Embed Size (px)
Citation preview

Thorax, 1980, 35, 936-940
Lung folding simulating peripheral pulmonaryneoplasm (Blesovsky's syndrome)C R PAYNE, P JAQUES, AND I H KERR
From the Brompton Hospital, London
ABSTRACT Six cases are reported in whom the diagnosis of benign pleural thickening with lungfolding simulating peripheral pulmonary neoplasm was made. Three patients presented withchest pain, two were asymptomatic, and the abnormality was a chance finding in one patient withasthma. The radiographs in all cases showed similar appearances-a peripheral opacity appearingto lie within the lung, usually the lower lobe, and characteristic curvilinear shadows extending fromthe opacity to the hilum. At thoracotomy, predominantly visceral pleural thickening had caused theunderlying lung to fold. Hyaline plaques were present on the parietal pleura elsewhere and pleuraladhesions were usually absent. Adequate removal of the thickened visceral pleura in five patientsallowed the folded lung to re-expand, with reversion of the chest radiograph to normal. One patientin whom the underlying lung folding was not appreciated at operation still has chest pain and thechest radiograph is unchanged. The radiographic appearances of this non-malignant condition,especially the appearances on lateral tomography, are diagnostic, and recognition may obviate theneed for operation in asymptomatic patients. For those patients with chest pain, thoracotomywith removal of the visceral pleura and release of the folded lung appears to be effective in relievingthis symptom.
Benign pleural thickening may occur in the formof localised hyaline plaques or generalised pleuraldisease covering one or more lobes. The affectedpleura consists of glistening, cartilage-like areasof thickening on either the visceral or parietallayers. As organisation proceeds, infolding of theunderlying lung occurs which on the radiographproduces the appearance of a peripheral massand may mimic a peripheral carcinoma of thelung.' Tomography, however, frequently revealsthe presence of curvilinear shadows connectingthe "mass" to the hilum of the lung. Theseshadows are not seen with peripheral pulmonaryneoplasms. Volume loss may be apparent in theaffected lobe. These signs are of value in thedifferential diagnosis of such cases.
Patients
Six cases are reported in whom the diagnosis ofpleural thickening with lung folding was madeat thoracotomy. Five patients were male and one(case 6) female. The age range was from 31 to
Address for reprint requests: Dr IH Kerr, Department of Radiology,Brompton Hospital, Fulham Road, London SW3 6HP.
60 years. Three patients presented with persistent,non-pleuritic chest pain and one with coincidentaldyspnoea on exertion related to reversible airwaysobstruction. The remaining two cases wereasymptomatic, having been discovered duringmass miniature radiography surveys. There wasno relevant occupational history and in particular,there was no known contact with asbestos. Fourpatients had physical signs compatible withpleural thickening. Sputum was examined in fivepatients and no acid-fast bacilli or malignant cellswere found. Erythrocyte sedimentation ratesranged from 5 to 48 mm in one hour. Four ofthese cases underwent bronchoscopy. Theappearances were entirely normal.
Radiographic and surgical findings
Each patient had frontal and lateral chestradiography, followed by relevant antero-posteriorand lateral tomography. In all six cases a quitedefinite peripheral mass was identifiable,apparently situated within the lung but attachedto the pleural surface. These patients underwentexploratory thoracotomy because of the radio-graphic features.
936

Lung folding simulating peripheral pulmonary neoplasm (Blesovsky's syndrome)
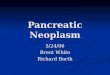
CASE 1 (AM)Plain radiographs showed a mass in the rightlower lobe posteriorly and calcified tuberculouslesions in the left upper lobe (fig la). There wasmarked pleural thickening in the costophrenicrecess. Lateral tomography demonstrated curvi-_.r.T... }..
L.(a)
(b)Fig 1 Case 1: (a) postero-anterior radiograph,(b) lateral tomograph showing right lower zoneopacity, pleural thickening, and curvilinear shadows.
linear shadows stretching from the mass to theright hilum (fig lb). At thoracotomy the rightlung was found to be encased in a thick fibrouscoat of visceral pleura, most dense over thelower and middle lobes. The diaphragmaticsurface of the right lower lobe had rotatedupwards and posteriorly almost to the apex ofthe right lower lobe. There was 60 ml of serouspleural fluid and minimal adhesions betweenvisceral and parietal layers. After pulmonarydecortication the right lower lobe expanded toits normal volume and shape. Histology of thethickened visceral pleura was reported as showingorganised fibrin and prominent lymphoid follicleswith no evidence of "collagen change."
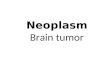
CASE 2 (DL)Radiography demonstrated an irregular opacityin the right lower lobe posteriorly, attached tothe pleura and with curvilinear streaks radiatingtowards the hilum (fig 2). There was an abnor-mal density in the middle lobe region. Thora-cotomy revealed grossly thickened visceral andparietal pleura encasing the middle and rightlower lobes and 600 ml of serous pleural fluid.The posterior part of the night lower lobe wasfolded. After decortication there was good re-expansion of the middle and right lower lobes.Histology of the excised pleura was fibrous tissueonly, without asbestos bodies.
Fig 2 Case 2: lateral tomograph showing anopacity lying posteriorly in the right lower lobe.
937

C R Payne, P Jaques, and I H Kerr
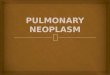
CASE 3 (GWB)Radiographs of this patient showed a roundopacity aipparently lying in the periphery of theleft lower lobe with curvilinear shadows connect-ing the opacity to the hilum (fig 3). At thora-cotomy, thick smooth fibrous plaques were pre-sent in the paravertebral gutter, on the dia-phragm, and on the lower lobe posteriorly, withinfolding of the left lower lobe. Wedge resectionof the folded lung segment with overlying pleurawas performed. Histology showed severe focal,pleural, and interlobular fibrosis with no evidenceof inflammation or neoplasm.
Fig 3 Case 3: lateral tomograph demonstratingopacity in left lower lobe with curvilinear shadows.
CASE 4 (GD)Radiography demonstrated pleural thickeningover the left lung with a 3 cm opacity in theleft lower zone attached to the pleural surface.Curvilinear shadows extended from this regionto the hilum (fig 4). At left thoracotomy thepleura was extremely thickened with extensiveadhesions. The lingula had folded into the fissure,and smaller areas of folding were also present inthe lower lobe. Pleurectomy was performed,releasing the areas of folded lung. Histology ofthe excised pleura showed marked fibrosis andfoci of chronic inflammatory cells without evi-dence of malignancy.
Fig 4 Case 4: (a) postero-anterior radiograph,(b) lateral tomograph showing pleural thickening,left lower lobe opacity and curvilinear shadows.
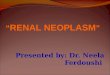
CASE 5 (GB)Plain radiography showed a poorly defined 5 cmmass lying posteriorly in the right lower lobewith pleural plaques on both chest walls (fig 5a).Tomography confirmed the pleural thickeningover the right lower lobe posteriorly with an ovalshaped opacity extending forward into the lowerlobe and curvilinear shadows radiating to thehilum (fig 5b). At thoracotomy, hard whiteplaques were present on the parietal pleura. Thevisceral pleura was abnormal over the greaterand lesser fissures and tended to enfold the right
938

Lung folding simulating peripheral pulmonary neoplasm (Blesovsky's syndrome)
lower lobe. This visceral layer was excised andthe underlying lung allowed to expand. Histologyshowed fibrosis with groups of reactive meso-thelial cells.
(a)
(h)Fig 5 Case 5: (a) postero-anterior radiograph,(b) lateral tomograph showing right lower lobeopacity and curvilinear shadows radiating to thehilum. Marked volume loss of the right lower lobeis apparent.
CASE 6 (Mw)Frontal and lateral chest radiography showed anopacity lying posteriorly, apparently within the
right lower lobe, with an associated pleural effu-sion (fig 6). Tomography confirmed the curvi-linear shadows extending towards the hilum.Five hundred millilitres of sterile straw-colouredpleural fluid were aspirated before operation.Cytological examination of this fluid revealedlymphocytes and a few polymorphs. At rightthoracotomy the visceral pleura was thickenedover the posterior basal segment and adherent tothe chest wall. Some areas of parietal pleuralthickening were noted. Biopsies of parietal andvisceral pleura showed dense fibrosis. Lung biopsyshowed thickening of alveolar septa by fibroustissue and foci of chronic inflammatory cells,predominantly lymphocytes. There was no evi-dence of malignancy. Pleurectomy and releaseof the underlying folded lung was not performedand postoperative chest radiographs still showedthe opacity in the right lower zone with pleuralthickening. This patient continued to complainof chest pain.
In summary all six cases showed discrete,peripheral, apparently intrapulmonary opacitieswith curvilinear shadows extending towards thehilum. The lower lobe was involved in all patientswith additional folding of the lingular segment inone. All cases showed evidence of pleural thick-ening elsewhere and five had volume loss of theaffected lobes.
.-
Fig 6 Case 6: postero-anterior radiographdemonstrating opacity in the right lower lobe,right pleural effusion, and curvilinear shadows.
939
--t -;
.Mw-

940
Discussion
Benign pleural plaques are an extremely com-
mon finding at necropsy, though only 15% ofsuch cases have radiologically visible signs.2Occasionally such plaques reach a size sufficientto make the radiologist uncertain as to whetherhe is dealing with a pleural or a penipheral pul-monary lesion. Tivenius drew attention to 10such cases of benign pleural lesions simulatingpulmonary tumours and recommended diagnosticpneumothorax as a means of localising thelesions to the pleura.3 In all his cases the pleuralplaque was parietal although, as in our cases,there was a surprising lack of adhesions betweenthe two pleural layers. This would have madediagnostic pneumothorax and thoracoscopy feasi-ble. Two similar cases were described byGalatius-Jensen and Halkier who also adviseddiagnostic pneumothorax.4 Dobrowolski andGlowacka reported five cases, four of whomunderwent thoracotomy before the diagnosis ofbenign hyaline pleural plaque was made.5 Inthese cases the plaque was associated with mini-mal adhesions and situated on the visceral pleura.Our approach would stress the value of tom-
ography. The appearances are so characteristicthat a diagnosis can be made with some confi-dence and, therefore, operation can be avoided.Since we began to recognise this condition, we
have seen several other asymptomatic cases withthe characteristic radiographic appearances oflung folding. These patients have not been sub-jected to thoracotomy and follow-up has beenuneventful. Surgical treatment may, however, benecessary for the relief of chest pain and toremove thickened pleura. Operation may alsobe indicated in those cases in whom doubtremains about the precise diagnosis after fullradiographic assessment. Our two patients whocomplained of chest pain at presentation and whohad removal of the pleura with release of thefolded lung have remained free of pain sinceoperation and their chest radiographs havereverted to normal. We have not seen recurrenceof the radiographic abnormality in any patientafter operation.The aetiology of these large plaques is un-
certain but asbestos has been incriminatedwhether there is recognised exposure or not.2 6 7
Pleural disease caused by asbestos is frequentlyparietal but involvement of the visceral pleurahas been noted.2 Pulmonary infarction or infec-tion is known on occasion to give rise to similarpleural thickening. The histopathology in eitherevent is relatively nonspecific.
C R Payne, P Jaques, and I H Kerr
Blesovsky was the first to describe the "lungfolding" which may occur in association withlarger pleural plaques or grossly thickenedpleural membrane.1 All three of his cases had afibrous membrane on the visceral pleura withoutadhesions to the parietal layer. Our cases werealso found to have predominantly visceral pleurallesions. Indeed, it is hard to visualise how lungfolding could arise without the pleural plaquebedng primarily on the visceral layer in theabsence of significant viscero-parietal pleuraladhesions. The illustrations of Blesovsky's cases2 and 3 elegantly demonstrate the pleural massassociated with volume loss in the adjacent lobeand curvilinear shadows radiating from thepleural mass towards the hilum of the lung.The pathological basis for these cuniously curvedshadows is not finally established, in spite ofadequate surgical inspection. One of the constantfeatures of these cases is the volume loss associ-ated with the plaque and the subsequent re-expansion of the lobe after pleurectomy. We feelthat the curvilinear shadows probably reflect themechanical distortion of the lobe produced bythe forcible contraction of the outer pulmonarysurface attached to the relatively fixed hilum,resulting in compression of pulmonary tissuealong bhe lines of the intralobar septa.
We would like to thank Miss Angela Parkinsonfor typing the manuscript and the Departmentof Medical Photography, Royal MarsdenHospital, for the illustrations.
References
1 Blesovsky A. The folded lung. Br J Dis Chest1966; 60:19-22.
2 Hourihane DO'B, Lessof L, Richardson PC.Hyaline and calcified pleural plaques as an indexof exposure to asbestos. A study of radiologicaland pathological features of 100 cases with aconsideration of epidemiology. Br Med J 1966;1: 1069-74.
3 Tivenius L. Benign pleural lesions simulatingtumour. Thorax 1963; 18:39-44.
4 Galatius-Jensen F, Halkier E. Radiologicalaspects of pleural hyalo-serositis. Br J Radiol1965; 38:944-6.
5 Dobrowolski J, Glowacka R. Pleural hyalo-serositis lesions imitating a lung tumour. RadiolDiagn (Bert) 1968; 9:199-205.
6 Collins TBF. Pleural reaction associated withasbestos exposure. Br J Radiol 1968; 41:655-61.
7 Kiviluoto R. Pleural plaques and asbestos:further observations on endemic and other non-occupational asbestosis. Ann NY Acad Sci 1965;132:235-9.