Embed Size (px)
Citation preview

Managing Shoulder Pain
Jesse Affonso, MD
©2011 Cape Cod Healthcare Inc.

Objectives
• Review relevant anatomy
• Discuss common causes of pain
• Treatment
©2011 Cape Cod Healthcare Inc.
2

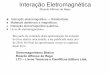
Anatomy – Bony Architecture
©2011 Cape Cod Healthcare Inc.
3

Anatomy – Soft Tissues – Rotator Cuff
©2011 Cape Cod Healthcare Inc.
4

Introduction
©2011 Cape Cod Healthcare Inc.
5
• Shoulder pain is an extremely common complaint (2nd most)
• Difficult joint to examine
• Multidirectional range of motion
• It is important to make an accurate diagnosis of the cause of your symptoms so that appropriate treatment can be directed at the cause

Where is the pain coming from?
• Pain arising from the shoulder • Rotator cuff disorders: rotator
cuff tendinopathy, impingement, subacromial bursitis, rotator cuff tears
• Glenohumeral disorders: capsulitis ("frozen shoulder"), arthritis, infection (rare)
• Acromioclavicular disease
• Traumatic dislocation©2011 Cape Cod Healthcare Inc.
6

Where is the pain coming from?
©2011 Cape Cod Healthcare Inc.
7
• Pain arising from elsewhere • Referred pain: neck pain,
myocardial ischemia, referred diaphragmatic pain
• Polymyalgia rheumatica / fibromyalgia
• Malignancy: apical lung cancers, metastases

Shoulder Examination
• Look
• Feel
• Move• Active + Passive• Resisted
• Special Tests
©2011 Cape Cod Healthcare Inc.
8
Symptoms:Pain overheadPain and weaknessPain with anything
Duration of symptoms

Shoulder Pain - Diagnoses
• Impingement / Bursitis• Rotator Cuff Tendinitis / Tendinopathy • Rotator Cuff Tear – Partial vs. Full
thickness
• Adhesive Capsulitis• Arthritis
©2011 Cape Cod Healthcare Inc.
9

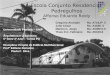
Impingement / Bursitis
©2011 Cape Cod Healthcare Inc.
10
Repetitive overhead activities
Subacromial bursa and/or rotator cuff impinged between acromion & humerus

Impingement

Impingement
©2011 Cape Cod Healthcare Inc.
12

Impingement - Treatment
• Activity modification: no activity with elbow away from side, in the gym, or at the computer.
• Once a day stretch fully overhead.• NSAID and Ice• Injection in 3-6 weeks• Physical Therapy: After pain
subsides:• Regain ROM / Strengthen
• Surgery
©2011 Cape Cod Healthcare Inc.
13

Rotator Cuff Disease
• Rotator cuff disease is a large spectrum from tendinitis to full thickness tears
©2011 Cape Cod Healthcare Inc.
14

Rotator Cuff Tears – How to tell?
• Pain and Weakness
• Does this mean a Rotator Cuff Tear?
• Cannot assess rotator cuff when there is pain
• Treat pain first: NSAID, PT, ice, rest-4 weeks
• Cortisone shot (once) if above doesn’t work
• Test cuff when pain subsides.
©2011 Cape Cod Healthcare Inc.
15

Rotator Cuff Tendinitis - Treatment
• Physical Therapy / Activity Modification
• Anti-inflammatories• Ice / Heat• Tylenol• Steroid Injections• Repeat
• Surgery
©2011 Cape Cod Healthcare Inc.
16

Rotator Cuff Tear
©2011 Cape Cod Healthcare Inc.
17
Acute vs. Gradual
Repetitive overhead activity or by wear and degeneration of the tendon.
Over time the pain may become noticeable at rest or with no activity at all
There may be pain when you lie on the affected side and at night

18
Rotator Cuff Tear
• Atrophy or thinning of the muscles about the shoulder
• Pain when someone lift the arm • Pain when someone lower the arm from a fully
raised position • Weakness when someone lift or rotate the arm • Crackling sensation when someone move his
shoulder in certain positions

Rotator Cuff Tear
MRI?
Based on:
duration of symptoms
location
patient age
severity
physical exam
©2011 Cape Cod Healthcare Inc.
19

20
Rotator Cuff Tear
• Pain relief• Improve the function of shoulder. • It may take several weeks or months to restore the strength and
mobility to ones shoulder.
• Rest and limited overhead activity • Anti-inflammatory medication • Steroid injection • Strengthening exercise and physical therapy

Adhesive Capsulitis
©2011 Cape Cod Healthcare Inc.
21
Frozen shoulder (adhesive capsulitis) is a disorder characterized by pain and loss of motion or stiffness in the shoulder.
It affects about two percent of the general population.
It is more common in women between the ages of 40 years to 70 years old.
• The causes of frozen shoulder are not fully understood.
• The process involves thickening and contracture of the capsule surrounding the shoulder joint.

Adhesive Capsulitis
• Frozen shoulder occurs much more commonly in individuals with diabetes, affecting 10 percent to 20 percent of these individuals.
• Other medical problems associated with increased risk of frozen shoulder include: hypothyroidism, hyperthyroidism, Parkinson's disease, and cardiac disease or surgery.
• Frozen shoulder can develop after a shoulder is injured or immobilized for a period of time.
©2011 Cape Cod Healthcare Inc.
22

Adhesive Capsulitis
• Pain due to frozen shoulder is usually dull or aching.
• It can be worsened with attempted motion.
• The pain is usually located over the outer shoulder area and sometimes the upper arm.
• The hallmark of the disorder is restricted motion or stiffness in the shoulder.
©2011 Cape Cod Healthcare Inc.
23

Adhesive Capsulitis
• The first goal is pain control.
• To restore motion, physical therapy is usually started. This may be under the direct supervision of a therapist or via a home program.
• Therapy includes stretching or range-of-motion exercises for the shoulder. Sometimes heat is used to help decrease pain. ©2011 Cape Cod Healthcare Inc.
24

Adhesive Capsulitis
• Nerve blocks: Suprascapular nerve block
• Surgical: manipulation under anesthesia and shoulder arthroscopy
• Often, manipulation and arthroscopy are used together in combination to obtain maximum results
• After surgery, physical therapy is important to maintain the motion that was achieved with surgery
©2011 Cape Cod Healthcare Inc.
25

Shoulder Arthritis
©2011 Cape Cod Healthcare Inc.
26
• Age: > 65
• Male > Female
• Monoarticular
• Account for 60% of Total Shoulder Replacements
• 5% with Rotator Cuff tears

Shoulder Arthritis
• Patient Age• Severity of Symptoms• Radiographs• Medical Co morbidities• Patient Characteristics

Viscosupplementation (HA)
• Hyaluronic Acid• Variable injection schedule• Theoretical benefit is to improve lubrication in the joint• FDA approved for the knee, and has some scientific
support Wang et al: JBJS 2004 Metaanalysis, confirmed efficacy and safety of treatment
• Minimal literature on usage in the shoulder Shibata et al (JSES 2001) found it to be equal to corticosteroids
in those with rotator cuff tears Silverstein et al AJSM 2007

• 30 patients w/ idiopathic glenohumeral OA• Statistically significant improvements in VAS, UCLA
score, and Simple Shoulder Test Score at 6 months• ~50% had less than 2 point improvement in VAS• No complications• Conclusion: HA may have a beneficial effect on some
patients with glenohumeral OA• Reasonable option in patients that are not surgical
candidates

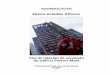
Hemiarthroplasty
Total Shoulder
Reverse Total Shoulder
Arthroplasty Options

Summary
• Shoulder pain is a common complaint and can be multifactorial
• Proper diagnosis is key to treatment
• Nonsurgical treatment is the first line
• Surgery only after nonsurgical treatments fail
©2011 Cape Cod Healthcare Inc.
31

Contact Information
• Jesse Affonso• [email protected]
• Cape Cod Orthopaedics & Sports Medicine
• 130 North Street• Hyannis, MA 02601
• 508-775-8282
©2011 Cape Cod Healthcare Inc.
32