Embed Size (px)
Citation preview

DOI: 10.1378/chest.118.6.1582 2000;118;1582-1590 Chest
Valle Velasco and Francisco Santolaria Ciro Casanova, Bartolome R. Celli, Lina Tost, Estanislao Soriano, Juan Abreu,
Patients With Severe COPDLong-term Controlled Trial of Nocturnal Nasal Positive Pressure Ventilation in
This information is current as of November 22, 2006
http://www.chestjournal.org/cgi/content/full/118/6/1582located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 0012-3692. may be reproduced or distributed without the prior written permission of the copyright holder. 3300 Dundee Road, Northbrook IL 60062. All rights reserved. No part of this article or PDFpublished monthly since 1935. Copyright 2005 by the American College of Chest Physicians, CHEST is the official journal of the American College of Chest Physicians. It has been
by on November 22, 2006 www.chestjournal.orgDownloaded from

Long-term Controlled Trial of NocturnalNasal Positive Pressure Ventilation inPatients With Severe COPD*
Ciro Casanova, MD; Bartolome R. Celli, MD, FCCP; Lina Tost, MD;Estanislao Soriano, MD; Juan Abreu, MD; Valle Velasco, MD; andFrancisco Santolaria, MD
Study objectives: To determine the 1-year efficacy of noninvasive positive pressure ventilation(NPPV) added to long-term oxygen therapy (LTOT) in patients with stable severe COPD.Patient selection and methods: We prospectively randomized 52 patients with severe COPD (FEV1< 45%) to either NPPV plus “standard care” (96% patients with LTOT) or to standard care alone(93% patients with LTOT). The outcomes measured included the following: rate of acute COPDexacerbations; hospital admissions; intubations; and mortality at 3 months, 6 months, and 12months. The patients were also evaluated at 3 months and 6 months for dyspnea using theMedical Research Council and Borg scales, gas exchange, hematocrit, pulmonary function,cardiac function with echocardiogram, and neuropsychological performance.Results: One-year survival was similar in both groups (78%). The number of acute exacerbationswas similar at all time points in patients receiving NPPV, compared with control subjects. Thenumber of hospital admissions was decreased at 3 months in the NPPV group (5% vs 15% ofpatients, p < 0.05), but this difference was not seen at 6 months (18% vs 19%, respectively). Theonly beneficial differences were observed in the Borg dyspnea rating, which dropped from 6 to5 (p < 0.039), and in one of the neuropsychological tests (psychomotor coordination) for theNPPV group at 6 months.Conclusions: Our study indicates that over 1 year, NPPV does not affect the natural course of thedisease and is of marginal benefit in outpatients with severe COPD who are in stable condition.
(CHEST 2000; 118:1582–1590)
Key words: COPD; noninvasive mechanical ventilation; respiratory failure
Abbreviations: EPAP 5 expiratory positive airway pressure; FRC 5 functional residual capacity; IPAP 5 inspiratorypositive airway pressure; LTOT 5 long-term oxygen therapy; MEP 5 maximal expiratory pressure; MIP 5 maximalinspiratory pressure; NPPV 5 noninvasive positive pressure ventilation; OSAS 5 obstructive sleep apnea syndrome;P0.1 5 mouth occlusion pressure; RV 5 residual volume; TLC 5 total lung capacity
T he clinical course of COPD is characterized by ahigh morbidity and mortality despite long-term
oxygen therapy (LTOT).1 Recent alternative thera-pies, including lung transplantation and lung volumereduction surgery, can only be undertaken in a small
number of patients, and there is no demonstration ofimproved long-term survival rate.2,3
Noninvasive positive pressure ventilation (NPPV)administered via a nasal mask has proven useful intreating restrictive extrapulmonary respiratory insuf-ficiency and in many patients with severe COPD andacute respiratory failure.4–6 Theoretically, NPPVcould also be beneficial in patients with severe stableCOPD, through several mechanisms. It could im-prove nocturnal ventilation, decrease the end-expi-ratory lung volume and hence the level of dynamichyperinflation (auto-positive end-expiratory pres-sure), and improve the response of the respiratorycenter to CO2. It could also decrease upper-airwayresistance and improve the quality of sleep. Inaddition, NPPV could improve respiratory musclefunction by resting the respiratory muscles.6–9 How-
*From the Departments of Pulmonary (Drs. Casanova, Soriano,Velasco, and Santolaria), Psychiatry (Dr. Tost), and Cardiology(Dr. Abreu), Hospital La Candelaria, Department of Pulmonaryand Internal Medicine, Hospital Universitario de Canarias,Tenerife, Spain; and Department of Pulmonary and Critical CareMedicine (Dr. Celli), St. Elizabeth’s Medical Center, TuftsUniversity School of Medicine, Boston, MA.Supported in part by a grant from the Spanish RespiratorySociety.Manuscript received November 9, 1999; revision accepted June29, 2000.Correspondence to: Bartolome R. Celli, MD, FCCP, Pulmonaryand Critical Care Division, St. Elizabeth’s Medical Center, 736Cambridge St, Boston, MA 02135; e-mail: [email protected]
1582 Clinical Investigations
by on November 22, 2006 www.chestjournal.orgDownloaded from

ever, the efficacy of this form of therapy in patientswith airflow obstruction who are in stable conditionremains controversial5,6 because the published re-ports, with a small number of patients and with shortfollow-up time, have shown conflicting results.10–13
We therefore completed a prospective random-ized controlled trial to assess the efficacy of noctur-nal NPPV vs conventional standard treatment inpatients with stable severe COPD. We analyzed at 3months and 6 months the effects of NPPV ondyspnea, arterial blood gases, pulmonary function,and neuropsychological, hematologic, and hemody-namic parameters (systemic arterial pressure andpulmonary artery pressure by echocardiography).Furthermore, we followed up the patients at 3months, 6 months, and 12 months to assess theinfluence of NPPV on COPD morbidity (acute ex-acerbations, intubation rate, and hospital admissions)and mortality.
Materials and Methods
Patient Selection
Eighty patients with severe COPD from the pulmonary clinicsof two hospitals in the Canary Islands (Hospital Clinico andHospital Nuestra Senora de La Candelaria, Canary Islands,Spain) were asked to participate in the study, which was approvedby the humans study committee at both institutions. All patientssigned the informed consent and were enrolled between 1995and 1997. The patients were included if they met the followingcriteria: age from 45 to 75 years, smoking history of . 20pack-years, FEV1 , 45% of predicted, FEV1/FVC , 70%, totallung capacity (TLC) $ 80% predicted, and a stable clinical state(no acute exacerbation for 3 months prior to the initiation of thestudy). Patients were excluded if they had the following: a 15%increase in FEV1 after the administration of an inhaled broncho-dilator (n 5 12); refusal to stop smoking (n 5 9); obstructivesleep apnea syndrome (OSAS); index of apneas-hypopneas . 10episodes per hour; n 5 3); other etiologies of chronic airwayobstruction (bronchiectasis and cystic fibrosis; n 5 2); active andimportant coexisting medical conditions, such as left ventricularfailure (n 5 2). The results of arterial blood gas tests were notused as criteria for enrollment.
The 52 patients who met the study criteria were randomized byan independent office into two groups using a table of randomnumbers. Twenty-six patients were maintained on standard treat-ment, and the other 26 patients received nocturnal nasal venti-lation with bilevel positive pressure ventilation added to theirtreatment.
Standard Treatment
The patients were evaluated and followed up at least every 2months in the pulmonary clinic. Bronchodilators were adjusted toachieve optimal symptomatic control. Antibiotics and corticoste-roids were administered during the episodes of acute exacerba-tion. Hospitalizations were advised for patients with the mostsevere episodes. The patients were encouraged to remain active.Forty-nine patients were receiving supplemental oxygen, whichhad been prescribed at the clinics because of resting hypoxemia(Pao2 , 55 mm Hg).
Initial Evaluation
Spirometry was completed with a constant-volume body ple-thysmograph (Materlab; Jaeger, Germany) following the guide-lines of the American Thoracic Society.14 The static pulmonaryvolumes (residual volume [RV], functional residual capacity[FRC], and TLC) were also measured using standard methods.15
The reference values were those of the European Community forSteel and Coal.16 The pulmonary transfer of carbon monoxidewas determined with a single-breath test.17 The maximal inspira-tory pressure (MIP) and maximal expiratory pressure (MEP)were measured at the mouth during a maximal respiratory effortat RV and TLC, respectively.18 Values were compared with theprediction equations of Morales et al11 proposed by the SpanishSociety of Respiratory and Thoracic Surgery.19 We also measuredthe mouth occlusion pressure (P0.1) and the DP0.1/D end-tidalCO2, using the method recommended by Cherniak.20 Arterialblood gas measures at rest were obtained from the radial artery(AVL-945; Graz, Austria) with the patient in the seated positionbetween 1 h and 3 h after having withdrawn oxygen in the controlgroup, or this plus the ventilatory support in the patients assignedto NPPV. Dyspnea was assessed using the Medical ResearchCouncil and modified Borg dyspnea scales.21
At the time of initiation of the study, there were no validatedhealth-related quality-of-life questionnaires in the Spanish lan-guage. Therefore, we chose a group of neuropsychological teststhat have been validated in that language. A psychiatrist blindedto the treatment conducted the tests. The tests assessed a widerange of neurobehavioral functions, including attention andconcentration tests,22 visual memory, verbal memory, associationcapacity and learning capabilities,23 construction praxis (Struband Black test adapted from Pena-Casanova),22 and gestual praxisas described by Luria.24 Standard administration and scoringprocedures were utilized for all neuropsychological measures.
A cardiologist blinded to treatment performed the assessmentof cardiac function. An echocardiographic Doppler study wasperformed from the parasternal projection.25 The pulmonaryarterial pressure was calculated from the gradient of the systolicpressure peak between the right ventricle and the right atriumadded to normal right atrial pressure.26,27
To rule out the coexistence of OSAS, all the patients werescreened with a nocturnal respiratory polysomnography (Apnea-screen Type I; Jaeger). This test continuously recorded oxygensaturation and heart rate by pulse oximetry, oronasal flow bythermistor, body activity, and position. During this study, thepatients maintained their normal oxygen flow. In doubtful cases,a full polysomnogram was completed. Sleep studies were stagedaccording to the Rechtschaffen and Kales method.28 OSAS wasdefined as an apnea-hypopnea index $ 10 episodes per hour. Thepatients included in the study had a mean (6 SD) apnea-hypopnea index of 3 6 1.5 episodes per hour without arousals.
Institution of Mechanical Ventilation
For those patients randomized to NPPV, ventilation wasinitiated as an inpatient and administered via a standard nasalpositive airway pressure mask using a bilevel pressure ventilationsystem (model DP-90; Taema; Antony Cedex, France). Theventilation system used in our study has a highly sensitiveelectrical trigger that senses very small changes in airflow in thenasal mask. The ventilator was set in the spontaneous mode. Wetargeted an expiratory positive airway pressure (EPAP) of 4 cmH2O and an inspiratory positive airway pressure (IPAP) of at least8 cm H2O above EPAP in an attempt to reach the higherpressure, as was the case in the majority of our patients. Adequatemechanical ventilation was attempted by closely observing thepatient during the day and the night. Once the mask was
CHEST / 118 / 6 / DECEMBER, 2000 1583
by on November 22, 2006 www.chestjournal.orgDownloaded from

comfortably adjusted, the pressures were adjusted to achieve avisual decrease in accessory muscle use,6,29 a decrease in percep-tion of dyspnea,10–13 and a 20% decrease in respiratory rate.5,6,29
Subsequently, the patients were observed in the hospital for atleast 2 nights. The ventilatory pressure settings were adjusted tomaintain the target goals. During NPPV, oxygen was deliveredusing a cannula attached to a port on the nasal mask. Oxygen flowwas titrated to achieve a minimum oxygen saturation $ 90%. Thehighest required level was 6 L/min. All patients and their relativeswere informed on the proper use of mechanical ventilation. Thepatients were discharged from the hospital only after the inves-tigators had been assured that ventilation was adequate and thatproper training was completed. Twenty-five patients in the NPPVgroup and 24 patients in the control group received long-termhome oxygen therapy. Within 48 h of hospital discharge, techni-cally skilled personnel performed the installation of the apparatusin the patient’s home. During the first 3 weeks, close contact wasmaintained with the patient in order to ensure good couplingwith the ventilator during sleep.
Clinical Course and Outcomes
The outcomes and clinical course were evaluated with personalinterviews. In the case of failure to attend an appointment, thepatient or relatives were contacted by telephone. All patientswere contacted at all follow-up points. The number of respiratoryexacerbations was recorded. Acute exacerbation was defined asan increase in dyspnea, cough, and sputum production, or changein the character and color of the sputum where the patientrequired a medical evaluation.30 We also recorded all hospitaladmissions, episodes of endotracheal intubation, and all pulmo-nary or extrapulmonary causes of death at 3 months, 6 months,and 12 months.
Statistics
Survival was assessed by Kaplan-Meier actuarial curve analysis.A power analysis using death as the outcome variable showed that20 subjects in each group would have a 92% chance of proving a10% difference if there was one. Therefore, 26 patients in eacharm of the trial were more than enough to test the hypothesis.After the study, a post hoc power analysis using the 1-yearmortality value showed that there would have been no differencein mortality independent of the number of patients recruited intothe study. Comparison of the other outcomes was completedusing Student’s t test and two-way analysis of variance forrepeated measures using the Statistical Package for Social Sci-ences (SPSS/PC; SPSS; Chicago, IL). Differences were consid-ered statistically significant at values of p , 0.05.
Results
Patient Characteristics
The 52 patients were randomized into one grouptreated with NPPV (n 5 26) and a control group(n 5 26). In spite of the encouragement, five pa-tients from the treatment group did not tolerateventilation within the first 3 weeks. All complainedabout pressures being too high. Another patientstopped participation after a significant aortic steno-sis was diagnosed at a follow-up echocardiography.Two patients from the control group also abandoned
the trial because of abnormal echocardiographicfindings detected during routine follow-up. There-fore, the study was completed in 44 patients (84%):20 in the NPPV group and 24 in the control group.Inclusion of the patients who did not complete thetrial (intent to treat) did not affect any of theoutcomes.
All patients in the treated group were men. Onlyone woman was included in the control group. Allpatients were white. Patients in the NPPV groupwere younger than those in the control group(64 6 5 years vs 68 6 4 years, respectively;p 5 0.005). The body mass index and LTOT timewere similar in both groups. There were no differ-ences in FVC (62 6 17% predicted in control sub-jects and 59 6 15% in NPPV patients); FEV1(31 6 7% predicted in control subjects and 29 6 8%in NPPV patients); lung volumes; respiratory musclestrength (MIP and MEP); and blood gas analysesbetween groups (Table 1).
Ventilator Tolerance and Compliance
The average time of ventilation was 6.2 h/d at thethird month and sixth month, and decreased slightly(5.9 h/d) during the following 6 months. Thesenumbers were obtained from the quotient of thetotal number of hours of apparatus use (electricaltime counter, which measures the number of hourssince the moment the machine is turned on) and thenumber of days from the time the ventilator wasinstalled at home. Although it would have been moreaccurate to use ventilators that also monitor theactual pressure delivered, they were not availablewhen the study was performed. Eleven percent ofour patients had a compliance rate , 3 h/d. All
Table 1—Patient Characteristics*
CharacteristicsControl(n 5 24)
NPPV(n 5 20)
Age, yr 68 6 4 64 6 5†Gender, M/F 23/1 20BMI, kg/m2 25 6 4 25 6 4FEV1, L 0.87 6 0.22 0.82 6 0.23FVC, L 2.09 6 0.66 2.12 6 0.56FRC, L 5.58 6 1.31 5.8 6 1.58MIP, % 48 6 22 46 6 15MEP, % 39 6 23 41 6 19Pao2, mm Hg 57.5 6 7.2 55.7 6 8.6Paco2, mm Hg 53.2 6 8.6 50.7 6 7.9Patient with LTOT, No. 22 19LTOT, mo 21 6 19 30 6 19
*Data are presented as mean 6 SD unless otherwise indicated.BMI 5 body mass index; M 5 male; F 5 female.
†Significant difference is in comparison with control group(p 5 0.005).
1584 Clinical Investigations
by on November 22, 2006 www.chestjournal.orgDownloaded from

patients reached an IPAP of at least 12 cm H2O andan EPAP of 4 cm H2O, with the exception of twopatients who reached an IPAP of 10 cm H2O andcould not tolerate higher pressure. The mean IPAPpressure achieved was 12 6 2 cm H2O.
Morbidity and Mortality
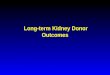
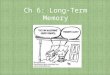
There were no significant differences in the num-ber or severity of the acute exacerbations. Thenumber of hospital admissions and episodes of en-dotracheal intubations were lower for the NPPVgroup during the first 3 months (Fig 1, upper panel)but this difference was not statistically significant.This difference was not observed at 6 months and 1year (Fig 1, lower panel). Survival at all points duringa 1-year follow-up was similar for both groups (Fig2). Two patients in the NPPV group died during thefirst 3 months (one from sudden death, and one froma respiratory tract infection) and two died during thelast 6 months (one from prostate carcinoma, and onefrom a respiratory tract infection). During the sameperiod (12 months), there also were four deaths inthe control group (one from a respiratory tractinfection, another one from a stroke, and two suddendeaths). From the group of patients who did not
tolerate NPPV treatment, only one patient died(unknown cause) between the sixth month and the12th month.
Physiologic Outcomes
Respiratory Parameters: There were no significantchanges in the arterial blood gas tests results, FEV1,FVC, lung volumes (TLC, FRC, RV/TLC), and inmuscular strength (MIP and MEP). The P0.1 de-creased significantly in the NPPV group by the thirdmonth (p 5 0.035), but this difference was not ob-served at sixth month. The DP0.1/DCO2 did not changeduring our study. No patients showed a deterioration inblood gas measures or pulmonary function test resultswhile receiving nasal ventilation (Table 2).
Hemodynamic Parameters: The levels of BP andhematocrit were normal and did not change through-out the study. For the seven patients in the NPPVgroup in whom all the echocardiographic measure-ments at all time points were available, the rightventricle/right atrium systolic gradient was elevatedin the treated group at baseline, compared with thesix control subjects (p 5 0.004). It decreased signif-icantly by the third month (p 5 0.009) and was
Figure 1. Long-term morbidity (acute exacerbations, admissions to the hospital, and endotrachealintubation) in patients with severe COPD after oxygen treatment alone and oxygen plus NPPV. Therewere no significant differences in any outcome at either 3 months or 12 months.
CHEST / 118 / 6 / DECEMBER, 2000 1585
by on November 22, 2006 www.chestjournal.orgDownloaded from

nearly significant by the sixth month (p 5 0.09). Therest of the hemodynamic parameters did not differbetween groups.
Dyspnea improved significantly (p 5 0.035, Med-ical Research Council scale; p 5 0.039, Borg scale)in the NPPV group by the third month. By the sixthmonth, the difference was less evident and only theevaluation with the Borg scale continued to showsignificant differences (p 5 0.033; Table 2). Thesechanges were not seen in the control group.
Neuropsychological Tests: The compliance wasexcellent (93%). We only found significant improve-ment in the treatment group in one of the psychomo-tor coordination tests (specifically, the right posturessequence at the sixth month; p 5 0.024; Table 3).
Subgroup Analysis
To determine if any clinical or functional variablecould predict an improvement associated withNPPV, we independently analyzed subgroups ofpatients in each of the following conditions: Pao2, 50 mm Hg (n 5 41), Paco2 . 50 mm Hg (n 5 12;, 50%), and compliance with the ventilator treat-ment of $ 5 h/d (n 5 16). This analysis did notreveal any significant differences.
Discussion
To our knowledge, this prospective study is thelargest and longest prospective, randomized, controlledtrial of NPPV in patients with stable severe COPD.10–
14,31–33 In addition, it is the only one that analyzes theinfluence of NPPV on 1-year morbidity and mortality.Over this time, we were unable to demonstrate animportant benefit of NPPV when added to standardtreatment. There was an improvement in the Borg
dyspnea scale and in one neuropsychological test at 6months, but the clinical importance of these changesappeared minimal.
Our results support the studies10,13,33 that dem-onstrated little benefit of NPPV in patients withstable severe COPD, and contradict some of thosewith more favorable results.12,34 To our knowl-edge, there are only six published prospective,randomized trials. All of them have in common ahigh intraindividual and interindividual variabilitywhen the efficacy of NPPV is analyzed.10–12,35–37
The differences may stem from the way in which thestudies were conducted. Three of them have afollow-up time of , 2 weeks,35–37 and the otherfollowed up the patients for only 3 months.10–13 Oursis the first study following up patients for 1 full year.
None of the short follow-up studies demonstratedbenefits on gas exchange.35–37 Renston et al36 docu-mented an improvement in dyspnea (Borg scale) andin the walk test, whereas Mezzanotte and cowork-ers37 showed an improvement in MIP and in theelectromyographic activity of the diaphragm. Al-though suggestive of some short-term beneficialphysiologic effect, the clinical importance of thesefindings remains speculative.
This difference in results is more evident in thestudies with longer follow-up time (3 months). Withthe exception of Morales et al,11 who used continu-ous positive airway pressure, bilevel positive pres-sure-type ventilation was used in all of the otherstudies. The different results cannot be attributed todifferences in disease severity, as the degree ofairflow obstruction in the patients in the studies wassimilar. Strumpf et al10 in 19 patients and Gay et al13
in 13 patients showed no difference between thebaseline and posttreatment values in respiratorymuscle strength, pulmonary function tests, arterialblood gas measures, or dyspnea. Similar to ourresults, in the largest of those studies,10 there was animprovement in some neuropsychological parame-ters after treatment, but this was not associated withany clinically detectable change. In contrast, Moraleset al11 found an improvement in dyspnea, which wasrelated to an increase in MIP and a decrease in RVthat is difficult attribute to the continuous positiveairway pressure treatment. It is unlikely that revers-ible airways disease accounted for the decrease inlung volume, the improvement in dyspnea, and theincrease in MIP, as there was no change in FEV1after treatment. However, an effect on respiratorymuscle fatigue can be documented only if there is nochange in resting lung volume, a finding that was notobserved in that study.
The most quoted positive study is the one byMeecham Jones et al,12 which had a run-in periodand a 3-month follow-up time. As in our study,
Figure 2. One-year survival was similar in patients with severeCOPD after oxygen treatment alone and oxygen plus NPPV.
1586 Clinical Investigations
by on November 22, 2006 www.chestjournal.orgDownloaded from

patients in the control group received supplementaltreatment with oxygen, an important component inthe treatment of patients with COPD, and a factorthat was not clearly detailed in all the other studies.In contrast to our negative results, Meecham Joneset al12 reported improvements in daytime gas ex-change, sleep quality, and health-related quality oflife, but no change in pulmonary function. Thedifferences between this and all the studies, includ-ing ours, are difficult to explain. It is not due to lungmechanics, as the degree of airflow obstruction in allthe studies was similar. In both studies, oxygen wassupplemented in treated and control groups andgreat care was devoted to the correct implementa-tion of ventilatory support, as shown by a high overallpatient compliance. Perhaps the most importantdifference is the initial level of gas exchange dysfunc-tion (hypoxemia and hypercapnia). Indeed, bothcomponents of the arterial blood gas measuresshowed worse values in the patients described byMeecham Jones et al.12 The effect of baseline hy-
poxemia can be discarded because oxygen wasclosely titrated in all patients. That leaves the level ofhypercapnia as the most important difference be-tween both studies. The patients in the MeechamJones et al12 study had higher mean levels of Paco2.In an attempt to test this hypothesis, we analyzed allof our outcomes stratifying the patients by their CO2level, but this failed to reveal any benefit even in thepatients with Paco2 . 50 mm Hg. Although thenumber of hypercapnic patients in our series wassmall, our results are consistent with the results ofthe study of Gay et al,13 in which the patients had alevel of Paco2 similar to the patients treated byMeecham Jones et al.12
Another possible factor that may explain the dif-ference between the studies was the level of venti-latory pressure utilized and its consequences oneffective ventilation. Whereas we used levels ofIPAP that fall within the clinically tolerated range(IPAP of around 12 cm H2O), this level is lower thanthat utilized by Meecham Jones et al12 (close to 18
Table 3—Neuropsychological Function (Psychomotor Coordination)*
Variables
Control(n 5 22)
Initial
NPPV(n 5 19)
InitialControl
6 moNPPV6 mo
Process speed 8.3 6 8.5 10.2 6 8.6 11.5 6 9.4 13.0 6 10.9Constructive praxis 19.1 6 6.4 20.5 6 8.0 20.9 6 7.4 21.4 6 7.0LP sequences 2.4 6 0.9 2.6 6 1.0 2.5 6 1.2 3.0 6 1.1RP sequences 2.5 6 0.9 2.7 6 1.0 2.4 6 1.2 3.0 6 1.0†LR coordination 1.4 6 0.5 1.6 6 0.5 1.9 6 0.4 1.7 6 0.5RR coordination 1.4 6 0.5 1.6 6 0.5 1.9 6 0.4 1.7 6 0.4Graphics 2.8 6 1.2 3.1 6 1.2 2.6 6 1.3 3.2 6 1.0
*Data are presented as mean 6 SD. LP 5 left posture; RP 5 right posture; RR 5 right reciprocal; LR 5 left reciprocal.†Significant difference compared with the control group (p 5 0.024).
Table 2—Baseline and Follow-up Values of Dyspnea, Pulmonary Function, CO2 Response, and Arterial Blood Gasesin the Patients Who Completed the Trial*
Variables
Control(n 5 24)
Initial
NPPV(n 5 20)
InitialControl
6 moNPPV6 mo
Dyspnea MRC scale 2 3 2 2Dyspnea BORG scale 4 6 4 5†FEV1, % 31 6 7 29 6 8 31 6 7 30 6 9FVC, % 62 6 17 59 6 14 65 6 18 59 6 19FRC, % 165 6 38 165 6 4 156 6 40 154 6 50RV/TLC, % 158 6 23 166 6 29 154 6 19 159 6 37MIP, % 48 6 22 46 6 15 50 6 19 44 6 15MEP, % 39 6 23 41 6 19 41 6 22 30 6 18DP0.1/DCO2, % 46 6 26 55 6 34 54 6 24 56 6 32Pao2, mm Hg 57.5 6 7.2 55.7 6 8.6 57.3 6 6.5 56.3 6 8.2Paco2, mm Hg 53.2 6 8.1 50.7 6 7.9 52.3 6 6.1 51.1 6 8.8
*Data are presented as mean 6 SD unless otherwise indicated. All volumes are expressed as percent of predicted values. MRC 5 MedicalResearch Council; DP0.1/DCO2 5 hypercapnic response.
†Significant difference is in comparison with control group (p 5 0.033).
CHEST / 118 / 6 / DECEMBER, 2000 1587
by on November 22, 2006 www.chestjournal.orgDownloaded from

cm H2O). However, we did use higher EPAP (4 cmH2O vs 1.9 cm H2O). Overall, our ventilatory pres-sures were significantly higher than those used byothers,13,35 and similar to those used by Strumpf etal.10 We began treatment in the hospital and at-tempted to provide adequate ventilation by achiev-ing a decrease in baseline respiratory rate and de-creased accessory muscle use.5,29 We tailored thepressure to the patient’s perception of dyspnea andoverall comfort. Higher pressures were not welltolerated; indeed, the patients who refused to con-tinue NPPV did so because they believed the venti-latory pressure was too high, an observation that wasfrequently reported in at least two of the studies.10,13
Although we do not believe that poor ventilation atnight was a factor that affected our outcomes, itcertainly remains a possibility.
Finally, one other potential difference betweenour patients and those of Meecham Jones et al12 wasthe degree of sleep-related hypopneic/apneic epi-sodes. We excluded patients who had . 10 hourlyepisodes of hypopneas during the sleep study. In-deed, our patients only had 3.5 episodes per hour pernight, whereas those treated by Meecham Jones etal12 had an average of 10 episodes per hour. Al-though unlikely, this small difference could helpexplain the difference between the two studies.
The results of all of the trials suggest that if NPPVis to be implemented, it may need to be used only inselected patients capable of tolerating the higherpressures and with close nighttime monitoring.However, if the treatment is applicable only to asmall proportion of patients with COPD, its clinicalapplicability is limited at best.
It could be said that our control patients shouldhave received a sham treatment. Initially, we triedsham NPPV in the control group (the first fourpatients) but could not continue its use due to nasaldiscomfort. Because one of the previous randomizedtrials used sham controls and found no differencesbetween control and treated patients,13 we believedit was unjustified to submit patients to a 1-year trialof an uncomfortable machine without a theoreticalbenefit.
The most important contribution of our study isthat we extended our treatment and evaluation for 1year. After 6 months, we only found an improvementin the Borg scale and in the right posture sequence.Although the improvement in dyspnea may be im-portant in the quality of life of patients with severeCOPD,38 we should keep in mind the possibleplacebo effect of NPPV. The right posture sequence,which might reflect the function of an area in thebrain very sensitive to oxygen,38 was the only testamong the 20 neuropsychological parameters thatshowed a significant improvement. We believe that
this single test change is best explained by chancealone; although statistically significant, it carries littleclinical relevance.
Our study is unique in that it evaluated 1-yearmortality. The patients in the NPPV group were onaverage 4 years younger, but if anything, this shouldfavor mortality in the NPPV group. It could beargued that the number of patients in the study wastoo small to detect changes in mortality. However,we completed a power analysis choosing a 1-year10% mortality difference between groups, based ona study39 that suggests this to be the death rate forpatients with severe COPD, and found that 20patients in each group were enough to detect thatchange. In addition, a post hoc power analysis usingthe observed mortality in our study showed thatthere would be no mortality differences independentof the number of patients enrolled. It is possible that1 year is not enough time to determine the mortalityof patients with COPD. However, our finding issupported by that of Muir et al40 who, in abstractform, reported no difference in overall mortality at 4years in 123 patients randomized to NPPV plusoxygen, vs oxygen therapy alone.
We consider the number and severity of respira-tory infections to be of great relevance. There werefewer hospital admissions and intubations in theNPPV group at 3 months, but the difference was notstatistically different. Furthermore, this finding dis-appeared after 6 months. We believe that disease-specific health-related quality of life would havebeen a desirable outcome to measure, but at the timeof the study, there were no tools validated in theSpanish language. However, we did use validatedneuropsychological tests. The changes observed indyspnea and neuropsychological testing were mini-mal, and very much in agreement with the findingsof Strumpf et al.10 We also addressed utilization ofhealth-care resources by evaluating the number ofhospital admissions, a very important outcome giventhe ever-debated problem of health-care cost.41 Thelack of significant benefit in any of these areasconstitutes an incentive to reevaluate the use ofNPPV in patients with stable COPD. We did not findany selected subgroups, based on gasometric criteria,respiratory function, and treatment compliance, thatspecifically benefit from NPPV treatment. It is pos-sible, but highly unlikely, that a bigger patientsample size could be necessary to demonstrate smalldifferences.
We conclude that NPPV with bilevel-type ventila-tion in the spontaneous mode when used in additionto LTOT has limited efficacy in patients with stablesevere COPD. Perhaps a large, multicenter trialaimed at patients with important hypercapnia andwithout sleep apnea should be implemented. The
1588 Clinical Investigations
by on November 22, 2006 www.chestjournal.orgDownloaded from

results of the large, multicenter trial in Europe41
could help clarify this debate. If we could developtechnology that may better unload the ventilatorypump, such treatment may result in a more signifi-cant benefit. However, it is possible that NPPV mayhave little impact on a system that, in patients inchronic stable condition, is functioning at its optimallevel.
ACKNOWLEDGMENT: The authors wish to thank AngelaMontejo de Garcini and Sandra de Armas, pulmonary nurses, fortechnical assistance.
References1 Chailleaux E, Faraux B, Binet F, et al. Predictors of survival
in patients receiving domiciliary oxygen therapy or mechani-cal ventilation. Chest 1996; 109:741–749
2 Lung transplantation: report of the ATS workshop on lungtransplantation: American Thoracic Society, Medical Sectionof the American Lung Association. Am Rev Respir Dis 1993;147:772–776
3 Benditt JO, Albert RK. Lung reduction surgery: great expec-tation and a cautionary note. Chest 1995; 107:297–298
4 Meyer TJ, Hill NS. Noninvasive positive pressure ventilationto treat respiratory failure. Ann Intern Med 1994; 120:760–770
5 Ambrosino N. Noninvasive mechanical ventilation in acuterespiratory failure. Eur Respir J 1996; 9:795–807
6 Clinical indications for noninvasive positive pressure ventila-tion in chronic respiratory failure due to restrictive lungdisease, COPD, and nocturnal hypoventilation: a consensusconference report. Chest 1999; 116:521–534
7 Catterall JR, Calverley PMA, MacNee W, et al. Mechanism oftransient hypoxemia in hypoxic chronic bronchitis and em-physema. J Appl Physiol 1985; 59:1698–1703
8 Ballard RD, Clover CW, Suh BY. Influence of sleep onrespiratory function in emphysema. Am J Respir Crit CareMed 1995; 151:945–951
9 Elliot MW, Mulvey DA, Moxham J, et al. Domiciliarynocturnal nasal intermittent positive pressure ventilation inCOPD: mechanisms underlying changes in arterial blood gastensions. Eur Respir J 1991; 4:1044–1052
10 Strumpf DA, Millman RP, Carlisle CC, et al. Nocturnalpositive pressure ventilation via nasal mask in patients withsevere chronic obstructive pulmonary disease. Am Rev RespirDis 1991; 144:1234–1239
11 Morales MA, Otero R, Medina JF, et al. The short-termeffects of nocturnal domiciliary mechanical ventilation withnasal continuous positive pressure in patients with chronicobstructive pulmonary disease. Arch Bronconeumol 1993;29:220–225
12 Meecham Jones DJ, Paul EA, Jones PW, et al. Nasal pressureventilation plus oxygen compared with oxygen therapy alonein hypercapnic COPD. Am J Respir Crit Care Med 1995;152:538–544
13 Gay PC, Hubmayr RD, Stroetz RW. Efficacy of nocturnalnasal ventilation in stable, severe chronic obstructive pulmo-nary disease during a 3-month controlled trial. Mayo ClinProc 1996; 71:533–542
14 Standardization of spirometry–1987 update: statement of theAmerican Thoracic Society. Am Rev Respir Dis 1987; 136:1285–1298
15 Dubois AB, Botelho SY, Bedell GN, et al. A rapid plethys-mographic method for measuring thoracic gas volume: a
comparison with a nitrogen washout method for measuringfunctional residual capacity in normal subjects. J Clin Invest1956; 35:322–326
16 Quanjer PhH. Standardized lung function testing: reportWorking Party for the European Community for Steel andCoal. Bull Eur Physiopathol Respir 1983; 19(suppl 5):22–27
17 American Thoracic Society. Single breath carbon monoxidediffusing capacity (transfer factor): recommendations for astandard technique. Am Rev Respir Dis 1987; 136:1299–1307
18 Black LF, Hyatt RE. Maximal respiratory pressures: normalvalues and relationship to age and sex. Am Rev Respir Dis1969; 99:696–702
19 Casan P, Mayos M, Galdiz J, et al. Presiones respiratoriasmaximas: normativas y controversias. Arch Bronconeumol1989; 26:223–228
20 Cherniak NS. Workshop on assessment of respiratory controlsin humans: methods of measurement of ventilatory responsesto hypoxia and hypercapnia. Am Rev Respir Dis 1977;115:177–181
21 Mahler DA, Wells CK. Evaluation of clinical methods forrating dyspnea. Chest 1988; 93:580–586
22 Weschler DA. Weschler adult intelligence scale. New York,NY: Manual Psychological Corporation, 1955; 155–176
23 Strub RL, Black FW. The mental status examination inneurology. 2nd ed. Philadelphia, PA: FA Davis Company,1985; 75–92
24 Luria AR. Bases of neuropsychology. Moscow, USSR: Mos-cow University, 1973
25 Weyman AE. Right ventricle. In: Weyman AE. Cross sec-tional echocardiography. Philadelphia, PA: Lea & Febiger;1982; 383–395
26 Kitabatake A, Inque M, Asao M, et al. Noninvasive evaluationof pulmonary hypertension by a pulsed Doppler technique.Circulation 1984; 68:302–309
27 Nakao S, Come PC, McKay RG, et al. Effects of positionalchanges on inferior vena caval size and dynamics and corre-lations with right-sided cardiac pressure. Am J Cardiol 1987;59:125–132
28 Rechtschaffen A, Kales A. A manual of standardized termi-nology, techniques and scoring systems for sleep stages ofhuman subjects. Bethesda, MD: National Institute of Neuro-logical Disease and Blindness, 1968. National Institutes ofHealth publication No. 204.
29 Brochard L, Harf A, Lorino H, et al. Inspiratory pressuresupport prevents diaphragmatic fatigue during weaning frommechanical ventilation. Am Rev Respir Dis 1989; 139:513–521
30 Anthonisen NR, Manfreda J, Warren CPW, et al. Antibiotictherapy in exacerbations of chronic obstructive pulmonarydisease. Ann Intern Med 1987; 106:196–204
31 Sivasothy P, Smith IE, Shneerson JM. Mask intermittentpositive pressure ventilation in chronic hypercapnic respira-tory failure due to chronic obstructive pulmonary disease.Eur Respir J 1998; 11:34–40
32 Jones SE, Packham S, Hebden M, et al. Domiciliary noctur-nal intermittent positive pressure ventilation in patients withrespiratory failure due to severe COPD: long-term follow upand effect on survival. Thorax 1998; 53:495–498
33 Clini E, Sturani C, Porta R, et al. Outcome of COPD patientsperforming nocturnal non-invasive mechanical ventilation.Respir Med 1998; 92:1215–1222
34 Wedzicha JA, Meecham Jones DJ. Domiciliary ventilation inchronic obstructive pulmonary disease: where are we? Thorax1996; 51:455–457
35 Lin CC. Comparison between nocturnal nasal positive pres-sure ventilation combined oxygen therapy and oxygen mono-
CHEST / 118 / 6 / DECEMBER, 2000 1589
by on November 22, 2006 www.chestjournal.orgDownloaded from

therapy in patients with severe COPD. Am J Respir Crit CareMed 1996; 154:353–358
36 Renston JP, Dimarco AF, Supinski GS. Respiratory musclerest using BiPAP ventilation in patients with stable severeCOPD. Chest 1994; 105:1053–1060
37 Mezzanotte WS, Tangel DJ, Fox AM, et al. Nocturnal nasalcontinuous positive airway pressure in patients with chronicobstructive pulmonary disease. Chest 1994; 106:1100–1108
38 Mahler DA, Faryniar K, Tomlinson D, et al. Impact ofdyspnea and physiologic function on general health status inpatients with chronic pulmonary disease. Chest 1992; 102:395–401
39 Gerardi D, Lovett L, Benoit-Connors J, et al. Variablesrelated to increased mortality following outpatient pulmonaryrehabilitation. Eur Respir J 1996; 9:431–435
40 Muir JF, De La Salmoniere P, Cuvelier A, et al. Survivalof severe hypercapnic COPD under long-term home me-chanical ventilation with NIPPV1oxygen versus oxygen ther-apy alone: preliminary results of a European multicentrestudy [abstract]. Am J Respir Crit Care Med 1999; 159:A295
41 Pelletier-Fleury N, Lanoe JL, Fleury J, et al. The cost oftreating COPD patients with long-term oxygen therapy in aFrench population. Chest 1996; 110:411–416
1590 Clinical Investigations
by on November 22, 2006 www.chestjournal.orgDownloaded from

DOI: 10.1378/chest.118.6.1582 2000;118;1582-1590 Chest
Valle Velasco and Francisco Santolaria Ciro Casanova, Bartolome R. Celli, Lina Tost, Estanislao Soriano, Juan Abreu,
Patients With Severe COPDLong-term Controlled Trial of Nocturnal Nasal Positive Pressure Ventilation in
This information is current as of November 22, 2006
& ServicesUpdated Information
http://www.chestjournal.org/cgi/content/full/118/6/1582figures, can be found at: Updated information and services, including high-resolution
References
Lhttp://www.chestjournal.org/cgi/content/full/118/6/1582#BIBfree at: This article cites 33 articles, 18 of which you can access for
Citations
articleshttp://www.chestjournal.org/cgi/content/full/118/6/1582#otherThis article has been cited by 21 HighWire-hosted articles:
Permissions & Licensing
http://www.chestjournal.org/misc/reprints.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://www.chestjournal.org/misc/reprints.shtml
Information about ordering reprints can be found online:
Email alerting servicesign up in the box at the top right corner of the online article. Receive free email alerts when new articles cite this article
Images in PowerPoint format
article figure for directions. teaching purposes in PowerPoint slide format. See any online Figures that appear in CHEST articles can be downloaded for
by on November 22, 2006 www.chestjournal.orgDownloaded from