Upload
whinolyn-jardeleza
View
222
Download
1
Embed Size (px)
Citation preview
8/7/2019 The Kidneys and How They Work
1/33
The Kidneys and How They Work On this page:
What do the kidneys do? What is renal function? Why do kidneys fail? How do kidneys fail? What are the signs of chronic kidney disease (CKD)? What medical tests detect kidney disease? What are the stages of CKD? What can be done about CKD? What happens if the kidneys fail completely? Points to Remember Hope through Research For More Information Acknowledgments
The kidneys are a pair of vital organs that perform many functions to keep the bloodclean and chemically balanced. Understanding how the kidneys work can help a personkeep them healthy.
What do the kidneys do?
The kidneys are bean-shaped organs, each about the size of a fist. They are located near
the middle of the back, just below the rib cage, one on each side of the spine. Thekidneys are sophisticated reprocessing machines. Every day, a persons kidneys
process about 200 quarts of blood to sift out about 2 quarts of waste products and extrawater. The wastes and extra water become urine, which flows to the bladder throughtubes called ureters. The bladder stores urine until releasing it through urination.
The kidneys remove wastes and water from the blood to form urine. Urine flows fromthe kidneys to the bladder through the ureters.
Wastes in the blood come from the normal breakdown of active tissues, such as
muscles, and from food. The body uses food for energy and self-repairs. After the bodyhas taken what it needs from food, wastes are sent to the blood. If the kidneys did notremove them, these wastes would build up in the blood and damage the body.
The actual removal of wastes occurs in tiny units inside the kidneys called nephrons.Each kidney has about a million nephrons. In the nephron, a glomeruluswhich is atiny blood vessel, or capillaryintertwines with a tiny urine-collecting tube called atubule. The glomerulus acts as a filtering unit, or sieve, and keeps normal proteins and
http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#kidneyshttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#renalhttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#whyhttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#howhttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#signshttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#testshttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#stageshttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#CKDhttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#failhttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#pointshttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#hopehttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#infohttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#acknowledgmentshttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#renalhttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#whyhttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#howhttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#signshttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#testshttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#stageshttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#CKDhttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#failhttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#pointshttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#hopehttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#infohttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#acknowledgmentshttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#kidneys8/7/2019 The Kidneys and How They Work
2/33
cells in the bloodstream, allowing extra fluid and wastes to pass through. Acomplicated chemical exchange takes place, as waste materials and water leave the
blood and enter the urinary system.
In the nephron (left), tiny blood vessels intertwine with urine-collecting tubes. Eachkidney contains about 1 million nephrons.
At first, the tubules receive a combination of waste materials and chemicals the bodycan still use. The kidneys measure out chemicals like sodium, phosphorus, and
potassium and release them back to the blood to return to the body. In this way, thekidneys regulate the bodys level of these substances. The right balance is necessary for life.
In addition to removing wastes, the kidneys release three important hormones:
erythropoietin, or EPO, which stimulates the bone marrow to make red bloodcells
renin, which regulates blood pressure calcitriol, the active form of vitamin D, which helps maintain calcium for bones
and for normal chemical balance in the body
[Top ]
What is renal function?
The word renal refers to the kidneys. The terms renal function and kidneyfunction mean the same thing. Health professionals use the term renal function totalk about how efficiently the kidneys filter blood. People with two healthy kidneyshave 100 percent of their kidney function. Small or mild declines in kidney function as much as 30 to 40 percentwould rarely be noticeable. Kidney function is nowcalculated using a blood sample and a formula to find the estimated glomerular filtration rate (eGFR). The eGFR corresponds to the percent of kidney functionavailable. The section What medical tests detect kidney disease? contains moredetails about the eGFR.
Some people are born with only one kidney but can still lead normal, healthy lives.
Every year, thousands of people donate one of their kidneys for transplantation to afamily member or friend.
For many people with reduced kidney function, a kidney disease is also present andwill get worse. Serious health problems occur when people have less than 25 percent of their kidney function. When kidney function drops below 10 to 15 percent, a personneeds some form of renal replacement therapyeither blood-cleansing treatments
http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#tophttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#testshttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#testshttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#tophttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#tests8/7/2019 The Kidneys and How They Work
3/33
called dialysis or a kidney transplantto sustain life.
Why do kidneys fail?
Most kidney diseases attack the nephrons, causing them to lose their filtering capacity.Damage to the nephrons can happen quickly, often as the result of injury or poisoning.But most kidney diseases destroy the nephrons slowly and silently. Only after years or even decades will the damage become apparent. Most kidney diseases attack bothkidneys simultaneously.
The two most common causes of kidney disease are diabetes and high blood pressure.People with a family history of any kind of kidney problem are also at risk for kidneydisease.
Diabetic Kidney Disease
Diabetes is a disease that keeps the body from using glucose, a form of sugar, as itshould. If glucose stays in the blood instead of breaking down, it can act like a poison.Damage to the nephrons from unused glucose in the blood is called diabetic kidneydisease. Keeping blood glucose levels down can delay or prevent diabetic kidneydisease. Use of medications called angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) to treat high blood pressure can also slow or delay the progression of diabetic kidney disease.
High Blood Pressure
High blood pressure can damage the small blood vessels in the kidneys. The damagedvessels cannot filter wastes from the blood as they are supposed to.
A doctor may prescribe blood pressure medication. ACE inhibitors and ARBs have been found to protect the kidneys even more than other medicines that lower blood pressure to similar levels. The National Heart, Lung, and Blood Institute (NHLBI), oneof the National Institutes of Health, recommends that people with diabetes or reducedkidney function keep their blood pressure below 130/80.
Glomerular Diseases
Several types of kidney disease are grouped together under this category, includingautoimmune diseases, infection-related diseases, and sclerotic diseases. As the nameindicates, glomerular diseases attack the tiny blood vessels, or glomeruli, within thekidney. The most common primary glomerular diseases include membranousnephropathy, IgA nephropathy, and focal segmental glomerulosclerosis. The first signof a glomerular disease is often proteinuria, which is too much protein in the urine.Another common sign is hematuria, which is blood in the urine. Some people mayhave both proteinuria and hematuria. Glomerular diseases can slowly destroy kidney
8/7/2019 The Kidneys and How They Work
4/33
function. Blood pressure control is important with any kidney disease. Glomerular diseases are usually diagnosed with a biopsya procedure that involves taking a pieceof kidney tissue for examination with a microscope. Treatments for glomerular diseasesmay include immunosuppressive drugs or steroids to reduce inflammation and
proteinuria, depending on the specific disease.
Inherited and Congenital Kidney Diseases
Some kidney diseases result from hereditary factors. Polycystic kidney disease (PKD),for example, is a genetic disorder in which many cysts grow in the kidneys. PKD cystscan slowly replace much of the mass of the kidneys, reducing kidney function andleading to kidney failure.
Some kidney problems may show up when a child is still developing in the womb.Examples include autosomal recessive PKD, a rare form of PKD, and other
developmental problems that interfere with the normal formation of the nephrons. Thesigns of kidney disease in children vary. A child may grow unusually slowly, vomitoften, or have back or side pain. Some kidney diseases may be silentcausing no signsor symptomsfor months or even years.
If a child has a kidney disease, the childs doctor should find it during a regular checkup. The first sign of a kidney problem may be high blood pressure; a low number of red blood cells, called anemia; proteinuria; or hematuria. If the doctor finds any of these problems, further tests may be necessary, including additional blood and urinetests or radiology studies. In some cases, the doctor may need to perform a biopsy.
Some hereditary kidney diseases may not be detected until adulthood. The mostcommon form of PKD was once called adult PKD because the symptoms of high
blood pressure and renal failure usually do not occur until patients are in their twentiesor thirties. But with advances in diagnostic imaging technology, doctors have foundcysts in children and adolescents before any symptoms appear.
Other Causes of Kidney Disease
Poisons and trauma, such as a direct and forceful blow to the kidneys, can lead tokidney disease.
Some over-the-counter medicines can be poisonous to the kidneys if taken regularlyover a long period of time. Anyone who takes painkillers regularly should check with adoctor to make sure the kidneys are not at risk.
[Top ]
How do kidneys fail?
http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#tophttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#top8/7/2019 The Kidneys and How They Work
5/33
Many factors that influence the speed of kidney failure are not completely understood.Researchers are still studying how protein in the diet and cholesterol levels in the bloodaffect kidney function.
Acute Kidney Injury
Some kidney problems happen quickly, such as when an accident injures the kidneys.Losing a lot of blood can cause sudden kidney failure. Some drugs or poisons canmake the kidneys stop working. These sudden drops in kidney function are called acutekidney injury (AKI). Some doctors may also refer to this condition as acute renalfailure (ARF).
AKI may lead to permanent loss of kidney function. But if the kidneys are notseriously damaged, acute kidney disease may be reversed.
Chronic Kidney Disease
Most kidney problems, however, happen slowly. A person may have silent kidneydisease for years. Gradual loss of kidney function is called chronic kidney disease(CKD) or chronic renal insufficiency. People with CKD may go on to develop
permanent kidney failure. They also have a high risk of death from a stroke or heartattack.
End-stage Renal Disease
Total or nearly total and permanent kidney failure is called end-stage renal disease
(ESRD). People with ESRD must undergo dialysis or transplantation to stay alive.
[Top ]
What are the signs of chronic kidney disease (CKD)?
People in the early stages of CKD usually do not feel sick at all.
People whose kidney disease has gotten worse may
need to urinate more often or less often feel tired lose their appetite or experience nausea and vomiting have swelling in their hands or feet feel itchy or numb get drowsy or have trouble concentrating have darkened skin have muscle cramps
http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#tophttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#top8/7/2019 The Kidneys and How They Work
6/33
[Top ]
What medical tests detect kidney disease?
Because a person can have kidney disease without any symptoms, a doctor may firstdetect the condition through routine blood and urine tests. The National KidneyFoundation recommends three simple tests to screen for kidney disease: a blood
pressure measurement, a spot check for protein or albumin in the urine, and acalculation of glomerular filtration rate (GFR) based on a serum creatininemeasurement. Measuring urea nitrogen in the blood provides additional information.
Blood Pressure Measurement
High blood pressure can lead to kidney disease. It can also be a sign that the kidneysare already impaired. The only way to know whether a persons blood pressure is highis to have a health professional measure it with a blood pressure cuff. The result isexpressed as two numbers. The top number, which is called the systolic pressure,represents the pressure in the blood vessels when the heart is beating. The bottomnumber, which is called the diastolic pressure, shows the pressure when the heart isresting between beats. A persons blood pressure is considered normal if it stays below120/80, stated as 120 over 80. The NHLBI recommends that people with kidneydisease use whatever therapy is necessary, including lifestyle changes and medicines,to keep their blood pressure below 130/80.
Microalbuminuria and Proteinuria
Healthy kidneys take wastes out of the blood but leave protein. Impaired kidneys mayfail to separate a blood protein called albumin from the wastes. At first, only smallamounts of albumin may leak into the urine, a condition known as microalbuminuria, asign of deteriorating kidney function. As kidney function worsens, the amount of albumin and other proteins in the urine increases, and the condition is called
proteinuria. A doctor may test for protein using a dipstick in a small sample of a persons urine taken in the doctors office. The color of the dipstick indicates the presence or absence of proteinuria.
A more sensitive test for protein or albumin in the urine involves laboratorymeasurement and calculation of the protein-to-creatinine or albumin-to-creatinine ratio.
Creatinine is a waste product in the blood created by the normal breakdown of musclecells during activity. Healthy kidneys take creatinine out of the blood and put it into theurine to leave the body. When the kidneys are not working well, creatinine builds up inthe blood.
The albumin-to-creatinine measurement should be used to detect kidney disease in people at high risk, especially those with diabetes or high blood pressure. If a personsfirst laboratory test shows high levels of protein, another test should be done 1 to 2
http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#tophttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#top8/7/2019 The Kidneys and How They Work
7/33
weeks later. If the second test also shows high levels of protein, the person has persistent proteinuria and should have additional tests to evaluate kidney function.
Glomerular Filtration Rate (GFR) Based on Creatinine Measurement
GFR is a calculation of how efficiently the kidneys are filtering wastes from the blood.A traditional GFR calculation requires an injection into the bloodstream of a substancethat is later measured in a 24-hour urine collection. Recently, scientists found theycould calculate GFR without an injection or urine collection. The new calculationtheeGFRrequires only a measurement of the creatinine in a blood sample.
In a laboratory, a persons blood is tested to see how many milligrams of creatinine arein one deciliter of blood (mg/dL). Creatinine levels in the blood can vary, and eachlaboratory has its own normal range, usually 0.6 to 1.2 mg/dL. A person whosecreatinine level is only slightly above this range will probably not feel sick, but the
elevation is a sign that the kidneys are not working at full strength. One formula for estimating kidney function equates a creatinine level of 1.7 mg/dL for most men and1.4 mg/dL for most women to 50 percent of normal kidney function. But becausecreatinine values are so variable and can be affected by diet, a GFR calculation is moreaccurate for determining whether a person has reduced kidney function.
The eGFR calculation uses the patients creatinine measurement along with age andvalues assigned for sex and race. Some medical laboratories may make the eGFR calculation when a creatinine value is measured and include it on the lab report. The
National Kidney Foundation has determined different stages of CKD based on thevalue of the eGFR. Dialysis or transplantation is needed when the eGFR is less than 15
milliliters per minute (mL/min).
Blood Urea Nitrogen (BUN)
Blood carries protein to cells throughout the body. After the cells use the protein, theremaining waste product is returned to the blood as urea, a compound that containsnitrogen. Healthy kidneys take urea out of the blood and put it in the urine. If a
persons kidneys are not working well, the urea will stay in the blood.
A deciliter of normal blood contains 7 to 20 milligrams of urea. If a persons BUN ismore than 20 mg/dL, the kidneys may not be working at full strength. Other possible
causes of an elevated BUN include dehydration and heart failure.
Additional Tests for Kidney Disease
If blood and urine tests indicate reduced kidney function, a doctor may recommendadditional tests to help identify the cause of the problem.
Kidney imaging. Methods of kidney imagingtaking pictures of the kidneys
8/7/2019 The Kidneys and How They Work
8/33
include ultrasound, computerized tomography (CT) scan, and magnetic resonanceimaging (MRI). These tools are most helpful in finding unusual growths or blockagesto the flow of urine.
Kidney biopsy. A doctor may want to examine a tiny piece of kidney tissue with amicroscope. To obtain this tissue sample, the doctor will perform a kidney biopsyahospital procedure in which the doctor inserts a needle through the patients skin intothe back of the kidney. The needle retrieves a strand of tissue less than an inch long.For the procedure, the patient lies facedown on a table and receives a local anesthetic tonumb the skin. The sample tissue will help the doctor identify problems at the cellular level.
For more information, see the fact sheet Kidney Biopsy from the National Kidney andUrologic Diseases Information Clearinghouse.
[Top ]
What are the stages of CKD?
A persons eGFR is the best indicator of how well the kidneys are working. An eGFR of 90 or above is considered normal. A person whose eGFR stays below 60 for 3months or longer has CKD. As kidney function declines, the risk of complicationsrises.
Moderate decrease in eGFR (30 to 59). At this stage of CKD, hormones and mineralscan be thrown out of balance, leading to anemia and weak bones. A health care
provider can help prevent or treat these complications with medicines and advice aboutfood choices.
Severe reduction in eGFR (15 to 29). The patient should continue following thetreatment for complications of CKD and learn as much as possible about the treatmentsfor kidney failure. Each treatment requires preparation. Those who choosehemodialysis will need to have a procedure to make veins in their arms larger andstronger for repeated needle insertions. For peritoneal dialysis, one will need to have acatheter placed in the abdomen. A catheter is a thin, flexible tube used to fill theabdominal cavity with fluid. A person may want to ask family or friends to consider donating a kidney for transplantation.
Kidney failure (eGFR less than 15). When the kidneys do not work well enough tomaintain life, dialysis or a kidney transplant will be needed.
In addition to tracking eGFR, blood tests can show when substances in the blood areout of balance. If phosphorus or potassium levels start to climb, a blood test will
prompt the health care provider to address these issues before they permanently affect
http://kidney.niddk.nih.gov/kudiseases/pubs/biopsy/index.htmhttp://kidney.niddk.nih.gov/kudiseases/pubs/biopsy/index.htmhttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#tophttp://kidney.niddk.nih.gov/kudiseases/pubs/biopsy/index.htmhttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#top8/7/2019 The Kidneys and How They Work
9/33
the persons health.
[Top ]
What can be done about CKD?
Unfortunately, CKD often cannot be cured. But people in the early stages of CKD may be able to make their kidneys last longer by taking certain steps. They will also want tominimize the risks for heart attack and stroke because CKD patients are susceptible tothese problems.
People with reduced kidney function should see their doctor regularly. The primary doctor may refer the patient to a nephrologist, a doctor who specializesin kidney disease.
People who have diabetes should watch their blood glucose levels closely tokeep them under control. They should ask their health care provider about thelatest in treatment.
People with reduced renal function should avoid pain pills that may make their kidney disease worse. They should check with their health care provider beforetaking any medicine.
Controlling Blood Pressure
People with reduced kidney function and high blood pressure should control their blood pressure with an ACE inhibitor or an ARB. Many people will require two or more types of medication to keep their blood pressure below 130/80. A diuretic is an
important addition when the ACE inhibitor or ARB does not meet the blood pressuregoal.
Changing the Diet
People with reduced kidney function need to be aware that some parts of a normal dietmay speed their kidney failure.
Protein. Protein is important to the body. It helps the body repair muscles and fightdisease. Protein comes mostly from meat but can also be found in eggs, milk, nuts,
beans, and other foods. Healthy kidneys take wastes out of the blood but leave in the
protein. Impaired kidneys may fail to separate the protein from the wastes.
Some doctors tell their kidney patients to limit the amount of protein they eat so thekidneys have less work to do. But a person cannot avoid protein entirely. People withCKD can work with a dietitian to create the right food plan.
Cholesterol. Another problem that may be associated with kidney failure is high
http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#tophttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#top8/7/2019 The Kidneys and How They Work
10/33
cholesterol. High levels of cholesterol in the blood may result from a high-fat diet.
Cholesterol can build up on the inside walls of blood vessels. The buildup makes pumping blood through the vessels harder for the heart and can cause heart attacks and
strokes.
Sodium. Sodium is a chemical found in salt and other foods. Sodium in the diet mayraise a persons blood pressure, so people with CKD should limit foods that containhigh levels of sodium. High-sodium foods include canned or processed foods likefrozen dinners and hot dogs.
Potassium. Potassium is a mineral found naturally in many fruits and vegetables, suchas oranges, potatoes, bananas, dried fruits, dried beans and peas, and nuts. Healthykidneys measure potassium in the blood and remove excess amounts. Diseased kidneysmay fail to remove excess potassium. With very poor kidney function, high potassium
levels can affect the heart rhythm.
Not Smoking
Smoking not only increases the risk of kidney disease, but it also contributes to deathsfrom strokes and heart attacks in people with CKD.
Treating Anemia
Anemia is a condition in which the blood does not contain enough red blood cells.These cells are important because they carry oxygen throughout the body. A person
who is anemic will feel tired and look pale. Healthy kidneys make the hormone EPO,which stimulates the bones to make red blood cells. Diseased kidneys may not makeenough EPO. A person with CKD may need to take injections of a form of EPO.
Preparing for End-stage Renal Disease (ESRD)
As kidney disease progresses, a person needs to make several decisions. People in thelater stages of CKD need to learn about their options for treating the last stages of kidney failure so they can make an informed choice between hemodialysis, peritonealdialysis, and transplantation.
[Top ]
What happens if the kidneys fail completely?
Total or nearly total and permanent kidney failure is called ESRD. If a personskidneys stop working completely, the body fills with extra water and waste products.This condition is called uremia. Hands or feet may swell. A person will feel tired and
http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#tophttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#top8/7/2019 The Kidneys and How They Work
11/33
weak because the body needs clean blood to function properly.
Untreated uremia may lead to seizures or coma and will ultimately result in death. A person whose kidneys stop working completely will need to undergo dialysis or kidney
transplantation.
Dialysis
The two major forms of dialysis are hemodialysis and peritoneal dialysis.Hemodialysis uses a special filter called a dialyzer that functions as an artificial kidneyto clean a persons blood. The dialyzer is a canister connected to the hemodialysismachine. During treatment, the blood travels through tubes into the dialyzer, whichfilters out wastes, extra salt, and extra water. Then the cleaned blood flows throughanother set of tubes back into the body. The hemodialysis machine monitors bloodflow and removes wastes from the dialyzer. Hemodialysis is usually performed at a
dialysis center three times per week for 3 to 4 hours. A small but growing number of clinics offer home hemodialysis in addition to standard in-clinic treatments. The patientfirst learns to do treatments at the clinic, working with a dialysis nurse. Daily homehemodialysis is done 5 to 7 days per week for 2 to 3 hours at a time. Nocturnal dialysiscan be performed for 8 hours at night while a person sleeps. Research as to which is the
best method for dialysis is under way, but preliminary data indicate that daily dialysisschedules such as short daily dialysis or nocturnal dialysis may be the best form of dialysis therapy.
Hemodialysis
In peritoneal dialysis, a fluid called dialysis solution is put into the abdomen. This fluidcaptures the waste products from a persons blood. After a few hours when the fluid isnearly saturated with wastes, the fluid is drained through a catheter. Then, a fresh bagof fluid is dripped into the abdomen to continue the cleansing process. Patients can
perform peritoneal dialysis themselves. Patients using continuous ambulatory peritoneal dialysis (CAPD) change fluid four times a day. Another form of peritonealdialysis, called continuous cycling peritoneal dialysis (CCPD), can be performed atnight with a machine that drains and refills the abdomen automatically.
Peritoneal dialysis
Transplantation
A donated kidney may come from an anonymous donor who has recently died or froma living person, usually a relative. The kidney must be a good match for the patients
body. The more the new kidney is like the person receiving the kidney, the less likelythe immune system is to reject it. The immune system protects a person from disease
8/7/2019 The Kidneys and How They Work
12/33
by attacking anything that is not recognized as a normal part of the body. So theimmune system will attack a kidney that appears too foreign. The patient will takespecial drugs to help trick the immune system so it does not reject the transplantedkidney. Unless they are causing infection or high blood pressure, the diseased kidneys
are left in place. Kidneys from living, related donors appear to be the best match for success, but kidneys from unrelated people also have a long survival rate. Patientsapproaching kidney failure should ask their doctor early about starting the process toreceive a kidney transplant.
Kidney transplantation
Points to Remember
The kidneys are two vital organs that keep the blood clean and chemically balanced.
Kidney disease can be detected through a spot check for protein or albumin inthe urine and a calculation of glomerular filtration rate (GFR) based on a bloodtest.
The progression of kidney disease can be slowed, but it cannot always bereversed.
End-stage renal disease (ESRD) is the total or nearly total and permanent lossof kidney function.
Dialysis and transplantation can extend the lives of people with kidney failure. Diabetes and high blood pressure are the two leading causes of kidney failure. People with reduced kidney function should see their doctor regularly. Doctors
who specialize in kidney disease are called nephrologists. Chronic kidney disease (CKD) increases the risk of heart attacks and strokes. People in the early stages of CKD may be able to save their remaining kidney
function for many years byo controlling their blood glucoseo controlling their blood pressureo following a low-protein dieto maintaining healthy levels of cholesterol in the bloodo taking an angiotensin-converting enzyme (ACE) inhibitor or an
angiotensin receptor blocker (ARB)o not smoking
[Top ]
Hope through Research
As understanding of the causes of kidney failure increases, so does the ability to predictand prevent these diseases. Recent studies have shown that intensive control of
http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#tophttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#top8/7/2019 The Kidneys and How They Work
13/33
diabetes and high blood pressure can prevent or delay the onset of kidney disease.
In the area of genetics, researchers supported by the National Institute of Diabetes andDigestive and Kidney Diseases (NIDDK) have located two genes that cause the most
common form of PKD and learned that a person must have two defective copies of the PKD1 gene to develop PKD. Researchers have also found a gene in the roundwormthat is identical to the PKD1 gene. This new knowledge will be used in the search for effective therapies to prevent or treat PKD.
In the area of transplantation, new drugs to help the body accept foreign tissue increasethe likelihood that a transplanted kidney will survive and function properly. Scientistsat the NIDDK are also developing new techniques to induce a persons tolerance for foreign tissue before receiving a transplanted organ. This technique will eliminate or reduce the need for immunosuppressive drugs and thereby reduce expense andcomplications. In the future, scientists may develop an artificial kidney for
implantation.
Participants in clinical trials can play a more active role in their own health care, gainaccess to new research treatments before they are widely available, and help others bycontributing to medical research. For information about current studies, visitwww.ClinicalTrials.gov .
[Top ]
For More Information
American Association of Kidney Patients3505 East Frontage Road, Suite 315Tampa, FL 33607Phone: 18007492257 or 8136368100Fax: 8136368122Email: [email protected]: www.aakp.org
American Kidney Fund6110 Executive Boulevard, Suite 1010Rockville, MD 20852
Phone: 18006388299 or 18663002900Fax: 3018810898Email: [email protected]: www.kidneyfund.org
Life Optionsc/o Medical Education Institute, Inc.414 DOnofrio Drive, Suite 200
http://www.clinicaltrials.gov/http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#topmailto:[email protected]://www.aakp.org/mailto:[email protected]://www.kidneyfund.org/http://www.clinicaltrials.gov/http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#topmailto:[email protected]://www.aakp.org/mailto:[email protected]://www.kidneyfund.org/8/7/2019 The Kidneys and How They Work
14/33
Madison, WI 53719Phone: 18004687777Fax: 6088338366Email: [email protected]
Internet: www.lifeoptions.orgwww.kidneyschool.org
National Kidney Foundation30 East 33rd Street
New York, NY 10016Phone: 18006229010 or 2128892210Internet: www.kidney.org
The NephCure Foundation15 Waterloo Avenue, Suite 200
Berwyn, PA 19312Phone: 1866NEPHCURE(18666374287) or 6105400186Fax: 6105400190Email: [email protected]: www.nephcure.org
Polycystic Kidney Disease (PKD) Foundation8330 Ward Parkway, Suite 510Kansas City, MO 641142000Phone: 1800PKDCURE
(18007532873) or 8169312600Fax: 8169318655Email: [email protected]: www.pkdcure.org
You may also find additional information about this topic by visiting MedlinePlus atwww.medlineplus.gov .
This publication may contain information about medications. When prepared, this publication included the most current information available. For updates or for questions about any medications, contact the U.S. Food and Drug Administration toll-
free at 1888INFOFDA (18884636332) or visit www.fda.gov . Consult your doctor for more information.
[Top ]
Acknowledgments
Publications produced by the Clearinghouse are carefully reviewed by both NIDDK
mailto:[email protected]://www.lifeoptions.org/http://www.kidneyschool.org/http://www.kidney.org/mailto:[email protected]://www.nephcure.org/mailto:[email protected]://www.pkdcure.org/http://www.medlineplus.gov/http://www.fda.gov/http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#topmailto:[email protected]://www.lifeoptions.org/http://www.kidneyschool.org/http://www.kidney.org/mailto:[email protected]://www.nephcure.org/mailto:[email protected]://www.pkdcure.org/http://www.medlineplus.gov/http://www.fda.gov/http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#top8/7/2019 The Kidneys and How They Work
15/33
scientists and outside experts. This publication was reviewed by William McClellan,M.D., Emory University, Atlanta, and Bessie Young, M.D., University of Washington,Seattle.
[Top ]
National Kidney Disease Education Program
3 Kidney Information WayBethesda, MD 20892Phone: 18664KIDNEY (18664543639)TTY: 18665691162Fax: 3014028182Email: [email protected]: www.nkdep.nih.gov
The National Kidney Disease Education Program (NKDEP) is an initiative of the National Institute of Diabetes and Digestive and Kidney Diseases, National Institutesof Health, U.S. Department of Health and Human Services. The NKDEP aims to raiseawareness of the seriousness of kidney disease, the importance of testing those at highrisk, and the availability of treatment to prevent or slow kidney disease.
National Kidney and Urologic Diseases InformationClearinghouse
3 Information WayBethesda, MD 208923580Phone: 18008915390TTY: 18665691162Fax: 7037384929Email: [email protected]: www.kidney.niddk.nih.gov
The National Kidney and Urologic Diseases Information Clearinghouse (NKUDIC) isa service of the National Institute of Diabetes and Digestive and Kidney Diseases(NIDDK). The NIDDK is part of the National Institutes of Health of the U.S.Department of Health and Human Services. Established in 1987, the Clearinghouse
provides information about diseases of the kidneys and urologic system to people withkidney and urologic disorders and to their families, health care professionals, and the
public. The NKUDIC answers inquiries, develops and distributes publications, andworks closely with professional and patient organizations and Government agencies tocoordinate resources about kidney and urologic diseases.
http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#topmailto:[email protected]://www.nkdep.nih.gov/http://kidney.niddk.nih.gov/about/contact.htmhttp://www.kidney.niddk.nih.gov/http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#topmailto:[email protected]://www.nkdep.nih.gov/http://kidney.niddk.nih.gov/about/contact.htmhttp://www.kidney.niddk.nih.gov/8/7/2019 The Kidneys and How They Work
16/33
Publications produced by the Clearinghouse are carefully reviewed by both NIDDK scientists and outside experts.
This publication is not copyrighted. The Clearinghouse encourages users of this
publication to duplicate and distribute as many copies as desired.
NIH Publication No. 093195February 2009
[Top ]
http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/
HemodialysisFrom Wikipedia, the free encyclopediaJump to: navigation , search
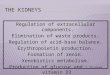
Hemodialysis in progress
http://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#tophttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/http://en.wikipedia.org/wiki/Hemodialysis#mw-headhttp://en.wikipedia.org/wiki/Hemodialysis#mw-headhttp://en.wikipedia.org/wiki/Hemodialysis#p-searchhttp://en.wikipedia.org/wiki/File:Plugged_into_dialysis.jpghttp://en.wikipedia.org/wiki/File:Plugged_into_dialysis.jpghttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/#tophttp://kidney.niddk.nih.gov/kudiseases/pubs/yourkidneys/http://en.wikipedia.org/wiki/Hemodialysis#mw-headhttp://en.wikipedia.org/wiki/Hemodialysis#p-search8/7/2019 The Kidneys and How They Work
17/33
Hemodialysis machine
In medicine , hemodialysis (also haemodialysis ) is a method for removing waste products suchas creatinine and urea , as well as free water from the blood when the kidneys are in renal failure .Hemodialysis is one of three renal replacement therapies (the other two being renal transplant ;
peritoneal dialysis ).
Hemodialysis can be an outpatient or inpatient therapy. Routine hemodialysis is conducted in adialysis outpatient facility, either a purpose built room in a hospital or a dedicated, stand aloneclinic. Less frequently hemodialysis is done at home . Dialysis treatments in a clinic are initiatedand managed by specialized staff made up of nurses and technicians; dialysis treatments at homecan be self initiated and managed or done jointly with the assistance of a trained helper who isusually a family member. [1]
Contents
[hide ]
1 Principle 2 History 3 Prescription 4 Side effects and complications 5 Access
o 5.1 Catheter o 5.2 AV fistulao 5.3 AV graft
http://en.wikipedia.org/wiki/Medicinehttp://en.wikipedia.org/wiki/Creatininehttp://en.wikipedia.org/wiki/Creatininehttp://en.wikipedia.org/wiki/Ureahttp://en.wikipedia.org/wiki/Ureahttp://en.wikipedia.org/wiki/Bloodhttp://en.wikipedia.org/wiki/Kidneyhttp://en.wikipedia.org/wiki/Renal_failurehttp://en.wikipedia.org/wiki/Renal_failurehttp://en.wikipedia.org/wiki/Renal_replacement_therapyhttp://en.wikipedia.org/wiki/Renal_replacement_therapyhttp://en.wikipedia.org/wiki/Renal_transplanthttp://en.wikipedia.org/wiki/Peritoneal_dialysishttp://en.wikipedia.org/wiki/Outpatienthttp://en.wikipedia.org/wiki/Outpatienthttp://en.wikipedia.org/wiki/Inpatienthttp://en.wikipedia.org/wiki/Inpatienthttp://en.wikipedia.org/wiki/Hospitalhttp://en.wikipedia.org/wiki/Hospitalhttp://en.wikipedia.org/wiki/Home_hemodialysishttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-0http://en.wikipedia.org/wiki/Hemodialysishttp://en.wikipedia.org/wiki/Hemodialysis#Principlehttp://en.wikipedia.org/wiki/Hemodialysis#Historyhttp://en.wikipedia.org/wiki/Hemodialysis#Prescriptionhttp://en.wikipedia.org/wiki/Hemodialysis#Side_effects_and_complicationshttp://en.wikipedia.org/wiki/Hemodialysis#Accesshttp://en.wikipedia.org/wiki/Hemodialysis#Catheterhttp://en.wikipedia.org/wiki/Hemodialysis#AV_fistulahttp://en.wikipedia.org/wiki/Hemodialysis#AV_grafthttp://en.wikipedia.org/wiki/File:Hemodialysismachine.jpghttp://en.wikipedia.org/wiki/File:Hemodialysismachine.jpghttp://en.wikipedia.org/wiki/Medicinehttp://en.wikipedia.org/wiki/Creatininehttp://en.wikipedia.org/wiki/Ureahttp://en.wikipedia.org/wiki/Bloodhttp://en.wikipedia.org/wiki/Kidneyhttp://en.wikipedia.org/wiki/Renal_failurehttp://en.wikipedia.org/wiki/Renal_replacement_therapyhttp://en.wikipedia.org/wiki/Renal_transplanthttp://en.wikipedia.org/wiki/Peritoneal_dialysishttp://en.wikipedia.org/wiki/Outpatienthttp://en.wikipedia.org/wiki/Inpatienthttp://en.wikipedia.org/wiki/Hospitalhttp://en.wikipedia.org/wiki/Home_hemodialysishttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-0http://en.wikipedia.org/wiki/Hemodialysishttp://en.wikipedia.org/wiki/Hemodialysis#Principlehttp://en.wikipedia.org/wiki/Hemodialysis#Historyhttp://en.wikipedia.org/wiki/Hemodialysis#Prescriptionhttp://en.wikipedia.org/wiki/Hemodialysis#Side_effects_and_complicationshttp://en.wikipedia.org/wiki/Hemodialysis#Accesshttp://en.wikipedia.org/wiki/Hemodialysis#Catheterhttp://en.wikipedia.org/wiki/Hemodialysis#AV_fistulahttp://en.wikipedia.org/wiki/Hemodialysis#AV_graft8/7/2019 The Kidneys and How They Work
18/33
o 5.4 Fistula First project 6 Types
o 6.1 Conventional hemodialysiso 6.2 Daily hemodialysiso 6.3 Nocturnal hemodialysis
7 Advantages and disadvantageso 7.1 Advantageso 7.2 Disadvantages
8 Equipmento 8.1 Water systemo 8.2 Dialyzer
9 Membrane and fluxo 9.1 Membrane flux and outcomeo 9.2 Membrane flux and beta-2-microglobulin amyloidosiso 9.3 Dialyzer size and efficiencyo 9.4 Reuse of dialyzers
10 Nursing care for hemodialysis patient 11 See also 12 References
13 External links
[edit ] Principle
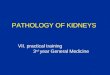
Semipermeable membrane
The principle of hemodialysis is the same as other methods of dialysis ; it involves diffusion of solutes across a semipermeable membrane. Hemodialysis utilizes counter current flow , where thedialysate is flowing in the opposite direction to blood flow in the extracorporeal circuit. Counter-current flow maintains the concentration gradient across the membrane at a maximum andincreases the efficiency of the dialysis.
Fluid removal ( ultrafiltration ) is achieved by altering the hydrostatic pressure of the dialysatecompartment, causing free water and some dissolved solutes to move across the membrane alonga created pressure gradient.
http://en.wikipedia.org/wiki/Hemodialysis#Fistula_First_projecthttp://en.wikipedia.org/wiki/Hemodialysis#Typeshttp://en.wikipedia.org/wiki/Hemodialysis#Conventional_hemodialysishttp://en.wikipedia.org/wiki/Hemodialysis#Daily_hemodialysishttp://en.wikipedia.org/wiki/Hemodialysis#Nocturnal_hemodialysishttp://en.wikipedia.org/wiki/Hemodialysis#Advantages_and_disadvantageshttp://en.wikipedia.org/wiki/Hemodialysis#Advantageshttp://en.wikipedia.org/wiki/Hemodialysis#Disadvantageshttp://en.wikipedia.org/wiki/Hemodialysis#Equipmenthttp://en.wikipedia.org/wiki/Hemodialysis#Water_systemhttp://en.wikipedia.org/wiki/Hemodialysis#Dialyzerhttp://en.wikipedia.org/wiki/Hemodialysis#Membrane_and_fluxhttp://en.wikipedia.org/wiki/Hemodialysis#Membrane_flux_and_outcomehttp://en.wikipedia.org/wiki/Hemodialysis#Membrane_flux_and_beta-2-microglobulin_amyloidosishttp://en.wikipedia.org/wiki/Hemodialysis#Dialyzer_size_and_efficiencyhttp://en.wikipedia.org/wiki/Hemodialysis#Reuse_of_dialyzershttp://en.wikipedia.org/wiki/Hemodialysis#Nursing_care_for_hemodialysis_patienthttp://en.wikipedia.org/wiki/Hemodialysis#See_alsohttp://en.wikipedia.org/wiki/Hemodialysis#Referenceshttp://en.wikipedia.org/wiki/Hemodialysis#External_linkshttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=1http://en.wikipedia.org/wiki/Dialysishttp://en.wikipedia.org/wiki/Diffusionhttp://en.wikipedia.org/wiki/Diffusionhttp://en.wikipedia.org/wiki/Counter-current_exchangehttp://en.wikipedia.org/wiki/Counter-current_exchangehttp://en.wikipedia.org/wiki/Blood_flowhttp://en.wikipedia.org/wiki/Blood_flowhttp://en.wikipedia.org/wiki/Extracorporealhttp://en.wikipedia.org/wiki/Extracorporealhttp://en.wikipedia.org/wiki/Ultrafiltration_(renal)http://en.wikipedia.org/wiki/Hydrostatic_pressurehttp://en.wikipedia.org/wiki/Hydrostatic_pressurehttp://en.wikipedia.org/wiki/File:Semipermeable_membrane.pnghttp://en.wikipedia.org/wiki/File:Semipermeable_membrane.pnghttp://en.wikipedia.org/wiki/Hemodialysis#Fistula_First_projecthttp://en.wikipedia.org/wiki/Hemodialysis#Typeshttp://en.wikipedia.org/wiki/Hemodialysis#Conventional_hemodialysishttp://en.wikipedia.org/wiki/Hemodialysis#Daily_hemodialysishttp://en.wikipedia.org/wiki/Hemodialysis#Nocturnal_hemodialysishttp://en.wikipedia.org/wiki/Hemodialysis#Advantages_and_disadvantageshttp://en.wikipedia.org/wiki/Hemodialysis#Advantageshttp://en.wikipedia.org/wiki/Hemodialysis#Disadvantageshttp://en.wikipedia.org/wiki/Hemodialysis#Equipmenthttp://en.wikipedia.org/wiki/Hemodialysis#Water_systemhttp://en.wikipedia.org/wiki/Hemodialysis#Dialyzerhttp://en.wikipedia.org/wiki/Hemodialysis#Membrane_and_fluxhttp://en.wikipedia.org/wiki/Hemodialysis#Membrane_flux_and_outcomehttp://en.wikipedia.org/wiki/Hemodialysis#Membrane_flux_and_beta-2-microglobulin_amyloidosishttp://en.wikipedia.org/wiki/Hemodialysis#Dialyzer_size_and_efficiencyhttp://en.wikipedia.org/wiki/Hemodialysis#Reuse_of_dialyzershttp://en.wikipedia.org/wiki/Hemodialysis#Nursing_care_for_hemodialysis_patienthttp://en.wikipedia.org/wiki/Hemodialysis#See_alsohttp://en.wikipedia.org/wiki/Hemodialysis#Referenceshttp://en.wikipedia.org/wiki/Hemodialysis#External_linkshttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=1http://en.wikipedia.org/wiki/Dialysishttp://en.wikipedia.org/wiki/Diffusionhttp://en.wikipedia.org/wiki/Counter-current_exchangehttp://en.wikipedia.org/wiki/Blood_flowhttp://en.wikipedia.org/wiki/Extracorporealhttp://en.wikipedia.org/wiki/Ultrafiltration_(renal)http://en.wikipedia.org/wiki/Hydrostatic_pressure8/7/2019 The Kidneys and How They Work
19/33
The dialysis solution that is used may be a sterilized solution of mineral ions or comply withBritich Pharmacopea. Urea and other waste products, potassium , and phosphate diffuse into thedialysis solution. However, concentrations of sodium and chloride are similar to those of normal
plasma to prevent loss. Sodium bicarbonate is added in a higher concentration than plasma tocorrect blood acidity. A small amount of glucose is also commonly used.
Note that this is a different process to the related technique of hemofiltration .
[edit ] History
Many have played a role in developing dialysis as a practical treatment for renal failure, startingwith Thomas Graham of Glasgow , who first presented the principles of solute transport across asemipermeable membrane in 1854 .[2] The artificial kidney was first developed by Abel , Rountreeand Turner in 1913, [3] the first hemodialysis in a human being was by Hass (February 28, 1924) [4]
and the artificial kidney was developed into a clinically useful apparatus by Kolff in 1943 - 1945.[5] This research showed that life could be prolonged in patients dying of renal failure .
Dr. Willem Kolff was the first to construct a working dialyzer in 1943. The first successfullytreated patient was a 67-year-old woman in uremic coma who regained consciousness after 11hours of hemodialysis with Kolffs dialyzer in 1945. At the time of its creation, Kolffs goal wasto provide life support during recovery from acute renal failure. After World War II ended, Kolff donated the five dialyzers he had made to hospitals around the world, including Mount SinaiHospital, New York . Kolff gave a set of blueprints for his hemodialysis machine to GeorgeThorn at the Peter Bent Brigham Hospital in Boston . This led to the manufacture of the nextgeneration of Kolffs dialyzer, a stainless steel Kolff-Brigham dialysis machine.
By the 1950s, Willem Kolffs invention of the dialyzer was used for acute renal failure, but itwas not seen as a viable treatment for patients with stage 5 chronic kidney disease (CKD). At thetime, doctors believed it was impossible for patients to have dialysis indefinitely for two reasons.First, they thought no man-made device could replace the function of kidneys over the long term.In addition, a patient undergoing dialysis suffered from damaged veins and arteries, so that after several treatments, it became difficult to find a vessel to access the patients blood.
Dr. Nils Alwall : The original Kolff kidney was not very useful clinically, because it did notallow for removal of excess fluid. Dr. Nils Alwall [6] encased a modified version of this kidneyinside a stainless steel canister, to which a negative pressure could be applied, in this wayeffecting the first truly practical application of hemodialysis, which was done in 1946 at theUniversity of Lund . Alwall also was arguably the inventor of the arteriovenous shunt for dialysis.He reported this first in 1948 where he used such an arteriovenous shunt in rabbits. Subsequentlyhe used such shunts, made of glass, as well as his canister-enclosed dialyzer, to treat 1500
patients in renal failure between 1946 and 1960, as reported to the First International Congress of Nephrology held in Evian in September 1960. Alwall was appointed to a newly-created Chair of Nephrology at the University of Lund in 1957. Subsequently, he collaborated with Swedish businessman Holger Crafoord to found one of the key companies that would manufacturedialysis equipment in the past 50 years, Gambro . The early history of dialysis has been reviewed
by Stanley Shaldon. [7]
http://en.wikipedia.org/wiki/Ureahttp://en.wikipedia.org/wiki/Ureahttp://en.wikipedia.org/wiki/Potassiumhttp://en.wikipedia.org/wiki/Phosphatehttp://en.wikipedia.org/wiki/Sodiumhttp://en.wikipedia.org/wiki/Blood_plasmahttp://en.wikipedia.org/wiki/Sodium_bicarbonatehttp://en.wikipedia.org/wiki/Sodium_bicarbonatehttp://en.wikipedia.org/wiki/Hemofiltrationhttp://en.wikipedia.org/wiki/Hemofiltrationhttp://en.wikipedia.org/wiki/Hemofiltrationhttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=2http://en.wikipedia.org/wiki/Thomas_Graham_(chemist)http://en.wikipedia.org/wiki/Glasgowhttp://en.wikipedia.org/wiki/Glasgowhttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-1http://en.wikipedia.org/wiki/Hemodialysis#cite_note-1http://en.wikipedia.org/wiki/John_Jacob_Abelhttp://en.wikipedia.org/wiki/John_Jacob_Abelhttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-2http://en.wikipedia.org/wiki/Georg_Haashttp://en.wikipedia.org/wiki/Georg_Haashttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-3http://en.wikipedia.org/wiki/Willem_Johan_Kolffhttp://en.wikipedia.org/wiki/Willem_Johan_Kolffhttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-4http://en.wikipedia.org/wiki/Renal_failurehttp://en.wikipedia.org/wiki/Willem_Kolffhttp://en.wikipedia.org/wiki/Uremiahttp://en.wikipedia.org/wiki/Uremiahttp://en.wikipedia.org/wiki/World_War_IIhttp://en.wikipedia.org/wiki/World_War_IIhttp://en.wikipedia.org/wiki/Mount_Sinai_Hospital,_New_Yorkhttp://en.wikipedia.org/wiki/Mount_Sinai_Hospital,_New_Yorkhttp://en.wikipedia.org/wiki/Mount_Sinai_Hospital,_New_Yorkhttp://en.wikipedia.org/wiki/Peter_Bent_Brigham_Hospitalhttp://en.wikipedia.org/wiki/Bostonhttp://en.wikipedia.org/wiki/Stainless_steelhttp://en.wikipedia.org/wiki/Chronic_kidney_diseasehttp://en.wikipedia.org/wiki/Nils_Alwallhttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-5http://en.wikipedia.org/wiki/University_of_Lundhttp://en.wikipedia.org/wiki/Holger_Crafoordhttp://en.wikipedia.org/wiki/Gambrohttp://en.wikipedia.org/wiki/Gambrohttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-6http://en.wikipedia.org/wiki/Ureahttp://en.wikipedia.org/wiki/Potassiumhttp://en.wikipedia.org/wiki/Phosphatehttp://en.wikipedia.org/wiki/Sodiumhttp://en.wikipedia.org/wiki/Blood_plasmahttp://en.wikipedia.org/wiki/Sodium_bicarbonatehttp://en.wikipedia.org/wiki/Hemofiltrationhttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=2http://en.wikipedia.org/wiki/Thomas_Graham_(chemist)http://en.wikipedia.org/wiki/Glasgowhttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-1http://en.wikipedia.org/wiki/John_Jacob_Abelhttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-2http://en.wikipedia.org/wiki/Georg_Haashttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-3http://en.wikipedia.org/wiki/Willem_Johan_Kolffhttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-4http://en.wikipedia.org/wiki/Renal_failurehttp://en.wikipedia.org/wiki/Willem_Kolffhttp://en.wikipedia.org/wiki/Uremiahttp://en.wikipedia.org/wiki/World_War_IIhttp://en.wikipedia.org/wiki/Mount_Sinai_Hospital,_New_Yorkhttp://en.wikipedia.org/wiki/Mount_Sinai_Hospital,_New_Yorkhttp://en.wikipedia.org/wiki/Peter_Bent_Brigham_Hospitalhttp://en.wikipedia.org/wiki/Bostonhttp://en.wikipedia.org/wiki/Stainless_steelhttp://en.wikipedia.org/wiki/Chronic_kidney_diseasehttp://en.wikipedia.org/wiki/Nils_Alwallhttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-5http://en.wikipedia.org/wiki/University_of_Lundhttp://en.wikipedia.org/wiki/Holger_Crafoordhttp://en.wikipedia.org/wiki/Gambrohttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-68/7/2019 The Kidneys and How They Work
20/33
Dr. Belding H. Scribner working with a surgeon, Dr. Wayne Quinton, modified the glass shuntsused by Alwall by making them from Teflon . Another key improvement was to connect them toa short piece of silicone elastomer tubing. This formed the basis of the so-called Scribner shunt ,
perhaps more properly called the Quinton-Scribner shunt. After treatment, the circulatory accesswould be kept open by connecting the two tubes outside the body using a small U-shaped Teflon
tube, which would shunt the blood from the tube in the artery back to the tube in the vein .[8]
In 1962, Scribner started the worlds first outpatient dialysis facility, the Seattle Artificial KidneyCenter, later renamed the Northwest Kidney Centers . Immediately the problem arose of whoshould be given dialysis, since demand far exceeded the capacity of the six dialysis machines atthe center. Scribner decided that the decision about who would receive dialysis and whowouldnt, would not be made by him. Instead, the choices would be made by an anonymouscommittee, which could be viewed as one of the first bioethics committees.
For a detailed history of successful and unsuccessful attempts at dialysis, including pioneers suchas Abel and Roundtree, Haas, and Necheles, see this review by Kjellstrand .[9]
[edit ] Prescription
A prescription for dialysis by a nephrologist (a medical kidney specialist) will specify various parameters for a dialysis treatment. These include frequency (how many treatments per week),length of each treatment, and the blood and dialysis solution flow rates, as well as the size of thedialyzer. The composition of the dialysis solution is also sometimes adjusted in terms of itssodium and potassium and bicarbonate levels. In general, the larger the body size of anindividual, the more dialysis he/she will need. In the North America and UK , 3-4 hour treatments(sometimes up to 5 hours for larger patients) given 3 times a week are typical. Twice-a-week sessions are limited to patients who have a substantial residual kidney function. Four sessions per week are often prescribed for larger patients, as well as patients who have trouble with fluidoverload. Finally, there is growing interest in short daily home hemodialysis , which is 1.5 - 4 hr sessions given 5-7 times per week, usually at home. There also is interest in nocturnal dialysis ,which involves dialyzing a patient, usually at home, for 810 hours per night, 3-6 nights per week. Nocturnal in-center dialysis, 3-4 times per week is also offered at a handful of dialysisunits in the United States .
[edit ] Side effects and complications
Hemodialysis often involves fluid removal (through ultrafiltration ), because most patients with
renal failure pass little or no urine. Side effects caused by removing too much fluid and/or removing fluid too rapidly include low blood pressure , fatigue , chest pains, leg-cramps, nausea and headaches . These symptoms can occur during the treatment and can persist post treatment;they are sometimes collectively referred to as the dialysis hangover or dialysis washout. Theseverity of these symptoms is usually proportionate to the amount and speed of fluid removal.However, the impact of a given amount or rate of fluid removal can vary greatly from person to
person and day to day. These side effects can be avoided and/or their severity lessened bylimiting fluid intake between treatments or increasing the dose of dialysis e.g. dialyzing more
http://en.wikipedia.org/wiki/Belding_H._Scribnerhttp://en.wikipedia.org/wiki/Polytetrafluoroethylenehttp://en.wikipedia.org/wiki/Scribner_shunthttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-7http://en.wikipedia.org/wiki/Hemodialysis#cite_note-7http://en.wikipedia.org/wiki/Northwest_Kidney_Centershttp://en.wikipedia.org/wiki/Northwest_Kidney_Centershttp://en.wikipedia.org/wiki/Bioethicshttp://en.wikipedia.org/wiki/Bioethicshttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-8http://en.wikipedia.org/wiki/Hemodialysis#cite_note-8http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=3http://en.wikipedia.org/wiki/Nephrologisthttp://en.wikipedia.org/wiki/North_Americahttp://en.wikipedia.org/wiki/United_Kingdomhttp://en.wikipedia.org/wiki/United_Kingdomhttp://en.wikipedia.org/wiki/Home_hemodialysishttp://en.wikipedia.org/wiki/Home_hemodialysishttp://en.wikipedia.org/wiki/Nocturnal_dialysishttp://en.wikipedia.org/wiki/Nocturnal_dialysishttp://en.wikipedia.org/wiki/United_Stateshttp://en.wikipedia.org/wiki/United_Stateshttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=4http://en.wikipedia.org/wiki/Ultrafiltration_(renal)http://en.wikipedia.org/wiki/Ultrafiltration_(renal)http://en.wikipedia.org/wiki/Renal_failurehttp://en.wikipedia.org/wiki/Renal_failurehttp://en.wikipedia.org/wiki/Blood_pressurehttp://en.wikipedia.org/wiki/Fatigue_(physical)http://en.wikipedia.org/wiki/Fatigue_(physical)http://en.wikipedia.org/wiki/Nauseahttp://en.wikipedia.org/wiki/Headacheshttp://en.wikipedia.org/wiki/Headacheshttp://en.wikipedia.org/wiki/Belding_H._Scribnerhttp://en.wikipedia.org/wiki/Polytetrafluoroethylenehttp://en.wikipedia.org/wiki/Scribner_shunthttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-7http://en.wikipedia.org/wiki/Northwest_Kidney_Centershttp://en.wikipedia.org/wiki/Bioethicshttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-8http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=3http://en.wikipedia.org/wiki/Nephrologisthttp://en.wikipedia.org/wiki/North_Americahttp://en.wikipedia.org/wiki/United_Kingdomhttp://en.wikipedia.org/wiki/Home_hemodialysishttp://en.wikipedia.org/wiki/Nocturnal_dialysishttp://en.wikipedia.org/wiki/United_Stateshttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=4http://en.wikipedia.org/wiki/Ultrafiltration_(renal)http://en.wikipedia.org/wiki/Renal_failurehttp://en.wikipedia.org/wiki/Blood_pressurehttp://en.wikipedia.org/wiki/Fatigue_(physical)http://en.wikipedia.org/wiki/Nauseahttp://en.wikipedia.org/wiki/Headaches8/7/2019 The Kidneys and How They Work
21/33
often or longer per treatment than the standard three times a week, 34 hours per treatmentschedule.
Since hemodialysis requires access to the circulatory system, patients undergoing hemodialysismay expose their circulatory system to microbes , which can lead to sepsis , an infection affecting
the heart valves ( endocarditis ) or an infection affecting the bones ( osteomyelitis ). The risk of infection varies depending on the type of access used (see below). Bleeding may also occur,again the risk varies depending on the type of access used. Infections can be minimized bystrictly adhering to infection control best practices.
Heparin is the most commonly used anticoagulant in hemodialysis, as it is generally welltolerated and can be quickly reversed with protamine sulfate . Heparin allergy can infrequently bea problem and can cause a low platelet count. In such patients, alternative anticoagulants can beused. In patients at high risk of bleeding, dialysis can be done without anticoagulation.
First Use Syndrome is a rare but severe anaphylactic reaction to the artificial kidney . Its
symptoms include sneezing, wheezing, shortness of breath, back pain, chest pain, or suddendeath. It can be caused by residual sterilant in the artificial kidney or the material of themembrane itself. In recent years, the incidence of First Use Syndrome has decreased, due to anincreased use of gamma irradiation , steam sterilization, or electron-beam radiation instead of chemical sterilants, and the development of new semipermeable membranes of higher
biocompatibility . New methods of processing previously acceptable components of dialysis mustalways be considered. For example, in 2008, a series of first-use type or reactions, includingdeaths occurred due to heparin contaminated during the manufacturing process with oversulfatedchondroitin sulfate .[10]
Longterm complications of hemodialysis include amyloidosis , neuropathy and various forms of
heart disease . Increasing the frequency and length of treatments have been shown to improvefluid overload and enlargement of the heart that is commonly seen in such patients. [11] [12]
Listed below are specific complications associated with different types of hemodialysis access.
[edit ] Access
In hemodialysis, three primary methods are used to gain access to the blood: an intravenouscatheter, an arteriovenous (AV) fistula and a synthetic graft. The type of access is influenced byfactors such as the expected time course of a patient's renal failure and the condition of his or her vasculature. Patients may have multiple accesses, usually because an AV fistula or graft ismaturing and a catheter is still being used. The creation of all these three major types of vascular accesses requires surgery. [13]
[edit ] Catheter
Catheter access, sometimes called a CVC ( Central Venous Catheter ), consists of a plasticcatheter with two lumens (or occasionally two separate catheters) which is inserted into a largevein (usually the vena cava , via the internal jugular vein or the femoral vein ) to allow large flows
http://en.wikipedia.org/wiki/Microbeshttp://en.wikipedia.org/wiki/Microbeshttp://en.wikipedia.org/wiki/Sepsishttp://en.wikipedia.org/wiki/Endocarditishttp://en.wikipedia.org/wiki/Osteomyelitishttp://en.wikipedia.org/wiki/Infection_controlhttp://en.wikipedia.org/wiki/Infection_controlhttp://en.wikipedia.org/wiki/Heparinhttp://en.wikipedia.org/wiki/Protamine_sulfatehttp://en.wikipedia.org/wiki/Anaphylaxishttp://en.wikipedia.org/wiki/Anaphylaxishttp://en.wikipedia.org/wiki/Artificial_kidneyhttp://en.wikipedia.org/w/index.php?title=Gamma_irradiation&action=edit&redlink=1http://en.wikipedia.org/wiki/Biocompatibilityhttp://en.wikipedia.org/wiki/Biocompatibilityhttp://en.wikipedia.org/wiki/Chondroitin_sulfatehttp://en.wikipedia.org/wiki/Chondroitin_sulfatehttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-9http://en.wikipedia.org/wiki/Amyloidosishttp://en.wikipedia.org/wiki/Amyloidosishttp://en.wikipedia.org/wiki/Neuropathyhttp://en.wikipedia.org/wiki/Neuropathyhttp://en.wikipedia.org/wiki/Heart_diseasehttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-10http://en.wikipedia.org/wiki/Hemodialysis#cite_note-11http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=5http://en.wikipedia.org/wiki/Hemodialysis#cite_note-12http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=6http://en.wikipedia.org/wiki/Central_venous_catheterhttp://en.wikipedia.org/wiki/Vena_cavahttp://en.wikipedia.org/wiki/Internal_jugular_veinhttp://en.wikipedia.org/wiki/Internal_jugular_veinhttp://en.wikipedia.org/wiki/Femoral_veinhttp://en.wikipedia.org/wiki/Microbeshttp://en.wikipedia.org/wiki/Sepsishttp://en.wikipedia.org/wiki/Endocarditishttp://en.wikipedia.org/wiki/Osteomyelitishttp://en.wikipedia.org/wiki/Infection_controlhttp://en.wikipedia.org/wiki/Heparinhttp://en.wikipedia.org/wiki/Protamine_sulfatehttp://en.wikipedia.org/wiki/Anaphylaxishttp://en.wikipedia.org/wiki/Artificial_kidneyhttp://en.wikipedia.org/w/index.php?title=Gamma_irradiation&action=edit&redlink=1http://en.wikipedia.org/wiki/Biocompatibilityhttp://en.wikipedia.org/wiki/Chondroitin_sulfatehttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-9http://en.wikipedia.org/wiki/Amyloidosishttp://en.wikipedia.org/wiki/Neuropathyhttp://en.wikipedia.org/wiki/Heart_diseasehttp://en.wikipedia.org/wiki/Hemodialysis#cite_note-10http://en.wikipedia.org/wiki/Hemodialysis#cite_note-11http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=5http://en.wikipedia.org/wiki/Hemodialysis#cite_note-12http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=6http://en.wikipedia.org/wiki/Central_venous_catheterhttp://en.wikipedia.org/wiki/Vena_cavahttp://en.wikipedia.org/wiki/Internal_jugular_veinhttp://en.wikipedia.org/wiki/Femoral_vein8/7/2019 The Kidneys and How They Work
22/33
of blood to be withdrawn from one lumen, to enter the dialysis circuit, and to be returned via theother lumen. However, blood flow is almost always less than that of a well functioning fistula or graft.
Catheters are usually found in two general varieties, tunnelled and non-tunnelled.
Non-tunnelled catheter access is for short-term access (up to about 10 days, but often for onedialysis session only), and the catheter emerges from the skin at the site of entry into the vein.
Tunnelled catheter access involves a longer catheter, which is tunnelled under the skin from the point of insertion in the vein to an exit site some distance away. It is usually placed in theinternal jugular vein in the neck and the exit site is usually on the chest wall. The tunnel acts as a
barrier to invading microbes, and as such, tunnelled catheters are designed for short- to medium-term access (weeks to months only), because infection is still a frequent problem.
Aside from infection, venous stenosis is another serious problem with catheter access. The
catheter is a foreign body in the vein and often provokes an inflammatory reaction in the veinwall. This results in scarring and narrowing of the vein, often to the point of occlusion. This cancause problems with severe venous congestion in the area drained by the vein and may alsorender the vein, and the veins drained by it, useless for creating a fistula or graft at a later date.Patients on long-term hemodialysis can literally 'run out' of access, so this can be a fatal problem.
Catheter access is usually used for rapid access for immediate dialysis, for tunnelled access in patients who are deemed likely to recover from acute renal failure , and for patients with end-stage renal failure who are either waiting for alternative access to mature or who are unable tohave alternative access.
Catheter access is often popular with patients, because attachment to the dialysis machine doesn'trequire needles. However, the serious risks of catheter access noted above mean that such accessshould be contemplated only as a long-term solution in the most desperate access situation.
[edit ] AV fistula
http://en.wikipedia.org/wiki/Stenosishttp://en.wikipedia.org/wiki/Scarringhttp://en.wikipedia.org/wiki/Scarringhttp://en.wikipedia.org/wiki/Acute_renal_failurehttp://en.wikipedia.org/wiki/End-stage_renal_failurehttp://en.wikipedia.org/wiki/End-stage_renal_failurehttp://en.wikipedia.org/wiki/End-stage_renal_failurehttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=7http://en.wikipedia.org/wiki/Stenosishttp://en.wikipedia.org/wiki/Scarringhttp://en.wikipedia.org/wiki/Acute_renal_failurehttp://en.wikipedia.org/wiki/End-stage_renal_failurehttp://en.wikipedia.org/wiki/End-stage_renal_failurehttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=78/7/2019 The Kidneys and How They Work
23/33
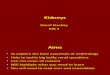
A radiocephalic fistula.
AV (arteriovenous) fistulas are recognized as the preferred access method. To create a fistula , avascular surgeon joins an artery and a vein together through anastomosis . Since this bypasses thecapillaries , blood flows rapidly through the fistula. One can feel this by placing one's finger over
a mature fistula. This is called feeling for "thrill" and produces a distinct 'buzzing' feeling over the fistula. One can also listen through a stethoscope for the sound of the blood "whooshing"through the fistula, a sound called bruit .
Fistulas are usually created in the nondominant arm and may be situated on the hand (the'snuffbox ' fistula'), the forearm (usually a radiocephalic fistula, or so-called Brescia- Ciminofistula , in which the radial artery is anastomosed to the cephalic vein ), or the elbow (usually a
brachiocephalic fistula, where the brachial artery is anastomosed to the cephalic vein ). A fistulawill take a number of weeks to mature, on average perhaps 46 weeks. During treatment, twoneedles are inserted into the fistula, one to draw blood and one to return it.
The advantages of the AV fistula use are lower infection rates, because no foreign material isinvolved in their formation, higher blood flow rates (which translates to more effective dialysis),and a lower incidence of thrombosis . The complications are few, but if a fistula has a very high
blood flow and the vasculature that supplies the rest of the limb is poor, a steal syndrome canoccur, where blood entering the limb is drawn into the fistula and returned to the generalcirculation without entering the limb's capillaries. This results in cold extremities of that limb,cramping pains, and, if severe, tissue damage. One long-term complication of an AV fistula can
be the development of an aneurysm, a bulging in the wall of the vein where it is weakened by the
http://en.wikipedia.org/wiki/Fistulahttp://en.wikipedia.org/wiki/Fistulahttp://en.wikipedia.org/wiki/Vascular_surgeonhttp://en.wikipedia.org/wiki/Arteryhttp://en.wikipedia.org/wiki/Arteryhttp://en.wikipedia.org/wiki/Veinhttp://en.wikipedia.org/wiki/Anastomosishttp://en.wikipedia.org/wiki/Anastomosishttp://en.wikipedia.org/wiki/Anastomosishttp://en.wikipedia.org/wiki/Capillarieshttp://en.wikipedia.org/wiki/Capillarieshttp://en.wikipedia.org/wiki/Stethoscopehttp://en.wikipedia.org/wiki/Stethoscopehttp://en.wikipedia.org/wiki/Bruithttp://en.wikipedia.org/wiki/Bruithttp://en.wikipedia.org/wiki/Snuffboxhttp://en.wikipedia.org/wiki/Snuffboxhttp://en.wikipedia.org/wiki/Snuffboxhttp://en.wikipedia.org/wiki/Cimino_fistulahttp://en.wikipedia.org/wiki/Cimino_fistulahttp://en.wikipedia.org/wiki/Radial_arteryhttp://en.wikipedia.org/wiki/Cephalic_veinhttp://en.wikipedia.org/wiki/Cephalic_veinhttp://en.wikipedia.org/wiki/Brachial_arteryhttp://en.wikipedia.org/wiki/Cephalic_veinhttp://en.wikipedia.org/wiki/Cephalic_veinhttp://en.wikipedia.org/wiki/Thrombosishttp://en.wikipedia.org/wiki/Thrombosishttp://en.wikipedia.org/wiki/Vascular_access_steal_syndromehttp://en.wikipedia.org/wiki/File:Radiocephalic_fistula.svghttp://en.wikipedia.org/wiki/File:Radiocephalic_fistula.svghttp://en.wikipedia.org/wiki/Fistulahttp://en.wikipedia.org/wiki/Vascular_surgeonhttp://en.wikipedia.org/wiki/Arteryhttp://en.wikipedia.org/wiki/Veinhttp://en.wikipedia.org/wiki/Anastomosishttp://en.wikipedia.org/wiki/Capillarieshttp://en.wikipedia.org/wiki/Stethoscopehttp://en.wikipedia.org/wiki/Bruithttp://en.wikipedia.org/wiki/Snuffboxhttp://en.wikipedia.org/wiki/Cimino_fistulahttp://en.wikipedia.org/wiki/Cimino_fistulahttp://en.wikipedia.org/wiki/Radial_arteryhttp://en.wikipedia.org/wiki/Cephalic_veinhttp://en.wikipedia.org/wiki/Brachial_arteryhttp://en.wikipedia.org/wiki/Cephalic_veinhttp://en.wikipedia.org/wiki/Thrombosishttp://en.wikipedia.org/wiki/Vascular_access_steal_syndrome8/7/2019 The Kidneys and How They Work
24/33
repeated insertion of needles over time. To a large extent the risk of developing an aneurysm can be reduced by carefully rotating needle sites over the entire fistula, or using the"buttonhole"(constant site) technique. Aneurysms may necessitate corrective surgery and mayshorten the useful life of a fistula. To prevent damage to the fistula and aneurysm or
pseudoaneurysm formation, it is recommended that the needle be inserted at different points in a
rotating fashion. Another approach is to cannulate the fistula with a blunted needle, in exactly thesame place. This is called a 'buttonhole' approach. Often two or three buttonhole places areavailable on a given fistula. This also can prolong fistula life and help prevent damage to thefistula.
[edit ] AV graft
An arteriovenous graft.
AV (arteriovenous) grafts are much like fistulas in most respects, except that an artificial vesselis used to join the artery and vein. The graft usually is made of a synthetic material, often PTFE ,
but sometimes chemically treated, sterilized veins from animals are used. Grafts are insertedwhen the patient's native vasculature does not permit a fistula. They mature faster than fistulas,and may be ready for use several weeks after formation (some newer grafts may be used evensooner). However, AV grafts are at high risk to develop narrowing, especially in the vein justdownstream from where the graft has been sewn to the vein. Narrowing often leads to clotting or thrombosis. As foreign material, they are at greater risk for becoming infected. More options for sites to place a graft are available, because the graft can be made quite long. Thus a graft can be
placed in the thigh or even the neck (the 'necklace graft').
[edit ] Fistula First project
AV fistulas have a much better access patency and survival than do venous catheters or grafts.They also produce better patient survival and have far fewer complications compared to grafts or venous catheters. For this reason, the Centers for Medicare & Medicaid (CMS) has set up aFistula First Initiative, [14] whose goal is to increase the use of AV fistulas in dialysis patients.
There is ongoing research to make bio-engineered blood vessels, which may be of immenseimportance in creating AV fistulas for patients on hemodialysis, who do not have good blood
http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=8http://en.wikipedia.org/wiki/Polytetrafluoroethylenehttp://en.wikipedia.org/wiki/Polytetrafluoroethylenehttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=9http://en.wikipedia.org/wiki/Hemodialysis#cite_note-13http://en.wikipedia.org/wiki/File:Arteriovenous_graft_(en).svghttp://en.wikipedia.org/wiki/File:Arteriovenous_graft_(en).svghttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=8http://en.wikipedia.org/wiki/Polytetrafluoroethylenehttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=9http://en.wikipedia.org/wiki/Hemodialysis#cite_note-138/7/2019 The Kidneys and How They Work
25/33
vessels for creation of one. It involves growing cells which produce collagen and other proteinson a biodegradable micromesh tube followed by removal of those cells to make the 'bloodvessels' storable in refrigerators. [15]
[edit ] Types
There are three types of hemodialysis: conventional hemodialysis, daily hemodialysis, andnocturnal hemodialysis. Below is the adaption and summary from a brochure of The OttawaHospital.
[edit ] Conventional hemodialysis
Chronic hemodialysis is usually done three times per week, for about 34 hours for eachtreatment, during which the patient's blood is drawn out through a tube at a rate of 3-400 cc/min.The tube is connected to a 15, 16, or 17 gauge needle inserted in the dialysis fistula or graft, or connected to one port of a dialysis catheter . The blood is then pumped through the dialyser, andthen the processed blood is pumped back into the patient's bloodstream through another tube(connected to a second needle or port). During the procedure, the patient's blood pressure isclosely monitored, and if it becomes low, or the patient develops any other signs of low bloodvolume such as nausea, the dialysis attendant can administer extra fluid through the machine.During the treatment, the patient's entire blood volume (about 5000 cc) circulates through themachine every 15 minutes.
[edit ] Daily hemodialysis
Daily hemodialysis is typically used by those patients who do their own dialysis at home. It isless stressful (more gentle) but does require more frequent access. This is simple with catheters,
but more problematic with fistulas or grafts. The "buttonhole technique" can be used for fistulasrequiring frequent access. Daily hemodialysis is usually done for 2 hours six days a week.
[edit ] Nocturnal hemodialysis
the procedure of nocturnal hemodialysis is similar to conventional hemodialysis except it is performed six nights a week and six-ten hours per session while the patient sleeps. [16]
[edit ] Advantages and disadvantages
[edit ] Advantages
Low mortality rate Better control of blood pressure and abdominal cramps Less diet restriction Better solute clearance effect for the daily hemodialysis: better tolerance and fewer
complications with more frequent dialysis [17]
http://en.wikipedia.org/wiki/Hemodialysis#cite_note-14http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=10http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=11http://en.wikipedia.org/wiki/Catheterhttp://en.wikipedia.org/wiki/Catheterhttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=12http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=13http://en.wikipedia.org/wiki/Hemodialysis#cite_note-15http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=14http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=15http://en.wikipedia.org/wiki/Hemodialysis#cite_note-Daugirdas-16http://en.wikipedia.org/wiki/Hemodialysis#cite_note-14http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=10http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=11http://en.wikipedia.org/wiki/Catheterhttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=12http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=13http://en.wikipedia.org/wiki/Hemodialysis#cite_note-15http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=14http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=15http://en.wikipedia.org/wiki/Hemodialysis#cite_note-Daugirdas-168/7/2019 The Kidneys and How They Work
26/33
[edit ] Disadvantages
Restricts independence, as people undergoing this procedure cannot travel around because of supplies availability
Requires reliable technology such as high water quality and electricity
Requires more supplies like dialysis machines The procedure is complicated and requires that care givers have more knowledge Requires time to set up and clean dialysis machines, and expense with machines and
associated staff [17]
[edit ] Equipment
Schematic of a hemodialysis circuit
The hemodialysis machine pumps the patient's blood and the dialysate through the dialyzer. Thenewest dialysis machines on the market are highly computerized and continuously monitor anarray of safety-critical parameters, including blood and dialysate flow rates; dialysis solutionconductivity, temperature, and pH; and analysis of the dialysate for evidence of blood leakage or
presence of air. Any reading that is out of normal range triggers an audible alarm to alert the patient-care technician who is monitoring the patient. Manufacturers of dialysis machinesinclude companies such as Fresenius , Gambro , Baxter, B. Braun, NxStage and Bellco.
[edit ] Water system
http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=16http://en.wikipedia.org/wiki/Hemodialysis#cite_note-Daugirdas-16http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=17http://en.wikipedia.org/wiki/Fresenius_AGhttp://en.wikipedia.org/wiki/Fresenius_AGhttp://en.wikipedia.org/wiki/Gambrohttp://en.wikipedia.org/wiki/Gambrohttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=18http://en.wikipedia.org/wiki/File:Hemodialysis-en.svghttp://en.wikipedia.org/wiki/File:Hemodialysis-en.svghttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=16http://en.wikipedia.org/wiki/Hemodialysis#cite_note-Daugirdas-16http://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=17http://en.wikipedia.org/wiki/Fresenius_AGhttp://en.wikipedia.org/wiki/Gambrohttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=188/7/2019 The Kidneys and How They Work
27/33
A hemodialysis unit's dialysate solution tanks
An extensive water purification system is absolutely critical for hemodialysis. Since dialysis patients are exposed to vast quantities of water, which is mixed with dialysate concentrate toform the dialysate, even trace mineral contaminants or bacterial endotoxins can filter into the
patient's blood. Because the damaged kidneys cannot perform their intended function of removing impurities, ions introduced into the bloodstream via water can build up to hazardouslevels, causing numerous symptoms or death . Aluminum, chloramine, fluoride, copper, and zinc,as well as bacterial fragments and endotoxins, have all caused problems in this regard.
For this reason, water used in hemodialysis is carefully purified before use. Initially it is filteredand temperature-adjusted and its pH is corrected by adding an acid or base. Then it is softened.
Next the water is run through a tank containing activated charcoal to adsorb organiccontaminants. Primary purification is then done by forcing water through a membrane with verytiny pores, a so-called reverse osmosis membrane. This lets the water pass, but holds back evenvery small solutes such as electrolytes. Final removal of leftover electrolytes is done by passingthe water through a tank with ion-exchange resins, which remove any leftover anions or cationsand replace them with hydroxyl and hydrogen molecules, respectively, leaving ultrapure water.
Even this degree of water purification may be insufficient. The trend lately is to pass this final purified water (after mixing with dialysate concentrate) through a dialyzer membrane. This provides another layer of protection by removing impurities, especially those of bacterial origin,that may have accumulated in the water after its passage through the original water purificationsystem.
Once purified water is mixed with dialysate concentrate, its conductivity increases, since water that contains charged ions conducts electricity. During dialysis, the conductivity of dialysissolution is continuously monitored to ensure that the water and dialysate concentrate are beingmixed in the proper proportions. Both excessively concentrated dialysis solution and excessivelydilute solution can cause severe clinical problems.
[edit ] Dialyzer
The dialyzer is the piece of equipment that actually filters the blood. Almost all dialyzers in usetoday are of the hollow-fiber variety. A cylindrical bundle of hollow fibers, whose walls arecomposed of semi-permeable membrane, is anchored at each end into potting compound (a sortof glue). This assembly is then put into a clear plastic cylindrical shell with four openings. One
http://en.wikipedia.org/wiki/Water_purificationhttp://en.wikipedia.org/wiki/Endotoxinshttp://en.wikipedia.org/wiki/Endotoxinshttp://en.wikipedia.org/wiki/Deathhttp://en.wikipedia.org/wiki/Deathhttp://en.wikipedia.org/wiki/Adsorbhttp://en.wikipedia.org/wiki/Reverse_osmosishttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=19http://en.wikipedia.org/wiki/File:CentralDialysatedelivery.JPGhttp://en.wikipedia.org/wiki/File:CentralDialysatedelivery.JPGhttp://en.wikipedia.org/wiki/Water_purificationhttp://en.wikipedia.org/wiki/Endotoxinshttp://en.wikipedia.org/wiki/Deathhttp://en.wikipedia.org/wiki/Adsorbhttp://en.wikipedia.org/wiki/Reverse_osmosishttp://en.wikipedia.org/w/index.php?title=Hemodialysis&action=edit§ion=198/7/2019 The Kidneys and How They Work
28/33
opening or blood port at each end of the cylinder communicates with each end of the bundle of hollow fibers. This forms the "blood compartment" of the dialyzer. Two other ports are cut intothe side of the cylinder. These communicate with the space around the hollow fibers, the"dialysate compartment." Blood is pumped via the blood ports through this bundle of very thincapillary -like tubes, and the dialysate is pumped through the space surrounding the fibers.
Pressure gradients are applied when necessary to move fluid from the blood to the dialysatecompartment.
[edit ] Membrane and flux
Dialyzer membranes come with different pore sizes. Those with smaller pore size are called"low-flux" and those with larger pore sizes are called "high-flux." Some larger molecules, suchas beta-2-microglobulin, are not removed at all with low-flux dialyzers; lately, the trend has beento use high-flux dialyzers. However, such dialyzers require newer dialysis machines and high-quality dialysis solution to control the rate of fluid removal properly and to prevent backflow of dialysis solution impurities into the patient through the membrane.
Dialyzer membranes used to be made primarily of cellulose (derived from cotton linter). Thesurface of such membranes was not very biocompatible, because exposed hydroxyl groupswould activate complement in the blood passing by the membrane. Therefore, the basic,"unsubstituted" cellulose membrane was modified. One change was to cover these hydroxylgroups with acetate groups (cellulose acetate); another was to mix in some compounds thatwould inhibit complement activation at the membrane surface (modified cellulose). The original"unsubstituted cellulose" membranes are no longer in wide use, whereas cellulose acetate andmodified cellulose dialyzers are still used. Cellulosic membranes can be made in either low-fluxor high-flux configuration, depending on their pore size.
Another group of membranes is made from synthetic materials, using polymers such as polyarylethersulfone , polyamide , polyvinylpyrrolidone , polycarbonate, and polyacrylonitrile.These synthetic membranes activate complement to a lesser degree than unsubstituted cellulosemembranes. Synthetic membranes can be made in either low- or high-flux configuration, butmost are high-flux.
Nanotechnology is being used in some of the most recent high-flux membranes to create auniform pore size. The goal of high-flux membranes is to pass relatively large molecules such as
beta-2-microglobulin (MW 11,600 daltons), but not to pass albumin (MW ~66,400 daltons).Every membrane has pores in a range of