Embed Size (px)
Citation preview
AHCA Form 5000-3549, October 2013 1 Rule Number 59G-6.010, FAC
NFQA HELP INSTRUCTIONS - MONTHLY REPORTING
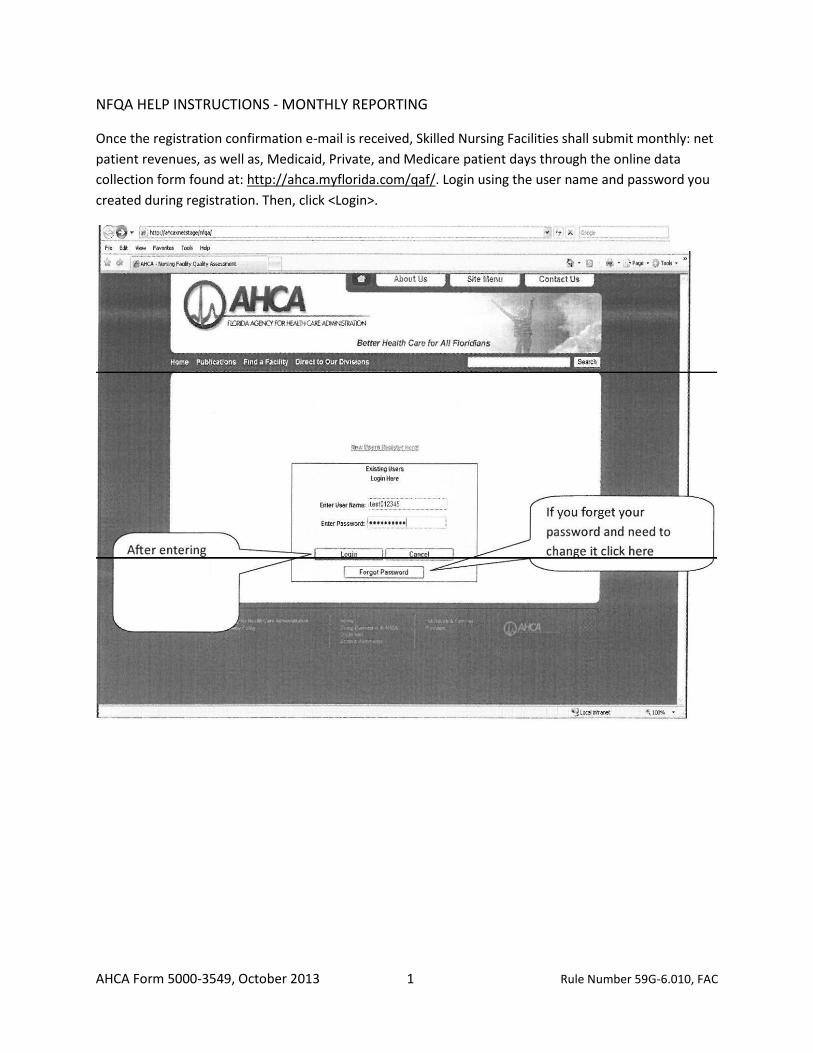
Once the registration confirmation e-mail is received, Skilled Nursing Facilities shall submit monthly: net
patient revenues, as well as, Medicaid, Private, and Medicare patient days through the online data
collection form found at: http://ahca.myflorida.com/qaf/. Login using the user name and password you
created during registration. Then, click <Login>.
NFQA HELP INSTRUCTIONS-MONTHLY REPORTING
AHCA Form 5000-3549, October 2013
Rule Number 59G-6.010, FAC
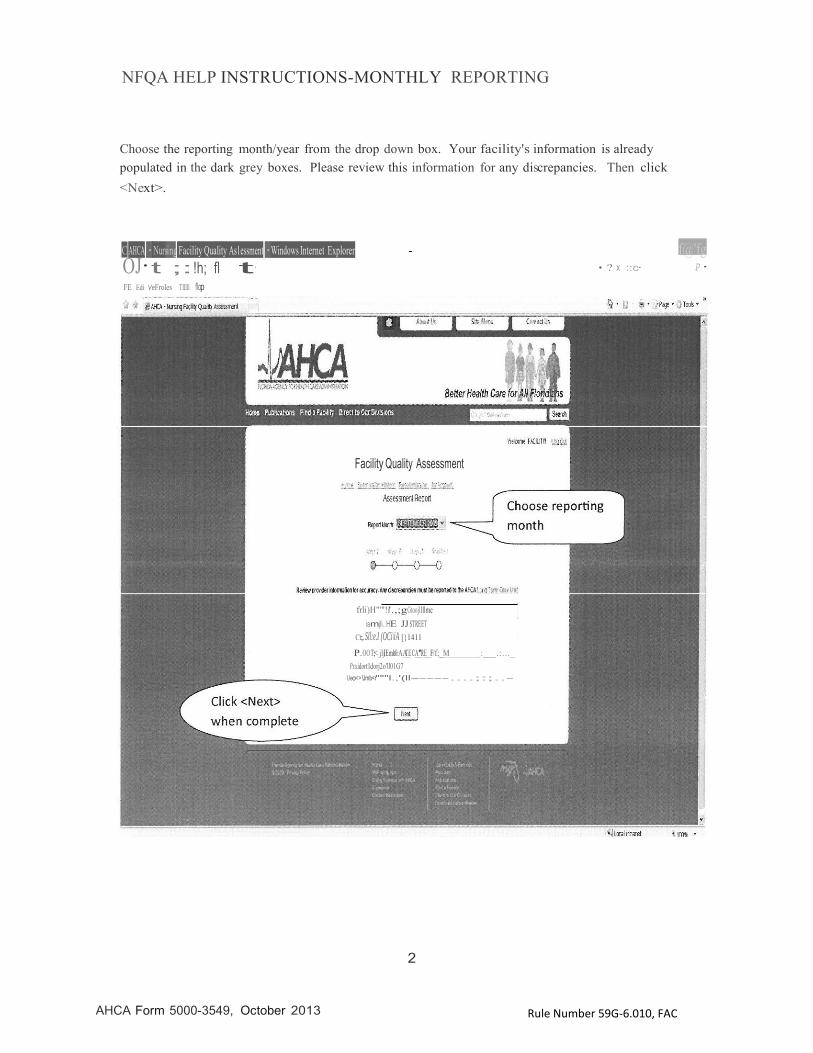
Choose the reporting month/year from the drop down box. Your facility's information is already populated in the dark grey boxes. Please review this information for any discrepancies. Then click <Next>.
C_AHCA ·Nursing Facility Quality As1essment ·Windows Internet Explorer - f@'fg OJ·t ;:!h; fl t· FE Edi VeFroles Tlllll flop
• ? X ::c· P·
Facility Quality Assessment
frli)H"'"!i'.,;gGtoojllllme iamjli..HE JJ STREET
Ct;.Sll:e.I (OCi\iA [}1411
P..OOT;< jljlEmo'frAATE CA_'RE_F/f;_M Pra.idortl.dorj2o'll01G7
_: .:..._
Ueo<>!Jmb<r"""l.,'(ll ----....;:;..-
2
NFQA HELP INSTRUCTIONS-MONTHLY REPORTING
AHCA Form 5000-3549, October 2013
Rule Number 59G-6.010, FAC
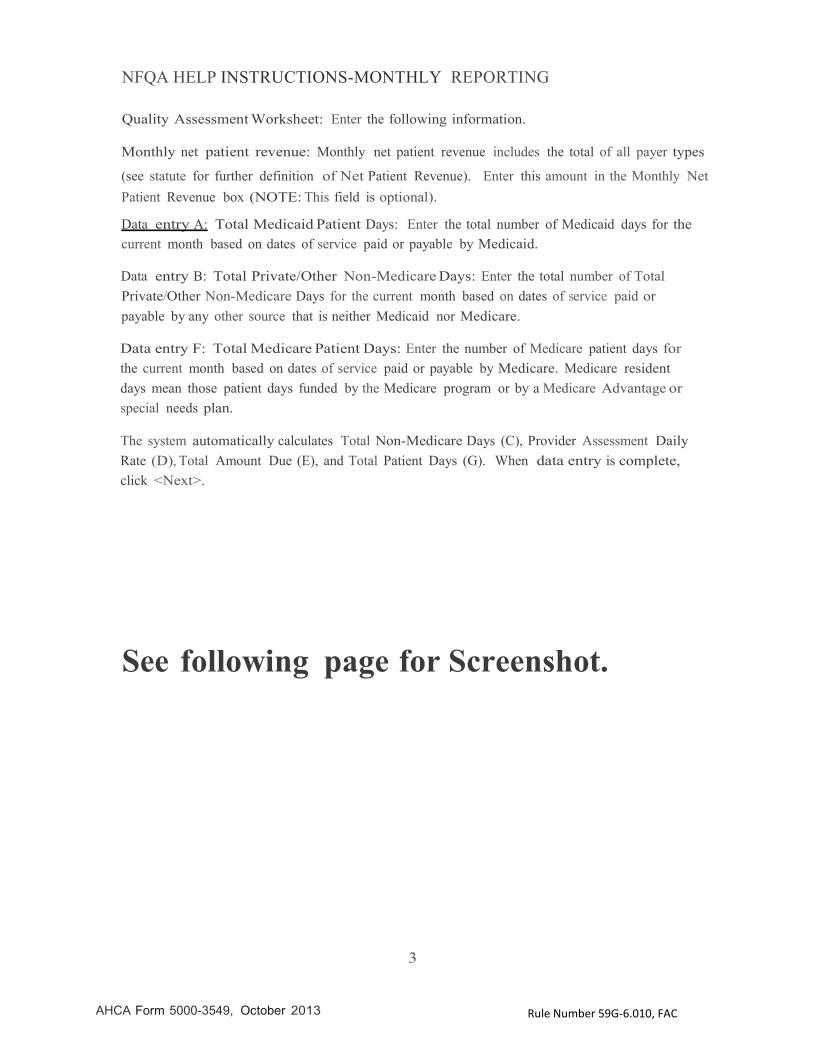
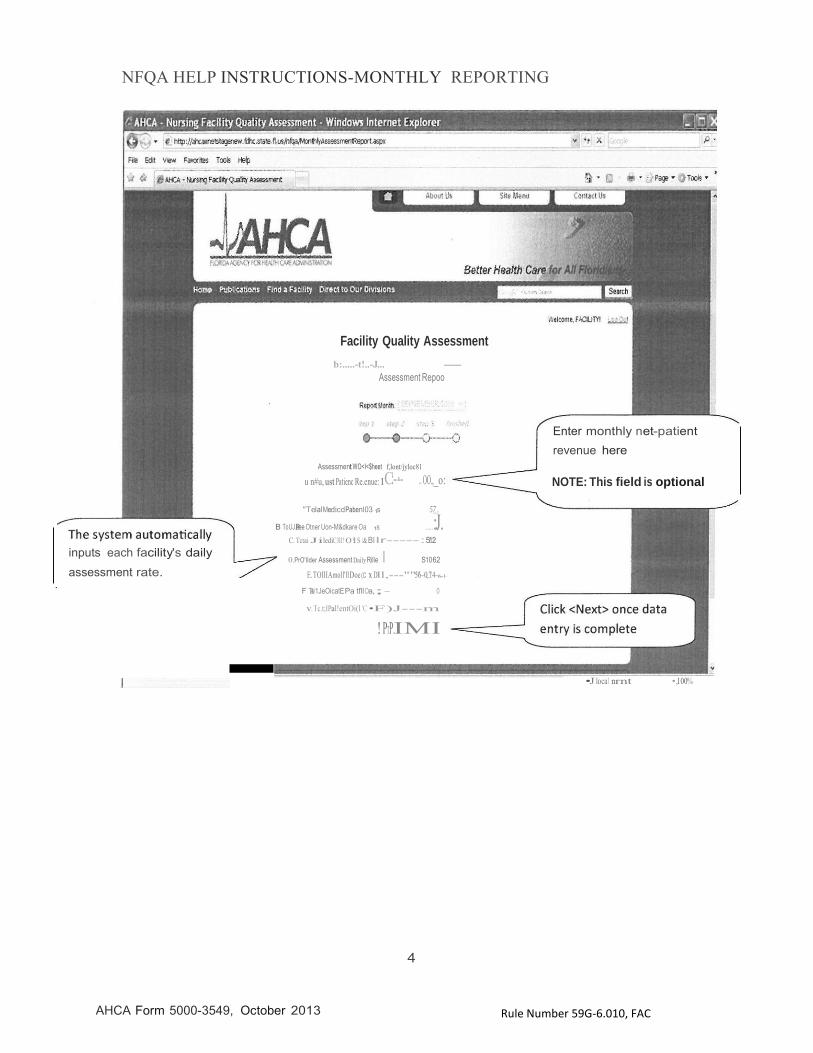
Quality Assessment Worksheet: Enter the following information.
Monthly net patient revenue: Monthly net patient revenue includes the total of all payer types
(see statute for further definition of Net Patient Revenue). Enter this amount in the Monthly Net Patient Revenue box (NOTE: This field is optional).
Data entry A: Total Medicaid Patient Days: Enter the total number of Medicaid days for the current month based on dates of service paid or payable by Medicaid.
Data entry B: Total Private/Other Non-Medicare Days: Enter the total number of Total Private/Other Non-Medicare Days for the current month based on dates of service paid or payable by any other source that is neither Medicaid nor Medicare.
Data entry F: Total Medicare Patient Days: Enter the number of Medicare patient days for the current month based on dates of service paid or payable by Medicare. Medicare resident days mean those patient days funded by the Medicare program or by a Medicare Advantage or special needs plan.
The system automatically calculates Total Non-Medicare Days (C), Provider Assessment Daily Rate (D), Total Amount Due (E), and Total Patient Days (G). When data entry is complete, click <Next>.
See following page for Screenshot.
3
NFQA HELP INSTRUCTIONS-MONTHLY REPORTING
AHCA Form 5000-3549, October 2013
Rule Number 59G-6.010, FAC
Facility Quality Assessment
b:.....-t!..-J... -
Assessment Repoo
Assessment WO<I<$heet f,lont/jyloc81
Enter monthly net-patient
revenue here
u n#u, ust Patienc Re.enue:1C:--·- .. OO.,_o: NOTE: This field is optional
inputs each facility's daily
assessment rate.
"TelalMedicdPabenl03 1s 57_,
B ToUJ.Paee Otner Uon-M&dkare Oa 1s .....:J. C. Tctai JilediC3ll! O!i S I& Bl lr----- :5:1:2::
0.PrO'IIder Assessment Daily Rille I S1062
E.TOIIIAmoll'll Doe (C x Dll,---""56'-0,7:4-6-:--1:-
F Tati1JeOicatE Pa tfllOa,;- 0
v.Tc.t;IPal!entOi(l 'C •F)J---m
!PrP.IMI
•Jlocal nrnt •,100%
4
NFQA HELP INSTRUCTIONS-MONTHLY REPORTING
AHCA Form 5000-3549, October 2013
Rule Number 59G-6.010, FAC
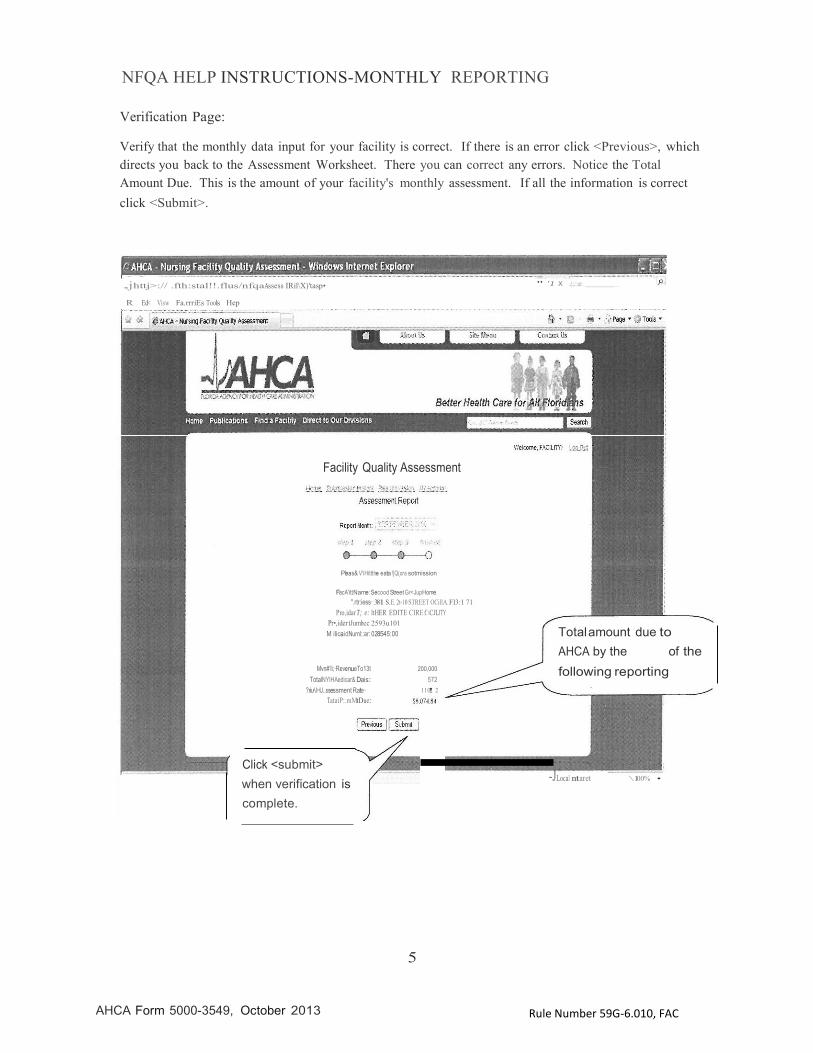
Verification Page:
Verify that the monthly data input for your facility is correct. If there is an error click <Previous>, which directs you back to the Assessment Worksheet. There you can correct any errors. Notice the Total Amount Due. This is the amount of your facility's monthly assessment. If all the information is correct click <Submit>.
..jhttj>:// .fth:stal!!.flus/nfqaAssess IRil\X)'tasp•
R Ed< Visw Fa.rrriEs Tools Hep
" '1 X .(..:;:.::,v::..c:.· _
Facility Quality Assessment
Pleas& V'iHittthe eata !}Q(ora sotmission
FacA'ittName: Secood Street Gr<JupHome
".rtr:iess·381 S.E. 2t-10 STREET OCillA. Fl3:1 71 Pro,idar T; e: ltHER EDITE CIRE f.\CJLJTY
Pr•,ider tJumbec 2593u101 M ilicaidNurnl::ar: 028545:00
Total amount due to
AHCA by the of the
Mvn#'li;·RevenueTo13t
TotalNYIHAedicar& Dais:
?riu·\HJ..ssessment Rate·
TataiP:.mMtDue:
200,000
572
110! 2
following reporting
Click <submit>
when verification is
complete.
-JLocal ntaret \ 100% •
5
NFQA HELP INSTRUCTIONS-MONTHLY REPORTING
AHCA Form 5000-3549, October 2013
Rule Number 59G-6.010, FAC
ent :-Wi ndo lnl;rne
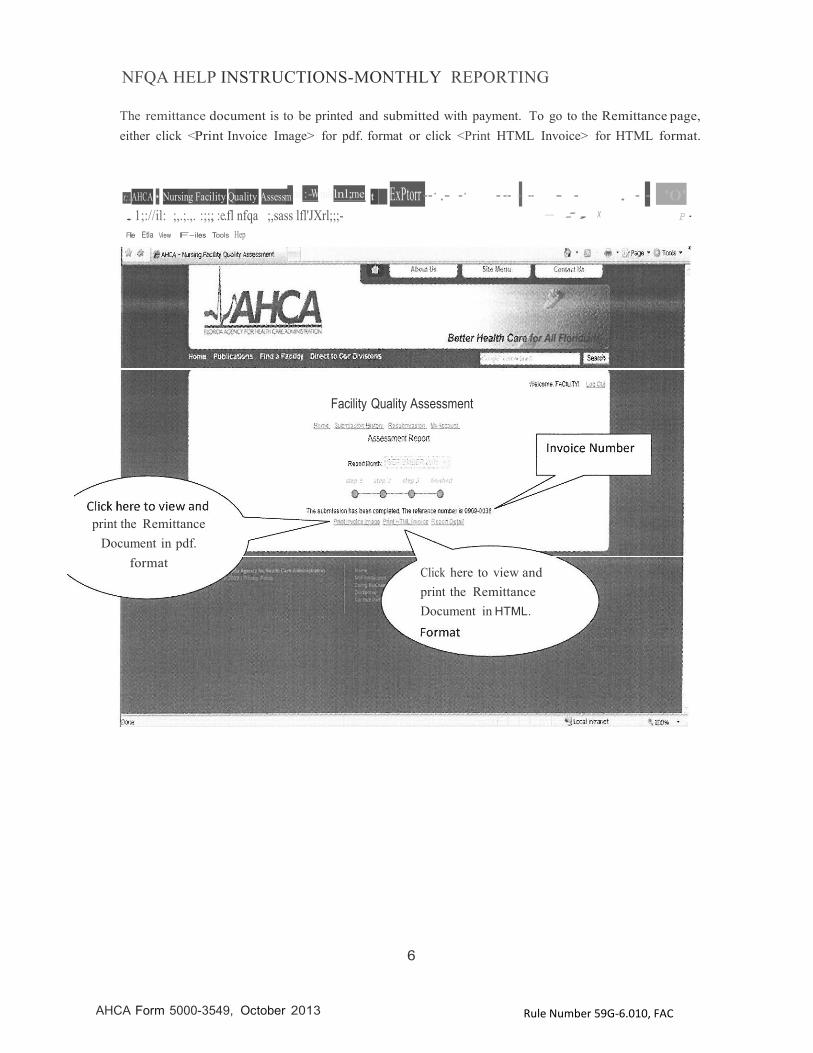
The remittance document is to be printed and submitted with payment. To go to the Remittance page, either click <Print Invoice Image> for pdf. format or click <Print HTML Invoice> for HTML format.
t;.AHCA • Nursing Facility Quality Assessm .1;://il: ;,.;.,. :;;,; :e.fl nfqa ;,sass lfl'JXrl;;;- Flie Etla View F- iles Tools Hep
t ExPtorr --· .- -· - -- - -- - - . - - '0' - :, X P·
Facility Quality Assessment
print the Remittance Document in pdf.
format
Click here to view and print the Remittance Document in HTML.
6
NFQA HELP INSTRUCTIONS-MONTHLY REPORTING
AHCA Form 5000-3549, October 2013
Rule Number 59G-6.010, FAC
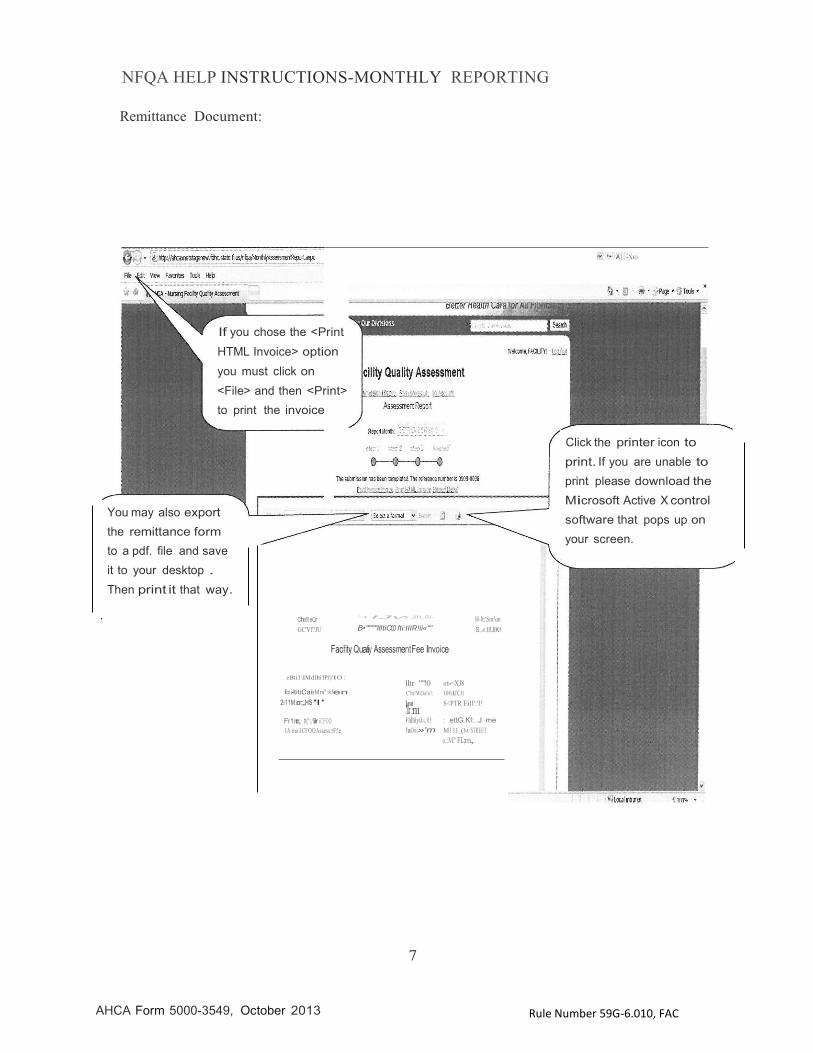
Remittance Document:
If you chose the <Print
HTML Invoice> option
you must click on
<File> and then <Print>
to print the invoice
You may also export
the remittance form
to a pdf. file and save
it to your desktop .
Then print it that way.
Click the printer icon to
print. If you are unable to
print please download the
Microsoft Active X control
software that pops up on
your screen.
Cha!l!eCr
GC'Vf?JU
"'.- • IJvo ..IIH,;RI-
B•""""llltiCf,O fti:IIIR!ii«""
Facifity Quatiy AssessmentFee Invoice
H-lt;'Sm!on S..«:II!JIKI
eBti1\IMdllti'IPJ)'IO :
for i-ltitiCaieMni":kfen
lltr '"'10 ot»<XJ8 C'lti!WOa!o!: 10fi1,l'CJI
2i11M;cnr;,,HS'I' l'.llocpro,r·tm S<PTR Eill':'l!
Fr1mc,:·.tt(':;/ll,ir iCFOO IA mo:ICFOOAssess:rF:!e
FldlilyiJa,'ilf: : ettG.Kl:..J me
FaOiii»'m M I $.E_ (ht STREET o.:M." FL;m,
7
NFQA HELP INSTRUCTIONS-MONTHLY REPORTING
AHCA Form 5000-3549, October 2013
Rule Number 59G-6.010, FAC
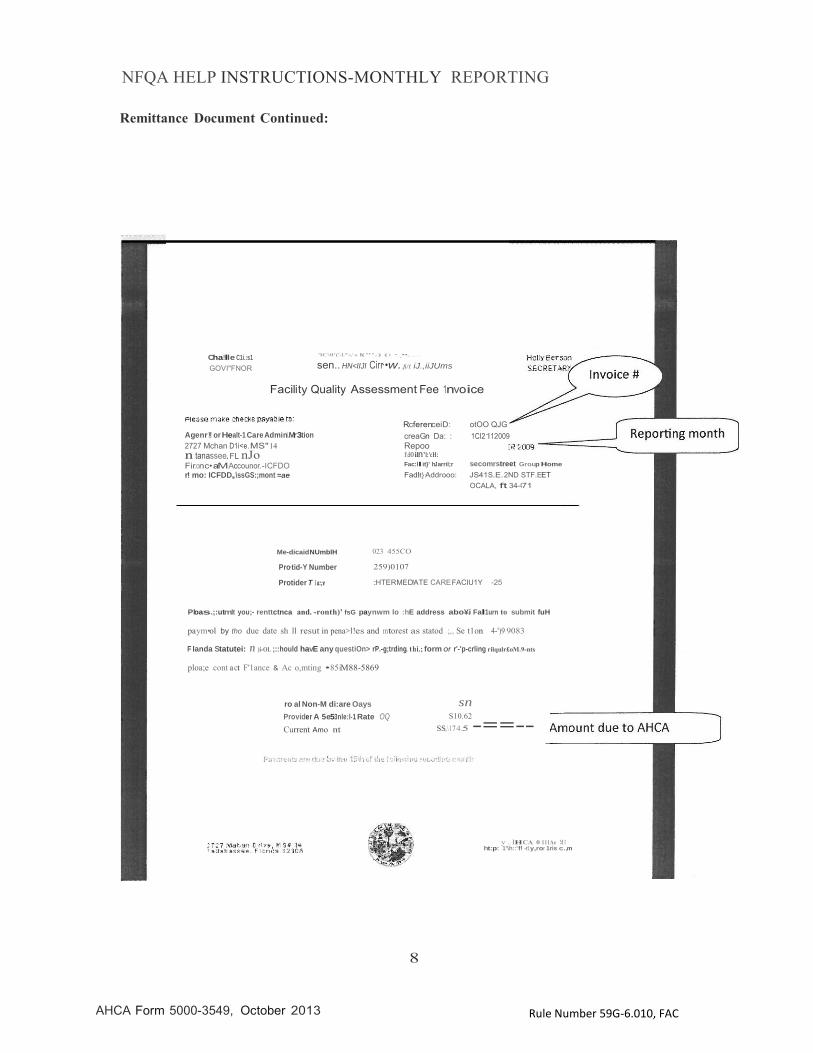
Remittance Document Continued:
Cha!lle C1i.:s1
GOVI"FNOR
'lC\0'('-L"'«,'-o. l("'.) (: ·._••,......
sen.. HN<IIJI Cirr·•w.. fi/1 iJ.,iiJUms
Facility Quality Assessment Fee 1nvoice
Agenr!or Healt-1 Care Admini.Mr3tion
2727 Mchan D1i<e. MS" 14 n tanassee. FL nJo Fir.onc•aMAccounor.-ICFDO r! mo: ICFDD,\ssGS:;mont =ae
RcferenceiD: otOO QJG
creaGn Da: : 1CI2112009
Repoo 1\:lO ilfY'l:'cH: Fac:ll it}' hJ arril;r secomrstreet Group Home
Fad!it}·Addrooo: JS41S.E. 2ND STF.EET
OCALA, ft 34-471
Me-dicaidNUmblH 023 455CO
Pro·tid-Y Number
Protider T 1a:;e
259)0107 :HTERMED!ATE CARE FACIU1Y -25
Ploas.;:utmlt you;- renttctnca and. -ronth)' fsG paynwm lo :hE address abo¥.i Fal1urn to submit fuH
paym•ol by tho due date sh ll resut in pena>l!es and mtorest as statod ;,., Se t1on 4-')9 9083
F Ianda Statutei: n )i-OL ;::hould havE any questiOn> rP.-g;trding. t hi.; form Of r'-'p-crling rilqulr£oM.9-nts
ploa;e cont a ct F'1ance & Ac o,mting •85iM88-5869
ro al Non-M di:are Oays
Provider A 5e53nle:l-1 Rate OQ
Current Amo nt
8
sn S10.62
SS,\17 4.5 -==--
y ,. lHCA 0 111Ae !:1 1 ht:p: 1'\h::'f! -r1y,ror 1ris c.,m
NFQA HELP INSTRUCTIONS-MONTHLY REPORTING
AHCA Form 5000-3549, October 2013
Rule Number 59G-6.010, FAC
COMPLETE!
9