Embed Size (px)
Citation preview

Monitored Abstinence
Martin H. Plawecki MD, PhD
Indiana University School of MedicineDepartment of Psychiatry
Alcohol Medical Scholars Program

Introduction• Many diseases are chronic, relapsing and remitting
• Controlled, not cured
• Examples
• Type I diabetes: 30-50% relapse rate
• High blood pressure: 50-70% relapse rate
• Substance use disorders (SUDs): 40-60% relapse rate
© Alcohol Medical Scholars Program 2

Goals of SUD Treatment
• Harm reduction
• Abstinence
• Abstinence monitoring has a role in both
© Alcohol Medical Scholars Program 3

This Lecture Covers
• Definition/course of Substance Use Disorders (SUDs)
• Treatments, including with monitored abstinence
• Methods of monitoring abstinence
• Efficacy of monitored abstinence
© Alcohol Medical Scholars Program 4

This Lecture Covers
• Definition/course of Substance Use Disorders (SUDsDefinition/course of Substance Use Disorders (SUDs)
• Treatments, including with monitored abstinence
• Methods of monitoring abstinence
• Efficacy of monitored abstinence
© Alcohol Medical Scholars Program 5

Substance Use DisorderIn Same Year, ≥2 of:
• Tolerance• Withdrawal• Use longer/more• Unable to ↓• Lots time use• ↓ Activities• Use despite probs• Craving
© Alcohol Medical Scholars Program 6
• Failed roles• Hazardous use• Social problems

Remission and Relapse
• Remission
• Early: no symptoms ≥ 3 months but < 1 year
• Sustained: no symptoms ≥ 1 year
• Relapse: back to problematic substance use
© Alcohol Medical Scholars Program 7

Substance Use Disorder
© Alcohol Medical Scholars Program 8

Post Recovery
© Alcohol Medical Scholars Program 9
>26 % 7 %
Within 3 years

This Lecture Covers
• Definition/course of Substance Use Disorders (SUDs)
• Treatments, including with monitored abstinence
• Methods of monitoring abstinence
• Efficacy of monitored abstinence
© Alcohol Medical Scholars Program 10

Treatment• General treatments
• 12-step programs: Alcoholics Anonymous (“AA”)• Cognitive behavioral treatment (CBT)
• Alcohol Rx meds examples• Naltrexone• Acamprosate
• Opioid Rx meds examples• Naltrexone• Buprenorphine• Methadone (to be discussed below)
• Many treatments include abstinence monitoring
© Alcohol Medical Scholars Program 11

12 step programs (e.g., Alcoholics Anonymous)
• Goal: commonly abstinence
• Self-help recovery group
• Very common: ~50 meetings/day in Indianapolis
• Difficult to study given program nature
• AA keeps people in and accepting of intervention
• Limited-unequivocal evidence for ↑abstinence
© Alcohol Medical Scholars Program 12

Cognitive Behavioral Therapy: (The Core of Rehab Rx)• ↓ Dysfunctional thinking
• Substitute rational thoughts
• Relapse prevention
• Anticipate triggers
• Learn to cope w/triggers
• Change behaviors
• Evidence for ↓drinking/use, ↑abstinence© Alcohol Medical Scholars Program 13

Alcohol Rx - Naltrexone• Goal: reduce drinking
• Thought to reduce enjoyment of alcohol
• Daily and long-acting injectable forms
• Reduces drinking
• Return to heavy drinking ↓17%
• Return to any drinking ↓4% → ↑abstinence
• Drinking days ↓4%
© Alcohol Medical Scholars Program 14

Alcohol Rx - Acamprosate• Goal: reduce drinking
• Thought to reduce withdrawal
• Oral only (3x/Day)
• Reduces drinking
• Return to heavy drinking ↓1%
• Return to any drinking ↓14% → ↑abstinence
• Abstinence duration ↑11%
© Alcohol Medical Scholars Program 15

Opioid Rx - Naltrexone• Goal: commonly abstinence
• Blocks all opioid highs
• Daily and long-acting injectable (LAI) forms
• Not well accepted by patients → high drop out
• May be especially useful for docs, nurses, etc
• Daily – some evidence for ↑abstinence, ↑ Rx
• LAI - emerging Data for ↓ heroin, ↑abstinence, ↑ Rx
© Alcohol Medical Scholars Program 16

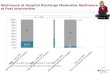
Opioid Rx – Buprenorphine Maintenance• Goal: abstinence (harm reduction)
• Long-acting opioid replaces short-acting heroin
• Daily medication
• Increases treatment acceptance - ↑50%
• Decreases heroin and morphine usage• ↓17% vs placebo, ↓11% vs methadone
• Dose dependent effect (↑dose → ↑results)
© Alcohol Medical Scholars Program 17

Methadone Maintenance• Goal: ↓ health risk, ↓ crime, ↑ family/job
• Replacement: Methadone vs heroin• Lasts >24hours → 1x/day dosing
• Allows work; avoids withdrawal and prevent “high”
• Cheaper & from clinic → ↓ risky bx, ↓crimes
• Highly structured and federally regulated• Administer methadone daily, usually at clinic
• Monitor for abstinence – urine drug screens
• Requires counselling
© Alcohol Medical Scholars Program 18

Court Mandated Rx• Goal: ↓ drug use → ↓ crime
• Links highly structured Rx to legal system• Residential and outpatient treatment
• Random urine drug screens
• Routine judicial interaction and progress monitoring
• Success → avoid jail
• Failure→
• ↑ Monitoring frequency/intensity
• ↑ Punishment up to jail© Alcohol Medical Scholars Program 19

Physician Health Programs• Goal: ↓ patient harm• Links highly structured Rx to medical license• Residential and outpatient treatment• Random urine drug screens• +/- Random office visit• ≥5 Yr follow-up • Success → practice medicine, keep job• Failure →• Treatment, ↑monitoring frequency/intensity• Referral to medical licensing board
© Alcohol Medical Scholars Program 20

Chronic Pain Management• Goal: control pain, minimize substance misuse• Adherence monitoring and risk minimization• Explicit behavior agreements
• Estimate risk
• Use difficult-to-abuse medications
• Rx drug monitoring programs• Urine drug screens
• Success → continue in program
• Failure → lose access to prescription opioids
© Alcohol Medical Scholars Program 21

This Lecture Covers• Definition/course of Substance Use Disorders (SUDs)
• Treatments, including with monitored abstinence
• Methods of monitoring abstinenceMethods of monitoring abstinence
• Efficacy of monitored abstinence
© Alcohol Medical Scholars Program 22

Monitoring Abstinence - Breath• Advantages
• Easy, non-invasive
• Cost – reusable device
• Disadvantages
• Must be done properly
• Possibly non-specific
© Alcohol Medical Scholars Program 23

Monitoring Breath Alcohol & Nicotine• Breath alcohol concentration• Alcohol is water soluble -> appears in the breath
• Electrochemical detection (burns alcohol)
• Deep breath is proportional to blood level
• Detects low alcohol concentration (1 drink in last hour)
• Nicotine• Carbon monoxide (CO) from burning tobacco in breath
• Electrochemical detection (burns CO)
• Detected up to 2 days; “smoker” sensitivity < 10 hours
© Alcohol Medical Scholars Program 24

Monitoring Abstinence - Urine• Advantages• Easy to obtain/non-invasive
• Detection via specific antibodies
• Common and inexpensive
• Disadvantages• Positive test → expensive replication
• Replication takes weeks to get results
• Specific drugs detected for different time lengths
• Cheating
© Alcohol Medical Scholars Program 25

Monitoring Abstinence - Urine• Urine drug screen• Specific antibody screening for substances/byproducts• Many substances can be screened in a single test
© Alcohol Medical Scholars Program 26

Times for Useful Urine Monitoring
• Opioids – 1-3 days
• Cannabinoids
• Single use – 3 days
• Daily – 10-15 days
• Heavy – >30 days
• Amphetamines – 2 days
Detection Times
• Cocaine – 2-4 days
• PCP – 8 days
• Alcohol – ¼ - ½ day
• Sedatives
• Short-acting – 3 days
• Long-acting – 30 days
© Alcohol Medical Scholars Program 27

A Problem With Urine Monitoring• Cheating• Adulterants - substances added to urine sample• Dilution - intentional fluid over-ingestion• Substitution - use of another’s, old, or synthetic urine• False attribution - claimed use of one to hide another
© Alcohol Medical Scholars Program 28

Monitoring Abstinence - Blood• Advantages
• Highly specific → confirm other tests
• Difficult to cheat, low false positives
• Direct and indirect measurements possible
• Disadvantages
• Invasive – requires a blood draw
• Expensive – includes testing and procedure fees
© Alcohol Medical Scholars Program 29

Monitoring Blood Alcohol and Cannabis
• Alcohol: Blood Alcohol Concentration• Direct detection of alcohol• Limited to recent consumption only
• Alcohol: Carbohydrate deficient transferrin (CDT)• Indirect marker - ↑ alcohol > 2 wks → ↑ CDT• Timing: abstinence → ↓ CDT in 2-5 weeks
• Cannabis• Direct detection of cannabinoids• Acute use: peaks in minutes, ↓ <1 hr but > 0 for 1 day• Chronic: detectable up to 30 days
© Alcohol Medical Scholars Program 30

Monitoring Abstinence - Electronic• Advantages
• Continuous monitoring
• Data can be monitored remotely
• Disadvantages
• Intrusive and highly visible
• Expensive
• Optimized for forensics
© Alcohol Medical Scholars Program 31

Electronic Monitoring - Scram
• Alcohol → sweat
• Samples every 30 minutes
• Automatic alerts
• Tamper Resistant
• Cost
• Lease: $6-8/day lease
• Purchase: $1,400-1,800 + $5/day
© Alcohol Medical Scholars Program 32

This Lecture Covers
• Definition/course of Substance Use Disorders (SUDs)
• Treatments, including with monitored abstinence
• Methods of monitoring abstinence
• Efficacy of monitored abstinenceEfficacy of monitored abstinence
© Alcohol Medical Scholars Program 33

Efficacy of Monitored Abstinence• Methadone clinic
• 3x ↑ Remain in Rx vs no opiate replacement
• 2/3x ↓ Positive opioid hair/urine samples
• 2 ½x ↓ Crime involvement
• Chronic Pain Management
• Urine drug testing → ↓ illicit drug usage
• ↑ Urine drug tests → ↑ prescription adherence
• ↑ Urine drug tests → ↓ non-prescribed medications
© Alcohol Medical Scholars Program 34

Efficacy of Monitored Abstinence• Court mandated Rx• 12% ↓ Criminal relapse
• No clear effect on SUD outcomes• Difficult to quantify
• Highly variable population
• Different Rx approaches/referral networks
• Physicians health programs• Only ~20% w/ positive UDS at any time during 5 yrs
• 70-80% Physicians still licensed/employed at 5 yrs
© Alcohol Medical Scholars Program 35

Summary
• SUDs are chronic relapsing/remitting conditions
• Interventions can include abstinence monitoring
• Monitoring - chemical and electronic forms
• Monitored abstinence → better outcomes
© Alcohol Medical Scholars Program 36

Questions
© Alcohol Medical Scholars Program 38