Embed Size (px)
Citation preview

Nasopharyngeal CarcinomaNasopharyngeal Carcinoma
Dr Ravikumar

Nasopharyngeal CarcinomaNasopharyngeal Carcinoma

AnatomyAnatomy



EpidermiologyEpidermiology

IncidenceIncidence
• Rare neoplasm in most parts of worldRare neoplasm in most parts of world
• Higher incidence in Chinease & TaiwanHigher incidence in Chinease & Taiwan
• Chinease gene increase incidence of NPC Chinease gene increase incidence of NPC
• Age Age > > 40 years 40 years

IncidenceIncidence
• EmigrationEmigration from from high incidencehigh incidence to to low incidlow incidence areaence area reduces incidence of NPC reduces incidence of NPC
• Male : female = 3:1Male : female = 3:1

• Age wise bimodal distribution is also common. In this type of age distribution two peaks are noted, i.e. 1. between ages 15 - 20,
• 2. the second peak during the 4th and 5th decades. This type of distribution is common in India.

Risk factorRisk factor
• Genetic maker of NPC Genetic maker of NPC HLA-A2HLA-A2 ( found in Chinease( found in Chinease populationpopulation ) )
• EB-virusEB-virus
• Nitrosamines Nitrosamines
• Polycyclic hydrocarbonsPolycyclic hydrocarbons
• Chronic nasal sinus infectionChronic nasal sinus infection
• Poor hygienePoor hygiene

PathologyPathology

PathologyPathology
• The most common is The most common is squamous cell carcinsquamous cell carcinomaoma
• Most common position is Most common position is Rosenmuller fosRosenmuller fossasa
• Mass lesionMass lesion– exophytic massexophytic mass– Ulcerative massUlcerative mass– Infiltrative massInfiltrative mass



HistopathologyHistopathology

HistopathologyHistopathology
• Base on predominant histologic typeBase on predominant histologic type
• WHO type 1WHO type 1 : Squamous cell carcinoma n : Squamous cell carcinoma nonkeratizingonkeratizing
• WHO type 2WHO type 2 : Trasitional cell carcinoma : Trasitional cell carcinoma

HistopathologyHistopathology
• WHO type 3WHO type 3 : Undifferentiated carcimoma : Undifferentiated carcimomass– Lymphoepitheliomas Lymphoepitheliomas – Anaplastic carcinomasAnaplastic carcinomas

WHO type 1WHO type 1
• Squamous cell carcinoma nonkeratizingSquamous cell carcinoma nonkeratizing– Strong intracellular bridgesStrong intracellular bridges– Less keratin productionLess keratin production
• Less associate EBVLess associate EBV
• 25% of case25% of case
• Radioresistant tumorRadioresistant tumor

WHO type 2WHO type 2
• Trasitional cell carcinoma Trasitional cell carcinoma
• Not produce keratin Not produce keratin
• Greater degree of tumor pleomorphismGreater degree of tumor pleomorphism
• Most common is papillary morphologyMost common is papillary morphology
• 12% of case12% of case

WHO type 3WHO type 3
• Undifferentiated carciUndifferentiated carcinnomasomas• Lymphoepitheliomas, Anaplastic carcinomLymphoepitheliomas, Anaplastic carcinom
as, Clear cell carcinoma, Spindle cell carcinas, Clear cell carcinoma, Spindle cell carcinomaoma
• Most common cell type of NPCMost common cell type of NPC• Clear nucleus Clear nucleus • 63% aggressive behavior63% aggressive behavior• RadiosensitiveRadiosensitive


Tumor SpreadingTumor Spreading

Local Spread
Nasal cavity & PNS
Orbital invasionBase of Skull, Clivus
Sphenoid sinus
Cavernous Sinus
Lateral Parapharyngeal space
Middle ear cavity
Oropharynx (tonsillar pillars)
C1 vertebrae

Local invasionLocal invasion
• AnteriorAnterior : involve hard palate, medial ptery : involve hard palate, medial pterygoid plate, ethmoid & maxillary sinusgoid plate, ethmoid & maxillary sinus
• LateralLateral : involve internal jugular V, internal : involve internal jugular V, internal carotid A, CN IX X XI XII, carotid A, CN IX X XI XII,

Local invasionLocal invasion
• MedialMedial : Eustachian tube involvement, ma : Eustachian tube involvement, mastoid air cellstoid air cell
• SuperiorSuperior : involve base of skull, throught fo : involve base of skull, throught foramen lacerum & cavernous sinus ramen lacerum & cavernous sinus
• InferiorInferior : oropharynx : oropharynx
& soft palate& soft palate


Lymphatic spreadingLymphatic spreading
• Most common is neck node spreadingMost common is neck node spreading
• BBilateral involvementilateral involvement
• MMost common position is ost common position is upper jugular noupper jugular nodede
• LLeast east at submandibular at submandibular
& submental node& submental node

Distance metastasisDistance metastasis
• Most common isMost common is– Bone Bone – LungLung– LiverLiver
• Other sites are rareOther sites are rare

Clinical ManifestationClinical Manifestation

Clinical ManifestationClinical Manifestation
• Related to location of primary tumor & couRelated to location of primary tumor & course of diseaserse of disease
• Most common complaint is Hearing loss & Most common complaint is Hearing loss & lump in the necklump in the neck

Neck massNeck mass
• Most common spread to neck lymph nodeMost common spread to neck lymph node
• Complaint neck massComplaint neck mass
• Bilateral metastasis to lymph node is comBilateral metastasis to lymph node is commonmon

Neck massNeck mass
• Most common location is Most common location is Upper jugular noUpper jugular node de ( compose of jugular node, spinal acce( compose of jugular node, spinal accessory node ) ssory node )
• retropharyngeal node induce headacheretropharyngeal node induce headache


Frequency of lymph node Frequency of lymph node manifestrationmanifestration
• Upper jugular regionUpper jugular region
• Posterior cervical groupPosterior cervical group
• Middle & lower jugular groupMiddle & lower jugular group
• Supraclavicular groupSupraclavicular group


Nasal cavity involvementNasal cavity involvement
• Blood-tinge anterior or posteriornasal drainBlood-tinge anterior or posteriornasal drainageage
• Obstruction of nasal pathwayObstruction of nasal pathway
• EpistaxisEpistaxis
• HalithosisHalithosis

Ear involvementEar involvement
• Result fromResult from eustachian tube eustachian tube involvementinvolvement
• Sensation of ear blockageSensation of ear blockage
• Serous otitis mediaSerous otitis media
• Conductive hearing lossConductive hearing loss
• TinTinnnitusitus

Neurologic involvementNeurologic involvement
• Cranial nerve involvement found Cranial nerve involvement found 25 - 28%25 - 28%
• Pain in the neck, facial pain, facial pareathPain in the neck, facial pain, facial pareathesia ( CN V )esia ( CN V )
• Diplopia ( CN VI ) Diplopia ( CN VI )

Neurologic involvementNeurologic involvement
• CN III & IVCN III & IV late phase late phase
• CN VII & VIII CN VII & VIII less involvement less involvement
• CN IX, X & XI CN IX, X & XI can be found can be found

Clinical ManifestationClinical Manifestation
• Neck lumpNeck lump 60%60%• Ear (s) plugging & fullnessEar (s) plugging & fullness 41%41%• Hearing lossHearing loss 37%37%• Nasal bleeding Nasal bleeding 30% 30% • Nasal obstructionNasal obstruction 29%29%• Head painHead pain 16% 16% • Ear pain Ear pain 14%14%• Neck pain Neck pain 13%13%• Weight loss Weight loss 10%10%• Diplopia Diplopia 8%8%

Clinical ManifestationClinical Manifestation
• Neck massNeck mass 68%68%• HeadacheHeadache 58%58%• Ear painEar pain 52%52%• Nasal obstruction, bloody discharge Nasal obstruction, bloody discharge 48%48%• Facial pareathesia Facial pareathesia 22%22%• DysphagiaDysphagia 16%16%• Diplopia, strabismusDiplopia, strabismus 14%14%• Facial pain, eye painFacial pain, eye pain 12%12%• HalithosisHalithosis 12%12%• ExopthalmosExopthalmos 2%2%


Other sign & symptomOther sign & symptom
• Weight Weight
• AnorexiaAnorexia
• low grade feverlow grade fever
• TrismusTrismus
• Nasal regurgitation of fluidNasal regurgitation of fluid

TROTTER’S TRAID
• Conductive deafness
• Ipsilateral temporoparietal neuralagia
• Palatal paralysis

• Presence of unilateral serous otitis media in an adult should raise suspicion of nasopharyngeal growth

Diagnostic EvaluationDiagnostic Evaluation

Clinical evaluationClinical evaluation
• History takingHistory taking
• Physical examinationPhysical examination
• NasopharyngoscopyNasopharyngoscopy
• Endoscopic nasopharyngoscopyEndoscopic nasopharyngoscopy


Radiologic evaluationRadiologic evaluation
• Plain film head & neck Plain film head & neck
• CT scan head & neck ( for evaluation & treCT scan head & neck ( for evaluation & treatment planning ) atment planning )
• MRI ( if intracranial extension )MRI ( if intracranial extension )



Histopathologic evaluationHistopathologic evaluation
• BiopsyBiopsy
• Most common site are roof of nasophalynx Most common site are roof of nasophalynx & Rosenmuller fossa& Rosenmuller fossa

ImmunologyImmunology
• Indirect immunofluorescence for IgG & IgA Indirect immunofluorescence for IgG & IgA antibodies to viral capsid antigen (VCA) & antibodies to viral capsid antigen (VCA) & early antigen (EA)early antigen (EA)– Most specific test for diagnosisMost specific test for diagnosis– Highly predictive of the clinical courseHighly predictive of the clinical course– not yet commercially availablenot yet commercially available

ImmunologyImmunology
• Antibody-dependent cellular cytotoxicity ( Antibody-dependent cellular cytotoxicity ( ADCC )ADCC )– Often predict the clinical course of WHO type Often predict the clinical course of WHO type
2&32&3

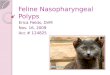
Clinical StagingClinical Staging

Staging: AJCC 2002
Stage I Stage IIA Stage IIB
Stage III Stage IVA Stage IVB

Clinical StagingClinical Staging
• T classificationT classification– TisTis carcinoma in situcarcinoma in situ– T1T1 tumor confine in tumor confine in one siteone site of nasopharynx no of nasopharynx no
tumor visible tumor visible – T2T2 tumor involve tumor involve 2 site2 site– T3T3
extension of tumor into extension of tumor into nasal cavity or oropharynxnasal cavity or oropharynx– T4T4
tumor invasion of tumor invasion of skull or cranial skull or cranial involvementinvolvement

58
Treatment
• Radiotherapy is the definitive treatment.
• Chemotherapy is used to supplement R.T. in advanced cases with cervical metastasis
• Role of surgery is only to take biopsy or to deal with cervical metastasis after the primary has been sterilized.

59
Complications of R.T.
• Mucositis
• Xerostomia
• Dental caries
• Radiation myelitis
• Optic atrophy
• Brain stem damage

ChemotherapyChemotherapy
• Control distance metastasisControl distance metastasis
• ComplicationComplication– Hair lossHair loss– Nausea & vomittingNausea & vomitting– Weight lossWeight loss– AnorexiaAnorexia

SurgerySurgery
• Lymph node present after radiotherapy 4 - Lymph node present after radiotherapy 4 - 6 weeks6 weeks
• Recurrent lymph node enlargement Recurrent lymph node enlargement

PrognosisPrognosis

PrognosisPrognosis
• 5 years survival ( A.C. 1965 )5 years survival ( A.C. 1965 )– Stage IStage I 44%44%– Stage IIStage II 30%30%
• Radiotherapy + Chemotherapy Radiotherapy + Chemotherapy good re good result sult

Conclusions
• Nasopharyngeal malignancies make up a different population of head and neck malignancies.
• These are eminently radio sensitive and curable.• Treatment planning is by necessity complicated
and time consuming.• Brachytherapy can be used for boosting the
local activities.• Chemoradiation is standard treatment in locally
advanced tumors

THANK U