Embed Size (px)
Citation preview

PRENATAL DIAGNOSIS, VOL. 7,377-38 1 (1987)
SHORT COMMUNICATION
MISDIAGNOSIS OF OMPHALOCELE ASSOCIATED WITH EDWARDS SYNDROME
AND CONGENITAL HEART DISEASE
N. COLLEY, P. D. KNOTT AND s. J. GOULD* Department of Obstetrics and Gynaecology, *Department of Histopathology. School of Medicine.
University College London, University Street, London WCl . U.K.
SUMMARY We present a case in which an apparent omphalocele, diagnosed at 30 weeks gestation by ultrasound, led to identification of fetal trisomy 18 and congenital heart disease. At delivery, the fetus had the features of trisomy 18 and congenital heart disease but the omphalocele was absent. We suggest that the appearances seen are easily confused with a small omphalo- cele and could potentially result in unnecessary further investigations being performed.
KEY WORDS Omphalocele Umbilical hernia Prenatal diagnosis
INTRODUCTION
Defects of the fetal anterior abdominal wall such as omphalocele and gastroschisis are now often diagnosed by ultrasound. The ability to diagnose these lesions prenatally is important for two reasons. First, omphalocele is often associated with other problems, particularly abnormal fetal karyotype and congenital heart disease. Second, once other anomalies are excluded the delivery and post natal care can be carefully planned.
Although abdominal wall defects may be identified during maternal serum alpha- fetoprotein screening or routine second trimester ultrasound examinations, they may also present later in pregnancy when termination is no longer possible, but knowledge of a severe associated anomaly may prevent unnecessary intervention in labour. We report a case where the ultrasound diagnosis of an omphalocele led to further investigations which disclosed fetal trisomy 18 and a congenital heart defect. At delivery, however, the fetal abdominal wall was normal.
CASE REPORT
A 30-year-old primagravid patient was referred for detailed ultrasound scan at 31 weeks gestation because of polyhydramnios. The pregnancy had hitherto been con- sidered normal. An ultrasound scan at 17 weeks gestation had confirmed the patient’s dates and a serum alpha-fetoprotein estimation at the same time was within normal limits.
0 197-385 1/87/050377-05$05.00 0 1987 by John Wiley & Sons, Ltd.
Received 25 March 1986 Revised 18 August 1986
Accepted 25 August 1986
378 N. COLLEY ET. AL.
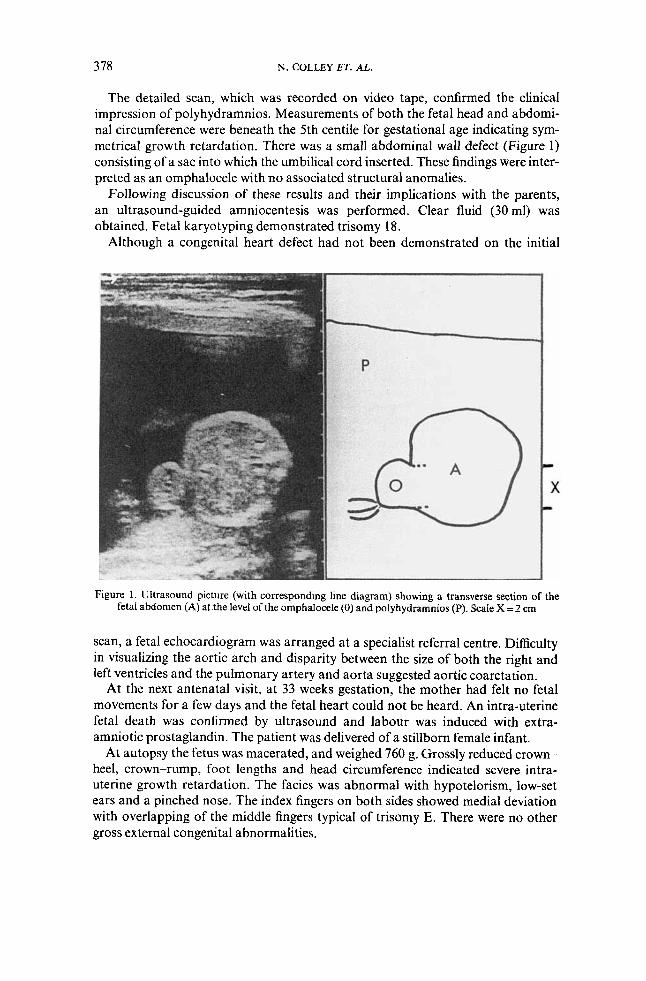
The detailed scan, which was recorded on video tape, confirmed the clinical impression of polyhydramnios. Measurements of both the fetal head and abdomi- nal circumference were beneath the 5th centile for gestational age indicating sym- metrical growth retardation. There was a small abdominal wall defect (Figure 1) consisting of a sac into which the umbilical cord inserted. These findings were inter- preted as an omphalocele with no associated structural anomalies.
Following discussion of these results and their implications with the parents, an ultrasound-guided amniocentesis was performed. Clear fluid (30 ml) was obtained. Fetal karyotyping demonstrated trisomy 18.
Although a congenital heart defect had not been demonstrated on the initial
Figure 1. Ultrasound picture (with corresponding line diagram) showing a transverse section of the fetal abdomen (A) atthe level of the omphaIocele (0) and poiyhydramnios (P). Scale X=2 cm
scan, a fetal echocardiogram was arranged at a specialist referral centre. Difficulty in visualizing the aortic arch and disparity between the size of both the right and left ventricles and the pulmonary artery and aorta suggested aortic coarctation.
At the next antenatal visit, at 33 weeks gestation, the mother had felt no fetal movements for a few days and the fetal heart could not be heard. An intra-uterine fetal death was confirmed by ultrasound and labour was induced with extra- amniotic prostaglandin. The patient was delivered of a stillborn female infant.
At autopsy the fetus was macerated, and weighed 760 g. Grossly reduced crown- heel, crown-rump, foot lengths and head circumference indicated severe intra- uterine growth retardation. The facies was abnormal with hypotelorism, low-set ears and a pinched nose. The index fingers on both sides showed medial deviation with overlapping of the middle fingers typical of trisomy E. There were no other gross external congenital abnormalities.
MISDIAGNOSIS OF OMPHALOCELE 379
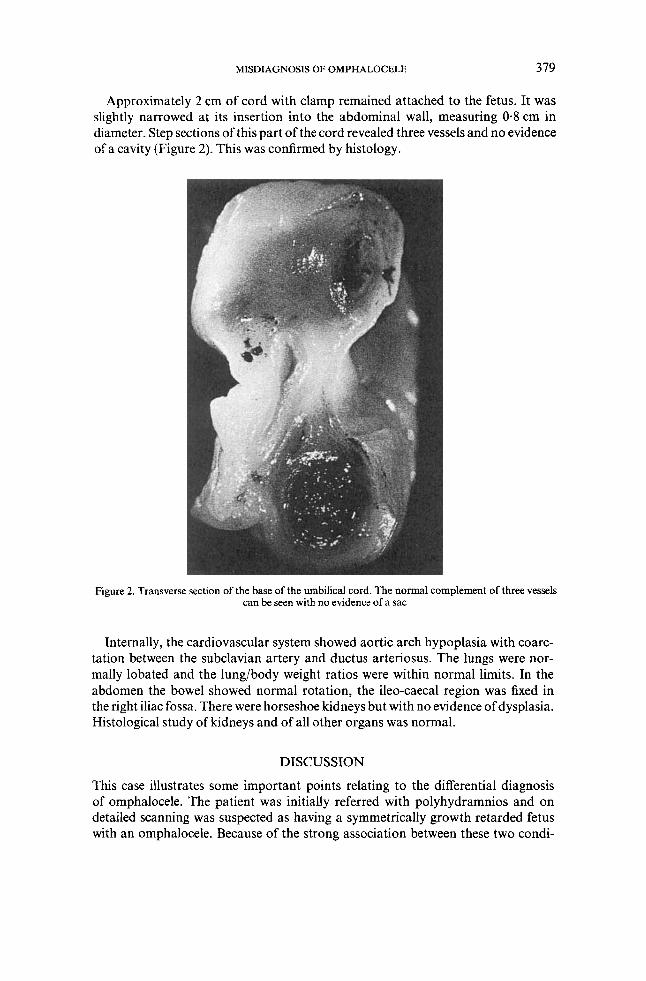
Approximately 2 cm of cord with clamp remained attached to the fetus. It was slightly narrowed at its insertion into the abdominal wall, measuring 0.8 cm in diameter. Step sections of this part of the cord revealed three vessels and no evidence of a cavity (Figure 2). This was confirmed by histology.
Figure 2. Transverse section of the base of the umbilical cord. The normal complement of three vessels can be seen with no evidence of a sac
Internally, the cardiovascular system showed aortic arch hypoplasia with coarc- tation between the subclavian artery and ductus arteriosus. The lungs were nor- mally lobated and the lung/body weight ratios were within normal limits. In the abdomen the bowel showed normal rotation, the ileo-caecal region was fixed in the right iliac fossa. There were horseshoe kidneys but with no evidence of dysplasia. Histological study of kidneys and of all other organs was normal.
DISCUSSION
This case illustrates some important points relating to the differential diagnosis of omphalocele. The patient was initially referred with polyhydramnios and on detailed scanning was suspected as having a symmetrically growth retarded fetus with an omphalocele. Because of the strong association between these two condi-
380 N. COLLEY ET. AL.
tions and chromosomal abnormalities, amniocentesis was performed (Davidson er af., 1984; Nicholaides et al., 1986). Even in the absence of achromosomal abnor- mality, ompholoceles may be associated with a cardiac malformation (Seashore, 1978), the commonest of which is a ventricular septa1 defect. This may be part of a more complex anomaly (Crawford et al., 1985), and to enable more accurate assessment, the patient was referred to a specialist centre for fetal echocardiography (Allan et al., 1984). Both the further investigations initiated following the diagnosis of omphalocele proved of value; the fetus was trisomy 18 and had a congenital cardiac malformation.
However, when the infant was delivered the abdominal wall was normal. Critical review of the ultrasound video tapes (Mr J.M. Pearce, St. George’s Hospital) did not indicate the structure seen at the base of the cord to be an artefact. The sac is well seen in continuity with the abdominal wall and the cord inserts into it, these being the well described ultrasonic appearances of an omphalocele (Nielsen et al., 1985).
One possible explanation for these findings is that this was a small omphalocele or umbilical hernia (Cambell and Pearce, 1983) which reduced in the interval between final ultrasound and delivery. However, the briefness of this interval and the absence of any sign of an omphalocele at delivery makes this explanation unlikely.
A more probable explanation is that a relatively thickened umbilical cord in association with a severely growth retarded abdomen led to a misinterpretation of the ultrasound findings. This is of importance in that a misdiagnosis of an omphalocele may led to unnecessary further investigations. However, in this instance, the ‘false positive’ finding resulted in the diagnosis of trisomy 18 and the subsequent investigations proved to be justified.
ACKNOWLEDGEMENTS
We should like to thank Miss G. Lachelin, Consultant Obstetrician UCH, for allowing us to report this case, Dr M. Lucas, Department of Genetics UCH for the chromosomal studies and Mr Malcolm Pearce, Senior Lecturer St. George’s Hospital Medical School for reviewing the ultrasound tapes. We would also like to thank Dr Lindsey Allen at Guys Hospital for performing the echocardiography.
REFERENCES
Allan, L.D., Crawford, D.C., Anderson, R.H., Tynan, M. (1984). Electrocardiographic and anatomical correlates in fetal congenital heart disease, Br. Heart. J . 52,542-548.
Campbell, S., Pearce, J.M. (1983). The prenatal diagnosis of fetal structural anomalies by ultrasound. In : Campbell, S . (Ed.). Clinics in Obstetrics and Gynaecology. Ultrasound in Obstetrics and Gynaecology : Recent Advances, London, Philadelphia, Toronto : W.B. Saunders Company Ltd, 475-506.
Crawford, D.C., Chapman, MG., Allan, L.D. (1985). Echocardiography in the investigation of anterior abdominal wall defects in the fetus, Br. J. Obstet. Gynaecol., 92, 1034-1036.

MISDIAGNOSIS OF OMPHALOCELE 38 I
Davidson, J.M. Johnson, Jr., T.R.B., Rigdon, D.T., Thompson, B.H. (1984). Gastroschisis and omphalocele : Prenatal diagnosis and perinatal management, Prenat. diagn., 4,
Nicolaides, K.H., Rodeck, C.H., Gosden, C.M. (1986). Rapid karyotyping in non-lethal
Nielson, L.B., Bang, J., Norgaard-Pedersen,, B. (1985). Prenatal diagnosis of omphalocele
Seashore, J.H. (1978). Congenital abdominal wall defects, Clinics in Perinatology, 5,61-77.
355-363.
fetal malformations, Lancet, i, 283-287.
and gastroschisis by ultrasonography, Prenat. diagn., 5,38 1-392.