SE9700368 " M T C - D M S A RENAL SCINTIGRAPHY IN THE DIAGNOSIS AND FOLLOW-UP OF ACUTE PYELONEPHRITIS IN CHILDREN Ll \ \ \ V v i I IN DEPARTMENT OF CLINICAL PHYSIOLOGY LUND UNIVERSITY LUND, SWEDEN
" M T C - D M S A RENAL SCINTIGRAPHY IN
THE DIAGNOSIS AND FOLLOW-UP OF ACUTE
PYELONEPHRITIS IN CHILDREN
DEPARTMENT OF CLINICAL PHYSIOLOGY
Sweden SE9700368 LUMEDW-MEFL--1012
99mTc-DMSA renal scintigraphy in the diagnosis and follow-up of
acute pyelonephritis in children
Akademisk avhandling
som med vederbOrligt tillstand av Medicinska Fakulteten vid Lunds
Universitet for avlaggande av doktorsexamen i medicinsk vetenskap
kommer att offentligen
forsvaras i forelasningssal 5, Universitetssjukhuset i Lund,
onsdagen den 28 maj 1997, kl. 13.00
av
LUND 1997
Department of Clinical Physiology University Hospital S-221 85
LUND, Sweden
AuthoKs)
Date of issue 1997-05-28 CODEN: I5RN LUMEDW/MEFL--1012--SE
Sponsoring organization Malmbhus lans landsting, Faculty of
Medicine. University of Lund.
Title and subtitle Tc-DMSA Renal Scintigraphy in the Diagnosis and
Follow up of Acute Pyelonephritis in Children.
Abstract
The aim of the present thesis was to define and evaluate a strategy
for identification of children who are at risk of developing
progressive renal lesions after acute pyelonephritis. Tc-DMSA renal
scintigraphy is widely accepted as the most sensitive method for
detecting parenchymal lesions and diagnosing acute pyelonephritis.
Qualitative and quantitative evaluation standards were elaborated
to improve the interpretation of DMSA scintigraphy. The normal DMSA
distribution pattern, the average background uptake, and
scintigraphic kidney length according to age were assessed in 95
presumably healthy kidneys. Furthermore, typical DMSA distribution
patterns in acute pyelonephritis were assessed on 65 kidneys in 38
children, and typical DMSA distribution patterns of 152 kidneys
with VUR in 101 children with and without previous pyelonephritis.
Measurement of scintigraphic kidney length, width and volume was
validated in piglets and on a kidney phantom. The scintigraphic
kidney length was found to be an accurate measure of renal size,
whereas kidney width and volume were less reliable, at least on
small kidneys. Criteria of kidney swelling in acute pyelonephritis
were defined, and found to be beneficial for identifying
reinfections in the absence of clinical symptoms. In 34 children
with acute pyelonephritis quantitative and qualitative DMSA
scintigraphic findings were correlated to clinical symptoms and
laboratory data, in the acute stage and at follow up. We found that
quantitative DMSA scintigraphy in the acute stage of pyelonephritis
and again after one year will identify children who are at risk of
developing progressive renal lesions. Qualitative assessment of
DMSA distribution pattern is not reliable enough in this
respect.
Key words DMSA-scintigraphy, pyelonephritis, kidney length, kidney
radioactive uptake, progressive renal damage
Classification system and/or index terms (if any)
Supplementary bibliographical information
14111811888 E n g l i s h
ISBN
Price
Distribution by (name and address)
I, the undersigned, being the copyright owner of the abstract of
the above-mentioned dissertation, hereby grant to all reference
sources permission to publish and disseminate the abstract of the
above-mentioned dissertation.
Signature 1997-04-
This thesis is based on the following articles, which will be
referred to in the text by their Roman numerals.
I ""Tc-DMSA renal scintigraphy during kidney maturation. Marika
Bajc and Lena Wallin. Clin Nucl Med 20:211-214, 1995.
II Typical technetium dimercaptosuccinic acid distribution patterns
in acute pyelonephritis. Lena Wallin and Marika Bajc. Acta Pediatr
82:1061-1065, 1993.
III The significance of vesicoureteric reflux on kidney development
assessed by dimercaptosuccinate renal scintigraphy. Lena Wallin and
Marika Bajc. Br J Urol 73:607-611, 1994.
IV Kidney size estimation by DMSA scintigraphy in piglets. Lena
Wallin, Johan Thome, John Palmer and Marika Bajc. Submitted for
publication.
V Kidney swelling - findings on DMSA scintigraphy. Lena Wallin,
Ingemar Helin and Marika Bajc. Clin Nucl Med, May 1997. In
press.
VI Follow up of acute pyelonephritis in children by DMSA
scintigraphy. Quantitative and qualitative assessment. Lena Wallin,
Ingemar Helin and Marika Bajc. Submitted for publication.
Articles I-III and V are reprinted with permission from the
publishers.
CONTENTS Page
ABBREVIATIONS 6
1 INTRODUCTION 7
1.1 Renal imaging agents 7 1.2 Static renal scintigraphy with DMSA
7
1.2.1 Biokinetic behaviour of DMSA 7 1.2.2 Time for imaging 8 1.2.3
Sensitivity for renal lesions 8 1.2.4 Quantification 8
1.3 Kidney size measurements 8 1.4 Urinary tract infection (UTI)
9
1.4.1 Prevalence and importance of UTI 9 1.4.2 The diagnosis of
acute pyelonephritis 9 1.4.3 Pathogenesis of pyelonephritis
10
1.5 Vesicoureteric reflux 10 1.5.1 Pathogenesis of VUR 10 1.5.2
Significance of VUR in renal scarring and controversies 11
1.6 Imaging in febrile UTI 11 2 AIMS OF THE STUDY 12
3 MATERIAL AND METHODS 12
3.1 Material 12 3.1.1 Kidneys with normal distribution pattern 12
3.1.2 Children with acute pyelonephritis 13 3.1.3 Children with VUR
13 3.1.4 Piglets 13 3.1.5 Kidney phantom 13
3.2 Methods 14
3.2.2.1 Kidney size measurements 15
3.2.2.2 Separate renal function and background activity 15 3.2.2.3
Kidney radioactive uptake 16
3.2.2.4 In "vivo" versus in vitro measurements on piglets 16
3.2.2.5 Kidney phantom 16
3.2.3 Statistical methods 16
4.1.2 Distribution patterns in acute pyelonephritis 17 4.1.3
Changes of distribution patterns at follow-up after
pyelonephritis 17 4.1.4 Distribution patterns in VUR 18
4.2 Quantitative evaluation 19 4.2.1 Kidney size measurements
19
4.2.2 Background activity 20 4.2.3 Kidney size measurements in
"vivo" versus in vitro 19 4.2.4 Kidney phantom 20 4.2.5 Kidney
radioactive uptake 20 4.2.6 Distribution pattern versus KU/AD
22
4.3 Microbiology 22 5 DISCUSSION 23
5.1 Material 23 5.1.1 Kidneys with normal distribution pattern 23
5.1.2 Children with acute pyelonephritis 24 5.1.3 Children with
swollen kidneys 24
5.2 Methods 24 5.2.1 Development of methods 24
5.2.1.1 Change of collimator and radioactive dose 24 5.2.1.2
Movement artefacts 25
5.2.2 Kidney delineation and choice of background 25 5.2.3 Kidney
size measurements 25 5.3 Results 26
5.3.1 Distribution patterns 26 5.3.2 Kidney length 28 5.3.3 Kidney
radioactive uptake 29 5.3.4 Quantitative versus qualitative
evaluation of DMSA
scintigraphy 29 5.3.5 Time for DMSA imaging in UTI 30
6 CONCLUSIONS 31
(Summary in Swedish)
megabecquerel
mercaptoacetyltriglycine
1.1 Renal imaging agents
Various substances have been used for the imaging of renal
parenchyma and renal excretory pathways. Substances excreted by the
urine are used for dynamic imaging. They also give a rough
estimation of the parenchymal morphology. Other substances,
accumulating in the parenchyma, are used for static imaging. They
give a more detailed image of the parenchymal function. The
earliest application of radionuclides in evaluation of renal
function was started with the work of Taplin (1956). He used
l3lI-hippuran that is excreted almost completely by the urine and
has been widely used for dynamic studies and renal clearance
measurement (Blaufox et al 1967). Subsequently l31I-hippuran was
replaced by ""Tc compounds which have better properties for imaging
with gamma camera techniques. The most widely used agents for
evaluation of renal function and morphology are 99mTc-DTPA and
99mTc-MAG3 (Taylor 1991). Because the renal extraction of MAG3 is
twice that of DTP A, MAG3 has to a great extent replaced DTPA for
the evaluation of renal excretory pathways and differential renal
function. For static imaging of renal parenchyma mercurial
diuretics were first utilised (McAfee & Wagner 1960). They were
marked with 203Hg that was later replaced by 197Hg (Sodee 1964).
The mercurials delivered a high radiation dose, a circumstance that
urged the development of 99mTc compounds for substitution. One of
the first ""Tc compounds introduced for imaging of renal
parenchymal was ""Tc-gluconate (Charamasa & Budikova 1969).
Thereafter ^ T c - penicillamine substances were developed (Halpern
et al 1972, Taylor et al 1977). Those compounds did not became
widely used. A new substance, dimercaptosuccinic acid (DMSA), was
introduced in 1974 by Lin et al. It showed excellent imaging
properties and has become the predominantly used compound for
evaluation of renal parenchyma.
1.2 Static renal scinrigraphy with DMSA
1.2.1 Biokinetic behaviour of DMSA
Dimercaptosuccinic acid accumulates in epithelial cells of the
proximal tubules (Lin et al 1974). It is extracted from the blood
in pentubular capillaries (Muller- Suur & Gutsche 1995). The
image shows the functioning renal cortex. Uptake defects represent
areas where the mechanism for uptake in tubular epitelial cells is
blocked by impaired blood flow and/or impaired tubular uptake from
blood. The biokinetic behaviour of DMSA was studied by Enlander et
al (1974) by cumulative urine excretion of DMSA. They found that 4
- 8 % of the injected dose was excreted after one hour and 26-30%
after 14 hours. The renal extraction was estimated to 4 - 5 % per
renal passage with about 50% accumulated in the kidneys after one
hour. A more recent study of the biokinetic behaviour of DMSA in
children was presented by Evans et al (1996). They found
a slightly lower maximal renal uptake, 42 ± 5 % of the administered
dose, which occurs after 6 - 7 hours. Liver uptake was 5 ± 2 % and
the uptake in the spleen 2 ± 1 %.
1.2.2 Time for imaging
Arnold et al (1975) found that the DMSA scintigram visualises the
parenchyma without interference from pelvocalyceal system.
Therefore he recommended DMSA imaging for the detection of
parenchymal lesions such as infarcts and pyelonephritic scars.
Subsequently, DMSA scintigraphy was evaluated in a variety of renal
diseases (Handmaker et al 1975). They showed that imaging performed
two hours after the injection provided an excellent evaluation of
functional renal anatomy. DMSA uptake reaches its maximum within 7
hours (Gordon et al 1987, Evans et al 1996). Because the half life
time for " "Tc is 6 hours scintigraphy should be performed within 6
hours after administration. In most centres scintigraphy is
generally performed 2 - 4 hours after DMSA administration.
1.2.3 Sensitivity for renal lesions
Studies in animals show that static renal scintigraphy with DMSA is
the most sensitive imaging method to identify parenchymal lesions
(Rushton et al 1988, Parkhouse et al 1989, Risdon et al 1994).
Typically the sensitivity is 80 - 90 % at a specificity above 90%
with planar imaging. Using tomographic technique some authors have
reported higher sensitivity compared to planar images (Giblin et al
1993, Majd et al 1996). This result was not reached by Mouratidis
et al (1993).
1.2.4 Quantification
Quantitative evaluation of absolute renal DMSA uptake has been
reported but no method has yet been generally accepted (Gordon et
al 1987, Groshar et al 1991, 1994, Evans et al 1996). In most
studies with DMSA scintigraphy evaluation is based on qualitative
data, describing parenchymal distribution/uptake defects.
Occasionally quantitative data of separate renal function are
presented (Stokland 1996).
1.3 Kidney size measurements
Measurement of renal size in adults was practised as early as in
the 1950s on intravenous urography (IVU) (Billing 1954, Moell
1956). In children normal renal growth is accepted as an indication
of a healthy kidney. Kidney size has been related to age, height,
weight and body surface area (Hodson et al 1962, Simon 1964,
Currarino 1965, Gatewood et al 1965). Geometric formulas have been
used to increase the exactness of evaluation (Friedenberg et al
1965, Guy & Mounic 1971, Hegediis 1972). For estimation of
kidney size the relation between kidney length and vertebral height
was found to be the most adequate guide (Eklof &
Ringertz 1976). Ultrasonography (US) offered a new possibility for
renal size measurement. Comparing sonographic kidney length with
urographic kidney length it was observed that the urographic length
exceeded the sonographic by 16 % (Haugstvedt & Lundberg 1980).
This discrepancy was not confirmed when compensation for the
magnification factor was practised (Hederstrom & Forsberg
1985a). A difficulty with measurement of renal size with US is that
the method is operator dependent. Inter- and intra-operator
variability of typically 7-13 % and 1-7 %, respectively have been
reported (Hederstrom & Forsberg 1985b, Schlesinger et al 1991,
Sargent & Wilson 1992 Emamian et al 1995). Normal values for
kidney length on DMSA scintigraphy were presented by Sisayan et al
(1994). They related kidney length to age, height and weight. They
found that kidney length had non-linear relationships with the age
and weight of the patients but correlated linearly with the height.
Comparing scintigraphic and sonographic length they found that the
scintigraphic length exceeded the sonographic by on average 10
mm.
1.4 Urinary tract infection (UTI)
1.4.1 Prevalence and importance of UTI
Urinary tract infection occurs in 1 - 4 % of all children (Winberg
et al 1975, Dickinson 1979). Reduction of renal parenchyma is found
in 5 - 10 % either at the first infection or later (Winberg et al
1975). Establishing the diagnosis of UTI is difficult in children,
particularly so in infants. Therefore UTI in children is often
unrecognised and untreated (Jadresic et al 1993). According to
Clarke et al (1995) more than 90 % of children over 5 years with
renal lesions on DMSA scintigraphy have a history of symptomatic
recurrent UTI. Decreased renal function is probably more common in
UTI than previously believed (Pead and Maskell 1994). Progressive
renal scarring (chronic pyelonephritis), may lead to hypertension,
maternal and fetal complications during pregnancy and in some
patients renal insufficiency (Torres et al 1980, Jacobsson et al
1989). About 23 % of end-stage renal disease is thought to be
related to UTI and vesicoureteric reflux (VUR) (Chantler et al
1980, NAPRTCS 1993). Therefore optimal management of UTI in
children is important.
1.4.2 The diagnosis of acute pyelonephritis
The diagnosis of acute pyelonephritis is traditionally based on
clinical signs and symptoms of fever, abdominal or flank pain or
tenderness, associated with pyuria and positive urine culture.
However, infants, and neonates in particular, frequently present
with non-specific clinical findings such as irritability, poor
feeding, failure to thrive, vomiting and diarrhoea (Bergstrom et al
1972). Since the symptoms, especially in infants, are often vague
it is difficult to establish whether the infection involves the
kidneys or is confined to the bladder. Different examinations, such
as ureteral catheterisation, bladder washout, have been used to
determine the site of the infection (Sheldon & Gonzales 1984).
For a variety of
reasons, including unreliability, invasiveness and nonavailability,
these have not gained widespread acceptance for the evaluation of
children with UTI. When the infection involves the kidneys most
children, except neonates, present with fever (Winberg et al 1974).
Other inflammatory parameters i.e. CRP, ESR, and IL-6 in urine and
serum, are in general elevated in pyelonephritis and are widely
used for the diagnosis (Majd et al 1991, Benador et al 1994, Melis
et al 1992). Renal DMSA scintigraphy is highly sensitive and
specific for the diagnosis of pyelonephritis and has emerged as the
method of choice. It is significantly more sensitive in the
detection of acute pyelonephritis than IVU and US (Conway &
Cohn 1994, Rushton 1997).
1.4.3 Pathogenesis of pyelonephritis
The pathogenesis of pyelonephritis is not yet fully understood. It
has been attributed to the interaction of bacterial virulence and
host defence factors. In the presence of VUR infected urine allows
ingress of bacteria into the renal parenchyma and precipitates
infection. In the absence of VUR, ascending infection is related to
the ability of uropathogenic bacteria to adhere to the
uroepithelium (Roberts et al 1985, Bahrani et al 1994).
Experimental studies have shown that P-fimbriated E Coli are more
prone to ascend from the bladder to the kidneys than non-fimbriated
E Coli (Roberts et al 1985). Furthermore, only one type of
P-fimbriae, i.e. mannose-sensitive, has shown to be closely related
to renal scarring (Harber et al 1986). In a majority of patients
with acute pyelonephritis P-fimbriated E Coli are found in urine
cultures. However, this finding does not identify children who
develop parenchymal lesions as demonstrated by DMSA scintigraphy
(Majd et al 1991). In the development of renal lesions the interest
has been focused on the patients' immunological response to
infection (Haraoka et al 1993, Jacobsson et al 1994). An increased
level of the cytokine IL-6 in serum is related to renal involvement
in UTI according to Hedges et al (1992). Bacteria producing
hemolysin and cytotoxic neeroti sing factor seem to induce higher
concentrations of IL-6 in serum (Jacobsson et al 1994). The spread
of IL-6 to serum in patients with acute pyelonephritis may
contribute to the fever and the elevation of CRP.
1.5 Vesicoureteric reflux
1.5.1 Pathogenesis of VUR
Retrograde flow of urine to the ureter is normally prevented by the
valvular action of the ureterovesical junction. Inadequate fixation
of the longitudinal muscle of the ureter to the trigonal
musculature of the bladder leads to VUR. Moreover, it has been
assumed that infection with inflammatory swelling around the
intramural portion of the ureter may be a precipitating factor for
reflux (Whitaker 1976). It is also believed that VUR can be caused
by reversed ureteric peristalsis or urethral- bladder dysfunction
(Jdrgensen 1986).
10
1.5.2 Significance of VUR in renal scarring and controversies
Several systems are used to grade the severity of VUR. They are
based on whether the reflux reaches the ureter, the renal pelvis
and calyces, or whether dilatation occurs (White 1989). However,
the presence or degree of VUR does not seem to influence the long
term renal function according to Berg (1992). Different theories
have been developed to explain renal scarring associated with VUR.
Some authors believe that high renal pressure alone in association
with VUR may cause scarring (Jorgensen & Stodkilde-Jorgensen
1985). Others have shown that changed morphology and dysplasia
develop already in the prenatal period (Anderson & Rickwood
1991, Najmaldin et al 1990). However, VUR without dilatation of the
ureter and pelvis, seen during the first years of life, usually
diminishes or disappears (Edwards et al 1977). Such VUR is more
likely a sign of urinary tract immaturity than of anatomical
abnormality. On the other hand, some authors argue that infected
urine in VUR is the precipitating factor that causes renal scarring
(Smellie et al 1981b, Hannerz et al 1987, White 1989). It remains
controversial whether VUR or infection is the most important factor
behind renal scarring. Many authors have advocated that VUR is the
main cause (Hodson and Edwards 1960, Hinman and Hutch 1962, Hannerz
et al 1987, Smellie et al 1975, White 1989). Others have presented
materials where all children with progressive renal damage had
experienced breakthrough infections in the presence of VUR (Smellie
et al 1981b, Verber & Meller 1989). By using DMSA scintigraphy
it was found that that renal lesions occur even in the absence of
VUR. The authors concluded that presence of VUR is not a
prerequisite for renal scarring (Winberg et al 1982, Jakobsson et
al 1992, Majd & Rushton et al 1992, Benador et al 1994,
Ditchfield et al 1994, Stokland et al 1996). VUR in the absence of
infection causes renal lesions in only about half of the kidneys as
visualised by DMSA scintigraphy (Kass et al 1992). Presumably, VUR
is only one of several risk factors for progressive renal scarring.
Parenchymal lesion after pyelonephritis and repeated UTI are other
factors associated with progressive scarring (Merrick et al
1995a,b).
1.6 Imaging in febrile UTI
Intravenous urography was introduced in the 1920s. The features of
post- pyelonephritic scarring found on IVU have been described by
Hodson (1959). IVU has become a traditional method for the
examination of children with UTI. However, IVU has a low
sensitivity for diagnosing acute pyelonephritis (Little et al 1965,
Silver et al 1976, Traisman et al 1986, Sty et al 1987). Renal US
was subsequently introduced for the diagnosis of pyelonephritis
(Dinkel et al 1986, June et al 1985). Unfortunately, US sensitivity
was not satisfactory for recognising parenchymal lesions
(Bjorgyinsson et al 1991, Rickwood et al 1992, Tasker et al 1993,
Stokland et al 1994). The introduction of DMSA scintigraphy in the
1980s gave a new possibility to visualise renal parenchymal
function. The method was found to have a high sensitivity for
detecting parenchymal lesions
11
(Parkhouse et al 1989, Rushton et al 1988, Risdon et al 1994).
Using DMSA scintigraphy as gold standard it was found that IVU had
a sensitivity of 50 - 59 % and US 26 - 54 % (Bjorgvinsson et al
1991, Rickwood et al 1992, Tasker et al 1993, Stokland et al 1994).
Thereafter many authors have suggested that renal scintigraphy with
DMSA should be the first method for renal imaging in febrile UTI
(Verber et al 1988, Conway & Conn 1994, Merrick 1995b, Rushton
1997).
2 AIMS OF THE STUDY
The overall aim of the present thesis was to define and evaluate a
strategy for identification of children who are at risk of
developing progressive renal lesions after acute pyelonephritis.
For that purpose we chose
- to study the normal DMSA distribution pattern in the kidneys
according to age
- to establish reference values for scintigraphic kidney length
according to age
- to delineate DMSA distribution patterns in acute
pyelonephritis
- to delineate different DMSA distribution patterns in kidneys with
VUR in children with and without a history of pyelonephritis
- to establish the accuracy of scintigraphic kidney size
determination
- to establish criteria of kidney swelling
- to correlate DMSA distribution pattern and kidney activity uptake
to clinical symptoms and microbiological data at follow-up after
acute pyelonephritis
3 MATERIAL AND METHODS
3.1 Material
The patients, 283 children aged 10 days - 13 years, had been
referred to our department with suspected or known renal disease.
For the specific purpose of this study all 282 scintigrams (238
children) in our data base were re-evaluated.
3.1.1 Kidneys with normal distribution pattern (I)
For evaluation of the normal distribution pattern 85 children, aged
10 days - 13 years, were included. In 9 of the children suspicion
of renal disease was subsequently dismissed and both kidneys were
considered healthy. Seventy-six of the children had unilateral
renal disease or malformation and a presumably healthy
contra-lateral kidney. All included kidneys had normal findings on
US and IVU. In 19 children (27 kidneys) scintigraphic kidney length
was compared to sonographic length and in 10 children (17 kidneys)
to urographic length.
12
3.1.2 Children with acute pyelonephritis (II, V, VI)
For the retrospective study of pyelonephritic patterns (II) 38
children, aged 15 days - 7 years, with clinical diagnosis of acute
pyelonephritis were included. In 18 of the children a repeat
scintigraphy after 5 - 8 months was obtained. All children had
undergone renal US before scintigraphy. Micturating
urethrocystography (MUCG) was performed on 34 children, and 8
children had undergone IVU. In the prospective study of
pyelonephritis (VI) 34 consecutive children, aged 14 days - 24
months, were included. All had clinical and microbiological signs
of first time acute pyelonephritis. On all children US was
performed in the acute stage, scintigraphy within a week from onset
of symptoms, and MUCG within 8 weeks. The study of scintigraphic
signs of kidney swelling (V) comprised 38 children with clinical
diagnosis of pyelonephritis, aged 15 days - 7 years (median 6
months). All children who were imaged two or three times by
identical techniques were included. None of the children had
hydronephrosis or other renal anomalies. The initial renal
scintigraphy was performed on 24 children within a month after
onset of symptoms, and on 14 children in a later phase. All
underwent follow-up scintigraphies within 2 years.
3.1.3 Children with VUR (III)
For the study of distribution patterns in VUR 101 children (152
kidneys) with VUR in one or both kidneys were included. Children
with acute pyelonephritis, and kidneys with VUR associated with
additional abnormalities, were excluded from the study. Patients
whose kidneys or ureters had been operated on were also
excluded.
3A A Piglets (IV)
For the validation of size measurements we used ten healthy
piglets, weighing 4 - 18 kg.
3.1.5 Kidney phantom (IV)
A kidney phantom was made from Plexiglas. It had an oval-shaped
cavity with length 120 mm and width 60 mm. A central mass was
inserted (like the yolk in an egg) simulating the marrow and
pelvis. The remaining space (the egg white), representing the
cortex, was 1 - 2 cm wide and had a volume of 155 ml.. The kidney
phantom, surrounded by plastic bags filled with water to simulate
viscera in the abdomen, was placed in a Plexiglas container
simulating the abdominal walls and the spine.
13
3.2 Methods
The children were examined at the Department of Pediatrics. They
were referred to us on the basis of clinical symptoms, biochemical
and microbiological findings and urine specimens indicating acute
pyelonephritis. Urine specimens were analysed according to growth
and type of bacteria at the Department of Clinical Microbiology.
MUCG, US, and IVU were performed at the Department of
Roentgenology. VUR was graded on a scale of 1-5 (Lebowitz et al
1985). Renal scintigraphy was performed 3 hours after intravenous
injection of 99mTc- DMSA. Acquisition was performed in the
posterior view with the child lying supine using a
large-field-of-view (27x50 cm2) gamma camera equipped with a
low-energy, parallel-hole collimator, interfaced to a computer.
Data were collected in a 256x256 matrix, with zoom factor 2.5. In
the retrospective studies (I-m) acquisition was performed in one
static image during 10 minutes (ca 300 kcounts), using a
general-purpose collimator. The dose was 0.5 MBq ""Tc-DMSA per kg
body weight (minimum 10 Mbq). In the study of kidney swelling (V)
and the prospective study (VI) acquisition was performed in dynamic
mode with 10 one-minute images (15 for children under 7.5 kg) using
a high-resolution, parallel-hole collimator. The dose was 2 MBq
""Tc-DMSA per kg body weight, (minimum dose 15 MBq). The activity
in the syringe was measured before and after injection. Images were
checked for possible movements. Alignment of individual images was
performed when necessary. The dynamic study images were then added
to yield one static image on which evaluation was performed.
3.2.1 Qualitative evaluation
In the qualitative evaluation distribution pattern was analysed.
For the purpose of making the evaluation more objective images were
prepared and presented in a standardised manner with both smoothed
and unprocessed versions of the image (Fig 1). Irregularities in
kidney activity uptake were delineated by iso-count level contours
of 20, 40, 60 and 80% of maximum pixel count in the entire image
after smoothing 9x9 twice. Criteria for kidney swelling: 1)
isocount level contours of 20 % - 60 % wider apart than ordinary in
the whole kidney (Fig 1) 2) localised widening between isocount
level contours of 20 % - 60 % (can occur together with 1) above) 3)
kidney length >110 % of expected according to age 4) ratio
between kidney width and length > 0.55 5) average kidney uptake
divided by average background activity < 10.0 6) kidney length
increase since a previous investigation 1.5 mm more than expected
according to age Swollen kidney was defined when three or more of
the above criteria were fulfilled.
SIN FUNCT!0M OX
SIN OX
63 nun LENGTH 54 nit
27 MM WIDTH 34 MM
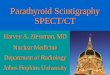
Figure 1 An image presentation, comprising 4 panels was used for
the evaluation. The upper panels show smoothed images. The lower
panels show unsmoothed images. Iso-contours are presented at the
upper right panel. ROIs over the kidneys and illustration of kidney
length and width measurements are presented at the lower right
panel. The scintigraphy shows the dorsal view of the kidneys of a
1-month-old girl with acute pyelonephritis. The left kidney has a
normal distribution pattern. The right kidney fulfils the criteria
for swollen kidney. It shows a large uptake defect in the upper
pole and a smaller defect in the lower pole.
3.2.2 Quantitative evaluation
Quantitative evaluation includes the measurement of kidney length
and width, separate renal function, background activity, and kidney
uptake in percent of administered dose (KU/AD).
3.2.2.1 Kidney size measurements
Kidney length was measured as the longest distance from pole to
pole on the 20 % iso-contour (I-VI). Kidney width was measured on
the 20 % iso-contour on hilus level at right angle to renal length
axis (Fig. 1) (IV - VI).
3.2.2.2 Separate renal function and background activity (I,
VI)
For the measurement of separate renal function regions of interest
(ROIs) were defined over each kidney by the 20 % iso-contour.
Separate renal function was expressed as fraction of the total
renal function. Accordingly, the number of counts in each kidney
was divided by the sum of counts in both kidneys without background
subtraction (I-VI). For background estimation a T-shaped region
above and between the upper kidney poles was used (I, V, VI).
15
3.2.2.3 Kidney radioactive uptake (V, VI)
For calculation of KU/AD the administered dose was corrected for
physical decay and camera sensitivity. The total number of counts
in the kidneys was calculated in percent of administered dose and
corrected for background activity. To calculate KU/AD in each
kidney the separate renal function was used. No correction for
tissue attenuation was applied.
3.2.2.4 In "vivo" versus in vitro measurements on piglets
The piglets were sacrificed 3 hours after injecting 2 Mbq ""Tc-DMSA
per kg body weight. Renal scintigraphy was then immediately
performed with the pig in the prone position. Planar 10 minute
images were acquired simultaneously from the posterior and the
anterior view with a large-field-of-view (27x50 cm2) two headed
gamma camera equipped with low-energy, high-resolution,
parallel-hole collimators, and a computer. Data were collected and
managed as for children. Tomography was performed immediately after
planar imaging with a two headed large-field-of-view (38x51 cm2)
gamma camera with 90 degrees between the heads equipped with low
energy high resolution collimators. Data were collected in 128x128
matrix with a zoom factor of 2.19. Rotation time was 30 minutes
with rotation in 45 angular steps (90 azimuths) yielding 180
degrees of acquisition. Kidney volume was estimated from the 30 %
isocount level of maximum voxel count in a set of transversal
slices. Scintigraphic data obtained in the body of the piglet are
denoted "in vivo". After scintigraphy of the piglets the kidneys
were removed. Kidney length was measured from pole to pole and
width at the hilus by callipers. Kidney volume was measured by
submerging it in water in a measuring glass (mean of two
measurements). Planar scintigraphy of the excised kidneys was
performed with the kidneys lying horizontally with each gamma
camera head at a distance of 10 cms from the kidneys.
3.2.2.5 Kidney phantom
The phantom was filled with 25, 50 or 100 MBq pertechnetate
dispersed in 160 ml water. Planar and tomographic images were
acquired. Acquisition and calculations were made as for
piglets.
3.2.3 Statistical methods
Comparisons between different measurements and estimations are
presented as regression diagrams and equations. Statistical
significances were calculated by Student's paired t-test. Values
are expressed by their means ± 1 standard deviation. For
calculating statistical significances of comparisons between
patient groups we used chi-square test for two-by-two contingency
tables with Yates' correction for continuity.
16
4.1.1 Normal distribution pattern (I)
In infants the distribution of DMSA in the kidney is homogenous
(see Fig. 1). Lower activity in the medial part of the kidney is
seen after 2 years of age. This characteristic is more prominent in
older children.
4.1.2 Distribution patterns in acute pyelonephritis (II)
Four different distribution patterns in acute pyelonephritis were
in order of prevalence: (i) pole defect(s), usually wedge-shaped
(Fig. 1), (ii) scattered multiple defects, (iii) swollen kidney
without areas of diminished uptake, and (iv) lateral wedge shaped
defect. Distribution changes were, in the absence of VUR, found in
69 % of the kidneys.
4.1.3 Changes of distribution patterns at follow-up after
pyelonephritis (II, VI)
Six months after acute pyelonephritis complete normalisation or
improvement of the distribution pattern was found in 66-81 % of
kidneys. Unchanged distribution pattern was found in 7 - 12 %. On
the other hand, more pronounced changes were found in 11 - 22 %. At
the 1 year control no further improvement of the distribution
pattern was seen in the kidneys which showed improved or unchanged
pattern at 6 months. On the contrary in 34 % of the kidneys new
parenchymal changes appeared. These distribution changes, not
visible on the 6 month control, were always on the same locations
as changes in the acute stage (Fig 2).
4.1.4 Distribution patterns in VUR (III)
Three main types of pathological DMSA patterns were found in VUR:
(i) dysplasia, i.e. a small kidney with generally decreased uptake
(23 %), (ii) medial defect (25 %) and (iii) pole defects (17 %).
Normal distribution pattern was found in 31 % and atypical patterns
in 4 %. Normal pattern was significantly more frequent in kidneys
with reflux grade 1-2. Dysplasia was significantly more frequent in
kidneys with reflux grade 4-5.
4.2 Quantitative evaluation
4.2.1 Kidney size measurements
Average kidney length is 56 mm at birth (I). The kidney length
increases with 12 mm during the first year and with 4 mm per year
thereafter to puberty (Fig 3). In the younger children
scintigraphic length was in most cases larger than the sonographic
length (I). In the older children similar values were obtained with
both techniques. Urographic values were in general higher. In
children with VUR (III), and no history of pyelonephritis 42 % of
kidneys
17
were smaller than expected, according to age. In children with VUR
and a history of pyelonephritis 52 % of kidneys were smaller than
expected. In the acute stage of pyelonephritis (VI) mean kidney
length was 101 ± 9 % of expected, according to age. After 6 months
the length had decreased slightly, but significantly, to 99 ± 7 %
(p = 0.002).
51 H DX
51 i FUNCTION 49*:
SIN OX 79 raw LENGTH 98 vn 42 Hi WIDTH 46 m»
'51 "j D;<
'^' FUNCTION 55*
SIN DX 79 wra LENGHT 93 mm 43 ma WIDTH 44 nut
•31 -i
MM
Figure 2 DMSA scintigraphies (dorsal view) on a 16 months old girl.
Left panels show unprocessed images. Right panels show smoothed
images with iso-count level contours of 20, 40, 60, and 80% of
maximum pixel count. In the acute stage (upper panels) there is a
large uptake defect in the upper pole of the right kidney. After 6
months (middle panels) this defect has disappeared. Decreased
uptake has appeared in both poles of the left kidney. After another
6 months (lower panels) the uptake has improved in the left kidney.
In the right kidney a new uptake defect has appeared in the upper
pole.
18
4 7 10
13
Figure 3 Kidney length in relation to age of 94 healthy kidneys in
85 children, aged 10 days to 13 years. The dotted lines show ± 2
standard deviations of the regression lines. (Regression lines are
not shown.)
One year after pyelonephritis the length was 100 ± 7 %. Also this
slight increase, compared to the 6-month observation, was
significant (p = 0.004). A different behaviour of kidney length was
observed in six children with verified reinfection on the second
DMSA scintigraphy (V). At that time criteria for swollen kidney
were fulfilled in these children. On the initial scintigraphy the
kidney length was 94 ± 5 % of expected according to age. The length
had increased to 99 ± 6 % on the second scintigraphy (p - 0.01). On
the third scintigraphy the length had decreased to 94 ± 5 % (p <
0.001) (Fig 4).
4.2.2 Background activity (I, V, VI)
In healthy children the background activity is low. It is fairly
low even in the youngest infants, e.g. 14 % at birth, decreasing to
6 % during the first year of life, with no further change
thereafter (I). In the acute stage of pyelonephritis the background
activity was on average higher than at follow-up i.e. 14 ± 4 % and
10 ± 2 %, respectively (p< 0.001) (V, VI).
4.2.3 Kidney size measurements in "vivo" versus in vitro (IV)
Scintigraphic kidney length in vivo overestimated anatomical kidney
length by 2.6 ±2.0 mm (3.9 ±2.4 %) (Fig 5). Overestimation of
scintigraphic width in vivo, 2.4 ±1.9 mm, was similar to that of
length which means that the difference in percent was larger (7.8
±3.9%).
19
120% ->
110%
100% -
90% -
80% -
70%
1 :st 2:nd 3:rd 1:st 2:nd 3:rd scan
Figure 4 Kidney length in percent of expected according to age on
the initial, second, and third scintigraphy in 6 children (11
kidneys) with signs of swollen kidney on the second scintigraphy
(filled circles), and in 11 children (19 kidneys) with no signs of
swelling on any scintigraphy.
The tomographic in vivo volume determination showed differences
from submersion data which tended to decrease with increasing
kidney size (Fig. 6). The average difference was 4.4 ± 5.0 ml (23
±13 %). Change of cut-off level for renal delineation did not alter
the overestimation of volume in vivo.
4.2.4 Kidney phantom (IV)
At a cut-off level of 20 % of maximum pixel count, the
scintigraphic phantom length overestimated the phantom callipers
length by 6 mm (5 %). The corresponding figure for width was 5 mm
(8 %). At a 35 % cut-off level the scintigraphic length and width
underestimated the phantom length and width by 2 mm (2 %) and 3 mm
(5 %), respectively. At a cut-off level of 30 % of maximum voxel
count the tomographic phantom volume overestimated the phantom
volume by 17 ml (11 %). With a cut-off level of 35 % of maximum
voxel count the tomographic volume underestimated the phantom
volume by 15 ml (10 %).
4.2.5 Kidney radioactive uptake (V, VI)
The kidney uptake (KU/AD) was lowest in the acute stage of
pyelonephritis i.e. 9.6 ± 2.5 At follow-up KU/AD had increased to
12.1 ± 2.2 (p < 0.001) at 6 months without further significant
increase.
10
100
90
80
70
60
1
50 60 70 80 90 100
Callipers length of excised kidneys (mm)
Figure 5 Relation between scintigraphic kidney length in situ of 10
piglets and calliper length of excised kidneys.
Tomographic kidney volume in vivo (ml) 76
65
55
45
35
25
15
4 •
Submersion volume of excised kidneys (ml)
Figure 6 Relation between tomographic kidney volume in situ of 10
piglets and submersion volume of excised kidneys.
21
20% -
18%
16%
14%
12%
10%
8%
6%
4%
1:st 2:nd 3:rd 1:st 2:nd 3:rd scan
Figure 7 Kidney radioactive uptake in percent of administered dose
(KU/AD) on the initial, second, and third scintigraphy in 6
children (11 kidneys) with swollen kidney on the second
scintigraphy (filled circles), and in 11 children (19 kidneys) not
fulfilling the criteria of swollen kidney on any occasion (open
circles).
A different behaviour of KU/AD was observed in six children with
verified reinfection on the second DMSA scintigraphy (V). They had
on the initial scintigraphy a KU/AD of 11.7 ± 2.0. On the second
scintigraphy KU/AD had decreased slightly, but significantly to
10.4 ± 2.5 (p = 0.005). On the third scintigraphy KU/AD had
increased to 13.8 ± 1.5 (p < 0.001) (Fig 7).
4.2.6 Distribution pattern versus KU/AD (VI)
Distribution pattern and KU/AD did not correlate closely.
Normalised distribution pattern or less pronounced uptake defect
was found in 35 % of kidneys with decreased KU/AD. On the other
hand it was found that in 30 % of kidneys with increased KU/AD the
distribution pattern showed more pronounced uptake defects. A
closer relation was found between KU/AD and infection.
4.3 Microbiology (VI)
All children with urine cultures growing < 104 bacteria/ml at
follow-up had increased KU/AD compared to the preceding
scintigraphy. Conversely, 83 % of children with urine cultures
growing > 104 bacteria/ml at follow-up had decreased KU/AD
compared to the preceding scintigraphy. P-fimbriated strains of E
Coli were infecting agents in 53 % of children in the acute stage.
At follow-up E Coli was infecting agent in 24 % of children with
urine cultures growing > 104
22
Table 1 Infecting agent in the acute stage and in urine cultures at
6 months and 1 year controls ™_____
Number of children
Infecting agent
Acute Culture > 104 bact/ml and Culture > 104 bact/ml and
stage decreased KU/AD at increased KU/AD at
control control
Enterobacter 1
Klebsiella 1
Proteus 1
P-pos. signifies P-fimbriated strains of E Coli, and P-neg.
non-fimbriated strains.
bacteria/ml (Table 1). One of 4 children with progressively
decreased KU/AD had growth of P-fimbriated of E Coli in urine at
each control, whereas two had growth of non- fimbriated E Coli and
one had growth of Proteus at each control.
5 DISCUSSION
5.1 Material
5.1.1 Kidneys with normal distribution pattern (I)
To be able to identify pathological features on DMSA scintigraphy
it is essential to know the normal distribution pattern, according
to age. A reference material is especially important in infancy
because of the kidney maturation process (Aperia et al 1981,
Strauss et al 1981). The difficulties in obtaining reference
material in children are well known. It is in general not ethically
justifiable to perform studies on children without suspected or
known disease. The "normal" material for our study (I) is based on
two groups of children. The first group comprised children with
subsequently dismissed suspicion of renal disease, in whom kidneys
were normal as demonstrated by US, MUCG and IVU. The second group
were children with unilateral renal disease in whom those kidneys
were excluded only because they had duplex ureter/pelvis,
hydronephrosis or VUR. It need to be pointed out that the excluded
kidneys did not have seriously reduced uptake and
23
therefore would presumably not have lead to compensatory
hypertrophy of the studied kidneys. For the purpose of this study
it is reasonable to assume that the studied kidneys were also
normal as regards function and size. In other studies of normal
renal properties patients have been selected on similar grounds.
(Gordon et al 1987, Sisayan et al 1993, Groshar et al 1994, Evans
et al 1997)
5.1.2 Children with acute pyelonephritis (II, VI)
The study of the pyelonephritic distribution patterns was
retrospective (II). We have reason to believe that they are
representative because clinical, laboratory and roentgenologic
data, in this material, do not differ significantly from those in
the prospective study of pyelonephritis (VI). The main difference
between the retrospective and prospective studies is the timing for
follow-up scintigraphy. During the period of the prospective study
special attention was paid to strictly defined times for performing
the clinically indicated scintigraphies. Furthermore, our results
from both studies are in agreement with other studies according to
the distribution of parenchymal changes and the prevalence of VUR
(Melis et al 1992, Majd & Rushton 1992, Benador et al 1994,
Stokland et al 1996). In study VI only children with first time
pyelonephritis under 2 years of age were included. The reason was
to avoid children with previous undiagnosed infections that may
compromise the interpretation of scintigrams.
5.1.3 Children with swollen kidneys (V)
In the study of swollen kidneys the scintigraphies were performed
at varying times. Children who developed infections during the
study were identified by DMSA scintigraphy. We therefore believe
that the results of this study can contribute to the understanding
of scintigraphic findings in acute pyelonephritis and influence the
management of children with UTI. We recognise that the study design
has limited the possibility of drawing further conclusions.
5.2 Methods
5.2.1 Development of methods (V, VI)
During the progress of this study the scintigraphic method for
clinical routine was gradually refined.
5.2.1.1 Change of collimator and radioactive dose
To increase image quality a high-resolution collimator, and a
higher dose of DMSA (2 Mbq/kg body weight, minimum 15 Mbq) were
introduced. The dose is similar to that recommended by the European
Association of Nuclear Medicine. The change was introduced between
studies III and V. The effect of the change on image interpretation
was evaluated on repeated scintigraphies in children referred for
examination both before and after the change. With high-resolution
collimator small pattern inhomogeneities became slightly more
distinct, without significant influence on the distribution
pattern. The collimator change may,
24
however, have increased the sensitivity for detecting small
pyelonephritic lesions. In the retrospect study of acute
pyelonephritis (II), before the change we found pyelonephritic
lesions in 80 % of the kidneys. In the prospective pyelonephritic
study (VI) after the change, the frequency of pyelonephritic
lesions was slightly higher i.e. 90 % of the kidneys. However, both
frequencies are in the same range as that of others who found a
sensitivity of 80 - 90 % for detecting renal pyelonephritic lesions
in experimental studies (Rushton et al 1988, Parkhouse et al 1989,
Majd & Rushton 1992, Risdon et al 1994).
5.2.1.2 Movement artefacts
Immobilisation of the child by a vacuum pillow was introduced
between studies III and V. By changing acquisition from static to
dynamic mode with 10 one- minute images we were able to register
movements. The vacuum pillow minimises, but does not completely
prevent, movements of the child. In the dynamic study images can be
corrected for movements, when necessary, by shifting one or more of
the images. Thus re-acquisition can to a great extent be avoided.
The possible effect of movement corrections on image quality was
evaluated by comparing length measurements and distribution
patterns on corrected and uncorrected summation images. Movements
of 2 mm or less were found in 26/30 patients. These movements did
not influence length measurements or the uptake pattern. Movements
of 3 - 4 mm were found in 4 children. These movements caused less
distinct uptake defects on uncorrected images (unpublished data).
The improvements gained by the vacuum pillow and the dynamic
acquisition were modest. We conclude that the principal findings in
studies I-III are valid also after the modification of the
method.
5.2.2 Kidney delineation and choice of background (I-VI)
To get a standardised and objective kidney outline, the margins
were defined by the iso-contour of 20 % of maximum pixel count,
estimated in the entire image. This approach yields a cut-off level
that is the same for both kidneys. A problem can arise when renal
function is severely reduced, i.e. when background is high (near 20
%). As the background activity in general is low, correction for
background was used only for calculating K.U/AD but not for
separate renal function. Comparing different background regions it
was found that the choice of background is unimportant at near
normal renal function. If the renal function is poor the choice of
background could be critical when measuring separate renal function
(Gordon etall987).
5.2.3 Kidney size measurements (IV)
For validation of kidney size measurements (IV) we chose piglets
with kidney size of relevance for pediatnc practice. The kidney
phantom was of adult kidney
25
size to represent the upper part of the size range. Because imaging
was performed with equipment that was also used for clinical
studies, the piglets had to be sacrificed before imaging. We have
therefore not taken into account the possible effect of respiratory
movements. The tomographic kidney volume overestimated the
anatomical volume consistently. The overestimation of the volume
was greatest for the smallest kidneys. Thus kidney volume is not a
reliable measure of kidney size in pediatric praxis. Kidney length
was the most accurate measure of kidney size. The cut-off level of
20 % of maximum pixel count was chosen to define kidney margins, in
the planar image, because on that level the border between kidney
and background is particularly sharp. For lower cut-off levels the
delineation of the kidneys may be less distinct, particularly in
the diseased kidney. We found that with a cut-off level of 20 % the
scintigraphic kidney length overestimates the anatomical kidney
length by 4 % on average. This overestimation is a systematic error
that, to some extent, can compensate for the inclination of the
kidneys to the image plane. This inclination averages 25-30 degrees
according to Farrant & Meire (1978). Considering the shape of
the kidney such an inclination would render an underestimation of
the kidney length of approximately 6 %. The positions of the
kidneys do not generally vary between examinations, as shown on
consecutive scintigraphies. Therefore, such systematic errors are
less important on subsequent examinations, when the child is its
own control. Our measurements of renal length on the scintigraphic
image is standardised and essentially operator independent, with
inter- and intra-observer variability below 2 % (unpublished data).
On the contrary, US inter- and intra-operator variability are high,
on average 7-13 % and 1-7 %, respectively, as reported by
HederstrGm & Forsberg (1985), Schlesinger et al (1991), and
Sargent & Wilson (1992). On repeated examinations this
variability cause difficulties of knowing whether changes in renal
size are due to observer variability, kidney growth, or diminished
renal size.
5.3 Results
5.3.1 Distribution patterns (I-III, V-VI)
In the normal kidney the DMSA distribution is described as
homogeneous throughout the cortex. In the medial part of the kidney
lowered and heterogeneous uptake, corresponding to pelvis and areas
overlying the pyramids is reported as normal in all ages (Piepsz et
al 1991, Majd & Rushton 1992, Eggli & Tulchinsky 1993). We
have developed the pattern recognition further by describing the
change of the distribution with age (I). During the first two years
of life the DMSA distribution is fairly homogeneous in the entire
kidney that often has a rounded form. This pattern very probably
reflects the lobular architecture of the immature kidney (Chantler
1976). From about two years of age the uptake in the medial part of
the kidney is slightly lowered and heterogeneous. The older the
child the more evident is this heterogeneity. We believe that
during the maturation
26
process the kidney changes form and becomes more elongated with the
pelvis gradually growing wider. Unawareness of this different
distribution pattern in the youngest children may lead to
underdiagnosis of pyelonephritis, and may have contributed to the
lower incidence of pyelonephritic changes at lower ages (Benador et
al 1994, Stokland et al 1996). Acute pyelonephritis is usually
manifested at scintigraphy as single or multiple areas of varying
degrees of diminished cortical uptake of DMSA. We found that the
majority of lesions occur typically in both poles (II, V, VI). The
second most common pattern is scattered multiple areas of
diminished uptake. Similar results are reported by others (Monsour
et al 1987, Majd & Rushton 1992, Eggli & Tulchinsky 1993).
The third most common pattern in our material was enlarged kidney
without distinct uptake defects. Such a pattern was described as a
less common finding by Majd & Rushton (1992). Some authors
believe that this pattern represents the most severe form of
pyelonephritis (e.g. Eggli & Tulchinsky 1993). An enlarged
kidney with generally decreased uptake fulfil our criteria of
swollen kidney. Swelling of the kidney is often present
simultaneously with cortical uptake defects, and then often escapes
attention on scintigraphy evaluation. However, swelling of the
whole kidney, without distinct uptake defects, appear more
frequently than generally appreciated. Such a DMSA distribution may
be interpreted as normal and result in inaccurate treatment. The
recognition of the swollen kidney is particularly important when
clinical symptoms are not specific. Normalisation/improvement of
the distribution pattern at six months after acute pyelonephritis
was found in 66 - 81 % of the kidneys. This rate of improvement is
similar to data reported by Rosenberg et al (1992). However, it is
difficult to find comparable studies in the literature because of
the different times for follow-up scintigraphy. At the 1 year
control no further improvement of the distribution pattern was seen
in kidneys which showed improved or unchanged pattern at the 6
month control. This is in agreement with Eggli & Tulchinsky
(1993). In other studies with follow-up at 1 -2 years the rate of
normalisation of pathological acute scintigrams varies between 44
and 64 % (Jakobsson et al 1994, Stokland et al 1996). The reason
for this variation may depend on the selection of patients that
varies according to age and previous infections. Those factors can
greatly influence the distribution pattern. Moreover, subjective
variations in interpretation may contribute (Piepsz et al 1993,
Patel et al 1993). More pronounced distribution changes at one year
control compared to 6 months was found in 34 % of the kidneys. A
similar finding was observed by Stokland et al (1996). They found
an abnormal DMSA scintigram at follow-up after a normal initial
scintigram in 24 % of the kidneys. An important finding is new
distribution changes, not visible at 6 months, appearing at the one
year control. Interestingly, they were always on the same locations
as changes in the acute stage. Similar results have been reported
by Jakobsson et al (1994). A possible explanation is a silent or a
breakthrough infection between the occasions for imaging. Another
possibility is silent or breakthrough infection with swollen kidney
pattern at the first control. A pattern
27
of such nature may obscure small uptake defects which are otherwise
typical signs of pyelonephritis. In study VI we found a higher
incidence of bilateral changes (93 %) than in study II (58 %). The
main reason for this is probably a learning effect, particularly
for recognition of the swollen pattern. The change to
high-resolution collimator may have contributed. The incidence of
bilateral changes in our material is similar to that reported by
Clarke et al (1995). They found bilateral changes in 78 % of boys
under the age of 1 year and in 73 % of girls aged 5 years and over.
On the contrary others have reported bilateral changes in less than
25 % of children (Majd & Rushton 1992, Benador et al 1994,
Stokland et al 1996). In study III we were able to delineate three
main pathological patterns occurring in VUR, pole defects, medial
defect and dysplasia. The types and frequencies of pathological
patterns in the group with VUR without known infection did not
differ from those in the group with VUR and pyelonephritis.
Under-diagnosed pyelonephritis may have contributed to this result.
On the other hand, the pathogenesis of renal scarring is complex
and the mechanisms are not yet fully understood (Risdon 1997). The
pattern with pole defects is in agreement with experimental studies
on animals, where reflux was shown to cause damages with pole
predominance (Jorgensen & Stodkilde-Jorgensen 1985, Ransley
& Risdon 1975). The pattern with medial defect partly reflects
dilated pelvis and calyces. Dysplasia, most frequently found in
kidneys with higher degrees of reflux, may, to a great extent,
represent maldevelopment as a result of prenatal reflux, as argued
by Najmaldin et al (1990), Andersson & Rickwood (1991), and
Risdon (1993).
5.3.2 Kidney length (I-III, V-VI)
Normal renal size and renal growth is in children a recognised
indication of a healthy kidney. There is a close relation between
kidney size and age as found by IVU and US (Hodson et al 1962,
Eklof & Ringertz 1976, Haugstvedt & Lundberg 1980). US has
been proposed as the method of choice for measuring kidney size
(Gordon 1990). Concerning IVU and US kidney length has shown to be
the most convenient measure of renal size (Eklof & Ringertz
1976, Emamian et al 1995). The possibility of using DMSA
scintigraphy for estimation of kidney size was dismissed by Monsour
et al (1987). However, others found it valuable (Sisayan et al
1993). We found that kidney length was not only the most convenient
measure of renal size but also the most accurate (IV). Comparing
scintigraphic to urographic kidney length (I) we found that the
scintigraphic length is in general smaller than the urographic.
Comparing scintigraphic and sonographic measurements no significant
difference was found in the older children, while in infants, the
scintigraphic kidney length was larger. On the other hand, some
authors found that the scintigraphic kidney length exceeded the
sonographic in all children (Sisayan et al 1993). Our results are
partly in disagreement with studies showing no systematic
difference between urographic and sonographic length (Hederstrom
& Forsberg 1985). The renal growth in
28
healthy children was in our material 12 mm during the first year of
life and 4 mm/year thereafter to puberty. Similar results are
reported by others using US and scintigraphy (Rosenbaum et al 1984,
Sisayan et al 1993). We found that renal growth is impaired for
some time after an episode of pyelonephritis but kidney length
usually returns to the expected value a year later (V, VI). A
similar observation was reported by SmeUie et al (1981a). VUR is
another cause of renal growth impairment. Anderson & Rickwood
(1991) found smaller kidneys in the presence of higher grade of
VUR. In our results reduced kidney size was also a frequent finding
among kidneys with higher degrees of VUR (IE). Moreover, we found a
high incidence of kidney growth impairment associated even with low
grade of VUR and in the absence of infection or other
pathology.
5.3.3 Kidney radioactive uptake (V, VI)
An important finding was low KU/AD in the acute stage of
pyelonephritis. At follow-up KU/AD had increased in all children
without bacterial growth in urine. The magnitude of changes was
small but statistically significant. Nevertheless, the KU/AD values
in our results were for many patients within the "normal" range as
estimated by Gordon et al (1985) and Evans et al (1996). However,
in their work the "normal" range is rather wide. On the other hand
we used each patient as her/his own control. Then even small
changes become perceivable. Moreover, our results are not directly
comparable to those of Gordon et al (1985) and Evans et al (1996).
They used attenuation correction which we avoided because the
estimation of kidney depth is operator dependent and may introduce
an additional error.
5.3.4 Quantitative versus qualitative evaluation qfDMSA
scintigraphy (V, VI)
Uptake defects assessed by qualitative evaluation on DMSA
scintigraphy are accepted for the diagnosis of pyelonephritis
(Parkhouse et al 1989, Rushton et al 1988, Risdon et al 1994).
However, we showed that even kidneys without distinct uptake
defects, but fulfilling the criteria for swollen kidney indicate
pyelonephritis. Furthermore, quantification showed low KU/AD in all
kidneys with acute pyelonephritic pattern. When considering only
qualitative assessment of the DMSA image we found that 35 % of
kidneys would have been judged as improved at follow-up, whereas
quantitative measurement showed decreased KU/AD. On the other hand
71 % of kidneys, with qualitative signs of deterioration, showed
increased KU/AD at follow-up. Moreover, 59 % of kidneys without
changes of the distribution pattern showed increased KU/AD. Low
KU/AD was found in children in the acute stage of pyelonephritis
and in 83 % of those with bacterial growth of > 104 bacteria/ml
in urine cultures at follow-up. Therefore KU/AD gives a relevant
estimation of renal function. The frequency of pathological changes
on DMSA scintigraphy in infants were in our results higher compared
to others (Benador et al 1994, Stokland et al 1996).
Unrecognised pattern of the swollen kidneys and small scattered
uptake defects may contribute to this discrepancy. Quantitative
assessment makes it possible to detect decreasing renal function in
the absence of distinct parenchymal lesions. That increases the
sensitivity of DMSA scintigraphy and makes it an important means to
identify children who need further follow-up. An interesting
observation is that recurrent infections caused changes always on
the same locations, a finding also reported by Jakobsson et al
(1994). Therefore it is impossible with only qualitative assessment
to distinguish whether changes are new or have occurred in the
event of breakthrough or silent infection.
5.3.5 Time for DMSA imaging in UTI (VI)
It is important to establish the parenchymal state at the first
infection to allow studies of the progression of renal damage and
of functional loss thereafter. Moreover, DMSA scintigraphy in the
acute stage helps to establish the correct diagnosis of
pyelonephritis in the situation when clinical and laboratory
findings are not clear.
Kidneys which showed improved or unchanged distribution pattern at
6 month follow-up did not show any further improvement at the
1-year control. Therefore it is reasonable to believe that these
changes are permanent. This finding speaks in favour of a 6-month
control for identifying children with permanent lesions as proposed
by Eggli & Tulchinsky (1993). Some authors stressed the
importance of identifying children with permanent lesions (Smellie
1995, Stokland et al 1996). In addition to that we argue that it is
crucial to recognise children who are at risk of developing
progressive renal damage. For this purpose the finding of new
distribution changes at the one year control, not obvious at 6
months, is an important observation. In the kidneys with new
changes decreased KU/AD was found in 70 %. All but one of these
children were free of typical clinical symptoms but had bacterial
growth of > 104 bacteria/ml in urine cultures. With only a 6
month control we would miss those children.
During the year after the first UTI the children are vulnerable and
recurrent infections are common (Winberg et al 1975). Therefore a
1-year follow-up after the first infection is more appropriate for
recognising children who will benefit from further follow-up.
30
6 CONCLUSIONS
Qualitative and quantitative DMSA scintigraphy is a reliable method
to identify children with renal involvement in UTI and
bacteriuria.
Quantitative analysis is a necessary complement to qualitative
assessment of DMSA distribution pattern.
Kidney length is an accurate scintigraphic measure of renal
size.
KU/AD is a reliable index for measurement of renal function.
Renal growth is impeded for some time after pyelonephritis.
Moderate bacteriuria of 104 bacteria/ml of urine is associated with
renal functional deterioration.
In the strategy of identifying children at risk for developing
progressive renal lesions it is necessary to perform DMSA
scintigraphy in the acute stage and at follow-up - preferably after
one year.
31
ACKNOWLEDGEMENTS
I wish to express my sincere gratitude to all those who have
encouraged and helped me to complete this work, especially my
co-authors and the staff at the Department of Clinical Physiology.
In particular I wish to thank:
Associate professor Marika Bajc for her generous guidance and
invaluable support
Professor Bjorn Jonson for constructive criticism and for sharing
his great knowledge
Associate professor Ingemar Helin for fruitful discussions and for
contributing with clinical experience
Associate professor Olle Pahlm for showing interest in my
work
Part of this study was financially supported by grants from the
Faculty of Medicine, University of Lund and Malmohus Lans
Landsting.
32
REFERENCES
Anderson P A M, Rickwood A M K , Features of primary vesicoureteric
reflux detected by prenatal sonography. Br J Urol 67:267-271,
1991.
Aperia A, Broberger O, Elinder G, et al: Post natal development of
renal function in preterm and full term infants. Acta Pediatr Scand
70: 183, 1981.
Arnold R V, Subramanian G, McAfee J G, et al. Comparison of ""Tc
complexes for renal imaging. J Nucl Med 16:357-367, 1975.
Bahrani F K, Massad G, Lockatell C V, Johnson D E, Russell R G,
Warren J W, et al. Construction of an MR/P fimbrial mutant of
proteus mirabilis: Role in virulence in a mouse model of ascending
urinary tract infection. Inf Immun 62(8):3363-3371, 1994.
Benador D, Benador N, Slosman D O, et al. Cortical scintigraphy in
the evaluation of renal parenchymal changes in children with
pyelonephritis. J Pediatr 124:17-20, 1994.
Berg U B. Long-term follow-up of renal morphology and function in
children with recurrent pyelonephritis. J Urol 148:1715-1720,
1992.
Bergstrom T, Larsson H, Lincoln K, et al. Studies of urinary tract
infections in infancy and childhood. J Pediatr 80:858-866,
1972.
Billing L. The roentgen diagnosis of polycystic kidneys. Acta
Radiol 41:305, 1954.
Bjorgvinsson E, Majd M, Eggli K D, et al. Diagnosis of acute
pyelonephritis in children: Comparison of sonography and ""Tc-DMSA
scintigraphy. A J R 157:539-543, 1991.
Blaufox M D, Potchen E J, Merrill J P. Measurement of effective
renal plasma flow in man by external counting methods. J Nucl Med
8:77, 1967.
Chantler C, Carter J E, Bewick M, et al. 10 years' experience with
regular haemodialysis and renal transplantation. Arch Dis Child
55:435-445, 1980.
Chantler C: Newborn disorders. In E Lieberman (ed): Clinical
Pediatric Nephrology. Philadelphia: J B Lippincott, pp 310-316,
1976.
Charamasa O, Budikova M. Method of preparation of a ""To-complex
for renal scintigraphy. Nucl Med 8:301, 1969.
Clarke S E M, Smellie J M, Prescod N, Gurney S, West D J.
Technetium-99m- DMSA studies in pediatric urinary tract infection.
J Nucl Med 37:823-828, 1995.
Conway J J, Cohn R A. Evolving role of nuclear medicine for the
diagnosis and management of urinary tract infection. (Editorial) J
Pediatr 124:87-90, 1994.
Currarino G. Roentgenographic estimation of kidney size in normal
individuals with emphasis on children. Amer J Roentgenol 93:464,
1965.
Dickinson J A. Incidence and outcome of symptomatic urinary tract
infection in children. BrMed J 1:1330-1332, 1979.
Dinkel E, Orth S, Dittrich M, et al. Renal sonography in the
differentiation of upper from lower urinary tract infection. A J R
146:775-778, 1986.
33
Ditchfield M R, De Campo J F, Cook D J, et al. Vesicoureteral
reflux: an accurate predictor of acute pyelonephritis in childhood
urinary tract infection? Radiol 190:413-415, 1994.
Edwards D, Normand I C S, Prescod N, Smellie J M. Disappearance of
vesicoureteric reflux during long-term prophylaxis of urinary tract
infection in children. Br Med J 2:285-288, 1977.
Eggli D F, Tulchinsky M. Scintigraphic evaluation of pediatric
urinary tract infection. Semin Nucl Med 23(3): 199-218, 1993.
Eklof O, Ringertz H: Kidney size in children - a method of
assessment. Acta Radiol Diag 17: 617, 1976.
Emamian S A, Nielsen M B, Pedersen J F. Intraobserver and
interobserver variation in sonographic measurements of kidney size
in adult volunteers. A comparison of linear measurements and
volumetric estimates. Acta Radiol 36:399-401, 1995.
Enlander D, Weber P M, dos Remedios L V. Renal cortical imaging in
35 patients: Superior quality with ""Tc-DMSA. J Nucl Med
15:743-748, 1974.
Evans K, Lythgoe M F, Anderson P J, et al. Biokinetic behaviour of
technetium- 99m-DMSA in children. J Nucl Med 37:1331-1335,
1996.
Farrant P, Meire H B. Ultrasonic measurement of renal inclination:
its importance in measurements of renal length. Br J Radiol
51:628-630, 1978.
Friedenberg M J, Bruce J, Walz A B, et al. Roentgen size of normal
kidneys. Computer analysis of 1286 cases. Amer J Roentgenol
84:1022, 1965.
Gatewood O M B , Glasser R J, Vanhoutte J J. Roentgen evaluation of
renal size in pediatric age groups. Amer J Dis Child 110:162,
1965.
Giblin J G, O'Connor K P, Fildes R D, et al. The diagnosis of acute
pyelonephritis in the piglet using single photon emission
computerized tomography dimercaptosuccinic acid scintigraphy: a
pathological correlation. J Urol 150:759-762, 1993.
Gordon I, Evans K, Peters A M, et al. The quantitation of ""Tc-DMSA
in paediatrics. Nucl Med Commun 8:661-670, 1987.
Gordon I: Urinary tract infection in pediatrics: the role of
diagnostic imaging. Br J Radiol 63: 507, 1990.
Groshar D, Embon O M, Frenkel A, et al. Renal function and
technetium-99m- dimercaptosuccinic acid uptake in single kidneys:
the value of in vivo SPECT quantitation. J Nucl Med 32:766-788,
1991.
Groshar D, Moskovitz B, Gorenberg M, et al. Quantitative SPECT of
Technetium-99m-DMSA uptake in the kidneys of normal children and in
kidneys with vesicoureteral reflux: Detection of unilateral kidney
disease. J Nucl Med 35:445-449, 1994.
Guy E, Mounic M. A propos des mesures des reins. Ann Radiol 14:13,
1971. Halpem S E, Tubis M, Endow J, et al. ""Tc-penicillamine
acetazolamide
complex - a new renal scanning agent. J Nucl Med 13:45-50, 1972.
Handmaker H, Young B W, Lowenstein J M. Clinical experience with "
T c -
DMSA (dimercaptosuccinic acid), a new renal-imaging agent. J Nucl
Med 16:28-32, 1975.
34
Hannerz L, Wikstad I, Johansson L, et al. Distribution of renal
scars and intrarenal reflux in children with a past history of
urinary tract infection. Acta Radiol 28:443-446, 1987.
Haraoka M, Matsumoto T, Mizunoe Y, Kubo S, Koichi T, Ogata N, et
al. Effect of recombinant human granulocyte-colony-stimulating
factor on renal scarring following infection with MS-piliated
bacteria. Renal Failure 15(2): 141-148, 1993.
Harber M J, Topley N, Jenner D E, Mackenzie R K, Steadman R,
Knowlden J M, et al. Virulence factors of urinary pathogens in
relation to kidney scarring. In: Asscher A W, Brumfitt W, editors.
Microbial diseases in nephrology. London, Chichester: John Wiley
& sons Ltd, pp 69-82, 1986.
Haugstvedt S, Lundberg J: Kidney size in normal children measured
by sonography. Scand J Urol Nephrol 14: 251, 1980.
Hederstrom E, Forsberg L. The accuracy of repeated kidney size
estimation by ultrasonography and urography in children. Acta
Radiol 26:603-607, 1985.
Hederstom E, Forsberg L: Kidney size in children assessed by
ultrasonography and urography. Acta Radiol 26: 85-91, 1985.
Hedges S, Stenqvist K, Lidin-Jansson G, Martinell J, Sandberg T, et
al. Comparison of urine and serum concentrations of interleukin-6
in women with acute pyelonephritis or asymptomatic bacteriuria. J
Infect Dis 166:653-656, 1992.
Hegediis V. Three-dimensional estimation of renal shape and volume
at angiography. Acta Radiol Diagnosis 12:87, 1972.
Hinman F Jr, Hutch J A. Atrophic pyelonephritis from ureteral
reflux without obstructive signs ("reflux pyelonephritis"). J Urol
87(3):230-242, 1962.
Hodson C J, Edwards D. Cronic pyelonephritis and vesico-ureteric
reflux. Clin Radiol 11:219-231, 1960.
Hodson C J. The radiological diagnosis of pyelonephritis. Proc R
Soc Med 52:669-672, 1959.
Hodson C J, Drewe J A, Karn M N, et al: Renal size in normal
children. A radiological study during life. Arch Dis Child 37: 612,
1962.
Jacobson S H, Eklof O, Eriksson C G, et al. Development of
hypertension and uremia after pyelonephritis in childhood: 27 years
follow-up. Br Med J 299:703-706, 1989.
Jacobsson S H, Hylander B, Wretlind B, Brauner A. Interleukin-6 and
interleukin-8 in serum and urine in patients with acute
pyelonephritis in relation to bacterial-virulence-associated traits
and renal function. Nephron 67:172- 179, 1994.
Jadresic L, Cartwright K, Cowie N, et al: Investigation of urinary
tract infection in childhood. Brit Med J 307:761-764, 1993.
Jakobsson B, Berg U, Svensson L. Renal scarring after acute
pyelonephritis. Arch Dis Child 70:111-115, 1994.
Jakobsson B, Nolstedt L, Svensson L, SOderlundh S, Berg U.
""Technetium- dimercaptosuccinic acid scan in the diagnosis of
acute pyelonephritis in
35
children: relation to clinical and radiological findings. Pediatr
Nephrol 6:328- 334, 1992
June C H, Browning M D, Smith L P, et al. Ultrasonography and
computed tomography in severe urinary tract infection. Arch Intern
Med 145:841-845, 1985.
Jorgensen T M, Stddkilde-JOrgensen H. Dynamics of the upper urinary
tract during induced vesico-ureteric reflux in pigs. Scand J Urol
Nephrol 19:173- 182, 1985.
Jdrgensen T M. Pathogenetic factors in vesicoureteral reflux.
Neurol Urodyn 5:153-183, 1986.
Kass E J, Fink-Bennet D, Cacciarelli A A, et al. The sensitivity of
renal scintigraphy and sonography in detecting nonobstructive acute
pyelonephritis. J Urol 148:606-608, 1992.
Lebowitz R L, Olbing H, Parkkulainen K V, Smellie J M, Tamminen-
Mobius T E. International system of radiographic grading of
vesicoureteric reflux. Paediatr Radiol 15:105-109, 1985.
Lin T H, Khentigan A, Winchell H S. A ""Tc-chelate substitute for
organoradiomercunal renal agents. J Nucl Med 15:34-35, 1974.
Little P J, McPherson D R , De Wardener H E. The appearance of
intravenous pyelogram during and after acute pyelonephritis. Lancet
1:1186-1188, 1965.
Majd M, Rushton H G, Chandra R, et al.Technetium-99m-DMSA renal
cortical scintigraphy to detect experimental acute pyelonephritis
in piglets: Comparison of planar (pinhole) and SPECT imaging. J
Nucl Med 37:1731-1734, 1996.
Majd M, Rushton H G, Jantaussch B, et al. Relationship among
vesicoureteral reflux, P-fimbriated Escherichia Coli, and acute
pyelonephritis in children with febrile urinary tract infection. J
Pediatr 119:578-585, 1991.
Majd M, Rushton H G. Renal cortical scintigraphy in the diagnosis
of acute pyelonephritis. Semin Nucl Med 2:98-111, 1992.
McAfee J G, Wagner H N Jr. Visualisation of renal parenchyma:
Scintiscanning with 203Hg neohydrin. Radiology 75:820-821,
1960.
Melis K, Vandevivere J, Hoskens C, et al. Involvment of the renal
parenchyma in acute urinary tract infection: the contribution of
""Tc dimercaptosuccinic acid scan. Eur J Pediatr 151:536-539,
1992.
Merrick M V, Notghi A, Chalmers N, Wilkinson A G, Uttley W S. Long
term follow-up to determine the prognostic value of imaging after
urinary tract infections. Part 1: reflux. Arch Dis Child
72:388-392, 1995.
Merrick M V, Notghi A, Chalmers N, Wilkinson A G, Uttley W S. Long
term follow-up to determine the prognostic value of imaging after
urinary tract infections. Part 2: scarring. Arch Dis Child
72:393-396, 1995.
Moeil H. Size of normal kidneys. Acta Radiol 46:650, 1956. Monsour
M, Azmy A F, MacKenzie J R: Renal scarring secondary to
vesicoureteric reflux. Critical assessment and new grading. Br J
Urol 60: 320- 324, 1987.
36
Mouratidis B, Ash J M, Gilday D L. Comparison of planar and SPECT
""Tc- DMSA scintigraphy for the detection of renal cortical defects
in children. Nucl MedComm 14:82-86, 1993.
Müller-Suur R, Gutsche H U. Tubular reabsorption of
technetium-99m-DMSA. J Nucl Med 36:1654-1658, 1995.
Najmaldin A, Bürge D M, Atwell J D. Reflux nephropathy secondary to
intrauterine vesicoureteric reflux. J Pediatr Surg 25:387-390,
1990.
NAPRTCS. Annual Report of the North American Pédiatrie Renal
Transplant Co-operative Study Emmes Corp., 9, 1993.
Parkhouse H F, Godley M L, Cooper J, et al. Renal imaging with
""Tc-labelled DMSA in the detection of acute pyelonephritis: an
experimental study in the pig. Nucl Med Commun 10:63-70,
1989.
Patel K, Charron M, Hobermann A, et al. Intra and interobserver
variability in interpretation of DMSA scans using a set of
standardized criteria. Pediatr Radiol 23:506-509, 1993.
Pead L, Maskell R. Study of urinary tract infection in children in
one health district. Br Med J 309:631-634, 1994.
Piepsz A, Clarke S E M , MacKenzie R, et al. A study on the
interobserver variability in reporting on ""Tc DMSA scintigraphy
(abstract). Eur J Nucl Med 20:867, 1993.
Piepsz A, Gordon I, Hann K: Pédiatrie nuclear medicine. Eur J Nucl
Med 18: 41- 66, 1991.
Raynaud C, Desgrez A, Kellershohn C. Measurement of renal mercury
uptake by external counting: Separate functional testing of each
kidney. J Urol 99:248- 263, 1968.
Rickwood A M K, Carty H M, McKendrick T, et al. Current imaging of
childhood urinary tract infections: prospective survey. Br Med J
304:663-65, 1992.
Risdon R A, Godley M L, Parkhouse H F, et al. Renal pathology and
the ""Tc- DMSA image during the evolution of the early
pyelonephritic scar: an experimental study. J Urol 151:767-773,
1994.
Risdon R A. The small scarred kidney in childhood. Pediatr Nephrol
7:361-364, 1993.
Roberts J A, Suarez G M, Kaack B, Kallenius G, Svensson S B.
Experimental pyelonephritis in the monkey. VII. Ascending
pyelonephritis in the absence of vesicoureteral reflux. J Urol
133:1068-1075, 1985.
Rosenbaum D M, Korngold E, Teele R L. Sonographicassessment of
renal length in normal children. Am J Roentgenol 142:467-469,
1984.
Rosenberg A R, Rossleigh M A, Brydon M P, et al. Evaluation of
acute urinary tract infection in children by dimercaptosuccinic
acid scintigraphy: prospective study. J Urol 148:1746-1749,
1992.
Rushton G H. The evaluation of acute pyelonephritis and renal
scarring with technetium 99m-dimercaptosuccinic acid renal
scintigraphy: evolving concepts and future directions. Pediatr
Nephrol 11:108-120, 1997.
37
Rushton H D, Majd M, Chandra R, et al. Evaluation of
""Tc-dimercaptosuccinic acid renal scans in experimental acute
pyelonephritis in piglets. J Urol 140:1169-1174, 1988.
Sargent M A, Wilson B P M. Observer variability in the sonographic
measurement renal length in childhood. Clin Radiol 46:344-347,
1992.
Schlesinger A E, Hernandez R J, Zerin J M, et al. Interobserver and
intraobserver variations in sonographic renal length measurements
in children. A J R 156:1029-1032, 1991.
Sheldon C A, Gonzales R. Differentiation of upper and lower urinary
tract infections: How and when? Med Clin North Am 2:321-333,
1984.
Silver T M, Kass E J, Thornburg J R, et al. The radiological
spectrum of acute pyelonephritis in adults and adolescents.
Radiology 118:65-71, 1976.
Simon A L. Normal renal size. An absolute criterion. Amer J
Roentgenol 92:270, 1964.
Sisayan M R, Rossleigh M A, Mackey D W J. Nomograms of renal length
in children obtained from DMSA scintigraphy. Clin Nucl Med
18(11):970-973, 1993.
Smellie J M, Edwards D, Hunter N, Normand I C S, Prescod N.
Vesico-ureteric reflux and renal scarring. Kidney Int 8 suppl
4:65-72, 1975.
Smellie J M, Edwards D, Normand I C S, et al. Effect of
vesicoureteric reflux on renal growth in children with urinary
tract infection. Arch Dis Child 56:593- 600, 1981.
Smellie J M, Normand I C S, Katz G. Children with urinary
infection: A comparison of those with and those without
vesicoureteric reflux. Kidney Int 20:717-722, 1981.
Smellie J M. The intravenous urogram in the detection and
evaluation of renal damage following urinary tract infection.
Pediatr Nephrol 9:213-220, 1995.
Sodee D B. A new scanning isotope, 197Hg neohydrin. J Nucl Med 5,
1964. Stokland E, Hellstrdm M, Hansson S, et al. Reliability of
ultrasonography in
identification of reflux nephropathy in children. BR MED J
309:235-239, 1994.
Stokland E, Hellstrom M, Jacobsson B, Jodal U, Lundgren P, Sixt R.
Early ""Tc-dimercaptosuccinic acid (DMSA) scintigraphy in
symptomatic first-time urinary tract infection. Acta Paediatr
85:430-436, 1996.
Strauss J, Daniel S S, James L S: Post natal adjustment in renal
funktion. Pediatrics 68: 802-808, 1981.
Sty J R, Wells R G, Storshak R J, et al. Imaging in acute renal
infection in children. A J R 148:471-477, 1987.
Talner L B, Davidson A J, Lebowitz R L, et al: Acute
pyelonephritis: Can we agree on terminology? Radiology 192:297-305,
1994.
Tasker A D, Lindsell D R M, Moncrieff M. Can ultrasound reliably
detect renal scarring in children with urinary tract infection?
Clin Radiol 47: 177-179, 1993.
Taylor A Jr. Radionuclide evaluation of renal function. Critical
Reviews in Diagnostc Imaging 32( 1): 1 -36, 1991.
38
Taylor A, Davis G, Halpern S, et al. ""Tc-penicillamine: A renal
cortical scanning agent. J Urol 117: 418-420, 1977.
Torres V E, Velosa J A, Holley K E, et al. The progression of
vesicoureteral reflux nephropathy. Ann Intern Med 92:776-784,
1980.
Traisman E S, Conway J J, Traisman H S, et al. The localization of
urinary tract infection with """Tc glucoheptonate scintigraphy.
Pediatr Radiol 16:403-406, 1986.
Verber I G, Meller S T. Serial ""Technetium-dimercaptosuccinic acid
(DMSA) scans after urinary tract infections presenting before the
age of 5 years. Arch Dis Child 64:1533-1537, 1989.
Verber I G, Strudley M R, Meller S T. """To dimercaptosuccinic acid
(DMSA) scan as a first investigation of urinary tract infection.
Arch Dis Child 63:1320- 1325, 1988.
Whitaker R H. Congenital malformations of the urinary tract with
and without infection. In Lieberman E, editor; Clinical Pediatric
Nephrology 2nd ed. pp. 225-271. Philadelphia, Lippincott
1976.
White R H R. Vesicoureteric reflux and renal scanning. Arch Dis
Child 64:407- 412, 1989.
Winberg J, Andersen H J, Bergstrom T, et al. Epidemiology of
symptomatic urinary tract infection in childhood. Acta Paediatr
Scand 252, suppl.:l-20, 1974.
Winberg J, BergstrGm T, Jacobsson B. Morbidity, age and sex
distribution, recurrences and renal scarring in symptomatic urinary
tract infection in childhood. Kidney Int 8:101-106, 1975.
Winberg J, Bollgren I Kallenius G, et al. Clinical pyelonephritis
and focal renal scarring. A selected review of pathogenesis,
prevention and prognosis. Ped Clin North Am 29:801-814, 1982.
39
Populärvetenskaplig sammanfattning
Urinvägsinfektioner är vanliga och förekommer hos 1 - 4 % av alla
barn. Urinvägsinfektion kan ge upphov till njurinflammation och
ibland kvarstående njurskada (ärr) efter läkning. Det finns risk
för fortskridande njurskada om det finns kvarstående njurskada
efter en urinvägsinfektion, om barnet får upprepade
urinvägsinfektioner eller om det finns reflux (tillbakaflöde) av
urin från urinblåsan till njurarna. Fortskridande njurskador kan
leda till högt blodtryck, komplikationer hos fostret och modern vid
graviditet och ibland till njursvikt. För att inte behöva utföra
onödiga undersökningar på många barn är det därför viktigt att
kunna identifiera de barn, som riskerar att få fortskridande
njurskador. Dessa barn måste undersökas och behandlas på ett sådant
sätt att vidare njurskador om möjligt förhindras.
Avsikten med detta arbete var att förbättra diagnostiken av
njurskador vid njurscintigrafi med DMSA så att vi bland barn med
njurinflammation kan identifiera dem, som riskerar att få
fortskridande njurskador.
DMSA (dimercaptosuccinic acid) är ett ofarligt ämne, som tas upp i
njurarna sedan det sprutats i en blodåder. Genom att tillsätta en
liten mängd radioaktivt teknetium (^Tc) kan man registrera DMSA i
njurarna med en gammakamera - scintigrafi, och presentera
resultatet i form av bilder. Bilderna avspeglar njurarnas funktion.
Njurscintigrafi med DMSA infördes på 1970-talet, och är den
känsligaste metoden för att påvisa njurskada. Bildtagningen tar ca
10 minuter och innebär inget obehag för patienten.
Vi standardiserade utförande och utvärdering av njurscintigrafi och
började mäta njurstorlek. För att systematisera tolkningen av
bilderna utvärderade vi på nytt, med den standardiserade metoden,
282 tidigare utförda njurscintigrafi er på 238 barn.
För att kunna upptäcka en njurskada måste man veta hur friska
njurar ser ut. Vi valde för detta ändamål njurar hos barn, som
undersökts för misstänkt njursjukdom, men denna misstanke kunde
avskrivas, och förmodat friska njurar på motsatta sidan hos barn
med ensidig njursjukdom. Upptagsmönster, bakgrundsaktivitet och
storlek i förhållande till åldern kartlades för dessa njurar (94
st).
Vi kartlade därefter de typiska skademönstren vid njurinflammation
hos barn, som undersökts i samband med njurinflammation och efter
tillfrisknandet.
Vi kartlade även olika skademönster på njurar med reflux från
urinblåsan hos barn med respektive utan tidigare
njurinflammation.
För att undersöka hur njurstorleken mätt på scintigrafi ska bilder
stämmer med den verkliga storleken scintigraferade och mätte vi
njurarna på 10 smågrisar. Vi konstruerade och scintigraferade en
njurmodell i plexiglas. Vi fann att
40
scintigrafisk njurlangd stammer val med den verkliga njurlangden
medan matning av bredd och volym ar mindre tillforlitliga,
atminstone pa sma njurar.
Med hjalp av njurarnas scintigrafiska monster och matt kunde vi
upptacka nya urinvagsinfektioner med njurinflammation hos nagra
barn trots att de saknade typiska symptom. Infektionerna kunde
bekraftas med urinodlingar, och barnen tick
antibiotikabehandling.
Darefter foljde vi barn med akut njurinflammation. De
scintigraferades i samband med insjuknandet, efter 6 manader och
igen efter 1 ar. Vi borjade da kvantifieria DMSA, dvs vi matte
mangden DMSA i njurarna vid de olika undersokningstillfallena
Mangden DMSA i njurarna ar ett matt pa deras funktion.
Vi farm att njurtillvaxten hammas en tid efter njurinflammation men
aterhamtar sig, om nya infektioner inte tillstoter. Njurfunktionen
ar fbrsamrad vid insjuknandet i njurinflammation men ocksa hos de
fiesta barn, som vid uppfoljning har bakterier i urinen, aven om de
inte har symptom pa urinvagsinfektion eller njurinflammation. Bam,
som hade bakterier i urinen, med eller utan symptom, bade 6 manader
och 1 ar efter insjuknandet fick fortsatt forsamrad njurfunktion.
Enbart granskning av njurarnas skademonster rackte inte for att
identifiera dessa barn.
Slutsats: Med hjalp av kvantitativ njurscintigrafi med DMSA kan man
identifiera de barn som riskerar att fa fortskridande njurskador
efter njurinflammation. Enbart granskning av njurarnas utseende ar
inte en tillrackJigt kanslig metod. Vi rekommenderar darfor att
kvantitativ njurscintigrafi gors pa barn med urinvagsinfektion vid
insjuknandet och 1 ar efterat. Med regelbundna tata urinodlinga