Embed Size (px)
Citation preview

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 1 of 62
LUNG CANCER Section by: Dr Conrad Lewanski, Dr Danielle Power, Dr Tom Newsom-Davis Version; Lung Cancer Regimens v5.02 NWLCN 31Jan14 Section last reviewed: 13th December 2013 Section last corrected: 31st January 2014 Approved by Oncology Lung Clinician: Dr C Lewanski Date Review date: December 2015 INDEX
Page
Non Small Cell Lung Cancer
Neo-Adjuvant Chemotherapy; according to current trial protocols
Adjuvant Chemotherapy 1. Vinorelbine-25/Cisplatin-80 (chemo alone) 4 2. Gemcitabine-1250/Carboplatin-5AUC 5
Locally Advanced CHEMO ALONE (Stage 3a-3b, Inoperable stage 2) Locally Advanced NON Squamous Chemo Alone Regimens
3. Pemetrexed-500/Cisplatin-75 (NICE TA181) 7 4. Pemetrexed-500/Carboplatin-5AUC (NICE TA181) 10 5. Gemcitabine-1250/Carboplatin-5AUC 13 6. Paclitaxel-175/Carboplatin-5AUC 14
Locally advanced Squamous Chemo Alone Regimens
7. Gemcitabine-1250/Carboplatin-5AUC 16 8. Gemcitabine-1250/Cisplatin-80 16 9. Paclitaxel-175/Carboplatin-5AUC 18
Locally Advanced Chemo-Radiation (Stage 3a-3b, Inoperable stage 2) Locally Advanced Non Squamous Chemo-radiation Regimens
10. Etoposide-50/Cisplatin-50 (concurrent radiotherapy) 19 11. Pemetrexed-500/Cisplatin-75 (concurrent radiotherapy) 20
Locally advanced Squamous Chemo-radiation regimens
12. Etoposide-50/Cisplatin-50 (concurrent radiotherapy) 22
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 2 of 62
Page
Non Small Cell Lung Cancer Patients Possessing EGFR Activating Mutations
EGFR general skin and care advice 22 First line
13. Gefitinib-250 (Iressa) (NICE TA192) 23 14. Erlotinib-150 (Tarceva) (NICE TA258) 24 15. Afatinib-40 (Giotrif) (Additional private care only) 27
Maintenance Chemotherapy (Within 6 weeks of initial chemotherapy)
Maintenance Chemotherapy Non Squamous cell
16. Pemetrexed-500 single agent (NICE TA190/Cancer Drugs Fund) 31 17. Erlotinib-150 (Tarceva) (Additional private care only) 33
Maintenance Chemotherapy Squamous cell 18. Erlotinib-150(Tarceva) (Additional private care only) 34
Relapse Regimens All patients
19. Docetaxel-75 35 20. Erlotinib-150 (Tarceva) (NICE TA162) 36
Non Squamous Cell 21. Pemetrexed-500 single agent (Cancer Drugs Fund) 37
Patient possessing ALK positive carcinoma 22. Crizotinib (Cancer Drugs Fund) 38
Palliative Chemotherapy (Stage 4, or Stage 3 or 2 if unsuitable for radical treatment) Palliative Regimens Non Squamous cell
23. Pemetrexed-500/Cisplatin-75 (additional private care) 41 24. Pemetrexed-500/Carboplatin-5AUC (additional private care) 42 25. Gemcitabine 1250/Carboplatin-5AUC 43 26. Paclitaxel-175/Carboplatin-5AUC 44
Palliative Regimens Squamous cell
27. Gemcitabine-1250/ Carboplatin-5AUC 44 28. Gemcitabine-1250/Cisplatin-80 45 29. Paclitaxel-175/Carboplatin-5AUC 46
Additional Private Care regimens 30. Paclitaxel/Carboplatin/Bevacizumab 47

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 3 of 62
Page
Small Cell Lung Cancer First Line:
31. Etoposide/Platinum combination EP oral 52 32. E-Carbo 53
Relapse regimens Late Relapse (beyond 6 months)
33. E-Carbo 54
Early Relapse (within 6 months) 34. CAV 55 35. Topotecan Oral (NICE TA184) 56
Palliative Chemotherapy 36. Oral etoposide 14day 58
Mesothelioma First Line
37. Pemetrexed-500/Cisplatin-75 (NICE TA135) 59
Second Line: Clinical Trials if available
38. Vinorelbine-30 IV 60 39. Vinorelbine-25/Cisplatin-80 61
Version control box 62

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 4 of 62
Non Small Cell Lung Cancer Section by: Dr Conrad Lewanski, Dr Danielle Power, Dr Tom Newsom-Davis Version; Lung Cancer Regimens v5.02 NWLCN 31Jan14 Section last reviewed: 13th December 2013 Section last corrected: 31st January 2014 Approved by Oncology Lung Clinician: December 2013 Review date: December 2015
Neo-Adjuvant Chemotherapy (prior to surgery) Clinical Trials if available or at discretion of consultant after discussion at the MDT.
Adjuvant Chemotherapy (CHEMO ALONE) Preferred option based on available evidence is Cisplatin/Vinorelbine 1. Cisplatin-80/Vinorelbine-25
Vinorelbine 25mg/m2 IV minibag over 10 mins Day 1 and 8 Prehydrations Day 1 Cisplatin 80mg/m2 IV over 2 hours Day 1 Post hydrations Day 1 March 2011; Vinorelbine dose reduced to 25mg/m
2
Oral vinorelbine see additional information below
Interval between cycles: Repeat every 21 days Number of cycles: 4 cycles Tests before starting course of chemo: FBC, U&Es, LFTs, CrCl (calculated). Do
EDTA if <60ml/min. Tests to ok/confirm each cycle of chemo: Day 1: FBC, U&Es, LFTs, CrCl (calculated). Day 8: FBC, U&Es Do EDTA if serum creatinine is rising.
Supportive drugs with each cycle: Laxatives Antiemetics below as per NWLCN
guidelines or as per local policy; Day 1: Very High Risk antiemetics Day 8: Low risk antiemetics Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Vinorelbine is a vesicant and must be administered according to NWLCN administration policy. Vinorelbine minibag should be administered over 10minutes with a fast running drip of sodium chloride 0.9% through the same cannula. Day 8 Vinorelbine IV can be replaced with oral if necessary and where there is local approval/funding for this. Bloods must be done on day 8 irrespective of route of vinorelbine administration. Pierre Fabre SPC 20/09/2010 states that based on
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 5 of 62
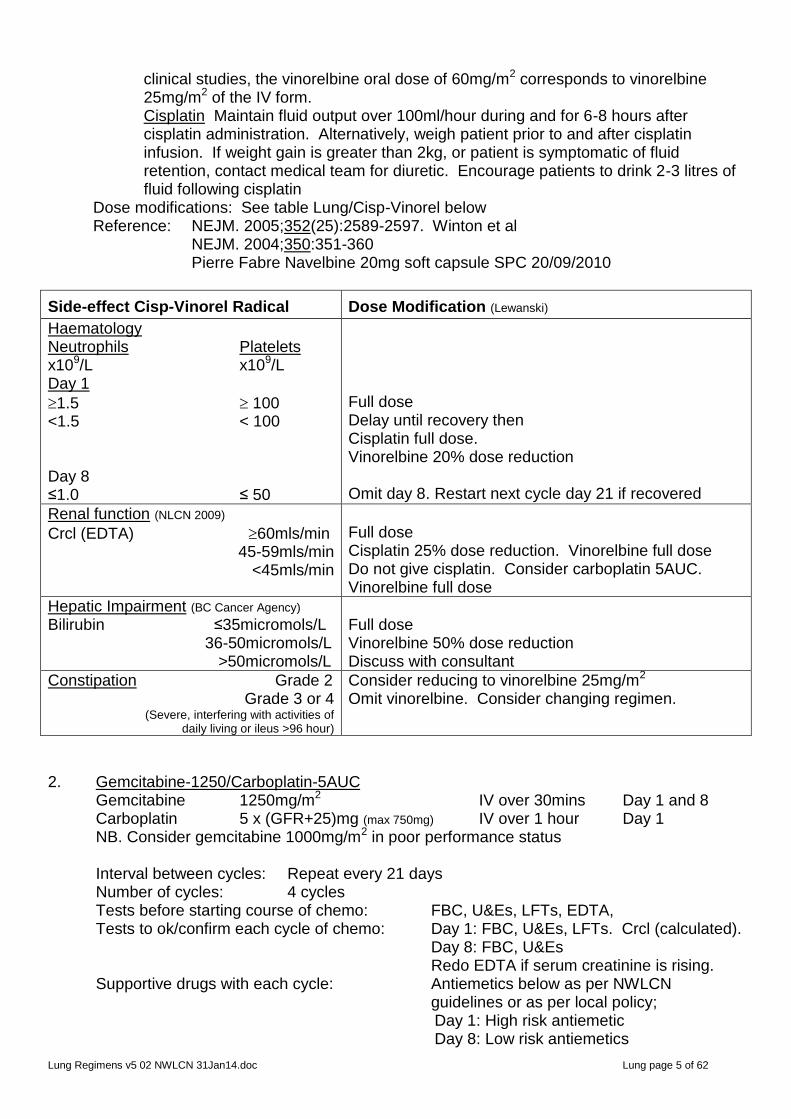
clinical studies, the vinorelbine oral dose of 60mg/m2 corresponds to vinorelbine 25mg/m2 of the IV form. Cisplatin Maintain fluid output over 100ml/hour during and for 6-8 hours after cisplatin administration. Alternatively, weigh patient prior to and after cisplatin infusion. If weight gain is greater than 2kg, or patient is symptomatic of fluid retention, contact medical team for diuretic. Encourage patients to drink 2-3 litres of fluid following cisplatin
Dose modifications: See table Lung/Cisp-Vinorel below Reference: NEJM. 2005;352(25):2589-2597. Winton et al NEJM. 2004;350:351-360 Pierre Fabre Navelbine 20mg soft capsule SPC 20/09/2010
Side-effect Cisp-Vinorel Radical
Dose Modification (Lewanski)
Haematology Neutrophils Platelets x109/L x109/L Day 1
1.5 100 <1.5 < 100 Day 8 ≤1.0 ≤ 50
Full dose Delay until recovery then Cisplatin full dose. Vinorelbine 20% dose reduction Omit day 8. Restart next cycle day 21 if recovered
Renal function (NLCN 2009)
Crcl (EDTA) 60mls/min 45-59mls/min
<45mls/min
Full dose Cisplatin 25% dose reduction. Vinorelbine full dose Do not give cisplatin. Consider carboplatin 5AUC. Vinorelbine full dose
Hepatic Impairment (BC Cancer Agency) Bilirubin ≤35micromols/L 36-50micromols/L >50micromols/L
Full dose Vinorelbine 50% dose reduction Discuss with consultant
Constipation Grade 2 Grade 3 or 4
(Severe, interfering with activities of daily living or ileus >96 hour)
Consider reducing to vinorelbine 25mg/m2 Omit vinorelbine. Consider changing regimen.
2. Gemcitabine-1250/Carboplatin-5AUC Gemcitabine 1250mg/m2 IV over 30mins Day 1 and 8 Carboplatin 5 x (GFR+25)mg (max 750mg) IV over 1 hour Day 1 NB. Consider gemcitabine 1000mg/m2 in poor performance status Interval between cycles: Repeat every 21 days Number of cycles: 4 cycles Tests before starting course of chemo: FBC, U&Es, LFTs, EDTA, Tests to ok/confirm each cycle of chemo: Day 1: FBC, U&Es, LFTs. Crcl (calculated). Day 8: FBC, U&Es Redo EDTA if serum creatinine is rising. Supportive drugs with each cycle: Antiemetics below as per NWLCN
guidelines or as per local policy; Day 1: High risk antiemetic Day 8: Low risk antiemetics

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 6 of 62
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate
NWLCN Neutropenia DVD
Additional information: Gemcitabine; Do not administer this regimen with concurrent radiotherapy. Gemcitabine must be administered over 30 minutes. In the case of injection site reaction (vein irritation), the infusion may be slowed down slightly but must not be infused over more than 60minutes as prolonged infusion increases the treatment toxicity. Peripheral venous comfort may be increased by warming the arm with a heat pad. Hypersensitivity reaction Gemcitabine Rash with gemcitabine; retreat with hydrocortisone 100mg IV cover. Hypersensitivity reaction Carboplatin Reactions may occur to carboplatin, see SPC information below If any reaction occurs: stop infusion and discuss with consultant. If mild reaction; Consultant in charge may consider re-challenge with chlorphenamine 10mg IV and hydrocortisone 100mg IV cover. If moderate/severe reaction. Do not re-challenge and seek alternative treatment. Carboplatin SPC Hospira (09 June 2009); Infrequent allergic reactions to carboplatin have been reported, e.g. erythematous rash, fever with no apparent cause or pruritus. Rarely, anaphylaxis, angio oedema and anaphylactoid reactions including bronchospasm, urticaria and facial oedema have occurred. These reactions are similar to those observed after administration of other platinum containing compounds and may occur within minutes. The incidence of allergic reactions may increase with previous exposure to platinum therapy; however, allergic reactions have been observed upon initial exposure to carboplatin.
Dose modifications: See table Gem/Carbo lung below Reference:
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 7 of 62
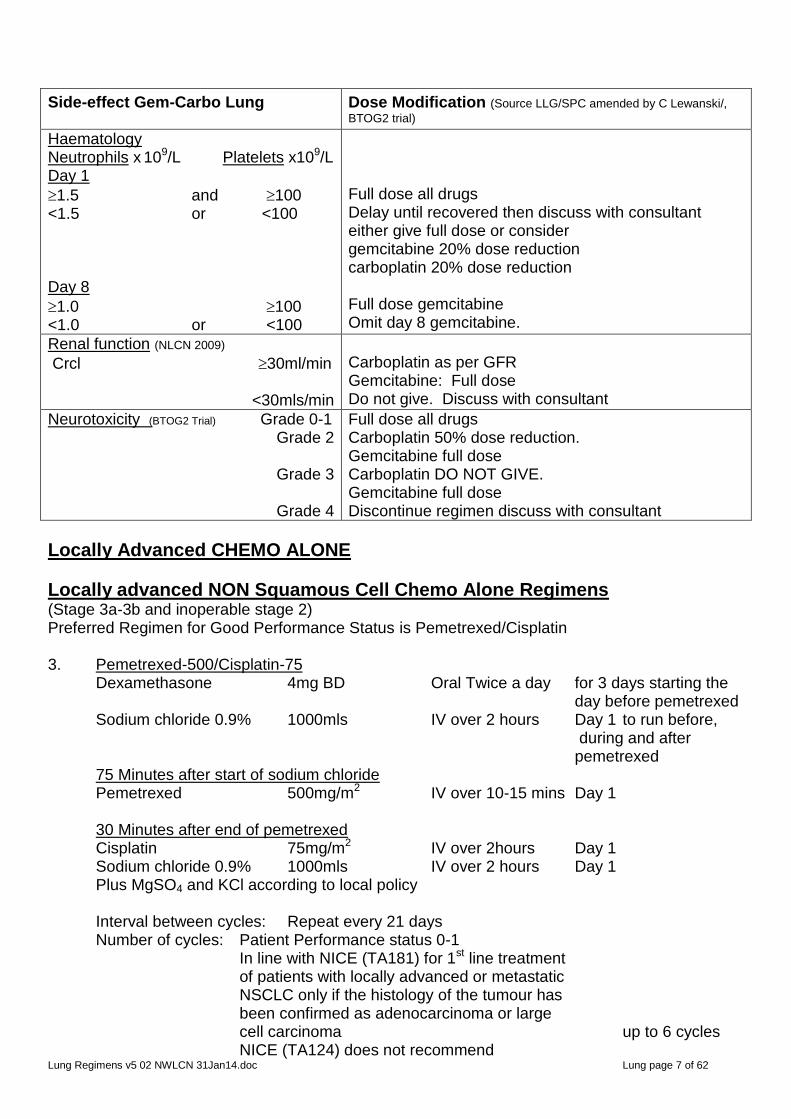
Side-effect Gem-Carbo Lung Dose Modification (Source LLG/SPC amended by C Lewanski/,
BTOG2 trial)
Haematology Neutrophils x 109/L Platelets x109/L x109/L Day 1
1.5 and 100 <1.5 or <100 Day 8
1.0 100 <1.0 or <100
Full dose all drugs Delay until recovered then discuss with consultant either give full dose or consider gemcitabine 20% dose reduction carboplatin 20% dose reduction Full dose gemcitabine Omit day 8 gemcitabine.
Renal function (NLCN 2009)
Crcl 30ml/min
<30mls/min
Carboplatin as per GFR Gemcitabine: Full dose Do not give. Discuss with consultant
Neurotoxicity (BTOG2 Trial) Grade 0-1 Grade 2
Grade 3
Grade 4
Full dose all drugs Carboplatin 50% dose reduction. Gemcitabine full dose Carboplatin DO NOT GIVE. Gemcitabine full dose Discontinue regimen discuss with consultant
Locally Advanced CHEMO ALONE
Locally advanced NON Squamous Cell Chemo Alone Regimens (Stage 3a-3b and inoperable stage 2) Preferred Regimen for Good Performance Status is Pemetrexed/Cisplatin 3. Pemetrexed-500/Cisplatin-75 Dexamethasone 4mg BD Oral Twice a day for 3 days starting the day before pemetrexed Sodium chloride 0.9% 1000mls IV over 2 hours Day 1 to run before, during and after pemetrexed 75 Minutes after start of sodium chloride Pemetrexed 500mg/m2 IV over 10-15 mins Day 1 30 Minutes after end of pemetrexed Cisplatin 75mg/m2 IV over 2hours Day 1 Sodium chloride 0.9% 1000mls IV over 2 hours Day 1 Plus MgSO4 and KCl according to local policy Interval between cycles: Repeat every 21 days Number of cycles: Patient Performance status 0-1 In line with NICE (TA181) for 1st line treatment of patients with locally advanced or metastatic NSCLC only if the histology of the tumour has been confirmed as adenocarcinoma or large cell carcinoma up to 6 cycles NICE (TA124) does not recommend
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 8 of 62
pemetrexed for NSCLC patients who have had prior chemotherapy - Tests before starting course of chemo FBC, U&Es, LFTs, CrCl calculated. Do
EDTA if <60ml/min Tests to OK/Confirm each cycle of chemo: FBC, U&Es, LFTs, CrCl calculated. Do EDTA if rising serum creatinine Supportive drugs with each cycle: Very high risk antiemetics as per NWLCN
guidelines or as per local policy Vitamin supplementation to reduce toxicity and incidence of grade 3/4 haematological and non-haematological toxicities Folic acid 400microgram oral daily, starting 7 days before 1st pemetrexed dose and continuing for 21days after last pemetrexed dose Vitamin B12 1000micrograms IM, first dose must be given one week before the 1st pemetrexed dose and then once every 3 cycles thereafter, (subsequent doses may be given on the same day as pemetrexed.
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Sodium chloride is the pre-hydration for cisplatin. It should start approx. 75 minutes before pemetrexed and run before, during and for 30minutes after the pemetrexed. Cisplatin must not start until 30minutes after the pemetrexed and the sodium chloride will keep the line patent whilst during this delay. Pemetrexed is mainly eliminated unchanged renally by tubular excretion and to a lesser extent by glomerular filtration. Concomitant administration of nephrotoxic drugs (eg aminoglycosides, loop diuretics, platinum compounds) could potentially result in delayed clearance of pemetrexed. Use with caution.
Dose modifications: See table below Reference:

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 9 of 62
Side effect: Pemetrexed/Cisplat
Dose Modification (SPC)
Haematology (SPC)
Neutrophils Platelets x109/L x109/L
1.5 100 <1.5 <100 Nadir Counts Dose reductions should be based on nadir counts. Wait for recovery to above levels then dose as below
<0.5 and 50 Any and <50 Any and <50 With bleeding
Full dose all drugs Delay until recovery then dose should be based on nadir blood counts below Wait until recovery then give Pemetrexed 25% dose reduction Cisplatin: 25% dose reduction Wait until full recovery then give Pemetrexed 25% dose reduction Cisplatin: 25% dose reduction Wait until full recovery then discuss with consultant Consider: Pemetrexed: 25-50% dose reduction Cisplatin: 25-50% dose reduction
Renal function (NLCN 2009/SPC)
Crcl (EDTA) >60mls/min 45-59mls/min
<45mls/min
Full dose Cisplatin 25% dose reduction. Pemetrexed full dose but avoid NSAID 2days before and after pemetrexed dose Do not give regimen. Discuss with consultant
Hepatic function (SPC)
Bilirubin ≤1.5xULN > 1.5xULN Alk Phos, AST (or SGOT), ALT (or SGPT) ≤3 xULN 3 to 5 xULN
>5 xULN
Full dose Discuss with consultant SPC recommends do not give pemetrexed because patient group not specifically studied. Full dose pemetrexed Do not give pemetrexed except If liver has tumour involvement, then full dose pemetrexed is permitted. Do not give pemetrexed (patient group not studied) Discuss with consultant
Neurotoxicity: NCICTC Grade Grade 0-1
Grade 2
Grade 3 or 4
Full dose all drugs Cisplatin 50% dose reduction Pemetrexed full dose Discontinue regimen immediately
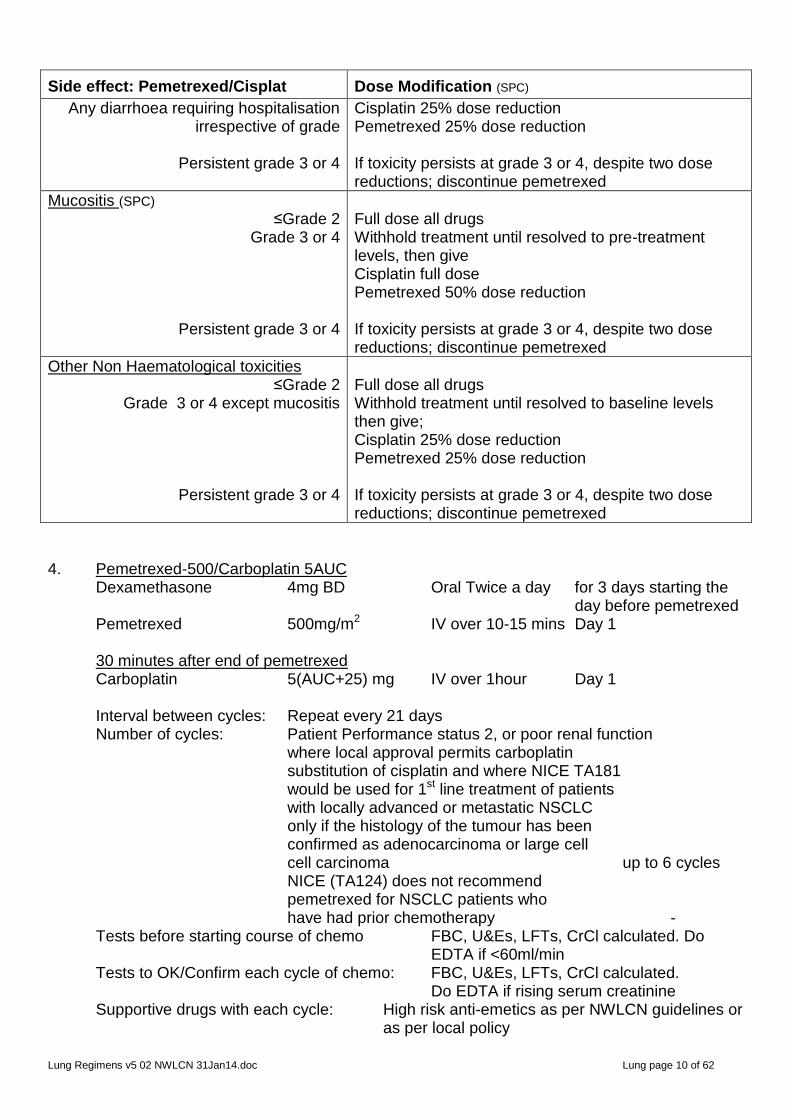
Diarrhoea (SPC) ≤Grade 2 Grade 3 or 4
Full dose all drugs Withhold treatment until resolved to baseline levels then give; Cisplatin 25% dose reduction Pemetrexed 25% dose reduction
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 10 of 62
Side effect: Pemetrexed/Cisplat
Dose Modification (SPC)
Any diarrhoea requiring hospitalisation irrespective of grade
Persistent grade 3 or 4
Cisplatin 25% dose reduction Pemetrexed 25% dose reduction If toxicity persists at grade 3 or 4, despite two dose reductions; discontinue pemetrexed
Mucositis (SPC) ≤Grade 2
Grade 3 or 4
Persistent grade 3 or 4
Full dose all drugs Withhold treatment until resolved to pre-treatment levels, then give Cisplatin full dose Pemetrexed 50% dose reduction If toxicity persists at grade 3 or 4, despite two dose reductions; discontinue pemetrexed
Other Non Haematological toxicities ≤Grade 2
Grade 3 or 4 except mucositis
Persistent grade 3 or 4
Full dose all drugs Withhold treatment until resolved to baseline levels then give; Cisplatin 25% dose reduction Pemetrexed 25% dose reduction If toxicity persists at grade 3 or 4, despite two dose reductions; discontinue pemetrexed
4. Pemetrexed-500/Carboplatin 5AUC Dexamethasone 4mg BD Oral Twice a day for 3 days starting the day before pemetrexed Pemetrexed 500mg/m2 IV over 10-15 mins Day 1 30 minutes after end of pemetrexed Carboplatin 5(AUC+25) mg IV over 1hour Day 1 Interval between cycles: Repeat every 21 days Number of cycles: Patient Performance status 2, or poor renal function where local approval permits carboplatin substitution of cisplatin and where NICE TA181 would be used for 1st line treatment of patients with locally advanced or metastatic NSCLC only if the histology of the tumour has been confirmed as adenocarcinoma or large cell cell carcinoma up to 6 cycles NICE (TA124) does not recommend pemetrexed for NSCLC patients who have had prior chemotherapy - Tests before starting course of chemo FBC, U&Es, LFTs, CrCl calculated. Do
EDTA if <60ml/min Tests to OK/Confirm each cycle of chemo: FBC, U&Es, LFTs, CrCl calculated. Do EDTA if rising serum creatinine Supportive drugs with each cycle: High risk anti-emetics as per NWLCN guidelines or as per local policy
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 11 of 62
Dexamethasone as above to reduce the incidence and severity of skin reactions. Vitamin supplementation to reduce toxicity and incidence of grade 3/4 haematological and non-haematological toxicities Folic acid 400microgram oral daily, starting 7 days before 1st pemetrexed dose and continuing for 21days after last pemetrexed dose Vitamin B12 1000micrograms IM. first dose must be given one week before the 1st pemetrexed dose and then once every 3 cycles thereafter, (subsequent doses may be given on the same day as pemetrexed.
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Carboplatin starts 30minutes after the pemetrexed.
Hypersensitivity reaction Carboplatin Reactions may occur to carboplatin, see SPC information page 6 If any reaction occurs, stop infusion and discuss with consultant. If mild reaction; Consultant in charge may consider re-challenge with chlorphenamine 10mg IV and hydrocortisone 100mg IV cover. If moderate/severe reaction. Do not re-challenge and seek alternative treatment.
Dose modifications: See Pemetrexed/carbo table below Reference:
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 12 of 62
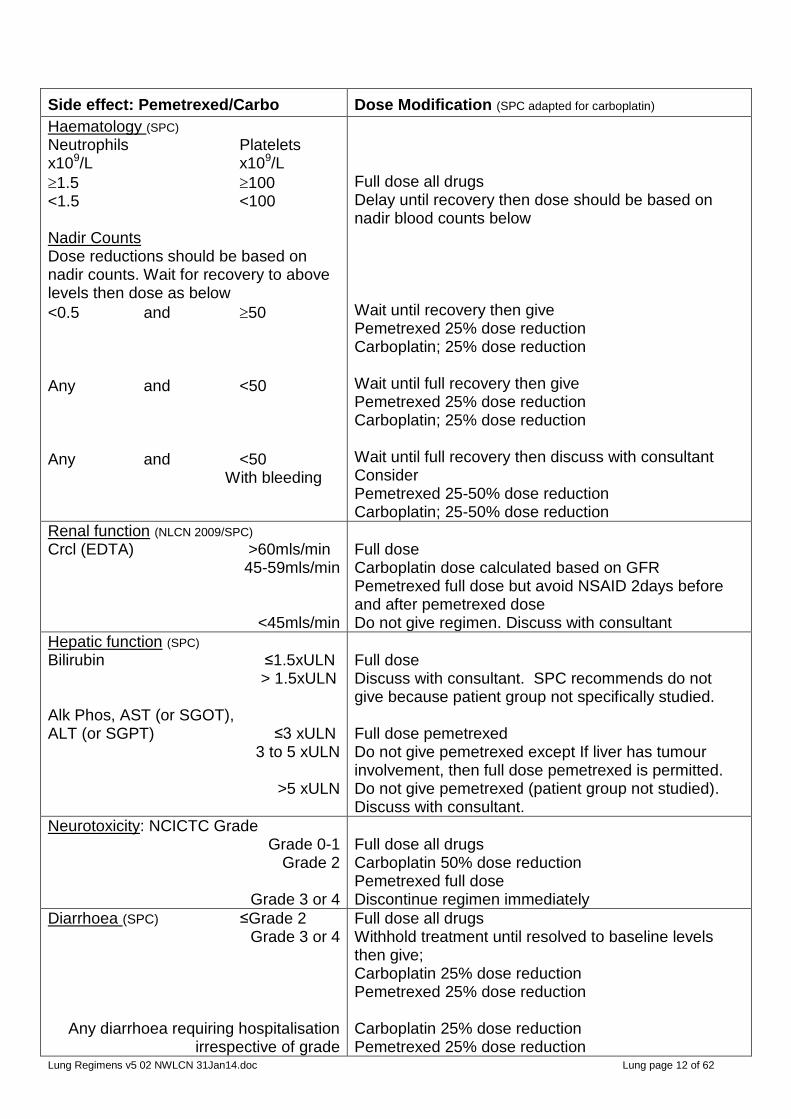
Side effect: Pemetrexed/Carbo
Dose Modification (SPC adapted for carboplatin)
Haematology (SPC)
Neutrophils Platelets x109/L x109/L
1.5 100 <1.5 <100 Nadir Counts Dose reductions should be based on nadir counts. Wait for recovery to above levels then dose as below
<0.5 and 50 Any and <50 Any and <50 With bleeding
Full dose all drugs Delay until recovery then dose should be based on nadir blood counts below Wait until recovery then give Pemetrexed 25% dose reduction Carboplatin; 25% dose reduction Wait until full recovery then give Pemetrexed 25% dose reduction Carboplatin; 25% dose reduction Wait until full recovery then discuss with consultant Consider Pemetrexed 25-50% dose reduction Carboplatin; 25-50% dose reduction
Renal function (NLCN 2009/SPC)
Crcl (EDTA) >60mls/min 45-59mls/min
<45mls/min
Full dose Carboplatin dose calculated based on GFR Pemetrexed full dose but avoid NSAID 2days before and after pemetrexed dose Do not give regimen. Discuss with consultant
Hepatic function (SPC)
Bilirubin ≤1.5xULN > 1.5xULN Alk Phos, AST (or SGOT), ALT (or SGPT) ≤3 xULN 3 to 5 xULN
>5 xULN
Full dose Discuss with consultant. SPC recommends do not give because patient group not specifically studied. Full dose pemetrexed Do not give pemetrexed except If liver has tumour involvement, then full dose pemetrexed is permitted. Do not give pemetrexed (patient group not studied). Discuss with consultant.
Neurotoxicity: NCICTC Grade Grade 0-1
Grade 2
Grade 3 or 4
Full dose all drugs Carboplatin 50% dose reduction Pemetrexed full dose Discontinue regimen immediately
Diarrhoea (SPC) ≤Grade 2 Grade 3 or 4
Any diarrhoea requiring hospitalisation
irrespective of grade
Full dose all drugs Withhold treatment until resolved to baseline levels then give; Carboplatin 25% dose reduction Pemetrexed 25% dose reduction Carboplatin 25% dose reduction Pemetrexed 25% dose reduction
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 13 of 62
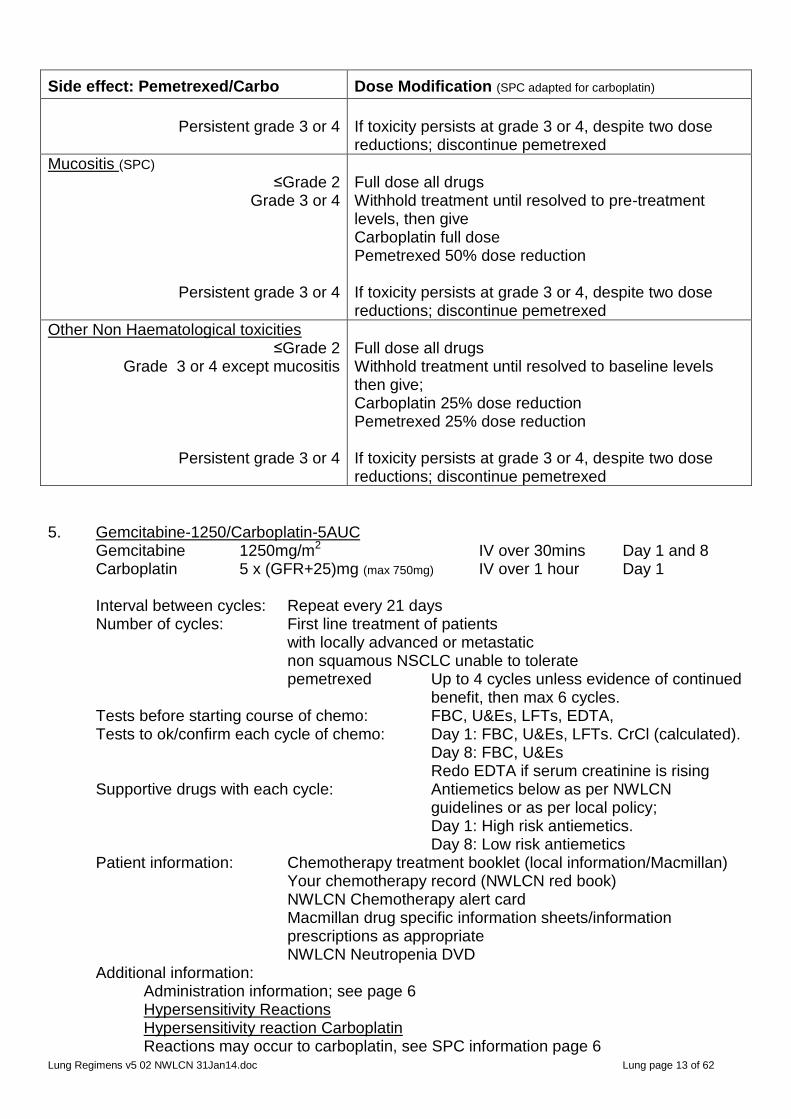
Side effect: Pemetrexed/Carbo
Dose Modification (SPC adapted for carboplatin)
Persistent grade 3 or 4
If toxicity persists at grade 3 or 4, despite two dose reductions; discontinue pemetrexed
Mucositis (SPC) ≤Grade 2
Grade 3 or 4
Persistent grade 3 or 4
Full dose all drugs Withhold treatment until resolved to pre-treatment levels, then give Carboplatin full dose Pemetrexed 50% dose reduction If toxicity persists at grade 3 or 4, despite two dose reductions; discontinue pemetrexed
Other Non Haematological toxicities ≤Grade 2
Grade 3 or 4 except mucositis
Persistent grade 3 or 4
Full dose all drugs Withhold treatment until resolved to baseline levels then give; Carboplatin 25% dose reduction Pemetrexed 25% dose reduction If toxicity persists at grade 3 or 4, despite two dose reductions; discontinue pemetrexed
5. Gemcitabine-1250/Carboplatin-5AUC Gemcitabine 1250mg/m2 IV over 30mins Day 1 and 8 Carboplatin 5 x (GFR+25)mg (max 750mg) IV over 1 hour Day 1 Interval between cycles: Repeat every 21 days Number of cycles: First line treatment of patients with locally advanced or metastatic non squamous NSCLC unable to tolerate pemetrexed Up to 4 cycles unless evidence of continued benefit, then max 6 cycles. Tests before starting course of chemo: FBC, U&Es, LFTs, EDTA, Tests to ok/confirm each cycle of chemo: Day 1: FBC, U&Es, LFTs. CrCl (calculated). Day 8: FBC, U&Es Redo EDTA if serum creatinine is rising Supportive drugs with each cycle: Antiemetics below as per NWLCN
guidelines or as per local policy; Day 1: High risk antiemetics. Day 8: Low risk antiemetics Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Administration information; see page 6 Hypersensitivity Reactions Hypersensitivity reaction Carboplatin Reactions may occur to carboplatin, see SPC information page 6

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 14 of 62
If any reaction occurs: stop infusion and discuss with consultant. If mild reaction; Consultant in charge may consider re-challenge with chlorphenamine 10mg IV and hydrocortisone 100mg IV cover. If moderate/severe reaction. Do not re-challenge and seek alternative treatment. Hypersensitivity reaction Gemcitabine Rash with gemcitabine; retreat with hydrocortisone 100mg IV cover.
Dose modifications: See table Gem/Carbo page 7 Reference: J. Chemother 2002;14(3):296-300 Tognoni A et al J. Clin Oncol 2005;23(1):142-153 Rudd RM et al 6. Paclitaxel-175/Carboplatin5AUC Dexamethasone* 20mg Oral 12 hours pre paclitaxel Day 1 Dexamethasone* 20mg Oral 3-6 hours pre paclitaxel Day 1 Ranitidine 50mg IV bolus 30-60mins pre-paclitaxel Day 1 Chlorphenamine 10mg IV bolus 30-60mins pre-paclitaxel Day 1 Paclitaxel 175mg/m2 IV over 3 hours Day 1 Carboplatin 5(GFR+25)mg IV over 1 hour Day 1 *Dexamethasone premed may be changed to a single dose dexamethasone 20mg IV bolus
30-60minutes pre paclitaxel Interval between cycles: Repeat every 21 days Number of cycles: After discussion with consultant for rarer histologies; 6 cycles. Tests before starting course of chemo: FBC, U&Es, LFTs, EDTA, Tests to ok/confirm each cycle of chemo: FBC, U&Es, LFTs. Creatinine clearance
(calculated). Redo EDTA if serum creatinine is rising
Supportive drugs with each cycle: High risk antiemetics as per NWLCN guidelines or as per local protocol
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Paclitaxel: must be administered via a PVC free giving set. Polyethylene lined paclitaxel giving set with inline filter <0.22microns will be provided by pharmacy if necessary. Paclitaxel is a vesicant and must be administered according to Trust administration policy. Ensure patient has received appropriate pre-medication to prevent hypersensitivity reaction. Acute hypersensitivity reactions can occur, observe closely especially during the first two cycles. Assess for any drug-induced neuropathy. Paclitaxel Hypersensitivity Reactions Paclitaxel may cause allergic reactions, see below for SPC information. If any reaction occurs: stop infusion and discuss with consultant. After discussion with consultant; Mild reactions eg rash; May consider re-challenge after discussion with consultant Severe reactions; Do not re-challenge, discuss with consultant Paclitaxel SPC Hospira 31 Nov 2010 Significant hypersensitivity reactions: As characterised by dyspnoea and hypotension requiring treatment, angioedema, and generalised urticaria have

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 15 of 62
occurred in <1% of patients receiving paclitaxel after adequate premedication. These reactions are probably histamine-mediated. In the case of severe hypersensitivity reactions, paclitaxel infusion should be discontinued immediately, symptomatic therapy should be initiated and the patient should not be rechallenged with paclitaxel. Macrogolglycerol ricinoleate (polyoxyl castor oil), an excipient in this medicinal product, can cause these reactions Care should be exercised if using another taxane. Carboplatin Hypersensitivity reactions Reactions may occur to carboplatin, see SPC information page 6 If any reaction occurs: stop infusion and discuss with consultant. If mild reaction; Consultant in charge may consider re-challenge with chlorphenamine 10mg IV and hydrocortisone 100mg IV cover. If moderate/severe reaction. Do not re-challenge and seek alternative treatment.
Dose modifications: Reference: J. Chemother 2002;14(3):296-300 Tognoni A et al J. Clin Oncol 2005;23(1):142-153 Rudd RM et al
Side-effect: Carbo/Taxol
Dose Modification
Neutrophils Platelets x109/L x109/L ≥1.5 and ≥100
1.0-1.4 and/or 75-99
<1.0 and/or <75
Carboplatin Full dose Delay 1 week until counts recovered then consider dose reduction Delay 1 week initially then subsequently 20% dose reduction
Paclitaxel Full dose Delay 1 week then Full dose Delay 1 week then 20% dose reduction
Neurotoxicity Grade 2
Full dose
20% dose reduction. If recurs after dose reduction, omit paclitaxel
Hepatic function (NLWN 2009)
Bilirubin <26 micromol/L 27-51 micromol/L
>51 micromol/L Severe liver impairment
Full dose Full dose Discuss with consultant Discuss with consultant
Give 135mg/m2 Give 75mg/m2 Discuss with consultant Omit paclitaxel
Renal function (NLWN 2009)
60ml/min 45-59mls/min
<45mls/min
Recalculate dose using standard formula Crcl <20mls/min DO NOT give carboplatin
Full dose Full dose Discuss with consultant

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 16 of 62
Locally Advanced CHEMO ALONE Locally advanced Squamous Cell Chemo Alone Regimens (Stage 3a-3b and inoperable stage 2) 7. Gemcitabine-1250/Carboplatin 5AUC Gemcitabine 1250mg/m2 IV over 30mins Day 1 and 8 Carboplatin 5 x (GFR+25)mg (max 750mg) IV over 1 hour Day 1 Interval between cycles: Repeat every 21 days Number of cycles: First line treatment of patients with locally advanced or metastatic squamous cell NSCLC Up to 6 cycles. Tests before starting course of chemo: FBC, U&Es, LFTs, EDTA, Tests to ok/confirm each cycle of chemo: Day 1: FBC, U&Es, LFTs. Crcl (calculated). Day 8: FBC, U&Es Redo EDTA if serum creatinine is rising Supportive drugs with each cycle: Antiemetics below as per NWLCN
guidelines or as per local protocol Day 1: High risk antiemetics Day 8: Low risk antiemetics Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Gemcitabine; Do not administer this regimen with concurrent radiotherapy. Gemcitabine must be administered over 30 minutes. In the case of injection site reaction (vein irritation) the infusion may be slowed down slightly but must not be infused over more than 60minutes. Prolonged infusion increases the treatment toxicity and should be avoided. Peripheral venous comfort may be increased with warming the arm with a heat pad. Gemcitabine Hypersensitivity reactions Rash with gemcitabine; retreat with hydrocortisone 100mg IV cover. Carboplatin Hypersensitivity reactions Reactions may occur to carboplatin, see SPC information page 6 If any reaction occurs: stop infusion and discuss with consultant. If mild reaction; Consultant in charge may consider re-challenge with chlorphenamine 10mg IV and hydrocortisone 100mg IV cover. If moderate/severe reaction. Do not re-challenge and seek alternative treatment.
Dose modifications: See table Gem/Carbo page 6 Reference: 8. Gemcitabine-1250/Cisplatin-80 Gemcitabine 1250mg/m2 IV over 30mins Day 1 and 8 Prehydrations Cisplatin 80mg/m2 IV over 1 hour Day 1 Post hydrations Interval between cycles: Repeat every 21 days Number of cycles: Locally advanced or metastatic

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 17 of 62
Squamous cell NSCLC Up to 6 cycles. Tests before starting course of chemo: FBC, U&Es, LFTs, EDTA, Tests to ok/confirm each cycle of chemo: Day 1; FBC, U&Es, LFTs. Crcl(calculated). Day 8; FBC, U&Es Redo EDTA if serum creatinine is rising Supportive drugs with each cycle: Antiemetics below as per NWLCN
guidelines or as per local policy Day 1: Very High risk antiemetics Day 8: Low risk antiemetics Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information Gemcitabine; Do not administer this regimen with concurrent radiotherapy. Gemcitabine must be administered over 30 minutes. In the case of injection site reaction (vein irritation) the infusion may be slowed down slightly but must not be infused over more than 60minutes. Prolonged infusion increases the treatment toxicity and should be avoided. Peripheral venous comfort may be increased with warming the arm with a heat pad. Gemcitabine Hypersensitivity reactions Rash with gemcitabine; retreat with hydrocortisone 100mg IV cover. Cisplatin Maintain fluid output over 100ml/hour during and for 6-8 hours after cisplatin administration. Alternatively, weigh patient prior to and after cisplatin infusion. If weight gain is greater than 2kg, or patient is symptomatic of fluid retention, contact medical team for diuretic. Encourage patients to drink 2-3 litres of fluid following cisplatin
Dose modifications: See Gem-Cisp below Reference
Side-effect Gem-Cisplatin Lung Dose Modification
Haematology Neutrophils x 109/L Platelets x109/L x109/L Day 1
1.5 and 100 <1.5 or <100 Day 8
1.0 100 <1.0 or <100
Full dose all drugs Delay until recovered then discuss with consultant either give full dose or consider gemcitabine 20% dose reduction Full dose gemcitabine Omit day 8 gemcitabine
Renal function (NLCN 2009)
Crcl (EDTA)
60mls/min 45-59mls/min
<45mls/min
Full dose Cisplatin 25% dose reduction. Gemcitabine full dose Do not give cisplatin. Discuss with consultant.

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 18 of 62
Side-effect Gem-Cisplatin Lung Dose Modification
Hepatic function (NLWN 2009)
Bilirubin <26 micromol/L 27-51 micromol/L
>51 micromol/L
Severe liver impairment
Full dose Full dose cisplatin Consider dose reduction for gemcitabine Discuss with consultant. Discuss with consultant.
Neurotoxicity ≥Grade 2
Discuss with consultant
9. Paclitaxel-175/Carboplatin 5AUC Dexamethasone* 20mg Oral 12 hours pre paclitaxel Day 1 Dexamethasone* 20mg Oral 3-6 hours pre paclitaxel Day 1 Ranitidine 50mg IV bolus 30-60mins pre-paclitaxel Day 1 Chlorphenamine 10mg IV bolus 30-60mins pre-paclitaxel Day 1 Paclitaxel 175mg/m2 IV over 3 hours Day 1 Carboplatin 5(GFR+25)mg IV over 1 hour Day 1 *Dexamethasone premed may be changed to a single dose dexamethasone 20mg IV bolus
30-60minutes pre paclitaxel Interval between cycles: Repeat every 21 days Number of cycles: Locally advanced or metastatic squamous cell NSCLC if gemcitabine intolerant and so unable to have Gem-Carbo 6 cycles. Tests before starting course of chemo: FBC, U&Es, LFTs, EDTA, Tests to ok/confirm each cycle of chemo: FBC, U&Es, LFTs. Creatinine clearance
(calculated). Redo EDTA if serum creatinine is rising
Supportive drugs with each cycle: High risk antiemetics as per NWLCN guidelines or as per local protocol
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Carboplatin Hypersensitivity reactions Reactions may occur to carboplatin, see SPC information page 6 If any reaction occurs: stop infusion and discuss with consultant. If mild reaction; Consultant in charge may consider re-challenge with chlorphenamine 10mg IV and hydrocortisone 100mg IV cover. If moderate/severe reaction. Do not re-challenge and seek alternative treatment.
Paclitaxel: See page 14 Paclitaxel Hypersensitivity Reactions Paclitaxel may cause allergic reactions, see below for SPC information. If any reaction occurs: stop infusion and discuss with consultant. After discussion with consultant; Mild reactions eg rash; May consider re-challenge after discussion with consultant

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 19 of 62
Severe reactions; Do not re-challenge, discuss with consultant Dose modifications: See Carbo-Taxol page 15 Reference
CHEMO-RADIATION REGIMENS
NSCLC Locally Advanced CHEMO-RADIATION
NSCLC Locally advanced NON Squamous Cell Chemo-Radiation Regimens (Stage 3a-3b and inoperable stage 2) 10. Etoposide-50/Cisplatin-50 Plus Radiotherapy Etoposide 50mg/m2 IV over 1 hour Days 1 to 5 and 29 to 33 Prehydration Days 1 and 8, 29 and 36 Cisplatin 50mg/m2 IV over 1 hour Days 1 and 8, 29 and 36 Post hydration Days 1 and 8, 29 and 36 Interval between cycles: 1 cycle only administer on days 1 to 5 and 29 to 33 of 6 weeks
of radiotherapy Number of cycles: 1 cycle during 6 weeks of radiotherapy Tests before starting course of chemo: FBC, U&Es, LFTs, CrCl calculated. If
<60ml/min do EDTA Tests to ok/confirm each cycle of chemo: Day 1: FBC, U&Es, LFTs, Crcl calculated., Day 8: FBC, U&Es, calculated CrCl Day 29: FBC, U&Es, LFTs, Crcl calculated., Day 33: FBC, U&Es, calculated CrCl Do EDTA if serum creatinine is rising Supportive drugs with each cycle Antiemetics below as per NWLCN
guidelines or as per local policy Day 1: High risk antiemetics Day 8: High risk antiemetics. Day 29: High risk antiemetics Day 33: High risk antiemetics. Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Dose modifications: See table page 20 Reference: PROCLAIM Trial
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 20 of 62
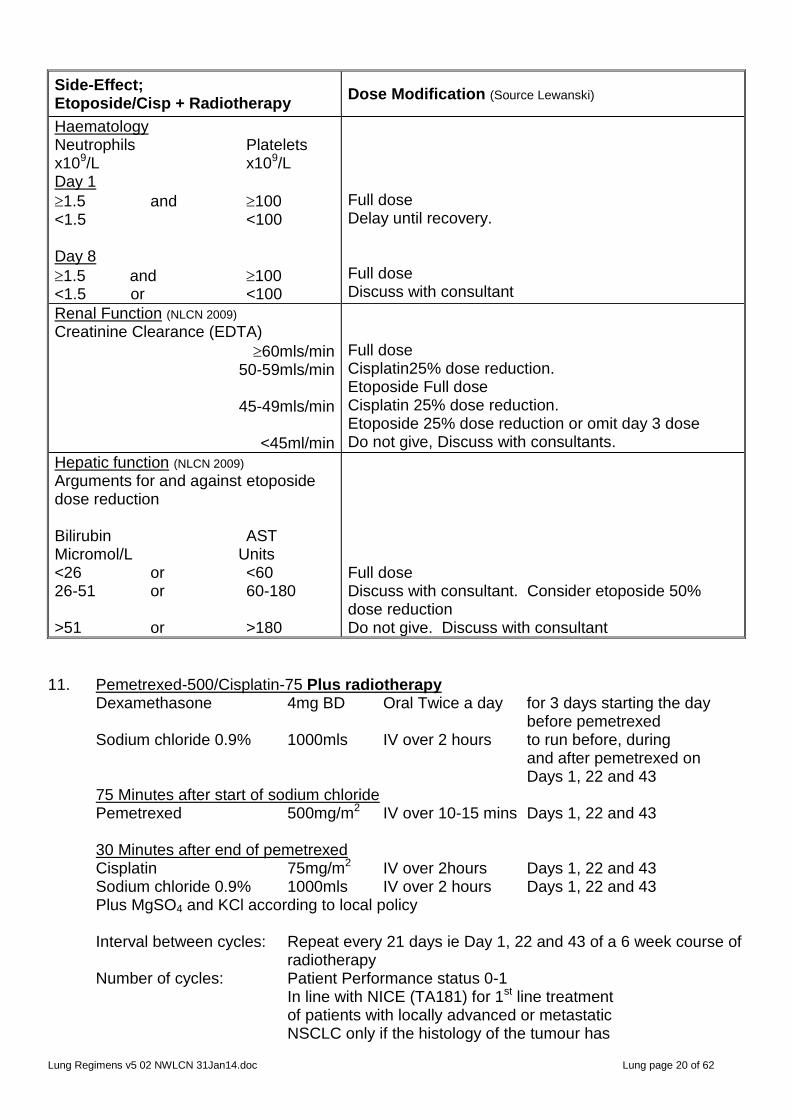
Side-Effect; Etoposide/Cisp + Radiotherapy
Dose Modification (Source Lewanski)
Haematology Neutrophils Platelets x109/L x109/L Day 1
1.5 and 100 <1.5 <100 Day 8
1.5 and 100 <1.5 or <100
Full dose Delay until recovery. Full dose Discuss with consultant
Renal Function (NLCN 2009)
Creatinine Clearance (EDTA)
60mls/min 50-59mls/min
45-49mls/min
<45ml/min
Full dose Cisplatin25% dose reduction. Etoposide Full dose Cisplatin 25% dose reduction. Etoposide 25% dose reduction or omit day 3 dose Do not give, Discuss with consultants.
Hepatic function (NLCN 2009)
Arguments for and against etoposide dose reduction Bilirubin AST Micromol/L Units <26 or <60 26-51 or 60-180 >51 or >180
Full dose Discuss with consultant. Consider etoposide 50% dose reduction Do not give. Discuss with consultant
11. Pemetrexed-500/Cisplatin-75 Plus radiotherapy Dexamethasone 4mg BD Oral Twice a day for 3 days starting the day before pemetrexed Sodium chloride 0.9% 1000mls IV over 2 hours to run before, during and after pemetrexed on Days 1, 22 and 43 75 Minutes after start of sodium chloride Pemetrexed 500mg/m2 IV over 10-15 mins Days 1, 22 and 43 30 Minutes after end of pemetrexed Cisplatin 75mg/m2 IV over 2hours Days 1, 22 and 43 Sodium chloride 0.9% 1000mls IV over 2 hours Days 1, 22 and 43 Plus MgSO4 and KCl according to local policy Interval between cycles: Repeat every 21 days ie Day 1, 22 and 43 of a 6 week course of
radiotherapy Number of cycles: Patient Performance status 0-1 In line with NICE (TA181) for 1st line treatment of patients with locally advanced or metastatic NSCLC only if the histology of the tumour has

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 21 of 62
been confirmed as adenocarcinoma or large usually 3 cycles cell carcinoma where radiotherapy also during 6 weeks administered during this chemo of radiotherapy NICE (TA124) does not recommend pemetrexed for NSCLC patients who have had prior chemotherapy - Tests before starting course of chemo FBC, U&Es, LFTs, CrCl calculated. Do
EDTA if <60ml/min Tests to OK/Confirm each cycle of chemo: Day 1: FBC, U&Es, LFTs, CrCl calculated. Day 22: FBC, U&Es, LFTs, CrCl calculated Day 43: FBC, U&Es, LFTs, CrCl calculated Do EDTA if rising serum creatinine Supportive drugs with each cycle: Anti-emetics below as per NWLCN guidelines or
as per local policy Day 1: Very High Risk antiemetics Day 22: Very High Risk antiemetics Day 43: Very High Risk antiemetics
Dexamethasone as above to reduce the incidence and severity of skin reactions. Vitamin supplementation to reduce toxicity and incidence of grade 3/4 haematological and non-haematological toxicities Folic acid 400microgram oral daily, starting 7 days before 1st pemetrexed dose and continuing for 21days after last pemetrexed dose Vitamin B12 1000micrograms IM. first dose must be given one week before the 1st pemetrexed dose and then once 9 weeks later (ie administer every 9 weeks with last dose given 3 weeks after last dose of pemetrexed).
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Sodium chloride is the pre-hydration for cisplatin. It should start approx. 75 minutes before pemetrexed and runs before, during and for 30minutes after the pemetrexed. Cisplatin must not start until 30minutes after the pemetrexed and the sodium chloride will keep the line patent whilst during this delay.
Dose modifications: See page 9 Reference:

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 22 of 62
NSCLC Locally Advanced CHEMO-RADIATION NSCLC Locally advanced Squamous Cell Chemo-Radiation Regimens (Stage 3a-3b and inoperable stage 2) 12. Etoposide-50/Cisplatin-50 Plus Radiotherapy Etoposide 50mg/m2 IV over 1 hour Days 1 to 5 and 29 to 33 Prehydration Days 1 and 8, 29 and 36 Cisplatin 50mg/m2 IV over 1 hour Days 1 and 8, 29 and 36 Post hydration Days 1 and 8, 29 and 36 Interval between cycles: Repeat once after 28 days, ie administer on days 1 to 5 and 29
to 33 of a 6 week course of radiotherapy Number of cycles: 1 cycle during 6 weeks of radiotherapy Tests before starting course of chemo: FBC, U&Es, LFTs, CrCl calculated. If
<60ml/min do EDTA Tests to ok/confirm each cycle of chemo: Day 1: FBC, U&Es, LFTs, Crcl calculated., Day 8: FBC, U&Es, calculated CrCl Day 29: FBC, U&Es, LFTs, Crcl calculated., Day 33: FBC, U&Es, calculated CrCl Do EDTA if serum creatinine is rising Supportive drugs with each cycle Antiemetics below as per NWLCN
guidelines or as per local policy Day 1: High risk antiemetics Day 8: High risk antiemetics. Day 29: High risk antiemetics Day 33: High risk antiemetics. Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Dose modifications: See table page 20 Reference:
Patients possessing EGFR Activating Mutations EGFR Related Skin Reactions General advice: Sun: Advise patient to avoid sun and use sun-block Dry Skin: Use oil for washing instead of soap Avoid hot water for baths/shower Topical corticosteroid creams NOT recommended
Fissures may occur in dry skin and topical dressings eg. hydrocolloid dressings as advised by dermatologist are helpful
Pruritis: Consider oral antihistamines Nail toxicity: Seek Dermatological advice Daily salt baths and local antiseptic/astringent ointments have been found to be helpful Anti-inflammatory drugs may help to ease the pain

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 23 of 62
First Line 13. Gefitinib-250 (Iressa) Gefitinib 250mg Oral once a day Continuous treatment Interval between cycles: Continuous treatment, repeat tests every 30 days initially, once
stabilised repeat tests every 2-3 months Number of cycles: In line with NICE (TA192) for 1st line treatment of patients with locally advanced or metastatic non small cell lung cancer if the patient tests positive for the epidermal growth factor receptor tyrosine kinase (EGFR-TK) AND gefitinib is provided at the fixed price under the patient access scheme (see additional information; Continue until no longer gaining clinical benefit Tests before starting course of chemo EGFR-TK status, FBC, U&Es, LFTs Tests to OK/Confirm each cycle of chemo: FBC, U&Es, LFTs initially with each cycle
once stabilised tests every 2-3 cycle Supportive drugs with each cycle: No routine medications Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD EGFR specific guidance of EGFR related skin reactions
Additional information (SPC): See SPC for list of drug interactions.
Swallow whole with or without food about the same time every day. See SPC for details of dispersing tablets in water.
If a dose of gefitinib is missed;
If it is more than 12 hours until the next dose, then it should be taken as soon as the patient remembers.
If it is less than 12 hours to the next dose, then the patient should not take the missed dose.
Patients should NOT take double dose (two doses at the same time) to make up for the forgotten dose.
NICE Information on patient access scheme The manufacturer has agreed with the Dept of Health a patient access scheme in which gefitinib for 1st line treatment of NSCLC will be available at a single fixed cost of £12,200 per patient irrespective of the duration of treatment. The manufacturer will not invoice the NHS until the 3rd monthly pack of gefitinib is supplied. This means that patients who need less than 3 months of treatment will not incur a charge. The Dept of Health considered that this patient access scheme does not constitute an excessive administrative burden on the NHS.
Each NHS patient must have
funding approved by the PCT before starting treatment
been registered and accepted by the manufacturer for the patient access scheme (SPA). This is done using the single payment access scheme patient registration form (Form 1) which is completed and sent to pharmacy.
a SPA order form completed for each cycle (pharmacy to complete)
only one cycle can be ordered at a time. Manufacturers guarantee that orders received by 12pm will be delivered the following day.
Reference: IPASS Study

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 24 of 62
IPASS data supports 1st line use in chemo naïve, never or light ex smokers, with adenocarcinoma, PS0-2, stage IIIB or IV Dose modifications: see table below
Side effect: Gefitinib (Iressa) Dose Modification (SPC)
Haematology (SPC) Neutrophils Platelets x109/L x109/L
1.5 100 <1.5 <100
Full dose Discuss with consultant
Renal function (SPC)
Crcl >20mls/min ≤20mls/min
Full dose Do not give regimen. Discuss with consultant
Hepatic function (SPC) Moderate to severe hepatic impairment (child Pugh B or C) due to cirrhosis have increased plasma concentration of gefitinib Elevated Aspartate Transaminases (AST), alkaline phosphate or bilirubin due to liver metastases did NOT have increase plasma levels of gefitinib.
Monitor closely for adverse events. No dose modification necessary.
Diarrhoea (SPC)
Patients with poorly tolerated diarrhoea adverse reactions, 1st occurrence
Repeat recurrence after break in therapy
Patients with poorly tolerated diarrhoea adverse reactions may be successfully managed by providing a brief (up to 14 days) therapy interruption followed by reinstatement of the 250mg dose If unable to tolerate treatment after a therapy interruption, gefitinib should be discontinued.
Skin Reactions (SPC) Patients with poorly tolerated skin adverse reactions, 1st occurrence
Repeat recurrence after break in therapy
Patients with poorly tolerated skin adverse reactions may be successfully managed by providing a brief (up to 14 days) therapy interruption followed by reinstatement of the 250mg dose If unable to tolerate treatment after a therapy interruption, gefitinib should be discontinued.
14. Erlotinib-150 Erlotinib 150mg Oral once a day continuous treatment Take at least 1 hour before or 2 hours after food Interval between cycles: Continuous treatment, repeat tests every 30 days initially, once stabilised repeat tests every 2-3 months Number of cycles: In line with NICE (TA258) as an option for 1st line treatment of locally advanced or metastatic NSCLC in EGFR positive patients using the Roche reimbursement program up to 6 cycles
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 25 of 62
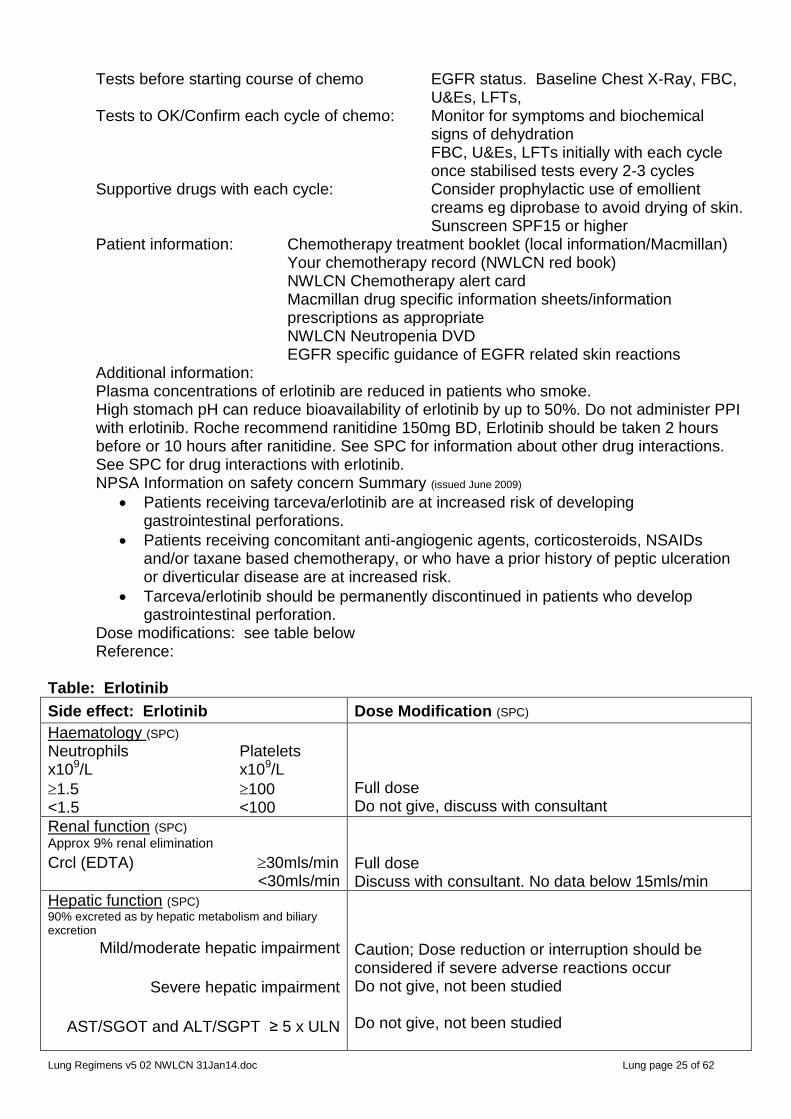
Tests before starting course of chemo EGFR status. Baseline Chest X-Ray, FBC, U&Es, LFTs,
Tests to OK/Confirm each cycle of chemo: Monitor for symptoms and biochemical signs of dehydration
FBC, U&Es, LFTs initially with each cycle once stabilised tests every 2-3 cycles
Supportive drugs with each cycle: Consider prophylactic use of emollient creams eg diprobase to avoid drying of skin.
Sunscreen SPF15 or higher Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD EGFR specific guidance of EGFR related skin reactions
Additional information: Plasma concentrations of erlotinib are reduced in patients who smoke.
High stomach pH can reduce bioavailability of erlotinib by up to 50%. Do not administer PPI with erlotinib. Roche recommend ranitidine 150mg BD, Erlotinib should be taken 2 hours before or 10 hours after ranitidine. See SPC for information about other drug interactions. See SPC for drug interactions with erlotinib.
NPSA Information on safety concern Summary (issued June 2009)
Patients receiving tarceva/erlotinib are at increased risk of developing gastrointestinal perforations.
Patients receiving concomitant anti-angiogenic agents, corticosteroids, NSAIDs and/or taxane based chemotherapy, or who have a prior history of peptic ulceration or diverticular disease are at increased risk.
Tarceva/erlotinib should be permanently discontinued in patients who develop gastrointestinal perforation.
Dose modifications: see table below Reference: Table: Erlotinib
Side effect: Erlotinib Dose Modification (SPC)
Haematology (SPC) Neutrophils Platelets x109/L x109/L
1.5 100 <1.5 <100
Full dose Do not give, discuss with consultant
Renal function (SPC)
Approx 9% renal elimination
Crcl (EDTA) 30mls/min <30mls/min
Full dose Discuss with consultant. No data below 15mls/min
Hepatic function (SPC)
90% excreted as by hepatic metabolism and biliary excretion
Mild/moderate hepatic impairment
Severe hepatic impairment
AST/SGOT and ALT/SGPT ≥ 5 x ULN
Caution; Dose reduction or interruption should be considered if severe adverse reactions occur Do not give, not been studied Do not give, not been studied
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 26 of 62
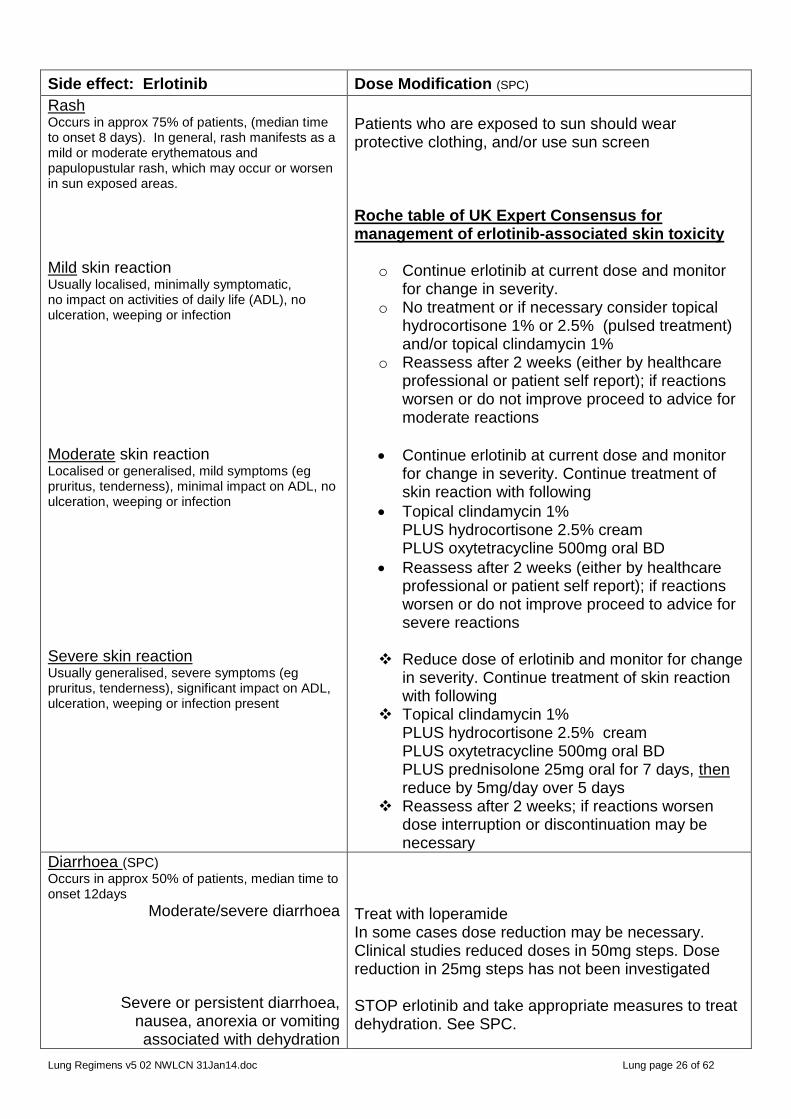
Side effect: Erlotinib Dose Modification (SPC)
Rash Occurs in approx 75% of patients, (median time to onset 8 days). In general, rash manifests as a mild or moderate erythematous and papulopustular rash, which may occur or worsen in sun exposed areas.
Mild skin reaction Usually localised, minimally symptomatic, no impact on activities of daily life (ADL), no ulceration, weeping or infection
Moderate skin reaction Localised or generalised, mild symptoms (eg pruritus, tenderness), minimal impact on ADL, no ulceration, weeping or infection
Severe skin reaction Usually generalised, severe symptoms (eg pruritus, tenderness), significant impact on ADL, ulceration, weeping or infection present
Patients who are exposed to sun should wear protective clothing, and/or use sun screen Roche table of UK Expert Consensus for management of erlotinib-associated skin toxicity
o Continue erlotinib at current dose and monitor for change in severity.
o No treatment or if necessary consider topical hydrocortisone 1% or 2.5% (pulsed treatment) and/or topical clindamycin 1%
o Reassess after 2 weeks (either by healthcare professional or patient self report); if reactions worsen or do not improve proceed to advice for moderate reactions
Continue erlotinib at current dose and monitor for change in severity. Continue treatment of skin reaction with following
Topical clindamycin 1% PLUS hydrocortisone 2.5% cream PLUS oxytetracycline 500mg oral BD
Reassess after 2 weeks (either by healthcare professional or patient self report); if reactions worsen or do not improve proceed to advice for severe reactions
Reduce dose of erlotinib and monitor for change
in severity. Continue treatment of skin reaction with following
Topical clindamycin 1% PLUS hydrocortisone 2.5% cream PLUS oxytetracycline 500mg oral BD PLUS prednisolone 25mg oral for 7 days, then reduce by 5mg/day over 5 days
Reassess after 2 weeks; if reactions worsen dose interruption or discontinuation may be necessary
Diarrhoea (SPC)
Occurs in approx 50% of patients, median time to onset 12days
Moderate/severe diarrhoea
Severe or persistent diarrhoea, nausea, anorexia or vomiting associated with dehydration
Treat with loperamide In some cases dose reduction may be necessary. Clinical studies reduced doses in 50mg steps. Dose reduction in 25mg steps has not been investigated STOP erlotinib and take appropriate measures to treat dehydration. See SPC.

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 27 of 62
Side effect: Erlotinib Dose Modification (SPC)
Gastrointestinal perforation Permanently Discontinue erlotinib
Interstitial lung disease (ILD)-like events (SPC) ILD-like events, including fatalities, have been reported uncommonly in patients receiving erlotinib.
If patient develops acute onset of new and/or progressive unexplained pulmonary symptoms such as dyspnoea, cough and fever, interrupt erlotinib therapy pending diagnostic evaluation. If ILD is diagnosed discontinue erlotinib.
15. Afatinib (Giotrif) Additional Private Care Only Afatinib 40mg Oral Once a day Days 1 to 28
A dose escalation to a maximum dose of afatinib 50mg/day may be considered in patients who tolerate 40mg/day without diarrhoea, skin rash, stomatitis or any other adverse reaction with CTCAE > grade 1 in the first 3 weeks The dose should NOT be escalated in any patient with a prior dose reduction. Do not exceed 50mg/day Interval between cycles: Repeat every 28 days (ie. continuous treatment) Number of cycles: For Additional Private Care Only for monotherapy for the treatment of EGFR TKI-naïve patients with locally advanced Or metastatic NSCLC with activating EGFR mutations. Continue until progression or until no longer tolerated Tests before starting course of chemo: EGFR mutation status using a well
validated and robust methodology. FBC, U&Es, LFTs
For patients with cardiac risk factors see SPC for additional baseline tests/assessments
Tests to OK/Confirm each cycle of chemo: FBC. U&Es, LFTs Supportive drugs with each cycle: No routine medications. All patients should be
given a supply of loperamide in anticipation of diarrhoea. SPC states 95% experience grade ≥1 diarrhoea
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD EGFR skin reaction advice Patient must be counselled on sunscreen and protective clothing Patient must be counselled on adequate hydration and use of loperamide should diarrhoea develop and how to contact the hospital if diarrhoea is severe
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 28 of 62
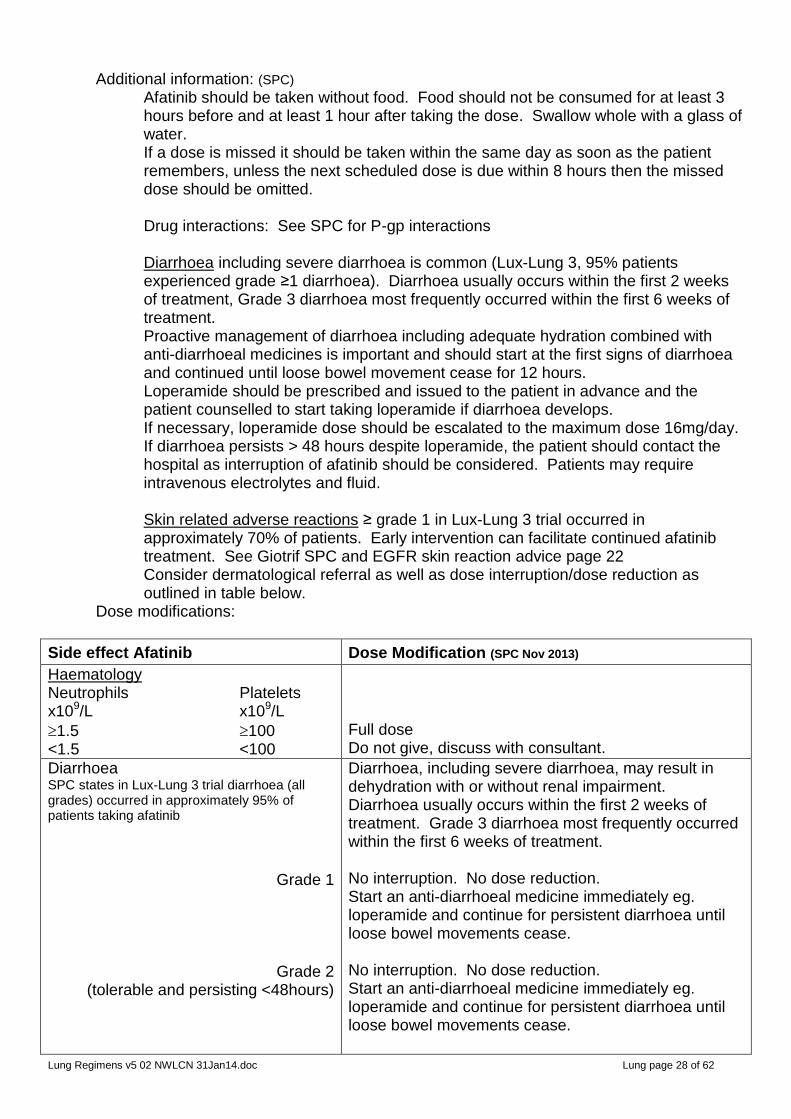
Additional information: (SPC) Afatinib should be taken without food. Food should not be consumed for at least 3 hours before and at least 1 hour after taking the dose. Swallow whole with a glass of water. If a dose is missed it should be taken within the same day as soon as the patient remembers, unless the next scheduled dose is due within 8 hours then the missed dose should be omitted. Drug interactions: See SPC for P-gp interactions Diarrhoea including severe diarrhoea is common (Lux-Lung 3, 95% patients experienced grade ≥1 diarrhoea). Diarrhoea usually occurs within the first 2 weeks of treatment, Grade 3 diarrhoea most frequently occurred within the first 6 weeks of treatment. Proactive management of diarrhoea including adequate hydration combined with anti-diarrhoeal medicines is important and should start at the first signs of diarrhoea and continued until loose bowel movement cease for 12 hours. Loperamide should be prescribed and issued to the patient in advance and the patient counselled to start taking loperamide if diarrhoea develops. If necessary, loperamide dose should be escalated to the maximum dose 16mg/day. If diarrhoea persists > 48 hours despite loperamide, the patient should contact the hospital as interruption of afatinib should be considered. Patients may require intravenous electrolytes and fluid. Skin related adverse reactions ≥ grade 1 in Lux-Lung 3 trial occurred in approximately 70% of patients. Early intervention can facilitate continued afatinib treatment. See Giotrif SPC and EGFR skin reaction advice page 22 Consider dermatological referral as well as dose interruption/dose reduction as outlined in table below.
Dose modifications:
Side effect Afatinib Dose Modification (SPC Nov 2013)
Haematology Neutrophils Platelets x109/L x109/L
1.5 100 <1.5 <100
Full dose Do not give, discuss with consultant.
Diarrhoea SPC states in Lux-Lung 3 trial diarrhoea (all grades) occurred in approximately 95% of patients taking afatinib
Grade 1
Grade 2 (tolerable and persisting <48hours)
Diarrhoea, including severe diarrhoea, may result in dehydration with or without renal impairment. Diarrhoea usually occurs within the first 2 weeks of treatment. Grade 3 diarrhoea most frequently occurred within the first 6 weeks of treatment. No interruption. No dose reduction. Start an anti-diarrhoeal medicine immediately eg. loperamide and continue for persistent diarrhoea until loose bowel movements cease. No interruption. No dose reduction. Start an anti-diarrhoeal medicine immediately eg. loperamide and continue for persistent diarrhoea until loose bowel movements cease.

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 29 of 62
Side effect Afatinib Dose Modification (SPC Nov 2013)
Grade 2 persisting 48 hours or intolerable
Grade 2 Repeat occurrence >48 hours or intolerable
≥ Grade 3
If grade 2 diarrhoea persists for more than 48 hours: Interrupt afatinib treatment until diarrhoea resolved to grade 0/1. Once resolved afatinib may be resumed with a dose reduction of 10mg Interrupt until resolved to grade 0/1. Once resolved and if treatment is to be resumed reduce dose by a further 10mg. If repeated dose reductions are necessary and the dose is reduced to 20mg/day and the patient is unable to tolerate 20mg/day, consider permanent discontinuation of afatinib. Interrupt treatment until diarrhoea resolved to grade 0/1. Once resolved, resume treatment with a dose reduction of 10mg. If repeated dose reductions are necessary and the dose is reduced to 20mg/day and the patient is unable to tolerate 20mg/day, consider permanent discontinuation of afatinib.
Rash SPC states in Lux-Lung 3 trial rash (all grades) occurred in approximately 70% of patients taking afatinib.
Grade 1 or Grade 2
Grade 2 persisting >7 days or intolerable
≥ Grade 3
NB. Bulbous, blistering and exfoliative skin conditions have been reported, including rare cases suggestive of Stevens-Johnson syndrome
No interruption, no dose reduction Consider emollients – see general EGFR skin advice. Interrupt afatinib until resolved to grade 0/1. Once resolved resume with dose reduction of 10mg/day. If repeated dose reduction are necessary and the dose is reduced to 20mg/day and the patient is unable to tolerate 20mg/day, consider permanent discontinuation of afatinib. Interrupt afatinib until resolved to grade 0/1. Once resolved resume with dose reduction of 10mg/day. If repeated dose reduction are necessary and the dose is reduced to 20mg/day and the patient is unable to tolerate 20mg/day, consider permanent discontinuation of afatinib. Discontinue afatinib. See SPC for further information and refer for dermatological advice urgently.
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 30 of 62
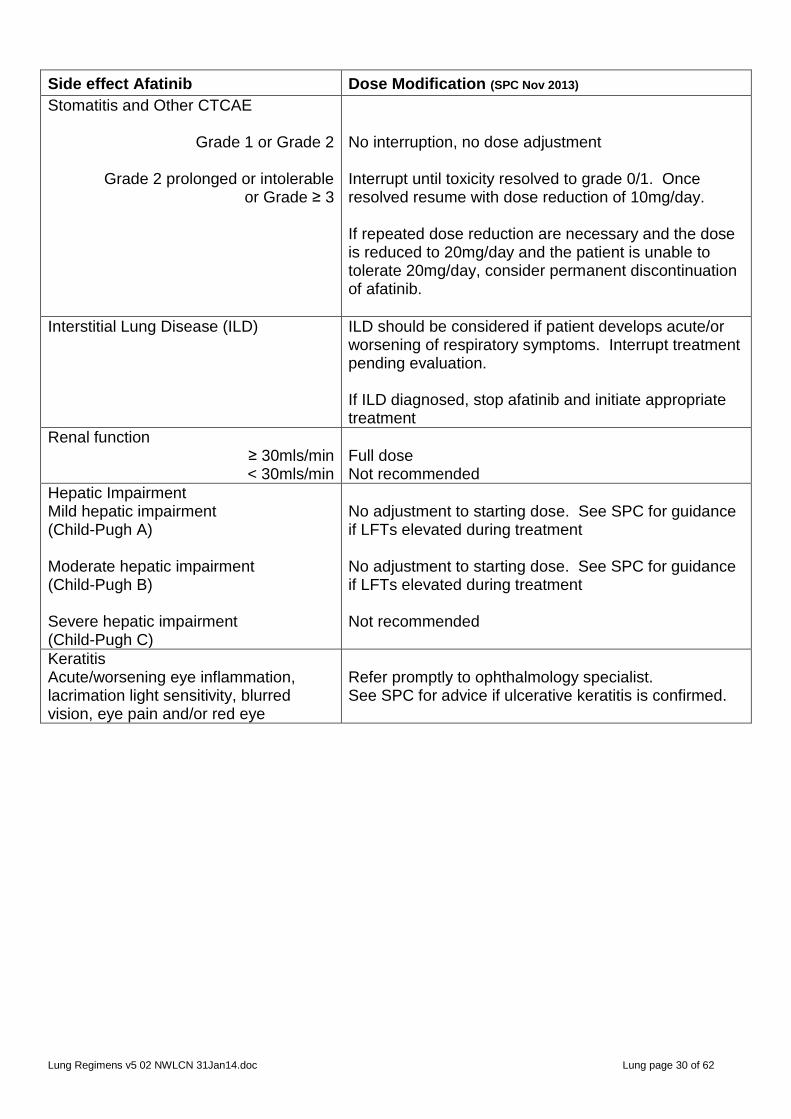
Side effect Afatinib Dose Modification (SPC Nov 2013)
Stomatitis and Other CTCAE
Grade 1 or Grade 2
Grade 2 prolonged or intolerable or Grade ≥ 3
No interruption, no dose adjustment Interrupt until toxicity resolved to grade 0/1. Once resolved resume with dose reduction of 10mg/day. If repeated dose reduction are necessary and the dose is reduced to 20mg/day and the patient is unable to tolerate 20mg/day, consider permanent discontinuation of afatinib.
Interstitial Lung Disease (ILD) ILD should be considered if patient develops acute/or worsening of respiratory symptoms. Interrupt treatment pending evaluation. If ILD diagnosed, stop afatinib and initiate appropriate treatment
Renal function ≥ 30mls/min < 30mls/min
Full dose Not recommended
Hepatic Impairment Mild hepatic impairment (Child-Pugh A) Moderate hepatic impairment (Child-Pugh B) Severe hepatic impairment (Child-Pugh C)
No adjustment to starting dose. See SPC for guidance if LFTs elevated during treatment No adjustment to starting dose. See SPC for guidance if LFTs elevated during treatment Not recommended
Keratitis Acute/worsening eye inflammation, lacrimation light sensitivity, blurred vision, eye pain and/or red eye
Refer promptly to ophthalmology specialist. See SPC for advice if ulcerative keratitis is confirmed.
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 31 of 62
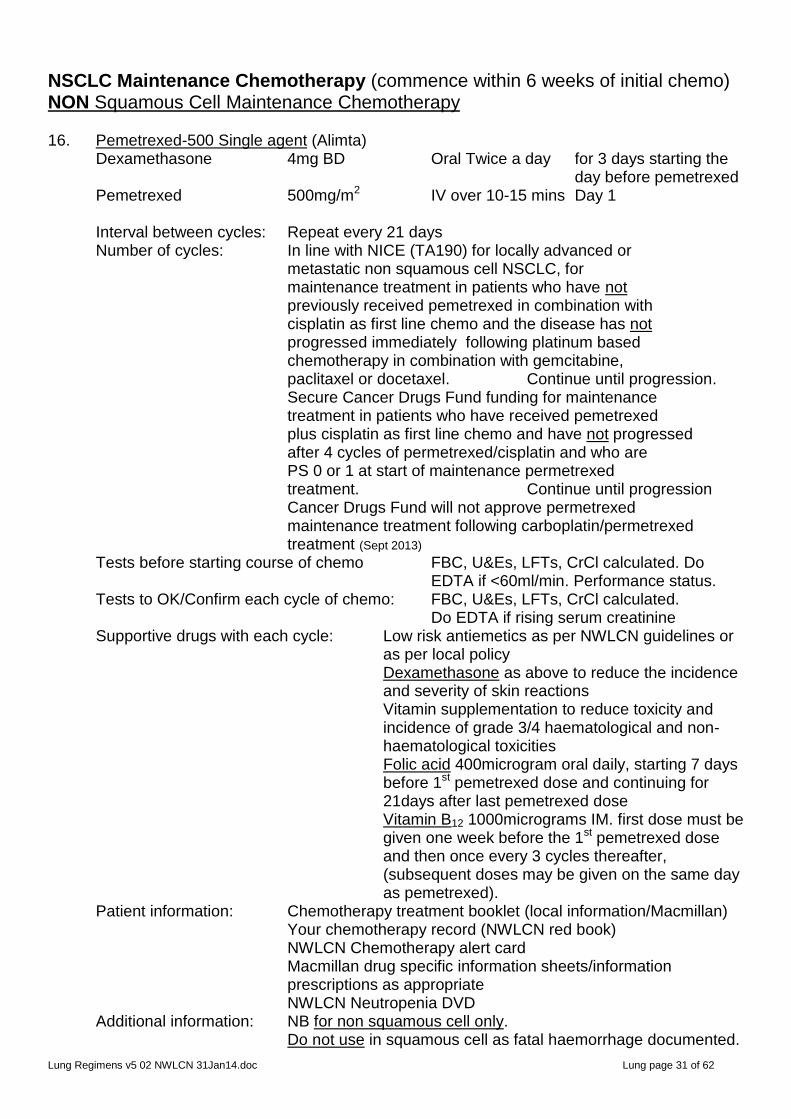
NSCLC Maintenance Chemotherapy (commence within 6 weeks of initial chemo) NON Squamous Cell Maintenance Chemotherapy 16. Pemetrexed-500 Single agent (Alimta) Dexamethasone 4mg BD Oral Twice a day for 3 days starting the day before pemetrexed Pemetrexed 500mg/m2 IV over 10-15 mins Day 1 Interval between cycles: Repeat every 21 days Number of cycles: In line with NICE (TA190) for locally advanced or
metastatic non squamous cell NSCLC, for maintenance treatment in patients who have not previously received pemetrexed in combination with cisplatin as first line chemo and the disease has not progressed immediately following platinum based chemotherapy in combination with gemcitabine, paclitaxel or docetaxel. Continue until progression. Secure Cancer Drugs Fund funding for maintenance treatment in patients who have received pemetrexed plus cisplatin as first line chemo and have not progressed after 4 cycles of permetrexed/cisplatin and who are PS 0 or 1 at start of maintenance permetrexed treatment. Continue until progression Cancer Drugs Fund will not approve permetrexed maintenance treatment following carboplatin/permetrexed treatment (Sept 2013)
Tests before starting course of chemo FBC, U&Es, LFTs, CrCl calculated. Do EDTA if <60ml/min. Performance status.
Tests to OK/Confirm each cycle of chemo: FBC, U&Es, LFTs, CrCl calculated. Do EDTA if rising serum creatinine Supportive drugs with each cycle: Low risk antiemetics as per NWLCN guidelines or
as per local policy Dexamethasone as above to reduce the incidence and severity of skin reactions
Vitamin supplementation to reduce toxicity and incidence of grade 3/4 haematological and non-haematological toxicities Folic acid 400microgram oral daily, starting 7 days before 1st pemetrexed dose and continuing for 21days after last pemetrexed dose Vitamin B12 1000micrograms IM. first dose must be given one week before the 1st pemetrexed dose and then once every 3 cycles thereafter, (subsequent doses may be given on the same day as pemetrexed).
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: NB for non squamous cell only. Do not use in squamous cell as fatal haemorrhage documented.
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 32 of 62
Refer to company for info on reimbursement plan. Dose modifications: See table below Reference: www.nice.org.uk/guidanceTA190
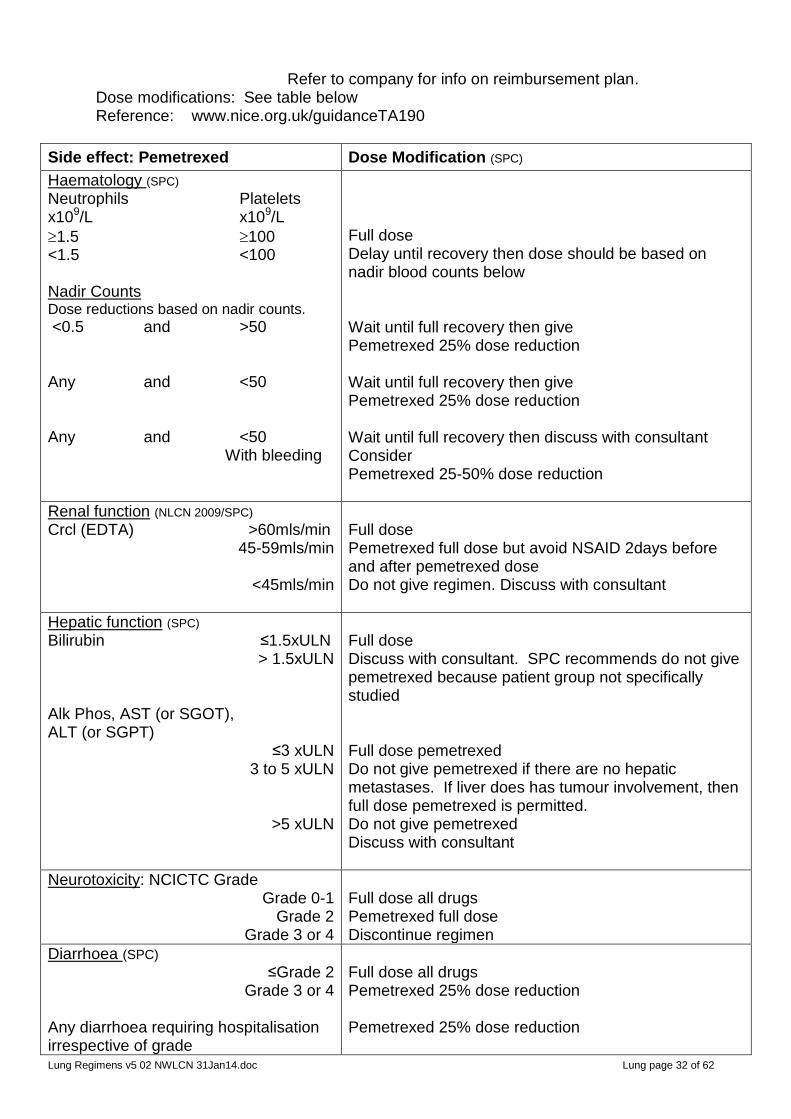
Side effect: Pemetrexed Dose Modification (SPC)
Haematology (SPC) Neutrophils Platelets x109/L x109/L
1.5 100 <1.5 <100 Nadir Counts Dose reductions based on nadir counts.
<0.5 and >50 Any and <50 Any and <50 With bleeding
Full dose Delay until recovery then dose should be based on nadir blood counts below Wait until full recovery then give Pemetrexed 25% dose reduction Wait until full recovery then give Pemetrexed 25% dose reduction Wait until full recovery then discuss with consultant Consider Pemetrexed 25-50% dose reduction
Renal function (NLCN 2009/SPC)
Crcl (EDTA) >60mls/min 45-59mls/min
<45mls/min
Full dose Pemetrexed full dose but avoid NSAID 2days before and after pemetrexed dose Do not give regimen. Discuss with consultant
Hepatic function (SPC)
Bilirubin ≤1.5xULN > 1.5xULN
Alk Phos, AST (or SGOT), ALT (or SGPT)
≤3 xULN 3 to 5 xULN
>5 xULN
Full dose Discuss with consultant. SPC recommends do not give pemetrexed because patient group not specifically studied Full dose pemetrexed Do not give pemetrexed if there are no hepatic metastases. If liver does has tumour involvement, then full dose pemetrexed is permitted. Do not give pemetrexed Discuss with consultant
Neurotoxicity: NCICTC Grade Grade 0-1
Grade 2 Grade 3 or 4
Full dose all drugs Pemetrexed full dose Discontinue regimen
Diarrhoea (SPC)
≤Grade 2 Grade 3 or 4
Any diarrhoea requiring hospitalisation irrespective of grade
Full dose all drugs Pemetrexed 25% dose reduction Pemetrexed 25% dose reduction

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 33 of 62
Side effect: Pemetrexed Dose Modification (SPC)
Mucositis (SPC) ≤Grade 2
Grade 3 or 4
Persistent grade 3 or 4
Full dose all drugs Withhold treatment until resolved to pre-treatment levels, then give Pemetrexed 50% dose reduction If toxicity persists at grade 3 or 4, despite two dose reductions; discontinue pemetrexed
Other Non Haematological toxicities ≤Grade 2
Grade 3 or 4 except mucositis
Full dose all drugs Pemetrexed 25% dose reduction
17. Erlotinib-150 (Tarceva) For Additional Private Care only (not recommended by NICE TA227 June 2011 NOT Cancer Drug funded) Erlotinib 150mg Oral once a day continuous treatment Take at least 1 hour before or 2 hours after food Interval between cycles: Continuous treatment. Repeat tests every 30 days initially, once
stabilised test may be repeated every 2-3 months Number of cycles: Monotherapy for maintenance treatment of patients with locally advanced or metastatic NSCLC with stable disease after 4 cycles of platinum based first line chemotherapy. Until disease progression Tests before starting course of chemo Baseline Chest X-Ray, FBC, U&Es, LFTs, Tests to OK/Confirm each cycle of chemo: Monitor for symptoms and biochemical
signs of dehydration FBC, U&Es, LFTs initially with each cycle
once stabilised tests every 2-3 cycles Supportive drugs with each cycle: Consider prophylactic use of emollient
creams eg diprobase to avoid drying of skin. Sunscreen SPF15 or higher Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Plasma concentrations of erlotinib are reduced in patients who smoke.
High stomach pH can reduce bioavailability of erlotinib by up to 50%. Do not administer PPI with erlotinib. Roche recommend ranitidine 150mg BD, Erlotinib should be taken 2 hours before or 10 hours after ranitidine. See SPC for information about other drug interactions
NPSA Information on safety concern Summary (issued June 2009)
Patients receiving tarceva/erlotinib are at increased risk of developing gastrointestinal perforations.
Patients receiving concomitant anti-angiogenic agents, corticosteroids, NSAIDs and/or taxane based chemotherapy, or who have a prior history of peptic ulceration or diverticular disease are at increased risk.
Tarceva/erlotinib should be permanently discontinued in patients who develop gastrointestinal perforation
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 34 of 62
Dose modifications: See table page 25 Reference: BO18192, SATURN Trial
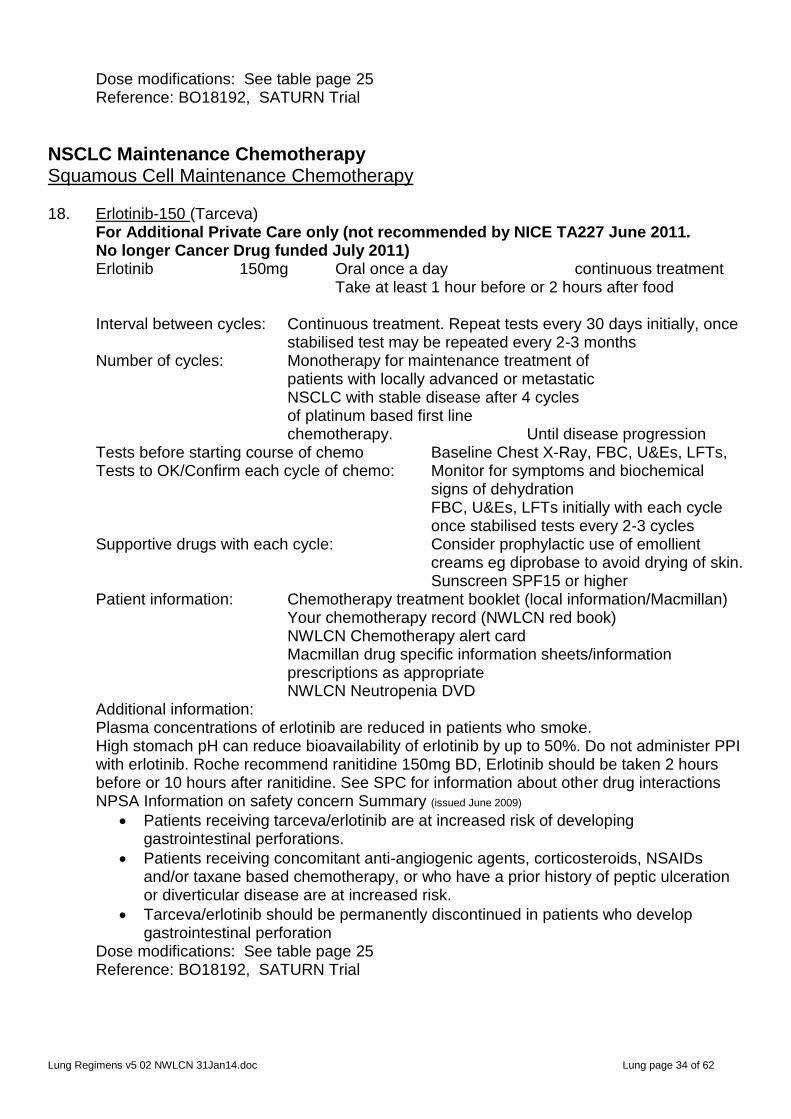
NSCLC Maintenance Chemotherapy Squamous Cell Maintenance Chemotherapy 18. Erlotinib-150 (Tarceva) For Additional Private Care only (not recommended by NICE TA227 June 2011. No longer Cancer Drug funded July 2011) Erlotinib 150mg Oral once a day continuous treatment Take at least 1 hour before or 2 hours after food Interval between cycles: Continuous treatment. Repeat tests every 30 days initially, once
stabilised test may be repeated every 2-3 months Number of cycles: Monotherapy for maintenance treatment of patients with locally advanced or metastatic NSCLC with stable disease after 4 cycles of platinum based first line chemotherapy. Until disease progression Tests before starting course of chemo Baseline Chest X-Ray, FBC, U&Es, LFTs, Tests to OK/Confirm each cycle of chemo: Monitor for symptoms and biochemical
signs of dehydration FBC, U&Es, LFTs initially with each cycle
once stabilised tests every 2-3 cycles Supportive drugs with each cycle: Consider prophylactic use of emollient
creams eg diprobase to avoid drying of skin. Sunscreen SPF15 or higher Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Plasma concentrations of erlotinib are reduced in patients who smoke.
High stomach pH can reduce bioavailability of erlotinib by up to 50%. Do not administer PPI with erlotinib. Roche recommend ranitidine 150mg BD, Erlotinib should be taken 2 hours before or 10 hours after ranitidine. See SPC for information about other drug interactions
NPSA Information on safety concern Summary (issued June 2009)
Patients receiving tarceva/erlotinib are at increased risk of developing gastrointestinal perforations.
Patients receiving concomitant anti-angiogenic agents, corticosteroids, NSAIDs and/or taxane based chemotherapy, or who have a prior history of peptic ulceration or diverticular disease are at increased risk.
Tarceva/erlotinib should be permanently discontinued in patients who develop gastrointestinal perforation
Dose modifications: See table page 25 Reference: BO18192, SATURN Trial
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 35 of 62
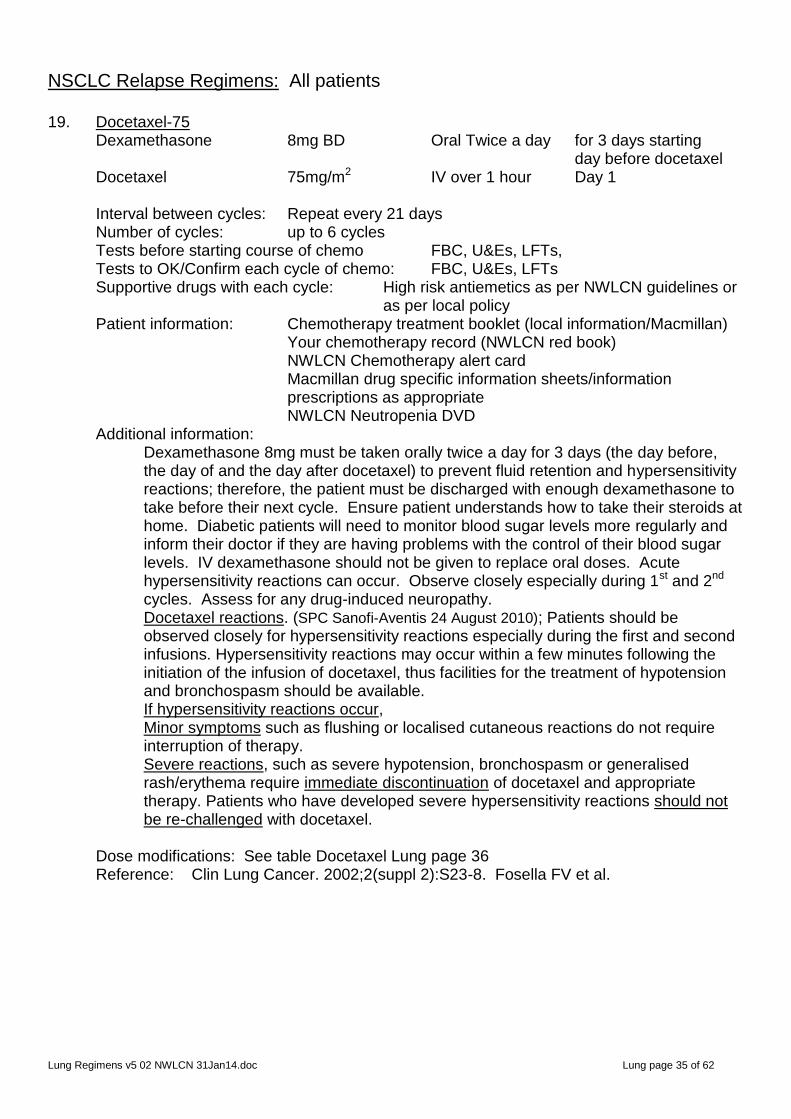
NSCLC Relapse Regimens: All patients 19. Docetaxel-75 Dexamethasone 8mg BD Oral Twice a day for 3 days starting day before docetaxel Docetaxel 75mg/m2 IV over 1 hour Day 1 Interval between cycles: Repeat every 21 days Number of cycles: up to 6 cycles Tests before starting course of chemo FBC, U&Es, LFTs, Tests to OK/Confirm each cycle of chemo: FBC, U&Es, LFTs Supportive drugs with each cycle: High risk antiemetics as per NWLCN guidelines or
as per local policy Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Dexamethasone 8mg must be taken orally twice a day for 3 days (the day before, the day of and the day after docetaxel) to prevent fluid retention and hypersensitivity reactions; therefore, the patient must be discharged with enough dexamethasone to take before their next cycle. Ensure patient understands how to take their steroids at home. Diabetic patients will need to monitor blood sugar levels more regularly and inform their doctor if they are having problems with the control of their blood sugar levels. IV dexamethasone should not be given to replace oral doses. Acute hypersensitivity reactions can occur. Observe closely especially during 1st and 2nd cycles. Assess for any drug-induced neuropathy. Docetaxel reactions. (SPC Sanofi-Aventis 24 August 2010); Patients should be observed closely for hypersensitivity reactions especially during the first and second infusions. Hypersensitivity reactions may occur within a few minutes following the initiation of the infusion of docetaxel, thus facilities for the treatment of hypotension and bronchospasm should be available. If hypersensitivity reactions occur, Minor symptoms such as flushing or localised cutaneous reactions do not require interruption of therapy. Severe reactions, such as severe hypotension, bronchospasm or generalised rash/erythema require immediate discontinuation of docetaxel and appropriate therapy. Patients who have developed severe hypersensitivity reactions should not be re-challenged with docetaxel.
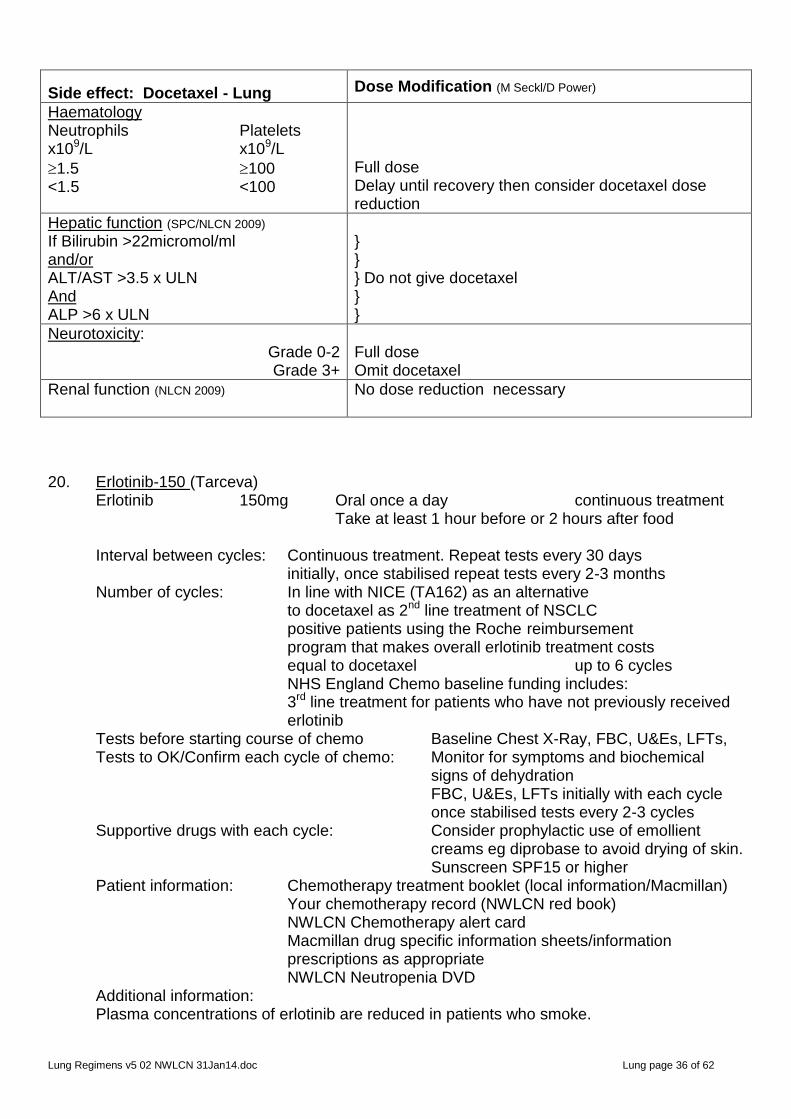
Dose modifications: See table Docetaxel Lung page 36 Reference: Clin Lung Cancer. 2002;2(suppl 2):S23-8. Fosella FV et al.
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 36 of 62
Side effect: Docetaxel - Lung
Dose Modification (M Seckl/D Power)
Haematology Neutrophils Platelets x109/L x109/L
1.5 100 <1.5 <100
Full dose Delay until recovery then consider docetaxel dose reduction
Hepatic function (SPC/NLCN 2009)
If Bilirubin >22micromol/ml and/or ALT/AST >3.5 x ULN And ALP >6 x ULN
} } } Do not give docetaxel } }
Neurotoxicity: Grade 0-2 Grade 3+
Full dose Omit docetaxel
Renal function (NLCN 2009) No dose reduction necessary
20. Erlotinib-150 (Tarceva) Erlotinib 150mg Oral once a day continuous treatment Take at least 1 hour before or 2 hours after food Interval between cycles: Continuous treatment. Repeat tests every 30 days initially, once stabilised repeat tests every 2-3 months Number of cycles: In line with NICE (TA162) as an alternative to docetaxel as 2nd line treatment of NSCLC positive patients using the Roche reimbursement program that makes overall erlotinib treatment costs equal to docetaxel up to 6 cycles NHS England Chemo baseline funding includes: 3rd line treatment for patients who have not previously received
erlotinib Tests before starting course of chemo Baseline Chest X-Ray, FBC, U&Es, LFTs, Tests to OK/Confirm each cycle of chemo: Monitor for symptoms and biochemical
signs of dehydration FBC, U&Es, LFTs initially with each cycle
once stabilised tests every 2-3 cycles Supportive drugs with each cycle: Consider prophylactic use of emollient
creams eg diprobase to avoid drying of skin. Sunscreen SPF15 or higher Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Plasma concentrations of erlotinib are reduced in patients who smoke.

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 37 of 62
High stomach pH can reduce bioavailability of erlotinib by up to 50%. Do not administer PPI with erlotinib. Roche recommend ranitidine 150mg BD, Erlotinib should be taken 2 hours before or 10 hours after ranitidine. See SPC for information about other drug interactions
NPSA Information on safety concern Summary (issued June 2009)
Patients receiving tarceva/erlotinib are at increased risk of developing gastrointestinal perforations.
Patients receiving concomitant anti-angiogenic agents, corticosteroids, NSAIDs and/or taxane based chemotherapy, or who have a prior history of peptic ulceration or diverticular disease are at increased risk.
Tarceva/erlotinib should be permanently discontinued in patients who develop gastrointestinal perforation
Dose modifications: See table page 25 Reference:
NSCLC Relapse Regimens: Non Squamous NSCLC only 21. Pemetrexed Single agent (Alimta) Secure Cancer Drugs Funding before commencing treatment Dexamethasone 4mg BD Oral Twice a day for 3 days starting the day before pemetrexed Pemetrexed 500mg/m2 IV over 10-15 mins Day 1 Interval between cycles: Repeat every 21 days Number of cycles: Secure Cancer Drugs Fund funding for 2nd line treatment of advanced or metastatic NON squamous NSCLC, if patient has not received previous pemetrexed, up to 6 cycles Tests before starting course of chemo FBC, U&Es, LFTs, CrCl calculated. Do
EDTA if <60ml/min Tests to OK/Confirm each cycle of chemo: FBC, U&Es, LFTs, CrCl calculated. Do EDTA if rising serum creatinine Supportive drugs with each cycle: Low risk anti-emetics as per NWLCN guidelines or as per local policy
Dexamethasone as above to reduce the incidence and severity of skin reactions
Vitamin supplementation to reduce toxicity and incidence of grade 3/4 haematological and non-haematological toxicities Folic acid 400microgram oral daily, starting 7 days before 1st pemetrexed dose and continuing for 21days after last pemetrexed dose Vitamin B12 1000micrograms IM. first dose must be given one week before the 1st pemetrexed dose and then once every 3 cycles thereafter, (subsequent doses may be given on the same day as pemetrexed).
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 38 of 62
NWLCN Neutropenia DVD
Additional information: NB for non squamous cell only. Do not use in squamous cell as fatal haemorrhage documented. Refer to company for info on reimbursement plan Dose modifications: See table page 32 Reference:
NSCLC Relapse Regimens: Patients Possessing ALK Positive Adenocarcinoma
22. Crizotinib Secure Cancer Drugs Fund funding before commencing treatment Crizotinib 250mg Oral twice a day Days 1 to 28 Swallow whole with water. Do not open capsules. Take with or without food. Avoid grapefruit juice and St John’s wort. Interval between cycles: Repeat every 28 days (continuous treatment) Number of cycles: Secure Cancer Drugs Fund funding for 2nd or subsequent line treatment of anaplastic lymphoma kinase (ALK) positive or advanced metastatic NSCLC. Continue until disease progression or unacceptable toxicity Tests before starting course of chemo: An accurate and validated ALK assay performed by a Lab with demonstrated proficiency in the specific technology being utilised. FBC, U&Es, LFTs, ECG. Chest X-ray. Ophthalmological assessment. Cardiac assessment: risk of QTc prolongations
may be increased in patients concomitantly taking anti-arrhythmics in patients with relevant pre-existing cardiac disease, bradycardia or electrolyte disturbances.
Tests to OK each cycle of chemo: FBC, U&Es, LFTs, (ALT, AST, total bilirubin) twice a month for the first 2 months, then once a month and as clinically indicated with more frequent testing for Grades 2, 3 or 4 elevation. Supportive drugs with each cycle: None Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Crizotinib is available as 250mg and 200mg tablets. If a dose is missed, then it should be taken as soon as the patient remembers unless it is less than 6 hours until the next dose in which case the dose should be omitted. Capsules should be swallowed whole with water. Do not crush, dissolve or open the capsules. Take dose with or without food. Avoid grapefruit juice and St John’s wort.

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 39 of 62
See SPC for interactions with strong CYP3A inhibitors, strong CYP3AL inducers, drugs that are CYP3A4 substrates and drugs that are known to prolong QT interval. Crizotinib has minor influence on ability to drive and/or use machinery. See SPC for caution when driving or operating machines as patient may experience vision disorder, dizziness or fatigue whilst taking Crizotinib.
Reference: Xalkori SPC 13 November 2012. Pfizer Ltd. Dose modifications: Dose interruption and/or dose reduction may be required. Dose levels are: Full dose 250mg Twice a day Level-1 200mg Twice a day Level-2 250mg ONCE a day Table: Crizotinib
Side effect: Crizotinib Dose modification (ref Xalkori SPC)
Haematology Neutrophils Platelet Hb x109/L x109/L g/L ≥1.0 and ≥50 and ≥80g 0.5-1.0 Or 25-50 Or 65-80 <0.5 Or <25 Or <65g
SPC permits full dose critzotinib if haematologigal parameters are ≤grade 2 ≤Grade 2; Full dose Grade 3, withhold until recovered to grade ≤2 then resume with same dose schedule. Grade 4, first occurrence: Withhold until recovered to grade ≤2 then resume with reduced dose; Crizotinib 200mg twice a day. Grade 4, 2nd occurrence: Withhold until recovered to grade ≤2 then resume with dose reduction; Crizotinib 250mg ONCE a day. Grade 4, 3rd occurrence: Permanently discontinue Crizotinib.
Renal Impariment Crcl ≥30mls/min <30mls/min
No adjustment to starting dose. No data. Do not give.
Hepatic impairment ALT/AST Bilirubin >5.0 x ULN and ≤1.5 x ULN (Grade 3) (Grade 1)
1st Occurrence:
2nd Occurrence:
3rd Occurrence:
Contd….
Withhold until recovery to Grade ≤1 (i.e. ALT/AST ≤ 3 xULN and Bilirubin ≤ 1.5 x ULN)
then resume with dose reduction; Crizotinib 200mg twice a day. Withhold until recovery to Grade ≤1 i.e. AST/ALT ≤3 xULN and Bilirubin ≤1.5 x ULN then resume with dose reduction; Crizotinib 250mg ONCE a day.
Permanently discontinue Crizotinib.

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 40 of 62
Side effect: Crizotinib Dose modification (ref Xalkori SPC)
Hepatic impairment ALT/AST Bilirubin >3 x ULN and >1.5 x ULN (in absence of cholestasis or haemolysis)
Permanently discontinue.
QTc Prolongation Grade 3 QTc Prolongation
1st Occurrence:
2nd Occurrence:
3rd Occurrence: Grade 4 QTc Prolongation
Withhold until recovered to Grade ≤1 then resume with reduced dose Crizotinib 200mg twice a day. Withhold until recovered to grade ≤1, then resume with further dose reduction Crizotinib 250mg ONCE a day. Discontinue permanently. Discontinue permanently.
Pneumonitis Any grade pneumonitis not attributable to NSCLC progression, other pulmonary disease, infection or radiation effect.
Crizotinib should be withheld if pneumonitis is suspected. See SPC Permanently discontinue if treatment related pneumonitis is diagnosed.
Visual effects Ophthalmological evaluation should be considered if vision disorder persists or worsens in severity.
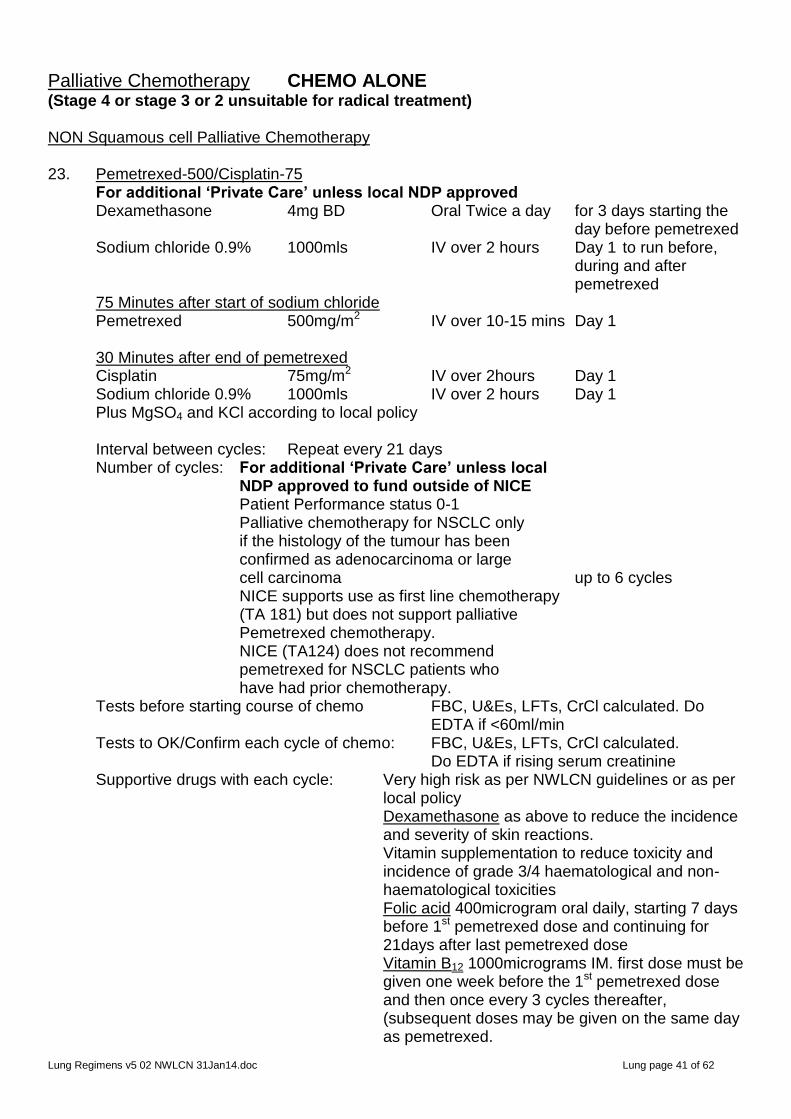
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 41 of 62
Palliative Chemotherapy CHEMO ALONE (Stage 4 or stage 3 or 2 unsuitable for radical treatment) NON Squamous cell Palliative Chemotherapy 23. Pemetrexed-500/Cisplatin-75 For additional ‘Private Care’ unless local NDP approved Dexamethasone 4mg BD Oral Twice a day for 3 days starting the day before pemetrexed Sodium chloride 0.9% 1000mls IV over 2 hours Day 1 to run before, during and after pemetrexed 75 Minutes after start of sodium chloride Pemetrexed 500mg/m2 IV over 10-15 mins Day 1 30 Minutes after end of pemetrexed Cisplatin 75mg/m2 IV over 2hours Day 1 Sodium chloride 0.9% 1000mls IV over 2 hours Day 1 Plus MgSO4 and KCl according to local policy Interval between cycles: Repeat every 21 days Number of cycles: For additional ‘Private Care’ unless local NDP approved to fund outside of NICE Patient Performance status 0-1 Palliative chemotherapy for NSCLC only if the histology of the tumour has been confirmed as adenocarcinoma or large cell carcinoma up to 6 cycles NICE supports use as first line chemotherapy (TA 181) but does not support palliative Pemetrexed chemotherapy. NICE (TA124) does not recommend pemetrexed for NSCLC patients who have had prior chemotherapy. Tests before starting course of chemo FBC, U&Es, LFTs, CrCl calculated. Do
EDTA if <60ml/min Tests to OK/Confirm each cycle of chemo: FBC, U&Es, LFTs, CrCl calculated. Do EDTA if rising serum creatinine Supportive drugs with each cycle: Very high risk as per NWLCN guidelines or as per
local policy Dexamethasone as above to reduce the incidence and severity of skin reactions. Vitamin supplementation to reduce toxicity and incidence of grade 3/4 haematological and non-haematological toxicities Folic acid 400microgram oral daily, starting 7 days before 1st pemetrexed dose and continuing for 21days after last pemetrexed dose Vitamin B12 1000micrograms IM. first dose must be given one week before the 1st pemetrexed dose and then once every 3 cycles thereafter, (subsequent doses may be given on the same day as pemetrexed.
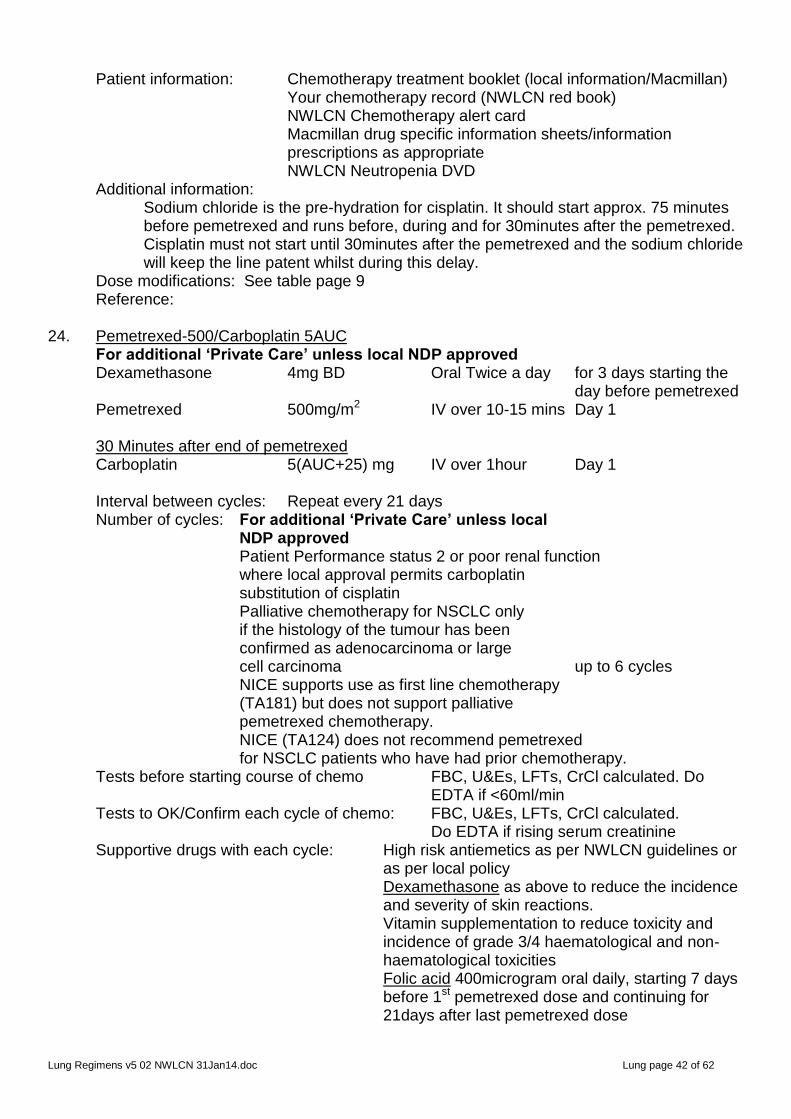
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 42 of 62
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Sodium chloride is the pre-hydration for cisplatin. It should start approx. 75 minutes before pemetrexed and runs before, during and for 30minutes after the pemetrexed. Cisplatin must not start until 30minutes after the pemetrexed and the sodium chloride will keep the line patent whilst during this delay.
Dose modifications: See table page 9 Reference: 24. Pemetrexed-500/Carboplatin 5AUC For additional ‘Private Care’ unless local NDP approved Dexamethasone 4mg BD Oral Twice a day for 3 days starting the day before pemetrexed Pemetrexed 500mg/m2 IV over 10-15 mins Day 1 30 Minutes after end of pemetrexed Carboplatin 5(AUC+25) mg IV over 1hour Day 1 Interval between cycles: Repeat every 21 days Number of cycles: For additional ‘Private Care’ unless local NDP approved Patient Performance status 2 or poor renal function where local approval permits carboplatin substitution of cisplatin Palliative chemotherapy for NSCLC only if the histology of the tumour has been confirmed as adenocarcinoma or large cell carcinoma up to 6 cycles NICE supports use as first line chemotherapy (TA181) but does not support palliative pemetrexed chemotherapy. NICE (TA124) does not recommend pemetrexed for NSCLC patients who have had prior chemotherapy. Tests before starting course of chemo FBC, U&Es, LFTs, CrCl calculated. Do
EDTA if <60ml/min Tests to OK/Confirm each cycle of chemo: FBC, U&Es, LFTs, CrCl calculated. Do EDTA if rising serum creatinine Supportive drugs with each cycle: High risk antiemetics as per NWLCN guidelines or
as per local policy Dexamethasone as above to reduce the incidence and severity of skin reactions. Vitamin supplementation to reduce toxicity and incidence of grade 3/4 haematological and non-haematological toxicities Folic acid 400microgram oral daily, starting 7 days before 1st pemetrexed dose and continuing for 21days after last pemetrexed dose
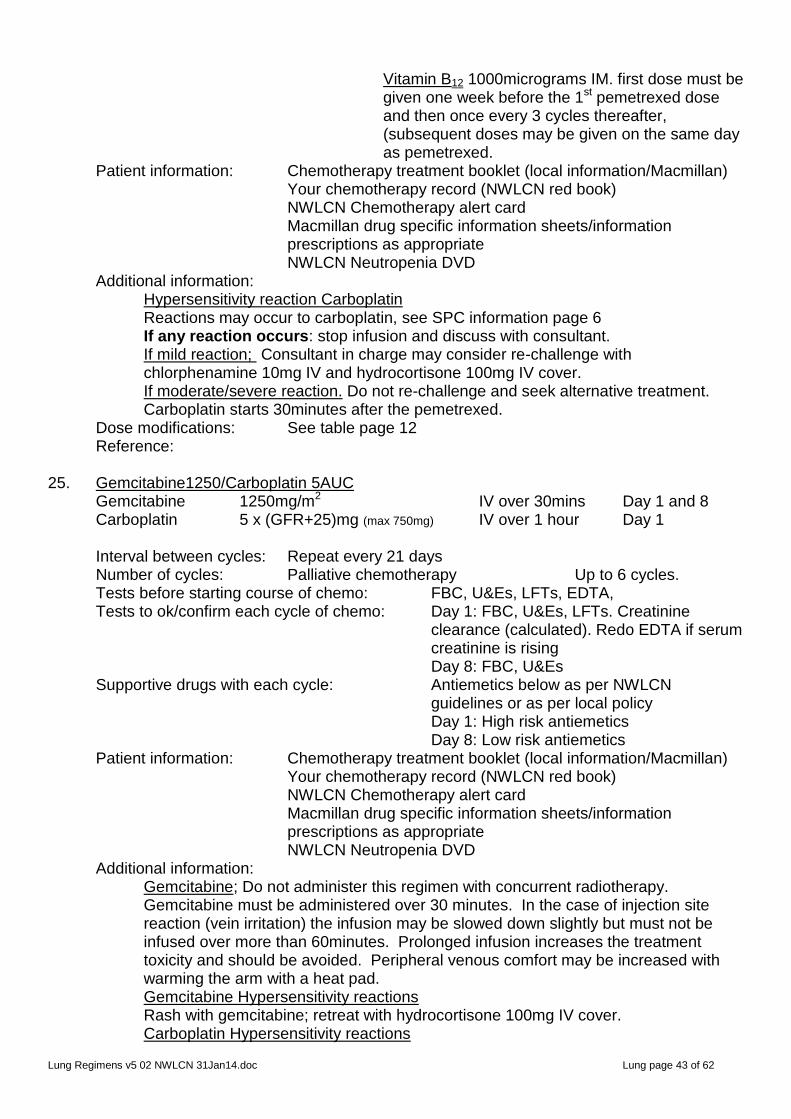
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 43 of 62
Vitamin B12 1000micrograms IM. first dose must be given one week before the 1st pemetrexed dose and then once every 3 cycles thereafter, (subsequent doses may be given on the same day as pemetrexed.
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Hypersensitivity reaction Carboplatin Reactions may occur to carboplatin, see SPC information page 6 If any reaction occurs: stop infusion and discuss with consultant. If mild reaction; Consultant in charge may consider re-challenge with chlorphenamine 10mg IV and hydrocortisone 100mg IV cover. If moderate/severe reaction. Do not re-challenge and seek alternative treatment.
Carboplatin starts 30minutes after the pemetrexed. Dose modifications: See table page 12 Reference: 25. Gemcitabine1250/Carboplatin 5AUC Gemcitabine 1250mg/m2 IV over 30mins Day 1 and 8 Carboplatin 5 x (GFR+25)mg (max 750mg) IV over 1 hour Day 1 Interval between cycles: Repeat every 21 days Number of cycles: Palliative chemotherapy Up to 6 cycles. Tests before starting course of chemo: FBC, U&Es, LFTs, EDTA, Tests to ok/confirm each cycle of chemo: Day 1: FBC, U&Es, LFTs. Creatinine
clearance (calculated). Redo EDTA if serum creatinine is rising
Day 8: FBC, U&Es Supportive drugs with each cycle: Antiemetics below as per NWLCN
guidelines or as per local policy Day 1: High risk antiemetics
Day 8: Low risk antiemetics Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Gemcitabine; Do not administer this regimen with concurrent radiotherapy. Gemcitabine must be administered over 30 minutes. In the case of injection site reaction (vein irritation) the infusion may be slowed down slightly but must not be infused over more than 60minutes. Prolonged infusion increases the treatment toxicity and should be avoided. Peripheral venous comfort may be increased with warming the arm with a heat pad. Gemcitabine Hypersensitivity reactions Rash with gemcitabine; retreat with hydrocortisone 100mg IV cover. Carboplatin Hypersensitivity reactions
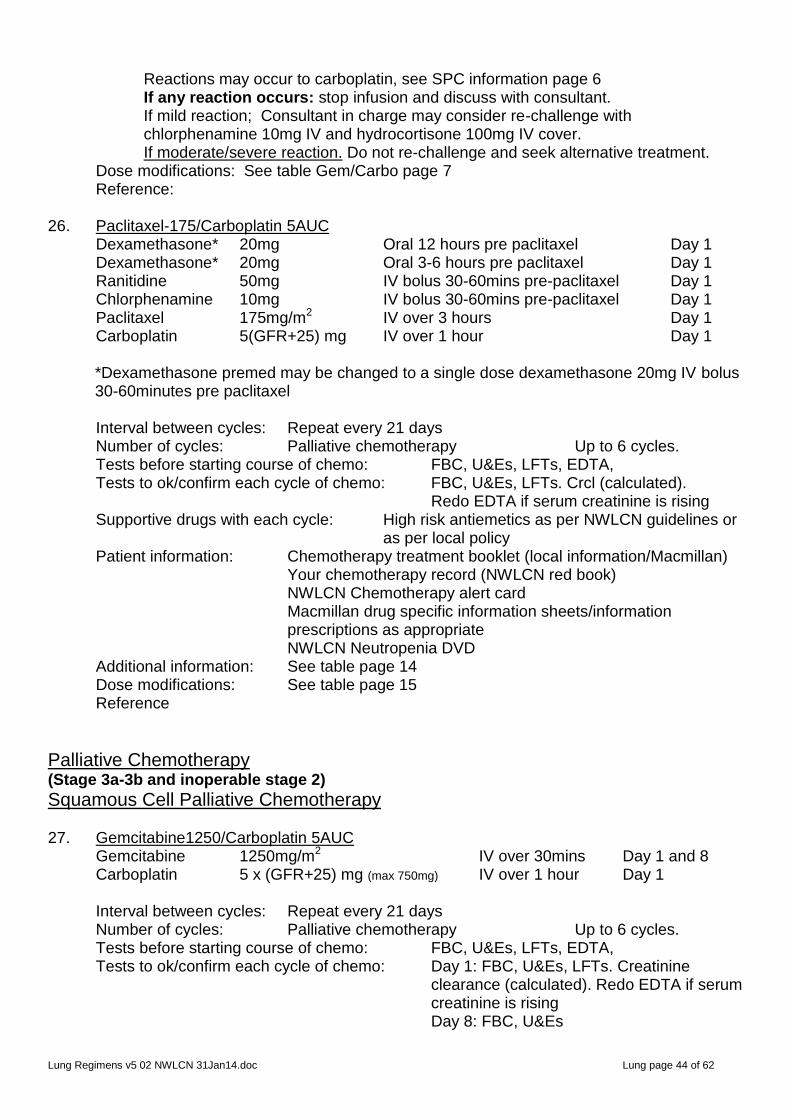
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 44 of 62
Reactions may occur to carboplatin, see SPC information page 6 If any reaction occurs: stop infusion and discuss with consultant. If mild reaction; Consultant in charge may consider re-challenge with chlorphenamine 10mg IV and hydrocortisone 100mg IV cover. If moderate/severe reaction. Do not re-challenge and seek alternative treatment.
Dose modifications: See table Gem/Carbo page 7 Reference: 26. Paclitaxel-175/Carboplatin 5AUC Dexamethasone* 20mg Oral 12 hours pre paclitaxel Day 1 Dexamethasone* 20mg Oral 3-6 hours pre paclitaxel Day 1 Ranitidine 50mg IV bolus 30-60mins pre-paclitaxel Day 1 Chlorphenamine 10mg IV bolus 30-60mins pre-paclitaxel Day 1 Paclitaxel 175mg/m2 IV over 3 hours Day 1 Carboplatin 5(GFR+25) mg IV over 1 hour Day 1 *Dexamethasone premed may be changed to a single dose dexamethasone 20mg IV bolus
30-60minutes pre paclitaxel Interval between cycles: Repeat every 21 days Number of cycles: Palliative chemotherapy Up to 6 cycles. Tests before starting course of chemo: FBC, U&Es, LFTs, EDTA, Tests to ok/confirm each cycle of chemo: FBC, U&Es, LFTs. Crcl (calculated). Redo EDTA if serum creatinine is rising Supportive drugs with each cycle: High risk antiemetics as per NWLCN guidelines or
as per local policy Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate
NWLCN Neutropenia DVD
Additional information: See table page 14 Dose modifications: See table page 15 Reference
Palliative Chemotherapy (Stage 3a-3b and inoperable stage 2)
Squamous Cell Palliative Chemotherapy 27. Gemcitabine1250/Carboplatin 5AUC Gemcitabine 1250mg/m2 IV over 30mins Day 1 and 8 Carboplatin 5 x (GFR+25) mg (max 750mg) IV over 1 hour Day 1 Interval between cycles: Repeat every 21 days Number of cycles: Palliative chemotherapy Up to 6 cycles. Tests before starting course of chemo: FBC, U&Es, LFTs, EDTA, Tests to ok/confirm each cycle of chemo: Day 1: FBC, U&Es, LFTs. Creatinine
clearance (calculated). Redo EDTA if serum creatinine is rising
Day 8: FBC, U&Es
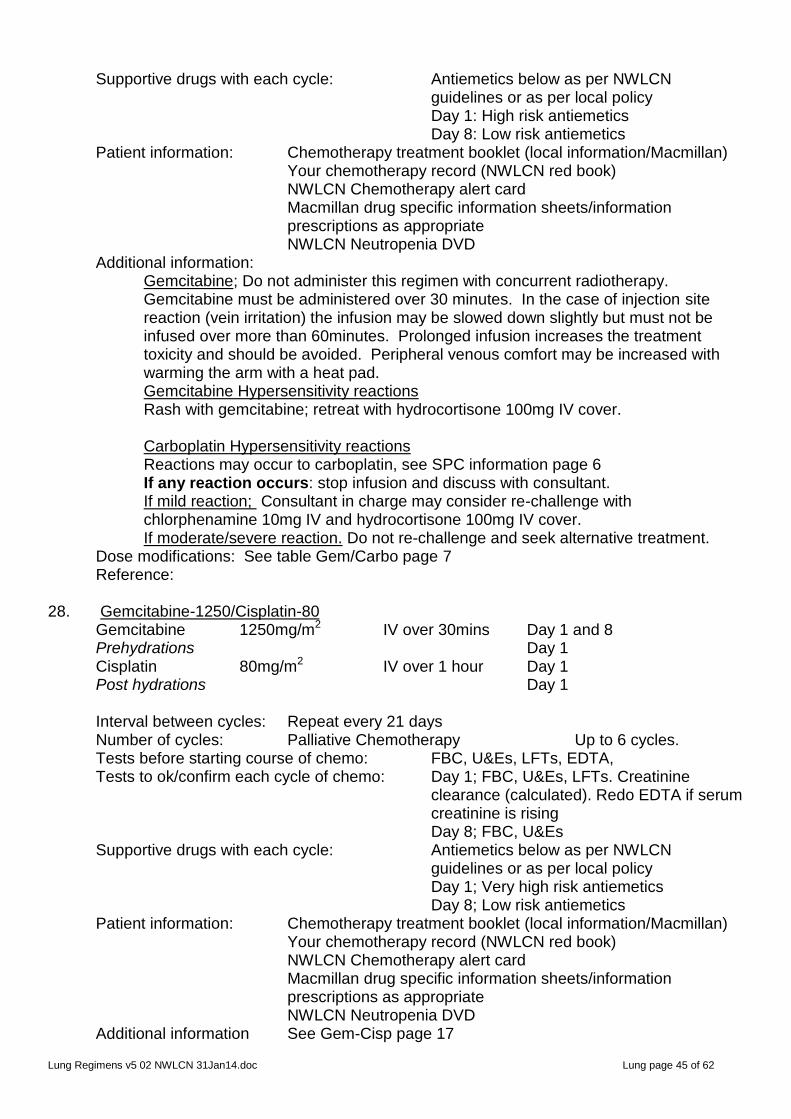
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 45 of 62
Supportive drugs with each cycle: Antiemetics below as per NWLCN guidelines or as per local policy Day 1: High risk antiemetics
Day 8: Low risk antiemetics Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Gemcitabine; Do not administer this regimen with concurrent radiotherapy. Gemcitabine must be administered over 30 minutes. In the case of injection site reaction (vein irritation) the infusion may be slowed down slightly but must not be infused over more than 60minutes. Prolonged infusion increases the treatment toxicity and should be avoided. Peripheral venous comfort may be increased with warming the arm with a heat pad. Gemcitabine Hypersensitivity reactions Rash with gemcitabine; retreat with hydrocortisone 100mg IV cover. Carboplatin Hypersensitivity reactions Reactions may occur to carboplatin, see SPC information page 6 If any reaction occurs: stop infusion and discuss with consultant. If mild reaction; Consultant in charge may consider re-challenge with chlorphenamine 10mg IV and hydrocortisone 100mg IV cover. If moderate/severe reaction. Do not re-challenge and seek alternative treatment.
Dose modifications: See table Gem/Carbo page 7 Reference: 28. Gemcitabine-1250/Cisplatin-80 Gemcitabine 1250mg/m2 IV over 30mins Day 1 and 8 Prehydrations Day 1 Cisplatin 80mg/m2 IV over 1 hour Day 1 Post hydrations Day 1 Interval between cycles: Repeat every 21 days Number of cycles: Palliative Chemotherapy Up to 6 cycles. Tests before starting course of chemo: FBC, U&Es, LFTs, EDTA, Tests to ok/confirm each cycle of chemo: Day 1; FBC, U&Es, LFTs. Creatinine
clearance (calculated). Redo EDTA if serum creatinine is rising
Day 8; FBC, U&Es Supportive drugs with each cycle: Antiemetics below as per NWLCN
guidelines or as per local policy Day 1; Very high risk antiemetics
Day 8; Low risk antiemetics Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information See Gem-Cisp page 17
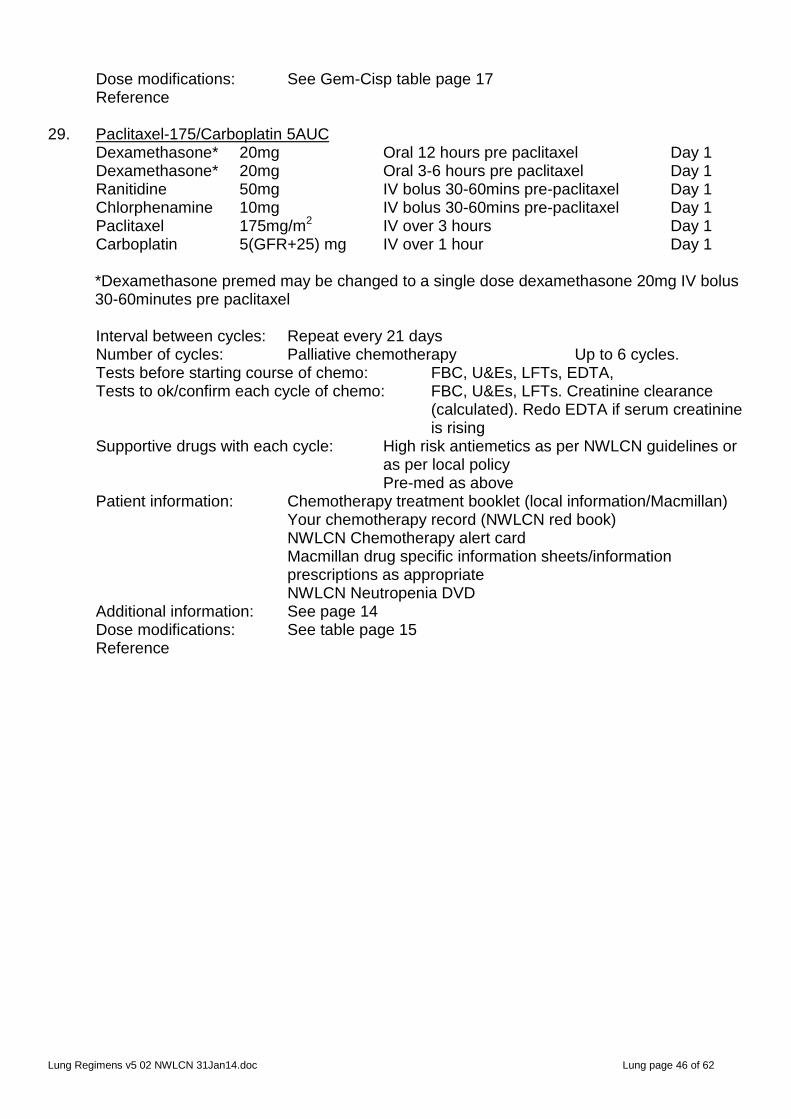
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 46 of 62
Dose modifications: See Gem-Cisp table page 17 Reference 29. Paclitaxel-175/Carboplatin 5AUC Dexamethasone* 20mg Oral 12 hours pre paclitaxel Day 1 Dexamethasone* 20mg Oral 3-6 hours pre paclitaxel Day 1 Ranitidine 50mg IV bolus 30-60mins pre-paclitaxel Day 1 Chlorphenamine 10mg IV bolus 30-60mins pre-paclitaxel Day 1 Paclitaxel 175mg/m2 IV over 3 hours Day 1 Carboplatin 5(GFR+25) mg IV over 1 hour Day 1 *Dexamethasone premed may be changed to a single dose dexamethasone 20mg IV bolus
30-60minutes pre paclitaxel Interval between cycles: Repeat every 21 days Number of cycles: Palliative chemotherapy Up to 6 cycles. Tests before starting course of chemo: FBC, U&Es, LFTs, EDTA, Tests to ok/confirm each cycle of chemo: FBC, U&Es, LFTs. Creatinine clearance
(calculated). Redo EDTA if serum creatinine is rising
Supportive drugs with each cycle: High risk antiemetics as per NWLCN guidelines or as per local policy Pre-med as above
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: See page 14 Dose modifications: See table page 15 Reference
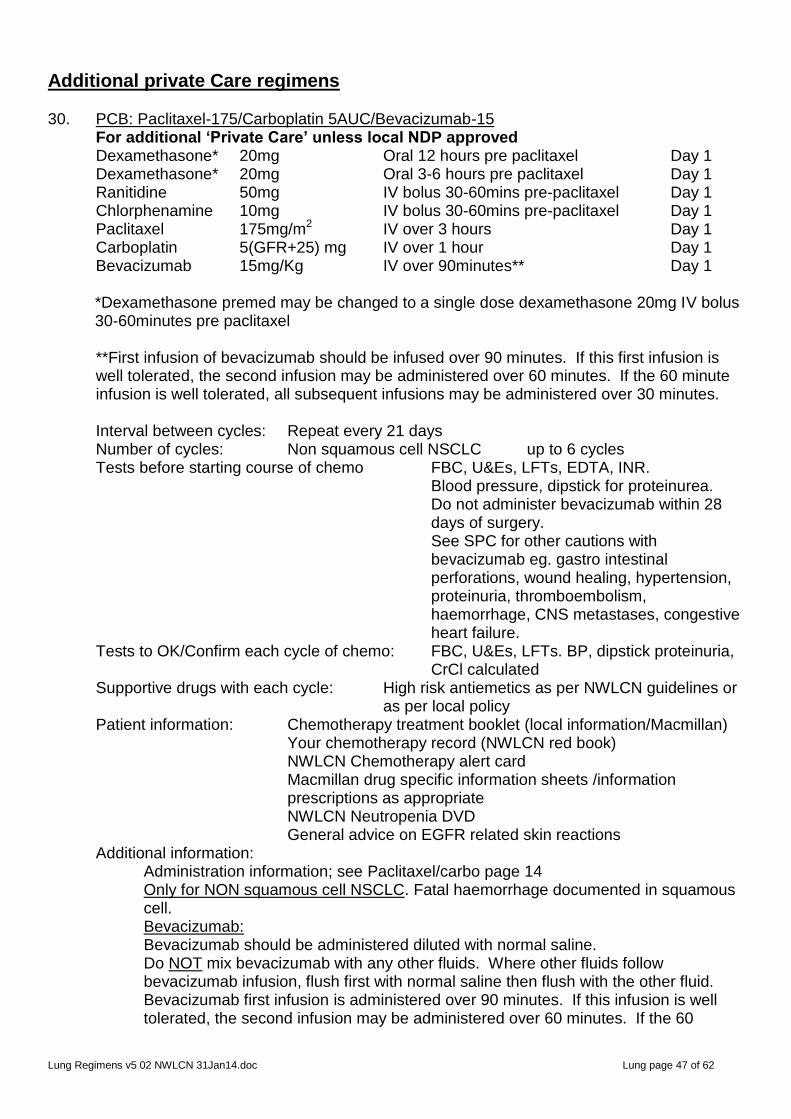
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 47 of 62
Additional private Care regimens 30. PCB: Paclitaxel-175/Carboplatin 5AUC/Bevacizumab-15 For additional ‘Private Care’ unless local NDP approved Dexamethasone* 20mg Oral 12 hours pre paclitaxel Day 1 Dexamethasone* 20mg Oral 3-6 hours pre paclitaxel Day 1 Ranitidine 50mg IV bolus 30-60mins pre-paclitaxel Day 1 Chlorphenamine 10mg IV bolus 30-60mins pre-paclitaxel Day 1 Paclitaxel 175mg/m2 IV over 3 hours Day 1 Carboplatin 5(GFR+25) mg IV over 1 hour Day 1 Bevacizumab 15mg/Kg IV over 90minutes** Day 1 *Dexamethasone premed may be changed to a single dose dexamethasone 20mg IV bolus
30-60minutes pre paclitaxel
**First infusion of bevacizumab should be infused over 90 minutes. If this first infusion is well tolerated, the second infusion may be administered over 60 minutes. If the 60 minute infusion is well tolerated, all subsequent infusions may be administered over 30 minutes.
Interval between cycles: Repeat every 21 days Number of cycles: Non squamous cell NSCLC up to 6 cycles Tests before starting course of chemo FBC, U&Es, LFTs, EDTA, INR. Blood pressure, dipstick for proteinurea. Do not administer bevacizumab within 28
days of surgery. See SPC for other cautions with
bevacizumab eg. gastro intestinal perforations, wound healing, hypertension, proteinuria, thromboembolism, haemorrhage, CNS metastases, congestive heart failure.
Tests to OK/Confirm each cycle of chemo: FBC, U&Es, LFTs. BP, dipstick proteinuria, CrCl calculated Supportive drugs with each cycle: High risk antiemetics as per NWLCN guidelines or
as per local policy Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets /information prescriptions as appropriate NWLCN Neutropenia DVD
General advice on EGFR related skin reactions Additional information: Administration information; see Paclitaxel/carbo page 14 Only for NON squamous cell NSCLC. Fatal haemorrhage documented in squamous cell. Bevacizumab: Bevacizumab should be administered diluted with normal saline. Do NOT mix bevacizumab with any other fluids. Where other fluids follow bevacizumab infusion, flush first with normal saline then flush with the other fluid. Bevacizumab first infusion is administered over 90 minutes. If this infusion is well tolerated, the second infusion may be administered over 60 minutes. If the 60

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 48 of 62
minute infusion is well tolerated all subsequent infusion may be administered over 30 minutes. See dose modification table for action of dose not tolerated. Dose modifications: For Paclitaxel/carbo see page 15 For bevacizumab see below Reference: Table: Bevacizumab
Side effect: Bevacizumab Dose modification (SPC)
All toxicities graded according to CTCAE v3.0 guidelines
Thrombosis/Embolism Venous thromboembolic event Grade 3 or incidentally discovered pulmonary embolus (first occurrence) Symptomatic Grade 4 venous thromboembolic event (first occurrence) Arterial thromboembolic event – any grade
Hold bevacizumab for 2 weeks. Bevacizumab may be resumed after initiation of therapeutic-dose anticoagulant therapy as soon as all of the following criteria are met:
The patient must be on a stable dose of anticoagulant and, if on an oral coumarin-derivative, have an INR within the target range (usually between 2 and 3) prior to restarting bevacizumab.
Permanently discontinue bevacizumab Permanently discontinue bevacizumab if patient develops any grade of arterial thromboembolic event.
Haemorrhage Grade 1 and 2 Grade 3 or 4 (first occurrence)
No schedule modifications Discontinue bevacizumab and institute appropriate treatment
Blank Proteinuria First occurrence of proteinuria:
1+ (dipstick)
2+, 3+ and 4+ dipstick
Blank Administer bevacizumab as scheduled. NO additional evaluation is required. Administer bevacizumab as scheduled and collect 24-hour urine to determine the total protein within 3 days prior to the next scheduled dose. If
24-hour proteinuria ≤2g: Administer bevacizumab as scheduled
24-hour proteinuria >2g: Bevacizumab treatment should be withheld pending next 24 hour total protein.
If
Repeat 24 hour urine protein ≤2g: Administer bevacizumab as schedule. 24-hour
protein should be further monitored prior to each

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 49 of 62
Side effect: Bevacizumab Dose modification (SPC)
Second and subsequent occurrence of ≥2+ proteinuria (dipstick)
2+ (dipstick)
3+ and 4+ (dipstick):
Nephrotic Syndrome (Grade 4)
administration of bevacizumab until it has decreased to ≤1g/24 hour.
Repeat 24-hour urine protein > 2g: Bevacizumab dose should be withheld until 24-
hour protein has decreased to ≤2g. 24-hour protein should be further monitored prior to each administration of bevacizumab until it has decreased to ≤1g/24 hour.
Administer bevacizumab as scheduled. NO additional evaluation is required. Administer bevacizumab as scheduled and collect 24-hour urine to determine the total protein within 3 days prior to the next scheduled dose is required: If
24-hour proteinuria ≤2g: Administer bevacizumab as scheduled
24-hour proteinuria >2g: Bevacizumab treatment should be withheld pending next 24 hour total protein.
If
Repeat 24 hour urine protein ≤2g: Administer bevacizumab as schedule. 24-hour
protein should be further monitored prior to each administration of bevacizumab until it has decreased to ≤1g/24 hour.
Repeat 24-hour urine protein > 2g: Bevacizumab dose should be withheld until 24-
hour protein has decreased to ≤2g. 24-hour protein should be further monitored prior to each administration of bevacizumab until it has decreased to ≤1g/24 hour.
Discontinue bevacizumab treatment
Gastro-intestinal perforation Gastro-intestinal perforation or dehiscence
Discontinue bevacizumab permanently and institute appropriate treatment
Wound healing complications Prevention of wound healing complications Wound healing complications
Bevacizumab therapy should not be initiated for at least 28 days following major surgery or until the surgical wound is fully healed. Bevacizumab therapy should be withheld for at least 28 days before elective surgery. In patients who experience wound healing complications during bevacizumab treatment, bevacizumab should be withheld until the wound is fully healed.
Fistula or intra-abdominal abscess Fistula or intra-abdominal abscess
Patients who develop a fistula or intra-abdominal abscess should discontinue bevacizumab
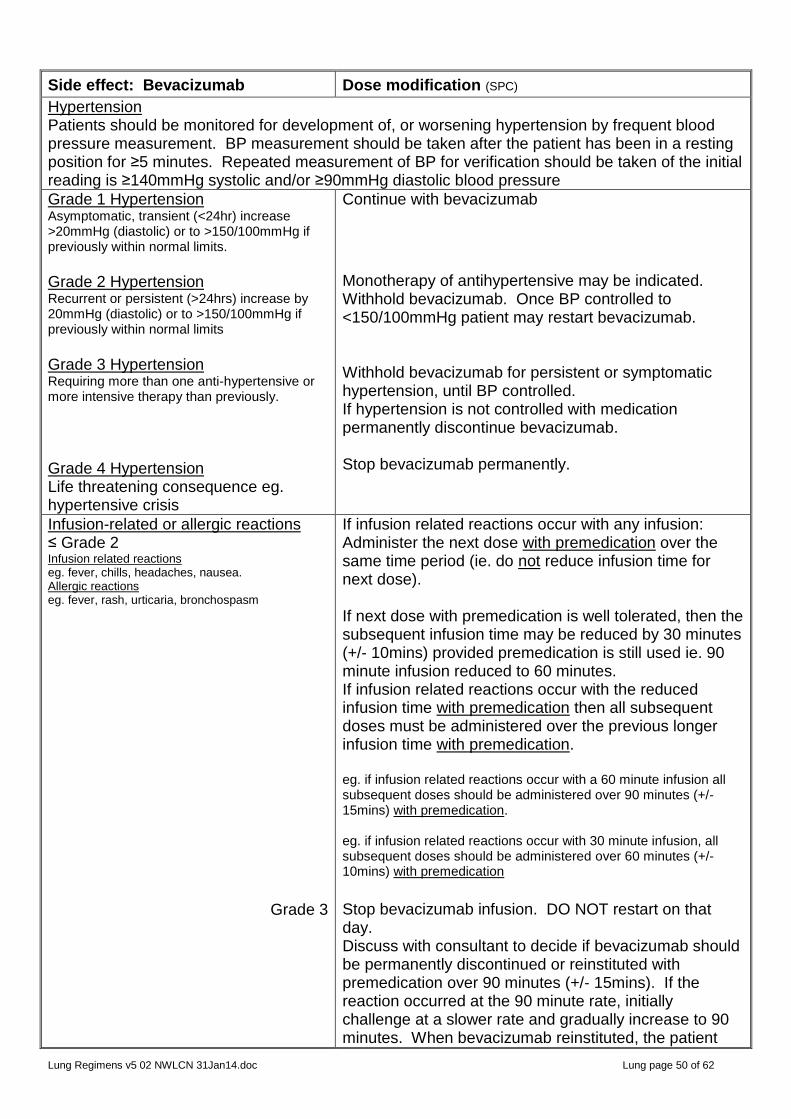
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 50 of 62
Side effect: Bevacizumab Dose modification (SPC)
Hypertension Patients should be monitored for development of, or worsening hypertension by frequent blood pressure measurement. BP measurement should be taken after the patient has been in a resting position for ≥5 minutes. Repeated measurement of BP for verification should be taken of the initial reading is ≥140mmHg systolic and/or ≥90mmHg diastolic blood pressure
Grade 1 Hypertension Asymptomatic, transient (<24hr) increase >20mmHg (diastolic) or to >150/100mmHg if previously within normal limits. Grade 2 Hypertension Recurrent or persistent (>24hrs) increase by 20mmHg (diastolic) or to >150/100mmHg if previously within normal limits Grade 3 Hypertension Requiring more than one anti-hypertensive or more intensive therapy than previously. Grade 4 Hypertension Life threatening consequence eg. hypertensive crisis
Continue with bevacizumab
Monotherapy of antihypertensive may be indicated. Withhold bevacizumab. Once BP controlled to <150/100mmHg patient may restart bevacizumab. Withhold bevacizumab for persistent or symptomatic hypertension, until BP controlled. If hypertension is not controlled with medication permanently discontinue bevacizumab. Stop bevacizumab permanently.
Infusion-related or allergic reactions ≤ Grade 2 Infusion related reactions eg. fever, chills, headaches, nausea. Allergic reactions eg. fever, rash, urticaria, bronchospasm
Grade 3
If infusion related reactions occur with any infusion: Administer the next dose with premedication over the same time period (ie. do not reduce infusion time for next dose). If next dose with premedication is well tolerated, then the subsequent infusion time may be reduced by 30 minutes (+/- 10mins) provided premedication is still used ie. 90 minute infusion reduced to 60 minutes. If infusion related reactions occur with the reduced infusion time with premedication then all subsequent doses must be administered over the previous longer infusion time with premedication. eg. if infusion related reactions occur with a 60 minute infusion all subsequent doses should be administered over 90 minutes (+/- 15mins) with premedication. eg. if infusion related reactions occur with 30 minute infusion, all subsequent doses should be administered over 60 minutes (+/- 10mins) with premedication
Stop bevacizumab infusion. DO NOT restart on that day. Discuss with consultant to decide if bevacizumab should be permanently discontinued or reinstituted with premedication over 90 minutes (+/- 15mins). If the reaction occurred at the 90 minute rate, initially challenge at a slower rate and gradually increase to 90 minutes. When bevacizumab reinstituted, the patient

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 51 of 62
Side effect: Bevacizumab Dose modification (SPC)
Grade 4
should be monitored for a duration comparable to duration of previous reaction,. If suspected anaphylactic reactions during bevacizumab infusion STOP bevacizumab infusion, institute usual medical response to reaction, consider application of tourniquet proximal to the injection site to slow systemic absorption of bevacizumab (do not obstruct arterial flow in the limb)
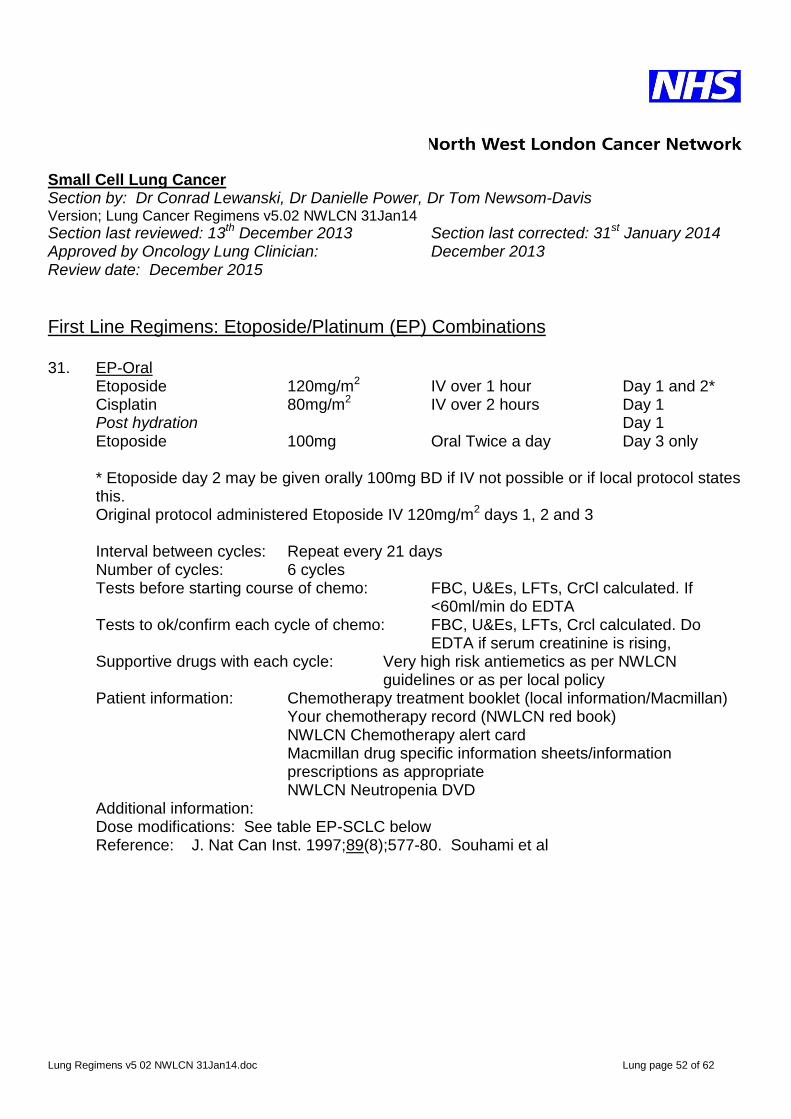
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 52 of 62
Small Cell Lung Cancer Section by: Dr Conrad Lewanski, Dr Danielle Power, Dr Tom Newsom-Davis Version; Lung Cancer Regimens v5.02 NWLCN 31Jan14
Section last reviewed: 13th December 2013 Section last corrected: 31st January 2014 Approved by Oncology Lung Clinician: December 2013 Review date: December 2015
First Line Regimens: Etoposide/Platinum (EP) Combinations 31. EP-Oral Etoposide 120mg/m2 IV over 1 hour Day 1 and 2* Cisplatin 80mg/m2 IV over 2 hours Day 1 Post hydration Day 1 Etoposide 100mg Oral Twice a day Day 3 only
* Etoposide day 2 may be given orally 100mg BD if IV not possible or if local protocol states this. Original protocol administered Etoposide IV 120mg/m2 days 1, 2 and 3
Interval between cycles: Repeat every 21 days Number of cycles: 6 cycles Tests before starting course of chemo: FBC, U&Es, LFTs, CrCl calculated. If
<60ml/min do EDTA Tests to ok/confirm each cycle of chemo: FBC, U&Es, LFTs, Crcl calculated. Do
EDTA if serum creatinine is rising, Supportive drugs with each cycle: Very high risk antiemetics as per NWLCN
guidelines or as per local policy Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Dose modifications: See table EP-SCLC below Reference: J. Nat Can Inst. 1997;89(8);577-80. Souhami et al
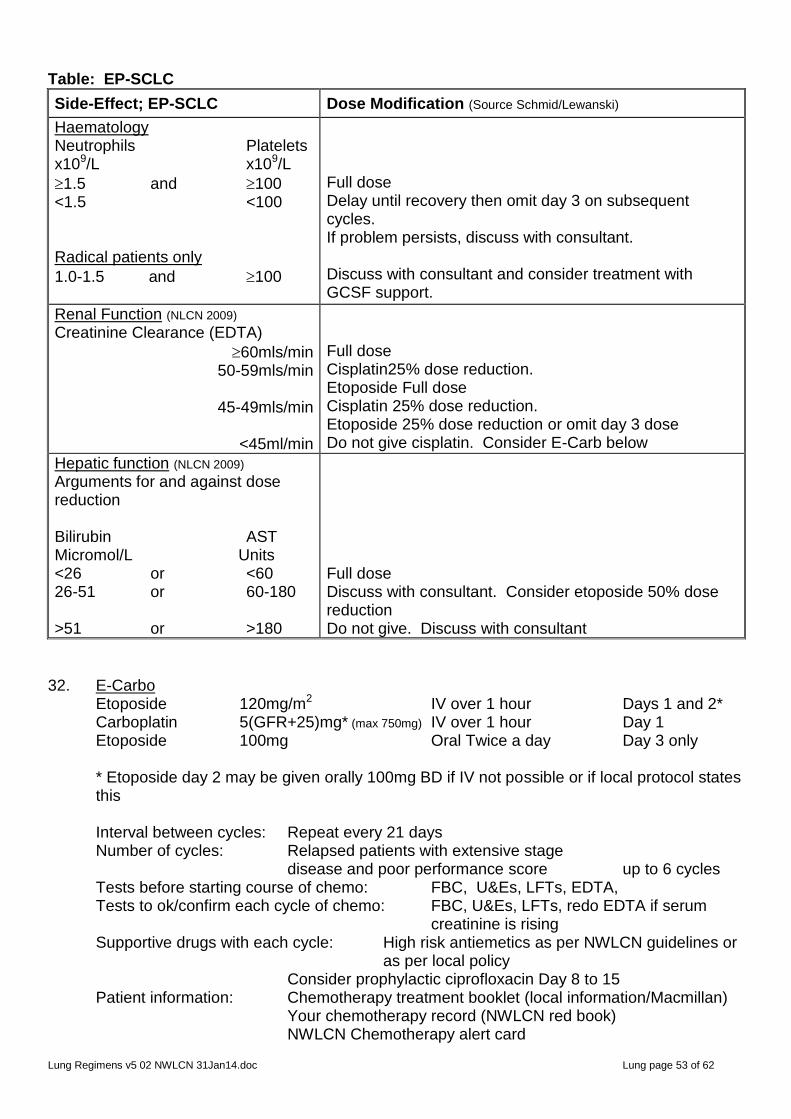
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 53 of 62
Table: EP-SCLC
Side-Effect; EP-SCLC
Dose Modification (Source Schmid/Lewanski)
Haematology Neutrophils Platelets x109/L x109/L
1.5 and 100 <1.5 <100 Radical patients only
1.0-1.5 and 100
Full dose Delay until recovery then omit day 3 on subsequent cycles. If problem persists, discuss with consultant. Discuss with consultant and consider treatment with GCSF support.
Renal Function (NLCN 2009)
Creatinine Clearance (EDTA)
60mls/min 50-59mls/min
45-49mls/min
<45ml/min
Full dose Cisplatin25% dose reduction. Etoposide Full dose Cisplatin 25% dose reduction. Etoposide 25% dose reduction or omit day 3 dose Do not give cisplatin. Consider E-Carb below
Hepatic function (NLCN 2009)
Arguments for and against dose reduction Bilirubin AST Micromol/L Units <26 or <60 26-51 or 60-180 >51 or >180
Full dose Discuss with consultant. Consider etoposide 50% dose reduction Do not give. Discuss with consultant
32. E-Carbo Etoposide 120mg/m2 IV over 1 hour Days 1 and 2* Carboplatin 5(GFR+25)mg* (max 750mg) IV over 1 hour Day 1 Etoposide 100mg Oral Twice a day Day 3 only
* Etoposide day 2 may be given orally 100mg BD if IV not possible or if local protocol states this
Interval between cycles: Repeat every 21 days Number of cycles: Relapsed patients with extensive stage disease and poor performance score up to 6 cycles Tests before starting course of chemo: FBC, U&Es, LFTs, EDTA, Tests to ok/confirm each cycle of chemo: FBC, U&Es, LFTs, redo EDTA if serum
creatinine is rising Supportive drugs with each cycle: High risk antiemetics as per NWLCN guidelines or
as per local policy Consider prophylactic ciprofloxacin Day 8 to 15 Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
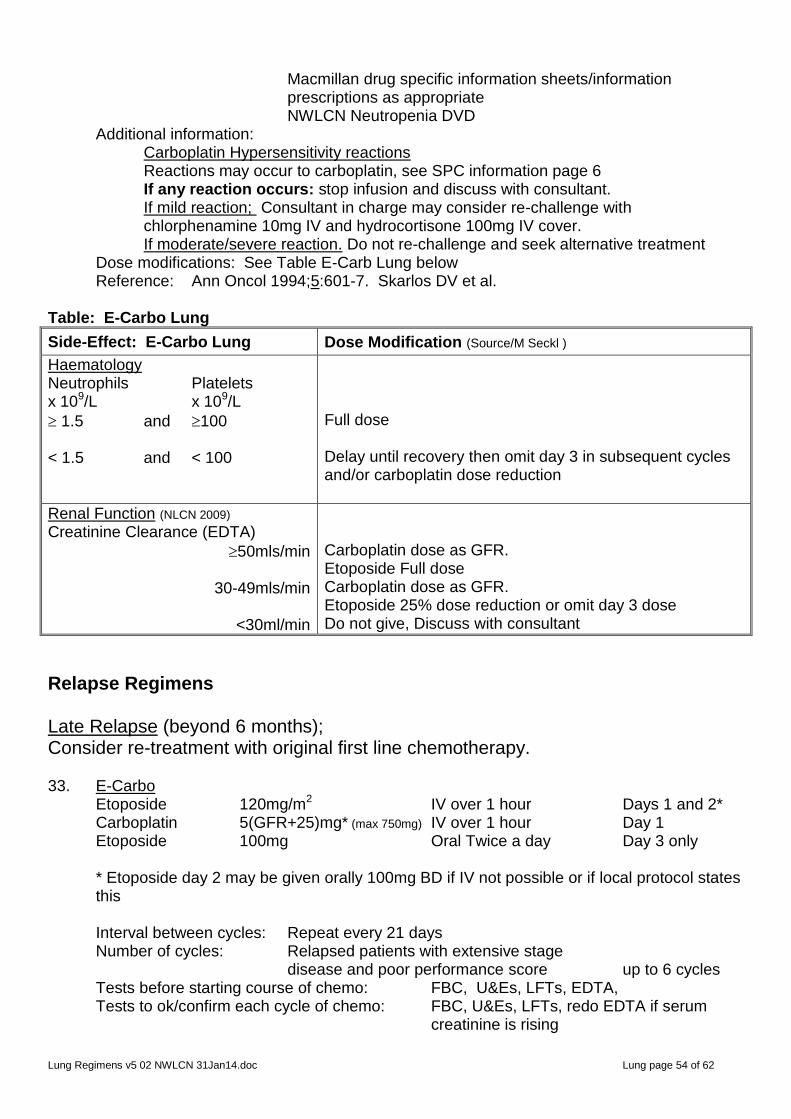
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 54 of 62
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Carboplatin Hypersensitivity reactions Reactions may occur to carboplatin, see SPC information page 6 If any reaction occurs: stop infusion and discuss with consultant. If mild reaction; Consultant in charge may consider re-challenge with chlorphenamine 10mg IV and hydrocortisone 100mg IV cover.
If moderate/severe reaction. Do not re-challenge and seek alternative treatment Dose modifications: See Table E-Carb Lung below Reference: Ann Oncol 1994;5:601-7. Skarlos DV et al. Table: E-Carbo Lung
Side-Effect: E-Carbo Lung
Dose Modification (Source/M Seckl )
Haematology Neutrophils Platelets x 109/L x 109/L
1.5 and 100 < 1.5 and < 100
Full dose Delay until recovery then omit day 3 in subsequent cycles and/or carboplatin dose reduction
Renal Function (NLCN 2009)
Creatinine Clearance (EDTA)
50mls/min
30-49mls/min
<30ml/min
Carboplatin dose as GFR. Etoposide Full dose Carboplatin dose as GFR. Etoposide 25% dose reduction or omit day 3 dose Do not give, Discuss with consultant
Relapse Regimens Late Relapse (beyond 6 months); Consider re-treatment with original first line chemotherapy. 33. E-Carbo Etoposide 120mg/m2 IV over 1 hour Days 1 and 2* Carboplatin 5(GFR+25)mg* (max 750mg) IV over 1 hour Day 1 Etoposide 100mg Oral Twice a day Day 3 only
* Etoposide day 2 may be given orally 100mg BD if IV not possible or if local protocol states this
Interval between cycles: Repeat every 21 days Number of cycles: Relapsed patients with extensive stage disease and poor performance score up to 6 cycles Tests before starting course of chemo: FBC, U&Es, LFTs, EDTA, Tests to ok/confirm each cycle of chemo: FBC, U&Es, LFTs, redo EDTA if serum
creatinine is rising
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 55 of 62
Supportive drugs with each cycle: High risk antiemetics as per NWLCN guidelines or as per local policy
Consider prophylactic ciprofloxacin Day 8 to 15 Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Carboplatin Hypersensitivity reactions Reactions may occur to carboplatin, see SPC information page 6 If any reaction occurs: stop infusion and discuss with consultant. If mild reaction; Consultant in charge may consider re-challenge with chlorphenamine 10mg IV and hydrocortisone 100mg IV cover.
If moderate/severe reaction. Do not re-challenge and seek alternative treatment Dose modifications: See Table E-Carb Lung page 54 Reference: Ann Oncol 1994;5:601-7. Skarlos DV et al.
Early Relapse Within 6 months of stopping original treatment 34. CAV (CTIS: 791) Vincristine 2mg IV minibag over 10 mins Day 1 Doxorubicin 50mg/m2 IV bolus Day 1 Cyclophosphamide 750mg/m2 IV over 30 mins Day 1 Interval between cycles: Repeat every 21 days Number of cycles: 6 cycles Tests before starting course of chemo: FBC, U&Es, LFTs, cardiac assessment/ ECG Tests to OK/Confirm each cycle of chemo: FBC, U&Es, LFTs Supportive drugs with each cycle: High risk antiemetics as per NWLCN guidelines or
as per local policy Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Vinorelbine is a vesicant and must be administered according to NWLCN administration policy. Vinorelbine minibag should be administered over 10minutes with a fast running drip of sodium chloride 0.9% through the same cannula
Dose modifications: Table CAV-SCLC Lung below Reference:
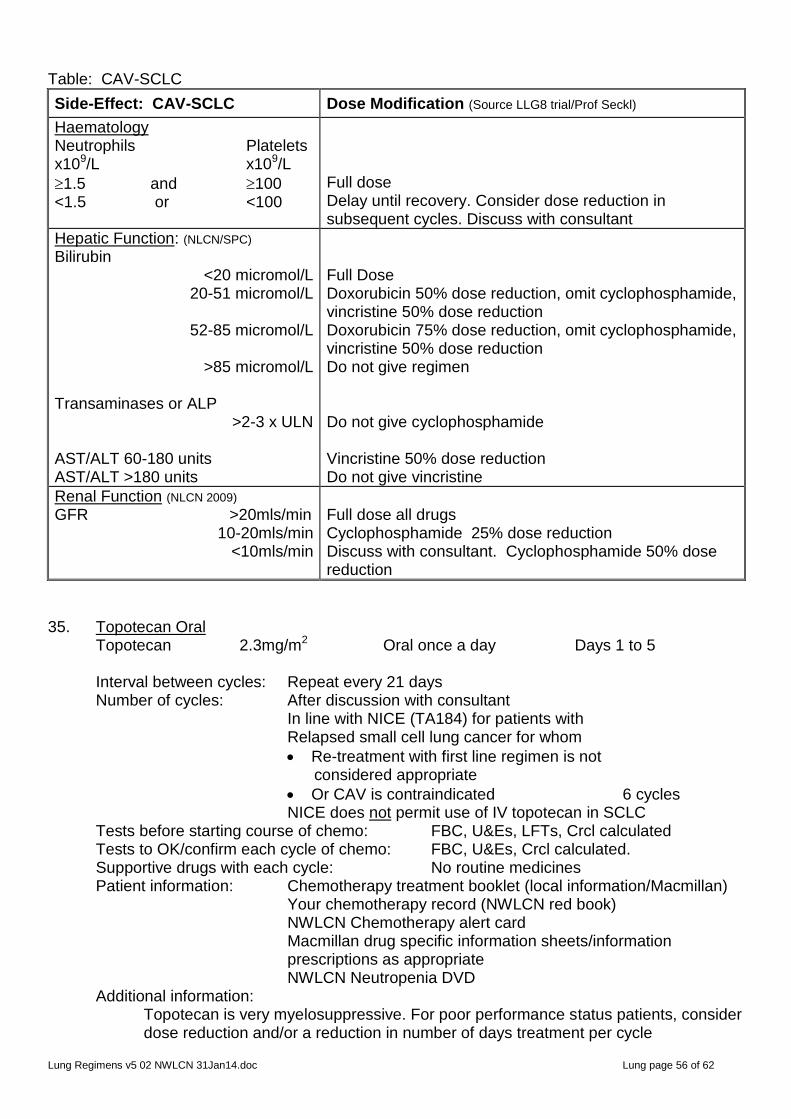
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 56 of 62
Table: CAV-SCLC
Side-Effect: CAV-SCLC
Dose Modification (Source LLG8 trial/Prof Seckl)
Haematology Neutrophils Platelets x109/L x109/L
1.5 and 100 <1.5 or <100
Full dose Delay until recovery. Consider dose reduction in subsequent cycles. Discuss with consultant
Hepatic Function: (NLCN/SPC)
Bilirubin <20 micromol/L
20-51 micromol/L
52-85 micromol/L
>85 micromol/L Transaminases or ALP
>2-3 x ULN AST/ALT 60-180 units AST/ALT >180 units
Full Dose Doxorubicin 50% dose reduction, omit cyclophosphamide, vincristine 50% dose reduction Doxorubicin 75% dose reduction, omit cyclophosphamide, vincristine 50% dose reduction Do not give regimen Do not give cyclophosphamide Vincristine 50% dose reduction Do not give vincristine
Renal Function (NLCN 2009)
GFR >20mls/min 10-20mls/min
<10mls/min
Full dose all drugs Cyclophosphamide 25% dose reduction Discuss with consultant. Cyclophosphamide 50% dose reduction
35. Topotecan Oral Topotecan 2.3mg/m2 Oral once a day Days 1 to 5 Interval between cycles: Repeat every 21 days Number of cycles: After discussion with consultant In line with NICE (TA184) for patients with Relapsed small cell lung cancer for whom
Re-treatment with first line regimen is not considered appropriate
Or CAV is contraindicated 6 cycles NICE does not permit use of IV topotecan in SCLC
Tests before starting course of chemo: FBC, U&Es, LFTs, Crcl calculated Tests to OK/confirm each cycle of chemo: FBC, U&Es, Crcl calculated. Supportive drugs with each cycle: No routine medicines Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Topotecan is very myelosuppressive. For poor performance status patients, consider dose reduction and/or a reduction in number of days treatment per cycle

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 57 of 62
Dose modifications: Table: Topotecan Oral below Reference: Table: Topotecan Oral
Side-effect (Topotecan Oral) Dose Modification (SPC 17Nov10)
Haematology SPC (17Nov10) states that prior to the first cycle of topotecan patients must have baseline
neutrophils 1.5 x109/L, platelets 100 x109/L
and haemoglobin 9 g/dL For subsequent cycles see below; Neutrophils Platelets Haemoglobin x109/L x109/L g/L
1.0 and 100 and 90 <1.0 or <100 or <90 If patient experiences severe neutropenia (<0.5x109/L) for 7 days or more Or Severe neutropenia associated with fever or infection Or If treatment is delayed due to neutropenia Or Platelet count falls below 25x109/L
Full dose Do not give chemo until recovered. Consider dose reduction and see notes below. Discuss with consultant Reduce dose by 0.4mg/m2/day to 1.9mg/m2/day (or subsequently down to 1.5mg/m2/day if necessary). In clinical trials topotecan oral was discontinued if the dose needed to be reduced below 1.5mg/m2/day (SPC)
Diarrhoea .
≤Grade 1 Grade 2
≥ Grade 3
Elderly (SPC) No overall differences in effectiveness were observed between patients over 65 years and younger adult patients. However, in the 2 studies administering both oral and IV topotecan patients older than 65 years receiving oral topotecan experienced an increase in drug related diarrhoea compared to those younger.
Proactive management of diarrhoea with anti-diarrhoeal agents is important. Severe cases of diarrhoea may require administration of oral or intravenous electrolytes and fluids, and interruption of topotecan therapy
Full dose Consider dose reduction specified in grade 3 (SPC) Reduce topotecan dose by 0.4mg/m2/day to 1.9mg/m2/day for subsequent courses.
Renal Impairment (SPC 17Nov10) Patients with SCLC participating in oral topotecan clinical trials had a serum creatinine ≥1.5mg/dl (133micromol/L) or Crcl ≥60mls/min
Dose recommendations in patients with Crcl <60mls/min have not been established

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 58 of 62
Side-effect (Topotecan Oral) Dose Modification (SPC 17Nov10)
Hepatic Impairment (SPC 17Nov10) Pharmacokinetics of oral topotecan has not been specifically studied in patients with impaired hepatic function
Insufficient data to make dose recommendation in hepatic impairment.
Palliative Chemotherapy for Poor Performance Status 36. Oral Etoposide Etop – oral 14Day Etoposide 50mg Oral Twice a day Days 1 to 14
(28 doses) Reduce dose/duration in poor performance status. Interval between cycles: Repeat every 3-4 weeks Number of cycles: 2-6 cycles Tests before starting course of chemo: FBC, U&Es, LFTs, Tests to OK/Confirm each cycle of chemo: FBC, U&Es, LFTs Supportive drugs with each cycle: Low risk antiemetics as per NWLCN guidelines or
as per local policy Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets /information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Dose Modifications: Discuss with consultant Reference: MRC 2001 Stenning Comparison IV vs Oral Etoposide J. Nat Cancer Inst 1997;89(8):577-80

Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 59 of 62
Mesothelioma Section by: Dr Conrad Lewanski, Dr Danielle Power, Dr Tom Newsom-Davis Version; Lung Cancer Regimens v5.02 NWLCN 31Jan14
Section last reviewed: 13thDecember 2013 Section last corrected: 31st January 2014 Approved by Oncology Lung Clinician: December 2013 Review date: December 2015
Mesothelioma First Line 37. Pemetrexed-500/Cisplatin-75 Dexamethasone 4mg BD Oral Twice a day for 3 days starting the day before pemetrexed Sodium chloride 0.9% 1000mls IV over 2 hours Day 1 to run before, during and after pemetrexed 75 Minutes after start of sodium chloride Pemetrexed 500mg/m2 IV over 10-15 mins Day 1 30 Minutes after end of pemetrexed Cisplatin 75mg/m2 IV over 2hours Day 1 Sodium chloride 0.9% 1000mls IV over 2 hours Day 1 Plus MgSO4 and KCl according to local policy Interval between cycles: Repeat every 21 days Number of cycles: In line with NICE (TA135) for patients with WHO status 0 or 1, with advanced, unresectable malignant pleural mesothelioma up to 6 cycles Tests before starting course of chemo FBC, U&Es, LFTs, CrCl calculated. If
<60ml/min do EDTA. Tests to OK/Confirm each cycle of chemo: FBC, U&Es, LFTs, CrCl calculated. Do EDTA if rising serum creatinine Supportive drugs with each cycle: Very high risk antiemetics as per NWLCN
guidelines or as per local policy Dexamethasone as above to reduce the incidence and severity of skin reactions. Vitamin supplementation to reduce toxicity and incidence of grade 3/4 haematological and non-haematological toxicities Folic acid 400microgram oral daily, starting 7 days before 1st pemetrexed dose and continuing for 21days after last pemetrexed dose Vitamin B12 1000micrograms IM. first dose must be given one week before the 1st pemetrexed dose and then once every 3 cycles thereafter, (subsequent doses may be given on the same day as pemetrexed.
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
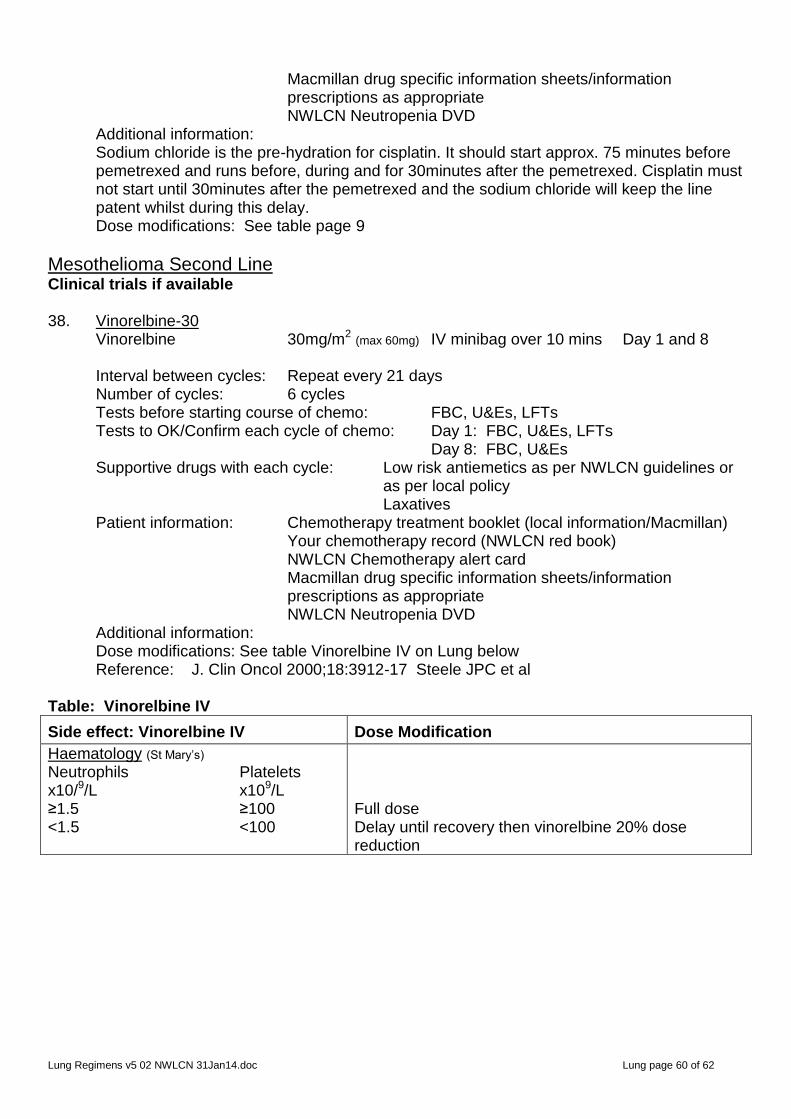
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 60 of 62
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Sodium chloride is the pre-hydration for cisplatin. It should start approx. 75 minutes before pemetrexed and runs before, during and for 30minutes after the pemetrexed. Cisplatin must not start until 30minutes after the pemetrexed and the sodium chloride will keep the line patent whilst during this delay.
Dose modifications: See table page 9
Mesothelioma Second Line Clinical trials if available 38. Vinorelbine-30 Vinorelbine 30mg/m2 (max 60mg) IV minibag over 10 mins Day 1 and 8 Interval between cycles: Repeat every 21 days Number of cycles: 6 cycles Tests before starting course of chemo: FBC, U&Es, LFTs Tests to OK/Confirm each cycle of chemo: Day 1: FBC, U&Es, LFTs Day 8: FBC, U&Es Supportive drugs with each cycle: Low risk antiemetics as per NWLCN guidelines or
as per local policy Laxatives Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Dose modifications: See table Vinorelbine IV on Lung below Reference: J. Clin Oncol 2000;18:3912-17 Steele JPC et al Table: Vinorelbine IV Side effect: Vinorelbine IV
Dose Modification
Haematology (St Mary’s)
Neutrophils Platelets x10/9/L x109/L ≥1.5 ≥100 <1.5 <100
Full dose Delay until recovery then vinorelbine 20% dose reduction
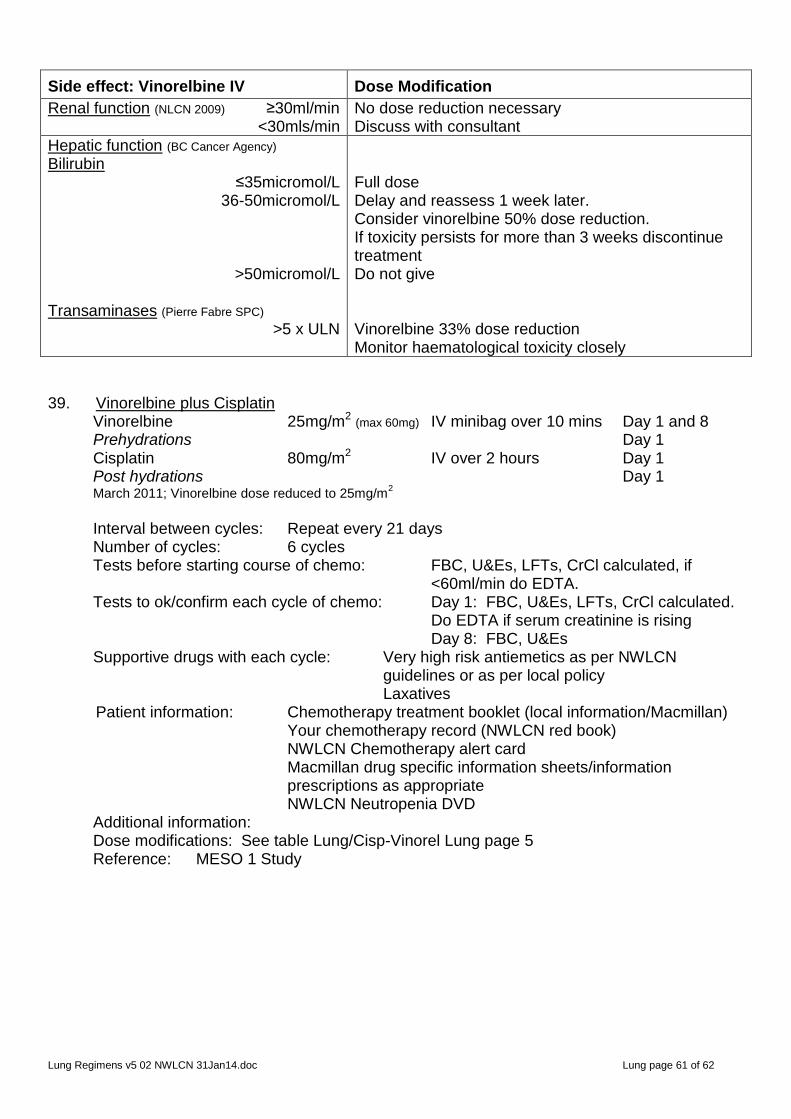
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 61 of 62
Side effect: Vinorelbine IV
Dose Modification
Renal function (NLCN 2009) ≥30ml/min <30mls/min
No dose reduction necessary Discuss with consultant
Hepatic function (BC Cancer Agency)
Bilirubin ≤35micromol/L
36-50micromol/L
>50micromol/L Transaminases (Pierre Fabre SPC)
>5 x ULN
Full dose Delay and reassess 1 week later. Consider vinorelbine 50% dose reduction. If toxicity persists for more than 3 weeks discontinue treatment Do not give Vinorelbine 33% dose reduction Monitor haematological toxicity closely
39. Vinorelbine plus Cisplatin
Vinorelbine 25mg/m2 (max 60mg) IV minibag over 10 mins Day 1 and 8 Prehydrations Day 1 Cisplatin 80mg/m2 IV over 2 hours Day 1 Post hydrations Day 1 March 2011; Vinorelbine dose reduced to 25mg/m
2
Interval between cycles: Repeat every 21 days Number of cycles: 6 cycles Tests before starting course of chemo: FBC, U&Es, LFTs, CrCl calculated, if
<60ml/min do EDTA. Tests to ok/confirm each cycle of chemo: Day 1: FBC, U&Es, LFTs, CrCl calculated.
Do EDTA if serum creatinine is rising Day 8: FBC, U&Es Supportive drugs with each cycle: Very high risk antiemetics as per NWLCN
guidelines or as per local policy Laxatives
Patient information: Chemotherapy treatment booklet (local information/Macmillan) Your chemotherapy record (NWLCN red book) NWLCN Chemotherapy alert card
Macmillan drug specific information sheets/information prescriptions as appropriate NWLCN Neutropenia DVD
Additional information: Dose modifications: See table Lung/Cisp-Vinorel Lung page 5 Reference: MESO 1 Study
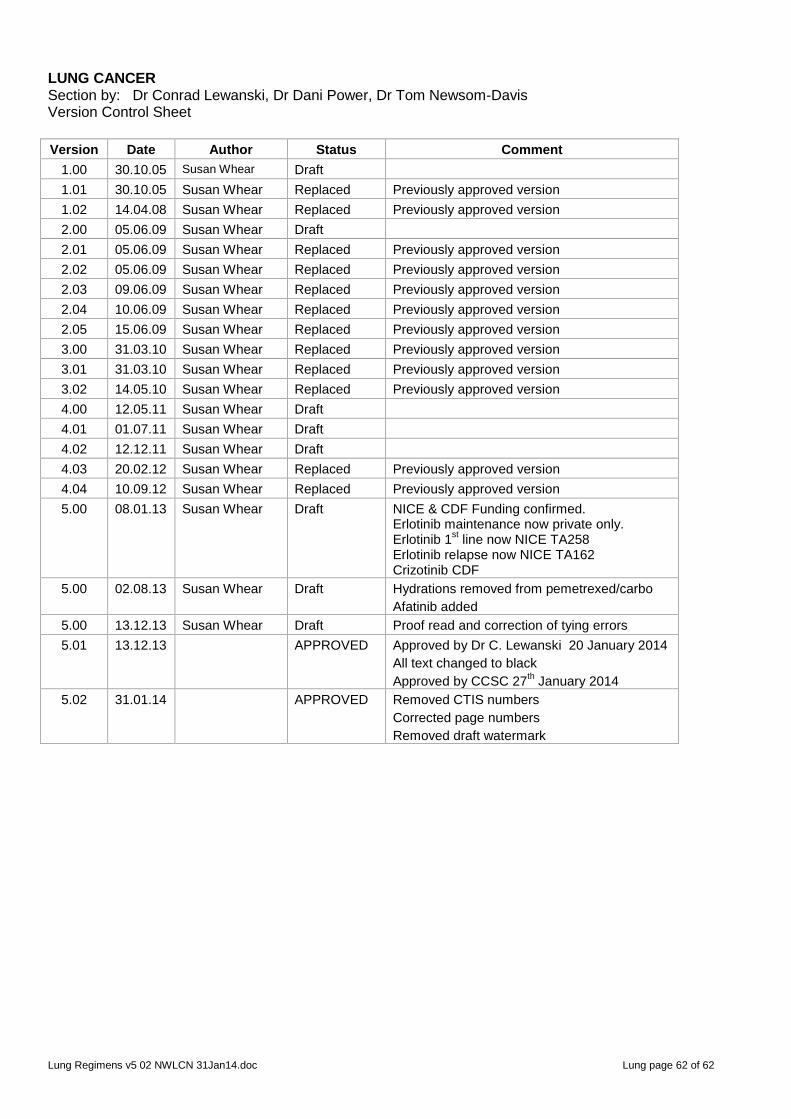
Lung Regimens v5 02 NWLCN 31Jan14.doc Lung page 62 of 62
LUNG CANCER Section by: Dr Conrad Lewanski, Dr Dani Power, Dr Tom Newsom-Davis Version Control Sheet
Version Date Author Status Comment
1.00 30.10.05 Susan Whear Draft
1.01 30.10.05 Susan Whear Replaced Previously approved version
1.02 14.04.08 Susan Whear Replaced Previously approved version
2.00 05.06.09 Susan Whear Draft
2.01 05.06.09 Susan Whear Replaced Previously approved version
2.02 05.06.09 Susan Whear Replaced Previously approved version
2.03 09.06.09 Susan Whear Replaced Previously approved version
2.04 10.06.09 Susan Whear Replaced Previously approved version
2.05 15.06.09 Susan Whear Replaced Previously approved version
3.00 31.03.10 Susan Whear Replaced Previously approved version
3.01 31.03.10 Susan Whear Replaced Previously approved version
3.02 14.05.10 Susan Whear Replaced Previously approved version
4.00 12.05.11 Susan Whear Draft
4.01 01.07.11 Susan Whear Draft
4.02 12.12.11 Susan Whear Draft
4.03 20.02.12 Susan Whear Replaced Previously approved version
4.04 10.09.12 Susan Whear Replaced Previously approved version
5.00 08.01.13 Susan Whear Draft NICE & CDF Funding confirmed. Erlotinib maintenance now private only. Erlotinib 1
st line now NICE TA258
Erlotinib relapse now NICE TA162 Crizotinib CDF
5.00 02.08.13 Susan Whear Draft Hydrations removed from pemetrexed/carbo
Afatinib added
5.00 13.12.13 Susan Whear Draft Proof read and correction of tying errors
5.01 13.12.13 APPROVED Approved by Dr C. Lewanski 20 January 2014
All text changed to black
Approved by CCSC 27th January 2014
5.02 31.01.14 APPROVED Removed CTIS numbers
Corrected page numbers
Removed draft watermark















