Embed Size (px)
Citation preview

THE MAINTENANCEOF A SUSTAINED THROMBOLYTICSTATE IN MAN.II. CLINICAL OBSERVATIONSON PATIENTS WITH MYO-
CARDIAL INFARCTION ANDOTHERTHROMBO-EMBOLIC DISORDERS* t
By ANTHONYP. FLETCHER, SOL SHERRY, NORMAALKJAERSIG, FOTIOS E.SMYRNIOTIS AND SIDNEY JICK
(From the Department of Medicine, Washington University School of Medicine, St. Louis, Mo.)
(Submitted for publication October 24, 1958; accepted February 6, 1959)
Acute thromboembolic occlusive vascular dis-ease is an important cause of human illness andthe possibility of its treatment by measures de-signed to produce dissolution of the causativethrombus or embolus by enzymatic means hasaroused much interest. Two preceding papers(3, 4) have been concerned with mechanisms ofenzymatic clot dissolution and with the establish-ment of intense and prolonged thrombolytic statesin man by the intravenous infusion of strepto-kinase.
These studies established the feasibility of us-ing an induced thrombolytic state as a therapeutictool for the treatment of thromboembolic diseasein the human. However the effect of the throm-bolytic state on infarcted tissue has never beentested and theoretically this effect could be harm-ful. Consequently the aim of the present clinicaltrial has been twofold, first to determine whetherhigh levels of plasma thrombolytic activity werelocally harmless to infarcted tissue and second totest the therapeutic value of this treatment. Thepresent communication describes our experiencewith this type of therapy in several classes ofhuman thromboembolic disease including patientssuffering from early myocardial infarction.
The results suggest that high levels of plasmathrombolytic activity are harmless to infarctedtissue, including the myocardium, and that at leastin a number of patients the clinical evidence wasconsistent with the view that thrombolysis of thecausative thrombus or embolus had occurred.
* This work was supported by grants from the NationalHeart Institute (H3745), Bethesda, Md., and LederleLaboratories Division, American Cyanamid Co., PearlRiver, N. Y.
t Presented in part at the 70th and 71st Meetings ofthe Association of American Physicians, Atlantic City,N. J., 1957 and 1958 (1, 2).
METHODS
Assay methods, materials and details of streptokinase 1dosage were as previously described (3, 4). Biochemi-cal and physiological findings obtained in the presentseries but pertaining to the induced thrombolytic statehave been described elsewhere (4). All 45 patients de-scribed in this communication developed and sustainedintense thrombolytic states (plasma activities of 100 to500 Atg. fibrin lysed per ml. plasma per hour) throughoutthe treatment period.
Myocardial infarction series. This group comprised 22patients of whom five were female. The average age ofthe group was 58 years and the age distribution: 30 to40 years, one patient; 40 to 50 years, five patients; 50to 60 years, eight patients; 60 to 70 years, two patients;and 70 to 80 years, six patients.
No patient was included in the series unless the clini-cal history and findings were of diagnostic significance,the electrocardiographic changes were confirmatory andreview of serial transaminase (SGO-T) assays sustainedthe diagnosis. Theoretically greater benefit should fol-low the early rather than the late use of thrombolytictherapy and consequently patients were treated as soonafter the onset of infarction as was practicable. The pa-tients have been divided into two groups, a main onecomprising 19 patients in whom thrombolytic treatmentwas started five to 16 hours (average nine hours) fromthe time of onset of symptoms and a subsidiary one ofthree patients in whom treatment was delayed 34 to 65hours after the onset of the illness. All of the latter pa-tients died and their course is considered in the sectionon autopsy evidence.
The main group contained five patients known to havebeen hypertensive for three to 15 years, two of whom hadradiologically demonstrable cardiac enlargement. Twopatients were known to have had previous attacks ofmyocardial infarction and this diagnosis had been stronglysuspected in a third. Three patients were obese (20 to40 per cent over ideal weight) and four patients wereconsidered to have suffered from unusually severe andprotracted pain following the onset of infarction. Thoughthree patients showed substantially depressed blood pres-sure, signs of shock were present in only one. Two pa-
1 Streptokinase was kindly supplied by Dr. J. Rueg-segger, Lederle Laboratories, Pearl River, N. Y.
1111

FLETCHER, SHERRY, ALKJAERSIG, SMYRNIOTIS ANDJICK
tients showed signs of early congestive failure but thesewere mild. All patients received streptokinase by in-travenous drip for 30 hours in sufficient doses to producea sustained and intense thrombolytic state and the lasteight patients in the series received supplemental intra-venous hydrocortisone for the duration of the infusionperiod (4). The initial organization of the trial in-volved a "double-blind" design and the decision as totreatment in the first 23 patients was made by the drawingof a lot. However this design was found to impede thecollection of physiological data (4) and its use wasabandoned, but later reference is made to the 11 con-trol patients in the series.
RESULTS
Pulmonary embolism, thrombophlebitis,botic arterial occlusion, and coronary
ciency
throm-insuffi-
Case histories 1 through 23 (see Appendix)describe the effects of the induced thrombolyticstate in these categories of patients.
Acute myocardial infarction
The clinical course of the patients during the 30hour streptokinase treatment period was rela-tively uneventful and there were no deaths at thistime. Eight of the patients, initially considered tobe gravely ill, improved considerably as did thoseothers whose conditions appeared to be less se-
rious. Two patients after six hours' treatmentexperienced a recurrence of moderately severe
chest pain of one to two hours' duration; in bothinstances the blood pressure fell and remained un-
stable for eight and 12 hours, respectively, thoughother signs of shock were absent. One patientexperienced moderate chest pain after 12 hours'treatment but the blood pressure remained stableand the pain only lasted 30 minutes. Two of thehypertensive patients showed a fall of blood pres-
sure to normotensive levels, a fall that was main-tained for the remainder of the hospital course.
Two patients, whose blood pressure had been ini-tially depressed, showed a rapid rise while on
streptokinase treatment. All patients were startedon DicumarolP therapy prior to the end of theinfusion and, except in two instances, were
maintained on this drug for the remainder of thehospital course. Nine patients received anticoagu-lant treatment after discharge from the hospital.
Later course
Following the initial treatment phase, there wasone death in a 72 year old male, who died threeweeks later from recurrent infarction; the autopsyfindings are described later. Three patients, allmales, experienced episodes of chest pain that mayhave been indicative of recurrent infarction three,six and 10 days, respectively, after the onset of theoriginal infarction. The pain in each instance wasof less than two hours' duration, but in two of thepatients, transient electrocardiographic changesoccurred, though in all of them serial transaminaseassays remained normal and no other evidence ofdeterioration was obtained. Four other patientscomplained intermittently throughout their hos-pital course of mild precordial aching sensations.However, two were nervous patients and in thecase of an obese 74 year old woman abdominaldiscomfort may have contributed to her difficulty.The convalescence of a 53 year old male was de-layed by the development, three weeks after ad-mission, of a severe attack of benign pericarditis,which ultimately resolved without disability. Em-bolic complications were absent from this series.Following discharge from hospital, two patients,respectively six and 12 weeks later, experiencedbouts of chest pain associated with the develop-ment of minor electrocardiographic abnormalities;in each instance the pain rapidly disappeared,serial transaminase assays remained in the normalrange and the patients are now symptom free.
Followup
Followup was usually conducted six monthslater but in four instances only the two monthfollowup is available, though the patients areknown to be alive and well after five months.In two instances followup was oral but all theother patients were fully investigated. Elevenpatients were symptom free and pursuing theirnormal vocation or activities (though in the caseof four elderly patients these were limited); fourpatients, two of whom were working, complainedof dyspnea on unusual exertion though their nor-mal activities were not limited by this disability.The remaining three patients, two of whom wereworking, experienced occasional very mild chestdiscomfort on moderate exertion. Physical ex-amination revealed no unsuspected findings and
1112

CLINICAL EFFECTS OF THE SUSTAINED THROMBOLYTICSTATE
clinically we gained the impression that the grouphad made a satisfactory recovery. Radiologicalexamination disclosed no evidence of aneurysmformation and in 13 of the patients the size of theheart shadow was within the limits of normal.Four patients showed mild to moderate cardiacenlargement, in all cases with enlargement of theleft ventricle, but in two of them, previous chestfilms showed that this enlargement had been pres-ent prior to the present illness. The other twopatients, in whom previous chest films were notavailable, had both previously suffered from myo-cardial infarction and in one of the patients, a clin-ical diagnosis of cardiac enlargement had beenmade prior to the present illness.
Electrocardiographic evidence
Serial electrocardiograms were recorded sev-eral times on the first and second day of therapyand subsequent records were then taken daily un-til the clinical course of the patient had stabilized.In all cases, the electrocardiograms were consid-ered to be either diagnostic of acute myocardialinfarction or consistent with the diagnosis.Weekly or semiweekly records were then obtaineduntil discharge from the hospital. In most in-stances the electrocardiographic evolution of theinfarct was not remarkable. However, in threecases, a subsequent bout of chest pain during theperiod of convalescence was accompanied by a re-currence of ST segment elevations in the leadspreviously involved in the original infarct, but innone did the Q waves change and the SGO-T de-terminations remained within normal limits.
The electrocardiograms were read as showinganterior or anteroseptal myocardial infarction in15 cases, diaphragmatic (posterior) in six casesand left bundle branch block was present in one.Significant Q waves were present initially or de-veloped subsequently in 20 cases. Of the 18 sur-viving patients, followup records (usually five tosix months after the acute infarct) were obtainedin 14 instances and in the remaining four patients,the followup was considered to be of insufficientlength to permit adequate assessment. Four ofthe patients showed a normal electrocardiogramon followup examination (one of the four has aslightly prolonged P-R interval which was prob-ably present prior to the infarct). Three of the
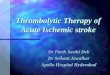
HOURS AFTER INFARCTION
FIG. 1. SERIAL SGO-TRANSAMINASEVALUES IN MYO-CARDIAL INFARCTION (SK TREATED)
The average delay between the time of infarction andthe start of streptokinase treatment was nine hours(range five to 16 hours). The highest average SGO-Tvalues were recorded in the specimens drawn just afterthe start of treatment (12 to 18 hour period) and thevalues thereafter declined.
four patients with normal followup records haddeveloped significant Q waves during the acuteinfarction. Of the 10 patients with abnormal fol-lowup electrocardiograms three were known tohave had abnormal records prior to the acute in-farction. In the remaining seven patients, previ-ous electrocardiograms were not available.
Arrhythmias or conduction disturbances de-veloped in seven patients. In six of these patientsarrhythmias or conduction disturbances were pres-ent prior to treatment with streptokinase, althoughother abnormalities in rhythm or conduction sub-sequently occurred in several of these patientsduring or following streptokinase therapy. Inone of the seven patients, ventricular prematurecontractions, auricular fibrillation and prolongedintraventricular conduction occurred after thestart of therapy, whereas no arrhythmia or con-duction disturbance was previously recorded.The conduction disturbance in this case wasthought to be due to quinidine therapy and thepatient subsequently made an uneventful recovery.In one of the patients who died, right bundlebranch block, ventricular premature contractionsand atrial tachycardia with block were present in-termittently before death. In another, ventricu-lar premature contractions and intraventricularconduction disturbance were present and this pa-tient also died. In the remaining five cases whosurvived, ventricular premature contractions were
1113

FLETCHER, SHERRY, ALKJAERSIG, SMYRNIOTIS ANDJICK
present in four, atrial fibrillation in three, pro-longed P-R interval in one and right bundlebranch block in one. These ectopic rhythms wereall transient. Right bundle branch block remainedin one case and prolonged P-R interval remainedin one.
Transaminase determinations (SGO-T)
The induced thrombolytic state does not alterSGO-T values (4) and consequently assay forthis enzyme could be used to follow the patient'sprogress. Figure 1 shows the combined SGO-Tdeterminations in Group 1 patients over a two dayperiod; the time scale corresponds, in the conven-tional manner, to hours after the onset of infarc-tion. The shape of the curve appears to differfrom that usually found in myocardial infarctionas peak values were noted as early as 15 hoursand the average level had almost returned to nor-mal by the third day. Comparison between thestreptokinase treated patients and those in thedouble-blind control group would at first sightappear to support this hypothesis, for thoughtransaminase values in the two groups were ini-tially similar (p > 0.1), the later readings (ob-tained between 30 to 50 hours) showed the con-trol values to be higher (p = 0.05). However,comparatively little weight can be attached to thisfinding as the control data show evidence of sam-pling bias.
Urokinase excretion
An interesting and unexplained finding in themyocardial infarction patients concerned theirurokinase excretion rates (rates of urinary plas-minogen activator excretion). Normally patientssuffering from myocardial infarction show a sub-stantial rise in urokinase excretion rates for themonth following its onset (p < 0.001) (5), butin the streptokinase treated group this rise occur-
red faster and was of greater magnitude (0.01 >p > 0.001) than in the control group. This find-ing may be of importance (5), but, at present,there is insufficient collateral data for its properinterpretation.
Autopsy evidence from the myocardial infarctionseriesFour patients died, though in the case of a 74
year old woman, originally in shock and in whom
only three hours' treatment was given, autopsypermission was refused.
A 72 year old male died suddenly three weeksafter his initial treatment while receiving Dicuma-rol®. Autopsy revealed a large normally healinginfarct (estimated to be two to four weeks old)and in its center a small very fresh infarct relatedto a new vessel thrombus. Though the coronaryvessels were grossly arteriosclerotic, search re-vealed no older thrombus to correspond with theoriginal infarct. A 53 year old male, admitted 48hours after the onset of infarction, showed shock,paroxysmal auricular fibrillation and an SGO-Tof over 200. He died 14 hours later, probablyfrom ventricular fibrillation. Though autopsyrevealed a huge posterolateral infarct with septalinvolvement, careful dissection of the coronaryvessels revealed only the presence of mild coro-nary sclerosis and failed to demonstrate the pres-ence of a coronary thrombus. A 49 year old male,admitted to hospital 34 hours after the onset ofinfarction, was in gross congestive failure and hisSGO-T peaked at 340. Though his congestivefailure showed an initial response to treatment, hedied from this cause, one day after the termina-tion of streptokinase therapy. Autopsy revealedan old large posterior wall infarct and a new ex-tensive anterolateral area of infarction. A smallthrombus was found arising from an arterio-sclerotic plaque in the left main coronary artery,but since its presence was only demonstrable bymicroscopy and it appeared to be very fresh, itmay have formed after the end of the streptokinasetreatment period. Neither in these nor in otherpatients (4) were myocardial lesions other thanthose attributable to the primary disease stateobserved.
Clinical toxicity
Neither pyrexia nor hypotension was notedafter streptokinase administration. The sole se-rious or potentially serious toxic effects of thetreatment have lain in the development of a hemor-rhagic diathesis, secondary to the induced throm-bolytic state (4). This complication can, at leastin part, be prevented by steroid administration(4). One patient developed, 24 hours after thetermination of the infusion, a 5 X 4 cm. erythe-matous area around the infusion site: This lesion,
114

CLINICAL EFFECTS OF THE SUSTAINED THROMBOLYTICSTATE
thought to represent a sensitization reaction, disap-peared three days later. Though streptokinasesolution occasionally has become infiltrated at theinfusion site, reactions have not resulted exceptin one patient in whom massive infiltration of theleg was produced and in this case the reaction wasslight. Minor thrombophlebitis subsequently de-veloped at the site of the indwelling needle in fourpatients.
DISCUSSION
The evaluation of a new therapeutic procedure indisease states that exhibit variable morbidity andmortality patterns is fraught with the possibilityof error. Evaluation must necessarily rest on aquasistatistical basis involving the observation ofa number of favorable results where the contrarywould normally be expected. Obviously, what-ever the outcome in an individual case, chancecan never be excluded. Accordingly the total casematerial has been presented, individually describedwhere the usual outcome would be customarilyjudged on the severity of the presenting diseasestate (see Appendix), but grouped together, as inthe myocardial infarction patients, where the ini-tial findings constituted a less certain guide to theeventual outcome.
The case histories 1 through 23 (described inAppendix), comprising patients suffering fromdisease states other than myocardial infarction, areconsistent with the view that, at least in a numberof patients, in vivo thrombolysis was produced asa result of the treatment. The series of eventsthat occurred in Patients 1 through 6, sufferingfrom pulmonary embolism, in Patients 7 through10 suffering from thrombophlebitis of the largeveins, in Patients 18 and 19 suffering from ar-terial obstruction and Patient 23 with a fibrinousexudate in the anterior chamber of the eye, thoughperhaps individually explainable as a series ofchance findings, are, taken as a whole, difficult toreconcile with such a view. A corollary to thesefindings would indicate that restoration of bloodflow to an infarcted area is not only of over-allbenefit but also without deleterious effect. Wherefailure was met with Patients 11 through 14 suf-fering from thrombophlebitis and Patients 15through 17 suffering from arterial disease, thereappeared to be an adequate reason for this result,either on the grounds of the unsuitable nature of
the disease condition or on the basis of the ir-reparable structural damage that had alreadyoccurred.
Theoretically there is a danger that the use ofthrombolytic therapy in venous thrombosis mightincrease the likelihood of pulmonary embolism.Though Cases 2, 8 and 10 experienced transientsymptomatic episodes that could have been indica-tive of pulmonary embolism, it is emphasized thatconfirmation of this diagnosis was not obtained;the patients were suffering from disease conditionswhere spontaneous pulmonary embolism is com-mon and unusual attention was being given to thepatient's symptomatic complaints. We do notregard the danger of pulmonary embolism as acontraindication to the treatment, since even if itwere to occur, rapid lysis of the embolus wouldbe expected to take place (see Patients 1 through6).
It is our present view, based solely on theo-retical conjecture, that thrombolytic treatmentshould be followed by anticoagulant treatment.However, not all our patients have been givenanticoagulant treatment and so far we have seenno ill effects from its omission.
Myocardial infarction presents a difficult thera-peutic problem, because of the numerous etiologicalfactors involved in its causation. The rapid dis-solution of a coronary thrombus by enzymaticmeans could result in reduction of the final areaof muscle infarction, reduction of the degree ofelectrical instability present during the early criti-cal phase of infarction and in the prevention orremoval of mural thrombi. However, the throm-bolytic state could conceivably cause deleteriouschanges within the infarcted area and perhaps in-crease the tendency to or the degree of subintimalhemorrhage. Moreover in those instances of in-farction, unrelated to thrombosis, benefit couldonly occur by the prevention of or by the lysis ofmural thrombi. These problems were similar insubstance but more acute in nature than those in-volving the therapeutic use of anticoagulants inthis condition. In contrast, while the aim of anti-coagulant treatment is to limit myocardial dam-age and prevent further spread of infarction, theaim with thrombolytic therapy is to restore thecirculation and permit the restoration of functionto still viable, but otherwise doomed, tissue.Clearly the timing of thrombolytic therapy is criti-
1115

FLETCHER, SHERRY, ALKJAERSIG, SMYRNIOTIS ANDJICK
cal and, theoretically at least, it should be startedas soon as possible after the onset of infarction.This therapeutic indication is fortunate since byfar the greatest mortality occurs in the first 24hours of the disease and conventional therapy islargely unavailing. Furthermore, thrombolytictherapy if used late in the disease, after the forma-tion of mural thrombi, might carry a serious riskof causing arterial embolism.
Evidence concerning the effect of the throm-bolytic state on the myocardial lesion was of a dualnature, that derived from the living and that ob-tained by postmortem examination. The threepatients treated late in the illness, 34 to 65 hoursafter its onset, died during the acute phase of thedisease. These patients were not included in themain group as the delay placed them outside thescope of the study and their treatment was onlyreluctantly undertaken as a measure of last resort.Postmortem examination was also made on theone patient in the main series who died threeweeks after his initial treatment. Pathologicalstudy was consistent with the belief that in vivothrombolysis had been produced and also with theview that the thrombolytic state had exerted noharmful effect upon the evolution of the infarcts.Of collateral interest are two reports (6, 7) of-fering suggestive evidence that the relief, by en-zymatic means, of acute coronary obstruction inthe dog lessens the final degree of myocardialdamage.
Patients treated early in the course of the dis-ease all survived the acute phase of the illness,though one of the 19 patients died three weekslater from recurrent infarction. It is probablethat these patients suffered from myocardial le-sions of greater than average severity since the in-cidence of features indicative of a poor prognosiswas high and the referring physicians naturallytended to favor the use of this treatment in pa-tients whose prognostic outlook, under conven-tional treatment, was deemed to be relatively un-favorable. The hospital course and the followupperiod have been devoid of unusual incident andit is our impression that the survivors have madegood recoveries. Radiological examination hasfailed to reveal aneurysm formation and the inci-dence of cardiac enlargement has been very low.The fact that four of 14 patients showed normalelectrocardiographic findings six months after the
attack is unusual, especially when three of these14 patients were known to have shown abnormalECG findings prior to the attack. Though themortality rate of the group appeared to be unusu-ally low testing of its statistical significance againstthe mortality rate in patients treated as double-blind controls (four out of 11 died) and alsoagainst the hospital mortality during the time ofthe trial (19.5 per cent) gave in each instance p =0.2 (x2 with Yates correction). Thus though ourfindings may suggest that the patients derivedclinical benefit from the treatment, on the crucialquestion of mortality we would have seen as fa-vorable a series, by chance alone, one trial in five.Clearly, while the number of patients treated hasbeen insufficient to arrive at a decision that benefitoccurred, it does appear to be sufficient to giveconsiderable assurance that certain theoreticalobjections that could be raised to this form oftreatment are without practical basis.
Though clinically we have been gratified by theresults of this treatment we would emphasize thatthese observations are of a preliminary nature andserve only to establish that the present therapeuticapproach is feasible. Clinical, pathological andbiochemical evidence all indicate that plasmathrombolytic states are harmless to the infarctedmyocardium and that the development of throm-bolytic therapy for the treatment of myocardialinfarction will not be impeded by deleterious con-sequences, secondary to its primary effect.
APPENDIX
Case histories 1 through 23. The effect of the inducedthrombolytic state upon the clinical course of patientssuffering from pulmonary embolism, thrombophlebitis,thrombotic arterial occlusion and coronary insufficiency.
Pulmonary embolism
Six patients, all gravely ill, have been treated. How-ever, absolute proof of the diagnosis was lacking inCase 1, a 32 year old male. Though there was adequateclinical evidence to support the diagnosis, his poor gen-eral condition precluded the obtaining of radiologicalconfirmation. He died two days after streptokinasetreatment from congestive cardiac failure of rheumaticetiology and, at autopsy, dissection of the pulmonaryvascular tree disclosed no abnormality.
Case 2. The successful treatment of a 53 year oldfarmer, suffering from acute cor pulmonale, secondaryto repeated pulmonary emboli has been previously re-ported (1).
1116

CLINICAL EFFECTS OF THE SUSTAINED THROMBOLYTICSTATE
Case 3. A 38 year old female gave a history suggestiveof four episodes of pulmonary embolization in two days;physical signs and chest film confirmed the diagnosis.Her last episode of pulmonary infarction, which oc-curred two hours before the start of treatment, wasmassive and had caused brisk hemoptysis. Rapid clini-cal improvement followed streptokinase therapy, nofurther emboli occurred and signs of phlebothrombosispresent in the calf rapidly regressed. Radiological ex-amination showed almost complete clearing of thechest in a two day period. This patient was awaitingoperation for uterine myomata and it was noteworthythat successful treatment was impeded neither by thepresence of vaginal bleeding nor by the hemoptysis.The extent of bleeding was not increased from eithersite by the establishment of a thrombolytic state.
Case 4. A 54 year old male had been treated one yearpreviously for multiple pulmonary embolization sec-ondary to thrombophlebitis. Conservative managementled to an excellent functional recovery. Three days priorto admission he experienced pain and tenderness in theleft popliteal region and shortly prior to admission, left-sided pleuritic chest pain, cough, sweating and dyspnea.He was acutely ill exhibiting cyanosis, tachycardia,tachypnea and had a cold clammy skin with a blood pres-sure of 80/60. The electrocardiogram showed a par-tial right bundle branch block and other signs suggestiveof pulmonary embolism. Twelve hours treatment withheparin and oxygen with a continuous norephinephrinedrip to maintain the blood pressure produced no improve-ment. Rapid improvement followed streptokinase treat-ment and after 10 hours his blood pressure rose tonormal values and remained stable without the use ofnorepinephrine. Cyanosis disappeared and oxygen wasdispensed with at the end of streptokinase treatment. Histransaminase (S-GOT) rose to over 200 units per ml.and, though this finding was regarded as rather unusualfor pulmonary embolism, his electrocardiogram returnedto normal after five days. Three days later despite theuse of Dicumarol®, the physical signs of acute throm-bophlebitis were apparent in the left thigh. In view ofhis history, left femoral ligation was performed and hewas discharged shortly afterwards symptom free exceptfor the residual functional effects of the femoral ligation.
Case 5. A 47 year old male was discharged fromhospital 14 days after the performance of a subtotalgastrectomy. Three days later the patient was seized byshaking chills and noted the sudden onset of severe painin the right chest. He was cyanosed, hypotensive andhad physical findings consistent with multiple pulmonaryembolism, a diagnosis confirmed radiologically. Thepatient's condition deteriorated rapidly and he died 16hours later, but for the last seven hours he received strep-tokinase therapy. Autospy revealed the primary causeof death to be generalized peritonitis secondary to aleaking suture line, but though three areas of recentlyinfarcted lung tissue were found, dissection of the pul-monary vascular tree revealed no emboli.
Case 6. A 43 year old female developed, followinghysterectomy, pelvic vein thrombosis. Despite adequate
treatment with Dicumarol®, repeated pulmonary em-bolism occurred over a 35 day period. Following strep-tokinase therapy, her chest film cleared and no furtherepisodes of embolization occurred.
ThrombophlebitisEight patients were treated in this group and though
patients suffering from severe clinical manifestationssecondary to lesions of large veins responded well tostreptokinase treatment, other patients with lesions ofsmall veins and few clinical manifestations, except thoseof local disease, apparently did little or no better thanwith conventional therapy. We attribute this somewhatparadoxical response to the fact that whereas with dis-ease of the large veins clinical disability is related pri-marily to venous obstruction, this fact is of little im-portance in disease of small veins, inflammation of thevein wall being the predominant clinical lesion.
Case 7. A 44 year old woman, who had had severalhospital admissions on account of idiopathic steatorrhea.developed acute ileofemoral thrombophlebitis secondaryto an indwelling catheter in the inferior vena cava.Three days' streptokinase therapy produced a rapidresolution of the condition. Her hospital stay was pro-longed on account of the intestinal disorder but ondischarge there was no evidence of venous insufficiency.
Case 8. A 53 year old male suffered from ileofemoralthrombophlebitis secondary to trauma and respondedrapidly to streptokinase therapy. During the course oftreatment he developed transient symptoms suggestiveof pulmonary embolism but further evidence to supportthis diagnosis could not be obtained. On discharge fromthe hospital eight days later there were no signs of ve-nous insufficiency.
Case 9. A 78 year old man with gouty arthritis de-veloped ileofemoral thrombophlebitis. The response totreatment was slower than in the other two cases andhe also developed an exacerbation of gout. Howeverhis leg was free from edema on discharge though he waswearing an elastic support. Two months later ileo-femoral thrombophlebitis recurred, temporary shortage ofstreptokinase prevented his retreatment and despite theuse of anticoagulants he developed a marked post-phlebitic syndrome.
Case 10. A 46 year old male developed calf, poplitealand femoral thrombophlebitis, following injury. Re-sponse to streptokinase therapy was very satisfactory andhe left the hospital without disability. During the firstday of treatment he experienced transient symptoms thatcould have been due to pulmonary embolism but in-vestigation failed to confirm the diagnosis.
Cases 11 and 12. Both suffered from long standingthrombophlebitis of the calf and though both were im-proved following streptokinase therapy, the improvementcould well have been a chance finding and was unimpres-sive.
Cases 13 and 14. These two patients had thrombophle-bitis of superficial veins and though clinical symptomsabated rapidly following treatment, venous cords re-mained palpable.
1117

FLETCHER, SHERRY, ALKJAERSIG, SMYRNIOTIS AND JICK
Peripheral arterial occlusions
Six patients have been treated.Cases 15, 16 and 17. All were elderly patients suffer-
ing from acute obstruction to the femoral artery. Thepatients were treated with streptokinase after extensiveand wholly unsuccessful surgical intervention had beenundertaken in each patient. Though in one instance apreviously absent popliteal pulse returned after treat-ment, lasting benefit was not obtained. Two patientsdied, one from myocardial infarction six weeks later,the other from acute renal tubular necrosis followingsurgery. Probably the condition of the artery wall afterunsuccessful surgical intervention is such as to pre-clude other treatment.
Case 18. One year previously an arterial homografthad been inserted to bridge the left iliac and femoral ar-teries in this 61 year old female. The limb circulationfailed suddenly and, on examination, signs of acute ar-terial insufficiency were apparent midway up the thigh.The graft, which was easily palpable throughout thegreater part of its course, was hard and pulseless. Eighthours after the start of streptokinase therapy the su-perior one-third of the graft was pulsatile. However,by next morning when treatment was restarted, the wholegraft was again hard and pulseless and further treat-ment failed to change its condition. Nevertheless, per-haps because the graft thrombosis was an incidental find-ing, the circulation of the leg improved during therapy.Gangrene did not develop and the patient's ambulatoryability on discharge from hospital was similar to thatpresent before her current admission.
Case 19. A 66 year old female, bedridden as the re-sult of a previous vascular accident, was admitted suffer-ing from pneumonia of great severity. Despite the ex-hibition of antibiotics her condition remained serious.Blood pressure could only be maintained by the ad-ministration of intravenous norepinephrine over the firstthree days. On the fourth day, two localized patches ofgangrene were apparent on the left limb in the distribu-tion of the anterior tibial artery. On the fifth day shedeveloped signs of acute arterial insufficiency in the limbwith the border of temperature change 5 cm. above theknee. During streptokinase therapy oscillometric pulsa-tions were again recorded in the lower limb, musclepower returned to the foot and the temperature differ-ential between the legs diminished to an insignificant dif-ference. However the original patches of gangrene wereunaltered by the treatment and since owing to her previ-ous bedfast state mobilization was impossible, below theknee amputation was performed.
Miscellaneous
This group consisted of three patients with coronary
insufficiency and one patient with an intraocular fibrinousexudate.
Case 20. A 61 year old male suffering from mild coro-
nary insufficiency received therapy; his course thereafterwas uneventful.
Case 21. A 44 year old male experienced an attack ofsevere and prolonged chest pain with electrocardiographicabnormalities and a slightly raised SGO-T assay; how-ever Q waves did not subsequently develop. Following 30hours' streptokinase treatment his course was satisfac-tory and he is now, five months later, symptom free.
Case 22. A 64 year old emaciated female was admittedwith gross congestive cardiac failure, an enlarged heartand severe chest pain. After an initial response to ther-apy she suddenly died three weeks later. Autopsy re-vealed severe coronary artery disease, several areas of oldhealed infarcted tissue and one fresh infarct estimatedto be no more than two days old.
Case 23 (1). A 71 year old male developed an intra-ocular infection following a cataract operation. Despiteintensive antibiotic therapy a dense fibrinous exudate de-veloped and completely filled the anterior chamber.Four days of streptokinase treatment was given andserial slit lamp examination revealed progressive resolu-tion until, at the end of treatment, the anterior chamberwas free of exudate. It is known that spontaneous reso-lution of such exudate seldom if ever occurs and thispatient was thought to provide a rather unique demon-stration of in vivo fibrinolysis.
SUMMARY
Fifty patients suffering from several varietiesof acute occlusive thromboembolic disease, includ-ing 22 patients suffering from early acute myo-cardial infarction, were treated by the intravenousinfusion of streptokinase in massive doses and forprolonged periods. Intense plasma thrombolyticactivity (100 to 500 /Ug. fibrin lysed per hour perml. plasma) developed and was maintained for 30or more hours.
The thrombolytic state produced no importantdeleterious consequence and there was evidence,at least in a number of patients, to suggest thatin vivo thrombolysis had been produced. The lowmortality rate and the relative absence of com-plications experienced by the myocardial infarc-tion patients suggested that the induced thrombo-lytic state was harmless to the infarcted myo-cardium.
ACKNOWLEDGMENTS
We are greatly indebted to Dr. Edward Massie andMiss Margaret Peteler for invaluable assistance with theelectrocardiographic examinations; to Dr. Jack Hassonwho performed the majority of the autopsy examinations;to Mr. Charles Chisenhall and Miss Geraldine Nelson fortechnical assistance and to many physicians at the Jew-ish and Barnes Hospitals who referred patients fortreatment.
1118

CLINICAL EFFECTS OF THE SUSTAINED THROMBOLYTICSTATE
REFERENCES
1. Sherry, S., Fletcher, A. P., Alkjaersig, N., andSmyrniotis, F. E. An approach to intravascularfibrinolysis in man. Trans. Ass. Amer. Phycns1957, 70, 288.
2. Fletcher, A. P., Alkjaersig, N., Smyrniotis, F. E., andSherry, S. The treatment of patients sufferingfrom early myocardial infarction by massive andprolonged streptokinase therapy. Trans. Ass.Amer. Phycns 1958, 71, 287.
3. Alkjaersig, N., Fletcher, A. P., and Sherry, S. Themechanism of clot dissolution by plasmin. J. clin.Invest. 1959, 38, 1086.
4. Fletcher, A. P., Alkjaersig, N., and Sherry, S. Themaintenance of a sustained thrombolytic state in
man. I. Induction and effects. J. clin. Invest.1959, 38, 1096.
5. Smyrniotis, F. E., Fletcher, A. P., Alkjaersig, N., andSherry, S. Urokinase excretion in health and itsalterations in certain disease states. Thromb.Diath. haem. 1959, 3, 257.
6. Agress, C. M., Jacobs, H. I., Binder, M. J., Clark,W. G., Kaplan, L., Lederer, M., and Glassner,H. F. Intravenous trypsin in experimental myo-
cardial infarction. Circulat. Res. 1954, 2, 397.7. Ruegsegger, P., Nydick, I., Hutter, R. C., Freiman,
A. H., Bang, N. U., Cliffton, E. E., and LaDue,J. S. Fibrinolytic (plasmin) therapy of experi-mental coronary thrombi with alteration of theevolution of myocardial infarction. Circulation1959, XIX, 7.
1119