Embed Size (px)
Citation preview
Maternal serum 25-hydroxyvitamin D levels at11+0–13+6 weeks in pregnant women withdiabetes mellitus and in those with macrosomicneonatesMD Savvidou,a,b R Akolekar,b RBB Samaha,b AP Masconi,b,c KH Nicolaides,b,c
a Department of Maternal Fetal Medicine, Imperial College School of Medicine, Chelsea and Westminster Hospital, London UK b Harris
Birthright Research Centre for Fetal Medicine, King’s College Hospital, London, UK c Department of Fetal Medicine, University College
Hospital, London, UK
Correspondence: Dr MD Savvidou, Department of Maternal Fetal Medicine, Imperial College School of Medicine, Chelsea and Westminster
Hospital, 369 Fulham Road, London SW10 9NH, UK. Email [email protected]
Accepted 8 March 2011.
Objective To investigate whether maternal serum levels of
25-hydroxyvitamin D [25(OH)D] in the first trimester are altered
in pregnant women with pre-existing type 2 diabetes, women who
subsequently develop gestational diabetes mellitus (GDM) and
women who deliver large for gestational age (LGA) neonates
compared with normoglycaemic pregnant women who deliver an
appropriate for gestational age (AGA) neonate.
Design Case–control study.
Setting Antenatal clinic.
Population Singleton pregnancies at 11+0–13+6 weeks, including
50 women with type 2 diabetes, 100 women who subsequently
developed GDM, 50 nondiabetic women who subsequently
delivered LGA neonates and 1000 nondiabetic controls who
delivered AGA neonates.
Methods Maternal serum total 25(OH)D levels were measured in
the four groups of pregnancies. Multiple regression analysis in the
controls was used to identify factors among maternal
characteristics with a significant contribution to the levels of
serum 25(OH)D, so that the values in all cases were expressed as
a multiple of the median (MoM) in the controls.
Main outcome measures Comparison of MoM 25(OH)D in the
four groups.
Results In controls, significant independent contributions to the
serum level of 25(OH)D were provided by maternal age, body
mass index, smoking status, racial origin and season of
sampling. The median and interquartile range (IQR) of serum
25(OH)D in the type 2 diabetes group (1.01; IQR, 0.68–1.47
MoM), GDM group (0.93; IQR, 0.67–1.23 MoM) and LGA
group (0.97; IQR, 0.67–1.25 MoM) were not significantly
different from those in the controls (0.99; IQR, 0.71–1.33 MoM)
(overall P = 0.643).
Conclusions The first-trimester maternal serum level of 25(OH)D
is not altered in women with type 2 diabetes, those who develop
GDM or those who deliver LGA neonates.
Keywords Gestational diabetes mellitus, large for gestational age
neonates, pregnancy, type 2 diabetes, vitamin D.
Please cite this paper as: Savvidou M, Akolekar R, Samaha R, Masconi A, Nicolaides K. Maternal serum 25-hydroxyvitamin D levels at 11+0–13+6 weeks in
pregnant women with diabetes mellitus and in those with macrosomic neonates. BJOG 2011;118:951–955.
Introduction
Vitamin D, which plays a central role in calcium homeosta-
sis, is implicated in the pathogenesis of cardiovascular
disease, cancer and diabetes mellitus.1–6 Deficiency in
25-hydroxyvitamin D [25(OH)D] predisposes to the devel-
opment of both type 1 and 2 diabetes.4,5,7 Pancreatic b-cells
express the vitamin D receptor, and allelic variations in the
genes involved in vitamin D metabolism and its receptor
are associated with glucose (in)tolerance.8 There is contra-
dictory evidence on the association of vitamin D deficiency
with gestational diabetes mellitus (GDM), with some stud-
ies reporting that, in affected pregnancies, maternal serum
or plasma levels of 25(OH)D are decreased,9,10 and others
reporting that there is no significant difference from
normoglycaemic controls.11,12 A case–control study reported
that the median maternal plasma 25(OH)D concentration
at an average of 16 weeks of gestation was significantly
ª 2011 The Authors BJOG An International Journal of Obstetrics and Gynaecology ª 2011 RCOG 951
DOI: 10.1111/j.1471-0528.2011.02982.x
www.bjog.orgMaternal medicine

lower in 57 pregnant women who subsequently developed
GDM compared with 114 who did not develop GDM.13
In a study of 90 pregnant women who developed GDM,
maternal serum 25(OH)D concentration at 11–13 weeks of
gestation was not significantly different from that of con-
trols.14 No studies have assessed the maternal 25(OH)D
levels in women who deliver large for gestational age
(LGA) neonates. There are several techniques for the quan-
tification of 25(OH)D, including radioimmunoassay,
chemiluminescent assays, high-performance liquid chroma-
tography and, more recently, liquid chromatography-mass
spectrometry/mass spectrometry, which is thought to pro-
vide the most accurate results, but is expensive to per-
form.15
The aim of this study was to investigate further possible dif-
ferences in maternal serum levels of 25(OH)D at 11+0–13+6
weeks of gestation in pregnant women with pre-existing
type 2 diabetes mellitus, those who subsequently develop
GDM and those who deliver a LGA neonate compared
with nondiabetic pregnant women who deliver an appro-
priate for gestational age (AGA) neonate.
Methods
Study populationThis was a case–control study drawn from a large prospec-
tive observational investigation of the early prediction of
pregnancy complications in women attending for their rou-
tine first hospital visit in pregnancy at King’s College Hos-
pital, London, UK, from March 2006 to June 2009. In this
visit, which is held at 11+0–13+6 weeks of gestation, we
record maternal characteristics and medical history and
perform combined screening for aneuploidies by measure-
ment of the fetal crown–rump length, nuchal translucency
thickness and maternal serum pregnancy-associated plasma
protein A and free b-human chorionic gonadotrophin.16,17
We stored serum and plasma at )80�C for subsequent bio-
chemical analysis from women who provided written
informed consent for participation in the study, which was
approved by King’s College Hospital ethics committee.
In this study, we measured maternal serum concentra-
tion of 25(OH)D2 and 25(OH)D3 in 1200 singleton preg-
nancies, including 50 with type 2 diabetes, 100 women who
subsequently developed GDM, 50 nondiabetic women who
subsequently delivered LGA neonates and 1000 nondiabetic
controls who delivered a phenotypically normal AGA neo-
nate at term. Cases were selected at random from our data-
base of stored samples. We then matched each case with
five controls who were examined on the same day.
Outcome measuresScreening for GDM in our hospital is based on a two-step
approach. In all women, random plasma glucose is mea-
sured at 24–28 weeks of gestation and, if the concentration
is more than 6.7 mmol/l, an oral glucose tolerance test
(OGTT) is carried out within the subsequent 2 weeks. The
diagnosis of GDM is made if the fasting plasma glucose
level is at least 6.1 mmol/l or the plasma glucose level
2 hours after the oral administration of 75 g glucose is
7.8 mmol/l or more.18 In women with normal random
blood sugar, an OGTT is performed if they have persistent
glucosuria, develop polyhydramnios or if the fetus becomes
macrosomic. Women with a diagnosis of GDM are given
dietary and exercise advise, and are encouraged to test cap-
illary blood glucose before and 1 hour after each meal.
If, during a period of 1–2 weeks, the pre-meal or 1-hour
post-meal blood glucose level is higher than 5.5 or
7 mmol/l, respectively, the women are treated with insulin.
The neonate was considered to be LGA if the birthweight
was above the 95th percentile for gestation at delivery,
using a reference range derived from our population.19
Neonates between the 5th and 95th percentiles were con-
sidered to be AGA.
Details of the maternal characteristics and the findings of
the 11+0–13+6-week assessment were recorded in our data-
base. Data on pregnancy outcome were obtained from the
maternity computerised records or the general medical
practitioners of the women, and were also recorded in our
database.
Sample analysisNone of the samples had been thawed and refrozen previ-
ously. Duplicate samples of 100 ll were used to analyse
25(OH)D2 and 25(OH)D3 by liquid chromatography-mass
spectrometry/mass spectrometry (Prominence HPLC sys-
tem, equipped with a Phenomenex Luna C8 3 · 50 mm
column and AB Sciex API-5000 ESI triple quadrupole;
Shimadzu Scientific Instruments, Columbia, OH, USA).
The analysis was performed using the MSMS Vitamin D
kit 3075-0010 (PerkinElmer, Inc., Turku, Finland). Individ-
ual runs were calibrated using National Institute of Stan-
dards and Technology (NIST) Standard Reference Material
(SRM) 2972. The average inter-assay coefficients of varia-
tion (CV) for 25(OH)D2 and 25(OH)D3 were 6.6% and
7.3%, respectively, and the intra-assay CVs were 6.3% and
6.5%, respectively. The total serum 25(OH)D concentration
was calculated by adding together the measured 25(OH)D2
and 25(OH)D3 concentrations.
Statistical analysisComparison between outcome groups was performed by
Mann–Whitney U-test with post hoc Bonferroni correction
for continuous variables, and v2 test or Fisher’s exact test
for categorical variables.
The distribution of 25(OH)D was made Gaussian by
square root transformation and the normality of distribution
Savvidou et al.
952 ª 2011 The Authors BJOG An International Journal of Obstetrics and Gynaecology ª 2011 RCOG
was assessed using histograms and probability plots.
In each case and control, the measured concentration of
total vitamin D was converted into a multiple of the med-
ian (MoM) in controls after adjusting for maternal age,
body mass index (BMI), smoking status, method of con-
ception, season of sampling and racial origin, as described
previously.20 Mann–Whitney U-test with post hoc Bonfer-
roni correction was used to compare median MoM values
of total 25(OH)D between the outcome groups. Nonpara-
metric correlation analysis was used to determine the sig-
nificance of association between total 25(OH)D and
birthweight percentile in the outcome groups.
The statistical software package spss 16.0 (SPSS Inc.,
Chicago, IL, USA) was used for data analyses.
Results
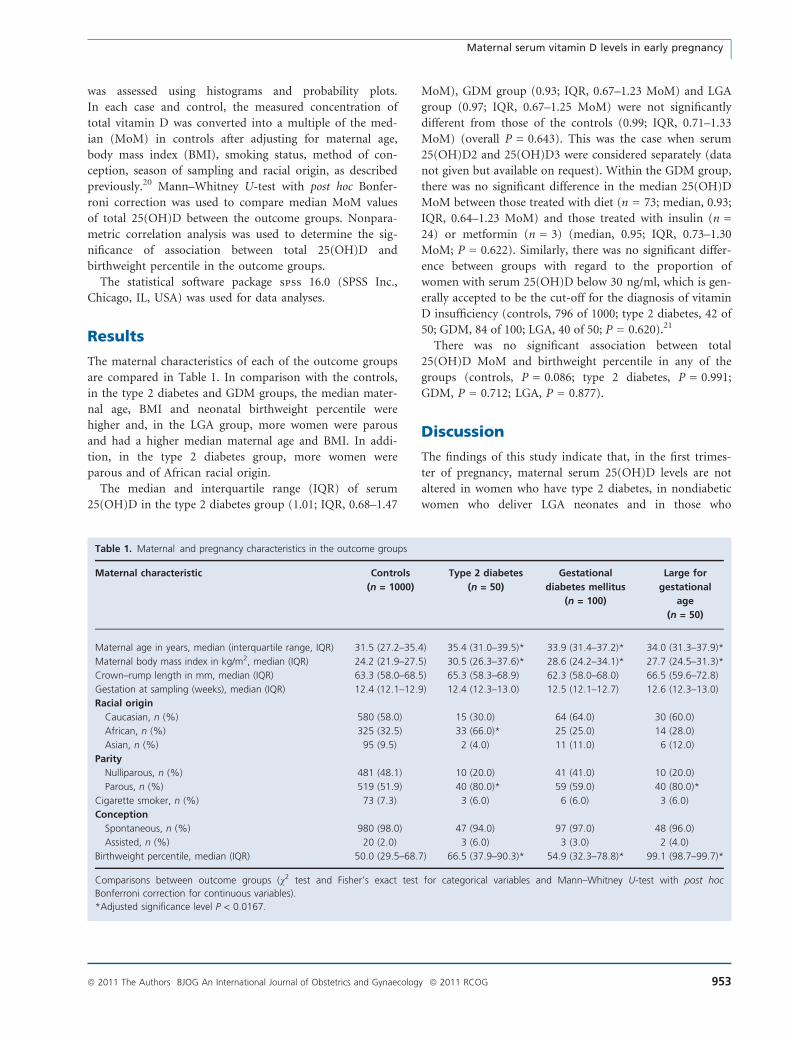
The maternal characteristics of each of the outcome groups
are compared in Table 1. In comparison with the controls,
in the type 2 diabetes and GDM groups, the median mater-
nal age, BMI and neonatal birthweight percentile were
higher and, in the LGA group, more women were parous
and had a higher median maternal age and BMI. In addi-
tion, in the type 2 diabetes group, more women were
parous and of African racial origin.
The median and interquartile range (IQR) of serum
25(OH)D in the type 2 diabetes group (1.01; IQR, 0.68–1.47
MoM), GDM group (0.93; IQR, 0.67–1.23 MoM) and LGA
group (0.97; IQR, 0.67–1.25 MoM) were not significantly
different from those of the controls (0.99; IQR, 0.71–1.33
MoM) (overall P = 0.643). This was the case when serum
25(OH)D2 and 25(OH)D3 were considered separately (data
not given but available on request). Within the GDM group,
there was no significant difference in the median 25(OH)D
MoM between those treated with diet (n = 73; median, 0.93;
IQR, 0.64–1.23 MoM) and those treated with insulin (n =
24) or metformin (n = 3) (median, 0.95; IQR, 0.73–1.30
MoM; P = 0.622). Similarly, there was no significant differ-
ence between groups with regard to the proportion of
women with serum 25(OH)D below 30 ng/ml, which is gen-
erally accepted to be the cut-off for the diagnosis of vitamin
D insufficiency (controls, 796 of 1000; type 2 diabetes, 42 of
50; GDM, 84 of 100; LGA, 40 of 50; P = 0.620).21
There was no significant association between total
25(OH)D MoM and birthweight percentile in any of the
groups (controls, P = 0.086; type 2 diabetes, P = 0.991;
GDM, P = 0.712; LGA, P = 0.877).
Discussion
The findings of this study indicate that, in the first trimes-
ter of pregnancy, maternal serum 25(OH)D levels are not
altered in women who have type 2 diabetes, in nondiabetic
women who deliver LGA neonates and in those who
Table 1. Maternal and pregnancy characteristics in the outcome groups
Maternal characteristic Controls
(n = 1000)
Type 2 diabetes
(n = 50)
Gestational
diabetes mellitus
(n = 100)
Large for
gestational
age
(n = 50)
Maternal age in years, median (interquartile range, IQR) 31.5 (27.2–35.4) 35.4 (31.0–39.5)* 33.9 (31.4–37.2)* 34.0 (31.3–37.9)*
Maternal body mass index in kg/m2, median (IQR) 24.2 (21.9–27.5) 30.5 (26.3–37.6)* 28.6 (24.2–34.1)* 27.7 (24.5–31.3)*
Crown–rump length in mm, median (IQR) 63.3 (58.0–68.5) 65.3 (58.3–68.9) 62.3 (58.0–68.0) 66.5 (59.6–72.8)
Gestation at sampling (weeks), median (IQR) 12.4 (12.1–12.9) 12.4 (12.3–13.0) 12.5 (12.1–12.7) 12.6 (12.3–13.0)
Racial origin
Caucasian, n (%) 580 (58.0) 15 (30.0) 64 (64.0) 30 (60.0)
African, n (%) 325 (32.5) 33 (66.0)* 25 (25.0) 14 (28.0)
Asian, n (%) 95 (9.5) 2 (4.0) 11 (11.0) 6 (12.0)
Parity
Nulliparous, n (%) 481 (48.1) 10 (20.0) 41 (41.0) 10 (20.0)
Parous, n (%) 519 (51.9) 40 (80.0)* 59 (59.0) 40 (80.0)*
Cigarette smoker, n (%) 73 (7.3) 3 (6.0) 6 (6.0) 3 (6.0)
Conception
Spontaneous, n (%) 980 (98.0) 47 (94.0) 97 (97.0) 48 (96.0)
Assisted, n (%) 20 (2.0) 3 (6.0) 3 (3.0) 2 (4.0)
Birthweight percentile, median (IQR) 50.0 (29.5–68.7) 66.5 (37.9–90.3)* 54.9 (32.3–78.8)* 99.1 (98.7–99.7)*
Comparisons between outcome groups (v2 test and Fisher’s exact test for categorical variables and Mann–Whitney U-test with post hoc
Bonferroni correction for continuous variables).
*Adjusted significance level P < 0.0167.
Maternal serum vitamin D levels in early pregnancy
ª 2011 The Authors BJOG An International Journal of Obstetrics and Gynaecology ª 2011 RCOG 953

subsequently develop GDM, irrespective of whether their
diabetes is controlled by diet alone or in combination with
pharmacological intervention.
Our findings of a lack of significant difference in mater-
nal vitamin D between pregnant women who develop
GDM and normoglycaemic controls are compatible with
those of two previous studies.11,12 Three other studies
reported an association between GDM and vitamin D defi-
ciency, but this apparent contradiction may be the conse-
quence of the small number of cases examined, the
gestational age at sampling (second or third trimester) and
the method used to measure vitamin D [(radio)immunoas-
say and enzyme-linked immunosorbent assay].9,10,13
The rationale for our study was based on the following:
first, evidence from investigations in nonpregnant women
which showed that serum 25(OH)D is decreased in type 2
diabetes mellitus and is inversely associated with plasma
glucose levels and abdominal obesity in those without dia-
betes;5,21–23 and, second, studies reporting decreased serum
25(OH)D in women with established GDM.9,10,13 In a pre-
vious study of pregnant women who developed GDM, we
reported that the maternal serum concentration of
25(OH)D at 11–13 weeks was not significantly different
from that in normal pregnancies.14 We wanted to investi-
gate this finding further by including women with pre-
existing diabetes and those with LGA neonates because, in
all three conditions, there may be a common pathophysio-
logical mechanism involving varying degrees of glucose
intolerance. About 20% of women with GDM develop type
2 diabetes within 10 years of the index pregnancy, com-
pared with 2% in those without GDM.25,26 Macrosomic
neonates of nondiabetic mothers have a similar metabolic
profile to the neonates of pregnant women affected by
GDM.27–29 In addition, in women with GDM, there is a
significant positive correlation between maternal glucose
levels and the incidence of macrosomia.30 Consequently, in
women with glucose challenge test results that do not fulfil
the current criteria for GDM, it is likely that there is an
association between neonatal macrosomia and a degree of
impaired maternal glucose tolerance.
The finding of our study that, in all three groups of
complicated pregnancies, the maternal serum level of
25(OH)D was not significantly different from controls sug-
gests that, in these conditions, at least at 11+0–13+6 weeks
of gestation, there is no evidence of an increased prevalence
of vitamin D insufficiency or deficiency. An alternative
explanation is that all three conditions are associated with
vitamin D insufficiency. We have certainly found that, in a
very high proportion of women with type 2 diabetes, GDM
and those delivering LGA neonates (84%, 84% and 80%,
respectively), the serum level of 25(OH)D is in the range
that, in nonpregnant women, is thought to be indicative of
vitamin D insufficiency or deficiency.21 Failure to demon-
strate such an insufficiency by comparison with controls
may be a mere consequence of the finding that a high pro-
portion of patients in the latter group were also insufficient
in vitamin D. Our findings are more applicable to Cauca-
sian or African women, and not to Asians, who represent
the minority of our population and are known to have a
higher incidence of glucose intolerance and vitamin D defi-
ciency.30,31 There are several reports suggesting that there
may be an epidemic of vitamin D deficiency in pregnancy,
and advocating the need for pharmacological intervention,
because this condition is thought to be associated with a
wide range of adverse pregnancy outcomes.33–35
In a previous study, we used the pragmatic approach of
examining the distribution of serum 25(OH)D values in a
diverse inner city population of singleton pregnancies with
normal outcome, and suggested that the cut-off for the
diagnosis of low levels should be about 10 ng/ml, which
corresponds to the 5th percentile.20 We suggested that, in
the absence of conclusive evidence that in pregnancies with
serum 25(OH)D below 30 ng/ml there is an increased risk
for specific pregnancy complications and adverse postnatal
outcome, it may be inappropriate to classify about 80% of
pregnancies with normal outcome as suffering from vita-
min D insufficiency in need of treatment with vitamin D
supplements.
Conclusion
In summary, we found that, at 11–13 weeks of gestation,
maternal serum levels of 25(OH)D in women with type 2
diabetes, in those who develop GDM and in nondiabetic
women who deliver LGA neonates are not significantly dif-
ferent from those in normal pregnancies delivering AGA
neonates at term.
Disclosure of interestNone.
Contribution to authorshipMDS is the main corresponding author, and she conceived
and designed the study. RA, RBBS and APM contributed
to the design and conduct of the study and the interpreta-
tion of the results. KHN is the main supervisor. All the
authors participated and contributed to the writing of the
manuscript.
Details of ethics approvalEthical approval was granted by the King’s College Hospital
Ethics Committee (02-03-033).
FundingThis study was supported by a grant from the Fetal Medi-
cine Foundation (United Kingdom Charity No. 1037116).
Savvidou et al.
954 ª 2011 The Authors BJOG An International Journal of Obstetrics and Gynaecology ª 2011 RCOG

The assays were performed by Dr Blas Cerda at Perkin-
Elmer Life & Analytical Sciences, Waltham, MA, USA.
AcknowledgementsThe assays were performed by Dr Blas Cerda at Perkin-
Elmer Life & Analytical Sciences, Waltham, MA, USA. j
References
1 Lind L, Hanni A, Lithell H, Hvarfner A, Sorensen OH, Ljunghall S.
Vitamin D is related to blood pressure and other cardiovascular risk
factors in middle-aged men. Am J Hypertens 1995;8:894–901.
2 Poole KE, Loveridge N, Barker PJ, Halsall DJ, Rose C, Reeve J, et al.
Reduced vitamin D in acute stroke. Stroke 2006;37:243–5.
3 Wang TJ, Pencina MJ, Booth SL, Jacques PF, Ingelsson E, Lanier K,
et al. Vitamin D deficiency and risk of cardiovascular disease. Circu-
lation 2008;117:503–11.
4 Mathieu C, Badenhoop K. Vitamin D and type 1 diabetes mellitus:
state of the art. Trends Endocrinol Metab 2005;16:261–6.
5 Pittas AG, Lau J, Hu FB, Dawson-Hughes B. The role of vitamin D
and calcium in type 2 diabetes. A systematic review and meta-analy-
sis. J Clin Endocrinol Metab 2007;92:2017–29.
6 Holick MF. Vitamin D deficiency. N Engl J Med 2007;357:266–81.
7 Mathieu C, Gysemans C, Giulietti A, Bouillon R. Vitamin D and dia-
betes. Diabetologia 2005;48:1247–57.
8 Takiishi T, Gysemans C, Bouillon R, Mathieu C. Vitamin D and diabe-
tes. Endocrinol Metab Clin North Am 2010;39:419–46.
9 Soheilykhah S, Mojibian M, Rashidi M, Rahimi-Saghand S, Jafari F.
Maternal vitamin D status in gestational diabetes mellitus. Nutr Clin
Pract 2010;25:524–7.
10 Maghbooli Z, Hossein-Nezhad A, Karimi F, Shafaei AR, Larijani B.
Correlation between vitamin D3 deficiency and insulin resistance in
pregnancy. Diabetes Metab Res Rev 2008;24:27–32.
11 Clifton-Bligh RJ, McElduff P, McElduff A. Maternal vitamin D defi-
ciency, ethnicity and gestational diabetes. Diabet Med 2008;25:678–
84.
12 Farrant HJ, Krishnaveni GV, Hill JC, Boucher BJ, Fisher DJ, Noonan
K, et al. Vitamin D insufficiency is common in Indian mothers but is
not associated with gestational diabetes or variation in newborn
size. Eur J Clin Nutr 2009;63:646–52.
13 Zhang C, Qiu C, Hu FB, David RM, van Dam RM, Bralley A, et al.
Maternal plasma 25-hydroxyvitamin D concentrations and the risk
for gestational diabetes mellitus. PLoS ONE 2008;3:e3753.
14 Makgoba M, Nelson SM, Savvidou M, Messow CM, Nicolaides K,
Sattar N. First-trimester circulating 25 Hydroxy vitamin D levels and
development of gestational diabetes. Diabetes Care 2011;34:1091–3
15 Hollis BW. Measuring 25-hydroxyvitamin D in a clinical environment:
challenges and needs. Am J Clin Nutr 2008;88:507S–10S.
16 Snijders RJ, Noble P, Sebire N, Souka A, Nicolaides KH. UK multicentre
project on assessment of risk of trisomy 21 by maternal age and fetal
nuchal-translucency thickness at 10–14 weeks of gestation. Fetal
medicine foundation first trimester screening group. Lancet 1998;
352:343–6.
17 Kagan KO, Wright D, Valencia C, Maiz N, Nicolaides KH. Screening
for trisomies 21, 18 and 13 by maternal age, fetal nuchal translu-
cency, fetal heart rate, free b-hCG and pregnancy-associated plasma
protein-A. Hum Reprod 2008;23:1968–75.
18 World Health Organization. Definition and Diagnosis of Diabetes
Mellitus and Intermediate Hyperglycaemia; Report of a WHO/IDF
Consultation. Geneva, Switzerland: World Health Organization, 2006.
pp. 1–46. [www.who.int/diabetes/publications/en/]. Last accessed 14
December 2010.
19 Poon LC, Karagiannis G, Staboulidou I, Shafiei A, Nicolaides KH.
Reference range of birth weight with gestation and first-trimester
prediction of small-for-gestation neonates. Prenat Diagn 2011;31:
58–65.
20 Yu CKH, Ertl R, Samaha R, Akolekar R, Nicolaides KH. Normal range
of vitamin D in maternal serum at 11–13 weeks’ gestation. Fetal
Diagn Ther 2011; Feb 24 [Epub ahead of print].
21 Holick MF. Vitamin D status: measurement, interpretation, and clini-
cal application. Ann Epidemiol 2009;19:73–8.
22 Pittas AG, Dawson-Hughes B, Li T, Van Dam RM, Willett WC, Man-
son JE, et al. Vitamin D and calcium intake in relation to type 2 dia-
betes in women. Diabetes Care 2006;29:650–6.
23 Chiu KC, Chu A, Go VL, Saad MF. Hypovitaminosis D is associated
with insulin resistance and beta cell dysfunction. Am J Clin Nutr
2004;79:820–5.
24 Ford ES, Ajani UA, McGuire LC, Liu S. Concentrations of serum vita-
min D and the metabolic syndrome among U.S. adults. Diabetes
Care 2005;28:1228–30.
25 Feig D, Zinman B, Wang X, Hux J. Risk of development of diabetes mell-
itus after a diagnosis of gestational diabetes. CMAJ 2008;179:229–34.
26 Bellamy L, Casas JP, Hingorani AD, Williams D. Type 2 diabetes
mellitus after gestational diabetes: a systematic review and meta-
analysis. Lancet 2009;373:1773–9.
27 Plagemann A, Hander T, Kohlhoff R, Rohde W, Dorner G. Glucose
tolerance and insulin secretion in children of mothers with pregesta-
tional IDDM or gestational diabetes. Diabetologia 1997;40:1094–100.
28 Dyer JS, Rosenfeld CR, Rice J, Rice M, Hardin DS. Insulin resistance
in Hispanic large-for-gestational-age neonates at birth. J Clin Endo-
crinol Metab 2007;92:3836–43.
29 Evagelidou EN, Kiortsis DN, Bairaktari ET, Giapros VI, Cholevas VK,
Tzallas CS, et al. Lipid profile, glucose homeostasis, blood pressure,
and obesity-anthropometric markers in macrosomic offspring of
nondiabetic mothers. Diabetes Care 2006;29:1197–201.
30 Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, Coustan
DR, et al. Hyperglycemia and adverse pregnancy outcomes. N Engl J
Med 2008;358:1991–2002.
31 Chu SY, Abe K, Hall LR, Kim SY, Njoroge T, Qin C. Gestational
diabetes mellitus: all Asians are not alike. Prev Med 2009;49:265–8.
32 Awumey EM, Mitra DA, Hollis BW, Kumar R, Bell NH. Vitamin D
metabolism is altered in Asian Indians in the southern United States:
a clinical research center study. J Clin Endocrinol Metab 1998;83:
169–73.
33 Hollis BW, Wagner CL. Vitamin D deficiency during pregnancy: an
ongoing epidemic. Am J Clin Nutr 2006;84:273.
34 Johnson DD, Wagner CL, Hulsey TC, McNeil RB, Ebeling M, Hollis BW.
Vitamin D deficiency and insufficiency is common during pregnancy.
Am J Perinatol 2011;28:7–12.
35 Barrett H, McElduff A. Vitamin D and pregnancy: an old problem
revisited. Best Pract Res Clin Endocrinol Metab 2010;24:527–39.
Maternal serum vitamin D levels in early pregnancy
ª 2011 The Authors BJOG An International Journal of Obstetrics and Gynaecology ª 2011 RCOG 955