Embed Size (px)
Citation preview
Case ReportMore Than a Decade of Misdiagnosis of Alternating Hemiplegiaof Childhood with Catastrophic Outcome
Hussein Algahtani1 Bashair Ibrahim2 Bader Shirah3
Ahmad Aldarmahi4 and Ahad Abdullah5
1King Abdulaziz Medical City King Saud bin Abdulaziz University for Health Sciences Jeddah Saudi Arabia2King Abdulaziz University Jeddah Saudi Arabia3King Abdullah International Medical Research Center King Saud bin Abdulaziz University for Health Sciences Jeddah Saudi Arabia4King Saud bin Abdulaziz University for Health Sciences Jeddah Saudi Arabia5Batterjee Medical College Jeddah Saudi Arabia
Correspondence should be addressed to Hussein Algahtani halgahtanihotmailcom
Received 26 March 2017 Revised 7 July 2017 Accepted 19 July 2017 Published 16 August 2017
Academic Editor Mamede de Carvalho
Copyright copy 2017 Hussein Algahtani et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
Alternating hemiplegia of childhood (AHC) is a distinct clinical disorder characterized by recurrent episodes of hemiplegiaabnormal ocular movement and progressive developmental delay It is an extremely rare genetic disorder related to ATP1A3 genemutations In this paper we present a case of AHC in which the diagnosis was missed for many years until severe hypoxic braininsult occurred from prolonged status epilepticus Not only we are presenting an interesting clinical entity and radiological imagesbut also we are shedding the light on a rare genetic disease with catastrophic sequelae The challenges in diagnosis and treatmentlead to a poor outcome as seen in our case Although early recognition and accurate diagnosis and treatment of the disease maynot change the outcome counseling of the family may change their expectation and reduce their frustration Referral to a centerwith expertise in genetic disorders and access to genetic laboratories is of paramount importance in the diagnosis of this diseaseDue to the rarity of this disease in Saudi Arabia a genotype-phenotype correlation is not feasible
1 Introduction
Alternating hemiplegia of childhood (AHC) is a distinctclinical disorder characterized by recurrent episodes ofhemiplegia abnormal ocular movement and progressivedevelopmental delay It is an extremely rare genetic disor-der related to ATP1A3 gene mutations with an estimatedprevalence of 11000000 children It is believed that thisnumber could be an underestimate due to variability inclinical presentation lack of knowledge about the diseaseand lack of advancement in the diagnostic laboratory andradiologic test that will confirm the diagnosis [1] AHC wasfirst described in 1971 by Verret and Steele [2] who initiallyattributed the disorder to be amigrainous phenomenonTheyreported 8 children with intermittent hemiparesis of varyingseverity with developmental delay speech difficulties andmovement disorder It was not until 1980 when Krageloh and
Aicardi [3] made the distinction between this disorder andmigraine Since then several case reports and large case serieshave been published which made the clinical spectrum of thedisorder clearer A thorough literature search yielded onlyone case study reported from Saudi Arabia [4] In this paperwe present a case of AHC in which the diagnosis was missedfor many years until severe hypoxic brain insult occurredfrom prolonged status epilepticusWe are not only presentingan interesting clinical entity and radiological images but weare also shedding the light on a rare genetic disease withcatastrophic sequelae
2 Case Report
A 15-year-old femalewas seen in neurology clinic after severalepisodes of transient paralysis that were started when she wasone year oldHermother stated that during these episodes she
HindawiCase Reports in MedicineVolume 2017 Article ID 5769837 5 pageshttpsdoiorg10115520175769837
2 Case Reports in Medicine
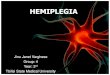
Figure 1 MRI of the brain showing evidence of diffuse asym-metrical left more than right cortical laminar necrosis secondaryto refractory status epilepticus with anoxic brain damage Theimages are FLAIR (upper two rows) and T2-weighted images (lowertwo rows) The changes are high signal intensity involving bothsupratentorial structures and brain stem
was fully conscious but half of her body was paralyzed andshe had difficulty in speakingTheparalysis was characterizedby recurrent episodes of transient hemiplegia alternating inlaterality or affecting both sides simultaneously There wasno associated or preceding vomiting fever seizures loss ofconsciousness or headache The episodes lasted from fewhours to few days and recurred every 10ndash30 days withoutleaving any residual deficit The paralysis disappeared after agood sleep and reappeared within half an hour after awak-ening She was dysarthric when the episode was unilateraland mute when it was bilateral The child became ataxicwith deterioration of cognitive and intellectual functions afterseven years of disease onset She also lagged developmentallybehind her chronological age She was a product of a non-consanguineous marriage at 39 weeks of gestation followinga spontaneous vaginal delivery The pregnancy and neonatalperiod were uneventful There was no family history of asimilar disease including migraine Her neuroimaging wasnormal on several occasions At the age of 14 she developedsudden onset of a partial motor seizure of the face withsecondary generalization and status epilepticus The seizureswere difficult to control lasted several hours and necessitatedan admission to the intensive care unit with intubation andmechanical ventilation The final diagnosis was AHC withstatus epilepticus and catastrophic cortical necrosis due tosevere hypoxic brain insult Figure 1 is showing her magneticresonance imaging (MRI) few months following dischargefrom the hospital on multiple antiepileptic drugs She wasmute quadriparetic and psychotic In a follow-up visit to theclinic three years following discharge from the hospital sheshowed some improvement in power and speech althoughcontinued to be fully dependent on the family for daily
activities She was also on multiple medications for herpsychotic symptoms
3 Discussion
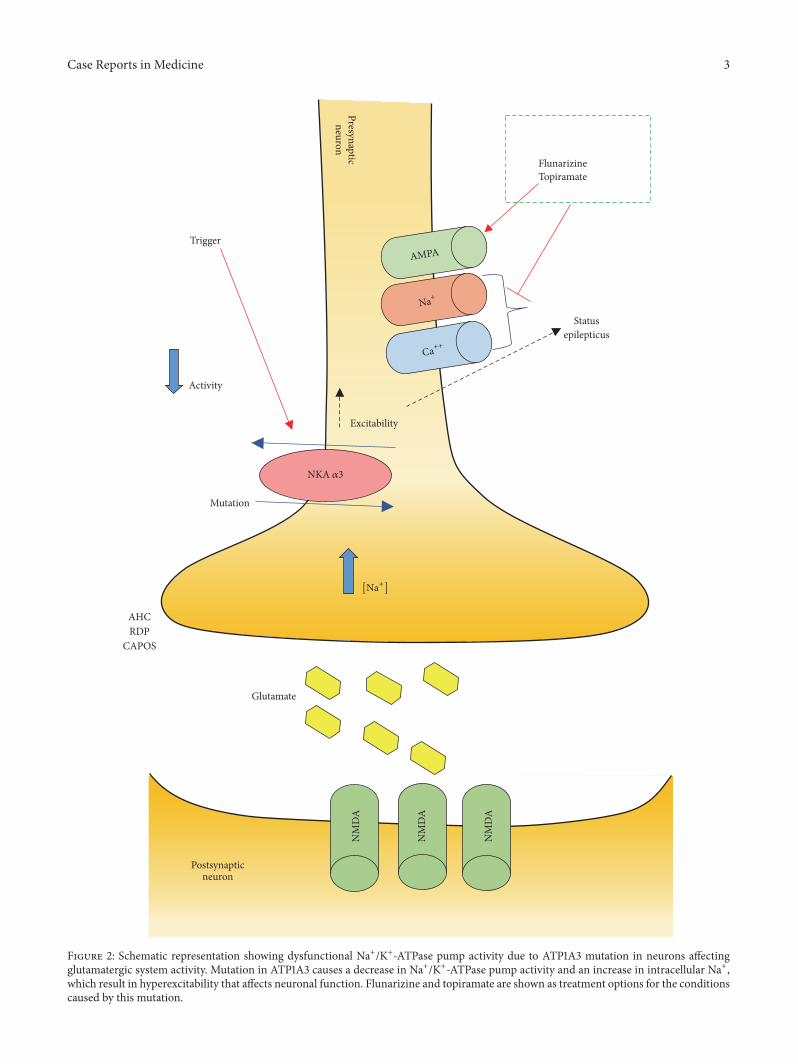
AHC is a genetic disorder caused bymutations in theATP1A3gene which encodes an 120572-subunit (the 1205723-isoform) of theNa+K+-ATPase pump The Na+K+-ATPase pump is partlyresponsible for establishing and maintaining electrochemicalgradients of sodium and potassium ions across the plasmamembrane of neurons The 1205723-isoform is primarily foundin the nervous system and is considered the most commonform of 120572-subunits of the basal ganglia hippocampus andcerebellum In addition to AHC heterozygous mutations ofthe ATP1A3 gene have been reported in association withrapid-onset dystonia parkinsonism (RDP) and cerebellarataxia areflexia pes cavus optic atrophy and sensorineuralhearing loss (CAPOS) (Figure 2) Several cases with ATP1A3gene mutation have been described with an intermediateAHCRDP phenotype ATP1A3 gene is responsible for 74of AHC cases However other genes have been reportedwith similar clinical presentation including the ATP1A2 geneGLUT-1 gene and CACNA1A gene [5]
The spectrum of clinical symptoms of AHC is broadwhich makes the differential diagnosis difficult The first signof AHC typically arises prior to one year of age often withevidence of mild developmental delay and abnormal eyemovements It is characterized by transient episodes of hemi-plegia which last minutes to days and affect either one or bothsides of the body Brief episodes of monocular or binocularmovements may occur including intermittent eye deviationnystagmus anddysconjugate gaze which last for 1ndash3minutesThe abnormal eye movements are most commonly unilateraland ipsilateral to the hemiplegia [6] Motor attacks could behemiplegia quadriplegia dystonia or a combination of anyof them As a general rule infants and young children haveflaccid hemiplegia and older children are more likely to havedystonic features Dystonia may last from seconds to hoursand it is mostly unilateral The attack onset is abrupt whichmakes dystonia often mistaken for a seizure and hemiplegiafor a stroke During a single hemiplegic attack the intensityof weakness is fluctuating During long attacks hemiplegiamay change from one side to the other or both sides may beaffected The arm is mostly weaker than the leg and walkingmay not be impaired Hemiplegia ceases during sleep andreappears on awakening but not immediately Deteriorationof consciousness was not associated with episodes of hemi-plegia Dystonic episodes may primarily affect the limbs onone side causing hemidystonia or affect the trunk causingopisthotonic posturing Headaches could occur at the onsetof an attack but not after it Writhingmovements that suggestchoreoathetosis could also be an associated feature Mentalslowing occurs early in the disease course while mentalregression and persistent neurological abnormalities couldfollow late in the course of the disease [7]
The evaluation of AHC is focused on excluding otherserious or treatable causes MRI magnetic resonance angiog-raphy (MRA) and magnetic resonance spectroscopy shouldbe performed to exclude structural vascular and metabolic
Case Reports in Medicine 3
NM
DA
NM
DA
NM
DA
Postsynapticneuron
Trigger
NKA 3
AHCRDP
CAPOS
Glutamate
Activity
Mutation
Statusepilepticus
FlunarizineTopiramate
Presynapticneuron
AMPA
+
++
Excitability
[+]
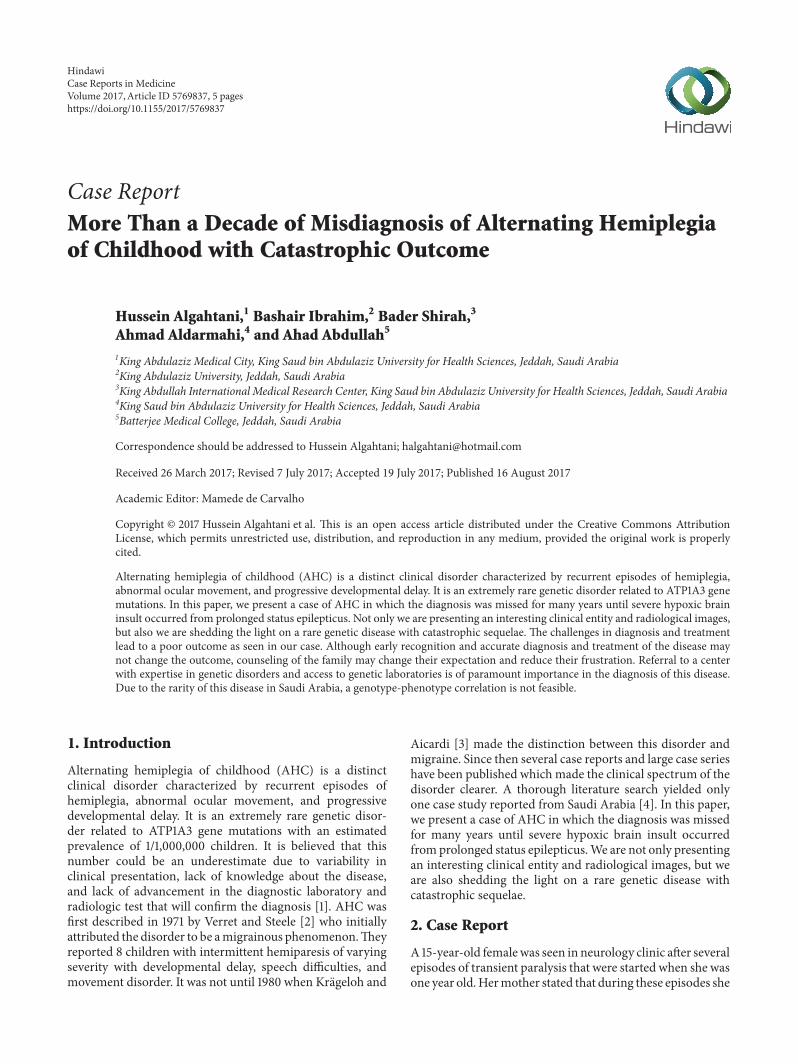
Figure 2 Schematic representation showing dysfunctional Na+K+-ATPase pump activity due to ATP1A3 mutation in neurons affectingglutamatergic system activity Mutation in ATP1A3 causes a decrease in Na+K+-ATPase pump activity and an increase in intracellular Na+which result in hyperexcitability that affects neuronal function Flunarizine and topiramate are shown as treatment options for the conditionscaused by this mutation
4 Case Reports in Medicine
disorders including mitochondrial myopathy encephalopa-thy lactic acidosis and stroke (MELAS) and pyruvate dehy-drogenase deficiency Other differential diagnoses includedifferent subgroups of stroke epilepsy syndromes and dif-ferent types of migraine Results of neuroradiological testsin AHC cases are usually normal However in the severelyaffected or older patients changes may include cerebel-lar atrophy polymicrogyria syringomyelia or hippocampalpathology Other testing may include electroencephalogram(EEG) metabolic screening with urine organic acids quanti-tative serum and cerebrospinal fluid (CSF) amino acids acyl-carnitine lactatepyruvate (serumandCSF) hypercoagulablestudies erythrocyte sedimentation rate and transferrin iso-electric focusing Genetic testing of the ATP1A3 gene is alsoimportant for AHC confirmation [8]
AHC treatment can be divided into acute managementof the attacks and episode prophylaxis Acute managementis focused towards removing known triggers and early sleepfacilitation The use of buccal midazolam or rectal diazepamhas been advocated by some authors to provide quick seda-tion Episode prophylaxis is focused towards avoiding knowntriggers and long-term drug treatment A variety of medica-tions have been proposed for the treatment of AHC but cal-cium channel blockers are the most effective The most com-mon calcium channel blocker used is flunarizine in a dose of5 to 20mg per day Flunarizine has been reported to reducethe frequency and severity of attacks but not to completelystop them and it is considered the drug of choice [9] Otherproposed treatments include beta blockers anticonvulsantsmethysergide amantadine aripiprazole and haloperidolAntiepileptic drugs are effective in treating seizures only Top-iramate has been reported to positively influence the severityin some patients with AHC [10] A recent article report-ing the use of adenosine-51015840-triphosphate orally with 2-yearfollow-up demonstrated promising and successful results[11] In addition some reports supported the use of a keto-genic diet in patients with AHC [12 13]
The long-term outcome of patients with AHC is gen-erally poor due to the associated developmental delays andgradual deterioration after severe attacks The clinical courseof AHC is more severe in sporadic cases than in familialones Prognosis is greatly influenced by the age of onsetespecially early occurrence of hemiplegic spells Childrenwith neonatal-onset manifestation usually suffer from severedevelopmental delay Recurrent convulsive status epilepticusleads to deterioration of psychomotor development In somechildren motor dysfunctions caused wheelchair-depend-ency but others were able to have an independent life inadulthood As patients become older hemiplegic spells andabnormal ocularmovements become less common andhypo-tonia less severe [7]
4 Conclusion
Since the original description of AHC many endeavourshave been made to understand the pathophysiology of thedisease which resulted in linking the disease with mutationsin the gene ATP1A3 Despite this substantial progress in theunderstanding of the disease no curative treatment has been
discovered and the disease continues to be challenging totreat All the current treatments are focused on reducingthe frequency duration and severity of AHC episodes Thechallenges in diagnosis and treatment lead to a poor outcomeas seen in our case Although early recognition and accuratediagnosis and treatment of the disease may not changethe outcome counseling of the family may change theirexpectation and reduce their frustration Referral to a centerwith expertise in genetic disorders and access to geneticlaboratories is of paramount importance in the diagnosis ofthis disease Due to the rarity of this disease in Saudi Arabia agenotype-phenotype correlation is not feasibleThe complex-ity and severity of this disordermakemore research crucial tofind the curative therapy and further understand the disease
Disclosure
Themanuscript was presented in ldquo2nd International Confer-ence onCentralNervous SystemDisorders andTherapeuticsrdquoin 2016
Conflicts of Interest
The authors declare that they have no conflicts of interest
References
[1] E Panagiotakaki E De Grandis M Stagnaro et al ldquoClinicalprofile of patients withATP1A3mutations inAlternatingHemi-plegia of Childhood - a study of 155 patientsrdquo Orphanet Jour-nal of Rare Diseases vol 10 no 1 article no 123 2015
[2] S Verret and J C Steele ldquoAlternating hemiplegia in childhooda report of eight patients with complicated migraine beginningin infancyrdquo Pediatrics vol 47 no 4 pp 675ndash680 1971
[3] I Krageloh and J Aicardi ldquoAlternating hemiplegia in infantsreport of five casesrdquoDevelopmentalMedicineampChildNeurologyvol 22 no 6 pp 784ndash791 1980
[4] B Al-Bulushi A Al-Hashem and B Tabarki ldquoA wide clinicalphenotype spectrum in patients with ATP1A2 mutationsrdquoJournal of Child Neurology vol 29 no 2 pp 265ndash268 2014
[5] M T Sweney TMNewcomb andK J Swoboda ldquoThe expand-ing spectrum of neurological phenotypes in children withATP1A3mutations alternating hemiplegia of childhood rapid-onset Dystonia-Parkinsonism CAPOS and beyondrdquo PediatricNeurology vol 52 no 1 pp 56ndash64 2015
[6] E L Heinzen A Arzimanoglou A Brashear et al ldquoDistinctneurological disorders with ATP1A3 mutationsrdquo The LancetNeurology vol 13 no 5 pp 503ndash514 2014
[7] A Gergont and M Kacinski ldquoAlternating hemiplegia of child-hood New diagnostic optionsrdquo Neurologia i NeurochirurgiaPolska vol 48 no 2 pp 130ndash135 2014
[8] M T Sweney K Silver M Gerard-Blanluet et al ldquoAlternatinghemiplegia of childhood early characteristics and evolution ofa neurodevelopmental syndromerdquo Pediatrics vol 123 no 3 ppe534ndashe541 2009
[9] B G R Neville and M Ninan ldquoThe treatment and manage-ment of alternating hemiplegia of childhoodrdquo DevelopmentalMedicine and Child Neurology vol 49 no 10 pp 777ndash780 2007
[10] J R Tenney andM B Schapiro ldquoChild Neurology Alternatinghemiplegia of childhoodrdquoNeurology vol 74 no 14 pp e57ndashe592010
Case Reports in Medicine 5
[11] J Ju S Hirose X-Y Shi A Ishii L-YHu and L-P Zou ldquoTreat-ment with Oral ATP decreases alternating hemiplegia of child-hoodwith de novoATP1A3MutationrdquoOrphanet Journal of RareDiseases vol 11 no 1 article no 55 2016
[12] A Roubergue B Philibert A Gautier et al ldquoExcellent responseto a ketogenic diet in a patient with alternating hemiplegia ofchildhoodrdquo in JIMD Reports vol 15 pp 7ndash12 Springer BerlinGermany 2014
[13] A Ulate-Campos C Fons R Artuch et al ldquoAlternating hemi-plegia of childhood with a de novo mutation in atp1a3 andchanges in SLC2A1 responsive to a ketogenic dietrdquo PediatricNeurology vol 50 no 4 pp 377ndash379 2014
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
2 Case Reports in Medicine
Figure 1 MRI of the brain showing evidence of diffuse asym-metrical left more than right cortical laminar necrosis secondaryto refractory status epilepticus with anoxic brain damage Theimages are FLAIR (upper two rows) and T2-weighted images (lowertwo rows) The changes are high signal intensity involving bothsupratentorial structures and brain stem
was fully conscious but half of her body was paralyzed andshe had difficulty in speakingTheparalysis was characterizedby recurrent episodes of transient hemiplegia alternating inlaterality or affecting both sides simultaneously There wasno associated or preceding vomiting fever seizures loss ofconsciousness or headache The episodes lasted from fewhours to few days and recurred every 10ndash30 days withoutleaving any residual deficit The paralysis disappeared after agood sleep and reappeared within half an hour after awak-ening She was dysarthric when the episode was unilateraland mute when it was bilateral The child became ataxicwith deterioration of cognitive and intellectual functions afterseven years of disease onset She also lagged developmentallybehind her chronological age She was a product of a non-consanguineous marriage at 39 weeks of gestation followinga spontaneous vaginal delivery The pregnancy and neonatalperiod were uneventful There was no family history of asimilar disease including migraine Her neuroimaging wasnormal on several occasions At the age of 14 she developedsudden onset of a partial motor seizure of the face withsecondary generalization and status epilepticus The seizureswere difficult to control lasted several hours and necessitatedan admission to the intensive care unit with intubation andmechanical ventilation The final diagnosis was AHC withstatus epilepticus and catastrophic cortical necrosis due tosevere hypoxic brain insult Figure 1 is showing her magneticresonance imaging (MRI) few months following dischargefrom the hospital on multiple antiepileptic drugs She wasmute quadriparetic and psychotic In a follow-up visit to theclinic three years following discharge from the hospital sheshowed some improvement in power and speech althoughcontinued to be fully dependent on the family for daily
activities She was also on multiple medications for herpsychotic symptoms
3 Discussion
AHC is a genetic disorder caused bymutations in theATP1A3gene which encodes an 120572-subunit (the 1205723-isoform) of theNa+K+-ATPase pump The Na+K+-ATPase pump is partlyresponsible for establishing and maintaining electrochemicalgradients of sodium and potassium ions across the plasmamembrane of neurons The 1205723-isoform is primarily foundin the nervous system and is considered the most commonform of 120572-subunits of the basal ganglia hippocampus andcerebellum In addition to AHC heterozygous mutations ofthe ATP1A3 gene have been reported in association withrapid-onset dystonia parkinsonism (RDP) and cerebellarataxia areflexia pes cavus optic atrophy and sensorineuralhearing loss (CAPOS) (Figure 2) Several cases with ATP1A3gene mutation have been described with an intermediateAHCRDP phenotype ATP1A3 gene is responsible for 74of AHC cases However other genes have been reportedwith similar clinical presentation including the ATP1A2 geneGLUT-1 gene and CACNA1A gene [5]
The spectrum of clinical symptoms of AHC is broadwhich makes the differential diagnosis difficult The first signof AHC typically arises prior to one year of age often withevidence of mild developmental delay and abnormal eyemovements It is characterized by transient episodes of hemi-plegia which last minutes to days and affect either one or bothsides of the body Brief episodes of monocular or binocularmovements may occur including intermittent eye deviationnystagmus anddysconjugate gaze which last for 1ndash3minutesThe abnormal eye movements are most commonly unilateraland ipsilateral to the hemiplegia [6] Motor attacks could behemiplegia quadriplegia dystonia or a combination of anyof them As a general rule infants and young children haveflaccid hemiplegia and older children are more likely to havedystonic features Dystonia may last from seconds to hoursand it is mostly unilateral The attack onset is abrupt whichmakes dystonia often mistaken for a seizure and hemiplegiafor a stroke During a single hemiplegic attack the intensityof weakness is fluctuating During long attacks hemiplegiamay change from one side to the other or both sides may beaffected The arm is mostly weaker than the leg and walkingmay not be impaired Hemiplegia ceases during sleep andreappears on awakening but not immediately Deteriorationof consciousness was not associated with episodes of hemi-plegia Dystonic episodes may primarily affect the limbs onone side causing hemidystonia or affect the trunk causingopisthotonic posturing Headaches could occur at the onsetof an attack but not after it Writhingmovements that suggestchoreoathetosis could also be an associated feature Mentalslowing occurs early in the disease course while mentalregression and persistent neurological abnormalities couldfollow late in the course of the disease [7]
The evaluation of AHC is focused on excluding otherserious or treatable causes MRI magnetic resonance angiog-raphy (MRA) and magnetic resonance spectroscopy shouldbe performed to exclude structural vascular and metabolic
Case Reports in Medicine 3
NM
DA
NM
DA
NM
DA
Postsynapticneuron
Trigger
NKA 3
AHCRDP
CAPOS
Glutamate
Activity
Mutation
Statusepilepticus
FlunarizineTopiramate
Presynapticneuron
AMPA
+
++
Excitability
[+]
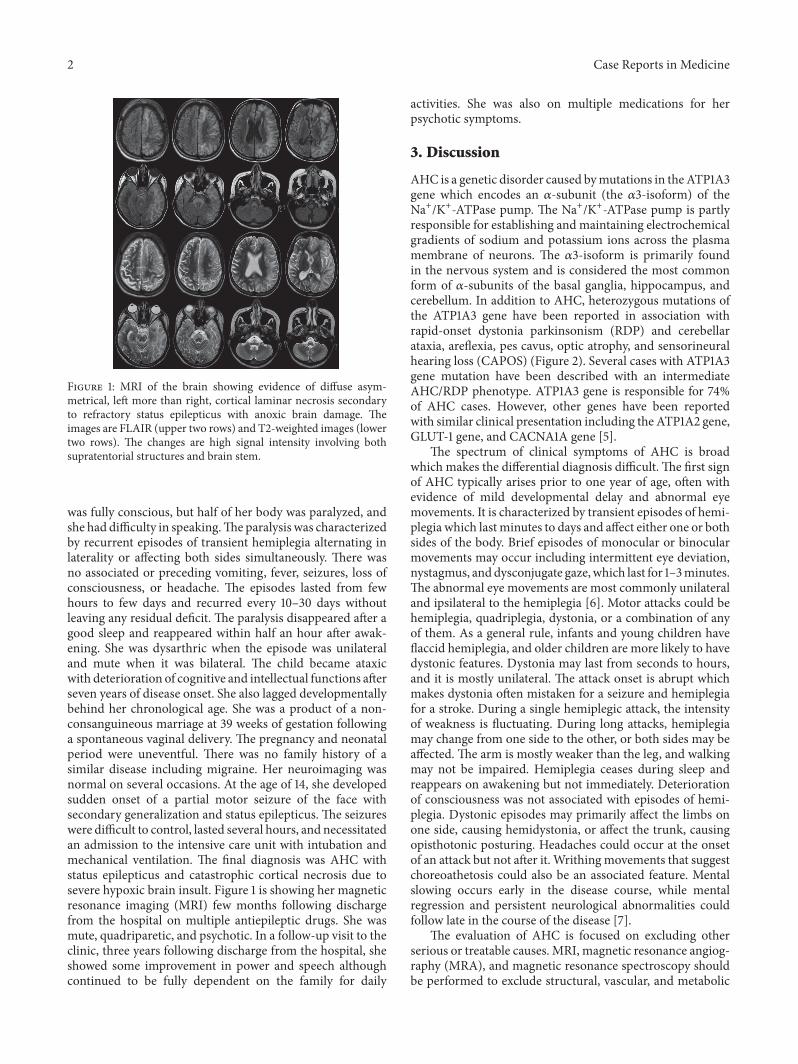
Figure 2 Schematic representation showing dysfunctional Na+K+-ATPase pump activity due to ATP1A3 mutation in neurons affectingglutamatergic system activity Mutation in ATP1A3 causes a decrease in Na+K+-ATPase pump activity and an increase in intracellular Na+which result in hyperexcitability that affects neuronal function Flunarizine and topiramate are shown as treatment options for the conditionscaused by this mutation
4 Case Reports in Medicine
disorders including mitochondrial myopathy encephalopa-thy lactic acidosis and stroke (MELAS) and pyruvate dehy-drogenase deficiency Other differential diagnoses includedifferent subgroups of stroke epilepsy syndromes and dif-ferent types of migraine Results of neuroradiological testsin AHC cases are usually normal However in the severelyaffected or older patients changes may include cerebel-lar atrophy polymicrogyria syringomyelia or hippocampalpathology Other testing may include electroencephalogram(EEG) metabolic screening with urine organic acids quanti-tative serum and cerebrospinal fluid (CSF) amino acids acyl-carnitine lactatepyruvate (serumandCSF) hypercoagulablestudies erythrocyte sedimentation rate and transferrin iso-electric focusing Genetic testing of the ATP1A3 gene is alsoimportant for AHC confirmation [8]
AHC treatment can be divided into acute managementof the attacks and episode prophylaxis Acute managementis focused towards removing known triggers and early sleepfacilitation The use of buccal midazolam or rectal diazepamhas been advocated by some authors to provide quick seda-tion Episode prophylaxis is focused towards avoiding knowntriggers and long-term drug treatment A variety of medica-tions have been proposed for the treatment of AHC but cal-cium channel blockers are the most effective The most com-mon calcium channel blocker used is flunarizine in a dose of5 to 20mg per day Flunarizine has been reported to reducethe frequency and severity of attacks but not to completelystop them and it is considered the drug of choice [9] Otherproposed treatments include beta blockers anticonvulsantsmethysergide amantadine aripiprazole and haloperidolAntiepileptic drugs are effective in treating seizures only Top-iramate has been reported to positively influence the severityin some patients with AHC [10] A recent article report-ing the use of adenosine-51015840-triphosphate orally with 2-yearfollow-up demonstrated promising and successful results[11] In addition some reports supported the use of a keto-genic diet in patients with AHC [12 13]
The long-term outcome of patients with AHC is gen-erally poor due to the associated developmental delays andgradual deterioration after severe attacks The clinical courseof AHC is more severe in sporadic cases than in familialones Prognosis is greatly influenced by the age of onsetespecially early occurrence of hemiplegic spells Childrenwith neonatal-onset manifestation usually suffer from severedevelopmental delay Recurrent convulsive status epilepticusleads to deterioration of psychomotor development In somechildren motor dysfunctions caused wheelchair-depend-ency but others were able to have an independent life inadulthood As patients become older hemiplegic spells andabnormal ocularmovements become less common andhypo-tonia less severe [7]
4 Conclusion
Since the original description of AHC many endeavourshave been made to understand the pathophysiology of thedisease which resulted in linking the disease with mutationsin the gene ATP1A3 Despite this substantial progress in theunderstanding of the disease no curative treatment has been
discovered and the disease continues to be challenging totreat All the current treatments are focused on reducingthe frequency duration and severity of AHC episodes Thechallenges in diagnosis and treatment lead to a poor outcomeas seen in our case Although early recognition and accuratediagnosis and treatment of the disease may not changethe outcome counseling of the family may change theirexpectation and reduce their frustration Referral to a centerwith expertise in genetic disorders and access to geneticlaboratories is of paramount importance in the diagnosis ofthis disease Due to the rarity of this disease in Saudi Arabia agenotype-phenotype correlation is not feasibleThe complex-ity and severity of this disordermakemore research crucial tofind the curative therapy and further understand the disease
Disclosure
Themanuscript was presented in ldquo2nd International Confer-ence onCentralNervous SystemDisorders andTherapeuticsrdquoin 2016
Conflicts of Interest
The authors declare that they have no conflicts of interest
References
[1] E Panagiotakaki E De Grandis M Stagnaro et al ldquoClinicalprofile of patients withATP1A3mutations inAlternatingHemi-plegia of Childhood - a study of 155 patientsrdquo Orphanet Jour-nal of Rare Diseases vol 10 no 1 article no 123 2015
[2] S Verret and J C Steele ldquoAlternating hemiplegia in childhooda report of eight patients with complicated migraine beginningin infancyrdquo Pediatrics vol 47 no 4 pp 675ndash680 1971
[3] I Krageloh and J Aicardi ldquoAlternating hemiplegia in infantsreport of five casesrdquoDevelopmentalMedicineampChildNeurologyvol 22 no 6 pp 784ndash791 1980
[4] B Al-Bulushi A Al-Hashem and B Tabarki ldquoA wide clinicalphenotype spectrum in patients with ATP1A2 mutationsrdquoJournal of Child Neurology vol 29 no 2 pp 265ndash268 2014
[5] M T Sweney TMNewcomb andK J Swoboda ldquoThe expand-ing spectrum of neurological phenotypes in children withATP1A3mutations alternating hemiplegia of childhood rapid-onset Dystonia-Parkinsonism CAPOS and beyondrdquo PediatricNeurology vol 52 no 1 pp 56ndash64 2015
[6] E L Heinzen A Arzimanoglou A Brashear et al ldquoDistinctneurological disorders with ATP1A3 mutationsrdquo The LancetNeurology vol 13 no 5 pp 503ndash514 2014
[7] A Gergont and M Kacinski ldquoAlternating hemiplegia of child-hood New diagnostic optionsrdquo Neurologia i NeurochirurgiaPolska vol 48 no 2 pp 130ndash135 2014
[8] M T Sweney K Silver M Gerard-Blanluet et al ldquoAlternatinghemiplegia of childhood early characteristics and evolution ofa neurodevelopmental syndromerdquo Pediatrics vol 123 no 3 ppe534ndashe541 2009
[9] B G R Neville and M Ninan ldquoThe treatment and manage-ment of alternating hemiplegia of childhoodrdquo DevelopmentalMedicine and Child Neurology vol 49 no 10 pp 777ndash780 2007
[10] J R Tenney andM B Schapiro ldquoChild Neurology Alternatinghemiplegia of childhoodrdquoNeurology vol 74 no 14 pp e57ndashe592010
Case Reports in Medicine 5
[11] J Ju S Hirose X-Y Shi A Ishii L-YHu and L-P Zou ldquoTreat-ment with Oral ATP decreases alternating hemiplegia of child-hoodwith de novoATP1A3MutationrdquoOrphanet Journal of RareDiseases vol 11 no 1 article no 55 2016
[12] A Roubergue B Philibert A Gautier et al ldquoExcellent responseto a ketogenic diet in a patient with alternating hemiplegia ofchildhoodrdquo in JIMD Reports vol 15 pp 7ndash12 Springer BerlinGermany 2014
[13] A Ulate-Campos C Fons R Artuch et al ldquoAlternating hemi-plegia of childhood with a de novo mutation in atp1a3 andchanges in SLC2A1 responsive to a ketogenic dietrdquo PediatricNeurology vol 50 no 4 pp 377ndash379 2014
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Case Reports in Medicine 3
NM
DA
NM
DA
NM
DA
Postsynapticneuron
Trigger
NKA 3
AHCRDP
CAPOS
Glutamate
Activity
Mutation
Statusepilepticus
FlunarizineTopiramate
Presynapticneuron
AMPA
+
++
Excitability
[+]
Figure 2 Schematic representation showing dysfunctional Na+K+-ATPase pump activity due to ATP1A3 mutation in neurons affectingglutamatergic system activity Mutation in ATP1A3 causes a decrease in Na+K+-ATPase pump activity and an increase in intracellular Na+which result in hyperexcitability that affects neuronal function Flunarizine and topiramate are shown as treatment options for the conditionscaused by this mutation
4 Case Reports in Medicine
disorders including mitochondrial myopathy encephalopa-thy lactic acidosis and stroke (MELAS) and pyruvate dehy-drogenase deficiency Other differential diagnoses includedifferent subgroups of stroke epilepsy syndromes and dif-ferent types of migraine Results of neuroradiological testsin AHC cases are usually normal However in the severelyaffected or older patients changes may include cerebel-lar atrophy polymicrogyria syringomyelia or hippocampalpathology Other testing may include electroencephalogram(EEG) metabolic screening with urine organic acids quanti-tative serum and cerebrospinal fluid (CSF) amino acids acyl-carnitine lactatepyruvate (serumandCSF) hypercoagulablestudies erythrocyte sedimentation rate and transferrin iso-electric focusing Genetic testing of the ATP1A3 gene is alsoimportant for AHC confirmation [8]
AHC treatment can be divided into acute managementof the attacks and episode prophylaxis Acute managementis focused towards removing known triggers and early sleepfacilitation The use of buccal midazolam or rectal diazepamhas been advocated by some authors to provide quick seda-tion Episode prophylaxis is focused towards avoiding knowntriggers and long-term drug treatment A variety of medica-tions have been proposed for the treatment of AHC but cal-cium channel blockers are the most effective The most com-mon calcium channel blocker used is flunarizine in a dose of5 to 20mg per day Flunarizine has been reported to reducethe frequency and severity of attacks but not to completelystop them and it is considered the drug of choice [9] Otherproposed treatments include beta blockers anticonvulsantsmethysergide amantadine aripiprazole and haloperidolAntiepileptic drugs are effective in treating seizures only Top-iramate has been reported to positively influence the severityin some patients with AHC [10] A recent article report-ing the use of adenosine-51015840-triphosphate orally with 2-yearfollow-up demonstrated promising and successful results[11] In addition some reports supported the use of a keto-genic diet in patients with AHC [12 13]
The long-term outcome of patients with AHC is gen-erally poor due to the associated developmental delays andgradual deterioration after severe attacks The clinical courseof AHC is more severe in sporadic cases than in familialones Prognosis is greatly influenced by the age of onsetespecially early occurrence of hemiplegic spells Childrenwith neonatal-onset manifestation usually suffer from severedevelopmental delay Recurrent convulsive status epilepticusleads to deterioration of psychomotor development In somechildren motor dysfunctions caused wheelchair-depend-ency but others were able to have an independent life inadulthood As patients become older hemiplegic spells andabnormal ocularmovements become less common andhypo-tonia less severe [7]
4 Conclusion
Since the original description of AHC many endeavourshave been made to understand the pathophysiology of thedisease which resulted in linking the disease with mutationsin the gene ATP1A3 Despite this substantial progress in theunderstanding of the disease no curative treatment has been
discovered and the disease continues to be challenging totreat All the current treatments are focused on reducingthe frequency duration and severity of AHC episodes Thechallenges in diagnosis and treatment lead to a poor outcomeas seen in our case Although early recognition and accuratediagnosis and treatment of the disease may not changethe outcome counseling of the family may change theirexpectation and reduce their frustration Referral to a centerwith expertise in genetic disorders and access to geneticlaboratories is of paramount importance in the diagnosis ofthis disease Due to the rarity of this disease in Saudi Arabia agenotype-phenotype correlation is not feasibleThe complex-ity and severity of this disordermakemore research crucial tofind the curative therapy and further understand the disease
Disclosure
Themanuscript was presented in ldquo2nd International Confer-ence onCentralNervous SystemDisorders andTherapeuticsrdquoin 2016
Conflicts of Interest
The authors declare that they have no conflicts of interest
References
[1] E Panagiotakaki E De Grandis M Stagnaro et al ldquoClinicalprofile of patients withATP1A3mutations inAlternatingHemi-plegia of Childhood - a study of 155 patientsrdquo Orphanet Jour-nal of Rare Diseases vol 10 no 1 article no 123 2015
[2] S Verret and J C Steele ldquoAlternating hemiplegia in childhooda report of eight patients with complicated migraine beginningin infancyrdquo Pediatrics vol 47 no 4 pp 675ndash680 1971
[3] I Krageloh and J Aicardi ldquoAlternating hemiplegia in infantsreport of five casesrdquoDevelopmentalMedicineampChildNeurologyvol 22 no 6 pp 784ndash791 1980
[4] B Al-Bulushi A Al-Hashem and B Tabarki ldquoA wide clinicalphenotype spectrum in patients with ATP1A2 mutationsrdquoJournal of Child Neurology vol 29 no 2 pp 265ndash268 2014
[5] M T Sweney TMNewcomb andK J Swoboda ldquoThe expand-ing spectrum of neurological phenotypes in children withATP1A3mutations alternating hemiplegia of childhood rapid-onset Dystonia-Parkinsonism CAPOS and beyondrdquo PediatricNeurology vol 52 no 1 pp 56ndash64 2015
[6] E L Heinzen A Arzimanoglou A Brashear et al ldquoDistinctneurological disorders with ATP1A3 mutationsrdquo The LancetNeurology vol 13 no 5 pp 503ndash514 2014
[7] A Gergont and M Kacinski ldquoAlternating hemiplegia of child-hood New diagnostic optionsrdquo Neurologia i NeurochirurgiaPolska vol 48 no 2 pp 130ndash135 2014
[8] M T Sweney K Silver M Gerard-Blanluet et al ldquoAlternatinghemiplegia of childhood early characteristics and evolution ofa neurodevelopmental syndromerdquo Pediatrics vol 123 no 3 ppe534ndashe541 2009
[9] B G R Neville and M Ninan ldquoThe treatment and manage-ment of alternating hemiplegia of childhoodrdquo DevelopmentalMedicine and Child Neurology vol 49 no 10 pp 777ndash780 2007
[10] J R Tenney andM B Schapiro ldquoChild Neurology Alternatinghemiplegia of childhoodrdquoNeurology vol 74 no 14 pp e57ndashe592010
Case Reports in Medicine 5
[11] J Ju S Hirose X-Y Shi A Ishii L-YHu and L-P Zou ldquoTreat-ment with Oral ATP decreases alternating hemiplegia of child-hoodwith de novoATP1A3MutationrdquoOrphanet Journal of RareDiseases vol 11 no 1 article no 55 2016
[12] A Roubergue B Philibert A Gautier et al ldquoExcellent responseto a ketogenic diet in a patient with alternating hemiplegia ofchildhoodrdquo in JIMD Reports vol 15 pp 7ndash12 Springer BerlinGermany 2014
[13] A Ulate-Campos C Fons R Artuch et al ldquoAlternating hemi-plegia of childhood with a de novo mutation in atp1a3 andchanges in SLC2A1 responsive to a ketogenic dietrdquo PediatricNeurology vol 50 no 4 pp 377ndash379 2014
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Case Reports in Medicine
disorders including mitochondrial myopathy encephalopa-thy lactic acidosis and stroke (MELAS) and pyruvate dehy-drogenase deficiency Other differential diagnoses includedifferent subgroups of stroke epilepsy syndromes and dif-ferent types of migraine Results of neuroradiological testsin AHC cases are usually normal However in the severelyaffected or older patients changes may include cerebel-lar atrophy polymicrogyria syringomyelia or hippocampalpathology Other testing may include electroencephalogram(EEG) metabolic screening with urine organic acids quanti-tative serum and cerebrospinal fluid (CSF) amino acids acyl-carnitine lactatepyruvate (serumandCSF) hypercoagulablestudies erythrocyte sedimentation rate and transferrin iso-electric focusing Genetic testing of the ATP1A3 gene is alsoimportant for AHC confirmation [8]
AHC treatment can be divided into acute managementof the attacks and episode prophylaxis Acute managementis focused towards removing known triggers and early sleepfacilitation The use of buccal midazolam or rectal diazepamhas been advocated by some authors to provide quick seda-tion Episode prophylaxis is focused towards avoiding knowntriggers and long-term drug treatment A variety of medica-tions have been proposed for the treatment of AHC but cal-cium channel blockers are the most effective The most com-mon calcium channel blocker used is flunarizine in a dose of5 to 20mg per day Flunarizine has been reported to reducethe frequency and severity of attacks but not to completelystop them and it is considered the drug of choice [9] Otherproposed treatments include beta blockers anticonvulsantsmethysergide amantadine aripiprazole and haloperidolAntiepileptic drugs are effective in treating seizures only Top-iramate has been reported to positively influence the severityin some patients with AHC [10] A recent article report-ing the use of adenosine-51015840-triphosphate orally with 2-yearfollow-up demonstrated promising and successful results[11] In addition some reports supported the use of a keto-genic diet in patients with AHC [12 13]
The long-term outcome of patients with AHC is gen-erally poor due to the associated developmental delays andgradual deterioration after severe attacks The clinical courseof AHC is more severe in sporadic cases than in familialones Prognosis is greatly influenced by the age of onsetespecially early occurrence of hemiplegic spells Childrenwith neonatal-onset manifestation usually suffer from severedevelopmental delay Recurrent convulsive status epilepticusleads to deterioration of psychomotor development In somechildren motor dysfunctions caused wheelchair-depend-ency but others were able to have an independent life inadulthood As patients become older hemiplegic spells andabnormal ocularmovements become less common andhypo-tonia less severe [7]
4 Conclusion
Since the original description of AHC many endeavourshave been made to understand the pathophysiology of thedisease which resulted in linking the disease with mutationsin the gene ATP1A3 Despite this substantial progress in theunderstanding of the disease no curative treatment has been
discovered and the disease continues to be challenging totreat All the current treatments are focused on reducingthe frequency duration and severity of AHC episodes Thechallenges in diagnosis and treatment lead to a poor outcomeas seen in our case Although early recognition and accuratediagnosis and treatment of the disease may not changethe outcome counseling of the family may change theirexpectation and reduce their frustration Referral to a centerwith expertise in genetic disorders and access to geneticlaboratories is of paramount importance in the diagnosis ofthis disease Due to the rarity of this disease in Saudi Arabia agenotype-phenotype correlation is not feasibleThe complex-ity and severity of this disordermakemore research crucial tofind the curative therapy and further understand the disease
Disclosure
Themanuscript was presented in ldquo2nd International Confer-ence onCentralNervous SystemDisorders andTherapeuticsrdquoin 2016
Conflicts of Interest
The authors declare that they have no conflicts of interest
References
[1] E Panagiotakaki E De Grandis M Stagnaro et al ldquoClinicalprofile of patients withATP1A3mutations inAlternatingHemi-plegia of Childhood - a study of 155 patientsrdquo Orphanet Jour-nal of Rare Diseases vol 10 no 1 article no 123 2015
[2] S Verret and J C Steele ldquoAlternating hemiplegia in childhooda report of eight patients with complicated migraine beginningin infancyrdquo Pediatrics vol 47 no 4 pp 675ndash680 1971
[3] I Krageloh and J Aicardi ldquoAlternating hemiplegia in infantsreport of five casesrdquoDevelopmentalMedicineampChildNeurologyvol 22 no 6 pp 784ndash791 1980
[4] B Al-Bulushi A Al-Hashem and B Tabarki ldquoA wide clinicalphenotype spectrum in patients with ATP1A2 mutationsrdquoJournal of Child Neurology vol 29 no 2 pp 265ndash268 2014
[5] M T Sweney TMNewcomb andK J Swoboda ldquoThe expand-ing spectrum of neurological phenotypes in children withATP1A3mutations alternating hemiplegia of childhood rapid-onset Dystonia-Parkinsonism CAPOS and beyondrdquo PediatricNeurology vol 52 no 1 pp 56ndash64 2015
[6] E L Heinzen A Arzimanoglou A Brashear et al ldquoDistinctneurological disorders with ATP1A3 mutationsrdquo The LancetNeurology vol 13 no 5 pp 503ndash514 2014
[7] A Gergont and M Kacinski ldquoAlternating hemiplegia of child-hood New diagnostic optionsrdquo Neurologia i NeurochirurgiaPolska vol 48 no 2 pp 130ndash135 2014
[8] M T Sweney K Silver M Gerard-Blanluet et al ldquoAlternatinghemiplegia of childhood early characteristics and evolution ofa neurodevelopmental syndromerdquo Pediatrics vol 123 no 3 ppe534ndashe541 2009
[9] B G R Neville and M Ninan ldquoThe treatment and manage-ment of alternating hemiplegia of childhoodrdquo DevelopmentalMedicine and Child Neurology vol 49 no 10 pp 777ndash780 2007
[10] J R Tenney andM B Schapiro ldquoChild Neurology Alternatinghemiplegia of childhoodrdquoNeurology vol 74 no 14 pp e57ndashe592010
Case Reports in Medicine 5
[11] J Ju S Hirose X-Y Shi A Ishii L-YHu and L-P Zou ldquoTreat-ment with Oral ATP decreases alternating hemiplegia of child-hoodwith de novoATP1A3MutationrdquoOrphanet Journal of RareDiseases vol 11 no 1 article no 55 2016
[12] A Roubergue B Philibert A Gautier et al ldquoExcellent responseto a ketogenic diet in a patient with alternating hemiplegia ofchildhoodrdquo in JIMD Reports vol 15 pp 7ndash12 Springer BerlinGermany 2014
[13] A Ulate-Campos C Fons R Artuch et al ldquoAlternating hemi-plegia of childhood with a de novo mutation in atp1a3 andchanges in SLC2A1 responsive to a ketogenic dietrdquo PediatricNeurology vol 50 no 4 pp 377ndash379 2014
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Medicine 5
[11] J Ju S Hirose X-Y Shi A Ishii L-YHu and L-P Zou ldquoTreat-ment with Oral ATP decreases alternating hemiplegia of child-hoodwith de novoATP1A3MutationrdquoOrphanet Journal of RareDiseases vol 11 no 1 article no 55 2016
[12] A Roubergue B Philibert A Gautier et al ldquoExcellent responseto a ketogenic diet in a patient with alternating hemiplegia ofchildhoodrdquo in JIMD Reports vol 15 pp 7ndash12 Springer BerlinGermany 2014
[13] A Ulate-Campos C Fons R Artuch et al ldquoAlternating hemi-plegia of childhood with a de novo mutation in atp1a3 andchanges in SLC2A1 responsive to a ketogenic dietrdquo PediatricNeurology vol 50 no 4 pp 377ndash379 2014
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom