Embed Size (px)
Citation preview
Decision – Paper-Lite Implementation Plan 5-1
Status This report contains: For decision Update Regular report
For information
MEMO
To: Board Members
From: Patrick Ng, GM IT & Infrastructure
Date: 18 May 2016
Subject: DECISION: PAPER-LITE IMPLEMENTATION PLAN
Preface Early in 2015 the Board approved the proposed technology strategy for Nelson Marlborough Health (NMH). The strategy proposed focusing on the achievement of paper-lite outcomes in the first 5 years of the strategy to enable NMH to then progressively move towards digital hospitals and a digital health system in the next 5 year period. At the time the strategy was presented, we had a reasonably good understanding of what would be required to achieve paper-lite outcomes, but we noted that we would need to spend a year on further developing our knowledge, in order to clarify what would be required in a paper-lite implementation programme. Through dialogue with a number of the largest health software vendors operating in New Zealand (including Apple Health, CSC, MKM and Orion Health), a visit to two digital hospitals (one in Brisbane, Australia, and one at Jurong in Singapore) and dialogue with key members of the technology innovation team at Waitemata DHB (a likewise minded DHB), and through our ongoing scanning of our local environment as we prepare for the HCS and PICS implementations, we believe we now have a robust view of what our paper-lite programme should entail. We have also been giving consideration to the role that Patient Portals will need to play in a future paper-lite environment as well as the potential role of Tele-Health. We believe that Tele-Health should be the subject of a separate strategy, to be developed in the 2016-2017 financial year. Executive Summary
This paper clarifies the progress in our thinking and notes the investments that have either been made or requested since our paper-lite focused strategy was approved in early 2015. Our paper-lite strategy is based on an investment in core underlying regional infrastructure, notably the Patient Information and Care System (PICS), and the Health Connect South Clinical Portal (HCS). There have been challenges at a regional level in getting the PICS programme to deliver within timeframes, and a full update will be provided clarifying when we expect to go live with PICS for the June Board meeting. HCS has encountered a number of implementation challenges, causing us to miss our planned software delivery date of May. However, as noted later in this paper, a relatively large proportion of the project has now been delivered and we are becoming increasingly confident that we can achieve an end of August ‘go-live’ date. In the current financial year we have had several important paper-lite initiatives approved and have opened capital projects for these initiatives. They are dependent on the HCS implementation, but pre-planning activities have progressed in the meantime. These initiatives are e-Laboratory sign-off, e-Referral Triaging and work has also progressed on proposing a capital substitution for eRadiology Ordering and Sign-Off.
Decision – Paper-Lite Implementation Plan 5-2
We are also hoping to make initial decisions about mobility devices before the end of the financial year and to implement an initial suite of devices in support of paper-lite. In the coming financial year the items at the top of our Software Capital List all support Paper-Lite. These include Patientrack for digital bedside care, the digitisation of what were previously paper-based forms and the establishment of electronic workflow. eRadiology Ordering is also on our list as is the first of the eMedicines and ePharmacy initiatives, MedChart. Also in our coming financial year plan is an operating cost initiative to systematically replace paper medical charts and migrate their content into the electronic health record found in HCS. This paper provides context for how these initiatives will systematically transform our current paper-based environment to one which is paper-lite and digitally focused. In this paper we also clarify the role we see for master scheduling and patient portals in the future, both of which we believe need to be implemented in a manner that directly supports paper-lite. The appendix provides a diagrammatic explanation of how our paper-based processes become paper-lite under the proposed programme. Our next step is to prepare a timeline which shows the timing for the implementation of the proposed initiatives to achieve the paper-lite outcomes over the remaining 4 years of the initial paper-lite strategy’s timeframe. Whether this proves achievable is dependent on the availability of capital and the organisation’s ability to absorb change. The subsequent digital hospital and health system strategy could then be aligned to the construction of the re-developed Nelson Hospital. It is our hope that this paper provides clarity about the paper-lite programme’s implementation and that the Board agrees with the proposed direction signalled by this paper, noting that the speed with which the strategy is ultimately implemented will be dependent on the organisation’s ability to continue to provide capital for investment and also on the organisation’s ability to absorb change. Progress on the Foundational Software Platforms
The strategy noted that where possible, we would build our paper-lite capabilities on top of the regional software implementations that have been approved and for which capital projects are underway. The status of the regional projects is as follows: Health Connect South (HCS): In 2015 we identified a number of initial paper-lite implementations, made successful cases for these and secured capital funding. These initiatives are electronic laboratory sign-off, electronic referral triaging and process re-engineering within the Emergency Department. All but the Emergency Department re-engineering initiative are dependent on the successful implementation of HCS. HCS was initially slated for May of this year, but technical and resource challenges have delayed successful implementation and we now believe the project will ‘go-live’ at the end of August of this year. Despite the technical challenges, good progress has been made, as follows:
Decision – Paper-Lite Implementation Plan 5-3
HCS Progress to Date
All NMH clinicians who currently have access to Concerto now also have access to HCS. They can log into it and access a number of information sources they currently access in Concerto. For example, all radiology and laboratory results are now accessible in HCS. ED and Inpatient transactions are also accessible in HCS, including all historic transactions
The most significant and complex component of the project – the flow of legacy information from the patient administration system, Ora*Care, has largely been completed. This required the Ora*Care vendor to undertake development in Ora*Care to create a number of ‘triggers’ by which information could be extracted. Where triggers were not available output data had to be ‘transformed’ to make it suitable for consumption by the HCS integration engine (Rhapsody)
99% of the Concerto templates for documents have successfully been recreated in HCS.
Remaining challenges prior to HCS ‘go-live’: The remaining challenges are primarily related to the development of key ‘Referral’ and ‘Waitlist’ functionality by Orion Health. The functionality is unique to NMH clinicians, who have had the ability to access all information concerned with a patient through Concerto for some time now. Clinicians elsewhere in the South Island have had to utilise a number of systems to review this information. One of our principals for an HCS go-live has been that NMH clinicians would not see a backward step in functionality. This has necessitated the development of Referral and Waitlist functionality. The main challenges throughout the programme have included Orion Health’s ability to deliver effective solutions in respect of the functional requirements, availability and responsiveness of Canterbury District Health Board technical resources and our own local team having to solve the issues related to extracting data from our legacy Patient Administration System. The good news is that most of the legacy data issues have been resolved, and development of the referral and wait-listing functionality is now well underway. We believe the project is now about 80% complete, and the team is working hard towards getting the project completed by the end of August. As noted earlier, having HCS in place is a crucial foundation for many of our paper-lite initiatives. PICS Progress to Date There have been a number of challenges related to the software vendor’s ability to estimate development effort and deliver the regional solution. These issues are now starting to be addressed, as Orion Health have introduced more experienced software delivery resources. A recent ‘elaboration’ exercise suggested that December 2017 was a realistic date for NMH to receive its foundational software, however, this timeframe is unacceptably too far away, so we have reviewed the assumptions with Orion Health. It appears that a software drop that would provide a full replacement for Ora*Care could be provided to us by July of next year, with the additional foundational functionality then provided as subsequent software releases. We will provide a full update on PICS, together with recommendations, for the June Board meeting. Paper-Lite Programme Plan
With increasing confidence that the regional software programmes are closer to delivery, the constraints for the paper-lite programme will shift to being the amount of

Decision – Paper-Lite Implementation Plan 5-4
capital available from year to year, and the capacity of the organisation to adapt to change. We believe that we now have a paper-lite plan that encompasses most areas of secondary care delivery. The following programme plan and accompanying diagram provides a systematic explanation by major process area of what we propose the tools will be. Before providing this explanation, however, it is useful to spend a bit of time explaining what the health software vendors operating in New Zealand are planning. ‘NZ Inc.’ We were lucky enough to receive an invitation from the National Health IT Board to participate in several workshops to help them to shape what a ‘National Electronic Health Record’ would look like. During these workshops it became clear that local and regional electronic health record information was likely to be a richer set of information, and that a sub-set of this information was likely to roll-up nationally to be the national record. We also tested the value proposition of a national record and the proposition appears to be that a trusted national information set would provide software vendors with the confidence to build an approved set of applications, which could access a common data-set. A similar and important theme was announced by three key software vendors who work in the New Zealand Health System – Orion Health, CSC and MedTech. These vendors made an unprecedented announcement, stating that they would work collaboratively in response to the Ministry’s announcements concerning a national electronic health record. Previously, our experience (with Orion Health and CSC in particular) has been that they have very much acted like they are in competition with each other. The concept of collaboration was extended on further this year, when we were told by the new Orion Health In-Country Manager that Orion intended to develop a master database (Amadeus), and was working with the 28 most important names in New Zealand health software to allow them access to this database. This would also mean that vendors could all build their own applications off a common set of data. This concept is known as ‘open API’, ‘open architecture’, ‘open platform.’ Basically, it means that vendor’s products will work well with other vendor’s products. What does this mean for us? It means we can work with all of the vendors, choose a particular vendor solution for a particular need, and have growing confidence that the solution will work with the overall suite of products that we have in our environment. HCS and Patientrack working well together is a prime example, which we will explain further, below. Before explaining the product choices, it is also worth grouping the key aspects of secondary care for the purpose of explaining what purpose the respective products would serve, as follows:
Entry point to the hospital system. Either on the basis of a referral or through an ED presentation
Pre-admission or Outpatient activities. These are primarily clinics or appointments.
Admission and surgery
Bedside care, treatment and discharge
Post discharge care
Maintenance of paper medical charts
Delivery of care in the community.
Decision – Paper-Lite Implementation Plan 5-5
For community care, our initial areas of focus are district nursing, and the sharing of information with GP’s and Pharmacists. Entry into the Hospital The receipt of referrals is currently electronic, but they are processed as paper. Once HCS is implemented we will implement the ‘e-Triage’ project. We have capital approved for this project already and have started pre-planning. E-Triage is expected to take 12 months to implement. Completion of e-Triage will mean that referrals are received electronically in HCS, but will still need to be keyed into PICS. The referral will now be presented to clinicians electronically (rather than as stacks of paper) and they will triage the referral electronically. The referral outcome will then need to be re-keyed into PICS. We are using our regional influence to get the integration between HCS and PICS prioritised for future PICS functional releases. Once this is developed, it will mean that the systems will handshake the referral across and there will be no manual keying of information anywhere in the referral information flow. Key systems used in this set of processes are already paid for and include HCS, regional Electronic Referrals Management System (ERMS), Orion Health Referrals 4.0 and, in the future, PICS. The process by which ED presentations are managed and then admitted into the hospital if required is currently almost paper-lite due to our use of the locally built Emergency Department at a Glance (EDaaG) system. Further process work has been occurring in the ED over the last 12 months and we have managed to eliminate the automatic requesting of paper medical charts, and to replace paper-based processes with digital processes for the transmission of information from St John to our ED department. Investment required: None – e-Triage has already been budgeted and approved in FY 2015-2016. Pre-Admission and Outpatient Activities Pre-admission and outpatient activities largely evolve around clinics / appointments and are currently very paper-based. For example, the patient is required to complete a 7 page paper booklet of information for a pre-admission clinic. Although we had some paper-lite capital available for pre-admissions in FY 2015-2016 we envisage rolling this into a major initiative we want to make a case for in FY 2016-2017. Tools we believe would provide paper-lite outcomes in this area are ‘Patientrack’ by MKM, and potentially a master scheduling tool called ‘Ultra-Genda’ by CSC. The Orion Health Clinical Workflow Suite (CWS) could also deliver value in this area. We plan to work out the best solution by completing an overall evaluation of how Patientrack could automate the workflow and make the Pre-Admission booklet a digital form. Investment required: Patientrack (on the FY ’16-17 CAPEX plan), potentially Ultra-Genda, and potentially some aspects of Clinical Workflow Suite. Admission and Surgery
PICS, once implemented, will provide an improved patient administration tool, when compared to Ora*Care today. However, the theatre module that was to be supplied with PICS will not be available for some time. This means that we must extend the life of the $35k Theatre Management System (TMS) which we developed in house two years ago. Discussions are now underway with the CEO to increase the level of investment in this
Decision – Paper-Lite Implementation Plan 5-6
tool to enhance reporting outcomes whilst we wait for the PICS theatre management module. Investment required: Minor enhancements to TMS. Bedside Care, Treatment and Discharge Bedside care is currently very paper-based. This includes bedside observations, collection of early warning scores, medicine recording, dispensing and so on. We believe the implementation of Patientrack, MedChart and eventually the implementation of the full suite of four eMedicines and ePharmacy initiatives, will make the whole bedside care process paper-lite and eventually paperless. Investment is simultaneously required in enhancements to the WIFI and in portable devices (we have seen i-Pad minis used successfully at Waitemata DHB). Patientrack will allow bedside observations to be captured digitally. MedChart will enable the dispensing of medicines to refer to electronic charts. In addition, Orion Health are developing a toolset called ‘Clinical Companion’ that would enable doctors to view key health record information on their smartphone and set simple tasks. Orion Health have asked us (NMH) to work with them to trial Clinical Companion. This is an area where we see the simultaneous use of several tools, ie Patientrack for observations / early warning scores, MedChart for medicine dispensing and Clinical Companion for the duty doctor. It is useful to note that Orion Health are currently in the process of integrating Patientrack into HCS at the request of CDHB. It should be noted that the digital hospital we visited in Brisbane showed us what would be possible for medicine dispensing, and that the four eMedicines / ePharmacy initiatives being planned for the region are still some way off from achieving full digital hospital outcomes, even once fully implemented (none of the South Island DHBs have implemented the full suite of initiatives yet). At St Stephens Hospital in Brisbane, pharmaceuticals coming into the hospital are removed from their packaging and are re-packaged and bar-coded as single doses, using a machine. The single doses are then distributed to a dispensing trolley (computer on wheels, COW) which the nurse pushes into the ward. The nurse scans the patient’s admission tag on their wrist, scans the barcode on the medication and these are matched in the electronic health record on the computer screen on her trolley. Assuming there is a match, a record is made. If there is an error, an error flashes up. This is a highly effective closed loop medication system which would produce extremely low rates of error, and we will aspire to this standard once the four eMedicine / ePharmacy initiatives are in place and giving us our initial paper-lite outcomes. Investment required: Clinical Companion will be free. It is built into HCS licencing. Investment in Patientrack will be required. This is on the FY ’16-’17 capital list. Investment in MedChart will be required. This is also on the FY ’16-’17 capital list. Future investments in the eMedicines, ePharmacy initiatives will be required. Investment in handheld devices and enhancements to the existing WIFI will also be required. These are on the FY ’15-’16 capital list and we plan to make the case for an initial suite of devices (or roll over the capital) soon. Post Discharge Care The coordination of care once a patient has been discharged is often challenging and has the potential for tasks to get missed (eg ACC follow up, district nursing visits or

Decision – Paper-Lite Implementation Plan 5-7
supply of Allied Health equipment). Orion Health have identified this as an area where further value could be added if their tools were enhanced to cope with the challenges of delivering post-discharge care. We also believe that Patientrack has the potential to automate workflow in this area, and Ultra-Genda could play a key part here too. Investment required: Patientrack and possibly an investment in Ultra-Genda. Maintenance of Paper Medical Charts Currently we have a very paper-based and very manual way of maintaining paper medical charts. This is similar for most hospitals in New Zealand, although Auckland has taken the step of simply turning their paper medical charts into a single PDF document that is accessed in place of the paper medical chart. Our proposal with paper medical charts is to systematically transform medical charts in our hospital environment. We will do this through the following steps:
Analyse all paper medical charts. Determine which are unlikely to be referenced again. Place these in archive storage with a just in time process to return these digitally
For those charts likely to be frequented, work through the chart and eliminate the 40% that is a duplication of the electronic health record (Concerto, soon to be HCS).
For the remaining content, index the content carefully and scan it. The scanned document can then be applied to the right part of the electronic health record through application of the index code
Discard paper medical charts that have been through this process and tag the patient’s electronic record to note that all medical chart information is now only available electronically.
Through the FY 2016-2017 budget process we have received tentative approval to initiate what will be a 2 year programme to achieve this transformation. The programme has a strong financial payback, particularly beyond the first year, as we systematically reduce the effort involved in maintaining and distributing paper medical charts. Future Considerations – Master Scheduling and Patient Self-Service We have been thinking carefully about the role of master scheduling and the role of the consumer in the management of their secondary health care. CDHB have licences for a product called ‘Ultra-Genda’. This product is a master scheduling tool provided by CSC that works with patient administration systems and other systems (e.g. radiology information systems) to surface master schedules to facilitate the booking of appointments in a cohesive manner. Master scheduling means that the tool (Ultra-Genda) acts as the overall schedule manager for all presentations (e.g. clinics, radiology appointments) that the patient is required to make as they progress through our hospital system. We have had initial conversations with CSC, who have collaborated with Orion Health overseas to integrate their tool with Orion Health products. Following the open architecture principles that are being agreed upon by the major Health Software vendors (as noted earlier), we believe there is the potential to implement Ultra-Genda in a complementary way with the other core systems, which are primarily supplied by Orion Health. We are further hoping to partner with CSC, who are very keen to have an Australasian customer implement Ultra-Genda and become a reference-able client. It is

Decision – Paper-Lite Implementation Plan 5-8
our hope that we may be able to reach a deal that would see us implement Ultra-Genda at a very low cost in exchange for being a fully reference-able client for the product. What benefits would Ultra-Genda provide? Ultra-Genda allows scheduling to be planned from an end to end perspective. Patients can then be tracked along that journey and reported on. This means that filling clinics etc can be better planned based on the upstream demands and the downstream capacity to meet demand. We further believe that a master scheduler, when used well in conjunction with a patient portal, would allow patients to better manage their own appointments by self-booking into available clinic spaces. This has the potential to significantly improve the convenience for patients, and to reduce the rate of non-attendances or re-scheduled appointments. Using Ultra-Genda as the master scheduling tool would mean that it becomes the master and that the clinic lists and schedules in PICS become the slave which supports the master. We believe that Orion Health and CSC have worked successfully in this manner in other countries, and that utilising the ‘out of the box’ Ultra-Genda solution in preference to further customisation of PICS will ultimately be a lower cost way of achieving the outcomes that we need.
At this stage we are still to formerly evaluate Ultra-Genda. However, we do want to note its potential. A Note on Community Based Care
We believe that an opportunity exists to transform the manner in which District Nursing delivers community based care. Currently, their workflow and tasks are managed with paper-based files, and key information is not available to them electronically as they dispense care in the home. Utilising tablets, combined with a mobile version of Health Connect South, and utilising Patientrack as the workflow tool, the delivery of this service could be transformed from paper-based to electronic. After the initial suite of Patientrack cases we hope to build a case that would utilise Patientrack to achieve this transformation for District Nursing, too. Investment required: Mobile devices, Patientrack. Please refer to Appendix 1 for a diagrammatic explanation of where the applications referred to in the above themes fit within our health care eco-system. An Associated Theme – Tele-Health We believe that a Tele-Health strategy is an important and complementary strategy to have. Whilst a Tele-Health strategy is more about change management / changes to work practices than about technology, the ability to engage patients through remote consultations has the potential to enhance processes, optimise resource use and improve convenience for patients in a manner that is highly complementary to the intended outcomes of the paper-lite programme. The Chief Information Officer (CIO) under the new structure will be tasked with developing a complementary Tele-Health strategy for consideration.
Patrick Ng
Decision – Paper-Lite Implementation Plan 5-9
GM IT & Infrastructure RECOMMENDATIONS: THAT THE BOARD: 1. NOTES HOW THE INVESTMENT CHOICES WE ARE PROPOSING ALIGN
WITH MOVING THE OVERALL NMH ECO-SYSTEM FROM BEING PAPER INTENSIVE TO BEING PAPER-LITE THROUGH THE SYSTEMATIC IMPLEMENTATION OF THE NMH PAPER-LITE IMPLEMENTATION PLAN.
2. APPROVES THE PAPER-LITE DIRECTION BEING TAKEN, NOTING THAT
INVESTMENT IN THE PROGRAMME REMAINS DEPENDENT ON AVAILABLE CAPITAL AND THAT EACH INITIATIVE MUST BE SUCCESSFULLY BUSINESS CASED AND APPROVED.
Decision – Paper-Lite Implementation Plan 5-10
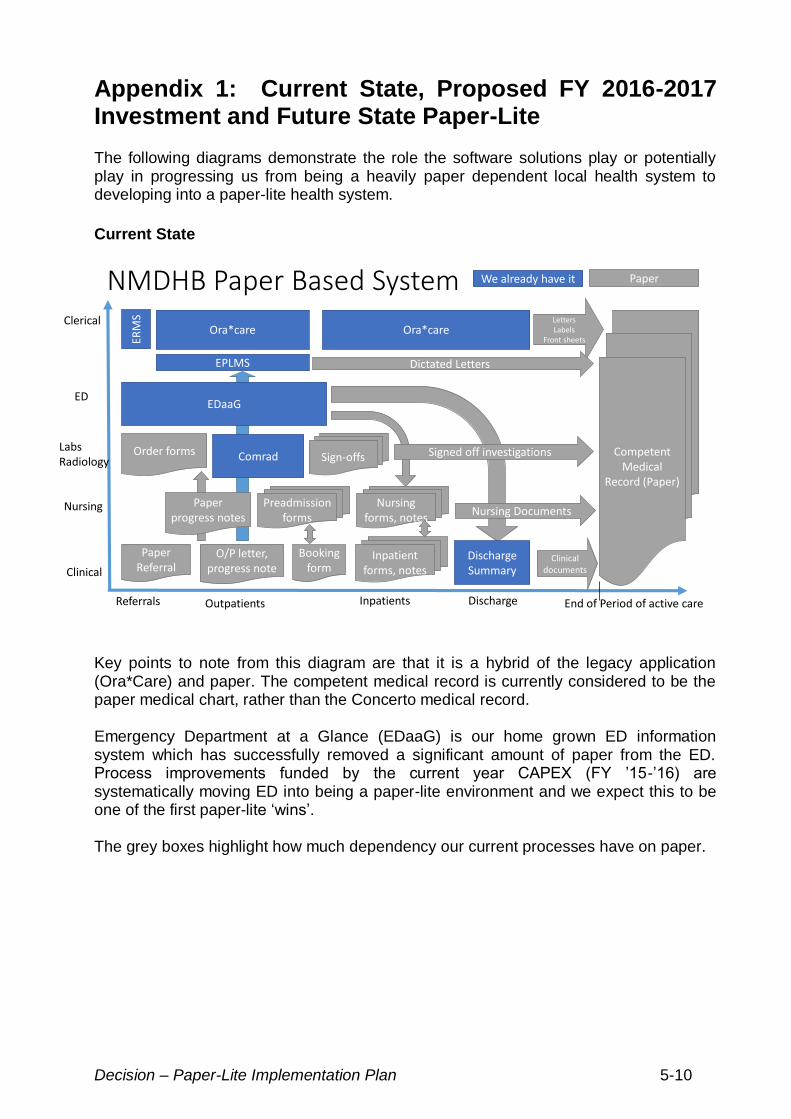
Appendix 1: Current State, Proposed FY 2016-2017 Investment and Future State Paper-Lite The following diagrams demonstrate the role the software solutions play or potentially play in progressing us from being a heavily paper dependent local health system to developing into a paper-lite health system.
Current State
Signed off investigations
Nursing Documents
ClericalOra*care
Referrals Outpatients Inpatients Discharge
Competent Medical
Record (Paper)
End of Period of active care
EDaaG
Paper Referral
O/P letter, progress note
Booking form
Inpatient forms, notes
Discharge Summary
Ora*care
ERM
S
Nursing forms, notes
Paper progress notes
Preadmission forms
Clinical
Nursing
Labs Radiology
Order forms Sign-offsComrad
Clinical documents
LettersLabels
Front sheets
ED
EPLMS Dictated Letters
NMDHB Paper Based System We already have it Paper
Key points to note from this diagram are that it is a hybrid of the legacy application (Ora*Care) and paper. The competent medical record is currently considered to be the paper medical chart, rather than the Concerto medical record. Emergency Department at a Glance (EDaaG) is our home grown ED information system which has successfully removed a significant amount of paper from the ED. Process improvements funded by the current year CAPEX (FY ’15-’16) are systematically moving ED into being a paper-lite environment and we expect this to be one of the first paper-lite ‘wins’. The grey boxes highlight how much dependency our current processes have on paper.
Decision – Paper-Lite Implementation Plan 5-11
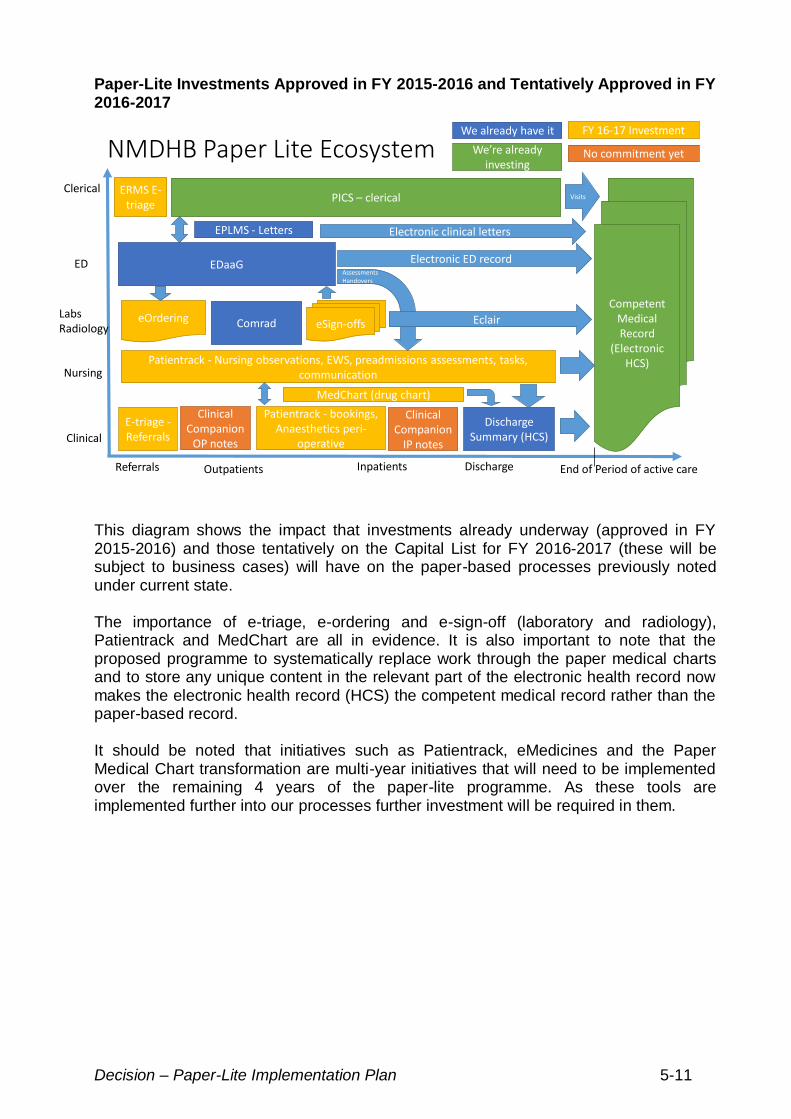
Paper-Lite Investments Approved in FY 2015-2016 and Tentatively Approved in FY 2016-2017
NMDHB Paper Lite Ecosystem
Clinical
ClericalPICS – clerical
Referrals Outpatients Inpatients Discharge
Competent Medical Record
(Electronic HCS)
End of Period of active care
E-triage -Referrals
EDaaG
Discharge Summary (HCS)
ERMS E-triage
EPLMS - Letters
eOrdering eSign-offsComrad
Patientrack - Nursing observations, EWS, preadmissions assessments, tasks, communication
Patientrack - bookings, Anaesthetics peri-
operative
Clinical Companion
OP notes
Clinical Companion
IP notes
MedChart (drug chart)
Electronic ED record
Eclair
Electronic clinical letters
Visits
AssessmentsHandovers
We already have it
We’re already investing
FY 16-17 Investment
No commitment yet
Nursing
Labs Radiology
ED
This diagram shows the impact that investments already underway (approved in FY 2015-2016) and those tentatively on the Capital List for FY 2016-2017 (these will be subject to business cases) will have on the paper-based processes previously noted under current state. The importance of e-triage, e-ordering and e-sign-off (laboratory and radiology), Patientrack and MedChart are all in evidence. It is also important to note that the proposed programme to systematically replace work through the paper medical charts and to store any unique content in the relevant part of the electronic health record now makes the electronic health record (HCS) the competent medical record rather than the paper-based record. It should be noted that initiatives such as Patientrack, eMedicines and the Paper Medical Chart transformation are multi-year initiatives that will need to be implemented over the remaining 4 years of the paper-lite programme. As these tools are implemented further into our processes further investment will be required in them.
Decision – Paper-Lite Implementation Plan 5-12
Future Paper-Lite Eco-System
Patient
GP Health One
HealthlinkDischarge summary
HealthlinkLettersER
MS
Patientrack – external access
Patient Portal including letters, bookings, demographics, records, workflow
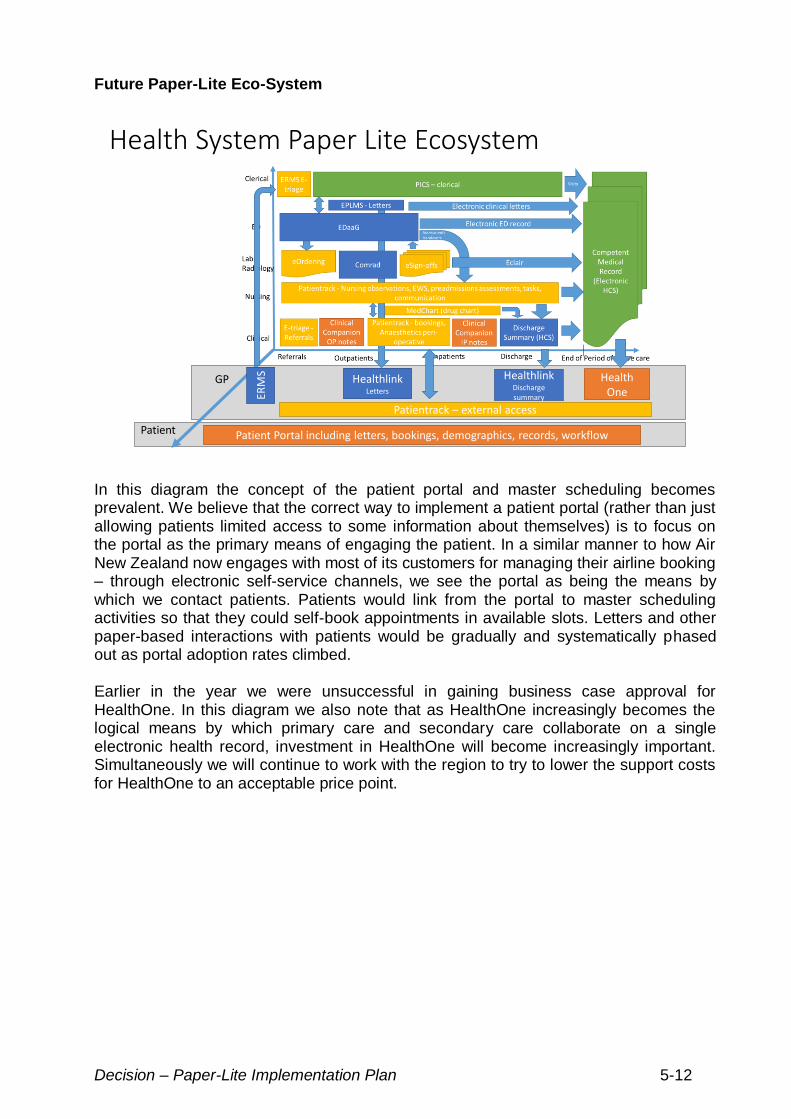
Health System Paper Lite Ecosystem
In this diagram the concept of the patient portal and master scheduling becomes prevalent. We believe that the correct way to implement a patient portal (rather than just allowing patients limited access to some information about themselves) is to focus on the portal as the primary means of engaging the patient. In a similar manner to how Air New Zealand now engages with most of its customers for managing their airline booking – through electronic self-service channels, we see the portal as being the means by which we contact patients. Patients would link from the portal to master scheduling activities so that they could self-book appointments in available slots. Letters and other paper-based interactions with patients would be gradually and systematically phased out as portal adoption rates climbed. Earlier in the year we were unsuccessful in gaining business case approval for HealthOne. In this diagram we also note that as HealthOne increasingly becomes the logical means by which primary care and secondary care collaborate on a single electronic health record, investment in HealthOne will become increasingly important. Simultaneously we will continue to work with the region to try to lower the support costs for HealthOne to an acceptable price point.





























