Embed Size (px)
Citation preview

Presented by: Dr. Neela Ferdoushi
“RENAL NEOPLASM”

6 October 2010 2
Background
Kidney cancers account for about 3% of all cancer cases as well as about 3% of all cancer deaths.
38,890 new diagnoses and 12,840 deaths were expected in 2006.
$1.9 billion is spent in the United States each year on treatment of kidney cancer.

6 October 2010 3
Kidney TumorsMost renal tumors arise from the renal parenchyma
(referred to as renal cell tumors, renal cortical tumors, or renal parenchymal tumors),
A much smaller number arising from the urothelium of the renal collecting system (urothelial carcinoma or transitional cell carcinoma [TCC]) or the mesenchyma (eg, angiomyolipoma, leiomyoma, liposarcoma).
Benign renal parenchymal tumors include renal oncocytoma (5%) and the rarer metanephric adenoma, metanephric adenofibroma, and papillary renal cell adenoma.

6 October 2010 4
Kidney TumorsMalignant renal cell tumors occur nearly twice
as often in men as in womenThe age at diagnosis is generally older than 40
years; the median age is in the mid-60sBilateral multifocal renal tumors are present in
approximately 5% of patients with sporadic renal tumors
As in solitary disease, conventional clear cell histology is the most common histologic subtype;

6 October 2010 5
Kidney Tumors PresentationCommon symptoms that lead to the
detection of a renal mass are hematuria, flank mass, and flank pain.
Less frequently, patients present with signs or symptoms resulting from metastatic disease, such as bone pain, adenopathy, and pulmonary symptoms.

6 October 2010 6
Benign renal neoplasms Benign renal neoplasms that occur in adults constitute
heterogeneous group of tumors with characteristic histology and variable clinicobiologic profiles.
The 2004 World Health Organization (WHO) classification schemata categorizes benign renal neoplasms on the basis of histogenesis (cell of origin) and histopathology. Renal neoplasms are thus classified into renal cell, metanephric, mesenchymal, and mixed epithelial and mesenchymal tumors.

6 October 2010 7
APPENDIX 1: World Health Organization (WHO) Histological Classification of Benign Renal Neoplasm's
Renal Cell TumorsMetanephric
TumorsMesenchymal
Tumors
Mixed Epithelial and Mesenchymal
Tumors
OncocytomaMetanephric
adenoma Angiomyolipoma Cystic nephroma
Papillary adenomaMetanephric
adenofibroma Leiomyoma
Mixed epithelial and stromal tumor
Metanephric stromal tumor Hemangioma
Lymphangioma
Reninoma
Fibroma
Schwannoma

6 October 2010 8
Renal Cell Neoplasms OncocytomaOncocytoma is a benign renal cell neoplasm that accounts
for approximately 5% of all adult primary renal epithelial neoplasms. Most tumors occur sporadically in asymptomatic patients.
Oncocytoma is histologically composed of nests and acini of large polygonal cells with mitochondria-rich eosinophilic cytoplasm . Oncocytomas typically appear as solitary, well-demarcated, unencapsulated, fairly homogeneous renal cortical tumors. Hemorrhage may be found in up to 20% of cases. A spoke-wheel pattern of feeding arteries associated with a homogeneous nephrogram is a characteristic finding on catheter angiography.

6 October 2010 9
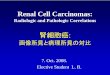
Fig. 1 —72-year-old man with hereditary oncocytosis syndrome. Coronal contrast-enhanced CT scan during nephrographic phase shows bilateral solid renal masses (arrows) that were characterized as oncocytomas on histopathology.
Fig. 2 —64-year-old man with histologically proven oncocytoma. K = kidney. Axial fat-saturated, gadolinium-enhanced T1-weighted 3D gradient-refocused echo image shows right kidney mass (arrow) with hypointense central scar (S).

6 October 2010 10
Papillary Adenoma Papillary adenomas are the most common
renal epithelial neoplasms. According to autopsy series, approximately 40% of patients older than 70 years harbor renal adenomas. Papillary adenomas are alsocommonly found in patients with acquired renal cystic disease and in patients undergoing long-term hemodialysis.
By definition, papillary adenomas measure 5 mm or less. They are usually subcapsular and solitary. Adenomas are histologically characterized by papillary or tubular cytoar-chitecture and frequent psammoma bodies.

6 October 2010 11
Cytogenetic changes of papillary adenomas include loss of the Y chromosome and combined trisomy of chromosomes 7 and 17. Histologic and genetic abnormalities of renal adenomas are indistinguishable from papillary RCCs.
Papillary adenomas are extremely small (< 5 mm) and may not be distinguished from other renal tumors (particularly RCC) and pseudotumors on imaging studies.

6 October 2010 12
Metanephric Neoplasms Metanephric neoplasms are a heterogeneous group of benign renal neoplasms that include metanephric adenoma (epithelial tumor), metanephric stromal tumor (stromal neoplasm), and metanephric adenofibroma (mixed epithelial and stromal neoplasm). These tumors are histogenetically related to Wilms' tumor and arepostulated to represent the most hyperdifferentiated, benign end of the nephroblastoma spectrum .

6 October 2010 13
Metanephric adenoma is a benign renal neoplasm with peak age of occurrence in the fifth or sixth decade and a 2:1 female preponderance. Metanephric adenoma is asymptomatic in approximately 50% of patients; abdominal pain and hematuria are common clinical symptoms. Polycythemia, a characteristic finding seen in approximately 10% of patients with metanephric adenoma, promptly disappears after surgical resection.

6 October 2010 14
Metanephric adenoma is histologically characterized by the arrangement of monotonous small blue embryonal epithelial cells in an acinar, tubular, or sheetlike configuration. Abundant psammoma bodies are commonly found.
Metanephric adenoma typically appears as a well-defined, unencapsulated, solitary solid mass. It commonly appears as a hyperattenuating mass on unenhanced CT; large tumors appear as heterogeneous, hypovascular masses with frequent foci of hemorrhage and necrosis. Calcification is seen in 20% of cases. Metanephric adenoma appears as an expansile hypoechoic or hyperechoic mass on sonography.

6 October 2010 15
Mesenchymal Neoplasms Angiomyolipoma
Angiomyolipoma (AML) is the most common benign mesenchymal neoplasm; it is composed of variable proportions of blood vessels, smooth muscle, and adipose tissue. Renal AMLs consist of two distinct histologic subtypes, classic triphasic and monotypic epithelioid. It will not be further discussed in this article.Classic AML may occur either sporadically or in association with tuberous sclerosis complex (TSC). Sporadic renal AMLs show a 4:1 female preponderance and are more likely to be solitary and symptomatic. Patients with TSC harbor small, multicentric, asymptomatic AMLs; 80% of patients with severe TSC have renal AMLs. The morphology of AMLs depends on the relative proportionsof various components. Profuse elastin-poor, dysmorphic blood vessels predispose to aneurysm formation and hemorrhage.

6 October 2010 16
Hemangioma Renal hemangioma is a rare benign mesenchymal neoplasm
that consists of multiple endothelium-lined, blood-filled vascular spaces. It commonly affects young adults with no specific sex predilection. Recurrent episodes of hematuria and renal colic are typical presenting symptoms; however, incidental diagnosis in asymptomatic patients is also common. Hemangioma of the kidney occurs as an unencapsulated, unicentric, solitary tumor that frequently arises from the renal pyramids or the pelvis.
LymphangiomaLymphangioma of the kidney is a rare benign cystic tumor that most often arises from the peripelvic region or renal sinus. It may also uncommonly arise from the lymphatics of the capsule or the cortex. Histologically, lymphangiomas consist of communicating endothelium-lined spaces that contain clear fluid. The septa may show lymphoid cells.

6 October 2010 17
Mixed epithelial and mesenchymal neoplasms comprise two
histologically distinct entities: mixed epithelial and stromal tumors and cystic nephromas.
Mixed Epithelial and Stromal Tumor:Mixed epithelial and stromal tumors occur almost exclusively in
perimenopausal women (6:1 female preponderance); most patients are receiving estrogen therapy. Twenty-five percent of the tumors present as incidental findings; most patients manifest nonspecific symptoms of flank pain and hematuria. Pathologically, mixed epithelial and stromal tumor is a benign, bimorphic solid-cystic neoplasm that consists of epithelium-lined cysts or microcysts and variably cellular spindle-cell, ovarianlike (estrogen- or progester-one-receptor positive) stroma.
Cystic NephromaCystic nephroma is a benign cystic neoplasm that affects
predominantly middle-aged, perimenopausal women. Adult-onset cystic nephroma is histogenetically and morphologically different from pediatric cystic nephroma. Morphologically, cystic nephromas are composed of encapsulated, noncommunicating cysts with thin septations.
Mixed Epithelial and MesenchymalNeoplasms

6 October 2010 18
Wilms tumor:It is the most common primary renal tumor of
childhood.Age Incidence: 2-5 years.Involve both kidneys either simultaneously or one
after other.Pathogenesis and genetics:There is association of at list three congenital
malformations with distinct chromosomal loci.WAGR Syndrome: aniridia, genital anomalies,
mental retardation, and wilms tumor. Denys-Drash Syndrome: gonadal dysgenesis,
nephropathy.Beck with Wiedemann Syndrome

6 October 2010 19
Wilms Tumor

6 October 2010 20
Morphology: The tumor is large solitary well
circumscribed mass either bilateral or multi centric.
On cut section it is soft, homogenous, with hemorrhage and necrosis.
On M/E: There is combination of blastemal, stromal, and epithelial cell types.
Other heterogonous elements- Squamous or mucinous epithelial adipose tissue and smooth muscle.

6 October 2010 21
Renal Cell CarcinomaRenal cell carcinoma is the most
common primary parenchymal malignancy of the kidney and accounts for 3% of all new cancers annually in the United States, with approximately 30,000 new cases per year.

6 October 2010 22
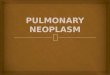
Histopathology of Renal Cell Adenocarcinoma, Kidney

6 October 2010 23
Renal Cell Cancer Risk FactorsSmoking: Cigarette smokers are twice as likely as
nonsmokers to develop kidney cancer. Obesity: People who are obese have an increased risk of
kidney cancer. High blood pressure: Increases the risk of kidney cancer. Long-term Dialysis: Being on dialysis for many years is a risk
factor for kidney cancer. Von Hippel-Lindau Syndrome: VHL is a rare disease that
runs in some families. An abnormal VHL gene increases the risk of kidney cancer.
Occupation: Coke oven workers in the iron and steel industry are at risk. Workers exposed to asbestos or cadmiumalso may be at risk.
Gender: Males are more likely than females to be diagnosed with kidney cancer.

6 October 2010 24
Renal Cell Cancer SymptomsBlood in the urine (making the urine
slightly rusty to deep red)
Pain in the side that does not go away
A lump or mass in the side or the abdomen
Weight loss, fever, anemia
Feeling very tired or having a general feeling of poor health

6 October 2010 25
Background and statisticsIn the United States, kidney cancer accounts for about 3%
of all cancers, with approximately 12,000 kidney cancer deaths each year.
Kidney cancer strikes more than 28,000 Americans each
year—many of whom have no overt symptoms.
The majority of people with kidney cancer are past the age of 40, and it strikes men twice as often as women. Kidney cancer is usually diagnosed between the ages of 50 and 70, but can occur at any age.
It is one of the fastest-growing cancers in the United Kingdom.
There are several genetic factors that predispose people to kidney cancer but this only happens in 5% of the cases.

6 October 2010 26
Classification Of Renal Cell Carcinoma
Clear Cell Carcinoma: 70% to 80% of renal cell cancers on histology. The tumors are made of cells clear or granular cytoplasm and are non-papillary.
They are associated with VHL disease. There is loss of sequence on the short arm of chromosome 3.

6 October 2010 27
Papillary Carcinoma 10% to 15% of renal cancer Papillary growth pattern occurs in both sporadic
and familial form. Cryptogenic abnormalities- Trisomy 7,16,17, loss
of Y.M/E: Complex Papillary formation are seen often
associated with prominent stromal infiltration by neutrophils or foamy macrophages. Psammoma bodies are numerous.
Immunohistochemistry- Expression of keratin. Type 1Type 2

6 October 2010 28
Cromophobe Renal Carcinoma:5% of renal cell cancer.
On cytogenetic examination these tumors exhibit multiple chromosome losses. The cells are composed with prominent cell membrane and pale eosonophilic cytoplasm with a halo around the nucleus.

6 October 2010 29
Collecting duct Carcinoma:1% of renal epithelial carcinoma.
Arise from collecting duct cells of medulla.
A number of chromosomal losses and deletions.
Histologically nests of malignant cells enmeshed within a prominent fibrotic stroma.

6 October 2010 30
Morphology of RCC:The tumor may arise in any portion of
kidney, but usually affects the upper pole.Clear cell neoplasm arise from proximal
tubular epithelium.They are spherical masses which may
distort the renal out line.The margins are sharply defined.In CCC the tumors cells have a rounded
or polygonal shape and abundant clear or granular cytoplasm.

6 October 2010 31
Papillary tumors arise form distal convoluted tubules.
They are typically hemorrhagic and cystic.As tumor enlarge they may bulge into the
calyces and pelvis and may extend into the ureter.
This tumor may invade the renal vein then to the inferior vena cava and even in the right side of heart.
The tumor composed of cuboidal or low columnar cells arranged in papillary formations.
The stroma is scanty but highly vascular.

6 October 2010 32
Metastasis:Characteristics: Its tendency to
metastasize before Clinical Sign/Symptom.
Common site of Metastasis: Lung- 50% Bone- 33% Regional Lymph nodes, Liver, Adrenals
and Brain.

6 October 2010 33
TreatmentSurgery is the standard treatment for
contained kidney cancer. Various surgical options may be available to you, depending on tumor size and location within the kidney capsule. Such surgery is performed by a urologic surgeon.
Radiation and chemotherapy are not very effective in treating kidney cancer. Biologic therapies are used more frequently.

6 October 2010 34
Urothelial Carcinoma of the Renal Pelvis:Benign papillomas, Invasive TCC.
Urolethelial tumors may be multiple involving
the pelvis, ureter and bladder. They may block the urinary out flow and
lead to hydronephrosis and flank pain.
5 year survival rate.

6 October 2010 35
Clear Cell CarcinomaContrast-enhanced CT
image during renal parenchymal phase shows a right renal mass with a mixed enhancement pattern containing enhancing solid soft tissue and low-attenuation areas that may represent cystic or necrotic changes.
Contrast-enhanced CT image during renal parenchymal phase shows a left renal mass with a mixed enhancement pattern with a greater amount of solid components

6 October 2010 36
OncocytomaOncocytomas may overlap, however, with clear cell RCC in terms of imaging features and degree of enhancement.
On CT scans, the diagnosis of oncocytoma may be suggested if a central stellate scar is identified within an otherwise homogeneous tumor.

6 October 2010 37
Oncocytoma58-year-old man
with left renal oncocytoma. Contrast-enhanced CT image during renal parenchymal phase shows a left renal mass with nearly homogeneous enhancement and a small low-attenuation central scar.

6 October 2010 38
Solid Renal Tumors- Papillary RCCPapillary RCCs are typically
less vascular compared with most other types of renal tumors and most commonly manifested as homogeneous or peripheral enhancement.
A58-year-old man with a 15-cm papillary RCC arising from the right kidney. Contrast-enhanced CT image during renal parenchymal phase shows a right renal mass with mild enhancementof 35 HU in peripherally distributed soft tissue. No enhancement is identified in the central low-attenuation region.

6 October 2010 39
Cystic Renal Cell Tumors(A)A 68-year-old woman
with breast cancer. T2-weighted FSE MRimage shows a complex cystic mass in the left kidney, which was proved to be a multilocular cystic nephroma on pathology.
(B) A 52-year-old woman with multilocular cystic RCC in the left kidney. Contrast-enhanced CT image at renal parenchymal phase shows a cystic mass containing several thickened enhancing septations in the left kidney

6 October 2010 40
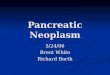
77-year-old woman with a malignant left renal cortical tumor showing venous invasion.
(A) Axial fat-suppressed T1-weighted image shows a left renal mass (short arrow) with tumor thrombus extending into the left renal vein (long arrow).
(B and C) Axial and coronal T2-weighted single-shot fast spin-echo sequences show marked expansion of the inferior vena cava from tumor thrombus (arrows).

6 October 2010 41
Thank you very much for kindattention!