Embed Size (px)
Citation preview

n engl j med
352;10
www.nejm.org march
10, 2005
The
new england journal
of
medicine
1011
review article
medical progress
Anemia of Chronic Disease
Guenter Weiss, M.D., and Lawrence T. Goodnough, M.D.
From the Department of General InternalMedicine, Clinical Immunology and Infec-tious Diseases, Medical University of Inns-bruck, Innsbruck, Austria (G.W.); and theDepartments of Pathology and Medicine,Stanford University, Stanford, Calif. (L.T.G.).Address reprint requests to Dr. Weiss atthe Department of General Internal Medi-cine, Clinical Immunology and InfectiousDiseases, Medical University of Innsbruck,Anichstr. 35, A-6020 Innsbruck, Austria, orat [email protected].
N Engl J Med 2005;352:1011-23.
Copyright © 2005 Massachusetts Medical Society.
nemia of chronic disease, the anemia that is the second most
prevalent after anemia caused by iron deficiency, occurs in patients with acuteor chronic immune activation.
1-4
The condition has thus been termed “anemiaof inflammation.”
1-4
The most frequent conditions associated with anemia of chronicdisease are listed in Table 1.
5-22
Anemia of chronic disease is immune driven; cytokines and cells of the reticuloendo-thelial system induce changes in iron homeostasis, the proliferation of erythroid pro-genitor cells, the production of erythropoietin, and the life span of red cells, all of whichcontribute to the pathogenesis of anemia (Fig. 1). Erythropoiesis can be affected by dis-ease underlying anemia of chronic disease through the infiltration of tumor cells intobone marrow or of microorganisms, as seen in human immunodeficiency virus (HIV)infection, hepatitis C, and malaria.
23,24
Moreover, tumor cells can produce proinflam-matory cytokines and free radicals that damage erythroid progenitor cells.
3,4,8
Bleedingepisodes, vitamin deficiencies (e.g., of cobalamin and folic acid), hypersplenism, auto-immune hemolysis, renal dysfunction, and radio- and chemotherapeutic interventionsthemselves can also aggravate anemia.
25,26
Anemia with chronic kidney disease shares some of the characteristics of anemia ofchronic disease, although the decrease in the production of erythropoietin, mediated byrenal insufficiency and the antiproliferative effects of accumulating uremic toxins, con-tribute importantly.
27
In addition, in patients with end-stage renal disease, chronic im-mune activation can arise from contact activation of immune cells by dialysis mem-branes, from frequent episodes of infection, or from both factors, and such patientspresent with changes in the homeostasis of body iron that is typical of anemia ofchronic disease.
27
dysregulation of iron homeostasis
A hallmark of anemia of chronic disease is the development of disturbances of ironhomeostasis, with increased uptake and retention of iron within cells of the reticuloen-dothelial system. This leads to a diversion of iron from the circulation into storage sitesof the reticuloendothelial system, subsequent limitation of the availability of iron forerythroid progenitor cells, and iron-restricted erythropoiesis.
In mice that are injected with the proinflammatory cytokines interleukin-1 and tumornecrosis factor
a
(TNF-
a
), both hypoferremia and anemia develop
28
; this combinationof conditions has been linked to cytokine-inducible synthesis of ferritin, the major pro-tein associated with iron storage, by macrophages and hepatocytes.
29
In chronic inflam-mation, the acquisition of iron by macrophages most prominently takes place througherythrophagocytosis
30
and the transmembrane import of ferrous iron by the protein di-valent metal transporter 1 (DMT1).
31
a
pathophysiological features
Copyright © 2005 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at CAUL on March 16, 2010 .
n engl j med
352;10
www.nejm.org march
10
,
2005
The
new england journal
of
medicine
1012
Interferon-
g
, lipopolysaccharide, and TNF-
a
up-regulate the expression of DMT1, with an increaseduptake of iron into activated macrophages.
32
Theseproinflammatory stimuli also induce the retentionof iron in macrophages by down-regulating the ex-pression of ferroportin, thus blocking the release ofiron from these cells.
32
Ferroportin is a transmem-brane exporter of iron, a process that is believed tobe responsible for the transfer of absorbed ferrousiron from duodenal enterocytes to the circulation.
33
Moreover, antiinflammatory cytokines such as inter-leukin-10 can induce anemia through the stimula-tion of transferrin-mediated acquisition of iron by
macrophages and by translational stimulation offerritin expression
34
(Fig. 1).The identification of hepcidin, an iron-regulated
acute-phase protein that is composed of 25 aminoacids, helped to shed light on the relationship of theimmune response to iron homeostasis and anemiaof chronic disease. Hepcidin expression is inducedby lipopolysaccharide and interleukin-6 and is in-hibited by TNF-
a
.
35
Transgenic or constitutive over-expression of hepcidin results in severe iron-defi-ciency anemia in mice.
36
Inflammation in mice thatare hepcidin-deficient did not lead to hypoferremia,a finding that suggests that hepcidin may be central-
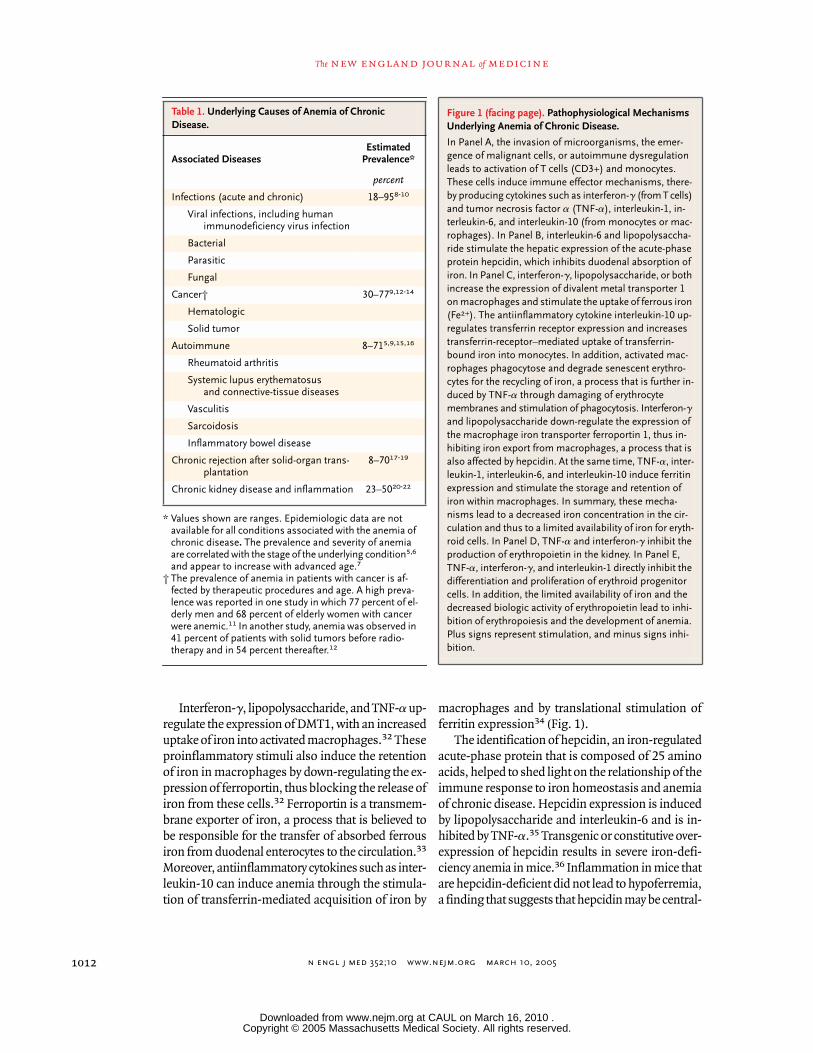
* Values shown are ranges. Epidemiologic data are not available for all conditions associated with the anemia of chronic disease
.
The prevalence and severity of anemia are correlated with the stage of the underlying condition
5,6
and appear to increase with advanced age.
7
† The prevalence of anemia in patients with cancer is af-fected by therapeutic procedures and age. A high preva-lence was reported in one study in which 77 percent of el-derly men and 68 percent of elderly women with cancer were anemic.
11
In another study, anemia was observed in 41 percent of patients with solid tumors before radio-
therapy and in 54 percent thereafter.
12
Table 1. Underlying Causes of Anemia of ChronicDisease.
Associated DiseasesEstimated
Prevalence*
percent
Infections (acute and chronic) 18–95
8-10
Viral infections, including human immunodeficiency virus infection
Bacterial
Parasitic
Fungal
Cancer† 30–77
9,12-14
Hematologic
Solid tumor
Autoimmune 8–71
5,9,15,16
Rheumatoid arthritis
Systemic lupus erythematosusand connective-tissue diseases
Vasculitis
Sarcoidosis
Inflammatory bowel disease
Chronic rejection after solid-organ trans-plantation
8–70
17-19
Chronic kidney disease and inflammation 23–50
20-22
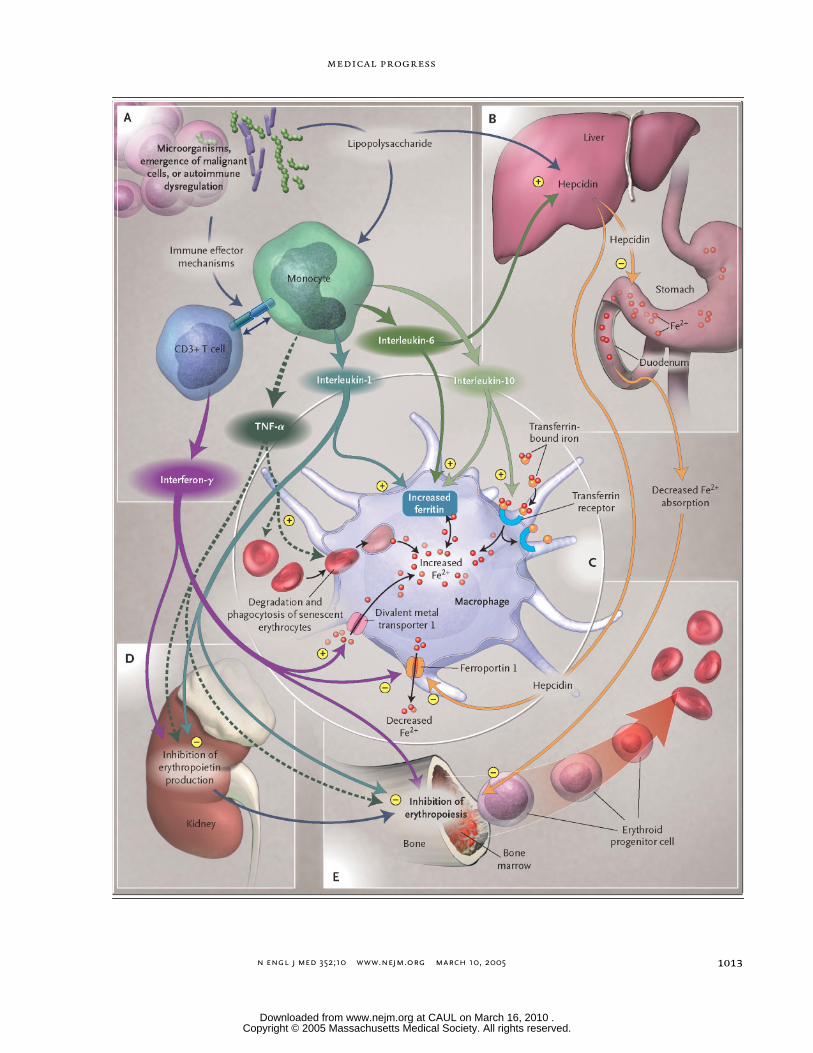
Figure 1 (facing page). Pathophysiological Mechanisms Underlying Anemia of Chronic Disease.
In Panel A, the invasion of microorganisms, the emer-gence of malignant cells, or autoimmune dysregulation leads to activation of T cells (CD3+) and monocytes. These cells induce immune effector mechanisms, there-by producing cytokines such as interferon-
g
(from T cells) and tumor necrosis factor
a
(TNF-
a
), interleukin-1, in-terleukin-6, and interleukin-10 (from monocytes or mac-rophages). In Panel B, interleukin-6 and lipopolysaccha-ride stimulate the hepatic expression of the acute-phase protein hepcidin, which inhibits duodenal absorption of iron. In Panel C, interferon-
g
, lipopolysaccharide, or both increase the expression of divalent metal transporter 1 on macrophages and stimulate the uptake of ferrous iron (Fe
2
+
). The antiinflammatory cytokine interleukin-10 up-regulates transferrin receptor expression and increases transferrin-receptor–mediated uptake of transferrin-bound iron into monocytes. In addition, activated mac-rophages phagocytose and degrade senescent erythro-cytes for the recycling of iron, a process that is further in-duced by TNF-
a
through damaging of erythrocyte membranes and stimulation of phagocytosis. Interferon-
g
and lipopolysaccharide down-regulate the expression of the macrophage iron transporter ferroportin 1, thus in-hibiting iron export from macrophages, a process that is also affected by hepcidin. At the same time, TNF-
a
, inter-leukin-1, interleukin-6, and interleukin-10 induce ferritin expression and stimulate the storage and retention of iron within macrophages. In summary, these mecha-nisms lead to a decreased iron concentration in the cir-culation and thus to a limited availability of iron for eryth-roid cells. In Panel D, TNF-
a
and interferon-
g
inhibit the production of erythropoietin in the kidney. In Panel E, TNF-
a
, interferon-
g
, and interleukin-1 directly inhibit the differentiation and proliferation of erythroid progenitor cells. In addition, the limited availability of iron and the decreased biologic activity of erythropoietin lead to inhi-bition of erythropoiesis and the development of anemia. Plus signs represent stimulation, and minus signs inhi-bition.
Copyright © 2005 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at CAUL on March 16, 2010 .
n engl j med
352;10
www.nejm.org march
10, 2005
medical progress
1013
Copyright © 2005 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at CAUL on March 16, 2010 .

n engl j med
352;10
www.nejm.org march
10
,
2005
The
new england journal
of
medicine
1014
ly involved in the diversion of iron traffic throughdecreased duodenal absorption of iron and theblocking of iron release from macrophages that oc-curs in anemia of chronic disease (Fig. 1).
35,37
Theinduction of hypoferremia by interleukin-6 and hep-cidin occurs within a few hours and is not observedin interleukin-6–knockout mice that are treated withturpentine as a model of inflammation, a findingthat suggests that hepcidin may be central to ane-mia of chronic disease.
38
A recently identified gene,hemojuvelin, may act in concert with hepcidin ininducing these changes.
39
Accordingly, the distur-bance of iron homeostasis with subsequent limita-tion of the availability of iron for erythroid progen-itor cells appears to impair the proliferation ofthese cells by negatively affecting heme biosynthe-sis (Table 2).
impaired proliferation of erythroid progenitor cells
In patients with anemia of chronic disease, the pro-liferation and differentiation of erythroid precursors— erythroid burst-forming units and erythroid col-ony-forming units — are impaired
4
and are linkedto the inhibitory effects of interferon-
a
, -
b
, and -
g
,TNF-
a
, and interleukin-1, which influence thegrowth of erythroid burst-forming units and eryth-roid colony-forming units.
4
Interferon-
g
appears tobe the most potent inhibitor,
40
as reflected by its in-verse correlation with hemoglobin concentrationsand reticulocyte counts.
6
The underlying mecha-nisms may involve cytokine-mediated induction ofapoptosis, which appears, in part, related to the for-mation of ceramide, the down-regulation of the ex-pression of erythropoietin receptors on progenitorcells, impaired formation and activity of erythro-poietin, and a reduced expression of other pro-hematopoietic factors, such as stem-cell fac-tor.
4,40,41
Moreover, cytokines exert direct toxiceffects on progenitor cells by inducing the forma-tion of labile free radicals such as nitric oxide or su-peroxide anion by neighboring macrophage-likecells (Table 2).
42
blunted erythropoietin response
Erythropoietin regulates erythroid-cell proliferationcentrally. Erythropoietin expression is inversely re-lated to tissue oxygenation and hemoglobin levels,and there is a semilogarithmic relation between theerythropoietin response (log) and the degree of ane-mia (linear). Erythropoietin responses in anemia of
chronic disease are inadequate for the degree ofanemia in most, but not all, conditions.
43,44
Thecytokines interleukin-1 and TNF-
a
directly inhibiterythropoietin expression in vitro
45
— a findingthat is probably due, at least in part, to cytokine-me-diated formation of reactive oxygen species, whichin turn affects the binding affinities of erythropoi-etin-inducing transcription factors and also dam-ages erythropoietin-producing cells. Althoughconvincing data from human studies are lacking,the injection of lipopolysaccharide into mice re-sults in reduced expression of erythropoietinmRNA in kidneys and decreased levels of circulat-ing erythropoietin.
45
The responsiveness of erythroid progenitor cellsto erythropoietin appears to be inversely related tothe severity of the underlying chronic disease andthe amount of circulating cytokines, since in thepresence of high concentrations of interferon-
g
orTNF-
a
, much higher amounts of erythropoietin arerequired to restore the formation of erythroid col-ony-forming units.
46
After binding to its receptor,erythropoietin stimulates members of the signaltransduction pathways and subsequently activatesmitogen and tyrosine kinase phosphorylation, pro-cesses affected by the inflammatory cytokines andthe negative-feedback regulation they induce.
45,47
The response to erythropoietin is further reducedby the inhibitory effects of proinflammatory cyto-kines toward the proliferation of erythroid progen-itor cells, the parallel down-regulation of erythro-poietin receptors, and the limited availability of ironto contribute to cell proliferation and hemoglobinsynthesis. Finally, increased erythrophagocytosisduring inflammation leads to a decreased erythro-cyte half-life, along with anticipated damage toerythrocytes that is mediated by cytokines and freeradicals (Table 2).
48,49
iron status
Anemia of chronic disease is a normochromic, nor-mocytic anemia that is characteristically mild (he-moglobin level, 9.5 g per deciliter) to moderate(hemoglobin level, 8 g per deciliter). Patients withthe condition have a low reticulocyte count, whichindicates underproduction of red cells. A definitivediagnosis may be hampered by coexisting bloodloss, the effects of medications, or inborn errors ofhemoglobin synthesis such as thalassemia. The
laboratory evaluation
Copyright © 2005 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at CAUL on March 16, 2010 .
n engl j med
352;10
www.nejm.org march
10, 2005
medical progress
1015
evaluation of anemia of chronic disease must alsoinclude a determination of the status of whole-bodyiron in order to rule out iron-deficiency anemia,
2-4,49
usually hypochromic and microcytic. The differencebetween anemia of chronic disease and iron-defi-
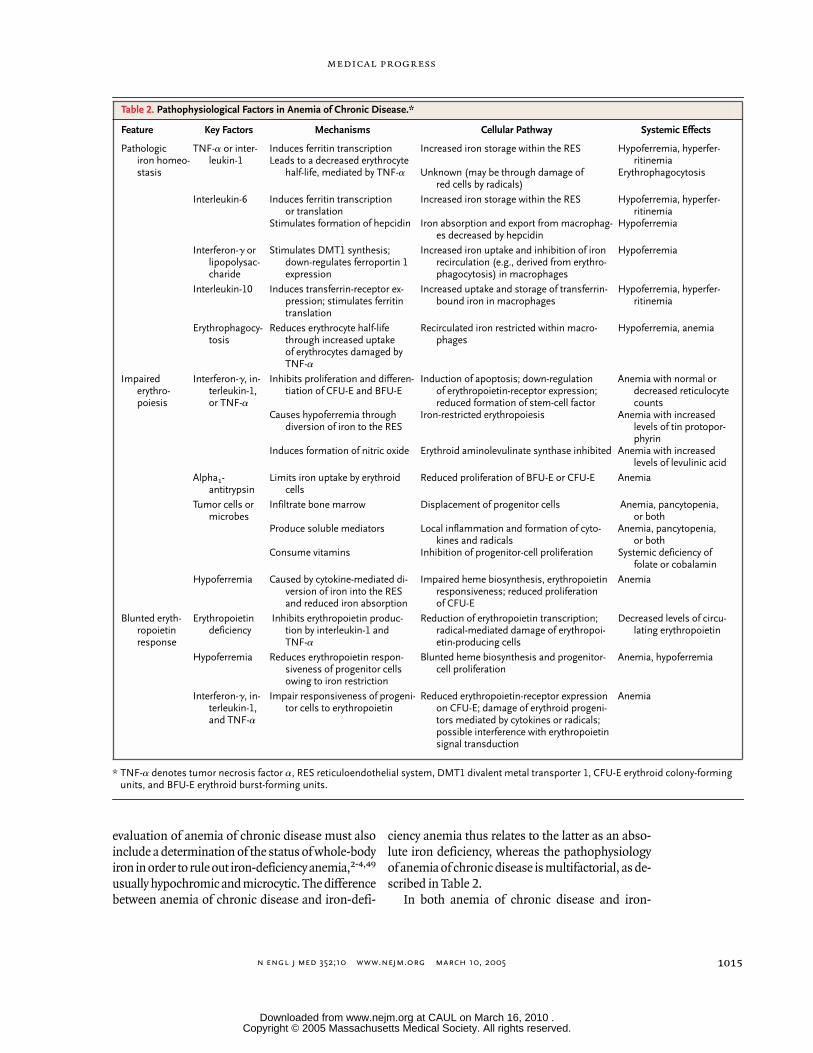
ciency anemia thus relates to the latter as an abso-lute iron deficiency, whereas the pathophysiologyof anemia of chronic disease is multifactorial, as de-scribed in Table 2.
In both anemia of chronic disease and iron-
* TNF-
a
denotes tumor necrosis factor
a
, RES reticuloendothelial system, DMT1 divalent metal transporter 1, CFU-E erythroid colony-forming
units, and BFU-E erythroid burst-forming units.
Table 2. Pathophysiological Factors in Anemia of Chronic Disease.*
Feature Key Factors Mechanisms Cellular Pathway Systemic Effects
Pathologiciron homeo-stasis
TNF-
a
or inter-leukin-1
Induces ferritin transcriptionLeads to a decreased erythrocyte
half-life, mediated by TNF-
a
Increased iron storage within the RES
Unknown (may be through damage ofred cells by radicals)
Hypoferremia, hyperfer-ritinemia
Erythrophagocytosis
Interleukin-6 Induces ferritin transcriptionor translation
Stimulates formation of hepcidin
Increased iron storage within the RES
Iron absorption and export from macrophag-es decreased by hepcidin
Hypoferremia, hyperfer-ritinemia
Hypoferremia
Interferon-
g
or lipopolysac-charide
Stimulates DMT1 synthesis; down-regulates ferroportin 1 expression
Increased iron uptake and inhibition of ironrecirculation (e.g., derived from erythro-phagocytosis) in macrophages
Hypoferremia
Interleukin-10 Induces transferrin-receptor ex-pression; stimulates ferritin translation
Increased uptake and storage of transferrin-bound iron in macrophages
Hypoferremia, hyperfer-ritinemia
Erythrophagocy-tosis
Reduces erythrocyte half-life through increased uptakeof erythrocytes damaged by TNF-
a
Recirculated iron restricted within macro-phages
Hypoferremia, anemia
Impaired erythro-poiesis
Interferon-
g
, in-terleukin-1, or TNF-
a
Inhibits proliferation and differen-tiation of CFU-E and BFU-E
Causes hypoferremia through diversion of iron to the RES
Induces formation of nitric oxide
Induction of apoptosis; down-regulationof erythropoietin-receptor expression; reduced formation of stem-cell factor
Iron-restricted erythropoiesis
Erythroid aminolevulinate synthase inhibited
Anemia with normal or decreased reticulocyte counts
Anemia with increased levels of tin protopor-phyrin
Anemia with increased levels of levulinic acid
Alpha
1
-antitrypsin
Limits iron uptake by erythroid cells
Reduced proliferation of BFU-E or CFU-E Anemia
Tumor cells or microbes
Infiltrate bone marrow
Produce soluble mediators
Consume vitamins
Displacement of progenitor cells
Local inflammation and formation of cyto-kines and radicals
Inhibition of progenitor-cell proliferation
Anemia, pancytopenia, or both
Anemia, pancytopenia, or both
Systemic deficiency of folate or cobalamin
Hypoferremia Caused by cytokine-mediated di-version of iron into the RES and reduced iron absorption
Impaired heme biosynthesis, erythropoietin responsiveness; reduced proliferation of CFU-E
Anemia
Blunted eryth-ropoietin response
Erythropoietin deficiency
Inhibits erythropoietin produc-tion by interleukin-1 and TNF-
a
Reduction of erythropoietin transcription; radical-mediated damage of erythropoi-etin-producing cells
Decreased levels of circu-lating erythropoietin
Hypoferremia Reduces erythropoietin respon-siveness of progenitor cells owing to iron restriction
Blunted heme biosynthesis and progenitor-cell proliferation
Anemia, hypoferremia
Interferon-
g
, in-terleukin-1, and TNF-
a
Impair responsiveness of progeni-tor cells to erythropoietin
Reduced erythropoietin-receptor expression on CFU-E; damage of erythroid progeni-tors mediated by cytokines or radicals; possible interference with erythropoietin signal transduction
Anemia
Copyright © 2005 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at CAUL on March 16, 2010 .

n engl j med
352;10
www.nejm.org march
10
,
2005
The
new england journal
of
medicine
1016
deficiency anemia, the serum concentration of ironand transferrin saturation are reduced, reflectingabsolute iron deficiency in iron-deficiency anemiaand hypoferremia due to acquisition of iron by thereticuloendothelial system in anemia of chronic dis-ease.
2-4
In the case of anemia of chronic disease,the decrease in transferrin saturation is primarily areflection of decreased levels of serum iron. In iron-deficiency anemia, transferrin saturation may beeven lower because serum concentrations of theiron transporter transferrin are increased, whereastransferrin levels remain normal or are decreasedin anemia of chronic disease.
The search for an underlying cause of iron defi-ciency should include a history taking to rule out adietary cause.
42
Frequently, iron deficiency indicatespathological blood loss such as an increased lossof menstrual blood in women or chronic gastroin-testinal bleeding in the setting of ulcerative gastro-intestinal disease, inflammatory bowel disease,angiodysplasia, colon adenomas, gastrointestinalcancer, or parasitic infections.
Ferritin is used as a marker of iron storage, anda level of 15 ng per milliliter is generally taken asindicating absent iron stores.
50
However, a ferritinlevel of 30 ng per milliliter provides better positivepredictive values for iron-deficiency anemia (92 to98 percent) when studied in several populations.
51
For patients with anemia of chronic disease, how-ever, ferritin levels are normal or increased (Table 3),reflecting increased storage and retention of iron
within the reticuloendothelial system, along with in-creased ferritin levels due to immune activation.
29
The soluble transferrin receptor is a truncatedfragment of the membrane receptor that is in-creased in iron deficiency, when the availability ofiron for erythropoiesis is low.
52
In contrast, levels ofsoluble transferrin receptors in anemia of chronicdisease are not significantly different from normal,because transferrin-receptor expression is negative-ly affected by inflammatory cytokines.
53
A determi-nation of the levels of soluble transferrin receptorsby means of commercially available assays can behelpful for differentiation between patients withanemia of chronic disease alone (with either nor-mal or high ferritin levels and low levels of solubletransferrin receptors) and patients with anemia ofchronic disease with accompanying iron deficiency(with low ferritin levels and high levels of solubletransferrin receptors).
52,54
As compared with patients who have anemiaof chronic disease alone, patients with anemia ofchronic disease and concomitant iron-deficiencyanemia more frequently have microcytes, and theiranemia tends to be more severe. The ratio of theconcentration of soluble transferrin receptors to thelog of the ferritin level may also be helpful.
52
A ra-tio of less than 1 suggests anemia of chronic dis-ease, whereas a ratio of more than 2 suggests ab-solute iron deficiency coexisting with anemia ofchronic disease (Table 3). The determination of thepercentage of hypochromic red cells or reticulocytehemoglobin content can also be useful in detectingaccompanying iron-restricted erythropoiesis in pa-tients with anemia of chronic disease.
54
erythropoietin
Measurement of erythropoietin levels is useful onlyfor anemic patients with hemoglobin levels of lessthan 10 g per deciliter, since erythropoietin levels athigher hemoglobin concentrations remain well inthe normal range.
43
Furthermore, any interpreta-tion of an erythropoietin level in anemia of chronicdisease with a hemoglobin level less than 10 g perdeciliter must take into account the degree of ane-mia.
55,56
Erythropoietin levels have been analyzedfor their predictive value with respect to the responseto treatment of anemia of chronic disease with eryth-ropoietic agents.
13,57
After treatment with recombi-nant human erythropoietin (epoetin) for two weeks,either a serum erythropoietin level of more than100 U per liter or a ferritin level of more than 400ng per milliliter predicts a lack of response in 88
* Relative changes are given in relation to the respective normal values.† Patients with both conditions include those with anemia of chronic disease
and true iron deficiency.
Table 3. Serum Levels That Differentiate Anemia of Chronic Diseasefrom Iron-Deficiency Anemia.*
VariableAnemia of
Chronic DiseaseIron-Deficiency
AnemiaBoth
Conditions†
Iron Reduced Reduced Reduced
Transferrin Reducedto normal
Increased Reduced
Transferrin saturation Reduced Reduced Reduced
Ferritin Normalto increased
Reduced Reducedto normal
Soluble transferrin receptor Normal Increased Normalto increased
Ratio of soluble transferrin receptor to log ferritin
Low (<1) High (>2) High (>2)
Cytokine levels Increased Normal Increased
Copyright © 2005 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at CAUL on March 16, 2010 .

n engl j med
352;10
www.nejm.org march
10, 2005
medical progress
1017
percent of patients with cancer who are not receiv-ing concomitant chemotherapy.
13
Such predictorshave not been validated in patients with cancer whoare undergoing chemotherapy.
57
Rather, changes inhemoglobin levels or reticulocyte counts over timeindicate a response to treatment with epoetin.
57
rationale for treatment
The rationale for the treatment of anemia of chron-ic disease is based on two principles. First, anemiacan be generally deleterious in itself, requiring acompensatory increase in cardiac output in order tomaintain systemic oxygen delivery; second, anemiais associated with a poorer prognosis in a variety ofconditions. Thus, moderate anemia warrants cor-rection, especially in patients older than 65 years ofage, those with additional risk factors (such as cor-onary artery disease, pulmonary disease, or chron-ic kidney disease), or a combination of these fac-tors.
7,58
In patients with renal failure who arereceiving dialysis and in patients with cancer whoare undergoing chemotherapy, correction of anemiaup to hemoglobin levels of 12 g per deciliter is asso-ciated with an improvement in the quality of life.
59,60
Anemia has been associated with a relatively poorprognosis among patients with various conditions,including cancer, chronic kidney disease, and con-gestive heart failure.
9
This relationship has been ex-plored most fully in patients undergoing long-termhemodialysis. In a retrospective review of nearly100,000 patients undergoing hemodialysis, levelsof hemoglobin of 8 g per deciliter or less were asso-ciated with a doubling of the odds of death, as com-pared with hemoglobin levels of 10 to 11 g per deci-liter.
61
Moreover, the odds ratios for death amongpatients who entered the study with hematocrit lev-els that were under 30 percent but that increased to30 percent or more did not differ from those of pa-tients who began and finished the study with he-matocrit levels of 30 percent or more. Subsequentanalyses have determined that hematocrit levels thatwere maintained between 33 and 36 percent wereassociated with the lowest risk of death among pa-tients undergoing dialysis.
20,21
This evidence con-tributed to the development of guidelines for themanagement of anemia in patients with cancer orchronic kidney disease, guidelines that recommenda target hemoglobin level of 11 to 12 g per deci-liter.
14,62,63
However, a normal target hematocrit may not
be optimal. A prospective, multicenter trial involv-ing patients who are undergoing dialysis — a studyof an intervention that is designed to achieve nor-mal hematocrit levels (above 42 percent), as com-pared with lower levels (above 30 percent), with theuse of a combination of erythropoietin therapy andintravenous iron dextran — was halted because ofincreased mortality in the high-hematocrit cohort.64
The patients who had high hematocrit levels in thatstudy received higher doses of erythropoietin andintravenous iron than did patients who had low he-matocrit levels. The link between iron stores andmorbidity or mortality rates is controversial, sinceit involves issues that are related to infections in pa-tients undergoing dialysis65 and detrimental coro-nary outcomes in men.66 An editorial67 concludedthat intravenous iron should be administered, ifnecessary, to improve the response to therapy withepoetin in order to reach a target hematocrit of 33 to36 percent in patients with chronic kidney disease.62
Careful studies of the potentially harmful effects ofiron supplementation in patients with various formsof anemia of chronic disease are still needed.
Despite management guidelines, anemia ofchronic disease remains underrecognized and un-dertreated. In a study of 200,000 patients enrolledin a health maintenance organization between 1994and 1997, 23 percent of patients with chronic kid-ney disease had hematocrit levels under 30 percent,and only 30 percent of those with hematocrit levelsbelow the target were receiving treatment for ane-mia.9 It is important to note that anemia of chronicdisease, if marked, can be a reflection of a more pro-gressive underlying disease.3,4,6,49 Thus, the notionthat correction of anemia alone may improve theprognosis of other underlying chronic diseasessuch as cancer or inflammatory disease remains un-proven.
treatment optionsWhen possible, treatment of the underlying diseaseis the therapeutic approach of choice for anemia ofchronic disease.3-5 Improvement in hemoglobinlevels has been demonstrated, for example, in pa-tients with rheumatoid disease68 who were receiv-ing therapy with anti-TNF antibodies. In cases inwhich treating the underlying disease is not feasi-ble, alternative strategies are necessary (Table 4).
TransfusionBlood transfusions are widely used as a rapid andeffective therapeutic intervention. Transfusions are
treatment
Copyright © 2005 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at CAUL on March 16, 2010 .

n engl j med 352;10 www.nejm.org march 10, 2005
The new england journal of medicine
1018
particularly helpful in the context of either severeanemia (in which the hemoglobin is less than 8.0 gper deciliter) or life-threatening anemia (in whichthe hemoglobin is less than 6.5 g per deciliter), par-ticularly when the condition is aggravated by com-plications that involve bleeding. Blood-transfusiontherapy has been associated with increased survivalrates in anemic patients with myocardial infarc-tion,69 but transfusion itself has also been associ-ated with multiorgan failure and increased mortal-ity in patients who are in critical care.70 Whetherblood transfusions modulate the immune system,causing clinically relevant adverse effects, remainsundetermined.71 It is important to note that exist-ing guidelines for the management of anemia ofchronic disease in patients with cancer or chronickidney disease do not recommend long-term bloodtransfusion therapy in their management algo-rithms because of the risks associated with long-term transfusion, such as iron overload and sensi-tization to HLA antigens that may occur in patientsbefore renal transplantation.53-55
Iron TherapyOral iron is poorly absorbed because of the down-regulation of absorption in the duodenum.37,38 Onlya fraction of the absorbed iron will reach the sitesof erythropoiesis, owing to iron diversion mediat-ed by cytokines, which directs iron into the reticu-loendothelial system. In addition, iron therapy for
patients with anemia of chronic disease is contro-versial.72 Iron is an essential nutrient for prolifer-ating microorganisms, and the sequestration of ironfrom microorganisms or tumor cells into the retic-uloendothelial system is believed to be a potential-ly effective defense strategy to inhibit the growth ofpathogens.72 A study investigating measures topredict the risk of bacteremia among patientsundergoing hemodialysis who are receiving ironparenterally showed that patients with a transfer-rin saturation above 20 percent and ferritin levelsgreater than 100 ng per milliliter had a significantlyhigher risk of developing bacteremia,73 possibly atleast in part because of the fact that iron has an in-hibitory effect on cellular immune function that canbe traced back to down-regulation of interferon-g–mediated immune effector pathways.53 In addi-tion, iron therapy in a setting of long-term immuneactivation promotes the formation of highly toxichydroxyl radicals that can cause tissue damage andendothelial dysfunction and increase the risk ofacute cardiovascular events.65,66,72
On the other hand, iron therapy may confer ben-efit. By inhibiting the formation of TNF-a, iron ther-apy may reduce disease activity in rheumatoid ar-thritis or end-stage renal disease.74,75 Furthermore,patients with inflammatory bowel disease and ane-mia respond well to parenteral iron therapy, with anincrease in hemoglobin levels.15
In addition to possible absolute iron deficiencyaccompanying the anemia of chronic disease, func-tional iron deficiency develops under conditionsof intense erythropoiesis54,76 during therapy witherythropoietic agents, with a decrease in transferrinsaturation and ferritin to levels 50 to 75 percent be-low baseline.54,76 Parenteral iron has been demon-strated to enhance rates of response to therapy witherythropoietic agents in patients with cancer whoare undergoing chemotherapy77 and in patients un-dergoing dialysis.62
On the basis of current data,77 patients with ane-mia of chronic disease and absolute iron deficiencyshould receive supplemental iron therapy.14,62,63
Iron supplementation should also be considered forpatients who are unresponsive to therapy with eryth-ropoietic agents because of functional iron deficien-cy. In this setting, iron is more likely to be absorbedand utilized by the erythron rather than by patho-gens, as indicated by an increase in hemoglobinlevels without demonstrable infectious complica-tions.73,77 However, iron therapy is currently notrecommended for patients with anemia of chronic
* This treatment is for the short-term correction of severe or life-threatening anemia. Potentially adverse immunomodulatory effects of blood transfusions are controversial.
† Although iron therapy is indicated for the correction of anemia of chronic dis-ease in association with absolute iron deficiency, no data from prospective studies are available on the effects of iron therapy on the course of underlying chronic disease.
‡ Overcorrection of anemia (hemoglobin >12 g per deciliter) may be potentially harmful to patients; the clinical significance of erythropoietin-receptor expres-sion on certain tumor cells needs to be investigated.
Table 4. Therapeutic Options for the Treatment of Patients with Anemiaof Chronic Disease.
TreatmentAnemia of Chronic
DiseaseAnemia of Chronic Diseasewith True Iron Deficiency
Treatment of underlying disease
Yes Yes
Transfusions* Yes Yes
Iron supplementation No Yes†
Erythropoietic agents Yes‡ Yes, in patients who do not have a response to iron therapy
Copyright © 2005 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at CAUL on March 16, 2010 .

n engl j med 352;10 www.nejm.org march 10, 2005
medical progress
1019
disease who have a high or normal ferritin level(above 100 ng per milliliter), owing to possible ad-verse outcomes in this setting.53,65,66,72,78,79
Erythropoietic AgentsErythropoietic agents for patients with anemia ofchronic disease are currently approved for use bypatients with cancer who are undergoing chemo-therapy, patients with chronic kidney disease, andpatients with HIV infection who are undergoingmyelosuppressive therapy. The percentage of pa-tients with anemia of chronic disease who respondto therapy with erythropoietic agents is 25 percent inmyelodysplastic syndromes,80 80 percent in multi-ple myeloma,81 and up to 95 percent in rheumatoidarthritis and chronic kidney disease.62 The thera-peutic effect involves counteracting the antiprolif-erative effects of cytokines,46,49 along with the stim-ulation of iron uptake and heme biosynthesis inerythroid progenitor cells.3 Accordingly, a poor re-sponse to treatment with erythropoietic agents isassociated with increased levels of proinflammato-ry cytokines, on the one hand, and poor iron avail-ability, on the other hand.13,76,82
Three erythropoietic agents are currently avail-able — epoetin alfa, epoetin beta, and darbepoetinalfa, which differ in terms of their pharmacologiccompounding modifications, receptor-binding af-finity, and serum half-life, thus allowing for alter-native dosing and scheduling strategies.83 Concernwas recently aroused by the identification of 191epoetin-associated cases of pure red-cell aplasia be-tween 1998 and 2004, as compared with only 3 suchcases between 1988 and 1998.84 The estimated ex-posure-adjusted incidence was 18 cases per 100,000patient-years for the formulation of epoetin alfa inEprex (Janssen-Cilag) without human serum albu-min, 6 cases per 100,000 patient-years for the Eprexformulation with serum albumin, 1 case per 100,000patient-years for epoetin beta, and 0.2 case per100,000 patient-years for the formulation of epoe-tin alfa in Epogen (Amgen). After procedures wereadopted to ensure appropriate storage, handling,and administration of Eprex to patients with chron-ic kidney disease, the exposure-adjusted incidencedecreased by 83 percent worldwide.
Although the positive short-term effects of ther-apy with erythropoietic agents on the correction ofanemia and avoidance of blood transfusions are welldocumented,14,60,76 few data are available on pos-sible effects on the course of underlying disease,particularly since epoetin can exert additional bio-
logic effects, including interference with the signal-transduction cascade of cytokines.45 For example,the long-term administration of epoetin has beenreported to decrease levels of TNF-a in patients withchronic kidney disease81; reportedly, those who re-sponded well to epoetin therapy had a significantlyhigher level of expression of CD28 on T cells andlower levels of interleukin-10, interleukin-12, in-terferon-g, and TNF-a than did those with a poorresponse.85 Such antiinflammatory effects mightbe of benefit in certain diseases such as rheumatoidarthritis, a disease in which combined treatmentwith epoetin and iron not only increased hemoglo-bin levels but also resulted in a reduction of diseaseactivity.74
In addition, erythropoietin receptors are foundon several malignant cell lines, including mamma-ry, ovarian, uterine, prostate, hepatocellular, and re-nal carcinomas, as well as on myeloid cell lines.86-88
However, there are contradictory reports concern-ing the effects of treatment with epoetin on suchcells. Although the drug led to tumor regression ina murine model of myeloma,89 administration toerythropoietin-receptor–expressing human renal-carcinoma cells in vitro stimulated their prolifera-tion.90 High amounts of erythropoietin receptorsare found in 90 percent of biopsies from humanbreast carcinomas.91 The production of erythropoi-etin receptors by cancer cells appears to be regulat-ed by hypoxia, and in clinical cancer specimens thehighest levels of erythropoietin receptors were as-sociated with neoangiogenesis, tumor hypoxia, andinfiltrating tumors.88,91 Potentially adverse effectsmay be due to induction of neoangiogenesis by thehormone, since erythropoietin increases inflamma-tion and ischemia-induced neovascularization byenhancing the mobilization of endothelial pro-genitor cells.92 Implantation of erythropoietin-receptor–expressing cell lines into nude mice withsubsequent inhibition of erythropoietin-receptorsignaling resulted in inhibition of angiogenesis anddestruction of tumor masses.87
A recent study investigating the effect of therapywith epoetin on the clinical course of patients withmetastatic breast carcinoma was discontinued be-cause of a trend toward higher mortality among pa-tients receiving the drug.93 Controversy concerningthe use of epoetin in patients with cancer who haveanemia of chronic disease has also arisen in twostudies involving patients with head and neck tu-mors. In one study, the increase in hemoglobin lev-els with epoetin therapy was associated with a
Copyright © 2005 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at CAUL on March 16, 2010 .
n engl j med 352;10 www.nejm.org march 10, 2005
The new england journal of medicine
1020
favorable clinical outcome, improved tumor oxy-genation, and increased susceptibility of tumorsto preoperative chemoradiation therapy.94 In con-trast, a double-blind prospective study investigat-ing whether target hemoglobin levels greater than13 g per deciliter for women and greater than 14 gper deciliter for men improved regional tumor con-trol among patients undergoing radiation therapyfor squamous-cell carcinoma of the head or neckshowed a recurrence rate among patients who weretreated with epoetin that was higher than thatamong patients treated with placebo.95
Current findings indicate that for patients receiv-ing erythropoietic agents, target hemoglobin levelsshould be 11 to 12 g per deciliter.14,62,63 Overcor-rection of anemia to normal hemoglobin levels95
and insufficient treatment64 have each been associ-ated with unfavorable clinical courses.
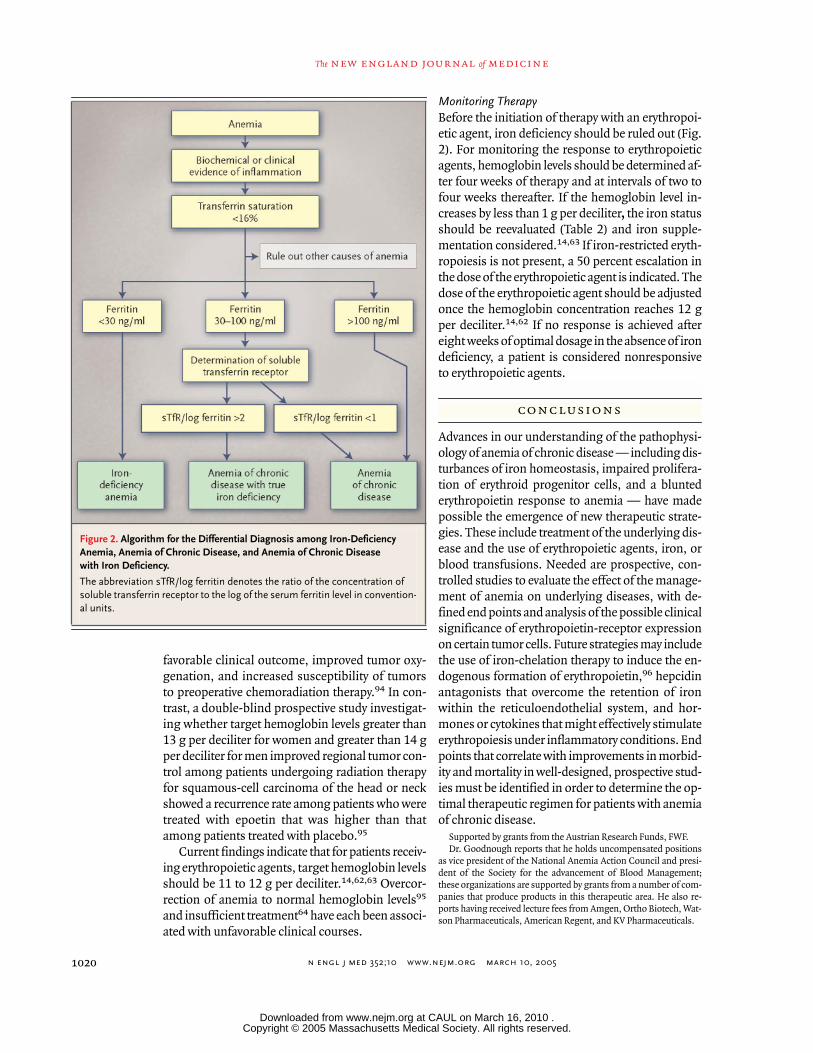
Monitoring TherapyBefore the initiation of therapy with an erythropoi-etic agent, iron deficiency should be ruled out (Fig.2). For monitoring the response to erythropoieticagents, hemoglobin levels should be determined af-ter four weeks of therapy and at intervals of two tofour weeks thereafter. If the hemoglobin level in-creases by less than 1 g per deciliter, the iron statusshould be reevaluated (Table 2) and iron supple-mentation considered.14,63 If iron-restricted eryth-ropoiesis is not present, a 50 percent escalation inthe dose of the erythropoietic agent is indicated. Thedose of the erythropoietic agent should be adjustedonce the hemoglobin concentration reaches 12 gper deciliter.14,62 If no response is achieved aftereight weeks of optimal dosage in the absence of irondeficiency, a patient is considered nonresponsiveto erythropoietic agents.
Advances in our understanding of the pathophysi-ology of anemia of chronic disease — including dis-turbances of iron homeostasis, impaired prolifera-tion of erythroid progenitor cells, and a bluntederythropoietin response to anemia — have madepossible the emergence of new therapeutic strate-gies. These include treatment of the underlying dis-ease and the use of erythropoietic agents, iron, orblood transfusions. Needed are prospective, con-trolled studies to evaluate the effect of the manage-ment of anemia on underlying diseases, with de-fined end points and analysis of the possible clinicalsignificance of erythropoietin-receptor expressionon certain tumor cells. Future strategies may includethe use of iron-chelation therapy to induce the en-dogenous formation of erythropoietin,96 hepcidinantagonists that overcome the retention of ironwithin the reticuloendothelial system, and hor-mones or cytokines that might effectively stimulateerythropoiesis under inflammatory conditions. Endpoints that correlate with improvements in morbid-ity and mortality in well-designed, prospective stud-ies must be identified in order to determine the op-timal therapeutic regimen for patients with anemiaof chronic disease.
Supported by grants from the Austrian Research Funds, FWF.Dr. Goodnough reports that he holds uncompensated positions
as vice president of the National Anemia Action Council and presi-dent of the Society for the advancement of Blood Management;these organizations are supported by grants from a number of com-panies that produce products in this therapeutic area. He also re-ports having received lecture fees from Amgen, Ortho Biotech, Wat-son Pharmaceuticals, American Regent, and KV Pharmaceuticals.
conclusions
Figure 2. Algorithm for the Differential Diagnosis among Iron-Deficiency Anemia, Anemia of Chronic Disease, and Anemia of Chronic Disease with Iron Deficiency.
The abbreviation sTfR/log ferritin denotes the ratio of the concentration of soluble transferrin receptor to the log of the serum ferritin level in convention-al units.
Copyright © 2005 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at CAUL on March 16, 2010 .

n engl j med 352;10 www.nejm.org march 10, 2005
medical progress
1021
references
1. Cartwright GE. The anemia of chronicdisorders. Semin Hematol 1966;3:351-75.2. Matzner Y, Levy S, Grossowicz N, IzakG, Hershko C. Prevalence and causes of ane-mia in elderly hospitalized patients. Geron-tology 1979;25:113-9.3. Weiss G. Pathogenesis and treatment ofanaemia of chronic disease. Blood Rev2002;16:87-96.4. Means RT Jr. Recent developments inthe anemia of chronic disease. Curr Hema-tol Rep 2003;2:116-21.5. Maury CP, Liljestrom M, Laiho K, Tiitin-en S, Kaarela K, Hurme M. Tumor necrosisfactor alpha, its soluble receptor I, and -308gene promoter polymorphism in patientswith rheumatoid arthritis with or withoutamyloidosis: implications for the pathogen-esis of nephropathy and anemia of chronicdisease in reactive amyloidosis. ArthritisRheum 2003;48:3068-76.6. Denz H, Huber P, Landmann R, Orth B,Wachter H, Fuchs D. Association betweenthe activation of macrophages, changes ofiron metabolism and the degree of anaemiain patients with malignant disorders. Eur JHaematol 1992;48:244-8.7. Guralnik JM, Eisenstaedt RS, Ferrucci L,Klein HG, Woodman RC. The prevalence ofanemia in persons age 65 and older in theUnited States: evidence for a high rate of un-explained anemia. Blood 2004;104:2263-8.8. Sullivan PS, Hanson DL, Chu SY, JonesJL, Ward JW. Epidemiology of anemia in hu-man immunodeficiency virus (HIV)-infect-ed persons: results from the multistate adultand adolescent spectrum of HIV disease sur-veillance project. Blood 1998;91:301-8.9. Nissenson AR, Goodnough LT, DuboisRW. Anemia: not just an innocent bystand-er? Arch Intern Med 2003;163:1400-4. [Er-ratum, Arch Intern Med 2003;163:1820.]10. van Iperen CE, van de Wiel A, Marx JJ.Acute event-related anaemia. Br J Haematol2001;115:739-43.11. Dunn A, Carter J, Carter H. Anemia atthe end of life: prevalence, significance, andcauses in patients receiving palliative care.J Pain Symptom Manage 2003;26:1132-9.12. Harrison L, Shasha D, Shiaova L, WhiteC, Ramdeen B, Portenoy R. Prevalence ofanemia in cancer patients undergoing radia-tion therapy. Semin Oncol 2001;28:54-9.13. Ludwig H, Fritz E, Leitgeb C, Pecher-storfer M, Samonigg H, Schuster J. Predic-tion of response to erythropoietin treatmentin chronic anemia of cancer. Blood 1994;84:1056-63.14. Rizzo JD, Lichtin AE, Woolf SH, et al.Use of epoetin in patients with cancer: evi-dence-based clinical practice guidelines ofthe American Society of Clinical Oncologyand the American Society of Hematology.J Clin Oncol 2002;20:4083-107.15. Gasche C, Waldhoer T, Feichtenschlag-er T, et al. Prediction of response to iron su-crose in inflammatory bowel disease-asso-
ciated anemia. Am J Gastroenterol 2001;96:2382-7.16. Wilson A, Reyes E, Ofman J. Prevalenceand outcomes of anemia in inflammatorybowel disease: a systematic review of the lit-erature. Am J Med 2004;116:Suppl 7A:44S-49S.17. Muller HM, Horina JH, Kniepeiss D, etal. Characteristics and clinical relevance ofchronic anemia in adult heart transplant re-cipients. Clin Transplant 2001;15:343-8.18. Frost AE, Keller CA. Anemia and eryth-ropoietin levels in recipients of solid organtransplants. Transplantation 1993;56:1008-11.19. Maheshwari A, Mishra R, Thuluvath PJ.Post-liver-transplant anemia: etiology andmanagement. Liver Transpl 2004;10:165-73.20. Collins AJ, Li S, St Peter W, et al. Death,hospitalization, and economic associationsamong incident hemodialysis patients withhematocrit values of 36 to 39%. J Am SocNephrol 2001;12:2465-73.21. Locatelli F, Pisoni RL, Combe C, et al.Anaemia in haemodialysis patients of fiveEuropean countries: association with mor-bidity and mortality in the Dialysis Out-comes and Practice Patterns Study (DOPPS).Nephrol Dial Transplant 2004;19:121-32.[Erratum, Nephron Dial Transplant 2004;19:1666.]22. Stenvinkel P. The role of inflammationin the anaemia of end-stage renal disease.Nephrol Dial Transplant 2001;16:Suppl 7:36-40.23. Yap GS, Stevenson MM. Inhibition of invitro erythropoiesis by soluble mediators inPlasmodium chabaudi AS malaria: lack of amajor role for interleukin 1, tumor necrosisfactor alpha, and gamma interferon. InfectImmun 1994;62:357-62.24. Gordeuk VR, Delanghe JR, LangloisMR, Boelaert JR. Iron status and the out-come of HIV infection: an overview. J ClinVirol 2001;20:111-5.25. Rodriguez RM, Corwin HL, GettingerA, Corwin MJ, Gubler D, Pearl RG. Nutri-tional deficiencies and blunted erythropoi-etin response as causes of the anemia of crit-ical illness. J Crit Care 2001;16:36-41.26. Groopman JE, Itri LM. Chemotherapy-induced anemia in adults: incidence andtreatment. J Natl Cancer Inst 1999;91:1616-34. [Erratum, J Natl Cancer Inst 2000;92:497.]27. Eschbach JW. Anemia management inchronic kidney disease: role of factors af-fecting epoetin responsiveness. J Am SocNephrol 2002;13:1412-4.28. Alvarez-Hernandez X, Liceaga J, McKayIC, Brock JH. Induction of hypoferremia andmodulation of macrophage iron metabo-lism by tumor necrosis factor. Lab Invest1989;61:319-22.29. Torti FM, Torti SV. Regulation of ferritingenes and protein. Blood 2002;99:3505-16.
30. Moura E, Noordermeer MA, VerhoevenN, Verheul AF, Marx JJ. Iron release from hu-man monocytes after erythrophagocytosisin vitro: an investigation in normal subjectsand hereditary hemochromatosis patients.Blood 1998;92:2511-9.31. Andrews NC. The iron transporterDMT1. Int J Biochem Cell Biol 1999;31:991-4.32. Ludwiczek S, Aigner E, Theurl I, WeissG. Cytokine-mediated regulation of irontransport in human monocytic cells. Blood2003;101:4148-54.33. Pietrangelo A. Physiology of iron trans-port and the hemochromatosis gene. Am JPhysiol Gastrointest Liver Physiol 2002;282:G403-G414.34. Tilg H, Ulmer H, Kaser A, Weiss G. Roleof IL-10 for induction of anemia during in-flammation. J Immunol 2002;169:2204-9.35. Nemeth E, Rivera S, Gabayan V, et al.IL-6 mediates hypoferremia of inflamma-tion by inducing the synthesis of the ironregulatory hormone hepcidin. J Clin Invest2004;113:1271-6.36. Nicolas G, Bennoun M, Porteu A, et al.Severe iron deficiency anemia in transgenicmice expressing liver hepcidin. Proc NatlAcad Sci U S A 2002;99:4596-601.37. Laftah AH, Ramesh B, Simpson RJ, et al.Effect of hepcidin on intestinal iron absorp-tion in mice. Blood 2004;103:3940-4.38. Andrews NC. Anemia of inflammation:the cytokine-hepcidin link. J Clin Invest2004;113:1251-3.39. Papanikolaou G, Samuels ME, LudwigEH, et al. Mutations in HFE2 cause ironoverload in chromosome 1q-linked juvenilehemochromatosis. Nat Genet 2004;36:77-82.40. Wang CQ, Udupa KB, Lipschitz DA. In-terferon-gamma exerts its negative regula-tory effect primarily on the earliest stages ofmurine erythroid progenitor cell develop-ment. J Cell Physiol 1995;162:134-8.41. Taniguchi S, Dai CH, Price JO, KrantzSB. Interferon gamma downregulates stemcell factor and erythropoietin receptors butnot insulin-like growth factor-I receptors inhuman erythroid colony-forming cells.Blood 1997;90:2244-52.42. Maciejewski JP, Selleri C, Sato T, et al.Nitric oxide suppression of human hemato-poiesis in vitro: contribution to inhibitoryaction of interferon-gamma and tumor ne-crosis factor-alpha. J Clin Invest 1995;96:1085-92.43. Miller CB, Jones RJ, Piantadosi S, Abe-loff MD, Spivak JL. Decreased erythropoi-etin response in patients with the anemia ofcancer. N Engl J Med 1990;322:1689-92.44. Cazzola M, Ponchio L, de Benedetti F, etal. Defective iron supply for erythropoiesisand adequate endogenous erythropoietinproduction in the anemia associated withsystemic-onset juvenile chronic arthritis.Blood 1996;87:4824-30.
Copyright © 2005 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at CAUL on March 16, 2010 .

n engl j med 352;10 www.nejm.org march 10, 2005
The new england journal of medicine
1022
45. Jelkmann W. Proinflammatory cyto-kines lowering erythropoietin production.J Interferon Cytokine Res 1998;18:555-9.46. Means RT Jr, Krantz SB. Inhibition ofhuman erythroid colony-forming units bygamma interferon can be corrected by re-combinant human erythropoietin. Blood1991;78:2564-7.47. Minoo P, Zadeh MM, Rottapel R, LebrunJJ, Ali S. A novel SHP-1/Grb2-dependentmechanism of negative regulation of cyto-kine-receptor signaling: contribution ofSHP-1 C-terminal tyrosines in cytokine sig-naling. Blood 2004;103:1398-407.48. Moldawer LL, Marano MA, Wei H, et al.Cachectin/tumor necrosis factor-alpha al-ters red blood cell kinetics and induces ane-mia in vivo. FASEB J 1989;3:1637-43.49. Spivak JL. Iron and the anemia of chron-ic disease. Oncology (Huntingt) 2002;16:Suppl 10:25-33.50. Lipschitz DA, Cook JD, Finch CA. A clin-ical evaluation of serum ferritin as an indexof iron stores. N Engl J Med 1974;290:1213-6.51. Mast AE, Blinder MA, Gronowski AM,Chumley C, Scott MG. Clinical utility of thesoluble transferrin receptor and compari-son with serum ferritin in several popula-tions. Clin Chem 1998;44:45-51.52. Punnonen K, Irjala K, Rajamaki A. Se-rum transferrin receptor and its ratio to se-rum ferritin in the diagnosis of iron defi-ciency. Blood 1997;89:1052-7.53. Weiss G. Iron and immunity: a double-edged sword. Eur J Clin Invest 2002;32:Suppl 1:70-8.54. Brugnara C. Iron deficiency and eryth-ropoiesis: new diagnostic approaches. ClinChem 2003;49:1573-8.55. Beguin Y, Clemons GK, Pootrakul P, Fil-let G. Quantitative assessment of erythro-poiesis and functional classification of ane-mia based on measurements of serumtransferrin receptor and erythropoietin.Blood 1993;81:1067-76.56. Barosi G. Inadequate erythropoietin re-sponse to anemia: definition and clinicalrelevance. Ann Hematol 1994;68:215-23.57. Henry D, Abels R, Larholt K. Predictionof response to recombinant human erythro-poietin (r-HuEPO/epoetin-alpha) therapy incancer patients. Blood 1995;85:1676-8.58. Murphy ST, Parfrey PS. The impact ofanemia correction on cardiovascular diseasein end-stage renal disease. Semin Nephrol2000;20:350-5.59. Moreno F, Sanz-Guajardo D, Lopez-Gomez JM, Jofre R, Valderrabano F. Increas-ing the hematocrit has a beneficial effect onquality of life and is safe in selected hemodi-alysis patients: Spanish Cooperative RenalPatients Quality of Life Study Group of theSpanish Society of Nephrology. J Am SocNephrol 2000;11:335-42.60. Littlewood TJ, Bajetta E, Nortier JW, Ver-cammen E, Rapoport B. Effects of epoetinalfa on hematologic parameters and qualityof life in cancer patients receiving nonplati-
num chemotherapy: results of a random-ized, double-blind, placebo-controlled trial.J Clin Oncol 2001;19:2865-74.61. Ma JZ, Ebben J, Xia H, Collins AJ. Hema-tocrit level and associated mortality in he-modialysis patients. J Am Soc Nephrol1999;10:610-9.62. NKF-K/DOQI Clinical Practice Guide-lines for anemia of chronic kidney disease:update 2000. Am J Kidney Dis 2001;37:Suppl 1:S182-S238. [Erratum, Am J KidneyDis 2001;38:442.]63. Winn RJ. The NCCN guidelines devel-opment process and infrastructure. Oncolo-gy (Huntingt) 2000;14:26-30.64. Besarab A, Bolton WK, Browne JK, et al.The effects of normal as compared with lowhematocrit values in patients with cardiacdisease who are receiving hemodialysis andepoetin. N Engl J Med 1998;339:584-90.65. Kletzmayr J, Sunder-Plassmann G, HorlWH. High dose intravenous iron: a note ofcaution. Nephrol Dial Transplant 2002;17:962-5.66. Sullivan JL. Iron therapy and cardiovas-cular disease. Kidney Int Suppl 1999;69:S135-S137.67. Adamson JW, Eschbach JW. Erythropoi-etin for end-stage renal disease. N Engl JMed 1998;339:625-7.68. Moreland LW, Baumgartner SW, SchiffMH, et al. Treatment of rheumatoid arthritiswith a recombinant human tumor necrosisfactor receptor (p75)-Fc fusion protein.N Engl J Med 1997;337:141-7.69. Goodnough LT, Bach RG. Anemia,transfusion, and mortality. N Engl J Med2001;345:1272-4.70. Vincent JL, Baron JF, Reinhart K, et al.Anemia and blood transfusion in critically illpatients. JAMA 2002;288:1499-507.71. Vamvakas EC, Blajchman MA. Deleteri-ous clinical effects of transfusion-associat-ed immunomodulation: fact or fiction?Blood 2001;97:1180-95.72. Weinberg ED. Iron loading and diseasesurveillance. Emerg Infect Dis 1999;5:346-52.73. Teehan GS, Bahdouch D, Ruthazer R,Balakrishnan VS, Snydman DR, Jaber BL.Iron storage indices: novel predictors ofbacteremia in hemodialysis patients initiat-ing intravenous iron therapy. Clin Infect Dis2004;38:1090-4.74. Kaltwasser JP, Kessler U, Gottschalk R,Stucki G, Moller B. Effect of recombinanthuman erythropoietin and intravenous ironon anemia and disease activity in rheuma-toid arthritis. J Rheumatol 2001;28:2430-6.75. Weiss G, Meusburger E, Radacher G,Garimorth K, Neyer U, Mayer G. Effect ofiron treatment on circulating cytokine levelsin ESRD patients receiving recombinant hu-man erythropoietin. Kidney Int 2003;64:572-8.76. Goodnough LT, Skikne B, Brugnara C.Erythropoietin, iron, and erythropoiesis.Blood 2000;96:823-33.77. Auerbach M, Ballard H, Trout JR, et al.
Intravenous iron optimizes the response torecombinant human erythropoietin in can-cer patients with chemotherapy-related ane-mia: a multicenter, open-label, randomizedtrial. J Clin Oncol 2004;22:1301-7.78. Stevens RG, Jones DY, Micozzi MS, Tay-lor PR. Body iron stores and the risk of can-cer. N Engl J Med 1988;319:1047-52.79. Jiang R, Manson JE, Meigs JB, Ma J, RifaiN, Hu FB. Body iron stores in relation to riskof type 2 diabetes in apparently healthywomen. JAMA 2004;291:711-7.80. Thompson JA, Gilliland DG, Prchal JT,et al. Effect of recombinant human erythro-poietin combined with granulocyte/macro-phage colony-stimulating factor in the treat-ment of patients with myelodysplasticsyndrome. Blood 2000;95:1175-9.81. Ludwig H, Fritz E, Kotzmann H, HockerP, Gisslinger H, Barnas U. Erythropoietintreatment of anemia associated with multi-ple myeloma. N Engl J Med 1990;322:1693-9.82. Cooper AC, Mikhail A, Lethbridge MW,Kemeny DM, Macdougall IC. Increased ex-pression of erythropoiesis inhibiting cyto-kines (IFN-gamma, TNF-alpha, IL-10, andIL-13) by T cells in patients exhibiting a poorresponse to erythropoietin therapy. J Am SocNephrol 2003;14:1776-84.83. Cella D, Dobrez D, Glaspy J. Control ofcancer-related anemia with erythropoieticagents: a review of evidence for improvedquality of life and clinical outcomes. AnnOncol 2003;14:511-9.84. Bennett CL, Luminari S, Nissenson AR,et al. Pure red-cell aplasia and epoetin thera-py. N Engl J Med 2004;351:1403-8.85. Aguilera A, Bajo MA, Diez JJ, et al. Ef-fects of human recombinant erythropoietinon inflammatory status in peritoneal dialy-sis patients. Adv Perit Dial 2002;18:200-5.86. Arcasoy MO, Amin K, Karayal AF, et al.Functional significance of erythropoietin re-ceptor expression in breast cancer. Lab In-vest 2002;82:911-8.87. Yasuda Y, Fujita Y, Matsuo T, et al. Eryth-ropoietin regulates tumour growth of hu-man malignancies. Carcinogenesis 2003;24:1021-9. [Erratum, Carcinogenesis 2003;24:1567.]88. Acs G, Zhang PJ, McGrath CM, et al. Hy-poxia-inducible erythropoietin signaling insquamous dysplasia and squamous cell car-cinoma of the uterine cervix and its potentialrole in cervical carcinogenesis and tumorprogression. Am J Pathol 2003;162:1789-806.89. Mittelman M, Neumann D, Peled A,Kanter P, Haran-Ghera N. Erythropoietin in-duces tumor regression and antitumor im-mune responses in murine myeloma mod-els. Proc Natl Acad Sci U S A 2001;98:5181-6.90. Westenfelder C, Baranowski RL. Eryth-ropoietin stimulates proliferation of humanrenal carcinoma cells. Kidney Int 2000;58:647-57.91. Acs G, Acs P, Beckwith SM, et al. Eryth-ropoietin and erythropoietin receptor ex-
Copyright © 2005 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at CAUL on March 16, 2010 .

n engl j med 352;10 www.nejm.org march 10, 2005
medical progress
1023
pression in human cancer. Cancer Res 2001;61:3561-5.92. Heeschen C, Aicher A, Lehmann R, et al.Erythropoietin is a potent physiologic stim-ulus for endothelial progenitor cell mobili-zation. Blood 2003;102:1340-6. [Erratum,Blood 2004;103:4388.]93. Leyland-Jones B. Breast cancer trial witherythropoietin terminated unexpectedly.Lancet Oncol 2003;4:459-60.
94. Glaser CM, Millesi W, Kornek GV, et al.Impact of hemoglobin level and use of re-combinant erythropoietin on efficacy of pre-operative chemoradiation therapy for squa-mous cell carcinoma of the oral cavity andoropharynx. Int J Radiat Oncol Biol Phys2001;50:705-15.95. Henke M, Laszig R, Rube C, et al.Erythropoietin to treat head and neck cancerpatients with anaemia undergoing radiother-
apy: randomised, double-blind, placebo-controlled trial. Lancet 2003;362:1255-60.96. Salvarani C, Baricchi R, Lasagni D, et al.Effects of desferrioxamine therapy on chron-ic disease anemia associated with rheuma-toid arthritis. Rheumatol Int 1996;16:45-8.Copyright © 2005 Massachusetts Medical Society.
Copyright © 2005 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at CAUL on March 16, 2010 .