Embed Size (px)
Citation preview
Miocardite a cellule
giganti prima del
trapianto di cuore:
possibili opzioni
terapeutiche
L'esperienza di Niguarda
Enrico Ammirati
Cardiologia 2
ASST Grande Ospedale
Metropolitano Niguarda
Enrico Ammirati, MD, PhD
GIANT CELL MYOCARDITIS BEFORE TRANSPLANTATION
- POSSIBLE THERAPEUTIC OPTIONS
Enrico Ammirati, MD, PhD
‘De Gasperis’ Cardio Center
Transplant Center
ASST Grande Ospedale
Metropolitano Niguarda
Milan, Italy
NO POTENTIAL CONFLICTS
of INTEREST for this lecture
INTRODUCTIONINTRODUCTION
• Giant cell myocarditis (GCM) is a rare disorder in which
survival beyond 1 year without Heart transplantation
(HTx) is uncommon.1
• GCM is attributed to a T-cell mediated inflammation of the
myocardium.2myocardium.
• The most common early manifestation is acute heart
failure (HF )(range from 31 to 64%).3,4
1. Maleszewski/Cooper LT, AJC 2015
2. Cooper LT, NEJM 1997
3. Kandolin R, CIRC HF, 2013
4. GCM Study Group, JACC 2003
INTRODUCTIONINTRODUCTION
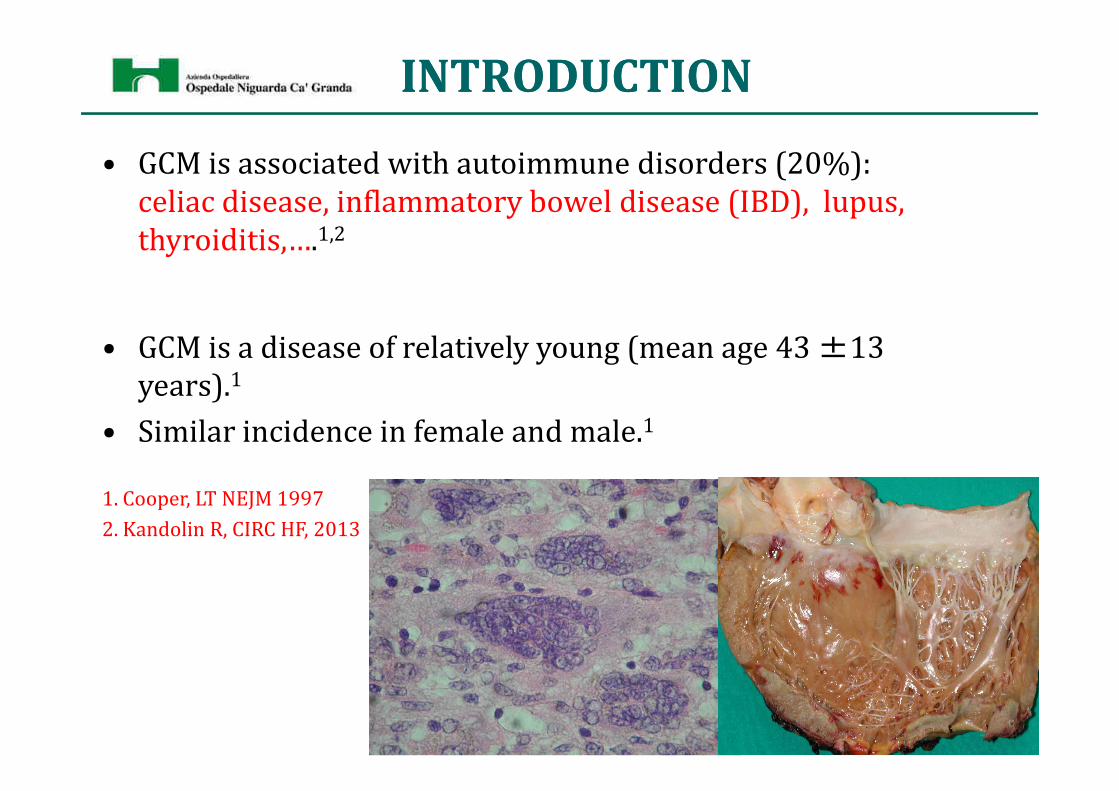
• GCM is associated with autoimmune disorders (20%):
celiac disease, inflammatory bowel disease (IBD), lupus,
thyroiditis,….1,2
• GCM is a disease of relatively young (mean age 43 ±13
years).1years).
• Similar incidence in female and male.1
1. Cooper, LT NEJM 1997
2. Kandolin R, CIRC HF, 2013
INTRODUCTIONINTRODUCTION
• Endomyocardial biopsy (EMB) is needed for final diagnosis
of GCM.1
• EMB is underutilized in the setting of fulminant
myocarditis (FM):2 only in 26% of patients with FM on
vaECMO in an Italian registry (N=57). Steroids were usedvaECMO in an Italian registry (N=57). Steroids were used
only in 18%.2
• 0 EMB in a single center experience of 22 cases of FM on
vaECMO in Japan.3
1. Caforio AL., ESC 2013
2. Lorusso, R, Ann Thorac Surg 2016
3. Nakamura, J Intens Care 2015
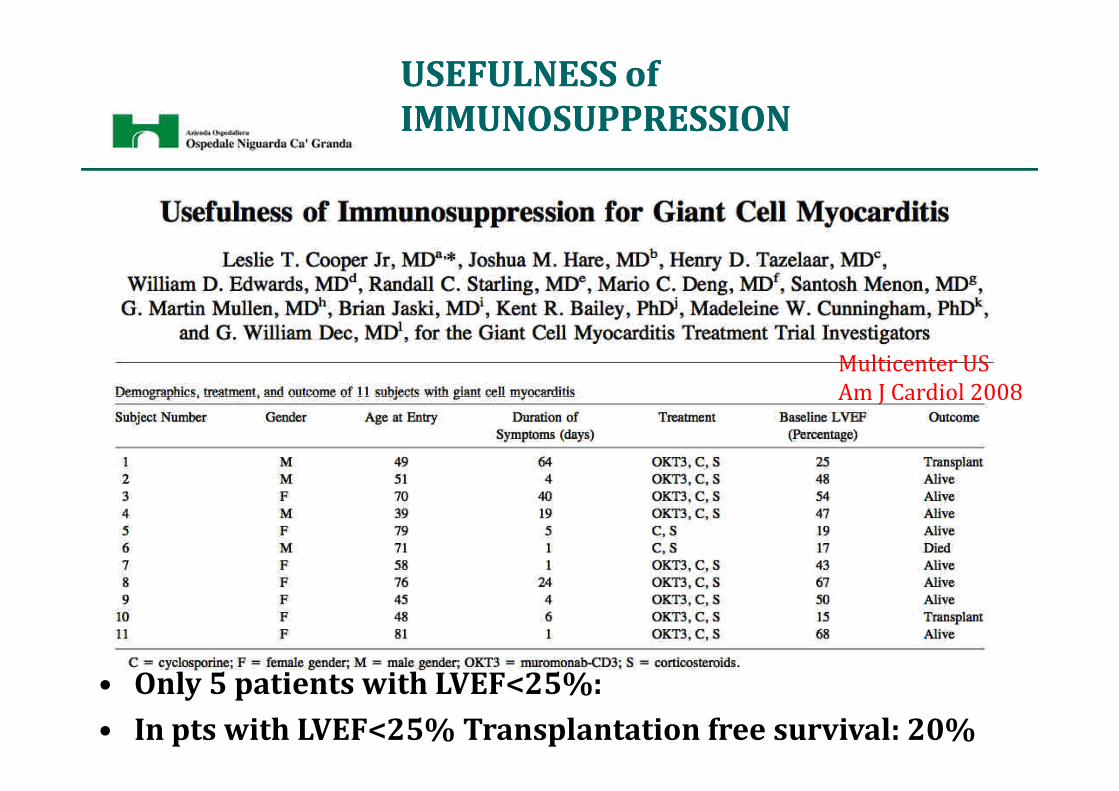
USEFULNESS of USEFULNESS of
IMMUNOSUPPRESSIONIMMUNOSUPPRESSION
Multicenter US
Am J Cardiol 2008
• Only 5 patients with LVEF<25%:
• In pts with LVEF<25% Transplantation free survival: 20%
Am J Cardiol 2008
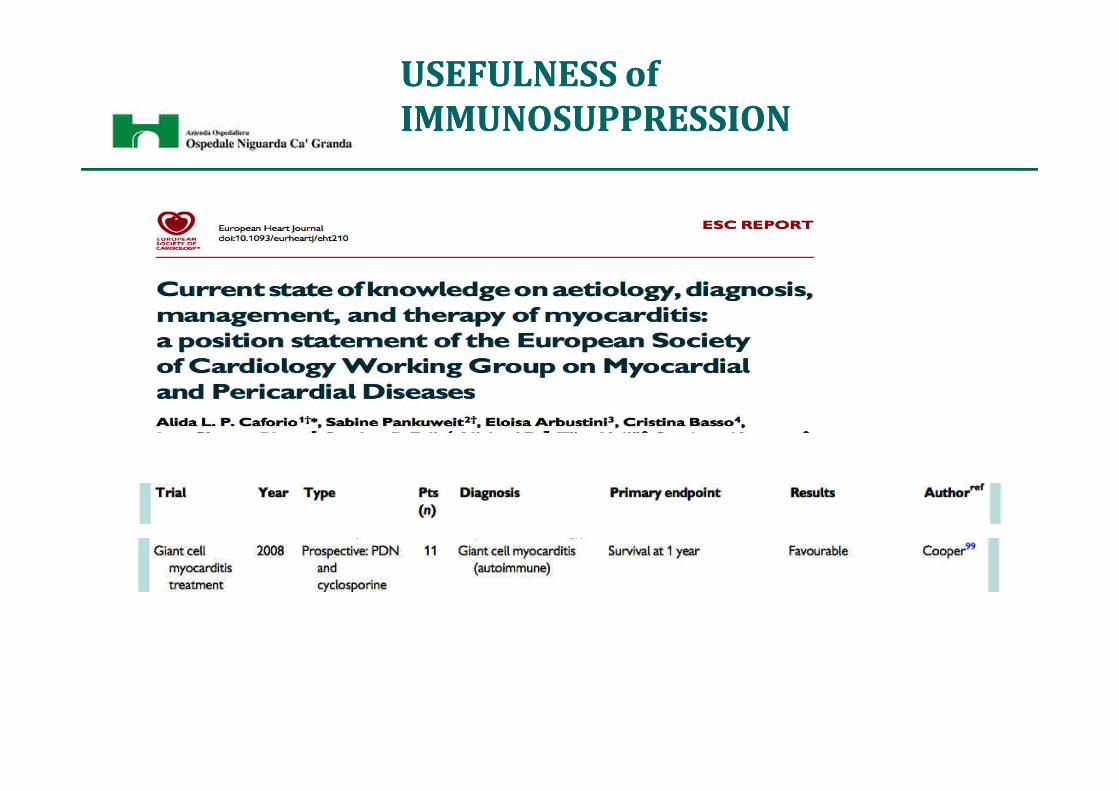
USEFULNESS of USEFULNESS of
IMMUNOSUPPRESSIONIMMUNOSUPPRESSION
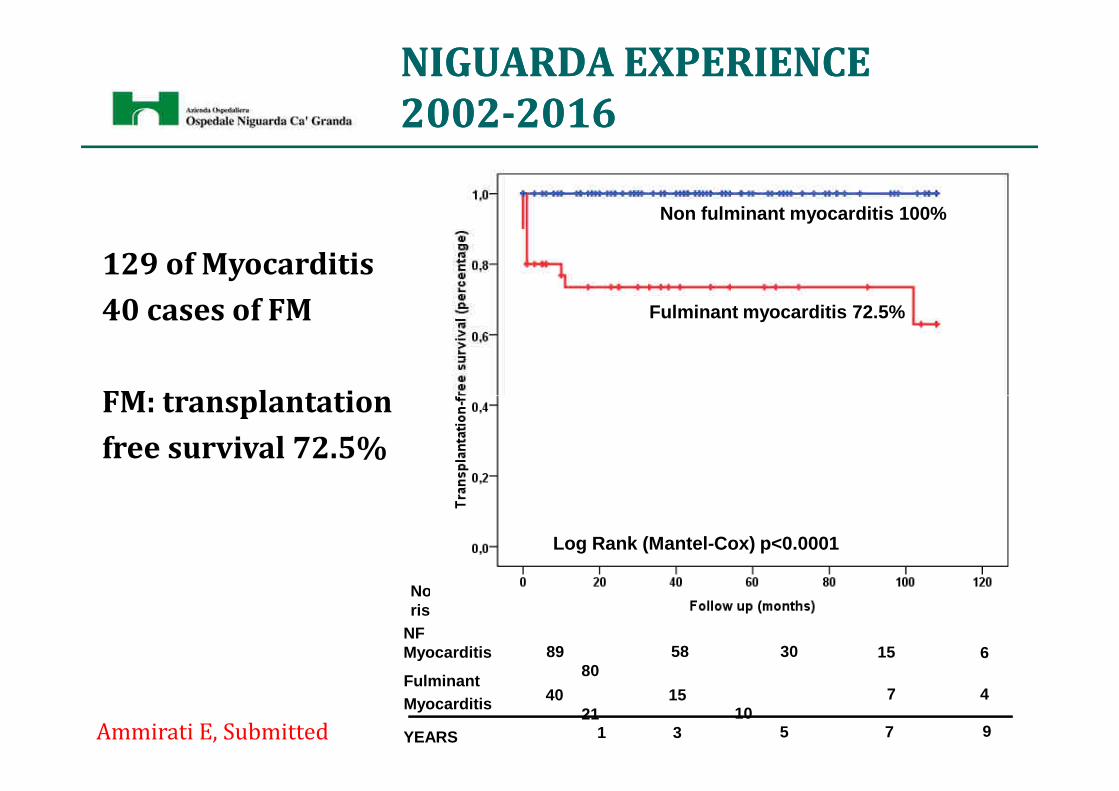
NIGUARDA EXPERIENCENIGUARDA EXPERIENCE
20022002--20162016
129 of Myocarditis
40 cases of FM
FM: transplantation
Non fulminant myocarditis 100%
Fulminant myocarditis 72.5%
FM: transplantation
free survival 72.5%
1015
2140
FulminantMyocarditis
305880
89NF Myocarditis
No. at risk
6
4
15
7
YEARS 1 3 5 7 9
Log Rank (Mantel-Cox) p<0.0001
Ammirati E, Submitted
NIGUARDA EXPERIENCENIGUARDA EXPERIENCE
20022002--20162016
40 cases of FM: 5 (12%) cases were GCM.
– 3 HTx during hospitalization
– 1 death during hospitalization
– 1 full recovery after 21 days on vaECMO. (Need for ICD due to – 1 full recovery after 21 days on vaECMO. (Need for ICD due to
VT after discharge despite LVEF 60%)
• Overall survival: 80%
• Transplantation-free survival: 20%
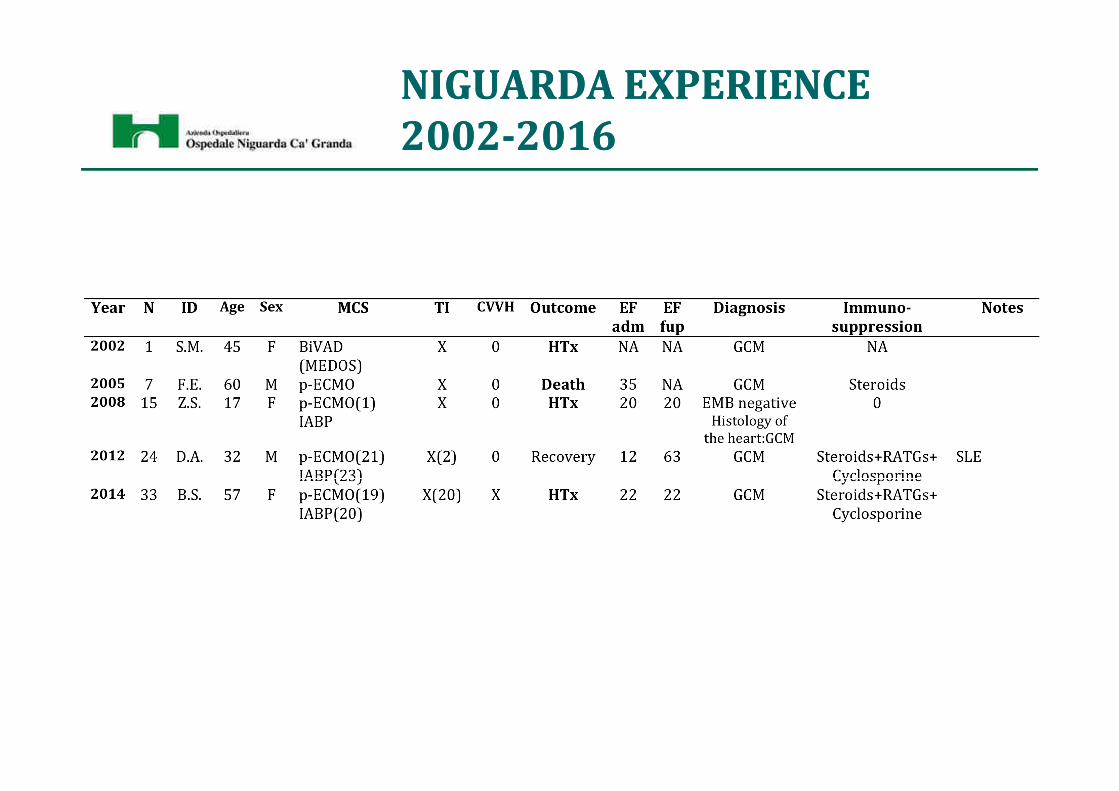
NIGUARDA EXPERIENCENIGUARDA EXPERIENCE
20022002--20162016
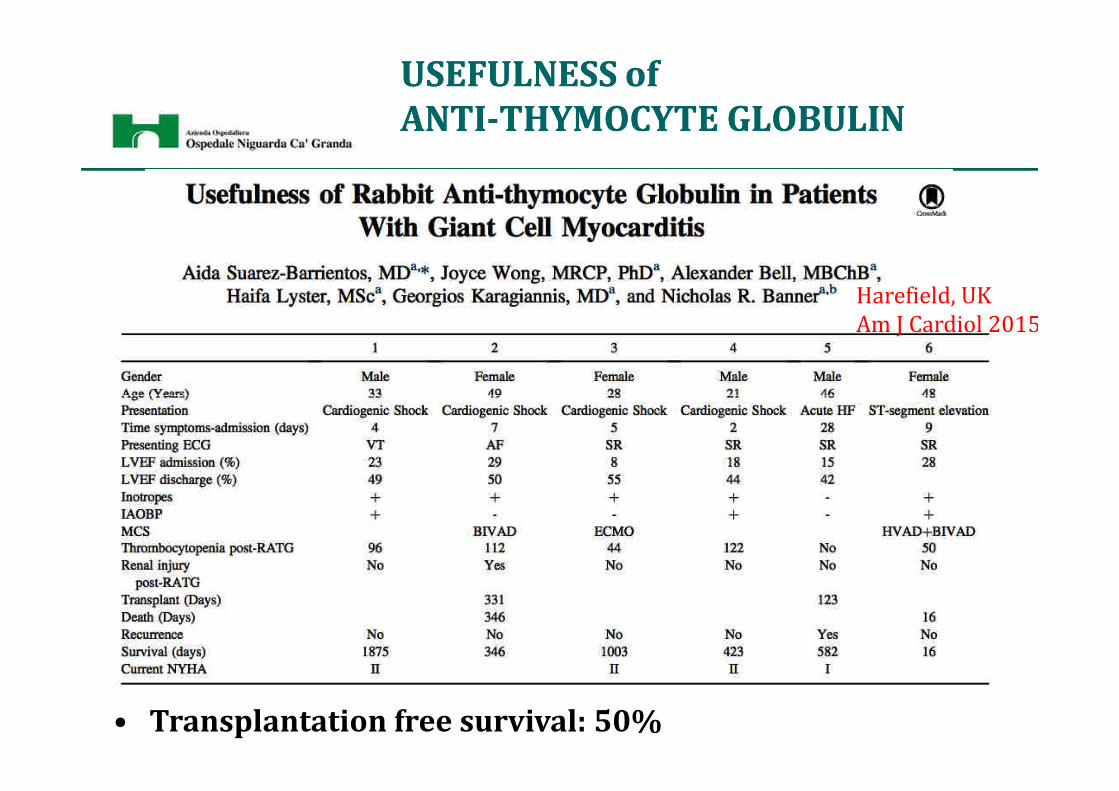
USEFULNESS of USEFULNESS of
ANTIANTI--THYMOCYTE GLOBULINTHYMOCYTE GLOBULIN
Harefield, UK
Am J Cardiol 2015
• Transplantation free survival: 50%
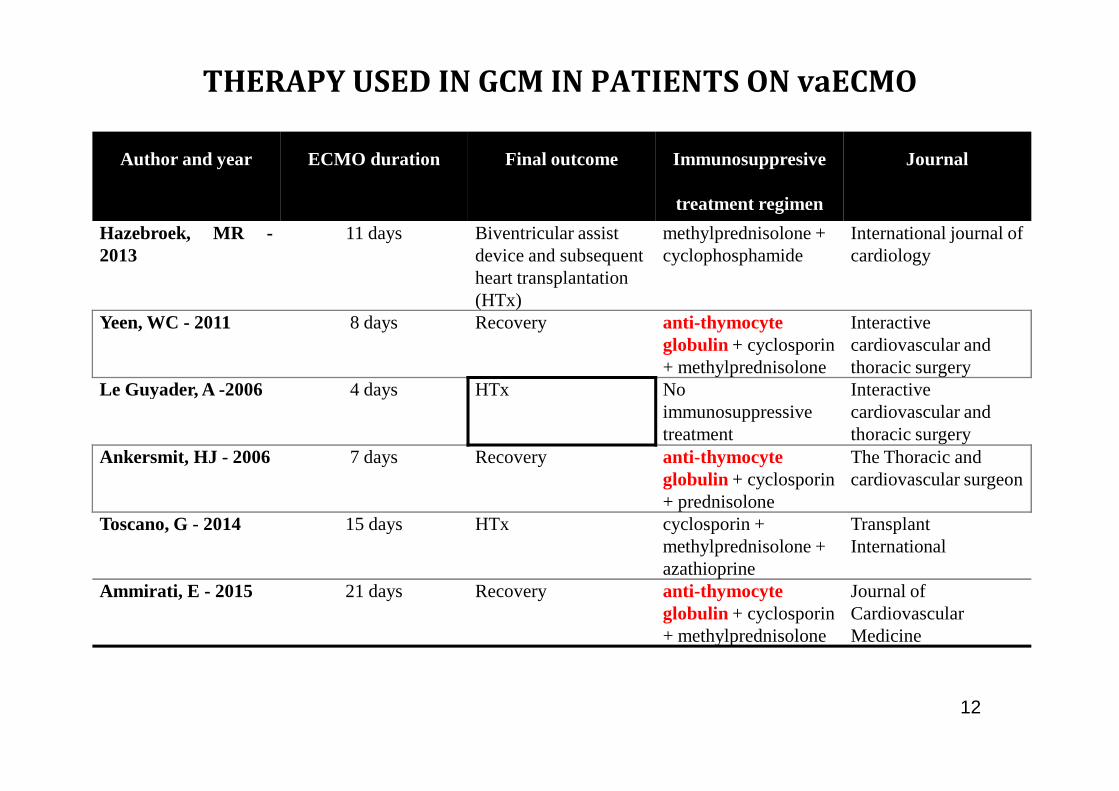
THERAPY USED IN GCM IN PATIENTS ON vaECMO
Author and year ECMO duration Final outcome Immunosuppresive
treatment regimen
Journal
Hazebroek, MR -2013
11 days Biventricular assist device and subsequent heart transplantation (HTx)
methylprednisolone + cyclophosphamide
International journal of cardiology
Yeen, WC - 2011 8 days Recovery anti-thymocyteglobulin + cyclosporin+ methylprednisolone
Interactive cardiovascular and thoracic surgery
Le Guyader, A -2006 4 days HTx No Interactive
12
Le Guyader, A -2006 4 days HTx No immunosuppressivetreatment
Interactive cardiovascular and thoracic surgery
Ankersmit, HJ - 2006 7 days Recovery anti-thymocyteglobulin + cyclosporin+ prednisolone
The Thoracic and cardiovascular surgeon
Toscano, G - 2014 15 days HTx cyclosporin + methylprednisolone + azathioprine
Transplant International
Ammirati, E - 2015 21 days Recovery anti-thymocyteglobulin + cyclosporin+ methylprednisolone
Journal of Cardiovascular Medicine
A CLINICAL CASE:
Mr A.D.• A 31-year-old man with a history of multiple autoimmune
disorders (thyroiditis, ulcerative colitis, autoimmune
hepatitis)
– Influenza-like illness 1 week before onset of cardiac symptoms
– progressive dyspnoea and severe biventricular dysfunction (left
Day 1
– progressive dyspnoea and severe biventricular dysfunction (left
ventricular ejection fraction –LVEF- of 30%)
– Coronary angiogram was normal (SUSPECTED MYOCARDITIS)
– VT treated with electrical cardioversion
– After 24 hrs TRANSFERRED TO OUR CENTRE (HTx/MCS
REFERRAL CENTRE in Milan)
CLINICAL AND ECHO DATA
BP: 85/40 mmHg with Dopamine
HR 122 bpm � + Epinephrine
SatO2 90% � NIMV
ECHO: LVEF 20%,EDD 53 mm MR ++
IVS 12 PW 12 mm, RV: TAPSE 16 mm
No pericardial effusion
Day 2
No pericardial effusion
No aortic regurgitation
SU
ND
AY
NIG
HT
ABG analysis pH 7.4 Lactate 7
BP 80/40 HR 135 bpm
OLIGURIA 70 ml/2hrs (<0.5 ml/kg/hr)
UNRESPONSIVE cardiogenic shock
after 48hrs since the onset
1:1 IABP +A 0.12+D in CCU
THE DAY AFTER
Morning, 19th November 2012:BP 105/50 mmHg HR 105 bpm on IABP + Adrenaline + Dopamine
CVP 8 mmHg T 37.2°C
Urinary output >100 ml/h ABG: lactate 1.5
Day 3
NT-proBNP 32,126 ng/L (n.v. 0-121)
Troponin T hs 2,065 ng/L (n.v. 0-14)
C-reactive protein 24.6 (n.v. 0-0.5 mg/dL)
WHITE BLOOD COUNT 15.5*109/L
Creatinin 1.26 mg/dL (n.v. 0.7-1.2)
ALT 127 U/L (n.v. 3-45)
SEVERE MYOCARDIAL INJURY
SYSTEMIC INFLAMMATORY
RESPONSE
RENAL and HEPATIC
INJURY
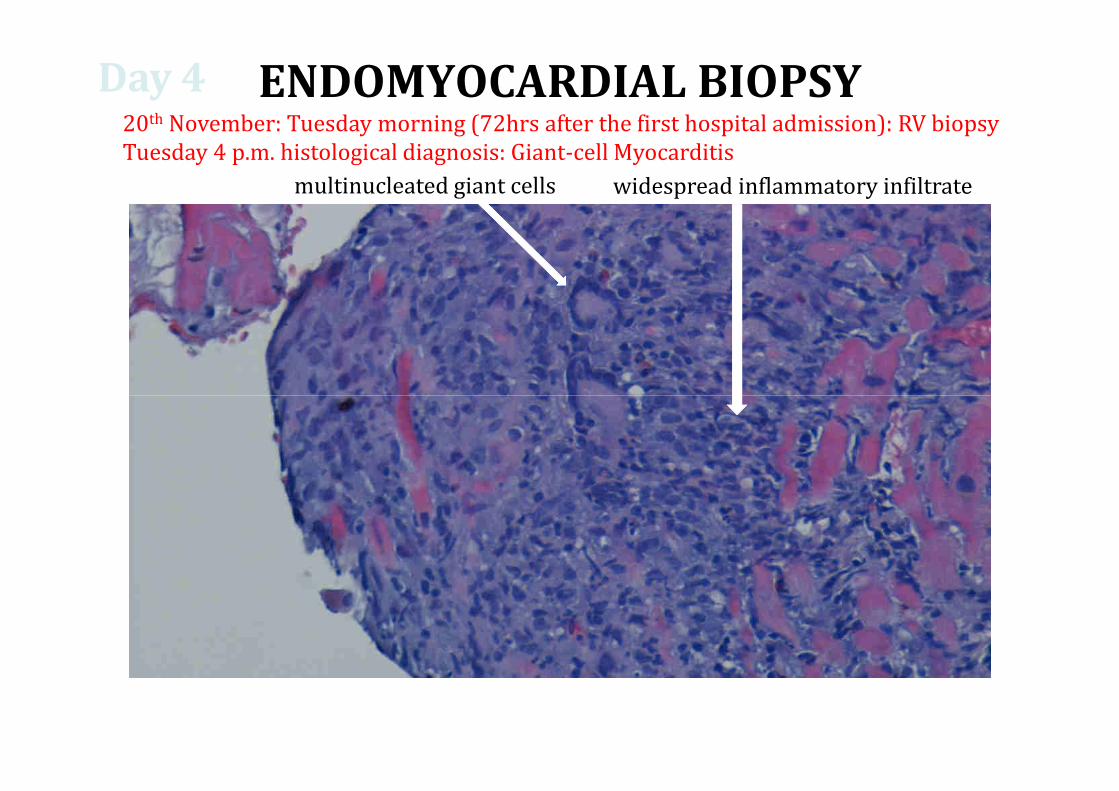
ENDOMYOCARDIAL BIOPSY
multinucleated giant cells widespread inflammatory infiltrate
20th November: Tuesday morning (72hrs after the first hospital admission): RV biopsy
Tuesday 4 p.m. histological diagnosis: Giant-cell Myocarditis
Day 4
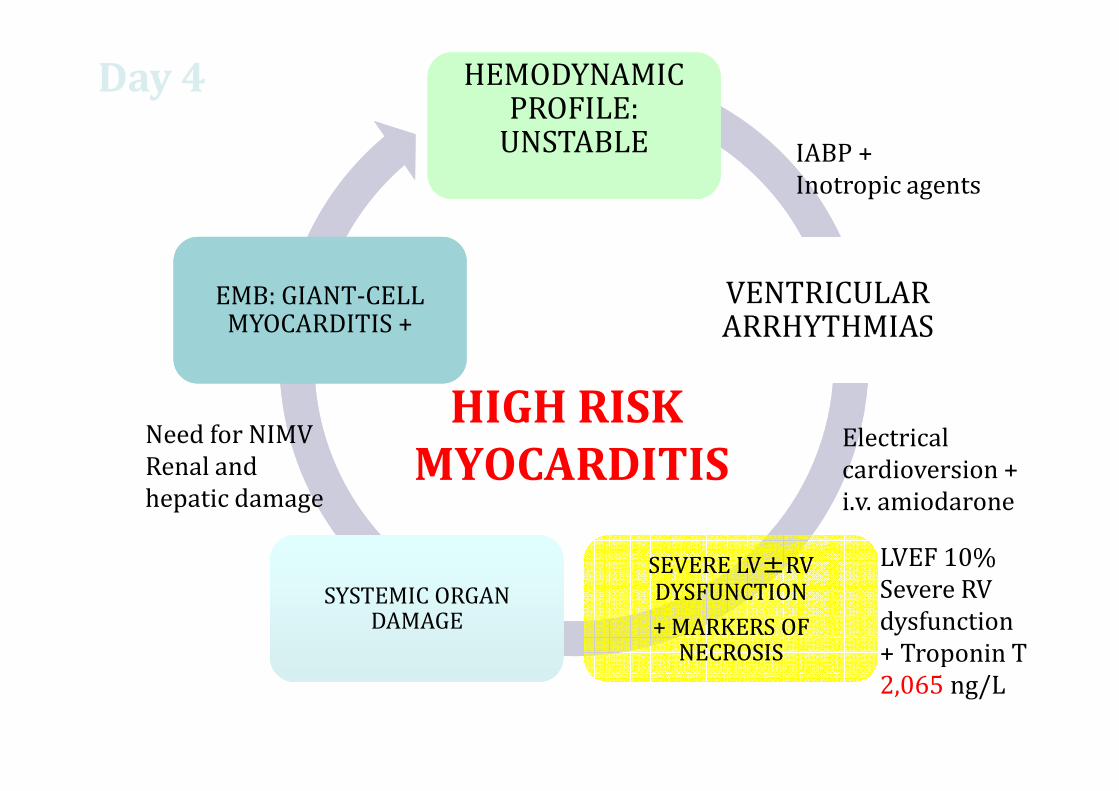
HEMODYNAMIC PROFILE:
UNSTABLE
HEMODYNAMIC PROFILE:
UNSTABLE
VENTRICULAR ARRHYTHMIASVENTRICULAR ARRHYTHMIAS
EMB: GIANT-CELL MYOCARDITIS +
EMB: GIANT-CELL MYOCARDITIS +
HIGH RISK
Day 4
IABP +
Inotropic agents
SEVERE LV±RV DYSFUNCTION
+ MARKERS OF NECROSIS
SEVERE LV±RV DYSFUNCTION
+ MARKERS OF NECROSIS
SYSTEMIC ORGAN DAMAGE
SYSTEMIC ORGAN DAMAGE
HIGH RISK
MYOCARDITISElectrical
cardioversion +
i.v. amiodarone
Need for NIMV
Renal and
hepatic damage
LVEF 10%
Severe RV
dysfunction
+ Troponin T
2,065 ng/L
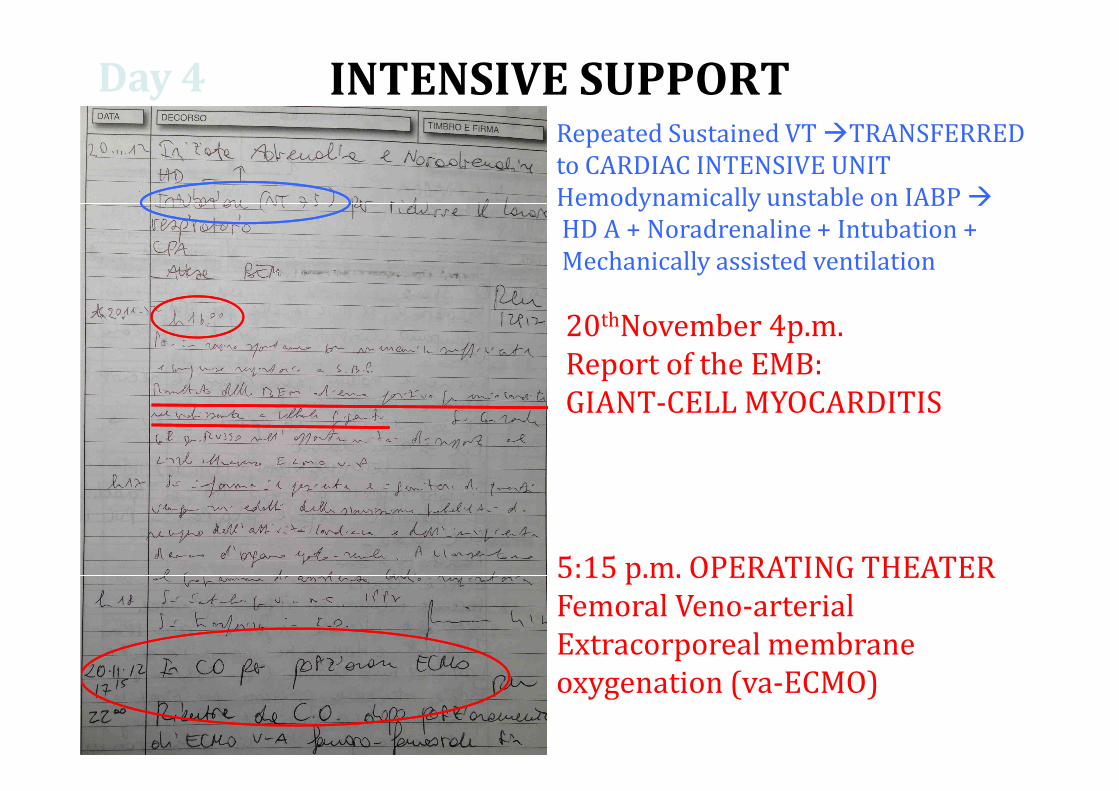
INTENSIVE SUPPORTDay 4
Repeated Sustained VT �TRANSFERRED
to CARDIAC INTENSIVE UNIT
Hemodynamically unstable on IABP �
HD A + Noradrenaline + Intubation +
Mechanically assisted ventilation
20thNovember 4p.m.
Report of the EMB:
GIANT-CELL MYOCARDITISGIANT-CELL MYOCARDITIS
5:15 p.m. OPERATING THEATER
Femoral Veno-arterial
Extracorporeal membrane
oxygenation (va-ECMO)
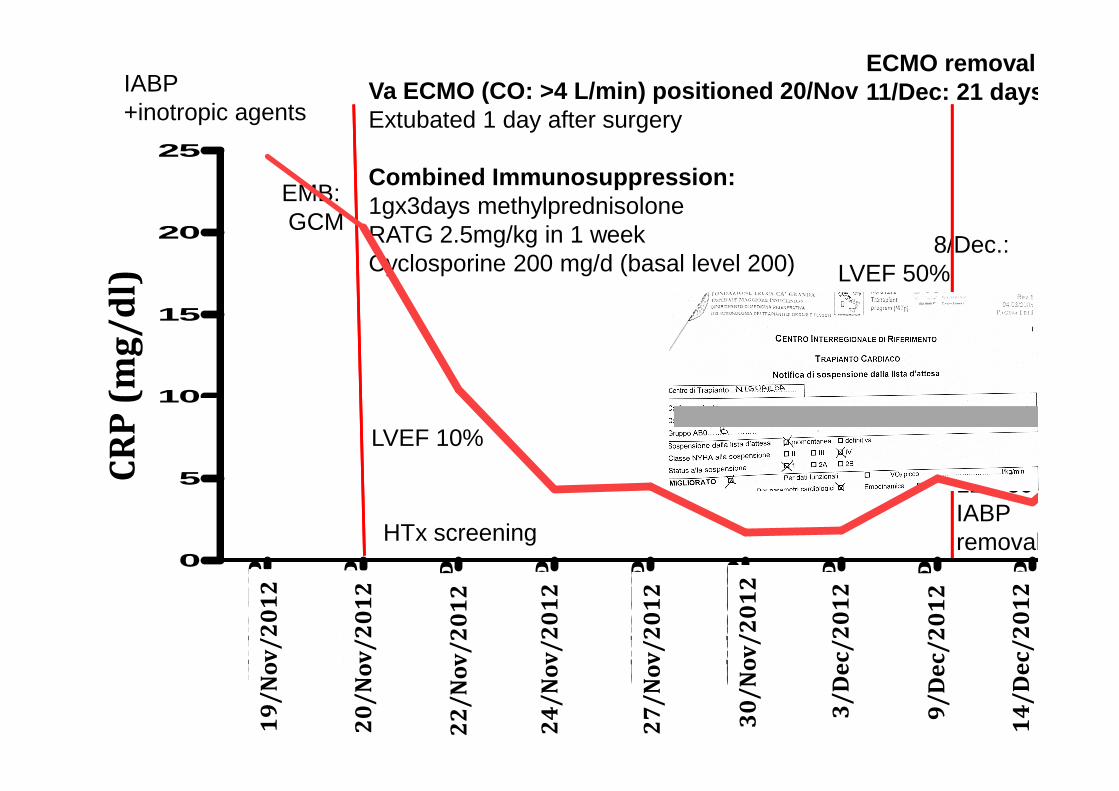
IABP+inotropic agents
Va ECMO (CO: >4 L/min) positioned 20/Nov Extubated 1 day after surgery
Combined Immunosuppression:1gx3days methylprednisoloneRATG 2.5mg/kg in 1 weekCyclosporine 200 mg/d (basal level 200)
EMB:GCM
Blood group BHTx Listing
8/Dec.:LVEF 50%
ECMO removal11/Dec: 21 days
CR
P (
mg
/d
l)
10
15
20
25
LVEF 10%
HTx screening
HTx ListingNATIONAL URGENCY5�8/Dec
12/DecIABPremoval
CR
P (
mg
/d
l)
19/11/12-15:00
20/11/12-07:00
22/11/12-07:00
24/11/12-07:00
27/11/12-07:00
30/11/12-07:00
03/12/12-07:00
09/12/12-07:00
14/12/12-07:00
0
5
10
19
/N
ov
/2
01
2
20
/N
ov
/2
01
2
24
/N
ov
/2
01
2
22
/N
ov
/2
01
2
27
/N
ov
/2
01
2
30
/N
ov
/2
01
2
3/
De
c/
20
12
14
/D
ec
/2
01
2
9/
De
c/
20
12
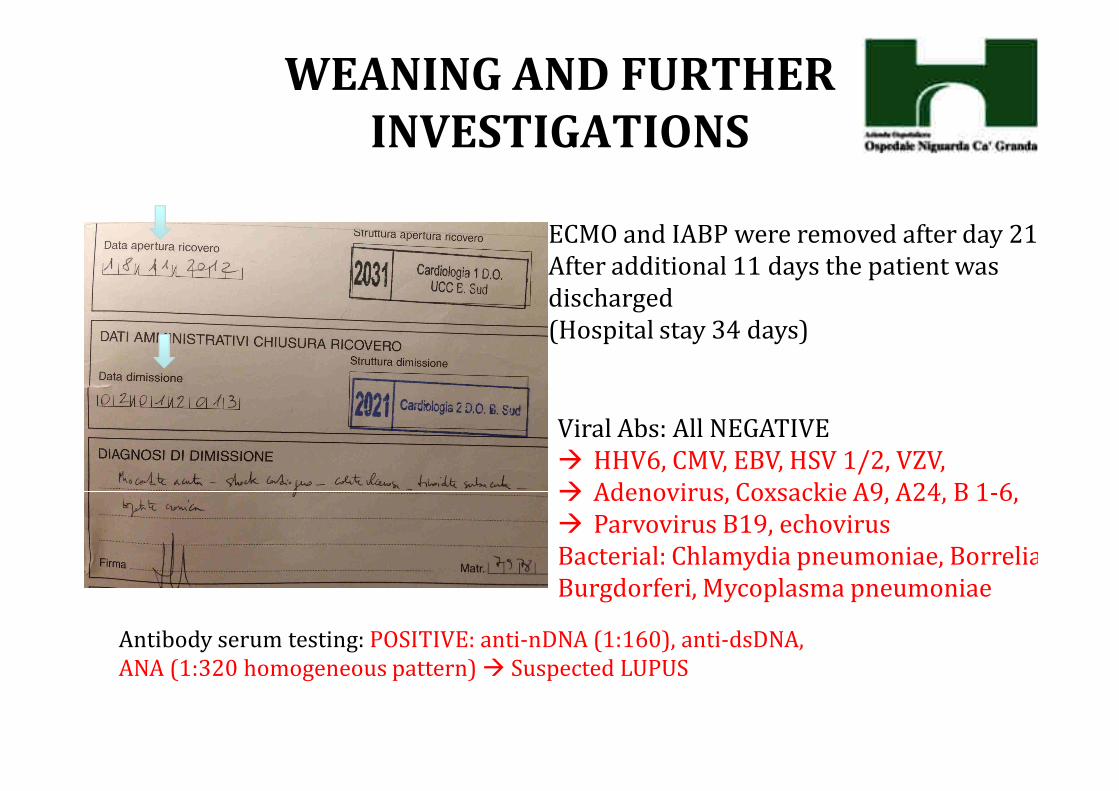
WEANING AND FURTHER
INVESTIGATIONS
ECMO and IABP were removed after day 21
After additional 11 days the patient was
discharged
(Hospital stay 34 days)
Viral Abs: All NEGATIVE
� HHV6, CMV, EBV, HSV 1/2, VZV,
� Adenovirus, Coxsackie A9, A24, B 1-6,
� Parvovirus B19, echovirus
Bacterial: Chlamydia pneumoniae, Borrelia
Burgdorferi, Mycoplasma pneumoniae
Antibody serum testing: POSITIVE: anti-nDNA (1:160), anti-dsDNA,
ANA (1:320 homogeneous pattern) � Suspected LUPUS
IMMUNOSUPPRESSIVE REGIMEN
Induction
Methylprednisolone (Solumedrol) i.v. 1 g qd x 3 days
Thymoglobuline i.v. 70 mg (1 mg/kg, day 1) + 56 mg
(0.8 mg/kg day 4) + 45 mg (0.6 mg/kg, day 7) [with CD (0.8 mg/kg day 4) + 45 mg (0.6 mg/kg, day 7) [with CD
3+ T cell count monitoring]
Cyclosporine 35 mg bd (day 2), 50+75 mg (day 3)+ 75
mg bd (day 4), 75+100 mg (day 5)
IMMUNOSUPPRESSIVE REGIMEN
Maintenance
Methylprednisolone i.v. 60 mg qd � 35 mg � oral
prednisone 35 mg
Cyclosporine (S. Neoral) Dosage 3-5 mg/kg/dieCyclosporine (S. Neoral) Dosage 3-5 mg/kg/die
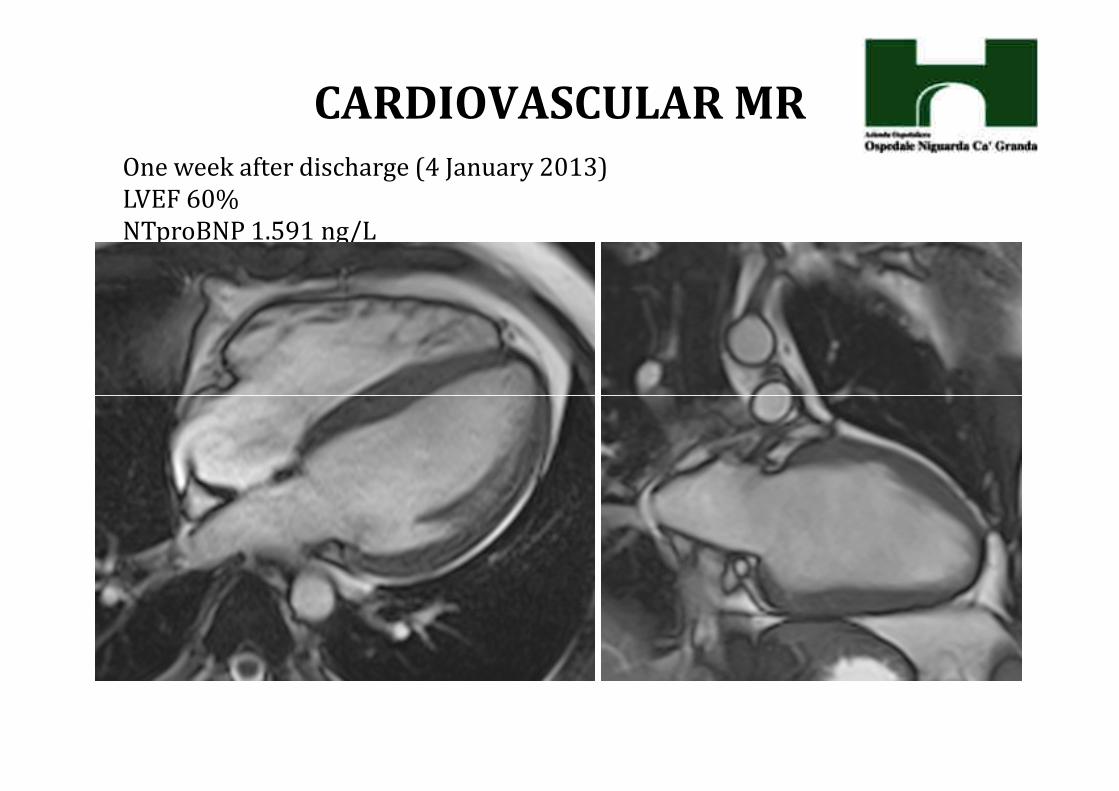
CARDIOVASCULAR MR
One week after discharge (4 January 2013)
LVEF 60%
NTproBNP 1.591 ng/L
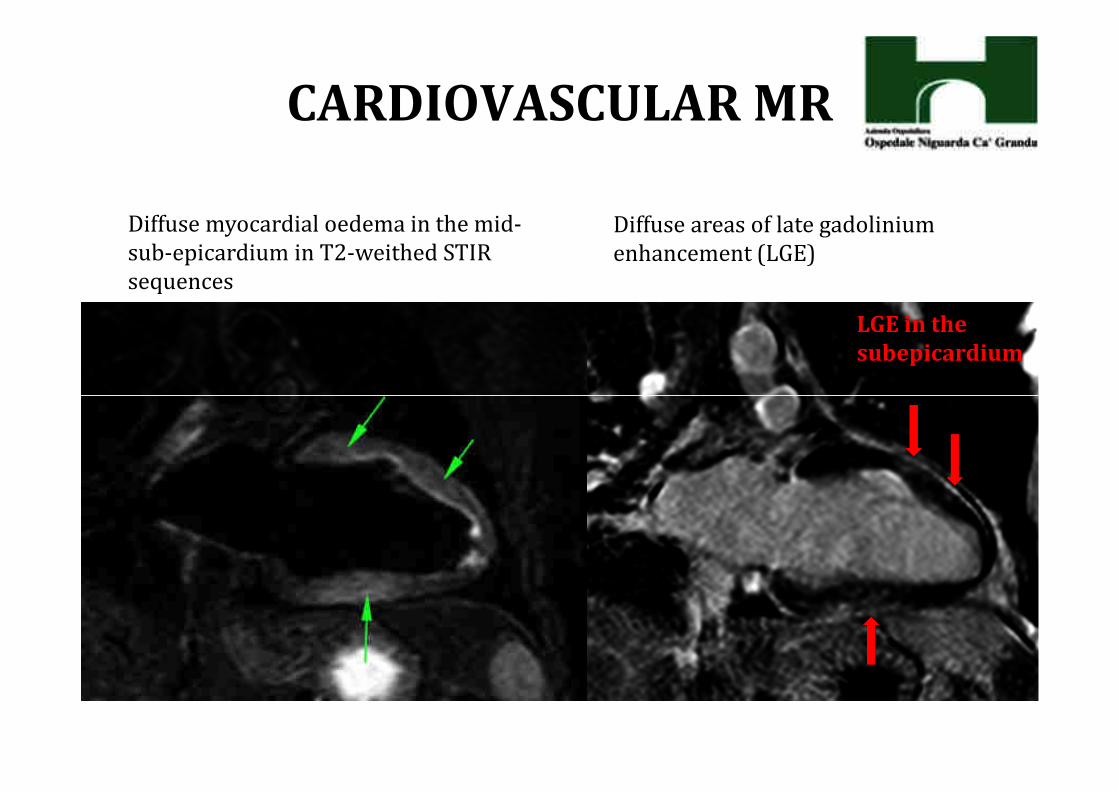
CARDIOVASCULAR MR
LGE in the
subepicardium
Diffuse myocardial oedema in the mid-
sub-epicardium in T2-weithed STIR
sequences
Diffuse areas of late gadolinium
enhancement (LGE)
• Cardiac function may recover completely in GCM
� but circulatory support (IABP+ECMO) to maintain
hemodynamics and oxygenation
• Immunosuppression may require days or weeks to
CAVEATs
• Immunosuppression may require days or weeks to
allow resolution of myocardial damage and
transplant-free survival
�but no specific raccomandation regarding drug
combination/dosage/duration
�Some studies suggest efficacy of combined
immunosuppresive regimen including
thymoglobulines
Increased risk of ventricular arrhythmias after GCM (consider ICD if ventricular arrhythmias are documented – 59% of GCM
transplant-free survivors experienced a sustained VT).1
Risk of recurrence of GCM when immunosuppressive
agents are weaned off (documented recurrence of GCM in native
CAVEATs
heart3 and also documented in Htx).1
Risk of subsequent dilated cardiomyopathy (DCM)(Transplant free survival: 69% at 1 year, 52% at 5 years ,1 in the GMC
Study Group: 22% at 5 years)2
2. Kandolin R, CIRC HF, 2013
4. Cooper, AJC 2008
3. GMC Study Group, JACC 2003
• Suspect the diagnosis of fulminant myocarditis due to GCM
(AHF+VT+ high levels of troponin)
• Transfer patients with unstable hemodynamics to
HTx/MCS centres
• Institute rapidly IABP and vaECMO if needed
CONCLUSIONS
• Confirm diagnosis of GCM by EMB
• Treat GCM with combined immunosuppression including
thymoglobines
• Enlist the patient if no recovery after 2 weeks or
complications due to vaECMO

Team:
M. Frigerio
M. Cipriani/
A. Garascia/
F. Oliva
HF Specialists
““DE GASPERISDE GASPERIS”” CARDIO CENTERCARDIO CENTERNIGUARDA CANIGUARDA CA’’ GRANDA HOSPITALGRANDA HOSPITAL
P. Gagliardone
Anesthetist
E. Bonacina
Pathologist
P. Pedrotti
CMR specialist
C.F.Russo
Cardiac Surgeon





























