Embed Size (px)
Citation preview
Annals of Otolofiy. Rhinology & Larynfiolo^y I2O( I ) : I -8 .© 2011 Annals Publishing Company. All rights reserved.
Laryngeal Features of External Superior Laryngeal NerveDenervation: Revisiting a Century-Old Controversy
Nelson Roy, PhD; Marshall E. Smith, MD; Daniel R. Houtz, MA
A iong-standing controversy exists regarding the iaryngoscopic features associated with unilateral denervation of the ex-ternal superior laryngeal nerve (ESLN). Recently, we modeled acute unilateral cricothyroid muscle paralysis by block-ing the ipsilateral ESLN with lidocaine hydrochloride, and identified epiglottic petiole deviation to the side of paralysisduring high-pitched voice production as a possible diagnostic sign. This study provides preliminary clinical evidencesupporting the presence of petiole deviation in cases of ESLN denervation. Epiglottic petiole deviation to the side ofweakness was present in electromyographically confirmed cases of unilateral partial or complete ESLN denervation, inisolation or in combination with denervation of other branches of the vagus nerve, hi addition, a ca.se of complete ESLNand recurrent laryngeal nerve (RLN) denervation showed return of the petiole to the midline 6 months after surgical rein-nervation of the ESLN and RLN. Finally, petiole deviation was not present in isolated RLN paralysis — a finding sug-gesting that the diagnostic sign is uniquely associated with ESLN denervation. We concluded that deviation of the petioleto the side of cricothyroid muscle weakness during high-pitched voice production represents a potential diagnostic signof unilateral ESLN denervation. Further research is necessary to determine factors that influence the expression and de-teetion of this sign, as well as its diagnostic precision.
Key Words: denervation, epiglottic petiole deviation, superior laryngeal nerve.
INTRODUCTION
The external branch of the superior laryngealnerve (SLN) innervates the cricothyroid (CT) mus-cle, which is divided into 3 distinct bellies or com-partments, including the pars oblique, the pars rec-ta, and a tnore recently discovered horizontal bel-ly.' The CT muscle contributes to control of vocalfundamental frequency (Fo) and its psychophysicalcorrelate "vocal pitch."^f" Although the CT muscleundoubtedly contributes to vocal fold lengthening— the primary geometric variable for adjustmentsof Fo^ — its effects on voice seem to extend well be-yond the Fo. For instance, in clinical circles, unilat-eral CT muscle dysfunction due to injury of the ex-ternal branch of the SLN (ESLN) allegedly produc-es a wide range of voice and laryngeal effects.^"'"However, their exact nature and degree, as well asthe tasks that seemingly provoke these phonatoryand laryngeal changes, are not well documented orunderstood, and have been the source of consider-able debate."
For more than a century, a controversy has existedregarding the laryngeal signs that are presumed to bepathognomonic for unilateral ESLN paralysis. Al-
though myriad descriptions exist of laryngeal behav-iors ostensibly associated with unilateral ESLN den-ervation, no consensus has emerged since Mygind'^in 1906 first reported that the glottis was obliqueduring phonation in patients with unilateral ESLNparalysis. Indeed, most early descriptions involvedrotation of the larynx, presumably due to asymmet-ric CT muscle dysfunction. This classic view heldthat ESLN denervation caused the weakened ipsilat-eral vocal fold to be shortened and to be at a lowerlevel, while the anterior larynx shifted to the sideof the intact CT muscle, creating an oblique glottiswith the posterior larynx rotated toward the weak-ened side.'^'-^''* However, as Abelson and Tucker'-''reported nearly 30 years ago, there was considei abledisagreement and controversy surrounding this view.For instance, although some authorities confirmedthat the anterior commissure rotated to the paralyzedside,'^ other experts asserted that the posterior lar-ynx rotated as well, but there was no consensus asto which side.'^ Still others failed to consistentlyfind an oblique glottis."* In an attempt to resolve thecontroversy, Abelson and Tucker'** used local anes-thetic to temporarily paralyze the ESLN in 4 vol-unteers. Laryngoscopy during the block showed a
From the Department of Communication Sciences and Disorders (Roy), the Division of Otolaryngology-Head and Neck Surgery(Smith), and the Voice Disorders Center (Houtz), University of Utah, Salt Lake City. Utah.
Presented in part at the Voiee Foundation's 39th Annual Symposium: Care of the Professional Voice, Philadelphia, Pennsylvania, June2-6.2010.
Correspondence: Nelson Roy, PhD, Dept of Communication Sciences and Disorders, University of Utah, 390 South 1530 East, Room1219. Salt Lake City, UT X4112-0252.
1
Roy et al, Laryn^eal Features of External Superior Laryn^eat Nerve Denervation
symmetric larynx at rest, but during phonation theposterior commissure pulled toward the side of tem-porary paralysis. Also, the affected vocal fold wasslightly bowed and appeared shorter, Abelson andTucker'-^ concluded that ESLN paralysis in humanscan be suspected when "an oblique glottic chink isobserved during phonatory efforts. Such a finding iscaused by rotation of the posterior commissure to-wards the side of paralysis. The aryepiglottic fold onthe side of paralysis is shortened, and the aryepiglot-tic fold on the opposite side is lengthened,"'''•P'*^*^*Later, Tanaka et al'^ confirmed that 9 of 12 patientswith SLN paralysis clearly showed rotation of theposterior glottis to the paralyzed side, primarily dur-ing pitch elevation.
Although the experiment of Abelson and Tuck-er,'-̂ combined with the clinical report of Tanaka etal,'*^ seemed to briefly quiet the controversy, morerecent findings have seriously questioned the valueof larynx rotation as a salient laryngoscopic sign ofESLN paralysis. Several researchers have identifieda number of additional laryngostroboscopic charac-teristics that seemingly occur more frequently. Forinstance, in a population of 126 patients with SLNparesis and paralysis, Dursun et al'' reported vocalfold lag, asymmetry, and height disparity (scissor-ing) as the most distinct findings of SLN dysfunc-tion, as well as decreased amplitude and mucosalwave of the affected fold. Interestingly, however,Dursun et al"̂ did not identify larynx rotation as a sa-lient feature of SLN paralysis. More recent studieshave also failed to identify larynx rotation as a keyfeature of SLN injury. Rather, sluggishness of theipsilateral vocal fold during repetitive adduction andabduction tasks and decreased longitudinal tensionhave been offered as the sine qua non of SLN injury.For example. Eckley et al-" reported on a group of56 adults with SLN paresis or paralysis diagnosedfrom laryngeal electromyographic (LEMG) find-ings. The authors described 3 severity levels of pa-resis with associated laryngeal findings. Mild SLNdenervation showed a slight sluggishness of the vo-cal fold on the weakened side and usually a milddeficit in the ability to increase longitudinal tensionduring pitch elevation. In moderate SLN denerva-tion, the sluggishness and deficit in pitch elevationwere obvious, and severe SLN denervation mani-fested as almost no motion of the CT muscle on theaffected side, but with tone still present. There wasno reporting of rotation of the larynx as a distinctfeature of SLN paresis or paralysis, however.
Like Eckley et al ,2" Heman-Ackah and Batory^'emphasized sluggishness of the affected vocal foldas evidence of SLN injury. The authors declared thatif the integrity of the CT and cricoarytenoid joints is
shown to be normal, hypomobility in the distributionof the SLN is manifested by sluggishness in adduc-tion and longitudinal tension, observed especiallyduring rapid repetition of "ee" and "hee" (ie, repeti-tive phonatory tasks [RPTs|), Rubin et aF^ echoedthe claims of Heman-Ackah and Batory^' that vo-cal fold lag (sluggishness), especially during fatigu-ing RPTs, was a hallmark of SLN injury, explainingthat paretic nerves fatigue more quickly than nor-mal nerves, Rubin et al warned that SLN paresiscan be misinterpreted as recurrent laryngeal nerve(RLN) paresis, because "vocal fold lag from SLNparesis can present as sluggish abduction as well asadduction ,"22(pf'Xi) They argued that RPTs were use-ful diagnostic tasks for identifying SLN paresis.
In an apparent reversal, however, Heman-Ackahand Barr"' later stated that in cases in which mildhypomobility is observed on physical examination,"no muscle pattern of hypomobility can identify theparetic nerve or nerves accurately,"'"*i'-^^' This re-treat from their previous conclusions presumably re-flects the authors' attempts to explain their finding ofpoor agreement between the actual LEMG evidence,which identified which side of the larynx was af-fected and/or which nerves (ie, RLN, SLN, or both)were affected on that side, and the clinician reportsof the sidedness of hypomobility observed duringlaryngoscopy. According to the authors, there wasfrequent disagreement between the LEMG findingsand the laterality of the hypomobility observed clin-ically. In an attempt to explain the poor agreementobserved between physical examination and LEMGdata, Heman-Ackah and Barr"* suggested that com-pensation for weakness may explain the disparateresults. They reasoned that "paresis of the laryngealnerves results in asymmetrical muscle forces in thelarynx, and depending upon the relative compensa-tion from the unaffected muscles and the degree ofpull from the affected muscle, the pattern of hypo-mobility observed may not necessarily coincide withtheexpected mobility pattern,"""p2'''^'Therefore,thisfinding not only cast doubt on the diagnostic preci-sion of vocal fold lag as a reliable marker of SLNinjury, but it raised the possibility that asymmetriesobserved in the larynx may actually reflect second-ary attempts to compensate for unilateral weakness,rather than the pure effects of the primary disorder(ie, SLN denervation). To date, no studies have ex-amined clinical manifestations of acute SLN injuryto determine whether some of the heterogeneity inthe reported findings may reflect merely individualdifferences in compensatory adjustments or the spe-cific vocal tasks used to evaluate patients.
In an attempt to shed light on this controversy,Roy et aP^ selectively blocked the ESLN using li-
Roy et al. Laryngeal Feature.^ of External Superior Laryngeal Nerve Denervation
docaine hydrochloride in order to identify the sa-lient laryngeal features associated with acute, uni-lateral CT muscle dysfunction. Ten vocally normalmen underwent lidocaine block of the right ESLNwith LEMG verification. Flexible videolaryngostro-boscopic recordings of participants performing awide variety of vocal tasks were acquired beforeand during the block. Eleven blinded, expert judgesrated randomized recordings from before and dur-ing the block of 10 vocal tasks using standardizedflexible videolaryngostroboscopic rating protocols.Contrary to clinical reports, the investigators report-ed no evidence of hypomobility or sluggishness ofthe ipsilateral vocal fold, nor a consistent pattern ofaxial rotation of the larynx. Instead, the analysis re-vealed deviation of the petiole of the epiglottis tothe side of CT muscle weakness in 60% of partic-ipants during an upward glissando maneuver pro-duced at normal volume. This finding had not beenreported previously as a manifestation of unilateralCT muscle paralysis. Several questions remained,however, regarding the validity of using lidocaine-induced paralysis to model selective ESLN damageonly. One limitation of the model involved the pos-sibility that lidocaine may have diffused into and/orinfiltrated surrounding ipsilateral extrinsic laryngealmuscles (ie, sternothyroid, stemohyoid, thyrohyoid)or nerves. Thus, by extension, epiglottic deviationmight have reflected the cumulative effects of ESLNdysfunction, as well as any regional extrinsic mus-cle dysfunction. A second limitation of lidocaine-induced paralysis is that it may not have replicatedthe mechanism of injury and repair seen clinically inthe postacute and chronic stages of neural recovery.There may be functional differences between lido-caine-induced CT muscle paralysis and what occursclinically when the nerve is damaged via trauma (ie,nerve sectioning, stretching, or compression) or, al-ternatively, via infectious processes, especially dur-ing the postacute recovery phase. Finally, the lido-caine-induced CT muscle paralysis model attempt-ed to simulate the effects oí acute paralysis, and itis possible that such a model differs substantiallyfrom what would be observed clinically in cases ofchronic denervation, wherein adaptive or maladap-tive compensatory muscle activation patterns canexist. Thus, Roy et al--̂ cautioned that clinical stud-ies were necessary to evaluate the presence of epi-glottic petiole deviation not only as a possible diag-nostic marker of acute, complete, unilateral ESLNdenervation, but also in cases of chronic partial orcomplete denervation, and/or in combination withother neuropathies, including those of the RLN.
In this regard, our report presents evidence fromseveral clinical cases that illustrate epiglottic peti-
ole deviation to the side of weakness (during high-pitched voice production) in the presence of con-firmed ESLN denervation. Clinical cases are pre-sented to illustrate either isolated unilateral partialor complete ESLN denervation, or denervation ofthe ESLN in combination with the other branchesof the vagus nerve. In addition, a case of completeRLN and ESLN denervation is presented that showsa return of the petiole to the midline 6 months af-ter surgical reinnervation of the ipsilateral ESLNand RLN. Finally, a case of isolated RLN paralysisis presented to suggest that petiole deviation is notnecessarily a consequence of ö«y asymmetric intrin-sic laryngeal muscle forces, but rather, seems to beuniquely associated with ESLN involvement. Thesecases of chronic partial or complete ESLN denerva-tion at various stages of reinnervation seem to pro-vide preliminary support for the finding of epiglotticpetiole deviation derived from the lidocaine-inducedmodel of acute CT muscle paralysis.
CASE REPORTSCase 1 : Right ESLN Paresis. A 7()-year-old man
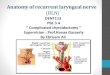
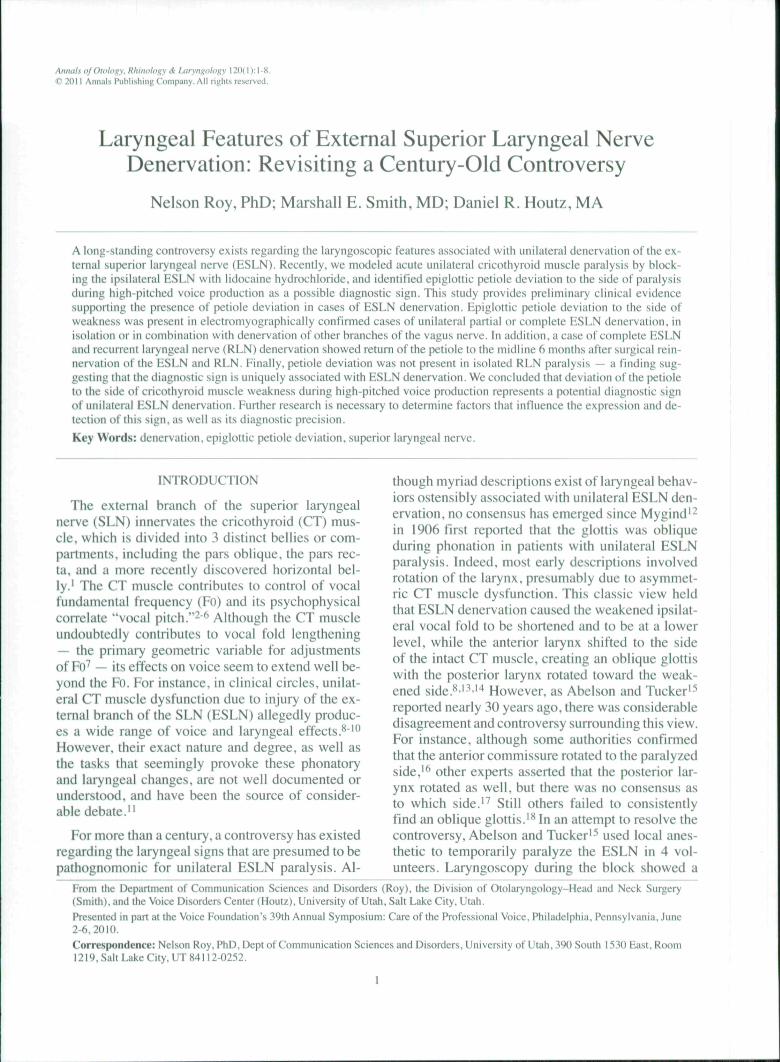
reported an 8-month history of voice difficulties fol-lowing right transcervical removal of a C4-5 verte-bral schwannoma. The patient's Voice Handicap In-dex (VHI) score was 35, indicating a mildly handi-capping voice disturbance. He also self-assessed hisvoice problem as mild. He presented with a mild tomoderate dysphonia, and his voice was rated by alaryngologist and a speech-language pathologistas G2 R2 BI Al SI on the GRBAS scale (grade,roughness, breathiness, asthenia, and strain). Duringflexible laryngoscopy, the vocal folds initially ab-ducted and adducted normally. However, after RPTsdesigned to fatigue the laryngeal mechanism (rapidrepetition of the syllable "hee" for approximately 15seconds), the right vocal fold began to lag during ab-duction, with slightly reduced mobility as comparedto the left. During vocal fold abduction, the petiolewas also observed to remain in the midline (Fig I A).During stroboscopy, phonation produced at normalpitch and loudness was associated with only touchclosure of the true vocal folds, with the open phasedominating the vibratory cycle. The petiole was ob-served to be in the midline (Fig 1B); however, therewas no evidence of a reduced mucosal wave, re-duced amplitude of vibration, or phase asymmetry.During phonation elicited at highest pitch and dur-ing upward glissando, there was obvious deviationof the petiole of the epiglottis to the right side (FiglC). After clinical examination, the patient under-went LEMG. Concentric-needle LEMG of the CTand thyroarytenoid (TA) muscles revealed normalelectrodiagnostic findings for the right TA muscle.However, there was electrodiagnostic evidence of
Roy et al. Laryngeal Features ofE.xternal Superior Laryngeal Nerve Denervation
Fig 1. (Case 1) Paresis of external branch of superior laryngeal nerve (ESLN) on right side. A) During vocal fold abduction,petiole is in midline. B) During phonation produced at normal pitch and loudness. petiole remains in midline. C) During phona-tion elicited at highest pitch during upward glissando maneuver, epiglottic petiole deviates to right side (arrow).
reduced recruitment and complex-appearing motorunits in the right CT muscle, indicating denervationand partial reinnervation consistent with axonal in-jury to the right SLN only. This finding not only pro-vides support for petiole deviation as a marker ofisolated ESLN denervation, but provides some evi-dence to support the contention of Rubin et aP-^ thatvocal fold lag during fatiguing RPTs may reflectSLN denervation.
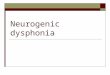
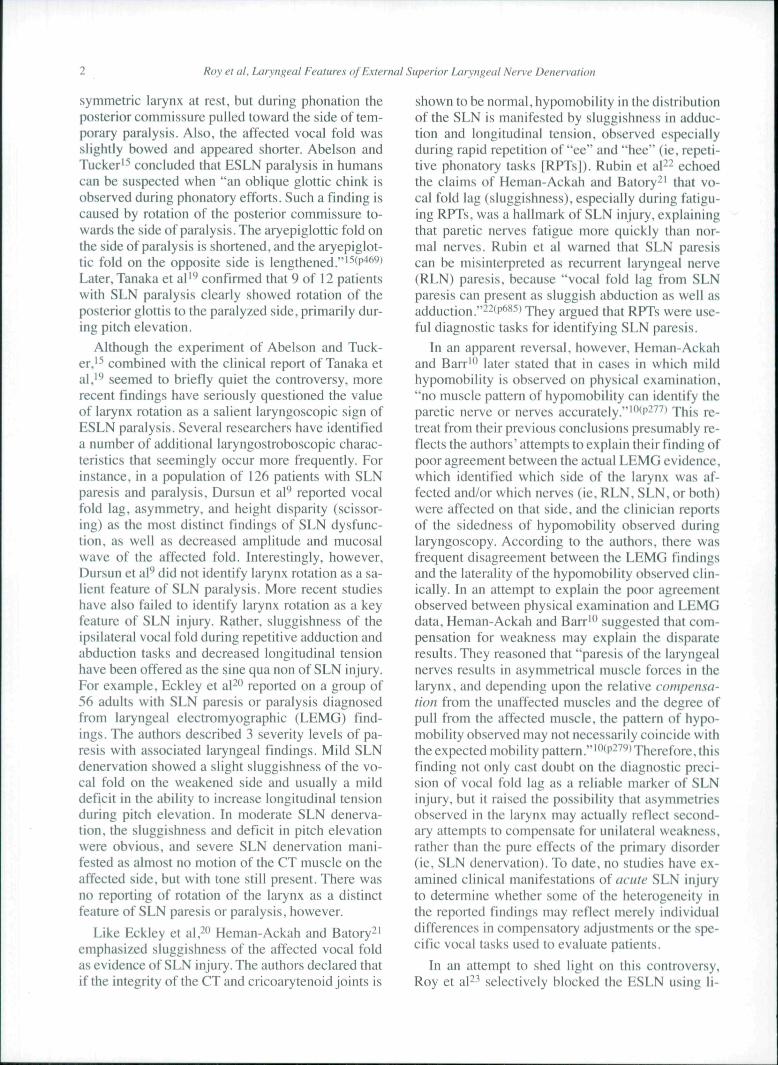
Case 2: Right ESLN and RLN Paresis. A 40-year-old man reported a 4-month history of globus sensa-tion, vocal fatigue, and increased physical effort as-sociated with voice production, especially after ex-tended voice use. The patient reported a VHI scoreof 16. indicating a mildly handicapping voice disor-der. He self-assessed his voice disturbance as mild.At the time of examination, his voice was judgedby both a laryngologist and a speech-language pa-thologist to be perceptually normal (ie, GO RO BOAO SO). Videolaryngostroboscopy showed a normalrange and speed of abductory and adductory move-ments of the vocal folds. During abduction, the peti-
ole was positioned in the midline, and there weretwo small vocal process granulomas (right greaterthan left; Fig 2A). During phonation at nonnal pitchand loudness, the right arytenoid cartilage hood-ed over the right vocal fold, with scissoring of thearytenoid cartilages. The petiole remained in a cen-tral position (Fig 2B). Vibratory characteristics werejudged to be within normal limits. During pitch ex-cursion into the uppermost region of the pitch rangeduring upward glissando, the petiole of the epiglot-tis was observed to deviate substantially to the right(Fig 2C). Concentric-needle LEMG completed afterthe clinical examination showed no abnormal spon-taneous activity, but showed increased complexityand amplitude of fast-firing motor units in the rightTA muscle and right CT muscle consistent with pre-vious injury to the right RLN and SLN with subse-quent partial reinnervation.
Case 3: Brain Stem Arteriovenous Malforma-tions and High Lefi Vagal Injury. The patient wasan 18-year-old man with a history of arteriovenousmalformations of the brain stem beginning at 2 years
m
\Fig 2. (Case 2) Paresis of ESLN and lecunent laryngeal nerve (RLN) on right side. A) During vocal fold abduction, petiole is inmidline. B) During phonation produced at normal pitch and loudness, petiole remains in midline. C) During phonation elicitedat highest pitch, epiglottic petiole deviates to right side (arrow).
Rov et at, Laryngeal Features of External Superior Laryngeal Nerve Denervation
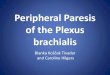
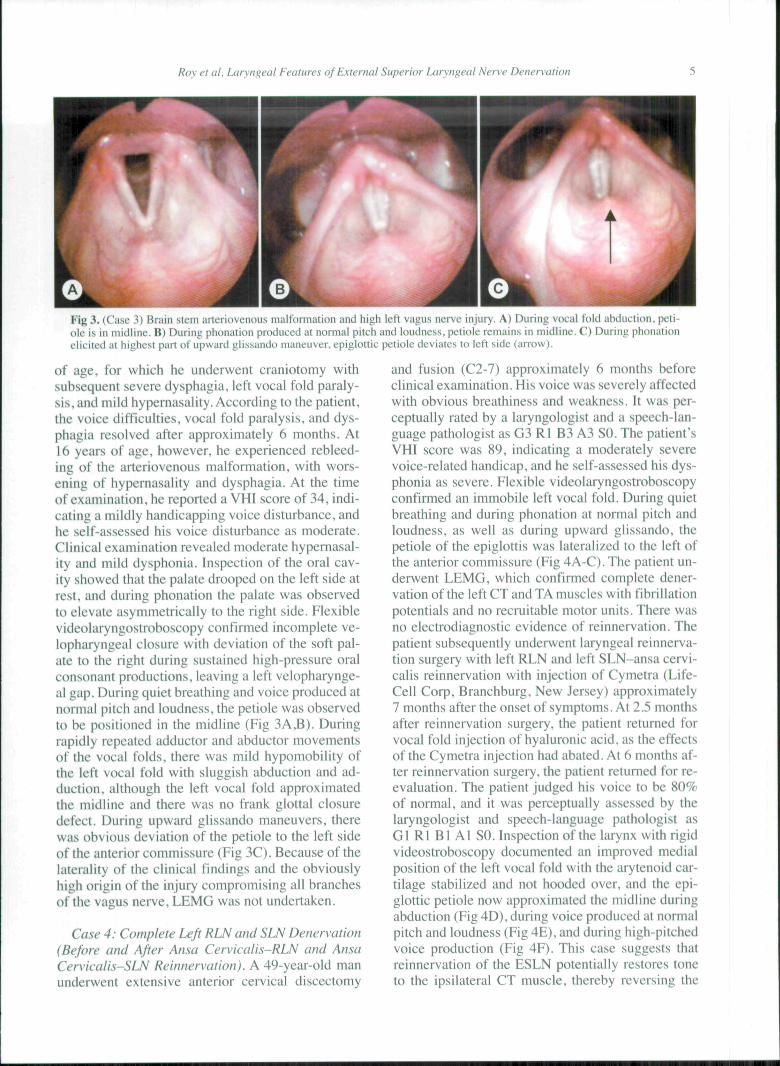
Fig 3. (Case 3) Brain stem arteriovenous malfonnation and high left vagus nerve injury. A) During vocal told abduction, peti-ole is in midline. B) During phonation produced at normal pitch and loudness, petiole remains in midline. C) During phonationelicited at highest part of upward glissando maneuver, epiglottic petiole deviates to left side (arrow).
of age, for which he underwent craniotomy withsubsequent severe dysphagia, left vocal fold paraly-sis, and mild hypernasality. According to the patient,the voice difficulties, vocal fold paralysis, and dys-phagia resolved after approximately 6 months. At16 years of age, however, he experienced rebleed-ing of the arteriovenous malformation, with wors-ening of hypernasality and dysphagia. At the timeof examination, he reported a VHI score of 34, indi-cating a mildly handicapping voice disturbance, andhe self-assessed his voice disturbance as moderate.Clinical examination revealed moderate hypernasal-ity and mild dysphonia. Inspection of the oral cav-ity showed that the palate drooped on the left side atrest, and during phonation the palate was observedto elevate asymmetrically to the right side. Flexiblevideolaryngostroboscopy confirmed incomplete ve-lopharyngeal closure with deviation of the soft pal-ate to the right during sustained high-pressure oralconsonant productions, leaving a left velopharynge-al gap. During quiet breathing and voice produced atnormal pitch and loudness, the petiole was observedto be positioned in the midline (Fig 3A,B). Duringrapidly repeated adductor and abductor movementsof the vocal folds, there was mild hypomobility ofthe left vocal fold with sluggish abduction and ad-duction, although the left vocal fold approximatedthe tnidline and there was no frank glottal closuredefect. During upward glissando maneuvers, therewas obvious deviation of the petiole to the left sideof the anterior commissure (Fig 3C). Because of thelaterality of the clinical findings and the obviouslyhigh origin of the injury compromising all branchesof the vagus nerve, LEMG was not undertaken.
Case 4: Complete Left RLN and SLN Denervation(Before and After Ansa Cervicalis-RLN and AnsaCervicalis-SLN Reinnervation). A 49-year-old manunderwent extensive anterior cervical discectomy
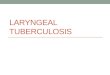
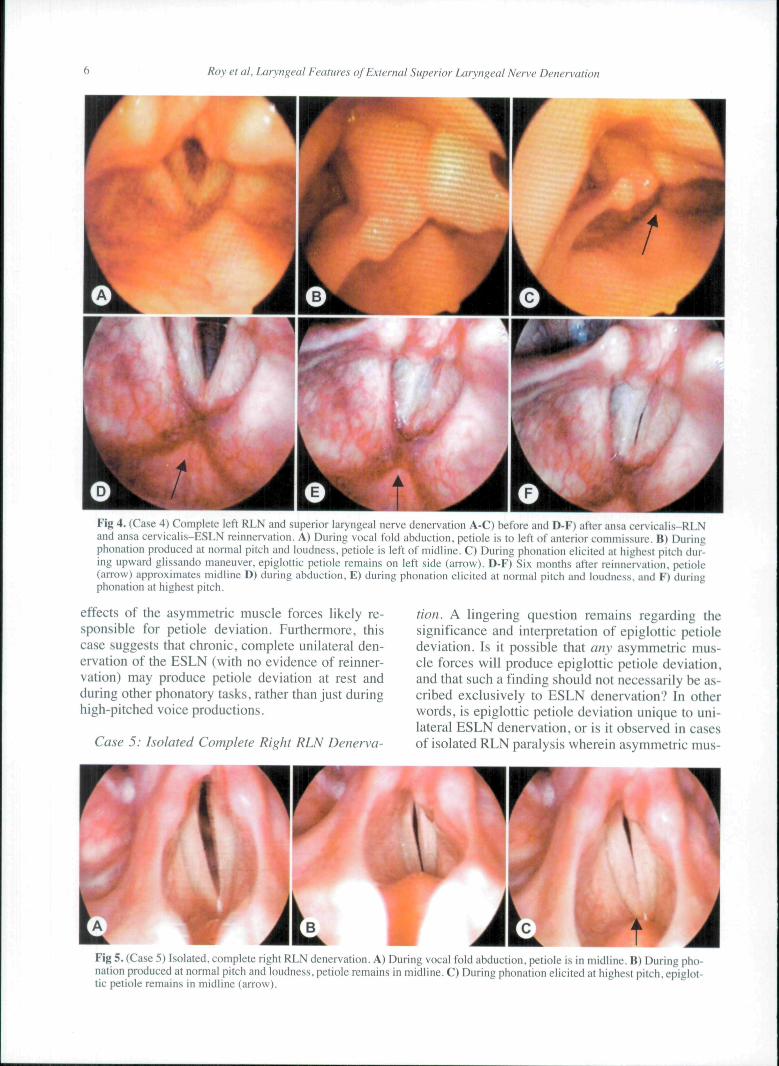
and fusion (C2-7) approximately 6 months beforeclinical examination. His voice was severely affectedwith obvious breathiness and weakness. It was per-ceptually rated by a laryngologist and a speech-lan-guage pathologist as G3 Rl B3 A3 SO. The patient'sVHI score was 89, indicating a rnoderately severevoice-related handicap, and he self-assessed his dys-phonia as severe. Flexible videolaryngostroboscopyconfirmed an immobile left vocal fold. During quietbreathing and during phonation at normal pitch andloudness, as well as during upward glissando, thepetiole of the epiglottis was lateralized to the left ofthe anterior commissure (Fig 4A-C). The patient un-derwent LEMG, which conflrmed complete dener-vation of the left CT and TA muscles with fibrillationpotentials and no recruitable motor units. There wasno electrodiagnostic evidence of reinnervation. Thepatient subsequently underwent laryngeal reinnerva-tion surgery with left RLN and left SLN-ansa cervi-calis reinnervation with injection of Cymetra (Life-Cell Corp, Branchburg, New Jersey) approximately7 months after the onset of symptoms. At 2.5 monthsafter reinnervation surgery, the patient returned forvocal fold injection of hyaluronic acid, as the effectsof the Cymetra injection had abated. At 6 months af-ter reinnervation surgery, the patient returned for re-evaluation. The patient judged his voice to be 80%of normal, and it was perceptually assessed by thelaryngologist and speech-language pathologist asGl Rl Bl Al SO. Inspection of the larynx with rigidvideostroboscopy documented an improved medialposition of the left vocal fold with the arytenoid car-tilage stabilized and not hooded over, and the epi-glottic petiole now approximated the midline duringabduction (Fig 4D), during voice produced at normalpitch and loudness (Fig 4E), and during high-pitchedvoice production (Fig 4F). This case suggests thatreinnervation of the ESLN potentially restores toneto the ipsilateral CT muscle, thereby reversing the
Roy et al, Laryngeal Features of External Superior Laryngeal Nerve Denervation
f
Fig 4. (Case 4) Complete left RLN and superior laryngeal nerve denervation A-C) before and D-F) after ansa cervicalis-RLNand ansa cervicalis-ESLN reinnervation. A) During vocal fold abduction, petiole is to left of anterior commissure. B) Duringphonation produced at normal pitch and loudness, petiole is left of midline. C) During phonation elicited at highest pitch dur-ing upward glissando maneuver, epiglottic petiole remains on left side (arrow). D-F) Six months after reinnervation, petiole(arrow) approximates midline D) during abduction, E) during phonation elicited at normal pitch and loudness, and F) duringphonation at highest pitch.
effects of the asymmetric muscle forces likely re-sponsible for petiole deviation. Furthermore, thiscase suggests that chronic, complete unilateral den-ervation of the ESLN (with no evidence of reinner-vation) may produce petiole deviation at rest andduring other phonatory tasks, rather than just duringhigh-pitched voice productions.
Case 5: Isolated Complete Right RLN Denerva-
tion. A lingering question remains regarding thesignificance and interpretation of epiglottic petioledeviation. Is it possible that any asymmetric mus-cle forces will produce epiglottic petiole deviation,and that such a finding should not necessarily be as-cribed exclusively to ESLN denervation? In otherwords, is epiglottic petiole deviation unique to uni-lateral ESLN denervation, or is it observed in casesof isolated RLN paralysis wherein asymmetric mus-
Fig 5, (Case 5) Isolated, complete right RLN denervation. A) During vocal fold abduction, petiole is in niidliiic. B) During pho-nation produced at normal pitch and loudness, petiole remains in midline. C) During phonation elicited at highest pitch, epiglot-tic petiole remains in midline (arrow).

Roy et al, Laryngeal Features of External Superior Laryngeat Nerve Denervation
de forces also exist? To explore this question, welooked at a case of isolated unilateral RLN dener-vation. The patient was a 40-year-old man who re-ported altered voice quality following a right ante-rior approach cervical laminectomy for C7 radicu-lopathy approximately 1 year earlier. On examina-tion, the voice was breathy and of decreased vol-ume. Concentric-needle LEMG of the right TA andCT inuscles was completed. The right TA muscleshowed profuse abnormal spontaneous activity butno recruitable motor units. The CT muscle motorunits appeared normal. There was electrodiagnos-tic evidence of complete denervation of the right TAmuscle consistent with right RLN denervation. Thefunction of the right SLN was considered normal.During videostroboscopy the petiole was observedto be positioned in the midline across all tasks, in-cluding quiet breathing (Fig 5A), voice produced atnormal pitch and loudness (Fig 5B), and voice pro-duced during highest pitch (Fig 5C), This case pro-vides preliminary evidence that epiglottic petioledeviation, if present, appears to be uniquely associ-ated with asymmetric CT muscle dysfunction, ratherthan general asymmetric muscle forces within thelarynx,
CONCLUSIONSThese clinical cases of chronic partial or com-
plete ESLN denervation, at various stages of rein-nervation, seem to provide preliminary support forthe findings derived from the lidocaine-induced
model oí acute CT paralysis, Epiglottic petiole de-viation to the side of CT muscle weakness duringhigh-pitched voice production represents a poten-tially valuable diagnostic sign of unilateral ESLNdenervation. However, further research is necessaryto establish the diagnostic precision of this sign, aswell as the factors that influence sign detection andexpression. Larger clinical studies are needed to de-termine whether petiole deviation routinely occursin vocally normal individuals, in those with isolatedRLN paralysis, and/or in those with other types ofvoice disorders not associated with ESLN or RLNdenervation. In addition, factors that may potential-ly influence the presence, detection, and interpreta-tion of this laryngoscopic sign or feature need to bebetter understood. For instance, anatomic variation(prominent versus fiat petiole), camera angle, flex-ible versus rigid endoscopy, the patient's ability ortalent in performing upward glissando, the degree ofpetiole deviation, the mobility of the CT joint, andthe presence and amount of supraglottic compres-sion are a few factors that may influence the degreeof petiole deviation, and the examiner's ability toaccurately detect and interpret it. In summary, rigor-ous evaluation of diagnostic test performance (us-ing conventional estimates of sensitivity, specificity,and positive and negative likelihood ratios) is criti-cal to establishing the diagnostic worth of epiglotticpetiole deviation as a potential marker of unilateralESLN denervation.
REFERENCES
1, Mu L. Sanders I, The human cricothyroid muscle: threemuscle bellies and their innervation patterns, J Voice 2009;23:21-8,
2, Atkinson JE, Correlation analysis of the physiologicalfactors controlling fundamental voice frequency, J Acoust SocAm 1978;63:211-22,
3, Faaborg-AndersenK, Electromyographic investigation ofintrinsic muscles in human. Acta Physiol Scand 1957;41:140,
4, Gay T.Hirose H,Strome M.Savvashima M. Electromyog-raphy of the intrinsic laryngeal muscles during phonation, AnnOtol Rhinol Laryngol l972;81:4()l-9,
5, Hirano M, Ohala J, Vennard W. The function of laryngealmu,scles in regulating fundamental frequency and intensity ofphonation, J Speech Hear Res l969:l2;6l6-28.
6, Hong KH, Ye M, Kim YM, Kevorkian KP. Kreiman J,Berke GS, Functional differences between the two bellies of thecricothyroid muscle, Otolaryngol Head Neck Surg 1998;118:714-22,
7, Titze I, Principles of voice production, Englewood Cliffs,NJ; Prentice-Hall, 1994,
8, Adour KK. Schneider GD. Hilsinger RL Jr, Acute superi-or laryngeal nerve palsy: analysis of 78 cases, Otolaryngol HeadNeck Surg 1980:88:418-24,
9, Dursun G, Sataloff RT, Spiegel JR, Mandel S, Heuer RJ,Rosen DC. Superior laryngeal nerve paresis and paralysis, J
Voice 1996;10:206-ll,
10, Heman-Ackah YD, Barr A, Mild vocal fold paresis: un-derstanding clinical presentation and electromyographic find-ings, J Voice 2006;20:269-81.
11, Sulica L, The superior laryngeal nerve: function and dys-function, Otolaryngol Clin North Am 2(X)4;37:183-201,
12, Mygind H, Die Paralyse des M. Cricothyreoideus, ArchLaryngol 1906:18:403-18,
13, Faaborg-Andersen K, Jensen AM, Unilateral paralysis ofthe superior laryngeal nerve. Acta Otolaryngol 1964:57:155-9,
14, Ward PH, Berci G, Calcaterra TC, Superior laryngealnerve paralysis: an often overlooked entity. Trans Sect Otolar-yngol Am Acad Ophthalmol Otolaryngol 1977:84:78-89,
15, Abelson TI, Tucker HM, Laryngeal findings in superi-or laryngeal nerve paralysis: a controversy, Otolaryngol HeadNeck Surg 1981:89:463-70.
16, New GB,Childrey JH, Paralysis of the superior laryngealnerve associated with arteriosclerosis of the central nervous sys-tem. Arch Otolaryngol 1930:11:752-4.
17, Arnold GF, Physiology and pathology of the cricothyroidmuscle. Laryngoscope 1961:1:687-753,
18, Dedo HH, The paralyzed larynx: an electromyographicstudy in dogs and humans. Laryngoscope 1970:80:1455-517,
19, Tanaka S, Hirano M, Umeno H, Laryngeal behavior in
8 Roy et al, Laryngeal Features of External Superior Laryngeal Nerve Denervation
unilateral superior laryngeal nerve paralysis. Ann Otol RhinolLaryngol 1994; 103:93-7.
20. Eckley CA, Sataloff RT, Hawkshaw M, Spiegel JR, Man-del S. Voice range in superior laryngeal nerve paresis and pa-ralysis. J Voice 1998;12:340-8.
21. Heman-Ackah YD, Batory M. Determining the etiologyof mild vocal fold hypomobility. J Voice 2003; 17:579-88.
22. Rubin AD. Praneetvatakul V, Heman-Ackah YD. MoyerCA, Mandel S. Sataloff RT. Repetitive phonatory tasks for iden-tifying vocal fold paresis. J Voice 2005;19:679-86.
23. Roy N, Barton ME. Smith ME. Dromey C. Merrill RM,SauderC.An in vivo model of external superior laryngeal nerveparalysis: laryngoscopic findings. Laryngoscope 2009; 119:1017-32.
Prtop«retlv* EmboiizJtIon In Carotid Body Tumor SurB'fyOanitt M. Z*««tr. MO: Jo*»« GHck; Oady Hir-Ei. MO
Extraiumlnal Ptrforstlon Comphcatlng Foreign Bodies In the Upper Aerodlgaatlva TractKhaitd Ai-S»twih. MO, FRCSC; Khairy<Aihag Abu-Shara. MO: Amro Sobain. MO
Endoscopie Managamtnt of Airway Venous Matformatlons With Nd:YAG LasarRobttt Glad*. MO: Kimbarly Vtnson. MO: Gresham Richter. MO: James Y Suen. MO: Liu M.Buchmllt*r. MO
Risk Factors for Haartng Loss Aftar Padlatrtc ManlngKls In JapanNodoka Adachi. MO: K*n to. MD: HidaaW Sakaia. MO
GOONLIN
12YEARS
OFISSUES
Ann als xom
Copyright of Annals of Otology, Rhinology & Laryngology is the property of Annals Publishing Company and
its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.