Embed Size (px)
Citation preview

Journal ofNeurology, Neurosurgery, and Psychiatry 1990;53:496-501
Saccadic function in spasmodic torticollis
R Stell, A M Bronstein, M Gresty, D Buckwell, C D Marsden
AbstractTwelve patients with idiopathic spas-modic torticollis were compared with 19normal controls on tests of saccadic eyemovements thought to depend upon nor-mal basal ganglia function. The patientswere able to make random, predictive,remembered, and self-paced saccadesequally as well as control subjects. Thissuggests that those parts of the basalganglia which may be damaged in spas-modic torticollis, are separate frompathways responsible for the normalinitiation and execution of saccades.
Medical ResearchCouncil Neuro-otologyUnit, Institute ofNeurology, NationalHospital, QueenSquare, LondonR StellA M BronsteinM GrestyD BuckwellUniversityDepartment ofClinical Neurology,Institute of Neurology,National Hospital,Queen Square,LondonC D MarsdenCorrespondence to:Dr Rick StellMRC Neuro-otology Unit,Institute of Neurology,National Hospital forNervous Diseases,Queen Square,London WC1N 3BG,United Kingdom.Received 14 July 1989and in revised form11 October 1989.Accepted 3 November 1989
The cause and pathophysiology of idiopathicspasmodic torticollis, the most common formof focal dystonia, is unknown. It is assumed tobe a disease of the basal ganglia by inferenceas occasionally it is produced by lesions in thisregion of the brain.' To date there have beenvery few reports of abnormalities in ocularmotor function in torticollis. These have dealtmainly with asymmetries in vestibularresponses on caloric and rotational tests.2 3Whilst no gross abnormalities of oculomotorfunction have been recognised, there havebeen no studies specifically focusing on thesaccadic subsystems requiring the integrity ofthe basal ganglia for their production.The saccadic ocular motor system utilises a
number of pathways subserving specificfunctions, namely predictive and rememberedsaccades, as well as saccades to voluntaryvisual and novel visual targets. In sub-humanprimates, pathways traversing the basalganglia are important for the generation ofpredictive and remembered saccades.4 Inhumans, the analysis of predictive andremembered saccades in diseases of the basalganglia, such as Parkinson's disease, hasconfirmed the presence of specific deficits inthis saccadic subsystem.56We report the results of tests of saccadic
function known to be sensitive to basal gangliadisease in a group of patients with idiopathictorticollis and compare them to a group ofage-matched normal subjects.
Patients and methodsTwelve patients with isolated spasmodictorticollis producing pure horizontal rotationof the head were studied (table 1). Patients withisolated rotation were chosen because we were
interested in right-left asymmetries of saccadicfunction; if such an asymmetry were present itwould be most likely manifested in patients
with a lateralised disoider of motor control.The direction of torticoilis referred to the sideto which the chin was displaced. There were 11females and one male, with a mean age of 50-6years (range 29-63). The mean disease dura-tion was 9 6 years (range 1-25). Seven patientshad rotation of the chin to the left and five tothe right. Three patients were not takingmedication at the time of the study, four weretaking benzhexol (Artane), three were takingdiazepam, one lorazepam and one mianserin.All had been on the stated medications for atleast six months without any change in dosage.All patients had previously received at least oneset of injections of botulinum toxin into theappropriate neck muscles, and some had beentreated at regular intervals for up to two years.The patients were compared to a group of 19normal controls; seven females and 12 maleswith a mean age of 43 years (range 30-65).Eye movements were recorded with DC
electronystagmography (ENG) onto paperwith an ink-jet polygraph (Mingograph) andrecordings were then analysed by hand.Electrodes were placed near the inner and outercanthi of each eye and a reference groundelectrode was placed onto the forehead. Thesubject's head was supported by a head rest. Inaddition, a binaural head clamp was used inpatients who could not keep their headsstraight voluntarily. The recordings were madewith the head directed to face the screen andwith eyes in the primary gaze position.
Saccadic eye movements were made to atarget projected onto a screen 1-3 metres fromthe patient by a video projector. The target, a10 pixel diameter spot of light subtending anangle of 1-30, was generated using a graphicsgenerator controlled by a micro-computer.The computer generated each of the targetdisplacement sequences, each sequence beingaccessed by selection from an on screen menu.An analogue signal of target displacement wastransformed to the paper recorder by a digitalto analogue converter, so that latencymeasurements could be made directly from therecording.The parameters of saccadic function exam-
ined were: random saccades, hidden predictivesaccades, predictive saccades, rememberedsaccades, and self-paced saccades. The targetmoved in a square wave step fashion across thescreen in the horizontal plane for each of theexperimental conditions. Subjects and controlsperformed all of the following experiments inone session. Each experimental paradigm wasseparated by a rest period ofapproximately twominutes.
496
on April 21, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.6.496 on 1 June 1990. D
ownloaded from

Saccadicfunction in spasmodic torticollis
Table 1 Clinical details
Patient Sex Age (yrs) Duration (yrs) Torticollis Drugs
1 M 29 1 Left Benzhexol2 F 43 4 Left Benzhexol3 F 63 25 Right Nil4 F 51 9 Right Diazepam5 F 55 3 Left Diazepam6 F 49 7 Right Lorazepam7 F 60 15 Left Nil8 F 54 22 Left Diazepam9 F 45 12 Right Benzhexol10 F 39 20 Left Nil11 F 60 5 Left Benzhexol12 F 60 6 Right Mianserin
Random saccades The target moved randomlybetween five different positions on the screen(one central and two on either side) generatingfour possible target amplitudes (150, 300,450, 60°). The time interval between targetdisplacements varied randomly between 0-5-2 s. The subject was instructed to look at thelight as quickly as possible as the target wouldbe moving in a random manner. The testduration was 78 s generating 36 steps.Hidden predictive saccades In this paradigm thesubject was given identical instructions as inthe random sequence. The experiment beganand ended with a series of random targetdisplacements, in the midst of which a regularsequence of 20 target displacements of 300 (150to either side of the midline with a time intervalof 1 s), appeared without warning. The testduration was 46 s.
Predictive saccades This paradigm consisted ofa regular sequence of30 target displacements of300 (150 to either side ofthe midline with a fixedtime interval ofone second). It was explained tothe subjects that the target would now move
regularly between two fixed points and that as
previously they should look at the light asquickly as possible (without any instructions onwhether they should try to predict or not). Thetest duration was 35 s.Analysis of results of random, hidden predictiveand predictive saccades Saccadic latencies andamplitudes (accuracy) were measured from therecord. Saccadic velocities were measured fromthe random sequence, 10 saccades of 300amplitude were used to calculate the meansaccadic velocity. The peak saccadic velocitywas measured from the slope of the selectedsaccade directly from the record, with thepaper speed at 100 mm/s and a calibration of10 = 1 mm. In the predictive saccadic sequencethe mean saccadic latency was calculated once arelatively stable plateau ofpredictive responseshad been achieved.Remembered saccades In this paradigm a centralfixation spot of light was presented to thesubject for a period oftwo seconds. One secondafter its onset a second light was illuminated200 to the right or left of the fixation spot, in asemi-randomised fashion, for a period of 200ms. Eight hundred milliseconds after theeccentric light was extinguished the fixationspot was also extinguished. A final spot of lightthen appeared two seconds later at the sameposition as the previously flashed eccentriclight and this remained on for five seconds. Thesubjects were instructed on the sequence of
lights that would be presented and were askedto fixate upon the central target whilst itremained illuminated. They were then instruc-ted to make a saccade to the position where theyhad seen the eccentric light, on extinction ofthecentral fixation spot, though no instruction asto how quickly this should be performed wasgiven. Subjects were asked to maintain fixationat this point until the final target was presentedand then to shift fixation to that position.Subjects were instructed that the sequenceconstituted one individual trial but no instruc-tions were given on the number of trials theywould receive. One "sample" trial was thenshown to the patient to establish whether thesubject had understood the instructions.Analysis of results The accuracy of the remem-bered saccades was analysed by measuring theamplitude of any corrective saccade made bysubjects from the point they judged to be theposition of the eccentric target (rememberedsaccade), to the true position of the eccentrictarget as represented by the final spot of light.Only the first four trials were analysed tominimise any learning effect. Unsuppressedsaccades made to the eccentric target before thefixation light was extinguished, were alsomeasured for their frequency, direction andrelationship to the direction of torticollis.Self-paced saccades In this experiment subjectswere instructed to make saccadic refixations asquickly as possible, between two fixed targetsthat were 150 to the right and left ofthe primaryfixation point. The test duration was 30 s.Analysis of results At least 20 gaze shifts wererecorded in each direction. Saccadic accuracywas expressed as a percentage of the amplitudeof the first saccade over total target dis-placement (300). The other variables measuredwere: 1) the half cycle time, that is, the timetaken from arrival at one target to arrival at theother; 2) the fixation time, the time of arrest onthe target; 3) the transit time, the time takenfrom leaving one target to arrival at the other.Statistical analysis of results Comparison wasmade between both patients and control groupsas a whole, and within the control and patientgroups for right and leftward saccades andipsilateral and contralateral saccades, respec-tively. Ipsilateral saccades were those saccadesmade in the direction ofchin displacement, andcontralateral saccades were those made in adirection opposite to that ofchin displacement.Initial analysis showed that, apart from meansaccadic velocities, the data was not distribu-ted normally, so non-parametric statisticalmethods were used. The non-parametric testsused were the Mann-Whitney U test and theWilcoxon Rank Sum test. A Student's t testwas used to analyse the result of the meansaccadic velocity. In all the statistical analysesonly values of p < 0-05 were consideredsignificant.
ResultsRandom saccades The mean latency of saccadesfor patients was 234 ms (SD 36), and forcontrols 208 ms (SD 29); this difference wasnot statistically significant (Z = 1-98). Nor
497
on April 21, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.6.496 on 1 June 1990. D
ownloaded from

Stell, Bronstein, Gresty, Buckwell, Marsden
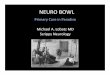
Figure I Mean saccadiclatency to the right andleft for controls, andipsilateral andcontralateral to thedirection of chindisplacement for patients,in the random, hiddenpredictive, and predictivesequences. No significantassymetry is evident foreither the control orpatient group.
-200
-100
000'
100.
200*
300
0,-i
Controls
Random saccades
Hidden predictive
Predictive
Ipsilateral--~~~~Contralateral
was there a significant difference when randomsaccades were related to the direction oftorticollis; the latency of ipsilateral randomsaccades was 233 ms (SD 18) and of contra-lateral random saccades 241 ms (SD 34),(Z = 1-18), fig 1. The mean peak saccadicvelocities for patients and controls were 452°/s(SD 86) and 434°/(SD 68) respectively; thisdifference was not significant (t = 0-36,Student's t test).Hidden predictive saccades Patients and controlswere equally able to make predictive andanticipatory saccades. The rate at which thelatency shortened appeared to be greater in thecontrol group. However, this difference was
not statistically significant using repeatedmeasures analysis of variance (MANOVA,F = 0 55). When hidden predictive saccadeswere related to the direction of the torticollis(fig 1), there was no assymetry in the patient'sability to progressively reduce their latencies,
either ipsilateral or contralateral to the direc-tion of torticollis.Predictive saccades Both groups rapidlydeveloped a predictive strategy and substan-tially reduced their latencies. There was no
significant difference between the mean latencyof predictive saccades for patients, -29-3 ms
(SD 15 9) and controls, -32-3 ms (SD 16-4),(Z = 0-08). When predictive saccades inpatients were related to the direction of theirtorticollis, the mean latency of ipsilateralsaccades was - 10-2 ms (SD 129) and ofcontralateral saccades was - 23-3 ms (SD 170);this difference was not significant (Z = 1-18),(fig 1).Remembered saccades Figure 2 shows therecords of one patient and one control anddemonstrates the ability of both to makeaccurate remembered saccades. In addition,the records show that both made occasionalpremature saccades to the eccentric target
Patients
498
on April 21, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.6.496 on 1 June 1990. D
ownloaded from

Saccadic function in spasmodic torticollis
Control200
-Vr
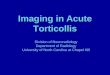
Figure 2 Saccadic eye Central fixation lightmovements for a normalcontrol and patient during Eccentric lightthe remembered saccadictask. The horizontal barsin the upper two tracesindicate the presence of thefixation and eccentriclights. The arrow indicatesthe occurrence of anunwanted saccade inresponse to theimmediately precedingappearance of the eccentriclight. Note that bothcontrol and patient madeaccurate rememberedsaccades as shown by theabsence of a correctivesaccade on reappearance ofthe eccentric light.
i-
ls
before the central fixation point was extin-guished. Such premature saccades were madeno more frequently by patients (18% of trials)than controls (170. of trials); nor was there a
difference in the frequency with which theywere made ipsilateral (510O) or contralateral(490°) to the direction of the torticollis(Z = 1-09). The latency of rememberedsaccades was 437 ms (SD 161) in controls and503 ms (SD 237) in patients; this differencewas not significant (t = 0O78). Rememberedsaccades which followed premature saccadestended to have much longer latencies thanthose not preceded by premature saccades.Occasionally latencies of up to two secondswere recorded as illustrated in fig 2.There was no significant difference between
the mean inaccuracy of remembered saccadesof patients 0.230 (SD 1-3) and controls 0A430(SD 1-54), (Z = 0 97). Nor was there a
significant difference in the mean inaccuracy ofremembered saccades made ipsilateral (0-31°,SD 1 12) and contralateral (0.160 SD 1-40) tothe direction of torticollis (Z = 0-38).Self-paced saccades Figure 3 shows the recordof a patient and a control, demonstrating thatboth were equally able to make rapid andaccurate self-paced saccades. Table 2 gives thecollective data for all the parameters of self-paced saccades. There was no difference be-tween mean half cycle times (Z = 1-03), or
fixation times (Z = 1 04) of patients comparedto controls. Both groups were able to makeaccurate saccades on rapid refixations. Withinthe patient group there was no differencebetween ipsilateral and contralateral saccadeseither for the fixation time (Z = 1 11) or halfcycle time (Z = 0 40). There was no differencein the mean accuracy of the first saccadebetween patients and controls, the value being98-3% (SD 1 7) for patients and 97X4% (SD3-8) for controls.
Control
I300
Patient
20ifPatient 0i
~~~~~~~~~~~~~~~~~~~~~~~~~~iI1 s
Figure 3 Saccadic eye movements of a normal controland patient made during the self-paced saccadicparadigm. The saccadic sequences above corresponds tosaccades made 20 s into the task, and show that controlsand patients were equally able to make rapid andaccurate refixations.
DiscussionPatients with torticollis showed no deficit in theproduction of random, predictive, remem-
bered or self-paced saccades. The ability tomake predictive and remembered saccades maydepend upon the integrity of projections fromthe frontal eye fields, via caudate nucleus, tothe substantia nigra reticulata, and from thereto cells within the intermediate and deep layersof the superior colliculus.89 It is via thispathway that the basal ganglia may exert theirinfluence on saccadic eye movements. Hiko-saka and Wurtz,4 using single cell recordings inprimates, localised a population of nigralreticulata cells whose high baseline dischargerates consistently fell 200 ms before theproduction of saccades made to rememberedtargets in the contralateral visual field. TheseGABAergic cells were found to exert tonicinhibition upon cells within the superiorcolliculus. The nigra reticulata cells (SNr), inturn, receive inhibitory GABAergic input fromthe corpus striatum.'0 Pathology affecting thebasal ganglia might be expected to interferewith this striato-nigro-collicular pathway, andthus impair the ability to make rememberedsaccades. In addition, the ability to makepredictive eye movements requires memory ofthe target both temporally and spatially, andtherefore may also be expected to be impaired.Reduction of inhibitory striatal output wouldincrease the tonic inhibition from nigrareticulata upon the cells of superior colliculus.These collicular cells are known to exhibitburst activity before saccades;1"1'3 increasedinhibition of superior collicular cells wouldtherefore be expected to produce prolongedlatencies and/or slowing of saccades. Experi-
Table 2 Parameters of self-paced saccades in torticollis patients and controls in ms, mean and (SD)
Fixation time Half cycle time
Bilateral* Ipsilateral Contralateral Bilateral* Ipsilateral Contralateral
Patients 414 (106) 426 (99) 401 (119) 497 (106) 505 (100) 490 (130)Controls 359 ( 99)
*Refers to ipsilateral/contralateral (right and left in controls), values combined.
499
on April 21, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.6.496 on 1 June 1990. D
ownloaded from

Stell, Bronstein, Gresty, Buckwell, Marsden
mental support for this prediction was found,in that injection of the GABA agonist, mus-cimol into the superior colliculus producedslow, hypometric saccades with long latencies,especially to remembered saccades.4 15
Clinical evidence supporting the role of thebasal ganglia in the production of predictive,remembered and self-paced saccades comesfrom several studies of eye movement inpatients with diseases of this region of thebrain, and in particular in Parkinson's disease.Dejong and Melvill Jones'6 found that whilstpatients with Parkinson's disease had normalsaccadic metrics to random target displace-ments, they took longer to make self-pacedsaccades between two stationary spots of light,and these were more inaccurate than thosemade by age matched controls. Bronstein andKennard5 found that Parkinsonian patients hadan impairment of predictive saccades and aninability to utilise verbal information on targetdisplacement to improve their performance. Inaddition, these patients had a tendency to makesaccades of longer latency than controls, re-gardless of the mode of presentation of thestimulus.5"' These abnormalities were ascribedto reduction of excitatory dopaminergic inputinto the caudate nucleus, producing disinhibi-tion of the SNr and subsequent inhibition ofthe superior colliculus.
In Huntington's disease (HD), in whichthere is a loss of caudate and SNr neurons'8with normal dopamine levels, a characteristicabnormality of saccadic function has beenfound. There is impairment in initiation ofvoluntary and remembered saccades, markedfixational instability, and an inability tosuppress unwanted saccades to new visualstimuli.'"2" Loss of GABAergic inhibition ofthe superior colliculus by the SNr wouldreasonably explain the above abnormalities.Dysfunction of the superior colliculus has alsobeen used to explain the more recent findingsof saccadic slowing in younger patients withHD.22Though no pathological or neurochemical
abnormality has been found in patients withtorticollis, this condition may result fromdysfunction of the basal ganglia.' Clinicalexamination of eye movements in patients withidiopathic dystonia is usually normal, apartfrom minor abnormalities of smooth pursuitrelated to medication. Whilst there are reportsdemonstrating a directional preponderance ofvestibular nystagmus23 and impaired ocularcounterolling in torticollis,23 there have been noother detailed studies analysing eye movementsin this condition. The absence of saccadicdysfunction in patients with torticollis shownby this investigation strongly suggests that,while other parts of the basal ganglia may beimplicated pathophysiologically, it is unlikelythat the striato(caudato)-nigro-collicularpathway is involved. It is now recognised thatthe basal ganglia are components of severalparallel, "basal ganglia-thalamocortical" cir-cuits, each receiving inputs from separatecortical areas, the above oculomotor pathwayrepresenting but one of these circuits. Eachhas functional specialisation and projects, in an
anatomically segregated fashion, within thebasal ganglia.24 The integrity of this "oculo-motor circuit" therefore does not exclude thepossibility of dysfunction in other regions ofthe basal ganglia in torticollis.An alternative interpretation of the negative
results in this study is that the basal gangliamay not be primarily involved in the patho-genesis of torticollis. There are very fewreports of spasmodic torticollis due to anidentified focal lesion in the basal ganglia.Focal lesions involving the caudate andputamen'25 have produced torticollis, but sotoo have lesions of the mesencephalic teg-mentum,62 spinal cord and posterior fossa. 29Unfortunately, many ofthe cases reported havehad lesions at other sites making interpretationdifficult. Experimental torticollis in primateshas been reported with lesions of selectedbrainstem reticular nuclei, in particular theInterstitial Nucleus of Cajal which is known tohave reciprocal connections with the vestibularnuclei and basal ganglia.03' It is possible thatthe basal ganglia themselves are not primarilyinvolved in the pathogenesis of spasmodictorticollis, which may be due instead to anabnormality of one or more brainstem struc-tures, with which the basal ganglia areintimately connected.
We thank the Dystonia Medical Research Foundation forfinancial support, and Marjan Jahanshahi for her help instatistical analysis of the results.
1 Marsden CD, Obeso JA, Zarranz JJ, Lang AE. Theanatomical basis of symptomatic hemidystonia. Brain1985;108:463-83.
2 Bronstein AM, Rudge P. Vestibular involvement in spas-modic torticollis. J Neurol Neurosurg Psychiatry 1986;49:290-5.
3 Stell R, Bronstein AM, Marsden CD. Vestibulo-ocularabnormalities in spasmodic torticollis before and afterbotulinum toxin injections. JNeurol Neurosurg Psychiatry1989;52:57-62.
4 Hikosaka 0, Wurtz RH. Visual and oculomotor functions ofmonkey substantia nigra pars reticulata. 111. Memory-contingent visual and saccade responses. J Neurophysiol1983;49: 1268-83.
5 Bronstein AM, Kennard C. Predictive ocular motor controlin Parkinson's disease. Brain 1985;108:925-40.
6 Carl JR, Wurtz RH. Asymmetry of saccadic control inpatients with hemi-parkinsonism. Assoc Res Vis Ophth1985:258.
7 Webster KE. The cortico-striatal projection in the cat. JAnat 1965;99:329-37.
8 Jayaraman A, Batton RR, Carpenter MB. Nigrotectal pro-jections in the monkey: an autoradiographic study. BrainResearch 1977;135:147-52.
9 Graybiel AM, Ragsdale CW. Fiber connections of the basalganglia. In: Cuenod M, Kreutzberg GW, Bloom FE, eds.Development and chemical specificity of neurons.Amsterdam: Elselvier, 1979:239-83.
10 Vincent SR, Hattori T, McGeer EG. The nigrotectalprojection: a biochemical and ultrastructural characterisa-tion. Brain Res 1978;151:159-64.
11 Wurtz RH, Goldberg ME. Activity of superior colliculus inbehaving monkey. III. Cells discharging before eyemovements. J Neurophysiol 1972;35:575-86.
12 Schiller PH, Koerner F. Discharge characteristics of singleunits in superior colliculus of the alert rhesus monkey.J Neurophysiol 1971 ;34:920-36.
13 Wurtz RH, Mohler CW. Organization of monkey superiorcolliculus: Enhanced visual response of superficial layercells. J Neurophysiol 1976;39(4):745-65.
14 Hikosaka 0, Wurtz RH. Modification of saccadic eyemovements by GABA related substances I. Effect ofmuscimol and bicuculline in monkey superior colliculus.J Neurophysiol 1985a;53:266-91.
15 Hikosaka 0, Wurtz RH. Modification of saccadicmovements by GABA related substances II Effects ofmuscimol in monkey substantia nigra pars reticulata. JNeurophysiol 1985b;53:292-308.
16 DeJong JD, Melvill Jones G. Akinesia, hypokinesia, andbradykinesia in the oculomotor system of patients withParkinson's disease. Exp Neurol 1971;32:58-68.
17 White OB, Saint-Cyr JA, Tomlinson RD, Sharpe JA.
500
on April 21, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.6.496 on 1 June 1990. D
ownloaded from

Saccadic function in spasmodic torticollis
Ocular motor deficits in Parkinson's disease. II. Control ofthe saccadic and smooth pursuit systems. Brain 1983;106:571-8.
18 Lange H, Thorner G, HopfA, Schroder KF. Morphometricstudies of the neuropathological changes in choreaticdiseases. J Neurol Sci 1976;28:401-25.
19 Starr A. A disorder ofrapid eye movements in Huntington'schorea. Brain 1967;90:545-64.
20 Petit H, Milbled G. Anomalies of conjugate ocular move-
ment in Huntington's chorea: application to early detec-tion. In: Barbeau A, Chase TN, Paulson TW, eds.Advances in Neurology, Vol 1. New York: Raven Press,1973:287-94.
21 Leigh JR, Newman SA, Folstein SE, Lasker AG, JensenBA. Abnormal oculomotor control in Huntington'sdisease. Neurology (Cleveland) 1983;33:1268-75.
22 Lasker AG, Zee DS, Hain TC, Folstein SE, Singer HS.Saccades in Huntington's disease: slowing and dysmetria.Neurology 1988;38:427-31.
23 Diamond SG, Markham CH, Baloh RW. Ocular counteroll-ing abnormalities in spasmodic torticollis. Arch Neurol
1988;45:164-9.24 Alexander GE, DeLong MR, Strick PL. Parallel organiza-
tion of functionally segregated circuits linking basalganglia and cortex. Ann Rev Neurosci 1986;9:357-81.
25 Maki Y, Akimoto H, Enomo T. Injuries of basal gangliafollowing head trauma in children. Child's Brain 1980;7:113-23.
26 Guillain G, Bize R. Sur un cas de scierose en plaques avectorticolis spasmodique. Rev Neurol 1933;40:133-8.
27 Herz E, Glaser GH. Spasmodic torticollis. Arch NeurolPsychiat 1949;61:227-39.
28 Kiwak KJ, Deray MJ, Shields WD. Torticollis in threechildren with syringomyelia and spinal cord tumor.Neurol (Cleveland) 1983;33:946-8.
29 Boiser E. Torticollis caused by an infratentorial tumor: threecases. B J Psychiat 1979;134:306-7.
30 Foltz EL, Knopp CM, Ward AA. Experimental spasmodictorticollis. J Neurosurg 1959;16:55-72.
31 Fukushima K, Takahashi J, Kudo J, Kato M. Interstitial-vestibular interaction in the control of head posture. ExpBrain Res 1985;57:264-70.
501
on April 21, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.6.496 on 1 June 1990. D
ownloaded from