Embed Size (px)
Citation preview
Product Dossier

1Clinical Research 6/97
Ketac Molar® for ART
Clinical Research 12/99
Contents
1. Preface.................................................................................... 1
2. Introduction............................................................................ 2
2.1 Atraumatic Restorative Treatment........................................ 22.2 Clinical procedure with the ART technique.......................... 32.3 History of glass ionomers ..................................................... 32.4 Motivation............................................................................... 52.5 Indications.............................................................................. 5
3. Chemical Background......................................................... 6
3.1 General overview................................................................... 63.2 Chemical background ........................................................... 6
4. Product Composition........................................................... 9
4.1 Presentation........................................................................... 94.2 Constituents ......................................................................... 10
5. Test Results ......................................................................... 10
5.1 Material properties............................................................... 105.2 Physico-technical data ........................................................ 115.3 Abrasion tests...................................................................... 135.4 Adhesion tests ..................................................................... 155.5 Marginal behaviour............................................................... 165.6 Fluoride release................................................................... 17
6. In vivo studies on KETAC MOLAR for ART ................... 18
6.1 Multi-centre study in China: ................................................. 186.2 Clinical study in South Africa............................................... 216.3 Clinical study in Peking........................................................ 22
7. Conclusion........................................................................... 22
8. Literature .............................................................................. 23
8.1 Clinical studies with KETAC MOLAR for the ART technique ..................................................................... 238.2 Further literature................................................................... 24
Clinical Research 12/99 1
1. Preface
Espe Dental AG played a major role in developing glass ionomers. Pioneering
inventions such as KETAC-SILVER, a glass ionomer cement reinforced with
sintered particles of silver (McLean, Gasser) were developed by Espe Dental AG
through to market launch in collaboration with well-known universities.
The glass ionomers developed in the 1960s and 70s have been successfully
used in dentistry for about two decades now. This class of material is
characterised by easy handling and self-adhesion, even to untreated dentine.
Glass ionomers possess a translucency similar to that of ceramic materials. Its
biocompatibility is excellent. It is particularly suitable for conservative dentistry but
it is also very successfully used for the cementation of indirect restorations.
Quite recently so-called heavy-bodied, "packable" glass ionomer cements were
developed which are especially indicated as restorative materials for molars and
premolars. One of the best known products in this class of material is KETAC
MOLAR. The mechanical properties, which are better than those of conventional
glass ionomer cements, and its packable consistency make KETAC MOLAR
ideal as a restorative material for primary tooth restorations and in the non-
occluded field for cavity class I restorations. Other fields of indication are semi-
permanent class II restorations and cavity class V restorations.
Since the middle of the 1990s this type of glass ionomer has been increasingly
used for the so-called ART technique (Atraumatic Restorative Treatment). Clinical
studies on this type of therapy testify to the fact that KETAC MOLAR produces
excellent results over a period of at least three years.
Clinical Research 12/99 2
2. Introduction
2.1 Atraumatic Restorative Treatment
The ART technique is a method of treatment with the aid of which caries can be
treated at an early stage. The aim of ART is to minimise loss of teeth caused by
caries. Only hand instruments are used. The ART technique is applied without the
need for electricity and without any other elaborate equipment so it can be used
anywhere. The method of treatment was presented by the World Health
Organization (WHO) for the first time in 1994. Areas of application are particularly
countries where it is not possible to ensure that the population has a general
supply of electricity and modern dental equipment is not available everywhere.
However, the ART technique also offers plenty of scope for use in more
developed countries, e.g. in treating the first primary teeth when they appear in
infants. Glass ionomers such as KETAC MOLAR FOR ART are ideal for use as
an ART restorative material on account of their excellent mechanical properties.
No other class of material is characterised by less sensitivity to technique or a
higher level of biocompatibility.
The ART technique already constitutes a form of therapy which has been
scientifically investigated in great detail. Clinical studies in Thailand, Zimbabwe
and China have demonstrated that particularly in the deciduous teeth excellent
results are achieved. In these studies, even after a wearing period of 3 years
retention rates of 90% can be observed in class I cavities.
Apart from the clinical success rates, patient satisfaction constitutes a further
elementary component contributing to the long-term success of the ART
technique. In projects conducted in Zimbabwe and Ghana the acceptance of this
type of therapy was surveyed among the children treated. It became evident that
between 80% and 90% were satisfied both with the treatment and the restoration.
As many as 96% of the patients said they were not afraid of undergoing further
treatment. This constitutes the basis for a long-term improvement in dental health.
Clinical Research 12/99 3
2.2 Clinical procedure with the ART technique
For the ART technique only a small number of dental instruments are necessary:
Hand excavator to remove the caries
Mirror for checking purposes
Rubber gloves for the "press finger" technique
Cotton swab for removing Ketac Conditioner
Plastic spatula for mixing Ketac Molar for ART
Rotating instruments, water and electricity are not required but, if they are
available, they can be used at any time. Children to be treated can, for example,
be examined on a table or on their parents' lap. On account of the highly
conservative removal of caries with a hand instrument the use of local
anaesthetics is unnecessary in most cases. When the caries has been removed,
the cavity is conditioned with KETAC MOLAR FOR ART liquid. The conditioning
liquid is applied inside the cavity with a cotton swab and removed again after 10
seconds. Then the cavity is filled with the mixed KETAC MOLAR FOR ART. With
the so-called "press finger" technique KETAC MOLAR FOR ART is pressed into
the cavity. The final modelling of the restoration is performed with a hand
instrument.
2.3 History of glass ionomers
The glass ionomers developed by Wilson and Kent in 1969 have become an
integral part of every dental surgery. Over the years the glass ionomers have
been repeatedly modified and enhanced in order to meet the increasing
requirements expected of this class of material.
Scientific research into glass ionomers pursued two objectives: on the one hand,
the aim was to develop an aesthetically attractive material for anterior teeth
restorations. The other aim was to improve the material properties in order to
expand the fields of application to include anterior teeth. KETAC MOLAR FOR
ART constitutes the logical enhancement of the proven ESPE glass ionomers.
Clinical Research 12/99 4

Clinical Research 12/99 5
KETAC MOLAR FOR ART is a conventional, metal-free glass ionomer which was
specially developed as a restorative material for molars and premolars. The
improved mechanical properties and the packable consistency were achieved
with an optimised size of glass particles.
2.4 Motivation
As already mentioned heavy-bodied glass ionomers constitute an extremely
promising class of material.
Numerous scientific studies indicate that the strength of heavy-bodied glass
ionomers in comparison with conventional glass ionomers is in some cases
much greater. Particularly the resistance of the heavy-bodied glass ionomers to
abrasion has been increased.
Improved polishability and radiopacity were further aspects which were taken into
account when developing KETAC MOLAR FOR ART.
2.5 Indications
After many years of clinical application of KETAC MOLAR, including applications
as a restorative material in the ART technique, use of the material can be
recommended for the following indications:
• core build-ups
• class I restorations
• semi-permanent class II restorations
• primary tooth restorations
Clinical Research 12/99 6
3. Chemical Background
3.1 General overview
Heavy-bodied glass ionomers are obtained not only by simply mixing glass
powder and a polycarbonic acid. As with conventional glass ionomers, the curing
takes place between the polycarbonic acids in the fluid and the reactive fluoro-
calcium-aluminium-silicate-glass of the glass powder. In contrast with
conventional glass ionomers these cements are characterised by a much higher
abrasive stability.
3.2 Chemical background
The curing of glass ionomers is a complex sequence of chemical reactions in
which water plays a major role. Whilst in the first curing phase the presence of
water as a solvent is crucial for starting the reaction between the powder and
polycarbonic acid, the glass ionomers are extremely sensitive to the ingress of
water in the subsequent curing phase. But excess drying should also be avoided.
The chemical processes in curing may be divided into different stages.
1) Decomposition of the glass structure:
A major requirement for the types of glass used is their solubility in acids. Whilst
cross-linked silicates are attacked by virtually no acid, calcium-aluminium-silicate
types of glass even react with a relatively weak polycarbonic acid. The reason for
this is the aluminium component in the glass. Aluminium is integrated into the
cross-linked silicate and ensures that the aluminosilicate acquires a formally
negative charge. As a result the glass turns alkaline and can therefore be attacked
by inorganic acids, but also by organic ones. These negative charges are
compensated for in the glass powder with alkaline ions or alkaline earth ions (see
Fig. 1).
Clinical Research 12/99 7
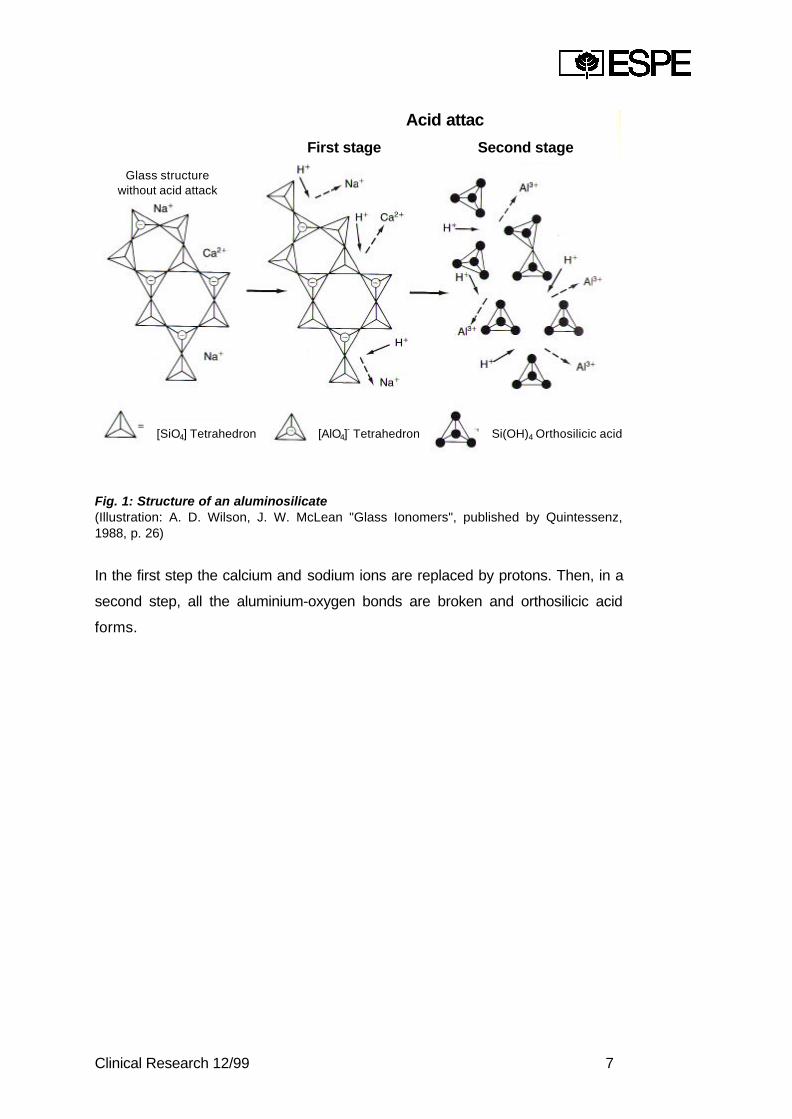
Fig. 1: Structure of an aluminosilicate(Illustration: A. D. Wilson, J. W. McLean "Glass Ionomers", published by Quintessenz,1988, p. 26)
In the first step the calcium and sodium ions are replaced by protons. Then, in a
second step, all the aluminium-oxygen bonds are broken and orthosilicic acid
forms.
Acid attac
Glass structurewithout acid attack
First stage Second stage
[SiO4] Tetrahedron [AlO4]- Tetrahedron Si(OH)4 Orthosilicic acid

Clinical Research 12/99 8
2) Curing
Fig. 2: Formation of the silica gel at the surface of the glass(Ill. A. D. Wilson, J. W McLean, "Glass Ionomers", published by Quintessenz, 1988, p. 45)
Acid attack takes place at the surface of the glass particles. It is a heterogeneous
reaction between a solid and a liquid. The resulting silicic acid reacts
spontaneously with other molecules of silicic acid causing polycondensation to
form a silica gel.
The ions which were originally firmly integrated into the glass are released and
migrate into the aqueous phase of the cement. This effect can be observed, for
example, during the release of fluoride ions from the glass ionomers. The cations
released react with the anions of the polycarbonic acids to form
polycarboxysilates which are insoluble in water.
Clinical Research 12/99 9
3) Action of the tartaric acid
To ensure adequate working time, tartaric acid is used as a complexation reagent
for the dissolved metal ions. The complexation during the first setting period
causes metal ions to be temporarily withdrawn from cross-linking with the
polyanions. This reaction is a reversible process. At the subsequent setting stage
the previously complexed metal ions are again available for cross-linking. In this
way the setting process can be optimised for a practical procedure. Working time
is extended and setting time is reduced ("Snap set").
4. Product Composition
Glass ionomers (polyalkenoate cements) consist of the powder/liquid combination
characteristic of dental cements. Conventional glass ionomers use polycarbonic
acids. The powder component includes special reactive types of glass. The
curing mechanism is an acid-base reaction between these types of glass and the
polycarbonic acid from the liquid.
4.1 Presentation
KETAC MOLAR FOR ART is a two-component, chemically curing, glass ionomerbased restorative material. The product is available both as a capsule version(KETAC MOLAR APLICAP) with its user-friendly direct application feature and asthe successful hand-mix version (KETAC MOLAR FOR ART).
Clinical Research 12/99 10
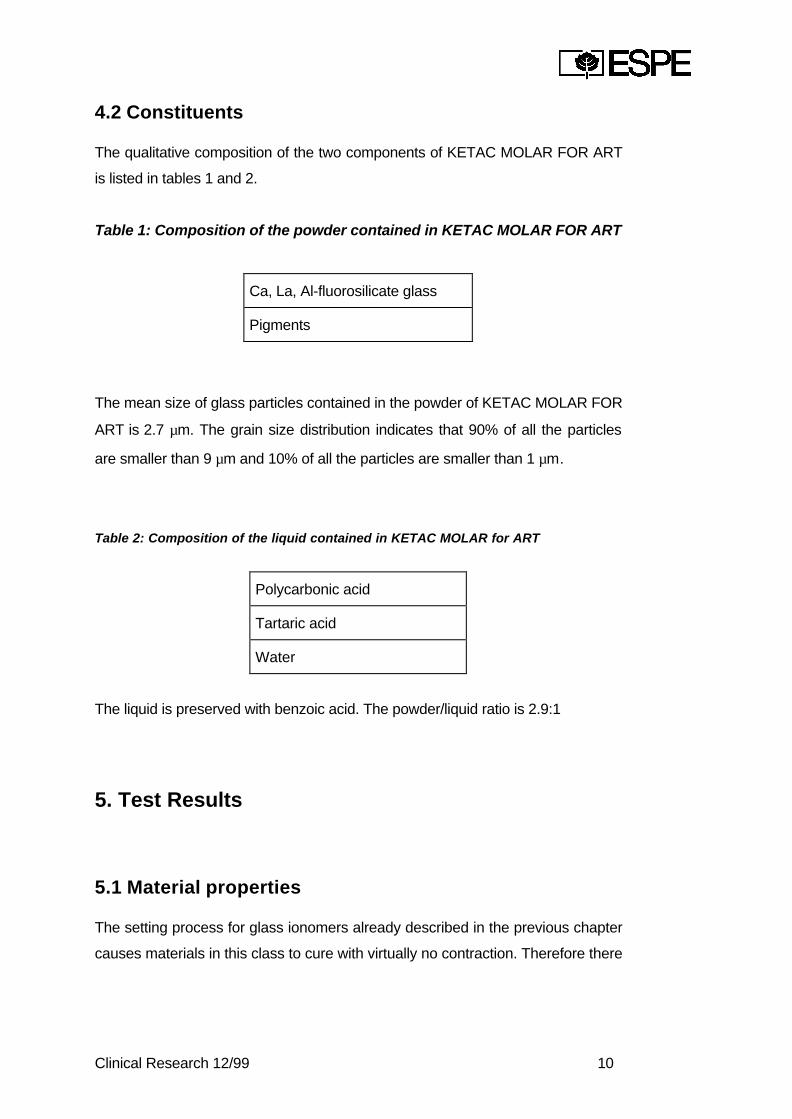
4.2 Constituents
The qualitative composition of the two components of KETAC MOLAR FOR ART
is listed in tables 1 and 2.
Table 1: Composition of the powder contained in KETAC MOLAR FOR ART
Ca, La, Al-fluorosilicate glass
Pigments
The mean size of glass particles contained in the powder of KETAC MOLAR FOR
ART is 2.7 µm. The grain size distribution indicates that 90% of all the particles
are smaller than 9 µm and 10% of all the particles are smaller than 1 µm.
Table 2: Composition of the liquid contained in KETAC MOLAR for ART
Polycarbonic acid
Tartaric acid
Water
The liquid is preserved with benzoic acid. The powder/liquid ratio is 2.9:1
5. Test Results
5.1 Material properties
The setting process for glass ionomers already described in the previous chapter
causes materials in this class to cure with virtually no contraction. Therefore there

Clinical Research 12/99 11
are only minimal stresses in the material which can lead to marginal gap
formation at the cavity margins. For this reason, when using glass ionomers no
additional complex bonding agents have to be applied as is normally necessary
with polymerisation products. Consequently there is no need for a high strength of
bond to the enamel and dentine, which tends to counteract contraction due to
setting.
Furthermore, glass ionomers have a coefficient of thermal expansion which is
similar to that of the teeth. Additional stress on the adhesive bond between the
restorative material and the hard tooth substance caused by large temperature
differences thus does not arise. These two material properties ensure that an
optimised clinical marginal behaviour of glass ionomers can be achieved without
having to specify high bond strength.
Another important material property of glass ionomers is resistance to abrasion.
When using conventional glass ionomers the abrasion/erosion of the restoration,
particularly in the molars and premolars, is a defect which is frequently observed.
In the oral cavity, glass ionomers are subject to chemical and mechanical
degradation. At the point of contact between the restoration and the tooth the
result is formation of "negative ledges". Consequently, for an aesthetically and
clinically attractive restoration it is not only the above-mentioned properties which
are desirable but also high resistance to abrasion.
5.2 Physico-technical data
5.2.1 Internal tests
The physical properties of KETAC MOLAR for ART are listed in table 3. The
figures are based on specification test procedures issued by the International
Standards Organization (ISO) and the German Institute for Standards (DIN).
Clinical Research 12/99 12
KETAC MOLAR is available both as a capsule version (KETAC MOLAR
APLICAP) with its user-friendly direct application feature, and as a tried and tested
hand-mix version (KETAC MOLAR for ART). The physico-technical
characteristics of
KETAC MOLAR APLICAP and KETAC MOLAR for ART are no different from one
another on account of the inaccuracy in measurement. Owing to this analogous
relationship the capsule version results listed in chapter 5 also apply to the hand-
mix version.
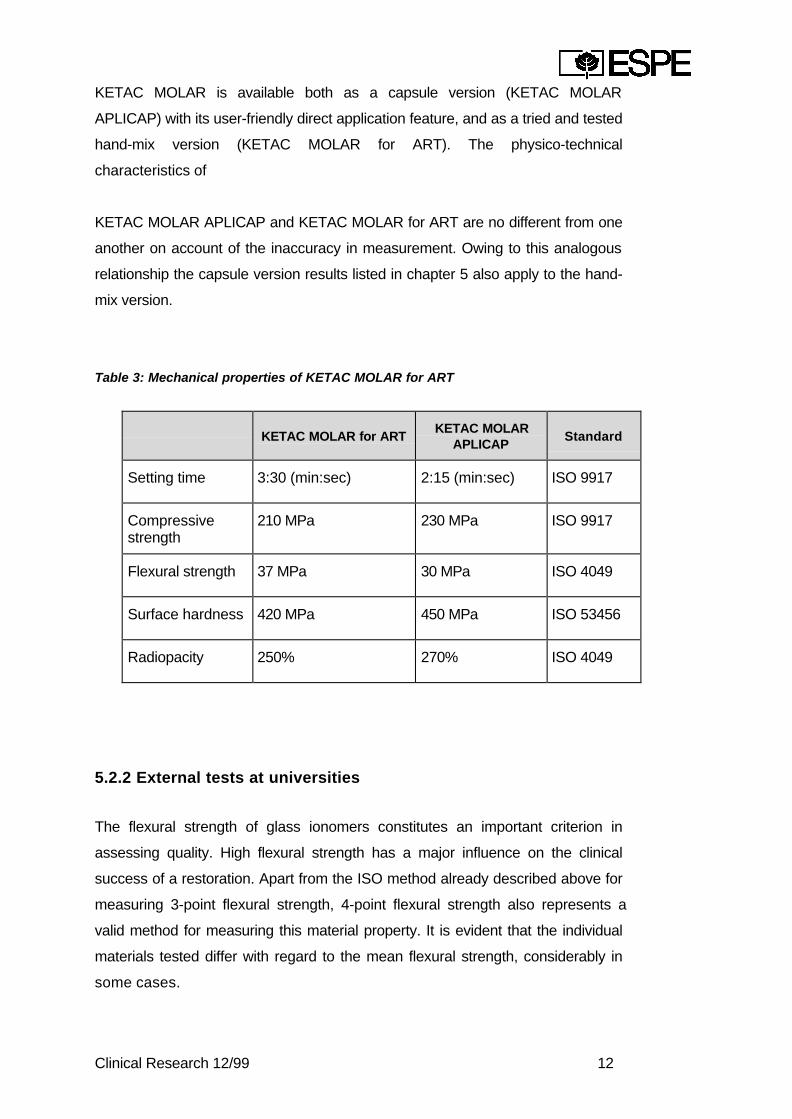
Table 3: Mechanical properties of KETAC MOLAR for ART
KETAC MOLAR for ARTKETAC MOLAR
APLICAPStandard
Setting time 3:30 (min:sec) 2:15 (min:sec) ISO 9917
Compressivestrength
210 MPa 230 MPa ISO 9917
Flexural strength 37 MPa 30 MPa ISO 4049
Surface hardness 420 MPa 450 MPa ISO 53456
Radiopacity 250% 270% ISO 4049
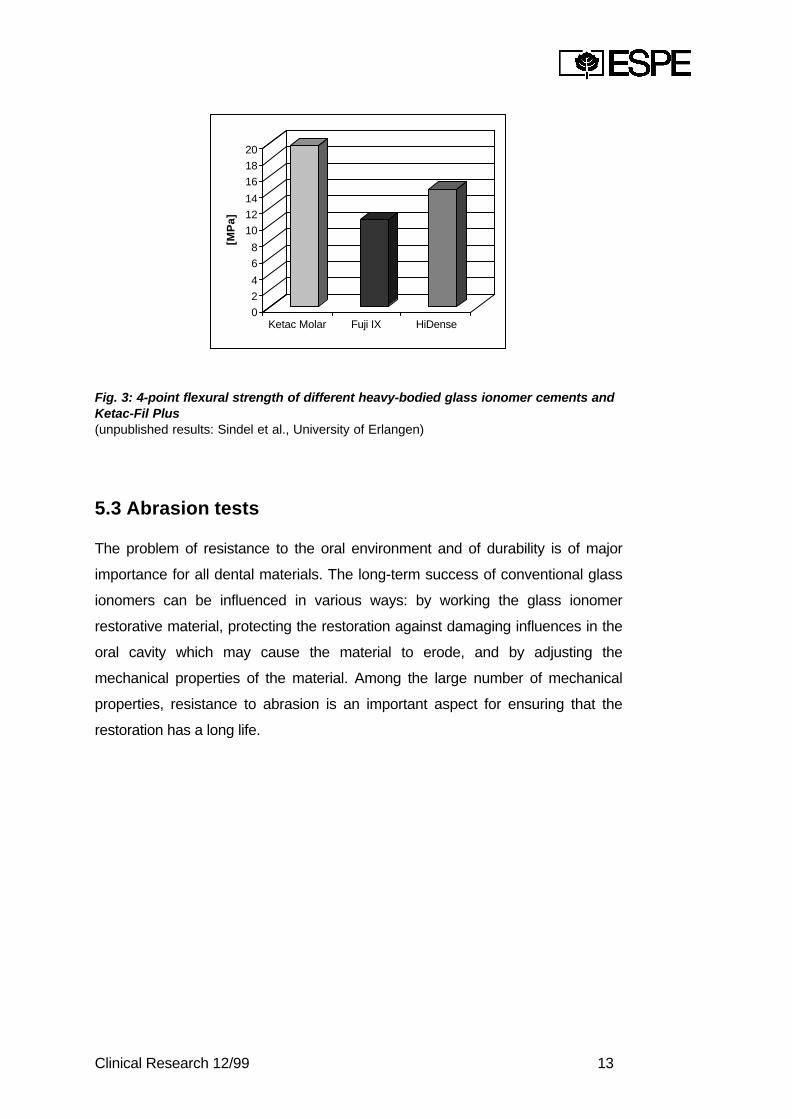
5.2.2 External tests at universities
The flexural strength of glass ionomers constitutes an important criterion in
assessing quality. High flexural strength has a major influence on the clinical
success of a restoration. Apart from the ISO method already described above for
measuring 3-point flexural strength, 4-point flexural strength also represents a
valid method for measuring this material property. It is evident that the individual
materials tested differ with regard to the mean flexural strength, considerably in
some cases.
Clinical Research 12/99 13
0
2
4
6
8
10
12
14
16
18
20
[MP
a]
Ketac Molar Fuji IX HiDense
Fig. 3: 4-point flexural strength of different heavy-bodied glass ionomer cements andKetac-Fil Plus(unpublished results: Sindel et al., University of Erlangen)
5.3 Abrasion tests
The problem of resistance to the oral environment and of durability is of major
importance for all dental materials. The long-term success of conventional glass
ionomers can be influenced in various ways: by working the glass ionomer
restorative material, protecting the restoration against damaging influences in the
oral cavity which may cause the material to erode, and by adjusting the
mechanical properties of the material. Among the large number of mechanical
properties, resistance to abrasion is an important aspect for ensuring that the
restoration has a long life.
Clinical Research 12/99 14
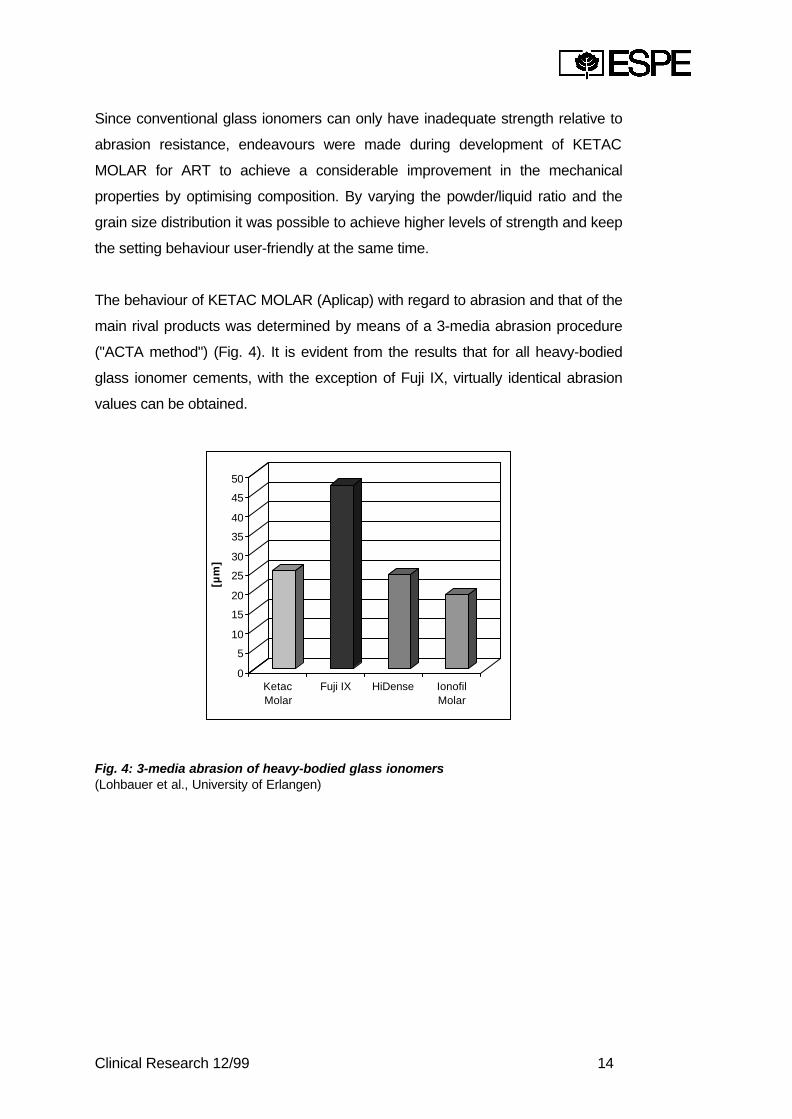
Since conventional glass ionomers can only have inadequate strength relative to
abrasion resistance, endeavours were made during development of KETAC
MOLAR for ART to achieve a considerable improvement in the mechanical
properties by optimising composition. By varying the powder/liquid ratio and the
grain size distribution it was possible to achieve higher levels of strength and keep
the setting behaviour user-friendly at the same time.
The behaviour of KETAC MOLAR (Aplicap) with regard to abrasion and that of the
main rival products was determined by means of a 3-media abrasion procedure
("ACTA method") (Fig. 4). It is evident from the results that for all heavy-bodied
glass ionomer cements, with the exception of Fuji IX, virtually identical abrasion
values can be obtained.
0
5
10
15
20
25
30
35
40
45
50
[µm
]
KetacMolar
Fuji IX HiDense IonofilMolar
Fig. 4: 3-media abrasion of heavy-bodied glass ionomers(Lohbauer et al., University of Erlangen)

Clinical Research 12/99 15
5.4 Adhesion tests
A durable bond between the glass ionomer and the hard tooth substances is
indispensable to ensure the durability of a restoration. Good marginal adaptation
prevents leakages, secondary caries and pulpal irritation. By contrast with the
acid etching technique for composites the adhesion of glass ionomers to the hard
tooth substances is of a purely chemical nature. Micromechanical retention
plays no role whatsoever in the adhesion of glass ionomers. With the proposed
adhesive mechanism, complexation of the carboxylate groups from the glass
ionomer with the calcium ions from the hydroxyl apatite of enamel and dentine is
crucial. Adhesion to the enamel tends to be greater than adhesion to the dentine.
The reason for this is that approx. 98% of enamel and only 70% of dentine is
made of hydroxyl apatite. In the case of dentine, therefore, a glass ionomer chiefly
adheres to the apatite components. There is only minimal or no adhesion
whatsoever to the collagen.
0
1
2
3
4
5
6
[MP
a]
Ketac Molar Fuji IX
Fig. 5: Shear bond strength of KETAC MOLAR to the enamel(K.-H. Friedl et al., University of Regensburg)
Clinical Research 12/99 16
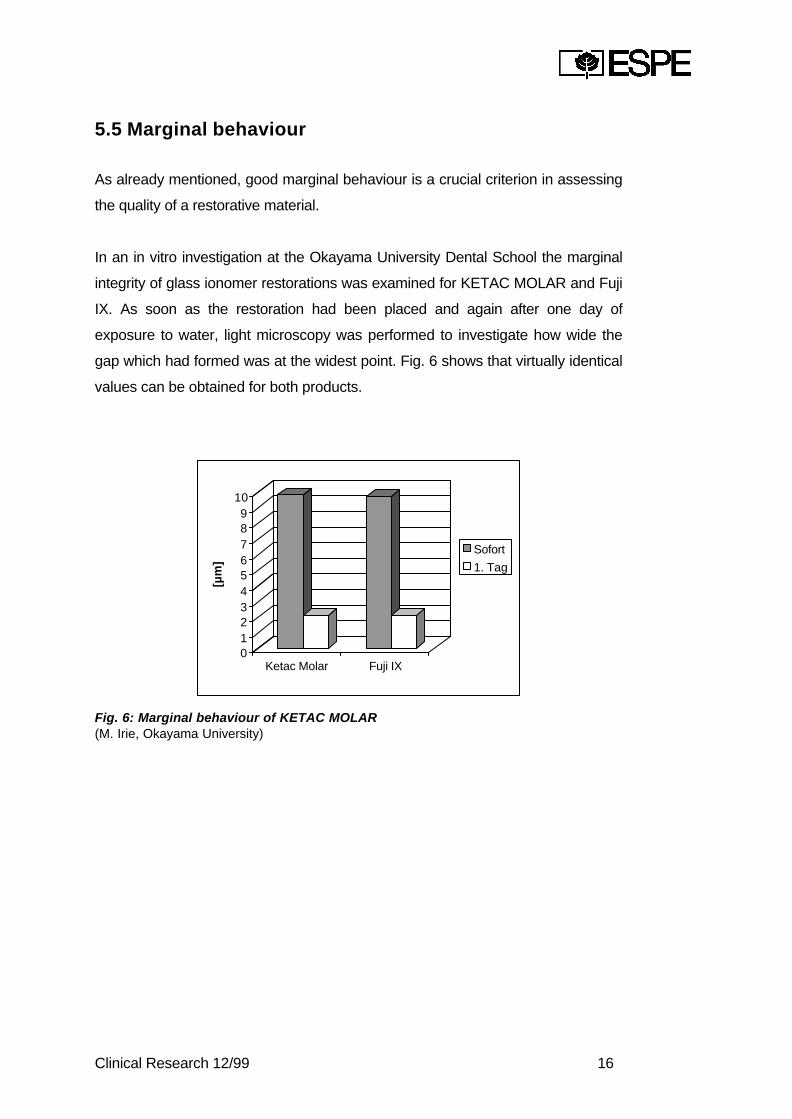
5.5 Marginal behaviour
As already mentioned, good marginal behaviour is a crucial criterion in assessing
the quality of a restorative material.
In an in vitro investigation at the Okayama University Dental School the marginal
integrity of glass ionomer restorations was examined for KETAC MOLAR and Fuji
IX. As soon as the restoration had been placed and again after one day of
exposure to water, light microscopy was performed to investigate how wide the
gap which had formed was at the widest point. Fig. 6 shows that virtually identical
values can be obtained for both products.
0123456789
10
[µm
]
Ketac Molar Fuji IX
Sofort
1. Tag
Fig. 6: Marginal behaviour of KETAC MOLAR(M. Irie, Okayama University)

Clinical Research 12/99 17
5.6 Fluoride release
Glass ionomers are generally characterised by a high release of fluoride. The
clinical relevance of this fluoride release has been discussed controversially for
many years now. Indications that glass ionomers have a cariostatic effect may,
inter alia, be found in a study by Mejàre and Mjör, in which glass ionomers were
used as fissure sealants. In none of the cases investigated was secondary caries
found, although over a total observation period of 5 years a loss rate of 61% in 6-
12 months and a loss rate of 84% in 30-36 months was established for glass
ionomer sealants. By comparison, the rate of caries in the resin sealant control
group was 5% over the same period.
A three-year study which was performed by Karlzén-Reuterving et al. resulted in a
similar picture. Whilst the retention of a resin-reinforced glass ionomer cement
was only 27.8% after three years, caries occurred in only 1.4% of the cases. By
comparison, the rate of caries for a resin sealant was 4.2%, although 79.2% of
the sealants were still present. The authors of that study maintain that the positive
effect of the glass ionomers was due to a cariostatic effect of glass ionomer
materials. Numerous other authors suggest a connection between the provable
fluoride release of glass ionomer cements and their action with regard to caries
prevention.
Clinical Research 12/99 18
0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
1. W
oche
2. W
oche
3. W
oche
4. W
oche
5. W
oche
6. W
oche
7. W
oche
8. W
oche
[pp
m]
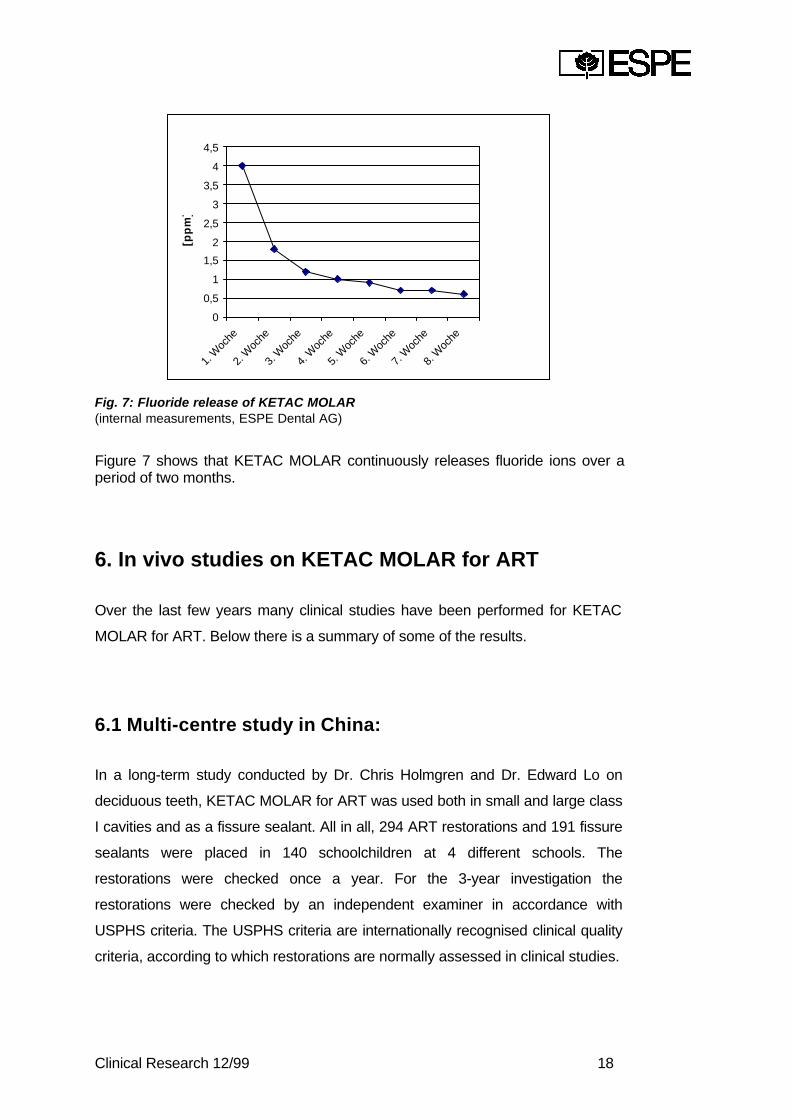
Fig. 7: Fluoride release of KETAC MOLAR(internal measurements, ESPE Dental AG)
Figure 7 shows that KETAC MOLAR continuously releases fluoride ions over aperiod of two months.
6. In vivo studies on KETAC MOLAR for ART
Over the last few years many clinical studies have been performed for KETAC
MOLAR for ART. Below there is a summary of some of the results.
6.1 Multi-centre study in China:
In a long-term study conducted by Dr. Chris Holmgren and Dr. Edward Lo on
deciduous teeth, KETAC MOLAR for ART was used both in small and large class
I cavities and as a fissure sealant. All in all, 294 ART restorations and 191 fissure
sealants were placed in 140 schoolchildren at 4 different schools. The
restorations were checked once a year. For the 3-year investigation the
restorations were checked by an independent examiner in accordance with
USPHS criteria. The USPHS criteria are internationally recognised clinical quality
criteria, according to which restorations are normally assessed in clinical studies.
Clinical Research 12/99 19
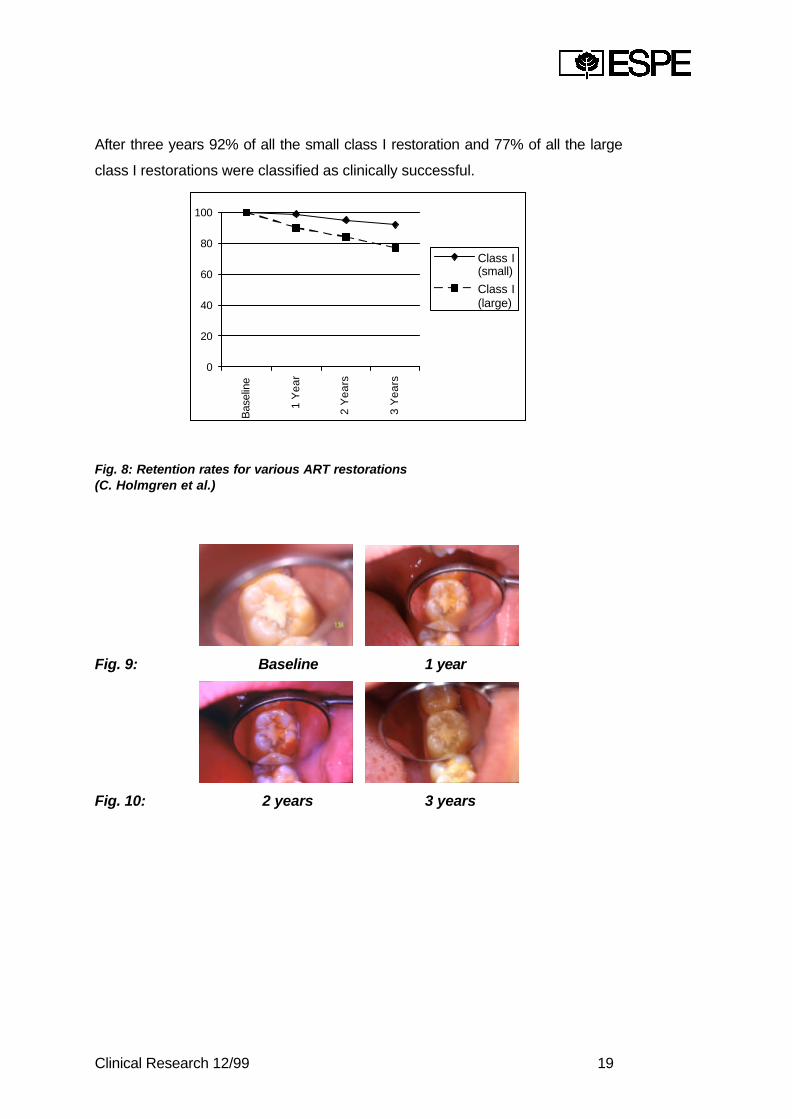
After three years 92% of all the small class I restoration and 77% of all the large
class I restorations were classified as clinically successful.
0
20
40
60
80
100
Bas
elin
e
1 Y
ea
r
2 Y
ea
rs
3 Y
ea
rs
Class I(small)
Class I(large)
Fig. 8: Retention rates for various ART restorations(C. Holmgren et al.)
Fig. 9: Baseline 1 year
Fig. 10: 2 years 3 years
Clinical Research 12/99 20
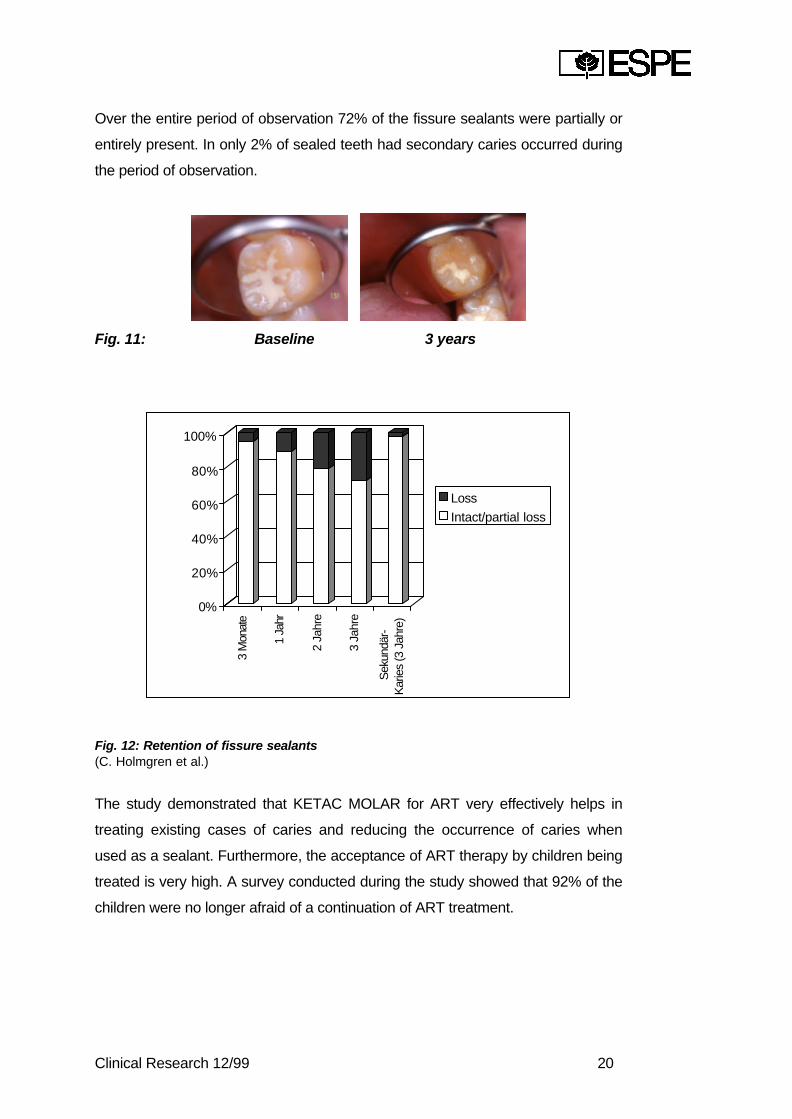
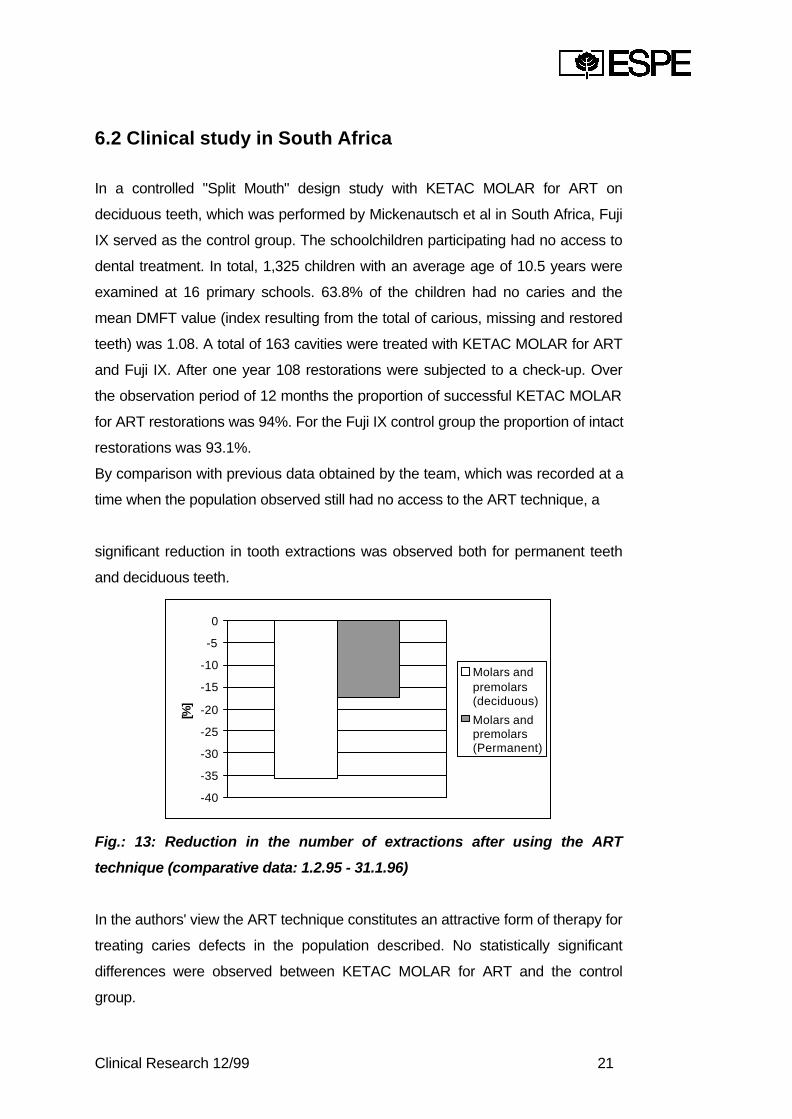
Over the entire period of observation 72% of the fissure sealants were partially or
entirely present. In only 2% of sealed teeth had secondary caries occurred during
the period of observation.
Fig. 11: Baseline 3 years
0%
20%
40%
60%
80%
100%
3 M
onat
e
1 Ja
hr
2 Ja
hre
3 Ja
hre
Sek
undä
r-K
arie
s (3
Jah
re)
Loss
Intact/partial loss
Fig. 12: Retention of fissure sealants(C. Holmgren et al.)
The study demonstrated that KETAC MOLAR for ART very effectively helps in
treating existing cases of caries and reducing the occurrence of caries when
used as a sealant. Furthermore, the acceptance of ART therapy by children being
treated is very high. A survey conducted during the study showed that 92% of the
children were no longer afraid of a continuation of ART treatment.
Clinical Research 12/99 21
6.2 Clinical study in South Africa
In a controlled "Split Mouth" design study with KETAC MOLAR for ART on
deciduous teeth, which was performed by Mickenautsch et al in South Africa, Fuji
IX served as the control group. The schoolchildren participating had no access to
dental treatment. In total, 1,325 children with an average age of 10.5 years were
examined at 16 primary schools. 63.8% of the children had no caries and the
mean DMFT value (index resulting from the total of carious, missing and restored
teeth) was 1.08. A total of 163 cavities were treated with KETAC MOLAR for ART
and Fuji IX. After one year 108 restorations were subjected to a check-up. Over
the observation period of 12 months the proportion of successful KETAC MOLAR
for ART restorations was 94%. For the Fuji IX control group the proportion of intact
restorations was 93.1%.
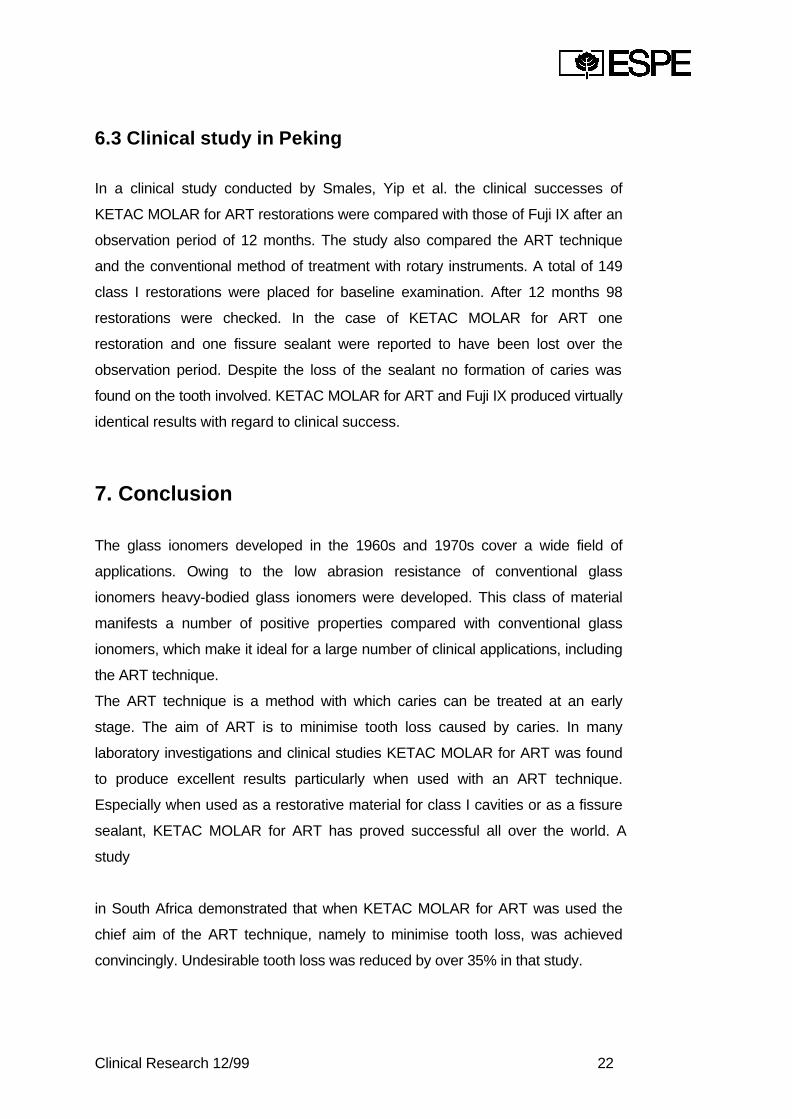
By comparison with previous data obtained by the team, which was recorded at a
time when the population observed still had no access to the ART technique, a
significant reduction in tooth extractions was observed both for permanent teeth
and deciduous teeth.
-40
-35
-30
-25
-20
-15
-10
-5
0
[%]
Molars andpremolars(deciduous)
Molars andpremolars(Permanent)
Fig.: 13: Reduction in the number of extractions after using the ART
technique (comparative data: 1.2.95 - 31.1.96)
In the authors' view the ART technique constitutes an attractive form of therapy for
treating caries defects in the population described. No statistically significant
differences were observed between KETAC MOLAR for ART and the control
group.
Clinical Research 12/99 22
6.3 Clinical study in Peking
In a clinical study conducted by Smales, Yip et al. the clinical successes of
KETAC MOLAR for ART restorations were compared with those of Fuji IX after an
observation period of 12 months. The study also compared the ART technique
and the conventional method of treatment with rotary instruments. A total of 149
class I restorations were placed for baseline examination. After 12 months 98
restorations were checked. In the case of KETAC MOLAR for ART one
restoration and one fissure sealant were reported to have been lost over the
observation period. Despite the loss of the sealant no formation of caries was
found on the tooth involved. KETAC MOLAR for ART and Fuji IX produced virtually
identical results with regard to clinical success.
7. Conclusion
The glass ionomers developed in the 1960s and 1970s cover a wide field of
applications. Owing to the low abrasion resistance of conventional glass
ionomers heavy-bodied glass ionomers were developed. This class of material
manifests a number of positive properties compared with conventional glass
ionomers, which make it ideal for a large number of clinical applications, including
the ART technique.
The ART technique is a method with which caries can be treated at an early
stage. The aim of ART is to minimise tooth loss caused by caries. In many
laboratory investigations and clinical studies KETAC MOLAR for ART was found
to produce excellent results particularly when used with an ART technique.
Especially when used as a restorative material for class I cavities or as a fissure
sealant, KETAC MOLAR for ART has proved successful all over the world. A
study
in South Africa demonstrated that when KETAC MOLAR for ART was used the
chief aim of the ART technique, namely to minimise tooth loss, was achieved
convincingly. Undesirable tooth loss was reduced by over 35% in that study.
Clinical Research 12/99 23
8. Literature
8.1 Clinical studies with KETAC MOLAR for the ARTtechnique
E. C. M. Lo, C.J. Holmgren"Eighteen-month evaluation of ART fillings placed in Chinese preschool children"J. Dent. Res. (IADR Abstract # 2101), 1999.
S. Mickenautsch, M.J. Rudolph, E. O. Ogunbodede"The impact of the ART approach on the treatment profile in a Mobile DentalSystem (MDS) in South Africa"Int. Dent. J. 49, 132-138, 1999.
E.C.M. Lo, C.J. Holmgren, H.C. Wan, D.Y. Hu"Provision of Atraumatic Restorative Treatment (ART) in Western China -one year results"J. Dent. Res. (IADR Abstract # 37), 1998.
W. Gao, D. Peng, R.J. Smales, M.S. Gale„Clinical trial of ART technique restorative Gl cements: initial findings"J. Dent. Res. (IADR Abstract # 40), 1998.
8.2 General literature on Ketac Molar
U. Lohbauer, M. Pelka, R. Frankenberger, N. Krämer"Influence of Mixing Procedures on Wear Resistance of Glass IonomerCements"J. Dent. Res. (IADR Abstract # 988), 1999.
R. Frankenberger, N. Krämer, A. Graf, A. Petschelt"Zyklische Ermüdung von Glasionomerzementen und Kompomeren"Dtsch. Zahnärztl. Z. 54, 269-271, 1999.
M. Pelka, J. Sindel, A. Petschelt"Lapping Abrasion Behavior of Condensable Glass-ionomers"J. Dent. Res. (IADR Abstract # 2739), 1999.
M. Irie, T. Yamada, H. Nakai"Marginal Adaptation of High-viscosity Glass lonomers in Enamel Margins"J. Dent. Res. (IADR Abstract # 1452), 1998.
C.C. France, M.R. Towler, R.W. Billington"Correlation between erosion and stress relaxation in maturing glass-ionomers"J. Dent. Res. (IADR Abstract # 463), 1998.

Clinical Research 12/99 24
M.C.P. Nunes, D.F.G. Cefaly, L. Tenuta, J.R.P. Lauris, M.F.L. Navarro"Compressive and Diametral Tensile Strength of Two Restorative Glasslonomer Cements"J.J. Dent. Res. (IADR Abstract # 458), 1998.
K.-P. Stefan"Early solubility of glass ionomer cements"J. Dent. Res. (IADR Abstract # 454), 1998.
J. Ellacuria, R. Triana, N. Minguez, E. Guinea, F. Soler, F. Garcia-Godoy"Effects of Aging Time on Microhardness of Glass Ionomer Cements"J. Dent. Res. (IADR Abstract # 459), 1998.
T.F. Watson, M. Naasan, M. Sherriff"Maturation of Glass Ionomer Cements and Shear Bond Strength (SBS)J. Dent. Res. (IADR Abstract # 384) 1998.
A. Peutzfeldt, F. Garcia-Godoy, E. Asmussen"Surface hardness and wear of glass ionomers and compomers"Am. J. Dent. 10. 15-17, 1997.
K.-H. Friedl, G. Schmalz, K.-A. Hiller, A. Gottlieb"Bond Strength of resin modified glass ionomer cements and compomers"J. Dent. Res. (IADR Abstract # 2400), 1997.
A. Graf, J. Sindel, N. Krämer, A. Petschelt"Wear and Cyclic Fatigue of new Glass Ionomer Cements"J. Dent. Res. (IADR Abstract # 2427), 1997.
R. Frankenberger, J. Sindel, N. Krämer"Stopfbare Glasionomerzemente - eine neue Amalgamalternative imMilchgebiß?"Quintessenz 47, 1535-1549, 1996.
8.2 Further literature
l. Mejàre, I.A. Mjör"Glass ionomer and resin-based fissure sealants: a clinical study"Scand. J. Dent. Res. 98, 345-350, 1990.
G. KarIzén-Reuterving, J.W.V. van Dijken"A three-year follow-up of glass (ionomer cement and resin fissure sealants"Journal of dentistry for children, 108-110, 1995.


























![Ketac(TM)-Cem Glass Ionomer Cement€¦ · GIZe [Ketac Molar Quick; Fuji IX Fast] 2001 Leicht mischbare GIZe [Ketac Cem µ] 7 Abbildung 2: Einteilung der Zemente Werkstoffkundliche](https://img.pdfslide.net/doc/110x75/5f0747457e708231d41c31cb/ketactm-cem-glass-ionomer-cement-gize-ketac-molar-quick-fuji-ix-fast-2001-leicht.jpg)