restoration of the airwayby surgical procedure; use of intravenous
“The soldier’s health must come before economy or any other consideration.”
Napoleon I
I-2
Chapter I
Join
t Pu
b 4
-02 Figure I-1. Echelons of Care and DOD Theater Combat Medical System
ARMY MARINE CORPSNAVY AIR FORCE
1 / WILL BE EMPLOYED IN BOTH COMBAT ZONE (ECHELONS II AND III) AND COMMUNICATION ZONE.2 / UNIT WILL BEGIN PHASE-OUT IN FY94.3 / NORMALLY EMPLOYED IN COMMUNICATION ZONE. CAN BE EMPLOYED IN THE COMBAT ZONE.4 / TYPICALLY HAVE DUTY HOSPITAL CORPSMAN AND NO MEDICAL OFFICER.5 / LST CLASS SHIPS DO NOT HAVE MEDICAL OFFICER ASSIGNED.6 / VERY LIMITED RESUSCITATIVE SURGICAL CAPABILITY. MISSION IS ORIENTED TO CARRIER AND CARRIER BATTLE GROUP.7 / WITH PERSONNEL AUGMENTATION, HAVE LIMITED RESUSCITATIVE SURGERY CAPABILITY.8 / HAVE ORGANIC LIMITED RESUSCITATIVE SURGERY CAPABILITY.9 / MAY, SCENARIO DEPENDENT, BE EITHER A SECOND OR THIRD ECHELON MTF.10 / LIMITED SPECIALTY CARE IN ECHELON III AND COMPREHENSIVE SPECIALTY CARE IN ECHELON IV.11 / FIXED TREATMENT FACILITIES NOT SHOWN.
NAVY CORPSMAN
BATTALION AIDSTATION
WING SPTSQDN AIDSTATION
COLLECTING &CLEARING COMPANY
8
SURGICAL SUPPORTCOMPANY8
SELF AID /BUDDY AID
SELF AID /BUDDY AID
SELF AID /BUDDY AID
NAVY CORPSMAN
SURFACECOMBATANT
SHIPS4
AMPHIB SECONDARYCASUALTY RECEIVINGTREATMENT SHIPS5
AMPHIB SECONDARYCASUALTY RECEIVINGTREATMENT SHIPS
COMBATZONE FLEET
HOSPITAL
HOSPITALSHIP
COMMUNICATIONZONE FLEET
HOSPITAL
OCONUSMTF
AIRCRAFTCARRIERS
6
COMBAT LIFESAVER
COMBAT MEDIC
BATTALION AIDSTATION
FORWARDSUPPORT
MED CO(DIVISION)
AREA SPTMEDICAL BN(CORPS)1
MOBILEARMY SURG
HOSPITAL
COMBATSUPPORTHOSPITAL
FIELDHOSPITAL
3
GENERALHOSPITAL
SQDN MEDICALELEMENT / AIR TRANS
CLINIC
AIR TRANSPORTABLEHOSPITAL9
AIRTRANSPORTABLEHOSPITAL9
CONTINGENCYHOSPITAL
10
CONTINGENCYHOSPITAL
10
ECHELON II
ECHELON III
ECHELON IV11
ECHELON I
ECHELON V
COMBATZONE
COMMZONE
CONUSCIVILIAN HOSPITALS (NDMS)VETERANS HOSPITALSMILITARY HOSPITALS
ECHELONS OF CARE AND DEPARTMENT OF DEFENSE THEATER COMBAT MEDICAL SYSTEM
SELF AID /BUDDY AID

I-3
The Health Service Support System
fluids, including Ringer's Lactate andHuman Albumin; antibiotics; andapplication of splints and bandages. Theseelements of medical management preparepatients for RTD or for transportation to ahigher echelon of care. Supportingmedical units are responsible forevacuation of patients from medicaltreatment facilities (MTFs) forward of thesupporting medical unit’s position.
b. Echelon II. Care is administered atan HSS organization by a team ofphysicians or physician assistants,supported by appropriate medical,technical, or nursing staff. As aminimum, this echelon of care includesbasic resuscitation and stabilization andmay include surgical capability, basiclaboratory, limited x-ray, pharmacy, and
temporary holding ward facilities. At thisechelon, examinations and observationsare accomplished more deliberately thanat Echelon I. This phase of treatmentapplies emergency procedures, such asresuscitation, to prevent death, loss of limb,or body functions. For those patients whorequire more comprehensive treatment,
surface or air evacuation is available to afacility possessing the required treatmentcapability. This is the first echelon at whichGroup O liquid packed red blood cells willbe available for transfusion.
c. Echelon III. Care administeredrequires clinical capabilities normallyfound in a MTF that is typically located ina lower-level enemy threat environment.The MTF is staffed and equipped to provideresuscitation, initial wound surgery, andpost operative treatment. This echelon’scare may be the first step towardrestoration of functional health, ascompared to procedures that stabilize acondition or prolong life. It does not havethe crises aspects of initial resuscitative careand can proceed with greater preparationand deliberation. Blood products available
include fresh frozen plasma, platelets,frozen Group O red cells, and Groups A,B, and O liquid cells.
d. Echelon IV. This echelon of care willprovide not only a surgical capability asprovided in Echelon III, but also furtherdefinitive therapy for patients in the
Hospital Ships, a mobile element of the Theater Combat Medical System, provideEchelon III medical care, a capability designed to restore functional health andreturn the wounded, injured, or ill to their units as soon as possible.

I-4
Chapter I
Joint Pub 4-02
VIETNAM: FROM THE FIELD TO THE HOSPITAL
Field evacuation and hospitalization of wounded in Vietnam was different fromany previously carried out in any war. In addition it varied both in time andplace within Vietnam. It was characterized by the absence of front lines andthe traditional chain of evacuation. In general, the wounded Soldier was aptto receive his wounds while with a small group or unit isolated deep in roadlessjungle, and the wounds were more apt to be multiple over all parts of the bodythan in any previous war. First aid and emergency medical treatment given onthe site by company aid men, however, differed little from previous times.Resuscitative equipment and procedures included pressure dressings,tourniquets, and airways. Morphine was available but seldom used, as painwas not usually a problem at this point and aid men were aware of thedepressant effects of morphine. In all likelihood, the patient would be evacuatedwithin a relatively few minutes by helicopter, either a medical ambulance craftor a tactical one. The facilities available for resuscitation aboard the helicoptervaried depending on whether it was a medical (“dust-off”) helicopter or acombat helicopter. IV fluid, usually Ringer’s Lactate solution, was oftenavailable, and trained medical technicians and emergency equipment werealso present on dust-off helicopters.
recovery phase who can return to dutywithin the theater evacuation policy.Definitive care is normally provided by acommunications zone Fleet Hospital,General Hospital, or overseas MTF. Ifrehabilitation cannot be accomplishedwithin a predetermined holding period, thecasualties/patients are evacuated to the zoneof Interior, Echelon V.
e. Echelon V. Care is convalescent,restorative, and rehabilitative and isnormally provided by military, Departmentof Veterans Affairs, or civilian hospitals inCONUS. This phase may include a periodof minimal care and increasing physicalactivity necessary to restore patients tofunctional health and allow their RTD oruseful life.
4. Patient Evacuation
Patient evacuation in the combat zoneor from Echelon I to Echelon II, fromEchelon II to Echelon III, and withinEchelon III is normally the responsibility
of the component commands and iscoordinated by a Theater PatientMovements Requirements Center(TPMRC). These movements can be bysurface (land or water), rotary-wingaircraft, or tactical aeromedical aircraft.Dedicated patient evacuation for Navyhospital ships is provided by Army airambulance assets. Tactical aeromedicalevacuation from the combat zone(Echelon III) to the communications zone(Echelon IV) is normally a responsibilityof the supporting Air Force component.Patient evacuation from the theater is theresponsibility of US Commander inChief, Transportation Command(USCINCTRANS), who is responsible forestablishing, operating, training, andmaintaining the common-user aeromedicalevacuation system worldwide. This missionis executed by the Air Mobility Command.Patient evacuation procedures in jointoperations are described in Joint Publication4-02.2, “Joint Tactics, Techniques, andProcedures for Patient Evacuation in JointOperations.”

I-5
The Health Service Support System
The destinations of the helicopters varied. In some areas patients were takento aid stations or medical companies. More often the helicopter flew thepatients directly to a surgical hospital where they could receive definitive care.Blood and electrolyte solutions were often available at aid stations and medicaland clearing companies, as was some surgical capability. Complete surgicalfacilities, including anesthetists, were available at clearing companies, butdefinitive surgery was usually not done here. At times battalion surgeonsflew forward to a site of combat, bringing blood and other supplies whichwere given on the spot.
Hospitals fulfilled much the same function for combat wounded, whether theywere surgical hospitals, field hospitals, or evacuation hospitals. By and largethey were all “semipermanent,” usually buildings set on a concrete floor, air-conditioned and with all utilities and other equipment of a first-rate hospital inthe continental United States.
Resuscitation of a Vietnam war casualty was an extremely rapid andsophisticated procedure. The patient would often be brought to the hospitaldirectly from the battlefield by medical evacuation helicopter, frequently inless than an hour. Usually he received emergency treatment on the battlefield,to include control of hemorrhage, wound dressing, respiratory control, andoften the starting of intravenous fluid. At the hospital, he was immediatelytaken to the resuscitation area where he was surrounded by a large team ofhighly trained physicians, nurses, and technicians.
The results of this prompt and efficient treatment may perhaps be bestillustrated by comparing them with similar statistics from previous wars. InVietnam, 46,000 of 346,000, or 13 percent, of all wounded American Soldiersdied. If 22 percent had died, as was true in Korea, there would have been77,840 deaths, 31,840 more than actually occurred. In World War II, 28 percentof all wounded American Soldiers died. If the medical treatment of Vietnamhad been available during World War II, 117,748 Soldiers would have beensaved.
SOURCE: Hardaway, Robert M., M.D., Care of the Wounded in Vietnam ,Sunflower University Press, 1988.
5. HSS Principles
As shown in Figure I-2, each Servicecomponent has an HSS system thatencompasses six health care principles:
a. Conformity. Integration andcompliance with the commander’s planare the basic elements of effective HSS.HSS planners can help ensure conformityby taking part in development of thecommander’s operation plan.
b. Proximity. The objective ofproximity is to provide HSS to thewounded, injured, or sick as close tocombat operations as the tacticalsituation permits. In many cases, time maybe as important a factor as distance.Patients are evacuated to an MTF, or theMTF is moved to the area where the patientpopulation is the greatest.
c. Flexibility. Changes in tactical plansor operations make this HSS principleessential. Units must be prepared to shift
I-6
Chapter I
Joint Pub 4-02
HSS resources to meet changingrequirements. All HSS units are usedwithin the theater with none held inreserve, so plans for redistribution of HSSresources are required.
d. Mobility. Using both organic andnonorganic transportation resources,c o m m a n d e r s s h o u l d a n t i c i p a t erequirements for rapid movement ofHSS units to support combat forcesduring operations. This HSS principle isclosely aligned to that of proximity.
e. Continuity. The objective is toprovide optimum, uninterrupted careand treatment to the wounded, injured,and sick. Continuity in care and treatmentis achieved by moving the patient througha progressive, phased HSS system, whichextends from the forward area of the combatzone to an area as far rearward as thepatient’s condition requires, possibly toCONUS. Continuity is also achieved byproviding continued care during movement.
f. Coordination. The objective of thisprinciple is to ensure that HSS resourcesin short supply are efficiently employed
and used to effectively support the plannedoperation. Continuous coordination ensuresthat MTFs are not placed in areas thatinterfere with combat operations.Additionally, continuous coordinationensures that the scope and quality ofmedical treatment and care meetprofessional standards and policies.
6. Relationships andResponsibilities for JointHSS
See Figure I-3.
a. Geographic combatant commandersare responsible for coordinating andintegrating HSS within their theaters.Where practical, joint use of availablemedical assets will be accomplished tosupport warfighting strategy and concept ofoperations.
b. A joint force surgeon (JFS) shouldbe appointed for each combatantcommand, subunified command, andjoint task force. As a specialty advisor,the JFS reports directly to the JFC. TheJFS will coordinate HSS matters for theJFC. The JFS section should be jointlystaffed and should be of sufficient size toeffectively facilitate:
• Joint coordination of HSS initiatives.
• Regionalization.
• Standardization and interoperability.
• Development of the HSS plan.
• Review of subordinate plans andoperations.
c. JFSs need to assess componentcommand HSS requirements andcapabilities, both quantitatively andqualitatively, and provide guidance to
CONFORMITY
PROXIMITY
FLEXIBILITY
MOBILITY
CONTINUITY
COORDINATION
HEALTH SERVICESUPPORT PRINCIPLES
Figure I-2. Health Service SupportPrinciples

I-7
The Health Service Support System
RESPONSIBILITIES FOR JOINT HEALTH
JOINT FORCE SURGEON (JFS)
Combatant commanders are responsible for coordinating andintegrating HSS within their theaters.
The JFS coordinates matters for the JFC.
Facilitates:Joint coordination of HSS initiatives.Regionalization.Standardization and interoperability.Development of HSS plan.Review of subordinate plans and operations.
Assesses component command HSS requirements and capabilities.
Provides guidance to enhance effectiveness of HSS.
Monitors the status of:Patient beds.Blood products.Health service logistics.HSS staffing.
Advises the JFC and informs on status of HSS units.
Coordinates medical intelligence and support for HSS organizations(including assistance from allies).
Supervises the activities of the Theater Patient MovementRequirements Center (TPMRC) and the Joint Blood Program Center(JBPO).
Prepares the HSS annex to joint force plans.
Prepares bed requirement estimates.
Liaison must be established between the JFS and each componentsurgeon.
COMBATANT COMMANDERS
Figure I-3. Responsibilities for Joint HSS

I-8
Chapter I
Joint Pub 4-02
enhance the effectiveness of HSS throughshared use of assets. JFSs should havethe responsibility to:
• Assist the combatant commander informulating a recommended patientevacuation policy within thegeographic area.
• Assist the component commands inidentifying HSS requirements of eachcomponent and assigning cross-Service support where practical.
• Advise the JFC concerning:
•• HSS aspects of combat operations.
•• Intratheater rest, rotation, andreconstitution policies.
•• Preventive medicine.
•• Other medical factors that couldaffect operations.
• Inform the JFC on the status of HSSunits, highlighting problems and otherareas of interest or concern.
• Monitor the status of:
•• Patient beds.
•• Blood products.
•• Health service logistics.
•• HSS staffing.
•• Other issues affecting medicalreadiness.
• Inform the JFC concerning the statusof HSS and any assistance requiredby and provided to the civilianpopulace, US nationals, and enemyprisoners of war (EPW). Advise
supporting civil affairs forces onhumanitarian and civic assistance(HCA) activities within the joint forceoperations area.
• Coordinate HSS provided to orreceived from allies or other friendlynations.
• Coordinate medical intelligencesupport for HSS organizations.
• Supervise the activities of theTPMRC and the Joint BloodProgram Office (JBPO).
• Prepare the HSS annex to joint forceplans.
• Prepare bed requirement estimatesbased on the casualty estimatesprovided by the appropriate staff (J1,DP, N1, and G1) and extracted fromthe Joint Operation Planning andExecution System (JOPES) medicalplanning module (MPM).
• In conjunction with the joint force’slegal office, advise the JFC on HSSaspects of the Geneva Conventions.
d. Liaison must be established betweenthe JFS and each component surgeon.This liaison ensures that mutualunderstanding of technical medical anddental procedures, unity of purpose andaction, and joint HSS are maintained.
e. Medical regulating of patients willoccur by the same process across the rangeof military operations. The movement ofcasualties to or between MTFs within thecombat zone or forward of corps level isa Service component responsibility. If,in the opinion of the attending physician, acasualty cannot be returned to duty withinthe theater evacuation policy, theoriginating MTF will request that the

I-9
The Health Service Support System
patient be regulated to another MTF formore definitive care. Patients may beregulated to destinations within thetheater, to another theater, or to CONUS.Patient regulating includes accounting forbed availability, medical airlift capability,and patient in-transit visibility (the abilityto track an individual patient’s status andlocation). This will be accomplishedthrough a command and control systemknown as TRANSCOM’s Regulating andCommand and Control EvacuationSystem (TRAC2ES). TRAC2ES is amulti-nodal system composed of three basiccollaborative parts:
• The first of these is the Global PatientMovements Requirements Center(GPMRC) located at Scott AFB, IL.T h e G P M R C c o o r d i n a t e saeromedical evacuation worldwideand encompasses those duties formerlyassociated with the Armed ServicesMedical Regulating Office and theAeromedical Evacuation CoordinationCenter (AECC). In practice, theGPMRC will coordinate and allocateassets to the TPMRCs. It will alsocollaborate and integrate TPMRCschedules and plans, and communicatelift/bed requirements.
• The second integral part of patientregulating is the TPMRC. TPMRCsassume responsibilities formerlyperformed by the Joint MedicalRegulating Office and theaterAECCs. Active TPMRCs are locatedin US European Command and USPacific Command. Other TPMRCswould be established in US AtlanticCommand (USACOM), US CentralCommand, US Southern Command,and CONUS as the need arose. Theprimary role of TPMRCs is to generatetheater plans and schedules, and thenmodify (as needed) and executeGPMRC-del ivered schedules,
ultimately delivering the patient to theMTF (which includes both fixed anddeployable, Veterans Administration,DOD, and National Disaster MedicalSystem hospitals).
• The last part of the patient regulatingprocess is the respective MTF thatreceives/sends patients.
f. The Single Integrated MedicalLogistics Management (SIMLM) missionspecifies that Class VIIIA and Class VIIIB(blood) sustainment be provided andmanaged by a single organization or Servicecomponent operating in a theater. TheArmy component has the responsibilityof providing, when tasked by a JFC,effective, responsive theater SIMLM.The Army component carries out thismission through its Medical LogisticsBattalions and theater medical materielm a n a g e m e n t c e n t e r s .T h eS I M L M m i s s i o n , r o l e s , a n dresponsibilities for supporting jointforces must be clearly identified inconcept and operation plans. Furtherinformation on SIMLM is in Joint Pub4-02.1, “Joint Tactics, Techniques, andProcedures for Health Service SupportLogistics in Joint Operations.”
g. The Armed Services BloodProgram Office (ASBPO), established bythe Assistant Secretary of Defense forHealth Affairs, is responsible for thecoordination of the blood programs of theMilitary Services and the combatantcommands. The Armed Services BloodProgram provides an orderly system forcollection, storage, and distribution ofblood products across the range of militaryoperations (Figure I-4). The primaryresponsibility of the ASBPO is to ensureblood products, in the required types andamounts, reach the theater in a ready-to-use condition.

I-10
Chapter I
Joint Pub 4-02
• Each theater has a standard jointlyoperated blood distribution system.A JBPO is established within the jointforce surgeon’s office and functions aspart of the staff. The JBPO is thesingle manager for blood products inthe combatant command and isresponsible for management andcoordination of the total joint bloodp ro d u c t s re q u i r e m e n t s a n dcapabilities in the theater. Each theateris subdivided and coordinated by anArea Joint Blood Program Office(AJBPO). Responsibilities of theJBPO and AJBPOs include:
•• Monitoring compliance with DODblood program policies.
•• Coordinating component bloodprograms.
•• Planning and executing bloodprogram exercises.
•• Managing the wartime theater blooddistribution system (JBPO only).
• Blood transshipment centers(BTCs), operated by the Air Force, areestablished in each theater and arelocated at major airheads. The BTCsserve as the central receiving pointof blood products from CONUS fordistribution within the theater. EachBTC has the capacity to re-ice andstore 7,200 units of liquid blood.Blood is provided to each Servicecomponent blood supply unit (BSU)and, in turn, distributed to each MTF.
• Each MTF is responsible for locatingand notifying its respective AJBPO for
Figure I-4. Armed Forces Blood Distribution System
USABDC
JOINTSTAFF
ASBPO
ASWBPL
USA SBPOUSAF SBPOUSN SBPO
USAFBDC
USNBDC
USNSHIPMTF
USMC2EMTF
SUPPORTING BASE THEATER
UNIFIEDCOMMAND
JBPO
AJBPO
BTC
BSU
USADMSO2E
USAFMTF
USAMTF
USNASHOREMTF
USMCBSU
TBTCCIVBDC
BPD
BLOOD FLOW
REPORTS
COORDINATION
LEGEND
ARMED FORCES BLOOD DISTRIBUTION SYSTEM

I-11
The Health Service Support System
coordination of blood requirementsand submission of blood reports(BLDREPs) and requests. MTFs willbe notified by the AJBPO which BSUis their supplier of blood and bloodproducts. During operations, MTFswill submit daily BLDREPs to the BSUwith an information copy to theAJBPO. Each AJBPO will submitdaily BLDREPs to the JBPO. TheJBPO, in turn, will submit dailyBLDREPs for the theater to theASBPO. Every blood shipment willrequire preparation and transmission ofthe blood shipment report.
h. While it is important that eachcomponent command properly plan tooperate its portion of the overallhospitalization and evacuation systems anddetermine its own requirements, it isimperative that prior joint planningoccur. Distr ibut ion of respect ivecomponent HSS capabilities, as directed bythe geographic combatant commander, willaid in ensuring efficient use of limited HSSresources, particularly assets and beds.
• Each component should providesufficient MTFs for its ownrequirements and provide alltreatment and evacuation support inan area occupied or used extensivelyby that component.
• Within each component command, thecommand surgeon should exercisetechnical supervision of all HSSfunctions.
• Each MTF will prepare and submit,within 24 hours of entering the theater,
a readiness report to the JFS. Thisreport briefly discusses resourcecapability and level of HSS that canbe readily provided to the geographiccombatant commander.
i. The Army veterinary serviceprovides support to all componentcommands, including:
• Control of zoonotic diseases.
• Veterinary care of DOD-ownedanimals.
• When authorized, veterinary care foranimals of local indigenouspersonnel in conjunction with medicalcivic action and civil affairs programsconducted by the Service components.
• Veterinary laboratory support.
• I n s p e c t i o n a n d l a b o r a t o r yexamination of subsistence items forwholesomeness and quality.
j. The Army veterinary serviceprovides the food safety service listedbelow to the Army, Navy, and Marine Corpscomponents. The Air Force provides thesame support to its forces when on AirForce installations:
• Inspection of all subsistence itemsthat are received, stored, and issued inthe theater following nuclear,biological, and chemical (NBC)exposure.
• Inspection of facilities supplying,storing, and issuing subsistence items.

I-12
Chapter I
Joint Pub 4-02
Intentionally Blank

CHAPTER IIJOINT HEALTH SERVICE SUPPORT PLANNING
II-1
1. The Joint OperationPlanning Process
Operational planners must take manyfactors into account to select the best ormost appropriate means of performing ajoint force mission. Because the planningprocess is complex, it must be orderly andthorough. The amount of time available forplanning influences the entire process. TheJOPES, established by the Chairman of theJoint Chiefs of Staff, is the policy,procedures, and automated dataprocessing system used by the jointplanning and execution community fordeveloping, coordinating, reviewing,approving, and disseminating jointoperation plans. Joint operation planningc o m p r i s e s t h e f o l l o w i n g t w otime-dependent planning methods:
a. Deliberate planning is the JOPESprocess involving the development ofoperation plans (OPLANs) forcontingencies identified in joint strategicplanning documents. Conductedprincipally in peacetime, deliberateplanning procedures are accomplished inprescribed cycles that complement otherDOD planning cycles and in accordancewith the formally established Joint StrategicP lann ing Sys tem. Deve lopment ,coordination, reviews, and approval of these
plans can take up to 18 months. Deliberateplanning procedures are described in JointPubs 5-03.1, 5-03.2, and 5-03.3 (“JointOperation Planning and Execution SystemVolumes I, II, and III”).
b. Crisis action planning is the JOPESprocess involving the time-sensitivedevelopment of operation orders(OPORDs) and campaign plans inresponse to an imminent crisis. Crisisaction planning follows prescribed crisisaction planning procedures to formulate andimplement an effective response within thetime frame permitted by the crisis. Crisisaction planning procedures are found inJoint Pub 5-03.1, “Joint Operation Planningand Execution System Volume I.”
2. Health Service SupportPlanning Considerations
Timely, effective planning andcoordination are essential to ensureadequate and sustainable HSS in atheater. Joint HSS planning demands theJFS remain sensitive to HSS requirementsgenerated from the operation. Properp l a n n i n g p e r m i t s a s y s t e m a t i cexamination of all factors in a projectedoperation and ensures interoperabilitywith the campaign or operation plan.Organization of the HSS system is
“A corps of Medical officers was not established solely for the purpose ofattending the wounded and sick...the labors of Medical officers cover a moreextended field. The leading idea, which should be constantly kept in view, isto strengthen the hands of the Commanding General by keeping his army inthe most vigorous health, thus rendering it, in the highest degree, efficientfor enduring fatigue and privation, and for fighting. In this view, the duties ofsuch a corps are of vital importance to the success of an army, andcommanders seldom appreciate the full effect of their proper fulfillment.”
Major Jonathan LettermanMedical Director of the Civil War Army of the Potomac

II-2
Chapter II
Joint Pub 4-02
determined largely by the joint force’smission, the medical threat, medicalintelligence, the theater evacuation policy,and hospitalization and evacuationrequirements. Plans for health care in thetheater should ensure proper interfacewith the evacuation health care plan
detailed in USACOM’s Integrated CONUSMedical Operations Plan.
a. The medical threat is a composite ofongoing or potential enemy actions andenvironmental conditions that might act toreduce the effectiveness of the joint forcethrough wounds, injuries, diseases, orpsychological stressors. Appendix A,“Medical Threat,” discusses the medicalthreat.
b. Medical intelligence is intelligenceproduced from the collection, evaluation,and analysis of information concerning themedical aspects of foreign areas that haveimmediate or potential impact on policies,plans, or operations. A more detaileddiscussion of medical intelligence can bef o u n d in A p p e n d i x B , “ M e d i c a lIntelligence.”
c. Timely patient evacuation plays animportant role in the design of thetreatment sequence from front to rear.When the echelons of HSS become moresophisticated, the means of patientevacuation also become more sophisticated.Patient evacuation involves route
planning, movement control, and thelocating of evacuation facilities. Theevacuation of patients in a theater willprimarily be by aircraft when airtransportation is available, feasible, and thepatient’s condition permits. The JFS mustplan the means for treatment, logisticssupport, and movement of joint forcepatients that exceed the capability ofindividual MTF’s, just as the individualMTFs and medical units must havee s t a b l i s h e d i n t e r n a l o p e r a t i n gprocedures for these unforeseen surges inpatient flow. The JFS must develop andexercise these plans for interorganizationalsupport within the joint force, as well asthose medical resources that will comefrom higher echelons or adjacent forces.
d . T h e geograph ic comba tan tcommander may issue specific guidance
Health service plans must consider the evacuation of patients/casualties whocannot be returned to duty in the combat zone (Echelons I-III) to more capablehospitals in the communication zone or CONUS.

II-3
Joint Health Service Support Planning
for the medical evacuation of formerdetained US forces, civilians accompanyingUS forces, EPW, and civilian internees.
e. Specific clinical capabilities, as wellas MTF location, logistics supportability,and number of beds, must be considered.MTFs must have the clinical capabilitiesnecessary to provide care for the expectednumber and types of patients in thetheater. The location of an MTF shouldbe determined by its specific clinicalcapability, relative mobility, logisticalsupportability, and the necessity to ensurea logical progression of MTF capabilitiesfrom the forward areas of the combat zoneto the rear of the joint force. The locationof MTFs is affected further by critical timeand distance factors that impact on mortalityand morbidity rates.
f. Recommendations must beprepared by the JFS to the geographiccombatant commander concerningsupply issues. Specifically, the followingshould be considered:
• Use of a SIMLM system.
• Types of medical supplies needed.
• Supply procedures.
• Stock levels.
• Size and location of medical supplyinstallations.
• Medical equipment maintenancesupport.
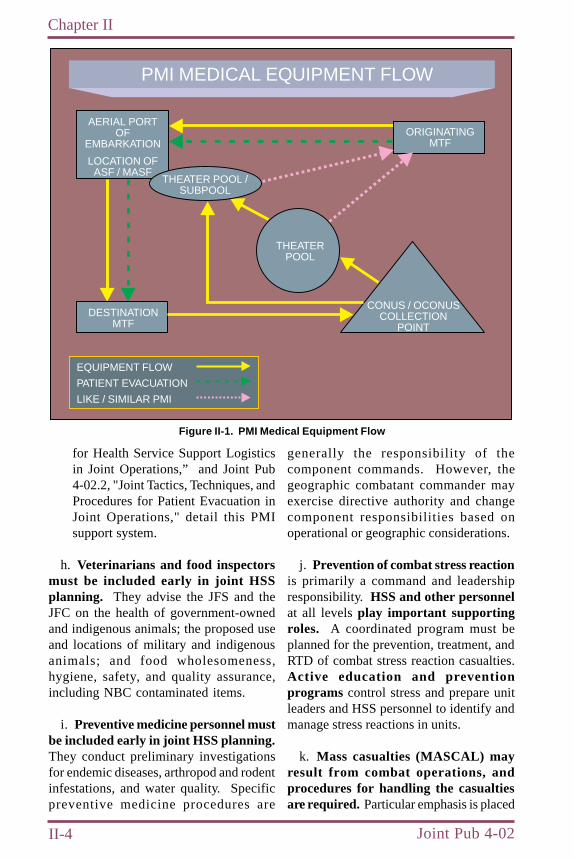
g. A major factor in the evacuation ofpatients through the five echelons ofmedical care is that specific medicalequipment and durable suppliesdesignated as patient movement items(PMI) must be available to support thepatient during the evacuation. Examples
of PMI include ventilators, litters, patientmonitors, and pulse oximeters.
• Theater-owned medical equipmentand supplies often depart theoriginating MTF as patients areevacuated. In general, the PMIaccompanies a patient throughout thechain of evacuation from theoriginating theater MTF to thedestination MTF, whether it is anintratheater or intertheater transfer.The JFC will ensure procedures areestablished for units to have theirPMIs replaced prior to their lossesbecoming a detriment to the airevacuation and patient care mission.
• An established concept which can beimplemented by the JFC to preventtheater and unit shortfalls of thecritical PMI —which are either aircertified, non-expendable, or essentialto the air evacuation mission—isillustrated in Figure II-1. A PMIpool(s) of these items can beestablished and operated by anydesignated Service, but is normallyoperated by the Army as a singleintegrated medical logist icsmanagement manager. When thetheater PMI pool is notified that a PMIis to leave the originating MTF for anintertheater transfer, a like PMI will beprovided to the losing organizationfrom the PMI pool. To the maximumextent possible, this exchange shouldtake place as the patient moves throughthe evacuation process. The PMIwhich accompanies the patient will becleaned and returned to the theater’sequipment pool through CONUScollection points located at a DefenseLogistics Agency depot. The PMI willbe inspected, repaired, refurbished, andresupplied prior to return to the theaterpool(s). Joint Pub 4-02.1, “JointTactics, Techniques, and Procedures
II-4
Chapter II
Joint Pub 4-02
Figure II-1. PMI Medical Equipment Flow
AERIAL PORTOF
EMBARKATION
LOCATION OFASF / MASF
ORIGINATINGMTF
DESTINATIONMTF
CONUS / OCONUSCOLLECTION
POINT
THEATERPOOL
THEATER POOL /SUBPOOL
EQUIPMENT FLOW
PATIENT EVACUATION
LIKE / SIMILAR PMI
PMI MEDICAL EQUIPMENT FLOW
generally the responsibility of thecomponent commands. However, thegeographic combatant commander mayexercise directive authority and changecomponent responsibilities based onoperational or geographic considerations.
j. Prevention of combat stress reactionis primarily a command and leadershipresponsibility. HSS and other personnelat all levels play important supportingroles. A coordinated program must beplanned for the prevention, treatment, andRTD of combat stress reaction casualties.Active education and preventionprograms control stress and prepare unitleaders and HSS personnel to identify andmanage stress reactions in units.
k. Mass casualties (MASCAL) mayresult from combat operations, andprocedures for handling the casualtiesare required. Particular emphasis is placed
for Health Service Support Logisticsin Joint Operations,” and Joint Pub4-02.2, "Joint Tactics, Techniques, andProcedures for Patient Evacuation inJoint Operations," detail this PMIsupport system.
h. Veterinarians and food inspectorsmust be included early in joint HSSplanning. They advise the JFS and theJFC on the health of government-ownedand indigenous animals; the proposed useand locations of military and indigenousanimals; and food wholesomeness,hygiene, safety, and quality assurance,including NBC contaminated items.
i. Preventive medicine personnel mustbe included early in joint HSS planning.They conduct preliminary investigationsfor endemic diseases, arthropod and rodentinfestations, and water quality. Specificpreventive medicine procedures are

II-5
Joint Health Service Support Planning
on the flexibility of HSS units to respondto sudden changes in the casualty situation.Successful management of MASCALs is acomplex task where success relies as muchon well-practiced logistics andcommunications as it does on skilledmedical treatment. While many medicalpersonnel receive basic exposure to theprinciples of battlefield triage andemergency management, there is much lessfamiliarity with communications,transportation, evacuation, and supplymanagement in a simulated MASCAL orcombat setting. JFSs must ensure that theMASCAL plan is rehearsed with allcomponents represented. Particularemphasis must be placed on the flexibilityof HSS units to respond to changes in thecasualty situation.
• Enemy employment of NBC weaponsproduces an unusually large numberof casualties and may impair existingprovisions for HSS. An NBC weaponsattack significantly hinders alloperations, including HSS operations.
• In an effort to provide adequate HSSin an NBC environment, definitiveplanning and coordination aremandatory at all command levels.Higher headquarters must distributetimely, well-understood plans anddirectives to subordinate units.
3. HSS Estimate of theSituation
a. The HSS estimate’s purpose is toprovide an analysis of HSS informationpertaining to enemy intentions, allied orcoalition partner’s capabilities, limitations,courses of action, and potential HSSconsequencesa s s o c i a t e d w i t h a
contemplated operation. The HSS estimatemay be written or oral.
b. The HSS estimate will include allHSS facts, assumptions, and deductionsthat can affect the operation. The JFSmust be familiar with the concept ofoperations and obtain medical intelligenceconcerning the theater from indigenoussources, the supporting intelligence activity,the Armed Forces Medical IntelligenceCenter, and national intelligence agencies.The JFS must conduct a thoroughevaluation of the enemy situation,friendly situation, and the theater fromthe standpoint of effects on the health ofthe joint force and HSS operations.
c. The HSS estimate is an analysis ofthe medical threat and HSS capabilitiesto determine vulnerabilities and estimatedrequirements of the joint force.
• Patient estimates are calculated fornumbers, distribution, areas of density,possible MASCALs, and evacuation.The JFS consults componentexperience tables to assist indetermining requirements for theoperation. Hospital estimates and othersupport requirements are derived fromthese data.
• H a v i n g d e t e r m i n e d t h e H S Srequirements, the JFS considers theresources that are readily availableto meet the requirements. Maximumuse of available personnel, supplies andequipment, and joint use of facilitiespromotes effectiveness of thecommand’sHSS. Consideringsupport requirements and resourcesavailable, the JFS determines theproposed course of action that canbe supported.

II-6
Chapter II
Joint Pub 4-02
4. HSS Planning Factors
In addition to coordinating joint forceHSS requirements, HSS planning for jointoperations involves other majorconsiderations, including coordinatingHSS requirements with other combatantcommands and coordinating with alliedand other friendly forces. The HSSplanning tool approved for medicalplanning is the JOPES MPM. Themodule is an automated applicationprogram that takes Service-specificcasualty figures using a deliberate planningtheater evacuation policy, merges them toprovide joint requirements, and projects theimpact of an operation on the HSS system.MPM provides an estimate ofrequirements for such things as themedical evacuation, requirements, andnumber of hospital beds at Echelons III,IV, and V. A more complete discussionon the use and application of the MPM canbe found in Joint Pub 5-03.2, “JointOperation Planning and Execution SystemVolume II (Planning and ExecutionFormats and Guidance)” and the MPMUsers Manual, DSSO UM 534-92.
a. The theater evacuation policy isestablished by the Secretary of Defenseupon the advice of the Chairman of the JointChiefs of Staff and recommendation of thegeographic combatant commander. (Thepolicy states, in number of days, themaximum period of noneffectiveness[hospitalization or convalescence] thatcasualties may be held within the theaterfor treatment.) The policy does not implythat a casualty must be held in the theaterfor the entire period for treatment.Casualties who are not expected to RTDwithin the number of days expressed inthe theater evacuation policy areevacuated as soon as their medicalcondition permits.
• Shorter evacuation policies withinthe theater reduce theater bedrequirements and increase the numberof beds required elsewhere. Shorterpolicies also increase evacuationrequirements.
• The time period stated in the theaterevacuation policy starts when a patientis admitted to the first hospital(Echelon III). The total time a patientspends in all MTFs in the theater fora single episode of wounding, injury,or illness should not exceed thenumber of allowable days ofnoneffectiveness stated in the theaterevacuation policy. This policy isflexible and changes as the tacticalsituation shifts. This ensures thatnonfixed MTFs retain mobility and thecapability to accommodate anticipatedsurges of patients.
b. The estimate for theater HSSrequirements is based on empirical dataaccumulated for each Service for the majorcategories of patients—wounded-in-actionand disease and nonbattle injury. As shownin Figure II-2, planning factors such as thetheater evacuation policy, bed availability,combat intensity rates, and admission ratesare analyzed to calculate HSS theaterrequirements.
• Population at risk.
• Accumulation factors.
•• Number of patients not evacuatedat the end of a specified time period(theater evacuation policy).
•• Proportion of patients admitted onany one day that will remain at the endof each specified period (length of stay/evacuation delay).

II-7
Joint Health Service Support Planning
Figure II-2. HSS Planning Factors
• Dispersion factor. (Factors,allowances, and other computationdetails are presented in FM 8-55, FM101-10-1, AFR 168-4, and NAVMATP-4000-2 series.)
c. The planning factor for bloodproducts in a theater is 4.0 units of liquidred cells per initial admission. Thereceipt, storage, and distribution of bloodproducts require special considerationand procedures to ensure a coordinatedeffort and maximum use ofcommunications, storage facilities, andtransportation. The Air Force componentwill staff and operate BTCs. The centersare located at major airfields, and bloodproducts are managed by the JBPO orAJBPO. One or more BTCs are located ineach joint force area. The BTCs:
• Receive blood products shipped to thetheater from other blood programagencies such as the Armed ServicesWhole Blood Processing Laboratory orBTCs.
• Receive and store up to 7,200 unitsof blood products for futuredistribution to theater MTFs whendirected by the AJBPO or the JBPO.
• Perform quality control checks onblood shipments, ensuring thatappropriate temperatures have beenmaintained during shipment and thereis no gross evidence of contaminationor cellular destruction.
• Provide resupply of blood productsto other BSUs or other BTCs.
5. HSS Policies and Procedures
Based upon the HSS estimate of thesituation, the JFS, in coordination with thecomponent command surgeons, must planfor medical policies and procedures thatcan be best adapted to the jointoperation. In many instances, existingstanding operating procedures can be usedwith little or no modification. In otherinstances, entirely new procedures may
HSS PLANNING FACTORS
EMPIRICAL DATAPOPULATION
AT RISKACCUMULATION
FACTORSDISPERSION
FACTORS
THEATER EVACUATION POLICYBED AVAILABILITYCOMBAT INTENSITY RATESADMISSION RATES
PLANNING FACTORS

II-8
Chapter II
Joint Pub 4-02
have to be developed and implemented.Standards must be established to deal withthe type and timing of physical, dental, andmental examinations and inspectionsnecessary to ensure that personnel in thetheater or those arriving are fit for duty.Physical standards are normallyService-specified; however, the geographiccombatant commander may directadditional or special requirements based onoperational, geographic, or climaticconditions.
6. Special HSS PlanningConsiderations
a. Amphibious task force medicalplanning responsibilities are closely relatedto those of the landing force; their facilitiesare mutually supporting. Detailed,coordinated, and parallel planning isrequired between the commanders,amphibious task force, and landing force.Each surgeon of these commands hasspecific medical planning responsibilitiesthat are detailed in Joint Pub 3-02, “JointDoctrine for Amphibious Operations.”
b. Combat search and rescue (CSAR)operations are specific tasks performedby rescue forces to recover distressedpersonnel during wartime or contingencyoperations. Each component commandperforms CSAR in support of its ownoperations. JFCs have the primary authorityand responsibility for CSAR in support ofUS forces within their area of responsibility/joint operations area and also must ensurecreation of a joint rescue capability. TheHSS capabilities of CSAR units vary fromcomponent to component, but are generallylimited. Certain component CSAR units arededicated to CSAR operations while othersperform CSAR as a secondary mission.Marine Corps aviation units currently donot conduct CSAR, they do, however,possess the capability to conduct tactical
recovery of aircraft and personnel, whichmay involve ground units as well. Thismission has a different emphasis andapplication than the traditional CSARmission. Additional information on CSARcan be found in the Joint Pub 3-50 series.
• Joint force CSAR HSS capabilitiesare limited to recovering or evacuatingthe sick or injured from low- tomedium-threat environments. Theyprovide medically supervisedevacuation of the sick and injured fromboth peacetime and wartime situations.HSS personnel on rescue aircraft arecapable of providing emergencymedical treatment (EMT) for traumaticinjuries as well as continuing treatmentof life-threatening injuries or diseasesduring transportation.
• Although CSAR units require HSSsimilar to other units, supportedgeographic combatant commandersmust establish a flexible HSS systemto meet the demands of CSARoperations. A majority of CSAR HSSrequirements can be met by thecomponent surgeon; however, severalkey issues must be emphasized in anyjoint CSAR HSS plan:
•• Adequate intelligence for thetheater is critical to the success ofCSAR operations.
•• Support requirements for CSARoperations are shown in Figure II-3.
•• Some CSAR units do not deploywith organic flight surgeon support.Other units require flight surgeonsupport for technical assistance in theareas of EMT and administration ofmedication, continuing medical careand education, and CSAR missionsupport requirements.

II-9
Joint Health Service Support Planning
SUPPORT REQUIREMENTS FOR COMBATSEARCH AND RESCUE (CSAR) OPERATIONS
Replenishment of used or outdated medical supplies(medication and material).
Oxygen supplies.
Medical equipment maintenance.
Narcotic storage and control.
Storage of temperature-sensitive medical material.
Optical fabrication.
Blood supply, storage, and distribution.
Figure II-3. Support Requirements for Combat Searchand Rescue Operations
7. HSS for the Return of USPrisoners of War
The geographic combatant commanderestablishes a theater protocol on theproper handling and provision of HSS forreturn of US prisoners of war (POWs).Detailed study of this subject area iscurrently under way; however, thefollowing basic assumptions must beincluded in the return of POW planningprocess:
a. In-theater HSS will be administeredwithin a reasonably short period upon returnto friendly forces.
b. Treatment assessments will beestablished, since short- and long-termtherapy may be required.
c. Group cohesiveness will bemaintained.
d. Operational specialty medicalsupport, such as flight surgeon support toaviators, will be provided immediately.
e. Multi-Service HSS units will beestablished to coordinate and assist inpossible contingencies.
8. HSS for EPWs
In consonance with provisions outlinedin the Geneva Conventions, patients whoare EPWs are afforded the same level ofHSS and medical care as patients of thedetaining power. Seriously wounded,injured, or sick EPWs will be evacuatedthrough medical channels, but will besegregated from US and allied patients.EPWs will be evacuated from the combatzone as soon as possible. The JFC mustensure appropriate security is provided toguard the EPWs while a patient is in theMTF and throughout evacuations.

II-10
Chapter II
Joint Pub 4-02
Nonmedical personnel should not be usedas guards if it can be avoided. Qualifiedmedical retained personnel (RP) will beused as much as possible in medical andhygiene work needed for the well-being ofEPWs; however, medical RP will belongto the same armed forces as the EPW.
9. Command, Control,Communications, andComputer Systems
Ef f e c t i v e c o m m a n d , c o n t ro l ,communications, and computer (C4)systems are vital to successful HSS injoint operations. HSS functions dependupon responsive C4 systems to tie togetherall aspects of support and to allow JFCs todirect, monitor, question, and react assituations develop.
a. Command and control (C2) of HSSorganizations normally rests with thecomponent commands. The geographiccombatant commander may providedetailed theater communication plans orassign theater communication managementresponsibilities to a single Servicecomponent for specific functions duringjoint operations.
b. Early identification of a theater’sC4 system requirements for HSSconnectivity is essential. At a minimum,HSS communications must supportreliable, constant communications withina theater, from the theater to CONUS, andlink the most forward HSS elements in thetheater through each echelon in the phasedHSS system to the final destination MTF.The success of HSS operations dependsupon reliable communications overdedicated and parallel systems. HSScommunications planners working with thejoint force communications section mustidentify frequencies that are commonbetween Service component support forces
assigned to HSS missions. If nocommonality exists, then planners shouldconsider assigning a component to developa theater plan that ensures adequatecommunications support to all components.
• Short-range radio communicationsshould be provided between MTFs andevacuation vehicles or aircraft. Theseradios should be provided bycomponent command HSS units.
• Depending on the theater infrastructureand deploying Service componentc a p a b i l i t i e s , l o n g - r a n g ecommunications will be provided byhigh-frequency radios, DefenseSwitched Network, Defense DataNetwork, and Automatic DigitalNetwork communications systems.
• Satellite communications offeringaccess to commercial phone systems orpoint-to-point systems may beavailable when ground-sourcedfacilities are unavailable.
• Secure communications are providedthrough the use of speech and datasecurity communications equipment.
• All frequency requirements fororganic equipment must be coordinatedwith the joint force commander’s J-6staff.
c. HSS system management informationsystems support the informationmanagement requirements of HSS unitsacross the range of military operations. Thesystems also assist the user in carrying outfunctional responsibilities.
• HSS management information systemsmust be interoperable with DODmedical management informationsystems.

II-11
Joint Health Service Support Planning
• HSS management information systemsshould provide timely, accurate, andrelevant information through thefollowing subsystems:
•• Blood management.
•• Patient tracking and movement.
•• Medical logistics.
• Each subsystem will have C2capabilities that provide the status(summary reports) of HSS units,evacuation work load, and criticalresources through predeterminedreports or from information selected bythe user.
d. Records and reports are required topass information and assist in theevaluation of policies and procedures.The JFS must determine the amount of HSSinformation essential to the geographiccombatant commander and make provisionsto obtain this information through aminimum number of medical records andreports. In making this determination, theJFS must be familiar with the records andreports required by the componentcommands involved in the operation. JFSshould recognize that these records andreports can serve information requirementswithout modification or supplementation.
e. Medical information in itself is notclassified. However, medical informationcan become an operations security(OPSEC) indicator in the context of aparticular military operation. OPSECmeasures to reduce or eliminate theseindicators may entail restrictions onmedical information dissemination andare detailed in OPLANs or OPORDs.OPSEC measures may require encryptionfor transmission only of medicalinformation.
10. Dental Services Support
a. The HSS dental service is a majorcontributor to maintaining unit fightingstrength. Joint operation planning mustinclude consideration of the various rolesof dental services. Historical reviewindicates that dental problems cause asmuch as 8 percent of a unit’s noncombatcasualty losses.
b. The planning process includes anevaluation of the size and anticipatedduration of the operation, along with thelevels of dental care as shown in FigureII-4 required throughout the operation.
• Level I--Emergency Dental Care.Austere treatment of dentalemergencies that immediately returntroops to duty. This minimal level ofcare does not require dental facilities.
• Level II--Sustaining Dental Care.Expedient dental treatment thatintercepts potential emergencies to
LEVELS OFDENTAL CARE
LEVEL IEMERGENCY DENTAL CARE
LEVEL IISUSTAINING DENTAL CARE
LEVEL IIIMAINTAINING DENTAL CARE
LEVEL IVCOMPREHENSIVE CARE
Figure II-4. Levels of Dental Care

II-12
Chapter II
Joint Pub 4-02
minimize troop loss to units in combatoperations. This level of care isessential to the preservation of fightingstrength early in the conflict, which isusually provided in combat servicesupport areas adjacent to Echelon IImedical support. Planners can includedental personnel to augment medicalunits during periods of MASCALsreception.
• Level III--Maintaining Dental Care.Definitive treatment to prevent andtreat dental and oral conditions earlyenough to preserve satisfactory oralhealth. This level of care is necessarywhen planning HSS for lengthymilitary operations.
• Level IV--Comprehensive Care.Treatment to restore an individual tooptimal oral health, functions, andesthetics. Comprehensive dental caremay be achieved incidental to
maintaining, sustaining, and providingemergency care in individuals whoseoral condition is healthy enough to beaddressed by the levels of careprovided. This level of care is usuallyreserved for HSS plans that anticipatean extensive period of reception andtraining in theater. The scope offacilities needed to provide this levelof detail support can equal that ofEchelon III medical facilities.
c. Deliberate planning for dentalservices must include the potential foraugmenting the medical effort duringMASCALs. Joint planning requires astatement specifically excluding dentalservices, if deemed appropriate. Jointoperations of limited size or duration maylimit dental services to predeploymentscreening, which eliminates planning fordeployment of dental personnel andequipment.

CHAPTER IIIHEALTH SERVICE SUPPORT IN SPECIAL OPERATIONS
III-1
“...for bad indeed is the condition of a General when he has a sicknessamong his men and an enemy to contend with at the same time.”
Niccolo MachiavelliThe Art of War
1. General
Special operations forces (SOF) arespecially organized, trained, andequipped forces of the Army, Navy, andAir Force that conduct the followingoperations: unconventional warfare,strategic reconnaissance, direct action,foreign internal defense, counterterrorism,civil affairs, and psychological operations.The nature of special operations requiresthat units be small, highly skilled,self-contained teams that can be easilyinserted and extracted by air, sea, and landdelivery methods. Medical support ofspecial operations units is characterizedby an austere structure and a limitednumber of medical personnel withenhanced medical skills. The specialoperations medical personnel provideemergency treatment and a basic level ofmedical care at the team level. To meet theoperational requirements of SOF infiltrationand exfiltration, characteristics of largermedical elements of Echelons II, III, andIV cannot be applied or incorporated.Medical support provided to the teamsin the area of operations is planned andconducted by SOF surgeons and medicalpersonnel. Provision of medical supportbeyond this area of influence or capabilitydepends on the thoroughness of advancedplanning so that the conventional medicalsupport structure umbrella is extended tocover lack of capability or meetrequirements for additional medical assets(i.e., medical evacuation). Medicalcapability that is not part of a Serviceconventional medical system will be basedon a complete mission analysis and a
coordinated support plan developed by themedical planner. SOF should be providedall functions of health service support at thepoint their personnel enter the conventionalforce medical structure.
2. Organic HSS Capability
a. Commander in Chief, US SpecialOperations Command, as a supportingcommander, normally provides SOF tothe commanders of other combatantcommands for operational employment.SOF based in-theater are under thecombatant command (command authority)of the geographic combatant commander.To provide the necessary unity of command,each geographic combatant commanderhas established a subordinate unifiedcommand to serve as the functional specialoperations component. The Armycomponent consists of Special Forces unitsthat are regionally oriented on specific areasof the world. Rangers can also be includedalong with Army Special OperationsAviation. The Navy component consists ofregionally oriented sea-air-land (SEAL)teams, as well as special boat units, andSEAL delivery vehicle teams. The AirForce component consists of regionallyoriented squadrons forward-deployed witha mix of aircraft specially suited to supportspecial operations missions. The specialoperations command (SOC) is the levelat which medical planning is coordinatedin sufficient detail to support specialoperations with conventional medicalpackages to augment the lack of SOForganic medical capability.

III-2
Chapter III
Joint Pub 4-02
to provide advice and expertise to thesupported missions and not medicalsupport to the force. Echelon IItreatment capability is not organic toall ARSOF. Army Special Forces andRanger battalions have limitedEchelon II capabilities. Casualty
evacuation by dedicated aeromedicalaircraft is the preferred method ofevacuation. ARSOF do not possess thiscapability. The other organic medicalcapabilities of preventive medicine,lab, veterinary, and dental support arelocated in the Special Forces groups.A medical supply capability exists inSpecial Forces groups and Rangerbattalions.
• Navy SOF HSS assets are organic tothe SEAL teams and provideEchelon I care. Health care andmedical evacuation beyond Echelon Iare supported by various Navyconventional units, such as the floatingplatform from which the team is staged,or Army and Air Force conventionalunits providing medical support on anarea basis. This can include ArmySpecial Forces forward operating
Special Operations Forces deploy with medical support capable of providingemergency treatment and a basic level of medical care (Echelon I).
b. Organic SOF HSS assets of theArmy, Navy, and Air Force are extremelyaustere. The nature of SOF missionsrequires that SOF medical personnelpossess a variety of enhanced medicalskills that enable them to operate under amultiplicity of circumstances. SOF
enlisted personnel receive enhancedmedical training that exceeds the level andscope of that training afforded theirconventional medical counterparts.
• Army SOF (ARSOF) HSS assets areorganic to Special Forces andRanger units and Army SpecialOperations Aviation units. SpecialForces teams and Ranger companiesare capable of providing Echelon Icare. Army Special OperationsAviation units have flight surgeons butdo not provide Echelon I capability.Civil affairs and psychologicaloperations battalions have no organicmedical assets for medical care to theirunit and are dependent on area medicalsupport from conventional forces.Civil affairs and psychologicaloperations battalions have medicalpersonnel assigned but are organized

III-3
Health Service Support in Special Operations
bases. Additionally, conventionalNavy and Marine units with organicEchelon II capability can providemedical support to the SEAL teams.Aeromedical evacuation is notavailable and must be provided bysupporting units. Navy SEAL teamshave no preventive medicine, lab,veterinary, and dental support. SEALteams deploy with basic loads ofmedical supplies and can be resupplied.
• Air Force Special Operations Forces(AFSOF) HSS capabilities arealigned with AFSOF operationalunits and consist of SOF medicalelements (SOFME) (flight surgeonsand aeromedical technicians) andpararescue specialists assigned tospecial tactics teams. AFSOF haveEchelon I and limited Echelon IIcapability. Echelons III and IVcapability must be provided to theforce. SOFME provide Echelons I andII care for AFSOF and other SOF andprovide flight medicine, limitedmilitary public health andbioenvironmental engineering, medicalintelligence, field laboratory, patientdecontamination, and short-termpatient holding and stagingcapabilities. Mission requirements willdictate deploying a stand-alonepersonnel package utilizing medicalrapid response deployment kits or inconjunction with a SOF airtransportable treatment unit.
•• Special tactics pararescuespecialists perform advancedbattlefield trauma care andemergency medical treatment(Echelon I and limited Echelon II)care. They function as the primaryresponders in support of personnelrecovery operations, conduct casualtycollection in direct action missions,and provide medical survival and
recovery assistance in sensitive,hostile, or denied areas.
•• Although AFSOF have no organicconventional tactical or strategicaeromedical evacuation (AE)capability, both SOFME and specialtactics teams have the capability toprovide medical treatment duringcasualty evacuation onboard SOFaircraft. AE for SOF is difficultbecause SOF frequently operate atdistant locations without any otherassets in theater. Remote locations inimmature theaters not served by thestrategic evacuation system requiresclose coordination between thesupporting Air Force componentcommand and joint medical plannersto identify the details and proceduresfor AE.
3. SOF Medical SupportPlanning
a. The goal of special operationsmedical support planning is twofold:first, provide integrated, augmentedconventional support into the concept of thespecial operating mission withoutcompromising the objectives; second,articulate the unique aspects of theoperation that will complicate the deliveryof medical care, evacuation, PM support,dental, combat stress, or veterinary supportby conventional units. The SOF medicalplanner must ensure that the conventionalmedical planner understands these aspects.The conventional medical planner musttranslate SOF-unique requirements into theconventional medical framework best suitedto support the mission.
b. These issues are complicated by thenature of SOF operations and the abilityof SOF units that routinely work togethermixing Army, Navy, and Air Force assets.SEAL teams could, for example, be
III-4
Chapter III
Joint Pub 4-02
evacuated by Army aircraft to an ArmyEchelon III facility. The issues that warrantattention are matters pertaining to thedifferent methods used by the Services forexecuting medical care and evacuation thatwill disrupt continuity or jeopardizemedical care for the casualty.
c. Unique aspects of medical support,as shown in Figure III-1, to SOF must beincorporated into medical planning at thetheater JFS staff level, with full knowledgeand concurrence of SOC planning staff.(SOC components are authorized medicalplanners and command surgeons during fullmobilization.) Medical support must beplanned and coordinated with subordinatejoint force elements by the theater JFS staff.The integration of medical support from theconventional side extended to the full rangeof missions conducted by SOF must besynchronized with the tactical plan prior toexecution.
• Extended distances and isolatedlocations create problems forconventional units if they have tosupport SOF. Extending the healthservice support functions to SOF is
beyond the normal missionresponsibility of the conventionalmedical units. The level of detail inplanning and coordination is muchgreater, and the difficulty of supportto SOF increases. An extendedevacuation mission with aeromedicalaircraft, such as an extended rangeUH-60 helicopter, requires detailedadvance planning. There are a limitednumber of these aircraft available tosupport medical missions. Allocatingthese aircraft for SOF missions alsoimpacts on the conventional force’smission. This allocation can be aproblem when there are competingmissions and the aircraft must be taskedto support a SOF mission that isexternal to the command and not theprimary mission of the medicalevacuation unit. The theater JFS mustprioritize the mission and planaccordingly.
• Conventional medical units often aretasked beyond their organiccapabilities to support, and oftentheir support missions are prioritizedaccordingly at the unified level. This
Figure III-1. Challenges of SOF Medical Support
CHALLENGES OF SPECIAL OPERATIONSFORCES (SOF) MEDICAL SUPPORT
Extended distances and isolated locations.
Limited organic capabilities to support.
Limited equipment capabilities.
Underdeveloped theaters with minimal health care support.
Operational security requires restricted access.
Politically sensitive missions.
Retaining injured personnel in-theater as critical assets.

III-5
Health Service Support in Special Operations
problem of multiple taskings andlimited resources makes theintegration of support to SOF anotherfocus of the exchange between SOCnonmedical planners and theater JFSplanners.
• Evacuation of casualties within thejoint special operations area can bedone by SOF aircraft, but these aircraftare not medically equipped or staffedto be used in a backhaul capacity. Theconventional planner must understandthis limitation when determining howto best support SOF-generatedevacuation requirements.
• SOF will often operate in theatersthat are underdeveloped with little orno health care support structure.Point-to-point movement or medicalregulating and strategic AE might berequired.
• Some programs or missions arecompartmented, and the need foroperational security requiresrestricted access for planningpurposes. The medical planner mustestablish an exchange of only sufficientinformation to provide medical supportfor the plan.
• SOF medical support beyondinherent unit capabilities is totallyreliant on the theater JFS for all othermedical support. The theater JFS hascoordinating responsibility for allmedical forces assigned to or operatingin the geographic area.
• There is often a requirement tosafeguard the patient’s identity,which might compromise the unit’spresence or jeopardize the mission.SOF missions are often politicallysensitive.
• A modified evacuation policy forSOF personnel must be published sothey can be retained in-theater as acritical asset. Transportation out oftheater should be precluded wheneverpossible, dependent on the condition ofthe casualty.
• The entry points into theconventional system might includenonmedical aircraft that could transportSOF casualties from point of injurydirectly to an Army, Navy, or Air ForceEchelon III MTF. The conventionalmedical planner must ensure that theMTF in that area is knowledgeable ofthis unique method and be prepared torespond. The MTF might be a hospitalship, casualty receiving and treatmentship, or an Air Force air transportablehospital.
• Communications and control ofmedical assets may be problematic.Conventional Army, Navy, or AirForce medical elements haveincompatible hardware and softwaretelecommunications equipment thatdiffers from SOF telecommunicationsequipment. Connectivity plans and theprocedures for communicating must bedeveloped in order to pass real-timeinformation across signal waves so thatcasualties can be moved with success.
d. The following list is provided as aguide for developing a joint HSS plan thatmeets the unique SOF operationalrequirements by focusing on the healthservice functions not organic to SOF thatthe conventional system would provide:
• A statement of the medical situation.
• A statement of the medical evacuationpolicy.

III-6
Chapter III
Joint Pub 4-02
• Clear delineation of the medicalresponsibilities, organizations, andemployment of available medicalsupport system elements, withparticular emphasis on shifts inresponsibility during the several phasesof the operation and on the measuresnecessary to ensure coordinatedmedical action by all elements of thetask force.
• Projection of the requirements formedical support and the existingcapabilities available to provide thatsupport at the projected location.
• Provisions for medical services inconnection with the evacuation ofcasualties from the objective area (enroute medical care).
• M e d i c a l s u p p l y , i n c l u d i n greplenishment of supplies andexchange of medical equipment.
• Procedures and responsibilities forkeeping necessary records andreports on the flow of casualties andindividual patient status information.
• Provisions for medical service topatients (dental, laboratory, X ray,combat stress).
• Provisions for obtaining medicalintelligence.
• Measures for preventive medicine;nuclear, biological, chemical warfaremedicine; and hygiene and sanitationprocedures.
• Procedures for distribution of bloodand blood products.
• Procedures for medical surveillance,collection, and reporting.

CHAPTER IVHEALTH SERVICE SUPPORT IN MILITARY
OPERATIONS OTHER THAN WAR
IV-1
1. General
Military operations other than war(MOOTW) encompass a wide range ofactivities where the military instrument of
national power is used for purposes otherthan the large-scale combat operationsusually associated with war. They caninvolve operations in support of foreigngovernments or US civil authorities. Theyare usually joint operations, oftenperformed in concert with othergovernment agencies, nongovernmentalorganizations, and private volunteerorganizations. Some military operations,such as disaster relief and combattingterrorism, may be conducted on US soil.Regardless of where these operations occur,
they are an important element of the USNational Military Strategy. They are basicbuilding blocks for two of the foundationsof that strategy: forward presence and crisisresponse. The provision of HSS becomes
a primary means of assistance in theseoperations.
a. HSS operations conducted to enhancethe stability of a host-nation (HN)government must be well-coordinatedwith all concerned agencies and integratedinto the respective US Embassy plan.Independent, unplanned medical civicaction programs should not be undertaken.Coordination by the geographic combatantcommander should be accomplished with:
“Pay every attention to the sick and wounded. Sacrifice your baggage,everything for them. Let the wagons be devoted to their use, and if necessaryyour own saddles...”
Napoleon I
Joint Task Force medical personnel provide assistance and process a Haitianrefugee who was rescued during Operation SEA SIGNAL.

IV-2
Chapter IV
Joint Pub 4-02
OPERATION IDA
On 1 September 1962, a series of earthquakes struck northwestern Iran, andon the 3rd the Joint Chiefs of Staff directed United States Army, Europe(USAREUR), to send aid to the victims. Early the next morning, the airlift ofthe 8th Evacuation Hospital with a professional staff drawn from severalhospitals in Europe began at Ramstein Air Force Base. With the 8th EvacuationHospital went helicopter elements of the 421st Medical Company (AirAmbulance), a field maintenance detachment from the 29th TransportationCompany, a preventive medicine detachment from the 485th Laboratory(Preventive Medicine), and a water purification unit from the 299th EngineerBattalion. Lt. Col. Alexander M. Boysen, 8th Evacuation Hospital commander,assumed command of the entire relief force.
When the Americans arrived in Tehran, Iranian officials instructed them tolocate their hospital on the plain of Kazvin, a site near the worst area ofdestruction but adjacent to a rail line and a hard surface road. Iranian driverstransported the unit, and the Americans worked through the night to becomeoperational at 0900 hours on 6 September. The next day the Americansestablished a base camp near Buin, further into the disaster area, to serveboth as a first aid station and as a helicopter base. From it, crews flew medicalteams into the distressed area and evacuated seriously injured victims to thehospital. On the flight back into the area to pick up the teams, the helicoptersbrought in food, tents, and other essentials. In all, the choppers flew 404sorties, delivered 45,000 pounds of supplies, and evacuated 66 patients.
Operations at the 8th Evacuation Hospital where the helicopters brought thecasualties did not proceed without difficulties. High winds wreaked havoc onthe unit’s tents because pegs did not hold in the sandy soil. After two days’service, the laundry exploded, badly burning three enlisted men. Supplyshortages developed, particularly of items not ordinarily required by a fighting
• Assistant Secretary of Defense(Operations and Low IntensityConflict)/Humanitarian and RefugeeAffairs.
• HN government and health serviceofficials.
• The Ambassador and the CountryTeam.
• The United States Agency forInternational Development.
• Security assistance forces.
• US military on-scene commander,including military civil affairselements.
• Nongovernment organizations, privatevolunteer organizations, and religiousgroups.
b . T h e S e c u r i t y A s s i s t a n c eOrganization monitors psychologicaloperations and alerts HN counterparts tothe psychological impact of all militaryactions, operations, and acts of the HN’sarmed forces. Medical assistance inoperations other than war include provisionof HSS for HCA programs. HSSpersonnel in this type of environment mustbe prepared to protect themselves from andinitiate appropriate responses to terroristactivity.
IV-3
Health Service Support in Military Operations Other Than War
unit—catheters for small children, for example. The professional staff drawnfrom various facilities in Europe had never trained with the hospital, and theresulting confusion hindered operations.
Another difficulty, the suspicion and hostility of the local population was onlyovercome through Iranian cooperation and American flexibility. Localgovernment officials, and the shah himself during a visit, urged the people tocooperate. Even with a royal endorsement, however, the 8th EvacuationHospital’s staff had to make minor adjustments to local customs—such asconstructing latrines that pointed south. Its commander reported: “Manydecisions that...were strange to Americans were made because they were notstrange to Iranians...When one helps a foreign nation you accept their strangephilosophy in many things, if by doing this it means you eventually gain yourobjective.”
As it solved its organizational problems and slowly secured the cooperationof the Iranians, the 8th Evacuation Hospital became an efficient emergencyhospital. It admitted 182 victims, provided a total of 794 patient-days of care,and reported five deaths. Its surgeons performed seventy-five surgicalprocedures, most involving multiple fractures or internal injuries. Many victimssuffered cuts and bruises; other patients had been badly burned, and one ofthe burn cases had a baby during her stay in the hospital. Fortunately, a doctorassigned for general medical work had an obstetrical specialty, and he delivereda healthy baby, promptly named Ida after the code name of the American reliefoperation (Iranian Disaster Assistance). Hospital staff members cut fingersfrom rubber gloves to make bottles, the kitchen crews and pharmacistsimprovised a formula, and a sergeant constructed a crib for Ida from packingcrates.
In addition to nursery service, hospitalization, and helicopter support, theAmerican relief force furnished preventive medicine assistance within thedisaster area. Working out of the base at Buin, Army specialists visited some150 villages where they supervised delousing and immunization teams andinstructed the local populace in personal hygiene and public health. TheAmericans also tried to ensure a clean, pure water supply for each of thevillages. The Erdlator, a water purification machine the engineers had broughtwith them, proved useless since the ambling, truck-mounted monster couldnot traverse the rugged terrain. The Americans relied on the simpler WaterPurification Set No. 3 or chlorinated water from deep wells distributed in tanktrucks.
By September the medical and sanitary situation in the area had stabilized,and the United States ambassador approved the withdrawal of the 8thEvacuation Hospital. Because of difficulties in air transportation, all were notable to leave until the middle of October; when they finally did depart, theAmericans left the equipped hospital for the Iranians.
SOURCE: Foster, Gaines M., The Demands of Humanity: Army MedicalDisaster Relief , US Army Center of Military History, 1983.

IV-4
Chapter IV
Joint Pub 4-02
2. Humanitarian and CivicAssistance, HumanitarianAssistance, and DomesticSupport Programs
a. As shown in Figure IV-1, HCAactivities are designed to provideassistance to HN populace in conjunctionwith US military operations or exercises.Humanitarian assistance (HA) operationsare conducted to relieve or reduce the resultsof natural or manmade disasters or otherendemic conditions such as human pain,disease, hunger, or privation that mightpresent a serious threat to life or that canresult in great damage to, or loss of propertyuntil the appropriate civilian agencies canaccept this responsibility. HSS has beeninvolved in domestic support operationswithin the United States. Both programs
focus on assisting the local populace byfurnishing assistance that the localgovernment is not capable of providing.These programs offer much-needed servicesto the populace, allowing time for the localmedical infrastructure to develop orregenerate. HSS is often provided withina larger military involvement. It may beconducted in any terrain or geographic area.Prior to undertaking such action, thegeographic combatant commandershould ensure that the mission statementof the HSS organization clearly supportsthe HA operation. Coordination with theJFS or component command surgeon isessential to ensure that the HSSorganization is capable of and legallyallowed to fulfill the requirements of themission statement. Organizations describedin subparagraphs 1a and 5d must make
Figure IV-1. Humanitarian and Civic Assistance (HCA)Program Overview
HUMANITARIAN AND CIVIC ASSISTANCE (HCA)PROGRAM OVERVIEW
HCA activities provide assistance to host-nation populace inconjunction with US military operations or exercises.
Conducted to relieve or reduce the results of:natural / manmade disastershuman paindiseasehungerthreats to lifethreats to property
Furnish assistance that the local government is not capable ofproviding.
Allows time for local medical infrastructure to develop or regenerate.
Often provided within a larger military involvement.
May be conducted in any terrain or geographic area.

IV-5
Health Service Support in Military Operations Other Than War
every effort to analyze and consider allpolitical and cultural factors prior tocommencing operations. In the case ofdomestic support operations and militarysupport to civil authorities within CONUS,the military HSS organizations mustconsider the various civilian agencies suchas the Federal Emergency ManagementAgency (FEMA) and the Department ofHealth and Human Service’s Public Health
Service, that play a significant role incivilian-managed relief operations.Consequently, the level of autonomousdecisionmaking ability characteristic ofmilitary operations is often restricted.
b. The parameters required to assessthe HN needs vary with each situationor country. Assessment factors are shownin Figure IV-2.
Figure IV-2. Assessment Factors in Assistance Programs
ASSESSMENT FACTORS IN ASSISTANCEPROGRAMS
Population demographics.
General health of the population (emphasis on nutrition).
Sanitation and personal hygiene.
Endemic diseases (emphasis on arthropod-borne and waterbornediseases).
Primary care capabilities, including dental, especially in rural areas.
Infant mortality rates.
Availability and accessibility of health care delivery systems andprocesses.
Secondary and tertiary hospital facilities and supportingtransportation capabilities.
Education and training levels of health service support professionalsand technicians.
Local facilities for production of medical equipment and supplies.
Political impact of providing care to the host-nation population.
Long-term requirements and the ability to provide continuity of care.

IV-6
Chapter IV
Joint Pub 4-02
3. Other HA
HSS planning factors include carefulconsideration of a wide variety ofpatients. There may be indigenous allies,friendly and unfriendly civilians orparamilitary organizations, representativesof various civilian and military agencies,and civilian contractor personnel employedby the United States. Any individual maybe treated on a humanitarian basis if spaceand staff are available.
4. HSS Aspects of CombattingTerrorism
All HSS units must have the capabilityto react quickly and decisively once a ter-rorist incident has occurred. Additionally,they must be prepared to defend themselvesand their patients.
a. Because terrorist acts can occur anytime and any place, it is imperative that allMTFs have well-conceived and updateddisaster casualty control plans and contin-gency support plans. The plans must includea strategy for conducting patient evacuationoperations under hazardous conditions.
b. Contingency plans must beestablished that consider the location andcapability of sources for HSS. At aminimum, these plans must considerterrain, population densities, major accessroads, and possible landing zones.
c. The JFS or component commandsurgeon may designate rapid responsemedical teams at specific MTFs. Theseteams must be able to rapidly deploy to thesite of an incident, assess the HSS require-ments, and obtain the needed assistance toeffectively manage the situation.
d. HSS staffs must be trained in thedebriefing process to assist victims ofterrorist-related activities in working
through the emotions and feelingsassociated with their experiences.
5. Disaster Relief Assistance
A significant number of HA programsinvolve disaster relief operations. Themilitary can provide assistance to help easethe effects of natural disasters and manmadeevents. Characteristics of Disaster ReliefAssistance are shown in Figure IV-3 and arediscussed below.
a. HSS assistance requires rapidassessment of the damage caused by thedisaster and a rapid tailoring of an HSSelement to meet the needs of the affectedpopulace. The HSS element should have awide range of specialties available toconduct an accurate assessment.
b. PVNTMED plays a key role in therelief effort since natural disasters candisrupt the ecological balance, causingpotential disease outbreaks. Measures toensure sanitation and disease vector controlmust be planned for and implemented assoon as possible.
c. The treatment rendered may beaustere and possibly provided inrudimentary facilities.
d. The HSS response must be able toreach the disaster site rapidly, with theright mix of specialties, and becoordinated with concerned agencies. Inaddition to applicable entities identified insubparagraph 1a, coordination should beestablished, as appropriate, with:
• Director of Military Support.
• FEMA.
• State and local office of emergencyservices.

IV-7
Health Service Support in Military Operations Other Than War
• Emergency medical systems.• Local US military medical treatment
facilities and Department of VeteransAffairs medical treatment facilities(including their role as coordinatorsof national disaster medical systems).
• Department of Health and HumanService’s Public Health Service.
6. The AE Role
The casualty evacuation policy duringmilitary operations for operations otherthan war may be substantially differentfrom the policy associated with a generalwar. Because of limited MTFs within the
operational area, the theater evacuationpolicy may call for AE within a few hoursof a casualty being wounded. In the caseof contingency or humanitarian operations,casualties may be moved as soon as theyare medically stabilized for airlift. Theregulating process may rapidly develop intoone that is fixed for the duration, withevacuation limited to one destination. Anoperation could normally employ thesame AE elements that are found in thewartime scenario, with the type, number ofelements employed, and location(s) tailoredto fit the contingency situation. Mostlimited AE operations are expected torapidly develop into a repeatable pattern oforigin locations, destination locations, and afixed frequency of operational missions.
Figure IV-3. Disaster Relief Assistance
DISASTER RELIEF ASSISTANCE
Health service support (HSS) assistance requires rapid assessment ofthe damage caused by the disaster.
Rapid tailoring of an HSS element to meet the needs of the affectedpopulace.
Preventive medicine (PVNTMED) plays a key role in the relief effort.
Measures to ensure sanitation and disease vector control must beplanned for and implemented as soon as possible.
Treatment rendered may be austere and provided in rudimentaryfacilities.
HSS response must be able to reach the disaster site rapidly, with theright specialties.
Coordination should be established, as appropriate, with:Director of Military SupportFederal Emergency Management Agency (FEMA)State and local office of emergency servicesEmergency medical systemsLocal US military medical treatment facilitiesLocal Department of Veterans Affairs (DVA)Department of Health and Human Service's Public HealthService

IV-8
Chapter IV
Joint Pub 4-02
Intentionally Blank

APPENDIX AMEDICAL THREAT
A-1
• Leptospirosis.
• Arbovirus infections.
• Hemorrhagic fever with renalsyndrome.
• Schistosomiasis.
b. Extreme environmental conditionsin the form of heat, cold, high humidity, andhigh altitude can pose significant healthhazards to an unacclimated, unprepared,and poorly conditioned military force.Employment of US forces into areas wherethese conditions exist without adequateopportunity for acclimatization maysignificantly decrease combat performance.Appendix C, “References,” containsreferences concerning HSS in differentgeographic areas and climates, such asdesert, tropics, arctic, and mountains.
c. Conventional warfare munitionsinclude small arms, high velocity weapons,rockets, bombs, artillery, bayonets, andother wounding devices, either individualor crew-served. This threat may beencountered in all geographic areas andcan be employed by adversaries acrossthe range of military operations.Research and development in smartmunitions and extended range artillery,coupled with more powerful highexplosives, will increase the threat fromthese types of weapons. Area denialmunitions are likely to be present and posea major psychological and physical threat.Wounds from booby traps, mines, andnontraditional weapons can also beencountered.
1. General
The medical threat is the composite ofall ongoing or potential enemy actionsand environmental conditions that couldreduce the effectiveness of friendly forces.These actions and conditions includewounds, injuries, or diseases. Informationto assess the medical threat caused byenemy actions should be obtained from theJ2 and J3 community.
2. Elements of the MedicalThreat
a. Infectious diseases which occurnaturally are also referred to as endemicdisease. Historically, infectious diseaseshave been responsible for more casualtiesthan battle injuries. Many naturallyoccurring infectious diseases have shortincubation periods. They may causesignificant numbers of casualties within thefirst 48 hours of a deployment or contact.Others with longer incubation periodsmay not create casualties for several weeks.Some examples of militarily significantnaturally occurring infectious diseasethreats are:
• Acute diarrheal diseases.
• Viral hepatitis.
• Japanese encephalitis.
• Scrub typhus.
• Malaria.
• Sexually transmitted diseases.
• Leishmaniasis.

A-2
Appendix A
Joint Pub 4-02
d. Biological warfare is theemployment of biological agents toproduce casualties in humans or animalsor cause damage to plants or materiel.The intentional use of these disease-causingorganisms (pathogens), toxins, or otheragents of biological origin is designed toweaken resistance to attack and reduce thewill to wage war.
• Historically, biological warfare hasprimarily involved the use ofpathogens to sabotage food andwater supplies and spreadcontagious disease amongpopulations. These pathogens havegenerally fallen into one of thefollowing categories:
•• Naturally occurring, unmodifiedinfectious agents.
•• Toxins, venoms, and theirbiologically active fractions.
•• Modified infectious agents.
•• Bioregulators and physiologicallyactive compounds.
• Biotechnology is a tool for theproduction of biological warfareagents. Naturally occurring infectiousorganisms can be made more virulent,drug resistant, and can be manipulatedto render protective vaccinesineffective. Such developments couldgreatly complicate the ability to detectand identify biological warfare agentsand the ability to operate in areascontaminated by these agents. Thecausative agents for anthrax, tularemia,plague, and cholera, as well asbotulinum toxin, staphylococcus,enterotoxin, and mycotoxin, arebelieved to have been developed asbiological warfare agents by potentialUS adversaries.
e. As a result of confirmed chemicalwarfare agent use by Iraq against Iranianforces, probable use by the former SovietUnion in Afghanistan, and reported use ofchemical agents and toxins in SoutheastAsia, there is continuing heightened interestin the use of chemical munitions anddelivery methods. Nerve and blister agentsappear to be the agents most available indeveloping countries. Agents which couldbe employed by numerous conventionalweapons system include:
• Nerve agents—VX, thickened VX, GB(sarin), thickened GD (soman).
• Vesicants (thickened lewisite and amustard and lewisite mixture).
• Choking agents (phosgene).
• Cyanogens—AC (hydrogen cyanide)and CK (cyanogen chloride).
• Riot control agents.
f. Directed-energy weapons focusradiation on a target to induce electronic,thermal, or structural and human(particularly eye) damage and can causemission failure. The radiation is composedof three types: radio frequency, laser, andcharged particle beam. There have beennumerous reports of personnel sustainingeye damage while using optic devices andbeing exposed to a bright flashing lightemanating from warships or other sources.These reports suggest an increasing threatfrom lasers to both air and a ground forces.
g. Blast effect weapons such as fuel andair explosives represent an emergingmedical threat. Gas-filled body organssuch as ears, lungs, and digestive tract arethe most susceptible to primary blast injury.This emerging threat may result in lowerlethality but a greater number of woundedand a significantly increased workload.

A-3
Medical Threat
h. Strategic mobility of US forces is amajor element of US political and militarystrategy. Alert forces may be required tooperate without rest for extended periodsof time during mobilization, staging,airborne transportation, and combatinsertion into hostile areas. Moderncombat, with its increased lethality, rapidm a n e u v e r s , t e c h n o l o g i c a l s k i l lrequirements, exposure to NBC weapons,and day or night all-weather operations, willstress personnel to their endurance limits.Under these conditions, the significance ofstress as a major contributor of casualtiescannot be overstated.
i. Flame and incendiary systemsinclude napalm and white phosphorus foraerial delivered bombs. Possible uses offlame and incendiary weapons include theclearing of difficult defensive positions suchas caves, bunkers, buildings, and soft shelteror vehicular targets. Flame has also beenused quite effectively in previous conflictsin an antitank role.
j. Until recently, the primary nuclearwarfare threat has been from the SovietUnion. However, open-source informationsuggests that other countries may developnuclear weapons capability within the nextdecade. Planners expect a minimum of 10to 20 percent casualties within a division-size force that has experienced a nuclearstrike. This percentage may be a lowestimate, since proximity to ground zerois the critical factor in determiningweapon effects on the force. In additionto casualties, a nuclear weapon detonationcan generate an electromagnetic pulse thatwill result in catastrophic failure of someelectronic equipment components.
3. The Threat to HSS Personneland Operations
a. Commanders can ant ic ipateincreased casualty densities among HSSpersonnel over those experienced in mostprevious conflicts. Medical threatelements with the greatest potential forforce degradation during combat operationsare:
• Battle injuries because of artillery,small arms, and fragmentationweapons.
• Casualties caused by combat stress.
• NBC and combined casualties.
• Premeditated attack upon medicalorganizations, personnel, or Class VIIIsupplies.
• The continually increasing range ofindirect fire weapons.
• The enhanced wounding capabilityand destructiveness of munitions andweapon systems.
• The collective effects of conventional,chemical, biological, or nuclearweapons.
• Significant increases in casualtydensities that cause local or generaloverloads of the HSS system,r e s u l t i n g i n p h y s i c a l a n dpsychological stress.
• Infectious diseases and environmentalextremes.

A-4
Appendix A
Joint Pub 4-02
b. Enemy combat operations infriendly rear areas will interdict lines ofcommunications and disrupt necessarylogistic activity. This disruption willproduce a serious negative effect on theability of personnel to retrieve andevacuate wounded, injured, and sickpersonnel and deliver health care.Although enemy combat operations maythreaten the HSS combat mission bydisrupting HSS operations or threaten thesurvival of HSS, they are not considered tobe medical threats for the purposes of thispublication.
c. Prolonged periods of intense,continuous operations will tax HSSpersonnel to the limit of their psychologicaland emotional endurance. This stress andfatigue will cause both quantitative andqualitative degradation in the ability ofthe HSS system to deliver health care ata sustained level. Proper training, such astaking vital signs, or minor surgicalprocedures of dental personnel to augmentmedical staff, may provide some temporaryrelief.
d. HSS organizations are not expected tobe the primary target for biological orchemical attacks; however, logistic basecomplexes may be prime candidates forsuch enemy operations. As elements oflogistic complexes, medical organizationsmust anticipate collateral contaminationfrom attacks on adjacent facilities.Forward HSS assets have an even higherprobability of being required to operate inor in proximity to areas contaminated bybiological and chemical weapons.
4. The Medical Threat inMilitary Operations OtherThan War
a. The medical threat is traditionallyevaluated for its impact on US forcesalone. When preparing for and
conducting operations during MOOTW,elements of the medical threat to theindigenous population must also beassessed. The impact of the medical threatas a contributing factor to social, political,and economic stability in both peace andother operational environments must beconsidered. The general environment inwhich these types of operations areconducted ranges from peaceful,developing countries with no apparentinternal or external instabilities to countrieswith limited resources and a poorly ledpopulation assailed by active insurgentmovements, diseases, and dependent onHA.
b. Within the military operations, USefforts may focus on foreign internaldefense operations such as securityassistance, HA, or HN logistic support.These operations are often conducted inareas where social services have beendisrupted, resulting in poor sanitation,inadequate food distribution, possiblelawlessness, and general civil unrest.Significant medical threats are likely tobe naturally occurring infectious diseasesand environmental extremes.
c. There are varied scenarios underwhich US forces could be employed innation assistance, disaster relief, and HAmissions involving Third World countries.In general, areas where assistance teamsand units may be employed will likelyhave a very low standard of living andhigh levels of endemic infectious diseases.Many of these diseases could be consideredexotic to most US HSS personnel. USforces serving in these areas will enterwith very little, if any, natural immunityto many endemic diseases. The degree ofcultural and social interaction required tosupport the mission, as well as the sharingof food, quarters, and recreational facilitieswith local nationals, will increase exposureof US personnel to diseases endemic to the

A-5
Medical Threat
host country. For the most part, assistanceoperations will last a relatively extendedperiod of time (past 30 days) and willincrease the exposure to and raise the riskfrom endemic disease.
d. In these environments, protectionafforded to MTF and HSS personnel bythe Geneva Conventions may not berecognized by insurgent or terroristforces. HSS activities may be perceived asprime targets by these groups, especiallyif these facilities are seen as making a majorcontribution to the HN government.Medical facilities will also be vulnerableto theft and raids on Class VIII suppliesby insurgents or terrorists for their ownsupport or to support black market activities.
e. In some situations, the in-countrycomponents of the US logistic system in
support of US assistance forces will beaustere. Often the HSS structure willrequire significant reliance on contractingfor local food, water, sanitation, publichealth, localized medical treatment, andhealth industry resources. There will beincreased reliance on tactical medicalsupport and evacuation. Coordinationwith USCINCTRANS for intertheaterpatient evacuation can be greater in theseoperations than in other war scenarios. USNavy and US Marine Corps transportationassets should be used to support all aspectsof HSS in military operations other than warscenarios, based on the availability andlocation in coastal waters. Thesecircumstances will demand solid HSSplanning. This planning must be based oncurrent, accurate medical intelligence andinclude the total involvement of the CountryTeam prior to the execution of operations.

A-6
Appendix A
Joint Pub 4-02
Intentionally Blank

APPENDIX BMEDICAL INTELLIGENCE
B-1
1. General
a. The Defense Intelligence Agency(DIA) develops and disseminates medicalintelligence. The two major intelligencecategories of primary use to the HSSplanner are general medical intelligence(DOD 6420.1R) and medical intelligence(Joint Pub 1-02). For DIA, medicalintelligence is produced by the ArmedForces Medical Intelligence Center(AFMIC), Ft. Detrick, Maryland. AFMICcurrently produces and disseminatesfinished intelligence products via studies,message traffic, and online electronicsystems.
b. DOD military medical personnelfrequently use the term “medicalintelligence” incorrectly to mean anymedical information of military importance;however, the term “medical intelligence”officially refers to finished intelligence onmedical and related matters. By thisdefinition, medical intelligence includesonly finished intelligence productsproduced by an authorized intelligenceagency such as AFMIC through theintelligence cycle. Medical intelligence isintended to provide HSS operations andplanning staffs with basic guidance forunderstanding, acquiring, using, andapplying intelligence and intelligencesystems in the conduct of HSS operations,medical threat analysis and management,threat-based concept development, medicalresearch, and doctrine development. Othersources of medical information may beused in assessing potential threats (e.g.,Naval Environmental and PVNTMEDunits, Defense Pest ManagementInformation Analysis Center, and the WorldHealth Organization).
2. Significance of MedicalIntelligence
a. Accurate and timely intelligence isa critical combat support tool forplanning, executing, and sustaining militaryoperations. It is equally important inachieving optimum planning, execution,and sustainment of HSS operations, themedical readiness of the command, and theoverall combat readiness of the unit.
b. At the operational level, intelligencefocuses on the joint campaign andoperations. At the strategic level, theobjective is to contribute to the formulationof national and senior military policy. Atthe tactical level, intelligence is orientedtoward the specific area of operations anda given operation in greater detail.Intelligence, properly used and applied,can become a powerful force multiplierby providing the critical essential elementsof information required to assist HSS staffs.
3. Sources of MedicalIntelligence
Most AFMIC products commonly usedby HSS planners fall into the category ofRecurring Finished Intelligence. Theseproducts include (but are not limited to) thefollowing:
a. Medical Capabilities. Finishedintelligence studies prepared on foreigncountries that include, but are not restrictedto, environmental health factors, diseases,civilian health services, and military healthservices. (Medical capabilities are differentfrom the Medical Civilian Action Program.)

B-2
Appendix B
Joint Pub 4-02
b. Disease Occurrence Worldwide. Amonthly intelligence summary in electronicmessage format, provided as an unclassifiedmessage, supplemented by a separateclassified message. The primary focus of theproduct is on militarily or strategicallysignificant disease occurrences and events.
c. Scientific and Technical IntelligenceStudies. Finished intelligence studiesprepared by AFMIC on militarily significantlife science issues and published anddisseminated through DIA. Examples ofgeneric topics covered include biologicalwarfare and biotechnology.
d. AFMIC Wire. A summary of currentmedical intelligence prepared and transmittedin electronic message format on a biweeklybasis to authorized consumers. AFMIC’swires are classified through the level ofSECRET collateral material.
e. AFMIC Quick Reaction Support.AFMIC can respond to time-sensitive quickreaction intelligence production andsupport requests for operationalcontingencies. Quick reaction tasking isnormally accepted by AFMIC if the require-ments of the task can be completed in amaximum of 40 personnel hours of analyticalwork. Requests are accepted telephonically(open and secure communications) and bydirect correspondence or message format.Whenever possible, formal methods ofcommunications are encouraged.
f. Communications with AFMIC
• Mailing address:
Director, Armed Forces MedicalIntelligence Center (Operations)Building 1607, Fort Detrick,Frederick, MD 21701-5004
• Message: DIRAFMIC FT DETRICKMD//OPS//
APPENDIX CREFERENCES
C-1
1. Multinational Documents
a. NATO STANAG 2068, 17 October 1991, “Emergency War Surgery Handbook(Second United States Revision).”
b. NATO STANAG 2874, 27 November 1981, “Planning Guide for the Estimation ofBattle Casualties (Nuclear) (A Med P-8).”
c. “Geneva Convention for the Amelioration of the Condition of the Wounded andSick in Armed Forces in the Field,” 1949.
d. “Geneva Convention for the Amelioration of the Condition of Wounded, Sick, andShipwrecked Members of Armed Forces at Sea,” 1949.
e. “Geneva Convention Relative to the Treatment of Prisoners of War,” 1949.
f. “Geneva Conventions for the Protection of War Victims,” 12 August 1949.
2. DOD Directives
a. DODD 6480.5, 16 June 1972, “Military Blood Program.”
b. DODD 6015.5-M, March 1989, “Glossary of Healthcare Terminology.”
3. Joint Publications
a. Joint Pub 0-2, 24 February 1995, “Unified Action Armed Forces (UNAAF).”
b. Joint Pub 1-01, Change 1, 14 September 1993, “Joint Publication System, JointDoctrine and Joint Tactics, Techniques, and Procedures Development Program.”
c. Joint Pub 1-02, 23 March 1994, “Department of Defense Dictionary of Militaryand Associated Terms.”
d. Joint Pub 3-0, 1 February 1995, “Doctrine for Joint Operations.”
e. Joint Pub 3-02, 8 October 1992, “Joint Doctrine for Amphibious Operations.”
f. Joint Pub 3-05, 28 October 1992, “Doctrine for Joint Special Operations.”
g. Joint Pub 3-05.3, 25 August 1993, “Joint Special Operations OperationalProcedures.”

C-2
Appendix C
Joint Pub 4-02
h. Joint Pub 3-50.2, 12 July 1994, “Doctrine for Joint Combat Search and Rescue(CSAR).”
i. Joint Pub 3-57, (In Development), “Doctrine for Joint Civil Affairs.”
j. Joint Pub 4-0, 22 January 1995, “Doctrine for Logistic Support of Joint Operations.”
k. Joint Pub 4-01.1, In Development, “JTTP to Airlift Support to Joint Operations.”
l. Joint Pub 4-01.3, 26 January 1994, “JTTP for Joint Movement Control.”
m. Joint Pub 4-02.1, In Development, “JTTP for Health Service Support Logistics inJoint Operations.”
n. Joint Publication 4-02.2, In Development, “JTTP for Patient Evacuation in JointOperations.”
o. Joint Pub 5-03.1, 4 August 1993, “Joint Operation Planning and Execution System(JOPES), Volume I (Planning Policies and Procedures).”
p. Joint Pub 5-03.2, 10 March 1992, “Joint Operation Planning and Execution System(JOPES), Volume II, (Planning and Execution Formats and Guidance).”
q. Joint Pub 5-03.3 (In Development), “Joint Operation Planning and Execution(JOPES), Volume III, (ADP Support).”
r. CM-1502-92, 23 November 1992, “A Doctrinal Statement of Selected JointOperational Concepts.”
s. USACOM CONPLAN 2730-YR, “Integrated CONUS Medical Operations Plan.”
4. Multi-Service Publications
a. AFR 1687-11/AR40-350/BUMEDINST 6320.1E/(PHS) CCPM 60/COMDTINSTM6320.8B/NOAAR 56.52C, 30 March 1990, “Patient Regulating To and Within theContinental United States.”
b. AR 10-64/OPNAVINST 6700.2/AFR 16020/MCO 5420.18A, 16 August 1988,“Organizations and Functions—Joint Field Operating Functions of the Office of TheSurgeon General of the Army.”
c. FM 8-285/Navy NAVMED P5041/Air Force AFM 160-11, 28 February 1990,“Treatment of Chemical Agent Casualties and Conventional Military Chemical Injuries.”
d. TB MED 81/NAVMED P-5052-29/AFP 161-11, 30 September 1976, “Cold Injury.”

C-3
References
5. Army Publications
a. FM 8-10, 1 March 1991, “Health Service Support in a Theater of Operations.”
b. FM 8-55, 15 February 1985, “Planning for Health Service Support.”
c. FM 21-10, 22 November 1988, “Field Hygiene and Sanitation.”
d. FM 101-10-1/1, 7 October 1987, “Staff Officers Field Manual—Organizational,Technical, and Logistical Data (Volume I).”
e. FM 101-10-1/2, 7 October 1987, “Staff Officers Field Manual—Organizational,Technical, and Logistical Data, Planning Factors (Volume II).”
6. Navy and Marine Corps Publications
a. Naval Warfare Publication (NWP) 6 (REV C), March 1989, “Operational Medicaland Dental Support.”
b. BUMED 6440.5A, 19 April 1994, “Medical Augmentation Program.”
c. FMFM 4-50, 19 September 1990, “Health Service Support.”
d. OPNAVINST S3060.1 (RESTRICTED), “Navy Capabilities and MobilizationPlan.”
7. Air Force Publications
a. AFR 8-5, September 1983, “United States Air Force Foreign Clearance Guide.”
b. AFR 28-3, June 1986, “USAF Operations Planning Process.”
c. AFR 28-40, November 1991, “Mobility for Tactical Air and Strategic AerospaceDefense Forces.”
d. AFR 28-42, June 1986, “Mobility for Military Airlift Command Forces.”
e. AFR 160-15, August 1991, “Medical Support at Remote Sites.”
f. AFR 164-5, December 1975, “Worldwide Aeromedical Evacuation.”
g. AFR 168-4, April 1990, “Administration of Medical Activities.”
h. AFP 160-98, February 1991, “Air Force Medical Service Guidance for Wartimeand Peacetime Contingency Operations.”
i. USAF War and Mobilization Plan (WMP-1), Volume I, “Medical Service,” AnnexF, May 1988.

C-4
Appendix C
Joint Pub 4-02
Intentionally Blank

APPENDIX DADMINISTRATIVE INSTRUCTIONS
D-1
1. User Comments
Users in the field are highly encouraged to submit comments on this publication to theJoint Warfighting Center, Attn: Doctrine Division, Fenwick Road, Bldg 96, Fort Monroe,VA 23651-5000. These comments should address content (accuracy, usefulness,consistency, and organization), writing, and appearance.
2. Authorship
The lead agent for this publication is the US Army. The Joint Staff doctrine sponsorfor this publication is the Director for Logistics (J-4).
3. Change Recommendations
a. Recommendations for urgent changes to this publication should be submitted:
TO: HQDA WASHINGTON DC//DASG-HCD-D//FROM: JOINT STAFF WASHINGTON DC//J7-JDD//
Routine changes should be submitted to the Director for Operational Plans andInteroperability (J-7), JDD, 7000 Joint Staff Pentagon, Washington, D.C. 20318-7000.
b. When a Joint Staff directorate submits a proposal to the Chairman of the JointChiefs of Staff that would change source document information reflected in thispublication, that directorate will include a proposed change to this publication as anenclosure to its proposal. The Military Services and other organizations are requestedto notify the Director, J-7, Joint Staff, when changes to source documents reflected inthis publication are initiated.
c. Record of Changes
CHANGE COPY DATE OF DATE POSTEDNUMBER NUMBER CHANGE ENTERED BY REMARKS__________________________________________________________________________________________________________________________________________________________________________________________________________________

D-2
Appendix D
Joint Pub 4-02
4. Distribution
a. Additional copies of this publication can be obtained through Service publicationcenters.
b. Only approved pubs and test pubs are releasable outside the combatant commands,Services, and Joint Staff. Release of any joint publication to foreign governments orforeign nationals must be requested through the local embassy (Defense Attache Office)to DIA Foreign Liaison Branch, C-AS1, Room 1A674, Pentagon, Washington D.C.20301-7400.
c. Additional copies should be obtained from the Military Service assignedadministrative support responsibility by DOD Directive 5100.3, 1 November 1988,“Support of the Headquarters of Unified, Specified, and Subordinate Joint Commands.”
By Military Services:
Army: US Army AG Publication Center2800 Eastern BoulevardBaltimore, MD 21220-2898
Air Force: Air Force Publications Distribution Center2800 Eastern BoulevardBaltimore, MD 21220-2896
Navy: CO, Navy Aviation Supply OfficeDistribution Division (Code 03443)5801 Tabor AvenuePhiladelphia, PA 19120-5000
Marine Corps: Marine Corps Logistics BaseAlbany, GA 31704-5000
Coast Guard: Coast Guard Headquarters, COMDT (G-REP)2100 2nd Street, SWWashington, D.C. 20593-0001
d. Local reproduction is authorized and access to unclassified publications isunrestricted. However, access to and reproduction authorization for classified jointpublications must be in accordance with DOD Regulation 5200.1-R.

GLOSSARYPART I—ABBREVIATIONS AND ACRONYMS
GL-1
AE aeromedical evacuationAECC aeromedical evacuation coordination centerAFMIC Armed Forces Medical Intelligence CenterAFSOF Air Force special operations forcesAJBPO area joint blood program officeARSOF Army special operations forcesASBPO Armed Services Blood Program OfficeASWBPL Armed Services Whole Blood Products Laboratory
BDC Blood Distribution CenterBLDREP blood reportBPD Blood Product DepotBSU blood supply unitBTC blood transshipment center
C2 command and controlC4 command, control, communications, and computer systemsCINC Commander in ChiefCONUS continental United StatesCSAR combat search and rescue
DIA Defense Intelligence Agency
EMT emergency medical treatmentEPW enemy prisoner of war
FEMA Federal Emergency Management Agency
GPMRC Global Patient Movement Requirements Center
HA humanitarian assistanceHCA humanitarian and civic assistanceHN host nationHSS health service support
JBPO joint blood program officeJFC joint force commanderJFS joint force surgeonJOPES Joint Operation Planning and Execution System
MASCAL mass casualtyMOOTW military operations other than warMPM Medical Planning ModuleMTF medical treatment facility
GL-2
Glossary
Joint Pub 4-02
NBC nuclear, biological, and chemicalOPLAN operation planOPORD operation orderOPSEC operations security
PMI patient movement itemPOW prisoner of warPVNTMED preventive medicine
RP retained personnelRTD return to duty
SBPO Service Blood Program OfficeSEAL sea-air-land (US Navy)SIMLM single integrated medical logistics managementSOC special operations commandSOF special operations forcesSOFME special operations forces medical elements
TBTC Transportable Blood Transshipment CenterTPMRC Theater Patient Movement Requirements CenterTRAC2ES TRANSCOMs’ Regulating and Command and Control
Evacuation System
USACOM United States Atlantic CommandUSCINCTRANS Commander in Chief, US Transportation Command

GL-3
Glossary
aeromedical evacuation. The movementof patients under medical supervision toand between medical treatment facilitiesby air transportation. (Joint Pub 1-02)
casualty. Any person who is lost to theorganization by having been declareddead, duty status-whereabouts unknown,missing, ill, or injured. (Joint Pub 1-02)
casualty category. A term used tospecifically classify a casualty forreporting purposes based upon thecasualty type and the casualty status.Casualty categories include killed inaction, died of wounds received in action,and wounded in action. (Joint Pub 1-02)
casualty status. A term used to classify acasualty for reporting purposes. Thereare seven casualty statuses: (1) deceased,(2) duty status—whereabouts unknown,(3) missing, (4) very seriously ill orinjured, (5) seriously ill or injured, (6)incapacitating illness or injury, and (7)not seriously injured. (Joint Pub 1-02)
casualty type. A term used to identify acasualty for reporting purposes as eithera hostile casualty or a nonhostile casualty.(Joint Pub 1-02)
combatant command. A unified orspecified command with a broadcontinuing mission under a singlecommander established and so designatedby the President, through the Secretaryof Defense and with the advice andassistance of the Chairman of the JointChiefs of Staff. Combatant commandstypically have geographic or functionalresponsibilities. (Joint Pub 1-02)
combat service support. The essentialcapabilities, functions, activities, and
tasks necessary to sustain all elements ofoperating forces in theater at all levels ofwar. Within the national and theaterlogistic systems, it includes but is notlimited to the support rendered by serviceforces in ensuring the aspects of supply,maintenance, transportation, healthservices, and other services required byaviation and ground combat troops topermit those units to accomplish theirmissions in combat. Combat servicesupport encompasses those activities atall levels of war that produce sustainmentto all operating forces on the battlefield.(Joint Pub 1-02)
combat zone. 1. That area required bycombat forces for the conduct ofoperations. (Joint Pub 1-02)
command and control. The exercise ofauthority and direction by a properlydesignated commander over assigned andattached forces in the accomplishment ofthe mission. Command and controlfunctions are performed through anarrangement of personnel, equipment,communications, facilities, andprocedures employed by a commander inplanning, directing, coordinating, andcontrolling forces and operations in theaccomplishment of the mission. (JointPub 1-02)
communications zone. Rear part of theaterof operations (behind but contiguous tothe combat zone) which contains the linesof communications, establishments forsupply and evacuation, and otheragencies required for immediate supportand maintenance of the field forces.(Joint Pub 1-02)
directed energy. An umbrella termcovering technologies that relate to the
PART II—TERMS AND DEFINITIONS

GL-4
Glossary
Joint Pub 4-02
production of a beam of concentratedelectromagnetic energy or atomic orsubatomic particles. Also called DE.(Joint Pub 1-02)
disease and nonbattle injury casualty. Aperson who is not a battle casualty butwho is lost to the organization by reasonof disease or injury, including personsdying of disease or injury, by reason ofbeing missing where the absence does notappear to be voluntary, or due to enemyaction or to being interned. (Approvedfor inclusion in the next edition of JointPub 1-02)
evacuation. 1. The process of moving anyperson who is wounded, injured, or ill toand/or between medical treatmentfacilities. (Joint Pub 1-02)
evacuation policy. 1. Command decision,indicating the length in days of themaximum period of noneffectiveness thatpatients may be held within the commandfor treatment. Patients who, in theopinion of responsible medical officers,cannot be returned to duty status withinthe period prescribed are evacuated by thefirst available means, provided the travelinvolved will not aggravate theirdisabilities. (Joint Pub 1-02)
foreign internal defense. Participation bycivilian and military agencies of agovernment in any of the action programstaken by another government to free andprotect its society from subversion,lawlessness, and insurgency. Also calledFID. (Joint Pub 1-02)
Global Patient Movement RequirementsCenter. A joint activity reportingdirectly to the Commander in Chief, USTransportation Command, the DODsingle manager for the regulation ofmovement of uniformed servicespatients. The GPMRC authorizes
transfers to medical treatment facilitiesof the Military Departments or theDepartment of Veterans Affairs andcoordinates intertheater and insideCONUS patient movement requirementswith the appropriate transportationcomponent commands of USTransportation Command. (Approvedfor inclusion in the next edition of JointPub 1-02)
health service support. All servicesperformed, provided, or arranged by theServices to promote, improve, conserve,or restore the mental or physical well-being of personnel. These servicesinclude, but are not limited to, themanagement of health services resources,such as manpower, monies, and facilities;preventive and curative health measures;evacuation of the wounded, injured, orsick; selection of the medically fit anddisposition of the medically unfit; bloodmanagement; medical supply, equipment,and maintenance thereof; combat stresscontrol; and medical, dental, veterinary,laboratory, optometric, medical food, andmedical intelligence services. (Approvedfor inclusion in the next edition of JointPub 1-02)
hostile casualty. A person who is thevictim of a terrorist activity or whobecomes a casualty “in action.” “Inaction” characterizes the casualty ashaving been the direct result of hostileaction, sustained in combat or relatingthereto, or sustained going to or returningfrom a combat mission provided that theoccurrence was directly related to hostileaction. Included are persons killed orwounded mistakenly or accidentally byfriendly fire directed at a hostile force orwhat is thought to be a hostile force.However, not to be considered assustained in action and not to beinterpreted as hostile casualties areinjuries or death due to the elements, self-
GL-5
Glossary
inflicted wounds, combat fatigue, andexcept in unusual cases, wounds or deathinflicted by a friendly force while theindividual is in an absent-without-leave,deserter, or dropped-from-rolls status oris voluntarily absent from a place of duty.(Joint Pub 1-02)
host-nation support. Civil and/or militaryassistance rendered by a nation to foreignforces within its territory duringpeacetime, crisis or emergencies, or warbased upon agreements mutuallyconcluded between nations. (Joint Pub1-02)
intertheater evacuation. Evacuation ofpatients between the originating theaterand points outside the theater, to includethe continental United States and othertheaters. En route care is provided bytrained medical personnel. (Approved forinclusion in the next edition of Joint Pub1-02)
intratheater evacuation. Evacuation ofpatients between points within the theater.En route care is provided by trainedmedical personnel. (Approved forinclusion in the next edition of Joint Pub1-02)
joint force. A general term applied to aforce composed of significant elements,assigned or attached, of two or moreMilitary Departments, operating under asingle commander authorized to exerciseoperational control. (Joint Pub 1-02)
joint force commander. A general termapplied to a combatant commander,subunified commander, or joint task forcecommander authorized to exercisecombatant command (commandauthority) or operational control over ajoint force. Also called JFC. (Joint Pub1-02)
joint force surgeon. A general termapplied to an individual appointed by thejoint force commander to serve as thetheater or joint task force special staffofficer responsible for establishing,monitoring, or evaluating joint forcehealth service support. (Approved forinclusion in the next edition of Joint Pub1-02)
medical intelligence. That category ofintelligence resulting from collection,evaluation, analysis, and interpretation offoreign medical, bio-scientific, andenvironmental information which is ofinterest to strategic planning and tomilitary medical planning and operationsfor the conservation of the fightingstrength of friendly forces and theformation of assessments of foreignmedical capabilities in both military andcivilian sectors. (Joint Pub 1-02)
medical regulating. The actions andcoordination necessary to arrange for themovement of patients through theechelons of care. This process matchespatients with a medical treatment facilitythat has the necessary health servicesupport capabilities, and it also ensuresthat bed space is available. (Approved forinclusion in the next edition of Joint Pub1-02)
medical threat. A collective term used todesignate all potential or continuingenemy actions and environmentalsituations that could possibly adverselyaffect the combat effectiveness of friendlyforces, to include wounding, injuries, orsickness incurred while engaged in a jointoperation. (Approved for inclusion in thenext edition of Joint Pub 1-02)
medical treatment facility. A facilityestablished for the purpose of furnishingmedical and/or dental care to eligibleindividuals. (Joint Pub 1-02)

GL-6
Glossary
Joint Pub 4-02
National Command Authorities. ThePresident and the Secretary of Defenseor their duly deputized alternates orsuccessors. Also called NCA. (Joint Pub1-02)
nonhostile casualty. A person whobecomes a casualty due to circumstancesnot directly attributable to hostile actionor terrorist activity. Casualties due tothe elements, self-inflicted wounds, andcombat fatigue are nonhostile casualties.(Joint Pub 1-02)

Assess-ments/
Revision
CJCSApproval
TwoDrafts
ProgramDirective
ProjectProposal
J-7 formally staffs withServices and CINCS
Includes scope of project,references, milestones,and who will developdrafts
J-7 releases ProgramDirective to Lead Agent.Lead Agent can beService, CINC, or JointStaff (JS) Directorate
STEP #2Program Directive
l
l
l
The CINCS receive the pub andbegin to assess it during use
18 to 24 months followingpublication, the Director J-7, willsolicit a written report from thecombatant commands andServices on the utility and qualityof each pub and the need for anyurgent changes or earlier-than-scheduled revisions
No later than 5 years afterdevelopment, each pub is revised
STEP #5Assessments/Revision
l
l
l
Submitted by Services, CINCS, or Joint Staffto fill extant operational void
J-7 validates requirement with Services andCINCs
J-7 initiates Program Directive
l
l
l
STEP #1Project Proposal
All joint doctrine and tactics, techniques, and procedures are organized into a comprehensive hierarchyas shown in the chart above. is in the series of joint doctrine publications.The diagram below illustrates an overview of the development process:
Joint Pub 4-02 Logistics
JOINT DOCTRINE PUBLICATIONS HIERARCHY
JOINT PUB 1-0 JOINT PUB 3-0 JOINT PUB 5-0 JOINT PUB 6-0
JOINT PUB 0-2
JOINT PUB 1
UNAAF
JOINTWARFARE
JOINTDOCTRINE
PUBLICATION
Lead Agent forwards proposed pub to Joint Staff
Joint Staff takes responsibility for pub, makesrequired changes and prepares pub forcoordination with Services and CINCS
Joint Staff conducts formalstaffing for approval as a Joint Publication
STEP #4CJCS Approval
l
l
l
Lead Agent selects Primary Review Authority(PRA) to develop the pub
PRA develops two draft pubs
PRA staffs each draft with CINCS, Services,and Joint Staff
l
l
l
STEP #3Two Drafts
ENHANCEDJOINT
WARFIGHTINGCAPABILITY
JOINT PUB 2-0 JOINT PUB 4-0
C4 SYSTEMSPLANSLOGISTICSOPERATIONSINTELLIGENCEPERSONNEL
andADMINISTRATION






























