Embed Size (px)
Citation preview

Management of Giant Retinal Tears without Scleral Buckling Use of Radical Dissection of the Vitreous Base and Per/luoro--octane and Intraocular Tamponade
Allan E. Kreiger, MD, Hilel Lewis, MD
The introduction of intraoperative perfluorocarbon liquids in the management of giant retinal tears has allowed exact anatomic reapposition of the retina and the giant
retinal tear. Therefore, the authors managed 11 eyes with giant retinal tears and no proliferative vitreoretinopathy without scleral buckling. Maximum removal of the basal vitreous gel was performed in all cases, and perfluoro-octane was used intraoperatively to unfold the inverted posterior flap and reattach the retina completely. Endophotocoagulation was applied to the edges of the tear and perfluoropropane or silicone oil was used as an intraocular tamponade. Although 1 eye required reoperation for a redetachment from posterior proliferative vitreoretinopathy, all retinas were reattached with final visual acuity of 5/200 or better in 9 eyes. Eight additional major procedures were necessary in seven eyes: removal of silicone oil in four (with removal of peri silicone proliferation in three), repeat vitrectomy and membrane removal with photocoagulation twice in one eye, cataract extraction in one eye, and removal of a macular pucker in one eye. Four eyes required postoperative fluid-gas exchange and three eyes had tissue plasminogen activator injections into the anterior chamber for postoperative fibrin reactions. Ophthalmology 1992;99:491-497
Anatomic and visual results of repair of retinal detachment from giant retinal tears have steadily improved since the development of vitreous surgery. 1 Modem surgical techniques have resulted in better intraoperative management of the retina and the giant retinal tear so that closure of the break at the end of the procedure is assured. Perfluorocarbon liquids have been shown to greatly facilitate this goal.2 The problem of recurrent detachment,
however, continues to be vexing. A number of factors contribute to redetachment, including extension of the giant tear, formation of new retinal breaks, or reopening of tears from proliferative vitreoretinopathy (PVR). Traditionally, scleral buckling has been used in an attempt to minimize such complications.
Originally received: October 13, 1991. Revision accepted: December 5, 1991.
From the Department of Ophthalmology, UCLA School of Medicine, Jules Stein Eye Institute, Los Angeles.
Presented at the American Academy of Ophthalmology Annual Meeting, Anaheim, October 1991.
Reprint requests to Allan E. Kreiger, MD, Jules Stein Eye Institute, UCLA Medical Center, 100 Stein Plaza, Los Angeles, CA 90024-7007.
Scleral buckles are believed to reduce early and late traction within the vitreous base. Thus, they insure that the giant retinal tear will remain closed and will not extend, and they decrease the likelihood of recurrent retinal detachment due to the formation of new anterior retinal breaks. 1,3-10 Conversely, scleral buckling procedures have been suspected to complicate the closure of giant retinal tears because of their distortion of the shape of the eye, their tendency to exacerbate "slippage" of the retina posteriorly, and the possibility that the additional trauma they cause might lead to PVR.2,11,12 It is also plausible
491
..r:..
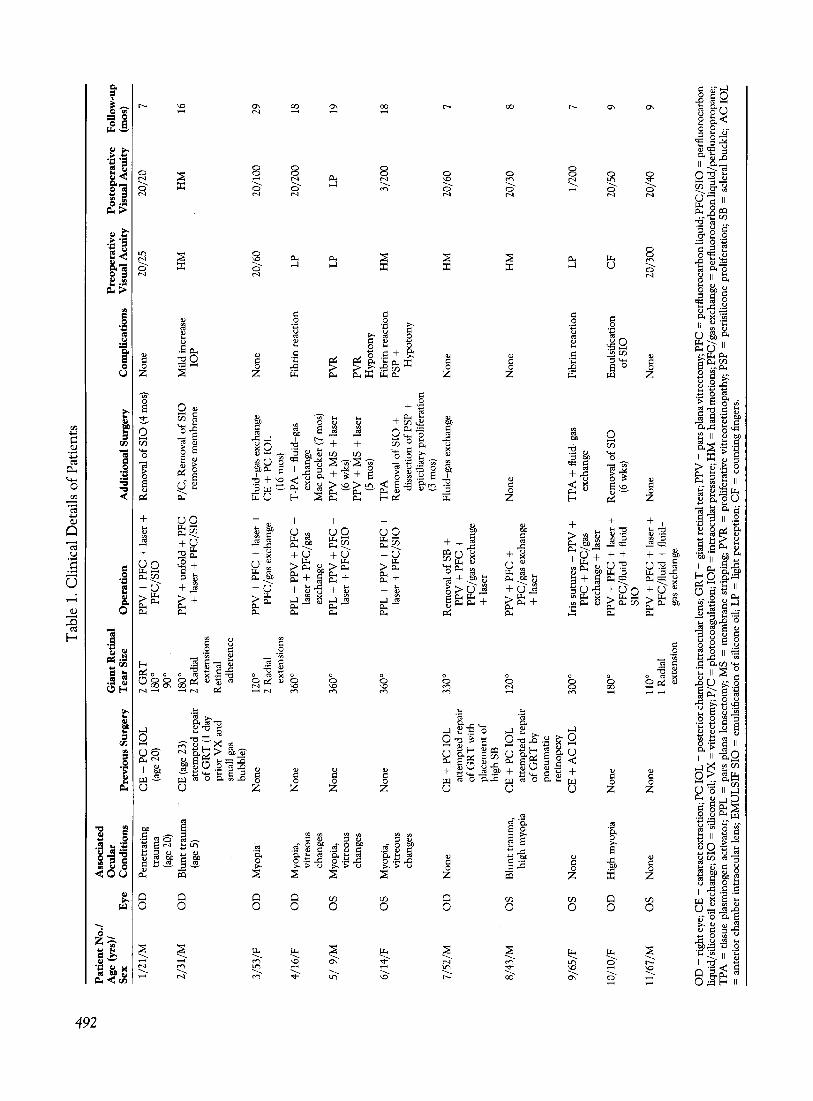
Tab
le 1
. Cli
nica
l D
etai
ls o
f P
atie
nts
\0
N
Pat
ien
t N
o.!
A
ssoc
iate
d A
ge (
yrs)
/ O
cula
r G
ian
t R
etin
al
Pre
op
erat
ive
Po
sto
per
ativ
e F
ollo
w-u
p S
ex
Eye
C
ondi
tion
s P
revi
ous
Sur
gery
T
ear
Size
O
per
atio
n
Add
itio
nal S
urge
ry
Com
plic
atio
ns
Vis
ual A
cuit
y
Vis
ual
Acu
ity
(m
os)
1/21
/M
OD
P
enet
rati
ng
CE
+ P
C 1
0L
2
GR
T
PP
V +
PF
C +
lase
r +
R
emov
al o
f S
IO (4
mos
) N
one
20/2
5 20
/20
7 tr
aum
a (a
ge 2
0)
180
0 P
FC
/SIO
(a
ge 2
0)
900
2/3
1/M
O
D
Blu
nt t
raum
a C
E (a
ge 2
3)
180
0 P
PV
+ u
nfol
d +
PF
C
P /C
, R
emov
al o
f S
IO
Mild
inc
reas
e H
M
HM
16
(a
ge 5
) at
tem
pted
rep
air
2 R
adia
l +
lase
r +
PF
C/S
IO
rem
ove
mem
bran
e lO
P
ofG
RT
(1 d
ay
exte
nsio
ns
pri
orV
X a
nd
Ret
inal
sm
all
gas
adhe
renc
e bu
bble
)
3/5
3/F
O
D
Myo
pia
Non
e 12
00
PP
V +
PF
C +
lase
r +
F
luid
-gas
exc
hang
e N
one
20/6
0 20
/100
29
2
Rad
ial
PF
C/g
as e
xcha
nge
CE
+ P
C 1
0L
ex
tens
ions
(1
6 m
os)
4/1
6/F
O
D
Myo
pia,
N
one
360
0 PP
L +
PP
V +
PF
C +
T
-PA
+ fl
uid-
gas
Fib
rin
reac
tion
L
P 20
/200
18
vi
treo
us
lase
r +
PF
C/g
as
exch
ange
ch
ange
s ex
chan
ge
Mac
puc
ker
(7 m
os)
5/9
/M
OS
M
yopi
a,
Non
e 36
00
PPL
+ P
PV
+ P
FC
+
PP
V +
MS
+ la
ser
PV
R
LP
LP
19
vitr
eous
la
ser
+ P
FC
/SIO
(6
wks
) ch
ange
s P
PV
+ M
S +
lase
r P
VR
(5
mos
) H
ypot
ony
6/14
/F
OS
M
yopi
a,
Non
e 36
00
PPL
+ P
PV
+ P
FC
+
TP
A
Fib
rin
reac
tion
H
M
3/20
0 18
vi
treo
us
lase
r +
PF
C/S
IO
Rem
oval
of S
IO +
PS
P +
ch
ange
s di
ssec
tion
of
PSP
+
Hyp
oton
y ep
icili
ary
prol
ifer
atio
n (3
mos
)
7/52
/M
OD
N
one
CE
+ P
C 1
0L
33
00
Rem
oval
of
SB +
F
luid
-gas
exc
hang
e N
one
HM
20
/60
7 at
tem
pted
rep
air
PP
V +
PF
C +
o
fGR
Tw
ith
P
FC
/gas
exc
hang
e pl
acem
ent o
f +
lase
r hi
ghS
B
8/4
3/M
O
S
Blu
nt tr
aum
a,
CE
+ P
C I
OL
12
00 P
PV
+ P
FC
+
Non
e N
one
HM
20
/30
8 hi
gh m
yopi
a at
tem
pted
rep
air
PF
C/g
as e
xcha
nge
ofG
RT
by
+ la
ser
pneu
mat
ic
reti
nope
xy
9/65
/F
OS
N
one
CE
+ A
C I
OL
30
00
Iris
sut
ures
+ P
PV
+
TP
A +
flui
d-ga
s F
ibri
n re
acti
on
LP
1/20
0 7
PF
C +
PF
C/g
as
exch
ange
ex
chan
ge +
lase
r
1O/1
0/F
O
D
Hig
h m
yopi
a N
one
1800
PP
V +
PF
C +
lase
r +
R
emov
al o
f SIO
E
mul
sifi
catio
n C
F
20/5
0 9
PF
C/f
luid
+ fl
uid
(6w
ks)
ofS
IO
SIO
11/6
7/M
O
S
Non
e N
one
110
0 P
PV
+ P
FC
+ la
ser +
N
one
Non
e 20
/300
20
/40
9 1
Rad
ial
PF
C/f
luid
+ fl
uid-
exte
nsio
n ga
s ex
chan
ge
OD
= ri
ght e
ye; C
E =
cat
arac
t ext
ract
ion;
PC
10
L =
pos
teri
or c
ham
ber i
ntra
ocul
ar le
ns; G
R T
= g
iant
ret
inal
tear
; PP
V =
par
s pl
ana
vitr
ecto
my;
PF
C =
per
fluo
roca
rbon
liqu
id; P
FC
/SIO
= p
erfl
uoro
carb
on
liqu
id/s
ilic
one
oil e
xcha
nge;
SIO
= s
ilico
ne o
il; V
X =
vit
rect
omy;
P /C
= p
hoto
coag
ulat
ion;
lO
P =
intr
aocu
lar p
ress
ure;
HM
= h
and
mot
ions
; PF
C/g
as e
xcha
nge
= p
erfl
uoro
carb
on li
quid
/per
fluo
ropr
opan
e;
TP
A =
tis
sue
plas
min
ogen
act
ivat
or;
PPL
= p
ars
plan
a le
nsec
tom
y; M
S =
mem
bran
e st
ripp
ing;
PV
R =
pro
life
rati
ve v
itre
oret
inop
athy
; PS
P =
per
isil
icon
e pr
olif
erat
ion;
SB
= s
cler
al b
uckl
e; A
C I
OL
=
ant
erio
r ch
ambe
r in
trao
cula
r le
ns;
EM
UL
SIF
SIO
= e
mul
sifi
catio
n of
sili
cone
oil;
LP
= li
ght
perc
epti
on;
CF
= c
ount
ing
fing
ers.

Kreiger and Lewis' Management of Giant Retinal Tears
that an irregular eye wall surface might distort the retina lying on the posterior surface of a buckle, create gaping of retinal tissue, and foster recurrence of the detachment. Therefore, authors vary in their opinions regarding whether a scleral buckle is necessary in the management of giant retinal tears without PVR. Most surgeons agree, however, that the presence of PVR preoperatively is an indication for scleral buckling as a part of the repair. 1,3,4,13
This pilot study was done to test the hypothesis that in retinal detachment from giant retinal tears with no PVR, excellent anatomic reapposition of the giant retinal tears facilitated by the intraoperative use of perfluorocarbon liquids, along with meticulous removal of the vitreous in the region of the vitreous base is sufficient to permanently repair the retinal detachment, without the need for scleral buckling.
Subjects and Methods
Table 1 summarizes the clinical details of the 11 eyes included in this study. Entry criteria were: retinal detachment from a giant retinal tear (tear greater than 90 0 with a posteriorly inverted flap), no evidence of PVR, and informed consent. Other patients seen during the same time interval with giant retinal tears and PVR were managed with conventional techniques including scleral buckling. Follow-up ranges from 7 to 29 months (average, 13 months).
Three patients had no previous eye disease, but two of these had prior cataract extraction with posterior chamber intraocular lens implantation. Three patients had a history of trauma (1 penetrating, 2 blunt). There were 6 myopic eyes (3 had vitreous liquefaction, 2 were classified as highly myopic-greater than 10.00 diopters).
Three patients were seen shortly after an attempt to repair the giant retinal tear had failed. The size of the retinal tears varied from 1100 to 3600
• Radial extensions of the tears were noted in 3 eyes, and 1 eye contained 2 separate giant retinal tears (patient 1).
The initial surgical procedure or the reoperation in those three patients referred for reoperation was done without delay in all cases, under general anesthesia. Longterm tamponade was accomplished with intraocular perfluoropropane in six eyes and with silicone oil in five eyes. Indications for the use of silicone were young age (inability to maintain postoperative positioning) in three eyes, intraoperative posterior slipping of the giant retinal tear after perfluorocarbon liquid-air exchange in one eye, and patient preference in another eye. In four of five eyes, the silicone oil has been removed.
Operative Procedure
A standard three-port vitrectomy was performed in all cases. The lens was removed by ultrasonic fragmentation in five of six phakic eyes. The lens capsule was completely removed, as has been previously described. 14 In the four
eyes with previous cataract surgery and pseudophakos, the intraocular lens was left in place.
The posterior vitreous detachment was identified, and the vitreous was removed out to the vitreous base. A special effort was made to trim the residual base down as close to the retina as possible. This was accomplished by deep scleral indentation as shown in Figure 1. The anterior vitreous behind the intraocular lens was removed meticulously in pseudophakic eyes. The anterior retinal flap of the giant retinal tear was resected up to the ora serrata. In eyes undergoing lensectomy, the anterior hyaloid was identified and removed back to its origin at the anterior vitreous base.
Injection of perfluoro-octane as has been described by Chang et af was performed to flatten the posterior retina first and then to unroll and flatten the flap of the giant tear (Fig 2). Simultaneously, subretinal fluid was removed with aspiration through a soft-tipped cannula. Once the tear was completely flat and the subretinal fluid was removed, endophotocoagulation was applied to the anterior and posterior edges of the tear and to the basal retina for 3600 (Fig 3). Either perfluoropropane or silicone oil was exchanged for the perfluoro-octane. In most of the silicone oil cases, a silicone oil-perfluorocarbon liquid exchange was performed. In one eye, a perfluorocarbon liquid-air exchange was performed followed by an air-silicone oil exchange.
Results
When last examined, all of the retinas were attached (Table 1). One of the 11 eyes (patient 5) developed recurrence
Figure 1. The basal vitreous gel is removed using deep scleral depression. The anterior retinal flap of the giant retinal tear is resected up to the ora serrata.
493

Ophthalmology Volume 99, Number 4, April 1992
A
c
of the retinal detachment from PVR, which required 2 further operations to repair.
Nine of 11 eyes needed additional surgery (Table 1). Two eyes had a gas-fluid exchange to maintain the intraocular bubble at an appropriate size. One of these patients needed cataract surgery 16 months later. Three eyes, all with very large tears, had severe enough fibrin reaction in the anterior chamber to indicate injection of tissue plasminogen activator. Of these three eyes, two with intraocular gas had gas-fluid exchanges at the same time. Removal of silicone oil was performed in four eyes. Three of the four had removal of peri silicone proliferation at the same timeY In one eye, the silicone oil has been left in place because of postoperative hypotony.
Two eyes, both with 3600 giant retinal tears, developed
494
Figure 2. After vitrectorny, the retina is reattached (A,S) and the giant tear closed securely (C) with intraocular injection of perfluro-octane and simultaneous internal drainage of the subretinal fluid.
postoperative hypotony. One developed PVR and required repeat vitrectomy and membrane stripping on two occasions. This eye now has retinal reattachment, but the intraocular pressure is low and the visual prognosis is guarded. Another eye had removal of perisilicone proliferation and epiciliary scar tissue at the time of silicone oil removal. Despite retinal reattachment, the intraocular pressure is low.
A macular pucker developed postoperatively in 1 eye (patient 4). This was removed successfully 7 months after surgery; however, the visual acuity returned only to 20/200.
Visual acuity improved in 8 of the 11 eyes. In 2 there was no change, and in 1 the visual acuity dropped from 20/60 preoperatively to 20/100 after cataract extraction

Kreiger and Lewis . Management of Giant Retinal Tears
Figure 3. After the tear is completely flat and the subretinal fluid is removed, endophotocoagulation is applied to the edges of the tear, including the posterior pars plana. This is continued to include the basal retina for 360° (not shown).
16 months later. In general, however, the final visual acuity depended in large measure on whether the macula was detached preoperatively.
Discussion
Although the series is small and the follow-up is limited, the results would tend to support the view that a scleral buckle is not uniformly needed in all cases of giant retinal tears without PVR if one maximally removes the anterior vitreous in the vitreous base and uses perfluorocarbon liquid to insure complete reattachment of the retina and excellent reapposition of the edge of the tear intraoperatively. In only 1 of the 11 eyes was a recurrent detachment noted and this was from posterior PVR that reopened the 360 0 giant retinal tear. It was judged that a scleral buckle would not have prevented this redetachment in any case. In this eye, two further vitrectomies with membrane removal (without a scleral buckle) reattached the retina. Unfortunately, hypotony occurred and the visual prognosis is guarded. It is doubtful that a scleral buckle in this eye, or in the eye of patient 6, which also developed hypotony, would have altered the course or prevented the low pressure. Both eyes in which hypotony developed occurred in 3600 giant tears in children. It is our experience that most cases of hypotony are the result of epiciliary scarring, and it is likely that this was the cause in these two cases rather than some other effect of the surgical procedure.
It should be emphasized that, in this study, a special effort was made to remove as much vitreous as possible and to trim the vitreous base as close to the retina and
pars plana as could be done safely.16 Most vitrectomies do not require such radical removal of tissue, so the technique to do this is not widely used. We believe, however, that the main justification for not using a scleral buckle is the reduction of the risk of subsequent traction within the vitreous base internally so that an external buckle is redundant.
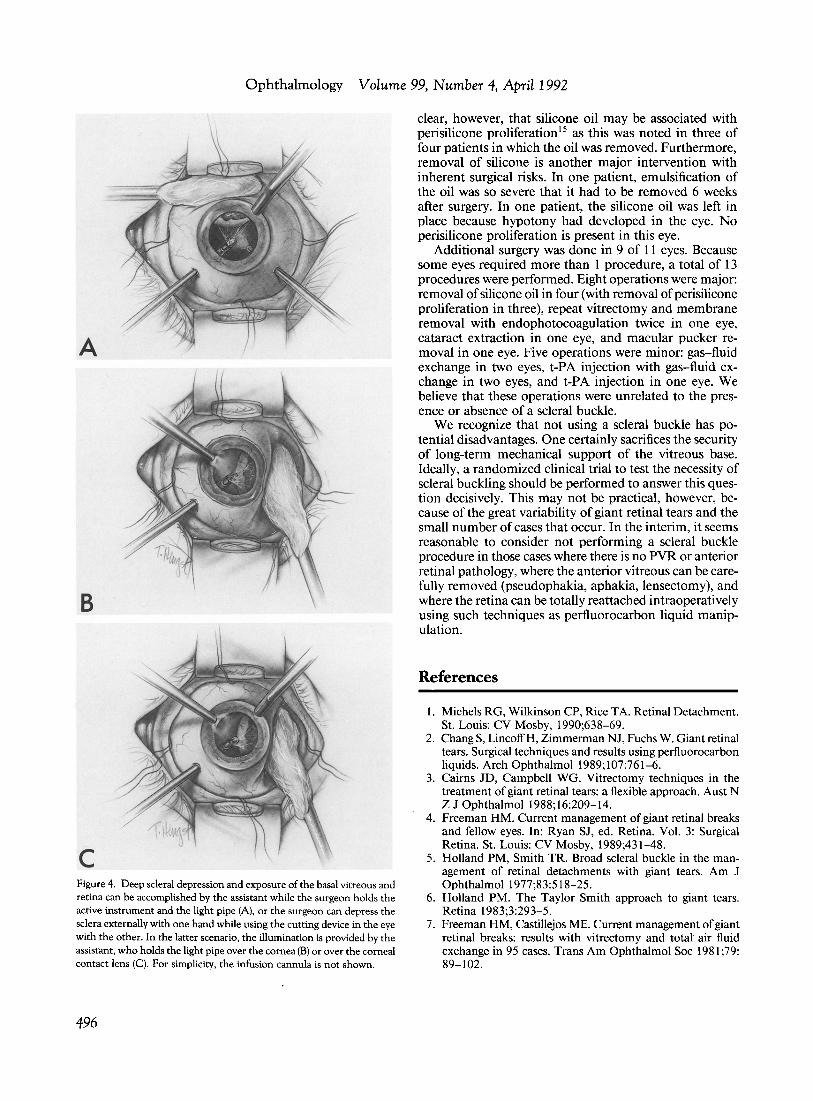
To accomplish maximum removal of the vitreous base, there must be excellent pupillary dilation and good illumination of the surgical field. Exposure of the anterior retina and ciliary body is only possible if deep scleral depression is done. This can be achieved by the assistant while the surgeon holds the active instrument and the light pipe, or the surgeon can depress the sclera externally with one hand while using the cutting device in the eye with the other. In the latter scenario, the illumination is provided by the assistant, who holds the light pipe over the cornea or the corneal contact lens (Fig 4). The infusion cannula may hinder depression with a scleral depressor or cotton applicator, however indentation of the cannula itself by grasping the hub with a forceps may provide good exposure of the meridian where it is located.
Trauma to the lens is very likely when working in the anterior vitreous. To remove basal vitreous gel, a lensectomy must be performed in most phakic eyes and is clearly a disadvantage of this technique. Certainly, preservation of the crystalline lens permits more physiologic postoperative rehabilitation. In this series, five of six phakic eyes required lensectomy to adequately accomplish the surgical goals. In one case, the surgeon judged that the vitreous could be removed adequately without lensectomy. In this patient, a cataract later developed, which was removed. The presence of a pseudophakos makes the anterior dissection more difficult and it is often necessary to widen the posterior capsulotomy in order to see. One patient needed iris sutures to provide sufficient pupillary dilation.
The use of perfluoro-octane was essential to flatten the retina and the giant retinal tear completely intraoperatively.2 Because of the absence of PVR or retinal shortening in these selected cases, the technique eliminated the subretinal fluid, provided excellent reapposition of the tear, and allowed for endophotocoagulation in all eyes. We believe that this intraoperative secure reattachment of the retina and closure of the tear are as important as radical removal of the anterior vitreous in justifying not performing a scleral buckle. Also, the use of perfluorocarbon liquid facilitates retinal reattachment without manipulation of the posterior retinal flap and edge of the giant retinal tear, thus decreasing the risk of iatrogenic retinal breaks, hemorrhage, and retinal trauma, all of which contribute to PVR formation.
It is logical that intraocular tamponade is needed until the chorioretinal adhesions are sufficiently strong. Intraocular perfluoropropane was used in six eyes. Silicone oil was used in five eyes. The justification for its use was the young age and inability to reliably maintain postoperative positioning in three patients, intraoperative retinal slipping in one eye, and patient preference in one eye. Because of the small numbers, it is not warranted to speculate regarding the effectiveness of silicone oil versus gas. It is
495
Ophthalmology Volume 99, Number 4, April 1992
A
B
c Figure 4. Deep scleral depression and exposure of the basal vitreous and retina can be accomplished by the assistant while the surgeon holds the active instrument and the light pipe (A), or the surgeon can depress the sclera externally with one hand while using the cutting device in the eye with the other. In the latter scenario, the illumination is provided by the assistant, who holds the light pipe over the cornea (B) or over the corneal contact lens (C). For simplicity, the infusion cannula is not shown.
496
clear, however, that silicone oil may be associated with perisilicone proliferation 15 as this was noted in three of four patients in which the oil was removed. Furthermore, removal of silicone is another major intervention with inherent surgical risks. In one patient, emulsification of the oil was so severe that it had to be removed 6 weeks after surgery. In one patient, the silicone oil was left in place because hypotony had developed in the eye. No perisilicone proliferation is present in this eye.
Additional surgery was done in 9 of 11 eyes. Because some eyes required more than 1 procedure, a total of 13 procedures were performed. Eight operations were major: removal of silicone oil in four (with removal of perisilicone proliferation in three), repeat vitrectomy and membrane removal with endophotocoagulation twice in one eye, cataract extraction in one eye, and macular pucker removal in one eye. Five operations were minor: gas-fluid exchange in two eyes, t-PA injection with gas-fluid exchange in two eyes, and t-PA injection in one eye. We believe that these operations were unrelated to the presence or absence of a scleral buckle.
We recognize that not using a scleral buckle has potential disadvantages. One certainly sacrifices the security of long-term mechanical support of the vitreous base. Ideally, a randomized clinical trial to test the necessity of scleral buckling should be performed to answer this question decisively. This may not be practical, however, because of the great variability of giant retinal tears and the small number of cases that occur. In the interim, it seems reasonable to consider not performing a scleral buckle procedure in those cases where there is no PVR or anterior retinal pathology, where the anterior vitreous can be carefully removed (pseudophakia, aphakia, lensectomy), and where the retina can be totally reattached intraoperatively using such techniques as perfluorocarbon liquid manipulation.
References
1. Michels RG, Wilkinson CP, Rice TA. Retinal Detachment. St. Louis: CV Mosby, 1990;638-69.
2. Chang S, LincoffH, Zimmerman NJ, Fuchs W. Giant retinal tears. Surgical techniques and results using perfluorocarbon liquids. Arch Ophthalmol 1989; 107:761-6.
3. Cairns JD, Campbell WG. Vitrectomy techniques in the treatment of giant retinal tears: a flexible approach. Aust N Z J Ophthalmol 1988;16:209-14.
4. Freeman HM. Current management of giant retinal breaks and fellow eyes. In: Ryan SJ, ed. Retina. Vol. 3: Surgical Retina. St. Louis: CV Mosby, 1989;431-48.
5. Holland PM, Smith TR. Broad scleral buckle in the management of retinal detachments with giant tears. Am J Ophthalmol 1977;83:518-25.
6. Holland PM. The Taylor Smith approach to giant tears. Retina 1983;3:293-5.
7. Freeman HM, Castillejos ME. Current management of giant retinal breaks: results with vitrectomy and total air fluid exchange in 95 cases. Trans Am Ophthalmol Soc 1981;79: 89-102.

Kreiger and Lewis . Management of Giant Retinal Tears
8. Michels RG, Rice TA, Blankenship G. Surgical techniques for selected giant retinal tears. Retina 1983;3: 139-53.
9. Vidaurri-Leal J, de Bustros S, Michels RG. Surgical treatment of giant retinal tears with inverted posterior retinal flaps. Am J Ophthalmol 1984;98:463-6.
10. Lewis JS, McCuen BW II, Tiedeman JS, Awan KJ. Current views on giant retinal tears. Pak J OphthalmoI1985;1:215-21.
11. Hoffman ME, Sorr EM. Management of giant retinal tears without scleral buckling. Retina 1986;6: 197-204.
12. Leaver PK, Billington BM. Vitrectomy and fluid/siliconeoil exchange for giant retinal tears: 5 years follow-up. Graefes Arch Clin Exp Ophthalmol 1989;227:323-7.
13. Glaser BM. Treatment of giant retinal tears combined with proliferative vitreoretinopathy. Ophthalmology 1986;93: 1193-7.
14. Lewis H, Aaberg TM, Abrams GW, et al. Management of the lens capsule during pars plana lensectomy [letter]. Am J Ophthalmol 1987;103:109-10.
15. Lewis H, Burke JM, Abrams GW, Aaberg TA. Perisilicone proliferation after vitrectomy for proliferative vitreoretinopathy. Ophthalmology 1988;95:583-91.
16. Lewis H, Aaberg TA, Abrams GW. Causes of failure after initial vitreoretinal surgery for severe proliferative vitreoretinopathy. Am J Ophthalmol 1991; III :8-14.
Discussion by
BrooksVV.~cCuenII,~
Drs. Kreiger and Lewis present a series of II patients with uncomplicated giant retinal tears treated by vitrectomy, radical dissection of the vitreous base, fluid-perfluorocarbon liquid exchange, endophotocoagulation, and no scleral buckle. Six eyes received perfluoropropane gas and 5 eyes received silicone oil. They achieved ultimate retinal reattachment with a minimum of7 months follow-up in all II of the operated eyes, with vision improving in 8 eyes.
There have been several previous reports of the treatment of giant retinal tears without scleral buckling, also with good results. In 1986 Hoffman and Sorr1 reported success in 6 of 6 patients using vitrectomy and an expanding gas bubble technique. In 1987, Kreissig and associates2 reported success in 4 of 5 eyes using a modified pneumatic retinopexy technique without either vitrectomy or scleral buckling. In 1989 Chang and associates3
reattached 7 of 7 eyes using vitrectomy and liquid perfluorocarbon exchange without scleral buckling. At this year's Retina Society meeting, Freeman presented his series of20 giant retinal tears that he treated in a manner very similar to Kreiger and Lewis, including vitrectomy, lensectomy, radical dissection of the vitreous base, and liquid perfluorocarbon injection without the use of a scleral buckle (Freeman, unpublished data). Freeman used intraocular gas in all cases and was successful in reattaching 16 (80%) of these eyes.
The results in the series by Kreiger and Lewis are impressive, but as the authors correctly point out, there are some other factors to consider. To adequately dissect the vitreous base, the crystalline lens had to be removed in 5 of the 6 eyes that were phakic preoperatively. Conventional vitreous surgery with the use of a scleral buckle to support the region of the vitreous base, rather than the radical dissection ofthe base advocated by the authors, allows the retention of the crystalline lens in selected cases. Leaving the lens in place at the time of the primary vitrectomy allows for conventional cataract surgery and posterior chamber intraocular lens implantation, should later cataract develop.
While the anatomic retinal reattachment rate is excellent in this series, more than a single operative procedure was required
From the Duke University Eye Center, Durham.
in 9 of the II eyes (82%). Excluding postoperative fluid-gas exchange and tissue plasminogen activator injection, both of which the authors considered minor, 8 ofthe 13 total secondary procedures performed were considered major. As found in this series, other reports of giant retinal tear surgery without scleral buckling document a frequent necessity for reoperation. 1
-3 But
would the addition of a scleral buckle reduce the need for reoperations in eyes with giant retinal tears? The difficulty in answering this question stems from a lack of adequate controls, thus making a critical interpretation of the authors' findings impossible. For this reason, I would suggest caution in concluding that scleral buckles are not indicated in uncomplicated giant retinal tear surgery.
In summary, Drs. Kreiger and Lewis have presented an increasingly popular technique for the management of selected giant retinal tears in which vitrectomy is combined with the use of perfluorocarbon liquids, vitreous base surgery, extended intraocular tamponade, and omission of a scleral buckle. Their ultimate anatomic and visual results are excellent, but intraoperative lensectomy in phakic eyes is usually required, and multiple operative procedures are frequently necessary to achieve these results. As they correctly point out, this series is small, uncontrolled, and has limited long-term follow-up. Whether the addition of an intraoperative scleral buckle would reduce the necessity for lensectomy or the need for additional surgical procedures is not possible to determine in the absence of an adequate control group.
References
1. Hoffman ME, Sorr EM. Manageplent of giant retinal tears without scleral buckling. Retina 1986;6: 197 -204.
2. Kreissig I, Lincoff H, Stanowsky A. The treatment of giant tear detachments using retrohyaloidal perfluorocarbon gases without drainage or vitrectomy. Graefes Arch Clin Exp Ophthalmol 1987;225:94-8.
3. Chang S, LincoffH, Zimmerman NJ, Fuchs W. Giant retinal tears: surgical techniques and results using perfluorocarbon liquids. Arch Ophthalmol 1989; 1 07:761-6.
497