Embed Size (px)
Citation preview
629
Alimentary tract duplications have been described for hun-dreds of years, and multiple terms have been used in the literature. The term duplication of the alimentary tract was coined by William Ladd in 1937.1 He described three com-mon findings: a well-developed smooth muscle coat, an epithelial lining, and attachment to the alimentary tract. In 1952 Gross et al. reported the first large series describ-ing 67 patients with these findings.2 These duplications are relatively rare congenital anomalies found anywhere from the mouth to the anus with an incidence reported to be 1 in 4500 births.3 Presentation is variable, and resection is usu-ally recommended in order to prevent worsening symptoms or malignant transformation.
Embryology
Alimentary tract duplications take many forms, and one unifying embryologic theory is unlikely to encompass all variations. The associated findings of vertebral, spinal cord, and genitourinary (GU) malformations, as well as malrota-tion and intestinal atresia, suggest a multifactorial process in their development.2,4,5 There are five prevailing theo-ries: partial twinning, split notochord, diverticular defects, canalization defects, and environmental factors. The par-tial twinning theory states that organs can be doubled as a result of partial twinning. This theory may be pertinent in hindgut duplications associated with GU tract duplica-tions.6,7 The split notochord theory centers around noto-chord separation in the first month of gestation. This theory postulates that gaps in the notochord develop and allow gut endoderm to herniate and form diverticula. This theory could account for the association of duplications with spi-nal defects.8–10 A persistent embryonic diverticulum from the gastrointestinal (GI) tract was the first theory described in the literature, and a defect in lumen canalization was proposed years later. The theory of defective canalization is based on the finding that GI organs begin as solid tubes and vacuolate to form lumens. During this process, diverticula form but regress during fetal life. If they persist, duplications could form.11,12 Finally, environmental factors including hypoxia, vascular accidents, and trauma have been impli-cated in the development of these anomalies.13,14
Clinical Presentation and Diagnosis
GI duplications are found incidentally, or they can mani-fest with a wide range of symptoms, including abdominal
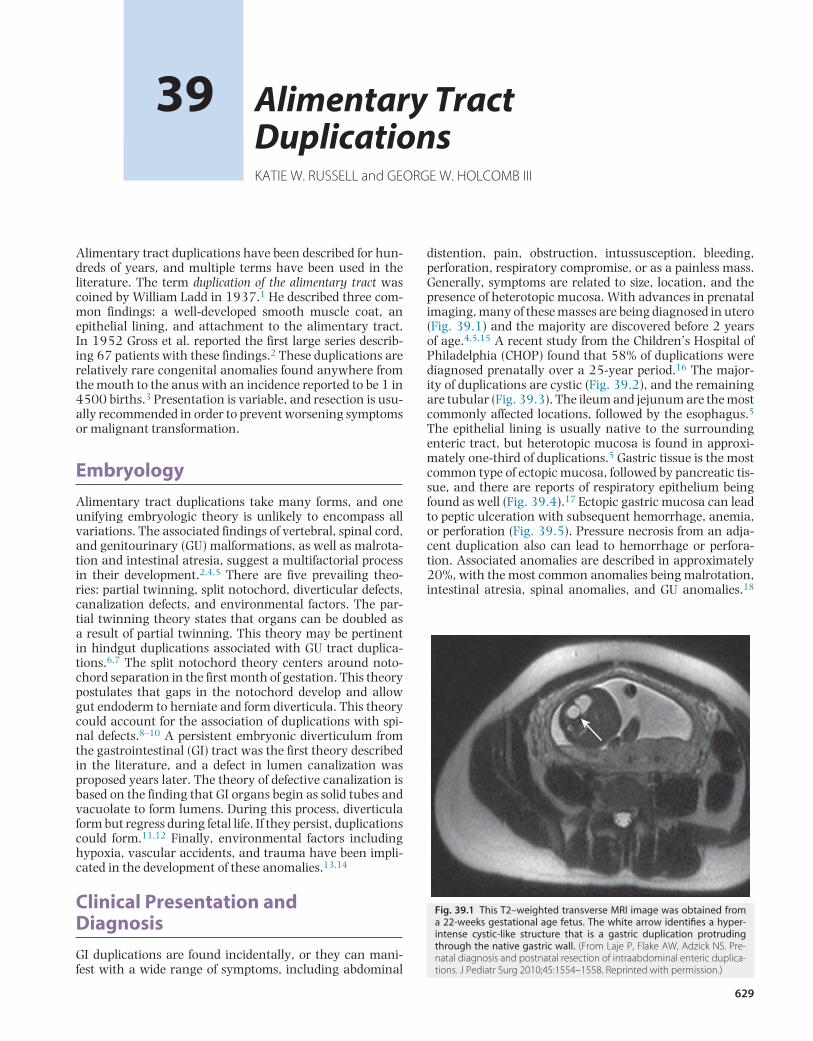
distention, pain, obstruction, intussusception, bleeding, perforation, respiratory compromise, or as a painless mass. Generally, symptoms are related to size, location, and the presence of heterotopic mucosa. With advances in prenatal imaging, many of these masses are being diagnosed in utero (Fig. 39.1) and the majority are discovered before 2 years of age.4,5,15 A recent study from the Children’s Hospital of Philadelphia (CHOP) found that 58% of duplications were diagnosed prenatally over a 25-year period.16 The major-ity of duplications are cystic (Fig. 39.2), and the remaining are tubular (Fig. 39.3). The ileum and jejunum are the most commonly affected locations, followed by the esophagus.5 The epithelial lining is usually native to the surrounding enteric tract, but heterotopic mucosa is found in approxi-mately one-third of duplications.5 Gastric tissue is the most common type of ectopic mucosa, followed by pancreatic tis-sue, and there are reports of respiratory epithelium being found as well (Fig. 39.4).17 Ectopic gastric mucosa can lead to peptic ulceration with subsequent hemorrhage, anemia, or perforation (Fig. 39.5). Pressure necrosis from an adja-cent duplication also can lead to hemorrhage or perfora-tion. Associated anomalies are described in approximately 20%, with the most common anomalies being malrotation, intestinal atresia, spinal anomalies, and GU anomalies.18
Alimentary Tract DuplicationsKATIE W. RUSSELL and GEORGE W. HOLCOMB III
39
Fig. 39.1 This T2–weighted transverse MRI image was obtained from a 22-weeks gestational age fetus. The white arrow identifies a hyper-intense cystic-like structure that is a gastric duplication protruding through the native gastric wall. (From Laje P, Flake AW, Adzick NS. Pre-natal diagnosis and postnatal resection of intraabdominal enteric duplica-tions. J Pediatr Surg 2010;45:1554–1558. Reprinted with permission.)
Holcomb and Ashcraft’s Pediatric Surgery630
Although duplications are benign, the potential for malig-nant degeneration remains a concern.19–21
Multiple imaging modalities are utilized to make the diagnosis. Prenatal ultrasound (US) can be followed with US postnatally, which may be sufficient, especially for dis-tal small bowel lesions. The typical sonographic appear-ance of a duplication (the double wall sign) demonstrates a cystic rim of hyperechoic serosa and an inner hyper-echoic rim of mucosa and submucosa with a hypoechoic muscular layer sandwiched between the two hyperechoic layers (Fig. 39.6).22 For foregut lesions, more information in the form of computed tomography (CT) or magnetic resonance imaging (MRI) may prove valuable in operative planning.23 Plain radiographs may reveal a mediastinal
mass, which requires further workup with either CT or MRI. Contrast studies may show a mass effect or com-munication with the alimentary tract and can help with the diagnosis, particularly in hindgut and foregut lesions. Technetium-99m scintigraphy may be used as adjuvant imaging but is likely unnecessary in most cases.24,25 The presence of a vertebral abnormality and a duplication is best investigated with MRI to evaluate communication with the spinal canal.26
Classification and Treatment by Location
To better understand the wide presentation and surgical treatment of duplications, they are best discussed accord-ing to anatomic location. A compilation of major case series reported in the last 75 years from 23 different institutions is seen in Table 39.1.2,4,5,16,18,27–44 The goal of operative management is to remove the duplication, but the surgi-cal procedure should not be more radical than necessary to eliminate the patient’s complaints and prevent recurrence. Simple cyst resection without violating the native GI tract is one option, but because most share a common blood sup-ply to the native alimentary tract, resection with primary anastomosis is often needed and curative, depending on the location.
In the recent CHOP 25-year review, bowel resection was required in 34% of the cases.16 Long tubular, thoracoab-dominal, and gastroduodenal duplications may present a more difficult challenge as resection can carry significant morbidity. Partial excision with mucosal stripping may be the best option in these situations. Overall prognosis is favorable, but associated malformations, location, and pre-senting illness can factor into the final outcome.
ESOPHAGEAL DUPLICATIONS
Approximately 16% of duplications arise from the esopha-gus (see Table 39.1). Although cervical and abdominal esophageal duplications occur, the majority are located along the thoracic esophagus and in the right chest. Most are cystic and share a muscular wall with the esophagus but do not communicate with the lumen. Clinical presenta-tion will depend on whether there is a mass effect. Esopha-geal compression can lead to dysphagia or regurgitation while respiratory symptoms such as cough or pneumonia can result from airway or lung compression. Almost 40% of esophageal duplications contain ectopic gastric mucosa (Table 39.2), so peptic ulceration leading to anemia or hematemesis can be seen, albeit rare. Esophageal dupli-cations also can have respiratory epithelium or primitive lung tissue associated with the lesion (Fig. 39.7). Despite the wide range of potential clinical manifestations, esopha-geal duplications are most commonly asymptomatic and diagnosed incidentally either prenatally or during workup for an unrelated problem such as a respiratory infection or trauma. Duplications should be included in the differential diagnosis for any patient presenting with a posterior medi-astinal mass.
Once a duplication is suspected, axial imaging with either CT or MRI is helpful (Fig. 39.8). When a thoracic duplication
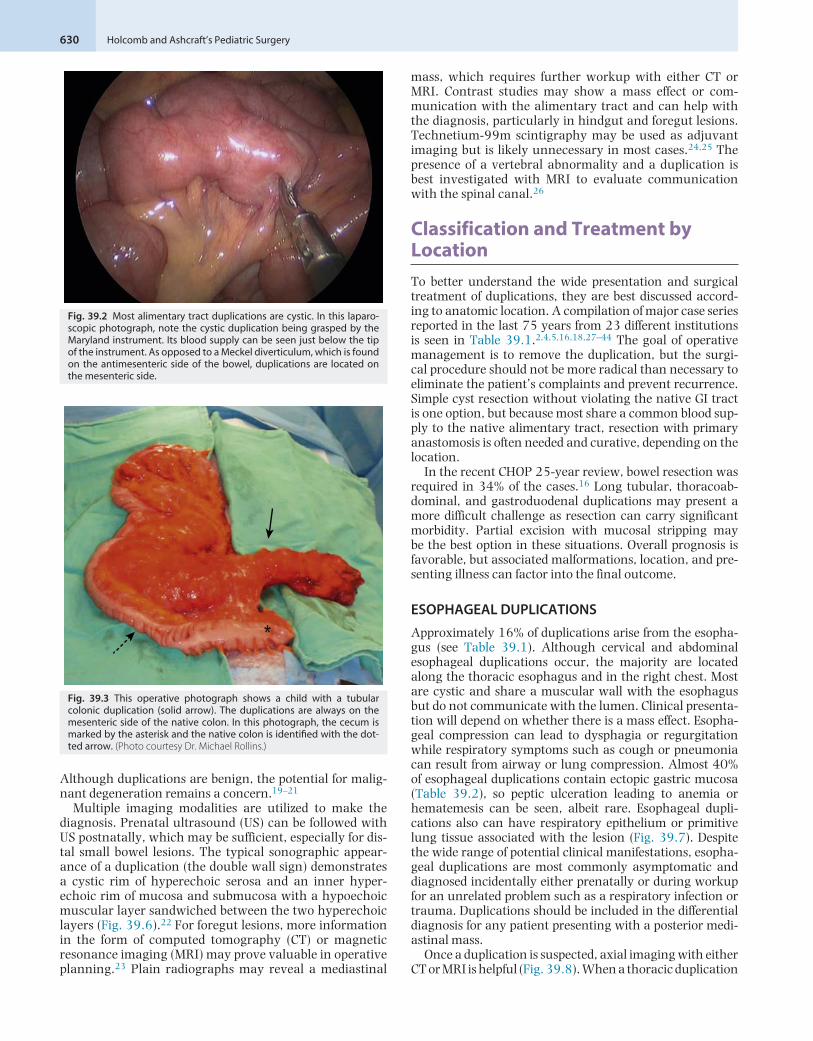
Fig. 39.2 Most alimentary tract duplications are cystic. In this laparo-scopic photograph, note the cystic duplication being grasped by the Maryland instrument. Its blood supply can be seen just below the tip of the instrument. As opposed to a Meckel diverticulum, which is found on the antimesenteric side of the bowel, duplications are located on the mesenteric side.
*
Fig. 39.3 This operative photograph shows a child with a tubular colonic duplication (solid arrow). The duplications are always on the mesenteric side of the native colon. In this photograph, the cecum is marked by the asterisk and the native colon is identified with the dot-ted arrow. (Photo courtesy Dr. Michael Rollins.)
39 • Alimentary Tract Duplications 631
is identified, some advocate for US of the abdomen to eval-uate for synchronous abdominal duplications as a 25% incidence has been described.5 US is efficient, inexpensive, and has little risk to the patient. Esophageal duplications should be removed because of the risk of malignancy and the risk that they will become symptomatic at some point. With the increased use of thoracoscopy, many esophageal duplications are being resected with a minimally invasive approach rather than traditional thoracotomy.45,46 Typi-cally they can be removed by carefully creating a cleav-age plane within the muscular wall that is shared with the native esophagus. As with any chest operation, care must be taken to avoid injury to adjacent structures, including the phrenic and vagus nerves. If there is any concern for esophageal violation, a postoperative esophagram should be done to evaluate for leak.
THORACOABDOMINAL DUPLICATIONS
Extension of an esophageal duplication into the abdomen is known as a thoracoabdominal duplication. These are quite rare and account for approximately 2% of all duplications (see Table 39.1). Typically, they originate in the right chest and at least half communicate with the intestinal tract distally, most commonly at the level of the jejunum.4,5,47 Similar to esophageal duplications, presentation is variable. These duplications are tubular, and ectopic gastric mucosa is found in a high percentage. These patients also have a high incidence of vertebral anomalies (88%) (Fig. 39.9),
A B
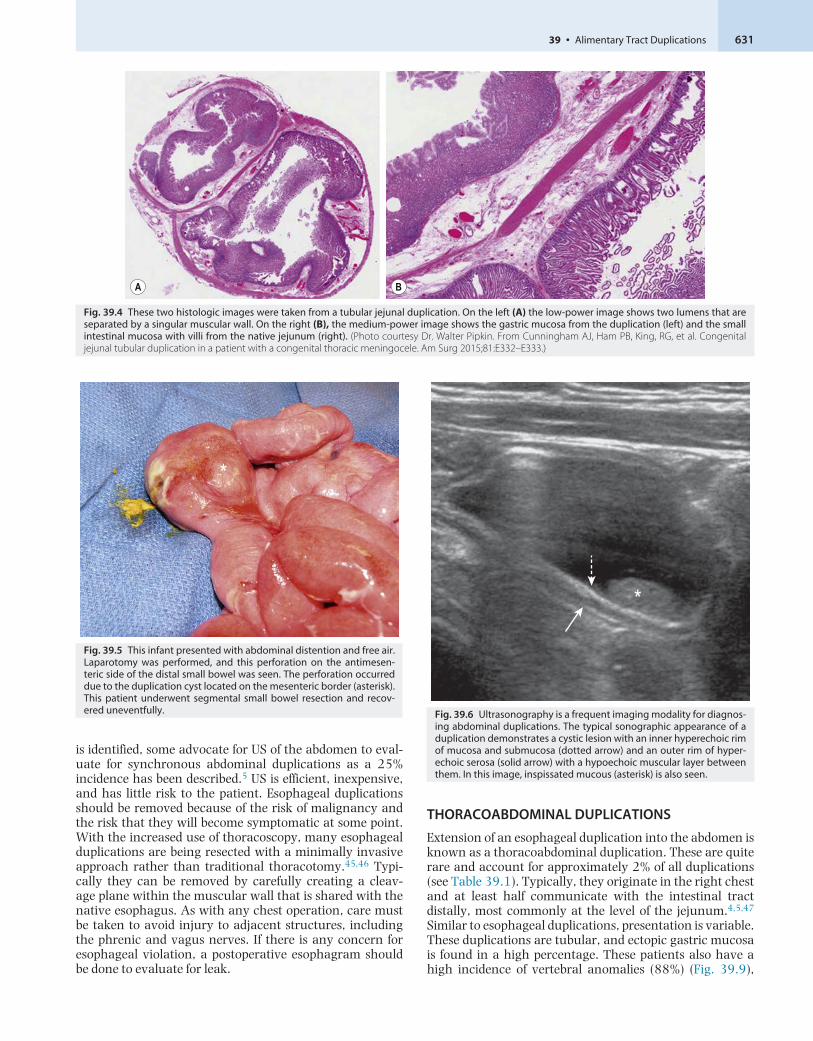
Fig. 39.4 These two histologic images were taken from a tubular jejunal duplication. On the left (A) the low-power image shows two lumens that are separated by a singular muscular wall. On the right (B), the medium-power image shows the gastric mucosa from the duplication (left) and the small intestinal mucosa with villi from the native jejunum (right). (Photo courtesy Dr. Walter Pipkin. From Cunningham AJ, Ham PB, King, RG, et al. Congenital jejunal tubular duplication in a patient with a congenital thoracic meningocele. Am Surg 2015;81:E332–E333.)
*
Fig. 39.5 This infant presented with abdominal distention and free air. Laparotomy was performed, and this perforation on the antimesen-teric side of the distal small bowel was seen. The perforation occurred due to the duplication cyst located on the mesenteric border (asterisk). This patient underwent segmental small bowel resection and recov-ered uneventfully.
*
Fig. 39.6 Ultrasonography is a frequent imaging modality for diagnos-ing abdominal duplications. The typical sonographic appearance of a duplication demonstrates a cystic lesion with an inner hyperechoic rim of mucosa and submucosa (dotted arrow) and an outer rim of hyper-echoic serosa (solid arrow) with a hypoechoic muscular layer between them. In this image, inspissated mucous (asterisk) is also seen.
Holcomb and Ashcraft’s Pediatric Surgery632
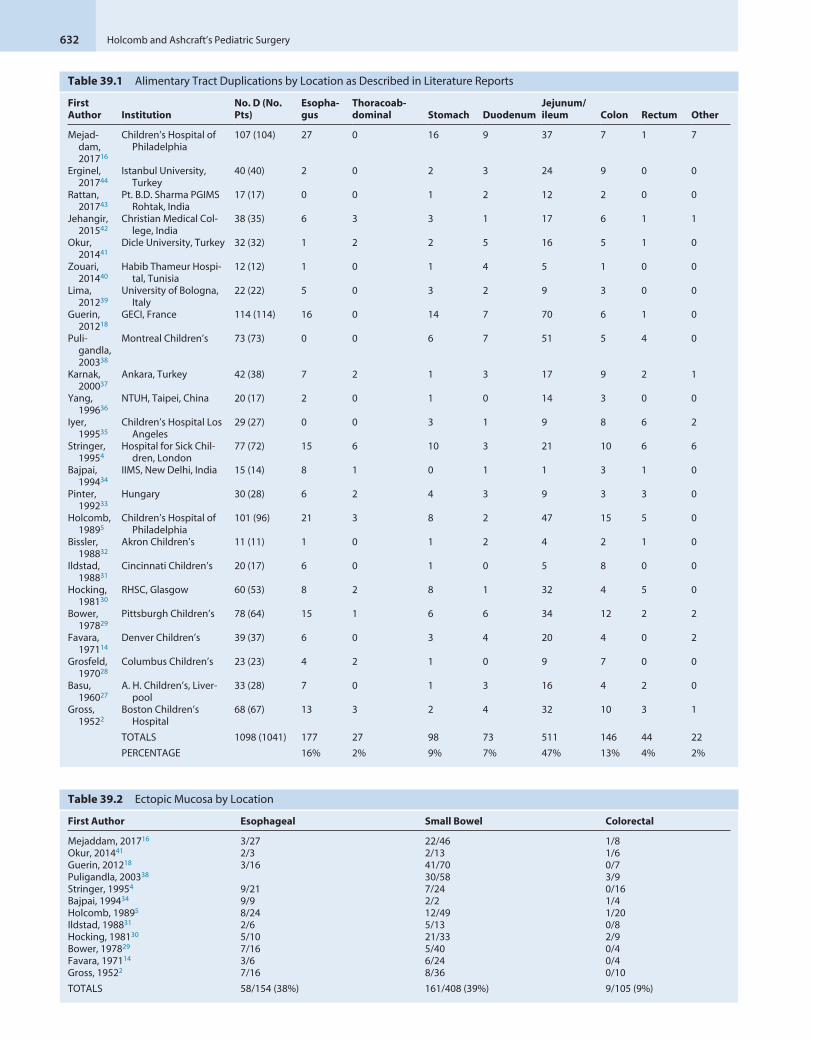
Table 39.1 Alimentary Tract Duplications by Location as Described in Literature Reports
First Author Institution
No. D (No. Pts)
Esopha-gus
Thoracoab-dominal Stomach Duodenum
Jejunum/ileum Colon Rectum Other
Mejad-dam, 201716
Children’s Hospital of Philadelphia
107 (104) 27 0 16 9 37 7 1 7
Erginel, 201744
Istanbul University, Turkey
40 (40) 2 0 2 3 24 9 0 0
Rattan, 201743
Pt. B.D. Sharma PGIMS Rohtak, India
17 (17) 0 0 1 2 12 2 0 0
Jehangir, 201542
Christian Medical Col-lege, India
38 (35) 6 3 3 1 17 6 1 1
Okur, 201441
Dicle University, Turkey 32 (32) 1 2 2 5 16 5 1 0
Zouari, 201440
Habib Thameur Hospi-tal, Tunisia
12 (12) 1 0 1 4 5 1 0 0
Lima, 201239
University of Bologna, Italy
22 (22) 5 0 3 2 9 3 0 0
Guerin, 201218
GECI, France 114 (114) 16 0 14 7 70 6 1 0
Puli-gandla, 200338
Montreal Children’s 73 (73) 0 0 6 7 51 5 4 0
Karnak, 200037
Ankara, Turkey 42 (38) 7 2 1 3 17 9 2 1
Yang, 199636
NTUH, Taipei, China 20 (17) 2 0 1 0 14 3 0 0
Iyer, 199535
Children’s Hospital Los Angeles
29 (27) 0 0 3 1 9 8 6 2
Stringer, 19954
Hospital for Sick Chil-dren, London
77 (72) 15 6 10 3 21 10 6 6
Bajpai, 199434
IIMS, New Delhi, India 15 (14) 8 1 0 1 1 3 1 0
Pinter, 199233
Hungary 30 (28) 6 2 4 3 9 3 3 0
Holcomb, 19895
Children’s Hospital of Philadelphia
101 (96) 21 3 8 2 47 15 5 0
Bissler, 198832
Akron Children’s 11 (11) 1 0 1 2 4 2 1 0
Ildstad, 198831
Cincinnati Children’s 20 (17) 6 0 1 0 5 8 0 0
Hocking, 198130
RHSC, Glasgow 60 (53) 8 2 8 1 32 4 5 0
Bower, 197829
Pittsburgh Children’s 78 (64) 15 1 6 6 34 12 2 2
Favara, 197114
Denver Children’s 39 (37) 6 0 3 4 20 4 0 2
Grosfeld, 197028
Columbus Children’s 23 (23) 4 2 1 0 9 7 0 0
Basu, 196027
A. H. Children’s, Liver-pool
33 (28) 7 0 1 3 16 4 2 0
Gross, 19522
Boston Children’s Hospital
68 (67) 13 3 2 4 32 10 3 1
TOTALS 1098 (1041) 177 27 98 73 511 146 44 22
PERCENTAGE 16% 2% 9% 7% 47% 13% 4% 2%
Table 39.2 Ectopic Mucosa by Location
First Author Esophageal Small Bowel Colorectal
Mejaddam, 201716 3/27 22/46 1/8Okur, 201441 2/3 2/13 1/6Guerin, 201218 3/16 41/70 0/7Puligandla, 200338 30/58 3/9Stringer, 19954 9/21 7/24 0/16Bajpai, 199434 9/9 2/2 1/4Holcomb, 19895 8/24 12/49 1/20Ildstad, 198831 2/6 5/13 0/8Hocking, 198130 5/10 21/33 2/9Bower, 197829 7/16 5/40 0/4Favara, 197114 3/6 6/24 0/4Gross, 19522 7/16 8/36 0/10
TOTALS 58/154 (38%) 161/408 (39%) 9/105 (9%)

39 • Alimentary Tract Duplications 633
*
Fig. 39.7 This thoracoscopic view shows an esophageal duplication (asterisk) that is adjacent to the esophagus (arrow) and attached to a piece of primi-tive lung. Histologic analysis confirmed the mass as a duplication with primitive lung. (Photograph courtesy Dr. Thane Blinman.)
A B C
Fig. 39.9 A 3-year-old child was found to have a right paravertebral mass. (A) A large anterior defect in the vertebral bodies of the upper thoracic spine (arrow) is seen. (B) This myelogram shows the filling defect caused by a neuroenteric cyst. (C) The contrast agent from the myelogram is seen in the neuroenteric cyst (upper arrow) with extension subdiaphragmatically (black arrow) into the distal small intestine. (From Holcomb GW III, Gheissari A, O’Neill JA, et al. Surgical management of alimentary tract duplications. Ann Surg 1989;209:167–174.)
A B
Fig. 39.8 This 16-year-old patient was found to have a posterior mediastinal mass on chest radiograph. CT scan (A) shows the duplication (arrow) to be adjacent to the trachea and the esophagus. On the right (B), the duplication is visualized at thoracoscopy and was excised without complications.
Holcomb and Ashcraft’s Pediatric Surgery634
and MRI is often useful to evaluate for neuroenteric com-munication. The current treatment is a one-stage combined thoracoabdominal approach for resection. This can be done open or by a minimally invasive thoracoscopic approach followed by an incision in the diaphragm to access the abdominal component.
GASTRIC DUPLICATIONS
Gastric duplications account for 9% of alimentary tract duplications (see Table 39.1) and usually become symptom-atic early in life, frequently presenting with pain, emesis, or melena. Most are cystic, arise from the greater curvature, and do not communicate with the lumen (Fig. 39.10).5,16 Peptic ulceration with hemorrhage or perforation can develop. Abdominal US usually can diagnose the duplica-tion, but pancreatic pseudocysts or choledochal cysts may have similar appearances and be difficult to differentiate. If there is any uncertainty, CT or MRI is recommended to help clarify the anatomy before attempting surgical resec-tion. As with most duplications, resection is recommended to prevent complications such as bleeding, perforation, and malignancy. Depending on the location and ease of opera-tion, resection through the shared muscular wall or wedge resection of the native stomach along with the duplication are both acceptable. In more difficult locations, such as the lesser curve, gastroesophageal junction, and pylorus, the cyst can be partially excised in a safe manner followed by mucosal stripping of any remaining mucosa in order to avoid a significant gastrectomy.
DUODENAL DUPLICATIONS
Duodenal duplications account for 7% of all duplications (see Table 39.1) and may be asymptomatic or can mani-fest with bleeding, intestinal obstruction, or obstruction of the biliopancreatic ducts causing jaundice or pancreatitis. Most are cystic and noncommunicating with the lumen,
but occasionally tubular variants are seen.48,49 These fre-quently contain rests of gastric or pancreatic tissue. Abdom-inal US is often used as an initial study, but most surgeons elect for CT or magnetic resonance cholangiopancreatogra-phy (MRCP) to better delineate the anatomy prior to opera-tion (Fig. 39.11). The anatomic location and tenuous blood supply of these duplications dictate the operative approach. Simple excision is preferred, but the intimate relationship to the biliary and/or pancreatic ducts may warrant Roux-en-Y cystjejunostomy.50 In complicated cases, endoscopic ret-rograde cholangiopancreatography (ERCP) may be useful in the diagnosis. Endoscopy for the treatment of duodenal duplications also has been described.51
PANCREATIC DUPLICATIONS
Pancreatic duplications are the rarest type of GI duplica-tion. Commonly manifesting with abdominal pain that is often recurrent and chronic, they can easily be mistaken for a pancreatic pseudocyst. What differentiates them from other alimentary duplications is that there is communica-tion with the main or accessory pancreatic duct. The cysts are similar to gastric duplications both grossly and micro-scopically, but they may or may not have attachment to the stomach. They can be intrapancreatic or extrapancreatic, and may be combined with duplicated pancreatic tissue along an aberrant duct. The location of ductal communi-cation can be anywhere in the pancreas. On exploration, there is often significant fibrosis, likely from chronic inflam-mation. Intraoperative frozen section evaluation will differ-entiate a duplication from a pseudocyst based on the cyst wall cellularity. Simple cyst resection is preferred, but the location may dictate a more complex resection.52–54
*
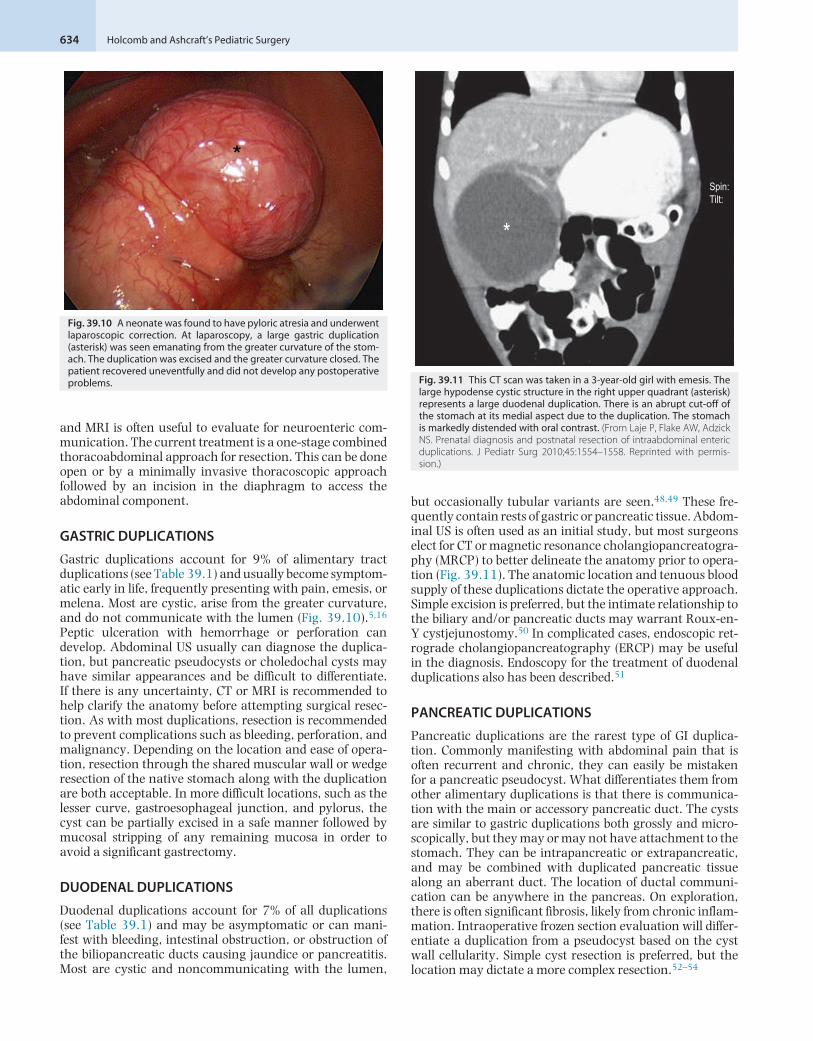
Fig. 39.10 A neonate was found to have pyloric atresia and underwent laparoscopic correction. At laparoscopy, a large gastric duplication (asterisk) was seen emanating from the greater curvature of the stom-ach. The duplication was excised and the greater curvature closed. The patient recovered uneventfully and did not develop any postoperative problems.
*
Spin:Tilt:
Fig. 39.11 This CT scan was taken in a 3-year-old girl with emesis. The large hypodense cystic structure in the right upper quadrant (asterisk) represents a large duodenal duplication. There is an abrupt cut-off of the stomach at its medial aspect due to the duplication. The stomach is markedly distended with oral contrast. (From Laje P, Flake AW, Adzick NS. Prenatal diagnosis and postnatal resection of intraabdominal enteric duplications. J Pediatr Surg 2010;45:1554–1558. Reprinted with permis-sion.)
39 • Alimentary Tract Duplications 635
SMALL BOWEL DUPLICATIONS
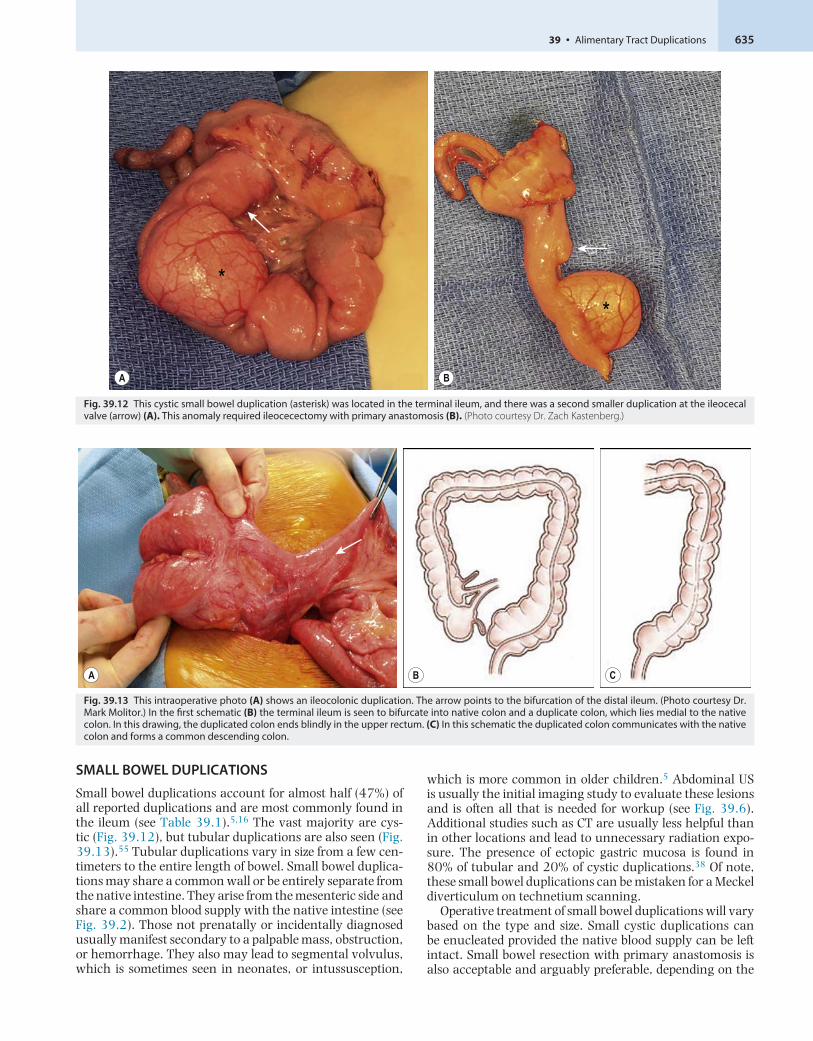
Small bowel duplications account for almost half (47%) of all reported duplications and are most commonly found in the ileum (see Table 39.1).5,16 The vast majority are cys-tic (Fig. 39.12), but tubular duplications are also seen (Fig. 39.13).55 Tubular duplications vary in size from a few cen-timeters to the entire length of bowel. Small bowel duplica-tions may share a common wall or be entirely separate from the native intestine. They arise from the mesenteric side and share a common blood supply with the native intestine (see Fig. 39.2). Those not prenatally or incidentally diagnosed usually manifest secondary to a palpable mass, obstruction, or hemorrhage. They also may lead to segmental volvulus, which is sometimes seen in neonates, or intussusception,
which is more common in older children.5 Abdominal US is usually the initial imaging study to evaluate these lesions and is often all that is needed for workup (see Fig. 39.6). Additional studies such as CT are usually less helpful than in other locations and lead to unnecessary radiation expo-sure. The presence of ectopic gastric mucosa is found in 80% of tubular and 20% of cystic duplications.38 Of note, these small bowel duplications can be mistaken for a Meckel diverticulum on technetium scanning.
Operative treatment of small bowel duplications will vary based on the type and size. Small cystic duplications can be enucleated provided the native blood supply can be left intact. Small bowel resection with primary anastomosis is also acceptable and arguably preferable, depending on the
A B
**
Fig. 39.12 This cystic small bowel duplication (asterisk) was located in the terminal ileum, and there was a second smaller duplication at the ileocecal valve (arrow) (A). This anomaly required ileocecectomy with primary anastomosis (B). (Photo courtesy Dr. Zach Kastenberg.)
A B C
Fig. 39.13 This intraoperative photo (A) shows an ileocolonic duplication. The arrow points to the bifurcation of the distal ileum. (Photo courtesy Dr. Mark Molitor.) In the first schematic (B) the terminal ileum is seen to bifurcate into native colon and a duplicate colon, which lies medial to the native colon. In this drawing, the duplicated colon ends blindly in the upper rectum. (C) In this schematic the duplicated colon communicates with the native colon and forms a common descending colon.
Holcomb and Ashcraft’s Pediatric Surgery636
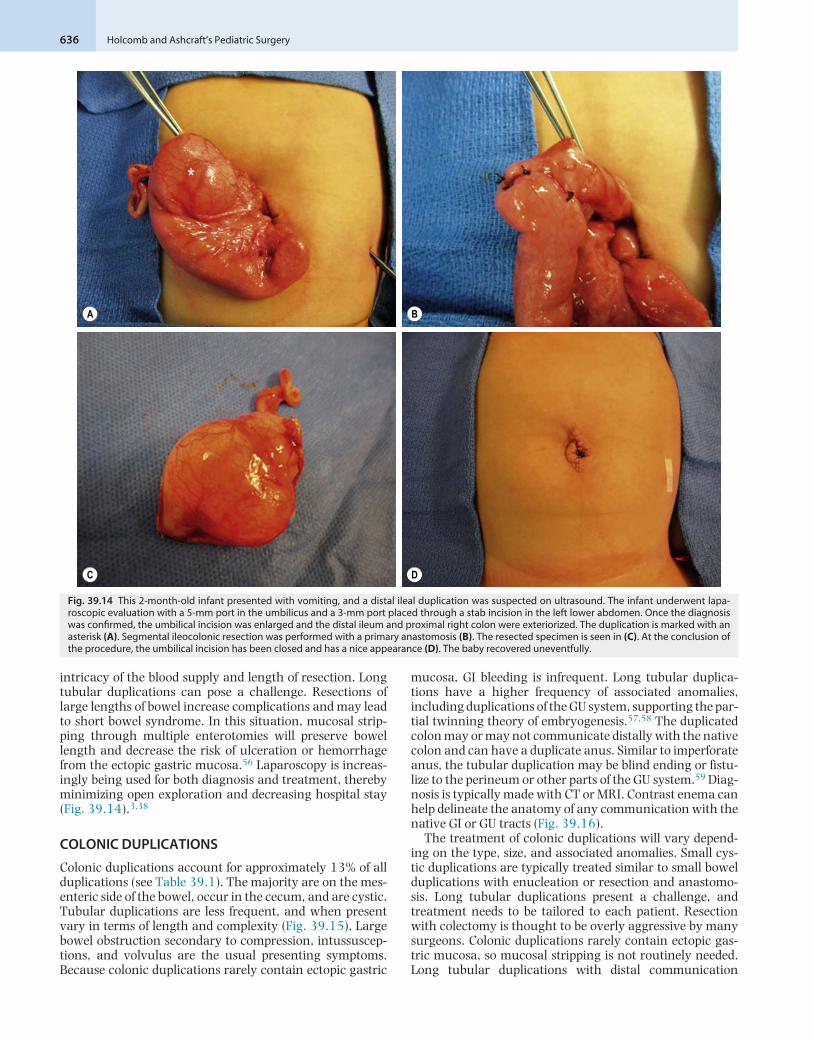
intricacy of the blood supply and length of resection. Long tubular duplications can pose a challenge. Resections of large lengths of bowel increase complications and may lead to short bowel syndrome. In this situation, mucosal strip-ping through multiple enterotomies will preserve bowel length and decrease the risk of ulceration or hemorrhage from the ectopic gastric mucosa.56 Laparoscopy is increas-ingly being used for both diagnosis and treatment, thereby minimizing open exploration and decreasing hospital stay (Fig. 39.14).3,38
COLONIC DUPLICATIONS
Colonic duplications account for approximately 13% of all duplications (see Table 39.1). The majority are on the mes-enteric side of the bowel, occur in the cecum, and are cystic. Tubular duplications are less frequent, and when present vary in terms of length and complexity (Fig. 39.15). Large bowel obstruction secondary to compression, intussuscep-tions, and volvulus are the usual presenting symptoms. Because colonic duplications rarely contain ectopic gastric
mucosa, GI bleeding is infrequent. Long tubular duplica-tions have a higher frequency of associated anomalies, including duplications of the GU system, supporting the par-tial twinning theory of embryogenesis.57,58 The duplicated colon may or may not communicate distally with the native colon and can have a duplicate anus. Similar to imperforate anus, the tubular duplication may be blind ending or fistu-lize to the perineum or other parts of the GU system.59 Diag-nosis is typically made with CT or MRI. Contrast enema can help delineate the anatomy of any communication with the native GI or GU tracts (Fig. 39.16).
The treatment of colonic duplications will vary depend-ing on the type, size, and associated anomalies. Small cys-tic duplications are typically treated similar to small bowel duplications with enucleation or resection and anastomo-sis. Long tubular duplications present a challenge, and treatment needs to be tailored to each patient. Resection with colectomy is thought to be overly aggressive by many surgeons. Colonic duplications rarely contain ectopic gas-tric mucosa, so mucosal stripping is not routinely needed. Long tubular duplications with distal communication
A B
C D
*
Fig. 39.14 This 2-month-old infant presented with vomiting, and a distal ileal duplication was suspected on ultrasound. The infant underwent lapa-roscopic evaluation with a 5-mm port in the umbilicus and a 3-mm port placed through a stab incision in the left lower abdomen. Once the diagnosis was confirmed, the umbilical incision was enlarged and the distal ileum and proximal right colon were exteriorized. The duplication is marked with an asterisk (A). Segmental ileocolonic resection was performed with a primary anastomosis (B). The resected specimen is seen in (C). At the conclusion of the procedure, the umbilical incision has been closed and has a nice appearance (D). The baby recovered uneventfully.
39 • Alimentary Tract Duplications 637
A B
DC
*
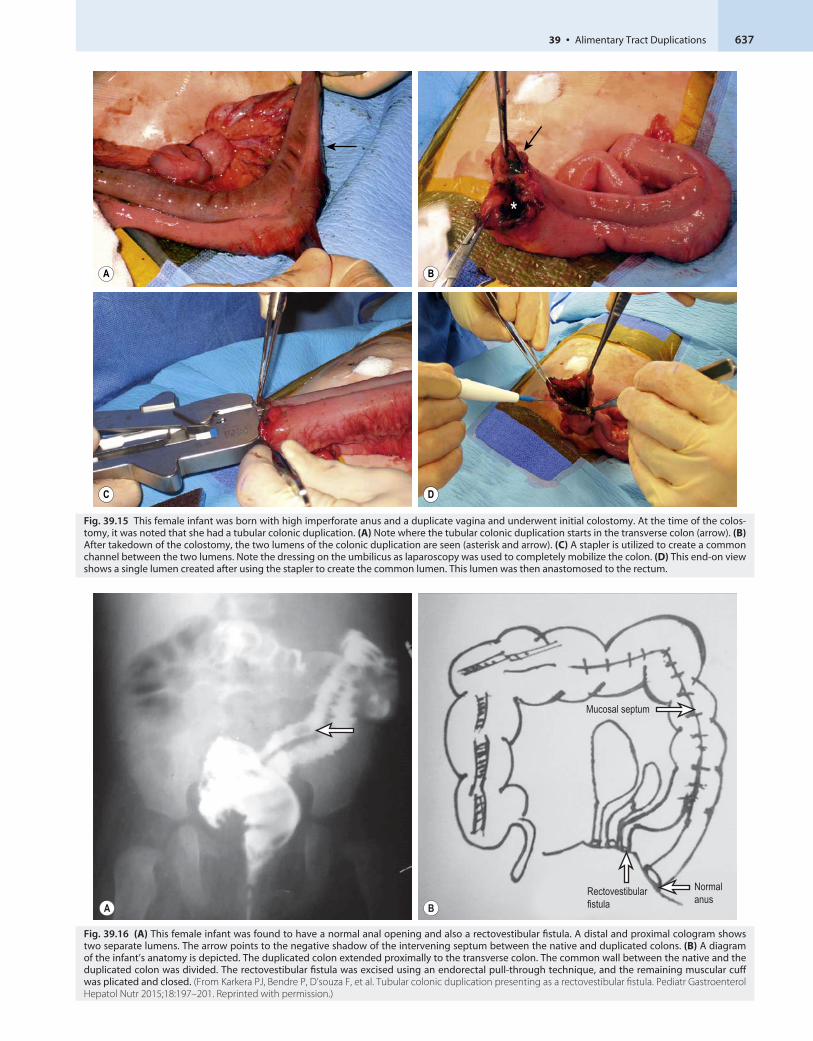
Fig. 39.15 This female infant was born with high imperforate anus and a duplicate vagina and underwent initial colostomy. At the time of the colos-tomy, it was noted that she had a tubular colonic duplication. (A) Note where the tubular colonic duplication starts in the transverse colon (arrow). (B) After takedown of the colostomy, the two lumens of the colonic duplication are seen (asterisk and arrow). (C) A stapler is utilized to create a common channel between the two lumens. Note the dressing on the umbilicus as laparoscopy was used to completely mobilize the colon. (D) This end-on view shows a single lumen created after using the stapler to create the common lumen. This lumen was then anastomosed to the rectum.
A BRectovestibularfistula
Normalanus
Mucosal septum
Fig. 39.16 (A) This female infant was found to have a normal anal opening and also a rectovestibular fistula. A distal and proximal cologram shows two separate lumens. The arrow points to the negative shadow of the intervening septum between the native and duplicated colons. (B) A diagram of the infant’s anatomy is depicted. The duplicated colon extended proximally to the transverse colon. The common wall between the native and the duplicated colon was divided. The rectovestibular fistula was excised using an endorectal pull-through technique, and the remaining muscular cuff was plicated and closed. (From Karkera PJ, Bendre P, D’souza F, et al. Tubular colonic duplication presenting as a rectovestibular fistula. Pediatr Gastroenterol Hepatol Nutr 2015;18:197–201. Reprinted with permission.)
Holcomb and Ashcraft’s Pediatric Surgery638
are often treated conservatively with stool softeners. If there is no distal communication, one may be created to relieve obstruction (see Fig. 39.15). Fistulous tracts to the perineum or other organs need to be excised and closed. Associated anomalies also need attention.
RECTAL DUPLICATIONS
Rectal duplications account for approximately 3% of dupli-cations (see Table 39.1) and are most often found in the presacral space posterior to the rectum (Fig. 39.17). Chil-dren typically present with constipation due to a mass effect. Less frequently, rectal duplications can be associated with anorectal malformations, can fistulize to other pelvic organs, or can present in adulthood with obstruction or bleeding.42,60,61 Digital rectal examination may reveal a mass. Multiple imaging modalities including CT, MRI, and contrast enema can aid in making the diagnosis. Treatment options include transanal resection, division of the sep-tum between the duplication and the native rectum, or a
posterior sagittal approach for more extensive duplications. Some patients may require an initial colostomy for large or complicated duplications.
Summary
Alimentary tract duplications are rare congenital anom-alies that occur anywhere along the enteric tract, most commonly in the small bowel. (Gallbladder and appen-diceal duplications are also occasionally encountered [Figs. 39.18 and 39.19]). The mucosa is typically the same as adjacent bowel but can contain ectopic tissue, most commonly gastric mucosa, that can cause bleed-ing complications. They are usually cystic but also can be tubular. They are discovered prenatally or inci-dentally, and present with a wide variety of symptoms depending on location. Resection is recommended in most instances to prevent complications and potential malignant transformation.
A B
**
*
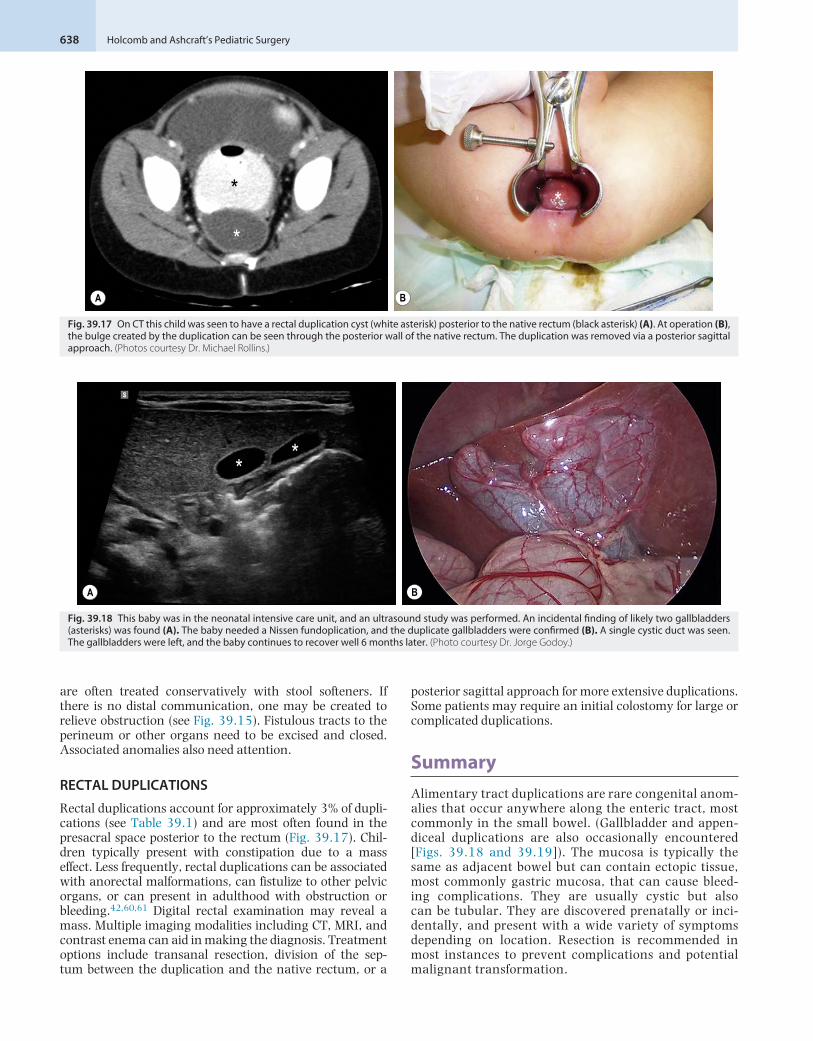
Fig. 39.17 On CT this child was seen to have a rectal duplication cyst (white asterisk) posterior to the native rectum (black asterisk) (A). At operation (B), the bulge created by the duplication can be seen through the posterior wall of the native rectum. The duplication was removed via a posterior sagittal approach. (Photos courtesy Dr. Michael Rollins.)
A B
* *
Fig. 39.18 This baby was in the neonatal intensive care unit, and an ultrasound study was performed. An incidental finding of likely two gallbladders (asterisks) was found (A). The baby needed a Nissen fundoplication, and the duplicate gallbladders were confirmed (B). A single cystic duct was seen. The gallbladders were left, and the baby continues to recover well 6 months later. (Photo courtesy Dr. Jorge Godoy.)

39 • Alimentary Tract Duplications 639
References 1. Ladd WE. Duplications of the alimentary tract. South Med J.
1937;30:363–371. 2. Gross RE, Holcomb GW, Farber S. Duplications of the alimentary tract.
Pediatrics. 1952;9:449–467. 3. Schalamon J, Schleef J, Hollworth ME. Experience with gastrointesti-
nal duplications in childhood. Langenbeck’s Arch Surg. 2000;385:402–405.
4. Stringer MD, Spitz L, Abel R, et al. Management of alimentary tract duplication in children. Br J Surg. 1995;82:74–78.
5. Holcomb III GW, Gheissari A, O’ Neill JA, et al. Surgical management of alimentary tract duplications. Ann Surg. 1989;209:167–174.
6. Smith ED. Duplication of the anus and genitourinary tract. Surgery. 1969;66:909–921.
7. Lewis PL, Holder T, Feldman M. Duplication of the stomach: report of a case and review of the English literature. Arch Surg. 1961;82:634–640.
8. Bentley JFR, Smith JR. Developmental posterior enteric remnants and spinal malformations: the split notochord syndrome. Arch Dis Child. 1960;35:76–86.
9. Qi BQ, Beasley SW, Williams AK. Evidence of a common pathogen-esis for foregut duplications and esophageal atresia with tracheo-esophageal fistula. Anat Rec. 2001;264:93–100.
10. Qi BQ, Beasley SW, Frizelle FA. Evidence that the notochord may be pivotal in the development of sacral and anorectal malformations. J Pediatr Surg. 2003;38:1310–1316.
11. Lewis FT, Thyng FW. Regular occurrence of intestinal diverticula in embryos of pig, rabbit, and man. Am J Anat. 1908;7:505–519.
12. Bremer JL. Diverticula and duplications of the intestinal tract. Arch Pathol. 1944;38:132–140.
13. Mellish RWP, Koop CE. Clinical manifestations of duplication of the bowel. Pediatrics. 1961;27:397–407.
14. Favara BE, Franciosi RA, Akers DR. Enteric duplications: thirty-seven cases: a vascular theory of pathogenesis. Am J Dis Child. 1971;35:501–506.
15. Laje P, Flake AW, Adzick NS. Prenatal diagnosis and postnatal resection of intraabdominal enteric duplications. J Pediatr Surg. 2010;45:1554–1558.
16. Mejaddam AY, Russell KW, Laje P, et al. Clinical Manifestations and Management of Alimentary Tract Duplication Cysts in Children. Abstract submitted APSA; 2018.
17. De Roeck A, Vervloessem D, Mattelaer C, et al. Isolated enteric dupli-cation cyst with respiratory epithelium: case report and review of the literature. Eur J Pediatr Surg. 2008;18:337–339.
18. Guerin F, Guillaume Podevin, Petit T, et al. Outcome of alimentary tract duplications operated on by minimally invasive surgery: a retrospective multicenter study by the GECI. Surg Endosc. 2012;26:2848–2855.
19. Hsu H, Gueng MK, Tseng YH, et al. Adenocarcinoma arising from colonic duplication cyst with metastasis to omentum; a case report. J Clin Ultrasound. 2011;39:41–43.
20. Blank G, Konigsrainer A, Sipos B, et al. Adenocarcinoma arising in a cystic duplication of the small bowel: case report and review of the literature. World J Surg Oncol. 2012;10:55.
21. Orr MM, Edwards AJ. Neoplastic change in duplications of the alimen-tary tract. Br J Surg. 1975;62:269–274.
22. Barr LL, Hayden Jr CK, Stansberry SD, et al. Enteric duplication cysts in children: are their ultrasonographic wall characteristics diagnos-tic? Pediatr Radiol. 1990;20:326–328.
23. Hur J, Yoon CS, Kim MJ, et al. Imaging features of gastrointestinal tract duplications in infants and children: from oesophagus to rectum. Pediatr Radiol. 2007;37:691–699.
24. Lecouffe P, Spyckerelle C, Venel H, et al. Use of pertechnetate 99mTc abdominal scanning in localizing an ileal duplication cyst: case report and review of the literature. Eur J Nucl Med. 1992;19:65–67.
25. Kumar R, Tripathi M, Chandrashekar N, et al. Diagnosis of ectopic gastric mucosa using 99mTc pertechnetate: a spectrum of scinti-graphic findings. Br J Radiol. 2005;78:714–720.
26. Haddon MJ, Bowen A. Bronchopulmonary and neuroenteric forms of foregut anomalies: imaging for diagnosis and management. Radiol Clin North Am. 1991;29:241–254.
27. Basu R, Forshall I, Rickham PP. Duplications of the alimentary tract. Br J Surg. 1960;47:477–484.
28. Grosfeld JL, O’ Neill JA, Clatworthy HW. Enteric duplications in infancy and childhood: an 18-year review. Ann Surg. 1970;172:83–90.
29. Bower RJ, Sieber WK, Kiesewetter WB. Alimentary tract duplications in children. Ann Surg. 1978;188:669–674.
30. Hocking M, Young DG. Duplications of the alimentary tract. Br J Surg. 1981;68:92–96.
31. Ildstad ST, Tollerud DJ, Weiss RG, et al. Duplications of the alimentary tract. Ann Surg. 1988;208:184–189.
32. Bissler JJ, Klein RL. Alimentary tract duplications in children: case and literature review. Clin Pediatr. 1988;27:152–157.
33. Pinter AB, Schubert W, Szemledy F, et al. Alimentary tract duplica-tions in infants and children. Eur J Pediatr Surg. 1992;2:8–12.
34. Bajpai M, Mathur M. Duplication of the alimentary tract: clues to the missing links. J Pediatr Surg. 1994;29:1361–1365.
35. Iyer CP, Mahour GH. Duplications of the alimentary tract in infants and children. J Pediatr Surg. 1995;30:1267–1270.
36. Yang MC, Duh YC, Lai HC, et al. Alimentary tract duplications. J For-mos Med Assoc. 1996;95:406–409.
37. Karnak I, Ocal T, Senocak ME, et al. Alimentary tract duplications in children: report of 26 years’ experience. Turk J Pediatr. 2000;42:118–125.
38. Puligandla PS, Nguyen LT, St-Vil D, et al. Gastrointestinal duplica-tions. J Pediatr Surg. 2003;38:740–744.
39. Lima M, Molinaro F, Ruggeri G, et al. Role of mini-invasive surgery in the treatment of enteric duplications in paediatric age: a survey of 15 years. Ped Med Chir. 2012;34:217–222.
40. Zouari M, Bouthour H, Abdallah RB, et al. Alimentary tract duplica-tions in children: report of 16 years’ experience. Afr J Paediatr Surg. 2014;11:330–333.
41. Okur MH, Arslan MS, Arslan S, et al. Gastrointestinal duplications in children. Eur Rev Med Pharmacol Sci. 2014;18:1507–1512.
42. Jehangir S, Ninan PJ, Jacob TJ, et al. Enteric duplication in children: experience from a tertiary center in South India. J Indian Assoc Pediatr Surg. 2015;20:174–178.
43. Rattan KN, Bansal S, Dhamija A. Gastrointestinal duplication pre-senting as neonatal intestinal obstruction: an experience of 15 years at tertiary care centre. J Neo Surg. 2017;6:5.
44. Erginel B, Soysal FG, Ozbey H, et al. Enteric duplications cysts in chil-dren: a single-institution series with forty patients in twenty-six years. World J Surg. 2017;41:620–624.
45. Bratu I, Laberge JL, Flageole H, et al. Foregut duplications: is there an advantage to thoracoscopic resection? J Pediatr Surg. 2005;40:138–141.
46. Merry C, Spurbeck W, Lobe TE. Resection of foregut-derived duplica-tions by minimal-access surgery. Pediatr Surg Int. 1999;15:224–226.
47. Pokorny WJ, Goldstein IR. Enteric thoracoabdominal duplications in children. J Thorac Cardiovasc Surg. 1984;87:821–824.
48. Vertruyen M, Cadiere GB, Jacobvitz D, et al. A propos de 2 cas de dupli-cation duodenale. Acta Chir Belg. 1991;91:140–144.
Fig. 39.19 This child presented with peritonitis and was found to have duplication of the appendix with infarction and necrosis of one appendix. He underwent removal of both appendices and recovered uneventfully.

Holcomb and Ashcraft’s Pediatric Surgery640
49. Merrot T, Anastasescu R, Pankevych T, et al. Duodenal duplications: clinical characteristics, embryological hypotheses, histological find-ings, treatment. Eur J Pediatr Surg. 2006;16:18–23.
50. Leenders EL, Odsman MZ, Sukarochana K. Treatment of duodenal duplication with international review. Am Surg. 1970;36:368–371.
51. Romeo E, Torroni F, Foschia F, et al. Surgery or endoscopy to treat duodenal duplications in children. J Pediatr Surg. 2011;40:874–878.
52. Hunter CJ, Connelly ME, Ghaffari N, et al. Enteric duplication cysts of the pancreas: a report of two cases and review of the literature. Pediatr Surg Int. 2008;24:227–233.
53. Christians KK, Pappas S, Pilgrim C, et al. Duplicate pancreas meets gastric duplication cyst: a tale of two anomalies. Int J Surg Case Rep. 2013;4:735–739.
54. Lee CL, binti Che Daud CZ, binti Ismail R. Intrapancreatic gastric duplication cyst- a rare cause of chronic abdominal pain in childhood. J Clin Ultrasound. 2014;42:42–44.
55. Cunningham AJ, Ham PB, King RG, et al. Congenital jejunal dupli-cation in a patient with a congenital thoracic meningocele. Am Surg. 2015;81:332–333.
56. Wrenn Jr EL. Tubular duplication of the small intestine. Surgery. 1962;52:494–498.
57. Smith ED, Stephens FD. Duplication and vesicointestinal fissure. Birth Defects Orig Artic Ser. 1988;24:551–580.
58. Ravitch MM. Hind gut duplication-doubling of colon and genital uri-nary tracts. Ann Surg. 1953;137:588–601.
59. Kottra JJ, Dodds WJ. Duplication of the large bowel. AJR Am J Roent-genol. 1971;113:310–315.
60. Pampal A, Ozbayoglu A, Kaya C, et al. Rectal duplications accom-panying rectovestibular fistula: report of two cases. Pediatr Int. 2013;55:86–89.
61. Jackson KL, Peche WJ, Rollins MD. An unusual presentation of a rec-tal duplication cyst. Int J Surg Case Rep. 1012;3:314–315.