Embed Size (px)
Citation preview

Anaesthesia, 1987, Volume 42, pages 871-874
C A S E R E P O R T
Miller’s syndrome
Anaesthetic management of postaxial acrofacial dysostosis
M . R I C H A R D S
Summary
A new cuse of Miller’s syndrome is reported and the characteristic features are described along with a brief outline of related conditions. The anaesthetic management is discussed and the problems which may be encountered when dealing with this syndrome are highlighted.
Key words
Complications; Miller’s syndrome. Intubation, tracheal; difficult.
The syndrome of postaxial acrofacial dysostosis was first described as a complete clinical entity by Miller in 1979.’ At that time there were six recorded cases, and few have been added to the literature since. The syndrome comprises cranio- facial abnormalities similar to those of the Treacher-Collins syndrome but associated with upper and lower limb defects mainly on the postaxial side of the limb (Fig. 1, Table 1). There are several closely related syndromes of acrofacial dysostosis (AFD) * z 3 (Table 2). No previous reports of the anaesthetic management of patients with Miller’s syndrome were found.
Case history
The patient was delivered by Caesarean section for failure to progress and was noted at birth to have gross physical abnormalities, which were identified as belonging to Miller’s syndrome. She did not have any cardiac abnormalities.
She presented for repair of cleft palate at the age of 12 months. She had been anaesthetised for corrective surgery for severe bilateral ectro-
Table 1. Miller’s syndrome: recognised features.
Malar hypoplasia Micrognathia Cleft lip and/or palate Ectropion Absent superior orbital ridges Hypoplastic ears
Postaxial deformities (i.e. ulnar aspect) Absence of 4th and 5th rays in hands and feet Shortening of limbs
Defects. e .g . ASD, VSD and patent ductus arterio-
Craniofacial
Limbs
Cardiac
sus
Mental development
Other stigmata
Normal intelligence usual
Accessory nipples
pion at the age of 4 weeks, at which time it had been noted that tracheal intubation was difficult. Unfortunately, the lids still did not protect the eyes.
Clinical examination revealed a 7.7-kg child
M. Richards, MB, BCh, FFARCS, Consultant, Middlemore Hospital, Otahuhu, Auckland 6, New Zealand.
0003-2409/87/080871 + 04 %03.00/0 @ 1987 The Association of Anaesthetists of Gt Britain and Ireland 871

872 M. Richards
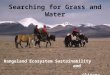
Fig. 1. Lateral view of the head of the patient aged 4 weeks. Note the Treacher-Collins-like features.
Table 2. Related or similar syndromes
Acrufucinl dysostosis ( A F D ) Miller’s AFD
See Table I Nagcr AFD
Malar hypoplasia Cleft palate Pre-axial limb defects
Split foot AFU Retro-micrognathia Cleft palate Split feet (normal upper limbs)
Distal-2q AFD * Micrognathia Abnormalities mainly confined to limbs
Cardiomelic AFD Hemifacial inicrosomia VSD
it4undihulufaciul dysosfosi.~ ( M F D ) Treacher-Collins MFD
Malar and mandibular hypoplasia Cleft palate Congenital heart defects
* Duplication of the distal Z q chromosome
with normal mental development but severe physical abnormalities. The most important to the anaesthetist were a relatively large head,
Fig. 2. The patient aged 12 months. Note the abnormal development of the face. The 4th and 5th rays of the hands are absent and the limbs are shortened and
require splinting.
malar hypoplasia, micrognathia, cleft palate and shortened limbs (Fig. 2). It was noted that par- ticular care would have to be taken of the eyes, as the lids did not cover the cornea at all. A second anaesthetist was requested for the case because of the possibility of a difficult induction and intubation.
Prcmedication with droperidol 0.15 mg and atropine 150 pg was given I .5 hours pre-opera- tively. She was calm and slightly drowsy on arrival for surgery, and this allowed inrravenous access to be established prior to induction with- out distress. The cannula was placed in the left foot bccausc of the paucity of developed veins at any other site. Previously. intravenous can- nulation had been successful only in scalp veins. Electrocardiograph monitoring was established and a precordial stethoscope attached.
Gaseous induction with halothane in 100% oxygen was then undertaken using a non- rebreathing system with reservoir bag. The fit of the mask was poor because of the facial abnormalities and a seal was achieved only by

Miller’s syndrome 873
present early for a course of plastic surgery which may last several decades. The anaesthetist must take time to establish a good rapport and consider the best anaesthetic approach to a child who will present for multiple interventions.
Pre-operativc assessment is important in order to establish the degree of abnormality. Malar hypoplasia, micrognathia and cleft palate imply possible pre- and postoperative respiratory obstruction as well as a poor mask fit and dif- ficult intubation. Similar problems are encoun- tered with Treacher-Collins ~ y n d r o m e . ~ , In this case, a premedication was chosen which would not produce deep sedation and thcreby compromise the airway. A gaseous induction was felt to be the safest approach; however, the airway was difficult to manage during induction. When it was established that manual ventilation could be achieved, it was considered that the risks of neuromuscular blockade with suxa- methonium were minimised and that relaxation would produce optimum intubation conditions. Pre-operative tracheostomy has been suggested for difficult intubation in the Treacher-Collins syndrome.6 However, this does not appear to be appropriate in Miller’s syndrome unless intu- bation is impossible by other means, as multiple anaesthetics are likely to be required over a 10-20-year period.
Limb shortening and deformity resulted in two arcas of difficulty in this case. One was patient positioning, as the limbs required extra support in the supine position to prevent stress on the joints and neighbouring neurovascular structures. The other was the dearth of reason- able limb veins for intravenous access; it was also difficult to secure the cannula in place.
Choanal atresia has not been described pre- viously in Miller’s syndromc and should be excluded before anaesthesia. The bleeding from attempted nasal intubation could have resulted in complete respiratory obstruction prior to intubation. It was fortunate that a nasal airway was not required during induction.
Cardiac abnormalities should always be sought before anaesthesia is started. Those associated with Miller’s syndrome are atrioseptal defects, ventriculoseptal defects and patent ductus arteriosus. When patients with a possible right- to-left shunt are anaeslhetised, extra care should be taken to avoid air bubbles in the in- travenous fluid because of the risk of cerebral embolus.
the use of two hands. Complctc obstruction of the airway occurred as the depth of anaesthesia increased and this was relicved only partly by the use of an oral airway and careful positioning of the head and neck. A nasal airway was con- sidered but rejected because assisted ventilation became possible shortly afterwards.
At this time suxamethonium 1.5 mg/kg was administered and ventilation continued by hand. Laryngoscopy did not reveal the cords, although the posterior aspect of the arytenoids could just be seen. A small gum-elastic introducer was manipulated blindly into the trachea with some difficulty and a non-cuffed Oxford orotracheal tube (size 3.5 mm) was inserted over this and guided into place. The eyelids were taped care- fully so as to cover the eyes and prevent desic- cation of the corneas.
Anaesthesia was maintained with nitrous oxide 60% in oxygen, supplemented by halothane, during which the child breathed spontaneously. The cleft palate was repaired without problcm and a tongue stitch was inserted to allow for- ward traction on the tongue during recovery. A nasopharyngeal airway could not be passed into either nostril prior to extubation, due to undiagnosed choanal atresia. Both sides were forcibly dilated using gum-clastic bougies and artery forceps, and the airway was positioned without further problem.
Extubation was accomplished while the pa- tient was deeply anaesthetised but with adequate spontaneous ventilation. The immediate post- operative period in the recovery room was uneventful and the infant was returned to the ward with special nursing cover. Three episodes of significant partial respiratory obstruction were noted during the following 18 hours. and all were relieved by gentle support of the jaw by the attending nurse. Subsequent progress was uneventful.
Discussion
The striking feature of Miller’s syndrome is the grossly abnormal physical development with normal intelligence. The normal menlal develop- ment makes cosmetic intervention important and rewarding. Normal psychological develop- ment is to be encouraged and, therefore, a normal physical appearance is the desired end point to surgical intervention.
Patients with Miller’s syndrome therefore

8 74 M . Richards
Conclusion
The postaxial acrofacial dysostosis (Miller’s) syndrome is compriscd of Treacher-Collins-like facics with abnormal limb development. One important aspect of the condition is that these children are usually of normal intelligence.
The main problems which may be encoun- tered by the anaesthetist are difficult intubation and airway management, poor intravenous ac- cess, the need for support for the limbs of the anaesthetised child and the possibility of cardiac abnormalities.
The othcr rclated acrofacial dysostosis syn- dromes may prcscnt similar problems that depend on the associated abnormalities and the degree of involvement.
Acknowledgments
I thank Mr M. Rees and Dr A. Elliott for their help with this case and Dr N. Rankin for reading the proofs.
References I . MII.LER M, FINEMAN R, SMITH DW. Postaxial
acrofacial dysostosis syndrome. Journal of Pedi- atrics 1979; 95: 97G5.
2. HALAL F, HEKRMANN J, PALLISTER PD, OPITZ JM. DESCKANGES M-F, GKENIEK G . Differential diag- nosis of Nager Acrofacial Dysostosis Syndrome: report of four patients with Nager syndrome and discussion of other related syndromes. Anwrican Journal of Medical Generics 1983; 14: 209-24.
3. KAWIRA EL. WEAVER DD, BENDER HA. Acro- facial dysostosis with severe facial clefting and limb reduction. American Journal of Medical Generics 1984: 17: 641-7.
4. Ross EDT. Treacher-Collins syndrome. An anaesthetic hazard. Anaesthesia 1963; 18: 35011.
5. DIVEKAK VM, SIRCAR BN. Anaesthetic manage- ment in Treacher-Collins syndrome. An- esthesiulogy 1965; 2 6 692-3.
6. SAIDMAK LJ, MOYA F. Complications of anaes- thesia. Springfield, IL: Charles, C. Thomas, 1970: 109.