-
AOP*** 1
IJO_479_10R11
Department of Oral Medicine and Radiology, Institute of Dental
Studies and Technologies, Modinagar, 1Department of Oral Medicine
and Radiology, Subharti Dental College and Hospital, Meerut, Uttar
Pradesh, 2Department of Ophthalmology, Moolchand Hospital, Meerut,
Uttar Pradesh, India
Correspondence to: Dr. Sumit Goel, B 202 Nandan Apartment, 31 A
Saket, Meerut, Uttar Pradesh, India. E‑mail:
[email protected]
Manuscript received: 11.08.10; Revision accepted: 09.07.12
Nager syndrome, also called preaxial acrofacial dysostosis, was
first described by Nager and Reynier in 1948.[1,2] It consists of a
defect in the development of the first and second branchial arches
and in the formation of cartilage.[1,2] Typically, Nager acrofacial
dysostosis (NAFD) comprises two groups of defects involving the
limbs and craniofacial region, respectively.[1,3] The former are
mainly deficiencies mostly affecting the upper limbs. The latter
form a complex indistinguishable from mandibulofacial dysostosis
(MFD).[2]
The prevalence is unknown; about 70 cases of Nager syndrome have
been published. The MFD complex is unmistakable and comprises
hypoplasia of the malar eminences and zygomata, hypoplasia of
maxilla with cleft of secondary palate or highly‑arched palate,
absence of velum (rarely with choanal atresia), and extension of a
“tongue” of temporal hair down the sides of the cheeks. The ocular
features are
important and include downward slant of palpebral fissures,
ptosis of upper lids, coloboma of lower lids, and deficiency of
eyelashes of the medial one‑third to two‑thirds of the lower
eyelids. Hypoplasia or absence of thumbs is the most characteristic
feature almost invariably associated with radio‑ulnar synostosis.
Triphalangeal thumbs and index finger are equally characteristic.
Most NAFD individuals have normal intelligence, and after infancy
most are healthy and are presumed to have a normal lifespan. All
acrofacial dysostosis must be considered as genetic disorders until
proven otherwise, and parents deserve careful scrutiny for mild
manifestations.[1‑3]
Limbal dermoids are benign congenital tumors that contain
choristomatous tissue. They appear most frequently at the inferior
temporal quadrant of the corneal limbus.We report limbal dermoid in
a patient with Nager syndrome. We did not find such an association
of “Limbal dermoid in Nager acrofacial dysostosis syndrome” on
PubMed using Nager acrofacial dysostosis, limbal dermoid and ocular
manifestations as the keywords.
Case ReportA 16‑year‑old female patient came to Department of
Oral Medicine and Radiology with chief complaints of bleeding from
gums. On examination, she was thin built. The right thumb of her
right upper extremity was absent. Right forearm appeared short. All
her vitals were within normal limits. Extraoral examination of face
and skull revealed hypoplasia of the malar eminences and zygomata,
hypoplasia of maxilla and underdevelopment of the mandible [Fig.
1]. Ears appeared low‑set and rotated with presence of skin tags
[Fig. 2]. Intraoral examination revealed inflamed gingiva due to
poor oral hygiene. Radiological examination supported the clinical
findings. Patient was then referred to ophthalmology department
where ocular examination showed downward slant of palpebral
fissures, ptosis of upper lids and limbal dermoid in right eye
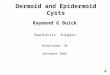
measuring around 1 × 1 cm in diameter [Fig. 3]. On the basis of
examination and radiographic investigations, the patient was
diagnosed as a case of Nager syndrome. The patient was
uncooperative and refused any other treatment except for oral
prophylaxis which we performed to relieve her from bleeding
gums.
DiscussionThis condition is described as a syndrome which
involves the upper limbs and skull. The most ordinary type of
acrofacial dysostosis is the Nager type (NAFD) of the so‑called
pre‑axial acrofacial dysostosis. This disorder is categorized by
the Office of Rare Diseases in the United States as a rare illness;
thus, it has only affected less than 200,000 of the country’s
population. This disorder is often sporadic although it can be
inherited too. Some studies have shown that the gene which causes
the illness might be located around 9q32 and it is possible that
the ZFP‑37 gene could also be involved.[2‑4]
The major symptoms of Nager syndrome often include the
underdevelopment of the jaw and cheek areas, a jaw that may appear
smaller than the usual or normal jaw, hearing problems (and some
defects on the external or internal ear area), cleft palate (which
is a congenital defect of the mouth or the lip), the absence or
underdevelopment of the thumb or thumbs, forearms that appear short
(the forearms could
Access this article onlineQuick Response Code: Website:
www.ijo.in
DOI:***
PMID: ***
Limbal dermoid in nager syndrome acrofacial dysostosis: A rare
case report
Rohit Malik, Sumit Goel, Saurabh Aggarwal1
Nager syndrome, also called preaxial acrofacial dysostosis,
comprises two groups of defects involving the limbs and
craniofacial region, respectively. This syndrome is rare and only
70 cases have been reported in the literature. The exact cause of
this syndrome is unknown, but there is indication that it is
genetically based. Ocular manifestations of this syndrome include
widely separated downward slanting eyes, absence of eyelashes,
ptosis of upper eyelids and colobomas on the inner aspect of lower
eyelids. We report limbal dermoid in a patient with Nager syndrome.
We did not find such an association of “Limbal dermoid in Nager
acrofacial dysostosis syndrome” on PubMed using Nager acrofacial
dysostosis, limbal dermoid and ocular manifestations as the
keywords.
Key words: Absent thumb, craniofacial defects, limbal dermoid,
Nager syndrome
-
2 Indian Journal of Ophthalmology Vol. ??? No. ???
altogether be absent of the radius bone), fusing of the bones of
the forearms, poor elbow movements (or limited extension of this
body part), ears that appear to be backward rotated, the ears
manifesting some skin tags (or they could be low‑set),
and feeding and breathing problems (especially among infants who
are afflicted with this syndrome).[3‑6] Our patient showed
underdevelopment of jaws, hypoplasia of the malar eminences,
zygomata and hypoplasia of maxilla. The ear showed presence of skin
tags. There was absence of thumb of her right hand which also
appeared short.
Ocular manifestations of this syndrome are rare and include
downward slant of palpebral fissures, ptosis of upper lids,
coloboma of lower lids, and deficiency of eyelashes of the medial
one‑third of the lower eyelids.[7] Our patient showed downward
slant of palpebral fissures, ptosis of upper lids and limbal
dermoid in right eye.
Traditionally, the differential diagnosis of Nager syndrome is
done with Treacher‑Collins, Pierre‑Robin and Goldenhar syndrome.
Treacher‑Collins syndrome is characterized by maxilla and mandible
hypoplasia, downslanting palpebral fissures, colobomas of inferior
eyelid and auricular malformation. Pierre‑Robin syndrome presents
with micrognathia, cleft palate and glossoptosis. In Goldenhar
syndrome, we find hemifacial microsomy, flattening of maxilla,
temporal and zygomatic bone, microtia, ocular and vertebral
alterations, and in 50% of cases, Fallot tetrad.[1,2,5]
Radiological findings are usually supportive of clinical
examination revealing hypoplasia of facial structures. The
echographic findings of these malformations become evident usually
in the third trimester, therefore a systematic ultrasound
exploration including visualization of fetal face line is essential
for its detection.[8]
The treatment is totally dependent on the symptoms manifested.
If the patient suffers from speech retardation, then a speech
therapist could help the patient. Physicians who specialize in ear
problems can also help. They may not totally cure the condition,
but they can help in managing the symptoms.[2,6] Treatment of
limbal dermoids may consist of periodic removal of irritating
cilia, topical lubrication to prevent foreign body sensation, or
excision of the lesion if it is causing significant cosmetic
disfigurement or interfering with vision.[9] Our patient refused to
take any ocular treatment and insisted on taking only the dental
treatment for which she visited our hospital.
ConclusionCorrect understanding of the underlying
pathophysiologic pattern of this disease is necessary for optimal
diagnosis and treatment planning. This should be supported with
appropriate investigations, both systemic and radiological.
Ophthalmological examination of these patients is a must as ocular
manifestations are not uncommon in these patients. We found limbal
dermoid associated with this syndrome.
References1. Jones KL. Pattern of malformation differential
diagnosis
by anomalies. In: Smith’s Recognizable Patterns of Human
Malformation. 6th ed. Philadelphia: WB Saunders Company; 2006. P.
891.
2. Opitz JM. Acrofacial Dysostosis 1, Nager type. Orphanet
Encyclopedia. Available from:
http://www.orphan.net/data/patho/GB/uk‑nager‑pdf. 2003.
3. Gorlin RJ, Cohen MM Jr, Hennekam RCM. The mandibulo and
acrofacial dysostosis In: Gorlin’s syndromes of the Head and
Neck.
Figure 1: Extraoral examination of face and skull showing
hypoplasia of the malar eminences and zygomata, hypoplasia of
maxilla and underdevelopment of the mandible
Figure 2: Low‑set ears along with presence of skin tags
Figure 3: Ocular examination showing limbal dermoid in right
eye
-
AOP*** 3AOP*** Brief Communications
4th ed. New York: Oxford University Press; 2001. p. 799‑8094.
Mayerson MD, Nisbet JB. Nager syndrome: An update of speech
and hearing characteristics. Cleft Palate J 1987;24:142‑51.5.
Hatal F, Herrmann J, Pallister PD, Opitz JM, Desgranges MF,
Grenier G. Differential diagnosis of Nager syndrome: Report of 4
patients. Am J Med Genet 1983;14:209‑24.
6. Kavadia S, Kaklamanos EG, Antoniades K, Lafazanis V, Tramma
D. Nager Syndrome: A case report. Oral surg Oral Med Oral Path Oral
Radiol Endod 2004;97:732‑8.
7. Thapa R, Pramanik S, Mukhopadhyay M, Ghosh A. Nager
Acrofacial Dysostosis: An Unusual Association with Both Upper
and Lower Eyelid Colobomas. Indian J Pediatr 2006;73:631‑2.8.
Paladini D, Tartaglione A, Lamberti A, Lapadula C, Martinelli
P.
Prenatal ultrasound diagnosis of Nager syndrome. Ultrasound
Obstet Gynecol 2003;21:195‑7.
9. Mohan M, Mukherjee G, Panda A. Clinical evaluation and
surgical intervention of limbal dermoid. Indian J Ophthalmol
1981;29:69‑73.
Cite this article as: Citation will be included before issue
gets online***