Embed Size (px)
Citation preview
Introduction to TBCP
A primary care guide project
by Dr Gerard Loh
MO
KK Bandar Miri
Acknowledgements:
Dr Wong Yong Kai, MO, TBCP KK Miri
TBCP Staff, KK MIRI
Note: These guides serve as introductory notes to the new MO in TBCP setting, always refer to CPG for more precise
guidelines.
The Primary Care Guide Project 2013
www.myhow.wordpress.com
TUBERCULOSIS
Cases:
1) New cases PTB Never treated for TB
2) Follow up – Intensive phase / Maintenance / Surveillance
3) Relapse
- D/S +ve relapse : after cured, came back with smear +ve
- D/S –ve relapse : after cured, came back with symptoms or CXR features
4) Chronic case remain smear +ve despite re-treatment
5) Treament failure after 5/12 treatment remain smear +ve
6) Treatment after interruption defaulter > 2/12 with smear +ve
7) Contact Tracing
Tuberculosis
- Pulmonary - Extra-pulmonary
Clinical:
Cough > 2/52, with sputum +/- blood stained
LOW/ LOA
Fever with chills, night sweats
TB Lympadenitis
Ix: FNAC / excisional biopsy
TB Pleura
Ix: thoracocentesis/pleural tapping for AFB
Radiological:
- Lesions or hazinesss in upper lobe, +/- cavities
TB Genitourinary
Ix: Urine AFB
Bacteriological
Sputum AFB +ve or C&S MTB +ve
TB Meningitis
Ix: CSF AFB
Immunological:
Mantoux > 10mm
ESR up to 100+
TB bone/joints
Miliary TB
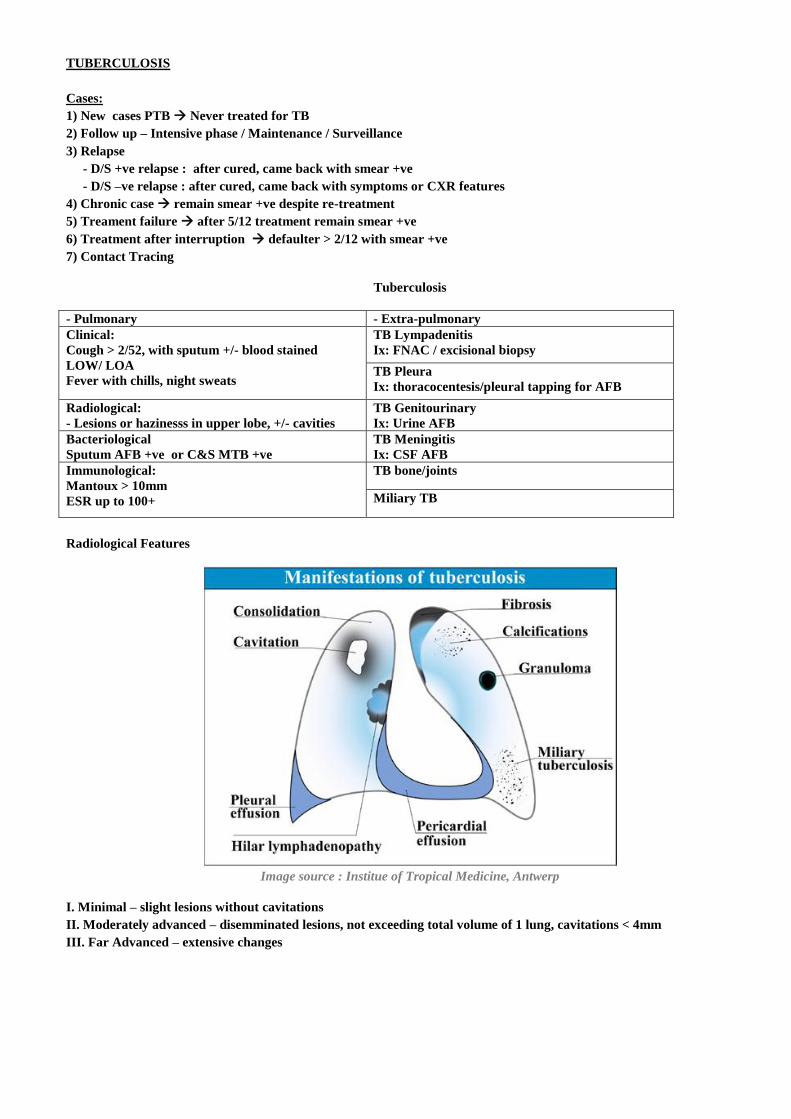
Radiological Features
Image source : Institue of Tropical Medicine, Antwerp
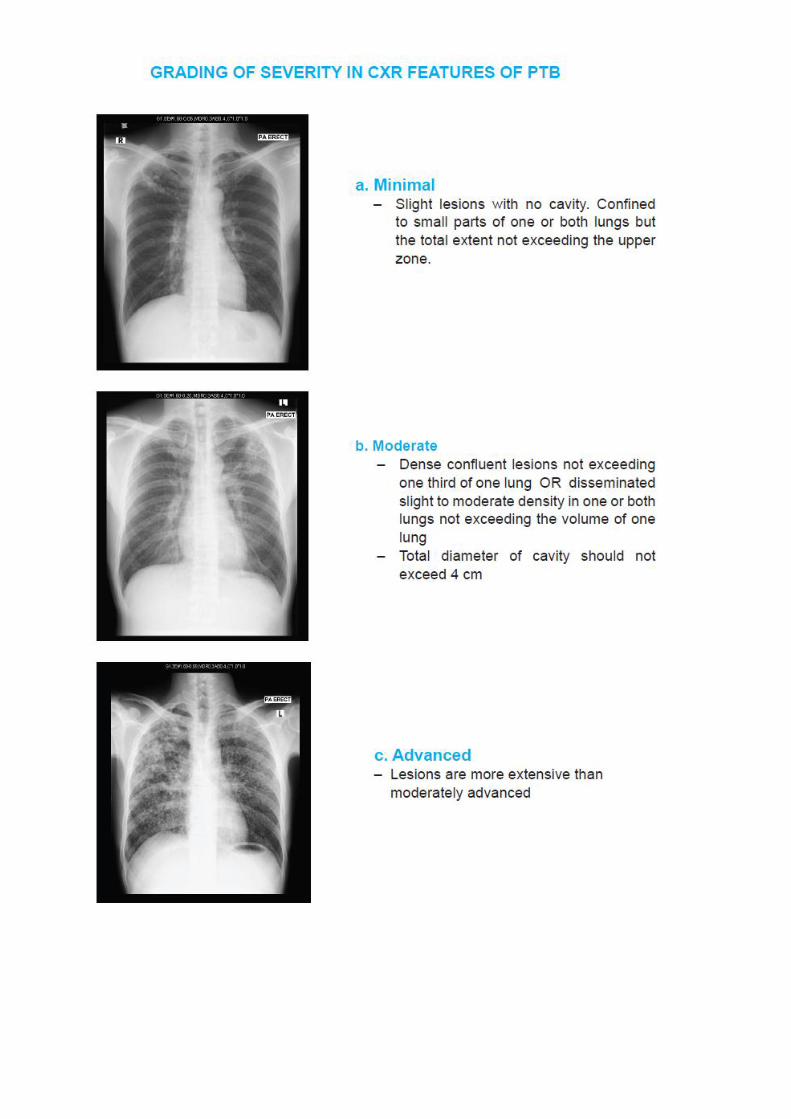
I. Minimal – slight lesions without cavitations
II. Moderately advanced – disemminated lesions, not exceeding total volume of 1 lung, cavitations < 4mm
III. Far Advanced – extensive changes
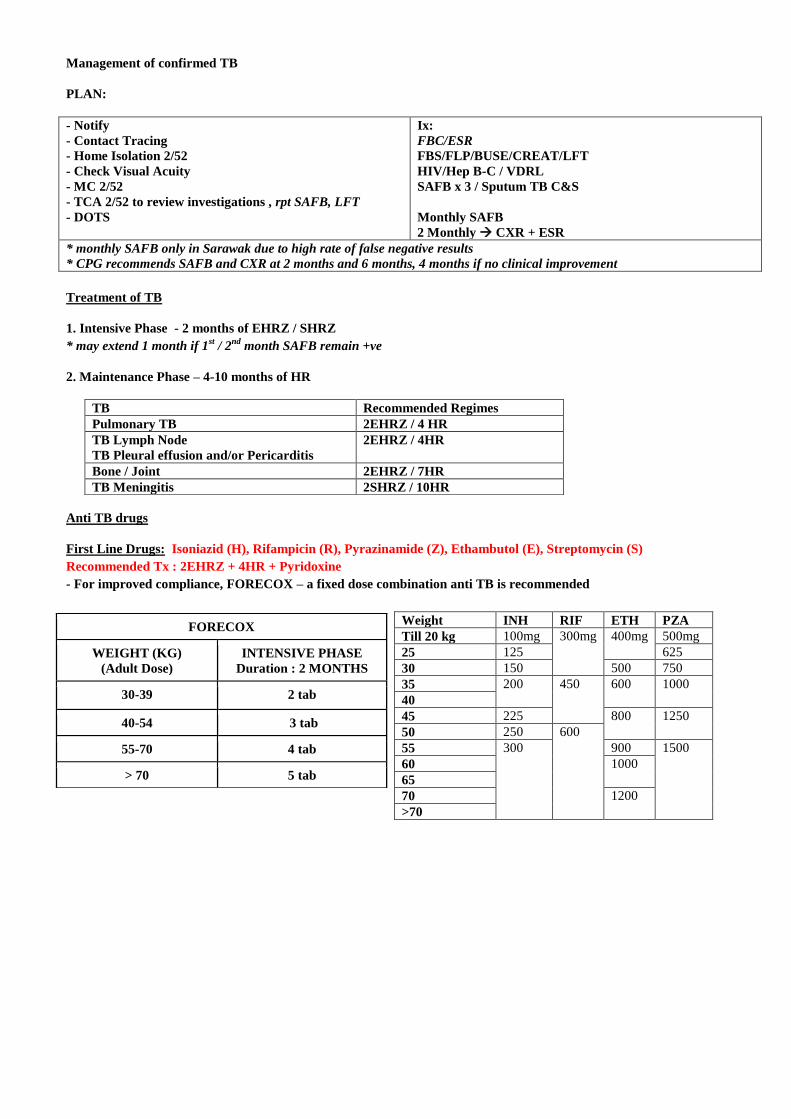
Management of confirmed TB
PLAN:
- Notify
- Contact Tracing
- Home Isolation 2/52
- Check Visual Acuity
- MC 2/52
- TCA 2/52 to review investigations , rpt SAFB, LFT
- DOTS
Ix:
FBC/ESR
FBS/FLP/BUSE/CREAT/LFT
HIV/Hep B-C / VDRL
SAFB x 3 / Sputum TB C&S
Monthly SAFB
2 Monthly CXR + ESR
* monthly SAFB only in Sarawak due to high rate of false negative results
* CPG recommends SAFB and CXR at 2 months and 6 months, 4 months if no clinical improvement
Treatment of TB
1. Intensive Phase - 2 months of EHRZ / SHRZ
* may extend 1 month if 1st / 2
nd month SAFB remain +ve
2. Maintenance Phase – 4-10 months of HR
Anti TB drugs
First Line Drugs: Isoniazid (H), Rifampicin (R), Pyrazinamide (Z), Ethambutol (E), Streptomycin (S)
Recommended Tx : 2EHRZ + 4HR + Pyridoxine
- For improved compliance, FORECOX – a fixed dose combination anti TB is recommended
TB Recommended Regimes
Pulmonary TB 2EHRZ / 4 HR
TB Lymph Node
TB Pleural effusion and/or Pericarditis
2EHRZ / 4HR
Bone / Joint 2EHRZ / 7HR
TB Meningitis 2SHRZ / 10HR
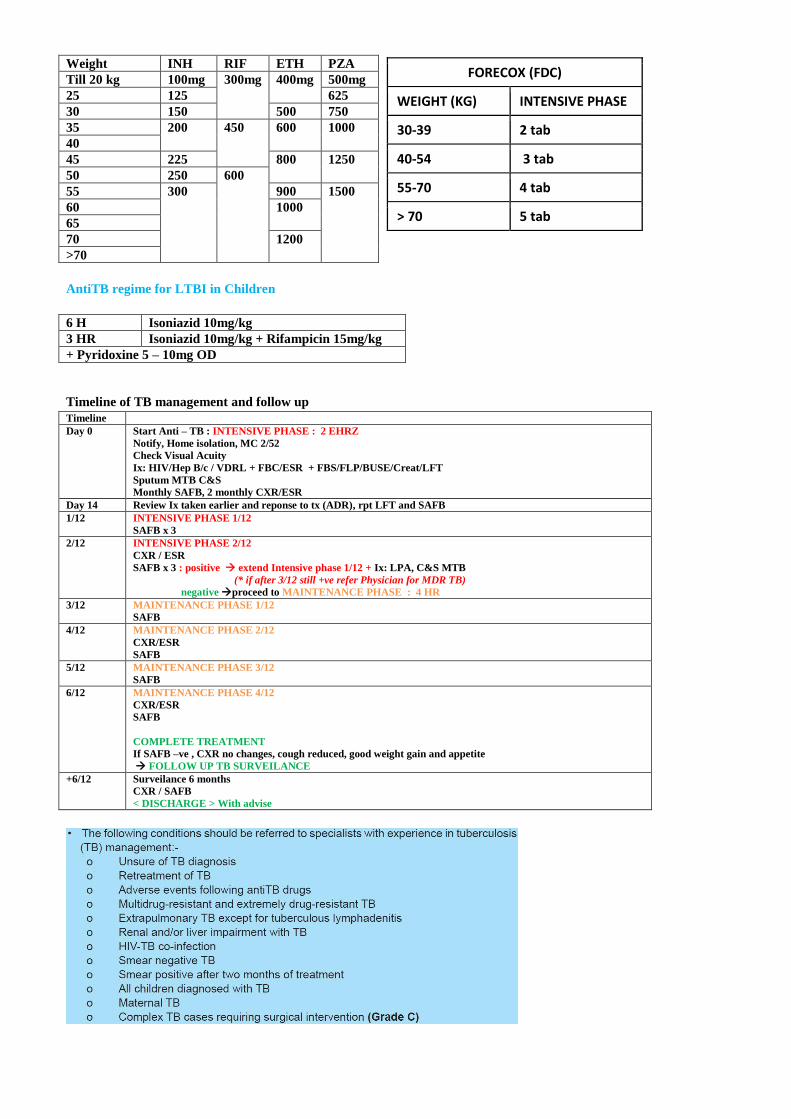
FORECOX
WEIGHT (KG)
(Adult Dose)
INTENSIVE PHASE
Duration : 2 MONTHS
30-39 2 tab
40-54 3 tab
55-70 4 tab
> 70 5 tab
Weight INH RIF ETH PZA
Till 20 kg 100mg 300mg 400mg 500mg
25 125 625
30 150 500 750
35 200
450 600 1000
40
45 225 800 1250
50 250 600
55 300 900 1500
60 1000
65
70 1200
>70
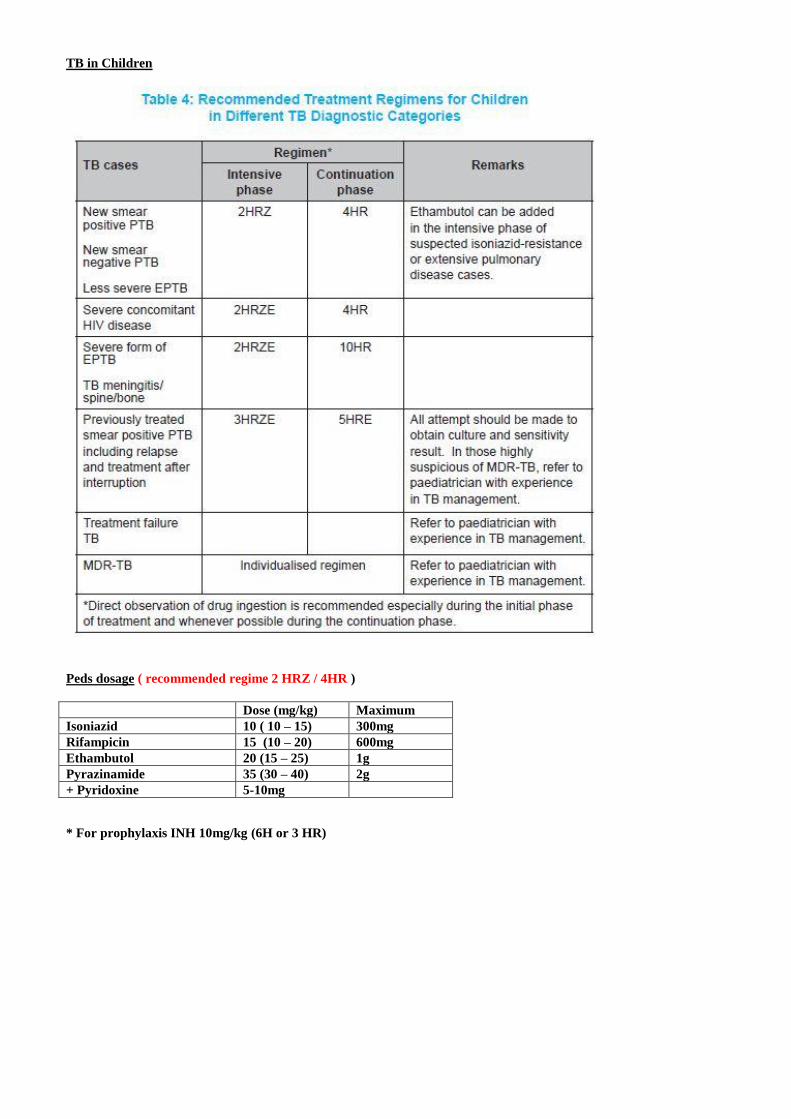
TB in Children
Peds dosage ( recommended regime 2 HRZ / 4HR )
* For prophylaxis INH 10mg/kg (6H or 3 HR)
Dose (mg/kg) Maximum
Isoniazid 10 ( 10 – 15) 300mg
Rifampicin 15 (10 – 20) 600mg
Ethambutol 20 (15 – 25) 1g
Pyrazinamide 35 (30 – 40) 2g
+ Pyridoxine 5-10mg
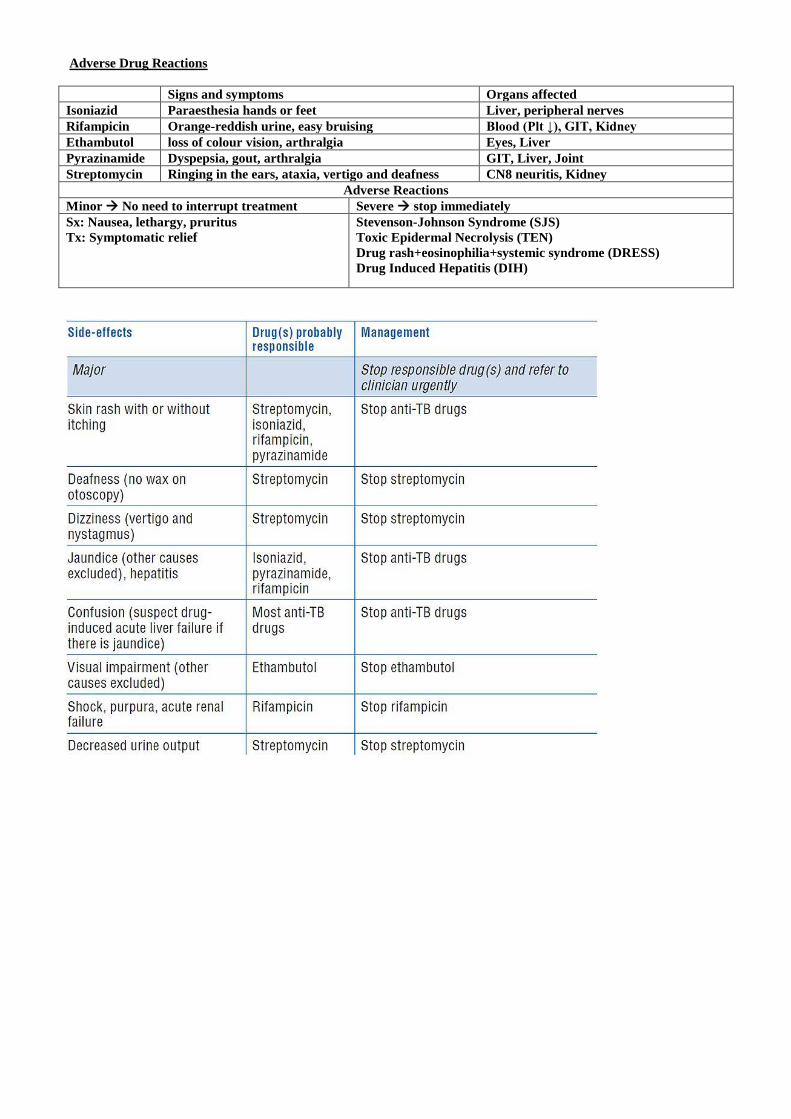
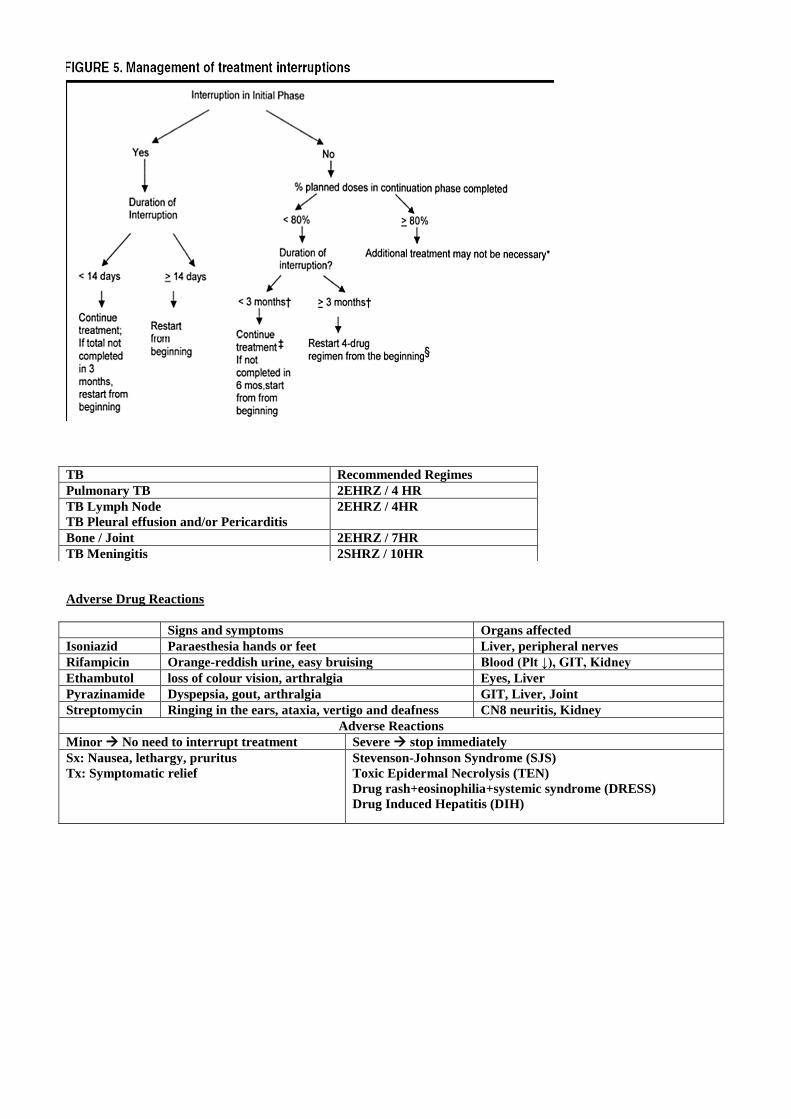
Adverse Drug Reactions
Signs and symptoms Organs affected
Isoniazid Paraesthesia hands or feet Liver, peripheral nerves
Rifampicin Orange-reddish urine, easy bruising Blood (Plt ↓), GIT, Kidney
Ethambutol loss of colour vision, arthralgia Eyes, Liver
Pyrazinamide Dyspepsia, gout, arthralgia GIT, Liver, Joint
Streptomycin Ringing in the ears, ataxia, vertigo and deafness CN8 neuritis, Kidney
Adverse Reactions
Minor No need to interrupt treatment Severe stop immediately
Sx: Nausea, lethargy, pruritus
Tx: Symptomatic relief
Stevenson-Johnson Syndrome (SJS)
Toxic Epidermal Necrolysis (TEN)
Drug rash+eosinophilia+systemic syndrome (DRESS)
Drug Induced Hepatitis (DIH)
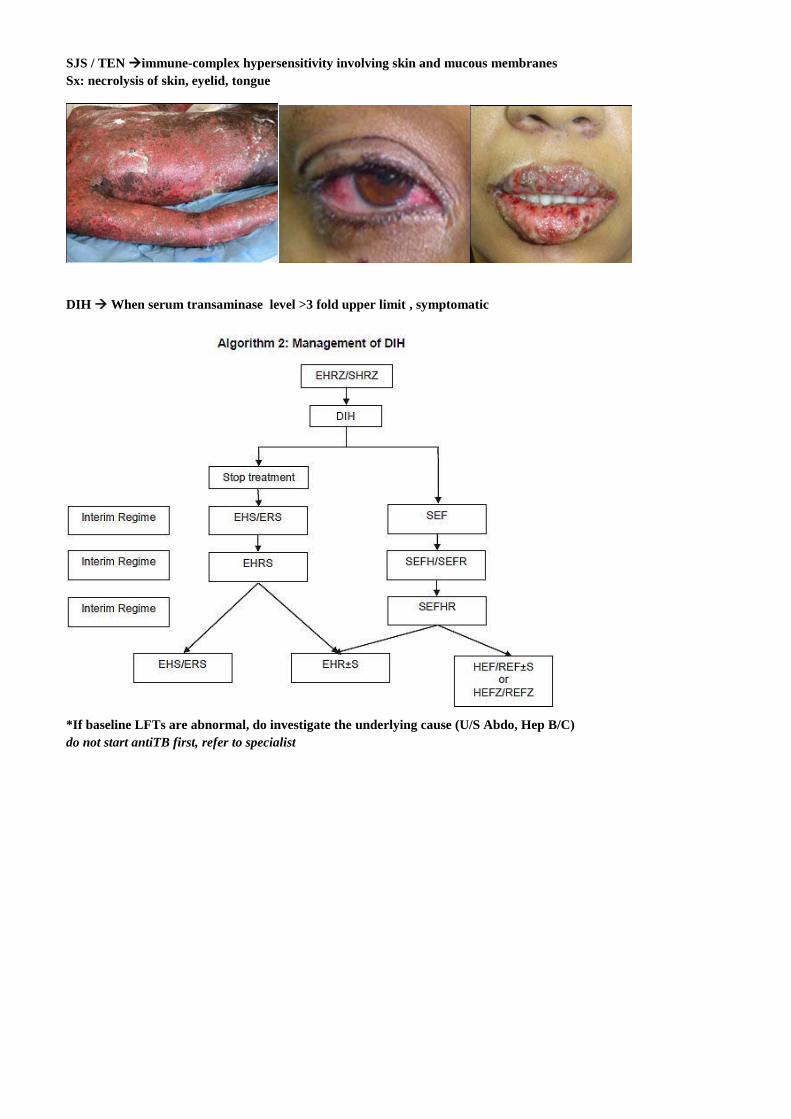
SJS / TEN immune-complex hypersensitivity involving skin and mucous membranes
Sx: necrolysis of skin, eyelid, tongue
DIH When serum transaminase level >3 fold upper limit , symptomatic
*If baseline LFTs are abnormal, do investigate the underlying cause (U/S Abdo, Hep B/C)
do not start antiTB first, refer to specialist
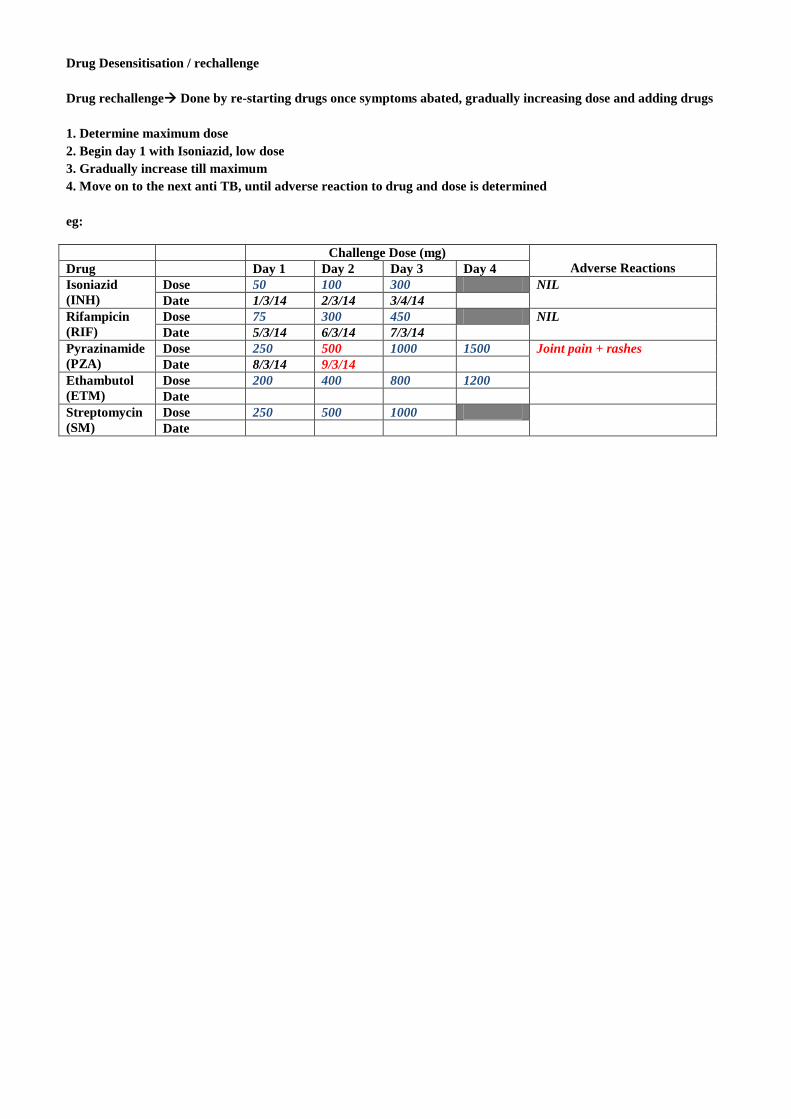
Drug Desensitisation / rechallenge
Drug rechallenge Done by re-starting drugs once symptoms abated, gradually increasing dose and adding drugs
1. Determine maximum dose
2. Begin day 1 with Isoniazid, low dose
3. Gradually increase till maximum
4. Move on to the next anti TB, until adverse reaction to drug and dose is determined
eg:
Challenge Dose (mg)
Adverse Reactions Drug Day 1 Day 2 Day 3 Day 4
Isoniazid
(INH)
Dose 50 100 300 NIL
Date 1/3/14 2/3/14 3/4/14
Rifampicin
(RIF)
Dose 75 300 450 NIL
Date 5/3/14 6/3/14 7/3/14
Pyrazinamide
(PZA)
Dose 250 500 1000 1500 Joint pain + rashes
Date 8/3/14 9/3/14
Ethambutol
(ETM)
Dose 200 400 800 1200
Date
Streptomycin
(SM)
Dose 250 500 1000
Date
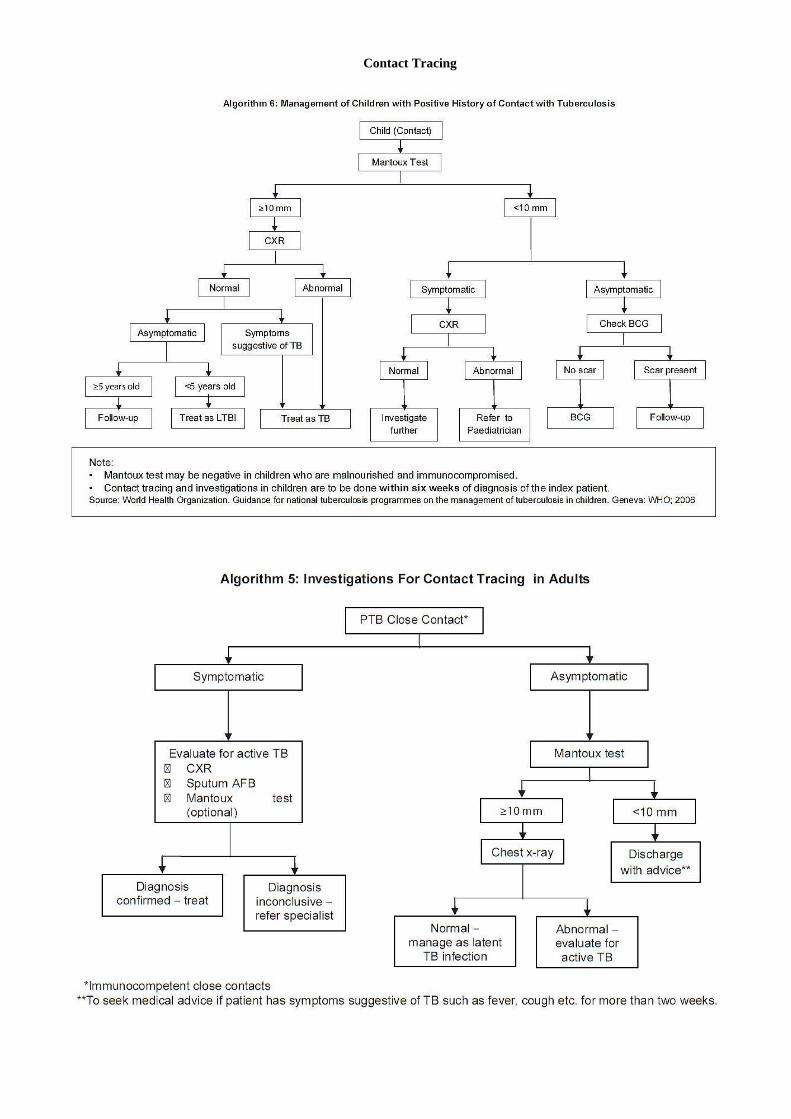
Contact Tracing
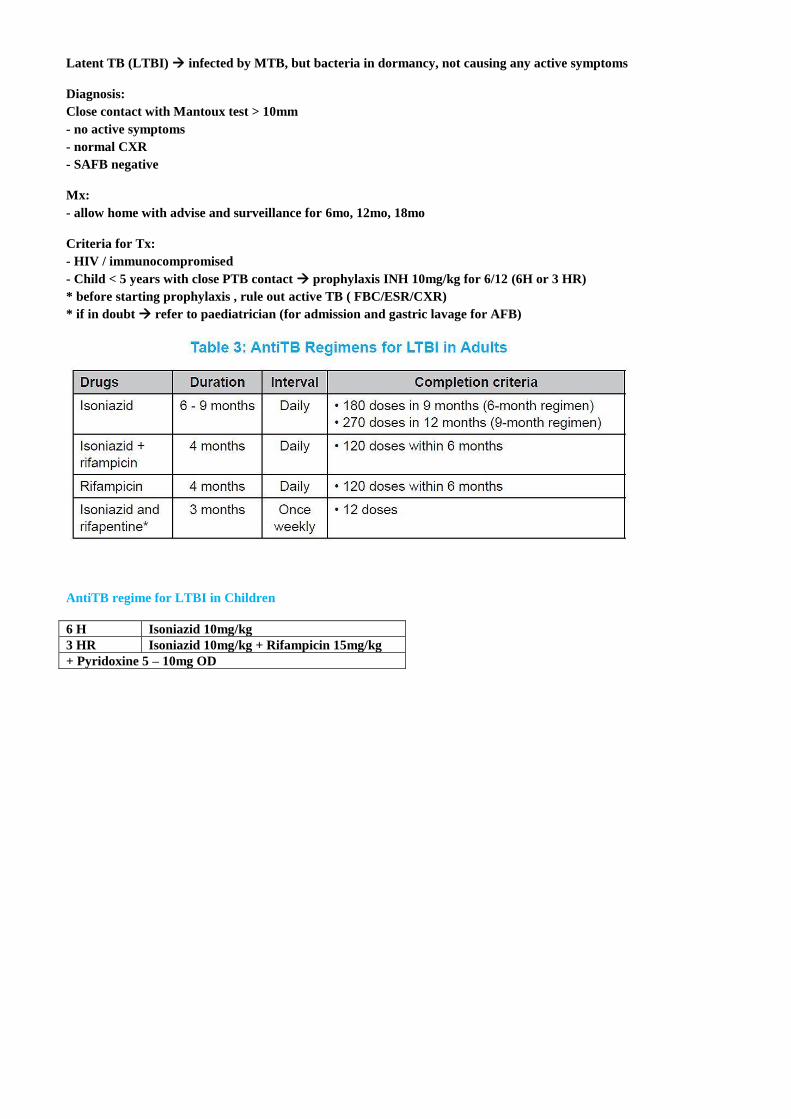
Latent TB (LTBI) infected by MTB, but bacteria in dormancy, not causing any active symptoms
Diagnosis:
Close contact with Mantoux test > 10mm
- no active symptoms
- normal CXR
- SAFB negative
Mx:
- allow home with advise and surveillance for 6mo, 12mo, 18mo
Criteria for Tx:
- HIV / immunocompromised
- Child < 5 years with close PTB contact prophylaxis INH 10mg/kg for 6/12 (6H or 3 HR)
* before starting prophylaxis , rule out active TB ( FBC/ESR/CXR)
* if in doubt refer to paediatrician (for admission and gastric lavage for AFB)
AntiTB regime for LTBI in Children
6 H Isoniazid 10mg/kg
3 HR Isoniazid 10mg/kg + Rifampicin 15mg/kg
+ Pyridoxine 5 – 10mg OD
Weight INH RIF ETH PZA
Till 20 kg 100mg 300mg 400mg 500mg
25 125 625
30 150 500 750
35 200
450 600 1000
40
45 225 800 1250
50 250 600
55 300 900 1500
60 1000
65
70 1200
>70
AntiTB regime for LTBI in Children
6 H Isoniazid 10mg/kg
3 HR Isoniazid 10mg/kg + Rifampicin 15mg/kg
+ Pyridoxine 5 – 10mg OD
Timeline of TB management and follow up
Timeline
Day 0 Start Anti – TB : INTENSIVE PHASE : 2 EHRZ
Notify, Home isolation, MC 2/52
Check Visual Acuity
Ix: HIV/Hep B/c / VDRL + FBC/ESR + FBS/FLP/BUSE/Creat/LFT
Sputum MTB C&S
Monthly SAFB, 2 monthly CXR/ESR
Day 14 Review Ix taken earlier and reponse to tx (ADR), rpt LFT and SAFB
1/12 INTENSIVE PHASE 1/12
SAFB x 3
2/12 INTENSIVE PHASE 2/12
CXR / ESR
SAFB x 3 : positive extend Intensive phase 1/12 + Ix: LPA, C&S MTB
(* if after 3/12 still +ve refer Physician for MDR TB)
negative proceed to MAINTENANCE PHASE : 4 HR
3/12 MAINTENANCE PHASE 1/12
SAFB
4/12 MAINTENANCE PHASE 2/12
CXR/ESR
SAFB
5/12 MAINTENANCE PHASE 3/12
SAFB
6/12 MAINTENANCE PHASE 4/12
CXR/ESR
SAFB
COMPLETE TREATMENT
If SAFB –ve , CXR no changes, cough reduced, good weight gain and appetite
FOLLOW UP TB SURVEILANCE
+6/12 Surveilance 6 months
CXR / SAFB
< DISCHARGE > With advise
FORECOX (FDC)
WEIGHT (KG) INTENSIVE PHASE
30-39 2 tab
40-54 3 tab
55-70 4 tab
> 70 5 tab
Adverse Drug Reactions
Signs and symptoms Organs affected
Isoniazid Paraesthesia hands or feet Liver, peripheral nerves
Rifampicin Orange-reddish urine, easy bruising Blood (Plt ↓), GIT, Kidney
Ethambutol loss of colour vision, arthralgia Eyes, Liver
Pyrazinamide Dyspepsia, gout, arthralgia GIT, Liver, Joint
Streptomycin Ringing in the ears, ataxia, vertigo and deafness CN8 neuritis, Kidney
Adverse Reactions
Minor No need to interrupt treatment Severe stop immediately
Sx: Nausea, lethargy, pruritus
Tx: Symptomatic relief
Stevenson-Johnson Syndrome (SJS)
Toxic Epidermal Necrolysis (TEN)
Drug rash+eosinophilia+systemic syndrome (DRESS)
Drug Induced Hepatitis (DIH)
TB Recommended Regimes
Pulmonary TB 2EHRZ / 4 HR
TB Lymph Node
TB Pleural effusion and/or Pericarditis
2EHRZ / 4HR
Bone / Joint 2EHRZ / 7HR
TB Meningitis 2SHRZ / 10HR
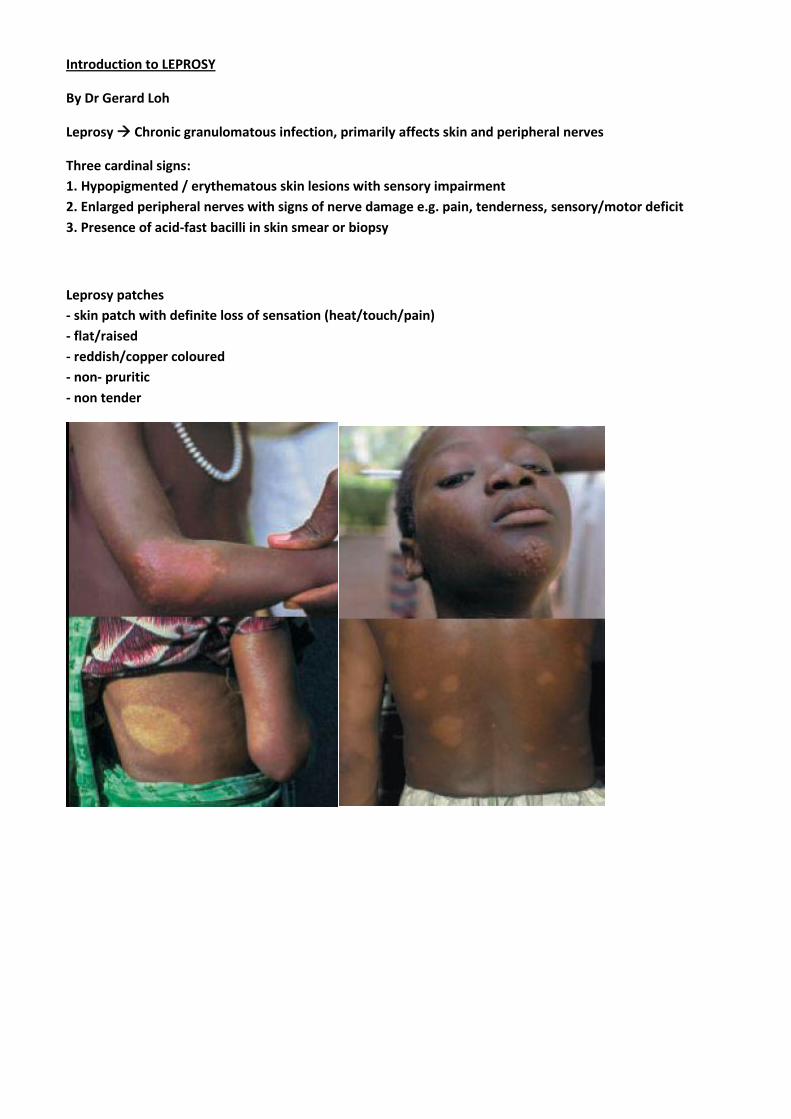
Introduction to LEPROSY
By Dr Gerard Loh
Leprosy Chronic granulomatous infection, primarily affects skin and peripheral nerves
Three cardinal signs:
1. Hypopigmented / erythematous skin lesions with sensory impairment
2. Enlarged peripheral nerves with signs of nerve damage e.g. pain, tenderness, sensory/motor deficit
3. Presence of acid-fast bacilli in skin smear or biopsy
Leprosy patches
- skin patch with definite loss of sensation (heat/touch/pain)
- flat/raised
- reddish/copper coloured
- non- pruritic
- non tender
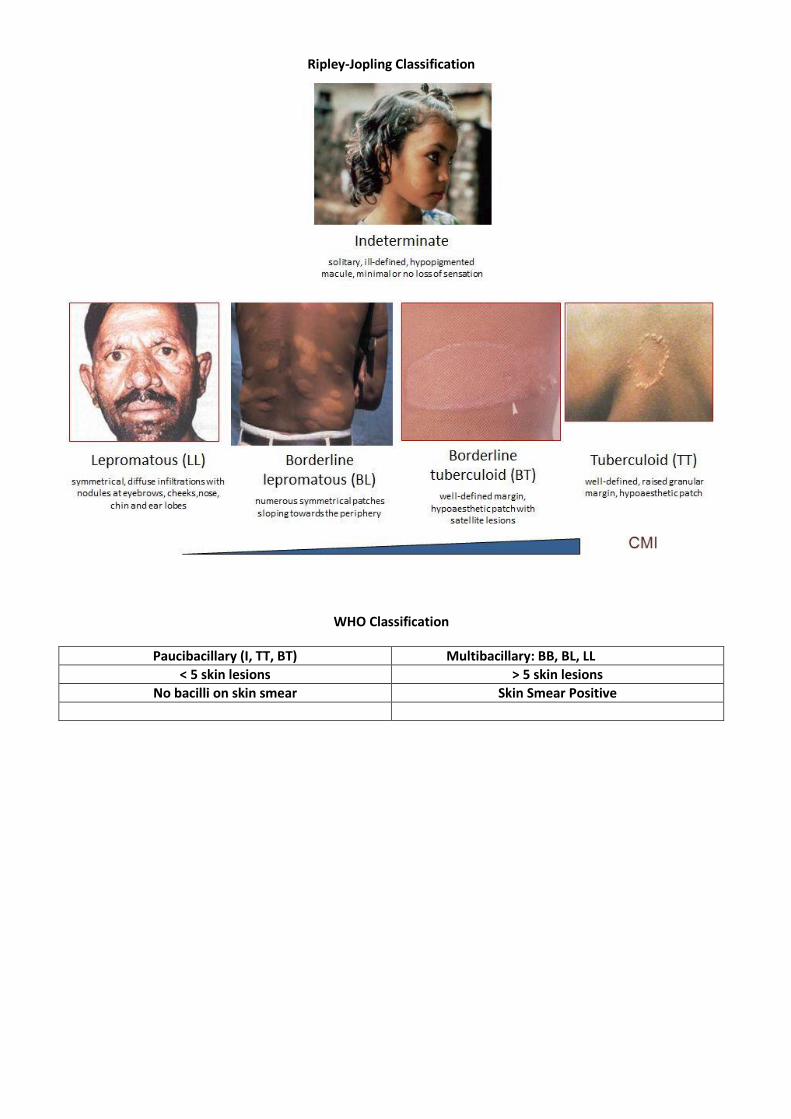
Ripley-Jopling Classification
WHO Classification
Paucibacillary (I, TT, BT) Multibacillary: BB, BL, LL
< 5 skin lesions > 5 skin lesions
No bacilli on skin smear Skin Smear Positive
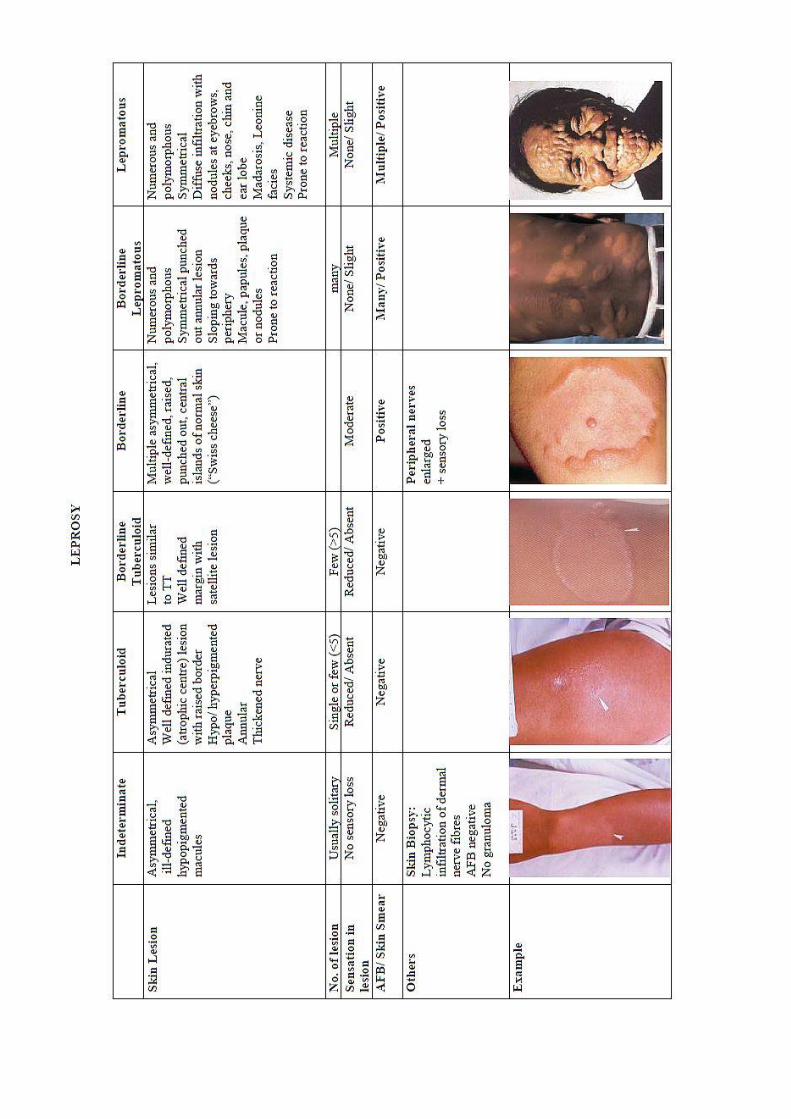
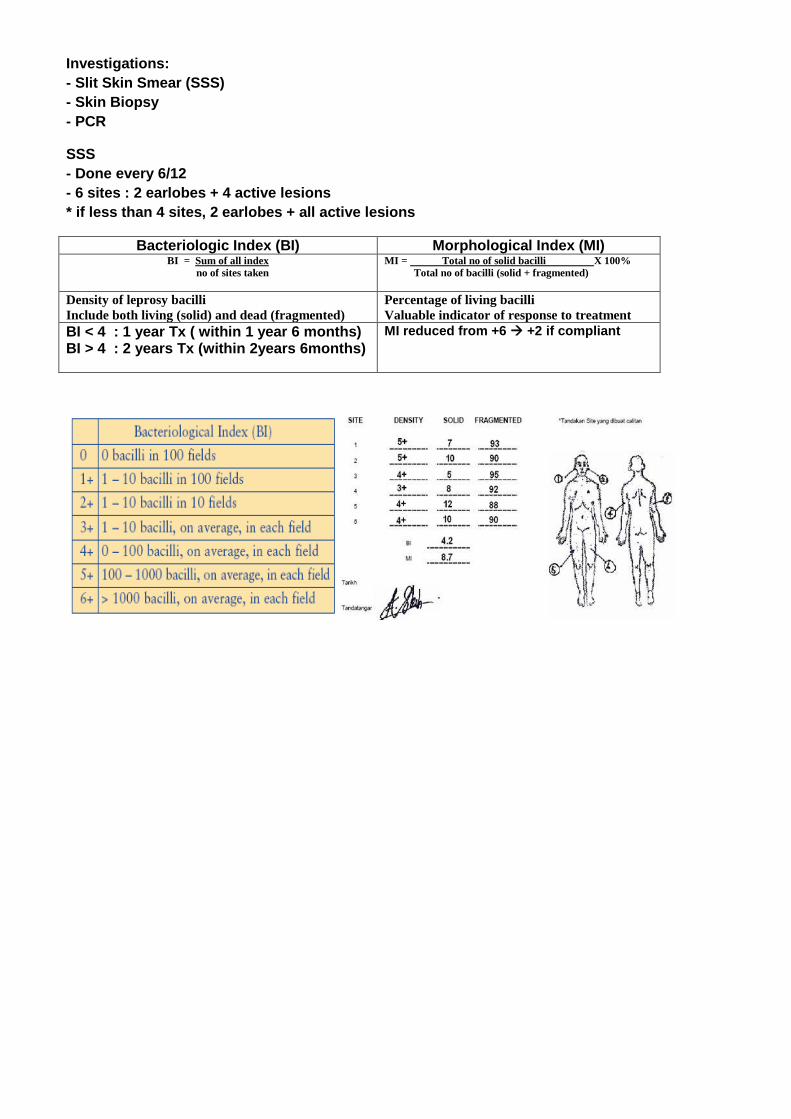
Investigations:
- Slit Skin Smear (SSS)
- Skin Biopsy
- PCR
SSS
- Done every 6/12
- 6 sites : 2 earlobes + 4 active lesions
* if less than 4 sites, 2 earlobes + all active lesions
Bacteriologic Index (BI) Morphological Index (MI) BI = Sum of all index
no of sites taken
MI = Total no of solid bacilli X 100%
Total no of bacilli (solid + fragmented)
Density of leprosy bacilli
Include both living (solid) and dead (fragmented) Percentage of living bacilli
Valuable indicator of response to treatment BI < 4 : 1 year Tx ( within 1 year 6 months) BI > 4 : 2 years Tx (within 2years 6months)
MI reduced from +6 +2 if compliant
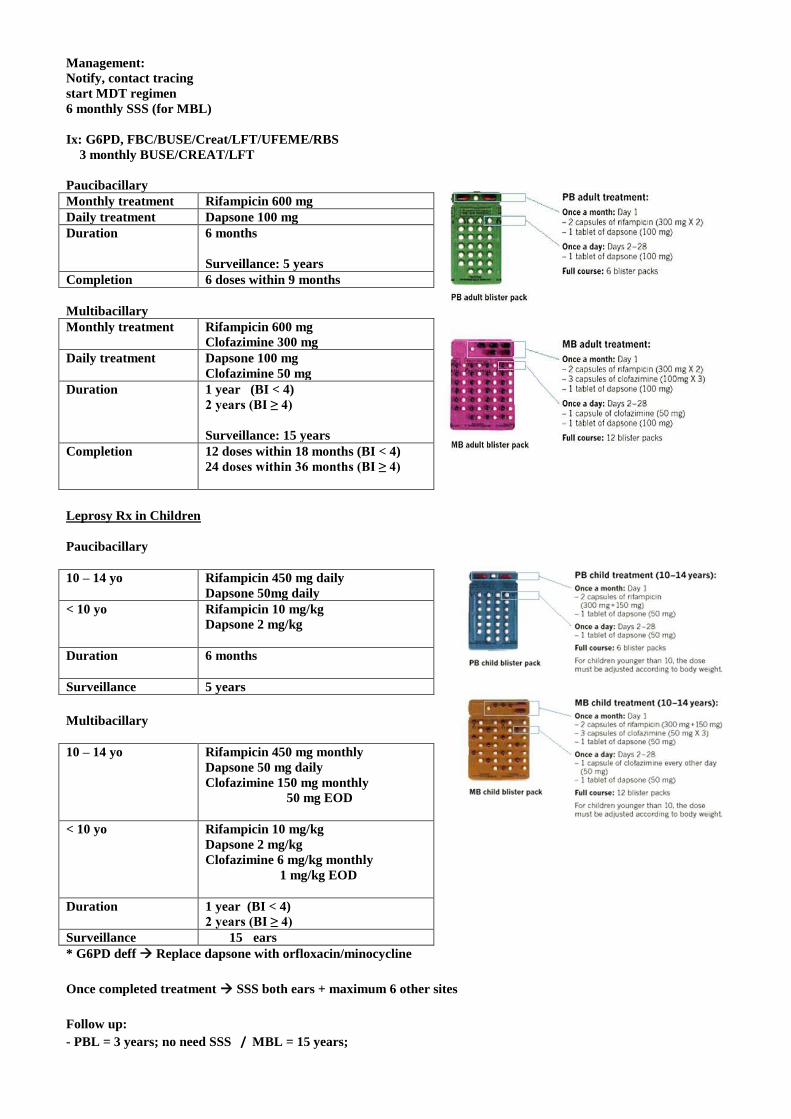
Management:
Notify, contact tracing
start MDT regimen
6 monthly SSS (for MBL)
Ix: G6PD, FBC/BUSE/Creat/LFT/UFEME/RBS
3 monthly BUSE/CREAT/LFT
Paucibacillary
Monthly treatment Rifampicin 600 mg
Daily treatment Dapsone 100 mg
Duration
6 months
Surveillance: 5 years
Completion 6 doses within 9 months
Multibacillary
Monthly treatment Rifampicin 600 mg
Clofazimine 300 mg
Daily treatment
Dapsone 100 mg
Clofazimine 50 mg
Duration
1 year (BI < 4)
2 years (BI ≥ 4)
Surveillance: 15 years
Completion 12 doses within 18 months (BI < 4)
24 doses within 36 months (BI ≥ 4)
Leprosy Rx in Children
Paucibacillary
10 – 14 yo Rifampicin 450 mg daily
Dapsone 50mg daily
< 10 yo
Rifampicin 10 mg/kg
Dapsone 2 mg/kg
Duration
6 months
Surveillance 5 years
Multibacillary
10 – 14 yo Rifampicin 450 mg monthly
Dapsone 50 mg daily
Clofazimine 150 mg monthly
50 mg EOD
< 10 yo
Rifampicin 10 mg/kg
Dapsone 2 mg/kg
Clofazimine 6 mg/kg monthly
1 mg/kg EOD
Duration
1 year (BI < 4)
2 years (BI ≥ 4)
Surveillance 15 ears
* G6PD deff Replace dapsone with orfloxacin/minocycline
Once completed treatment SSS both ears + maximum 6 other sites
Follow up:
- PBL = 3 years; no need SSS / MBL = 15 years;
- First 5 years = SSS yearly
- MBL contacts = examine yearly for 3 years
Adverse Drug Reactions
Dapsone Hemolysis, hepatitis, photosensitive dermatitis, pruritus, Dapsone Hypersensitivity Syndrome,
methaemoglobinaemia
Clofazimine Darkening of skin, GI complaints, dryness of the skin and eyes, pruritus
Rifampicin Reddish discoloration of urine, urticaria, GI complaints, leucopenia, eosinophilia, thrombocytopenia, liver
& renal dysfunction, flu-like syndrome, pruritus, Stevens Johnson Syndrome
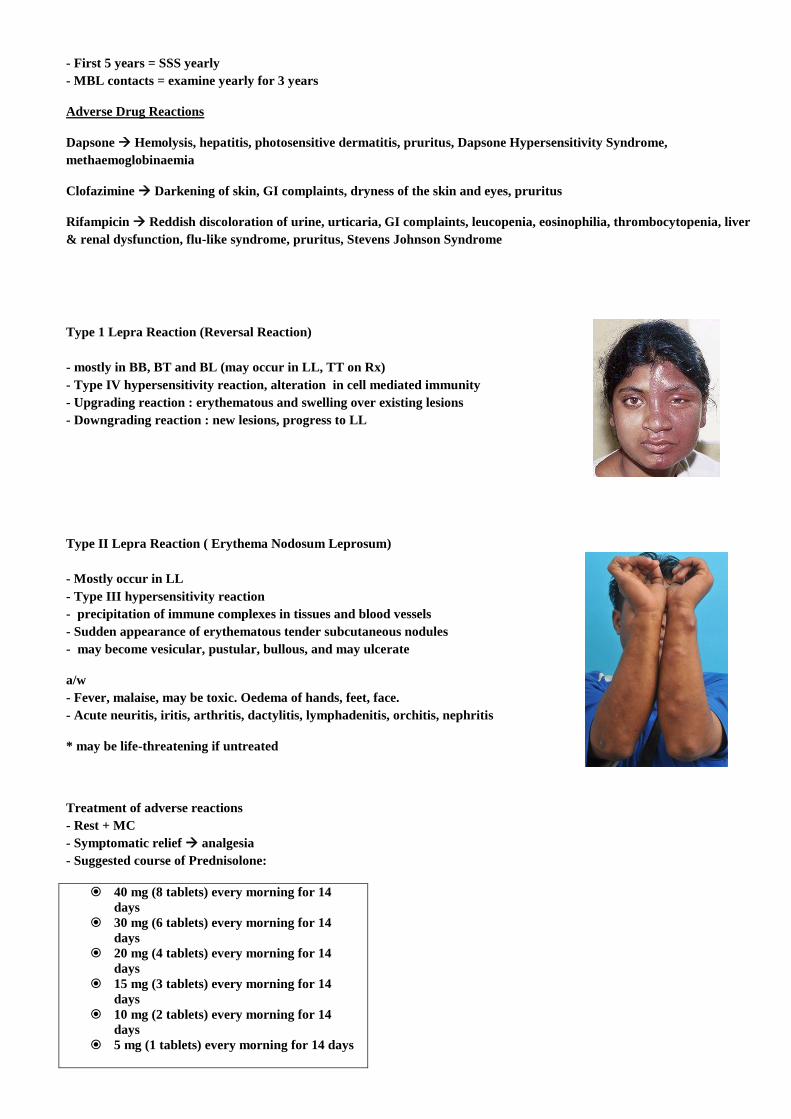
Type 1 Lepra Reaction (Reversal Reaction)
- mostly in BB, BT and BL (may occur in LL, TT on Rx)
- Type IV hypersensitivity reaction, alteration in cell mediated immunity
- Upgrading reaction : erythematous and swelling over existing lesions
- Downgrading reaction : new lesions, progress to LL
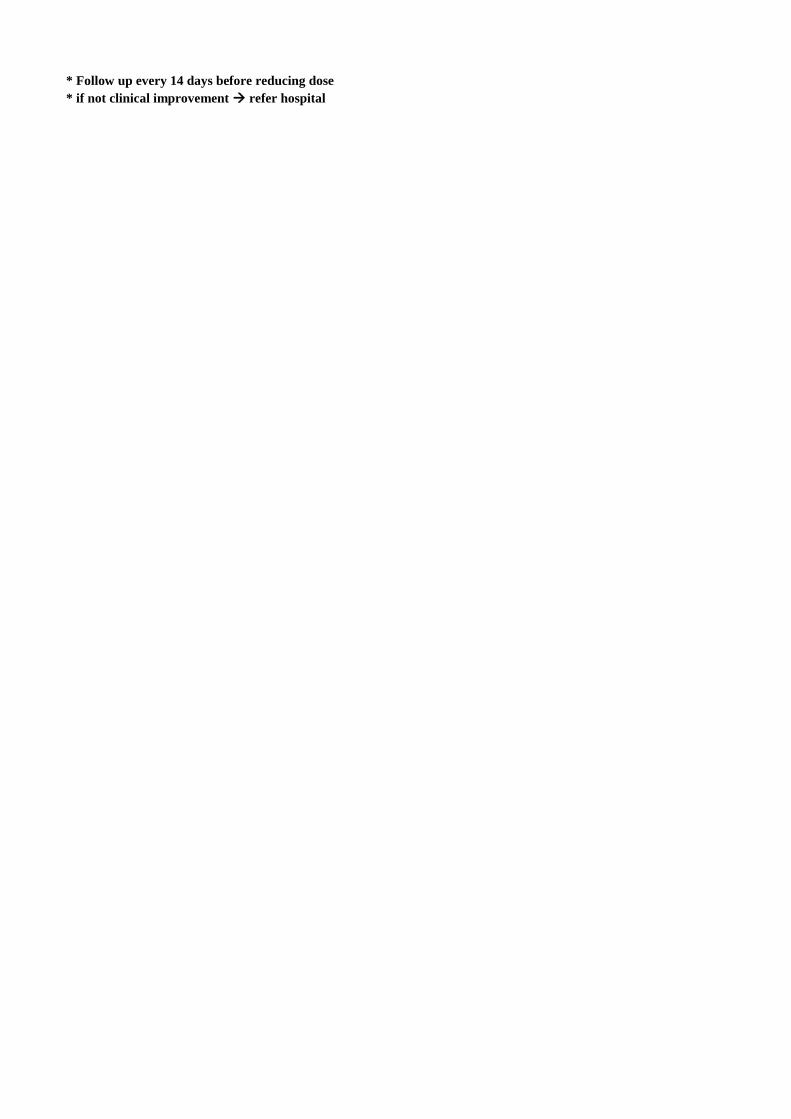
Type II Lepra Reaction ( Erythema Nodosum Leprosum)
- Mostly occur in LL
- Type III hypersensitivity reaction
- precipitation of immune complexes in tissues and blood vessels
- Sudden appearance of erythematous tender subcutaneous nodules
- may become vesicular, pustular, bullous, and may ulcerate
a/w
- Fever, malaise, may be toxic. Oedema of hands, feet, face.
- Acute neuritis, iritis, arthritis, dactylitis, lymphadenitis, orchitis, nephritis
* may be life-threatening if untreated
Treatment of adverse reactions
- Rest + MC
- Symptomatic relief analgesia
- Suggested course of Prednisolone:
40 mg (8 tablets) every morning for 14
days
30 mg (6 tablets) every morning for 14
days
20 mg (4 tablets) every morning for 14
days
15 mg (3 tablets) every morning for 14
days
10 mg (2 tablets) every morning for 14
days
5 mg (1 tablets) every morning for 14 days
* Follow up every 14 days before reducing dose
* if not clinical improvement refer hospital
References
Guide to Eliminate Leprosy as a Public Health Problem, WHO, 2000
Leprosy 2013, by Dr Maurice Steve Utap, Family Medicine Specialist, KK Tudan
Institute of Tropical Medicine, Antwerp
http://itg.content-e.eu/Generated/pubx/173/tuberculosis/clinical_aspects.htm
Tables, algoritms and management recommendations from
CPG Malaysia, Managment of TB (3rd
edition)
Acknowledgements:
Dr Maurice Steve Utap, FMS, KK Tudan
Dr Wong Yong Kai, Medical Officer, TBCP, KK Miri
TBCP staff KK Miri