Embed Size (px)
Citation preview

Eur Radio1 (2003) 13:M31-M41DOl 1O.1007/s00330-003-2129-8
© Springer-Verlag 2003
Pierre-Jean ValetteFrank PilleulArielle Crombe-Ternamian
MDCT of benign liver tumors and metastases
P.-J. Va1ette(~) . F. Pilleu1· A. Crombe-TernamianDepartment of Digestive Radiology,Pavillon H, Hopital Edouard Herriot,Place d' Arsonval, 69003 Lyon, Francee-mail: [email protected].: +33-47-2117540Fax: +33-47-2117541
Introduction
Multi-detector computed tomography (MDCT) theoretically presents several advantages for liver imaging including optimal timing of tumor contrast enhancementand increased spatial resolution. Such advantages havebeen advocated to improve diagnosis of benign tumorsand detection of metastases. The results, however,should be carefully analyzed with reference to the various objectives of a liver CT. When performed to diagnose a benign tumor, the role of CT is to demonstrate thenature of the liver mass. Highly specific and confidentdiagnosis with regard to the type of tumor is then expected. In the case of extra-hepatic malignancy, the aim ofCT is to evidence, or even more importantly, to rule outliver metastases. High sensitivity and negative predictivevalue are needed. The MDCT also brings with it newchallenges concerning the acquisition and contrast-injection protocols that should be adapted to the clinical situation and type of lesion expected. A clear understandingof all these clinical data and technical parameters is necessary to state what might be the real advances of MDCTfor liver tumors exploration and how this technologymay modify the diagnostic strategies.
Technique
Detection of lesions in the liver is determined by conspicuity which relates to the degree of liver-to-tumor con-
trast. This contrast is typically positive in cases of hypervascular lesion or negative in cases of hypovascularlesion. Some degree of characterization may also beobtained by analyzing the type of tumor enhancement incases of hypervascular tumor. Since the tumoral hypervascularity is related mainly to the arterial supply, a very sharptiming of acquisition is needed after contrast injection, tooptimize both, tumor conspicuity and characterization.
This timing of acquisition is described in severalphases [1, 2]. At 20 s, there is relatively little enhancement of the liver parenchyma and all types of tumors.!his very early phase, namely the "early arterial phase,"IS used only to determine the hepatic arterial anatomybefore hepatic surgery and has little interest in terms oftumor detection or characterization. At 30-35 s, sufficient time has elapsed for the tumoral vasculature to enhance the hypervascular lesions. Liver enhancement,which mainly results from later portal supply, is still limited at this point, and hypervascular tumors are moreconspicuous and typically appear hyperdense. This period is named the "late arterial phase." After 1 min, thedegree of enhancement of the liver and hypervascular lesions becomes similar and the lesions conspicuity dec~e~ses, whereas hypovascular lesions become clearlyvisible as hypodense masses inside the liver. This periodis termed the "portal venous phase." Late phases, afterseveral minutes, may also be of interest to demonstratelate tumoral enhancement as observed in hemangiomasand fibrotic lesions.
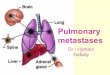
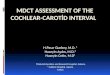
One of the advantages of MDCT is to provide fasteracquisitions compared with single-slice helical CT. Withrespect to the multiphase liver-to-tumor-contrast uptakedescription, MDCT, which allows a true late-arterialphase imaging of the entire liver, should improve hypervascular lesion exploration (Fig. 1). Imaging of hypovascular lesions (Fig. 2) should take less advantage of thistechnology except for the fact that thinner slices may beobtained with an increased spatial resolution and theoretically, produce better results in detection of small nod-

M32
Table 1 Scan protocols for liver imaging
MDCT diagnosis of benign liver tumors
Benign tumors are often discovered in patients free ofsymptoms while undergoing imaging examinations forunrelated reasons. Hemangioma is the most frequent ofthese tumors with a prevalence ranging from 2 to 20% inthe general population. Focal nodular hyperplasia is thesecond most frequent benign tumor, far behind hemangioma. Liver adenoma is extremely rare compared with thepreviously mentioned tumors. The classical issue of imaging is to characterize these liver lesions as benign andto rule out malignant tumors. A more practical approachis to demonstrate with full specificity the nature of thelesions, which deserve conservative management, in order to avoid unnecessary surgery. From this point ofview, the imaging strategy may be simplified by obtaining an unequivocal diagnosis of hemangioma or focal
4 slice
1201160/0.5s2.5mm
12.5 mm5mm3mm2 ml!kg4 mlls
Arterial phase 35 sPortal phase 55 s
KVlEffective mAslRotation time (s)Detector Collimation (mm)FeedIRotation (mm)Slice thickness (mm)IncrementIV Contrast Volume (400 mgUmg)/salineInjection RateScan Delay (s)
they are larger or equal to collimation. Finally, the userchoice may be resumed to the initial collimation thickness and to one or more sets of effective reconstructionwidths that suit the clinical situation. This choice is acompromise between spatial resolution, which is improved with thin sections, and image noise which growsdisproportionately when section width is forced to beidentical to collimation width. The last parameter to bechosen by the user, independently from the others, isslice overlapping which is needed when multiplanar reconstruction is performed.
In clinical practice, a typical MDCT protocol for hypervascular tumors (including benign tumors and hypervascular metastases) is a dual-phase acquisition at 5-mmsection thickness, after contrast bolus injection at 4 mllsdelivery rate for total volume of 1.7-2 mllkg (Table 1).Synchronization with the late arterial phase is obtainedby setting a 35-s delay, or even better, with the use a bolus-triggering system. Portal phase is obtained, after 60-sdelay, with the same scanning parameters. An additionallate phase may be performed after 3 min, if needed(hemangiomas). For hypovascular metastases, similarparameters can be chosen, except that a single acquisition, after 60-s delay, is often sufficient.
Fig. 1 Enhancement profile of liver hypervascular tumor, focalnodular hyperplasia (FNH)
Fig. 2 Enhancement profile of liver hypovascular tumor (livermetastases)
ules. A number of studies [3, 4, 5, 6] have now clearlydemonstrated how the injection parameters may influence the liver and tumor enhancement in terms of quantity, delivery rate, and type of contrast. The best visualization of hypervascular tumors is obtained at the arterialphase with the use of high-concentration contrast mediaand increased delivery rate. Enhancement during the portal phase is dependent mostly on the total dose of iodineadministered.
The other advantage of MDCT is the potential to reduce the effective section width without excessive scanduration or limited length [7]. Section width is the finalreconstruction result of multiple acquisition parametersincluding, collimation, table feed per rotation, and pitch.The available choices of section thickness are dependenton the manufacturer and the type of multislice raw-datainterpolation and reconstruction. Multiple data sets, withvarying section width, may also be reconstructed fromthe same raw data, with the only precondition being that

M33
Fig. 3 Typical hemangioma at CT: globular enhancement similarto blood attenuation, at rapid CT with bolus administration of contrast material, and late persistent opacification
nodular hyperplasia, when possible. Such strategy resolves over 90% of cases of benign liver tumors. It neglects the difficult problem of adenomas, but this is oflittle consequence considering the rarity of these tumors.Moreover, adenomas must theoretically be surgically removed because of a potential risk of rupture and of thepossible confusion or association with a hepatocellularcarcinoma, which can only be ruled out after the systematic screening of the entire lesion at pathology.
Hemangiomas
Most cavernous hemangiomas are easily diagnosed dueto characteristic features, such as near isoattenuationwith blood on nonenhanced images, globular or nodularperipheral enhancement similar to blood attenuation atrapid CT with bolus administration of contrast material,and late persistent opacification (Fig. 3). This typicalpresentation has been described for many years with theuse of monodetector CT, and the multidetector technology does not appear to be able to provide further diagnostic information in such cases. The presence of atypicalfeatures may, however, lead to misdiagnosis and confusion with other lesions [8]. Large heterogeneous hemangiomas with incomplete late filling, hyalinized hemangiomas with lack of peripheral enhancement, cystic hemangiomas, and hemangiomas with adjacent arterioportalshunts all result in atypical enhancement at CT. Sincemost of these atypical presentations are not related toany type of feature that could be more accurately explored at the arterial phase, there is little chance thatMDCT may improve the diagnosis in these cases. Moreover, MR imaging has been shown to have global sensi-
tivity and specificity of >90% due to a relatively strongT2 hyperintensity, and is able to diagnose most caseswithout the need for a CT study (Fig. 4).
The interest in the multiphase CT technique has, however, been specifically studied for the diagnosis of smallhemangiomas, which are difficult to characterize due tohomogeneous rapid filling at the arterial phase (Figs. 5,6), instead of early globular enhancement with late opacification. Kim et al. [9] reviewed 37 small hemangiomas and 49 malignant tumors in 86 patients in order toassess the accuracy of three-phase helical CT for differentiating small hemangiomas from small hypervascularmalignant tumors. Kim et al. [9] confirmed that smallhemangiomas frequently show atypical appearance atCT. They also showed that multiphase CT does not improve the sensivity but does improve the specificity ofthe diagnosis of hemangioma up to 95% when isoattenuation to the blood pool at the combined, nonenhanced,arterial and portal phases is observed.
Focal nodular hyperplasia
Although focal nodular hyperplasias (FNH) are rare tumors, improvements in modern cross-sectional imaginghave made diagnosis of these lesions more frequent. TheFNHs are probably caused by a hyperplastic response tolocalized vascular abnormality and are made of normalhepatocytes; therefore, needle biopsies are likely to benondiagnostic and specific diagnosis is based primarilyon imaging methods.
The CT characteristics of FNH have been describedin multiple publications [10, 11]. The FNH is usually homogeneous and isoattenuating to normal liver beforecontrast injection. At late arterial phase, FNH typicallypresents with a bright homogeneous enhancement and ahypodense central scar (Fig. 7). Infrequent, but also quitecharacteristic, are the radiating hypodense fibrous bands,

M34
Fig. 5 Atypical rapid fillingsmall hemangioma at CT: differential diagnosis with hypervascular tumor cannot be assessed
Fig. 4a, b Typical hemangioma at MR (same patient as in Fig. 3):enhancement pattern after gadolinium injection is similar to CT,and typical marked T2 hyperintensity is observed

M35
Fig. 6 Atypical rapid filling small hemangioma at MR (same patient as in Fig. 5): diagnosis of hemangioma can be assessed because ofcharacteristic T2 hyperintensity
Fig. 7 Typical FNH at CT. At late arterial phase, typical brighthomogeneous enhancement and hypodense central scar containingfeeding arteries. At portal phase, isoattenuation to the normal liverand hypodense central scar. At delayed phase hyperdensity of thecentral scar. Draining peripheral veins are also visible
or septas, arising from the scar. At portal phase, FNH returns to isoattenuation to the normal liver and may bedifficult to detect. Delayed phase often shows hyperdensity of the central scar and septas due to the late opacification of the fibrotic content of these structures. Dilatedfeeding arteries penetrating the central scar, and drainingveins running at the surface of the lesion, may be recognized in large FNH. Additional common features of FNHare homogeneous pattern except for the scar area, welldefined margins without capsule , and lobulated contours.
When all these features are present, the diagnosis ofFNH may be considered as specific. Since early hyperdensity of the tumor is the most reliable sign, MDCT,which allows the rapid scanning of the entire liver at thelate arterial phase, should facilitate the characterization
of FNH, particularly when multiple lesions at differentlocation levels are present; however, MR is now considered as the imaging technique of choice in the case ofFNH. Before contrast medium injection, MR shows typical nearly isointensity of the tumor mass to normal liverand hyperintensity of the central scar on T2-weightedimages (Fig. 8). After gadolinium injection, MR demonstrates the same characteristics as CT, without the risk oflarge quantities of iodine contrast-agent injection and irradiation.
Atypical FNH represents almost 50% of cases. TheseFNH induce two types of situations: firstly, lesionswhich have all FNH characteri stics except for the centralscar. Such presentation is usual with small FNH. It mayalso be observed in large FNH, when the scar is verythin, located near the surface of the tumor, or missing.Confident differential diagnosis with any type of hypervascular tumor, including adenomas and hepatocellularcarcinomas, is then more difficult to assess, but the diagnosis of FNH still can be considered. Final diagnosis relies on MR, which sometimes is able to display a thin

M36
Fig. 8 Typical FNH at MR.Homogeneous isoattenuatingliver mass on TI and T2 sequences. Central scar is hypointense on TI sequence andhyperintense on T2 sequence.Bright homogeneous tumor hyperintensity at arterial-phase T1sequence, whereas at late portalphase the tumor returns to isointensity and the central scarbecomes hyperintense
Fig. 9 Atypical FNH at CT. Hypervascular tumor at late arterialphase with pseudocapule and missing clear picture of central scar.In addition, a peritumoral abnormal arterial liver perfusion is visible. Tumor is not any more visible at portal phase
scar that is not detectable on CT. The MR is also moreaccurate than CT in demonstrating the homogeneity andliver isointensity of the lesion on all sequences (Figs. 9,10). Ba-Ssalamah et al. [12] also advocated the use ofliver-specific MR contrast agents. These agents result inhomogeneous contrast uptake with better delineation ofcentral scar which may help to make confident diagnosis. Finally, some additional arguments may be obtained,

M37
Fig. 10 Atypical FNH at MR (same patient as in Fig. 9). Tl without contrast and TI-weighted images show an almost isointensenormal liver tumor. Diagnosis likely corresponds to FNH, although the central still remains undetectable. Final proof will beobtained at percutaneous biopsy
if needed, from large-needle percutaneous biopsies of thelesion and the adjacent liver. The histopathology of thesesamplings remains quite challenging but has been demonstrated to be of some value when performed into lesions with non-specific , but FNH-compatible, radiological features [13]. Such strategy results in a final and confident diagnosis in over 90% of cases in which surgerycan be avoided.
In the second type of presentation, FNH has atypicalfeatures that should preclude the diagnosis. It may be apseudocapsule or an inhomogeneous content due to focaltelangectasic areas, fat deposits, or necrosis. Differentialdiagnosis is, therefore, almost impossible to obtain onimaging techniques and resection surgery must be performed.
Liver adenomas
As FNH, adenomas typically present hyperdensity on enhanced scans at the late arterial phase. Ruppert-Kohlmayr et al. [14] have tried to evidence some differencesin the tumor attenuation, after contrast injection, on triple-phase CT to differenciate adenomas from FNH. Relative enhancement is significantly higher in 100% oflarge FNH and lower in 87% of large adenomas at the arterial phase. These results induce a promising, global accuracy of approximately 96%; however, they are of limited interest in clinical practice since they are not applicable to small tumors. Moreover, most large adenomasalso show a fibrotic capsule, subcapsular feeding arteries, or necrotic or fatty areas, which are even better
signs against the diagnosis of FNH (Figs. 11, 12). Another question is the differential diagnosis between adenomas and hepatocellular carcinomas developed on healthyliver. Both tumors may be very similar on imaging techniques and the final diagnosis of adenoma should beconsidered as almost impossible. This is the reason that adiagnosis of adenoma always induces a resection surgery.
Diagnosis of benign liver tumors in clinical practice
In clinical practice, with the sole objective of identifyinglesions that should not be resected, the diagnostics of benign liver tumor may be resumed for confident characterization of hemangiomas and FNH. This can beachieved with MDCT, but also with MR which demonstrates similar semiology after gadolinium and has theadvantage of providing additional information on the tumor content with the use of T I and T2 non-enhanced sequences; therefore, although MDCT certainly has improved the conditions of CT examination of liver benigntumors with the use of multiphase acquisitions, it remains less appropriate than MR when a benign liver lesion is suspected.
MDCT diagnosis of liver metastases
The diagnosis of liver metastases is often crucial for theinitial therapeutic management and follow-up of patientswith a malignant tumor. The CT is often used as ascreening method when a malignant tumor is discoveredto rule out metastases that may modify the treatmentplanning. Once liver metastases have been evidenced,CT provides information on size, number, and localization of the lesions that determine the feasibility of resection or percutaneous radio-frequency treatment. When

M38
Fig. 11 Liver adenoma at CT. Moderately hypervascular tumor with inhomogeneous content both at late arterial and portal phase. Afalse image of central scar is visible
Fig. 12 Liver adenoma at MR (same patient as in Fig. 11). T2weighted image shows an inhomogeneous tumor with hyperdenseareas that preclude the diagnosis of FNH. Gadolinium injection reveals slight opacification at arterial phase
liver metastases are treated by chemotherapy, the treatment protocol is adapted to the response as estimated onthe tumor size measurements on CT images. Accordingto these multiple clinical situations, an efficient imagingmodality would be one which provides a high negative

Fig. 13 Small colon metastasi snot visualized a at 8-mm scanwidth and clearly evidenced atb 5-mm scan width (arrow)
M39
predictive value to rule out metastatic disease in patientsapparently free of liver lesions, a high sensitivity to detect small metastases distant to ones that could be resected, and a minimally invasiveness since imaging techniques will have to be repeated several times during thecourse of the disease [15].
Hypervascular metastases come from thyroid, pancreatic islet-cell tumors, carcinoid tumors, renal cell carcinoma, and variable breast tumors and melanoma. As forbenign liver tumors and hepatocellular carcinoma, tumordetection should be better at the late arterial phase whenthe lesions are hyperdense compared with adjacent liver.The MDCT has not yet been evaluated in such indications, but some studies [16] have shown that late arterialphase provides added value in evaluating carcinoid livermetastasis .
Most liver metastases are hypovascular. The primarytumors which lead to hypovascular metastases includethose of the colon and rectum (most frequent), pancreas,lung, urothelium, prostate, and gynecological malignancies, except choriocarcinoma. At CT, these metastasesare hypodense, both at arterial and portal phases. Theymay also present with a thin peripheral enhancement, necrotic areas, or calcifications depending on the type ofprimary tumor. The portal phase is the one most adaptedto lesion detection since it provides the best tumor-to-liver ratio once the liver has been enhanced by the portaliodine supply; therefore, the scan timing does not appearto be as crucial as it is for examinations of tumors requiring a specific arterial phase evaluation. Valls et al. [17]showed, with a series of 157 patients with 290 provencolorectal metastases, that single-detector helical CT hasan overall detection rate of 85% with 4% false positivesonly. In terms of enhancement management , the rapidscanning provided by MDCT does not appear to be ableto improve these results; however, it would seem logicalthat MDCT could improve small metastases detection bythe systematic use of thin slices and higher spatial resolution (Fig. 13). In the study by Valls et al. [17], all falsenegative findings were for lesions <1 em in diameter.
Haider et al. [18] showed that thinner collimation significantly increases the number of small hypoattenuating lesions detected in metastatic livers. For a total number of88 liver lesions 1.5 ern or smaller, the pooled sensitivityfor all lesions was statistically different at 5-mm collimation (66%) and 2.5-mm collimation (82%); however,Haider et al. [18] indicated that no significant differencewas noted between collimations when only the metastatic lesions were considered (sensitivity of 80% at all collimations).
Such results induce two different comments; the firstone is that, with similar injection parameters and scantiming, thin collimation does not improve the small metastases detection rate. Several explanations may be advocated, including increased image noise and absence ofimproved tumor conspicuity. The well-demonstratedhigh sensitivity of CT arterial portography [19] indicatesthat the contrast material dose is probably the most significant factor of small-tumor conspicuity. The secondcomment raises the problem of small hypodense lesionsthat are better evidenced, but not related to the metastaticdisease. Jang et al. [20] specifically studied these lesionson single-phase helical CT. Among 1133 consecutive patients with proven gastric or colorectal cancer, 268 presented with 881 hypodense lesions 1.5 ern or smaller. Final diagnosis showed that 693 lesions (78%) in 248 patients (92%) were benign, and 188 (21%) in 30 patients(11%) were metastases. As mentioned in the same paper[20], helical CT shows a prevalence of small hypodenselesions (25%) higher than that previously reported onconventional CT, whereas the proportion of malignancyis lower. These results confirm that the increase in number of hypoattenuating lesions observed with recent CTtechniques is attributable mainly to improved visibilityof small benign tumors rather than better detection of tiny metastases. From a practical point of view, detectingmore metastases, but also more benign lesions that maybe confused with small metastases, would not be of greatclinical value unless differential diagnosis can be obtained. Most of these small benign tumors correspond to

M40
Fig. 14 Small liver hypoattenuating lesion revealed in courseof a preoperative study for aleft lobe colon metastasis (notvisible here). Hyperintensityon T2-weighted MR sequencereveals the cystic nature of thelesion (proven to be a biliaryhamartoma at surgery; arrows)
cystic lesions, including biliary hamartomas, and focalfatty sparing. For Jag et al. [20], differential diagnosiswith true metastases, based on water attenuation andsharp margins in case of liver cysts, angular margins, andtypical location in case of fatty infiltration, is possiblewith careful analysis of CT findings; however, the number of misclassified lesions did not decrease at thinnercollimation in the series of Haider et al. [18].
All these limitations bring into question the benefit ofcollimation of <5 mm for diagnosis of small metastases.A possible outcome would be the association of thin-collimation MDCT for lesion detection, and thereafter, MRfor characterization of small undetermined lesions, sincethis technique is probably of greater value in demonstrating small cysts on T2 sequences (Fig. 14) and focal fattyinfiltration on in/out-of-phase Tl sequences.
References
Conclusion
Multi-detector computed tomography reduces acquisition times allowing reasonable breath-hold lengths andbetter synchronization of scanning with liver opacification phases, and allows systematic use of 5-mm sectionthickness, inducing better spatial resolution. At least forthese reasons, MDCT has definitely improved CT imagequality and reproducibility in clinical practice. Publisheddata, however, have not yet demonstrated statistical improvements in the diagnosis of benign liver tumors andmetastases. Therefore, no significant changes in the diagnostic strategies can be advanced at the present time.The MR still remains the gold standard examinationwhen a benign tumor is suspected. There is little chancethat, whatever the future technical refinements are,MDCT will change this fact. The CT remains a majortechnique for detection of metastases. Further studies areneeded to determine if collimation <5 mm associatedwith high-concentration media, postcontrast saline bolus,or any other innovative form of contrast administrationmay be of any interest to improve liver metastases detection.
1. Spielman A, Nelson R (2003) Liver.In: Bonomo L, Foley DW, Imhof H,Rubin G (eds) Multidetector CT technology: advances in imaging techniques. Royal Society of MedicinePress, London, pp 129-139
2. Foley WD, Mallisee TA, HohenwalterMD (2000) Multiphase hepatic CTwith multirow-detector CT scanners.AJR 175:679-685
3. Berland LL, Lee JY (1988)Comparison of contrast media injectionrates and volumes for hepatic dynamicincremented CT. Invest Radiol23:918-922
4. Awai K, Takasa K, Ohishi H (2002)Aortic and hepatic enhancementand tumor-to-liver contrast:analysis of different concentrationsof contast material at multidetectorrow helical CT. Radiology224:757-763
5. Fleischmann D (2003) Use ofhigh-concentration contrast media:principles and rationale-vasculardistrict. In: Bonomo L, Foley DW,ImhofH, Rubin G (eds) MultidetectorCT technology: advances in imagingtechniques. Royal Society of MedicinePress, London, pp 27-38
6. Brink JA (2003) Use of highconcentration contrast media: principles and rationale: body CT. Eur JRadiol 45:S53-S58

7. Prokop M (2003) General principles ofMDCT. Eur J RadioI45:S4-SlO
8. Vi1grain V, Boulos L, Vullierme MP etal. (2000) Imaging of atypical hemangiomas of the liver with pathologiccorrelation. Radiographies 20:379-397
9. Kim T, Federle MP, Baron RL et al.(2001) Discrimination of small hemangiomas from hypervascular malignanttumors smaller than 3 em with threephase helical CT. Radiology219:699-706
10. Van Beers Be, Horsman Y, Sempoux C(2003) Scanner multi-detecteur faceal'IRM dans les tumeurs benignes dufoie. Eur J Radiol 84:445-456
11. Brancatelli G, Ferderle MP, Grazioli Let al. (2001) Focal nodular hyperplasia:CT findings with emphasis on multiphasic helical CT in 78 patients.Radiology 219:61-68
12. Ba-Ssalamah A, Schima W, SchmookMT et al. (2002) Atypical focal nodularhyperplasia of the liver: imaging features of nonspecific and liver-specificMR contrast agents. AIR179:1447-1456
13. Fabre M, Neyra M (1995) Role offine-needle puncture in the diagnosis ofa hepatic mass. Ann Pathol15:380-387
14. Ruppert-Kohlmayr A, Uggowitzer M,Kugler C et al. (2001) Focal nodulahyperplasia and hepatocellular adenoma of the liver: differentiation withmultiphasic helical CT. AJR176:1493-1498
15. Vilgrain V (2003) Scanner multi detecteur face al'IRM dans les tumeursmalignes du foie. Eur J Radiol84:459-470
16. Paulson EK, McDermott VG,Keogan MT et al. (1998) Carcinoidmetastases to the liver: role oftriple-phase helical CT. Radiology.206:143-150
17. Valls C, Andia E, Sanchez A, Guma A,Figueras J, Torras J, Serrano T (2001)Hepatic metastases from colorectalcancer: preoperative detection and assessment of resectability with helicalCT. Radiology 218:55-60
M41
18. Haider MA, Amitai, MM, RappaportDC et al. (2002) Multidetector-rowhelical CT in preoperative assessmentof small (~1.5 em) liver metastases: Isthinner collimation better? Radiology225:137-142
19. Kehagias D, Metafa A, Hatziioannou Aet al. (2000) Comparison of CT, MRIand CT during arterial portography inthe detection of malignant hepatic lesions. Hepatogastroenterology47:1399-1403
20. Jang HJ, Lim HK, Lee AJ et al. (2002)Small hypoattenuating lesions in theliver on single-phase helical CT inpreoperative patients with gastricand colorectal cancer: prevalence,significance and differentiatingfeatures. J Comput Assist Tomogr26:718-724