Embed Size (px)
Citation preview
Keeping it Simple: Using IVR to Enhance Wellness
Janelle HoweSr. Director, Health Enhancement
HealthCare Partners Medical GroupCo-Investigator, HealthCare Partners Institute
for Applied Research and Education
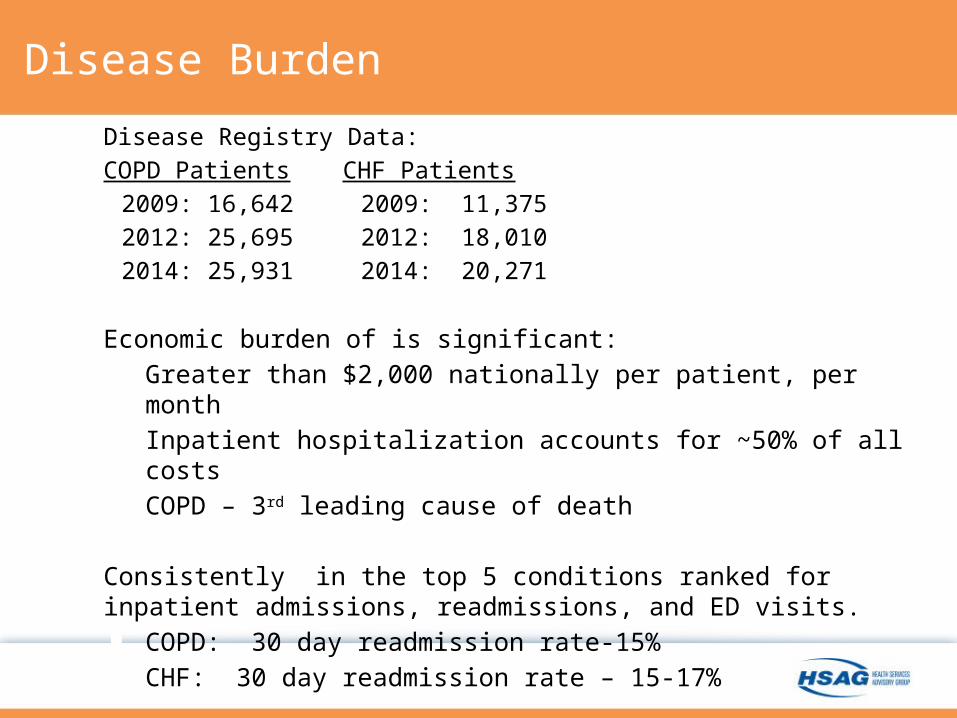
Disease Burden
Disease Registry Data: COPD Patients CHF Patients
2009: 16,642 2009: 11,3752012: 25,695 2012: 18,0102014: 25,931 2014: 20,271
Economic burden of is significant: Greater than $2,000 nationally per patient, per month Inpatient hospitalization accounts for ~50% of all costs COPD – 3rd leading cause of death
Consistently in the top 5 conditions ranked for inpatient admissions, readmissions, and ED visits. COPD: 30 day readmission rate-15% CHF: 30 day readmission rate – 15-17%
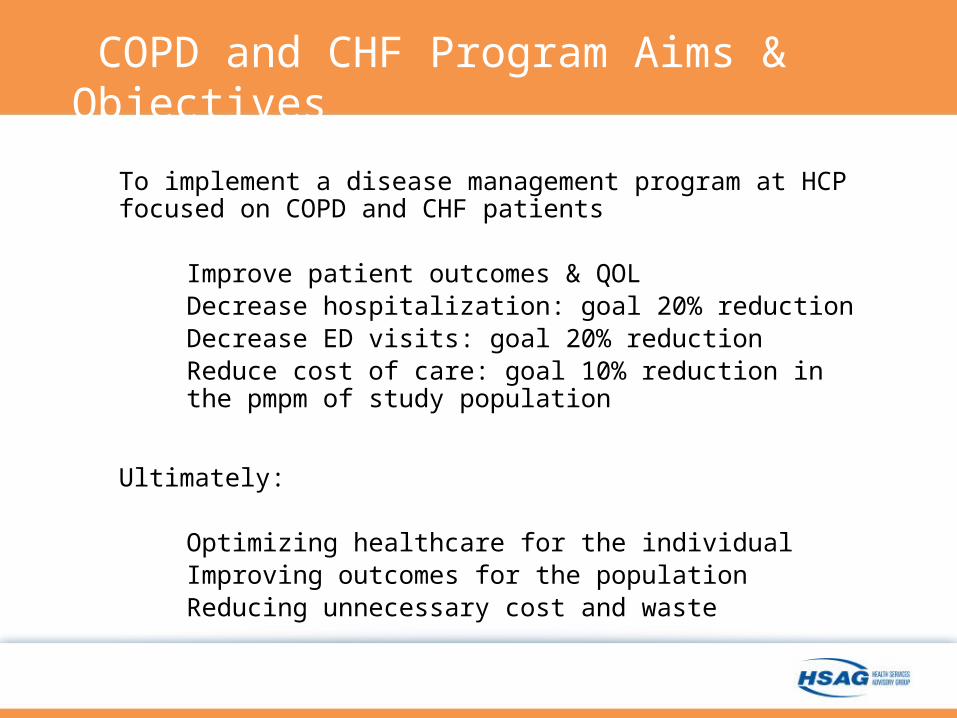
COPD and CHF Program Aims & Objectives
To implement a disease management program at HCP focused on COPD and CHF patients
Improve patient outcomes & QOL Decrease hospitalization: goal 20% reduction Decrease ED visits: goal 20% reduction Reduce cost of care: goal 10% reduction in the pmpm of
study population
Ultimately:
Optimizing healthcare for the individual Improving outcomes for the population Reducing unnecessary cost and waste
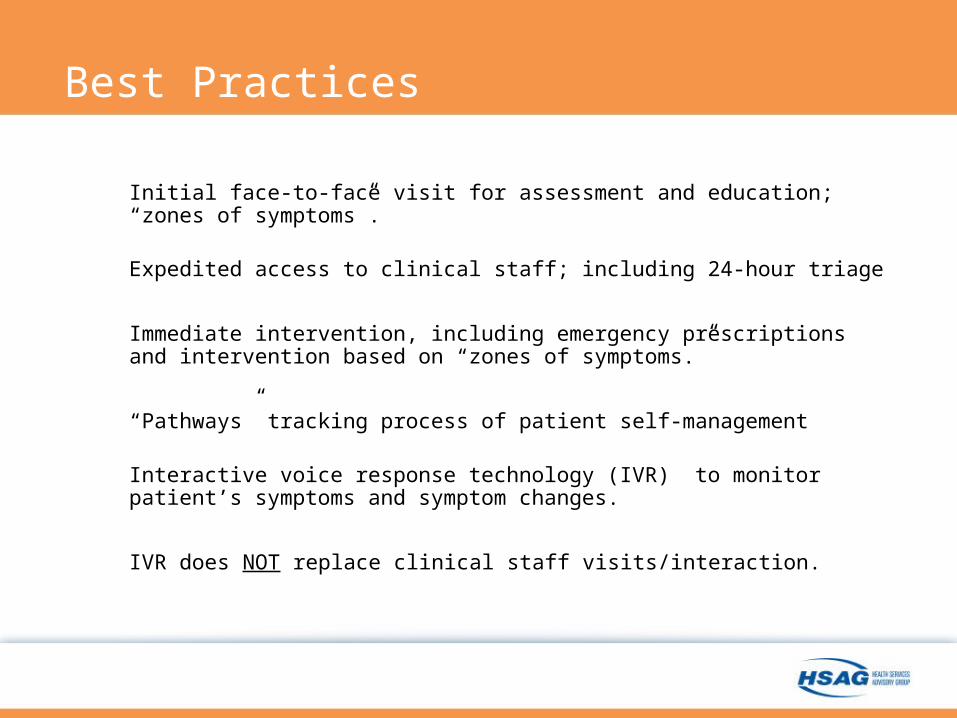
Best Practices
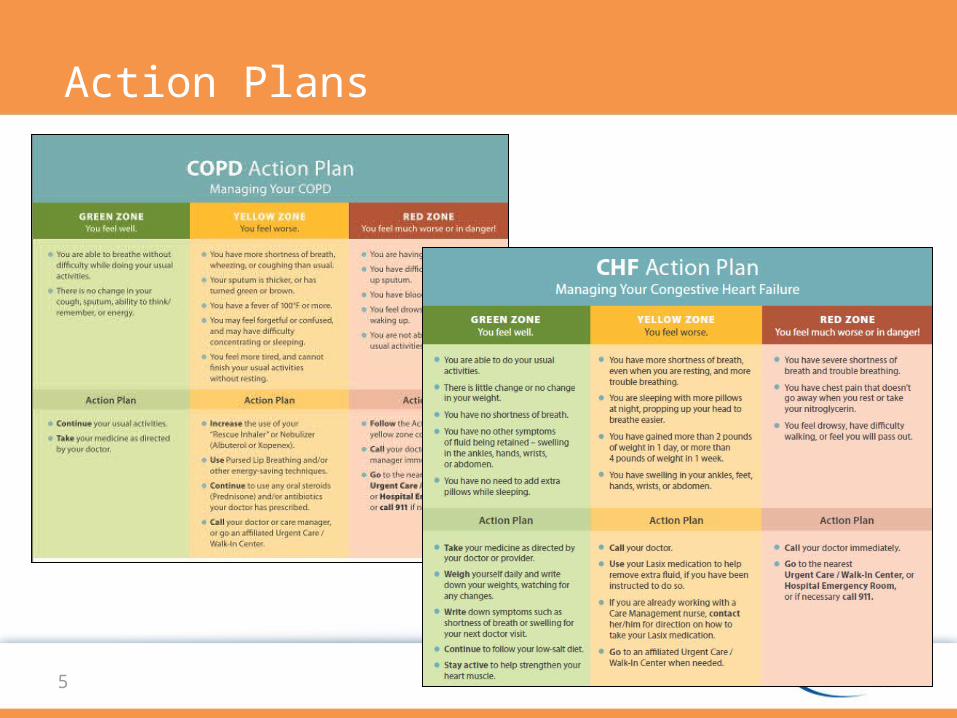
Initial face-to-face visit for assessment and education; “zones of symptoms”.
Expedited access to clinical staff; including 24-hour triage
Immediate intervention, including emergency prescriptions and intervention based on “zones of symptoms.”
“Pathways” tracking process of patient self-management
Interactive voice response technology (IVR) to monitor patient’s symptoms and symptom changes.
IVR does NOT replace clinical staff visits/interaction.
5
Action Plans
Expanding Clinical Capacity
IVR Technology Expands the clinical capacity of our nurses. Supports the administration of emergency prescriptions;
patients recognize worsening symptoms and are taking action.
Clinicians’ Reports Reports are easy to read/actionable; Nurses: “We know which
symptoms the patient is experiencing.” Frees-up time and allows clinicians to focus on patients who
are more at-risk.
6
Optimizing Telehealth Operations
Detecting Symptom Exacerbations Sooner
Not intrusive: brief calls that engage patients. Avoided timely and complicated set up: patient uses their own phone. Majority were Senior patients; majority use land-line phones,
however, increasing cell phone use. Convenient: calls occur either at noon with a back-up call early
evening. Provides critical and actionable information for clinicians. Survey captures yellow zone or red zone symptoms; reinforces
recognition on a regular basis.
8
Patient Monitoring Process
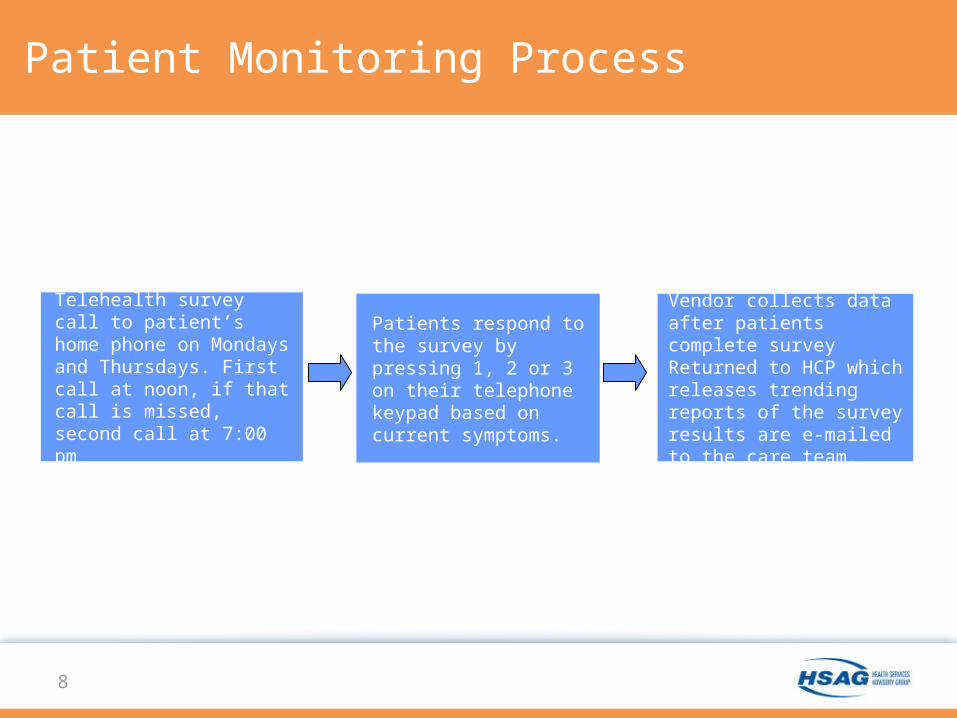
Telehealth survey call to patient’s home phone on Mondays and Thursdays. First call at noon, if that call is missed, second call at 7:00 pm
Patients respond to the survey by pressing 1, 2 or 3 on their telephone keypad based on current symptoms.
Vendor collects data after patients complete survey Returned to HCP which releases trending reports of the survey results are e-mailed to the care team.
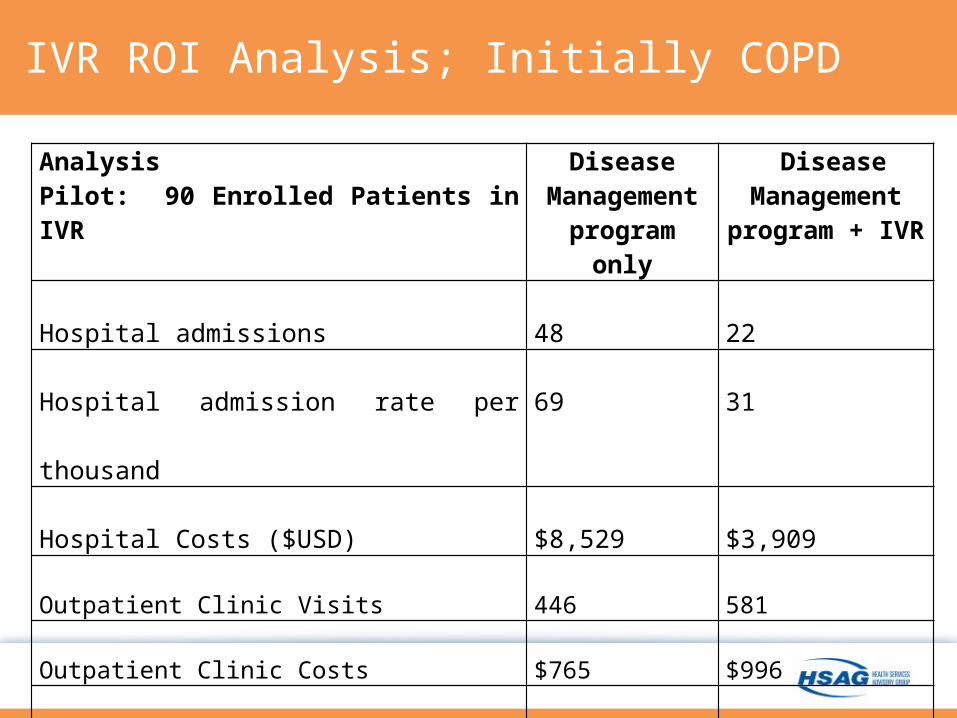
IVR ROI Analysis; Initially COPD
AnalysisPilot: 90 Enrolled Patients in IVR
Disease Management program only
Disease Management program + IVR
Hospital admissions 48 22
Hospital admission rate per thousand 69 31
Hospital Costs ($USD) $8,529 $3,909
Outpatient Clinic Visits 446 581
Outpatient Clinic Costs $765 $996
Return on Investment $4,388 (9:1)
Email Alerts
• Emails trigger at 7AM following day • Tuesday and Friday IVR Data Received
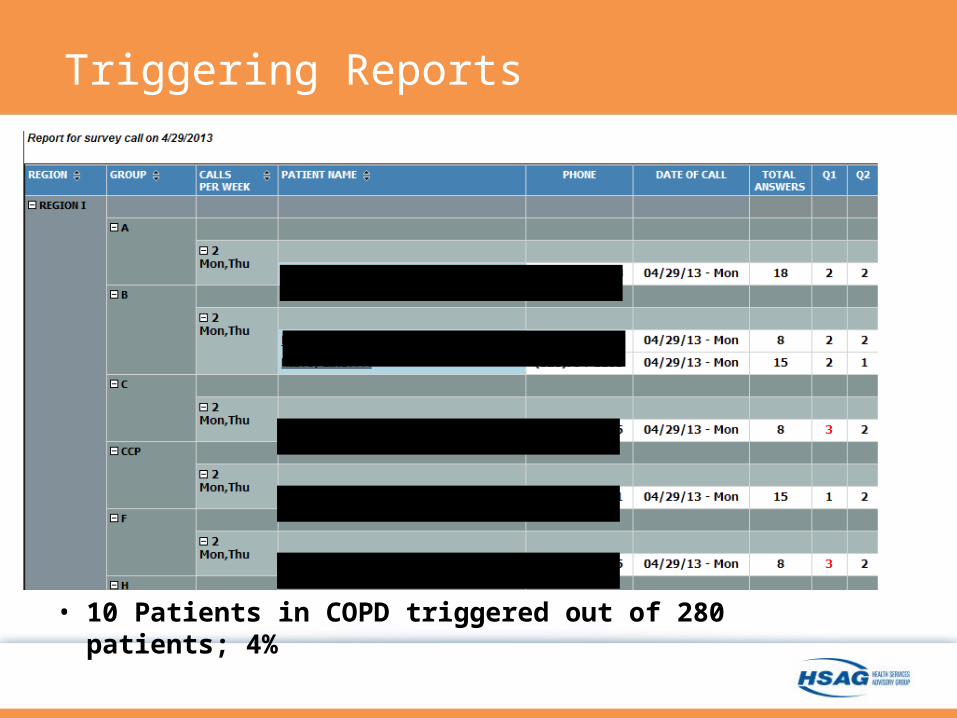
Triggering Reports
• 10 Patients in COPD triggered out of 280 patients; 4%
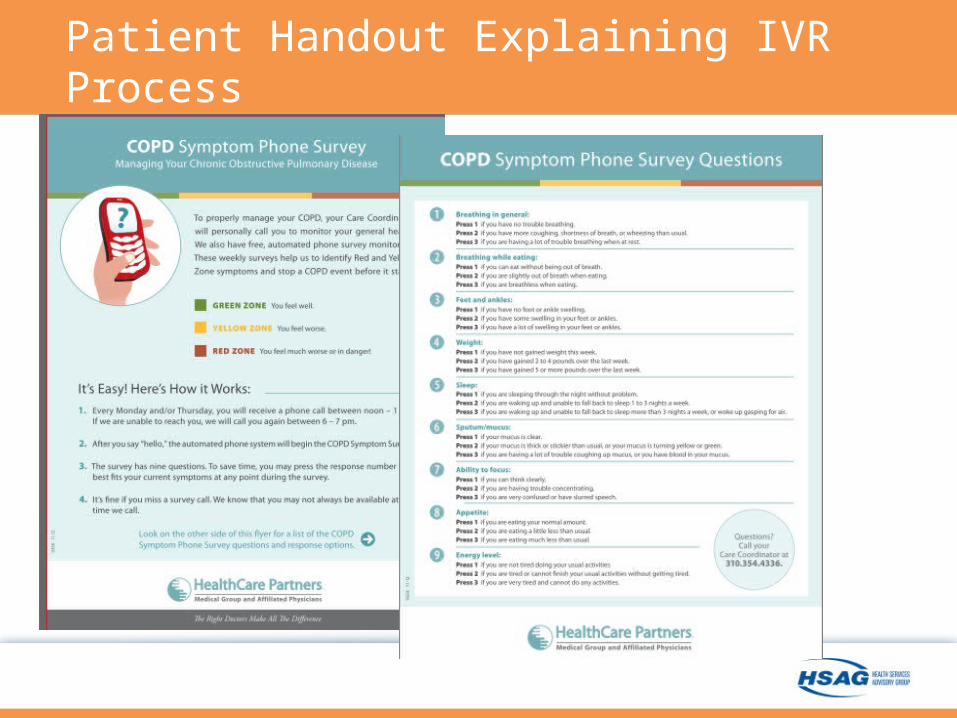
Patient Handout Explaining IVR Process
“Right Care at the Right Time.”
Does not substitute a nurse call or face-to-face meetings with patients and educational training; it supplements these Program activities
Patients/family need to know how to monitor and treat symptom exacerbation. Telemonitoring is implemented once the patient is confident that they understand their Action Plan.
Reinforces the need for patients to self-manage their own condition with appropriate support
Strategy also supports HCP goals for cost-effectiveness; expanding clinical capacity of the staff
Patient comments: “Calls were easy” “Did not take too much time” “Helped me become more involved in my healthcare”
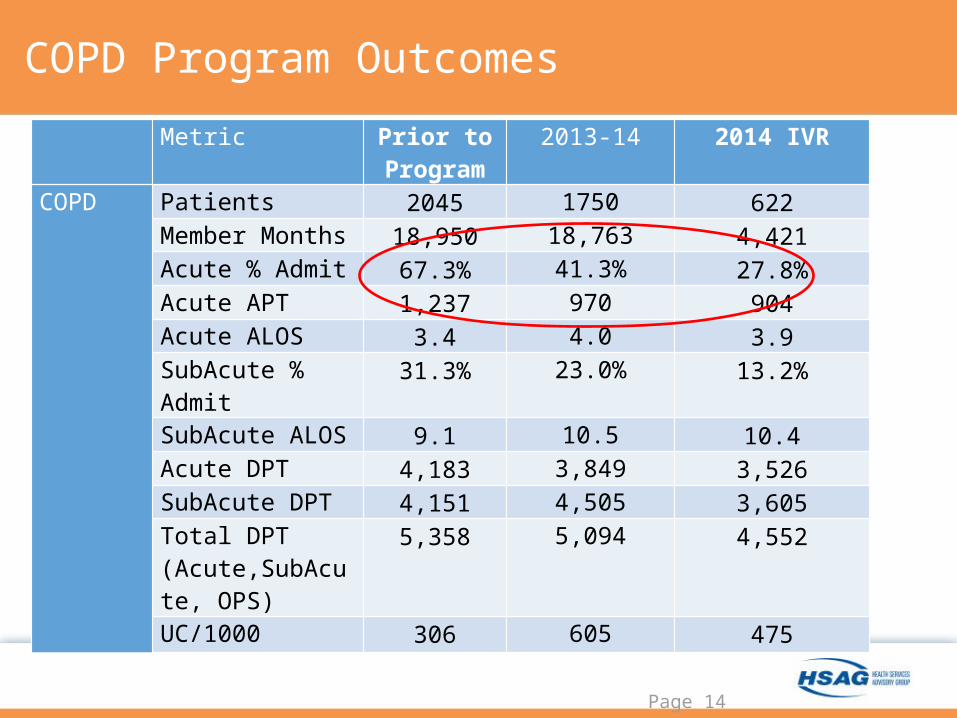
COPD Program Outcomes
Page 14
Metric Prior to Program
2013-14 2014 IVR
COPD Patients 2045 1750 622Member Months 18,950 18,763 4,421Acute % Admit 67.3% 41.3% 27.8%Acute APT 1,237 970 904Acute ALOS 3.4 4.0 3.9SubAcute % Admit 31.3% 23.0% 13.2%SubAcute ALOS 9.1 10.5 10.4Acute DPT 4,183 3,849 3,526SubAcute DPT 4,151 4,505 3,605Total DPT (Acute,SubAcute, OPS)
5,358 5,094 4,552
UC/1000 306 605 475
15
Take-Aways
• Additive: Supplements nurse calls and face-to-face meetings with patients.
• Simple: “Calls were easy, did not take too much time, helped me become more involved in my healthcare.”
• Activation: Patients are less hesitant to contact their care team for assistance.
• Enhanced Wellness: Encourages patients to monitor their own symptoms; appears more effective than brochures/handouts addressing symptoms.
• Adaptive: IVR can be used for diabetes, oncologic protocols, hospital to home transitions, ad infinitum.





























