Embed Size (px)
Citation preview
Reproductive Toxicology 21 (2006) 350–382
Review
Laboratory assessment and diagnosis of congenital viral infections:Rubella, cytomegalovirus (CMV), varicella-zoster virus (VZV),
herpes simplex virus (HSV), parvovirus B19 andhuman immunodeficiency virus (HIV)
Ella Mendelson a,∗, Yair Aboudy b, Zahava Smetana c, Michal Tepperberg d, Zahava Grossman e
a Central Virology Laboratory, Ministry of Health and Faculty of Life Sciences, Bar-Ilan University, Chaim Sheba Medical Center, Tel-Hashomer, 52621, Israelb National Rubella, Measles and Mumps Center, Central Virology, Laboratory, Ministry of Health, Chaim Sheba Medical Center, Tel-Hashomer, Israel
c National Herpesvirus Center, Central Virology Laboratory, Ministry of Health, Chaim Sheba Medical Center, Tel-Hashomer, Israeld CMV Reference Laboratory, Central Virology Laboratory, Ministry of Health, Chaim Sheba Medical Center, Tel-Hashomer, Israel
e National HIV, EBV and Parvovirus B19 Reference Laboratory, Central Virology Laboratory, Ministry of Health,Chaim Sheba Medical Center, Tel-Hashomer, Israel
Received 14 October 2004; received in revised form 30 January 2006; accepted 7 February 2006
Abstract
Viral infections during pregnancy may cause fetal or neonatal damage. Clinical intervention, which is required for certain viral infections, relieson laboratory tests performed during pregnancy and at the neonatal stage. This review describes traditional and advanced laboratory approachesand testing methods used for assessment of the six most significant viral infections during pregnancy: rubella virus (RV), cytomegalovirus(CMV), varicella-zoster virus (VZV), herpes simplex virus (HSV), parvovirus B19 and human immunodeficiency virus (HIV). Interpretation ofthe laboratory tests results according to studies published in recent years is discussed.© 2006 Elsevier Inc. All rights reserved.
Keywords: Laboratory diagnosis; Congenital viral infections; Rubella; Cytomegalovirus (CMV); Varicella-zoster virus (VZV); Herpes simplex virus (HSV);Parvovirus B19; Human immunodeficiency virus (HIV)
Contents
1. General introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3522. Rubella virus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 352
2.1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3522.1.1. The pathogen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3522.1.2. Immunity and protection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3522.1.3. Laboratory assessment of primary rubella infection in pregnancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3552.1.4. Pre- and postnatal laboratory assessment of congenital rubella infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 357
2.2. Laboratory assays for assessment of rubella infection and immunity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3582.2.1. Rubella neutralization test (NT) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3582.2.2. Hemagglutination inhibition test (HI) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3582.2.3. Rubella specific ELISA IgG. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3582.2.4. Rubella specific ELISA IgM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3582.2.5. Rubella specific IgG-avidity assay . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3592.2.6. Rubella virus isolation in tissue culture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 359
∗ Corresponding author. Tel.: +972 3 530 2421; fax: +972 3 535 0436.E-mail address: [email protected] (E. Mendelson).
0890-6238/$ – see front matter © 2006 Elsevier Inc. All rights reserved.doi:10.1016/j.reprotox.2006.02.001
E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 351
2.2.7. Rubella RT-PCR assay . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3592.3. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 359
3. Cytomegalovirus (CMV) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3603.1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 360
3.1.1. The pathogen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3603.1.2. Laboratory assessment of CMV infection in pregnant women. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3603.1.3. Prenatal assessment of congenital CMV infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 360
3.2. Laboratory assays for assessment of CMV infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3613.2.1. CMV IgM assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3613.2.2. CMV IgG assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3613.2.3. CMV IgG avidity assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3613.2.4. CMV neutralization assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3623.2.5. Virus isolation in tissue culture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3623.2.6. Detection of CMV by PCR . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3623.2.7. Quantitative PCR-based assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 362
3.3. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3634. Varicella-zoster virus (VZV) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 363
4.1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3634.1.1. The pathogen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3634.1.2. Assessment of VZV infection in pregnancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3634.1.3. Prenatal and perinatal laboratory assessment of congenital VZV infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 364
4.2. Laboratory assays for assessment of VZV infection and immunity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3644.2.1. VZV IgG assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3644.2.2. VZV IgM assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3644.2.3. Virus detection in clinical specimens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3644.2.4. Virus isolation in tissue culture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3644.2.5. Direct detection of VZV antigen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3644.2.6. Molecular methods for detection of viral DNA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 364
4.3. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3655. Herpes simplex virus (HSV) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 365
5.1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3655.1.1. The pathogen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3655.1.2. Laboratory assessment of HSV infection in pregnancy and in neonates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 365
5.2. Laboratory assays for assessment of HSV infection and immune status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3665.2.1. HSV IgG assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3665.2.2. HSV type-specific IgG assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3665.2.3. HSV IgM assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3665.2.4. Virus isolation in tissue culture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3665.2.5. Direct antigen detection of HSV . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3665.2.6. Detection of HSV DNA by PCR . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 366
5.3. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3676. Parvovirus B19 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 367
6.1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3676.1.1. The pathogen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3676.1.2. Laboratory assessment of parvovirus B19 infection in pregnancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3676.1.3. Prenatal laboratory assessment of congenital B19 infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 367
6.2. Laboratory assays for assessment of parvovirus B19 infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3686.2.1. B19 IgM and IgG assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3686.2.2. Detection of viral DNA in maternal and fetal specimens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3686.2.3. Quantitative assays for detection of viral DNA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 369
6.3. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3697. Human immunodeficiency virus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 369
7.1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3697.1.1. The pathogen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3697.1.2. Importance of laboratory assessment of HIV infection in pregnancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3707.1.3. Prenatal laboratory assessment of HIV infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 370
7.2. Laboratory assessment of HIV infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3707.2.1. HIV antibody assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3707.2.2. Detection of viral DNA in maternal and newborn specimens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 371
7.3. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 372Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 372References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 372

352 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
1. General introduction
Viral infections during pregnancy carry a risk for intrauterinetransmission which may result in fetal damage. The conse-quences of fetal infection depend on the virus type: for manycommon viral infections there is no risk for fetal damage, butsome viruses are teratogenic while others cause fetal or neonataldiseases ranging in severity from mild and transient symptomsto a fatal disease. In cases where infection during pregnancyprompts clinical decisions, laboratory diagnostic tests are anessential part of the clinical assessment process. This reviewdescribes the six most important viruses for which laboratoryassessement during pregnancy is required and experience hasbeen gained over many years. Rubella virus and CMV are ter-atogenic viruses, while VZV, HSV, parvovirus B19 and HIVcause fetal or neonatal transient or chronic disease.
The ability of viruses to cross the placenta, infect the fetusand cause damage depends, among other factors, on the mother’simmune status against the specific virus. In general, primaryinfections during pregnancy are substantially more damagingthan secondary infections or reactivations.
Laboratory testing of maternal immune status is required todiagnose infection and distinguish between primary and sec-ondary infections. Assessment of fetal damage and prognosisrequires prenatal laboratory testing primarily in those caseswhere a clinical decision such as drug treatment, pregnancy ter-m
ttbai
tdsfsustotaec
sf(uatbTt
Since the algorithm for maternal and fetal assessment and theinterpretation of tests results vary from one virus to another, wehave described the approach to each viral infection in a separatechapter. Figs. 1–6 depict the most common algorithms used forthe laboratory diagnosis of each of the viral infections
2. Rubella virus
2.1. Introduction
2.1.1. The pathogenRubella is a highly transmissible childhood disease which
can cause large outbreaks every few years. It is a vaccine pre-ventable disease and in developed countries outbreaks are mostlyconfined to unvaccinated communities [1]. Rubella reinfectionfollowing natural infection is very rare. Rubella virus (RV) isclassified as a member of the togaviridae family and is the onlyvirus of the genus rubivirus [2]. Hemagglutinating activity and atleast three antibody neutralization domains were assigned to theearly proteins E1 and E2 [3–5]. At least one weak neutralizationdomain was identified on E2 [5].
The main route of postnatal virus transmission is by directcontact with nasopharyngial secretions [6]. Postnatal RV infec-tion is a generally mild and self-limited illness [6–8], but primaryRV infections during the first trimester of pregnancy have highteratogenic potential leading to severe consequences, known ascoi(
2
mgnRfpvay
N(dtbtuaRoartf
ination or intrauterine IgG transfusion must be taken.This review describes basic virological facts and explains
he laboratory approaches and techniques used for the diagnos-ic process. It aims at familiarizing physicians with the rationalehind the laboratory requests for specific and timely specimensnd with the interpretation of the tests results including its lim-tations.
The laboratory methods used for assessment of viral infec-ions in general are of two categories: serology and virusetection. Serology is very sensitive but often cannot conclu-ively determine the time of infection, which may be criticalor risk assessment. Traditional serological tests, which mea-ure antibody levels without distinction between IgM and IgG,sually require two samples for determination of seroconver-ion or a substantial rise in titer. The modern tests can dis-inguish between IgG and IgM and may allow diagnosis inne serum sample. However, biological and technical difficul-ies are common and may cause false positive and false neg-tive results. The properties of all serological assays used forach of the viruses will be described in detail in the followinghapters.
Virus detection is used primarily for prenatal diagnosis. Inva-ive procedures must be used to obtain samples representing theetus such as amniotic fluid (AF), cord blood and chorionic villiCV). The traditional “gold standard” assay for virus detectionsed to be virus isolation in tissue culture, but other, more rapidnd sensitive methods were developed in recent years. Amonghe new methods are direct antigen detection by specific anti-odies and amplification and detection of viral nucleic acids.he general characteristics of all laboratory assays described in
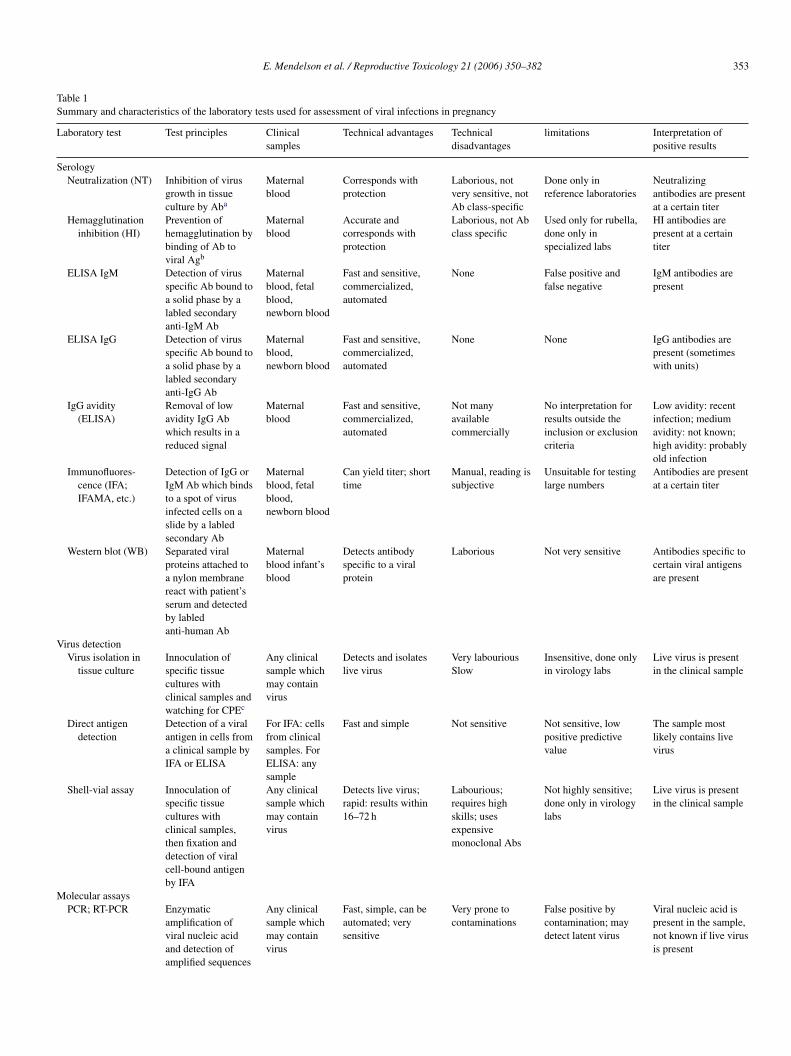
his article are summarized in Table 1.
ongenital rubella syndrome (CRS) which may occur in 80–85%f cases [8,9]. It should be emphasized that more than 50% of RVnfections in non-immunized persons in the general populationand in pregnant women) are subclinical [6–9].
.1.2. Immunity and protectionAntibody level of 10–15 international units (IU) of IgG per
illilitre is considered protective. Naturally acquired rubellaenerally confers lifelong and usually high degree of immu-ity against the disease for the majority of individuals [10,11].ubella vaccination induces immunity that confers protection
rom viraemia in the vast majority of vaccinees, which usuallyersists for more than 16 years [10–12]. A small fraction of theaccinees fail to respond or develop low levels of detectablentibodies which may decline to undetectable levels within 5–8ears from vaccination [13–17].
Several methods are used to determine immunity (Table 1).eutralization test (NT) and hemagglutination inhibition test
HI) correlate well with protective immunity, but since they areifficult to perform and to standardize, they were replaced byhe more rapid, facile and sensitive enzyme-linked immunosor-ant assay (ELISA) [5,18]. In our experience (unpublished data),here is a clear distinction between antibody levels measuredsing ELISA, and antibody levels measured using functionalssays such as NT and HI. Moreover, standardization of antiV antibody assays using different techniques and a varietyf antigens (i.e., whole virus, synthetic peptides, recombinantntigen, etc.) has not been achieved, leading to uncertaintiesegarding the antibody levels that confer immunity and protec-ion against reinfections and against virus transmission to theetus [19–26]. Most of the reinfection cases (9 out of 18 cases;
E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 353
Table 1Summary and characteristics of the laboratory tests used for assessment of viral infections in pregnancy
Laboratory test Test principles Clinicalsamples
Technical advantages Technicaldisadvantages
limitations Interpretation ofpositive results
SerologyNeutralization (NT) Inhibition of virus
growth in tissueculture by Aba
Maternalblood
Corresponds withprotection
Laborious, notvery sensitive, notAb class-specific
Done only inreference laboratories
Neutralizingantibodies are presentat a certain titer
Hemagglutinationinhibition (HI)
Prevention ofhemagglutination bybinding of Ab toviral Agb
Maternalblood
Accurate andcorresponds withprotection
Laborious, not Abclass specific
Used only for rubella,done only inspecialized labs
HI antibodies arepresent at a certaintiter
ELISA IgM Detection of virusspecific Ab bound toa solid phase by alabled secondaryanti-IgM Ab
Maternalblood, fetalblood,newborn blood
Fast and sensitive,commercialized,automated
None False positive andfalse negative
IgM antibodies arepresent
ELISA IgG Detection of virusspecific Ab bound toa solid phase by alabled secondaryanti-IgG Ab
Maternalblood,newborn blood
Fast and sensitive,commercialized,automated
None None IgG antibodies arepresent (sometimeswith units)
IgG avidity(ELISA)
Removal of lowavidity IgG Abwhich results in areduced signal
Maternalblood
Fast and sensitive,commercialized,automated
Not manyavailablecommercially
No interpretation forresults outside theinclusion or exclusioncriteria
Low avidity: recentinfection; mediumavidity: not known;high avidity: probablyold infection
Immunofluores-cence (IFA;IFAMA, etc.)
Detection of IgG orIgM Ab which bindsto a spot of virusinfected cells on aslide by a labledsecondary Ab
Maternalblood, fetalblood,newborn blood
Can yield titer; shorttime
Manual, reading issubjective
Unsuitable for testinglarge numbers
Antibodies are presentat a certain titer
Western blot (WB) Separated viralproteins attached toa nylon membranereact with patient’sserum and detectedby labledanti-human Ab
Maternalblood infant’sblood
Detects antibodyspecific to a viralprotein
Laborious Not very sensitive Antibodies specific tocertain viral antigensare present
Virus detectionVirus isolation in
tissue cultureInnoculation ofspecific tissuecultures withclinical samples andwatching for CPEc
Any clinicalsample whichmay containvirus
Detects and isolateslive virus
Very labouriousSlow
Insensitive, done onlyin virology labs
Live virus is presentin the clinical sample
Direct antigendetection
Detection of a viralantigen in cells froma clinical sample byIFA or ELISA
For IFA: cellsfrom clinicalsamples. ForELISA: anysample
Fast and simple Not sensitive Not sensitive, lowpositive predictivevalue
The sample mostlikely contains livevirus
Shell-vial assay Innoculation ofspecific tissuecultures withclinical samples,then fixation anddetection of viralcell-bound antigenby IFA
Any clinicalsample whichmay containvirus
Detects live virus;rapid: results within16–72 h
Labourious;requires highskills; usesexpensivemonoclonal Abs
Not highly sensitive;done only in virologylabs
Live virus is presentin the clinical sample
Molecular assaysPCR; RT-PCR Enzymatic
amplification ofviral nucleic acidand detection ofamplified sequences
Any clinicalsample whichmay containvirus
Fast, simple, can beautomated; verysensitive
Very prone tocontaminations
False positive bycontamination; maydetect latent virus
Viral nucleic acid ispresent in the sample,not known if live virusis present
354 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
Table 1 (Continued )
Laboratory test Test principles Clinicalsamples
Technical advantages Technicaldisadvantages
limitations Interpretation ofpositive results
Real-timePCR/RT-PCR
Detection ofaccumulating PCRproducts by afluorescent dye orprobe in aspecializedinstrument
Any clinicalsample whichmay containvirus
Very fast, simple notprone tocontaminations; canbe quantitative
Expensiveinstruments
Sometimes toosensitive,interpretation of verylow resultquestionable
Viral nucleic acid ispresent in the sample(at a certain amount),not known if live virusis present
In situhybridization
Detection of viralnucleic acid insmears or tissuesections by labledprobes
Cells or tissuefrom clinicalsamples
Sensitive and specific Difficult toperform
Done only inspecializing labs
Viral nucleic acid ispresent in the sample,not known if live virusis present
In situ PCR Detection of viralnucleic acid insmears or tissuesections by PCRusing labled primers
Cells or tissuefrom clinicalsamples
Sensitive and specific Difficult toperform
Doe only inspecializing labs
Viral nucleic acid ispresent in the sample,not known if live virusis present
a Antibody.b Antigen.c Cytopathic effect.
50%) which were detected during an outbreak in Israel in 1992occurred in the presence of low neutralizing antibody titers of1:4 (cut off level), and sharp decline in the reinfection rate corre-lated with the presence of higher titers of neutralizing antibodies(unpublished data). Reinfection rates following vaccination are
considerably higher than following natural infection, rangingbetween 10% and 20% [19].
Many developed countries adopted the infant routine vacci-nation policy using MMR (mumps measles and rubella) vaccinedesigned to provide indirect protection of child-bearing age
F m shoa womw nth ob tion.o ed onp testsradvs
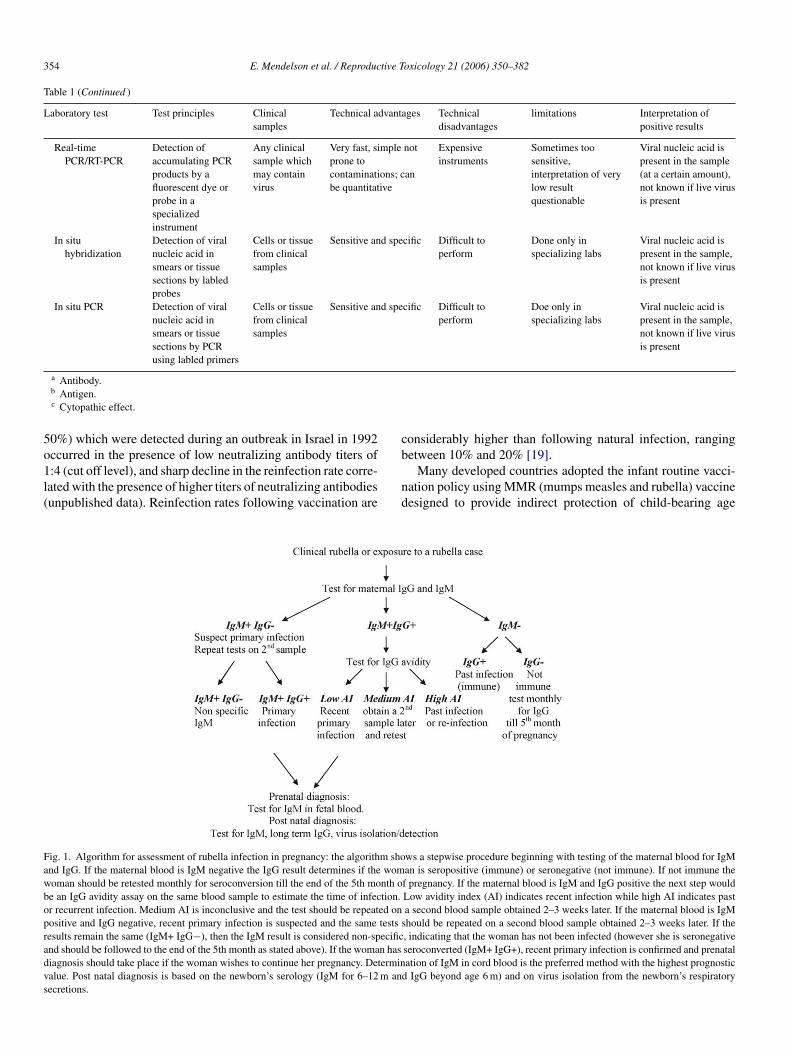
ig. 1. Algorithm for assessment of rubella infection in pregnancy: the algorithnd IgG. If the maternal blood is IgM negative the IgG result determines if theoman should be retested monthly for seroconversion till the end of the 5th moe an IgG avidity assay on the same blood sample to estimate the time of infecr recurrent infection. Medium AI is inconclusive and the test should be repeatositive and IgG negative, recent primary infection is suspected and the same
esults remain the same (IgM+ IgG−), then the IgM result is considered non-specificnd should be followed to the end of the 5th month as stated above). If the woman hasiagnosis should take place if the woman wishes to continue her pregnancy. Determinalue. Post natal diagnosis is based on the newborn’s serology (IgM for 6–12 m anecretions.ws a stepwise procedure beginning with testing of the maternal blood for IgMan is seropositive (immune) or seronegative (not immune). If not immune thef pregnancy. If the maternal blood is IgM and IgG positive the next step wouldLow avidity index (AI) indicates recent infection while high AI indicates pasta second blood sample obtained 2–3 weeks later. If the maternal blood is IgM
should be repeated on a second blood sample obtained 2–3 weeks later. If the
, indicating that the woman has not been infected (however she is seronegativeseroconverted (IgM+ IgG+), recent primary infection is confirmed and prenatalation of IgM in cord blood is the preferred method with the highest prognosticd IgG beyond age 6 m) and on virus isolation from the newborn’s respiratory
E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 355
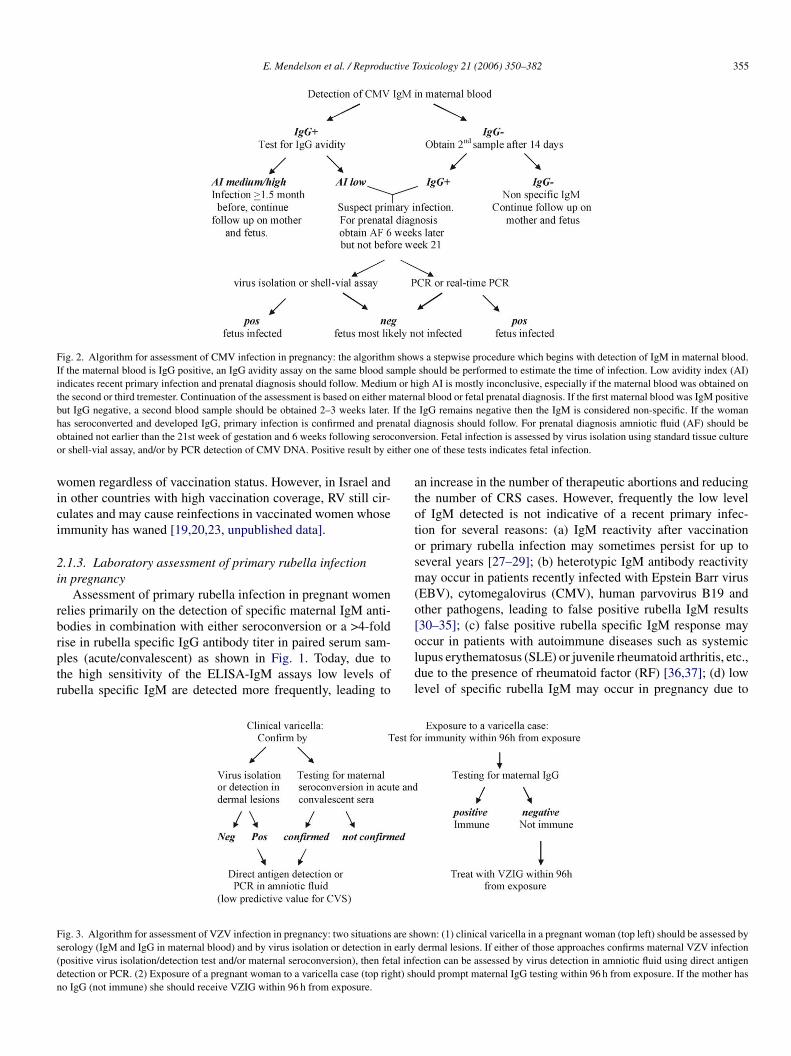
Fig. 2. Algorithm for assessment of CMV infection in pregnancy: the algorithm shows a stepwise procedure which begins with detection of IgM in maternal blood.If the maternal blood is IgG positive, an IgG avidity assay on the same blood sample should be performed to estimate the time of infection. Low avidity index (AI)indicates recent primary infection and prenatal diagnosis should follow. Medium or high AI is mostly inconclusive, especially if the maternal blood was obtained onthe second or third tremester. Continuation of the assessment is based on either maternal blood or fetal prenatal diagnosis. If the first maternal blood was IgM positivebut IgG negative, a second blood sample should be obtained 2–3 weeks later. If the IgG remains negative then the IgM is considered non-specific. If the womanhas seroconverted and developed IgG, primary infection is confirmed and prenatal diagnosis should follow. For prenatal diagnosis amniotic fluid (AF) should beobtained not earlier than the 21st week of gestation and 6 weeks following seroconversion. Fetal infection is assessed by virus isolation using standard tissue cultureor shell-vial assay, and/or by PCR detection of CMV DNA. Positive result by either one of these tests indicates fetal infection.
women regardless of vaccination status. However, in Israel andin other countries with high vaccination coverage, RV still cir-culates and may cause reinfections in vaccinated women whoseimmunity has waned [19,20,23, unpublished data].
2.1.3. Laboratory assessment of primary rubella infectionin pregnancy
Assessment of primary rubella infection in pregnant womenrelies primarily on the detection of specific maternal IgM anti-bodies in combination with either seroconversion or a >4-foldrise in rubella specific IgG antibody titer in paired serum sam-ples (acute/convalescent) as shown in Fig. 1. Today, due tothe high sensitivity of the ELISA-IgM assays low levels ofrubella specific IgM are detected more frequently, leading to
an increase in the number of therapeutic abortions and reducingthe number of CRS cases. However, frequently the low levelof IgM detected is not indicative of a recent primary infec-tion for several reasons: (a) IgM reactivity after vaccinationor primary rubella infection may sometimes persist for up toseveral years [27–29]; (b) heterotypic IgM antibody reactivitymay occur in patients recently infected with Epstein Barr virus(EBV), cytomegalovirus (CMV), human parvovirus B19 andother pathogens, leading to false positive rubella IgM results[30–35]; (c) false positive rubella specific IgM response mayoccur in patients with autoimmune diseases such as systemiclupus erythematosus (SLE) or juvenile rheumatoid arthritis, etc.,due to the presence of rheumatoid factor (RF) [36,37]; (d) lowlevel of specific rubella IgM may occur in pregnancy due to
F are shs early( al infd ht) shn
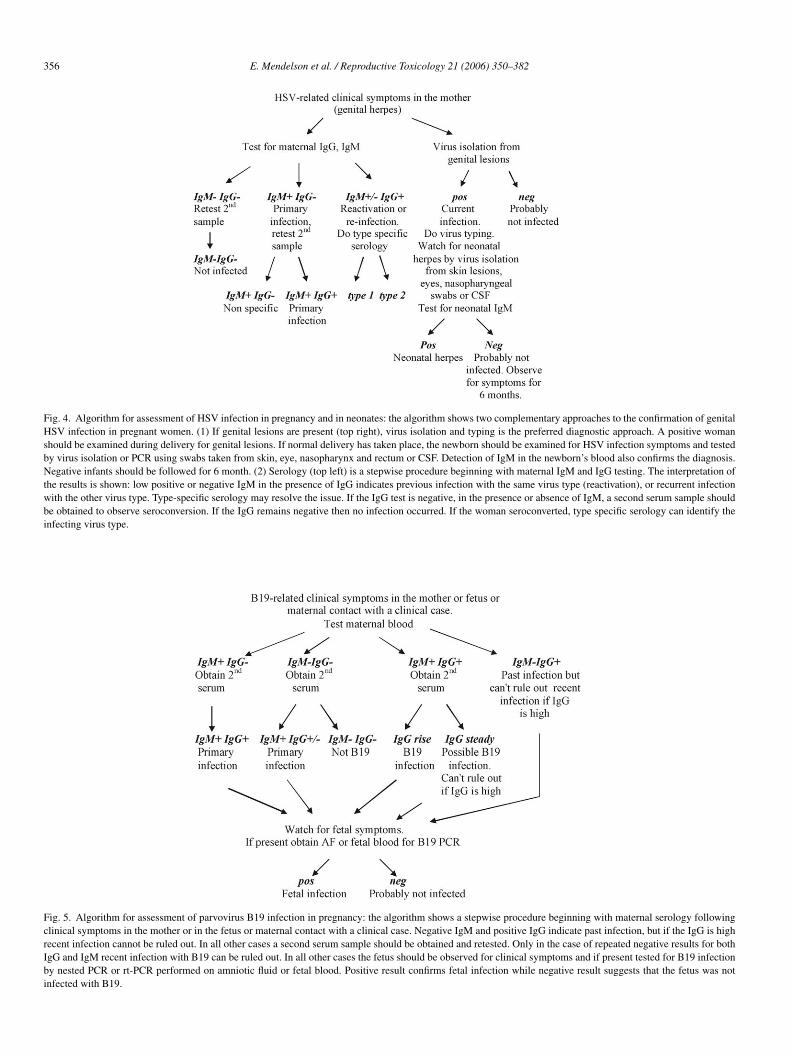
ig. 3. Algorithm for assessment of VZV infection in pregnancy: two situationserology (IgM and IgG in maternal blood) and by virus isolation or detection inpositive virus isolation/detection test and/or maternal seroconversion), then fetetection or PCR. (2) Exposure of a pregnant woman to a varicella case (top rigo IgG (not immune) she should receive VZIG within 96 h from exposure.
own: (1) clinical varicella in a pregnant woman (top left) should be assessed bydermal lesions. If either of those approaches confirms maternal VZV infection
ection can be assessed by virus detection in amniotic fluid using direct antigenould prompt maternal IgG testing within 96 h from exposure. If the mother has
356 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
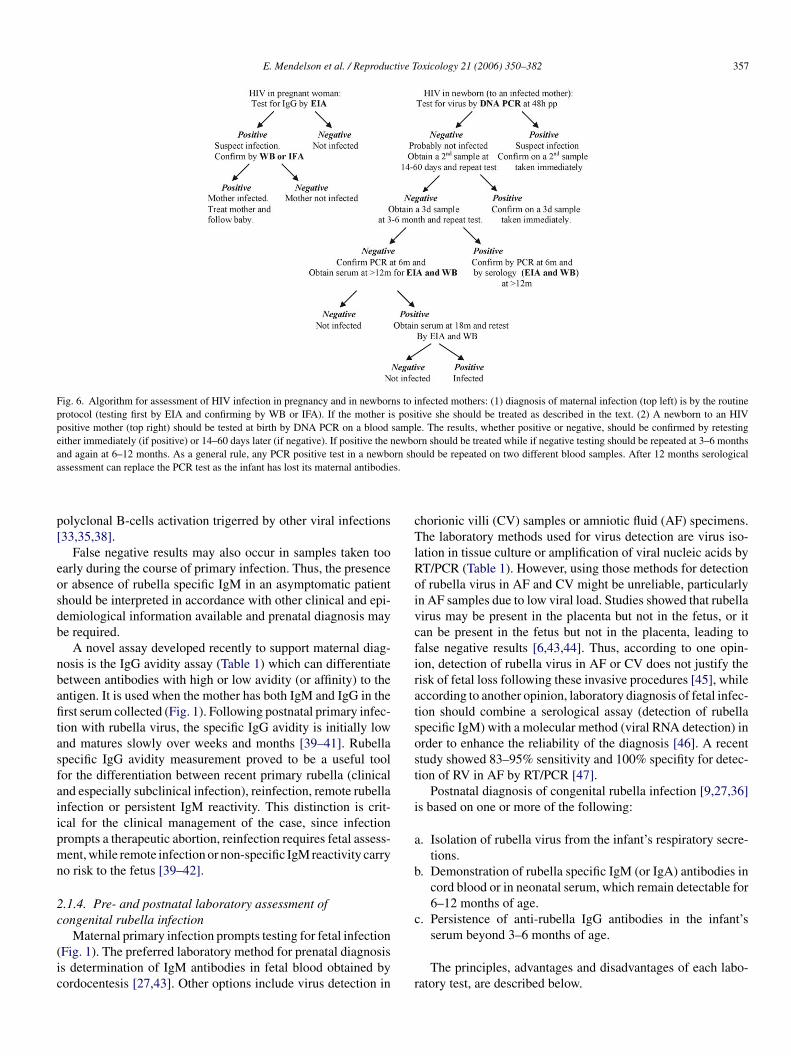
Fig. 4. Algorithm for assessment of HSV infection in pregnancy and in neonates: the algorithm shows two complementary approaches to the confirmation of genitalHSV infection in pregnant women. (1) If genital lesions are present (top right), virus isolation and typing is the preferred diagnostic approach. A positive womanshould be examined during delivery for genital lesions. If normal delivery has taken place, the newborn should be examined for HSV infection symptoms and testedby virus isolation or PCR using swabs taken from skin, eye, nasopharynx and rectum or CSF. Detection of IgM in the newborn’s blood also confirms the diagnosis.Negative infants should be followed for 6 month. (2) Serology (top left) is a stepwise procedure beginning with maternal IgM and IgG testing. The interpretation ofthe results is shown: low positive or negative IgM in the presence of IgG indicates previous infection with the same virus type (reactivation), or recurrent infectionwith the other virus type. Type-specific serology may resolve the issue. If the IgG test is negative, in the presence or absence of IgM, a second serum sample shouldbe obtained to observe seroconversion. If the IgG remains negative then no infection occurred. If the woman seroconverted, type specific serology can identify theinfecting virus type.
Fig. 5. Algorithm for assessment of parvovirus B19 infection in pregnancy: the algorithm shows a stepwise procedure beginning with maternal serology followingclinical symptoms in the mother or in the fetus or maternal contact with a clinical case. Negative IgM and positive IgG indicate past infection, but if the IgG is highrecent infection cannot be ruled out. In all other cases a second serum sample should be obtained and retested. Only in the case of repeated negative results for bothIgG and IgM recent infection with B19 can be ruled out. In all other cases the fetus should be observed for clinical symptoms and if present tested for B19 infectionby nested PCR or rt-PCR performed on amniotic fluid or fetal blood. Positive result confirms fetal infection while negative result suggests that the fetus was notinfected with B19.
E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 357
Fig. 6. Algorithm for assessment of HIV infection in pregnancy and in newborns to infected mothers: (1) diagnosis of maternal infection (top left) is by the routineprotocol (testing first by EIA and confirming by WB or IFA). If the mother is positive she should be treated as described in the text. (2) A newborn to an HIVpositive mother (top right) should be tested at birth by DNA PCR on a blood sample. The results, whether positive or negative, should be confirmed by retestingeither immediately (if positive) or 14–60 days later (if negative). If positive the newborn should be treated while if negative testing should be repeated at 3–6 monthsand again at 6–12 months. As a general rule, any PCR positive test in a newborn should be repeated on two different blood samples. After 12 months serologicalassessment can replace the PCR test as the infant has lost its maternal antibodies.
polyclonal B-cells activation trigerred by other viral infections[33,35,38].
False negative results may also occur in samples taken tooearly during the course of primary infection. Thus, the presenceor absence of rubella specific IgM in an asymptomatic patientshould be interpreted in accordance with other clinical and epi-demiological information available and prenatal diagnosis maybe required.
A novel assay developed recently to support maternal diag-nosis is the IgG avidity assay (Table 1) which can differentiatebetween antibodies with high or low avidity (or affinity) to theantigen. It is used when the mother has both IgM and IgG in thefirst serum collected (Fig. 1). Following postnatal primary infec-tion with rubella virus, the specific IgG avidity is initially lowand matures slowly over weeks and months [39–41]. Rubellaspecific IgG avidity measurement proved to be a useful toolfor the differentiation between recent primary rubella (clinicaland especially subclinical infection), reinfection, remote rubellainfection or persistent IgM reactivity. This distinction is crit-ical for the clinical management of the case, since infectionprompts a therapeutic abortion, reinfection requires fetal assess-ment, while remote infection or non-specific IgM reactivity carryno risk to the fetus [39–42].
2.1.4. Pre- and postnatal laboratory assessment ofcongenital rubella infection
(ic
chorionic villi (CV) samples or amniotic fluid (AF) specimens.The laboratory methods used for virus detection are virus iso-lation in tissue culture or amplification of viral nucleic acids byRT/PCR (Table 1). However, using those methods for detectionof rubella virus in AF and CV might be unreliable, particularlyin AF samples due to low viral load. Studies showed that rubellavirus may be present in the placenta but not in the fetus, or itcan be present in the fetus but not in the placenta, leading tofalse negative results [6,43,44]. Thus, according to one opin-ion, detection of rubella virus in AF or CV does not justify therisk of fetal loss following these invasive procedures [45], whileaccording to another opinion, laboratory diagnosis of fetal infec-tion should combine a serological assay (detection of rubellaspecific IgM) with a molecular method (viral RNA detection) inorder to enhance the reliability of the diagnosis [46]. A recentstudy showed 83–95% sensitivity and 100% specifity for detec-tion of RV in AF by RT/PCR [47].
Postnatal diagnosis of congenital rubella infection [9,27,36]is based on one or more of the following:
a. Isolation of rubella virus from the infant’s respiratory secre-tions.
b. Demonstration of rubella specific IgM (or IgA) antibodies incord blood or in neonatal serum, which remain detectable for6–12 months of age.
c. Persistence of anti-rubella IgG antibodies in the infant’s
r
Maternal primary infection prompts testing for fetal infectionFig. 1). The preferred laboratory method for prenatal diagnosiss determination of IgM antibodies in fetal blood obtained byordocentesis [27,43]. Other options include virus detection in
serum beyond 3–6 months of age.
The principles, advantages and disadvantages of each labo-atory test, are described below.

358 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
2.2. Laboratory assays for assessment of rubella infectionand immunity
2.2.1. Rubella neutralization test (NT)Virus neutralization is defined as the loss of infectivity due to
reaction of a virus with specific antibody. Neutralization can beused to identify virus isolates or, as in the case of rubella diagno-sis, to measure the immune response to the virus [24,36,48]. Asa functional test, neutralization has proven to be highly sensitive,specific and reliable technique, but it can be performed only invirology laboratories which comprise only a small fraction ofthe laboratories performing rubella serology.
Rubella virus produces characteristic damage (cytopathiceffect, CPE) in the RK-13 cell line that was found most sen-sitive and suitable for use in rubella neutralization test. Othercells such as Vero and SIRC lines can be used if conditionsare carefully controlled [36]. Principally, 2-fold dilutions ofeach test serum are mixed and incubated with 100 infectiousunits of rubella virus under appropriate conditions. Then cellmonolayers are inoculated with each mixture and followed forCPE. Control sera possessing known high and low neutralizingantibody levels and titrations of the virus are included in eachtest run. The neutralization titer is taken as the reciprocal ofthe highest serum dilution showing complete inhibition of CPE[25,36].
2
strpsatvit
tA1spbitttinr
trmo
2.2.3. Rubella specific ELISA IgGThe ELISA technique was established for detection of an
increasing range of antibodies to viral antigens. In 1976, Volleret al. [58] developed an indirect assay for the detection of anti-viral antibodies. The technique has been successfully appliedfor the detection of rubella specific antibodies.
Almost all commercially available ELISA kits for the detec-tion of rubella specific IgG are of the indirect type, employingrubella antigen attached to a solid phase (microtiter polystyreneplates or plastic beads). The source of the antigen (peptide,recombinant or whole virus antigen) affects the sensitivity andspecificity of the assay. After washing and removal of unboundantigen, diluted test serum is added and incubated with theimmobilized antigen. The rubella specific antibodies present inthe serum bind to the antigen. Then, unbound antibodies areremoved by washing and an enzyme conjugated anti-human IgGis added and further incubation is carried out. The quantity of theconjugate that binds to each well is proportional to the concen-tration of the rubella specific antibodies present in the patient’sserum. The plates are then washed and substrate is added result-ing in color development. The enzymatic reaction is stoppedafter a short incubation period, and optical density (OD) is mea-sured by an ELISA-reader instrument. The test principle allowsthe detection of IgM as well by using an appropriate anti-humanIgM conjugate [53,57].
In most commercial ELISA IgG assays the results are auto-mta[rat
itgaisiEtsai
2
a
a
.2.2. Hemagglutination inhibition test (HI)Until recently, assessment of rubella immunity and diagno-
is of rubella infection has been carried out mainly by the HIest which is based on the ability of rubella virus to agglutinateed blood cells [49]. HI test is labor intensive, and is currentlyerformed mainly by reference laboratories. HI is the “goldtandard” test against which almost all other rubella screeningnd diagnostic tests are measured. During the test, the agglu-ination is inhibited by binding of specific antibodies to theiral agglutinin. Titers are expressed as the highest dilutionnhibiting hemagglutination under standardized testing condi-ions [50–53].
The HI antibodies increase rapidly after RV infection sincehe test detects both, IgG and IgM class-specific antibodies.
titer of l:8 is commonly considered negative (cut off level::16) and a titer of ≥1:32 indicates an earlier RV infection oruccessful vaccination and immunity. Seroconversion is inter-reted as primary rubella infection, and a 4-fold increase in titeretween two serum samples (paired sera) in the same test series,s interpreted as a recent primary rubella infection or reinfec-ion [52]. Considerable experience has been accumulated overhe years in the interpretation of the clinical significance of HIiters [52–54], and the test results accurately correlate with clin-cal protection [5,18]. Although HI is generally considered asot sensitive enough, in certain situations it is still in use foresolution of diagnostic uncertainties.
Detection of rubella specific IgM class antibodies by HIest which requires tedious methods for purification of IgM oremoval of IgG [55,56], are no longer in use due to the develop-ent of a variety of rapid, easy to perform and sensitive methods,
f which ELISA is the most vastly used [18,57].
atically calculated and expressed quantitatively in interna-ional units (IU). When performed manually, the procedure takespproximately 3 h but automation has reduced it to about 30 min57–59]. It is important to note that in order to obtain reliableesults, determination of a significant change in specific IgGctivity in paired serum samples should always be performed inhe same test run and in the same test dilution.
The correlation between the ELISA and HI or NT titerss not always high. This may be explained by the fact thathe three methods detect antibodies directed to different anti-enic determinants [54]. Certain individuals fail to developntibodies directed to protective epitopes such as the neutral-zing domains of E1 and E2 due to a defect in their rubellapecific immune responses [21] but they do develop antibod-es directed to antigenic sub-regions of rubella virus proteins.LISA assays utilizing whole virus as antigen may fail to dis-
inguish between these different antibody specificities. Thus,eroconversion determined by ELISA based on a whole virusntigen does not necessarily correlate with protection againstnfection [52].
.2.4. Rubella specific ELISA IgMCommercially available ELISA kits for the detection of IgM
re mainly of two types:
. Indirect ELISA: The principle of the assay was describedabove for rubella IgG except for using enzyme labeled anti-human IgM as a conjugate. In this assay, false negative resultsmay occur due to a competition in the assay between specificIgG antibodies with high affinity (interfering IgG) while thespecific IgM have lower affinity for the antigen [31,32]. In the

E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 359
new generation ELISA assays this is avoided by the additionof an absorbent reagent for the removal of IgG from the testserum. False positive results may occur if rheumatoid factor(RF: IgM anti-IgG antibodies) is present along with specificIgG in the test serum. Absorption or removal of RF and/orIgG is necessary prior to the assay to avoid such reactions[30–32,60].
b. IgM capture ELISA: In these assays anti-human IgM anti-body is attached to the solid phase for capture of serumIgM. Rubella virus antigen conjugated to enzyme-labeledanti-rubella virus antibody is added for detection. This typeof assay eliminates the need for sample pretreatment priorto the assay [32,61]. As for the rubella virus antigens, mostassays are based on whole virus extracts, but recent develop-ments led to production of recombinant and synthetic rubellavirus proteins [5,62].
2.2.5. Rubella specific IgG-avidity assayThis assay is based on the ELISA IgG technique and
applies the elution principle in which protein denaturant, mostlyurea (but also diethylamine, ammonium thiocyanate, guanidinehydrochloride, etc.) is added after binding of the patient’s serum.The denaturant disrupts hydrophobic bonds between antibodyand antigen, and thus, low avidity IgG antibodies produced dur-ing the early stage of infection are removed. This results in asignificant reduction in the IgG absorbance level [63]. The avid-i[
A
tbwam
dwf
2
etdtbpbflsts4p
Rubella virus can be grown in a variety of primary cells andcell lines [36,65], but RK-13 and Vero cell lines are the most sen-sitive and suitable for routine use. In these cell systems rubellavirus produces characteristic CPE. Since the CPE is not alwaysclear upon primary isolation, at least two successive subpas-sages are required [66]. When CPE is evident the identity of thevirus isolates should be confirmed using immunological or othermethods [36,65,67].
2.2.7. Rubella RT-PCR assayReverse transcription followed by PCR amplification (RT-
PCR) is a rapid, sensitive and specific technique for detectionof rubella virus RNA in clinical samples using primers fromthe envelope glycoprotein E1 open reading frame [45,46,68,69].Coding sequences for a major group of antigenic determinantsare located between nucleotides 731 and 854 of the E1 geneof RV strain M33. This region is highly conserved in variouswild type strains and is likely to be present in most clinicalsamples from rubella infected patients. Specific oligonucleotideprimers located in this region were designed for amplificationby RT-PCR [70–72]. Following rubella genomic RNA extractionfrom clinical specimens and RT-PCR amplification, the productis visualized by gel electrophoresis. Positive samples show aspecific band of the expected size compared to size markers[68,69,72].
A nested RT-PCR assay, in which the RT-PCR productfpstl
iAb[nal
tt[idi
2
ticaMpa
ty index (AI) is calculated according to the following formula57]:
I = 100 × absorbance of avidity ELISA
absorbance of standard ELISA
The AI is a useful measure only when the IgG concentration inhe patient’s serum is not below 25 IU [39]. Low avidity (usuallyelow 50%) is associated with recent primary rubella infectionhile reinfection is typically associated with high avidity asresult of the stimulation of memory B cells (immunologicalemory) [39–41].In infants with CRS the low avidity IgG continues to be pro-
uced for much longer than in cases of postnatal primary rubella,here it lasts 4–6 week after exposure [39]. This may be used
or retrospective assessment of initially undiagnosed CRS cases.
.2.6. Rubella virus isolation in tissue cultureDiagnosis of prenatal or postnatal rubella infections are
ssentially based on the more reliable and rapid serologicalechniques. However, virus isolation is useful in confirming theiagnosis of CRS (Fig. 1) and rubella virus strain characteriza-ion required for epidemiological purposes. Rubella virus cane isolated using a variety of clinical specimens such as: res-iratory secretions (nasopharyngeal swabs), urine, heparinizedlood, CSF, cataract material, lens fluid, amniotic fluid, synovialuid and products of conception (fetal tissues: placenta, liver,kin, etc.) obtained following spontaneous or therapeutic abor-ion [6,36,44,64]. In order to avoid virus inactivation, specimenshould be inoculated into cell culture immediately or stored at◦C for not more than 2 days, or kept frozen (−70◦ C) for longereriods [36].
rom the first amplification reaction is re-amplified by internalrimers, was developed and shown to provide a higher level ofensitivity for the detection of rubella virus RNA [72]. However,he risk of contamination is markedly increased. The detectionimit of the RT-PCR assay is approximately two RNA copies.
Clinical specimens for rubella virus genome detectionnclude: products of conception (POC), CV, lens aspirate/biopsy,F, fetal blood, pharyngeal swabs and spinal fluid (CSF) orrain biopsy when the central nervous system (CNS) is involved68,69,73–75]. An additional advantage of RT-PCR is that it doesot require infectious virus [74]. RV is extremely thermo-labilend frequently is inactivated during sample transporation to theaboratory.
Finally, it should be noted that clinical samples may con-ain PCR inhibitors (such as heparin and hemoglobin), andhe extraction procedure itself may cause enzyme inhibition72,76,77]. This underscores the need and importance for strictnternal quality control during each step of the RT-PCR proce-ure and participation in external quality assessment programss of a high value.
.3. Summary
Rubella infection during pregnancy, although rare in coun-ries with routine vaccination programs, is still a problem requir-ng careful laboratory assessment. The laboratory testing shouldonfirm or rule-out recent rubella infection in pregnant womennd identify congenital rubella infections in the fetus or neonate.aternal infection is currently assessed by serological assays,
rimarily by ELISA IgM and IgG. Borderline results for the IgGssay can be further assessed by the HI or NT assays available

360 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
in reference laboratories. Confirmation of recent infection canbe sought using the IgG-avidity assay in addition to the othertests.
Intra-uterine infection is assessed by IgM assays in fetal bloodwhich can be accompanied by virus detection in CV or AF spec-imens, or, in case of induced abortion, in fetal tissue. Laboratoryassessment of congenital rubella infection in neonates relies onvirus detection by culture or RT-PCR in various clinical sam-ples taken early after birth, and by demonstration of IgM andlong-lasting IgG in neonatal serum. Due to the complexity ofthe current laboratory assays, cooperation between the physi-cian and the laboratory is of utmost importance to achieve areliable diagnosis.
An algorithm describing the laboratory diagnosis process forRV is shown in Fig. 1.
3. Cytomegalovirus (CMV)
3.1. Introduction
3.1.1. The pathogenCMV is a common pathogen which can cause primary and
secondary infections. CMV is a member of the herpesvirus fam-ily possessing a 235 kb double stranded linear DNA genome, acapsid and a loose envelope. Membranal glycoproteins embed-ded in the envelope carry neutralization epitopes. CMV canieferihait[t
lref
iTtbe
crvpsii
3.1.2. Laboratory assessment of CMV infection in pregnantwomen
CMV was recognized as the cause of fetal stillbirth followinga cytomegalic inclusion disease (CID) in the mid 1950s when itwas first grown in tissue cultures in three laboratories [80–82].Since then demonstration of CMV infection of the mother orfetus by laboratory testing has become an essential part of theassessment of pregnancies at risk [76,83]. Assessment of con-genital CMV infection begins with maternal serology whichshould establish recent primary or secondary infection (Fig. 2).
Not all maternal infections result in fetal transmission anddamage. Only 35–50% of maternal primary infections and0.2–2% of secondary infections lead to fetal infection, out ofwhich only 5–15% in primary infection and about 1% in sec-ondary infections are clinically affected [84–87]. Therefore,following maternal diagnosis, and if early pregnancy termina-tion was not chosen, subsequent prenatal diagnosis should takeplace using methods for virus detection in AF samples.
Demonstration of maternal infection relies on ELISA IgMand IgG assays and on CMV IgG avidity assay (Fig. 2). UnlikeHI and NT for rubella, for CMV there are currently no serolog-ical “gold standard” assays which can be used for confirmationand reassurance. Recently an attempt to find association betweenviral load in maternal blood and the risk for fetal infection didnot yield positive results [88].
3
indCvmtssoidgsoam
clHocTaaart
nfect all age groups usually causing mild and self-limited dis-ase. Its sero-prevalence in women of child-bearing age variesrom 50% to over 80%, with inverse correlation to socio-conomic levels. Primary CMV infection during pregnancy car-ies a high risk of intrauterine transmission which may resultn severe fetal damage, including growth retardation, jaundice,epatosplenomegaly and CNS abnormalities. Those who aresymptomatic at birth may develop hearing defects or learn-ng disabilities later in life. It is now recognized that intrauterineransmission may occur in the presence of maternal immunity78]. Pre-conceptional primary infection carries a high risk iden-ical to the risk of infection during early gestational weeks [79].
CMV, like other members of the herpesvirus family, estab-ishes a latent infection with occasional reactivations as well asecurrent infections in spite of the presence of immunity. How-ver, reactivation or recurrent infections carry a much lower riskor fetal infection and damage is much lower in such events.
The infectious cycle in vitro takes 24–48 h while in vivo thencubation period for postnatal infection can last for 4–8 weeks.he incubation period for congenital infection is not known and
he gestational age of congenital infection is currently definedy the maternal seroconversion, if known, which does not nec-ssarily reflect the actual timing of the fetal infection.
The host defense against CMV infection in immune-ompetent individuals combines cellular and humoral immuneesponses which together prevent a severe CMV disease in theast majority of infections. Antibodies of the IgM class areroduced immediately after primary infection and may last foreveral months. IgM can be produced in secondary infectionsn some cases. Antibodies of the IgG class are also producedmmediately after infection and last for life.
.1.3. Prenatal assessment of congenital CMV infectionMaternal infection during pregnancy prompts testing for fetal
nfection as outlined in Fig. 2. Prenatal CMV diagnosis can-ot rely on detection of fetal IgM since frequently the fetusoes not develop IgM [76,89–94]. On the other hand, becauseMV is excreted in the urine of the infected fetus, detection ofirus in the AF has proven to be a highly sensitive and reliableethod. Numerous studies have focused on the most appropriate
iming for performing amniocentesis which will yield the bestensitivity for detection of fetal infection [76,83,97–99]. Thesetudies clearly indicated that amniotic fluid should be collectedn 21–23 gestational week and at least 6–9 weeks past maternalnfection. If these requirements are met then the sensitivity ofetection of intrauterine infection can reach over 95% while theeneral sensitivity is only 70–80%. One study measured the sen-itivity for AF obtained at gestational weeks 14–20 and reportednly 45% [100]. Most of the studies state that the timing of themniocentesis is more critical for sensitivity than the laboratoryethods used to detect the virus in the AF.Initially, virus isolation in tissue culture and its more sophisti-
ated variation “Shell-Vial” technique (Table 1) were the leadingaboratory methods for detection of CMV in amniotic fluid.owever, during the late 1980s highly sensitive molecular meth-ds were developed for detection of specific viral DNA inlinical specimens such as dot-blot hybridization [101–103].hese methods were much faster, less laborious and repeat-ble compared to virus culturing. Performance of the biologicalnd molecular techniques in parallel assured that the preciousmniotic fluid sample will not be wasted and that false negativeesults will not be obtained by a technical problem in any ofhese “home-made” assays.

E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 361
Since the early 1990s the polymerase chain reaction (PCR)has become the preferred method for CMV detection in amnioticfluid [95,96,104–106]. Problems with molecular contaminationleading to false positive results and the need to address prog-nostic issues, led finally to the development of quantitative PCRassays with the highly advanced real-time PCR (rt-PCR) as themost updated method (Table 1). Current studies deal with thecorrelation between the “viral load” in the amniotic fluid andthe pregnancy outcome, in an attempt to establish the prognos-tic parameters of this powerful technique.
The laboratory methods used for assessment of maternal andfetal CMV infection are described in detail below.
3.2. Laboratory assays for assessment of CMV infection
3.2.1. CMV IgM assaysIgM detection is a hallmark of primary infection although it
may also be associated with secondary infections [90,107–109].Major efforts were put into developing sensitive and reliableassays for IgM detection using ELISA. The technical and bio-logical obstacles and their solutions which were described forrubella IgM assays apply for CMV as well, including long-termpersistence of IgM antibodies [110–114].
The source of the viral antigen affects sensitivity and speci-ficity [113,115–122], but in the absence of a gold standard assay,comparisons between various commercially available assayswbaoalacmdba[
3
utntsbrlIscbatt
since a “significant increase” is rarely defined for commercialELISA assays, it is up to the laboratory to define it.
3.2.3. CMV IgG avidity assaysThe IgG avidity assay was developed to circumvent diagnos-
tic problems as described for rubella [128–130]. It is performedwhen both IgM and IgG are positive on initial testing, but cannotbe performed on sera with very low IgG titers. Various commer-cial assays are calibrated in different ways for determination ofthe diagnostic threshold: some assays exclude recent infectionif the AI reaches a certain threshold level, yet others approverecent infection if the AI is lower than a certain threshold level.However, none of these assays can exactly determine when theinfection occurred or give any interpretation of results fallingoutside of its exclusion or inclusion criteria. Numerous studiespublished in recent years aimed at evaluating IgG-avidity assays(by commercial kits or “in-house” methods) for their ability toidentify or exclude recent primary CMV infection, and to predictcongenital infection. Concordance between different commer-cial assays for determination of low avidity was high (98–100%),but not for determination of high avidity (70%). Because the useof this assay is relatively new, some of these studies are describedin detail below.
One set of studies evaluated the ability of the assay to assessthe risk for fetal infection. [127,131–133]. In a cohort of womenconsidered at risk for transmitting CMV to their fetuses basedosttaa(cia
IfotdoaafiiatakAAwatd
ere based on multi-variant analyses of “consensus” resultsetween several assays. These studies demonstrated high vari-bility in specificity and sensitivity among assays and a high ratef discordance [123–126]. Thus, testing for IgM, particularly insymptomatic pregnant women, may frequently create a prob-em rather that solving it: borderline results or conflicting resultsmong two or more commercial kits are interpreted as incon-lusive and require further testing as described below. Otherethods, such as immunoblotting and IF assays (Table 1) were
eveloped to confirm positive IgM results and to distinguishetween specific and non-specific reactions [88]. However, thesessays did not gain vast usage because of lowered sensitivity127] and the lack of automation.
.2.2. CMV IgG assaysIgG assays which are currently based on ELISA, are generally
sed for determination of immune status but, unlike rubella,here is neither definition of a CMV-IgG international unit (IU)or of the protective antibody level. IgG assays may also helpo establish diagnosis of current CMV infection in suspectedecondary infections, or when the IgM result is inconclusive,y demonstration of IgG seroconversion or a significant IgGise between paired sera taken 2–3 weeks apart. This ability isimited in cases when women initially present with a high titer ofgG or when it is impossible or too late to obtain a second serumample. Commercial ELISA IgG assays are relatively simple,orrelate well with each other and most of them are quantitativeut are not yet internationally standardized. Commercial kits userbitrary units (AU) which differ from one assay to another andhus, to demonstrate an increase in antibody level, it is criticalo run the two samples in parallel in the same test. Additionally,
n demonstration of IgM or seroconversion, low avidity wastrongly associated with fetal infection (100% sensitivity) ifhe serum sample tested was collected at 6–18 weeks gesta-ion. Moderate or high AI levels were associated with 33%nd 11%, respectively, of cases with CMV genome-positivemniotic fluid, but with no fetal infection. Lowered sensitivity60–63%) for detection of primary infection was found for seraollected at 21–23 weeks gestation, since some of the mothers,nfected early in pregnancy, already developed moderate or highvidity.
Another set of studies [134–136] examined the ability of thegG-avidity assay to exclude those with past infection and there-ore with low risk of fetal transmission. Women with positiver equivocal IgM but without documented seroconversion wereested. High avidity was interpreted as remote infection whichid not occur within the last 3 months. The results of this seriesf studies also showed that congenital infection was stronglyssociated with low avidity, while moderate or high avidity weressociated with uninfected fetus. Additional studies further con-rmed the strong association between low avidity and primary
nfection, and thus risk for fetal infection, and between highvidity and past infection [130,136–140]. One study showedhe lack of full concordance between different commercial IgGvidity assays [141]. It showed that the ability of a commercialit to exclude recent infection by high avidity was restricted toI of >80% and to determine recent infection to AI of <20%.ny result in between those limits was inconclusive since seraith AI of 50–80% included 48 out of 257 (18%) women withhistory of past infection and 3 sera from 2 patients with a his-
ory of recent infection. Testing the latter three samples with aifferent kit yielded low avidity (30%).

362 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
In conclusion, the IgG-avidity assay is a powerful tool butit should be used and interpreted properly. The associationbetween low AI and recent primary infection with a high riskfor congenital infection is stronger than the association betweenmoderate or high AI and past infection with low risk. Inter-pretable results can be achieved mainly for sera obtained withinthe first 3–4 month of pregnancy. However both the inclusionand the exclusion approaches can be used and the IgG avidityassay is now implemented in a testing algorithm following theIgG test [142] as shown in Fig. 2.
3.2.4. CMV neutralization assaysNeutralizing antibodies appear only 13–15 weeks following
primary infection, thus the presence of high-titer of neutralizingantibodies during acute infection indicates a secondary ratherthan a primary infection. The neutralization assays have notreached a wide use as they are labor intensive, very slow andcannot be commercialized. Therefore, they are rarely performedby specialized reference laboratories. Attempts to correlate neu-tralization with specific response to the viral glycoprotein gBshowed promising results and were also commercialized in anELISA format [130,143–146]. However the utility of this assayrequires further studies.
3.2.5. Virus isolation in tissue cultureVirus is cultured from AF samples to assess fetal infection
(s4vl
amfiescnefirCdtbo
vdTcbpws
except for rare cases in which the monoclonal antibody does notrecognize the viral antigen [147–149].
Today, virus isolation from AF remains a key method fordemonstration of fetal infection and has been described exten-sively in many studies either exclusively or in conjunction withmolecular methods, particularly PCR [97,99,132,150–155]. Themain subject under investigation in recent years has been thecomparative sensitivity and specificity of the PCR and the virusisolation methods.
3.2.6. Detection of CMV by PCRDetection of viral DNA in clinical samples involves DNA
extraction and analysis. PCR has become the preferred methodfor rapid viral diagnosis in recent years. Its main disadvan-tage is the possible contamination leading to false positiveresults.
The PCR assay includes several components which can varyfrom test to test. Viral DNA can be extracted using in-housemethods or various commercial kits. The primers used can bederived from different viral genomic sites and the reaction con-ditions can be altered. For CMV, most assays utilize the early (E)or immediate-early (IE) genes which are highly conserved com-pared to the structural matrix or glycoprotein genes presentinghigher variability among wild-type isolates. To increase sensitiv-ity [95,156] some assays include a second round of amplificationusing nested or hemi-nested primers. The nested PCR is how-er
ifitCivct
3
DtadifflanarTahca
Fig. 2). Since CMV is a very labile virus, samples for culturinghould be kept at 4–8 ◦C and transported to the laboratory within8 h to be tested immediately. Freezing AF at −20 ◦C destroysirus infectivity and freezing at or below −70 ◦C requires stabi-ization by 0.4 M sucrose phosphate [147].
Culturing CMV from AF which was stored and transportedppropriately, has always been considered the gold standardethod for detection of fetal infection having 100% speci-city. CMV can be isolated in human diploid fibroblast cellsither primary, such as human embryonic cells and human fore-kin cells, or continuous cultures such as MRC-5 and WI-38ells [147]. The diploid cells should be used at low passageumber to avoid loss of sensitivity. Tissue culture monolay-rs inoculated with the clinical samples should be maintainedor up to 6 weeks since CMV is a slow growing virus. Dur-ng this period blind passages should be performed using cellsather than culture supernatant since the virus is cell-bound.MV produces a typical CPE which can appear within 2–3ays and up to 6 weeks, depending on the virus concentra-ion in the clinical sample. The CPE is easily recognizable,ut IF assay using specific antibodies can confirm the presencef CMV.
An alternative, much shortened procedure called the “shell-ial assay” was developed in which inoculated cultures are spunown at low velocity for 40–60 min before incubation at 37 ◦C.his procedure enhances and speeds-up viral infection of theultured cells. Infected cells are then detected within 16–72 hy IF using monoclonal antibodies directed against early viralroteins synthesized shortly after infection. This method gainedide acceptance and is now used by most laboratories. Its sen-
itivity and specificity are highly comparable to virus isolation
ver more prone to molecular contamination and false-positiveesults.
The comparative specificity and sensitivity of PCR and virussolation is dependent upon technical parameters which varyrom one laboratory to another with relation to the overall med-cal set-up in which they are placed and the technical skills ofhe laboratory personnel. However, it is generally agreed that forMV, PCR is more sensitive than tissue culture isolation. PCR
s also a repeatable assay which is of great advantage in contro-ersial cases. Original samples kept frozen at or below −70 ◦Can be re-processed and extracted DNA can be re-tested or sento another laboratory for confirmation.
.2.7. Quantitative PCR-based assaysMany previous studies have shown that detection of CMV
NA in AF by itself does not predict the outcome of fetal infec-ion. Clinical measures such as ultrasonographic examinationsre a key component in fetal assessment, but might also fail toetect affected fetuses. In an attempt to address prognostic issuest was suggested that symptomatic fetuses can be distinguishedrom asymptomatic ones based on the viral load in the amnioticuid. Quantitative PCR methods were developed as “in-house”ssays or are available as commercial kits using various tech-ologies. The most up-to date technology is the real-time PCRssay in which the amplified sequences are detected by a fluo-escent probe in a real-time and quantitative manner [157–159].hese assays, performed by dedicated instruments, carry thedvantages of high sensitivity and specificity conferred by theybridization probe, and the lack of contamination by amplifi-ation products, since the reaction tubes are never opened aftermplification.

E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 363
Few recent publications have addressed the prognostic valueof determination of viral load in AF with controversial results.Three studies [160–162] found no statistically significant differ-ence in viral load between symptomatic and asymptomatic fetalinfections. Yet other two studies reported predictive values forviral load [163,164]. In one of these two studies [164] the pres-ence of 103 or more CMV genome-equivalents per millilitres(GE/ml) predicted mother to child transmission with 100% prob-ability, and 105 GE/ml or more predicted symptomatic infection.In the second report [163] CMV DNA load with median of2.8 × 105 GE/ml was associated with major ultrasound abnor-malities while median values of 8 × 103 GE/ml was associatedwith normal ultrasound and asymptomatic newborn. The slightdiscordance between the two studies calls for further evaluationson a larger scale and underscores the need for standardization,since the quantitative assays may vary by orders of magni-tude using different methods or primers derived from differentgenomic regions [165,166].
3.3. Summary
Laboratory testing for determination of intrauterine CMVinfection involves several steps. Maternal primary or recurrentinfection is assessed by serology using IgM, IgG and IgG-avidityassays. In controversial cases a second blood sample should besought to demonstrate antibody kinetics typical of current infec-tmwgtQd
wipct
f
4
4
4
itpaAab
c
and the fetus. Complications and sequelae include pneumo-nia, increased rate of prematurity abortions, congenital varicellasyndrome (CVS), neonatal varicella and herpes zoster duringthe first year of life [171–177]. Rarely VZV may cause a lifethreatening CNS infection. The risk of adverse effects for themother is greatest in the third trimester of pregnancy, while forthe fetus the risk is greatest in the first and second trimesters.The risk of CVS for all pregnancies continuing for 20 weeks isabout 1%, but is lower (0.4%) between weeks 0 and 12 and ishigher (2%) between weeks 13 and 20. Maternal infection after20 weeks and up to 36 weeks is not associated with adversefetal effect, but may present as shingles in the first few yearsof infant’s life indicating reactivation of the virus after a pri-mary infection. If maternal infection occurs 1–4 weeks beforedelivery, up to 50% of the newborns are infected and 23%of them develop clinical varicella. Severe varicella occurs ifthe infant is born within seven days of the onset of maternaldisease.
4.1.2. Assessment of VZV infection in pregnancyLaboratory diagnosis of VZV in pregnancy is required in two
situations: (a) the pregnant woman has developed clinical symp-toms compatible with chickenpox or herpes zoster (Shingles) (b)The pregnant woman was exposed to a chickenpox or a zostercase (Fig. 3).
If the pregnant woman has developed clinical symptomstsm
wmroal(
cbspo
uopntfs8itwih
ion and not of remote infection or a non-specific reaction. Ifaternal primary infection was established and the pregnancyas not terminated, prenatal diagnosis follows at 21–23 weeksestation and 6–9 weeks after seroconversion (if known). Detec-ion of CMV in AF is done by virus culturing and/or PCR.uantitative PCR is still not established for assessment of fetalamage and prognosis.
During the diagnostic process, which may last for severaleeks, collaboration between the laboratory and the physician
s of utmost importance. Appropriate timing of sampling, sam-le treatment, usage of validated assays under quality assessmentonditions, and correct interpretation of the results are all essen-ial for obtaining a reliable diagnosis.
The algorithm describing the laboratory diagnostic processor CMV is shown in Fig. 2.
. Varicella-zoster virus (VZV)
.1. Introduction
.1.1. The pathogenVaricella-zoster virus (VZV) is a common pathogen belong-
ng to the herpesvirus family which can establish latent infec-ions and subsequent reactivations. Primary infection, chicken-ox, is a common childhood disease. Reactivation is manifesteds zoster and occurs in the presence of anti VZV antibodies.pproximately 90% of the adult population is positive for VZV
ntibodies and studies on pregnant and parturient women foundetween 80% and 91% seropositivity [167–170].
Primary infection with VZV (chickenpox) during pregnancyarries a risk for clinical complications for both the mother
he infection should be confirmed by laboratory testing usingerology or virus detection by culturing, antigen detection orolecular methods.Assessment of VZV IgM which remains in the blood for 4–5
eeks is diagnostic. However, false positive results are com-on in the presence of high VZV IgG antibodies and virus
eactivations may also induce IgM. Therefore, determinationf IgG seroconversion or a 4-fold rise in VZV IgG titer shouldccompany the IgM test. Virus isolation or PCR from dermalesions can be attempted and, if positive, confirm the diagnosisFig. 3).
If the pregnant woman has reported exposure to a case ofhickenpox or zoster, prompt assessment of her immune statusy testing for IgG within 96 h from exposure should be doneince varicella-zoster immunoglobulin (VZIG) given as a pro-hylactic measure at the time of exposure is known to preventr reduce the severity of chickenpox [178,179].
Serological screening for IgG of women with negative orncertain histories of illness, who are planning a pregnancy,r of women who give history of recent contact with chicken-ox, has been suggested as a strategy for preventing CVS andeonatal VZV [180,181]. In a study conducted in our labora-ory 52 pregnant women were assessed for immunity to VZVollowing exposure to chickenpox and 25% of them were foundusceptible. The attack rate among the susceptible women was5% [181]. In another study, Linder et al. [182] reported thatn 327 pregnant women assessed for VZV immunity, 95.8% ofhe women who recalled chickenpox in themselves and 100% ofomen who recalled chickenpox in their children were seropos-
tive, and only 6.8% of the women with a lack or uncertainistory of exposure were seronegative. The screening strategy

364 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
might gain momentum due to the availability of VZV vaccine,as seronegative women can be vaccinated.
4.1.3. Prenatal and perinatal laboratory assessment ofcongenital VZV infection
If VZV infection of the mother during the first or the sec-ond trimester has been confirmed, the need to diagnose the fetusarises. Unfortunately, laboratory methods for fetal assessmentare of limited value. Assessment of fetal infection by determi-nation of VZV IgM in fetal blood is not widely performed. IgMmay be manifested in the fetus only after 24 weeks of gesta-tion, thus in case of intrauterine infection during early gestation,functional immunity may not be present in the fetus [183].Alternatively, determination of fetal infection can be done bydemonstration of VZV DNA in AF using PCR, but its presenceis not synonymous with development of CVS [183]. Only onein 12 infected fetuses will develop pathological signs, so inter-pretation of a positive VZV DNA result is problematic if thefetus appears normal upon ultrasonograpic examination [180].Diagnosis of clinical varicella in neonates is based on serology(IgM) and virus isolation or detection in vesicle fluid or in CSF(in case of CNS infection).
4.2. Laboratory assays for assessment of VZV infection andimmunity
4
abotEdIgaaaisgr
4
ocCw
4
iDoi
4.2.4. Virus isolation in tissue cultureVZV isolation in tissue culture is not a very sensitive assay
and the isolation of the virus from skin lesions is possible onlyfrom early vesicles. VZV is a very labile virus which growsslowly in selected tissue cultures. Specimens for cell culture(vesicle fluid, skin-lesion swabs and AF) should be transportedto the laboratory as soon as possible after collection [196–198].Swabs should be put in a vial containing virus transport mediumand AF should be placed in a sterile container. Both should bekept at 4–8 ◦C during transportation. Inappropriate conditionsduring transportation may easily reduce virus viability [199].
Upon receipt, the specimen is inoculated into semi-continuous diploid cells such as human diploid fibroblasts(MRC-5) and continuous cell lines derived from tumors ofhuman or animal tissue such as A549. CPE may appear within 2weeks. AF should be sampled after 18 weeks of pregnancy andafter complete healing of skin lesions of the mother. Confirma-tion of virus isolation can be done by immunoflurescent stainingusing monoclonal anti-VZV antibody. Shell vial cultures asdescribed for CMV improve the sensitivity of VZV detectionand allow rapid identification of positive samples within 1–3days [196,200].
4.2.5. Direct detection of VZV antigenImmunofluorescence or immunoperoxidase assays use mon-
oclonal or polyclonal antibodies directed to VZV antigens todfrahoan
4
sMitptdodPampm[ln
ac
.2.1. VZV IgG assaysSeveral methods were applied for determination of VZV
ntibodies. In the past, specific IgG antibodies were measuredy the complement fixation (CF) assay, which can be usednly for diagnosis of recent infection or by the latex agglu-ination assay [184–188]. Today, highly sensitive and specificLISA and immunofluorescence (IF) methods are used foretermitation of VZV IgG antibodies. Several versions of theF assay exist (Table 1): fluorescent antibody to membrane anti-en (FAMA) and indirect fluorescent antibody to membranentigen (IFAMA) detect binding of antibodies to membranentigens in fixed VZV infected cells, and are highly specificnd sensitive [169,181,186,189]. ELISA is comparable to IFn sensitivity, specificity and cost and can be used for generalcreening purposes. Commercial ELISA kits for VZV IgG areenerally highly specific but demonstrate some false positiveesults compared to FAMA or IFAMA.
.2.2. VZV IgM assaysBoth the IF and ELISA methods are used for determination
f VZV IgM in the same manner as for IgG, except that theonjugate is an anti-human IgM rather than anti-human IgG.ommercial ELISA IgM kits may give false positive results asas described for RV and CMV.
.2.3. Virus detection in clinical specimensVirological methods for the diagnosis of VZV infection
nclude detection of infectious VZV, viral antigens and viralNA in clinical specimens. These include vesicular fluid, swabsr smears, AF in pregnant women or cerebrospinal fluid (CSF)n encephalitis cases [183,190–195].
etect VZV infection in epithelial cells isolated from AF, orrom suspected lesions (Table 1). This simple method allowsapid diagnosis (approximately 2 h) of VZV infection and isvailable to most laboratories [201,202]. It is highly specific andas sensitivity ranging from 73.6% to 86%. The preferred mon-clonal antibodies are those directed against the cell-membranessociated viral antigens [203]. Stained smears, in which multi-ucleated giant cells are seen are less sensitive, 60–75% [204].
.2.6. Molecular methods for detection of viral DNAPCR and hybridization methods to detect VZV DNA
equences are very sensitive and specific [183,191,205–208].odifications of the basic PCR technique have been used to
ncrease the sensitivity by using nested PCR assays. However,his assay is highly susceptible to contamination, leading to falseositive results. Rapid laboratory diagnosis is important whenhe CNS is involved, especially in cases with clinically confusedermal manifestations, and is crucial in neonates to prevent lethalutcome of disease. In recent years real-time PCR assays wereeveloped for VZV as for CMV and other viruses. Real-timeCR assays appear to have equal sensitivity as VZV nested PCRssays but are faster, easier and have markedly reduced risk forolecular contamination. Because of its high sensitivity com-
ared to other methods, PCR has become the most appropriateethod for detection of VZV DNA in AF and other specimens
183,206,209,210]. However, standardization is a major prob-em and should be done in order to avoid false positive or falseegative results.
In a study conducted in our laboratory AF samples werenalyzed either by PCR or real-time PCR in parallel to tissueulture isolation. The DNA amplification target was located in

E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 365
the viral UL gene. VZV DNA was detected in the amniotic fluidof two (7.4%) out of 27 women who developed chickenpox inthe second trimester of pregnancy. One gave birth to a normalchild while no follow-up was available for the second woman.All amniotic fluid cell cultures were negative. No case of CVSoccurred following negative PCR results (unpublished data).
4.3. Summary
VZV infection during pregnancy poses a risk to the motherand fetus. Laboratory assessment of maternal infection is basedon serology (both IgG and IgM), and on virus detection inskin lesions. Exposure of a pregnant woman to a varicella caseprompts immediate assessment of her immune status to deter-mine the need for VZIG administration. The availability of aVZV vaccine may encourage the screening of women for VZVimmunity before conception.
There are no fully reliable methods to assess fetal infectionand damage. Fetal IgM and virus detection in AF are used, butfalse negative results are common and positive results do notnecessarily correlate with fetal damage.
An algorithm describing the laboratory diagnostic assays forVZV infection in pregnancy is shown in Fig. 3.
5. Herpes simplex virus (HSV)
5
5
lac(
aHtaashpAdhaHob
nmcaie
infections are associated with prematurity and fetal growthretardation.
Herpes simplex is a devastating infection in the neonate,with primary asymptomatic and symptomatic maternal infec-tion near delivery carrying a greater risk to the newborn thanrecurrent infections [218,219]. Fourty percent of women whoacquired genital HSV during pregnancy but did not completetheir seroconversion prior to the time of delivery will infecttheir newborns. Transmission of genital herpes during vaginaldelivery is high in neonates exposed to asymptomatic shedding[220–223], since serial HSV genital cultures during the last fewweeks of gestation are no longer recommended as a methodto prevent neonatal herpes. Instead, women are examined at thetime of labour and caesarean section is carried out only if there isan identifiable lesion. The use of fetal scalp electrodes may alsoincrease the risk for neonatal infection [224,225]. HSV infec-tions should be suspected as the cause of any vesicle appearingin the neonate.
5.1.2. Laboratory assessment of HSV infection inpregnancy and in neonates
Clinical symptoms compatible with genital herpes duringpregnancy require laboratory assessment (Fig. 4). Diagnosis ofHSV infection relies on both serological and virological meth-ods, but the diagnostic process may be complicated due to thenature of the viral infection. Recurrent infections and reacti-vd
ig2g
i[ntatrmn
ifaieoapHcmcc
.1. Introduction
.1.1. The pathogenHerpes simplex virus (HSV) establishes latent infection fol-
owing primary infection which may lead to reactivation. It isneurotropic member of the herpesvirus family and the genus
onsists of two types: HSV type 1 (HSV-1) and HSV type 2HSV-2).
The consequences of infection with HSV can vary fromsymptomatic to the life-threatening diseases manifested asSV-encephalitis and neonatal herpes [211]. Recurrent infec-
ions with one type after primary infection with the other typere common. HSV-1 is usually transmitted through the oral routend causes disease in the upper part of the body, while HSV-2 is aexually transmitted virus which tends to cause primarily genitalerpes. However, both HSV-1 and HSV-2 can cause genital her-es which can be a severe disease in primary episodes [211–214].n increase in the prevalence of genital herpes infection has beenocumented worldwide: HSV-2 was the main cause of genitalerpes during the 1980s but since the 1990s HSV-1 constitutesn increasing proportion of the cases. This shift from HSV-2 toSV-1 may have implications for prognosis [215]. Assessmentf risk and diagnosis of HSV infections may involve testing foroth HSV-1 and HSV-2.
HSV infection has serious consequences for the fetus andeonate. Before 20 weeks of gestation, transplacental trans-ission can cause spontaneous abortion in up to 25% of the
ases [216,217]. Later in pregnancy HSV infections are notssociated with increase in spontaneous abortions but intrauter-ne infections may occur. Symptomatic and asymptomatic firstpisodes of genital herpes but not asymptomatic recurrent
ations pose a special challenge to serology, and therefore viraletection in genital lesions is more reliable as a diagnostic mean.
The standard laboratory method to confirm current HSVnfection is virus isolation and typing in cell culture since HSVrows readily in tissue culture. The virus may be isolated within–4 days from swabs taken from herpetic skin and laryngeal orenital lesions (Fig. 4).
PCR techniques improved the correct diagnosis of HSVnfections especially in cases without clear overt manifestations226–229] and can detect viral DNA from lesions that are cultureegative. For genital swabs it might be too sensitive to reflectrue reactivation, and it is not clear whether a positive PCR in
patient with a negative HSV culture reflects a true risk ofransmission of the virus. Therefore physicians should interpretesults with caution and according to additional criteria. Supple-ental serological testing can be used when genital lesions are
ot apparent.In primary infections antibodies appear within 4–7 days after
nfection and reach a peak at 2–4 weeks. Antibodies persistor life with minor fluctuations. Specific IgM antibodies appearfter primary infection but may be detectable during reccurentnfections as well [226]. HSV-1 and HSV-2 share cross reactivepitopes of the surface glycoproteins which are the major targetsf serum antibodies. Therefore it is difficult to identify a newlycquired infection with one HSV type on the background ofre-existing immunity to the other type (usually infection withSV-1 precedes infection with HSV-2). Type specific serologi-
al assays were developed [230] which may be valuable for theanagement of a pregnant woman and her partner: these assays
an identify previous infections, seroconversions and discordantouples. The results may provide information to the pregnant

366 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
woman about her risk of acquiring and transmitting HSV to herinfant (Fig. 4). The cost-benefit value of general screening fortype-specific antibodies in pregnant women and their partnerswere recently assessed [231,232].
Rapid and sensitive diagnosis of neonatal HSV diseaseis of utmost importance for initiation of acyclovir treatmentand improvement in the outcome of neonatal herpes has beenachieved due to the application of PCR as a diagnostic tool [233].Neonatal HSV infections are confirmed through positive viralculture or PCR from skin, eye lesion, nasopharynx, rectum orCSF and detection of IgM in a neonate is highly significant[234]. Neonatal HSV infection can occur in newborns withoutthe presence of any vesicular skin disease [229,235,236].
5.2. Laboratory assays for assessment of HSV infection andimmune status
5.2.1. HSV IgG assaysSeveral techniques are used for detection of HSV specific
IgG, among them CF, NT, IF and ELISA. The principles ofthese assays were described above for VZV and are shown inTable 1. There are assays which do not distinguish between IgGdirected to HSV-1 or HSV-2. These assays are useful in primaryinfection in the absence of prior immunity, and they use crudepreparations of cells infected with HSV-1 and/or HSV-2. Theymay detect infection with HSV-2 on the background of HSV-1o
5
Ntdniubw
fstIMir2ahawcatio
for HSV is the most accurate method for type-specific serology[241]. This method is the serology gold standard and is per-formed only by few laboratories. WB is expensive to performand requires 2–5 days for completion. New approaches to anti-gen preparation include the application of recombinant gG-1 andgG-2 from a mammalian expression systems to nitrocellulose,or purification of glycoprotein gG2 by lectin chromatography[242].
5.2.3. HSV IgM assaysThese assays are based primarily on ELISA and IF methods
as described for VZV. Due to the persistent nature of the viralinfection and the frequency of recurrent infections, the presenceof IgM is of high value primarily in neonates and infants. In mostcases testing for IgM must be accompanied by testing for IgG,since a negative IgM result does not rule out recent infection.
5.2.4. Virus isolation in tissue cultureHSV is a labile virus, and successful virus culturing from
clinical specimens depends on appropriate sample collection andmaintenance of the cold chain. Swabs should be placed into viraltransport medium and other samples should be placed in a sterilecontainer. Rapid transportation of specimens to the laboratoryand avoiding freeze-thawing cycles results in more than 90%sensitivity of culturing from skin lesions. However, poor samplequality due to inappropriate sampling or compromised transportcaaV1[wp
itmtcit[
5
ocvssa
5
na
[237]. More accurate type-specific assays were developed inrder to detect recurrent infections with either type.
.2.2. HSV type-specific IgG assaysType specific serological assays vary in their abilities [230].
T antibody level can be measured specifically for each type byhe plaque reduction assay using serial dilutions against a fixedose of HSV-1 or HSV-2, with 50% reduction in the plaqueumber as an endpoint. However these assays are accurate onlyn patients infected with only one virus type. NT assays weresed for determination of HSV-2 infection based on the ratioetween the antibody titers to the two viruses. Positive casesere those with HSV-2 to HSV-1 ratio of ≥1 [237,238].IF can be used for detection of antibodies to HSV cell sur-
ace and internal proteins. IF correlates well with NT titers butubtyping is difficult. ELISA assays utilize a variety of condi-ions and antigens. These tests are more sensitive than NT andF and can detect antibodies within the first week of infection.
anufacturers of those tests use mathematical calculations tonfer the presence of HSV-1 or HSV-2 antibodies based on theirelative ratios. New type-specific tests, which distinguish HSV-from HSV-1 are based on glycoproteins gG1 and gG2 [239]
nd can provide useful information on the etiology of the genitalerpes in the symptomatic patient when viral culture and PCRre not helpful. These tests allow the identification of patientsith unrecognized genital herpes [240,241]. There are few good
ommercial ELISA kits for type specific serology which werepproved by the FDA. Nevertheless, HSV type specific antibodyests are interpreted in the context of the clinical history, clin-cal presentation and other laboratory test results for herpes orther possible etiological agents. Finally, Western blotting (WB)
onditions may reduce sensitivity by 20% for primary episodesnd down to 50% for recurrent episodes even if herpetic lesionsre present. When an appropriate sensitive cell line (such asero cells) is used, appearance of a characteristic CPE within8–96 h after inoculation points to the presence of active HSV237]. Direct immuonofluorescence detection of HSV in culturesith CPE is regarded as the standard for confirmation of HSVresence.
The so-called “Shell vial” method, described earlier for CMVsolation (chapter 2.5 and Table 1) shortens the time requiredo identify HSV in specimens to 24–48 h. An innovated com-
ercially available diagnostic test for rapid detection of HSV inissue culture is the ELVIS HSV test kit. It utilizes a recombinantell system in which a reporter enzyme is quickly accumulatednside the infected cells and is detected by intense blue color. Theest is sensitive and specific and detects both HSV-1 and HSV-2243]. The kit is expensive and is used only by few laboratories.
.2.5. Direct antigen detection of HSVOther rapid assays such as the direct fluorescent assay (DFA)
r enzyme immunoassays (EIA) performed directly on smearedells recovered from lesions are rapid but less sensitive thanirus culturing. Accordingly, for detection of virus in genitalwabs they may have similar sensitivity to viral culture forymptomatic shedding but have reduced sensitivity for detectingsymptomatic viral shedding.
.2.6. Detection of HSV DNA by PCRMethods for detection of HSV DNA, particularly PCR tech-
iques (PCR, nested PCR and real-time PCR) were describedbove for other viruses. They are highly sensitive especially for

E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 367
samples with very low concentration of virus, as was demon-strated by numerous research studies. The performance of PCRanalysis is dependent upon the quality of the specimen. Thereported sensitivity for PCR is 75–100% for the diagnosis ofCNS HSV infection [228,244,245]. The reason for the broadrange in sensitivity is the differences in methodologies andvariability in performance of PCR between laboratories. Stan-dardization using reference samples to assure identical resultsis not yet in place [227].
5.3. Summary
HSV-2 is the main type involved in congenital and neonatalinfection, although genital HSV-1 infections have become morecommon in recent years. Primary maternal symptomatic andasymptomatic infections may cause a serious risk of abortionand fetal growth retardation, while infection during delivery maycause a devastating neonatal disease.
Laboratory assessment of maternal infection and immune sta-tus as well as neonatal infection is critical for timely managementand treatment. Virus isolation from genital lesions is the primarytool for assessment of maternal infection. Serological asays areuseful but are complicated by pre-existing heterotypic antibod-ies. Type-specific IgG assays must be applied for determinationof recurrent maternal infections.
Virus isolation, antigen detection or DNA detection by PCRid
fbma
HF
6
6
6
Iwsr[aecic[
tv
[261,262] and fetal infection may lead to severe anemia, general-ized edema, congestive heart failure, myocarditis, fetal hydropsand fetal death [263–267]. Fifty percent of women at childbear-ing age are susceptible to parvovirus B19 infection as judgedby the lack of IgG antibodies to the virus [267–272]. How-ever, transplacental transmission rates have been estimated atbetween 25% and 33%, and the incidence of fetal loss is con-sidered between 1.66% and 9% [271,273]. Since intrauterineblood transfusions can increase fetal survival rate if done earlyenough, it is critical to diagnose maternal and fetal infectionaccurately and timely, and laboratory testing is an essential partof the diagnosis [274–279].
6.1.2. Laboratory assessment of parvovirus B19 infectionin pregnancy
Laboratory diagnosis of parvovirus B19 infection has beencomplicated by the nature of the virus, the viral infection pro-cess and the immune response. Parvovirus B19 is a fastidiousvirus which cannot be grown in regular continuous cell lines. Inthose cells where it grows it replicates poorly and the virus yieldis minimal, thus viral culturing is not a diagnostic option andcannot be used for NT assays or for preparation of native viralantigens for serology [261,280,281].
Assessment of parvovirus B19 infection in pregnant womenrelies primarily on serology (Fig. 5). During acute infection IgMantibodies appear 7–14 days from infection with Parvovirus B19asdvor[lcb
twnht[itDotwh[P
6i
w
n skin lesions samples are additional tools for rapid and sensitiveiagnosis of symptomatic current infection.
Prenatal diagnosis is not common and has not been assessedor sensitivity and specificity. Neonatal infection is diagnosedy virus culturing or PCR in skin lesions or other clinical speci-ens in case of a disseminated disease, and by detection of IgM
ntibodies.An algorithm describing the laboratory diagnostic assays for
SV infection in pregnant women and neonates is shown inig. 4.
. Parvovirus B19
.1. Introduction
.1.1. The pathogenHuman parvovirus B19 (B19) can infect humans at all ages.
t is a member of the family Parvoviridae, genus Erythrovirushich comprise small, non-enveloped viruses containing linear
ingle-stranded DNA genomes. Most of the humoral immuneesponse is directed to the two capsid proteins VP1 and VP2246]. The seroprevalence is 50% by age 15 and exceeds 80% byge 70 [247]. Childhood infection is mild leading to the diseaserythema infectiosum (“fifth disease”) [248–251] In adults thelinical symptoms vary from asymptomatic or mild to severellness including exanthematous disease, arthropathies, aplasticrisis and, in immunocompromised patients, to chronic anemia252–260].
Maternal infection during pregnancy may lead to fetal infec-ion since viremia is very high and lasts for 6–8 days. Theirus replicates in erythroid precursor cells and fetal tissues
nd may last for 6 month or even longer. IgG antibodies appeareveral days after IgM and persist for life. The antibodies pro-uced specifically react with both structural and non-structuraliral proteins and recognize linear and conformational epitopesf the capsid proteins VP1 and VP2 [282–288]. The antibodiesecognizing conformational epitopes last longer for both IgM285] and IgG [282,284,286], and IgG antibodies recognizinginear epitopes disappear around 6 month post infection. Thisreates technical problems for serological assays as describedelow.
Maternal infection during pregnancy is frequently asymp-omatic and by the time of fetal infection and symptoms, 2–12eeks after maternal infection, she may have high IgG ando IgM responses [260,275,289,290]. Viral DNA detection byighly sensitive molecular assays such as dot-blot hybridiza-ion and PCR can be applied to maternal serum or whole blood276,291]. However, parvoviruses are known for their ability tontegrate into the host genome and to establish persistent infec-ions [292–296]. Recent studies [297–299] showed that B19NA can be detected in serum samples by highly sensitive meth-ds up to 6 months after acute phase viremia, although quanti-ative assays showed that the amount of DNA present decreasedith time [300]. It has also been shown that 0.01–0.03% of theealthy blood donors have B19 DNA detected in their serum301–303]. Thus, detection of B19 DNA in maternal blood byCR might not be related to recent infection.
.1.3. Prenatal laboratory assessment of congenital B19nfection
In many cases congenital B19 infection is suspected onlyhen typical fetal abnormalities are observed. Since the fetus

368 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
does not always develop IgM it is necessary to detect the virusitself in fetal samples. B19 cannot be cultivated and thereforedetection of viral DNA is sought. The type of specimen andthe detection methods are still controversial: fetal blood and AFare the most common specimens obtained and the most highlysensitive molecular methods are employed. However, 10–25%of the specimens from asymptomatic fetuses may have B19 DNA[289,290]. This drives the need to develop quantitative molecularassays which can determine viral load and possibly associateit with the risk to the fetus. Those assays include quantitativePCR-ELISA, in situ hybridization and rt-PCR. The latter hasadvantages which will be discussed below [304–308].
6.2. Laboratory assays for assessment of parvovirus B19infection
6.2.1. B19 IgM and IgG assaysSeveral commercial tests have been developed on the basis of
recombinant and synthetic antigens [309–311]. These recombi-nant antigens frequently lack important conformational epitopsreducing the sensitivity and specificity of the assays. More-over, “gold standard” methods like virus NT or HI assays areabsent, and it is difficult to assess the sensitivity and specificityof the serological assays. The variation in specificity and sensi-tivity among commercial assays is high, and discordant resultsare often obtained indicating false positive and false negativer
vasEg7taarsv
toafTtulc
Ipgcbu
serum samples from blood donors with no IgM were tested.Overall, 353 sera were found positive by all methods combined.Of those 98.6%, 94.6% and 89% were positive by assays a, band c, respectively. Some sera reacted only with conformationalepitops. The results of this study underscore the need to useELISA-IgG assays which include conformational epitopes ofboth VP1 and VP2 or VP2 alone, and demonstrate the lowersensitivity of the Western blot assay.
In conclusion, when evaluating recent or past infections inpregnant women it is important to use well-established ELISAassays, and in cases of discrepancy between the test results andthe clinical and epidemiological circumstances, confirmationmust be sought using other commercial assays as well as sup-portive molecular assays discussed next.
6.2.2. Detection of viral DNA in maternal and fetalspecimens
Due to the limitations of the serological assays describedabove and since viremia is long-lasting in B19 infections, molec-ular assays for detection of B19 viral DNA were developed early.The methods most frequently used are DNA hybridization andPCR.
Molecular hybridization assays employing DNA probesderived from most of the viral genome are labeled with 32P,biotin or digoxigenin [319–322] and are capable of detectingapproximately 104–105 genome copies/ml [275,323]. This assayivbPsbni1umtosahpisab
eesatCwfw
esponses [314–317].Studies aimed at evaluating the sensitivity and specificity of
arious such assays were mostly based on comparative evalu-tion, using samples selected on the basis of clinical diagno-is. In a study conducted in Norway [315], five commercialLISA and IF IgM kits were comparatively evaluated in threeroups of patients. The calculated specificities for the kits were0.1–94.8%, but the authors refrained from determining sensi-ivity because of the absence of suitable reference methods. Innother study conducted in Sweden [316], four commercial IgMssays were evaluated in comparison to an IgM antibody captureadioimmunoassay as a reference method [318]. The calculatedensitivity varied between 90% and 97% and the specificitiesaried from 88% to 96%.
In a third study conducted in the USA [314] three ELISA sys-ems utilizing one or more conformational antigens for detectionf B19 IgM or IgG in sera of 198 pregnant women were compar-tively evaluated. Agreement with the consensus results variedrom 92.3% to 100% for IgM and from 97.9% to 99.5% for IgG.he authors note the high agreement in this study compared to
heir previous study [312] relating to the fact that the antigenstilized in the two studies were substantially different: the ear-ier study used a linear VP1 antigen while the latter one used aonformational VP2 antigen.
A study designed to evaluate the most appropriate assays forgG detection was conducted in Italy [313] which compared theerformance of three commercial assays using different anti-ens: (a) an ELISA assay using VP1 + VP2 recombinant nativeonformational antigens, (b) an ELISA assay using VP2 recom-inant native conformational epitopes, (c) a Western blot assaysing denatured linear antigens. Four hundred and fourty six
s sensitive enough to detect viral DNA in serum during peakiremia since the viral load exceeds 1010 genome copies/ml,ut low levels of viremia may be missed [275,296,298]. TheCR assays, developed later relied on a variety of primerets derived from different genomic regions and were capa-le of detecting 102–105 genome copies/ml [324,325]. Theested PCR, the PCR-ELISA and the PCR-hybridization assaysncreased sensitivity and moved the detection limit down to–10 genome copies/ml [291,292,296,297,299,326–328]. Bysing those highly sensitive methods it was revealed that inany cases serology failed to detect maternal or fetal infec-
ions, as some seronegative mothers as well as fetuses turnedut positive in the DNA detection assays. This finding was noturprising in view of the known limitations of the serologicalssays. The ability to detect maternal and fetal infection by theighly sensitive molecular methods allowed correct diagnosis ofreviousely unresolved cases, particularly cases of intrauterinenfection which did not result in fetal hydrops or were completelyubclinical [275,276,290,292,296,297,324,327,329]. However,s stated above, low levels of B19 DNA in maternal blood cane unrelated to recent infection.
The use of various techniques without standardization, thepidemiologically variable circumstances (epidemic VS non-pidemic years), and the use of different primer sets and clinicalpecimens led to a high variability in the sensitivity, specificitynd interpretation of the assays results. Moreover, new geno-ypes discovered recently were missed by common primer sets.omparison of IgM and DNA detection by PCR in fetal bloodas conducted in a study done on 57 pregnant women and their
etuses who had abnormal ultrasonography [327]. Viral DNAas found by PCR in 16 out of 58 fetuses (27%) while IgM was

E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 369
detected only in 7 (12.3%). Two fetuses had false-positive IgMresult, not supported by any other findings. Other researchers[276] compared maternal IgM to fetal serum or AF PCR resultsin 56 women at high risk for B19 infection. They found pos-itive PCR in 24 IgM-negative/IgG-positive and 4 seronegative(total 50%) out of, in addition to positive PCR in 15 (26%) ofIgM-positive women. Another group [282] reported detection ofviral DNA in fetal serum or AF by a PCR-hybridization assayin 11 out of 80 cases of fetal hydrops (14%) while maternal IgMantibodies were detected only in 3 (3.7%). Finally, a compre-hensice prospective study in 18 fetal hydrops cases conductedin Italy [275] examined maternal serum, fetal cord blood andamniotic fluid using nested PCR, dot-blot hybridization and insitu hybridization (ISH). The results showed that the ISH assayin fetal blood cells was 100% sensitive while the other methodsmissed few to many cases. The conclusion drawn from this studyis that various assays have complementary roles, and reliablediagnosis can be achieved only by a combination of serologi-cal and molecular assays done on maternal and fetal samples asoutlined in Fig. 5.
6.2.3. Quantitative assays for detection of viral DNAThe need to determine the quantity of B19 viral DNA present
in clinical samples (viral load) arose because B19 can establishlong-lasting persistent infection in immunocompetent individ-uals. It is not clear if low viral loads reflect whole genomesoSriietov
omq[ufnmdntnwavPffana
6.3. Summary
Parvovirus B19 infection during pregnancy may cause fetaldamage resulting in fetal loss. Early diagnosis of maternal infec-tion will allow fetal assessment and treatment by intrauterineblood transfusion. Unfortunately, mothers often are not awareof their infection until fetal damage is observed.
Confirmation of B19 infection requires laboratory assess-ment, which is complicated by the nature of the viral infectionand immune response. Serology, performed by using ELISAassays rely on recombinant antigens and concordance is lowamong all commercial assays available. In the absence of a “goldstandard” assay false positive and false negative results prevail.Virus culturing is impossible and virus detection is based onvarious molecular assays.
In spite of several studies there is no consensus regarding themost appropriate clinical specimen and method for detection ofviral DNA. Currently, on practical grounds, it is recommendedto use ELISA IgM and IgG assays based on recombinant con-formational epitopes of VP1 and VP2 or VP2 alone, and to useAF or fetal serum for detection of fetal infection by the mostsensitive molecular methds available (nested PCR or rt-PCR).Since B19 may establish long lasting infection in the absenceof symptoms, interpretation of viral DNA detection in mater-nal blood is difficult. Assessment of fetal infection and riskshould rely on the clinical situation and other prenatal diagnosticm
oF
7
7
7
irfifobseD
ctwehmlsOo
r viable infectious virus particles, or only pieces of viral DNA.tudies in seronegative plasma-pool recipients showed that onlyecipients of plasma containing >107 genome copies/ml becamenfected or seroconverted [305]. B19 DNA can also be detectedn solid organ tissues by PCR for years [323,330,331]. As notedarlier viral DNA can be detected in fetal tissue or blood inhe absence of any detectable congenital abnormalities, and theutcome of detectable fetal infection, including fetal hydrops,aries from spontaneous resolution to still-birth.
Real-time PCR assays developed recently are equivalent tor more sensitive than nested PCR and PCR-ELISA but areuch less prone to molecular contamination and produce a
uantitative result which can be standardized and automated304,306–308,332]. In a retrospective study, Knoll et al. [332]sed real-time PCR to investigate the viral load in paired samplesrom mothers and their abnormal fetuses, and from mothers withormal fetuses who were exposed to B19. The viral load in theaternal serum ranged from 7.2 × 102 to 2.6 × 103. The authors
id not report statistically significant correlation between mater-al or fetal viral load and fetal condition. However, they notedhat they could not exclude a correlation between peak mater-al viremia levels and fetal condition since most of the mothersere not aware of their infection until onset of fetal symptoms,
nd their serum was collected after peak viremia. Although theiral load in fetal sera was higher than in AF samples, the rt-CR assay detected all positive cases using either one of theseetal specimens. The authors recommend testing AF rather thanetal blood because AF can be drawn earlier, is simpler to obtainnd less risky to the fetus. Clearly, more prospective studies areecessary on larger groups of patients to learn more about thessociation between viral load and pregnancy outcome.
eans.An algorithm describing the most practical approach to lab-
ratory assessment of B19 infection in pregnancy is shown inig. 5.
. Human immunodeficiency virus
.1. Introduction
.1.1. The pathogenHuman immunodeficiency virus (HIV) is a retrovirus that
nfects helper T cells of the immune system causing a progressiveeduction in their numbers, and eventually acquired immunode-ciency syndrome (AIDS). HIV is a member of the Retroviridaeamily [333], genus Lentivirus (or “slow” viruses). The coursef infection with these viruses is characterized by a long intervaletween initial infection and the onset of serious symptoms. Theingle-stranded RNA viruses exploit their reverse transcriptasenzyme to synthesize DNA using their RNA as a template. TheNA is then incorporated into the genome of infected cells.AIDS was first diagnosed in European sailors with African
onnections [334–336]. The first AIDS virus, HIV-1, was ini-ially identified in 1983 [337–341]. A second AIDS virus, HIV-2,as discovered in 1986 [342–344]. Forty million people were
stimated to be infected with HIV at the end of 2004 [345]. Theighest prevalence is found in Sub-Saharan Africa and it is risingainly in Asia and some of the former Soviet Union countries
ike Ukraine and the Russian Federation [345,346]. During itspread among humans, group M HIV-1 (one of three groups: M,
and M), has evolved into multiple subtypes that differ fromne another by 10–30% along their genomes [347–350].

370 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
HIV is passed on primarily via four routes: unprotectedsexual intercourse (both homosexual and heterosexual), shar-ing of needles by IV drug users, medical procedures usingHIV-contaminated blood, tissues or equipment, and mother-to-child transmission (MTCT). The likelihood of transmissionis increased by factors that may damage mucosal linings ofexposed tissues, especially by other sexually transmitted dis-eases that cause ulcers or inflammation.
HIV can be transmitted from infected mothers to infants dur-ing pregnancy (intrauterine) through transplacental passage ofthe virus [351], during labor and delivery (intrapartum) throughexposure to infected maternal fluids (blood or vaginal secretions)[352–355] and during the post partum period through breast-feeding [356–359]. Infants who have a positive virologic test(see below) at or before age 48 h are considered to have early(i.e., intrauterine) infection, whereas infants who have a negativevirologic test during the first week of life and subsequent posi-tive tests are considered to have late (i.e., intrapartum) infection[360]. In the absence of breast-feeding, intrauterine transmissionaccounts for 10–35% of infection, and 60–75% of transmissionoccurs during labor and delivery [361–363]. Without interven-tion, maternal infection leads to about 25–30% of babies beinginfected [364–369].
Use of anti-retroviral therapy (ART) during pregnancy inHIV-infected women is associated with improved obstetric out-come of reduced infection rates of babies to less than 2%[Uhpaastr
vrepitAft
7i
nwmdlTtt
Knowledge of maternal HIV infection during the antena-tal period enables HIV-infected women to receive appropriateantiretroviral therapy during pregnancy, during labor, and tonewborns to reduce the risk for HIV transmission from motherto child [370,383,384]. It also allows counseling of infectedwomen about the risks for HIV transmission through breastmilk and advising against breast feeding in countries where safealternatives to breast milk are available [385]. Early diagnos-tic evaluation of HIV-exposed infants permits early initiationof aggressive antiretroviral therapy in infected infants and ini-tiation of prophylaxis against Pneumocystis carinii pneumonia(PCP) in all HIV-exposed infants beginning at age 4–6 weeks inaccordance with Public Health Services (PHS) guidelines [386].
7.1.3. Prenatal laboratory assessment of HIV infectionPrenatal laboratory assessment of congenital HIV infection in
AF or cord blood is not recommended as the invasive proceduresincreases the risk of transmitting the virus from the maternal tothe fetal blood stream.
7.2. Laboratory assessment of HIV infection
7.2.1. HIV antibody assaysThe initial screening for HIV infection in adults and chil-
dren is done by testing for antibodies. Viral load assays arenot intended for routine diagnosis but could be used in clini-ccdithddittw
ssscrOti
ti(estoo
370–373] and little maternal toxicity [374–376]. The currentS guidelines are to offer all pregnant HIV-1-infected womenighly active antiretroviral therapy (HAART) to maximally sup-ress viral replication, reduce the risk of prenatal transmission,nd minimize the risk of development of resistant virus. Inddition, HIV-infected women are offered an elective caesareanection delivery [355]. The results also suggest that special atten-ion should be given to women belonging to previously identifiedisk groups.
Because testing has proven very successful in helping to pre-ent the spread of the disease to babies, a US federal panel hasecommended that all pregnant women, not just those consid-red at high risk, be screened for the AIDS virus [377–381]. Norenatal (intrauterine) diagnosis is performed because: (a) thenfection can occur during delivery and (b) the testing interven-ion may increase the chance of virus transmission to the baby.ssessing the infection status of the mother is critical [381] and
ollowing delivery the new-born should be tested. The laboratoryesting is essential for the diagnosis.
.1.2. Importance of laboratory assessment of HIVnfection in pregnancy
Identification of HIV-infected women before or during preg-ancy is critical to providing optimal therapy for both infectedomen and their children and to preventing perinatal trans-ission (see below). For women with unknown HIV status
uring active labor, ART can still be effective when given duringabor and delivery, followed by treatment of the newborn [382].his expedited intervention requires the use of rapid diagnos-
ic testing during labor or rapid return of results from standardesting.
al management of HIV-infected persons in conjunction withlinical signs and symptoms and other laboratory markers ofisease progression. Detection of HIV-1 p24 antigen (Table 1)s used for routine screening in blood and plasma centers butheir routine use for diagnosing HIV infection in individualsas been discouraged because the estimated average time frometection of p24 antigen to detection of HIV antibody by stan-ard enzyme-immuno-assay (EIA) is 6 days, and not all recentlynfected persons have detectable levels of p24 antigen [387]. Inhe USA several FDA approved tests are available that enablehe testing of HIV antibodies in different body fluids such ashole blood, serum, plasma, oral fluid and urine.The standard testing algorithm for HIV-1 consists of initial
creening with an EIA to detect antibodies to the virus. Reactivepecimens undergo confirmatory testing with a more specificupplemental test, usually a Western blot assay (WB) or, lessommonly, IFA (Table 1) [388]. Using both tests increases accu-acy of the results while maintaining their sensitivity [389–391].nly specimens that are repeatedly reactive by EIA and posi-
ive by IFA or reactive by WB are considered HIV-positive andndicative of HIV infection [389,390,392,393].
Incomplete antibody responses that produce negative or inde-erminate results on WB tests can occur among persons recentlynfected with HIV who have low levels of detectable antibodiesi.e., seroconverting), persons who have end-stage HIV dis-ase, and perinatally exposed but uninfected infants who areeroreverting (i.e., losing maternal antibody). Non-specific reac-ions producing indeterminate results in uninfected persons haveccurred more frequently among pregnant women than amongther persons [389–391,394].
False-positive WB results are rare [395].

E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 371
7.2.2. Detection of viral DNA in maternal and newbornspecimens7.2.2.1. Diagnosis of HIV infection in maternal specimens.Pregnant women are screened for the presence of antibodiesusing the standard testing algorithm for adults (EIA plus WB orIFA) as shown in Fig. 6. For women with unknown HIV statusduring active labor, rapid diagnostic tests are used if rapid returnof results from standard testing is not available.
7.2.2.2. Diagnosis of HIV infection in newborns. Infant HIVtesting should be done as soon after birth as possible soappropriate treatment interventions can be implemented quickly[377,384]. The standard antibody assays used for older childrenand adults are not useful for diagnosing children younger than18 months as the presence of maternal antibodies makes sero-logic tests uninformative. Therefore, a definitive diagnosis ofHIV infection in early infancy requires viral diagnostic assays,including HIV-1 p24 antigen assays, nucleic acid amplification(e.g., PCR) or viral culture. HIV infection can be definitivelydiagnosed in most infected infants by age 1 month and in vir-tually all infected infants by age 6 months. HIV infection isdiagnosed by at least two positive assays using two separatespecimens [378].
HIV DNA PCR is the preferred virologic method for diag-nosing HIV infection during infancy. It has 99% specificity toidentify HIV proviral DNA in peripheral blood mononuclearcE
iHo4sow
tf[biapttN3(t
tcP
gu
antigen testing alone is not recommended because of its sub-stantiallty reduced sensitivity and specificity compromising thecritical need for timely diagnosis [405].
Whether the current, more intensive antiretroviral combina-tion regimens women may receive during pregnancy for treat-ment of their own HIV infection will affect diagnostic test sen-sitivity in their infants is unknown. Similarly, if more complexregimens are administered to HIV-exposed infants for perinatalprophylaxis, the sensitivity of diagnostic assays will need to bere-examined [401].
7.2.2.3. Different subtypes. HIV subtype B is the predominantviral subtype found in the U.S. and western Europe. Non-subtypeB viruses predominate in other parts of the world, such as sub-type C in regions of Africa and India and subtype E in much ofsoutheast Asia.
Currently the available HIV DNA PCR commercial tests areless sensitive for detection for non-subtype B HIV, and falsenegative HIV DNA PCR assays have been reported in infantsinfected with non-subtype B HIV [406–410]. Caution should beexercised in the interpretation of negative HIV DNA PCR testresults in infants born to mothers who may have acquired an HIVnon-B subtype. Some of the currently available HIV RNA assayshave improved sensitivity for detection of non-subtype B HIVinfection [411–413], although even these assays may not detectsome non-B subtypes, particularly group O HIV strains [414]. IncsonHRPcec1
7nsb
(
(
(
ells (PBMC) obtained from whole blood samples collected inDTA-containing tubes [396].
A meta-analysis of published data from 271 infected childrenndicated that HIV DNA PCR was sensitive for the diagnosis ofIV infection during the neonatal period. Thirty-eight percentf infected children had positive HIV DNA PCR tests by age8 h, 93% by age 14 days and 96% by age 28 days. No sub-tantial change in sensitivity during the first week of life wasbserved, but sensitivity increased rapidly during the secondeek.Quantitative assays that detect HIV RNA in plasma (see Sec-
ion 7.2.2.3 below) appear to be as sensitive as HIV DNA PCRor early diagnosis of HIV infection in HIV-exposed infants397–402]. The specificity is comparable between the two tests,ut results of HIV RNA load below 104 copies/ml should benterpreted with caution [403]. Some clinicians use HIV RNAssay as the confirmatory test for infants testing HIV DNA PCRositive since it provides viral load measurement which guidesreatment decisions. Available quantitative RNA tests includehe Amplicor HIV-1 monitor test 1.5 (Roche Diagnostics), theASBA EasyQ HIV-1 (BioMerieux), the Quantiplex HIV RNA.0 (bDNA) (Bayer) and the LCx HIV RNA quantitative assayAbbott Laboratories) assays [416–421]. However, special atten-ion should be taken where non-B HIV is expected.
HIV culture for the diagnosis of infection has a sensitivityhat is similar to that of HIV DNA PCR [404]. However, HIVulture is more complex and expensive to perform than DNACR, and definitive results may not be available for 2–4 weeks.
Both standard and immune-complex-dissociated p24 anti-en tests are highly specific for HIV infection and have beensed to diagnose infection in children. However, the use of p24
ases of infants where non-subtype B perinatal exposure may beuspected and HIV DNA PCR is negative, repeat testing usingne of the newer RNA assays shown to be more sensitive foron-subtype B HIV is recommended (for example, the AmplicorIV-1 monitor test 1.5, Nuclisens HIV-1 qt or Quantiplex HIVNA 3.0 (bDNA) assays). In children with negative HIV DNACR and RNA assays but in whom non-subtype B infectionontinues to be suspected, the clinician should consult with anxpert in pediatric HIV infection and the child should undergolose clinical monitoring and definitive HIV serologic testing at8 months of age.
.2.2.4. Test algorithm for neonates. HIV infection is diag-osed by two virological tests performed on separate bloodamples, regardless of age. The testing rules are summarizedelow and shown in Fig. 6:
1) Initial testing is recommended by age 48 h. As many as40% of infected infants can be identified at this time. Bloodsamples from the umbilical cord should not be used for diag-nostic evaluations, because of concerns regarding potentialcontamination with maternal blood.
2) Repeated diagnostic testing can also be considered at age14 days in infants with negative tests at birth. The diag-nostic sensitivity of virological assays increases rapidly byage 2 weeks. Early identification of infection would permitdiscontinuation of neonatal ZDV chemoprophylaxis and afurther evaluation of the need for more aggressive drug com-bination therapy.
3) Retest infants with initially negative virological tests at age1–2 months. Using ZDV monotherapy to reduce perinatal

372 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
transmission did not delay the detection of HIV in infantsin PACTG protocol 076 [370,400–402,415].
(4) At age 3–6 months retest HIV-exposed children who havehad repeatedly negative virological assays at birth and atage 1–2 months.
(5) HIV infection can be reasonably excluded in non-breast fedinfants with two or more negative virologic tests performedat age >1 month, with one of those being performed at age>4 months [386].
(6) Two or more negative HIV immunoglobulin G (IgG) anti-body tests performed at age >6 months with an interval of atleast 1 month between the tests can also be used to reason-ably exclude HIV infection in HIV-exposed children with noclinical or virologic laboratory evidence of HIV infection.
(7) Serology after 12 months is recommended to confirm thatmaternal HIV antibodies transferred to the infant in uterohave disappeared if there has not been previous confirmationof two negative antibody tests.
(8) If the child is still antibody-positive at 12 months, then test-ing should be repeated between 15 and 18 months [387].Loss of HIV antibody in a child with previously negativeHIV DNA PCR tests definitively confirms that the child isHIV uninfected.
(9) A positive HIV antibody test at >18 months of age indicatesHIV infection [378].
7
nwsiotfsHvfb
HF
A
pti
R
[2] Melnick JL. Taxonomy of viruses. Prog Med Virol 1976;22:211–21.
[3] Oker-Blom C, Kalkkinen N, Kaariainen L, Pettersson RF. Rubella viruscontains one capsid protein and three envelope glycoproteins, E1, E2a,and E2b. J Virol 1983;46:964–73.
[4] Vesikari T. Immune response in rubella infection. Scand J Infect Dis1972;4:1–42.
[5] Mitchell LA, Zhang T, Ho M, Decarie D, Tingle AJ, Zrein M, et al.Characterization of rubella virus-specific antibody responses by usinga new synthetic peptide-based enzyme-linked immunosorbent assay. JClin Microbiol 1992;30:1841–7.
[6] Cooper LZ, Krugman S. Clinical manifestations of postnatal and con-genital rubella. Arch Ophthalmol 1967;77:434–9.
[7] Cooper LZ. The history and medical consequences of rubella. RevInfect Dis 1985;7(Suppl. 1):S2–S10.
[8] Coulter C, Wood R, Robson J. Rubella infection in pregnancy. Com-mun Dis Intell 1999;23:93–6.
[9] Webster WS. Teratogen update: congenital rubella. Teratology1998;58:13–23.
[10] Horstmann DM, Schluederberg A, Emmons JE, Evans BK, Ran-dolph MF, Andiman WA. Persistence of vaccine-induced immuneresponses to rubella: comparison with natural infection. Rev InfectDis 1985;7(Suppl. 1):S80–5.
[11] Harcourt GC, Best JM, Banatvala JE. Rubella-specific serum andnasopharyngeal antibodies in volunteers with naturally acquired andvaccine-induced immunity after intranasal challenge. J Infect Dis1980;142:145–55.
[12] Just M, Just V, Berger R, Burkhardt F, Schilt U. Duration of immunityafter rubella vaccination: a long-term study in Switzerland. Rev InfectDis 1985;7(Suppl. 1):S91–4.
[13] Balfour Jr HH, Amren DP. Rubella, measles and mumps antibodies
.3. SummaryIdentification of HIV-infected women before or during preg-ancy is critical to providing optimal therapy for both infectedomen and their children and to preventing perinatal transmis-
ion. Pregnant women are screened for the presence of antibod-es using the standard testing algorithm for adults (EIA plus WBr IFA). Prenatal laboratory assessment of congenital HIV infec-ion is not recommended as it increases the risk of infecting theetus, but extensive testing is performed to assess the infectiontatus of the baby following delivery. A definitive diagnosis ofIV infection in early infancy requires repeated testing usingirological assays, with HIV DNA PCR being the currently pre-erred method. All infected infants can be definitively diagnosedy age 6 months.
An algorithm describing the laboratory diagnostic assays forIV infection in pregnant women and neonates is shown inig. 6.
cknowledgments
We are grateful to Galit Zemel for her extensive technical sup-ort in organizing the citations and reference list and in preparinghe review for submission. We also thank Zehava Yosefi for help-ng in reference retrieval and typing.
eferences
[1] Hahne SJ, Abbink F, van Binnendijk RS, Ruijs WL, van SteenbergenJE, de Melker HE. [Rubella epidemic in the Netherlands 2004/’05:awareness of congenital rubella syndrome required]. Ned TijdschrGeneeskd 2005;149(21):1174–8.
following vaccination of children. A potential rubella problem. Am JDis Child 1978;132:573–7.
[14] Horstmann DM. Controlling rubella: problems and perspectives. AnnIntern Med 1975;83:412–7.
[15] Schiff GM, Young BC, Stefanovic GM, Stamler EF, Knowlton DR,Grundy BJ, et al. Challenge with rubella virus after loss of detectablevaccine-induced antibody. Rev Infect Dis 1985;7(Suppl. 1):S157–63.
[16] Horstmann DM, Liebhaber H, Le Bouvier GL, Rosenberg DA, Hal-stead SB. Rubella: reinfection of vaccinated and naturally immunepersons exposed in an epidemic. N Engl J Med 1970;283:771–8.
[17] Banatvala JE, Best JM. Rubella. In: Collier L, Timbury M, editors.Topley and Wilson’s principles of bacteriology, virology and immunity.London: Edward Arnold; 1990. p. 501–31.
[18] Herrmann KL. Available rubella serologic tests. Rev Infect Dis1985;7(Suppl. 1):S108–12.
[19] Aboudy Y, Fogel A, Barnea B, Mendelson E, Yosef L, Frank T, et al.Subclinical rubella reinfection during pregnancy followed by transmis-sion of virus to the fetus. J Infect 1997;34:273–6.
[20] Aboudy Y, Barnea B, Yosef L, Frank T, Mendelson E. Clinical rubellareinfection during pregnancy in a previously vaccinated woman. JInfect 2000;41:187–9.
[21] Best JM, Banatvala JE, Morgan-Capner P, Miller E. Fetal infectionafter maternal reinfection with rubella: criteria for defining reinfection.BMJ 1989;299:773–5.
[22] Kleeman KT, Kiefer DJ, Halbert SP. Rubella antibodies detectedby several commercial immunoassays in hemagglutination inhibition-negative sera. J Clin Microbiol 1983;18:1131–7.
[23] Cusi MG, Valensin PE, Cellesi C. Possibility of reinfection afterimmunisation with RA27/3 live attenuated rubella virus. Arch Virol1993;129:337–40.
[24] Fogel A, Handsher R, Barnea B. Subclinical rubella inpregnancy—occurrence and outcome. Isr J Med Sci 1985;21:133–8.
[25] Schluederberg A, Horstmann DM, Andiman WA, Randolph MF. Neu-tralizing and hemagglutination-inhibiting antibodies to rubella virus asindicators of protective immunity in vaccinees and naturally immuneindividuals. J Infect Dis 1978;138:877–83.
E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 373
[26] Best JM, Harcourt GC, Banatvala JE, Congenital. Rubella affecting aninfant whose mother had Rubella antibodies before conception. BMJ1981;282:1235–6.
[27] Best JM, Banatvala JE. Rubella. In: Zuckerman AJ, Banatvala JEJRP,editors. Principles and practice of clinical virology. Chichester: JohnWiley; 2000. p. 387–418.
[28] Fogel A, Barnea BS, Aboudy Y, Mendelson E. Rubella in pregnancyin Israel: 15 years of follow-up and remaining problems. Isr J MedSci 1996;32:300–5.
[29] Banatvala JE, Best JM, O’Shea S, Dudgeon JA. Persistence of rubellaantibodies after vaccination: detection after experimental challenge.Rev Infect Dis 1985;7(Suppl. 1):S86–90.
[30] Hudson P, Morgan-Capner P. Evaluation of 15 commercial enzymeimmunoassays for detection of Rubella specific IgM. Clin Diagn Virol1996;5:21–6.
[31] Matter L, Gorgievski-Hrisoho M, Germann D. Comparison of fourenzyme immunoassays for detection of immunoglobulin M antibodiesagainst rubella virus. J Clin Microbiol 1994;32:2134–9.
[32] Enders G, Knotek F. Detection of IgM antibodies against rubellavirus: comparison of two indirect ELISAs and an anti-IgM captureimmunoassay. J Med Virol 1986;19:377–86.
[33] Thomas HI, Morgan-Capner P, Roberts A, Hesketh L. Persistentrubella-specific IgM reactivity in the absence of recent primary rubellaand rubella reinfection. J Med Virol 1992;36:188–92.
[34] Kurtz JB, Anderson MJ. Cross-reactions in rubella and parvovirus spe-cific IgM tests. Lancet 1985;2:1356.
[35] Thomas HI, Barrett E, Hesketh LM, Wynne A, Morgan-Capner P.Simultaneous IgM reactivity by EIA against more than one virusin measles, parvovirus B19 and rubella infection. J Clin Virol1999;14:107–18.
[36] Best JM, O‘Shea S. Rubella virus. In: Lennette EH, Schmidt NY,
[51] Haukenes G, Blom H. False positive rubella virus haemagglutina-tion inhibition reactions: occurrence and disclosure. Med MicrobiolImmunol (Berl) 1975;161:99–106.
[52] Field PR, Gong CM. Diagnosis of postnatally acquired rubellaby use of three enzyme-linked immunosorbent assays for specificimmunoglobulins G and M and single radial hemolysis for specificimmunoglobulin G. J Clin Microbiol 1984;20:951–8.
[53] Vaheri A, Salonen EM. Evaluation of solid-phase enzyme-immunoassay procedure in immunity surveys and diagnosis of rubella.J Med Virol 1980;5:171–81.
[54] Shekarchi IC, Sever JL, Tzan N, Ley A, Ward LC, Madden D. Compar-ison of hemagglutination inhibition test and enzyme-linked immunosor-bent assay for determining antibody to rubella virus. J Clin Microbiol1981;13:850–4.
[55] Vesikari T, Vaheri A. Rubella: a method for rapid diagnosis of arecent infection by demonstration of the IgM antibodies. Br Med J1968;1:221–3.
[56] Handsher R, Fogel A. Modified staphylococcal absorption method usedfor detecting rubella-specific immunoglobin M antibodies during arubella epidemic. J Clin Microbiol 1977;5:588–92.
[57] Enders G, Knotek F, Pacher U. Comparison of various serologicalmethods and diagnostic kits for the detection of acute, recent, and pre-vious rubella infection, vaccination, and congenital infections. J MedVirol 1985;16:219–32.
[58] Voller A, Bidwell DE, Bartlett A. Enzyme immunoassays in diag-nostic medicine. Theory and practice. Bull World Health Organ1976;53:55–65.
[59] Field PR, Ho DW, Cunningham AL. Evaluation of rubella immunestatus by three commercial enzyme-linked immunosorbent assays. JClin Microbiol 1988;26:990–4.
[60] Salonen EM, Vaheri A, Suni J, Wager O. Rheumatoid factor in acute
editors. Diagnostic procedure for viral, Reckettsial and Chlamydialinfections. Washington, DC: American Public Health association; 1989.p. 731–95.[37] Ogra PL, Chiba Y, Ogra SS, Dzierba JL, Herd JK. Rubella-virus infec-tion in juvenile rheumatoid arthritis. Lancet 1975;1:1157–61.
[38] Wunderli W, Zbinden R, Biedermann K. Rubella IgM detection inpregnancy. Lancet 1990;335:1042–3.
[39] Hedman K, Seppala I. Recent rubella virus infection indicated by alow avidity of specific IgG. J Clin Immunol 1988;8:214–21.
[40] Thomas HI, Morgan-Capner P, Rubella-specific. IgG1 avidity: a com-parison of methods. J Virol Methods 1991;31:219–28.
[41] Bottiger B, Jensen IP. Maturation of rubella IgG avidity over time afteracute rubella infection. Clin Diagn Virol 1997;8:105–11.
[42] Pullen GR, Fitzgerald MG, Hosking CS. Antibody avidity deter-mination by ELISA using thiocyanate elution. J Immunol Methods1986;86:83–7.
[43] Morgan-Capner P. Diagnosing rubella. BMJ 1989;299:338–9.[44] Cradock-Watson JE, Miller E, Ridehalgh MK, Terry GM, Ho-Terry
L. Detection of rubella virus in fetal and placental tissues and in thethroats of neonates after serologically confirmed rubella in pregnancy.Prenat Diagn 1989;9:91–6.
[45] D’Alton ME, DeCherney AH. Prenatal diagnosis. N Engl J Med1993;328:114–20.
[46] Tang JW, Aarons E, Hesketh LM, Strobel S, Schalasta G, Jauniaux E,et al. Prenatal diagnosis of congenital rubella infection in the secondtrimester of pregnancy. Prenat Diagn 2003;23:509–12.
[47] Mace M, Cointe D, Six C, et al. Diagnostic value of reversetranscription-PCR of amniotic fluid for prenatal diagnosis of congenitalrubella infection in pregnant women with confirmed primary rubellainfection. J Clin Microbiol 2004;42(10):4818–20.
[48] Skendzel LP. Rubella immunity. Defining the level of protective anti-body. Am J Clin Pathol 1996;106:170–4.
[49] Stewart GL, Parkman PD, Hopps HE, Douglas RD, Hamilton JP, MeyerJr HM. Rubella-virus hemagglutination-inhibition test. N Engl J Med1967;276:554–7.
[50] Enders G. Serologic test combinations for safe detection of rubellainfections. Rev Infect Dis 1985;7(Suppl. 1):S113–22.
viral infections: interference with determination of IgM, IgG, and IgAantibodies in an enzyme immunoassay. J Infect Dis 1980;142:250–5.
[61] Grangeot-Keros L, Pillot J, Daffos F, Forestier F. Prenatal and postnatalproduction of IgM and IgA antibodies to rubella virus studied byantibody capture immunoassay. J Infect Dis 1988;158:138–43.
[62] Starkey WG, Newcombe J, Corbett KM, Liu KM, Sanders PG, BestJM. Use of rubella virus E1 fusion proteins for detection of rubellavirus antibodies. J Clin Microbiol 1995;33:270–4.
[63] Condorelli F, Stivala A, Gallo R, Musumeci E, Scata MC, StranoL, et al. Improvement in establishing the period of rubella virusprimary infection using a mild protein denaturant. J Virol Methods1997;66:109–12.
[64] Thompson KM, Tobin JO. Isolation of rubella virus from abortionmaterial. Br Med J 1970;1:264–6.
[65] O’Neill HJ, Russell JD, Wyatt DE, McCaughey C, Coyle PV. Isola-tion of viruses from clinical specimens in microtitre plates with cellsinoculated in suspension. J Virol Methods 1996;62:169–78.
[66] Forsgren M, Carlstrom G, Strangert K. Congenital rubella after mater-nal reinfection. Scand J Infect Dis 1979;11:81–3.
[67] O’Shea S, Best JM, Banatvala JE. Viremia, virus excretion, and anti-body responses after challenge in volunteers with low levels of anti-body to rubella virus. J Infect Dis 1983;148:639–47.
[68] Bosma TJ, Corbett KM, O’Shea S, Banatvala JE, Best JM. PCR fordetection of rubella virus RNA in clinical samples. J Clin Microbiol1995;33:1075–9.
[69] Bosma TJ, Corbett KM, Eckstein MB, O’Shea S, Vijayalakshmi P,Banatvala JE, et al. Use of PCR for prenatal and postnatal diagnosisof congenital rubella. J Clin Microbiol 1995;33:2881–7.
[70] Terry GM, Ho-Terry L, Londesborough P, Rees KR. Localization ofthe rubella E1 epitopes. Arch Virol 1988;98:189–97.
[71] Frey TK, Marr LD, Hemphill ML, Dominguez G. Molecular cloningand sequencing of the region of the rubella virus genome coding forglycoprotein E1. Virology 1986;154:228–32.
[72] Revello MG, Baldanti F, Sarasini A, Zavattoni M, Torsellini M, GernaG. Prenatal diagnosis of rubella virus infection by direct detectionand semiquantitation of viral RNA in clinical samples by reversetranscription-PCR. J Clin Microbiol 1997;35:708–13.
374 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
[73] Katow S. Rubella virus genome diagnosis during pregnancy and mech-anism of congenital rubella. Intervirology 1998;41:163–9.
[74] Ho-Terry L, Terry GM, Londesborough P. Diagnosis of foetal rubellavirus infection by polymerase chain reaction. J Gen Virol 1990;71(Pt7):1607–11.
[75] Givens KT, Lee DA, Jones T, Ilstrup DM. Congenital rubella syn-drome: ophthalmic manifestations and associated systemic disorders.Br J Ophthalmol 1993;77:358–63.
[76] Enders G, Bader U, Lindemann L, Schalasta G, Daiminger A. Prenataldiagnosis of congenital cytomegalovirus infection in 189 pregnancieswith known outcome. Prenat Diagn 2001;21:362–77.
[77] Cone RW, Hobson AC, Huang ML. Coamplified positive controldetects inhibition of polymerase chain reactions. J Clin Microbiol1992;30:3185–9.
[78] Naessens A, Casteels A, Decatte L, Foulon W. A serologic strategyfor detecting neonates at risk for congenital cytomegalovirus infection.J Pediatr 2005;146(2):194–7.
[79] Daiminger A, Bader U, Enders G. Pre- and periconceptional primarycytomegalovirus infection: risk of vertical transmission and congenitaldisease. Obstet Gynecol Surv 2005;60(7):420–2.
[80] Rowe WP, Hartley JW, Waterman S, Turner HC, Huebner RJ.Cytopathogenic agent resembling human salivary gland virus recov-ered from tissue cultures of human adenoids. Proc Soc Exp Biol Med1956;92:418–24.
[81] Craig JM, Macauley JC, Weller TH, Wirth P. Isolation of intranu-clear inclusion producing agents from infants with illnesses resemblingcytomegalic inclusion disease. Proc Soc Exp Biol Med 1957;94:4–12.
[82] Smith MG. Propagation in tissue cultures of a cytopathogenic virusfrom human salivary gland virus (SGV) disease. Proc Soc Exp BiolMed 1956;92:424–30.
[83] Liesnard C, Donner C, Brancart F, Gosselin F, Delforge ML, Rodesch
congenital human cytomegalovirus infection. J Med Virol 1995;47:462–6.
[96] Revello MG, Sarasini A, Zavattoni M, Baldanti F, Gerna G. Improvedprenatal diagnosis of congenital human cytomegalovirus infectionby a modified nested polymerase chain reaction. J Med Virol1998;56:99–103.
[97] Bodeus M, Hubinont C, Bernard P, Bouckaert A, Thomas K, GoubauP. Prenatal diagnosis of human cytomegalovirus by culture and poly-merase chain reaction: 98 pregnancies leading to congenital infection.Prenat Diagn 1999;19:314–7.
[98] Catanzarite V, Dankner WM. Prenatal diagnosis of congenitalcytomegalovirus infection: false-negative amniocentesis at 20 weeks’gestation. Prenat Diagn 1993;13:1021–5.
[99] Gouarin S, Palmer P, Cointe D, Rogez S, Vabret A, Rozenberg F, et al.Congenital HCMV infection: a collaborative and comparative study ofvirus detection in amniotic fluid by culture and by PCR. J Clin Virol2001;21:47–55.
[100] Donner C, Liesnard C, Brancart F, Rodesch F. Accuracy of amnioticfluid testing before 21 weeks’ gestation in prenatal diagnosis of con-genital cytomegalovirus infection. Prenat Diagn 1994;14:1055–9.
[101] Chou S, Merigan TC. Rapid detection and quantitation of humancytomegalovirus in urine through DNA hybridization. N Engl J Med1983;308:921–5.
[102] Spector SA, Rua JA, Spector DH, McMillan R. Detection of humancytomegalovirus in clinical specimens by DNA–DNA hybridization. JInfect Dis 1984;150:121–6.
[103] Vonsover A, Gotlieb-Stematsky T, Sayar Y, Bardov L, Manor Y, Sie-gal B. Detection of CMV in urine: comparison between DNA–DNAhybridization, virus isolation, and immunoelectron microscopy. J VirolMethods 1987;16:29–37.
[104] Demmler GJ, Buffone GJ, Schimbor CM, May RA. Detection of
F. Prenatal diagnosis of congenital cytomegalovirus infection: prospec-tive study of 237 pregnancies at risk. Obstet Gynecol 2000;95:881–8.[84] Stagno S, Pass RF, Dworsky ME, Henderson RE, Moore EG, WaltonPD, et al. Congenital cytomegalovirus infection: the relative impor-tance of primary and recurrent maternal infection. N Engl J Med1982;306:945–9.
[85] Stagno S, Pass RF, Cloud G, Britt WJ, Henderson RE, Walton PD, etal. Primary cytomegalovirus infection in pregnancy. Incidence, trans-mission to fetus, and clinical outcome. JAMA 1986;256:1904–8.
[86] Boppana SB, Pass RF, Britt WJ, Stagno S, Alford CA. Symptomaticcongenital cytomegalovirus infection: neonatal morbidity and mortality.Pediatr Infect Dis J 1992;11:93–9.
[87] Raynor BD. Cytomegalovirus infection in pregnancy. Semin Perinatol1993;17:394–402.
[88] Lazzarotto T, Gabrielli L, Lanari M, et al. Congenital cytomegalovirusinfection: recent advances in the diagnosis of maternal infection. HumImmunol 2004;65(5):410–5.
[89] Boppana SB, Miller J, Britt WJ. Transplacentally acquired antiviralantibodies and outcome in congenital human cytomegalovirus infec-tion. Viral Immunol 1996;9:211–8.
[90] Gaytant MA, Steegers EA, Semmekrot BA, Merkus HM, Galama JM.Congenital cytomegalovirus infection: review of the epidemiology andoutcome. Obstet Gynecol Surv 2002;57:245–56.
[91] Lipitz S, Yagel S, Shalev E, Achiron R, Mashiach S, Schiff E. Prenataldiagnosis of fetal primary cytomegalovirus infection. Obstet Gynecol1997;89:763–7.
[92] Melish ME, Hanshaw JB. Congenital cytomegalovirus infection. Devel-opmental progress of infants detected by routine screening. Am J DisChild 1973;126:190–4.
[93] Reimer CB, Black CM, Phillips DJ, Logan LC, Hunter EF, Pender BJ,et al. The specificity of fetal IgM: antibody or anti-antibody? Ann NY Acad Sci 1975;254:77–93.
[94] Stagno S, Pass RF, Reynolds DW, Moore MA, Nahmias AJ, AlfordCA. Comparative study of diagnostic procedures for congenitalcytomegalovirus infection. Pediatrics 1980;65:251–7.
[95] Revello MG, Baldanti F, Furione M, Sarasini A, Percivalle E, Zavat-toni M, et al. Polymerase chain reaction for prenatal diagnosis of
cytomegalovirus in urine from newborns by using polymerase chainreaction DNA amplification. J Infect Dis 1988;158:1177–84.
[105] Lazzarotto T, Guerra B, Spezzacatena P, Varani S, Gabrielli L, PradelliP, et al. Prenatal diagnosis of congenital cytomegalovirus infection. JClin Microbiol 1998;36:3540–4.
[106] Levy R, Najioullah F, Thouvenot D, Bosshard S, Aymard M, LinaB. Evaluation and comparison of PCR and hybridization methods forrapid detection of cytomegalovirus in clinical samples. J Virol Methods1996;62:103–11.
[107] Boppana SB, Fowler KB, Britt WJ, Stagno S, Pass RF. Symp-tomatic congenital cytomegalovirus infection in infants born to motherswith preexisting immunity to cytomegalovirus. Pediatrics 1999;104:55–60.
[108] Boppana SB, Rivera LB, Fowler KB, Mach M, Britt WJ. Intrauterinetransmission of cytomegalovirus to infants of women with preconcep-tional immunity. N Engl J Med 2001;344:1366–71.
[109] Kyriazopoulou V, Bondis J, Frantzidou F, Athanasiadis A, Diza E, Sim-itsopoulou M, et al. Prenatal diagnosis of fetal cytomegalovirus infec-tion in seropositive pregnant women. Eur J Obstet Gynecol ReprodBiol 1996;69:91–5.
[110] Joassin L, Reginster M. Elimination of nonspecific cytomegalovirusimmunoglobulin M activities in the enzyme-linked immunosorbentassay by using anti-human immunoglobulin G. J Clin Microbiol1986;23:576–81.
[111] Deyi YM, Goubau P, Bodeus M, False-positive. IgM antibody tests forcytomegalovirus in patients with acute Epstein-Barr virus infection. EurJ Clin Microbiol Infect Dis 2000;19:557–60.
[112] Moller E, Strom H, Al-Balaghi S. Role of polyclonal activation inspecific immune responses Relevance for findings of antibody activityin various diseases. Scand J Immunol 1980;12:177–82.
[113] Re MC, Landini MP. IgM to human cytomegalovirus: comparisonof two enzyme immunoassays and IgM reactivity to viral polypep-tides detected by immunoblotting. J Clin Lab Anal 1989;3:169–73.
[114] Kangro HO, Griffiths PD, Huber TJ, Heath RB. Specific IgM classantibody production following infection with cytomegalovirus. J MedVirol 1982;10:203–12.
E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 375
[115] Demmler GJ, Six HR, Hurst SM, Yow MD. Enzyme-linkedimmunosorbent assay for the detection of IgM-class antibodies tocytomegalovirus. J Infect Dis 1986;153:1152–5.
[116] Lazzarotto T, Maine GT, Dal Monte P, Ripalti A, Landini MP. A novelWestern blot test containing both viral and recombinant proteins foranticytomegalovirus immunoglobulin M detection. J Clin Microbiol1997;35:393–7.
[117] Lazzarotto T, Ripalti A, Bergamini G, Battista MC, Spezzacatena P,Campanini F, et al. Development of a new cytomegalovirus (CMV)immunoglobulin M (IgM) immunoblot for detection of CMV-specificIgM. J Clin Microbiol 1998;36:3337–41.
[118] Maine GT, Lazzarotto T, Chovan LE, Flanders R, Landini MP. TheDNA-binding protein pUL57 of human cytomegalovirus: comparisonof specific immunoglobulin M (IgM) reactivity with IgM reactivityto other major target antigens. Clin Diagn Lab Immunol 1996;3:358–60.
[119] Schaefer L, Cesario A, Demmler G, Plotkin S, Stagno S, Elrod C,et al. Evaluation of Abbott CMV-M enzyme immunoassay for detec-tion of cytomegalovirus immunoglobulin M antibody. J Clin Microbiol1988;26:2041–3.
[120] Zerbini M, Musiani M, Gentilomi G, La Placa M. Detection of specificimmunoglobulin M antibodies to cytomegalovirus by using monoclonalantibody to immunoglobulin M in an indirect immunofluorescenceassay. J Clin Microbiol 1986;24:166–8.
[121] van Zanten J, Harmsen MC, van der Giessen M, van der Bij W,Prop J, de Leij L, et al. Humoral immune response against humancytomegalovirus (HCMV)-specific proteins after HCMV infection inlung transplantation as detected with recombinant and naturally occur-ring proteins. Clin Diagn Lab Immunol 1995;2:214–8.
[122] Greijer AE, van de Crommert JM, Stevens SJ, Middeldorp JM.Molecular fine-specificity analysis of antibody responses to human
[132] Lazzarotto T, Varani S, Gabrielli L, Spezzacatena P, Landini MP. Newadvances in the diagnosis of congenital cytomegalovirus infection.Intervirology 1999;42:390–7.
[133] Lazzarotto T, Galli C, Pulvirenti R, Rescaldani R, Vezzo R, La GioiaA, et al. Evaluation of the Abbott AxSYM cytomegalovirus (CMV)immunoglobulin M (IgM) assay in conjunction with other CMVIgM tests and a CMV IgG avidity assay. Clin Diagn Lab Immunol2001;8:196–8.
[134] Bodeus M, Goubau P. Predictive value of maternal-IgG avidity forcongenital human cytomegalovirus infection. J Clin Virol 1999;12:3–8.
[135] Bodeus M, Beulne D, Goubau P. Ability of three IgG-avidity assays toexclude recent cytomegalovirus infection. Eur J Clin Microbiol InfectDis 2001;20:248–52.
[136] Bodeus M, Van Ranst M, Bernard P, Hubinont C, Goubau P. Anticy-tomegalovirus IgG avidity in pregnancy: a 2-year prospective study.Fetal Diagn Ther 2002;17:362–6.
[137] Grangeot-Keros L, Mayaux MJ, Lebon P, Freymuth F, Eugene G,Stricker R, et al. Value of cytomegalovirus (CMV) IgG avidity indexfor the diagnosis of primary CMV infection in pregnant women. JInfect Dis 1997;175:944–6.
[138] Prince HE, Leber AL. Validation of an in-house assay forcytomegalovirus immunoglobulin G (CMV IgG) avidity and rela-tionship of avidity to CMV IgM levels. Clin Diagn Lab Immunol2002;9:824–7.
[139] Ruellan-Eugene G, Barjot P, Campet M, Vabret A, Herlicoviez M,Muller G, et al. Evaluation of virological procedures to detectfetal human cytomegalovirus infection: avidity of IgG antibodies,virus detection in amniotic fluid and maternal serum. J Med Virol1996;50:9–15.
[140] Schoppel K, Kropff B, Schmidt C, Vornhagen R, Mach M. The
cytomegalovirus and design of novel synthetic-peptide-based serodi-agnostic assays. J Clin Microbiol 1999;37:179–88.[123] Daiminger A, Bader U, Eggers M, Lazzarotto T, Enders G. Evaluationof two novel enzyme immunoassays using recombinant antigens todetect cytomegalovirus-specific immunoglobulin M in sera from preg-nant women. J Clin Virol 1999;13:161–71.
[124] Genser B, Truschnig-Wilders M, Stunzner D, Landini MP, Halwachs-Baumann G. Evaluation of five commercial enzyme immunoassays forthe detection of human cytomegalovirus-specific IgM antibodies in theabsence of a commercially available gold standard. Clin Chem LabMed 2001;39:62–70.
[125] Maine GT, Stricker R, Schuler M, Spesard J, Brojanac S, Iriarte B, etal. Development and clinical evaluation of a recombinant-antigen-basedcytomegalovirus immunoglobulin M automated immunoassay using theAbbott AxSYM analyzer. J Clin Microbiol 2000;38:1476–81.
[126] Weber B, Berger A, Rabenau H. Human cytomegalovirus infection:diagnostic potential of recombinant antigens for cytomegalovirus anti-body detection. J Virol Methods 2001;96:157–70.
[127] Lazzarotto T, Varani S, Spezzacatena P, Gabrielli L, Pradelli P, GuerraB, et al. IgG avidity and IgM detected by blot as diagnostic tools toidentify pregnant women at risk of transmitting cytomegalovirus. ViralImmunol 2000;13:137–41.
[128] Blackburn NK, Besselaar TG, Schoub BD, O’Connell KF. Differen-tiation of primary cytomegalovirus infection from reactivation usingthe urea denaturation test for measuring antibody avidity. J Med Virol1991;33:6–9.
[129] Fowler KB, Stagno S, Pass RF, Britt WJ, Boll TJ, Alford CA. Theoutcome of congenital cytomegalovirus infection in relation to maternalantibody status. N Engl J Med 1992;326:663–7.
[130] Sipewa MJ, Goubau P, Bodeus M. Evaluation of a cytomegalovirusglycoprotein B recombinant enzyme immunoassay to discrimi-nate between a recent and a past infection. J Clin Microbiol2002;40:3689–93.
[131] Lazzarotto T, Spezzacatena P, Varani S, Gabrielli L, Pradelli P, GuerraB, et al. Anticytomegalovirus (anti-CMV) immunoglobulin G avidityin identification of pregnant women at risk of transmitting congenitalCMV infection. Clin Diagn Lab Immunol 1999;6:127–9.
humoral immune response against human cytomegalovirus is charac-terized by a delayed synthesis of glycoprotein-specific antibodies. JInfect Dis 1997;175:533–44.
[141] Baccard-Longere M, Freymuth F, Cointe D, Seigneurin JM, Grangeot-Keros L. Multicenter evaluation of a rapid and convenient methodfor determination of cytomegalovirus immunoglobulin G avidity. ClinDiagn Lab Immunol 2001;8:429–31.
[142] Mace M, Sissoeff L, Rudent A, Grangeot-Keros L. A serological test-ing algorithm for the diagnosis of primary CMV infection in pregnantwomen. Prenat Diagn 2004;24(11):861–3.
[143] Daiminger A, Bader U, Enders G. An enzyme linked immunoas-say using recombinant antigens for differentiation of primary fromsecondary or past CMV infections in pregnancy. J Clin Virol1998;11:93–102.
[144] Eggers M, Metzger C, Enders G. Differentiation between acute primaryand recurrent human cytomegalovirus infection in pregnancy, using amicroneutralization assay. J Med Virol 1998;56:351–8.
[145] Eggers M, Bader U, Enders G. Combination of microneutralizationand avidity assays: improved diagnosis of recent primary humancytomegalovirus infection in single serum sample of second trimesterpregnancy. J Med Virol 2000;60:324–30.
[146] Eggers M, Radsak K, Enders G, Reschke M. Use of recombi-nant glycoprotein antigens gB and gH for diagnosis of primaryhuman cytomegalovirus infection during pregnancy. J Med Virol2001;63:135–42.
[147] Hodinka RL. Human cytomegalovirus. In: Murphy PR, Baron EJ,Pfaller MA, Tenover FC, Yolken RH, editors. Manual of Clinicalmicrobiology. 1999. p. 889–991.
[148] Gerna G, Baldanti F, Percivalle E, Zavattoni M, Campanini G, RevelloMG. Early identification of human cytomegalovirus strains by the shellvial assay is prevented by a novel amino acid substitution in UL123IE1 gene product. J Clin Microbiol 2003;41:4494–5.
[149] Zipeto D, Sarasini A, Rossi F, Baldanti F, Revello MG, MilanesiG, et al. Identification of human cytomegalovirus strain withimmediate-early (IE) antigen-specific monoclonal antibody is pre-vented by point mutation in IE gene. J Clin Microbiol 1994;32:1402–5.
376 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
[150] Donner C, Liesnard C, Content J, Busine A, Aderca J, Rodesch F. Pre-natal diagnosis of 52 pregnancies at risk for congenital cytomegalovirusinfection. Obstet Gynecol 1993;82:481–6.
[151] Grose C, Meehan T, Weiner CP. Prenatal diagnosis of congenitalcytomegalovirus infection by virus isolation after amniocentesis. Pedi-atr Infect Dis J 1992;11:605–7.
[152] Hagay ZJ, Biran G, Ornoy A, Reece EA. Congenital cytomegalovirusinfection: a long-standing problem still seeking a solution. Am J ObstetGynecol 1996;174:241–5.
[153] Nicolini U, Kustermann A, Tassis B, Fogliani R, Galimberti A, Perci-valle E, et al. Prenatal diagnosis of congenital human cytomegalovirusinfection. Prenat Diagn 1994;14:903–6.
[154] Skvorc-Ranko R, Lavoie H, St-Denis P, Villeneuve R, Gagnon M,Chicoine R, et al. Intrauterine diagnosis of cytomegalovirus and rubellainfections by amniocentesis. CMAJ 1991;145:649–54.
[155] Weiner CP, Grose C. Prenatal diagnosis of congenital cytomegalovirusinfection by virus isolation from amniotic fluid. Am J Obstet Gynecol1990;163:1253–5.
[156] Avidor B, Efrat G, Weinberg M, Kra-oz Z, Satinger J, Mitrani-Rosenbaum S, et al. Insight into the intrinsic sensitivity of the PCRassay used to detect CMV infection in amniotic fluid specimens. J ClinVirol 2004;29:260–70.
[157] Boeckh M, Huang M, Ferrenberg J, Stevens-Ayers T, StenslandL, Nichols WG, et al. Optimization of quantitative detection ofcytomegalovirus DNA in plasma by real-time PCR. J Clin Microbiol2004;42:1142–8.
[158] Gouarin S, Vabret A, Gault E, Petitjean J, Regeasse A, Hurault deLigny B, et al. Quantitative analysis of HCMV DNA load in wholeblood of renal transplant patients using real-time PCR assay. J ClinVirol 2004;29:194–201.
[159] Piiparinen H, Hockerstedt K, Gronhagen-Riska C, Lautenschlager I.
[169] Gershon AA, Raker R, Steinberg S, Topf-Olstein B, Drusin LM. Anti-body to varicella-zoster virus in parturient women and their offspringduring the first year of life. Pediatrics 1976;58:692–6.
[170] Linder N, Waintraub I, Smetana Z, Barzilai A, Lubin D, Mendelson E,et al. Placental transfer and decay of varicella-zoster virus antibodiesin preterm infants. J Pediatr 2000;137:85–9.
[171] Enders G, Miller E, Cradock-Watson J, Bolley I, Ridehalgh M. Conse-quences of varicella and herpes zoster in pregnancy: prospective studyof 1739 cases. Lancet 1994;343:1548–51.
[172] Chapman SJ. Varicella in pregnancy. Semin Perinatol 1998;22:339–46.[173] Pastuszak AL, Levy M, Schick B, Zuber C, Feldkamp M, Gladstone J,
et al. Outcome after maternal varicella infection in the first 20 weeksof pregnancy. N Engl J Med 1994;330:901–5.
[174] Paryani SG, Arvin AM. Intrauterine infection with varicella-zostervirus after maternal varicella. N Engl J Med 1986;314:1542–6.
[175] Dufour P, de Bievre P, Vinatier D, Tordjeman N, Da Lage B, VanhoveJ, et al. Varicella and pregnancy. Eur J Obstet Gynecol Reprod Biol1996;66:119–23.
[176] Nikkels AF, Delbecque K, Pierard GE, Wienkotter B, Schalasta G,Enders M. Distribution of varicella-zoster virus DNA and gene prod-ucts in tissues of a first-trimester varicella-infected fetus. J Infect Dis2005;191(4):540–5.
[177] Sauerbrei A, Pawlak J, Luger C, Wutzler P. Intracerebral varicella-zoster virus reactivation in congenital varicella syndrome. Dev MedChild Neurol 2003;45(12):837–40.
[178] Enders G. Varicella-zoster virus infection in pregnancy. Prog Med Virol1984;29:166–96.
[179] Prober CG, Gershon AA, Grose C, McCracken Jr GH, Nelson JD.Consensus: varicella-zoster infections in pregnancy and the perinatalperiod. Pediatr Infect Dis J 1990;9:865–9.
[180] Grose C. Varicella infection during pregnancy. Herpes 1999;6:33–7.
Comparison of two quantitative CMV PCR tests, Cobas AmplicorCMV Monitor and TaqMan assay, and pp65-antigenemia assay in thedetermination of viral loads from peripheral blood of organ transplantpatients. J Clin Virol 2004;30:258–66.[160] Nedelec O, Bellagra N, Devisme L, Hober D, Wattre P, DewildeA. Congenital human cytomegalovirus infection: value of humancytomegalovirus DNA quantification in amniotic fluid. Ann Biol Clin(Paris) 2002;60:201–7.
[161] Revello MG, Zavattoni M, Furione M, Baldanti F, Gerna G. Quantifi-cation of human cytomegalovirus DNA in amniotic fluid of mothersof congenitally infected fetuses. J Clin Virol 1999;37:3350–2.
[162] Picone O, Costa JM, Leruez-Ville M, Ernault P, Olivi M, Ville Y,et al. Cytomegalovirus (CMV) glycoprotein B genotype and CMVDNA load in the amniotic fluid of infected fetuses. Prenat Diagn2004;24(12):1001–6.
[163] Gouarin S, Gault E, Vabret A, Cointe D, Rozenberg F, Grangeot-KerosL, et al. Real-time PCR quantification of human cytomegalovirus DNAin amniotic fluid samples from mothers with primary infection. J ClinMicrobiol 2002;40:1767–72.
[164] Guerra B, Lazzarotto T, Quarta S, Lanari M, Bovicelli L, Nicolosi A,et al. Prenatal diagnosis of symptomatic congenital cytomegalovirusinfection. Am J Obstet Gynecol 2000;183:476–82.
[165] Herrmann B, Larsson VC, Rubin CJ, Sund F, Eriksson BM, Arvidson J,et al. Comparison of a duplex quantitative real-time PCR assay and theCOBAS Amplicor CMV Monitor test for detection of cytomegalovirus.J Clin Microbiol 2004;42:1909–14.
[166] Kalpoe JS, Kroes AC, de Jong MD, Schinkel J, de BrouwerCS, Beersma MF, et al. Validation of clinical application ofcytomegalovirus plasma DNA load measurement and definition oftreatment criteria by analysis of correlation to antigen detection. JClin Microbiol 2004;42:1498–504.
[167] O’Riordan M, O’Gorman C, Morgan C, Mc Cafferkey M, Henry G,McKenna PI. Sera prevalence of varicella zoster virus in pregnantwomen in Dublin Ir. J Med Sci 2000;169:288.
[168] Leikin E, Figueroa R, Bertkau A, Lysikiewicz A, Visintainer P, TejaniN. Seronegativity to varicella-zoster virus in a tertiary care obstetricpopulation. Obstet Gynecol 1997;90:511–3.
[181] Stein O, Smetana Z, Dulitzki M, Stevenson DK, Mashiach S, Seid-man DS, et al. Zoster antibody status in pregnant women exposed tovarricella. Isr J Obst Gynecol 1996;7:106–10.
[182] Linder N, Ferber A, Kopilov U, Smetana Z, Barzilai A, MendelsonE, et al. Reported exposure to chickenpox: a predictor of positiveanti-varicella-zoster antibodies in parturient women. Fetal Diagn Ther2001;16:423–6.
[183] Mouly F, Mirlesse V, Meritet JF, Rozenberg F, Poissonier MH, LebonP, et al. Prenatal diagnosis of fetal varicella-zoster virus infection withpolymerase chain reaction of amniotic fluid in 107 cases. Am J ObstetGynecol 1997;177:894–8.
[184] Steinberg SP, Gershon AA. Measurement of antibodies to varicella-zoster virus by using a latex agglutination test. J Clin Microbiol1991;29:1527–9.
[185] Landry ML, Ferguson D. Comparison of latex agglutination test withenzyme-linked immunosorbent assay for detection of antibody tovaricella-zoster virus. J Clin Microbiol 1993;31:3031–3.
[186] Leventon-Kriss S, Yoffe R, Rannon L, Modan M. Seroepidemiologicaspects of varicella zoster virus infections in an Israeli Jewish popu-lation. Isr J Med Sci 1978;14:766–70.
[187] Haikin H, Leventon-Kriss S, Sarov I. Antibody to varicella-zostervirus-induced membrane antigen: immunoperoxidase assay with air-dried target cells. J Infect Dis 1979;140:601–4.
[188] Shehab Z, Brunell PA. Enzyme-linked immunosorbent assay for sus-ceptibility to varicella. J Infect Dis 1983;148:472–6.
[189] Waner LJ, Weller TH. In: Emmons NJSRW, editor. Varicella zostervirus diagnostic procedures for viral, Rickettsial and Chlamydial infec-tion. ApHA American public Health Association; 1989. p. 379–406.
[190] Qureshi F, Jacques SM. Maternal varicella during pregnancy: correla-tion of maternal history and fetal outcome with placental histopathol-ogy. Hum Pathol 1996;27:191–5.
[191] Puchhammer-Stockl E, Kunz C, Wagner G, Enders G. Detection ofvaricella zoster virus (VZV) DNA in fetal tissue by polymerase chainreaction. J Perinat Med 1994;22:65–9.
[192] Mehraein Y, Rehder H, Draeger HG, Froster-Iskenius UG, SchwingerE, Holzgreve W. [Diagnosis of fetal virus infections by in situhybridization]. Geburtshilfe Frauenheilkd 1991;51:984–9.
E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 377
[193] Gottardi H, Rabensteiner A, Delucca A, Lobbiani A, Nocco A, ColucciG. [Detection of varicella virus with a DNA probe in fetal blood andamniotic fluid]. Geburtshilfe Frauenheilkd 1991;51:63–4.
[194] Schmidt NJ, Gallo D, Devlin V, Woodie JD, Emmons RW. Directimmunofluorescence staining for detection of herpes simplex andvaricella-zoster virus antigens in vesicular lesions and certain tissuespecimens. J Clin Microbiol 1980;12:651–5.
[195] Ziegler T. Detection of varicella-zoster viral antigens in clini-cal specimens by solid-phase enzyme immunoassay. J Infect Dis1984;150:149–54.
[196] Brinker JP, Doern GV. Comparison of MRC-5 and A-549 cells inconventional culture tubes and shell vial assays for the detection ofvaricella-zoster virus. Diagn Microbiol Infect Dis 1993;17:75–7.
[197] Gershon AA, LaRussa P, Steinberg SP. Varicella-zoster virus. In: Mur-ray RR, Barron EJ, Pfaller MA, Tenover FC, Yolken RH, editors.Manual of Clinical Microbiology. 7th ed. Washington, DC: AmericanSociety for Microbiology; 1999. p. 900–11.
[198] Arvin AM. In: Fields B, editor. Varicella-zoster virus virology. NewYork: Raven Press; 1995. p. 2547–86.
[199] Levin MJ, Leventhal S, Masters HA. Factors influencing quantitativeisolation of varicella-zoster virus. J Clin Microbiol 1984;19:880–3.
[200] Arvin AM. Varicella-zoster virus. Clin Microbiol Rev 1996;9:361–81.[201] Rawlinson WD, Dwyer DE, Gibbons VL, Cunningham AL. Rapid
diagnosis of varicella-zoster virus infection with a monoclonal anti-body based direct immunofluorescence technique. J Virol Methods1989;23:13–8.
[202] Sadick NS, Swenson PD, Kaufman RL, Kaplan MH. Comparisonof detection of varicella-zoster virus by the Tzanck smear, directimmunofluorescence with a monoclonal antibody, and virus isolation.J Am Acad Dermatol 1987;17:64–9.
[203] Perez JL, Garcia A, Niubo J, Salva J, Podzamczer D, Martin R. Com-
[215] Nilson A, Myrmel H. Changing trends in genital herpes simplex virusinfection. Obstet Gynecol 2000;79:693–6.
[216] Hutto C, Arvin A, Jacobs R, Steele R, Stagno S, Lyrene R, et al.Intrauterine herpes simplex virus infections. J Pediatr 1987;110:97–101.
[217] Stagno S, Whitley RJ. Herpes virus infections in the neonate andchildren. In: K.K.H., editor. Sexully transmitted diseases. New York:McGraw Hill; 1990. p. 872–3.
[218] Brown ZA, Benedetti J, Selke S, Ashley R, Watts DH, Corey L.Asymptomatic maternal shedding of herpes simplex virus at the onsetof labor: relationship to preterm labor. Obstet Gynecol 1996;87:483–8.
[219] Brown ZA, Benedetti J, Ashley R, Burchett S, Selke S, Berry S,et al. Neonatal herpes simplex virus infection in relation to asymp-tomatic maternal infection at the time of labor. N Engl J Med1991;324:1247–52.
[220] Malkin JE, Beumont MG. Herpes simplex virus infection in pregnancy.Herpes 1999;6(2):47–50.
[221] Gibbs RS, Dinsmoor MJ, Newton ER, Ramamurthy RS. A randomizedtrial of intrapartum versus immediate postpartum treatment of womenwith intra-amniotic infection. Obstet Gynecol 1988;72:823–8.
[222] Blanchier H, Huraux JM, Huraux-Rendu C, Sainte-Croix le BaleurA. Genital herpes and pregnancy—preventive measures. Eur J ObstetGynecol Reprod Biol 1994;53:33–8.
[223] Brown ZA, Selke S, Zeh J, Kopelman J, Maslow A, Ashley RL, etal. The acquisition of herpes simplex virus during pregnancy. N EnglJ Med 1997;337:509–15.
[224] ACOG criteria set. Cesarean delivery. Number 35, July 1998. Com-mittee on quality assessment. American College of Obstetricians andGynecologists. Int J Gynaecol Obstet 1998;63:206–7.
[225] Amann ST, Fagnant RJ, Chartrand SA, Monif GR. Herpes simplex
parison of techniques and evaluation of three commercial monoclonalantibodies for laboratory diagnosis of varicella-zoster virus in muco-cutaneous specimens. J Clin Microbiol 1994;32:1610–3.[204] Nahass GT, Goldstein BA, Zhu WY, Serfling U, Penneys NS, LeonardiCL. Comparison of Tzanck smear, viral culture, and DNA diagnosticmethods in detection of herpes simplex and varicella-zoster infection.JAMA 1992;268:2541–4.
[205] Kido S, Ozaki T, Asada H, Higashi K, Kondo K, Hayakawa Y, etal. Detection of varicella-zoster virus (VZV) DNA in clinical samplesfrom patients with VZV by the polymerase chain reaction. J ClinMicrobiol 1991;29:76–9.
[206] Weidmann M, Meyer-Konig U, Hufert FT. Rapid detection of herpessimplex virus and varicella-zoster virus infections by real-time PCR. JClin Microbiol 2003;41:1565–8.
[207] Cuthbertson G, Grose C. Biotinylated and radioactive DNA probes fordetection of varicella-zoster virus genome in infected human cells. MolCell Probes 1988;2:197–207.
[208] Vonsover A, Leventon-Kriss S, Langer A, Smetana Z, Zaizov R,Potaznick D, et al. Detection of varicella-zoster virus in lymphocytesby DNA hybridization. J Med Virol 1987;21:57–66.
[209] Stranska R, Schuurman R, de Vos M, van Loon AM. Routine use ofa highly automated and internally controlled real-time PCR assay forthe diagnosis of herpes simplex and varicella-zoster virus infections. JClin Virol 2004;30:39–44.
[210] Stocher M, Holzl G, Stekel H, Berg J. Automated detection of fivehuman herpes virus DNAs by a set of LightCycler PCRs complementedwith a single multiple internal control. J Clin Virol 2004;29:171–8.
[211] Whitley RJ. Neonatal herpes simplex virus infections. Clin Perinatol1988;15:903–16.
[212] Lafferty WE, Downey L, Celum C, Wald A. Herpes simplex virus type1 as a cause of genital herpes: impact on surveillance and prevention.J Infect Dis 2000;181:1454–7.
[213] Nahmias AJ, Keyserling HL, Lee FK. Herpes simplex virus 1 and 2.In: Evans AS, editor. Viral infections of humans: epidemiology andcontrol. 3rd ed. 1989. p. 393–417.
[214] Corey L, Spear PG. Infections with herpes simplex viruses (2). N EnglJ Med 1986;314:749–57.
infection associated with short-term use of a fetal scalp electrode. Acase report. J Reprod Med 1992;37:372–4.
[226] Kimura H, Futamura M, Kito H, Ando T, Goto M, Kuzushima K, etal. Detection of viral DNA in neonatal herpes simplex virus infections:frequent and prolonged presence in serum and cerebrospinal fluid. JInfect Dis 1991;164:289–93.
[227] Malm G, Forsgren M. Neonatal herpes simplex virus infections: HSVDNA in cerebrospinal fluid and serum. Arch Dis Child Fetal NeonatalEd 1999;81:F24–9.
[228] Lakeman FD, Whitley RJ. Diagnosis of herpes simplex encephalitis:application of polymerase chain reaction to cerebrospinal fluid frombrain-biopsied patients and correlation with disease. National Insti-tute of Allergy and Infectious Diseases Collaborative Antiviral StudyGroup. J Infect Dis 1995;171:857–63.
[229] Kimberlin DW, Lakeman FD, Arvin AM, Prober CG, Corey L, PowellDA, et al. Application of the polymerase chain reaction to the diagnosisand management of neonatal herpes simplex virus disease. NationalInstitute of Allergy and Infectious Diseases Collaborative AntiviralStudy Group. J Infect Dis 1996;174:1162–7.
[230] Ashley LR. Type specific antibodies to HSV1 and 2 Review of methol-ogy. Herpes 1998;5:33–8.
[231] Cleary KL, Pare E, Stamilio D, Macones GA. Type-specific screeningfor asymptomatic herpes infection in pregnancy: a decision analysis.BJOG 2005;112(6):731–6.
[232] Baker D, Brown Z, Hollier LM, et al. Cost-effectiveness of herpes sim-plex virus type 2 serologic testing and antiviral therapy in pregnancy.Am J Obstet Gynecol 2004;191(6):2074–84.
[233] Twagira M, Hadzic N, Smith M, et al. Disseminated neonatal herpessimplex virus (HSV) type 2 infection diagnosed by HSV DNA detec-tion in blood and successfully managed by liver transplantation. Eur JPediatr 2004;163(3):166–9.
[234] Leventon-Kriss S, Rannon L, Smetana Z, Yoffe R. Increase inlaboratory-confermed cases of herpes genitalis and neonatal herpesinfection in Israel. Isr J Med Sci 1983;19:946–9.
[235] Kimberlin DW, Whitley RJ. Antiviral resistance: mechanisms, clin-ical significance, and future implications. J Antimicrob Chemother1996;37:403–21.
378 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
[236] Stamos JK, Rowley AH. Timely diagnosis of congenital infections.Pediatr Clin North Am 1994;41:1017–33.
[237] Ashley LR, Corey L. Herpes simplex viruses. In: Schmidt N, WhitelyR, Emmons, editors. Diagnostic procedures for viral, Rickettial andChlamydial infection. ApHA American Public Health Association;1989. p. 265–319.
[238] Rawls WE, Iwamato K, Adam E, Melnick JL. Measurement of anti-bodies to herpesvirus type 1 and type 2 in human sera. J Immunol1970;104:599–606.
[239] Strick L, Wald A. Type-specific testing for herpes simplex virus. ExpertRev Mol Diagn 2004;4(4):443–53.
[240] Ashley RL, Wald A. Genital herpes: review of the epidemic and poten-tial use of type-specific serology. Clin Microbiol Rev 1999;12:1–8.
[241] Ashley RL. Performance and use of HSV type-specific serology testkits. Herpes 2002;9:38–45.
[242] Olofsson S, Lundstrom M, Marsden H, Jeansson S, Vahlne A. Charac-terization of a herpes simplex virus type 2-specified glycoprotein withaffinity for N-acetylgalactosamine-specific lectins and its identificationas g92K or gG. J Gen Virol 1986;67(Pt 4):737–44.
[243] Proffit MR, Schindler SA. Rapid detection of HSV with enzyme-linkedvirus inducible system employing a genetically modified cell line. ClinDiagn Virol 1995;4:175–82.
[244] Kimberlin DW. Advances in the treatment of neonatal herpes simplexinfections. Rev Med Virol 2001;11:157–63.
[245] Espy MJ, Uhl JR, Mitchell PS, Thorvilson JN, Svien KA, Wold AD,et al. Diagnosis of herpes simplex virus infections in the clinical lab-oratory by LightCycler PCR. J Clin Microbiol 2000;38:795–9.
[246] Ozawa K, Ayub J, Hao YS, Kurtzman G, Shimada T, Young N. Noveltranscription map for the B19 (human) pathogenic parvovirus. J Virol1987;61:2395–406.
[247] van Elsacker-Niele AM, Kross AC. Human parvovirus B19: relevance
[261] Takahashi T, Ozawa K, Takahashi K, Okuno Y, Muto Y, Takaku FSS.DNA replication of Parvovirus B19 in a human erythrooid leukemiacell-line (TK-1) in vitro. Arch Virol 1993;131:201–8.
[262] Ozawa K, Kurtzman G, Young N. Replication of the B19 parvovirusin human bone marrow cell cultures. Science 1986;233:883–6.
[263] Anand A, Gray ES, Brown T, Clewley JP, Cohen BJ. Human par-vovirus infection in pregnancy and hydrops fetalis. N Engl J Med1987;316:183–6.
[264] Morey AL, Keeling JW, Porter HJ, Fleming KA. Clinical andhistopathological features of parvovirus B19 infection in the humanfetus. Br J Obstet Gynaecol 1992;99:566–74.
[265] Brown T, Anand A, Ritchie LD, Clewley JP, Reid TM. Intrauter-ine parvovirus infection associated with hydrops fetalis. Lancet1984;2:1033–4.
[266] Knott PD, Welply GA, Anderson MJ. Serologically proved intrauterineinfection with parvovirus. Br Med J (Clin Res Ed) 1984;289:1660.
[267] Mortimer PP, Cohen BJ, Buckley MM, Cradock-Watson JE, Ride-halgh MK, Burkhardt F, et al. Human parvovirus and the fetus. Lancet1985;2:1012.
[268] Cohen BJ, Buckley MM. The prevalence of antibody to human par-vovirus B19 in England and Wales. J Med Microbiol 1988;25:151–3.
[269] Harger JH, Adler SP, Koch WC, Harger GF. Prospective evaluation of618 pregnant women exposed to parvovirus B19: risks and symptoms.Obstet Gynecol 1998;91:413–20.
[270] Rodis JF. Parvovirus infection. Clin Obstet Gynecol 1999;42:107–20,quiz 74–5.
[271] Gratacos E, Torres PJ, Vidal J, Antolin E, Costa J, Jimenez de AntaMT, et al. The incidence of human parvovirus B19 infection dur-ing pregnancy and its impact on perinatal outcome. J Infect Dis1995;171:1360–3.
[272] Hemauer A, Gigler A, Searle K, Beckenlehner K, Raab U, Broliden
in internal medicine. Neth J Med 1999;54(6):221–30.[248] Anderson MJ, Jones SE, Fisher-Hoch SP, Lewis E, Hall SM, BartlettCL, et al. Human parvovirus, the cause of erythema infectiosum (fifthdisease)? Lancet 1983;1:1378.
[249] Anderson MJ, Pattison JR. The human parvovirus. Brief review. ArchVirol 1984;82:137–48.
[250] Anderson MJ, Lewis E, Kidd IM, Hall SM, Cohen BJ. An outbreakof erythema infectiosum associated with human parvovirus infection.J Hyg (Lond) 1984;93:85–93.
[251] Anderson MJ, Higgins PG, Davis LR, Willman JS, Jones SE, KiddIM, et al. Experimental parvoviral infection in humans. J Infect Dis1985;152:257–65.
[252] Reid DM, Reid TM, Brown T, Rennie JA, Eastmond CJ. Humanparvovirus-associated arthritis: a clinical and laboratory description.Lancet 1985;1:422–5.
[253] White DG, Woolf AD, Mortimer PP, Cohen BJ, Blake DR, Bacon PA.Human parvovirus arthropathy. Lancet 1985;1:419–21.
[254] Pattison JR, Jones SE, Hodgson J, Davis LR, White JM, Stroud CE, etal. Parvovirus infections and hypoplastic crisis in sickle-cell anaemia.Lancet 1981;1:664–5.
[255] Zerbini M, Musiani M, Venturoli S, Gallinella G, Gibellini D, Gen-tilomi G, et al. Different syndromes associated with B19 parvovirusviraemia in paediatric patients: report of four cases. Eur J Pediatr1992;151:815–7.
[256] Heegaard ED, Brown KE. Human parvovirus B19. Clin Microbiol Rev2002;15:485–505.
[257] Naides SJ. Rheumatic manifestations of parvovirus B19 infection.Rheum Dis Clin North Am 1998;24:375–401.
[258] Van Horn DK, Mortimer PP, Young N, Hanson GR. Human parvovirus-associated red cell aplasia in the absence of underlying hemolyticanemia. Am J Pediatr Hematol Oncol 1986;8:235–9.
[259] Kurtzman GJ, Ozawa K, Cohen B, Hanson G, Oseas R, Young NS.Chronic bone marrow failure due to persistent B19 parvovirus infec-tion. N Engl J Med 1987;317:287–94.
[260] Zerbini M. Human parvoviruses. In: Murray PR, Baron EJ, Pfallar MA,Tenover FC, Yolken RH, editors. Manual of clinical microbiol. Wash-ington, DC: American Society for Microbiology; 1999. p. 1089–98.
K, et al. Seroprevalence of parvovirus B19 NS1-specific IgG in B19-infected and uninfected individuals and in infected pregnant women. JMed Virol 2000;60:48–55.
[273] Enders M, Weidner A, Zoellner I, Searle K, Enders G. Fetal morbidityand mortality after acute human parvovirus B19 infection in preg-nancy: prospective evaluation of 1018 cases. Prenat Diagn 2004;24(7):513–8.
[274] Fairley CK, Smoleniec JS, Caul OE, Miller E. Observational study ofeffect of intrauterine transfusions on outcome of fetal hydrops afterparvovirus B19 infection. Lancet 1995;346:1335–7.
[275] Zerbini M, Musiani M, Gentilomi G, Venturoli S, Gallinella G,Morandi R. Comparative evaluation of virological and serologicalmethods in prenatal diagnosis of parvovirus B19 fetal hydrops. J ClinMicrobiol 1996;34:603–8.
[276] Torok TJ, Wang QY, Gary Jr GW, Yang CF, Finch TM, AndersonLJ. Prenatal diagnosis of intrauterine infection with parvovirus B19 bythe polymerase chain reaction technique. Clin Infect Dis 1992;14:149–55.
[277] Peters MT, Nicolaides KH. Cordocentesis for the diagnosis andtreatment of human fetal parvovirus infection. Obstet Gynecol1990;75:501–4.
[278] Forestier F, Tissot JD, Vial Y, Daffos F, Hohlfeld P. Haematologicalparameters of parvovirus B19 infection in 13 fetuses with hydropsfoetalis. Br J Haematol 1999;104:925–7.
[279] Kaliasam C, Brennand J, Cameron AD. Congenital parvoviralB19 infection: experience of a recent epidemic. Fetal Diagn Ther2001;16:18–22.
[280] Miyagawa E, Yoshida T, Takahashi H, Yamaguchi K, Nagano T,Kiriyama Y, et al. Infection of the erythroid cell line KU812Ep6 withhuman parvovirus B19 and its application to titration of B19 infectivity.J Virol Methods 1999;83:45–54.
[281] Shimomura S, Komatsu N, Frickhofen N, Anderson S, Kajigaya S,Young NS. First continuous propagation of B19 parvovirus in a cellline. Blood 1992;79:18–24.
[282] Soderlund M, Brown CS, Spaan WJ, Hedman L, Hedman K. Epitopetype-specific IgG responses to capsid proteins VP1 and VP2 of humanparvovirus B19. J Infect Dis 1995;172:1431–6.
E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 379
[283] Dorsch S, Kaufmann B, Schaible U, Prohaska E, Wolf H, Modrow S.The VP1-unique region of parvovirus B19: amino acid variability andantigenic stability. J Gen Virol 2001;82:191–9.
[284] Kerr S, O’Keeffe G, Kilty C, Doyle S. Undenatured parvovirus B19antigens are essential for the accurate detection of parvovirus B19 IgG.J Med Virol 1999;57:179–85.
[285] Manaresi E, Zuffi E, Gallinella G, Gentilomi G, Zerbini M, MusianiM. Differential IgM response to conformational and linear epitopesof parvovirus B19 VP1 and VP2 structural proteins. J Med Virol2001;64:67–73.
[286] Corcoran A, Mahon BP, Doyle S. B cell memory is directed towardconformational epitopes of parvovirus B19 capsid proteins and theunique region of VP1. J Infect Dis 2004;189:1873–80.
[287] Heegaard ED, Rasksen CJ, Christensen J. Detection of parvovirus B19NS1-specific antibodies by ELISA and Western blotting employingrecombinant NS1 protein as antigen. J Med Virol 2002;67:375–83.
[288] Manaresi E, Gallinella G, Zerbini M, Venturoli S, Gentilomi G,Musiani M. IgG immune response to B19 parvovirus VP1 and VP2linear epitopes by immunoblot assay. J Med Virol 1999;57:174–8.
[289] Nunoue T, Kusuhara K, Hara T. Human fetal infection with parvovirusB19: maternal infection time in gestation, viral persistence and fetalprognosis. Pediatr Infect Dis J 2002;21:1133–6.
[290] Koch WC, Harger JH, Barnstein B, Adler SP. Serologic and virologicevidence for frequent intrauterine transmission of human parvovirusB19 with a primary maternal infection during pregnancy. Pediatr InfectDis J 1998;17:489–94.
[291] Wattre P, Dewilde A, Subtil D, Andreoletti L, Thirion V. A clinicaland epidemiological study of human parvovirus B19 infection in fetalhydrops using PCR Southern blot hybridization and chemilumines-cence detection. J Med Virol 1998;54:140–4.
[292] Musiani M, Azzi A, Zerbini M, Gibellini D, Venturoli S, Zakrzewska
[303] McOmish F, Yap PL, Jordan A, Hart H, Cohen BJ, Simmonds P. Detec-tion of parvovirus B19 in donated blood: a model system for screeningby polymerase chain reaction. J Clin Microbiol 1993;31:323–8.
[304] Braham S, Gandhi J, Beard S, Cohen B. Evaluation of the RocheLightCycler parvovirus B19 quantification kit for the diagnosis of par-vovirus B19 infections. J Clin Virol 2004;31:5–10.
[305] Brown KE. Detection and quantitation of parvovirus B19. J Clin Virol2004;31:1–4.
[306] Aberham C, Pendl C, Gross P, Zerlauth G, Gessner M. A quanti-tative, internally controlled real-time PCR assay for the detection ofparvovirus B19 DNA. J Virol Methods 2001;92:183–91.
[307] Manaresi E, Gallinella G, Zuffi E, Bonvicini F, Zerbini M, Musiani M.Diagnosis and quantitative evaluation of parvovirus B19 infections byreal-time PCR in the clinical laboratory. J Med Virol 2002;67:275–81.
[308] Schorling S, Schalasta G, Enders G, Zauke M. Quantification of par-vovirus B19 DNA using COBAS AmpliPrep automated sample prepa-ration and LightCycler real-time PCR. J Mol Diagn 2004;6:37–41.
[309] Brown CS, van Bussel MJ, Wassenaar AL, van Elsacker-Niele AM,Weiland HT, Salimans MM. An immunofluorescence assay for thedetection of parvovirus B19 IgG and IgM antibodies based on recom-binant viral antigen. J Virol Methods 1990;29:53–62.
[310] Brown CS, Salimans MM, Noteborn MH, Weiland HT. Antigenic par-vovirus B19 coat proteins VP1 and VP2 produced in large quantitiesin a baculovirus expression system. Virus Res 1990;15:197–211.
[311] Fridell E, Trojnar J, Wahren B. A new peptide for human parvovirusB19 antibody detection. Scand J Infect Dis 1989;21:597–603.
[312] Jordan JA. Comparison of a baculovirus-based VP2 enzyme immunoas-say (EIA) to an Escherichia coli-based VP1 EIA for detection ofhuman parvovirus B19 immunoglobulin M and immunoglobulin G insera of pregnant women. J Clin Microbiol 2000;38:1472–5.
[313] Manaresi E, Gallinella G, Venturoli S, Zerbini M, Musiani M. Detec-
K, et al. Nested polymerase chain reaction assay for the detection ofB19 parvovirus DNA in human immunodeficiency virus patients. JMed Virol 1993;40:157–60.[293] Hamilton H, Gomos J, Berns KI, Falck-Pedersen E. Adeno-associated virus site-specific integration and AAVS1 disruption. J Virol2004;78:7874–82.
[294] Musiani M, Zerbini M, Gentilomi G, Rodorigo G, De Rosa V, GibelliniD, et al. Persistent B19 parvovirus infections in haemophilic HIV-1infected patients. J Med Virol 1995;46:103–8.
[295] Hendrie PC, Hirata RK, Russell DW. Chromosomal integrationand homologous gene targeting by replication-incompetent vectorsbased on the autonomous parvovirus minute virus of mice. J Virol2003;77:13136–45.
[296] Gallinella G, Zuffi E, Gentilomi G, Manaresi E, Venturoli S, BonviciniF, et al. Relevance of B19 markers in serum samples for a diagnosisof parvovirus B19-correlated diseases. J Med Virol 2003;71:135–9.
[297] Cassinotti P, Weitz M, Siegl G. Human parvovirus B19 infections:routine diagnosis by a new nested polymerase chain reaction assay. JMed Virol 1993;40:228–34.
[298] Musiani M, Zerbini M, Gentilomi G, Plazzi M, Gallinella G, VenturoliS. Parvovirus B19 clearance from peripheral blood after acute infection.J Infect Dis 1995;172:1360–3.
[299] Patou G, Pillay D, Myint S, Pattison J. Characterization of a nestedpolymerase chain reaction assay for detection of parvovirus B19. JClin Microbiol 1993;31:540–6.
[300] Searle K, Guilliard C, Wallat S, Schalasta G, Enders G. Acute par-vovirus B19 infection in pregnant women—an analysis of serial sam-ples by serological and semi-quantitative PCR techniques. Infection1998;26:139–43.
[301] Azzi A, Zakrzewska K, Bertoni E, Guidi S, Salvadori M. Persistentparvovirus B19 infections with different clinical outcomes in renaltransplant recipients: diagnostic relevance of polymerase chain reaction(PCR) and of quantification of B19 DNA in sera. Clin Microbiol Infect1996;2:105–8.
[302] Jordan J, Tiangco B, Kiss J, Koch W. Human parvovirus B19: preva-lence of viral DNA in volunteer blood donors and clinical outcomesof transfusion recipients. Vox Sang 1998;75:97–102.
tion of parvovirus B19 IgG: choice of antigens and serological tests.J Clin Virol 2004;29:51–3.
[314] Butchko AR, Jordan JA. Comparison of three commercially avail-able serologic assays used to detect human parvovirus B19-specificimmunoglobulin M (IgM) and IgG antibodies in sera of pregnantwomen. J Clin Microbiol 2004;42:3191–5.
[315] Bruu AL, Nordbo SA. Evaluation of five commercial tests for detectionof immunoglobulin M antibodies to human parvovirus B19. J ClinMicrobiol 1995;33:1363–5.
[316] Tolfvenstam T, Ruden U, Broliden K. Evaluation of serological assaysfor identification of parvovirus B19 immunoglobulin M. Clin DiagnLab Immunol 1996;3:147–50.
[317] Patou G, Ayliffe U. Evaluation of commercial enzyme linkedimmunosorbent assay for detection of B19 parvovirus IgM and IgG. JClin Pathol 1991;44:831–4.
[318] Cohen BJ, Mortimer PP, Pereira MS. Diagnostic assays with mono-clonal antibodies for the human serum parvovirus-like virus (SPLV). JHyg (Lond) 1983;91:113–30.
[319] Anderson MJ, Jones SE, Minson AC. Diagnosis of human parvovirusinfection by dot-blot hybridization using cloned viral DNA. J MedVirol 1985;15:163–72.
[320] Mori J, Field AM, Clewley JP, Cohen BJ. Dot blot hybridizationassay of B19 virus DNA in clinical specimens. J Clin Microbiol1989;27:459–64.
[321] Zerbini M, Musiani M, Venturoli S, Gallinella G, Gibellini D, Gen-tilomi G, et al. Rapid screening for B19 parvovirus DNA in clinicalspecimens with a digoxigenin-labeled DNA hybridization probe. J ClinMicrobiol 1990;28:2496–9.
[322] Zerbini M, Gentilomi G, Cricca M, Manaresi E, Bonvicini F, MusianiM. A system to enhance the sensitivity of digoxigenin-labelledprobe: detection of B19 DNA in serum samples. J Virol Methods2001;93:137–44.
[323] Wong S, Young NS, Brown KE. Prevalence of parvovirus B19 in livertissue: no association with fulminant hepatitis or hepatitis-associatedaplastic anemia. J Infect Dis 2003;187:1581–6.
[324] Sevall JS, Ritenhous J, Peter JB. Laboratory diagnosis of parvovirusB19 infection. J Clin Lab Anal 1992;6:171–5.
380 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
[325] Kovacs BW, Carlson DE, Shahbahrami B, Platt LD. Prenatal diagnosisof human parvovirus B19 in nonimmune hydrops fetalis by polymerasechain reaction. Am J Obstet Gynecol 1992;167:461–6.
[326] Carriere C, Boulanger P, Delsert C. Rapid and sensitive method forthe detection of B19 virus DNA using the polymerase chain reactionwith nested primers. J Virol Methods 1993;44:221–34.
[327] Dieck D, Schild RL, Hansmann M, Eis-Hubinger AM. Prenatal diag-nosis of congenital parvovirus B19 infection: value of serologicaland PCR techniques in maternal and fetal serum. Prenat Diagn1999;19:1119–23.
[328] Schwartz TF, Jager G, Holzgreve W, Roggendorf M. Diagnosis ofhuman parvovirus B19 by polymerase chain reaction scan. J InfectDis 1992;24:691–6.
[329] Eis-Hubinger AM, Dieck D, Schild R, Hansmann M, Schneweis KE.Parvovirus B19 infection in pregnancy. Intervirology 1998;41:178–84.
[330] Cassinotti P, Burtonboy G, Fopp M, Siegl G. Evidence for persis-tence of human parvovirus B19 DNA in bone marrow. J Med Virol1997;53:229–32.
[331] Soderlund M, von Essen R, Haapasaari J, Kiistala U, Kiviluoto O,Hedman K. Persistence of parvovirus B19 DNA in synovial mem-branes of young patients with and without chronic arthropathy. Lancet1997;349:1063–5.
[332] Knoll A, Louwen F, Kochanowski B, Plentz A, Stussel J, BeckenlehnerK, et al. Parvovirus B19 infection in pregnancy: quantitative viral DNAanalysis using a kinetic fluorescence detection system (TaqMan PCR).J Med Virol 2002;67:259–66.
[333] Varmus H. Retroviruses. Science 1988;240(4858):1427–35.[334] Zhu T, Korber BT, Nahmias AJ, Hooper E, Sharp PM, Ho DD. An
African HIV-1 sequence from 1959 and implications for the origin ofthe epidemic. Nature 1998;391(6667):594–7.
[335] Corbitt G, Bailey AS, Williams G. HIV infection in Manchester. Lancet
FE, Mellors J, Mullins JI, Wolanski S, Korber B, editors. Human retro-viruses and AIDS: a compilation and analysis of nucleic and aminoacid sequences. Los Alamos, NM: Los Alamos National Laboratory;2000. p. 492–505.
[349] Robertson DL, Anderson JP, Bradac JA, Carr JK, Foley B, FunkhouserRK, et al. HIV-1 nomenclature proposal. Science 2000;288(5463):55–6.
[350] Coffin JM. HIV population dynamics in vivo: implications for geneticvariation, pathogenesis, and therapy. Science 1995;267(5197):483–9.
[351] Lewis SH, Reynolds-Kohler C, Fox HE, Nelson JA. HIV-1 in tro-phoblastic and villous Hofbauer cells, and haematological precursorsin eight-week fetuses. Lancet 1990;335(8689):565–8.
[352] Rogers MF, Ou CY, Rayfield M, Thomas PA, Schoenbaum EE, AbramsE, et al. Use of the polymerase chain reaction for early detection ofthe proviral sequences of human immunodeficiency virus in infantsborn to seropositive mothers. New York City Collaborative Study ofMaternal HIV Transmission and Montefiore Medical Center HIV Peri-natal Transmission Study Group. N Engl J Med 1989;320(25):1649–54.
[353] Burgard M, Mayaux MJ, Blanche S, Ferroni A, Guihard-Moscato ML,Allemon MC, et al. The use of viral culture and p24 antigen testingto diagnose human immunodeficiency virus infection in neonates. TheHIV Infection in Newborns French Collaborative Study Group. N EnglJ Med 1992;327(17):1192–7.
[354] Goedert JJ, Duliege AM, Amos CI, Felton S, Biggar RJ. High riskof HIV-1 infection for first-born twins. The international registry ofHIV-exposed twins. Lancet 1991;338(8781):1471–5.
[355] Villari P, Spino C, Chalmers TC, Lau J, Sacks HS. Cesarean sectionto reduce perinatal transmission of human immunodeficiency virus Ametaanalysis. Online J Curr Clin Trials 1993. Doc No. 74:[5107 words;46 paragraphs].
[356] Oxtoby MJ. Human immunodeficiency virus and other viruses in
1990;336(8706):51.[336] Williams G, Stretton TB, Leonard JC. AIDS in 1959? Lancet1983;2(8359):1136.
[337] Barre-Sinoussi F, Chermann JC, Rey F, Nugeyre MT, Chamaret S,Gruest J, et al. Isolation of a T-lymphotropic retrovirus from a patientat risk for acquired immune deficiency syndrome (AIDS). Science1983;220(4599):868–71.
[338] Popovic M, Sarngadharan MG, Read E, Gallo RC. Detection, isolation,and continuous production of cytopathic retroviruses (HTLV-III) frompatients with AIDS and pre-AIDS. Science 1984;224(4648):497–500.
[339] Wain-Hobson S, Alizon M, Montagnier L. Relationship of AIDS toother retroviruses. Nature 1985;313(6005):743.
[340] Wain-Hobson S, Sonigo P, Danos O, Cole S, Alizon M. Nucleotidesequence of the AIDS virus, LAV. Cell 1985;40(1):9–17.
[341] Shaw GM, Hahn BH, Arya SK, Groopman JE, Gallo RC, Wong-StaalF. Molecular characterization of human T-cell leukemia (lymphotropic)virus type III in the acquired immune deficiency syndrome. Science1984;226(4679):1165–71.
[342] Clavel F. HIV-2, the West African AIDS virus. AIDS1987;1(3):135–40.
[343] Clavel F, Guetard D, Brun-Vezinet F, Chamaret S, Rey MA, Santos-Ferreira MO, et al. Isolation of a new human retrovirus from WestAfrican patients with AIDS. Science 1986;233(4761):343–6.
[344] Horsburgh Jr CR, Holmberg SD. The global distribution ofhuman immunodeficiency virus type 2 (HIV-2) infection. Transfusion1988;28(2):192–5.
[345] UNAIDS. 2004 Report on the global AIDS epidemic. Geneva:UnAIDS; 2004.
[346] Hahn BH, Shaw GM, De Cock KM, Sharp PM. AIDS asa zoonosis: scientific and public health implications. Science2000;287(5453):607–14.
[347] Korber B, Muldoon M, Theiler J, Gao F, Gupta R, Lapedes A,et al. Timing the ancestor of the HIV-1 pandemic strains. Science2000;288(5472):1789–96.
[348] Robertson DL, Anderson JL, Bradac JA, Carr JK, Foley B, FunkhouserRK, et al. HIV-1 nomenclature proposal: a reference guide to HIV-1classification. In: Kuiken CL, Foley B, Hahn BH, Marx P, McCutchan
human milk: placing the issues in broader perspective. Pediatr InfectDis J 1988;7(12):825–35.
[357] Hira SK, Mangrola UG, Mwale C, Chintu C, Tembo G, Brady WE, etal. Apparent vertical transmission of human immunodeficiency virustype 1 by breast-feeding in Zambia. J Pediatr 1990;117(3):421–4.
[358] Van de Perre P, Hitimana DG, Simonon A, Dabis F, Msellati P, KaritaP, et al. Postnatal transmission of HIV-1 associated with breast abscess.Lancet 1992;339(8807):1490–1.
[359] Van de Perre P, Simonon A, Msellati P, Hitimana DG, Vaira D, Bazuba-gira A, et al. Postnatal transmission of human immunodeficiency virustype 1 from mother to infant. A prospective cohort study in Kigali,Rwanda. N Engl J Med 1991;325(9):593–8.
[360] Bryson YJ, Luzuriaga K, Sullivan JL, Wara DW. Proposed definitionsfor in utero versus intrapartum transmission of HIV-1. N Engl J Med1992;327(17):1246–7.
[361] Fowler MG, Simonds RJ, Roongpisuthipong A. Update on perinatalHIV transmission. Pediatr Clin North Am 2000;47(1):21–38.
[362] Mohlala BK, Tucker TJ, Besser MJ, Williamson C, Yeats J, Smit L, etal. Investigation of HIV in amniotic fluid from HIV-infected pregnantwomen at full term. J Infect Dis 2005;192(3):488–91.
[363] Magder LS, Mofenson L, Paul ME, Zorrilla CD, Blattner WA, TuomalaRE, et al. Risk factors for in utero and intrapartum transmission of HIV.J Acquir Immune Defic Syndr 2005;38(1):87–95.
[364] Newell ML, Dunn DT, Peckham CS, Semprini AE, Pardi G. Verticaltransmission of HIV-1: maternal immune status and obstetric factors.The European Collaborative Study. AIDS 1996;10(14):1675–81.
[365] Pitt J, Brambilla D, Reichelderfer P, Landay A, McIntosh K, Burns D,et al. Maternal immunologic and virologic risk factors for infant humanimmunodeficiency virus type 1 infection: findings from the Women andInfants Transmission Study. J Infect Dis 1997;175(3):567–75.
[366] Orloff SL, Simonds RJ, Steketee RW, St Louis ME. Determinants ofperinatal HIV-1 transmission. Clin Obstet Gynecol 1996;39(2):386–95.
[367] Dabis F, Msellati P, Dunn D, Lepage P, Newell ML, Peckham C, et al.Estimating the rate of mother-to-child transmission of HIV. Report of aworkshop on methodological issues Ghent (Belgium), 17–20 February1992. The Working Group on Mother-to-Child Transmission of HIV.AIDS 1993;7(8):1139–48.
E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382 381
[368] De Cock KM, Fowler MG, Mercier E, de Vincenzi I, Saba J, HoffE, et al. Prevention of mother-to-child HIV transmission in resource-poor countries: translating research into policy and practice. JAMA2000;283(9):1175–82.
[369] Best JM. Laboratory diagnosis of intrauterine and perinatal virus infec-tions. Clin Diagn Virol 1996;5(2–3):121–9.
[370] Connor EM, Sperling RS, Gelber R, Kiselev P, Scott G, O’SullivanMJ, et al. Reduction of maternal-infant transmission of human immun-odeficiency virus type 1 with zidovudine treatment. Pediatric AIDSClinical Trials Group Protocol 076 Study Group. N Engl J Med1994;331(18):1173–80.
[371] Simonds RJ, Steketee R, Nesheim S, Matheson P, Palumbo P, AlgerL, et al. Impact of zidovudine use on risk and risk factors for peri-natal transmission of HIV. Perinatal AIDS Collaborative TransmissionStudies. AIDS 1998;12(3):301–8.
[372] Shaffer N, Chuachoowong R, Mock PA, Bhadrakom C, SiriwasinW, Young NL, et al. Short-course zidovudine for perinatal HIV-1 transmission in Bangkok Thailand: a randomised controlled trial.Bangkok Collaborative Perinatal HIV Transmission Study Group.Lancet 1999;353(9155):773–80.
[373] Garcia PM, Kalish LA, Pitt J, Minkoff H, Quinn TC, BurchettSK, et al. Maternal levels of plasma human immunodeficiency virustype 1 RNA and the risk of perinatal transmission. Women andInfants Transmission Study Group. N Engl J Med 1999;341(6):394–402.
[374] Tuomala RE, Watts DH, Li D, Vajaranant M, Pitt J, Hammill H, et al.Improved obstetric outcomes and few maternal toxicities are associatedwith antiretroviral therapy, including highly active antiretroviral therapyduring pregnancy. J Acquir Immune Defic Syndr 2005;38(4):449–73.
[375] Mofenson LM, Lambert JS, Stiehm ER, Bethel J, Meyer 3rd WA,Whitehouse J, et al. Risk factors for perinatal transmission of human
[386] CDC. 1995 revised guidelines for prophylaxis against Pneumocystiscarinii pneumonia for children infected with or perinatally exposed tohuman immunodeficiency virus. MMWR 1995;44(no. RR-4).
[387] CDC. Guidelines for national human immunodeficiency virus casesurveillance, including monitoring for human immunodeficiency virusinfection and acquired immunodeficiency syndrome. MMWR 1999;48(no. RR-13):1–31.
[388] George JR, Schochetman G. Detection of HIV infection using serologictechniques. In: Schochetman G, George JR, editors. AIDS testing: acomprehensive guide to technical, medical, social, legal, and manage-ment issues. 2nd ed. New York, NY: Springer-Verlag; 1994.
[389] Celum CL, Coombs RW, Lafferty W, Inui TS, Louie PH, Gates CA, etal. Indeterminate human immunodeficiency virus type 1 western blots:seroconversion risk, specificity of supplemental tests, and an algorithmfor evaluation. J Infect Dis 1991;164(4):656–64.
[390] Celum CL, Coombs RW, Jones M, Murphy V, Fisher L, Grant C, etal. Risk factors for repeatedly reactive HIV-1 EIA and indeterminatewestern blots. A population-based case-control study. Arch Intern Med1994;154(10):1129–37.
[391] Gwinn M, Redus MA, Granade TC, Hannon WH, George JR. HIV-1serologic test results for one million newborn dried-blood specimens:assay performance and implications for screening. J Acquir ImmuneDefic Syndr 1992;5(5):505–12.
[392] Celum CL, Coombs RW. Indeterminate HIV-1 western blots: impli-cations and considerations for widespread HIV testing. J Gen InternMed 1992;7(6):640–5.
[393] Dock NL, Kleinman SH, Rayfield MA, Schable CA, Williams AE,Dodd RY. Human immunodeficiency virus infection and indeterminatewestern blot patterns. Prospective studies in a low prevalence popula-tion. Arch Intern Med 1991;151(3):525–30.
[394] Jackson JB, MacDonald KL, Cadwell J, Sullivan C, Kline WE, Hanson
immunodeficiency virus type 1 in women treated with zidovudine.Pediatric AIDS Clinical Trials Group Study 185 Team. N Engl J Med1999;341(6):385–93.[376] Ioannidis JP, Abrams EJ, Ammann A, Bulterys M, Goedert JJ, GrayL, et al. Perinatal transmission of human immunodeficiency virus type1 by pregnant women with RNA virus loads <1000 copies/ml. J InfectDis 2001;183(4):539–45.
[377] CDC. Recommendations for use of antiretroviral drugs in pregnantHIV-1-infected women for maternal health and interventions to reduceperinatal HIV-1 transmission in the United States. MMWR 2005.
[378] CDC. Revised guidelines for HIV counseling, testing, and referraland revised recommendations for HIV screening of pregnant women.MMWR 2001;50(RR-19).
[379] ACOG educational bulletin. Human immunodeficiency virus infectionsin pregnancy. American College of Obstetricians and Gynecologists.Int J Gynaecol Obstet 1997;57(1):73–80.
[380] Mofenson LM. Technical report: perinatal human immunodeficiencyvirus testing and prevention of transmission. Committee on PediatricAids. Pediatrics 2000;106(6):E88.
[381] Institute of Medicine, National Research Council. Reducing the odds:preventing perinatal transmission of HIV in the United States. Wash-ington, DC: National Academy Press; 1999.
[382] Guay LA, Musoke P, Fleming T, Bagenda D, Allen M, NakabiitoC, et al. Intrapartum and neonatal single-dose nevirapine comparedwith zidovudine for prevention of mother-to-child transmission ofHIV-1 in Kampala Uganda: HIVNET 012 randomised trial. Lancet1999;354(9181):795–802.
[383] CDC. USPHS Task Force Recommendations for use of antiretroviraldrugs in pregnant HIV-1-infected women for maternal health and inter-ventions to reduce perinatal HIV-1 transmission in the United States.MMWR 2002;51(RR-18):1–38.
[384] CDC. Recommendations of the U.S. Public Health Service Task Forceon the use of zidovudine to reduce perinatal transmission of humanimmunodeficiency virus. MMWR 1994;43(no. RR-11).
[385] American Academy of Pediatrics CoPA. Human milk, breastfeeding,and transmission of human immunodeficiency virus in the UnitedStates. Pediatrics 1995;96:977–9.
M, et al. Absence of HIV infection in blood donors with indeter-minate western blot tests for antibody to HIV-1. N Engl J Med1990;322(4):217–22.
[395] MacDonald KL, Jackson JB, Bowman RJ, Polesky HF, Rhame FS,Balfour Jr HH, et al. Performance characteristics of serologic testsfor human immunodeficiency virus type 1 (HIV-1) antibody amongMinnesota blood donors. Public health and clinical implications. AnnIntern Med 1989;110(8):617–21.
[396] Dunn DT, Brandt CD, Krivine A, Cassol SA, Roques P, BorkowskyW, et al. The sensitivity of HIV-1 DNA polymerase chain reaction inthe neonatal period and the relative contributions of intra-uterine andintra-partum transmission. AIDS 1995;9(9):F7–F11.
[397] Steketee RW, Abrams EJ, Thea DM, Brown TM, Lambert G, OrloffS, et al. Early detection of perinatal human immunodeficiency virus(HIV) type 1 infection using HIV RNA amplification and detection.New York City Perinatal HIV Transmission Collaborative Study. JInfect Dis 1997;175(3):707–11.
[398] Delamare C, Burgard M, Mayaux MJ, Blanche S, Doussin A, IvanoffS, et al. HIV-1 RNA detection in plasma for the diagnosis of infectionin neonates. The French Pediatric HIV Infection Study Group. J AcquirImmune Defic Syndr Hum Retrovirol 1997;15(2):121–5.
[399] Simonds RJ, Brown TM, Thea DM, Orloff SL, Steketee RW, Lee FK,et al. Sensitivity and specificity of a qualitative RNA detection assay todiagnose HIV infection in young infants. Perinatal AIDS CollaborativeTransmission Study. AIDS 1998;12(12):1545–9.
[400] Cunningham CK, Charbonneau TT, Song K, Patterson D, Sullivan T,Cummins T, et al. Comparison of human immunodeficiency virus 1DNA polymerase chain reaction and qualitative and quantitative RNApolymerase chain reaction in human immunodeficiency virus 1-exposedinfants. Pediatr Infect Dis J 1999;18(1):30–5.
[401] Young NL, Shaffer N, Chaowanachan T, Chotpitayasunondh T, Van-parapar N, Mock PA, et al. Early diagnosis of HIV-1-infected infantsin Thailand using RNA and DNA PCR assays sensitive to non-B sub-types. J Acquir Immune Defic Syndr 2000;24(5):401–7.
[402] Nesheim S, Palumbo P, Sullivan K, Lee F, Vink P, Abrams E, etal. Quantitative RNA testing for diagnosis of HIV-infected infants. JAcquir Immune Defic Syndr 2003;32(2):192–5.

382 E. Mendelson et al. / Reproductive Toxicology 21 (2006) 350–382
[403] Frenkel LM, Mullins JI, Learn GH, Manns-Arcuino L, Herring BL,Kalish ML, et al. Genetic evaluation of suspected cases of transientHIV-1 infection of infants. Science 1998;280(5366):1073–7.
[404] McIntosh K, Pitt J, Brambilla D, Carroll S, Diaz C, HandelsmanE, et al. Blood culture in the first 6 months of life for the diagno-sis of vertically transmitted human immunodeficiency virus infection.The Women and Infants Transmission Study Group. J Infect Dis1994;170(4):996–1000.
[405] Nesheim S, Lee F, Kalish ML, Ou CY, Sawyer M, Clark S, et al.Diagnosis of perinatal human immunodeficiency virus infection bypolymerase chain reaction and p24 antigen detection after immunecomplex dissociation in an urban community hospital. J Infect Dis1997;175(6):1333–6.
[406] Haas J, Geiss M, Bohler T. False-negative polymerase chain reaction-based diagnosis of human immunodeficiency virus (HIV) type 1 inchildren infected with HIV strains of African origin. J Infect Dis1996;174(1):244–5.
[407] Kline NE, Schwarzwald H, Kline MW. False negative DNA polymerasechain reaction in an infant with subtype C human immunodeficiencyvirus 1 infection. Pediatr Infect Dis J 2002;21(9):885–6.
[408] Zaman MM, Recco RA, Haag R. Infection with non-B subtype HIVtype 1 complicates management of established infection in adultpatients and diagnosis of infection in newborn infants. Clin Infect Dis2002;34(3):417–8.
[409] Gottesman BS, Grosman Z, Lorber M, Levi I, Shitrit P, Mileguir F, etal. Measurement of HIV RNA in patients infected by subtype C byassays optimized for subtype B results in an underestimation of theviral load. J Med Virol 2004;73(2):167–71.
[410] Cunningham P, Marriott D, Harris C, Hancock S, Carr A, CooperD. False negative HIV-1 proviral DNA polymerase chain reaction ina patient with primary infection acquired in Thailand. J Clin Virol
with human immunodeficiency virus type 1 subtype G and BG recom-binant forms. J Clin Microbiol 2003;41(7):3361–7.
[413] Plantier JC, Gueudin M, Damond F, Braun J, Mauclere P, SimonF. Plasma RNA quantification and HIV-1 divergent strains. J AcquirImmune Defic Syndr 2003;33(1):1–7.
[414] Geelen S, Lange J, Borleffs J, Wolfs T, Weersink A, Schuurman R.Failure to detect a non-B HIV-1 subtype by the HIV-1 Amplicor Mon-itor test, version 1 5: a case of unexpected vertical transmission. AIDS2003;17(5):781–2.
[415] Kovacs A, Xu J, Rasheed S, Li XL, Kogan T, Lee M, et al. Compar-ison of a rapid nonisotopic polymerase chain reaction assay with fourcommonly used methods for the early diagnosis of human immunode-ficiency virus type 1 infection in neonates and children. Pediatr InfectDis J 1995;14(11):948–54.
[416] Lin HJ, Pedneault L, Hollinger FB. Intra-assay performance charac-teristics of five assays for quantification of human immunodeficiencyvirus type 1 RNA in plasma. J Clin Microbiol 1998;36(3):835–9.
[417] Erice A, Brambilla D, Bremer J, Jackson JB, Kokka R, Yen-LiebermanB, et al. Performance characteristics of the QUANTIPLEX HIV-1RNA 3 0 assay for detection and quantitation of human immunod-eficiency virus type 1 RNA in plasma. J Clin Microbiol 2000;38(8):2837–45.
[418] Murphy DG, Cote L, Fauvel M, Rene P, Vincelette J. Multicentercomparison of Roche COBAS AMPLICOR MONITOR version 1.5,Organon Teknika NucliSens QT with Extractor, and Bayer Quantiplexversion 3 0 for quantification of human immunodeficiency virus type1 RNA in plasma. J Clin Microbiol 2000;38(11):4034–41.
[419] Abravaya K, Esping C, Hoenle R, Gorzowski J, Perry R, Kroeger P, etal. Performance of a multiplex qualitative PCR LCx assay for detectionof human immunodeficiency virus type 1 (HIV-1) group M subtypes,group O, and HIV-2. J Clin Microbiol 2000;38(2):716–23.
2003;26(2):163–9.[411] Triques K, Coste J, Perret JL, Segarra C, Mpoudi E, Reynes J, et
al. Efficiencies of four versions of the AMPLICOR HIV-1 MONITORtest for quantification of different subtypes of human immunodeficiencyvirus type 1. J Clin Microbiol 1999;37(1):110–6.
[412] Antunes R, Figueiredo S, Bartolo I, Pinheiro M, Rosado L, Soares I, etal. Evaluation of the clinical sensitivities of three viral load assays withplasma samples from a pediatric population predominantly infected
[420] Zanchetta N, Nardi G, Tocalli L, Drago L, Bossi C, Pulvirenti FR, etal. Evaluation of the abbott LCx HIV-1 RNA quantitative, a new assayfor quantitative determination of human immunodeficiency virus type1 RNA. J Clin Microbiol 2000;38(10):3882–6.
[421] Katsoulidou A, Papachristou E, Petrodaskalaki M, Sypsa V, Anastas-sopoulou CG, Gargalianos P, et al. Comparison of three current viralload assays for the quantitation of human immunodeficiency virus type1 RNA in plasma. J Virol Methods 2004;121(1):93–9.