Embed Size (px)
Citation preview

OCULAR TORTICOLLIS*
BY
Paul R. Mitchell, MD
INTRODUCTION
Tortus, the Latin word for twisted, and collum, for neck, are the roots ofthe word torticollis.' The etiology of torticollis may be orthopedic2 (includ-ing osseous, ligamentous, and muscular), neurologic, or ocular.Orthopedic causes include acquired traumatic or inflammatory cervicalmyositis and congenital muscuiloskeletal abnormalities, such as shorteningand fibrosis of the sternocleidomastoid muscle, Klippel-Feil syndrome,and occipitocervical stenosis.3 Cervical spine subluxation4 is associatedwith congenital muscular torticollis and craniofacial asymmetry.Abnormalities of the skull, such as plagiocephaly, or unilateral coronalsuture stenosis, can result in underaction of the superior oblique, overac-tion of the ipsilateral inferior oblique, and ocular torticollis, with a positiveBielschowsky head tilt test.5 Torticollis associated with hiatus hernia isdescribed as Sandifer syndrome,69 with varying movements of the headand neck, often with twisting of the neck from side to side. Torticollis mayoccur in association with deafness, especially when unilateral, 1'-12 or func-tional or psychiatric disturbances.4"'
Torticollis with an ophthalmic etiology was first described by Cuignet in1873.13 Ocular torticollis is an abnormal head posture that may be adoptedby a patient in order to maintain binocular vision, with a twist or turn of theneck. There may be an associated head tilt, face turn, chin elevation, chindepression, or a combination of these postures.3"4'5 Scoliosis may resultfrom compensation for extraocular muscle paresis.'3 Verzella and associ-ates,'16 in their description of 8 patients, credited von Graefe for recogniz-ing this mechanism in 1864. Ruedemann' and Dietrich and Slack'8 alsodescribed scoliosis and spine misalignment secondary to ocular paresis ofone or more vertical eye muscles. According to Wesson,"' the purpose ofocular torticollis is to assist the patient's vision in 1 or more of 6 ways:
*From Connecticut Children's Medical Center, Hartford, Connecticut and University ofConnecticut Health Center, Department of Ophthalmology, Farmington, Connecticut.
TR. AM. OPHTH. SOC. VOL. XCVII, 1999

Mitchell
1. To improve vision.2. To bring the field of vision into a central area by reducing nasal field
occlusion.3. To strengthen or to achieve single binocular vision.4. To reduce eye discomfort (eg, presbyopia, diplopia).5. To afford eye protection.6. To offer relief from pain.
Nutt'" has described the compensatory head posture as a reflex activi-ty, the stimulus being the presence of diplopia, with the altered head posi-tion allowing stimulation of corresponding retinal areas to allow singlebinocular vision.
BACKGROUND FOR STUDY
In a 2-year prospective study of abnormal head postures based on ocularcauses, Kushner20 identified 8 basic mechanisms causing torticollis in 188patients, in an academic center. In his study, Kushner included patientswho did not demonstrate ocular torticollis but had conditions frequentlyassociated with head posture abnormalities, attempting to attain singlebinocular vision or some degree of fusion. Kushner identified incomitanceas the leading cause of torticollis in 118 patients (62.7%) and found 70cases of vertical incomitance, including 46 with superior oblique palsy, 7with inferior oblique palsy, 6 with Brown syndrome, 5 with blow-out frac-ture, 3 with double elevator palsy, and 3 with superior rectus palsy. Thehorizontal incomitance group consisted of 48 cases, including 31 withDuane syndrome, 7 with acquired horizontal incomitance, (4 after asym-metric surgery, and 3 with sixth nerve palsy), 4 with A or V pattern, and 6with torsional incomitance.
Kushner-2 found nystagmus in 38 cases as the second leading cause ofabnormal head posture (20.2%). Other groups included 12 cases withcongenital esotropia with ocular posture (6.3%), 10 cases permitting fovealfixation (5.3%), 4 cases with cosmetic etiology (2.1%), 3 cases with ocu-lar motor apraxia (1.6 %), 2 cases with spasmus nutans (1%), and 1 casewith astigmatism (0.5%).
MATERIALS AND METHODS
The clinical impression of this author was that the data presented byKushner2" would be somewhat similar to the clinical experience in thisprivate ophthalmology practice. What this author found, however, in com-paring this study to that of Kushner, was that while most cases of torticol-
698

Ocular Torticollis
lis could be explained, there remained a category of patients with torticol-lis without any apparent reason. Because this latter group of patients wasnot addressed in Kushner's study, the intent of this author is to comparethe known etiologies for ocular torticollis as described by Kushner, as wellas to reveal the incidence of, and to attempt to define the etiologies of,unexplained ocular torticollis.
Beginning on December 1, 1992, a 12-month prospective study of allpatients examined by this ophthalmology group was undertaken to identi-fy and categorize the various reasons for ocular torticollis. A total of15,168 patient visits were recorded, and 630 patients were identified withmeasurable ocular torticollis. From this group, a subset of 25 patients wereidentified with ocular torticollis in association with medical or neurologicconditions too complex to be studied in this paper. The remaining 605patients presented with torticollis with a presumed ocular etiology, with-out evidence of musculoskeletal or neurologic etiology.
Of the 15,168 recorded office visits during the year of the study, anumber of patients were examined more than once. After deleting repeat-ed office visits, a patient pool of 11,299 remained, resulting in an incidenceof torticollis of 630 of 11,299 (5.6%). Each of the 630 patients had ademonstrable head posture and had no prior history or evidence of ortho-pedic or neurologic abnormalities. Those without head posture abnor-malities were excluded, in contrast to Kushner's study, which included anumber of patients without head tilt but with a condition associated withhead tilt. Therefore, the percentage comparisons between the 2 studies isnot exact.
Each patient received a complete eye examination, including age-appropriate visual acuity testing, with the notations C, S, M for central,steady, andl maintained fixation for infants, to preferential looking with theTeller visual acuity cards, Mentor BVAT equipment using pictures, "E,""HOTV," and alphabet. Additional measurements included stereoscopictesting, Worth 4-dot test, convergence amplitudes, near point of conver-gence, pupil evaluation, anterior segment, eye rotations, cover testing,cycloplegic refraction, indirect ophthalmoscopy, observing for ocular tor-sion, and direct ophthalmoscopy. When possible, intraocular pressure byapplanation or digitally, red filter, double Maddox rod test, Bagolini striat-ed glasses, Hess screen, or the Lancaster red-green test were performed.
The torticollis of every patient in this study was measured with agoniometer, a protractor with extended, hinged arms, an instrument usedfor orthopedic mneasurements on x-rays. When measuring a face turn, onearm was directed at the fixation target, and the second arm was placedalong the sagittal axis of the head. Measurements were read (lirectly fromthe goniomieter in degrees 1,14,21 (Figs 1 and 2). When a head tilt or chin
699

Mitchell
FIGURE 1
Orthopedic gonioineter tise(l for imeasuremiieint of torticollis.
;,. OVIM A.W
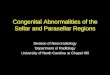
FIGURE 2
Patienit with groniometer place(d oni head, \Nwith one arins directced at fixationi target acnd( onie arimin directioni of head tuirni. Head turin is imeaistired directlx in degrees.
tuck or chin up position was measured, the patient fixated on a distant tar-get at eye level, while 1 arm of the gonioImeter was placed parallel to theaxis of the face, and the second arm perpendicular to the floor. Again, thedegrees of torticollis were read directly from the goniometer. (Thegoniometer is available withouit cost from the Upjohn PhalrmaceuticalCompaniy, 7000 Portage Dr., Kalamazoo, MI 49001; 616-329-8244).
Other deevices to measure torticollis halve been described by variousinvestigators. Cooper and Sandall22 recommended using a perimeter;however, this is very cumbersome and impractical with youing children.Schatz and Urist-3 described anl apparatuis that was strapped to the patient'shead, and involves a protractor, a level, and a directional pointer. Thisinstrument was never popuilarized, however, and is not available commner-cially. Younlg24 proposed a photographic techniquie, which requiires a lineinheadband, three hinged mirrors, and multiple photographs. This is alsoimpractical aind unrealistic when examining young patients. The hand-held goniometer remains the instrument of choice for measuring faceturns, head tilts and chin postures as the patient views age-appropriate dis-tant and near fixation targets.
700

Ocular Torticollis
A number of patients presented with a face turn, head tilt, or chin ele-vation or depression only, while others presented with postures combining2 or 3 of the head or face positions. To compare the measurements of tor-ticollis for patients within each group, as well as for comparison fromgroup to group, it was determined that the degrees of face turn, head tilt,and chin posture for each patient should be combined and listed as "totaldegrees" in each table. This method was deemed the most logical mech-anism for reporting and for comparison purposes, not only of groups with-in this stud, but also for comparison with other studies as well.
RESULTS
Of the 630 patients with ocular torticollis, this author found 330 patientswith incomitance (52.4%), 120 patients with nystagmus (19%), 69 patientswith congenital esotropia with ocular posture (10.9%), and 27 patients withtorticollis permitting foveal fixation (4.3%). Two patients had spasmusnutans (0.3%). No patients were found to have ocular torticollis relating tocosmetic reasons or ocular motor apraxia. Twenty-five patients were deter-mined to have ocular torticollis in association with medical or neurologicconditions (4%). An unexpected high number, 57 patients (9%), werefound with ocular torticollis without any apparent or obvious reason.
Table I summarizes the diagnostic groups described by Kushner2" andgives comparison figures for this study. Kushner described a higher per-centage of patients with incoinitance and with permitting foveal fixation(eg, ptosis, fibrosis syndrome, Moebius syndrome). He noted a total of 8patients with ocular torticollis as a result of cosmetic reasons, ocular motorapraxia, or astigmatism. This study revealed a similar incidence of nys-tagmus as an etiology for torticollis. In this study, however, a higher per-centage of patients presented with congenital esotropia with ocular pos-ture than described by Kushner.20 The 57 patients with unexplained torti-collis comprised 9% of the total group. A comparable group was notdescribed in Kushner's study.
Table II summarizes those patients with ocular posture secondary toincomitance, with nearly 10% of the total group demonstrating superioroblique palsy. Acquired horizontal incomitance, including asymmetricsurgery, A and V pattern, and 6th nerve palsy, accounts for nearly 30% ofthe torticollis pool. The groups of Duane and Brown syndrome combinedfor slightly more than 11% of the torticollis pool.
Several diagnostic categories were extracted from the total patient poolto allow for the calculation of incidence of each group. The office com-puter system in use at the time of this study did not allow for the record-ing of more than 3 diagnoses per office visit. This limits the accuracy of
701

702 Mitchell
TABLE I: ETIOLOGY OF TORTICOLLIS
FACTOR KUSHNER STUDY20 PRESENT STUDY
NO. OF PATIENTS (%) NO. OF PATIENTS (%)
Iincomitaince 118 (62.7) 330 (52.4)Nystagmuts 38 (20.2) 120 (19)Congenital esotropia w,ith
ocular postuire 12 (6.3) 69 (10.9)
Permitting foveal fixationi 10 (5.3) 27 (4.3)Cosmetic 4 (2.1) ( (0)Ocular motor apra:xia 3 (1.6) ( (0)Spasimuts niutanis 2 (1) 2 (0.3)Astigmatism 1 (0.5) 0 (0)No apparenit reason for
torticollis NA 57 (9)Ocular torticollis wvith
associatedmedical/neuirologicconditionis NA 25 (4)
TABLE II: OCULAR POSTURE SECONDARY TO INCOMITANCE
INCOMITANCE NO. OF PATIENTS % OF 630 PATIENTS
WITH TORTICOLLIS
VerticalSuperior oblique palsy 59 9.4Inferior oblique palsy 6 1.0Bro-wn syndrome 25 4.0Double elevator palsy 9 1.4Superior recttus palsy 1 0.2
HorizontalDuane synidromne 46 7.3Acquiredlhorizonitalincomitaince - asymmetricsurgery 48 7.6
Acquire(d horizonitalincomitance - A/V patterni 116 18.4
Acquired hiorizontalincomitance - sixth nervepalsy 1 (0.2
Third nerve pals\ 1 0.2Torsional incomuitanice 4 0.6
Total 330

Octular Torticollis 703
the data to some extent, because there were frequently 4 or more diag-noses recorded for each visit. For example, a child with myopia, torticol-lis, nystagmus, esotropia, and amblyopia could not be categorized withevery disorder. Therefore, the diagnoses in the central column in TableIII are necessarily underreported, and the incidence of torticollis for eachgroup may be slightly higher than would be calculated if all diagnoseswere available.
TABLE III: TORTICOLLIS INCIDENCE*
NO. OF PATIENTS INCIDENCE OF
TORTICOLLIS
Superior obli(quie palsy 59Inferior obli(qtue palsy 6Double elevator palsy 9 PATIENTS WITHSuperior rectius palsy 1 ( "EYE MIUSCLE PALSY"Sixth nerve palsy 1.5Third uerve pals 1, J
Total 91 279 33%
Browvn syodromiie 25 86 30%Duane syndromle 46 128 36%ET-A patterni 29 124ET-V pattern 40 213XT-A pattern 16 129XT-V patteni 31 144All patterns 116 610 19%
Nystagmus 120 290 41%Infantile esotropia 69 812 8.5%Ptosis 16 343 7%
'Total No. of office visits = 15,168Total No. of patients seen = 11,299Total No. of patienits Nwith torticollis = 630Incidence of torticollis (630/11,299) = 5.6%
The classification "eye muscle palsy" was identified 279 times among11,299 patients. A total of 91 patients presented with torticollis and eyemuscle palsies, including 59 superior oblique palsies, 6 inferior obliquepalsies, 9 double elevator palsies, 1 superior rectus palsy, 15 sixth nervepalsies, and 1 third nerve palsy. Therefore, the incidence of torticollis in thepresence of eye palsy was 91 of 279, or 33%. Of the 86 patients examinedwith Brown syndrome, 25 had torticollis (30%). These findings were iden-

Alitchell
tical to Kushneris'2 group of patients witlh Brown syndrome. Nine of the 25patients with Brown Sypndrome demonstrated head tilt, higlher thaln the 5%found by Kushner, and simuilar to a stud(y by, Urist.25 Of the 128 patients withDuiane syndrome, 46 had torticollis (36%). Of the 610 patients with A or V'pattern, 116 demonstrated torticollis (19%). These results are higlher thlathe 9% reported by Kushner" or the 11% reported by Campion.21
The presence of torticollis with nvstagmtus occtur^red in 120 patients of290 with a (liagnosis of nystagmius (41%). There were 812 patients dciag-nosed witlh congenital or infantile esotropia, and 69 diagniosed witlh con-genital esotropia wvith ocular posture (8.5%). A number of infants in the Aand V pattern category had infantile esotropia, but did not develop the full"syndrome" including dissociated vertical dev,iation, excyclotorsion, latentnystagmus, and torticollis, and therefore this category may be unlderre-ported. In his 1987 Edward Jackson Memorial Lecture, von Noorden2-reported that only 26 (6%) of406 patients witlh essential infantile esotropia(lemonstrated anomialouis head postuire, similar to the 8.5% incidenicefounld in this study.
The major causes for ocular posture secondary to incoimitanice aresummarized aind explainied in detail in subsequenit sections of this studc1\;,followved by reviews of nvstagmus, congenital esotropia with ocular pos-ture, perimitting foveal fixationi, n1o apparenit reasoni for torticollis, torticol-lis associated with medical and neurologic conditions, and supelior rectuspalsy) tlhird nerve palsy; and spasmuitis nutitanis.
SUPERIOR OBLIQUE PALSY
Fourtlh nerve palsy is the milost coimImloIn isolated cyClovertical eve mlusclepalsv.2S Congenital fourth nerve palsy occurs because of a defect in thenucleus or the imotor portion of the nerve. Closed head traiumiia is the clhiefcatuse of acquired four-tlh nerve palsy; buit other etiologic factors, includingcerebrovascular accidlent, dliabetes, intracranial tu1mors, ethmoiditis, mas-toiditis, hemiatomia, aneurvssm, aind orbit surgery; have also beeni report-ed243 Plagiocephlyvwith superior oblique weakening, which is not etruepalsy, but does exhibit a similar clinical presentation, hals also been report-ed.5 Despite extensive cliinical aind laboratory testing, the etiology7 offourth nerve palsy mn-ay remiain obscure.3"-34 4- In his study of 121 childrenranginlg in age fro)m birth to 16 years, Harley4'2 was unable to determiine theorigin of fourth nerve palsy in 67°7% of his patients. Kodsi and Youinge43found trauma to be the most comlilmoni etiology for acquiired crallial nler-vepalsies in a study of 160 pediatric patients at the Mayo Clinic. Traiumiia Nvasthe predomiiniant etiology in the oculomotor (40%), trocllear (:37%), ancdalbdlucent palsy group (42%), aS well as the multltiple palsy grouip (56%).
The uisuial clinical presenitationi of superior obliq1ue palsy is a head tilt
704

Ocildar Torticolli.s
away from the side involved with the snperior oblique palsy, along with achin depression posture. Not all patients, however, demonstrate typicalhead postuire. Some miay present with absence of any discernable head tiltor chin depression, while others tilt toward the side with the superioroblique palsy.:' 5 Spontaneonis absence of torticollis is most common inthe presence of poor vision in one eye, where there is no need to developa posture to restore binocuilar vision.'
The Bielschowsky head tilt test is of the utmost importance in diagno-sis of fourth nerve palsy.4" Parks3"' 5 popnlarized his "three-step test," whichincluides the Bielschowsky heald tilt test, to distinguish a paretic obliquemuscle or vertical rectns muscle. The first step, which asks if there is ahypertropia in the primary position, immediately eliminates 4 of the 8cyclovertical mnscles if a hypertropia is present. Step 2 determineswhether the vertical deviation increases in left or right gaze, thus elimi-nating 2 more possible mnscles. After step 2, only 2 muiscles remain, andthey mnst both be either intorters or extorters, never 1 intorter and 1extorter. It is in step 3 that the BielschoNwsky head tilt test then differen-tiates whiicl of the 2 remaining muiscles is at fauilt.
The Parks three-step test is the standard for diagnosing isolatedcyclovertical palsies. However, Kushner7 has described conditions thatmay lead to diagnostic errors xvitlh the three-step test, snch as contractnresof the vertical rectns muscles, previons extraocular musele snrgery, myas-thenia gravis, skew deviationi, dissociated vertical divergence, paresis ofmore thain 1 vertical mulscle, and small nonparalytic vertical deviationsseen in association with horizontal strabismults. The three-step test is alsouseful in the diagnosis of bilateral masked snperior oblique palsy.49
Kraft and associates49 analyzed compensatory head postnire, before andafter surgery, in a gronp of 381 patients with the diagnoses of lateral rec-tus paresis, superior oblique paresis, Duane syndrome, Brown syndrome,and congenital nystagmnis. Suiperior oblique palsy was found in 139patients. Ninety-nine patienits (71%) presented with compensatory headpostuire. Robbl5 described 63 patients with idiopathic superior obliquepalsies, all of wlhom presented witlh unilateral palsies. One of Robb'spatienits was found to have masked bilateral superior obliquie palsy aftersurgery for an apparent unilateral palsy.
The superior oblique palsy group in the current stuidy was composedof 59 patients, summiarized in Table IV and( Table XVIII. Thirty-one maleand 28 female patients presente(l with aln average torticollis of 13.90. Aface turn was measure(l in 39 patients, alhead tilt in 46 patients, and a chinposture surprisingly in only 6 patients. The average age was 14 years aind6 moniths, with a range in age from 2 to 76 years. In all tables, age isrecorded as years pluis muontlhs.
705

Alitchell
+ I -+ +1-
.44-:1
c
;S
5~11
-tI + ++in t-
C>1 t
0
o-E5CC1j,~~~Z~ 4
Q-:..z11-1
C-.L.rl
-L..11
.Z111-;z
I r-iz.: 1-11,L 1-1
t-C .. *..*
.: .4 .:zr,. , ,
I--,.4 .4
x r-l- =
c
~~ I
C42-'
+ O;r CC =4 ++-
x = r
.- ~~74 Hz 4-~>
X oC OCC1c0 C Cl]
CC cCC
-t csC c *2 -t a c 1- o=+ + + + + + + + +'t LO cC in It Cl t It l
-CC C C
ClCC
-It 'C 1-(c :l - x Oa
;4
Q
IQ C O+ + +Clt<
706
_FO
w
*0
V:M
H4
CsI C-M Z> C CC l N 1
-0
E
3
C O -t (-,-4 _
CZ In 1-
I- 't n t in
C Cl - O 5+ + - + +
C, 5 +)'C1 -IC
Cl + +Cl ~-Z
CC)
= .. .; , , .--, .. .. .. P. 4. ."",-lo = ---. = I .-) --l ..
>rl cl t In-

Octular Torticollis
Q: ~G-~ C1 - C+ _+ + + + +X + c'i- 1 r; +C~~~
o ~ ~ C
C _ OJ C,8 C
e ._~~
,--
-
A
C ciCr_-1t ~rl)inC-rZcIr_ irO GO (0 cO Ci ic i.c ciIn x c r-1 10 n --
O t
I r rkr1
C0 C O CC
+ + +
C>AI1- + + 1- 1- +
0~ x circc
,1i X l ' - 0t 0-+ + + - + + + +
I'l + C')-c_ C 0c
~ 0-
~~ ~~ ~ C,=- .c0c c0--
--~Ci cc- t In- (0c I-
707
+ +
b-c
X
Qr
0
0
c
E
-2P4
t. 1 t
= PO Jz
;4
;QcO
"I .
1=
2;4
goEv °
j;a:
0
.2_2p
'PC.tliH ;,
O CC Lf
I C+ + +t -I 0(0 _
Wu
I I
w.r
.-o0
z0-0
Wcr-11,
I rl I.r_ v-_, -= I.r_ "C x .;r_

Mitchell
c,.~C
cc"
-t -,t ;, Il
0 C~ 0-~
*-
U UUz UX4 X4 4 t+ X4
= = Z>
CC Ci1+ +{1 C>1
1 -1
.- V0
I I)U4
UO1, Ep.:
n 0 5 ifin O- iC i cn cic'i- -_ -
-- In-U! 3 - sCCi 1,
+ +sC + ur-
Cc1
ci
. i 0cc 0. z -
z 0 -.0zr
._ U CU.
C . K
C0 c.
0. H.
It t- I- I'll z IC G_1- Ci- cct
z 1- 45 i Ccil
O UD V) Q cct zCC i O C_ I-- - c_ c
CD - - o - lC iCn- X I+ + + + + + + + +'t + + + Cccz -ctc zCc O cc c. _
in C cq z ,C cn in c+ + +~ + + + + +,t cc ci + Ic 1- in rc r
C) C-,
° O;O'.C> = = Vz C/~ ~t Uc Ci¢ - UU;fi s H
C - r r t I C I- X - O't ct ct ct ct ct cct IQ
ci i CC I 00I- In I- L( Ic- I- Ic
708
cil +
cc
GCx0
t-
0
U-;4
Q
VI'
CzQC
0
0
i-C
C.)
ccS H cC) =p
0;Lw
Ol00
_00
94:PO
"Z
z*0
1-
t-
ICzCi]
Q
z,

Ocuilar Torticollis
Not all patients in this gronp requiired surgery either because the tor-ticollis was not sym-ptomiatic or severe, or becanise the parents or thepatient did not elect surgery. The procednres performned anid age atsurgery are compiled in Table IN7 Of those patients selecting surgery, 27inferior oblique recession procedures were performed, as were 4 superiorobliquie tnicks, 2 inferior rectus recessions, and 1 sniperior rectus recession.One bilateral Haradcl-Ito procedure was performed, witl an advancementof the anterior one half of each superior oblique tendon to a position at thesniperior border of the lateral rectus, 8 mm posterior to the insertion.
The etiology was obscure in inost patients, with documnentation of 2motor vehicle accidents and 1 bicycle accident, which shattered the rider'shelmet. Patient 19 snistained a head injury at work in another state, andalthouigh corrective surgery was recomm-nended, the patient was lost to fol-low-nip. The spectrum of superior oblique palsy classified by KnLpp28 wasnot apparent in reviewing this series of patients, hence the surgical optionswere liimited to the above described proceduures.
INFERIOR OBLIQUE PALSY
Inferior oblique palsy is the rarest of all extraocular muscle palsies.) In1977, Scott and Nankin52 reported the first series of patients with isolatedinferior oblique paresis. An intrasheath tenotomy on the overacting ipsi-lateral superior oblique was performed on 6 patients, with excellentresults. Olixier and von Noorden5' performed tenectomny proceduires on 6patients, 3 of wlhom developed progressive paralysis of the tenectomuizedsnperior obliquie mntscle, with deterioration of binocular vision. Reese andScott53 performed a tenotomy on 16 patients. Six of their patients alsorequired a contralateral superior rectuis recession becauise of concernswith losing binocularity with the tenectomy procednre. Only 2 patientswere classified as overcorrected withl postoperative suiperior oblique palsyin a 5-year follow-uip period. Pollard54 described 25 patients with inferioroblique palsy, 2 of which were bilateral. Twenty patients in his group of23 with unilateral palsy presented with a head tilt to the side of the paret-ic inferior oblique miuscle. Nineteen requiired suirgery, with superioroblique tenotoml-y or with contralateral superior rectus recession. Only 2developed superior oblique palsy postoperatively, requiring suibsequentsurgery. Seventeen were able to fuise in the primary position, with1outhead tilt, after suirgerv.
Kushner2" reporte(d that each of his 7 cases of vertical incomitancefrom inferior oblique palsy had significan-t hea(l tilt toward the affectedside. Five were iatrogenic, anid 2 were presumed idiopathic inferioroblique palsy.
Tables V and XVIII summarize the inferior oblique palsy group found
709

-~~~~~~z
--~~~~~~~~0
+~~~~
:
Z c>l 1- ,°1
F
~ ~ ~ ~ ~ t1I1+~
+ +0X + Ot S
>
t <5~~~~~~~
Z < 2
,1
C k-]
710 Mitchell

Ocuilar Torticollis7
in the present stndcly, including 2 muale and 4 female patients, ranging in agefrom 6 years 10 months to 45 years 11 months, with an average age of 21.The average torticollis was 16.80. Only 2 of the 6 patients demonstrated ahead turn to the affected side. Patient 3 was first examined at 8 years ofage, with marked overaction of the right inferior oblique muscsle. An extir-pation procedure of the right inferior obliqnie resulted in marked under-action of the inferior oblique, with a 15° head tilt to the right. There wasa right hypotropia of 25 diopters in left head tilt, and 25 seconds ofstereoacuity on the random dot test in the position of torticollis.
Patient 2 had 2 emergency procedures for epistaxis, which could not becontrolled in the conventional manner. After a ligation of the right internalmaxillary artery, the bleeding persisted, requiiring ligation of the anteriorand posterior ethmoidal arteries. These procednres led to an underactionof the right inferior oblique, hypotropia in left gaze, and a marked face turnof 220 to the left, with gaze right preference. There was also a large area offacial anesthesia. Patient 6 had presumned congenital inferior oblique palsyand cerebral palsy and did not require surgery.
BROWN SYNDROME
Brown55,5f is credited with the first description of the eye motility defect,known as Brown syndrome, demonstrated by an inability to raise theadducted eye above the midline horizontal plane. There is usually lessrestriction in the primary position, and little or no limitation of elevationin abduction of the affected eye. There is a slight downshoot of the adduct-ing eye, simulating superior oblique muscle overaction. In associationwith the restriction of elevation is an occasional widening of the palpebralfissures in adduction. Exodeviation in upgaze in a V pattern 575 is present.
Initially, Brown5556 felt there was a simulated inferior oblique musclepalsy due to a deficit in innervation to the inferior oblique, witlh secondarycontracture of the anterior sheath of the superior oblique tendon. Thiswas proved erroneous by electromyography. Brown59 redefined the ten-don sheath syndrome as being more complex than initially suspected anddescribed the true sheath syndrome as congenital, permanent, and associ-ated with a positive traction test in adduiction. Most patients do notdemonstrate a vertical misalignment in the primary position, but ifhypotropia is present in the involved eye, there may be a compensatorychin up posture to allow fuision in downgaze.
Various superior oblique surgical weakening proce(duires have beendescribed, including removal of the suiperior oblique tendon sheath. Theterm "sheath," however, is a misnomer. There exists an intermultscuilarseptum suirroun(ling the superior oblique tendon, buit the "sheath" isnonexistent. When the Tenon's capsuile and intermuscular septuim are
711

booked witlhout directly obserxing the suiperior oblique ten(lon, the thick-ened, redund(lanit layers of Te1onI's capsule and(1 intermnscnlar septnlm onthe tip of the imulscle hook are interpreted as a "sheath."5'7i" The preferredsurgical teclhnique requires leavNing Tenon's capsule intact acnd nnopened,beyond 10 nmm from the limibns, to avoid orbital fat. The intermntscularseptnm mnlst remlain intact except at the placement of the tenotonmv.Superior oblique tenectomy temporarily improves the snperior obliquetightness in Bro\vn syndromiie bnt frequentlyv leads to a palsy of the tenec-tomized sniperior oblique, witlh opposite vertical tropia and snbsequenttorticollis.5
Parks and Eustis"5 recommlnended simultaneonis snperior oblique teno-tomn an(l ipsilateral inferior oblique recession for true Brown syndrome.This Wcas suggested to avoid reoperation for iatrogenic superior obliquepalsy, which frequiently occurre(l when the suiperior oblique tenotomy wasthe sole procedure. Underaction of the inferior oblique may persist insome patienits. The silicone expander has been advocated by Wright andassociates." The silicone spacer is sutured to the cut ends of the superioroblique ten(loni, nasally to the superior rectus muscle, after a tenotomvprocedure. This techniqtue offers more predictable results, Withloutrequir^ing inferior oblique surgery. Major advantages of' this techniqueinclude controlled elongation of the superior oblique tendon, preservationof fusion an(d stereopsis, wlhiclh may be comzpromised when iatrogenicsuperior oblique palsy occurs, aind preservation of inferior obliqcue func-tion througlh avoiding surgery on that muscle.
Tables III, VI, and XVIII summarize the findings of 25 patients withBrown syndromiie. Ten mn-ale and 15 female patients were fouind( to have anaverage torticollis of 9.40. The average age was 11 years, 3 months,with anage range of 2 to 49 years. Torticollis was foundl in 25 of 86 patients, or in30% in the group diagnosedl with Brown syndrome. The incidence of tor-ticollis was higher than that reported by Kraft and associates," whodescribed a comlpensatory head posture in 6 of 35 patients with Brownsyndrome (17%). In the current group of 25 studied, 16 patienits experi-ence(l face turni, 9 had a head tilt, and 7 (lem)onstrated clhin postuires. Ofthe 5 patients who electedl surgery, all had tenotomyn procedures and 3 hadsurgery before their incluision in this study. Two patients received surgervafter their inclusioni in the study. The average degrees of torticollis ofthose patienits who had stirgeiy was 9.20, with a range of 6 to 14".
DOUBLE ELEVATOR PALSY
Third nerve palsy may be partial or complete. 3 -3-4.3943 Double elevator palsyoccurs wheni both elevators of the eve are affected. There may be varying(legrees of ptosis or pseuidoptosis. Pseudoptosis occurs when the upper
A\litcXlell712

Ocuilar Torticollis 713
+ s + C t+
QC OC
rl r5-C_ntCltS rl q i- rl in ;5tr C~ rX~ In1- ;5In- CAt
H-(>1--__ >_____
C ciCn}nOC51
F~~~~~~~~~~~~~~ +
+nnKLOncC5-5ie5-p_ _ _L;sOn5 -tZnO-C DO; -; SO>+

eyelid folloxvs the hypotropic eye, but whlen the hypotropic eye fixates,the pseuidoptosis disappears. True ptosis may occur in associationwith psendoptosis.
In double elevator palsy, the traction test is nisnially negative. In thecase of a negative traction test, the treattment of clhoice is the Knapp pro-cedurejI`8 a fuill tendon transfer of the medial recttis and lateral rectns tothe insertion of the superior rectns. WVIhen there is douible depressor palsy,the horizontal rectnis mutscles are transferred to the insertion of the inferi-or rectus muscle. In double elevator palsy, the elevation of the eye isrestored only to midline, but the hypotropia is improved or eliminated.When a fuill tendon transfer was performed for double elevator or douibledepressor palsy, Knapp"' reported an average correction of 38 diopters inprimary position, and movement of 250 in the field of action of the paret-ic mutscles fromn primary position.
In the presence of a positive traction test with an absent or poor Bell'sphenomenon, Scott and Jackson" advocate recession of the inferior rectusmuscle as the initial procedure and recommend a full Knapp proceduire ifthe traction test is negative.
Douible elevator palsy results in the present study are suimmarized inTables VII and XVIII. Three male acnd 6 female patients, ranging in agefrom 4 months to 73 years 6 months (average age, 19 years 1 month), wereexamined. The average torticollis found was 19.3°, with 7 of the 9 patientsdemonstrating a face turn, 4 with a head tilt, and 4 with a chin posture.Patient 4 presented with elevator palsy induced at cataract surgery. Thismight be more accurately categorized as a pseudo-double elevator palsy,induced by complications of periocular anesthetic injection to the extraoc-ular mnuscles. Two patients required only inferior rectus recession for theirpalsy. A Knapp procedure and a Fasanella procedure for residual ptosiswas performed in 1 patienit, in addition to 2 other proceduires for comipli-cated strabisinus.
DUANE SYNDROME
Dulane syndrome, as described by Duane7" in 1905, is more precisely des-ignated the Stilling-Turk-Duane sy,ndrome because of earlier descriptionscompiled by Stilling7' and Turk.72 Duane emphasized retraction, an essen-tial feature of the syndrome. Clinical presentation includes retraction ofthe globe and a horizontal motility (lefect. Huber73 described three typesof retraction syndromes based on electromyography.
Type I includes ahsent abduction, normal or restricted addluction withglobe retraction, and palpebral fissure widening on attempted abduiction.Electromyographic findings include absent electrical activity in the lateralrectus on abduction, but para(loxical activity on adduction.
7i14 MitcSlell

Ocuilar Torticollis
(C (C IC (C F- C. C+ + + + + + + + +..-zz.1r. (C +
C- 1-(IL
(.(C .
(C .C -r z .
(. -. -.-2 .- . c.ZU
>IC C Cl --.Ir I -tCil Ci,
t- O V1D 12
C1
mC>1rIn C - Cl1CiC'1ICCC C_
C t- "t (C+ + ++ ++
+ I-O on C +tII- l_ f-i-
-C1+ X+
XC
715
v
z
Z
uV~
z

Mitchell
Tvlpe II inicludes exotropia with restricte(l adduction an(l abduction,with retraction of the globe on adduction. Electromyographic findingsinclude electrical activity with contraction of the lateral rectuis on bothabductioni anid adduction.
Type III includes severe restriction of both abduction and adduction,with orthoplhoria or minimial esophoria or exophoria, and retraction of theglobe on adduction. XVideuliing of the palpebral fissures occuirs on abduc-tion. The electroimyographic findings reveal co-contractioni of the horizon-tal rectuis mtuscles on both ab(duction and adduction.
Clinical presentation is variable,7- and observable retraction rangesfrom minimu-al to conspicuous. An upshoot, downshoot, or both may bepresent in the adducting eye, simulating oblique muscle overactions.Upshoot and(I downlshoot of the affected eye have been described as the"leash" or "bridle" phenomenon and are cauised by a tight lateral rectusslipping over or unlder the globe with subse(quent anomalous vertical eyemovemenit.'5-'7
Bloom anid associates"" described minim-al vertical displacemient of thelateral rectuis in relation to the orbit, with mlagnetic resonance imaging in2 patients with upslhoot and(I dovwnshoot, suggesting a modification of thebridle effect theory. Vlon Noorden 9noted that the globe slips beneath orabove the horizontal rectus muscles, whiclh mlaintain their vertical positionwith referenice to the orbit wall. Von Noorden believed that the magnet-ic resonanice imaging (MRI) study provided further proof for the bridletheory. Therefore, witlh sliglht elevation or depression of the eye from pri-mary positioni, a co-contractioni occurs, with subsequent upslloot or down-shoot of the globe.
Duane retraction syn(drome may present bilaterally'"' and occursmore freqileintly in females.'*-254`6 Associated findings include the Klippel-Feil anomialy in 3% to 4% of patients" -12 anid the congenital labyrinthinedeafness in 11% of patienits.' The Wildeiranck syndromnes includesDuane retraction synidromne, Klippel-Feil aniomaly, an(d congenitallabyrinithine deaffness. A comprelhensive list of associated findings, anom-alies, and synidromes has beein published.74
The majority of patients with Duiane syndlrome have straight eyes inthe primary position dui-inig infancy and childlhood. In timne, however,some patients with ty\pe I Duianie syndromne wvill develop an esodeviation inthe primary position, with restricted ab(duiction in the involved eye. Acompenisatoly hea(l postur-e develops, wvitlh a face tuirn toward the side ofthe involved eve, in or(ler to mlaintaini binocuilar vision. Surgery for Duianesyndrome is not usucally necessary unless a significant hea(l posture hasdeveloped.7' Because the suirgery cannot correct the anomalous innerva-tion, the purpiose of surgery is to restore the eyes to a parallel aligillnent in
716

Ocular Torticolli.s
primary position, and to reduce the compensatory face turn. Surgery forDuane svnedromne was first suggested by Nutt,j' who recommnended medi-al rectus recession in the involved eye witlh uncomplicated Duane syni-drome and abduction limitation. A maximial recession of the tight medi-al rectus mnuscle has been recommended,74 alonig with a Z-tenotomy whennecessary. Lateral rectus resection is discouraged becauise of increasedrestriction following this procedure. If there is marked retraction of theglobe, along with marked narrowing of the fissures on attemupted adduic-tion, a recession of the lateral rectus at the time of recession of the medi-al rectus can be performed.
Either partial or total vertical muscle transposition to the border of thelateral rectus muscle has been recommended,`'' but this has also beendiscouriaged by others-' because of further limitation to adduction.However; Molarte and Rosenibaumn92 demonstrated a 77% improvement inesotropia, and a 100% improvement in face turn in 13 patients who hadfull transposition of the superior and inferior rectus muscles to the lateralrectus insertion.
In patients with bilateral Duane syn-idromiie, secondary exotropia hasbeen known to occur after bilateral medial rectus recessions."3Simultaneous miedial rectus and lateral rectus recessions may be requiredto reduce this complication. Despite large medial rectus muscle reces-sions, Pressmcan and Scott94 did not report aany significant overcorrections,nor did they gain significcant increase in abdtuction. Nelson,' however,described severe adduction deficiency following large medial rectus reces-sions in 2 patients, 1 with a 7 mIm medial rectus recession anid a secondwith a 5 mm-u recession followed by a 2 mm re-recession.
Eisenbauim and Parks96 addressed the leaslh effect of overelevation andoverdepressioni of the involved eye in adduction, wherein the tight lateralrectus muiscle slips over the surface of the eye in adduction, simulatinginferior obli(que overaction, or superior obli(que overaction. The leasheffect of the lateral rectus was successfully eliminated by placinig a permlna-nent posterior fixation suture 14 mm from the insertion, at the superiorand inferior one third of the muscle. Von Noorden and Murray'7 alsodescribed suiccess with posterior fixation of the horizontal rectus musclesin 5 patients with upshoot and downshoot in Duane retraction syndromiie.
In discussing the Eisenbaum-i and Parks paper, Jampolskyr'9 proposed a"Y, splitting of the lateral rectus tendon insertion to reduce the upshootan(d downslhoot in Duanie syndrome. Rogers and Bremer"' (lescribed amarked redcietion in upshoot and downshoot in their series of patientswith a "Y' splitting of the lateral rectus, witlh or WithoUt recession of theipsilateral miedial rectus muscle.
Duane syn-dromie is summllllarized in Tables III, VIII, and(l XVIII. Of
717

Mitchell
X+ +
QC
cc
t-
04;u
.r
0
0
04
0.-4
el.-4
.-o
4
k*
;4u
xwUn
E*4
64
in in in t in C>1 in in C in in I1- 0 C> O'c=, n in I1- In X sC 0C]-r",I cl1 -- r -- -4 - - (' -
-t n_ ooD sC
In- ci Ic- 7to-4 ur (>1 n °
in c1 cn O in
CC It 1- It O o+ + + + +
c,1 a~ 0)3: X
ciCC _ cc +
XC -
-C CC- 1l-)
"c Ic- ~C ii- CC
cc c cc 1- ic O
U: Cccc+ + + + +CC + C3: O O ci
Cr C Cs1c i ccc
G X
---
+ +ci cc--4
c cc
I- Cirl Crq
718
a 1-+ +cc_
ci Lc
1- I+ +l-
-e1 _
;.-
In O t n
-,It I- O-
+ + + _+ l- n- In +C 1-
.-;2 *1;2
m4 m~m~;
CICcc cc Il-
r'1l
x .Ir_= -2114
11-1
.4 ;4

Octular Torticollis 719
I+6-
vr Ir oC_= t t- o;r ,+-
V 1- 0 t n + +) rn
f I _ C] S: iCI
z ,° H1-~ ~~~kr= ;
Q + +- coo 1 - Z 1 h-1C- to o 1nZ > >1-- .1c s sQ~~~~~~~~~~~~~~~~~~~~~~~~~~CZ ~~~~~~~~~~~~~~~~~~~~~~~~L- r6 CC
_, CI1iCCCCCCCCCCCCCCC CCCC t

128 patients with the diagnosis of Duane syndrome, 46 presented with tor-ticollis, resulting in a torticollis incidence of 36%. Kraft and associates49found compensatory head posture in 62 of 91 patients, or 68% of thosewith Duane syndrome. The current series reflects 22 male and 24 femalepatients, ranging in age from 7 months to 34 years 8 months, with an aver-age age of 9 years 1 month. The average torticollis was 14.30, and all 46patients demonstrated a face turn. Eleven patients also demonstrated ahead tilt, and 6 presented with a chin posture. Thirteen patients requiredsurgery, including 2 who received a "Y" splitting procedure. Each of the 8unilateral cases involved the left eye. The 3 remaining cases were bilater-al. Patient 44 achieved a fair response to the "Y" splitting. Patient 46, withbilateral Duane syndrome and evidence of congenital aberrant innerva-tion, required 3 procedures to provide satisfactory alignment. The faceturn is evident at times, but the patient has markedly improved from hisinitial presentation.
ACQUIRED HORIZONTAL INCOMITANCE
Kushner:" described 7 patients with acquired horizontal incomitance, 4 ofwhom had asymmetric surgery. Three patients had overcorrectedexotropia, with esotropia in the primary position but experienced fusionwith a compensatory head posture. The fourth patient had esotropia witha recession of the right medial rectus and an undercorrection, presentingwith a compensatory head posture. After a recess-resect procedure on thefellow eye, the torticollis resolved, and stereoscopic vision was achieved.
Kushner described 48 patients with A or V patterns, but only 4 had achin elevation or depression posture, which he reported as a 9% incidenceof torticollis. Of the 44 with A or V pattern without torticollis, the devia-tion was so marked that fusion was not possible in 35 patients. Theremaining 9 patients had deviations of less than 10 D but failed to demon-strate fusion. The 3 patients with sixth nerve palsy were listed in this studybut were not discussed.
Acquired horizontal incomitance was included in this studly, butbecause of the number of patients reviewed, 3 separate categories werenecessary for tabulating acquired horizontal incomitance. Table IXincludes data on acquired horizontal incomitance as well as asymmetricsurgery. Table X includes A or V pattern, and Table XI includes sixth nervepalsy.
ACQUIRED HORIZONTAL INCOMITANCE/ASYMMETRIC SURGERY
This group of 48 patients (22 male and 26 female) is summarized in TablesIX and XVIII. Age range was 3 years 2 months to 82 years 7 months (aver-age, 21 years 3 months). Average torticollis was 13.3°. A face turn
Mitchell720

Ocular Torticollis
w C 0a oo = - = = Qcsro - Ic o" = oc I'l. . . + +. + ++ + ++++ + + +. . + +u -I o t t c -o + CQ o = c
1_ V- U: m n-
_
zr in- ion-t°a in- ltn_ G q InS "Icoxtln_ N2
F -4 °° °°° N4
CX'n ctMX= X
X o= o rc"t Cq
CZ Co CiCIA
C C
0C>I-c-CI
Cil~CN
CCI N i c
ci- =CI
t- L0
C C C C
C) C=, IC- C
0z -: t~ i'i--C CC-= =
iq i- i,
w ..+ +. + +
U + in r. -,t - I_¢c0 t ~r
C
Cs1 C>l Cs1 CsEl C,-) Cl C>1 C,-)
1- Ci_ Cil C:Q+ + + + + +
cC5 CO + t
m z :
-I-C---
721
x o~+ +1- X
0
00
#_O_
i
0C.)
0z
0N
0
0
0
"I
C)Nu
C t- cn o t--I ---I -
t- n- sC Q
-C\I'l Il cli
ciq rj ci
t-

Mitchell
, + . . . . +r_cixn. -
--111~,= ClZ ~CZCl -t Cli't+ + +-+ + - + + C(> t in_ +-V =Z+ cl -±+ ZC1
-4 --Vx _ x ; x~~~-V94r
3CX ;S 1 - O C~ l-O X, I cs-c~
I- IC- C I-C
CC- .C C I1- Cl
Cn C
ClClI l CI In_
I CC 5_ > >1riC-IC Cll Cl C1
+ + + + +
c ~V C-
IC- CI C.C Cl-II <>1
Il Cli Cl- Cli
I - -
Cli Cl Cll Cl
_-o c+ ++ :a XI +n
ar4 <4 1H
1- X _ - C1- - - Cl
- t I_ ;CCl Cl Cl,] Cl,
722
z
0;i.4
9
ZI
I..
N
ol
-0
a
zZ
x
+-t
0
0
E0

Ocuilar Torticollis
C C l- In+ + +I- + It
U-C
3D1 ~c X = = - C o C] oI1-+ + + +++. . . . +l- C C,C + CCC]C] i Z CiIOQC l S~oo In- In-
Cd InA-C ; - SC c X
0zO0° a, X c, b .X
b6c: COb o0 Q0b b Ht* 9: NO °0 ; ;: b S - W < 3 X t t
C
H X- _ £ -XF XF-;£=S E z;Q F-^ --XXF -
z => _ _ '= e ;X===
('Il C - O CC O O_ > 1 4 --4 CN
I-
o o o o-I -_ C> -
cC' C,] CC1. (Z CC) t IC) rl~
C]i C.] Cl r'C] C] ,lC]C] C~] ]C]ll
C,- C- cl- .cC1- Cq c~lc] C] o] C0D cs 02 s~C
IC1 C CQ C
C]1
CC-= lC_ Inc] oc ]c c]
csl csl- C1 c"l cq
x --c o C. C,, C+ + _ + + + ++
C5C ln_ + (c Z :C- +r_ -S-4:
_ _~~~~~~~~~~~.
CC l-+ +z1csl_- sc
C cs C]+ + +CZx x
C.C
0-~-~, g~,P.- (: ~ jOr--- -, ~ 04
l- C-, - C]CCC tnl- X_] CI Cl CC cC Cn CC CC CCCC CC cC CC
723
Q00
EH
#"
-o
uz
0-0
ze;0C
N
0..
C
C~
zC
Q
X C>1
Cc CC]~ c], C]
Q;4
z
6z
Vj~I"
- In. .c .c.. -4
<- Z E-

Mitchell
+_O- "t 5 1- t- _ c-D -
+ + + + ++-++CC~~~~~~~~~~~~~~~~~.IC~~~~C
~~~~~C~~~IQC2tt~~~~~~~~~~~
C. bt C. ;)
oc C)°c- a ;;>°c>C) In- _
X~~~~~~~~c(_- ==Xa W L1 XIc1=OPOO XX X
q
) O lQ C
i C c
O -)0 C-O -
C] C] Cq C] Cq Cq c] C CNl
In.+
+ CCC]
Cq s0 -
+ + _- _t CC + +
C_ I-
__--
+ +ICC] CC
WI Sz 4. x Jo> 0 ~ -;-~
o ~- 2s oo t
C) rlC CC v I-
724
Qz
0z
z0N
~-o
00
z
0-
oluX~
o
u00
0
0
z
z
0r0
00
0
E-z
6z
CCr.)
---WCC
C.)a)
bO
1 rq

Ocular Torticollis 725
z~~~~~~
rq C= C-1 ~ ~ H C~~
10~~~ cq~~
Itooo 00- ooo 0 0
N 7 --
0]In Z _Zn_ I_ In- Z
c, I in- N- xx c Z0]- C In
~~ CO0]I00]QC Z QCZ Z0]10CO Z1~~In-0 0-,t n-t-x C- N, q N N~qCO

726 Mitchell
~000
N
10 x
I- r= CIC IC r
2~~~~~~~~~~~e 11- oe , , i,, a
¢ ;
u C,o r q.-E _ocou c, ooo
Z~CkCcC +ICL-CC c'~ + ICCCCO1- 1-C
Z O
CO

Ocuilar Torticollis
-^ e x_ . _ _ _O s O n5o ' _ t_t ,_ t ft t_ _ e . er X r tl -r.t e V: V: V:
r., O ,X,, <_ b _ _ _o 2 w: 2 2 2
0o 00 800 00<<m°°
OzO i1K- Zo t t1~~~~c
ory.
ell0 0~3- o4 VDo^o:o)C 00 0C) --
= = (-l= - - 1-t 1-
= t Z~ h-
dt C L- 0I-
in. _t 1- to N t1l- r- n- -t
IO :;C Ieo -- I >o e Leq In C
c- t- -C
X~ O _l. t- + r_ -t ; -#xj
t C-~ _t t: X 1 -+l-crr c-,
HHHHHHHEf E EH EHII tt
- -X L C5 - Xc - c>1
o X +c -ct o
HH v vEFHH HHEoH H
¢1l ¢ ¢
22/aR 2 2 > XLIt
;rC
Q
c
c
727
C
z
-
V
C
..
-11
Ez9V~0X
zC
CE-
Cc
C
Q
LA
C
6
4~-
e-
Eu
X
E-4
-44
O5;!

Mitchell
p0
v:7
c+'7.-
0 °
=D3 D 3 ~D 3 D 8 8: 00 co o°°°°30
0 0000«! 0<~~r -cr - O - )0 C',0
It X X
1-
- -1,,
;~~~~~~~~~~~~. c_2C)~~~C
>
00 0
0< 0
= = . O
= =. 1-L = z-
O Cl cO OZ t
CO CO
O O/t1 l- ,01 0 0I
O 01'C O0
ocCCil
O(0 "It "I o c~~~~~~~~~~~~~_-_oC O 1n-0 CO I- C O1 ,I X C C in C .-I CO
+ + + + + + + + + + + + + + + + + + ++
CD + , + t- C0 in + t t- in XC + + (C + 1n + on +
_1 C -<( Z 4 -1 CO tCl C"
--HE - E HH-H
In- QC cCM
O CM CO m (0- 7-1 (C. C
(CEO FFFFFFF~HFCCCFFF~
728
-
0z
u
C
0
0w
w;r
0
0
04
0
z0-4
C.;
1:.0
z
wu
0
xW;PI
4
z0-4
6z
C
0.
z
0-z
.0
CW
00

QO O Q
rq~~~~1
n- n- oo I'l n_ o o o
100loCS c+ +- + + - + +o0 00 + CI _ - + X -
C,.)1 00 1- -r
- I>1 t ;c 1- X O31
Ocuilar Torticollis 729
=-tlC'l t-+ +
r- 10
4
zr V:
5t _
I I
424
=1 =
+
LO
Y;
100c*, Zoz
zX
~-
I.,
N
C-
0ciz0*
7;45obN
w0
aE4
Q
Q
C-
Q
6z
o01CIo00t 1-02l. _ 00 1-
00+ +CR 00
10
16-
Cc_C)
C.LbtfzP
oO-- -C1 Cn---. -L -

Mitchell
occulrred in 40 of the 48 patienits, a head tilt in 19 patients, an(d a clhin pos-ture in only 4 patients. Only 3 patients 1, 5, and 14 did not have eyesurgery. Of the 45 patients wlho had surgery, all had eye muscle surgeryexcept for patient 2, who had retina detachlment surgery only. The major-ity of the patients had symmetrical surgery, but all presented with incomi-tance and torticollis. Only 12 patients had (lifferences in vision of 2 ormore Snellen lines, and the torticollis can not be explained on the basis ofvision alone.
A number of patients presented with lateral incomitance along withhorizontal incom-itance, contribuiting to torticollis in an attempt to main-tain fuision. The Worth 4-dot responses ranged from fusion, to alternation,to suippression, and the randomii-dot stereoscopic testing ranged from 20seconds to negative. On the basis of these sensory findings, it would havebeen possible to classify some of these patients in the group sulmmarizedin Table XVI with no apparent reason for torticollis. However, the asym-metry of the motility finidings directed their placement to this group. Theplacemenit of a patient in anly of these diagnostic groups was arbitrary, andthe overlap of prior history; surgery; and preoperative or postoperativemeasuremnents created a redistribution of a numiber of patients during andat the completion of this 1-year prospective study.
ACQUIRED HORIZONTAL INCOMITANCE/A OR V PATTERN
The A and V patterns are clharacterized by a horizontal eye alignmentchange in midline upgaze and downgaze as the eyes shift from the prima-ry position.""' Vertical incomitance was first (lescribed by Duiane,"" but itssignificance and importancie were not appreciated until the work byUrrets-Zavalia''02 "' and Urist. "';5 Albert suggested the "A" syndrome andJampolsky advocated the tent or teepee syncdrome (A), with the A and Vterminology gaining universal acceptance. I
In the primary positionl, orthophoria, esotropia, or exotropia in associ-ation vith the A or V pattern may be present. By definition, ain A or V pat-tern involves a change of 10 prismi diopters in the horizontal alignmentbetween u-pgaze and downgaze."` Urist suggested that the etiology of theA and V patterns was related to the horizontal rectus muscles. Howevei;overactions of the inferior and suiperior obli(ue muscles are frequentlyassociated vith the A and VI patterns. Surgery on the oblique mnuscles cor-rects these patterns, suggesting that the etiology of the A an(d V patternsis related to oblique mutscle overactions.
Tables III, X, and XVIII summarize the findings of patients with A andV pattern with horizontal incomiitance. In the current series, 116 patientspresented with A or V patterns with torticollis, categorized by type inTable III. The diagnosis of A and V pattern was found in the office review
'730

Ocuilar Torticolli.s
610 timnes, for an incidenice of torticollis of 19%, almiiost doutble the per-centage described by Kuslhner.2 Sixty-seven male and 49 female patientsranging in age from 1 year to 87 years 6 miiontlhs (average age, 10 years 9months) presented with torticollis averaging 12.1°. Forty-four patientspresented with a face turn averaging 10.2°, and(I 40 patients presenited witha head tilt averaging 8.5°. Sixty-seven patients demonstrate(I a chindepression or elevation postture, yet the degree of chin postnire averagedonly 9.0°. The average degree of chin posture was lower than anticipated,since a chin posture with elevation or depression would be expected morefrequently with obliquie muscle overaction.
Overactioni of 1 inferior oblique was note(d in 17 patients but occurredbilaterally in 45 patients. Un(leraction was seen bilaterally in 2 patienits.Overaction of the superior oblique muscles was noted to be unilateral in 3patients but bilateral in 21. Three patients had underactive superioroblique muscles in both eyes. Stereoscopic vision could not be recordedin 15 patients, and therefore they were deleted from the group total of116. There was no measurable stereoscopic vision in 63 patients. Theincidence of absent stereoscopic vision was 63 of 101 patients, or 62%.From the group of 48 witlh A anid V patternis, Kushner described 35patients witlhout torticollis, who had large deviations prohibiting fusion,inicludinig 9 patients with less than 10 D of deviation. Althouglh Kushner'sgroup lacke(d torticollis, it also lacked fusioni, with an incidence of 73%,higher than in this study .
Eight patients wvith Down syndroime were included in the currelntgroup, only 1 of whom had oblique muscle overaction. This group ofDown patienits merits further investigation because of their apparent con-centration in the group with A and V pattern, and becauise of the lack ofoblique overactions reported in this study.
SIXTH NERVE PALSY
Sixth nerve palsy may be conigenital,32-:34394243. though extremely rare,or imiay be acluired. 32-34,39A42,43,14 The long intracranial course predisposesthe sixth nerve to increased intracranial pressuire, trauma, edemua of themeninges, inflammation, and brain stem displacement."5 Sixth nerveparalysis has muany etiologies, including traum-a, neoplasm, inflamnmation,undeterminie(d causes, and imiscellaneous causes. An extensive summaryof the literature concerning the etiology of sixth nerve palsy anld manyassociated conditions has been described."5
Sixth nerve palsy clinically presents with esotropia in the primncary posi-tion, with a compensatory hea(l posture to muaintain binocular vision.Recovery often occurs withinl 3 months of onset, and if contracture of theipsilateral me(lial rectus has not occurred, theni surgical intervention may
731

not be required. In a young child who does not assume a compensatoryhead postuire, patching may be necessary to preserve vision and preventamblyopia. Surgery may be necessary if normal function does not returnafter 6 months. A recession of the medial rectus or a resection of thepalsied lateral rectus muscle may prove to be sufficient. If there is a neg-ative forced duction test, a transposition procedure with a Hummelscheimor a Jensen operation may be required.
The acquired horizontal incomitance group, with sixth nerve palsy, issummarized in Tables XI and XVIII. Fifteen patients compose this group,including 6 males and 9 females ranging in age from 1 year 2 months to 81years (average age, 32 years 11 months). The average torticollis was 15.5°.All except 1 patient demonstrated a face turn, and only 4 presented withhead tilt and 2 with chin postures. Four patients required surgery, includ-ing patient 9, who had a severe sixth nerve palsy and contractures, even-tually requiring three surgical procedures. Kraft and associates49 foundcompensatory head posture in 26 of 93 patients (29%) in their study of 381patients with compensatory head posture.
In the current series, patient 3 was comatose for a brief period after amotor vehicle accident at age 10. She presented with 75 D of esotropia,which spontaneously improved in slow increments, to E(T)' of 0-10 D.Stereo returned to 20 seconds of arc with the random-dot test . She wasscheduled for surgery several times but was canceled each time owing togradual improvement of the esotropia over 18 months. Her only signifi-cant eye motility finding at this time is E(T) of 6 to 8 D, only in right gaze,and a residuial face turn of 80.
TORSIONAL INCOMITANCE
A compensatory head posture to the right or left shoulder may be presentwith cyclovertical strabismus or in the presence of nystagmus. Conrad anddeDecker"" have combined a recess-resect procedure at the anterior polesof the obli(ue muscles, with transposition of their insertions toward theposterior-anterior pole. The procedure is directed at rotating the globestoward the side of the tilt position by shortening and by lengthening theanterior parts of the oblique muscles. Cyclotorsional diplopia has beendescribed following retina detachment surgery, although the overall inci-dence is low.", A compensatory head tilt may be evident in the presenceof cyclovertical strabismus in order to permit fusion.
Von Noorden"i presented 5 patients, one of whom was lost to follow-up. The remaining 4 patients had horizontal transposition of the superiorand inferior rectus muiscles, which eliminated the head posture by rotat-ing the eyes around the sagittal axis. The clinical assessment of ocular tor-sion, as described by Guyton,"9 has been a valuable objective test, not only
732 Mitchell

Ocuilar Torticolli.s
with torsional incomitance, but also with cyclovertical palsies. As Guytonhas described, the clinical torsion noted with overacting inferior obliquesnp to 15° or 20) does not correlate with the double Maddox rod test, whichinvariably fails to demonstrate subjective torsion.
In a study of cyclovertical displacement of the blind spot, Locke '2
abandoned the double Maddlox rod test because of a high incidence ofnegative results, while torsional deviation was revealed by blind spot plot-ting monocuilarly and binocularly. V7on Noorden"-' has described limita-tions of the double Maddox rod test in that only the central portion of thevisual field is being tested, where cyclodisparity is less significant than inthe retinal periphery. Fusable visual material in the periphery of the visuI-al field is not available when the red and white streaks are seen.
Cyclofiusion may compensate for a symptomlatic cyclodeviation, althoughthere may be several degrees of cyclotropia measuirable on double Maddoxrod testiing. Although cyclovertical muscle anomalies occur with relativefrequency, patients rarely complain of tilting of images, cyclodeviationsseem to rarely play a role in head tilting, and imost cyclodeviations are welltolerated."'3I2' Despite objective cyclotorsion of the globe in cyclotropia,subjective testing may yield negative results because of sensorial adapta-tions. 122,12:
In the current study, there were 4 patients with torsional incoomitance,as summarized in Table XII. Patient 1 had stereo of 25 seconds with no
obvious reason for torticollis, and intorsion of the fundi, whiclh was notsevere enough to require surgery. Patient 2 had a Harada-Ito procedureon both eyes, with a smiall residual degree of torsion, not significantenouglh to re(uire further suirgery. Patient 3 was lost to follow-llp. Patient4 has one nonseeing eye and ocuilar torsion with ac marked heald tilt; assess-
ment for nystagmus has been difficult, even at high-power illulmination inthe slit-lamp microscope. He may be a candidate for the operative proce-
(Ilire described bv von NooIrden1; however, the facmily is reluctanit to allowsuirgical intervention oni hiis only seeing eye.
TABLE XII: TORSIONAL INCONIITANCE
NO. INIT SEX AGE TURN TILT CHIN TOTAL(0)° SURGERY AGE
1 PS NI 5+9 15 152 SG F' 30+1 1( 10 Haradlat-Ito OU
27+13 HV7 M 61+11 15 1( 2.54 Gr NI 8+4 2(0 2(0 (Blinld OD, OS
excvlotorsion)
'Average derl((S 17.5.
733

Mitchell
NYSTAGMUS
Kushner-" described 38 patients in his group of 118 (20%) with nystagmusas an etiology for abnormal head posture. The results of the current studyare summarized in Tables I, III, XIII, and XVIII. In the group of 630patients with torticollis, 120 presented with nystagmus, for an incidence ofnystagmus of 19%, compared to Kushner's study. In the current study, 290patients presented with a diagnosis of nystagmus, for an incidence of tor-ticollis of 41% (120/290). Seventy-five male and 45 female patients pre-sented with torticollis and nystagmus; age range was 9 months to 65 years6 months (average age, 9 years 2 months). The average torticollis was21.1°. Stereoscopic vision was not measurable because of age or compre-hension in 20 patients, was absent in 53 patients, and varied from 20 to3,000 seconds of arc in 47 patients. Seventeen patients presented withalbinism or macula hypoplasia, 13 with neurologic-related disorders and 7with Down syndrome. Patient 16 was seen for the first time at 9 monthsof age, with recent onset of nystagmus and no other apparent problems.Results of her eye examination were normal except for the nystagmus.Neurologic testing and studies revealed a grade 3 astrocytoma requiringimmediate therapy.
Eighteen patients have had a conventional Kestenbaum operation, and4 have had a variation becauise of marked head tilt, face turn, or chin pos-ture. The Kestenbaum modification includes recession of 2 vertical mus-cles to compensate for the chin posture, recessing the inferior rectus mus-cles or the superior rectus muscles from 7 to 9 mm, and using theKestenbaum guidelines for recessing two horizontal muscles for a faceturn (Fig 3).
In 1950, Metzger'24 recommended the use of eyeglasses with prisms,
L GAZE R GAZER FACE L FACE
RESECT RECESS RESECT RECESS RECESS RESECT RECESS RESECT
PARKS 10 6.5 8 9 9 8 6.5 10
CLASSIC 8 5 6 7 7 6 5 8
CLASSIC+ 402 + 3.2 + 2.0 + 2.4 + 2.8 + 2.8 + 2.4 + 2.0 + 3.2
11.2 7.0 8.4 9.8 9.8 8.4 7.0 11.2
CLASSIC+ 602 4.8 + 3.0 + 3.6 + 4.2 + 4.2 + 3.6 + 3.0 + 4.8
12.8 8.0 9.6 11.2 11.2 9.6 8.0 12.8
FIGURE 3Kestenbaum surgical diagramii placed in each patients chart prior to surgery for notationof appropriate rooiiscles for soirgerv.
734

Ocular Torticollis
Cl z .Cl . + +.i
.i.(O 4U . i.Z.
00
-z .-.-.QUz,..
735
1
I+
U1-
+ dC +
,_ oo
z XU
11 , 11 11Io &g
_l Cl Cl U
c-c
l- OlC U
o~~~~~~~~l
11II1
Cl Cl
ln_ CCl r
Cs1UCl1 Cil
., CII II II
H4 H4 ~
O Oc-c .c-c -
C C UC1 Cl U
I- CSl /-iC'l (Ill -l
Cl ln_ V IOO C c-rC In_It r , ..I rClC
OCnCrl-
VrO-Z ln_
1'-
Ier- Lr- OC,,
OC_l _ _
+ + + +cIr C1 ;c Cn
It
CS~ ~
4e ;: I-
c It 1- C++ + +Z dC Cl + O
-1c Il U U
C'l XCl -~-C~-11 II II II IIHHHHH-
CC:Cl_ C-1 l 1- cl
C C C C C CCl Cl Cil Cl Cl C>1
O C O
CSOC C
Cl1 Cil Cl-C1 Cl cl
n n C1 inry
Hc11
C
C,
Cl1
C1r'll
V.0
0C11",
;10.
C..;
1-1i-O
.111
0;4
w.r
0
CA
wu
xwV.
0*
0-4
6
C C C C1- Cl
C C. C C
+ )C. C/ + + CI.- CCl-
<0U.Z.
Cl C. t c-c
cL-c
+C-c
!. *-O
4 cr
0 000i* U*0
.z 4gz C.
cr;m)1-00.Z
m
wU,

AMitchell
1 0
= : 1-+Pt~
1-~
-_
CD+
In_ It
11 11 11 11H HHE4 S
C CN C" C-1C1Ct1 o o co o c ~~~~~~~~~~~~~~~~~~~o c--
C C--l rll C>l"Cl ClCl
CooC-CoCC -CC
CC C1 >1 >clClCl Cl1ClCCl
11
In-
CC1
l-CA
1r Cl1 0
ii H H H Ho
C C oCCC CC ;s CS CCo C o o oC] C]1 C] cCl1>
C C - C o
Cl Cl Cl C>1 Cl
C'l
Cv-)
Cl clC C0 2X
C
L LD CLn nO
C--C) t ICn-ICt1
Cl11
C'l I
CC1Cn C IC-
l c Cl
t- C CCo
t- C1 0+ + + +
CC A
,1
t- XC Co
C oC o CC_ Ct- C°
_ _I _C o
oC
za Cou12au 1 C1 f1C1f1c
fA-
1- cll+ +
736
z+.+
.
.c
CD
t-O
oUl-_o
+I+Cl Cl>
-I-~
; '-
;4 ;
0-t.-*4
0
4
C.;
.410
x;m)
0W
414.-o.r
0.-ocr
Wu1.
xW.rl
7
6x
.r
e.u
CA
24;
;Pl0*
40C.;00P-40*x
4;

Ocular Torticollis
+
t-
- .0|~~~ | -t r1G0 0
HE v ;EH HzH ><HH i 1< g
cct ci Z
C zci Oi ci
11
p1
zzCii ici Ic-lc-l
4 sc xcr-1 rC -
1-+
+(0
1-0
Qr:
C
.- .-
z. .
H
C
4ci
cil
8ccC,-n_ 'tc o
ci ci
c -CIn- i Drc >ic
i_ _ _
C In rci (0c 1I ln_ OC- in.c1i 1i -, Ci1
Cq
(=_+-( +
0 't+ + +
rn C C.1 +1-
QcCrI cl cc
+ +
V
mA 2lI'll It
0- ;4= ;: =
+ + + + .
CC 0t -ct2D 2 2_:; C/
It n- cc I- CO
1O O O
1-
+ + +
O'C2 C2
737
V73D
E-
z0
0-
*. j.0.4
Z 4.
C) 0*0.* U
z 4n 21.
z
e-cr
m.019i-Oz
cr0
0
C
z
C-
z

+n
+ f
O:-;J 2:
0Clr;
cID ClH Ho H
CC CC 1-
CKl Csl C>1
2C CC 2
COCl C
i CC
CC IC r
`-~
cq
+
Cil
csl+ +
-n
Alitchell
!IC-
C-
zw:
O<0
Cc
2 ;5 2 _ >10(1 °
CC CCN C C rCCC ° Ct
Cl1 C> cl r >;r7l csl C-] r1 C1
OC C~C=
CCO O OO O 2
C
C C 2 CI C- O -C o -I o1cl C1 t CC
C C1 1- Q0
1- X O
-n
QC~ ~ ~
n -CC- QC-
1- ~ 2 C 2 l
~~~~CCC
l-
738
~z4
el
40
¢U:
ao
4
4
F*
z
o0
E.-
L;u0
X,Wi
4
z5
ICCC
=
II II
IC 4:0
Cl
CI- .4C:0Cl
IC Cl-t
Cl
ICCC
C
C
+ CCCl
1- :c

Ocuilar Torticollis
2~~~~~~~
,~~ ~ ~ ~~~~~~~~~~~~~~~~~~~~~in-, U-)
-~~~~~~~~~~~~~~~~~~~~;=- I rl t- It X ' 8
22
_~~~~~~~~~~
C=~~~~~~
t~~~~~~~~~~~~~~~~~~~~~iC Z
I l_ OI
;t CC! Q: X 1 0 UCSXr" Cn :O Y 110-
_ ~~~~~~11HHEE H H HH HH H z- H _ii
cr.~ ~ ~ ~ ~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~~~~~I
-ltCi
O r O _~~~~In C,IOO lO cC Cl- C,t; t
U c ciN&1 t1 t
; K X OC
z
In- cc t(CI
o A o O ~~~c
1
+ ccX + - ccciC.cX Co + +
2 1 r;; 2 2 ; 2 /
z > z25m ZU S 3 2 s <Ut2O 1~cic - C -
Z (Ct- t- -t- t- t-I t- t-I- t-- t 0 X S (CCC
739

Mitchell
CN ~C
e r~~~(On c:~~
a
, n
+
ic0
et
4-1 :
11 II
In-
Cl
_ Cr-)
C-1
+ ci
ciC"l
,; +
2r;4
It11 11
*&o
C iI C 11
C O
CO1- i
ci1 cil
C CC C
-0
0- =
cil 1-+ +r,j
t-
c2 il
CccI- In-
11 11H H
CC InC1 C1- ci
IC C1C CCi ci
i-c -cD
1-+c2
It+cc_1.
_
0
V +
O so
OtXO z=D¢ A < j
IC Ct O O ~~~~~~Cc1111 11 11 1111
2 OCi1 Z >1ict1 1 C;1
ci1 Z ciicC1 Csil
_~- IC 1 Cc
Oii-c i-c~~~~~~~~~~>
i-c C ci(( Cc+ + + ++ +
C>1 IC cclfc C Uc
j,X, 't X,,; ,2
001-OC H-:¢ -4
cCc 1- O c0 t Ic 1C t x nOC 30 X CM C- CC. C
740
CA
u:
9zw
;P
O H H
OCciilt
ICC (C
CI C
CL. C C
sCC C+~ +ci1+ C
(C C>1
-z
0
00
0
0
Q
6z

Ociilar Torticollis
C:
:t
ir. ir.
C CCC1- i(C C
C
.t QC L-(NC+ + ++-
C Cl' +
C/C C/CC/CZJC
.
.l'
F- P.
_ _
(Nl (-,,
_ _
_ _
11 11 1II II-
(N] (N (N> (N (N1 (N (N (N1
C)C11
z3ZzQ
- (N . (N -
z . zir.
. ir.zz QC
.(N -(N-- -
zzzzzz..z
I
+ +
(1N CZ
C C
--C: -+ ++C(Z + +N
ICC>>
741
I I
~4 +--t
5s e
=i 12r- )
= (5 24
C._
C.)
-! 4
;, 51 QCX
_N _
ir1 V C-1Ol- O)r
EC X-1
CZ
CIA
INI
C"l
11 11 11 11z
X x v- x
t-~-r> ><H >
Z :-in- l_v l--c i-oZ3
cr
0;-u
..o
z4
x
C
(N CIT N_
>1 In ln_o on
ICC CC
U,1-
I - 5
+ + +C _'-H-,. =
t-
_ 1_ _
_- I _0in CC
c
cll'.--I
ln_Lnoc.
7 i-_zr.
.4 -

Mitchell
+-
(CA
Clq
.z
c
It c0n+ +
C9
N
N
742
0
0
0
v:
Fzo
W_44"I
0-4;?, ;r
C) C0-4F* U*0
.z 4
.z 9z1.
U.
01-490
E-.r
C
C~z0
0
E-o
ct
40-
C
w
0
6n
-6.
_-:
14
a,;El'
^:
C.r
_. X
.1to -tC,*-bt

Ociilar Torticollis
with the apex directed toward the null point, in order to correct or controlthe torticollis, but subsequent patients adapted to the prisms and torti-collis failed to be controlled. In 1953 and 1954, three independent reportsaclvocated treatment for the torticollis. Kestenbaum"' snggested shiftingthe eyes away from the null point by an eqnal amonnt of recession andresection, or controlled tenotomy on 1 eye, followed by a similar proce-dure on the fellow eye after a period of stabilization. Anderson"'2described recessing the horizontal rectus muscles to shift the eyes awayfrom the null point, with the exclusion of resection procedtures. Goto'-advanced the horizontal rectus muscles to puill the eyes from the null posi-tion. Subsequently, many others have provided guidelines for surgical cor-rection of torticollis caused by nystagmus. Cooper and Sandall"'2 per-formed surgery on the fixating eye first, with a recess-resect procedure,followed by surgery on the nonfixating eye, with appropriate adjustmentfor the strabismic angle. This was felt to be especially sound advice intreating torticollis with strabismus. Pratt-Johnson '29 was the first to rec-ommend equal amounts of surgery on all 4 rectus muscles but notedrecurrence of the torticollis after a period.
Parks'3: was concerned that the pulling power varied between themedial and lateral rectus muscles and that identical amounts of recessionand resection would turn the eye on the rotation center by different quan-tities. Parks modified the Kestenbaum procedure so that the 4 horizontalrectus muscles would receive the maxim-al amount of surgery withoutcompromising the ductions of the eyes and would not induce strabismuswhen the pulling power was altered. The medial rectus was recessed 5mm, and the lateral rectus of the same eye was resected 8 mm. On the fel-low eye, the lateral rectus was recessed 7 mm and the medial rectus wasresected 6 mm. This became known as the "classic maximuim,"' asdescribed by Calhoun and Harley,"' who noted undercorrections withinthese guidelines for the Kestenbaum operation. Calhoun and Harley aug-mented these surgical guidelines by 40% and noted improved surgicalresponses. Subsequently, Nelson and associates"12 described a 60% aug-mentation and guidelines for torticollis surgery for nystagmus. For a faceturn of 15°, surgery was not recommended. For a face turn of 300, surgerywas recommended with the classic maximum plus 40%, and for 450 of faceturn, the classic maximumn plus 60%.
Fig 3 describes the surgical guidelines for the Kestenbauim procedure.A copy of this diagram is placed in the chart of eaclh patient requiringextraocuilar muscle surgery because of nystagmus and torticollis. Theappropriate muscles are marked on the diagramn to ensure acculracy in thesurgical procedure.
Concern has been expressed that very large recessions and resections
7i43

may result in limnitatioin of ductionis. Any slight limuitations in extrelme gaze,however, imust be compared with reductioni in torticollis andnmarkedimproveimlenlt in appearance as well as frequienlt improvemnent in vision.'-'
When Calhoun and Harley's guidelines halve been followed, the long-term results hlave proven to be promising. In a review of 79 patients2' w\vithan average follow-uip of 5 years, the average face tuirn of nearly 40° preop-erativelv was reduiced to less than 10° in the series of patienits receivinghorizontal suirgery. Stereoscopic vision was not compromuised in anypatients who demonstrated stereoacuiity preoperatively and was actuallyenhanced in several patients postoperatively. The visual acuity was thesaime or improved in all patieints, and the Visionl was not compromised inany patient.
NMost patients maiintaiii a stable hea(l posture after surgery. Wlhilesome patieints mu-ay reveal a tendency to gra(duially shift towar(d the preop-erative state, the patients almost never return to the original head position.
CONGENITAL ESOTROPIA WITH OCULAR POSTURE
In a seIies of .58 patients with essential infantile esotropia, Lang'" report-ed 38 patienits (70%) with anomalous head posture. Dissociated verticaldivergence was seen in 54 patients (93%), latent nystagmus in 29 patients(50%), annd excyclorotationi of the nonfixing eye in 35 patients (60%). Langstressed that the head postture was not adopted to avoid (liplopia. Hispatients dlemionstrated different combinations of these condlitions, xvithsome more proiouinced thlan others. In hlis 1982 Costenbacder MemorialLectuire, Lang'34 described hiis series of the congenital strabismus syn-drome, totaling 82 cases, with 70% demonstrating abnormcal head posture,92% with (lissociated vertical divergence, 57% with latent nystagmlus, and65% with excyclorotation of the nonfixating eye. In addition, 20% demon-strated A pattern, 17% hlad V pattern, and 15% hcad cerebral daamlage. Healso fouin(d that when an abnormial head posture was present, the head wasusually tilte(d towvard the shoul(ler of the fixating eye, xvitlh the face turnie(lto that side. Lang suggested that the congenital esotropia synd(rome wasdue to an imnbbalance in the midbrain, between the geniculo-striate and theextra-genicuilo-striate system, 'and he noted that a dominant feature of thesyndrome was the latent nystagmus. Lang fiurther speculated that thecatuse of the head tilt was related to a more filly developed vestibular sys-temn at birth, anud that the vestibular system in the patient with congen-italesotropia mntay have excessive (lominance. 20,3
In diseussing the relationslhip between (lissociated vertical divergenceand hea(l tilts, Bechtel aind associates"35 reported an incidelnce of malnifesthead tilt of 35% in a series of patients xvith (lissociated vertical divergence(DVD) associated wvith infantile esotropia. The DVD increased on forced
7_`44 Mitch1ell

Ociular Torticollis7
contralateral head tilting ani(l decreased on ipsilateral tilting. The investi-gators sniggest that some of the head tilts an(l canomalous head posturesattributed to the congenital esotropia syndromne may actuially be dtue toDVD and that DVD is a fre(uent cauise of head tilts.
Early reports by Crone'" on alternating hyperphoria, by Anderson"' onalternating hyperphoria aand( latent nystagmulls, and by Ciancia'35s 40 onesotropia in infants witlh abduction limitation hcave contribuited to this svn-drome of congenital esotropia with ocular posture.
Tables III, XIV, and XVIII suimmiiarize this group of 69 patients withcongenital esotropia and ocular torticollis. Table III notes that 812patients were seen with infantile or congenital esotropia. Tlle percentageof patients with torticollis and( conigenital esotropia is 69 of 812, or 8.5 %.This group consisted of 39 m-ales and 30 femcales, ranging in age from 8months to 32 years 1 month (iaverage age, 7 years 4 months). The averagetorticollis was 14.1°. There were 119 operative procedures performled, foran average of 1.7 operations per patient. Dissociated vertical deviationwas present in 61 of 69 patients (88%), and lateInt nystagmus was presentin 18 of 67 (271%). This low incidence of nystagmiius is more closely relat-ed to the study of infantile esotropia by von Noorden,' who fouind 15%with manifest nystagmus and 10% with manifest-latent nystagmtus.
Comparison between these series is difficult becaause von Noordendescribed 408 patients with esseintial infantile esotropia, while the currentseries compares the findings of all patients with esotropia an(l torticollis.In his series of 408 patients with essential infantile esotropia, von Noordenfound 26 of 408 (6%) with anomalouis head posture. In comparing the 69patients presenting with congenital esotropia or infantile esotropia of the812 patients incluided in the cuirrent study, von Noorden's figllre of 6% iscomparable to the 8.5% witlh torticollis, noted in Table III.
The initial surgical proceduire in this grouip was mlost commiuonly carecession of the medial rectuis muscle of both eyes. WVith residuialesotropia, the second procedcure was usually a resection of the lateral rec-tus muscle of both eyes. There were 24 inferior oblique proce(lLlres and11 procedures on vertical rectus muscles.
Of interest is the limited response to stereoscopic testing, with onlly 1patient achieving 140 seconds acndl only 7 patieints recognizing tlle Titmusstereo fly, at 3,000 seconds. Six patieints were too young to comiiprelhenidthe stereo testing. In agreement with Lang,'29'3"' these limite(d binocularresponses suiggest that the ainom-nalouis head postuires are not adopted andare not assumined for the purpose of achievinig or m-aintaining binocularvision, or to avoid diplopia.
Becacuse of the low incidence of positive stereoscopic responises post-operatively, a future study is planniied to review the recor(ds of those
745

Mitchell
+ + +
+ + + +
+ +
+.+ + + + +
++++ ++++ cq.CSO c O'c s - O O c t-+ + + + + + --- + +.+ .
t- (" C1r-Ncs~ n v + + + + N oC cs+ + sxoC
'-~~~~~~~~~~~CI Cs1- t* r~0.4~ ~ Q
333°-03 c u
x;x, x x xxCO'½S Q 1r=X C CC t
oCX 00X X CQOOXX v v X v v v v X X v X X X X
XX X X 4 X P;X;
In C] - O--i ---4 rq Cq = in C] In-In-Cs.1-1 X n s
C)o o-oo- Ct- oo ooC oC)CC
_ C] Il I- - o c] QC_ + _ + +
+ t C I' Cq + l- CO--I _ _-- --- CC _
04V m LD m =
+ + + + +
(C
0U.-
C] C,-)C,- I'l In- C I- X C;~----I--
746
+ + +
0
0
,;r
0z
0C"I
E
0-o
0
0
0
WK0
z
u0
04
~0
-
0
0
zx
en
x
E-
z

Ocular Torticollis
+ + +
+ . . + +
+- + -+_+ + + + +- ++ "I + ci + t ic C ' C + = + +
C -C CC
+
+ + +.+ + + + + +
37D- Z Ci- :c_ C= h- - C0 (I C+ + +T+. + + + + + + ++ + + Cc]z- C z
cc cl
N ~~~~~~~~~~~~~~~~~~~~~~~~~- ~ ~ ~ ~ ~ ~
C ~ ~ UC
_ A_1tN -z 4
- t I ICI - t _ n1-
tCCC~~ DoCCo~~oCCDtA^ W D D D D ^ D t > D D O DIn
I- C n- It on- Xc,i
o X_ ic
OCicXC_Z- CS.-, C rt In_+.+ + + + +++ + + + + +ct C c ci cc z= IC * tcc, 1 C
I- ct+ +
CC~4 .~ ;",:. . t --,- 4~
-F ~ 4 ~ P ~-.
X_ 0C cli C C ~~ i--C C"l ri i c-i i ir
747
Z
Vo
I
Z
U,
w
el
w
0
0
Z
E-
Z
U,
C X "Ccl c1 C

Mitchell
+ + + +
+ + + + + + + + +++ +
GYO N 51- 0 C '5t O XC ;S- 51- n O~ - C 1 C>1 .C DO1-+ + . . + . . . . . + + .. + + + + ++ + + +
ci~ ~ ~~~ ~ ~ ~ ~~~~~~~~~~i
Co 4 oc; C;
Ii-c°s c¢DDn= O~~~~~~~~~~~-c p;; icOO=O=OO1- = V i-c ==J== _== ; ;=
_iC1-c , I- - -
i- xc cilx nxci-ct ici i- iczc cx
- ic c c-
o z zc o oct_ c c
cc CcI cclz
.--O -- :; . ;
cc cc 1-0 CC -Ccm -~' cc4-I
--~zi c]c.cc i + OC
1' 2 >
;7; NZ O¢ v
Ci1 cc -t U-D C zI Icr I,-c C.Cc ccc C cccc ccc c It ct I'l l t
748
p
Q
Q
¢
z
6
.. 4. :;. 4., 4.
C) p. .,., =e- .- .1 .- .4

Ocular Torticollis
+
+ + + + + . . .
+ +
+ + + + +.+ + +
t- t- XC.C C X -C Ci XX_ Z: :c tI -t ZC C C+ + ++ + + + + + +i < >++ + + + + +CCCiCC+C-~cCC OC1-OOCl- 0 5 ZCQO+
(c("1 z:-CO 1- C t-
C CC C C C CO o
In~~ ~~~~~~C
-t~~~~~~~~~~~~~~~~~~-
~4 4 4 ~ 4~~4~42 2 ~ ~4 ~ -~ 044 ~4
Cit- CCCCt = cCC C-In-r'l ---~~~~ rl~i
C - C-CC In.InC>I C1CI Cl1 -
1- -t
Ci X cC C C CC I n-
Ci- Cc C:c in CC CCICi1 1 _
COC C CCCCCCC
O~1t(>1 02cl~- _-i-~--++ +- ++ -+XC 1- + -It + C1 +
1- Cl (I+
-it CC+ + +
C CC C5+.+ + +C I1- ac C
1- 3 0 Ci1 C tt t In- V I, Ln L
CC 1- C Co CO - " C
In- I__i I- cc .cC cC C
749
Q4
CQ
i-
V~0
1
C.
0
Ct
cr
;404
.
I4
w
uV
;n
4
z

W; + ,+..+
Q ++ ++++++C0-CCC O
£ C
z A e tn;
ci r= c czz ==
icoc1- 1 z1
O ~~ci: t1
> ~~ -
z-=~ i
_i cc. i-cz <
750 Alitchell

Ocuilar Torticollis7
patients witlh conigeniital esotropia who do not present witlh a head tilt. Thegroup of patieints in this study hald early surgery for congenital esotropia,yet the sensory test results are not as successfuil as those reported by Ingand associates. lI"1.42
In a retrospective study of 118 patients with the congenital esotropiasyndrome, Pratt-Johnson'43 di(d not find any patient with cenitral fnsion,and only 24% of the total demonstrated measurable stereopsis from with-in the group that demonistrated peripheral fulsion. Absence of centralfusion is closely related to the sensory findings in this study and also mer-its fuirther inivestigation.
PERMITTING FOVEAL FIXATION
Kushner-2 described 10 patients who adopte(l anl abnormal head posture inorder to achieve foveal fixationi. In his study, he noted 3 patients with pto-sis, 3 with ocular muscle fibrosis, 3 with Moebius syndrome, an(d 1 monoc-ular patient with sixth nerve palsy. The current study included 27 patients,summarized in Tables XV anid XVIII. There were 15 male an(d 12 femalepatients, ranging in age fromn 4 months to 18 years 1 month (average age,5 years),with an average of 12.8' torticollis. Seven patients had observableface turins, and 4 had head tilts. Twenty of the 27 had chin postures, pri-marily chiin up, with 16 patienits demonstratinig ptosis. Two patients pre-sented w7ith large chalazia occluiding the visuial axis. Marked ptosis wasproduced in patient 27 becauise of the chalazia. Patient 10 presented witha marked chinl tuck in ordler to see over her incorrectly placed bifocal.Only onie hemiaingioIma Wcas detected as a cauise for ocular torticollis.
NO APPARENT REASON FOR TORTICOLLIS
A group with this title was not described by Kushner.- Tables XVI andXVIII summlllarize this group. There were 57 patients assigned to thisgroup, whiclh accounted for 9% of all patients seen with torticollis. Thirty-two male anid 25 female patients, ranging in age from 5 months to 29 years5 months, with an average age of 8 years 6 months, presented with torti-collis averaginlg 14.1°. There were 28 patients with face turn, at an aver-age of 12°. Tlhirty-five presented with head tilt, at an average of 11.7°, and7 presente( with chin posttires, at an average of 11°. The turni, tilt, andchin postuire mneasuiremiienits did not suggest any specific pattern or com-mon denomninator. Stereoscopic vision was present, ranging from 20 sec-onds, to 3,000 seconds in 34 patients. Stereoscopic vision was not mea-suirable in 17 patients, an(d it could not be tested in 6 patients. The asso-ciated diagnioses are tabuilated in Table XVI. The spectrumll includesesotropia, exotropia, hypertropia, hypotropia, no surgery, multiple surg-eries, amblyopia, retinal diseases, chromosomie abnormalities, myopia,
751

Mitchell
TABLE XV: PERMIITTING FOVEAL FIXATION
NO. INIT SEX AGE TURN TILT CHIN TOTAL (O)* DIAGNOSIS
1 MB M 0+7 5 5 Ptosis2 JB M 2+6 5 5 Ptosis3 IIB F 0+9 5 5 Ptosis4 BC M 3+7 5 5 Ptosis, jaw w;ink5 DD F 0+7 25 25 Ptosis, nvstagmnts6 CT M 6+0 3 10 1:3 ROP, dragged frindi7 BR M 5+3 10 10 ROP8 MF M 5+9 12 8 20 Ptosis, Noonani syndrome9 EH M 2+3 5 5 Chalazion10 CH F 12+5 15 15 Bifocal too high11 LI M 0+8 8 8 Ptosis12 NL F 4+1 5 5 Hvpotropia13 RM M 6+10 10 10 Ptosis14 JN M 1+2 15 15 ? Visual fiel(l dlefect15 SP M 0+7 12 12 Ptosis16 JP F 0+8 5 5 Hlemanigioma17 SP F 0+4 30 30 Ptosis18 AR F 4+10 15 15 Ptosis19 TlI M 1+3 15 15 Moebius syndrome20 FS M 2+4 10 10 Ptosis21 SS F 3+5 10 10 Ptosis, hvliotropia22 HS F 3+10 10 10 Traumatic ptosis23 JS F 9+9 7 5 12 Ptosis24 MS M 18+1 10 10 Fibr-osis syndrome25 JVr M 12+9 11) 10 Moebius syndrome26 RT F 13+4 5 5 Ptosis27 \V;B F 10+2 50 6 56 Chalazionl/tosis
'Average degrees 12.8.
hyperopia, astigmatism, nystagmuis, "normal" eyes, macuila scar, plagio-cephaly without superior oblique compromise, cataract, binocular vision,absent binocular vision, limited cooperation because of age or develop-mental status, or excellent cooperation.
Campos'2 recommended an occluision test to rule out nonocular torti-collis. Each eye is occluded separately while a fixation target is observed.If there is no change in the torticollis, then the etiology is considerednonocular. If the headl remains straight after the occlusion of either eye,or if there is a shift in head posture with only one eye occluded, then thetorticollis is considered to be ocular in origin. This test should be per-formed as part of the total evcaluation of a patient with torticollis, especial-ly when the etiology is obscure. A change in the fixation pattern may sug-gest a source of the torticollis. Fine latent nystagmus may be revealed witlh
752

Ocular Torticollis 753
TABLE XVI: NO APPARENT REASON FOR TORTICOLLIS
NO. INIT SEX AGE STEREO TURN TILT CHIN TOTAL (°)* DIAGNOSIS
1 CA M 7+6 0 15 10 25 ET, HT, XT'2 SB M 12+11 0 6 6 ET, HT, amblyopia3 CB M 15+1 0 10 10 V ET4 AB M 3+0 0 4 5 9 Accommodative ET5 SB F 7+7 140 20 20 Recess MROU6 LB M 3+3 200 5 5 X'7 RC M 17+5 70 6 6 -5.00 OU8 NC M 4+11 100 10 10 Anisocoria9 AC M 5+8 0 8 8 EOM snirgeryx210 RC M 10+2 70 10 10 Herpes encephalitis11 MC M 7+5 100 20 20 Chin tuick, 1+ OA
IOOU12 KC M 0+5 N.A. 10 10 Infant posture13 SC F 1+10 N.A. 10 10 20 X(T)14 PC M 12+9 50 12 12 Overactive
RIO/ET' =215 CD F 7+6 0 8 8 Optic nerve
hypoplasia16 ED F 10+2 :30 10 25 35 Accommodative ET17 SD F 2+1 N.A. 30 30 X'18 RD F 4+5 3000 10 10 20 HT19 CE M 5+6 70 15 15 Amblyopia20 MF M 10+4 40 5 5 ET21 JG M 12+1 0 20 20 Recess MROU,
IOOU22 AG F 11+3 20 8 8 X, X'23 RG F 24+5 0 12 12 ET, HT24 GH M 29+5 0 5 15 20 ET, HT25 BH F 11+3 50 10 10 X'26 JJ M 3+3 200 30 30 XI27 CJ M 10+1 20 5 5 E'28 MJ F 0+11 N.A. 8 8 Plagiocephaly,
infant postuire29 LL F 14+6 0 8 8 5 21 Chromosome 5
deletion30 ML F 6+0 0 5 5 Macula scar left31 EL F 3+2 3000 5 5 Hypotropia32 SL F 14+0 20 8 8 Normal33 JL F 4+7 0 20 20 Aphakia, aiihbly
opia/XT34 KL M 7+0 0 15 15 Arthritis, right
aphakia35 DM M 9+3 70 15 15 X(T)36 PM M 5+6 3000 8 20 15 43 Doni syndrome,
ET37 SM F 8+4 ? 30 25 55 XT, +7.50 OU

Mitchell
TABLE XVI (CONTINUED): NO APPARENT REASON FOR TORTICOLLIS
NO. INIT SEX AGE STEREO TURN TILT CHIN TOTAL (O)* DIAGNOSIS
38 SN F 1:3+3 0 5 5 ET,IIT39 MO M 13+1 70 15 5 20 Astigmatism40 KP F 9+8 0 10 10 ET, IT41 KP F 5+6 10( 10 10 Accommodative ET42 AP F 3+2 30)00 15 15 X', lid lag43 FP F 11+6 30 5 5 Nor44 NIP M 9+8 3000 1( 10 XT45 CR F 6+6 20 10 10 NoIrImal1146 JR M 13+3 70 6 6 Accommodative ET47 NIR NI 6+9 0 8 8 HT48 CR NI 1+8 ? 15 15 Astigmriacltism49 PS NI 5+3 30 15 15 E50 RS F 7+4 10( 10 1( Cataract51 AT F 9+:3 3000 10 10 ET52 AU M 17+6 25 8 8 Myopia53 JU F 4+5 3000 8 8 ET54 13W NI 2+9 200 25 25 Norolal55 JX NI 9+6 1) 8 8 ET56 AB NI 6+5 25 5 5 X' 1557 SlI NI 6+11 10( 7 7 14 X(T)
'Average deg,rees 14.1.
careful observation, with the slit-lacmp biomiiiocroscope or by incdirect oph-thalmoscopy.
Hertle and Zhul 4 studie(d 298 patients with abnormal head posturing,with use of infrared ocuilography (IROG) to assist in diagnosis. Of thegroup studied, 116 patients (39%) had head posturing with or without nys-tagmus. Eleven children, ranging in age from 11 to 39 months, withabnormal lhead and face posturing, lacking; evidence of strabismnus, ortho-pedic neck disorders, ancd clinical nystagmus, were found to have congen-ital nystagmnus revealed by IROG. These 11 patients represenited 4% oftheir total stud(ly grouip, an(l 10% of their patients with torticollis. Patient47 and his family were able to travel to Dr Hertle's laboratory for IROG,and his results were normual.
The grouip of patients with uinexplained ocular torticollis in this stuclyalso accouint for almost 10% of the total patienits with torticollis. It is cer-tainly possible that one or imore of the patienits have nystagmulis detectableonly by IROG. However, all patients were examnined for nystagmus in theslit-lamp biomicroscope and by indirect oplhtlhalmnoscopy, an(d the likeli-hood of the mnajority of this grouip dem-onstrating nystagmults l)y IROG asthe etiology for torticollis seemns remote. Eleven patients of the 57 witl
754

Ocular Torticollis
nnexplained torticollis fell within the age range described by Hertle andZhu, where nystagmus was fouind with IROG.
Bagolini striated glasses are useful in assessment of torticollis.Campos'2 described ARC, anomalous retinal correspondence with striatedlenses, only in the position of torticollis, with diplopia or suppression in theother head positions. The anomalous type of binocularity or binocularvision provides the patient with a more advantageous visual state, with thepatient assuming a pathological head position in order to achieve anom-alouis binocuilar vision. The results of testing with Bagolini striated glasseshave been inconsistent, especially with children under 8 or 9 years of age,who have difficulty uinderstanding the concept and verbalizing a matuireresponse, even after various diagrams or charts are uised.
von Noorden'2' recommended the Bagolini striate lenses because thelenses permit a nearly normal view of the visuial environment, are not dis-sociating, and do not interfere with cyclofusion. The streaks of the lensesare placed on the horizontal axis in the trial frame, and a vertical prism isplaced before one eye to separate the streaks.
The pathophysiology of idiopathic torticollis was investigated byStrauibe and Dieterich.'45 Possible disturbance of the vestibular systemwas investigated in 40 patients with idiopathic torticollis by using elec-troystagmography, fundus photography, measurement of the subjectivevisual vertical, and posturograplhy. Results of the measuirement of thevisual vertical and the neuro-ophthalmologic testing were normal. Therewas slight pathologic monocular torsion in the fundus photography in 38%and a slight central vestibular preponderance in the electroystagmographyin 53% of the patients. There were some indications of slightly decreasedgain in visual contribution to the postural control process as measured pos-turographically. However; none of the resuilts could be correlated with theextent of torticollis in each case. The investigators proposed that theresults did not confirm the hypothesis of a primary vestibular lesion in thepathogenesis of the idiopathic torticollis. They suggested the possibility ofa common basic lesion causing the torticollis as well as affecting the cen-tral vestibular system.
OCULAR TORTICOLLIS ASSOCIATED WITH MEDICAL AND NEUROLOGIC
CONDITIONS
Table XVII and XVIII summarize this grouip, which comprises 25 patients,14 male and 11 femiale, ranging in age from 6 months to 83 years (averageage, 13 years 2 months). The average torticollis was 17.30, primarily fromface turns or head tilts, and occasionally from a chin posture. These med-ical and neuirologic conditions are all present in the general populationwithout ocular torticollis. This group of patients having ocular torticollis,
755

Mitchell
TABLE XVII: OCULAR TORTICOLLIS WITH ASSOCIATED MEDICALINEUROLOGIC CONDITIONS
NO. INIT SEX AGE STEREO TURN TILT CHIN TOTAL (°)* DIAGNOSIS
1 SB M 3+2 100
2 JB M 7+2 1003 FC M 83 304 NC F 5+9 ?5 TD M 7+2 ?6 KE F 3+6 1007 NF F 3+1 ?
8 LF F 4+7 2009 SG F 10+7 0
10 AH F
5
15107
25
1010
33 70
11 JJ M 13+1 50
12 SL F 0+713 LM M 23+6 0
14 JM M 62 3000
15 JM M 5+5 ?16 MN F 4+3 10017 MP M 8+5 50
18 RR F 9+5 019 NR M 3+0 ?
12
12
201010
715
20 KS M 2+10 10021 JV F 0+6 ?22 DA M 5+0 3000
23 SB F 14+5
24 DB M 11+0
?p 5
? 12
25 JP M 3+1 0 20
12 17 Traulmatic braininjury
10 10 Scoliosis12 12 Thyroid
15 Brain tumor10 Hydrocephalus
20 27 Vertebral fusion25 Traumatic brain
injliry
10 20 Myelomeningocele5 15 Neurological/
plagiocephaly10 10 Trauimatic brain
injutry/fuision15 15 Osteogenesis
imperfecta/ankspon
8 8 Inifatnt posture12 Tumor/lhydro-
cephalus/shunt7 19 Ependymoma/
myasthenia gravis20 Hypotonia10 Cerebral palsy
10 5 25 Spinal muscularatrophy
5 12 Cerebral palsy10 25 Arthrogryposis
syn(Iroine10 10 Macrocephaly5 5 Myelomeningocele
20 20 cerebral hemorrhage/hemianopsia
25 30 TBI/brain stemconttusion
15 27 Trauumatic brainijury
15 35 Ventricularhemorrhlage/cerebellarEncephalomalacia
'Average degrees 17.3.
included patient 6, whose torticollis was not orthopedic in nature, despitethe vertebral fusion. The response to stereopsis testing was varied, as seen
756

Ocular Torticollis 757
TABLE XVIII: SUMMARY OF TORTICOLLIS GROUPS
TABLE DIAGNOSIS PATIENTS MIALE FEMALE AVE AVERAGE AGE RANGE
TORT (°) AGE
IN Superior 59oblique palsy
VI Inferior 6oblique pals)
\I Browns 25VII Douible 9
elevator palsy\VIII DuaIie 46
syndromeIX Acq bor
ilIC'OOl asvin 48surgery
X Acq bor 116ilcoilCi-A or V patterni
XI 6tb nerve palsy 15XII Torsionial 4
inicomuitanceXIII Nystagmn-us 120XIV Conigeniial 69
esotropia/octularposture
XV; Permuittinig 27foveal
XV\I No apparenit .57reasoni for-torticollis
X\VII Assocwx/ 25miied/neuirolcoIlditions
None Superior rectuis 1pals),
Nonie Tbird nerve palsy, 1Nonie Spasiults uutauis 2
31 28 13.9 14+6 2+0 76+0
2 4 16.8 21+0 6+10 45+11
10 15 9.4 11+3 2+0 49+03 6 19.3 19+1 0+4 73+6
22 24 14.3 9+1 0+7 34+8
22 26 13.3 21+3 3+2 82+7
67 49 12.1 10+9 1+0 87+6
6 9 15.5 32+11 1+2 81+03 1 17.5 26+6 8+4 61+11
75 45 21.1 9+2 0+9 65+639 30 14.1 7+4 0+8 32+1
15 12 12.8 5+0 0+4 18+1
32 25 14.1 8+6 0+5 29+5
14 1 1 17.3 13+2 0+6 83+0
0 1 23 3+9 3+9 3+9
1 0 17 14+0 14+0 14+01 1 20 2+6 2+5 2+7
Sumnmuarv 630 343 287 15.7 13+3 0+4 87+6
in other groupings, ranging from 30 seconds to 3,000 seconds; 4 patientswere without stereoscopic vision, and 8 who could not be tested. A com-mon factor to explain the head postures in this group was not apparent.Because of the various medical and neurologic associations in this grolup,the etiology of the torticollis could not be objectively compared betweenpatients, and further evaluation of this group was not considered for this

studly.
SUPERIOR RECTUS PALSY, THIRD NERVE PALSY, SPASMUS NUTANS
One patient with a vague history of trauimla presented with left hypertropiaand underaction of the right superior rectuis at age 2. She initiallyresponded to a recession of tlhe right inferior rectus, but in timne (levelopedright hypertropia, with a 15° left head tilt acnd( 80 right face tuirn.
A 14-year-old boy had partial third nerve paralysis after falling out of atree and was not a candidate for surgery. He lacked many of the findingsusually seen in complete third nerve palsy.
One infant with spasnius nutans had suirgety for esotropia at 11 monthsof age, andl the other infant did not requiire surgery. Both patients havedemonstrated reduction in inystagmus and in heald bobbing.
DISCUSSION
During the past 20 years, this ophthalmology practice has seen a numberof patients exhibiting ocular toiticollis for nlO apparent or obviouis reasons.The impetus for this study Wcas to determine the cause of ocular torticolliswithin this group of patients and to comppare results with otlhers who halvestudied ocular torticollis, especially Kushiner,2 who found 8 basic imechl-nisms responsible for abnormal head postures. The intent of this paper,therefore, was to prospectively study, for 1 year, all patients whlo present-ed with torticollis of ocular origin and to idlentify and reevaluiate the etiol-ogy of ocuilar torticollis among different grouips, including tllose with uinex-plained ocuilar torticollis.
Unexplained ocuilar torticollis has been a historical reality. In a reviewof nonophthalmologic causes of torticollis, Bouitros and Al-Mateen'46 state,"There remain a grouip of patients, where the cauise will remain unclear."In reviewing causes for ocular torticollis, Kuslhner21 states, "Care, howev-er, mutst be taken to evaluate these patients properly, as the mneclhanism ofthe head posture is not always obvious." In their review of ocuilar torticol-lis, Rubin and Wagner'47 concluide, "Some patients may have an abnormalhead position with no satisf:actoiy explanation: This is a diagnosis of exclu-sion after all ocular andc nonocuilar causes halve been eliminiated." VonNoorden'" states, "The cauise of an ocular lhead tilt in the absence of acyclovertical muscle imbalanice is not always clear," an(d in reviewing clin-ical and theoretical aspects of cyclotropia, von Noorden'2' states that "in anumber of patients inconsistent (sensory) responses were obtained thatdefy explaniation at this time and will not be considered here." In con-genital esotropia with ocuilar posture, witlh a high incidenlce of DVD,Lang13 1'3-' notes that the head posttire is not a mechanisml for avoidance of
MIitchell758

Ocuilar Torticolli.s
diplopia, since binocular xision is required for diplopia to be experienced.Bechtel anid associates 35 reported a high inci(lence of head tilts in patientswith DVD and congenital esotropia and also claiim that DVD is a frequentcause of head tilts. Lang,I33134 Bechtel and associates,35 an(l others 136-140have thus described head tilting in association with congenital esotropiaand DVD blut have not explained the mechanism of the head tilting. Theocular torticollis in these auitlhors' series, as well as the torticollis in thegroup in this study, without apparent reason, maintains a head posturebecause of a presumed sensory adaptation or advantage, whiclh is difficultor impossible for most patients to verbalize.
This authlor was successful in determining a nuimber of the etiologiesfor ocular torticollis. In addition, after evaluation and reevaluation ofpatients Withl unexplained ocuilar torticollis, this author was able to reducethe number of cases of unlexplained ocular torticollis. The resuilts of thepresent stutdy are best compared with that of Kushner,2 who found 62.7%of patients with incomitance, compared with 52.4% found in this study. Asimilar incidence of nystagmus, 20.2%, paralleled this study at 19%.Congenital esotropia with ocular posture occurred in 6.3%, wllile thisstudy foundl 10.9%. Permitting foveal fixation produced 5.3% in Kushner'sstudy, as comppared to 4.3% with this study. The remaininlg categoriesincluded a few patients with ocular posture for cosmetic reasons, ocularmotor apraxia, spasmus nutans, and astigmiatismn. However, this studyfound 57 patients, or 9%, witlhout obvious or apparent reasons for oculartorticollis. While many parami-eters were reviewed and possible reasonsexplored, no (lefinite common factor or factors were found to explain thelarge number of patients in this group with varied visual and sensoryresponses demonstrating ocular torticollis, also without any evidence ofmusculoskeletal or neuirologic etiology. All of the usual sensory tests avail-able to the general ophtlhalmlologist were use(l, buit etiological questionsreImain.
Some pattients were recategorized, redutcing the number of cases oftorticollis without any apparent reason. A few patients with several oph-thalmic diagnoses couild be placed in different categories. Each patientwith torticollis above 50 was evaluiated in the prospective study of torticol-lis in this practice and classified within a categoiy ouitlined by Kushner.-Torticollis mieasurements were obtained by goniometer for optimal accu-racy and reproducibility, anid the 630 patients were classified within spe-cific categories during the 1-year prospective study.
It should be noted that this auithor's effort to recategorize thosepatients with unexplained torticollis may not be without criticism. Anyeffort at reevaluating only one group of patients could potentially compro-mise the results of the study by affecting various other outcomes and
759

percentages within each category of patients. In addition, it should benoted that upon reevaluation, some patients with unexplained ocular tor-ticollis demonstrated improvement or resolution of their head posture. Itis therefore also quite possible that patients in other categories experi-enced similar outcomes.
With these concerns in mind, specific reexamination was undertakenof those 57 patients in the group with unexplained torticollis, in an effortto define the etiology of the torticollis. Fourteen of the 57 patients werelost to follow-up, despite extensive and careful searches. Of those patientswho were able to return for reevaluation of the torticollis, 9 haLve shown areduction or resolution of their torticollis. Of the 34 remaining patientswithout change or improvement in their torticollis, 7 could not compre-hend sensory testing by way of double Maddox rod testing, Bagolini stri-ated glass testing, Lancaster red-green testing, and objective torsion eval-nations.
In Table XVI, the patients who were unable to be reevaluated sensori-ally included patient 11, who has developmental delay; patient 21, who isin special education and exhibits behavior problems; patient 29, who haschromosome 5 deletion and developmental delay and is nonverbal; patient34, who is now blind from severe uveitis; patient 35, who has develop-mental delay; patient 36, who has Down syndrome with limited testingcapability; and patient 54, who has developmental delay. While the initialfindings of these patients did not merit classification under medical/neu-rologic conditions, some of the patients in this group could now be reclas-sified in Table XVII as patients exhibiting ocular torticollis with associatedmedical or neurologic conditions. Other reclassifications might includedissociated vertical deviation as a probable etiologic factor for the torticol-lis in patients 18 and 40, and incyclotorsion in patient 7, which may explainhis right head tilt, to be described below.
Table XIX summarizes the sensory findings of 16 patients from thegroup who were reevaluated. The first column lists the patient numberpreviously used in table XVI. The total degrees of torticollis are listed forcomuparison with the initial evaluation. Under the headings "DoubleMaddox" and "Bagolini," "Ex" represents excyclotorsion and "In" repre-sents incyclotorsion. Under "Fundus torsion," the notations 1+, 2+, and 3+are based on the grading system for estimating abnormal torsion estab-lished by Guyton.119 The diameter of the disc is used as a guide, and abnor-mal torsion is graded according to each eighth of a disc diameter of abnor-mal displacement of the fovea from the normal range, which is within theupper third of the disc in the indirect ophthalmoscopic view. Of note ispresence of torticollis in the absence of binocular vision in several patients.
Several reevaluated patients are worthy of discussion. Patient 7
760 Mitchell

Ocular Torticollis
r4~
z
Z~~~~ ~ ~~~~~XN c !co r1 rq
z
t - ~ s_ ;rq Q +
o X o o I- t- oC c - c
CC tC C,-,
z c Oc.C t- O lr ,~r,)c~ ,),, ~ I
z~~~~ ~ ~
O~
zZ
761
I

preferred fixation with the right eye, with a persistent right head tilt. Thedouble Maddox rod test, Bagolini, and Lancaster red-green tests revealedincyclotorsion of both eyes. Although cyclotorsion is a rare cauise of torti-collis, this patient stated that the horizontal lines of the eye chart, as well asdistant objects, appeared parallel to the floor when he tilted his head to theright. However, when his head was held in primary position or in left tilt,he described the lines on the eye chart and distant objects at an "angle" tothe floor. He preferred using his right eye, with right head tilt posture, pre-sumably to reduce the right incyclotorsion, rather than upright posture orleft head tilt with increasing right incyclotorsion. Patient 7 had not beenable to describe this preference when last seen at age 17. Therefore, thispatient could be reclassified as torticollis due to torsional incomitance.
Patient 53 has persistent torticollis, suppression of OD, and inconsis-tent sensory responses, including 100 right incyclotorsion and 100 leftexcycltorsion confirmed with double Maddox rod testing and Lancasterred-green tests (Fig 4). However, torsion was not detected with the
HESS SCREEN CHARTFIELD OF LEFT EYE fi.i.gwith ,ghl eye) FIEW OF RIGHT EYE (fi.igwith left eye)
DIAGNOSIS Gpint 2WasrL morEya Greenbtive Right Eye
FIGURE 4Lancaster redl-greenl test deiiionstralting incyclotorsioil OD allld excvclotorsionl OS.
Bagolini striated glasses, and her fundus examination revealed 2+ incyclo-torsion, both eyes. Patient 55 still presents with torticollis yet has hadinconsistent sensory responses and no fundus torsion. Of the 2 patientswith autism, patient 26 was more able and cooperative than patient 13, yetboth patients' tests did not reveal the etiology of the torticollis. Patient 32has now shown resolution of her torticollis, and the etiology of her previ-ous torticollis remains unknown. The remainder of the patients in TableXIX demonstrate varying degrees of torticollis and strabismus, and almost
Mitchell762

Ocular Torticollis
all have normal douible Maddox rod testing, Bagolini striated glass testing,and Lancaster red-green testing, yet several demonstrated objective fYin-dus torsion.
The statns of the torticollis of the 14 patients lost to follow-up isunknown, and until proven otherwise, these patients should remain classi-fied as having torticollis without apparent reason. The torticollis of 9patients has been resolved. Two additional patients could be reclassifiedwith dissociated vertical deviation as the etiology of their torticollis, andone patient could be reclassified with ocuilar torsion as his torticollis etiol-ogy. This reduiced the nuimber of patients with uinexplained torticollisfrom 57 to 45, reducing the percentage of unexplained torticollis to 45 of630, or 7%.
CONCLUSION
This stuidy has fouind patients with ocular torticollis not of orthopedic orneuirologic etiology, which defies clinical explanation. Because a numberof patients demonstrate contradictory sensory testing, unanticipated andunpredictable testing responses, and the frequent and consistent inabilityto verbalize the reasons for their preferred head tilt, further studies areindicated.
Other areas for futuire stuidy incluide an evaluation of patients withDown syndrome, with a seemingly high number fouind with A and V pat-tern, as comnpared with all other groups. The limited response to sensorytesting in the group with congenital esotropia has been well documentedin other sttudies.133-13613S-140'43 A future study is planned to review our largegrouip of infants with congenital esotropia without torticollis for compari-son of their sensory findings, as published in other studies.'34,'"4-'3 Therange of stereoscopic vision in the A and V pattern groups also suiggestsfuirther investigation, as the head postures did not consistently correlatewith the clinical eye muscle patterns.
ACKNOWLEDGMENTS
The author gratefuilly acknowledges the suipport and encouragement of hissponsors, the late David S. Friendly, MD, and Edward A. Jaeger, MD, aswell as Marshall M. Parks, MD. Appreciation is extended to my col-leaguies, Maynard B. Wheeler, MD, and Peter G. Walden, MD, for refer-ring patients for this study. Finally, special thanks to Sarah E. Mitchell andDavid P Mitchell for their comnpuiter assistance and to Grace P. Mitchelland Jessica J. Mitchell, JD, for their editorial assistance.
763

764 Mitchell
REFERENCES
1. Mitclhell PR. Surgery for congeniital muotor nystagnmus. Regionial uipdate course. SanFranicisco: Amiiericani Acadel(emy of Ophthalmology; 1983;203-210.
2. Clark RN. Diagnosis anid managemeint of torticollis. Pediatr Annll 1976;43-57.3. (laser JS, Bachynski B. Congenital motor and sensory anomalies. In: Tasmnan X\Nled.
Duanie's Cliniical Ophlthalilomlogy. V6ol 2. Philadelphia: Lippincott; 1990;1-30.4. Slate RK, Posniick JC, Armstrong DC, et al. Cervical spine stubltuxation associated wvith
conigenital mnuscutlar torticollis anid craniiofacial asymmiiiietry. Plast Recon.str So rg1993;91:1187-119-7.
5. Bagolinii B, Camiipos EC, Chiesi C. Plagiocephaly causing superior oblique deficiencyanid ocuilar torticollis. Arclh Ophlthalmtiol 1982; 100:1093-1096.
6. Kiinsborne M. Hiatuis lerniia writh conitortionis of the nieck. Lancet 1964;1058-1061.7.Sidavay M. Torsion spasmii anid hiiattus lherniia. Ainn Radiol 1965;8:15-19.
8. Sutcliffe J. Torsioni spasmsis anid ahnormal posture iu children with hiattushernia-Sanidifer's syndelromiie. Progr Pcliatr Radiol 1969;2:196-197.
9. O'Doinnell JJ, Ho-ward RO. Torticollis associated Nxith hiattus hernia (Sandifers syn-dromi-e). Amit J Ophthaliioml 1971;71:1134-1137.
10. Ntitt AB. Abhormnal head postuire. Br Orthop J 1963;20:18-28.11. Hiatt RL, Cope-Tromipe C. Alnormal head positions due to ocular problemns. Ann
Ophthlalmtiol 1978;10:881-892.12. Caimipos EC. Ocutlar torticollis. Int Ophlthloiazol 1983;6:49-53.13. Cuignet. Des attitudes dans les miialadies des yetux et dti torticollis ocuilaire. Recelil
Ophithlalotiol 1873;1:199-206.14. Mitchell PR, \Vllhceler MB, Parks MM. Kestenbaunm surgical procedture for torticollis
secondary to conigeniital nystagmnus. J Pediatr Ophitlalmliol Strabi.sllis 1987;24:87-93.15. von Noordeni GK. Nystagmus. Ini: vonl Noordlen: Binioculair Visioni an-id Ocular M1otility:
Theory ani(d MWaniagement of Strabistiu.s. St Louis: Mosby; 1990;435-454.16. Verzella M, Graciaino W27 Dal Fiumiie E. Eight cases of octilartorticollis. Annll D'Ocl
1950;192:736-750.1 7. Rtuedemiiannii AD Jr. Scoliosis andI vertical ocuilar mulscle imnbsalance. Arcli Ophthialmtiol
1956;56:389-414.18. Dietrich DE, Slack W\J. Scoliosis seconidary to uniiilater-al extraocuilar lutiscle paresis
(octular torticollis). Radiology 1967;88:538-532.19. Wesson ME. The ocular significanice of abhuormiial lheadl positiolls. Br Orth1opt J
1964;21:14-28.20. Kuishnler BJ. Octular catuses of abniormiial head posttures. Ophthialmlology 1979;86:2115-
2125.21. Mitchell P1l. Sturgical miianiaagemnenit of nystagimtis. Ophithlalmiol Cliii North Aoi
1992;5:115-129.22. Cooper EL, Sauidall GS. Sur-aical treatmienit of conigeniital nvystagmus. Arc/li Opltlalmlol
1969;81:47:3-480.23. Sclhatz H, Urist Ml. Ani instrumiiienit for mieasturinig octular torticollis (head tuirni, tilt, anid
benrd). 1971;75:650-653.24. Youniig JDH. Heacl posttur-e miieastur-emiient. J PeFliatr Ophithalmitol Strabivsoiu.s 1988;25:86-
89.25. Urist MJ. Head tilt ini vertical muitiscle paresis. Aum J Ophithlalmtiol 1970;69:440-442.26. Camiipion CGS. Clinlical pictture anld(liagnlosis. Tranis Aoii Acad Ophthialmtiol Otolaryngol
1964;68:356-362.27. von Noordleni CK. A reassessmiienit of infantile esotropia, XLIV Edwacird Jacksoi

Ociular Torticollis 765
Meimiorial Lecture. Aoit J Ophithalmol 1988;105:1-10.28. Koiapp P. Classificationi anid treatmnient of suiperior oblique palsy. Am Orthop J
1974;24: 18-22.29. Khawam E, Scott AB, Jamiipolsky A. Acquired suiperior oblliqiue paIlsy. Arch Ophlthalmol
1967;77:761.30. Mittelmani D, Folk ER. The evaluation anid treatmiienit of'superior olblique muiscle palsy.
Tratns Am,l Acad Ophlthlalmtaol Otolarnjgaol 1976;81:893-898.31. Parks MM, Mitchell PR. Craniial nerve palsies. In: Tasman WN7 ed. Dulalas Clinlical
Ophlthalmology. Vol 1. Plhiladelplhia: Lippinicott; 1994;2,5-12.32. Ricker CNN' Paralvsis of the third, fourth anlad sixth cranial nernes. Am J Ophtlalmol
1958;46:787.33. Roicker CNN. The cauises of paralysis of the third, foutrth anid sixth craniial nerves. Amii J
Ophthialmol 1966;61:1293.34. Ruislh JA, Yoiiunge BR. Paraly-sis of craniial nerves III, IN' anld VI: Cauise an1d prognlosis in
1,00() cases. Arch Ophlthalmol 1981;99:76.35. Miller MT, Urist MJ, Folk ER, et al. Stiperior- obliquie pals> pr-esenitinig in late child-
hood. AmiJ Ophthalol 1970;70:212.36. Raskinid RH1. Acquir-ed bilateral suiperior obliquie palsy. Doc Ophithalouiol 1973;34:335.37. Fells P. Managemiienit of paralytic stabismus. BrJ Ophlthalmllvo 1974;58:255.38. Yominige BR. Analysis of troehlear nerve palsies. Wayo Clini Proc 1977;52:11.39. Riclhard BWN, Joines FR Jr, Youinige BR. Causes and progniosis in 4,278 cases of the ocuI-
lomiiotor, troclilear, aind abducens craniial nierves. Anii J Ophltalmtiol 1992;113:489-496.40. Lavin PJ, Troost BT. Traumiiiatic 4th nerve palsy. Ar^ch Neural 1984;41:679.41. Coppeto JM, Lessell S. Crvptogenic uinilateral paral>sis of tile suiperior oblique imiuscle.
Arch Ophithalmool 1978;96:27.5.42. Harley RD. ParalNtic strabisniitis in childrein. Ophlthlalmtiology 1980;87:24-43.43. Kodsi SR, Youniige BR. Acquired ocuilomiiotor, trochlclar and abducent craniial nerve
palsies in pediatric patieints. Aiim J Ophthaslmtiol 1992;114:568-574.44. Buiriain HM, Rowan PJ, Sullivan MS. Absenice of sponitanieous head tilt in superiol-
ol)li(que muscle pillsy. Amit J Ophithalmol 1975;79:972-977.45. Parks MM. Isolated cyclovertical imiuscle palsy. Archi Ophlthlalmtiol 1958;60:1027-1035.46. Bielschovwskv A. Lectuires oni miiotor aniomiialies of the eyes. II. Paralysis of ind(lividuial eve
mnuscles. Archi Ophthialmtiol 1935;13:33-59.47. Kuishner- BJ. Errors in the three-step test in the diagnosis of vertical strabismus.
Ophthalmology 1989;96:127-1:32.48. Kuishlier BJ. The diagniosis anid treatmlenit of bilateral masked suiperior oblique palsy.
Anii J Ophthlal:mol 1988;)105:186-194.49. Kraft SP, O'Doniogliue EP, Roarty JD. Improvensent of coimpensatory hiead postuires
after strabismus siirgerv. Ophthtalmology 1992;99:1301-1:308.50. liobb RNM. Idiopathic suiperior oblique palsies in children. J Pcdiatr- Ophthlalmol
Strahi.snn.s 1990;27:66-69.51. Olivier P, von Noordeni GK. liesuilts of suipe-ior obliquie tenectomy in inferior oblique
paresis. Arclh Ophlthalmol 1982;100:581-584.52. Scott WVE, Nankin Sj. Isolated iniferior oblique paresis. Arclh Ophithalmol 1977;95:1586-
1593.5:3. Reese PD, Scott WE. Suiperior ohlique tenotomiv in the treatmtienit of isolatted iniferior
oblique paresis. J Pcdiatr Ophlthl(loiiol Strabhismns 1987;24:4-9.54. Pollard ZP. Diagnosis aud(I treatmiienit of iniferior oblique pals>. J Pediatr Ophlthalmol
Strahbism.s 1993;:30: 15-18.55. Broxvv H\W. Congeiital struictuiral Imullscle anomalies. In: Alleni JH, e(l. Strabisimus

766 Mitchell
Ophithlalmic Symnposlo to I. St Lotiis: Mosby; 1950;205.56. Brown I1W' Isolate(d iniferior obliquie paralysis: Analysis of 97<caseS. Tran.s Ato
Opltlialmiol Soc 1957;55:415.57. Parks MM, Mitchell PR. Ophithialimologic syndromes anid trauim.a. In: Tasman \NN ed.
Duanc s Clitnical Oplhtlhalmology. Plhiladelplhia: Lippinicott; 1994;5-7.58. von Noordeni GK. Special forms of strabisiminls. In: von Noordlen, ed. Bioiocuilar V'isioni
anid Oculair Allotility. Theor7 ant(I Mlanagcment of St-abismus. St Loiiis: Mosby;1990;404-408.
59. Brovn I-lW Truie anid simuilitted suiperior oblique tenidoni sheath syndiromes. DocOphthaltotol 1973;34:123.
60. Parks MM. Doyne Memorial Lectuire, 1977: The suiperior oblique tenk(loni. TransOplhthl(lmlol Soc U K 1977;97:288-304.
61. Crawford JS. Suirgical treatmuent of truie Browns syndrome. Aol J Ophthalmol1976;81:287.
62. Crawforl JS. Symposium. Inicomiiitanit strahism-uis, truie Brown's Sundrome:itrgicaltreatimienit. Amii Ortlhop J 1977:;27:15.
63. von) Noorden GK, Olivier P'. Suiperior obli(qtue tenectomlNy in Browns syndrome.Ophlthlalmology 1982;89:303.
64. Crafod-(l JS, Ortoin RB, Lahow-Daily OC. Late resiults of superior- oblique muscleteinotomy in true Brown'Is synudrom e. Amii ] Ophlthlalmol 1980;9:824.
65. Parks NMIM, Euistis HS. Simiuiltanieouis siuperior ol)Iique tenotomy and(I iniferior- obli(lerecessioni in Brown's syndrome. Ophlthlalmology 1987;94:1043-1048.
66. WNrighit K\V, Mimi B-M, Park(C. Comilpauisoni of stiperior obliqtie tendon expanider tostiperior oblique tenetomuy for the management of stiperior ob)liquie overactioni anilaBrown's syndrome. J Jcdiatri Ophthaloolo Strabi.s,ou.s 1992;29:92.
67. Parks MM, Mitchell PR. Cr-ianlial nerve palsies. In: Tasman W ed. Duan1CS Clinic(ilOphlthablology. Vol 1. Plhiladelpliia: Lippiiicott; I 994;2-3.
68. Knapp P. The surgical treatmtnet of double elevator paralysis. Tramt.sAAm OphthialmiiolSoc 1969;67:304.
69. Scott WE. Jacksoni OB. Double elevator palsy: The significanice of inferior rectuisrestriction. Am71 Orthiop J 1977;27:5.
70. Duanl,e A. Congenital (leficiecy of abduictioni, associated with imipairimienit of adduictioii,retraction movements. Conitratctionis of the palpel)ral fisstire andl oblique movements ofthe eve. Ar-chi Oph1thalitiol 190(5;34:133-159.
71. Stillillg J. Unitersiuiclihiug uber (lie Ent.stchung (d('r Kurzsichtigkeit. Wiesbalen, XV'estGermanv': Bergman; 1887:1:3.
72. Ttiu-k S. Uber Retraktionshewegungen tier Auigeni. Deot.schl AIcd Wl"ochlctnschlr 1896;22: 199.
7:3. lHuber A. Electrophvsiologv of the retractioni syndromes. BrJ Ophtthalmol 1974;58:294-;43()0.
74. Parks MNM, Mitchell PR. Ophlthlmloplegic syndromes anid trautimia. In: Tasman W, ed.Dtnanv' s Clioical Ophlthlalmology. Plhiladelphiia: Lippincott; 1994;1-5.
75. Kr-aft SI'. A surgical approachl for Duiaine syndrome. J Pecliatr Ophithlamol Strabi.smtu.s1988;25: 119.
76. Jampolsky A. Surgical leaslies and reverse leashels in strabisimutis suirgicial management.Tlransactions of thec New Orleans Acad(elty of Ophlthllamtiology. Syoposiutm onlStrabisonms St Louiis: Moshy; 1978;252-253.
77. jampolsky A. Strategies in strahismus surgery. iratisactious of the Ncs Orlcan.sAcademy1 of Oplhthalmology. Pediaitric Ophthlttalology auid Strahi.sitois. New York:Raven Pr-ess; 1986;381-390.

Ocuilar Torticollis 767
78. Bloomii JN, Graxiss ER, Nalr-delli PG. A milaginetic resoInance imaging sti(lIv of theupshoot-downshoot phelloieieson of Dtiaoie's retractiooi syndrome. Aoii J Op)hthalmol1991;111:548-554.
79. von Noordeni GK. A miagnietic resoniaine imiiaginig study of the upslhoot-downishoot phe-inom11enIon of Duane's retractioni syndrome (letter). AII1 j Ophthalmnol 1991;112:358-359.
80. Alexander CM. Bilateral Duianie's retraction sisydrome. Am]tJ Ophthcledmol 1965;60:907.81. Kirkhamii TH. Inhlleritanice of Duianie's sndrome. Br J Oplithahoiiol 197(0;54:323.82. Pfaffenbach DD, Cross HE, Kearnis TP. Conigeniital aniomiialies in Duanie's retraction
snd(lrome. Arclh Ophltlalhiiol 1972;88:6:35-639.8:3. Metz HS, Scott ABR Scott NE. Ilorizonital saccadic velocities in Duane's syndrone. Am
J Oplhthlaloiiol 1975;80:901-906.84. Isenberg S, Urist NIJ. Cliniical observations in 101 consecutive patients wNith Duianie's
retraction syndrome. Amii J Ophtlalomol 1977;84:419-425.85. O'Mallev ER, Helxestoin EM, Ellis FD. Dutanie's r-etractioni syiidrome Plis. J Pediatr
Ophlthalmol Strabisoiiiis 1982;19:161.86. laab EL.Clinical featuires of Duianie's syndrome. J Pediatr Op/tilm/mol Strabi.som.s
1986;23:64.87. XWildervanck LS. Ecn servico-oculo acuisticus-syndrooIm. Ned Tijd.s'chir Gene'eskd
1960;104:2600.88. Nuitt AB. Thc signiificanice andcl sur-gical treatment of conigeniital octular palsies. Annii R
Coll Sm-g (Enl4and) 1955;:16:30.89. Gobin MI. Aspects of lhorizonital muiiiscle sugeryl par-ticularlyN in Duianle's syndrome.
Tranis Opit1halmol Soc U K 1972;92'685.90. Gobini MH. Suigical management of Duane's svndrome. Brj Ophthalmlo l 1974;58:301-
306.91. Feretis D, Papastratigakis J. Tsamparlakis J. Planning,? surgery in Duanie' syndrome.
Ophthalmolo(gica 1981;183:148.92. Molarte AB, Rosenbaum AL. Vertical rectus imiuscle tranispositioni suirgeery for Duiane's
syndrome. J Pediatr Oplitalmai7lol Strabiims' 1990;27: 171-177.93. Goldstein JH, Sacks DB. Bilateral Dtuane's syndrome.J Pediatr Ophthlalmol Strabismu.txs
1977; 14: 12:3.94. Pressmiiani 81, Scott N'E. Surgical treatmyieint of Duane's svy(nro( me. Ophthallolagy
1986;93:29-38.95. Nelsoni LB. Severe adduction deficiency follow\ring a large imiedial rectuis recessioni in
Duane's retractioni syndrome. Arcli Ophltalmalol 1986;104:859.96. Eisenhbam AM, Parks MNl. A study of various suirgical approaches for the lealsh effect
in Duane's syndrome. Presente(d at the joinit sessioni of the Amiiericain Associatioin forPediatric Ophthalmology and(I Strabismnius arsd tIme American Acadenmy ofOplhthalmologyt. 1980; Chlicagro.
97. von Noordenl GK, Murray E. Up aiid d(ownshoot in Duane's retraction synd(ro()me. JP'd(liatr Ophltalmalloo Strabi.sum.s 1986;23:2 12.
98. Jampolsky A. Discussioi of AM EisehbaumaniidiMM Parks: A studY of various su1r-gical approaclhes for the lealsh effect in Duane's s(llnromne. Presenited at the joinlt ses-sionl of the Amilericatin Associatioin for Pediatric Opihthalmology anid Strabisiotis aIId theAmerican Academy of Ophthalmology. 1980); Clhicago.
99. Rogers GL, Bremiier DL. Sutrgical treatmiienit of the tipshoot aind doNvwnshoot in Duane'sretractioin syndrome. Oplftialmologuy 1984;911:138).
100. Parks MM, Mitclhell PR. A and V l)atteriss. In: Tasman NN edl. Duianle's ClinlicallOplthalmomlogy. Philadelphiia: Lippiulcott; 1994;1-8.
101. Duane A. Isolatted paralvses of the ocuilar imuiiscles. Arc/l Oplithalmol 1897;26:317.

768 Mitchell
102. Urrets-Zavalia A. Abduccion en la elevacion. Arcli Ophthlalmiwl 1948;22:1.103. Urrets-Zavalia A. Paralysis bilateral congenita del musculo oblico inferior. Arcli
Oftalmol 1948;23:172.104. Urist JJ. Horizontal squint with secondary vertical deviations. Arch Ophthalmol
1951;46:245.105. Urist JJ. Surgical treatment of esotropia with bilateral elevation in adduction. Arch
Ophthalmol 1952;47:220.106. Parks MM. Strabismus anntual review. Arch Ophthalmol 1957;58:136-160.107. Knapp P. Vertically incomitant horizontal srabismus, the so-called A and V syndromes.
Trans Am Ophthalmol Soc 1959;57:666.108. Shrader EC, Schlezinger NS. Neuro-ophthalmologic evaluation of abducens nerve
paralysis. Arch Ophthalmol 1960;63:84.109. Ernest JT, Costenbader FD. Lateral rectus muscle palsy. Am J Ophthalmlol 1986;65:721.110. Reisner SH, Perlman M, et al. Transient lateral rectus muscle paresis in the newborn
infant. J Pediatr 1971;78:461.111. Robertson DM, Hines DJ, Rucker CW Acquired 6th nerve paresis in children. Arch
Ophthlalmtiol 1970;83:574.112. Werner DB, Savino PJ, Schatz NJ. Benign recurrent 6th nerve palsies in children. Arcli
Ophthalmitol 1983;101:607.113. Bixenman WVW, von Noorden GK. Benign recurrent 6th nerve palsy in childhood. J
Pediatr Ophithalml Strabismus 1981;18:29.114. Boger WP, Puliafito CA et al. Recurrent isolated 6th nerve palsy in children. Anni1
Ophthalnol 1984;16:237.115. Parks MM, Mitchell PR. Cranial nerve palsies. In: Tasman W, ed. Duane' Clinical
Ophthalmtiology. Philadelphia: Lippincott; 1994;12-16.116. Conrad HG, de Decker W Torsional Kestenbaum procedure: Evolution of a surgical
concept. In: Reinecke RD, ed. Strabismus II. Orlando, Fla: Grnne & Stratton;1984;301-315.
117. Metz HS, Norris A. Cyclotorsional diplopia following retinal detachmenit surgery. JPediatr Ophthalmol Strabismus 1987;24:287-290.
118. von Noorden GK, Jenkins RH, Rosenbaum AL. Horizontal transposition of the verticalrectus muscles for treatment of ocular torticollis. J Pediatr Ophthalbnol Strabislmlus1993;30 8-14.
119. Guyton DL. Clinical assessment of ocular torsion. Atmt Orthop J 1983;33:7-16.120. Locke JC. Heterotopia of the blind spot in octular vertical muscle imbalance. Amll J
Ophlthalmol 1968;65:362-374.121. von Noorden GK. Clinical and theoretical aspects of cyclotropia. J Pcdiatr Ophthalmnol
Strabismus 1984;21:126-132.122. von Noorden GK. Clinical observations in cyclodeviations. Ophthalmology
1979;86:1451-1461.123. Bixen-man WW, von Noorden GK. Apparent foveal displacement in normal subjects
and in cyclotropia. Ophthalmology 1982;89:58-62.124. Metzger EL. Correction of congenital nystagmuis. AmiJ Ophthalmlwl 1950;33:1796-1797.125. Kestenbaum A. A nystagmus operation. Proc XVII Council Ophthallol 1953;2:1071-
1078.126. Anderson JR. Causes and treatment of congenital eccentric niystagmus. Br J
Ophthalmtwl 1953;37:267-281.127. Goto N. A study of optic nystagmus by electroculogram. Acta Soc Oph1thalmCol Jap
1954;58:851-965.128. Cooper EL, Sandall GS. Sturgical treatment of conigenital nystagmus. Arch Ophthalmol

Ocil(ar Torticollis 769
1969;81:473-480.129. Pratt-jolmisoni JA. The stirgeir of conigeniital nvstagmus. Caln] Ophlthalou)l 1971;5(4):268-
272.130. Parks MNI. Conigeinital nvstagmns surgey. Ani Ortliop J 1973;23:35-39.131. Ccallhobti JH, HLarley RD. Surgery for abniormiial hea(l positioni in coingeniital inystagimuiis.
Tranis Aoii Oplhthlalzniol Soc 197:3;71:70-87.132. Nelsoni LB, Ervin-Mulvey LI), Calhotuni Jil, et al. Suirgical imianiagemilenit for abnormal
hea(l positioin in nvstagmus: The auigmiienited imio(lifie(l Kestenibauihim proceduire. Br JOphlthalmol 1984;68:786-800.
133. Lang J. Der kongenitale oder- Fiiihkinicdlicbe strabismus. Ophlthlalmologica 1967;154:201-2()8.
134. Lancrg J. Special formiis of comiiitanit str-abismnus. The 1982 Franik D. Costenibader Lecture.In: Reiniecke RD, e(l. Strabi.su.s II. Orland(lo, Fla: Groniie & Strattoni; 1984:769-786.
135. Beclhtel RT, Kuishlner BJ, NMortoni GCV The relatioinship bet-ween dissociated verticaldivergence (DVTD) anid hleadl tilts. J Pediatr Ophthlaltito/ Strabisml.s 1996;33:303-306.
136. Cronie KA. Alterniatinig IhN4erphoria. BrJ Ophltha/mol 1954;38:591-604.137. Anldersoin JR. Ocuilar Vertical Dcviation.s an1d Ny.stagmuii.s. Lonidoni: British Medical
Associationi; 1959.138. Ciancia A. La esotropia eni el lactanite diagniostico v tratamiiienito. Arc/i Chlil Oftalouiol
1962;9:117.139. Cianlcia A. La esotropia coni limitacion bilateral de la abdticcioll ell el lactalnte. Arc/u
Oftailmiiol Buetinos Aircs 1962;37:207-211.140. Ciancia A. Infantile esoptr-opia wxith abduictioni nvstagnuus. Ilt Ophthalomol Clin
1989;29:24-29.141. Ing NI, Costenibader FD, Parks N.MM, et al. EarlyN sugerv for congenital esotropia. Am]iJ
Op/ltlualailol 1966;61:1419-1428.142. Inog M. Early7 surgical alignnient for conigeniital esotropia. Trans Anii Op/lt/lalmool Soc
1981:;LXXIX:625-663.143. Pr-att-Johlmsoni JA. Ftusioni anid stippressioin: Development and loss. (18th Annuiiial Frank
D. Costenbader Lectiure). J Pecdiatr Op/ut/laloult Strabi.s,nu.s 1992;29:411.144. Hertle IRN' Zluu X. Inifrar-ed oculograplic uniiiaskiing of idiopathic abnormal head pos-
tiiring duie to occnlt nystagmius (in the absence of clinically detectable octilar oscilla-tionis). Binioc Vli.s Strabi.sonu.s Qtly 1997;12:91-98.
145. Stranbe A, Dieterich M. Neniro-ophtihalimsologic anid posttiu-ogr-aphic sttidies of patienitsNitl idiopatlic torticollis. Nerren(,iarzt 1993;12:787-792.
146. Bouitros GS, Al-NMateen NI. Non-ophthialmological cauises of torticollis. Ani Ort/lop J1995;45:68-7:3.
147. Rnhin SE, Wanger RS. Oenlar torticollis. Suirr Op/lt/lalmuol 1986;30:366-376.