Embed Size (px)
Citation preview

Neurological EmergenciesGuest Editors: Joseph R. Shiber, Chamisa Macindoe, Oliver Flower, William A. Knight IV, and Julian Bösel
Emergency Medicine International

Neurological Emergencies

Emergency Medicine International
Neurological Emergencies
Guest Editors: Joseph R. Shiber, Chamisa Macindoe,Oliver Flower, William A. Knight IV, and Julian Bosel

Copyright © 2012 Hindawi Publishing Corporation. All rights reserved.
This is a special issue published in “Emergency Medicine International.” All articles are open access articles distributed under the CreativeCommons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the originalwork is properly cited.

Editorial Board
Marc Afilalo, CanadaPraveen Aggarwal, IndiaJeffrey R. Avner, USAGuttorm Brattebø, NorwayF. Burkle, USAWen-Jone Chen, TaiwanChee-Fah Chong, TaiwanRobert W. Derlet, USATheodore J. Gaeta, USAMassimo Gallerani, Italy
Stephen W. Hargarten, USAChak W. Kam, Hong KongNiranjan Kissoon, CanadaChristian K. Lackner, GermanyPhilippe E. R. Lheureux, BelgiumWalter Mauritz, AustriaOscar Miro, SpainSeiji Morita, JapanLewis S. Nelson, USAJoe Nemeth, Canada
Edward A. Panacek, USAE. P. Rivers, USAMiquel Sanchez, SpainHarold K. Simon, USAMarco L. A. Sivilotti, CanadaSelim Suner, USARade B. Vukmir, USATzong-Luen Wang, Taiwan

Contents
Neurological Emergencies, Joseph R. Shiber, Chamisa Macindoe, Oliver Flower, William A. Knight IV,and Julian BoselVolume 2012, Article ID 208193, 1 page
Sedation in Traumatic Brain Injury, Oliver Flower and Simon HellingsVolume 2012, Article ID 637171, 11 pages
Diagnosis and Management of Bacterial Meningitis in the Paediatric Population: A Review,Catherine L. Tacon and Oliver FlowerVolume 2012, Article ID 320309, 8 pages
Prehospital Medication Administration: A Randomised Study Comparing Intranasal and IntravenousRoutes, Cian McDermott and Niamh C. CollinsVolume 2012, Article ID 476161, 5 pages
Avoiding Misdiagnosis in Patients with Neurological Emergencies,Jennifer V. Pope and Jonathan A. EdlowVolume 2012, Article ID 949275, 10 pages
Reversible Cerebral Vasoconstriction Syndrome: An Important Cause of Acute Severe Headache,Li Huey Tan and Oliver FlowerVolume 2012, Article ID 303152, 8 pages

Hindawi Publishing CorporationEmergency Medicine InternationalVolume 2012, Article ID 208193, 1 pagedoi:10.1155/2012/208193
Editorial
Neurological Emergencies
Joseph R. Shiber,1 Chamisa Macindoe,2 Oliver Flower,3
William A. Knight IV,4 and Julian Bosel5
1 Departments of Emergency Medicine and Critical Care College of Medicine, University of Florida, Jacksonville, FL 32209, USA2 Departments of Emergency Medicine and Surgery, University of New Mexico, Albuquerque, NM 87131, USA3 Department of Intensive Care Medicine, E25—Royal North Shore Hospital, The University of Sydney, Sydney, NSW 2006, Australia4 Departments of Emergency Medicine and Neurosurgery, University of Cincinnati, Cincinnati, OH 45267-0769, USA5 Neurological Clinic, University of Heidelberg, Im Neuenheimer Feld 400, 69120 Heidelberg, Germany
Correspondence should be addressed to Joseph R. Shiber, [email protected]
Received 6 September 2012; Accepted 6 September 2012
Copyright © 2012 Joseph R. Shiber et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Emergency departments (EDs) are the typical initial contactfor seriously ill and injured patients. Although diverse andsometimes subtle in presentation, acute neurological diseaseshave an urgency that makes their rapid diagnosis andtreatment crucial for improving outcomes. These patientsmay need to go to the intensive care unit, the interventionalradiology suite, or the operating room and may requirevarious consulting services but all of their care begins withthe emergency physician (EP). It is therefore vital that EPshave expertise in recognizing these disorders and rapidlyinitiating appropriate treatments.
Investigators and clinicians from around the worldsubmitted manuscripts for consideration in this special issuefocusing on neurological emergencies. We are pleased topresent this special issue in order to stimulate internationaldialogue and advance efforts for improving the diagnosis,close monitoring, and initial treatment of these potentiallydevastating disorders.
This special issue includes a significant article by Dr.L. H. Tan and Dr. O. Flower from Royal North ShoreHospital, Australia on “Reversible cerebral vasoconstrictionsyndrome: An important cause of acute severe headache” theauthors describe the epidemiology, pathophysiology, clinicaland diagnostic features, and a summary of the treatmentsof this under-recognized syndrome. Dr. C. Tacon fromSydney Children’s Hospital, Australia and Dr. O. Flowerpresent an excellent review on “Diagnosis and management ofbacterial meningitis in the paediatric population” it discussesthe changing epidemiology due to new childhood vaccines,
current laboratory testing, and clinical tools that can aid indiagnosing bacterial meningitis, as well as the controversiesand advances in patient management. Dr. C. McDermottand Dr. N. Collins from University College Dublin, Irelandoffer a noteworthy research article “Prehospital medicationadministration: A randomised study comparing intranasaland intravenous routes” the authors investigate the safetyand effectiveness of intranasal naloxone administration byparamedic trainees. An indispensable review on “Sedationin traumatic brain injury” by Dr. O. Flower and Dr. S.Hellings from Royal North Shore Hospital, Australia presentsand compares the medication choices using evidence-basedsupport for recommendations on the optimal clinical contextfor the use of each agent. Lastly, Dr. J. V. Pope and Dr. J.A. Edlow from Harvard Medical School, USA present anoutstanding article “Avoiding misdiagnosis in patients withneurologic emergencies” this valuable paper is intended toassist EPs and other healthcare providers in understandinghow diagnostic errors occur in order to make an accuratediagnosis and improve patient care for the common present-ing complaints of headache, dizziness, back pain, weakness,and seizure.
Joseph R. ShiberChamisa Macindoe
Oliver FlowerWilliam A. Knight IV
Julian Bosel

Hindawi Publishing CorporationEmergency Medicine InternationalVolume 2012, Article ID 637171, 11 pagesdoi:10.1155/2012/637171
Review Article
Sedation in Traumatic Brain Injury
Oliver Flower1, 2 and Simon Hellings2
1 University of Sydney, Sydney, NSW, Australia2 Department of Intensive Care, Royal North Shore Hospital, Sydney, NSW 2065, Australia
Correspondence should be addressed to Simon Hellings, [email protected]
Received 8 March 2012; Revised 16 May 2012; Accepted 22 June 2012
Academic Editor: William A. Knight IV
Copyright © 2012 O. Flower and S. Hellings. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Several different classes of sedative agents are used in the management of patients with traumatic brain injury (TBI). These agentsare used at induction of anaesthesia, to maintain sedation, to reduce elevated intracranial pressure, to terminate seizure activityand facilitate ventilation. The intent of their use is to prevent secondary brain injury by facilitating and optimising ventilation,reducing cerebral metabolic rate and reducing intracranial pressure. There is limited evidence available as to the best choice ofsedative agents in TBI, with each agent having specific advantages and disadvantages. This review discusses these agents and offersevidence-based guidance as to the appropriate context in which each agent may be used. Propofol, benzodiazepines, narcotics,barbiturates, etomidate, ketamine, and dexmedetomidine are reviewed and compared.
1. Introduction
Several different classes of drugs are used as sedatives inpatients with traumatic brain injury (TBI). Several of theseagents may also have other uses, for example as anticonvul-sants or analgesics. Whilst none are perfect, they all havepotential roles in managing a condition that is a major causeof disability, death, and economic cost to society. This paperdiscusses and compares these agents and offers evidence-based guidance as to the appropriate context in which eachagent may be used.
It is important to delineate the contexts in which sedativeagents are used in the setting of TBI and what is considereda sedative. For the purposes of this paper, sedative agentsare considered to be drugs that decrease consciousness andhave therapeutic applications in the management of TBI.After primary brain injury, airway protection and controlof ventilation are often required. Induction sedative agents(distinct from muscle relaxants) are used to safely facilitateendotracheal intubation in a manner that minimises haemo-dynamic instability and secondary brain injury. Maintenanceof sedation is then employed as part of the overall manage-ment of TBI to permit manipulation of ventilation, optimi-sation of cerebral metabolic rate (CMRO2), cerebral blood
flow (CBF), and intracranial pressure (ICP). See Table 1for abbreviations with explanations. In TBI confounded byalcohol or illicit drug intoxication, sedative agents facilitatesafe management whilst these confounding drugs wear off.For refractory, elevated ICP in severe TBI, sedative agentsplay a key role in the escalating tiers of therapy to reduceICP. Sedative hypnotics are also employed in seizure controlfor refractory acute posttraumatic epilepsy. As with allventilated patients, sedatives act as anxiolytics whilst patientsare mechanically ventilated [1].
The primary injury of TBI causes diffuse axonal injury,cerebral oedema, intracranial haematoma, elevated ICP,reduced cerebral perfusion pressure (CPP), and cerebralischaemia. Therapeutic efforts focus on reducing the sec-ondary insults of hypoxia, hypercapnea, systemic hypoten-sion and intracranial hypertension. Sedatives address theseissues in several ways. They allow optimisation of ventilationto prevent hypoxia and achieve normocapnea (and hypocap-nea for brief episodes of elevated ICP); they reduce CMRO2
and therefore CBF and cerebral blood volume (CBV) andreduce ICP. However they may reduce systemic bloodpressure, thereby reducing CPP, and have other adverseeffects. Even a single episode of hypotension is a powerfulpredictor of outcome following TBI [2, 3].

2 Emergency Medicine International
Table 1
Abbreviations and explanations
(i) AMPA: α-amino-3-hydroxy-5-methyl-4-isoxazolepropionicacid, GABA: γ-Aminobutyric acid(ii) EEG: Electroencephalogram(iii) CMRO2: Cerebral Metabolic Rate of Oxygen(iv) CPP: Cerebral Perfusion Pressure(v) ICP: Intracranial Pressure(vi) IV: Intravenous(vii) MAP: Mean Arterial Pressure(viii) t1/2: Half-life(ix) Context sensitive t1/2: the time taken for blood plasmaconcentration of a drug to decline by one half after an infusiondesigned to maintain a steady state (i.e., a constant plasmaconcentration) has been stopped. The “context” is the durationof infusion [5].
There is limited evidence available to guide the choiceof specific sedative agents in TBI. A recent systematic reviewexamining a range of outcomes in TBI concluded that therewas no convincing evidence that any one of the sedativeagent was superior to another [4]. A number of these studiesincluded patients with less severe traumatic brain injuriesand spanned several decades, further limiting conclusionsthat can be made. Multiple sedative agents are often usedsynchronously, clouding assessment of individual agents.The guidelines from the Brain Trauma Foundation alsohighlight a lack of high quality evidence to recommend onesedative agent over another, with the exception of barbiturateuse for refractory elevated ICP. Despite this, each agent hasa potential role in TBI and clinicians must consider theadvantages and disadvantages when deciding what to use ineach context.
2. Propofol
See Table 2. Propofol is a phenol derivative with high lipidsolubility and a rapid onset of action. It has a very low solu-bility in water so is formulated as an emulsion in soya beanoil, glycerol, and egg phosphatide. A relatively rapid plasmaclearance ensures a reliable recovery of consciousness evenafter prolonged administration, thereby facilitating neuro-logical examination. However, the context-sensitive half timedoes increase with prolonged infusions, though to a muchlesser extent than seen with many other sedatives.
Since its introduction in 1986, propofol has increasinglybeen used both as an induction agent and as a maintenancesedative in the neurointensive care unit. Several studies havedemonstrated the favourable cerebral effects of propofol.ICP, CBF, and CMRO2, have all been shown to be reducedwith propofol [8, 9]. However, a fall in mean arterial bloodpressure (MAP) may reduce the CPP if this is not mitigatedwith adequate fluid resuscitation and vasopressors. Whencomparing propofol sedation with midazolam in medicaland surgical ICU patients, propofol has been associatedwith improved quality of sedation and a faster recovery ofconsciousness on discontinuation of sedation [10].
Table 2
Propofol
Group Phenol Derivative
Mechanism ofAction/Pharmakodynamics
Potentiation GABAA receptorsNa+ channel blocker
Neuroprotective effects
Reduces CBF, CMRO2 and ICPReduces MAP, therefore variableeffect on CPPIncreases seizure threshold
Pharmacokinetics
Rapid hepatic metabolised, withextra-hepatic metabolismt1/2 2–24 hours, but rapid peripheraldistributionShort context sensitive t1/2
Advantages
Favourable effects on CBF,CMRO2 and ICPRapid onset of actionRelatively short context sensitive t1/2facilitating neurological assessment
Disadvantages and majorside effects
Hypotension may worsen CPPHigh lipid loadAssociated with elevated liverenzymes & pancreatitisPotential for PRIS, particularly withprolonged, high dose infusionsFormulation may support bacterialand fungal growthContraindicated if allergic to egg orsoybeans
Dosage
Induction: 1–2.5 mg/kg,0.5–1.5 mg/kg in elderly or limitedcardiovascular reserveMaintenance of sedation:1.5–4.5 mg/kg/hour, titrated todesired effect
Other significant factsIncreased risk of PRIS at infusions>4 mg/kg/h for >48 h
Appropriate roles in TBI
Induction agent, caution inhypotensionContinuous infusion to providesedation in TBIRefractory elevated ICPRefractory seizures
There is increasing awareness in the literature of thecentral role of mitochondrial dysfunction and cerebral celldeath in areas of the brain with high oxidative stress [11,12]. Propofol may act as a neuroprotective agent throughlimitation of oxidative stress. An RCT employing cerebralmicrodialysis catheters compared sedation with midazolamand propofol, using several cerebral biomarkers as endpointsin the acute phase of TBI [13]. No difference was foundbetween the two groups over a 72-hour period in the lactateto pyruvate ratio, a marker of cerebral oxidative stress.This was a relatively small study and the concentrations ofpropofol used may not have been sufficient to produce anantioxidant effect nevertheless this is an interesting and novelarea of future research.

Emergency Medicine International 3
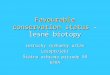
Figure 1: Brugada-like ECG changes that may be seen in propofolinfusion syndrome. Coved ST elevation, at least 2 mm J pointelevation and descending ST segment followed by a negative T wave(see [67]).
Aside from a reduction in MAP and the need forincreased vasopressor requirements to preserve CPP, thelipid formulation of propofol may be associated with otheradverse effects. Propofol infusion syndrome (PRIS) was ini-tially described in case studies of children who were sedatedwith propofol infusions. Subsequently it has been reported inadults, both with long-term infusions in ICU patients and inthe short term when used as a general anaesthetic. Clinicallypatients may present with a variety of findings includinglactic acidosis, cardiac dysfunction, and Brugada-like elec-trocardiogram changes (see Figure 1), which may heraldimminent malignant arrhythmias [14]. This can progressto rhabdomyolysis, renal failure, and cardiovascular collapse.The pathophysiology of PRIS is incompletely understoodand involves multiple different pathways. An underlyingimbalance between energy utilization and demand at themitochondrial level and effects on lipid metabolism arepostulated mechanisms.
Importantly, it is thought that PRIS is more common inpatients with TBI. In one retrospective cohort study of adultneurosurgical patients in ICU, 7 of 67 patients displayedsigns of PRIS and died. There was an increased incidence ofPRIS with higher doses [15]. PRIS may be more common in
TBI because large doses of propofol can be used to controlelevated ICP [16]. It has been argued that PRIS may limit theusefulness of propofol as a sedative agent in traumatic braininjury, particularly when used in higher doses.
Other potential complications associated with the useof propofol include an elevation in pancreatic enzymesand pancreatitis [17]. Concerns have also been raised thatpropofol offers a good medium for microbial growth [18],although this may be less significant with newer formula-tions. Propofol has a significant calorific content, and thisshould be taken into account when performing nutritionalassessments.
Initial reports suggested that propofol may increaseseizure activity in susceptible patients [19]. The extent towhich this activity represented disordered muscle tone ortrue seizure activity is unclear [20]. Conversely, propofol hasalso been demonstrated to increase seizure threshold and hasbeen successfully used in the treatment of status epilepticus.Much of the evidence for the use of propofol in refractorystatus epilepticus is derived from case series that demon-strated cessation of seizure activity with infusions of propofol[21]. Propofol has been demonstrated to achieve and main-tain burst suppression, although at the expense of significantdecreases in mean arterial pressure and cardiac index [22].
Therefore, propofol is indicated as a sedative agent inTBI. It has the advantage of a relatively quick onset and offsetof action facilitating neurological assessment. Cliniciansshould be mindful of the risk of PRIS, particularly whenusing >4 mg/kg/hour for >48 hours [23]. As an inductionagent it may cause a fall in MAP and thus CPP, and thisshould be mitigated through the judicious use of vasopres-sors and fluid boluses. Propofol may be indicated in thetreatment of refractory status epilepticus. Its use as an agentto achieve burst suppression may come at the expense ofworsening haemodynamics.
3. Benzodiazepines
See Table 3. Benzodiazepines are commonly used as sedativeagents in patients with TBI. They are nonselective CNSdepressants that augment the action of GABA at GABAA
receptors, causing increased conductance of chloride ions.They have anxiolytic, amnesic, and anticonvulsant proper-ties. Prior to the advent of propofol, midazolam was themost frequently used sedative in TBI in the UK [24], withlorazepam frequently being used in the US [25]. Midazolamoffers the most benefits of the benzodiazepines for sedationin TBI, due to its shorter context sensitive t1/2 (2–2.5 hours)and faster onset and offset of action, compared to lorazepam(t1/2 10–20 h) or diazepam (t1/2 20–40 hours) [26]. It has arapid onset as a result of high lipid solubility at physiologicalpH due to the closure of the imidazole ring. Its rapid hepaticmetabolism accounts for its rapid offset of action [27]however some metabolites are active and accumulate withprolonged infusions. This may result in continued sedationeven after drug cessation, particularly in the elderly or withliver impairment.
Whilst benzodiazepines reduce CBF, CMRO2, and ICPand increase seizure threshold, there is evidence that bolus

4 Emergency Medicine International
Table 3
Midazolam
Group Imadobenzodiazepine
Mechanism ofAction/Pharmakodynamics
GABAA receptor agonistChloride channel activation,Kappa opioid agonist
Neuroprotective effects
Reduces CBF, CMRO2 and ICP butminimal effect beyond that ofsedationReduces MAP, variable effect on CPPRaises seizure threshold
Pharmacokinetics
Onset of action 2–4 minutes94% protein boundHighly lipid solubleHepatic metabolismRenal excretion (some bile)Short context sensitive t1/2 (2.4 h)
Advantages
Shorter t1/2 than otherbenzodiazepinesCauses less hypotension thanbarbiturates or propofol
Disadvantages and majorside effects
Metabolites accumulate delayingneurological assessment postcessation of infusionBoluses in TBI reduce MAP (andCPP)Withdrawal syndromeDeliriumRespiratory and cough reflexsuppressionTachyphylaxis after 72 hoursPlateau effect on reducing ICP, whereincreasing doses have no effect
DosageInduction: 0.1 mg/kgMaintenance of sedation:0.01–0.2 mg/kg/hour
Other significant facts
Interaction with peripheralbenzodiazepine leucocyte receptorsso may have immunosuppressanteffect
Appropriate roles in TBI
Induction of anaesthesiaMaintenance of sedation inhypotensive patients with TBIMaintenance of sedation whenimminent neurological assessmentnot requiredTreatment of seizures
doses significantly reduce MAP and CPP in severe TBI [28].The depth of CMRO2 reduction possible with benzodi-azepines is not as profound as barbiturates or etomidate, andburst suppression cannot be achieved [29].
Other disadvantages include significant respiratorydepression and inhibition of the cough reflex, limiting itsuse in non-intubated patients. After prolonged sedation withbenzodiazepines, tolerance develops, and on cessation, with-drawal symptoms including tremors, seizures, hypertension,and insomnia may occur, requiring ongoing longer actingbenzodiazepines to be prescribed [30]. Benzodiazepines are
a risk factor for ICU delirium [31], which is independentlyassociated with poor outcomes [32].
There have been several studies comparing the safetyand efficacy of benzodiazepines with other commonly usedagents. In one RCT, 63 trauma patients, the majority withsevere TBI, were randomised to receive either midazolamor 2% propofol infusions. Patients in both groups receivedmorphine for analgesia. No significant difference in ICP orin wake-up time was demonstrated between the two groups.Similarly no significant differences were seen in haemody-namic variables between the two groups. Interestingly, therewas a higher incidence of therapeutic failure in the propofolgroup either because of inadequate sedation or hypertriglyc-eridemia [33]. Other smaller, underpowered studies havealso failed to demonstrate a difference in outcomes betweenthese two agents [34].
Therefore benzodiazepines have a role in the sedationof patients where imminent neurological assessment isnot required. They have significant disadvantages includingan accumulation of metabolites, increasing tolerance withprolonged infusions, and an increased likelihood of delirium.
4. Narcotics
See Table 4. Opioid narcotics primarily have analgesic prop-erties, and their sedative action may even be considered aside effect. However, various opioids are used in the sedationof patients with TBI, usually in combination with hypnoticagents to ensure analgesia and reduce hypnotic dose require-ments. Analgesia-based protocols are feasible, with certainadvantages over hypnotic (propofol and midazolam) seda-tive regimens [35]. Intravenous opioids used include mor-phine, fentanyl, sufentanil, and more recently remifentanil.
Opiates act on μ1 receptors (supraspinal analgesia),μ2 receptors (ventilatory depression, bradycardia, physicaladdiction), κ receptors (sedation, spinal analgesia), ε recep-tors (dysphoria, hallucinations, respiratory stimulation),and Δ receptors (analgesia, behavioural effects, and epilep-togenic). The different opioids have variable effects on eachreceptor [26]. Opioids can produce hypotension by a numberof mechanisms including a reduction in sympathetic toneand the stimulation of histamine release. This hypotensionmay be detrimental in patients with TBI in whom mainte-nance of cerebral perfusion pressure is vital.
Prior to the advent of newer agents morphine has beenmost commonly used as a narcotic in TBI. However, pro-longed use of opioids such as morphine can lead to redis-tribution and accumulation, with potentially unpredictabledelays in awakening. The t1/2 of morphine is increased inrenal failure, as a proportion of both the parent drug andan active metabolite, morphine-6-glucuronide, are excretedrenally [36]. In addition, tachyphylaxis can lead to increasingdose requirements with subsequent withdrawal phenomenaand a possible rebound increase in ICP on cessation.
Shorter acting opioids include fentanyl, alfentanil, sufen-tanil, and remifentanil. These are more lipid soluble thanmorphine and so have a faster onset of action [37]. Metab-olism to inactive metabolites leads to less accumulation inrenal failure. Nevertheless, with prolonged infusion shorter

Emergency Medicine International 5
Table 4
Morphine Fentanyl Alfentanil Sufentanil Remifentanil
Pharmacodynamics μ1, μ2, κ and Δ agonists
Elimination t1/2 (h) 3 3.7 1.5 2.2 0.25
Distribution t1/2 3–11 min 10–30 min 15 min 5 min 1 min
Neuroprotective effects May increase ICP Minimal effect beyond the analgesic effect on CBF and CMRO2
Pharmacokinetics
Onset 6 minPeak effect 20 min(IV)30% protein boundHepaticallymetabolised to activemetabolitesRenal clearance
95% protein boundHigh lipid solubility75% first passpulmonary uptakeHepaticallymetabolised to activemetabolitesRenal clearance
OnsetPeak 90 sDuration 5–10 min90% protein boundHepaticallymetabolisedRenal clearance
HepaticallymetabolisedRenal clearance
Peak 60 sSmall VdRapid clearanceRapid esterhydrolysis byplasma esterasesto inactivemetabolite(Independent ofrenal & hepaticfunction)
Advantages
Lower costRelativehaemodynamicstabilityHypnotic agentsparingAnalgesic properties
Lower costRelativehaemodynamicstabilityHypnotic agentsparingAnalgesic properties
RelativehaemodynamicstabilityHypnotic agentsparingAnalgesic properties
RelativehaemodynamicstabilityHypnotic agentsparingAnalgesic properties
Very rapidonset/offsetLess nauseaRelativehaemodynamicstabilityHypnotic agentsparingAnalgesicproperties
Disadvantages and majorside effects
HypotensionBradycardiaRespiratorydepressionCough reflexsuppressionSeizuresRigidityConstipationSpasm sphincter ofOddiNauseaPruritis
Dosage 0.05–0.1 mg/kg/hr
Induction:1–3 mcg/kgMaintenance:0.5–2 mcg/kg/h
Induction:10–50 mcg/kgInfusion:0.5–1 mcg/kg/min
Induction: 4 mcg/kgBolus: 1 mcg/kgInfusion: 0.0125–1 mcg/kg/min
Appropriate uses in TBILong term analgesiaPalliation
Co-Induction agentContinuous infusionPalliation
Co-Induction agent Co-Induction agent
Co-InductionagentContinuousinfusioninfusion
acting opioids can accumulate and impede neurologicalassessment. For example, with an increasing duration offentanyl infusion, saturation of inactive tissue sites and areturn of opioid from peripheral compartments mean thatthere is a prolonged context-sensitive half time relative tosufentanil.
Studies of the effects of opioids on ICP have beeninconsistent. However, there is evidence that the adminis-tration of high bolus doses of opioids may have potentially
deleterious effects in TBI, with some studies showing anincrease in ICP and a fall in CPP. These effects occurreddespite controlling PaCO2. Interestingly, in those studiesthat prevented hypotension, an increase in ICP was notseen. It is suggested that hypotension may increase ICP anddecrease CPP through cerebral autoregulatory reflexes [9]. Itis unclear to what extent opioids may induce seizure activity.Whilst there are numerous case reports of clinical seizureactivity, it has been argued that many of these represent

6 Emergency Medicine International
muscle rigidity associated with high doses of opioid ratherthan seizure activity per se [38].
There has been increased interest in remifentanil as analternative opioid sedative in TBI. Remifentanil is a potent,synthetic opioid receptor agonist, which differs from othersynthetic opioids in that it undergoes rapid hydrolysis bytissue and plasma esterases. This rapid metabolism and lackof accumulation facilitate faster waking and neurologicalassessment of patients with TBI [39]. An RCT on neuro-intensive care patients showed analgesia-based sedation withremifentanil offered faster and more predictable time toassessment of neurological function than a hypnotic-basedtechnique (propofol or midazolam) [40]. Furthermore,remifentanil was well tolerated in patients with TBI, witha significantly shorter time to extubation in patients whohad received remifentanil compared with patients who hadreceived morphine [11].
Opioids have a role as an adjunct to other sedativeagents, for example in combination with propofol. They mayreduce sedative requirements of other agents and provideeffective analgesia and anxiolysis. Prolonged infusions ofopioids, particularly morphine, may accumulate and hinderneurological assessment. When opioids are administered as abolus, there is a risk of increasing the ICP, particularly whenthe MAP is allowed to fall.
5. Barbiturates
See Table 5. Barbiturates, particularly pentobarbital andthiopentone, have previously played a central role in thesedation of patients with TBI [41]. However, with theadvent of newer agents with less disadvantages, thiopentoneis largely confined to use as an induction agent, for thetreatment of refractory elevated ICP and for status epilep-ticus. Barbiturates stimulate γ-aminobutyric acid (GABA)receptors and inhibit α-amino-3-hydroxy-5-methyl-4-isoxa-zolepropionic acid (AMPA) receptors in the CNS producingdose-dependent sedation and general anaesthesia.
High lipid solubility allows rapid transfer across theblood-brain barrier and exceptionally fast onset of action.The induction of anaesthesia sufficient for intubation withinone arm-brain circulation time initially popularized the useof thiopentone as an induction agent in rapid-sequenceintubation (RSI) [42]. The hypotensive effects caused bydirect myocardial and central vasomotor depression shouldbe anticipated and addressed by using only low dosesand coadministering vasopressors such as metaraminol orphenylephrine if the blood pressure is suboptimal before RSI.
A recent Cochrane review concluded that barbituratesare not indicted as a maintenance sedative agent or foruse prophylactically to prevent elevations in ICP [43], pre-dominantly because the hypotension and other side effectsoffset any ICP lowering effect on CPP.
Significant accumulation will occur with repeated dosesor infusions due to the long context-sensitive t1/2 and theelimination kinetics changing from 1st to zero order atplasma levels >30 mg/L. To treat refractory elevated ICPor refractory status epilepticus, a clinical endpoint of burstsuppression on EEG is targeted, which requires plasma levels
Table 5
Thiopentone
Group Barbiturate
Mechanism ofAction/Pharmacodynamics
Stimulate GABA receptorsInhibit AMPA receptors
Neuroprotective effects
Reduces CBF, CMRO2 and ICPReduces MAP, therefore variableeffect on CPP Raises seizurethreshold
Pharmacokinetics [6]
Hepatically metabolised0.5% renal excretion unchangedElimination t1/2 11.6 hFirst to zero order kinetics if plasmahighSignificant accumulation
Advantages
Rapid onset of action as inductionagentFavourable effects on CBF,CMRO2 and ICPInexpensive
Disadvantages and majorside effects
Accumulation with prolongedinfusionHypotensionGastroparesisLoss of thermoregulationImmunosuppressionHypokalaemia during infusionHyperkalaemia on emergenceLife threatening arrhythmias oncoma emergence
Dosage
Induction of anaesthesia: 2–5 mg/kgEEG burst suppression: 40 mg/kgfollowed by infusion at 4–8 mg/kg/h,titrated to EEG
Other significant factsMay precipitate if given concurrentlywith IV muscle relaxants [7]
Appropriate uses in TBI
Induction of anaesthesia, withcaution regarding hypotensionRefractory elevated ICPRefractory status epilepticus
>40 mg/L. Unfortunately, the high doses of thiopentonerequired to achieve this preclude neurological assessment forseveral days.
Therefore thiopentone may be used as an inductionagent in TBI if hypotension is not already problematic andprecautions are taken. It has a role in treatment of refractoryelevated ICP and refractory status epilepticus, but not as amaintenance sedative in TBI.
6. Etomidate
See Table 6. Etomidate is a carboxylated imidazole derivativepredominantly used as an intravenous induction agent in thesetting of haemodynamic instability. It causes less hypoten-sion and cardiovascular depression than other sedatives inthis context [44], with the exception of ketamine. Otheradvantages include a rapid onset of anaesthesia (10s) lasting

Emergency Medicine International 7
Table 6
Etomidate
Group Caroboxylated imidazole derivative
Mechanism ofAction/Pharmakodynamics
GABAA receptor agonist
Neuroprotective effectsReduces CBF, CMRO2 and ICPMaintains or increases CPPLowers seizure threshold
Pharmacokinetics
75% protein boundHighly lipid solubleHigh volume of distribution, threecompartment modelHepatic metabolismRenal excretion (some bile)Short context sensitive t1/2 (4.8 h)
Advantages
Rapid onset of action as inductionagentOnly lasts 3–5 minutes after singlebolusFavourable effects on CBF, CMRO2
and ICP
Disadvantages and majorside effects
Adrenal suppressionMetabolic acidosis from propyleneglycol vehiclePain on injectionMyoclonic movementsNausea and vomiting
Dosage Induction: 0.2–0.4 mg/kg
Other significant factsOriginally developed as ananti-fungal agent
Appropriate uses in TBIInduction of anaesthesia, withcaution regarding adrenalsuppression
3–5 minutes following a dose of 0.3 mg/kg, and a shortelimination t1/2 of 2.6 h [45]. There is a reduction in CBF andICP [46] and it can even achieve burst suppression on EEG[47].
However, the safety of etomidate has been questioned.Continuous infusions have been shown in a retrospectivestudy to cause a significant increase in mortality [48].Etomidate causes adrenal suppression by suppressing corti-costeroid synthesis through the inhibition of the enzyme 11-β-hydroxylase, which converts 11-deoxycortisol to cortisol.This effect has been demonstrated with both infusions andwith a single bolus. A single dose of etomidate reducesthe synthesis of cortisol and aldosterone and increases therisk of relative adrenocortical insufficiency (RAI) for at least24 hours [49]. Hypotension related to RAI has implicationsfor CPP and neurological outcome. Etomidate may alsolower seizure threshold [50]. Other adverse effects includepain on injection, myoclonic movements, and nausea andvomiting [51].
Therefore etomidate should be avoided as a continuoussedative agent in TBI but may be considered with cautionas an induction agent, although ketamine offers many of thesame advantages without the risks of adrenal suppression.
Table 7
Ketamine
Group Phencyclidine derivative
Mechanism ofAction/Pharmacodynamics
Competitive NMDA receptorantagonistInteraction with opioid andmuscarinic receptorsNa+ Channel
Effect on ICP None or decrease
Neuroprotective effects Decreased glutamate
Pharmacokinetics
20% Bioavailability40% protein boundDistribution t1/2 10 minutesHepatic metabolismElimination t1/2 2.5 h
Advantages Preserves MAP and CPP
Disadvantages and majorside effects
Early studies ↑ICP, ?epileptogenicHallucinations/Emergencephenomena
DosageInduction: 2 mg/kgMaintenance: 50 mcg/kg/min
Other significant facts
Appropriate uses in TBI Haemodynamic instability
7. Ketamine
See Table 7. Ketamine is an N-methyl-D-aspartate receptorantagonist. It has traditionally been avoided in the manage-ment of patients with traumatic brain injury owing to con-cerns that it may increase intracranial pressure. Furthermore,there are theoretical concerns regarding its epileptogenicpotential. Indeed, it receives little attention in guidelines forthe management of TBI [1]. Conversely, it has been arguedthat in comparison to most widely used sedative agentsketamine does not decrease blood pressure and therefore maypreserve cerebral perfusion pressure. In particular, it has beenargued that this haemodynamic stability enables ketamine tobe used as a safe induction agent in patients with TBI [52].
Concerns regarding the potential for ketamine to raiseICP stem from small case control series several decades agoin patients with abnormal CSF flow dynamics [53]. A risein ICP was observed in spontaneously breathing patients,undergoing diagnostic pneumoventriculography, in whomketamine was administered to. However, this rise in ICP onlyoccurred in those patients with abnormal CSF pathways. Inthe remaining patients there was an overall rise in MAP,an increase in cerebral blood flow, and improved cerebralperfusion pressure [54, 55].
Several recent studies have refuted the original find-ings and showed no statistically significant rise in ICP inbrain injured patients who are sedated with ketamine [56].Bourgoin et al. randomised patients with TBI to receiveeither sufentanyl-midazolam or ketamine-midazolam seda-tion using target controlled infusions. The target con-centrations of sufentanil and ketamine were doubled for15 minutes, and the plasma concentrations of both weremeasured. There was no significant change in ICP or CPP

8 Emergency Medicine International
Table 8
Dexmedetomidine
Group Selective α2 adrenergic agonist
Mechanism ofAction/Pharmacodynamics
Peripheral α2A, brain & spinal cordα2B, α2C adrenoreceptor subtypes
Neuroprotective effects Reduces CBF and ICP
PharmacokineticsHepatic metabolismDistribution t1/2 6 minutesElimination t1/2 2 hours
AdvantagesMinimal respiratory depressionReduction in delerium
Disadvantages and majorside effects
Hypotension (28%)BradycardiaArrhythmias including atrialfibrillationRelatively high cost
DosageLoading dose: 1 mcg/kgInfusion: 0.42–1.0 mcg/kg/hour
Other significant factsMinimal effect on respiratoryfunction
Appropriate uses in TBIMaintenance sedation agent pre &post extubationManagement of agitated delirium
with increased plasma concentrations. In an interesting edi-torial, the possibility that cerebral haemodynamics are betterpreserved through the use of target controlled infusion wasdiscussed [57]. Whilst bolus doses of some commonly usedsedatives may adversely affect haemodynamics and increaseICP, it is argued that a system relying on pharmacokineticmodels alone is insufficient in managing patients with TBI.
Another study looked at the use of ketamine in 30 sedatedand ventilated children with TBI and raised ICP resistantto first-tier therapies [58]. Variables examined included ICP,hemodynamic variables, and CPP. Ketamine was admin-istered as a single dose of 1–1.5 mg/kg either to preventfurther ICP increases during distressing procedures or asan additional measure to lower ICP. There was an overalldecrease in ICP and increase in CPP in both situations. Theauthors conclude that ketamine is a safe and effective sedativeagent to use in patients with TBI.
There is conflicting data as to whether ketamine inducesepileptiform activity. The blocking of NMBA receptors andsubsequent entry of calcium into neurons may limit seizureactivity. Furthermore, the use of ketamine as an adjunct inthe treatment of status epliepticus is well described in the lit-erature [59]. The antagonism of NMDA receptors decreasesthe release of neurotoxic glutamate and may impart aprotective effect in patients with traumatic brain injury [60].
Therefore ketamine is indicated particularly as an induc-tion agent in patients with TBI and haemodynamic instabil-ity. It may have a role for refractory seizure activity.
8. Dexmedetomidine
See Table 8. Dexmedetomidine is a highly selective alpha-2 receptor agonist that acts by a receptor distinct from the
GABA receptor utilised by propofol and the benzodiazepines.A high selectivity for alpha-2 receptors, seven to eight timesthat of clonidine, explains its anxiolytic and sedative effects.A relatively short elimination t1/2 of two hours enables intra-venous titration to effect. Furthermore, dexmedetomidinedoes not appear to cause respiratory depression, with onestudy reporting no significant difference in respiratory rateand oxygen saturations between dexmedetomidine recipientsand those that received placebo. This enables it to becontinued after-extubation [61, 62]. Hypotension and brady-cardia are among the most commonly reported side effectsof dexmedetomidine, particularly when using a loadingdose. For this reason, some commentators recommend anavoidance of a loading dose in patients with TBI.
Several trials have examined the use of dexmedetomidinesedation in ICU patients.
Riker et al. performed a prospective, double-blinded RCTin medical and surgical ICU patients comparing the efficacyand safety of dexmedetomidine with midazolam sedation[63]. Patients in the dexmedetomidine arm spent less timeon the ventilator and experienced less hypertension andtachycardia. 42.2% of patients in the dexmedetomidine armexperienced bradycardia compared to 18.9% of patients whoreceived midazolam sedation.
A potential advantage of dexmedetomidine may be indecreasing the incidence or severity of delirium. Manycommonly used sedatives, including opioids and benzodi-azepines, have been shown to increase the risk of delirium. Inone prospective, double-blinded RCT, patients after cardiacsurgery were randomised to receive either a dexmedetomi-dine or morphine-based sedative regimen [64]. Patients inthe dexmedetomidine arm showed a significant reduction inthe duration of delirium, although there was no statisticallysignificant reduction in the incidence of delirium. A reduc-tion in the incidence of delirium was also found in an a priorisubgroup analysis of the MENDS trial. There was a reducedduration of brain dysfunction, particularly in septic patients[58].
There have been relatively few studies examining therole of dexmedetomidine in patients with TBI. Its use inneurosurgical patients was described in a retrospective studyby Aryan et al. [65]. They describe a mean increase in cerebralperfusion pressure and a decrease in intracranial pressurein the 39 patients studied. The relatively small sample sizeand retrospective nature of this study limit its conclusions,and the authors argue for further studies to establish anoptimal dosage regimen in neurosurgical patients. Grof etal. undertook a small, prospective, observational study, ofpatients receiving dexmedetomidine on a neurosurgical ICU[66]. The majority of these patients had traumatic braininjury. Dexmedetomidine was utilised in an attempt to weanpatients off other sedative regimens. Relatively high doses ofdexmedetomidine were required to achieve the desired levelof sedation, up to a rate of 2.5 mcg/kg/hour. The authorspostulate that significant changes in neurotransmitter sys-tems in TBI might explain the need for higher doses ofdexmedetomidine in this patient population.
There is a need for further high-quality RCTs to evaluatethe use of dexmedetomidine as a sedative agent both in

Emergency Medicine International 9
Table 9
Induction agents
(i) Haemodynamically unstableKetamine (2 mg/kg) ORMidazolam (0.1 mg/kg) andfentanyl (1–3 mcg/kg)
(ii) Haemodynamically stableThiopentone (1–3 mg/kg ORpropofol (0.5–2.5 mg/kg),with fentanyl (1–3 mcg/kg)
Maintenance agentsPropofol (1.5–4.5 mg/kg/h)and fentanyl (0.5–2 mcg/kg/h)
general ICU patients and in patients with TBI. The SPICEpilot study will examine the feasibility of conducting a largemulti-centre trial, comparing current sedation practice witha dexmedetomidine-based sedation regimen. The DahLIAtrial is currently recruiting patients and is a prospec-tive, double-blinded RCT comparing dexmedetomidine toplacebo in the treatment of delirium and agitation.
Therefore dexmedetomidine has a number of potentialadvantages as a sedative agent in TBI. There is evidence thatit may reduce delirium and a lack of respiratory depressanteffects enables it to be used in non-intubated patients.
9. Conclusion
Sedation is a vital component of the management of patientswith traumatic brain injuries. However, there is limited high-quality evidence examining outcomes in TBI to guide clini-cians on their choice of agent. Consequently a wide varietyof agents and dosages are used. Recent work has challengedtraditional views on the best agents to use in TBI. For exam-ple, there is increasing evidence that ketamine may be safe touse in TBI as an induction agent and has advantages overtraditional agents such as the barbiturates. There has alsobeen increased interest in shorter acting, newer agents suchas remifentanil and dexmedetomidine. These offer potentialadvantages in allowing faster recovery of consciousness andassessment of neurology in patients.
There is a need for further prospective, randomisedcontrolled trials, examining both physiological and clinicaloutcomes, to assess these agents in the context of traumaticbrain injury. Meanwhile, in the absence of extensive high-quality evidence to guide clinicians in their choice of agent,there is a need for a pragmatic approach, based on the clinicalsituation and knowledge of the potential advantages anddisadvantages of each agent.
10. Recommendations
See Table 9. For induction of anaesthesia in TBI, there is nosingle agent that is perfect and the way in which the medica-tion is given, and the dose used, may be more important thanthe agents themselves. Considered preparation, experiencedassistants and meticulous control and monitoring of bloodpressure are essential. Thiopentone remains a reasonablechoice, with the proviso that it is used judiciously in thehaemodynamically unstable patient. Alternative induction
agents include propofol (usually requiring a concomitantvasopressor bolus) or ketamine. There is little role foretomidate either as an agent for induction or continuedsedation.
Propofol as an agent for continued sedation, usuallyadministered with a short-acting narcotic, offers the advan-tage of a relatively rapid offset of sedation, facilitatingneurological assessment. Remifentanil has many advantagesover other narcotics in this setting as long as hyperalgesia oncessation is considered. In patients who require high doses ofpropofol, hypotensive patients, or for more prolonged seda-tion, midazolam is a suitable alternative. Thiopentone is notindicated as a maintenance sedative agent in TBI, and its useis primarily limited to the treatment of refractory intracranialhypertension. Dexmedetomidine shows promise as a sedativeagent in TBI, particularly in the non-intubated patient.
Thanks to Professor Richard Lee for his helpful sugges-tions regarding this review.
References
[1] “Guidelines for the management of severe traumatic braininjury,” Journal of Neurotrauma, vol. 24, supplement 1, pp. S1–S106, 2007.
[2] M. R. Fearnside, R. J. Cook, P. McDougall, and R. J. McNeil,“The Westmead Head Injury Project outcome in severe headinjury. A comparative analysis of pre-hospital, clinical and CTvariables,” British Journal of Neurosurgery, vol. 7, no. 3, pp.267–279, 1993.
[3] R. M. Chesnut, L. F. Marshall, M. R. Klauber et al., “The roleof secondary brain injury in determining outcome from severehead injury,” Journal of Trauma, vol. 34, no. 2, pp. 216–222,1993.
[4] D. J. Roberts, R. I. Hall, A. H. Kramer et al., “Sedation forcritically ill adults with severe traumatic brain injury: a sys-tematic review of randomized controlled trials,” Critical CareMedicine, vol. 39, no. 12, pp. 2743–2751, 2011.
[5] C. Barash, R. K. Stoelting, M. Cahalan, and M. C. Stock, Eds.,Clinical Anesthesia, Lippencott Williams & Wilkins, Philade-phia, PA, USA, 2009.
[6] A. Turcant, A. Delhumeau, and A. Premel-Cabic, “Thiopentalpharmacokinetics under conditions of long-term infusion,”Anesthesiology, vol. 63, no. 1, pp. 50–54, 1985.
[7] S. Khan, N. Stannard, and J. Greijn, “Precipitation of thiopen-tal with muscle relaxants: a potential hazard,” JRSM ShortReports, vol. 2, no. 7, article 58, 2011.
[8] M. Pinaud, J. N. Lelausque, A. Chetanneau, N. Fauchoux,D. Menegalli, and R. Souron, “Effects of propofol on cere-bral hemodynamics and metabolism in patients with braintrauma,” Anesthesiology, vol. 73, no. 3, pp. 404–409, 1990.
[9] P. A. Farling, J. R. Johnston, and D. L. Coppel, “Propofolinfusion for sedation of patients with head injury in intensivecare. A preliminary report,” Anaesthesia, vol. 44, no. 3, pp.222–226, 1989.
[10] K. P. Ronan, T. J. Gallagher, B. George, and B. Hamby, “Com-parison of propofol and midazolam for sedation in intensivecare unit patients,” Critical Care Medicine, vol. 23, no. 2,pp. 286–293, 1995.
[11] A. G. Mustafa, I. N. Singh, J. Wang, K. M. Carrico, and E. D.Hall, “Mitochondrial protection after traumatic brain injuryby scavenging lipid peroxyl radicals,” Journal of Neurochem-istry, vol. 114, no. 1, pp. 271–280, 2010.

10 Emergency Medicine International
[12] A. R. Jayakumar, K. V. Rao, K. S. Panickar et al., “Trauma-induced cell swelling in cultured astrocytes,” Journal ofNeuropathology and Experimental Neurology, vol. 67, no. 5, pp.417–427, 2008.
[13] M. Tanguy, P. Seguin, B. Laviolle et al., “Cerebral microdialysiseffects of propofol versus midazolam in severe traumatic braininjury,” Journal of Neurotrauma, vol. 29, no. 6, pp. 1105–1110,2012.
[14] M. J. Junttila, M. Gonzalez, E. Lizotte et al., “Induced brugada-type electrocardiogram, a sign for imminent malignantarrhythmias,” Circulation, vol. 117, no. 14, pp. 1890–1893,2008.
[15] O. L. Cremer, K. G. M. Moons, E. A. C. Bouman, J. E.Kruijswijk, A. M. G. A. De Smet, and C. J. Kalkman, “Long-term propofol infusion and cardiac failure in adult head-injured patients,” The Lancet, vol. 357, no. 9250, pp. 117–118,2001.
[16] L. C. Otterspoor, C. J. Kalkman, and O. L. Cremer, “Updateon the propofol infusion syndrome in ICU management ofpatients with head injury,” Current Opinion in Anaesthesiology,vol. 21, no. 5, pp. 544–551, 2008.
[17] A. Donmez, G. Arslan, A. Pirat, and B. Demirhan, “Ispancreatitis a complication of propofol infusion?” EuropeanAcademy of Anaesthesiology, vol. 16, no. 6, pp. 367–370, 1999.
[18] P. B. Langevin, N. Gravenstein, T. J. Doyle et al., “Growth ofStaphylococcus aureus in Diprivan and Intralipid: implica-tions on the pathogenesis of infections,” Anesthesiology, vol.91, no. 5, pp. 1394–1400, 1999.
[19] B. P. Hodkinson, R. W. Frith, and E. W. Mee, “Proprofol andthe electroencephalogram,” The Lancet, vol. 2, no. 8574, p.1518, 1987.
[20] M. J. Sutherland and P. Burt, “Propofol and seizures,” Anaes-thesia and Intensive Care, vol. 22, no. 6, pp. 733–737, 1994.
[21] S. Carley and I. Crawford, “Towards evidence based emer-gency medicine: best BETs from the Manchester Royal Infir-mary. Propofol for resistant status epilepticus,” Emergencymedicine Journal, vol. 19, no. 2, pp. 143–144, 2002.
[22] U. M. Illievich, W. Petricek, W. Schramm, M. Weindlmayr-Goettel, T. Czech, and C. K. Spiss, “Electroencephalographicburst suppression by propofol infusion in humans: hemody-namic consequences,” Anesthesia and Analgesia, vol. 77, no. 1,pp. 155–160, 1993.
[23] J. M. Wong, “Propofol infusion syndrome,” American Journalof Therapeutics, vol. 17, no. 5, pp. 487–491, 2010.
[24] B. Matta and D. Menon, “Severe head injury in the UnitedKingdom and Ireland: a survey of practice and implicationsfor management,” Critical Care Medicine, vol. 24, no. 10, pp.1743–1748, 1996.
[25] D. H. Rhoney and D. Parker, “Use of sedative and analgesicagents in neurotrauma patients: effects on cerebral physiol-ogy,” Neurological Research, vol. 23, no. 2-3, pp. 237–259, 2001.
[26] S. C. Urwin and D. K. Menon, “Comparative tolerability ofsedative agents in head-injured adults,” Drug Safety, vol. 27,no. 2, pp. 107–133, 2004.
[27] H. Allonen, G. Ziegler, and U. Klotz, “Midazolam kinetics,”Clinical Pharmacology and Therapeutics, vol. 30, no. 5, pp.653–661, 1981.
[28] L. Papazian, J. Albanese, X. Thirion, G. Perrin, O. Durbec, andC. Martin, “Effect of bolus doses of midazolam on intracranialpressure and cerebral perfusion pressure in patients withsevere head injury,” British Journal of Anaesthesia, vol. 71, no.2, pp. 267–271, 1993.
[29] J. E. Fleischer, J. H. Milde, T. P. Moyer, and J. D. Michenfelder,“Cerebral effects of high-dose midazolam and subsequent
reversal with Ro 15–1788 in dogs,” Anesthesiology, vol. 68, no.2, pp. 234–242, 1988.
[30] B. Mets, A. Horsell, and D. M. Linton, “Midazolam-inducedbenzodiazepine withdrawal syndrome,” Anaesthesia, vol. 46,no. 1, pp. 28–29, 1991.
[31] P. Pandharipande, B. A. Cotton, A. Shintani et al., “Prevalenceand risk factors for development of delirium in surgical andtrauma intensive care unit patients,” The Journal of Trauma,vol. 65, no. 1, pp. 34–41, 2008.
[32] A. Morandi and J. C. Jackson, “Delirium in the intensive careunit: a review,” Neurologic Clinics, vol. 29, no. 4, pp. 749–763,2011.
[33] A. S. Camps, J. A. Sanchez-Izquierdo Riera, D. T. Vazquez, M.Sa Borges, J. P. Rodriguez, and E. A. Lopez, “Midazolam and2% propofol in long-term sedation of traumatized, criticallyill patients: efficacy and safety comparison,” Critical CareMedicine, vol. 28, no. 11, pp. 3612–3619, 2000.
[34] K. A. Ghori, D. C. Harmon, A. Elashaal et al., “Effect of mida-zolam versus propofol sedation on markers of neurologicalinjury and outcome after isolated severe head injury: a pilotstudy,” Critical Care and Resuscitation, vol. 9, no. 2, pp. 166–171, 2007.
[35] I. Egerod, M. B. Jensen, S. F. Herling, and K. L. Welling, “Effectof an analgo-sedation protocol for neurointensive patients:a two-phase interventional non-randomized pilot study,”Critical Care, vol. 14, no. 2, article R71, 2010.
[36] R. J. Osborne, S. P. Joel, and M. L. Slevin, “Morphine intoxi-cation in renal failure: the role of morphine-6-glucuronide,”British Medical Journal, vol. 292, no. 6535, pp. 1548–1549,1986.
[37] J. Scholz, M. Steinfath, and M. Schulz, “Clinical pharma-cokinetics of alfentanil, fentanyl and sufentanil. An update,”Clinical Pharmacokinetics, vol. 31, no. 4, pp. 275–292, 1996.
[38] N. T. Smith, J. L. Benthuysen, R. G. Bickford et al., “Seizuresduring opioid anesthetic induction—are they opioid-inducedrigidity?” Anesthesiology, vol. 71, no. 6, pp. 852–862, 1989.
[39] T. D. Egan, H. J. M. Lemmens, P. Fiset et al., “The pharmacoki-netics of the new short-acting opioid remifentanil (GI87084B)in healthy adult male volunteers,” Anesthesiology, vol. 79, no. 5,pp. 881–892, 1993.
[40] A. Karabinis, K. Mandragos, S. Stergiopoulos et al., “Safetyand efficacy of analgesia-based sedation with remifentanil ver-sus standard hypnotic-based regimens in intensive care unitpatients with brain injuries: a randomised, controlled trial[ISRCTN50308308],” Critical Care, vol. 8, no. 4, pp. R268–280, 2004.
[41] D. R. Jeevaratnam and D. K. Menon, “Survey of intensivecare of severely head injured patients in the United Kingdom,”British Medical Journal, vol. 312, no. 7036, pp. 944–947, 1996.
[42] W. J. Stept and P. Safar, “Rapid induction-intubation for pre-vention of gastric-content aspiration,” Anesthesia and Analge-sia, vol. 49, no. 4, pp. 633–636, 1970.
[43] I. Roberts, “Barbiturates for acute traumatic brain injury,”Cochrane Database of Systematic Reviews, no. 2, Article IDCD000033, 2000.
[44] J. M. Gooding, J. T. Weng, and R. A. Smith, “Cardiovascularand pulmonary responses following etomidate induction ofanesthesia in patients with demonstrated cardiac disease,”Anesthesia and Analgesia, vol. 58, no. 1, pp. 40–41, 1979.
[45] M. J. Van Hamme, M. M. Ghoneim, and J. J. Ambre, “Phar-macokinetics of etomidate, a new intravenous anesthetic,”Anesthesiology, vol. 49, no. 4, pp. 274–277, 1978.
[46] E. Moss, D. Powell, R. M. Gibson, and D. G. McDowall, “Effectof etomidate on intracranial pressure and cerebral perfusion

Emergency Medicine International 11
pressure,” British Journal of Anaesthesia, vol. 51, no. 4, pp. 347–352, 1979.
[47] P. A. Modica and R. Tempelhoff, “Intracranial pressure duringinduction of anaesthesia and tracheal intubation with etomi-date-induced EEG burst suppression,” Canadian Journal ofAnaesthesia, vol. 39, no. 3, pp. 236–241, 1992.
[48] I. Watt and L. I. McA, “Mortality amongst multiple traumapatients admitted to an intensive therapy unit,” Anaesthesia,vol. 39, no. 10, pp. 973–981, 1984.
[49] G. Malerba, F. Romano-Girard, A. Cravoisy et al., “Risk factorsof relative adrenocortical deficiency in intensive care patientsneeding mechanical ventilation,” Intensive Care Medicine, vol.31, no. 3, pp. 388–392, 2005.
[50] Z. Ding and P. F. White, “Anesthesia for electroconvulsivetherapy,” Anesthesia and Analgesia, vol. 94, no. 5, pp. 1351–1364, 2002.
[51] S. A. Forman, “Clinical and molecular pharmacology ofetomidate,” Anesthesiology, vol. 114, no. 3, pp. 695–707, 2011.
[52] Y. Filanovsky, P. Miller, and J. Kao, “Myth: ketamine shouldnot be used as an induction agent for intubation in patientswith head injury,” Canadian Journal of Emergency Medicine,vol. 12, no. 2, pp. 154–201, 2010.
[53] J. M. Gibbs, “The effect of intravenous ketamine on cere-brospinal fluid pressure,” British Journal of Anaesthesia, vol. 44,no. 12, pp. 1298–1302, 1972.
[54] J. Evans, M. Rosen, R. D. Weeks, and C. Wise, “Ketamine inneurosurgical procedures,” The Lancet, vol. 1, no. 7688, pp.40–41, 1971.
[55] H. M. Shapiro, S. R. Wyte, and A. B. Harris, “Ketamine anaes-thesia in patients with intracranial pathology,” British Journalof Anaesthesia, vol. 44, no. 11, pp. 1200–1204, 1972.
[56] A. Bourgoin, J. Albanese, M. Leone, E. Sampol-Manos, X.Viviand, and C. Martin, “Effects of sufentanil or ketamineadministered in target-controlled infusion on the cerebralhemodynamics of severely brain-injured patients,” CriticalCare Medicine, vol. 33, no. 5, pp. 1109–1113, 2005.
[57] A. Lele and W. C. Ziai, “Target-controlled infusion for seda-tion of traumatic brain-injured patients: role uncertain,” Crit-ical Care Medicine, vol. 33, no. 5, pp. 1172–1174, 2005.
[58] P. P. Pandharipande, R. D. Sanders, T. D. Girard et al., “Effectof dexmedetomidine versus lorazepam on outcome in patientswith sepsis: an a priori-designed analysis of the MENDSrandomized controlled trial,” Critical Care, vol. 14, no. 2,article R38, 2010.
[59] R. D. Sheth and B. E. Gidal, “Refractory status epilepticus:response to ketamine,” Neurology, vol. 51, no. 6, pp. 1765–1766, 1998.
[60] G. Bar-Joseph, Y. Guilburd, A. Tamir, and J. N. Guilburd,“Effectiveness of ketamine in decreasing intracranial pressurein children with intracranial hypertension: clinical article,”Journal of Neurosurgery, vol. 4, no. 1, pp. 40–46, 2009.
[61] D. S. Carollo, B. D. Nossaman, and U. Ramadhyani, “Dexme-detomidine: a review of clinical applications,” Current Opinionin Anaesthesiology, vol. 21, no. 4, pp. 457–461, 2008.
[62] E. Martin, G. Ramsay, J. Mantz, and S. T. J. Sum-Ping,“The role of the α2-adrenoceptor agonist dexmedetomidinein postsurgical sedation in the intensive care unit,” Journal ofIntensive Care Medicine, vol. 18, no. 1, pp. 29–41, 2003.
[63] R. R. Riker, Y. Shehabi, P. M. Bokesch et al., “Dexmedeto-midine vs midazolam for sedation of critically Ill patients Arandomized trial,” Journal of the American Medical Association,vol. 301, no. 5, pp. 489–499, 2009.
[64] Y. Shehabi, P. Grant, H. Wolfenden et al., “Prevalence ofdelirium with dexmedetomidine compared with morphine
based therapy after cardiac surgery: a randomized controlledtrial (DEXmedetomidine compared to morphine-DEXCOMstudy),” Anesthesiology, vol. 111, no. 5, pp. 1075–1084, 2009.
[65] H. E. Aryan, K. W. Box, D. Ibrahim, U. Desiraju, and C. P.Ames, “Safety and efficacy of dexmedetomidine in neurosur-gical patients,” Brain Injury, vol. 20, no. 8, pp. 791–798, 2006.
[66] T. M. Grof and K. A. Bledsoe, “Evaluating the use of dexme-detomidine in neurocritical care patients,” Neurocritical Care,vol. 12, no. 3, pp. 356–361, 2010.
[67] P. Allely, “What Is Brugada Syndrome?” 2009, http://lifeinthe-fastlane.com/2009/09/what-is-brugada-syndrome/.

Hindawi Publishing CorporationEmergency Medicine InternationalVolume 2012, Article ID 320309, 8 pagesdoi:10.1155/2012/320309
Review Article
Diagnosis and Management of Bacterial Meningitis inthe Paediatric Population: A Review
Catherine L. Tacon1 and Oliver Flower2
1 Sydney Children’s Hospital, Randwick, NSW, Australia2 Intensive Care Unit, Royal North Shore Hospital, St Leonards, NSW 2065, Australia
Correspondence should be addressed to Catherine L. Tacon, [email protected]
Received 3 March 2012; Accepted 3 August 2012
Academic Editor: Chamisa Macindoe
Copyright © 2012 C. L. Tacon and O. Flower. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Paediatric bacterial meningitis is a neurological emergency which, despite advances in medical management, still has a significantmorbidity and mortality. Over recent decades new vaccines have led to a change in epidemiology of the disease; however, it remainsa condition that requires a high index of suspicion, prompt diagnosis, and early management in the emergency department. Newlaboratory techniques and clinical tools are aiding the diagnosis of bacterial meningitis, yet some controversies still exist in itsmanagement. This paper outlines the changing epidemiology of the disease, current diagnostic techniques as well as controversiesand advances in the management of bacterial meningitis in the paediatric population.
1. Introduction
Bacterial meningitis is a medical emergency characterised byinflammation of the meninges in response to bacterial infec-tion. Untreated, its mortality approaches 100%, and evenwith current antibiotics and advanced paediatric intensivecare, the mortality rate of the disease is approximately 5–10% [1]. Worldwide, the risk of neurological sequelae insurvivors following hospital discharge approaches 20% [2].Early diagnosis and appropriate management of the childwith meningitis is therefore critical. The management andepidemiology of bacterial meningitis in the neonate differsfrom that of the infant and child; it will not be reviewed here.
2. Epidemiology
The incidence of bacterial meningitis is approximately 5–7per 100 000 population [1]. In developed countries, Neisseriameningitidis and Streptococcus pneumoniae are now thecommonest causes of acute bacterial meningitis in otherwisehealthy children [3] (see Table 1). Previously, Haemophilusinfluenzae type B (Hib) accounted for up to 48% of allbacterial meningitis cases [4]; however, the introduction of
the Hib vaccination program led to a dramatic reductionin the incidence of Hib meningitis. Hib now accountsfor only 7% of meningitis cases in the United States andis predominantly seen in unvaccinated adult patients [4].However, the burden of Hib in developing countries withoutadequate vaccination programs still remains significant; by2007 only 42% of children worldwide had access to the Hibimmunisation program [4].
Streptococcus pneumoniae is now the commonest causeof bacterial meningitis in the United States and Europe[4]. Although seen in the healthy child, children witha basilar skull or cribriform fracture with a CSF leak,asplenism or HIV infection are at particular risk of devel-oping pneumococcal meningitis [3]. Furthermore, patientswith cochlear implants have a 30 times increased risk ofdeveloping pneumococcal meningitis [5]. The developmentof pneumococcal conjugate vaccines has led to a decline inthe incidence of pneumococcal meningitis in countries withan active immunisation program; however, concern exists asto the emergence of pneumococcal serotypes not covered bythe vaccines [4]. This, coupled by the increasing resistanceof Streptococcus pneumoniae to conventional antibiotics, is ofgrowing concern [1].

2 Emergency Medicine International
Table 1: Causative organisms.
Organism Comment
Streptococcus pneumoniae
Commonest organismAffects healthy childrenAdditional risk factors: basilarskull or cribriform fracture,asplenism, HIV, and cochlearimplants
Neisseria meningitidisCan cause epidemic, endemic, orsporadic infections
Haemophilus influenzaetype B
Reduced incidence afterintroduction of vaccinationprogram
Group B streptococcus
The less common pathogensGroup B streptococcus, E. Coli andL. monocytogenes more commonin neonates
Escherichia coli
Non typeable H. influenzae
Other gram-negative bacilli
Listeria monocytogenes
Group A streptococci
Staphylococcal speciesPenetrating head trauma andneurosurgery
Streptococci
Aerobic gram-negativebacilli
There are six serogroups of Neisseria menigitidis with theability to cause severe meningitis: A, B, C, X, Y and W-135 [6]. Infection with Neisseria meningitidis can be eitherepidemic or endemic [3], and although the majority of casesin the United States are sporadic [4], N. meningitidis is theonly bacteria that can cause epidemics of meningitis [6].Throughout America and Europe serogroups B, C, and Yaccount for the majority of meningococcal meningitis cases[4], with serogroup B being the leading cause of endemicmeningitis in developed countries overall [6, 7]. SerogroupA N. meningitidis is also a significant problem, particularlyin the sub-Saharan “meningitis-belt,” where it is responsiblefor a number of large-scale epidemics [6]. While a conjugatemeningococcal vaccine for serogroups A, C, Y, and W-135has shown reductions in meningococcal disease in somepopulations [3], development of an effective vaccine againstserogroup B has been difficult. Recent trials have shownpromise in the use of a new multicomponent serogroup Bvaccine [7, 8], but currently the lack of a widely available,effective vaccination against N. meningitidis B, as well asthe lack of access to vaccinations in populations at riskof epidemics, such as in sub-Saharan Africa, means thatN. meningitidis still remains a significant cause of bacterialmeningitis [6].
In developed countries less than 20% of bacterialmeningitis in the paediatric population aged 3 monthsand over is caused by organisms other than S. pneumoniaeor N. meningitidis. The less-common causative organismsinclude Group B Streptococcus, Escherichia coli, nontypeable
H. influenzae, other gram-negative bacilli, Listeria monocyto-genes, and group A streptococci [4]. In addition patients whohave had penetrating head trauma or neurosurgery are alsoat risk of developing meningitis from staphylococcal species,streptococci, and aerobic gram-negative bacilli [3, 9], andthis should be considered in such a child presenting withpossible bacterial meningitis.
3. Diagnosis
Early diagnosis and treatment of bacterial meningitis iscritical, and a high index of clinical suspicion is essential.Diagnosis involves both clinical assessment and the use oflaboratory investigations.
3.1. Clinical. The clinical symptoms and signs of bacterialmeningitis in children vary depending on the age of the childand duration of disease. Nonspecific signs include abnormalvital signs such as tachycardia and fever, poor feeding,irritability, lethargy, and vomiting [4]. Signs of fulminantsepsis such as shock, disseminated intravascular coagulation(DIC), purpuric rash, and coma may be present and aremore common in meningococcal meningitis [1]. These signshowever are more likely to develop later in the course of theillness (median time between 13 and 22 hours) [10] whereasnonspecific, often overlooked symptoms, such as leg pain,may be present within 8 hours in more than 70% of childrenwith meningococcal meningitis and should prompt furtherimmediate evaluation [10, 11]. Classical signs of meningitissuch as nuchal rigidity, bulging fontanelle, photophobia, anda positive Kernig’s or Brudzinski’s sign (more common inchildren older than 12 to 18 months) may also be present[3]. A recent systematic review found that the presence ofmeningeal signs increased the likelihood of the diagnosisof meningitis, and conversely their absence decreased thelikelihood [12]; however, other studies have shown thatno classical symptoms and signs of meningitis are able todistinguish accurately between children with or withoutmeningitis [13], and so these signs should be interpretedwith caution.
Seizures may be present in 20–30% of children withbacterial meningitis, more commonly with S. pneumoniaeand Hib infections than with N. meningitidis [3]. A recentstudy has suggested that the presence of complex seizuresmore than doubles the risk of meningitis [12]. Focalneurological signs may also be found, as may a reduced levelof consciousness. Coma on presentation is associated with aworse prognosis than a child presenting with irritability orlethargy alone [3].
3.2. Laboratory Investigations
3.2.1. Lumbar Puncture. Whilst a lumbar puncture (LP) isnecessary for the definitive diagnosis of bacterial menin-gitis and should be performed where a clinical suspicionfor meningitis exists, contraindications often preclude thisinvestigation. These contraindications (see Table 2) includesigns of raised intracranial pressure, such as an alteration

Emergency Medicine International 3
Table 2: Contraindications to lumbar puncture [9].
Contraindication Comment
Raised intracranial pressure:
Alteration in level ofconsciousness
Papilloedema
Focal neurological signsExcluding an isolated cranialnerve VI or VII palsy
Prolonged seizuresDelay lumbar puncture for 30minutes in simple, short seizuresonly
History of selected CNSdisease
CSF shunts, hydrocephalus,trauma, post neurosurgery, orknown space-occupying lesion
ImmunocompromiseHIV/AIDS, onimmunosuppressive therapy,post-transplantation
Coagulation disorders
Cardiorespiratoryinsufficiency
Localised infection at site ofneedle insertion
in level of consciousness, papilloedema, prolonged seizures,or focal neurological signs, as well as coagulation disorders,cardiorespiratory instability, a history of immunosuppres-sion, certain central nervous syndrome (CNS) conditions,or localised infection at the site of insertion of the lumbarpuncture needle [1]. LP may be delayed until these con-traindications no longer exist; however, administration ofantibiotics and appropriate therapy should not be delayed ifthe LP cannot be performed immediately.
Initial analysis of the CSF should include microscopywith gram stain, culture and measurement of protein, andglucose levels. CSF findings suggestive of bacterial meningitisare outlined in Table 3. Typically the CSF white cell count(wcc) is >1000 cells/mm3 although it may not be elevatedin the early phase of the infection [3], and the majority ofwhite cells are polymorphonuclear (PMNs). CSF protein istypically elevated (100–200 mg/dL) and glucose low (CSFto serum ratio <0.4) [3]. In untreated bacterial meningitisthe CSF gram stain may be positive in 80–90% of patients[3] and varies with both the CSF concentration of bacteriaand type of bacteria [9]. The overall probability of obtaininga positive gram stain result increases 100 times by using acytospin technique [14] (the use of a high-speed centrifugeto concentrate cells). Patients with bacterial meningitis whohave been pretreated with antibiotics are more likely to havea higher glucose and lower protein level although the CSFwcc and absolute PMN count are not normally significantlyaffected [15].
A clinical prediction rule, the Bacterial Meningitis Score,has been developed to assess the risk of bacterial meningitisin patients with CSF pleocytosis. It assesses patients asbeing of very low risk of bacterial meningitis if none of thefollowing are present: positive CSF gram stain, CSF absolute
PMN count ≥1000 cells/mm3, CSF protein ≥80 mg/dL,peripheral blood absolute PMN count ≥10 000 cells/mm3,and history of seizure before, or at the time of presentation[17]. The score however is not applicable to childrenwith features of severe sepsis, known neurosurgical disease,known immunosuppression, traumatic lumbar puncture, orprevious antibiotic therapy within the past 48 hours [18].While a large multicentre study has validated this score,showing that if all criteria are absent, the risk of bacterialmeningitis is 0.1% [17], as the score has less than 100%sensitivity, its use alone to decide individual patient therapyis not currently recommended [9, 18].
While the presence of an organism on gram stain, orculture of bacteria from the CSF, is diagnostic of bacterialmeningitis, a number of other investigations may also beperformed on CSF to aid diagnosis. Latex agglutination maybe performed to detect the presence of bacterial antigens inthe CSF. It has the advantage of being able to be rapidlyperformed, with a result available in less than 15 minutes,well before culture results are available [9, 19]. Although itmay remain positive for up to 10 days after the initiation ofantibiotics [19], it is neither 100% sensitive or specific [9, 19].One study has shown a sensitivity of only 7% for detectingbacterial antigens in culture-negative bacterial meningitis[20]; hence, its use may be limited [4].
Polymerase chain reaction (PCR) may also be used todetect microbial DNA in CSF. It also has the advantage ofbeing relatively rapid and is able to detect low amountsof bacteria in the CSF [21]. PCR results may be positivedespite pre-treatment with antibiotics [21], and althoughnot 100% specific, some studies have found PCR to have100% sensitivity, allowing antibiotics to be ceased if PCR isnegative [9], although further refinements in PCR techniquesare probably necessary.
CSF lactate may be elevated in patients with bacterialcompared with viral meningitis. Two recent meta-analyseshave suggested that an elevated CSF lactate is a good dis-tinguishing marker of bacterial meningitis [22, 23]. Howeveras it may be affected by a number of factors, including pre-treatment with antibiotics (reducing the level), seizures, orcerebral hypoxia (increasing the level), its routine use inthe assessment of community-acquired meningitis is notcurrently recommended, and further prospective studies areneeded [9].
3.2.2. Other Laboratory Investigations. Initial blood testsshould be performed for full blood count, coagulationstudies, and electrolytes to assess for complications of sepsisand to guide fluid management. Serum glucose should beroutinely measured as it may be low in the child withmeningitis, contributing to seizures. Its measurement is alsoneeded to accurately interpret the CSF glucose.
Blood cultures should be performed in all patients withsuspected bacterial meningitis. They may be of particularvalue if a lumbar puncture is contraindicated. The likelihoodof a positive blood culture result varies with the infectingorganism; 40% of children with meningococcal meningitiswill have a positive blood culture, whereas 50–90% of H.

4 Emergency Medicine International
Table 3: Lumbar puncture findings1 [3, 9].
CSF finding Normal2 Viral Bacterial Partially treated bacterial
White cell count (cells/mm3) <5 <1000 >1000 >1000
PMNs 0 20–40% >85–90% >80%
Protein (mg/dL) <40 Normal or <100 >100–200 60–100+
Glucose (mmol/L) ≥2.5 Normal Undetectable–<2.2 <2.2
Blood to glucose ratio ≥0.6 Normal <0.4 <0.4
Positive gram stain — — 75–90% (depending on organism) 55–70%
Positive culture — — >70–85% <85%1Other investigations may also be performed on CSF to exclude nonbacterial causes of meningitis depending on the clinical scenario; including India Ink
staining or antigen testing for Cryptococcus neoformans, Herpes simplex virus (HSV), cytomegalovirus (CMV) and enterovirus PCR.2 Values for paediatric patients >1 month of age; some values vary for neonates [16].Neonates: white cell count may be higher (<20 in the form of lymphocytes); normally zero PMNs, however some studies have found up to 5% PMNs inneonates without meningitis.Neonates: normal protein <100 mg/dL.
influenzae and 75% of S. pneumonia meningitis patients willhave a positive culture result [4].
Both CRP and procalcitonin have been evaluated todistinguish between viral and bacterial meningitis. Severalstudies have shown procalcitonin to have a better diagnosticaccuracy than CRP in differentiating between aseptic andbacterial meningitis [24, 25]. Procalcitonin levels in com-bination with other clinical scoring systems have also beenstudied to evaluate the risk of bacterial meningitis [18, 26].Although potentially increasing the sensitivity of scoringsystems, the use of procalcitonin in association with clinicalscores to exclude the diagnosis of bacterial meningitis isnot currently recommended. As such, while an elevation ineither CRP or procalcitonin is more suggestive of bacterialinfection, neither can establish, nor exclude the diagnosis ofbacterial meningitis [4, 24].
PCR for bacteria may be performed on blood and urine,especially if CSF is not obtainable.
Investigations are summarised in Table 4.
3.3. Imaging. Computed tomography (CT) of the head isindicated if a child has signs of focal neurology, increasedintracranial pressure (including papilloedema) deterioratingneurological function (such as increasing obtundation orseizures), immunocompromise or history of neurosurgicalprocedures, and shunt or hydrocephalus [1, 9] (see Table 2).In these patients it should be performed before a lumbarpuncture is attempted although a normal CT scan does notentirely exclude the risk of raised intracranial pressure [1].
4. Management
Bacterial meningitis is a neurological emergency, and it iscritical that appropriate empirical antibiotics are adminis-tered as soon as possible after the diagnosis is considered.A flow chart for the management of suspected bacterialmeningitis is provided in Figure 1.
4.1. Specific Therapy
4.1.1. Antibiotics. The choice of empirical antibiotics isguided by knowledge of local resistance patterns ofpathogens. Antibiotics should be administered parenterally,preferably by the intravenous route. In patients whereintravenous access is not immediately possible, antibioticadministration should not be delayed, but given by theintraosseous or intramuscular routes. Most treatment guide-lines recommend the use of a third-generation cephalosporin(such as ceftriaxone or cefotaxime) in conjunction withvancomycin as initial antibiotic therapy [9, 27]. Cefotaximeand ceftriaxone have excellent activity against all Hib and N.meningitidis strains. Increasing resistance of S. pneumoniae topenicillins has been reported, and although cefotaxime andceftriaxone remain active against many penicillin-resistantpneumococcal strains, treatment failure has been reported[3], hence the addition of empirical vancomycin. Listeriamonocytogenes is an unlikely pathogen in the immunocom-petent child older than 3 months of age although the additionof benzylpenicillin to cover this organism may be consideredfor the immunocompromised patient [27].
Once the organism is isolated and sensitivities areconfirmed, antibiotics may be rationalised. The duration ofantibiotics is based primarily on expert opinion, rather thanevidence-based data, and, although dependent on clinicalresponse, common guidelines suggest a 7-day treatmentcourse for Hib or N. meningitides and a 10–14-day coursefor S. pneumoniae [9]. A recent multicentre trial found thatchildren with H. influenzae, S. pneumonia, or N. meningitidismeningitis could have antibiotics safely discontinued at 5days, rather than 10 days if they were clinically stable [28];this however has not been adopted as the current standard ofcare in most centres.
4.1.2. Steroids. Empirical use of adjuvant dexamethasone(0.15 mg/kg/dose, 4 times a day) given before or up to amaximum of 12 hours after the first dose of antibioticsand continued for 2 to 4 days is currently recommended[9, 27, 29, 30]. This is based on evidence from studies in the

Emergency Medicine International 5
Table 4: Investigations for suspected bacterial meningitis.
Investigation Comment
Blood:
Full blood count Neutrophilia suggestive of bacterial infection
Serum glucose Often low; allows interpretation of CSF glucose
Electrolytes, urea, and creatinine To assess for complications and fluid management
Coagulation studies To assess for complications
Blood cultures Positive in 40–90% depending on organism
Inflammatory markers Elevation suggestive of bacterial infection; procalcitonin of more value;neither can establish nor exclude diagnosisCRP, procalcitonin
CSF:
Protein and glucose
Microscopy, culture, and sensitivities
Gram stain:S. pneumoniae—gram +ve cocciN. menigitidis—gram −ve cocciH. influenzae—gram −ve rod
Latex agglutination1 Rapid; not 100% specific or diagnostic
PCR2 Rapid; good sensitivity, techniques improving
Lactate Routine use not currently recommended
Imaging:Computed tomography of the head
Indicated for focal neurology, signs of increased intracranial pressure (ICP),deteriorating neurological function, previous neurosurgical procedures, orimmunocompromisedMay show evidence of hydrocephalus, abscess, subdural empyema, orinfarctionNormal scan does not entirely exclude risk of raised ICP
Other:PCR on blood or urine
Useful if CSF not obtainable
1Latex agglutination depends on laboratory availability; including N. meningitidis, S. pneumoniae, H. influenzae type B, Escherichia coli and group B
streptococci.2PCR depends on laboratory availability; including N. meningitidis, S. pneumoniae, H. influenzae type b, L. monocytogenes, HSV, CMV, Enterovirus andMycobacterium tuberculosis.
late 1980s and 1990s that suggested improved neurologicaloutcomes, particularly in hearing impairment, in childrenwho had H. influenzae meningitis [9]. Recent studies havesuggested that, unlike adults with bacterial meningitis,steroids do not improve mortality in children [31], and,hence, with the decline in incidence of Hib meningitis, theuse of steroids in children with bacterial meningitis hasincreasingly been questioned.
The most recent Cochrane review of the use of steroidsin bacterial meningitis showed a significant reduction inhearing loss (from 20.1% to 13.6%) and severe hearingloss (from 11.2% to 7.3%) in children with meningitis, butno benefit on mortality [32]. Although overall this hearingbenefit was seen in children affected by Hib meningitis,a subgroup analysis of children in high-income countriesalso showed a protective effect of steroids on hearing lossin non-H. influenzae meningitis [32]. This was not seen inlow-income countries, in fact, overall no significant benefitof corticosteroids at all was found in children in low-income countries [32]. Other recent meta-analyses havefound no benefit in any subgroup of children receivingadjuvant dexamethasone [33]. Overall, despite theoreticalharmful effects of corticosteroids, no meta-analyses have
shown harm with their administration, and as such it is stillrecommended to administer steroids before, or with the firstdose of antibiotics, especially in the child with suspected Hibmeningitis. Adjuvant dexamethasone should not be givento children who have already received antibiotics, as thisis unlikely to improve outcome [9]. As dexamethasone hasbetter penetration into the CSF than other corticosteroids, itis considered to be the corticosteroid of choice.
4.1.3. Controversial Therapy: Glycerol. The use of oral adju-vant glycerol may be beneficial for children with bacterialmeningitis through its action in increasing plasma osmo-lality, without inducing diuresis, leading to a reductionin cerebral oedema and an improvement in cerebral cir-culation and brain oxygenation [34]. A large randomisedtrial in Latin America showed a significant reduction inneurological sequelae in children given adjuvant glycerol, orglycerol in combination with dexamethasone, as comparedwith placebo [35]. No reduction in mortality or hearingimpairment was seen [35, 36]. As glycerol is a relatively safe,cheap medication that can be administered orally, it maybe especially beneficial in resource-limited settings. Somecriticism however has been made about this large trial’s

6 Emergency Medicine International
Suspected
bacterial
meningitis
No
Immediate blood cultures and
lumbar puncture
Dexamethasone
and empirical
antibiotic therapy
Yes
Immediate
blood
cultures
Dexamethasone
and empirical
antibiotic therapy
CT scan of head shows no evidence
of raised ICP
Lumbar puncture
Contraindication to
lumbar puncture or delay
in performance of lumbar
puncture?
Figure 1: Management of suspected bacterial meningitis [9].
design. This, in addition to a recent trial which failed toshow any benefit of glycerol in adult meningitis patients [37],means that further well-designed prospective studies shouldbe performed before glycerol is recommended as routinetherapy.
4.2. Supportive Care. Any child with a diagnosis of bacterialmeningitis will need supportive therapy, which may includecardiorespiratory support in a paediatric intensive careunit and directed management of complications, such asseizures, cerebral oedema, SIADH, DIC, or shock. Early,protocolized, aggressive care by a consultant supervisedpaediatric team improves survival and outcomes [38]. Earlyintubation and ventilation should be considered for any childwith evidence of respiratory compromise, threatened airway,ongoing shock, retractable seizures, or elevated intracranialpressure [30]. A recent Cochrane meta-analysis found some
evidence to support the use of maintenance, rather thanrestrictive fluids in the first 48 hours [39]. This meta-analysis found an improvement in the rate of early spasticityand seizures and in later overall neurological sequelae inchildren receiving maintenance fluids [39]. These findingswere however based on studies where late presentation andhigh mortality rates were common. In areas where earlypresentation is more common there are currently insufficientstudies to definitively guide fluid management [39].
4.3. Chemoprophylaxis. Close contacts of all children withmeningococcal meningitis should receive chemoprophylaxis(ceftriaxone, rifampicin, or ciprofloxacin), and contacts ofthose with Hib should receive ceftriaxone or rifampicin[3, 27]. Unvaccinated children less than 5 years of age shouldalso be vaccinated against H. influenzae as soon as possible[27]. Patients should be kept in respiratory isolation for atleast the first 24 hours after commencing antibiotic therapy[1].
5. Conclusion
Paediatric bacterial meningitis is a medical emergency whichrequires a high index of clinical suspicion, prompt diag-nosis, and early, aggressive protocolized management. Newvaccination programs have led to a change in epidemiologyof the disease; however, it remains prevalent worldwide.Advances in clinical and investigation techniques are aidingthe diagnosis of bacterial meningitis, and a combination oftechniques is useful to confirm or exclude the diagnosis.While antibiotics, steroids, and supportive therapy remainthe mainstay of treatment, further research should beperformed into the roles of adjuvant therapy.
Conflict of Interests
The authors declare they have no conflict of interest.
Acknowledgment
The authors would like to thank Dr. Francis Lockie for hisinsightful comments about this paper.
References
[1] V. P. Novelli, M. Peters, and S. Dobson, “Infectious diseases,”in Care of the Critically Ill Child, A. J. Macnab, D. J. Macrae,and R. Henning, Eds., pp. 281–298, Churchill Livingstone,London, UK, 1999.
[2] K. Edmond, A. Clark, V. S. Korczak, C. Sanderson, U. K.Griffiths, and I. Rudan, “Global and regional risk of disablingsequelae from bacterial meningitis: a systematic review andmeta-analysis,” The Lancet Infectious Diseases, vol. 10, no. 5,pp. 317–328, 2010.
[3] X. M. Saez-Llorens and X. M. GH, “Acute bacterial meningitisbeyond the neonatal period,” in Long: Principles and Practice ofPediatric Infectious Diseases Revised Reprint, S. Long, Ed., pp.284–291, Churchill Livingstone, Philadelphia, Pa, USA, 3rdedition, 2008.

Emergency Medicine International 7
[4] M. C. Brouwer, A. R. Tunkel, and D. van de Beek, “Epidemiol-ogy, diagnosis, and antimicrobial treatment of acute bacterialmeningitis,” Clinical Microbiology Reviews, vol. 23, no. 3, pp.467–492, 2010.
[5] J. Reefhuis, M. A. Honein, C. G. Whitney et al., “Risk ofbacterial meningitis in children with cochlear implants,” TheNew England Journal of Medicine, vol. 349, no. 5, pp. 435–445,2003.
[6] WHO, “Bacterial Meningitis,” New and Under-utilized Vac-cines Implementation (NUVI), 2010, http://www.who.int/nuvi/meningitis/en/index.html.
[7] M. E. Santolaya, M. L. O’Ryan, M. T. Valenzuela et al.,“Immunogenicity and tolerability of a multicomponentmeningococcal serogroup B (4CMenB) vaccine in healthyadolescents in Chile: a phase 2b/3 randomised, observer-blind,placebo-controlled study,” The Lancet, vol. 379, no. 9816, pp.617–624, 2012.
[8] N. Gossger, M. D. Snape, L. M. Yu et al., “Immunogenicityand tolerability of recombinant serogroup B meningococcalvaccine administered with or without routine infant vac-cinations according to different immunization schedules: arandomized controlled trial,” The Journal of the AmericanMedical Association, vol. 307, no. 6, pp. 573–582, 2012.
[9] A. R. Tunkel, B. J. Hartman, S. L. Kaplan et al., “Practiceguidelines for the management of bacterial meningitis,”Clinical Infectious Diseases, vol. 39, no. 9, pp. 1267–1284, 2004.
[10] M. J. Thompson, N. Ninis, R. Perera et al., “Clinical recog-nition of meningococcal disease in children and adolescents,”The Lancet, vol. 367, no. 9508, pp. 397–403, 2006.
[11] T. A. Haj-Hassan, M. J. Thompson, R. T. Mayon-White etal., “Which early ‘red flag’ symptoms identify children withmeningococcal disease in primary care?” British Journal ofGeneral Practice, vol. 61, no. 584, pp. e97–e104, 2011.
[12] S. Curtis, K. Stobart, B. Vandermeer, D. L. Simel, and T.Klassen, “Clinical features suggestive of meningitis in children:a systematic review of prospective data,” Pediatrics, vol. 126,no. 5, pp. 952–960, 2010.
[13] G. Amarilyo, A. Alper, A. Ben-Tov, and G. Grisaru-Soen, “Dia-gnostic accuracy of clinical symptoms and signs in childrenwith meningitis,” Pediatric Emergency Care, vol. 27, no. 3, pp.196–199, 2011.
[14] K. Chapin-Robertson, S. E. Dahlberg, and S. C. Edberg,“Clinical and laboratory analyses of cytospin-prepared gramstains for recovery and diagnosis of bacteria from sterile bodyfluids,” Journal of Clinical Microbiology, vol. 30, no. 2, pp. 377–380, 1992.
[15] L. E. Nigrovic, R. Malley, C. G. Macias et al., “Effect of anti-biotic pretreatment on cerebrospinal fluid profiles of childrenwith bacterial meningitis,” Pediatrics, vol. 122, no. 4, pp. 726–730, 2008.
[16] RCH, “The Royal Children’s Hospital Melbourne Clinical Pra-ctice Guidelines: CSF Interpretation,” 2012, http://www.rch.org.au/clinicalguide/cpg.cfm?doc id=5185#normal values.
[17] L. E. Nigrovic, N. Kuppermann, C. G. Macias et al., “Clinicalprediction rule for identifying children with cerebrospinalfluid pleocytosis at very low risk of bacterial meningitis,” TheJournal of the American Medical Association, vol. 297, no. 1, pp.52–60, 2007.
[18] F. Dubos, A. Martinot, D. Gendrel, G. Breart, and M.Chalumeau, “Clinical decision rules for evaluating meningitisin children,” Current Opinion in Neurology, vol. 22, no. 3, pp.288–293, 2009.
[19] L. D. Gray and D. P. Fedorko, “Laboratory diagnosis ofbacterial meningitis,” Clinical Microbiology Reviews, vol. 5, no.2, pp. 130–145, 1992.
[20] K. Tarafdar, S. Rao, R. A. Recco, and M. M. Zaman, “Lackof sensitivity of the latex agglutination test to detect bacterialantigen in the cerebrospinal fluid of patients with culture-negative meningitis,” Clinical Infectious Diseases, vol. 33, no.3, pp. 406–408, 2001.
[21] C. Welinder-Olsson, L. Dotevall, H. Hogevik et al., “Compari-son of broad-range bacterial PCR and culture of cerebrospinalfluid for diagnosis of community-acquired bacterial meningi-tis,” Clinical Microbiology and Infection, vol. 13, no. 9, pp. 879–886, 2007.
[22] N. T. Huy, N. T. H. Thao, D. T. N. Diep, M. Kikuchi, J. Zamora,and K. Hirayama, “Cerebrospinal fluid lactate concentrationto distinguish bacterial from aseptic meningitis: a systemicreview and meta-analysis,” Critical Care, vol. 14, no. 6, articleR240, 2010.
[23] K. Sakushima, Y. Hayashino, T. Kawaguchi, J. L. Jackson,and S. Fukuhara, “Diagnostic accuracy of cerebrospinal fluidlactate for differentiating bacterial meningitis from asepticmeningitis: a meta-analysis,” Journal of Infection, vol. 62, no.4, pp. 255–262, 2011.
[24] U. M. Alkholi, N. Abd Al-Monem, A. A. Abd El-Azim, andM. H. Sultan, “Serum procalcitonin in viral and bacterialmeningitis,” Journal of Global Infectious Diseases, vol. 3, no. 1,pp. 14–18, 2011.
[25] F. Dubos, B. Korczowski, D. A. Aygun et al., “Serum pro-calcitonin level and other biological markers to distinguishbetween bacterial and aseptic meningitis in children: aEuropean multicenter case cohort study,” Archives of Pediatricsand Adolescent Medicine, vol. 162, no. 12, pp. 1157–1163, 2008.
[26] F. Dubos, B. Korczowski, D. A. Aygun et al., “Distinguishingbetween bacterial and aseptic meningitis in children: Euro-pean comparison of two clinical decision rules,” Archives ofDisease in Childhood, vol. 95, no. 12, pp. 963–967, 2010.
[27] Antibiotic Expert Group, Therapeutic Guidelines: Antibiotic,Therapeutic Guidelines, Melbourne, VIC, Australia, 2010.
[28] E. Molyneux, S. Q. Nizami, S. Saha et al., “5 Versus 10 days oftreatment with ceftriaxone for bacterial meningitis in children:a double-blind randomised equivalence study,” The Lancet,vol. 377, no. 9780, pp. 1837–1845, 2011.
[29] C. Visintin, M. A. Mugglestone, E. J. Fields et al., “Manage-ment of bacterial meningitis and meningococcal septicaemiain children and young people: summary of NICE guidance,”British Medical Journal, vol. 340, Article ID c3209, 2010.
[30] NICE, “Bacterial meningitis and meningococcal septicaemia.Management of bacterial meningitis and meningococcal sep-ticaemia in children and young people younger than 16 yearsin primary and secondary care,” NICE clinical guideline 102,2010, http://www.nice.org.uk/guidance/CG102.
[31] J. Mongelluzzo, Z. Mohamad, T. R. Ten Have, and S. S.Shah, “Corticosteroids and mortality in children with bacterialmeningitis,” The Journal of the American Medical Association,vol. 299, no. 17, pp. 2048–2055, 2008.
[32] M. C. Brouwer, P. McIntyre, J. de Gans, K. Prasad, and D. vande Beek, “Corticosteroids for acute bacterial meningitis,”Cochrane Database of Systematic Reviews, vol. 9, Article IDCD004405, 2010.
[33] D. van de Beek, J. J. Farrar, J. de Gans et al., “Adjunctive dexa-methasone in bacterial meningitis: a meta-analysis of individ-ual patient data,” The Lancet Neurology, vol. 9, no. 3, pp. 254–263, 2010.

8 Emergency Medicine International
[34] S. Singhi, A. Jarvinen, and H. Peltola, “Increase in serum osm-olality is possible mechanism for the beneficial effects ofglycerol in childhood bacterial meningitis,” Pediatric InfectiousDisease Journal, vol. 27, no. 10, pp. 892–896, 2008.
[35] H. Peltola, I. Roine, J. Fernandez et al., “Adjuvant glyceroland/or dexamethasone to improve the outcomes of childhoodbacterial meningitis: a prospective, randomized, double-blind,placebo-controlled trial,” Clinical Infectious Diseases, vol. 45,no. 10, pp. 1277–1286, 2007.
[36] H. Peltola, I. Roine, J. Fernandez et al., “Hearing impairmentin childhood bacterial meningitis is little relieved by dexam-ethasone or glycerol,” Pediatrics, vol. 125, no. 1, pp. e1–e8,2010.
[37] K. M. B. Ajdukiewicz, K. E. Cartwright, M. Scarborough et al.,“Glycerol adjuvant therapy in adults with bacterial meningitisin a high HIV seroprevalence setting in Malawi: a double-blind, randomised controlled trial,” The Lancet InfectiousDiseases, vol. 11, no. 4, pp. 293–300, 2011.
[38] N. Ninis, C. Phillips, and L. Bailey, “The role of healthcaredelivery in the outcome of meningococcal disease in children:case-control study of fatal and non-fatal cases,” British MedicalJournal, vol. 330, no. 7506, p. 1475, 2005.
[39] I. Maconochie, H. Baumer, and M. E. Stewart, “Fluid therapyfor acute bacterial meningitis,” Cochrane Database of System-atic Reviews, no. 3, Article ID CD004786, 2008.

Hindawi Publishing CorporationEmergency Medicine InternationalVolume 2012, Article ID 476161, 5 pagesdoi:10.1155/2012/476161
Research Article
Prehospital Medication Administration: A Randomised StudyComparing Intranasal and Intravenous Routes
Cian McDermott1 and Niamh C. Collins2
1 Centre for Emergency Medical Science, University College Dublin, Dublin, Ireland2 Medical Advisory Group of the Pre-hospital Emergency Care Council in Ireland, Naas, Ireland
Correspondence should be addressed to Cian McDermott, [email protected]
Received 3 April 2012; Revised 5 June 2012; Accepted 11 June 2012
Academic Editor: Oliver Flower
Copyright © 2012 C. McDermott and N. C. Collins. This is an open access article distributed under the Creative CommonsAttribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work isproperly cited.
Introduction. Opioid overdose is an ever-increasing problem globally. Recent studies have demonstrated that intranasal (IN)naloxone is a safe and effective alternative to traditional routes of naloxone administration for reversal of opioid overdose. Aims.This randomised controlled trial aimed to compare the time taken to deliver intranasal medication with that of intravenous (IV)medication by advanced paramedic trainees. Methods. 18 advanced paramedic trainees administered either an IN or IV medicationto a mannequin model in a classroom-based setting. The time taken for medication delivery was compared. End-user satisfactionwas assessed using a 5-point questionnaire regarding ease of use and safety for both routes. Results. The mean time taken forthe IN and IV group was 87.1 seconds and 178.2 seconds respectively. The difference in mean time taken was 91.1 seconds (95%confidence interval 55.2 seconds to 126.9 seconds, P ≤ 0.0001). 89% of advanced paramedic trainees reported that the IN route waseasier and safer to use than the IV route. Conclusion. This study demonstrates that, amongst advanced paramedic trainees, the INroute of medication administration is significantly faster, better accepted and perceived to be safer than using the IV route. Thus,IN medication administration could be considered more frequently when administering emergency medications in a pre-hospitalsetting.
1. Introduction
The mortality associated with opioid overdose has continuedto increase globally in recent years. In 2009, the number ofIrish drug-related deaths attributed to opioid intoxicationrose by 20% [1], while in Europe, opioids were responsiblefor 75% of all drug-related deaths [2]. In the United Statesin 2007, there were 11,499 deaths resulting from opioidoverdose [3]. The main cause of death is as a result of opioid-induced respiratory depression [4]. After the initiation ofbasic life support measures, naloxone is an opioid antagonistthat is used to reverse respiratory depression and mentalstate changes. It is widely marketed under the brand nameNarcan. The common routes of administration of naloxoneare intravenous (IV), intraosseous (IO), intramuscular (IM),and subcutaneous. Intranasal (IN) administration is analternative route for naloxone delivery [5].
When a patient presents in opioid-induced cardiorespi-ratory arrest, immediate effective antagonism by naloxone
reverses the opioid-induced side effects. Direct entry ofnaloxone into the systemic circulation is required and thisis most reliably achieved with IV or IO medication admin-istration. Vascular access is often a major challenge whentreating a patient with opioid overdose in the prehospitalsetting due to damage to veins from repeated drug use [6].Multiple attempts at intravenous cannulation may result inan increased risk of exposure to blood-borne infections,in a group of patients that have a high seroprevalenceof blood-borne transmissible viral infections (hepatitis B,C, and human immunodeficiency virus) [6]. The rate ofoccupational blood exposures for prehospital providers isestimated to be in excess of 49,000 per annum, whichincludes over 10,000 cases of needlestick injuries [7].
Most opioid overdoses occur in a prehospital setting,arising from unintentional self-poisoning [8]. Emergencymedical services (EMS) providers are usually the patient’sfirst contact with the health service. In many jurisdictionsworldwide, naloxone is used by EMS personnel to treat

2 Emergency Medicine International
opioid overdoses [9–13]. In Ireland, the prehospital emer-gency medical care system is regulated and governed by thePre-Hospital Emergency Care Council [14]. EMS personnel(paramedics and advanced paramedics) are permitted toadminister naloxone to treat a suspected opioid overdosein accordance with national clinical practice guidelines[15]. However, there is currently no provision for the useof IN naloxone in prehospital medicine in Ireland. Theintroduction of an alternative needle-free route of naloxonedelivery that is fast acting, effective, and safe would bebeneficial to patients and EMS providers.
Intranasal administration of naloxone obviates the needfor IV catheter placement in high-risk patients and couldreduce some of these associated risks. The nasal route is pre-sented as an alternative for drug delivery since the rich vas-cular plexus of the nose offers a direct route for medicationentry into the bloodstream [5, 8]. Also, especially relevant toprehospital clinical practice, the nasal cavity is a readily acces-sible and pain-free site for use in any emergency situation.
While the bioavailability of IN naloxone reaches almost100% that of IV naloxone and achieves peak plasmaconcentration in 3 minutes in animal studies [16], thereis a lack of human pharmacokinetic data. Previous studieshave demonstrated that IN naloxone is effective and safewhen used to treat an opioid overdose [9–11]. Several non-randomised pre-hospital studies have also shown that theoverall time interval from patient contact to patient recoveryis similar for IN and IV naloxone [12, 13].
The primary aim of this study is to compare the timetaken to administer a medication via the IN and IV routes. Asecondary aim is to assess the end-user satisfaction for bothroutes in a cohort of advanced paramedic trainees.
2. Methods
2.1. Study Setting and Design. This was a randomisedcontrolled trial that took place at the National AmbulanceServices College in Dublin, Ireland. A class of 18 advancedparamedic trainees, registered with a University CollegeDublin training programme, were asked to participate ina classroom-based study that was used to simulate a real-life patient encounter of an opioid overdose. Standardisedformal IV cannulation techniques had previously beentaught using a mannequin and each trainee had completeda five-week hospital placement during which time super-vised IV cannulations were performed on patients. Eachtrainee also received formal instruction regarding the useof a mucosal atomizer device (MAD) to deliver intranasalmedication. This is a single-use atomizer device with aluer-lock connector for delivery of a measured dose of INmedication via a syringe (Figure 1).
Block randomisation was used to assign trainees equallyto each study group—9 trainees were allocated to group A(IN) and the remainder was assigned to group B (IV).
The study was designed to mirror a real-life patientencounter. A table was arranged at bed height with amannequin for IN administration and a phlebotomy arm forIV cannulation (Figure 2). A standard advanced paramedickit bag, containing the MAD, a 3 ml plastic syringe, a 21G
Figure 1: Mucosal atomizer device for delivery of intranasalmedication (reproduced with permission from Wolfe Tory Medical,Inc., USA).
hypodermic needle, and a 20G IV cannula in a clear plasticpouch was placed beside the table. A clear glass vial, filledwith 1 ml of saline solution was used for both groups.Trainees were instructed to administer the medication as perthe route indicated at randomisation. A research assistantwho was not involved in the study design or result interpre-tation recorded the time taken for each trainee to preparethe medication and prepare the route of administration (i.e.,insert a cannula or check the nose). The clock was started asthe trainee opened the kit bag and stopped as the medicationwas delivered. Each trainee was permitted to complete thetask once only.
2.2. Outcome Measures. The primary outcome measure inthis study was the time taken by trainees for completion ofthe task in group A (IN) and group B (IV) as detailed above.
Practitioner satisfaction with each route of medicationadministration was the secondary outcome measure. Follow-ing completion of the procedure, each trainee was asked tofill out a 5-point Likert rating scale. This was used to measurethe trainees’ satisfaction in terms of user-friendliness andsafety of the procedure that they had been assigned to. Aprocedure was defined as “safe” if the trainee did not expectto encounter a blood exposures or needlestick injury whileusing that technique in a real-life scenario.
2.3. Data Analysis. Descriptive statistical analysis wasapplied to the data in this study (mean, median, standarddeviation and mean time difference with 95% confidenceintervals, CI). The data was found to follow a normaldistribution using the Anderson-Darling test; thus, thedifference in mean times for both groups was comparedusing a two-tailed student’s t-test. A P-value < 0.05 waschosen as significant.
3. Results
18 advanced paramedic trainees participated in this study—15 males and 3 females. The mean age of participants was

Emergency Medicine International 3
(a)
(b)
Figure 2: Materials used to carry out classroom-based study in theNational Ambulance Services Centre.
50.5 years and the age range was 32 years to 57 years. Table 1compares the route of medication administration and timetaken for each advanced paramedic trainee.
The mean time taken for group A to deliver medicationvia the IN route was 87.1 seconds. The standard deviationwas 20.35 (range 57.4 to 114.9 seconds). The mean timetaken for group B to insert a cannula and administer themedication IV was 178.2 seconds. The standard deviationwas 36.71 (range 133.7 to 240.6 seconds). There was adifference in mean delivery times of 91.1 seconds (P ≤0.0001) with 95% CI ranging from 55.2 seconds to 126.9seconds. Thus, there was a statistically significant differencein the primary outcome measure in this study in favour of INmedication administration.
Table 1: Advanced paramedic trainees shown by time taken formedication delivery.
TraineeGroup A
IN (s)Group B
IV (s)
1 185.4
2 159.4
3 240.6
4 103.8
5 103.4
6 133.7
7 231.6
8 152.2
9 95.7
10 82.3
11 114.9
12 186.2
13 95.3
14 68.8
15 62.3
16 161
17 153.4
18 57.4
Eighty-nine percent (8 out of 9) of trainees from group A“strongly agreed” that the IN technique was both easy to useand safe to use. Most trainees from group B regarded the IVtechnique as easy to use but most “disagreed” (67%) that thetechnique was safe to use (Figures 3(a) and 3(b)). All traineescompleted the study and no adverse incidents occurred.
4. Discussion
The findings of this study show that it is faster to delivera medication via the IN route than the IV route whenadministered by a cohort of advanced paramedic trainees. Toour knowledge, no study has yet attempted to quantify theactual time difference that occurs as a result of the route ofadministration used to deliver naloxone. In this study, the INroute was also preferred over the IV route, both in terms ofease of use and safety profile.
Two randomised controlled trials have compared thetime taken to achieve adequate patient response when usingIN and IM naloxone [9, 10]. A positive clinical response inboth of these studies was defined as the time taken to regaina respiratory rate of 10 breaths per minute. Patients in theinitial study had a slower response when given IN naloxone(IN 8 minutes versus IM 6 minutes, P = 0.006) [10] whilemean response times were similar in the more recent study(IN 8.0 minutes, IM 7.9 minutes, difference 0.1, 95% CI−1.3to 1.5) [9]. A more concentrated solution of IN naloxone wasspecifically manufactured for use in the later study—this wasthought to account for the difference in response time for INnaloxone between these studies.

4 Emergency Medicine International
0123456789
Group A Group B
EasyNot easy
(a)
0123456789
Group A Group B
SafeNot safe
(b)
Figure 3: (a) Advanced paramedic trainee response to question-naire regarding ease of use of IN or IV delivery. (b) Advancedparamedic trainee response to questionnaire regarding safety of useof IN or IV delivery.
Additional nonrandomised studies have shown thatthe overall time intervals from initial patient contact byparamedics to patient clinical response (defined as anincrease in respiratory rate and Glasgow Coma Score) werenot prolonged when using IN naloxone compared with IVnaloxone [12, 13]. The authors concluded that any delay inthe clinical response to IN naloxone is compensated for bythe time taken to establish IV access.
A mean time difference of 91.1 seconds was recordedin this study with the 95% confidence interval rangingfrom 55.2 seconds to 126.9 seconds. A clinically significantdifference in patient response times has previously beendefined as 1 minute, based on respiratory depression andoxygen desaturation that may occur after this time [9]. Thus,the use of the IN route of delivery of naloxone to treat anopioid overdose may have an important impact on successfulpatient resuscitation in a real-life clinical scenario.
The results of this study also concluded that therewas high level of practitioner satisfaction among advancedparamedic-trainees in relation to the ease of use of theIN route of administration. In this cohort, 89% of usersfound the IN route easy to use. Paramedics in other studiesperceived IN naloxone to be less effective than its parenteralcounterpart [11]. It has been reported that there is apreference by paramedics toward one route of delivery oranother based on personal experience and not on the level
of patient intoxication [11]. However, advanced paramedictrainees in this study expressed a clear preference for the INroute.
In the United States (US), in 2000, the Needlestick Safetyand Prevention Act was enacted into federal law [17]. Underthis new legislation, the Occupational Safety and HealthAdministration established requirements for all employersto reduce percutaneous injuries in at-risk employees fromcontaminated sharps by using safety-engineered medicaldevices [18]. Prior to this, the rate of needlestick injury wasestimated at 378,000 to 756,000 incidents per annum [19].Since its introduction, there has been a steady decline in theannual rate of percutaneous injuries in the US, for example,in 2001, a reduction of almost 38% was reported amongsthospital employees [20]. The results of this study show thatmost advanced paramedic trainees perceived the IN route(89%) to be safer than the IV route of administration (33%).
Thus, IN naloxone is proposed as one such needle-freeinitiative that may reduce exposure of EMS personnel toblood-borne viruses, when treating high-risk patients withan opioid overdose.
5. Limitations
The limitations of this study include its small sample size(n = 18) and that it lacked blinding. The small sample sizewas due to the availability of advanced paramedic traineesthat were enrolled in the teaching programme at the time ofthe study. Also, the participants were advanced paramedictrainees and may not yet have sufficient experience in IVcannulation techniques, which may have increased the timetaken to gain IV access in some cases. Finally, this was aclassroom-based study designed to simulate real-life events.In clinical practice, a field-based patient encounter may haveother confounding patient and environmental variables thatcould potentially affect the outcomes.
6. Conclusion
This study demonstrates that, amongst advanced paramedic-trainees, the IN route of medication administration issignificantly faster, better accepted, and perceived to be saferthan using an IV route of administration. The authorstherefore, propose that this needle-free route of medicationadministration be employed more frequently when treatinghigh-risk patients with an opioid overdose.
Conflict of Interests
The authors declare no conflict of interests.
Acknowledgments
The authors would like to thank the staff and students (class12) of the Centre for Emergency Medical Science, UniversityCollege Dublin, Ireland and the National Ambulance Ser-vices College, Dublin, Ireland. We are also grateful to NiallMcDermott, Centre of Business Analytics, University College

Emergency Medicine International 5
Dublin, Ireland and Niamh Cummins, Research Manager,Centre for Prehospital Research, Graduate Entry MedicalSchool, University of Limerick, Ireland.
References
[1] “Drug-related deaths and deaths among drug users inIreland—2009 figures from the National Drug-Related DeathsIndex,” Health Research Board, 2011.
[2] “The state of the drugs problem in Europe,” EuropeanMontoring Centre for Drugs and Drug Addiction, 2011.
[3] S. Okie, “A flood of opioids, a rising tide of deaths,” The NewEngland Journal of Medicine, vol. 363, no. 21, pp. 1981–1985,2010.
[4] A. Dahan, L. Aarts, and T. W. Smith, “Incidence, reversal,and prevention of opioid-induced respiratory depression,”Anesthesiology, vol. 112, no. 1, pp. 226–238, 2010.
[5] T. R. Wolfe and T. Bernstone, “Intranasal drug delivery: analternative to intravenous administration in selected emer-gency cases,” Journal of Emergency Nursing, vol. 30, no. 2, pp.141–147, 2004.
[6] J. M. Weber, K. L. Tataris, J. D. Hoffman et al., “Can nebulizednaloxone be used safely and effectively by emergency medicalservices for suspected opioid overdose?” Prehospital EmergencyCare, vol. 16, no. 2, pp. 289–292, 2012.
[7] J. K. Leiss, J. M. Ratcliffe, J. T. Lyden et al., “Blood exposureamong paramedics: incidence rates from the national study toprevent blood exposure in paramedics,” Annals of Epidemiol-ogy, vol. 16, no. 9, pp. 720–725, 2006.
[8] D. Kerr, P. Dietze, and A. M. Kelly, “Intranasal naloxone forthe treatment of suspected heroin overdose,” Addiction, vol.103, no. 3, pp. 379–386, 2008.
[9] D. Kerr, A. M. Kelly, P. Dietze, D. Jolley, and B. Barger,“Randomized controlled trial comparing the effectivenessand safety of intranasal and intramuscular naloxone for thetreatment of suspected heroin overdose,” Addiction, vol. 104,no. 12, pp. 2067–2074, 2009.
[10] A. M. Kelly, D. Kerr, P. Dietze, I. Patrick, T. Walker, and Z.Koutsogiannis, “Randomised trial of intranasal versus intra-muscular naloxone in prehospital treatment for suspectedopioid overdose,” Medical Journal of Australia, vol. 182, no. 1,pp. 24–27, 2005.
[11] M. A. Merlin, M. Saybolt, R. Kapitanyan et al., “Intranasalnaloxone delivery is an alternative to intravenous naloxonefor opioid overdoses,” The American Journal of EmergencyMedicine, vol. 28, no. 3, pp. 296–303, 2010.
[12] T. M. Robertson, G. W. Hendey, G. Stroh, and M. Shalit,“Intranasal naloxone is a viable alternative to intravenousnaloxone for prehospital narcotic overdose,” Prehospital Emer-gency Care, vol. 13, no. 4, pp. 512–515, 2009.
[13] E. D. Barton, C. B. Colwell, T. Wolfe et al., “Efficacy ofintranasal naloxone as a needleless alternative for treatmentof opioid overdose in the prehospital setting,” Journal ofEmergency Medicine, vol. 29, no. 3, pp. 265–271, 2005.
[14] Pre-Hospital Emergency Care Council, http://www.pheccit.ie.[15] Pre-Hospital Emergency Care Council, Clinical Practice
Guidelines, http://www.phecit.ie/DesktopDefault.aspx?tabin-dex=0&tabid=1117.
[16] A. Hussain, R. Kimura, C. H. Huang, and T. Kashihara,“Nasal absorption of naloxone and buprenorphine in rats,”International Journal of Pharmaceutics, vol. 21, no. 2, pp. 233–237, 1984.
[17] “Needlestick Safety and Prevention Act of 2000,” 2000, pp.106–430.
[18] Occupational Safety and Health Administration (OSHA),“Occupational exposure to bloodborne pathogens, needlestickand other sharps injuries, final rule,” Occupational Safety andHealth Administration (OSHA), Department of Labor, FedRegister, pp. 5318–5325, 2001.
[19] K. Henry and S. Campbell, “Needlestick/sharps injuries andHIV exposure among health care workers. National estimatesbased on a survey of U.S. hospitals,” Minnesota Medicine, vol.78, no. 11, pp. 41–44, 1995.
[20] E. K. Phillips, M. R. Conaway, and J. C. Jagger, “Percutaneousinjuries before and after the Needlestick Safety and PreventionAct,” The New England Journal of Medicine, vol. 366, no. 7, pp.670–671, 2012.

Hindawi Publishing CorporationEmergency Medicine InternationalVolume 2012, Article ID 949275, 10 pagesdoi:10.1155/2012/949275
Review Article
Avoiding Misdiagnosis in Patients with Neurological Emergencies
Jennifer V. Pope and Jonathan A. Edlow
Department of Emergency Medicine, Harvard Medical School, Beth Israel Deaconess Medical Center, Boston, MA 02215, USA
Correspondence should be addressed to Jennifer V. Pope, [email protected]
Received 8 March 2012; Accepted 11 June 2012
Academic Editor: Oliver Flower
Copyright © 2012 J. V. Pope and J. A. Edlow. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Approximately 5% of patients presenting to emergency departments have neurological symptoms. The most common symptomsor diagnoses include headache, dizziness, back pain, weakness, and seizure disorder. Little is known about the actual misdiagnosisof these patients, which can have disastrous consequences for both the patients and the physicians. This paper reviews theexisting literature about the misdiagnosis of neurological emergencies and analyzes the reason behind the misdiagnosis by specificpresenting complaint. Our goal is to help emergency physicians and other providers reduce diagnostic error, understand how theseerrors are made, and improve patient care.
1. Introduction
Approximately 5% of emergency department (ED) patientspresent with neurological symptoms [1]. The most commonsymptoms or diagnoses that these patients have are headache,dizziness, back pain, weakness, and seizure disorders [2–6]. In recent years, improved time-dependent treatmentsfor patients with acute neurological emergencies have beendeveloped, increasing the importance of a rapid and accu-rate diagnosis. Underdiagnosis may have disastrous conse-quences. Conversely, overtesting leads to inefficient resourceutilization that is undesirable for both economic and medicalreasons.
2. Methods
A PubMed search on February 8, 2012 for the intersectionof “misdiagnosis” and “neurological emergency” as title orabstract words resulted in 88 results. In addition to thisliterature review, we will incorporate experience from over 30years of ED clinical practice, teaching medical students, andresidents, over a decade of evaluation of medicolegal cases,and analyzing diagnostic errors committed by our colleaguesand ourselves in peer review.
We review the existing literature about misdiagnosis ofnontraumatic neurological emergencies in general, and then
by specific presenting complaints. We conclude by analyzingthe reasons for misdiagnosis. Our goals are to help emer-gency physicians (EPs) and other front-line clinicians reducemisdiagnosis of patients with neurological emergencies andto be hypothesis generating so that we can better study andunderstand misdiagnosis in these patients and to improvepatients’ clinical outcomes.
3. Results
3.1. General Studies about Misdiagnosis of Neurological Emer-gencies. Few high-quality data on the subject of ED mis-diagnosis of patients with neurological emergencies exist.Most papers on misdiagnosis of patients with neurologicalemergencies focus on patients with a particular diagnosis orpresenting symptom. Only a few analyze the general topicof all-comers with neurological symptoms [2–4]. There aremethodological problems with all of these articles. The EP’sdiagnosis is made earlier in a patient’s course. Therefore,less historical information is usually available, the naturalcourse of the disease process is less well defined, and almostalways, fewer results of diagnostic testing are available. Theprimary job of the EP is to ensure clinical stability and properdisposition of a patient, both of which are possible withoutnecessarily making a specific etiologic diagnosis. Therefore,EP’s charted diagnosis is often a tentative one, or even simply

2 Emergency Medicine International
a repetition of the major symptom or sign. Neurologists onthe other hand appropriately try to make a specific diagnosis.
For all these reasons, the comparisons being made are notequivalent. In addition, one must account for the underlyinginfrastructure of emergency services where the study wasdone. Some data originates from Europe where patients withacute neurological emergencies are often triaged directly toneurologists or the “EP” is actually a prehospital provider.The training of an EP differs across these locales.
Another limitation of all the studies is that they onlyexamine those patients whom the EP decided to consultthe neurologist; many patients with clear-cut diagnoses(e.g., peripheral 7th nerve palsy or benign paroxysmalpositional vertigo (BPPV)) may have been well managedwithout neurological consultation. Thus, the frequency ofmisdiagnosis of patients who did not have a neurologyconsultation is unknown. The ideal study would comparediagnostic accuracy of similar patients at the same phase oftheir care and using the same diagnostic information. Ofcourse it is very unlikely that such a study will ever be done.
A frequently cited article by Moulin and colleagues triedto assess the impact of neurology consultants on the outcomeof 1679 patients with neurological emergencies in a largeFrench ED [4]. Neurology consults were obtained in 14.7%of all patients. They found that there was a complete changein diagnosis in 52.5% of cases. They included both falsepositive (e.g., the EP diagnosed stroke, but the patient had atumor) and false negative (e.g., EP diagnosed benign vertigobut the patient had a stroke) diagnoses. By design, the EPswere blinded to the study that the neurologists had plannedand executed, clearly introducing potential bias. Moreimportantly, the neurologists’ diagnoses were made afteraccess to neurological tests such as computed tomography(CT), magnetic resonance imaging (MRI), lumbar puncture(LP), electroencephalogram (EEG), and others, which “couldnot have been previously conducted by the ER team.” It ishardly surprising that many diagnoses would change basedon adding all of those diagnostic modalities to the historyand physical examination. Finally, the training of theseemergency physicians is not specified. These methodologicalflaws make this article irrelevant to modern EM practice, atleast in North America.
In a large Canadian ED, Moeller and colleagues studied493 patients with neurological emergencies who had a neu-rologist consult in the ED [3]. In 60.4% of cases, the ED diag-nosis was the same as the final diagnosis. In 19.1% of cases,there was frank disagreement and in another 16.6%, therewas “significant uncertainly” between the two diagnoses.Importantly, the “gold standard” diagnosis for patients whowere admitted or had neurologic followup was the finalhospital discharge diagnosis and the ultimate outpatientneurological diagnosis respectively. When they compared theconsulting ED neurologist’s diagnosis with the final diagno-sis, there was agreement in 80% of cases. Some of the patientswere referred by family practitioners or other hospitals.The investigators found that diagnoses made by EPs weremore likely to be concordant with the final diagnoses thancompared with the ones made by the other sources. The vastmajority of the diagnostic error was over-diagnosis.
Two other studies did not so much compare EP versusneurologists’ diagnoses, as categorize the types of EDneurological emergencies [2, 5]. In all studies of emer-gency neurological consultations, stroke, headache disorders,seizures, and dizziness make up a large majority of thepatients [2–5, 7]. In Hansen’s study, which analyzed 500neurology consultations at a tertiary U.S. academic hospital,4.8% of total ED patients had a neurology consultation (1/3of the number in the French study). The mean length ofstay for those patients was 7.4 hours (significantly longerthan for the average ED patient—4.9 hours) and remarkablysimilar to the “just under 8 hours” in the Canadian study.In the latter study, it is interesting to note that patientswith diagnostic ambiguity stayed in the ED much longerthan those where there was either agreement or disagreement(between consulter and consultant) about the diagnosis.
Although all these studies have limitations, there isa common theme that runs through them. Diagnosis ofpatients with neurological emergencies is imperfect. Thereis significant underdiagnosis (which threatens patient safety)and overtesting (which wastes resources). Patients withstroke, dizziness, headache, and seizures are the mostcommon sources for these errors. In a study of unplannedED return visits, many of which were due to misseddiagnoses, headache and vertigo were among the mostcommon presenting symptoms [8]. Apart from the studiesdiscussed above, most others have analyzed misdiagnosis byeither specific presenting symptoms (e.g., headache) or byspecific diagnosis (e.g., SAH).
3.2. Headache. Headache accounts for roughly 2% of EDvisits, of which only a very small percentage have seri-ous secondary causes [9]. This “needle in the haystack”phenomenon may lead clinicians to not consider serioussecondary causes. Deciding which patients to investigatebeyond clinical evaluation can be difficult; history andphysical examination must focus on uncovering “red flags”that suggest the need for further testing [10].
Much of the literature about misdiagnosis of headachefocuses on subarachnoid hemorrhage (SAH) [11–13]. Whileolder literature showed a misdiagnosis rate from 12–25%, thelatest data based on misdiagnosis restricted to the ED putsthat figure at 5% [13]. Recurring reasons for misdiagnosisinclude not considering the full spectrum of presentations,not following an algorithmic workup and not understandingthe limitations of the tests in that workup [11, 12].
Regarding presentation, not all patients with SAH have atruly abrupt onset of their headache [14]. In some patients,the headache improves after analgesics including triptans[15]. Some patients present with prominent vomiting orfever and neck pain or with hypertension, each of which candivert the physician’s diagnosis to other less serious problemssuch as gastroenteritis, viral syndrome, or hypertensive crisis[11, 12]. Patients with SAH do not necessarily “look ill,” haveany neurological deficits or meningism.
Even in the less acuity-skewed population of a neurologypractice, some argue for a lower threshold for imaging inpatients with new-onset headache [16]. This is probably

Emergency Medicine International 3
even more important in an ED practice, where the incidenceof secondary causes may be higher. In ED populations,patients with thunderclap headache have an incidence ofSAH of between 8–16% [11, 14, 17]. In one large seriesof misdiagnosed SAH, failure to do a CT scan was themost common error [18]. However, a negative CT may notexclude SAH, especially if performed after 6 hours fromheadache onset, and if a CT shows findings of chronicsinusitis, physicians may inappropriately stop the work-upand diagnose sinusitis as a cause of an acute headache, whichis actually very uncommon [17, 19, 20].
It is not surprising that patients with less common causesof headache may be initially misdiagnosed. Most patientswith headache due to a brain tumor have no distinguishingpain characteristics [21, 22], although persistent vomitingwith headache, especially if associated with lethargy, sug-gests obstructive hydrocephalus [23]. Patients with otheruncommon causes of headache, such as cerebral venous sinusthrombosis (CVST) and cervicocranial arterial dissectionsare frequently misdiagnosed on the first physician encounter.These problems may also present with isolated headachewithout specific qualities in patients without risk factors [24,25]. For these diagnoses and other uncommon ones, the issueof diagnosing a rare condition without major distinguishingfeatures presents obvious difficulties.
3.3. Dizziness. As with headache, dizziness has both benignand serious causes that can be difficult to distinguish fromone another. Diagnosis of the dizzy patient is inherentlyfraught with problems. The diagnostic algorithms that doc-tors are taught may be flawed. Increasing evidence suggeststhat the traditional “symptom quality” approach (“what doyou mean by “dizzy”?”) is less effective that a new “timingand triggers” approach, in which the physician asks aboutthe temporal characteristics of the symptoms [26–28]. Datasuggests that whether the patient uses the word “vertigo” or“spinning” versus “dizzy” or “lightheaded” is not so useful indetermining etiology. “Vertigo” versus nonspecific dizzinessdoes not help predict etiology in dizzy patients [29, 30]. Forexample, patients with BPPV often use nonspecific (non-vertigo) descriptors for their symptoms [31] and patientswith clear-cut cardiac causes of dizziness often complain of“vertigo” [32].
Because of the prevailing paradigm, EPs may have anoverly generalized approach to dizzy patients [28]. There isalso a significant overlap between the presentations of benign(vestibular neuritis and labyrinthitis) from serious (cerebel-lar and brainstem stroke) presentations [33, 34]. Deficits inphysician knowledge may also contribute, for example, doc-umentation of nystagmus is often inaccurate [35]. Finally,lack of understanding of the limitations of neuroimaging isanother issue. Some EPs incorrectly believe in the sensitivityof CT to exclude posterior circulation stroke [28], which mayalso be undetected by MRI in the first 48 hours [33].
Neurologists may also have difficulty diagnosing dizzypatients in the ED. Royl reported on 475 patients seen ina German neurology ED staffed by neurologists. Of the124 patients for whom followup was available, 43% of ED
diagnoses were “corrected” [36]. Six percent of the patientsdiagnosed with benign conditions were changed to seriousones and 23% of the serious ones were reversed to benign.In a California study of ED patients discharged with an ICD-9 code compatible with dizziness, there was an increase inthe incidence of adverse cerebrovascular events in the next30 days, suggesting that an important diagnosis had beenmissed [37].
The most feared misdiagnosis of dizzy patients is stroke.These are usually ischemic strokes of the brainstem andcerebellum. In one series of 240 consecutive cerebellarstrokes, 10% presented as an acute vestibular syndrome(AVS) suggesting a peripheral cause [34]. Nearly all ofthese patients had posterior inferior cerebellar artery strokes.Patients with misdiagnosis may have poor outcomes dueto posterior fossa edema and brainstem compression [38].Distinguishing stroke from benign peripheral causes iscritical, not just to treat the acute complications, but also toevaluate and treat the underlying vascular lesion in order toprevent a second event [39].
3.4. Back Pain. Along with headache and dizziness, backpain is very common and most patients have benign, self-limited causes. With back pain, there are fewer “needles”in a larger “haystack.” Common causes of cord or caudaequina compression include herniated disk, tumor, abscess,and hematoma. In primary care practices, all four of theseetiologies amount to roughly 1% of patients with backpain [40]. Diagnoses generally require MRI, thus settingup the classic tension between resource utilization versuspatient outcomes [40]. Surprisingly, few data exist aboutprevalence in the ED, although it is likely higher due toskewed acuity. Red flags include new pain in patients >age 50 years, a history of cancer, fever, weight loss, animmunocompromised state, intravenous drug use, recentbacteremia or urinary tract infection, pain that is worse withrest or at night, sphincter symptoms, bilateral sciatica, failureto improve over weeks, anticoagulation, and recent spinalprocedure [41]. Some patients have no identifiable red flags.
Cauda equina syndrome (CES) can be misdiagnosedand/or lead to malpractice claims because of inadequatehistory, physical examination, or communication betweenphysicians and between physicians and nurses [42]. In onesmall series of 32 patients with CES, fewer than 20%presented with the classic presentation of bilateral sciatica,leg weakness, saddle anesthesia, and sphincter dysfunction[43]. The most common reason for misdiagnosis in thatseries was failure to consider the diagnosis. In a retrospectivestudy of 23 patients with suspected CES, the diagnostic accu-racy of individual findings of urinary retention, frequency,incontinence, or altered urinary or perineal sensation rangedfrom 57–65 percent [44]. In another retrospective study of58 consecutive patients of suspected CES, having 2 of thefollowing 3 findings (bilateral sciatica, subjective urinaryretention, or rectal symptoms) increased the likelihood of apositive MRI 48 folds [45].
Another finding that is often ignored is ataxia or new fre-quent falls. In a study of 63 patients with nontraumatic cord

4 Emergency Medicine International
compression or CES, nearly one in four patients had ataxia orgait difficulty with neither sensory nor motor findings [46].For spinal epidural abscess (SEA), the incidence of the typicaltriad of back pain, fever, and neurological deficit is low [47–49]. For all these reasons, misdiagnosis or delayed diagnosisis common [47, 50, 51].
Some algorithms include measuring inflammatorymarkers such as the erythrocyte sedimentation rate (ESR)or C-reactive protein (CRP). Sensitivity for an ESR(>20 mm/hour) in infectious causes of cord or caudaequina compression such as SEA or vertebral osteomyelitis,range from 76–95%; the corresponding figures for CRP are82–98% [41, 52, 53]. For neoplastic causes, the sensitivity ofESR (>20 mm/hour) is 78% [54]. For the ESR, increasing thethreshold value increases specificity at the cost of sensitivity.
MRI with gadolinium is the test of choice for most ofthese problems [50, 55]. A significant diagnostic issue isthat in many practice settings, obtaining an urgent MRIcan be difficult or impossible. In the absence of a strictdiagnostic algorithm that forces the clinician to get the MRI,even if that requires a transfer, the lack of availability of thediagnostic gold standard may lead to misdiagnosis. Both SEAand epidural tumor often affect multiple areas of the spine;therefore, it is important to decide which part of the spineto image. Some experts recommend that the entire spineshould be imaged [55]. Finally, there are issues of resourceutilization; in one study of 106 patients undergoing MRI forpossible SEA, only 7 were positive [56].
3.5. Weakness. The majority of patients presenting to anED with generalized weakness have a variety of “toxic-metabolic” problems including electrolyte abnormalities anddehydration, medication side effects, and systemic infections.Acute neurological causes of generalized weakness includeuncommon diagnoses such as Guillain-Barre syndrome(GBS), transverse myelitis, myasthenia gravis, and periodicparalysis, as well as rarer conditions such as tick paralysis,botulism, and others.
Misdiagnosis of GBS is common [57, 58]. In a series of 20ED cases, most patients complained of weakness but somepresented with paresthesia [57]. 15 of the 20 patients wereincorrectly diagnosed on their first ED visit. Four patientsinitially presented with sensory symptoms. Six of the 20had normal cerebrospinal fluid (CSF). The notion that theCSF protein is always elevated is wrong; normal CSF proteinis common in the first week of GBS [59]. Misdiagnosis ofLambert-Eaton syndrome is also common [60]. Similarlywith myasthenia gravis (MG), the mean time to correctdiagnosis is over a year [61]. The variability of specificsymptoms and their timing makes diagnosing MG difficult.Therefore, to diagnose MG in the ED, it is essential to knowthe full spectrum of possible presentations [62]. In transversemyelitis, asymmetric cord involvement can lead to atypicalpresentations that make diagnosis more difficult [63]. Unlessone checks the serum potassium at the time of symptoms,periodic paralysis may be missed. In very rare conditionssuch as botulism and tick paralysis, initial misdiagnosis isquite common [64, 65].
Serious misdiagnosis can occur in patients with strokeand transient cerebral ischemia (TIA) who present with focalweakness. Various studies have reported that the rate of EDmisdiagnosis of stroke varies widely, from as low as 2% toas high as 56% [66–72]. To some extent, the variation relatesto study design. The two most recent North American studiesfound rates of misdiagnosis of roughly 10% [69, 70]. Currentdiagnostic scoring systems for ischemic stroke emphasizelateralizing motor findings [72–74]. Factors associated withstroke misdiagnosis include young age, posterior circulationor sensory symptoms, and lack of lateralizing weakness [38,75, 76]. Some stroke patients have NIH stroke scores ofzero [77]. Many of the patients in that study had posteriorcirculation strokes. Finally, physicians must understand thatsome strokes, even of the anterior circulation, presentwith atypical symptoms like neuropsychiatric symptoms orabnormal movements at stroke onset [78].
Diagnosis of TIA is more difficult because most TIApatients are neurologically intact by the time they are in theED. An early study found a misdiagnosis rate by the emer-gency physician of 6% [79]. A major limitation of this studyis that neurologists made their diagnosis by reviewing the EDchart, not by independent clinical evaluation. Another studyfound a misdiagnosis rate by EPs of 60%, with factors leadingto misdiagnosis including gradual onset of symptoms, priorsimilar episodes, and nonspecific symptoms [80]. The mostrecent and methodologically sound study found an EDmisdiagnosis rate of 36% [81]. It also showed that thepresence of headache, involuntary movements, and dizzinesswere all associated with a non-TIA diagnosis.
Apart from the aforementioned studies of SAH, therehas not been much systematic study of misdiagnosis ofintracerebral hemorrhage (ICH). Both CT and MRI are verysensitive for ICH; therefore, when physicians perform brainimaging in patients with weakness, they will find ICH whenit exists. Although ICH often presents more dramaticallythan ischemic stroke, there is significant overlap. It iscertainly possible that patients who are not imaged will bemisdiagnosed.
3.6. Seizures. As with TIA, the diagnosis of a seizure oftendepends entirely upon the history of an event that thephysician has not witnessed. Therefore, it is important to tryto obtain information from any witnesses of the event, andto gather what data one can from the physical examinationto distinguish the causes of these transient episodes of lossof consciousness. The most common issue is distinguishingsyncope from seizure, but one must also separate trueseizures from pseudoseizures (also referred to as psychogenicseizures and nonepileptic attack disorder). Of these threeconditions, syncope is by far the most common.
In one review, the misdiagnosis rate overall for seizuresin both children and adults ranged from 5–30% [82]. Inadult patients incorrectly diagnosed with seizure, the mostcommon final diagnoses were syncope and pseudoseizures[82, 83]. In children, various benign paroxysmal disorderssuch as breathing holding spells and night terrors werethe most common final diagnoses [82]. The source of

Emergency Medicine International 5
misdiagnosis was not entirely from the ED. It is importantto note that electroencephalography (EEG) is not specific forseizures and lacks sensitivity. That is to say, an abnormal EEGdoes not exclude pseudoseizures and a normal EEG does notexclude true seizures or confirm pseudoseizures [84–87].
There are several characteristics that help emergencyclinicians to distinguish between syncope, epileptic seizures,and pseudoseizures. Syncope may have a prodromal sensa-tion of warmth, lightheadedness, sweating, and facial pallor,and is often precipitated by various triggers. The eventstarts rapidly and recovery is prompt. In cardiac causesof syncope, palpitations or chest pain may occur together.Importantly, however, “convulsive syncope,” in which thefaint is accompanied by some tonic-clonic jerking dueto brain hypoperfusion is common [85, 88, 89]. Tonguebiting may occur but it is usually at the tip of the tongue[90]. Urinary incontinence is unusual but may also occur[85, 86].
Patients with true seizures often have a preceding auraor repetitive movements (chewing or lip smacking), lateralbiting of the tongue or cheek, facial cyanosis, sphincterincontinence, head turning towards one side, and postictalconfusion that is slow to resolve [85, 90, 91]. Posteventneurological examination may show focal deficits [86].Though not extensively studied, transient anion gap acidosisis also associated with true seizure [92]. Up to 36% ofpatients with “intractable seizures” actually have pseudo-seizures [84]. Patients with pseudoseizures may show side-to-side head movements, changing symptoms if multiplespells, gradual onset and waxing and waning during thespell, rapid recovery, and bizarre movements involving theentire body without any “logical” march [86]. Tonguebiting and incontinence are less common in patients withpseudoseizures compared with true seizures [90].
In many ED patients with transient loss of consciousness,a definite diagnosis will not be possible. Coordination ofsubsequent care for testing not available in an ED suchas tilt-table testing, continuous loop ECG monitoring, orvideo-monitored 48-hour EEG testing may help to reducemisdiagnosis.
3.7. Conversion Reaction (Functional Neurological Symptoms).Conversion reactions overlap the symptom-oriented discus-sion above. The most common conversion reactions relateto weakness and seizures [93]. One report of ED patientsdiagnosed with conversion reaction who later proved tohave organic disease emphasizes that misdiagnosis oftenrelates to patients having symptoms atypical for organicdisease (e.g., “I’ve never seen anything like this before” orsymptoms being “non-anatomic”) [94]. Hoover’s sign (weakhip extension that becomes normal on testing contralateralhip flexion) was found to be moderately sensitive and veryspecific for functional weakness [95]. In the specific settingof possible ischemic stroke, it is obviously preferable to notgive thrombolytic therapy to someone who does not have astroke. However, patients with stroke mimics who are CTnegative, have never been reported to have hemorrhagiccomplications [96–98]. Although a high degree of diagnostic
accuracy is possible [99], EPs should be very hesitant to makea diagnosis of conversion reaction in the ED.
4. Discussion
Before discussing the data, it is important to acknowledgetheir limitations. The literature does not contain high-quality data on this subject, and the data derived fromour experience with quality assurance and medicolegal casereview is by definition skewed towards cases with pooroutcomes. We acknowledge that our conclusions are limitedby the weakness of the data upon which they are built;however, we believe that this is the best available analysis ofthe data.
Misdiagnosis contributes to medical malpractice in theED and patient harm [100, 101]. The underlying reasonsincluded inadequate history and physical examination, fail-ure to order and correctly interpret tests, and failure to obtaina consultation [101]. In Table 1, we have listed potentialreasons for misdiagnosis of patients with neurological emer-gencies. Researchers in the field of diagnostic error oftencharacterize errors in terms of cognitive analysis, which isuseful for research [102]. Herein, however, we will categorizereasons for error in everyday terms that average clinicianswill not only understand but also relate to.
Time pressures, frequent interruptions, and distractionsare common in the ED. For stroke, time pressures relatedto thrombolytic use force EPs to “diagnose” a stroke withinminutes of the patient’s presentation, when key historicaldetails may be unavailable. For the less common diagnoses,the “needle in the haystack” phenomenon exists. “Classic”triads and the “typical” symptoms that are emphasized inmedical education are often absent. Preconceived notionsare sometimes wrong. In addition, examining the nervoussystem is more complicated than examining the heartor lungs. Charting systems, designed to maximize billing,discourage good documentation. The best test for someconditions, MRI, is often unavailable. Incidental findings onphysical exam or imaging tests may distract and prematurelystop the workup. A false normal study (due to interpretationerror or imaging the wrong site or at the wrong time) may dothe same.
Over testing can also result in patient harm. Incorrectdiagnosis of a seizure often leads to anticonvulsant use ordriving restrictions. With respect to investigations, ED useof CT more than tripled over the period 1995–2007 [103]and interestingly there is a 3-fold variation of CT use acrossindividual physicians [104]. Apart from obvious issues ofdiagnostic accuracy, evidence is mounting about the long-term consequences of increasing radiation exposure [105].Furthermore, incidental findings drive further investigations,which may lead to adverse consequences [106].
Finally, it must be acknowledged that some degree ofmisdiagnosis is unavoidable [107]. Making every diagnosisevery time has costs. Even immediate ED neurologicalconsultation will not lead to diagnostic perfection. BothMoeller and Royl showed that neurologic evaluation in theED was still associated with some misdiagnosis [3, 36]. In

6 Emergency Medicine International
Ta
ble
1:So
me
reas
ons
for
mis
diag
nos
isin
pati
ents
wit
hn
euro
logi
cale
mer
gen
cies
.
Hea
dach
eD
izzi
nes
sB
ack
Pain
Wea
knes
sSe
izu
re
His
tory
Pati
ents
use
wor
dslik
e“m
igra
ine”
and
“sin
us
infe
ctio
n”th
atm
aym
isle
adth
eph
ysic
ian
.B
ewar
epr
evio
us
diag
nos
es;
they
mig
ht
bew
ron
g.
Th
eu
seof
the
wor
d“v
erti
go”
vers
us
oth
erdi
zzin
ess
desc
ript
ors
isn
otet
iolo
gica
llyu
sefu
l.
Pati
ents
use
wor
d“s
ciat
ica”
wh
ich
may
lead
phys
icia
ns
todi
agn
ose
scia
tica
.
Stro
kepa
tien
tsm
ayco
mpl
ain
of“c
lum
sin
ess”
or“m
yar
mfe
ltlik
ele
ad”
rath
erth
an“w
eakn
ess”
.
Pati
ent
(or
wit
nes
s)sa
ys“s
eizu
re”
afte
ra
fain
tSe
izu
repa
tien
tsof
ten
pres
ent
afte
rth
ese
izu
rew
ith
only
anal
tere
dm
enta
lsta
tus
orw
ith
apo
stic
tal“
Todd
’s”pa
raly
sis
Phy
sica
lexa
mPa
tien
tsw
ith
SAH
may
bew
ell
app
eari
ng
and
neu
rolo
gica
llyin
tact
.
Pati
ents
wit
hsm
allp
oste
rior
circ
ula
tion
stro
kes
can
mim
ica
per
iph
eral
vest
ibu
lar
pres
enta
tion
.
Pati
ents
wit
hse
riou
sca
use
sof
back
pain
can
pres
ent
wit
hou
tn
euro
logi
cald
efici
ts.
Pati
ents
wit
hst
roke
can
pres
ent
wit
hju
stab
out
any
foca
ldefi
cit
depe
ndi
ng
upo
nth
eoc
clu
ded
vess
el.
Mya
sth
enia
pati
ents
’sy
mpt
oms
wax
and
wan
e.G
BS
pati
ents
’firs
tsy
mpt
oms
may
bepu
rely
sen
sory
.
Pati
ents
may
bele
thar
gic,
but
neu
rolo
gica
llyin
tact
.
Dia
gnos
tic
test
ing
For
SAH
,CT
sen
siti
vity
isgo
odbu
tde
cays
wit
hti
me.
CT
has
poor
sen
siti
vity
for
CV
STan
ddi
ssec
tion
.
CT
isa
poor
test
for
cere
bella
ran
dbr
ain
stem
infa
rcti
on
No
MR
Iav
aila
ble
MR
Im
ust
targ
etth
eco
rrec
tse
gmen
t(s)
ofth
esp
ine.
Fals
en
orm
alC
Tin
earl
yst
roke
EE
Gof
ten
not
avai
labl
ein
the
emer
gen
cyde
part
men
t.N
otpe
rfor
min
gLP
inse
izu
repa
tien
tsw
ho
may
hav
een
ceph
alit
isor
neu
rocy
stic
erco
sis.
Pre
con
ceiv
edn
otio
ns
Hea
dach
eim
prov
edw
ith
trip
tan
sso
isn
ota
seri
ous
seco
nda
ryca
use
.
Post
erio
rci
rcu
lati
onst
roke
sar
eob
viou
sor
deva
stat
ing
even
ts
All
pati
ents
wit
hSE
Ah
ave
risk
fact
ors
orfe
ver,
orn
euro
logi
cald
efici
ts
You
ng
peop
ledo
not
get
stro
kes
Seiz
ure
s(o
rse
izu
re-l
ike
mov
emen
ts)
are
som
etim
esse
enw
ith
stro
kes.
Con
vuls
ive
mov
emen
tsar
eco
mm
onin
syn
cop
e.
CV
ST:c
ereb
ralv
enou
ssi
nu
sth
rom
bosi
s,SA
H:s
uba
rach
noi
dh
emor
rhag
e,C
T:C
AT
scan
,MR
I:m
agn
etic
reso
nan
ceim
agin
g,SE
A:s
pin
alep
idu
rala
bsce
ss.

Emergency Medicine International 7
a study of malpractice cases against neurologists, EPs werecodefendants in 44% of cases [108]. These data corroboratethe obvious conclusion that simply consulting a neurologistdoes not eliminate potential errors. Because some diagnosticuncertainly is inevitable, explicit communication betweenphysicians, physicians and patients and thoughtful coordi-nation of followup care after the ED phase become criticallyimportant.
5. Conclusions and Solutions
A full analysis of the reasons behind these potential errorsand solutions to the problems is beyond the scope ofthis review. However, several generic issues exist. Less than20% of emergency medicine residencies require a neurologyrotation [109]. Education is mostly lecture based; however,many of these lessons are best taught by studying real-lifepatients at the bedside. Important as education is, diagnosticerror is frequently not the fault of a misinformed individual.Numerous articles have addressed how to reduce diagnos-tic errors in medicine, from both practical and researchperspectives [110–117]. Some potential components to thesolution include better physician education in neurologicalemergencies that encourage detailed history-taking and sys-tematic physical examination, improved access to supportivediagnostic tests (MRI), real-time neurology consultationand communicate clearly with patients and other physicianswho will be seeing them in followup. Further well-designedstudies are needed in the area of misdiagnosis of neurologicalemergencies to improve patient care and the use of healthcareresources.
References
[1] S. R. Pitts, R. W. Niska, J. Xu, and C. W. Burt, “NationalHospital Ambulatory Medical Care Survey: 2006 emergencydepartment summary,” National Health Statistics Reports, no.7, pp. 1–38, 2008.
[2] C. K. Hansen, J. Fisher, N. Joyce, and J. A. Edlow, “Emergencydepartment consultations for patients with neurologicalemergencies,” European Journal of Neurology, vol. 18, no. 11,pp. 1317–1322, 2011.
[3] J. J. Moeller, J. Kurniawan, G. J. Gubitz, J. A. Ross, and V.Bhan, “Diagnostic accuracy of neurological problems in theemergency department,” Canadian Journal of NeurologicalSciences, vol. 35, no. 3, pp. 335–341, 2008.
[4] T. Moulin, D. Sablot, E. Vidry et al., “Impact of emergencyroom neurologists on patient management and outcome,”European Neurology, vol. 50, no. 4, pp. 207–214, 2003.
[5] T. Rizos, E. Juttler, M. Sykora, S. Poli, and P. A. Ringleb,“Common disorders in the neurological emergency room—experience at a tertiary care hospital,” European Journal ofNeurology, vol. 18, no. 3, pp. 430–435, 2011.
[6] G. Royl, C. J. Ploner, M. Mockel, and C. Leithner, “Neuro-logical chief complaints in an emergency room,” Nervenarzt,vol. 81, no. 10, pp. 1226–1230, 2010.
[7] F. A. Falco, R. Sterzi, V. Toso et al., “The neurologist in theemergency department. An Italian nationwide epidemiolog-ical survey,” Neurological Sciences, vol. 29, no. 2, pp. 67–75,2008.
[8] C. L. Wu, F. T. Wang, Y. C. Chiang et al., “Unplanned emer-gency department revisits within 72 hours to a secondaryteaching referral hospital in Taiwan,” Journal of EmergencyMedicine, vol. 38, no. 4, pp. 512–517, 2010.
[9] J. N. Goldstein, C. A. Camargo, A. J. Pelletier, and J. A. Edlow,“Headache in United States emergency departments: demo-graphics, work-up and frequency of pathological diagnoses,”Cephalalgia, vol. 26, no. 6, pp. 684–690, 2006.
[10] J. A. Edlow, P. D. Panagos, S. A. Godwin, T. L. Thomas,and W. W. Decker, “Clinical policy: critical issues in theevaluation and management of adult patients presenting tothe emergency department with acute headache,” Annals ofEmergency Medicine, vol. 52, no. 4, pp. 407–436, 2008.
[11] J. A. Edlow, A. M. Malek, and C. S. Ogilvy, “Aneurysmal sub-arachnoid hemorrhage: update for emergency physicians,”Journal of Emergency Medicine, vol. 34, no. 3, pp. 237–251,2008.
[12] J. A. Edlow and L. R. Caplan, “Avoiding pitfalls in thediagnosis of subarachnoid hemorrhage,” The New EnglandJournal of Medicine, vol. 342, no. 1, pp. 29–36, 2000.
[13] M. J. Vermeulen and M. J. Schull, “Missed diagnosis ofsubarachnoid hemorrhage in the emergency department,”Stroke, vol. 38, no. 4, pp. 1216–1221, 2007.
[14] S. H. Bø, E. M. Davidsen, P. Gulbrandsen, and E. Diet-richs, “Acute headache: a prospective diagnostic work-up ofpatients admitted to a general hospital,” European Journal ofNeurology, vol. 15, no. 12, pp. 1293–1299, 2008.
[15] J. V. Pope and J. A. Edlow, “Favorable response to analgesicsdoes not predict a benign etiology of headache,” Headache,vol. 48, no. 6, pp. 944–950, 2008.
[16] R. W. Evans and J. C. Johnston, “Migraine and medicalmalpractice,” Headache, vol. 51, no. 3, pp. 434–440, 2011.
[17] J. J. Perry, I. G. Stiell, M. L. A. Sivilotti et al., “Sensitivity ofcomputed tomography performed within six hours of onsetof headache for diagnosis of subarachnoid haemorrhage:prospective cohort study,” BMJ, vol. 343, no. 7817, 2011.
[18] R. G. Kowalski, J. Claassen, K. T. Kreiter et al., “Initialmisdiagnosis and outcome after subarachnoid hemorrhage,”JAMA, vol. 291, no. 7, pp. 866–869, 2004.
[19] N. S. Jones, “Sinus headaches: avoiding over-and mis-diagnosis,” Expert Review of Neurotherapeutics, vol. 9, no. 4,pp. 439–444, 2009.
[20] S. P. Mudgil, S. W. Wise, K. D. Hopper, C. J. Kasales, D.Mauger, and J. A. Fornadley, “Correlation between presumedsinusitis-induced pain and paranasal sinus computed tomo-graphic findings,” Annals of Allergy, Asthma and Immunology,vol. 88, no. 2, pp. 223–226, 2002.
[21] L. Valentinis, F. Tuniz, F. Valent et al., “Headache attributedto intracranial tumours: a prospective cohort study,” Cepha-lalgia, vol. 30, no. 4, pp. 389–398, 2010.
[22] C. J. Schankin, U. Ferrari, V. M. Reinisch, T. Birnbaum,R. Goldbrunner, and A. Straube, “Characteristics of braintumour-associated headache,” Cephalalgia, vol. 27, no. 8, pp.904–911, 2007.
[23] S. Shemie, V. Jay, J. Rutka, and D. Armstrong, “Acuteobstructive hydrocephalus and sudden death in children,”Annals of Emergency Medicine, vol. 29, no. 4, pp. 524–528,1997.
[24] M. G. Bousser and J. M. Ferro, “Cerebral venous thrombosis:an update,” The Lancet Neurology, vol. 6, no. 2, pp. 162–170,2007.

8 Emergency Medicine International
[25] M. R. Fusco and M. R. Harrigan, “Cerebrovasculardissections—a review part I: spontaneous dissections,” Neu-rosurgery, vol. 68, no. 1, pp. 242–257, 2011.
[26] K. A. Kerber, “Vertigo presentations in the emergencydepartment,” Seminars in Neurology, vol. 29, no. 5, pp. 482–490, 2009.
[27] D. E. Newman-Toker, “Charted records of dizzy patientssuggest emergency physicians emphasize symptom quality indiagnostic assessment,” Annals of Emergency Medicine, vol.50, no. 2, pp. 204–205, 2007.
[28] D. E. Newman-Toker, C. A. Camargo Jr., Y. H. Hsieh, A.J. Pelletier, and J. A. Edlow, “Disconnect between chartedvestibular diagnoses and emergency department manage-ment decisions: a cross-sectional analysis from a nationallyrepresentative sample,” Academic Emergency Medicine, vol.16, no. 10, pp. 970–977, 2009.
[29] K. A. Kerber, D. L. Brown, L. D. Lisabeth, M. A. Smith, andL. B. Morgenstern, “Stroke among patients with dizziness,vertigo, and imbalance in the emergency department: apopulation-based study,” Stroke, vol. 37, no. 10, pp. 2484–2487, 2006.
[30] C. S. K. Cheung, P. S. K. Mak, K. V. Manley et al.,“Predictors of important neurological causes of dizzinessamong patients presenting to the emergency department,”Emergency Medicine Journal, vol. 27, no. 7, pp. 517–521, 2010.
[31] J. Lawson, I. Johnson, D. E. Bamiou, and J. L. Newton,“Benign paroxysmal positional vertigo: clinical characteris-tics of dizzy patients referred to a Falls and Syncope Unit,”QJM, vol. 98, no. 5, pp. 357–364, 2005.
[32] D. E. Newman-Toker and C. A. Camargo, “‘Cardiogenicvertigo’—true vertigo as the presenting manifestation ofprimary cardiac disease,” Nature Clinical Practice Neurology,vol. 2, no. 3, pp. 167–172, 2006.
[33] J. C. Kattah, A. V. Talkad, D. Z. Wang, Y. H. Hsieh, andD. E. Newman-Toker, “HINTS to diagnose stroke in theacute vestibular syndrome: three-step bedside oculomo-tor examination more sensitive than early MRI diffusion-weighted imaging,” Stroke, vol. 40, no. 11, pp. 3504–3510,2009.
[34] H. Lee, S. I. Sohn, Y. W. Cho et al., “Cerebellar infarctionpresenting isolated vertigo: frequency and vascular topo-graphical patterns,” Neurology, vol. 67, no. 7, pp. 1178–1183,2006.
[35] K. A. Kerber, L. B. Morgenstern, W. J. Meurer et al., “Nys-tagmus assessments documented by emergency physicians inacute dizziness presentations: a target for decision support?”Academic Emergency Medicine, vol. 18, no. 6, pp. 619–626,2011.
[36] G. Royl, C. J. Ploner, and C. Leithner, “Dizziness in theemergency room: diagnoses and misdiagnoses,” EuropeanNeurology, vol. 66, no. 5, pp. 256–263, 2011.
[37] A. S. Kim, H. J. Fullerton, and S. C. Johnston, “Risk ofvascular events in emergency department patients dischargedhome with diagnosis of dizziness or vertigo,” Annals ofEmergency Medicine, vol. 57, no. 1, pp. 34–41, 2011.
[38] S. I. Savitz, L. R. Caplan, and J. A. Edlow, “Pitfalls inthe diagnosis of cerebellar infarction,” Academic EmergencyMedicine, vol. 14, no. 1, pp. 63–68, 2007.
[39] J. A. Edlow, D. E. Newman-Toker, and S. I. Savitz, “Diagnosisand initial management of cerebellar infarction,” The LancetNeurology, vol. 7, no. 10, pp. 951–964, 2008.
[40] R. A. Deyo and J. N. Weinstein, “Low back pain,” The NewEngland Journal of Medicine, vol. 344, no. 5, pp. 363–370,2001.
[41] B. N. Corwell, “The emergency department evaluation, man-agement, and treatment of back pain,” Emergency MedicineClinics of North America, vol. 28, no. 4, pp. 811–839, 2010.
[42] J. P. Kostuik, “Medicolegal consequences of cauda equinasyndrome: an overview,” Neurosurg Focus, vol. 16, no. 6,article e8, 2004.
[43] I. Jalloh and P. Minhas, “Delays in the treatment of caudaequina syndrome due to its variable clinical features inpatients presenting to the emergency department,” Emer-gency Medicine Journal, vol. 24, no. 1, pp. 33–34, 2007.
[44] D. A. Bell, D. Collie, and P. F. Statham, “Cauda equinasyndrome—what is the correlation between clinical assess-ment and MRI scanning?” British Journal of Neurosurgery,vol. 21, no. 2, pp. 201–203, 2007.
[45] P. M. Domen, P. A. Hofman, H. Van Santbrink, and W. E. J.Weber, “Predictive value of clinical characteristics in patientswith suspected cauda equina syndrome,” European Journal ofNeurology, vol. 16, no. 3, pp. 416–419, 2009.
[46] A. F. Dugas, J. M. Lucas, and J. A. Edlow, “Diagnosis of spinalcord compression in nontrauma patients in the emergencydepartment,” Academic Emergency Medicine, vol. 18, no. 7,pp. 719–725, 2011.
[47] R. O. Darouiche, “Spinal epidural abscess,” The New EnglandJournal of Medicine, vol. 355, no. 19, pp. 2012–2020, 2006.
[48] D. P. Davis, R. M. Wold, R. J. Patel et al., “The clinicalpresentation and impact of diagnostic delays on emergencydepartment patients with spinal epidural abscess,” Journal ofEmergency Medicine, vol. 26, no. 3, pp. 285–291, 2004.
[49] G. Pradilla, Y. Nagahama, A. M. Spivak, A. Bydon, and D.Rigamonti, “Spinal epidural abscess: current diagnosis andmanagement,” Current Infectious Disease Reports, vol. 12, no.6, pp. 484–491, 2010.
[50] E. Reihsaus, H. Waldbaur, and W. Seeling, “Spinal epiduralabscess: a meta-analysis of 915 patients,” NeurosurgicalReview, vol. 23, no. 4, pp. 175–205, 2000.
[51] H. J. Tang, H. J. Lin, Y. C. Liu, and C. M. Li, “SpinalEpidural Abscess-Experience with 46 patients and evaluationof prognostic factors,” Journal of Infection, vol. 45, no. 2, pp.76–81, 2002.
[52] M. Beronius, B. Bergman, and R. Andersson, “Vertebralosteomyelitis in Goteborg, Sweden: a retrospective study ofpatients during 1990–95,” Scandinavian Journal of InfectiousDiseases, vol. 33, no. 7, pp. 527–532, 2001.
[53] J. Chelsom and C. O. Solberg, “Vertebral osteomyelitis ata Norwegian university hospital 1987–97: clinical features,laboratory findings and outcome,” Scandinavian Journal ofInfectious Diseases, vol. 30, no. 2, pp. 147–151, 1998.
[54] R. A. Deyo and A. K. Diehl, “Cancer as a cause of back pain:frequency, clinical presentation, and diagnostic strategies,”Journal of General Internal Medicine, vol. 3, no. 3, pp. 230–238, 1988.
[55] K. Lury, J. K. Smith, and M. Castillo, “Imaging of SpinalInfections,” Seminars in Roentgenology, vol. 41, no. 4, pp.363–379, 2006.
[56] M. El Sayed and M. D. Witting, “Low yield of ED magneticresonance imaging for suspected epidural abscess,” AmericanJournal of Emergency Medicine, vol. 29, no. 9, pp. 978–982,2011.

Emergency Medicine International 9
[57] D. C. McGillicuddy, O. Walker, N. I. Shapiro, and J. A. Edlow,“Guillain-Barre syndrome in the emergency department,”Annals of Emergency Medicine, vol. 47, no. 4, pp. 390–393,2006.
[58] J. B. Winer, “Guillain-Barre syndrome,” BMJ, vol. 337, articlea671, 2008.
[59] P. A. van Doorn, L. Ruts, and B. C. Jacobs, “Clinical features,pathogenesis, and treatment of Guillain-Barre syndrome,”The Lancet Neurology, vol. 7, no. 10, pp. 939–950, 2008.
[60] M. J. Titulaer, B. Lang, and J. J. G. M. Verschuuren, “Lambert-Eaton myasthenic syndrome: from clinical characteristics totherapeutic strategies,” The Lancet Neurology, vol. 10, no. 12,pp. 1098–1107, 2011.
[61] K. Scherer, R. S. Bedlack, and D. L. Simel, “Does this patienthave myasthenia gravis?” JAMA, vol. 293, no. 15, pp. 1906–1914, 2005.
[62] P. B. Smulowitz, J. Zeller, L. D. Sanchez, and J. A. Edlow,“Myasthenia gravis: lessons for the emergency physician,”European Journal of Emergency Medicine, vol. 12, no. 6, pp.324–326, 2005.
[63] E. M. Frohman and D. M. Wingerchuk, “Transverse myelitis,”The New England Journal of Medicine, vol. 363, no. 6, pp. 564–572, 2010.
[64] M. E. S. Louis, S. H. S. Peck, D. Bowering et al., “Botulismfrom chopped garlic: delayed recognition of a major out-break,” Annals of Internal Medicine, vol. 108, no. 3, pp. 363–368, 1988.
[65] J. A. Edlow, “Tick paralysis,” Current Treatment Options inNeurology, vol. 12, no. 3, pp. 167–177, 2010.
[66] J. M. Ferro, A. N. Pinto, I. Falcao et al., “Diagnosis of Strokeby the Nonneurologist a validation study,” Stroke, vol. 29, no.6, pp. 1106–1109, 1998.
[67] R. U. Kothari, T. Brott, J. P. Broderick, and C. A. Hamilton,“Emergency physicians: accuracy in the diagnosis of stroke,”Stroke, vol. 26, no. 12, pp. 2238–2241, 1995.
[68] R. B. Libman, E. Wirkowski, J. Alvir, and T. H. Rao,“Conditions that mimic stroke in the emergency department:implications for acute stroke trials,” Archives of Neurology,vol. 52, no. 11, pp. 1119–1122, 1995.
[69] L. B. Morgenstern, L. D. Lisabeth, A. C. Mecozzi et al., “Apopulation-based study of acute stroke and TIA diagnosis,”Neurology, vol. 62, no. 6, pp. 895–900, 2004.
[70] D. E. Newman-Toker, K. A. Robinson, and J. A. Edlow,“Frontline misdiagnosis of cerebrovascular events in the eraof modern neuroimaging: a systematic review,” Annals ofNeurology, vol. 64, supplement 12, pp. S17–SS8, 2008.
[71] T. Rizos, P. A. Ringleb, H. B. Huttner, M. Kohrmann, andE. Juttler, “Evolution of stroke diagnosis in the emergencyroom—a prospective observational study,” CerebrovascularDiseases, vol. 28, no. 5, pp. 448–453, 2009.
[72] P. J. Hand, J. Kwan, R. I. Lindley, M. S. Dennis, and J. M.Wardlaw, “Distinguishing between stroke and mimic at thebedside: the brain attack study,” Stroke, vol. 37, no. 3, pp. 769–775, 2006.
[73] L. B. Goldstein and D. L. Simel, “Is this patient having astroke?” JAMA, vol. 293, no. 19, pp. 2391–2402, 2005.
[74] A. M. Nor, J. Davis, B. Sen et al., “The Recognition of Strokein the Emergency Room (ROSIER) scale: development andvalidation of a stroke recognition instrument,” The LancetNeurology, vol. 4, no. 11, pp. 727–734, 2005.
[75] A. Kuruvilla, P. Bhattacharya, K. Rajamani, and S.Chaturvedi, “Factors associated with misdiagnosis of acutestroke in young adults,” Journal of Stroke and CerebrovascularDiseases, vol. 20, no. 6, pp. 523–527, 2011.
[76] M. Nakajima, T. Hirano, and M. Uchino, “Patients with acutestroke admitted on the second visit,” Journal of Stroke andCerebrovascular Diseases, vol. 17, no. 6, pp. 382–387, 2008.
[77] S. Martin-Schild, K. C. Albright, J. Tanksley et al., “Zero onthe NIHSS does not equal the absence of stroke,” Annals ofEmergency Medicine, vol. 57, no. 1, pp. 42–45, 2011.
[78] J. A. Edlow and M. H. Selim, “Atypical presentations of acutecerebrovascular syndromes,” The Lancet Neurology, vol. 10,no. 6, pp. 550–560, 2011.
[79] S. C. Johnston, D. R. Gress, W. S. Browner, and S. Sidney,“Short-term prognosis after emergency department diagno-sis of TIA,” JAMA, vol. 284, no. 22, pp. 2901–2906, 2000.
[80] S. Prabhakaran, A. J. Silver, L. Warrior, B. McClenathan, andV. H. Lee, “Misdiagnosis of transient ischemic attacks in theemergency room,” Cerebrovascular Diseases, vol. 26, no. 6, pp.630–635, 2008.
[81] J. W. Schrock, M. Glasenapp, A. Victor, T. Losey, and R.K. Cydulka, “Variables associated with discordance betweenemergency physician and neurologist diagnoses of transientischemic attacks in the emergency department,” Annals ofEmergency Medicine, vol. 59, no. 1, pp. 19–26, 2011.
[82] F. A. Chowdhury, L. Nashef, and R. D. C. Elwes, “Misdi-agnosis in epilepsy: a review and recognition of diagnosticuncertainty,” European Journal of Neurology, vol. 15, no. 10,pp. 1034–1042, 2008.
[83] C. B. Josephson, S. Rahey, and R. M. Sadler, “Neuro-cardiogenic syncope: frequency and consequences of itsmisdiagnosis as epilepsy,” Canadian Journal of NeurologicalSciences, vol. 34, no. 2, pp. 221–224, 2007.
[84] P. Francis and G. A. Baker, “Non-epileptic attack disorder(NEAD): a comprehensive review,” Seizure, vol. 8, no. 1, pp.53–61, 1999.
[85] S. Petkar, P. Cooper, and A. P. Fitzpatrick, “How to avoida misdiagnosis in patients presenting with transient loss ofconsciousness,” Postgraduate Medical Journal, vol. 82, no.972, pp. 630–641, 2006.
[86] M. Carreno, “Recognition of nonepileptic events,” Seminarsin Neurology, vol. 28, no. 3, pp. 297–304, 2008.
[87] A. M. Kanner, “Common errors made in the diagnosis andtreatment of epilepsy,” Seminars in Neurology, vol. 28, no. 3,pp. 364–378, 2008.
[88] P. N. Cooper, M. Westby, D. W. Pitcher, and I. Bullock,“Synopsis of the national institute for health and clinicalexcellence guideline for management of transient loss ofconsciousness,” Annals of Internal Medicine, vol. 155, no. 8,pp. 543–550, 2011.
[89] A. P. Fitzpatrick and P. Cooper, “Diagnosis and managementof patients with blackouts,” Heart, vol. 92, no. 4, pp. 559–568,2006.
[90] M. Oliva, C. Pattison, J. Carino, A. Roten, Z. Matkovic, andT. J. O’Brien, “The diagnostic value of oral lacerations andincontinence during convulsive ”seizures”,” Epilepsia, vol. 49,no. 6, pp. 962–967, 2008.
[91] R. Sheldon, S. Rose, D. Ritchie et al., “Historical criteria thatdistinguish syncope from seizures,” Journal of the AmericanCollege of Cardiology, vol. 40, no. 1, pp. 142–148, 2002.
[92] K. M. Bakes, J. Faragher, V. J. Markovchick, K. Donahoe,and J. S. Haukoos, “The Denver Seizure Score: anion gapmetabolic acidosis predicts generalized seizure,” AmericanJournal of Emergency Medicine, vol. 29, no. 9, pp. 1097–1102,2011.
[93] J. Stone, “Functional neurological symptoms,” Journal of theRoyal College of Physicians of Edinburgh, vol. 41, no. 1, pp.38–42, 2011.

10 Emergency Medicine International
[94] T. H. Glick, T. P. Workman, and S. V. Gaufberg, “Suspectedconversion disorder: foreseeable risks and avoidable errors,”Academic Emergency Medicine, vol. 7, no. 11, pp. 1272–1277,2000.
[95] L. McWhirter, J. Stone, P. Sandercock, and W. Whiteley,“Hoover’s sign for the diagnosis of functional weakness:a prospective unblinded cohort study in patients withsuspected stroke,” Journal of Psychosomatic Research, vol. 71,no. 6, pp. 384–386, 2011.
[96] Y. Chen, V. Bogosavljevic, D. Leys, D. Jovanovic, L. Beslac-Bumbasirevic, and C. Lucas, “Intravenous thrombolytic ther-apy in patients with stroke mimics: baseline characteristicsand safety profile,” European Journal of Neurology, vol. 18, no.10, pp. 1246–1250, 2011.
[97] G. Tsivgoulis, A. V. Alexandrov, J. Chang et al., “Safety andoutcomes of intravenous thrombolysis in stroke mimics: a6-year, single-care center study and a pooled analysis ofreported series,” Stroke, vol. 42, no. 6, pp. 1771–1774, 2011.
[98] V. Artto, J. Putaala, D. Strbian et al., “Stroke mimics andintravenous thrombolysis,” Annals of Emergency Medicine,vol. 59, no. 1, pp. 27–32, 2012.
[99] J. Stone, R. Smyth, A. Carson et al., “Systematic review ofmisdiagnosis of conversion symptoms and ‘hysteria’,” BritishMedical Journal, vol. 331, no. 7523, pp. 989–991, 2005.
[100] T. W. Brown, M. L. McCarthy, G. D. Kelen, and F. Levy,“An epidemiologic study of closed emergency departmentmalpractice claims in a national database of physicianmalpractice insurers,” Academic Emergency Medicine, vol. 17,no. 5, pp. 553–560, 2010.
[101] A. Kachalia, T. K. Gandhi, A. L. Puopolo et al., “Missed anddelayed diagnoses in the emergency department: a study ofclosed malpractice claims from 4 liability insurers,” Annals ofEmergency Medicine, vol. 49, no. 2, pp. 196–205, 2007.
[102] D. E. Newman-Toker and P. J. Pronovost, “Diagnostic errorsthe next frontier for patient safety,” JAMA, vol. 301, no. 10,pp. 1060–1062, 2009.
[103] K. E. Kocher, W. J. Meurer, R. Fazel, P. A. Scott, H. M.Krumholz, and B. K. Nallamothu, “National trends in useof computed tomography in the emergency department,”Annals of Emergency Medicine, vol. 58, no. 5, pp. 452–462.e3,2011.
[104] L. M. Prevedello, A. S. Raja, R. D. Zane et al., “Variation in useof head computed tomography by emergency physicians,”American Journal of Medicine, vol. 125, no. 4, pp. 356–364,2012.
[105] R. Smith-Bindman, “Is computed tomography safe?” TheNew England Journal of Medicine, vol. 363, no. 1, pp. 1–4,2010.
[106] J. A. Edlow, “What are the unintended consequences ofchanging the diagnostic paradigm for subarachnoid hem-orrhage after brain computed tomography to computedtomographic angiography in place of lumbar puncture?”Academic Emergency Medicine, vol. 17, no. 9, pp. 991–997,2010.
[107] J. P. Kassirer, “Our stubborn quest for diagnostic certainty:a cause of excessive testing,” The New England Journal ofMedicine, vol. 320, no. 22, pp. 1489–1491, 1989.
[108] T. H. Glick, “The neurologist and patient safety,” Neurologist,vol. 11, no. 3, pp. 140–149, 2005.
[109] B. A. Stettler, E. C. Jauch, B. Kissela, and C. J. Lindsell,“Neurologic education in emergency medicine trainingprograms,” Academic Emergency Medicine, vol. 12, no. 9, pp.909–911, 2005.
[110] P. Croskerry and G. R. Nimmo, “Better clinical decisionmaking and reducing diagnostic error,” Journal of the RoyalCollege of Physicians of Edinburgh, vol. 41, no. 2, pp. 155–162,2011.
[111] K. W. Eva, C. L. Link, K. E. Lutfey, and J. B. McKinlay,“Swapping horses midstream: factors related to physicians’changing their minds about a diagnosis,” Academic Medicine,vol. 85, no. 7, pp. 1112–1117, 2010.
[112] M. L. Graber, “Educational strategies to reduce diagnosticerror: can you teach this stuff?” Advances in Health SciencesEducation, vol. 14, supplement 1, pp. 63–69, 2009.
[113] J. P. Kassirer, “Teaching clinical reasoning: case-based andcoached,” Academic Medicine, vol. 85, no. 7, pp. 1118–1124,2010.
[114] R. L. Trowbridge, “Twelve tips for teaching avoidance ofdiagnostic errors,” Medical Teacher, vol. 30, no. 5, pp. 496–500, 2008.
[115] R. L. Wears, “What makes diagnosis hard?” Advances inHealth Sciences Education, vol. 14, supplement 1, pp. 19–25,2009.
[116] I. A. Scott, “Errors in clinical reasoning: causes and remedialstrategies,” BMJ, vol. 338, Article ID b1860, 2009.
[117] A. Schattner, N. Magazanik, and M. Haran, “The hazards ofdiagnosis,” QJM, vol. 103, no. 8, pp. 583–587, 2010.

Hindawi Publishing CorporationEmergency Medicine InternationalVolume 2012, Article ID 303152, 8 pagesdoi:10.1155/2012/303152
Review Article
Reversible Cerebral Vasoconstriction Syndrome: An ImportantCause of Acute Severe Headache
Li Huey Tan and Oliver Flower
Intensive Care Medicine, Royal North Shore Hospital, St. Leonards, NSW 2065, Australia
Correspondence should be addressed to Li Huey Tan, [email protected]
Received 8 March 2012; Revised 30 April 2012; Accepted 10 May 2012
Academic Editor: Julian Boesel
Copyright © 2012 L. H. Tan and O. Flower. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Reversible cerebral vasoconstriction syndrome (RCVS) is an increasingly recognized and important cause of acute headache. Themajority of these patients develop potentially serious neurological complications. Rigorous investigation is required to excludeother significant differential diagnoses. Differentiating RCVS from subarachnoid haemorrhage (SAH) and primary angiitis ofthe central nervous system (PACNS) may be difficult but has important therapeutic implications. This paper describes what iscurrently known about the epidemiology, pathophysiology, clinical, and diagnostic features of the syndrome, an approach toinvestigation, a summary of treatments, and what is known of prognosis.
1. Introduction
Acute severe headache presenting to the Emergency Depart-ment (ED) accounts for 1-2% of admissions [1]. Whilst thedifferential diagnosis in the setting of nontraumatic head-ache is extensive, it is imperative that life-threatening causesof headache are identified in a timely fashion and treatedappropriately. Reversible cerebral vasoconstriction syndrome(RCVS) is one of these differentials that potentially hasdire consequences and, with improving technology andawareness, is being increasingly diagnosed.
The presence of acute severe headache and characteristicangiographic findings was initially described in a case seriesin which Gregory Call and Marie Fleming were leadauthors, hence the eponym Call-Fleming syndrome [2]. Theydescribed unique features in patients who presented withsudden onset severe headache and cerebral angiography thatdemonstrated reversibility of vasoconstriction of arteriesinvolving the Circle of Willis and its immediate branches[2]. Other literature has described similar clinical entitiesthat appear to fall under the descriptive heading of RCVS.This includes migrainous vasospasm or migraine angiitis[3–5], benign angiopathy of the central nervous system[6], postpartum angiopathy [7], thunderclap headache with
reversible vasospasm [3–5], and drug-induced angiopathy[7, 8]. Distinguishing all of these disorders from cerebralvasculitis has also been challenging but is a key diagnosticstep as the treatments are significantly different. The unifyingterm reversible cerebral vasoconstriction syndrome (RCVS)was proposed by Calabrese in 2007 [9]. It encompasses allof these clinical entities, which share similar clinical presen-tations, radiological findings, and sequelae. The diagnosticelements of RCVS are shown in Table 1.
Since the initial descriptions in 1988, much remainsunknown about RCVS and this is reflected in the paucity ofliterature on the topic. This is partially due to a previous lackof a consensus definition, deficits in understanding of theunderlying pathophysiology, and overlapping features withother conditions such as cerebral vasculitis. The incidenceof RCVS appears to be increasing. This may be due tothe increasing availability and advances in neurovascularimaging, or a genuine increase, perhaps related to moreprevalent use of vasoactive substances [10].
2. Epidemiology
There is a clear female predominance of RCVS in all pub-lished case series, with female to male ratios ranging from

2 Emergency Medicine International
Table 1: Diagnostic criteria for RCVS [9].
Summary of critical elements for the diagnosis of reversible cerebral vasoconstriction syndromes
(1) Angiography (DSA, CTA, or MRA) documenting multifocal segmental cerebral artery vasoconstriction
(2) No evidence of aneurysmal subarachnoid hemorrhage
(3) Normal or near-normal cerebrospinal fluid analysis (protein level <80 mg%, leukocytes <10 mm3, normal glucose level)
(4) Severe, acute headaches, with or without additional neurologic signs or symptoms.
(5) Reversibility of angiographic abnormalities within 12 weeks of symptom onset. If death occurs before the follow-up studies arecompleted, autopsy rules out such conditions as vasculitis, intracranial atherosclerosis, and aneurysmal subarachnoid hemorrhage, whichcan also manifest with headache and stroke
Table 2: Secondary precipitants of RCVS [9–12].
Vasoactive substances Predisposing conditions
Recreational drugs: Cannabis, cocaine, ecstasy, amphetamines,LSD, binge drinking
Pregnancy
Sympathomimetics, nasal decongestants: ephedrine,pseudoephedrine
Eclampsia, preeclampsia
Serotonergic drugs: selective serotonin reuptake inhibitors,triptans
Neoplasia: phaeochromocytoma, bronchial carcinoid, glomustumour
Immunosuppressants: tacrolimus, cyclophosphamide Neurosurgery, head injury
Nicotine patches Hypercalcaemia
Herbal medications: ginseng Porphyria
Blood products: erythropoietin, immunoglobulin, red celltransfusion
Intracerebral haemorrhage, subarachnoid haemorrhage
2.6 : 1 [11] to 10 : 1 [12]. These differences may be due togeographical and genetic reasons. Sex predilection seems tobe less significant in secondary RCVS [11]. The typical agegroup affected in adulthood is between 20 and 50 years old.However, there have been case reports of patients under 18years of age, the majority being male [13, 14].
RCVS can occur spontaneously or be secondary to aprecipitating factor. The proportion of spontaneous caseshas varied depending on the population studied, from 37%in a French study [14] to 96% in a Taiwanese cohort [12].Vasoactive drugs and the postpartum period are two com-mon associations [14], with several other associations beingsuggested from previous case series (see Table 2).
3. Pathophysiology
The pathogenesis of RCVS remains poorly understood.Current consensus on the aetiology focuses around alterationof cerebral vascular tone. This may occur spontaneously(primary RCVS) or be triggered by endogenous or exogenoussubstances (secondary RCVS) (see Table 2). There appearsto be interaction between sympathetic overactivity andendothelial dysfunction, resulting in dysautoregulation [11].With the radiological similarities with postsubarachnoidhaemorrhage vasospasm, it has been postulated that themediators of vasospasm in subarachnoid haemorrhage suchas endothelin-1, serotonin, nitric oxide, prostaglandins, andcatecholamines [15, 16] may also be invoked in RCVS bydifferent mechanisms. It has also been suggested that asudden central neuronal discharge may induce vasospasmand the severe headache be caused by stimulation of the
sensory afferents of the first division of the trigeminal nerveand dorsal root of C2 which supply these cerebral bloodvessels [9]. Resolution of symptoms does not always correlatewith radiological resolution of vasoconstriction, and thefactors perpetuating this process are also yet to be identified.Genetic factors are likely to play a role in the predispositionand development of RCVS.
Postpartum angiopathy is considered a variant of RCVSoccurring after pregnancy. It can occur following uncom-plicated pregnancy as well as in eclampsia [17]. Acutesevere headaches tend to occur within days or weeks afteruncomplicated deliveries unlike those seen in eclampsia. Theimbalance of angiogenic factors seen in eclamptic patientshas not been demonstrated in patients with uncomplicatedpregnancy that develop postpartum angiopathy.
4. Clinical Features
The most common symptom of RCVS is an acute severe“thunderclap” headache (TCH), typically in females betweenthe ages of 20 and 50 years, and this is often the onlysymptom at presentation [14]. This TCH is defined as asevere headache reaching its maximal intensity within oneminute [10]. The headache tends to be recurrent, over aperiod of days to weeks. Characteristics of the headache varywidely from occipital to diffuse and constant to throbbing. Itmay occur spontaneously or be precipitated by exercise or avalsalva manoeuvre. Systemic clinical features such as nausea,vomiting, and transient hypertension are not uncommon.
Neurological deficits may or may not be present ini-tially. In a recent cohort study from North America, focal

Emergency Medicine International 3
neurological deficits were present initially in 43% [14]. Thesedeficits include visual disturbances, photophobia, blind-ness, focal facial or limb weakness, dysarthria, and ataxia.Generalised tonic-clonic seizures occurred in 17%. Mostsignificantly, severe and permanent neurological deficits andeven death may occur as a consequence. The reversiblecomponent suggested in the description refers specifically tothe angiographic vasoconstriction, and the feared vascu-lar complications are surprisingly common (81%). Theseinclude ischaemic stroke, nonaneurysmal subarachnoid hae-morrhage, intracerebral haemorrhage, cerebral oedema andposterior reversible leucoencephalopathy syndrome (PRES).Most of these complications occur in the first week of pres-entation, except cerebral ischaemia, which is more commonin and after the second week [18]. Female gender and ahistory of migraines are both independent risk factors forintracranial haemorrhage [19]. Therefore, RCVS should beconsidered in patients presenting with cryptogenic stroke,particularly if there was an associated typical headache andimaging reveals symmetrical brain infarctions and oedema.
5. Investigations
An approach to investigation of acute severe nontraumaticheadache is outlined in Figure 1. A noncontrast CT brainshould be performed initially to exclude subarachnoid andintracerebral haemorrhage. If normal, this should be fol-lowed by a lumbar puncture (LP). In the majority of acutepresentations of RCVS, the noncontrast CT head showsno abnormalities [14]. Depending on the history, CTangiography at the time of a non-contrast CT may bewarranted, looking for evidence of RCVS, cervical arterydissection, or cerebral venous thrombosis. It should be notedthat all of these diagnoses require different CT imagingtechniques and this should be discussed with the radiologistand radiographer involved to obtain optimal images. Otherdifferentials to consider include pituitary apoplexy andintracranial hypotension. These both have characteristic CTfindings but are better visualised with an MRI, which mayfollow if the history and examination are suggestive andthe CT is nondiagnostic. The LP is performed looking forevidence of CNS infection, subarachnoid haemorrhage, orprimary angiitis of central nervous system (PACNS). Adistinguishing feature of RCVS is an initially normal CSFresult. After a single episode of an acute non-traumaticheadache that has resolved, if the CT with contrast and theLP are normal, it may be reasonable to consider discharge ifthey can be relied upon to return if their symptoms reoccur.
For persistent or recurrent acute severe headaches, fourdifferent imaging modalities are currently used to evaluatethe presence of vasospasm, summarized in Figure 1. Ingeneral, an approach starting with less invasive imagingis employed. Angiographic changes in cerebral arteries,described as a “string of beads,” are highly characteristic ofRCVS.
CT angiography (CTA) is readily available, fast, and canbe performed immediately after an initial non-contrast CT.It is not affected by flow-related inhomogeneities that canaffect MRI and can certainly reveal regions of vasospasm. CT
venography can also exclude cerebral sinus thrombosis, animportant differential diagnosis. However, CTA may lack thesensitivity of digital subtraction cerebral angiography (DSA),may poorly visualise smaller distal vessels, has no scope forintervention, and incurs contrast and radiation exposure.Modern multidetector-row spiral CT angiography producesvascular imaging potentially equivalent to DSA [20], unlikeolder generations of CT scanners. When looking for evidenceof RCVS with a CTA, the images must include all the cerebralarteries up to the vertex, so as not to miss spasm in thesevessels, which must also be considered when arranging theimaging.
MRI with angiography and venography has advantagesover CTA as the next radiological investigation following anormal CT [10] and has been validated in this context [21].The MR sequences should as a minimum include T1, T2,fluid attenuated inversion recovery imaging, gradient-echo(T2) imaging, diffusion weighted imaging, and apparentdiffusion coefficient mapping for differential diagnosis andevaluation of complications. Cervical MR using a T1 fat-saturation sequence with contrast should be considered ifcervical artery dissection is suspected [21]. MRA avoidspotential complications of repeated DSA’s, and the improvedsoft tissue imaging may demonstrate small areas of corticalhaemorrhage, ischaemic complications of RCVS not visiblewith CT, or changes consistent with PRES. However, MRAstill lacks the sensitivity for vascular imaging of DSA, andimaging small arteries in the setting of PACNS is moredifficult with MRA [22]. MRA is also not always imme-diately available and potentially carries the risks of trans-port, remote-site anaesthesia and the complications of thegadolinium contrast.
Currently, DSA is still considered to be the gold standardfor the diagnosis of RCVS. It allows real-time appreciation ofvessel calibre and flow and permits better visualization of thesmaller, peripheral vessels with superior spatial and temporalresolution. More significantly, there is also the potential forintervention with intra-arterial vasodilators in addition tothe diagnostic advantages. The disadvantages of DSA includethe invasiveness, potential vascular injury with stroke, andthe inherent radiation and contrast exposure. One case seriesreported a high incidence (9%) of transient neurologicaldeficit post-DSA in patients with RCVS [11] however, thiswas likely to be related to the underlying pathology, and ratesof 0.5% for permanent and 1% for transient neurologicalcomplications may be expected [23–25].
Transcranial doppler (TCD) imaging has a potential rolein monitoring vasospasm after RCVS has been diagnosedby another imaging modality. It is a noninvasive way toassess larger vessel vasospasm, and in one study of TCD inRCVS, a mean flow velocity of the middle cerebral arterygreater than 120 m/s was associated with a greater risk ofischaemic complications [26]. However, TCD does not allowassessment of smaller vessels, is not always available, maybe technically difficult on some individuals, and is subjectto significant inter-observer and interindividual variability.Centres where there is local expertise and the same operatoris available to repeat the imaging on a regular basis may useserial TCD to avoid the risks of the other imaging techniques.

4 Emergency Medicine International
CTA MRI/A DSA TCD
Advantages Less time consuming than DSA or MRAReadily availableNot affected by flow- relatedinhomogeneites
Better brain parenchyma visualisationBetter to diagnose:PRESPituitary apoplexySmall infarcts/haemorrhageIntracranial hypotension
Diagnostic gold standardBest small vessel imagingDynamic flow assessment
Non-invasiveNo contrastRepeatable
DisadvantagesPoor visualization of small vesselsIonizing radiationLess information on flow velocity and flow directionContrast-related complicationsDifferent imaging required for specific conditions
AvailabilitySpeedClaustrophobiaGeneral anaestheticContrast-related complicationsPotentially affected by flow-related
InvasiveNeurological complictionsCannulation site complicationsNo soft tissue imaging
between PACNS and Does not differentiate
RCVSIonizing radiationContrast-related complications
Only assesses large vesselsAvailability variesOperator
Need same operatoreach time
History including
About the headacheAgeSexAssociated featuresDrug history
Examination including
Level of consciousnessFocal neurological deficitsFeverMeningism
Acute severe nontraumatic headache
AbnormalConsiderSAHPACNSCerebral venous thrombosisCarotid or vertebral artery dissectionCNS infectionSpace occupying lesionPituitary apoplexy (MRI Better)Intracranial hypotension (MRI
LP
Abnormal
TreatSAHPACNSCNS infection
Normal
If headache persistent, recurrent or history suggestive of RCVS,
then further neurovascular imaging
Normal
Consider dischargeIf
Resolved single isolated headacheOther investigationsnormal
CT head∗
better)
(MRA)
inhomogeneites
dependence
Figure 1: An approach to investigation of RCVS [10]. ∗CT angiography may be considered at this stage, specifically looking for cervicalartery dissection, cerebral venous thrombosis or RCVS, depending on the history, clinical suspicion and contraindications to radiocontrast.
Cervical artery dopplers have been used to investigate forarterial dissection in the context of acute severe headache;whilst having a significantly favourable complication profilecompared to any form of angiogram, there are bony regionslimiting ultrasound imaging, greatly reducing the sensitivityof this investigation.
None of these imaging modalities give an irrefutablediagnosis of RCVS. The choice of imaging modality shouldbe chosen based upon the other differential diagnoses sug-gested from the history, and what is available. A CTA or MRAmay follow a non-contrast CT however, if both of these arenondiagnostic and clinical suspicion of RCVS exists, a DSA

Emergency Medicine International 5
Table 3: Distinguishing features of RCVS, cervical artery dissection, PACNS and SAH [9].
RCVS Cervical artery dissection PACNS SAH
History
Sudden onset headache,often thunderclap
Sudden or subacute, canhave thunderclap features
Insidious, constant,progressive, dull
Sudden onset headache,often thunderclap
More common infemales
No sex predilection No sex predilection More common in females
Age 20–50 years old Age less than 50 years old Age 40–60 years oldAge 40–60 years old
Risk increases with age
Likely to be younger infamilial SAH
Risk factorsDrugs, pregnancy,tumours, neuro injury,idiopathic
Atherosclerosis, cervicaltrauma, connective tissuedisease. Can be idiopathic
Family historyKnown cerebral aneurysm
ExaminationPresence or absence ofneurological deficit
Presence or absence ofneurological deficit.Important to rule out inyounger patients.
Presence or absence ofneurological deficit, 5%spinal involvement
Depends on severity ofhaemorrhage
CT brainMajority normalCortical SAH, ICH
Normal in the absence ofcerebral infarct (60%);crescenteric intramuralhaematoma on CTA
Majorityabnormal—diffuse,multiple small infarcts
Majority abnormal.SAH, cerebral oedema,hydrocephalus
CSF studies Majority normal NormalMajority abnormal—raisedprotein, cell count
Abnormal—xanthochromia, raised redcell count
MRI brain Majority normal
MRA may revealintramural haematoma aswell as demonstrate flowabnormalities. Moresensitive than CT or earlyinfarction
Nonspecific changesMultifocal, cortical orsubcortical infarcts, diffusewhite matter changes, orleptomeningealenhancement
Areas of infarctcorresponding to vascularterritory involved
Cerebralangiography
Considered goldstandard.Useful in recurrent TCHDiffuse segmentalstenosis—medium, largearteries
Long-segmental stenosis,intimal flaps, arterialpseudoaneurysm
Unable to visualise changesin small arteries
Aneurysm, arterio-venousmalformationVasospasm (not multifocal)at Day 4
CNS biopsy Not indicatedGold standard.Skip, segmental vascularlesions
should follow. Follow-up imaging may be with MRA or DSAif intra-arterial interventions are being considered. Table 3shows comparative features of RCVS, cervical artery dissec-tion, PACNS, and SAH to aid in diagnosis. Angiographically,SAH-induced vasospasm is more commonly longsegmentaland mainly around the bleeding focus [27], compared tothe multiple, short-segmental and diffuse changes seen inRCVS; however, this is not 100% specific and a DSA is alsorequired to look for evidence of an aneurysm if this hasnot already been identified. PACNS is radiologically identicalto RCVS, making the clinical history, risk, factors and CSFstudies important in differentiating these conditions. Thereversibility of the angiographic findings is a key componentto the diagnosis but only helpful retrospectively. Therefore,if a patient presents with a classic history of repetitivethunderclap headaches, has no evidence of SAH, has normalCSF analysis and a normal MRI, and shows the typical
findings of RCVS on vascular imaging (DSA, CTA, or MRA),a diagnosis of RCVS can be made. If the history or CSFanalysis is ambiguous, then the diagnosis of PACNS must beentertained.
Figure 2 shows some neuroimaging of a 61-year-old ladywith RCVS. These images illustrate the limitations of CTA indetecting peripheral vasospasm, the benefits of DSA imaging(which was obtained whilst intra-arterial verapamil wasadministered), the limitations of MRA compared to DSA,and the infarctions which can develop as a complication ofvasospasm.
6. Treatment
The evidence for effective treatment in RCVS is limited toobservational studies at present. Any potential drugs or trig-gers should be discontinued or avoided in secondary RCVS

6 Emergency Medicine International
(a) (b)
(c) (d)
Figure 2: Neuroimaging in a case of RCVS. Neuroimaging of a 61-year-old female with RCVS. (a) CT angiography demonstrated no evidenceof vasospasm. (b) DSA demonstrated diffuse areas of focal segmental narrowing affecting both the anterior and posterior circulation,particularly in the A2 segment of the left anterior cerebral artery (arrow). (c) MRA showed predominantly peripheral focal segmental spasm,though not as clearly as the DSA (d) MRI 6 weeks after presentation reveals high T2 signal representing right occipital cortical infarcts. CT:computerised tomography; DSA: digital subtraction angiogram; MRA: magnetic resonance angiogram; MRI: magnetic resonance imaging.
[9, 10, 14, 18]. Glucocorticoids were previously considered apotential treatment; however, they have more recently beenshown to be an independent predictor of poor outcome[14] and should be avoided. This highlights the importanceof distinguishing the two entities as the use of steroids(prednisolone 1 mg/kg/day) is the treatment of choice inPACNS [28].
The calcium channel blocker nimodipine is the mostwidely employed treatment for RCVS, although there are noprospective randomised placebocontrolled trials to supportthis. Nimodipine has been shown to terminate the headachein 64–83% of patients [11, 12, 29], although in the largestcase series reported, treatment with nimodipine showed nooutcome benefit over symptomatic treatment alone [14]. As
in SAH, both oral and intravenous nimodipine regimenshave been used and there is no published evidence support-ing one over the other.
Other systemic treatments that have been used includeintravenous and oral nicardipine [13], intravenous and oralverapamil [30], and intravenous magnesium sulphate (in thetreatment of postpartum angiopathy) [31]. These reports allhave the inherent limitations of case studies. Intra-arterial(IA) vasodilators injected during DSA with and withoutangioplasty are also used. These include IA milrinone [30],IA verapamil [32], and IA nimodipine as both a therapeuticand diagnostic agent [33], with the evidence, again, limitedto case reports. IA verapamil has been shown to improveradiological vasospasm [34, 35], but whether this translates

Emergency Medicine International 7
to improved clinical outcomes remains to be proven. Withthe current agnosticism regarding optimal treatment, mul-ticentre, prospective, randomized, placebocontrolled trialswould seem prudent, though logistically difficult.
7. Prognosis
The most serious complications of RCVS are permanentneurological deficit and death. In the largest North Americanstudy, 81% of patients developed radiological evidence ofbrain lesions as a consequence of RCVS 39% had ischemicinfarcts, 34% had convexity subarachnoid haemorrhage,20% developed lobar intracerebral haemorrhage, and 38%had cerebral edema [14]. Despite this, the rate of permanentneurological disability is surprisingly low. In this cohort,89% had a good clinical outcome (Modified Rankin Scoreat followup or discharge of 0–3) [14], and in a systematicreview, 71% had no evidence of any long-term disability,29% had only minor disability [18], and 6% had permanentneurological disability [11]. Cerebral infarction and intrac-erebral haemorrhage are predictors of a worse outcome [14].Deaths from RCVS have been reported in the literature butare rare [14, 36]. The rate of recurrence is approximately 8%[21].
8. Conclusion
RCVS is a clinical entity and neurological emergency thatis being diagnosed with increasing frequency but is stillunderrecognized, and a high index of suspicion is essential.There are characteristic features in the history and on neu-roimaging that are distinctive, but overlapping features withother conditions can make diagnosis difficult. DistinguishingRCVS from PACNS is important, as the glucocorticoidtreatment indicated for PACNS appears to be harmful inRCVS. The management is predominantly supportive, whilstruling out other life-threatening neurological conditions,identifying risk factors, and discontinuing offending agents.Intra-arterial vasodilators and balloon angioplasty offerpromise but as yet have not been proven to improveclinical outcomes. There are still many areas for futureresearch including the pathogenesis, the natural historyof the syndrome, the optimal diagnostic strategy and thetreatment.
References
[1] T. N. Ward, M. Levin, and J. M. Phillips, “Evaluation and man-agement of headache in the emergency department,” MedicalClinics of North America, vol. 85, no. 4, pp. 971–985, 2001.
[2] G. K. Call, M. C. Fleming, S. Sealfon, H. Levine, P. Kistler, andC. M. Fisher, “Reversible cerebral segmental vasoconstriction,”Stroke, vol. 19, no. 9, pp. 1159–1170, 1988.
[3] J. W. Day and N. H. Raskin, “Thunderclap headache: symptomof unruptured cerebral aneurysm,” The Lancet, vol. 2, no.8518, pp. 1247–1248, 1986.
[4] A. Slivka and B. Philbrook, “Clinical and angiographic featuresof thunderclap headache,” Headache, vol. 35, no. 1, pp. 1–6,1995.
[5] D. W. Dodick, R. D. Brown, J. W. Britton, and J. Huston,“Nonaneurysmal thunderclap headache with diffuse, multifo-cal, segmental, and reversible vasospasm,” Cephalalgia, vol. 19,no. 2, pp. 118–123, 1999.
[6] L. H. Calabrese, L. A. Gragg, and A. J. Furlan, “Benign angi-opathy: a distinct subset of angiographically defined primaryangiitis of the central nervous system,” Journal of Rheumatol-ogy, vol. 20, no. 12, pp. 2046–2050, 1993.
[7] J. Bogousslavsky, P. A. Despland, F. Regli, and P. Y. Dubuis,“Postpartum cerebral angiopathy: reversible vasoconstrictionassessed by transcranial Doppler ultrasounds,” European Neu-rology, vol. 29, no. 2, pp. 102–105, 1989.
[8] P. Y. Henry, P. Larre, and M. Aupy, “Reversible cerebral arte-riopathy associated with the administration of ergot deriva-tives,” Cephalalgia, vol. 4, no. 3, pp. 171–178, 1984.
[9] L. H. Calabrese, D. W. Dodick, T. J. Schwedt, and A. B. Singhal,“Narrative review: reversible cerebral vasoconstriction syn-dromes,” Annals of Internal Medicine, vol. 146, no. 1, pp. 34–44, 2007.
[10] S. P. Chen, J. L. Fuh, and S. J. Wang, “Reversible cere-bral vasoconstriction syndrome: an under-recognized clinicalemergency,” Therapeutic Advances in Neurological Disorders,vol. 3, no. 3, pp. 161–171, 2010.
[11] A. Ducros, M. Boukobza, R. Porcher, M. Sarov, D. Valade,and M. G. Bousser, “The clinical and radiological spectrum ofreversible cerebral vasoconstriction syndrome. A prospectiveseries of 67 patients,” Brain, vol. 130, no. 12, part 2, pp. 3091–3101, 2007.
[12] S. P. Chen, J. L. Fuh, J. F. Lirng, F. C. Chang, and S. J. Wang,“Recurrent primary thunderclap headache and benign CNSangiopathy: spectra of the same disorder?” Neurology, vol. 67,no. 12, pp. 2164–2169, 2006.
[13] H. Y. Liu, J. L. Fuh, J. F. Lirng, S. P. Chen, and S. J. Wang,“Three paediatric patients with reversible cerebral vasocon-striction syndromes,” Cephalalgia, vol. 30, no. 3, pp. 354–359,2010.
[14] A. B. Singhal, R. A. Hajj-Ali, M. A. Topcuoglu et al., “Re-versible cerebral vasoconstriction syndromes: analysis of 139cases,” Archives of Neurology, vol. 68, no. 8, pp. 1005–1012,2011.
[15] H. H. Dietrich and R. G. Dacey, “Molecular keys to theproblems of cerebral vasospasm,” Neurosurgery, vol. 46, no. 3,pp. 517–530, 2000.
[16] E. Tani, “Molecular mechanisms involved in development ofcerebral vasospasm,” Neurosurgical Focus, vol. 12, no. 3, articleECP1, 2002.
[17] E. V. Sidorov, W. Feng, and L. R. Caplan, “Stroke in pregnantand postpartum women,” Expert Review of CardiovascularTherapy, vol. 9, no. 9, pp. 1235–1247, 2011.
[18] A. Sattar, G. Manousakis, and M. B. Jensen, “Systematic reviewof reversible cerebral vasoconstriction syndrome,” ExpertReview of Cardiovascular Therapy, vol. 8, no. 10, pp. 1417–1421, 2010.
[19] A. Ducros, U. Fiedler, R. Porcher, M. Boukobza, C. Stapf,and M. G. Bousser, “Hemorrhagic manifestations of reversiblecerebral vasoconstriction syndrome: frequency, features, andrisk factors,” Stroke, vol. 41, no. 11, pp. 2505–2511, 2010.
[20] E. D. Greenberg, R. Gold, M. Reichman et al., “Diagnosticaccuracy of CT angiography and CT perfusion for cerebralvasospasm: a meta-analysis,” American Journal of Neuroradi-ology, vol. 31, no. 10, pp. 1853–1860, 2010.
[21] S. P. Chen, J. L. Fuh, S. J. Wang et al., “Magnetic reso-nance angiography in reversible cerebral vasoconstriction syn-dromes,” Annals of Neurology, vol. 67, no. 5, pp. 648–656, 2010.

8 Emergency Medicine International
[22] P. Gerretsen and R. Z. Kern, “Reversible cerebral vasocon-striction syndrome or primary angiitis of the central nervoussystem?” Canadian Journal of Neurological Sciences, vol. 34, no.4, pp. 467–477, 2007.
[23] J. T. Fifi, P. M. Meyers, S. D. Lavine et al., “Complications ofmodern diagnostic cerebral angiography in an academic med-ical center,” Journal of Vascular and Interventional Radiology,vol. 20, no. 4, pp. 442–447, 2009.
[24] J. E. Heiserman, B. L. Dean, J. A. Hodak et al., “Neurologiccomplications of cerebral angiography,” American Journal ofNeuroradiology, vol. 15, no. 8, pp. 1401–1411, 1994.
[25] R. A. Willinsky, S. M. Taylor, K. TerBrugge, R. I. Farb, G.Tomlinson, and W. Montanera, “Neurologic complications ofcerebral angiography: prospective analysis of 2,899 proceduresand review of the literature,” Radiology, vol. 227, no. 2, pp.522–528, 2003.
[26] S. P. Chen, J. L. Fuh, F. C. Chang, J. F. Lirng, B. C. Shia, andS. J. Wang, “Transcranial color doppler study for reversiblecerebral vasoconstriction syndromes,” Annals of Neurology,vol. 63, no. 6, pp. 751–757, 2008.
[27] A. Aralasmak, M. Akyuz, C. Ozkaynak, T. Sindel, and R.Tuncer, “CT angiography and perfusion imaging in patientswith subarachnoid hemorrhage: correlation of vasospasm toperfusion abnormality,” Neuroradiology, vol. 51, no. 2, pp. 85–93, 2009.
[28] C. Salvarani, R. D. Brown Jr., and G. G. Hunder, “Adultprimary central nervous system vasculitis: an update,” CurrentOpinion in Rheumatology, vol. 24, no. 1, pp. 46–52, 2012.
[29] S. R. Lu, Y. C. Liao, J. L. Fuh, J. F. Lirng, and S. J.Wang, “Nimodipine for treatment of primary thunderclapheadache,” Neurology, vol. 62, no. 8, pp. 1414–1416, 2004.
[30] M. Bouchard, S. Verreault, J. L. Gariepy, and N. Dupre, “Intra-arterial milrinone for reversible cerebral vasoconstrictionsyndrome,” Headache, vol. 49, no. 1, pp. 142–145, 2009.
[31] Y. Chik, R. E. Hoesch, C. Lazaridis, C. J. Weisman, and R.H. Llinas, “A case of postpartum cerebral angiopathy withsubarachnoid hemorrhage,” Nature Reviews Neurology, vol. 5,no. 9, pp. 512–516, 2009.
[32] H. Farid, J. K. Tatum, C. Wong, V. V. Halbach, and S. W.Hetts, “Reversible cerebral vasoconstriction syndrome: treat-ment with combined intra-arterial verapamil infusion andintracranial angioplasty,” American Journal of Neuroradiology,vol. 32, no. 10, pp. E184–E187, 2011.
[33] J. Linn, G. Fesl, C. Ottomeyer et al., “Intra-arterial appli-cation of nimodipine in reversible cerebral vasoconstrictionsyndrome: a diagnostic tool in select cases?” Cephalalgia, vol.31, no. 10, pp. 1074–1081, 2011.
[34] K. F. French, R. E. Hoesch, J. Allred et al., “Repetitive use ofintra-arterial verapamil in the treatment of reversible cerebralvasoconstriction syndrome,” Journal of Clinical Neuroscience,vol. 19, no. 1, pp. 174–176, 2012.
[35] J. V. Sehy, W. E. Holloway, S. P. Lin, D. T. M. Cross, C. P.Derdeyn, and C. J. Moran, “Improvement in angiographiccerebral vasospasm after intra-arterial verapamil administra-tion,” American Journal of Neuroradiology, vol. 31, no. 10, pp.1923–1928, 2010.
[36] A. B. Singhal, W. T. Kimberly, P. W. Schaefer, and E. T.Hedley-Whyte, “Case records of the Massachusetts GeneralHospital. Case 8-2009. A 36-year-old woman with headache,hypertension, and seizure 2 weeks post partum,” The NewEngland Journal of Medicine, vol. 360, no. 11, pp. 1126–1137,2009.