Embed Size (px)
Citation preview

J Nurs Care QitalVol. 22, No. I. pp. 4-7© 2007 Uppincott Williams & WUklns, toe.
Quality Improvement in Long-term CareThe purpose of this column is to discuss innovations and quality improvement efforts in a variety oflong-term care settings. These issues are of importance to healthcare professionals as our nationfaces the burgeoning growth of the aging population, creating increased demand for improved andinnovative long-term care services. This column is coordinated by Marilyn J. Rantz, PhD, RN, FAAN,NHA, e-mail: [email protected].
Measuring Quality of Care inAssisted LivingA New Tool for Providers,Consumers, and Researchers
Myra A. Aud, PhD, RN; Marilyn J. Rantz, PhD, RN, FAAN;Mary Zwygart-Stauffacher, PhD, RN, FAAN;Marcia Flesner, PhD, RN
ASSISTED LIVING FACIUTIES have ex-ploded in number in the United States,
particularly in the 1990s, wth an estimated8(H),(K)0 residents being cared for in 33.000assisted living facilities.' Actually, there arenow more assisted living facilities than nurs-
From the Sinclair School of Nursing attd Family andCommunity' Medicine. School of Medicine. Universityof Missouri-Columbia (Drs Au<l. Rantz, andFlesner): and College of Nursing and Health Sciences,Utiitvrsity of Wiscotisin-Eau Claire (DrZttrygartStauffacber).
T/je authors acknowledge the contributions of othermembers of the Unittersity of Missouri-Columbia MDSand Nursing Home Quality Research Team and consul-tants to this work. We gratefutly acknowledge the ongo-ing support ofthe Missouri Department of Health andSenior Services staff. Missouri Healthcare Association,and Missouri Association of Homes and Services for theAged.
Research activities uviv partially supported by NINRIR0INR/AG0'7287-01A2. Opinions are those of the au-thors and do not represent NINR.
Corres/xinding author Myra A. Aud. PhD, /tV SinclairSchool of Nursing, University of Missouri-Columbia,Columbia, MO 65211 (e-mail- atidm@missouriedu).
ing homes in the United States, but nursinghomes continue to care for more elders. Nurs-ing homes now number about 20,000 andcare for about 1.7 million frail older adultswith expected growth to 5 million in 2030.'It is likely that a parallel growth in assisted liv-ing can be anticipated as baby boomers ageand need long-term care.
As quality of care has been and continues tobe a key issue in nursing homes, ' there areconcerns about quality of care in assisted liv-ing facilities.'" Consumers need guidance asthey select an assisted living facility for a lovedone, providers need standards for judging thequality of their services, and researchers neednew tools for measuring the multidimensionalconcept of quality of care in assisted living.
Members of the MDS and Quality ResearchTeam at the University of Missouri-Columbiahave Ixren working for many years to under-stand and measure quality of care in nurs-ing homes in an effort to assist facilitiesin continuously improving their care quality.The team conducted initial qualitative studiesthat explored the multidimensional aspects of

Measuring Quality of Care in Assisted LiiHng 5
quality of nursing home care and developed atool to measure quality of care based on theresults of several studies.^''
As the development proceeded for thetool titled Observable Indicators of NursingHome Care Quality Instrument iOlQ-NH),members of the team were interested in ex-ploring the applicability of the measure forquality of care and tailoring it for the assistedliving environment. After an initial field test in35 facilities, the instrument was revised butretained its overall structure of a 5-point rat-ing scale for each question with anchoringdescriptors for each point." Similar to thenursing home version, nurse observers wereoriented to use the instrument with a user'sguide that provides directions about how toperform a 20- to 30-minute tour of a fiacilityprior to answering the questions.
A major field study of the OIQ-NH wasfunded by the National Institute of Nurs-ing Research of the National Institutes ofHealth to further develop the nursing homeversion of the quality-t>f-care measurementinstalment.'^ Wliile collecting data in nurs-ing homes, registered nurse (RN) observersalso completed the assisted living version ofthe Observable Indicators of Quality-AssistedLiving {OIQ-AL) scores when assisted livingfacilities were on the campuses of the nurs-ing homes in the primary study. Additionalfree-standing facilities (not on campuses withnursing homes) were visited to include themin the sample for the analysis of assisted living.In this column we review the major results ofthe field test in assisted living facilities and of-fer some practical guidance for the use of theOJQ-AL in quality improvement programs forthis growing environment of long-term care.
OVERVIEW OF RESULTS OF FIELD TESTIN ASSISTED LIVING USING THE OIQ-AL
The primary aim of the stud>' was to ad-vance the development of the OIQ-AL forase by researchers studying the dimensionsof care quality in assisted living. A secondarystudy aim was to assess the psychometricproperties of the OIQ-AL instrument when
used by nurse observers. Complete resultsare described in a psychometric article in re-view at this time (M. Rantz et al, unpublisheddata, 2006). In addition, it was anticipatedthat the mstrument would likely be helpful toproviders to use in their quality improvementprograms and consumers as they visit facilitiesfor themselves or loved ones.
In an earlier study, validity of the OIQ-ALwas judged as valid by a panel of experts woric-ing in assisted living.'' Relevance of each itemwas rated on a 4-point scale: not relevant,somewhat relevant, quite relevant, and veryrelevant.'^ The content v;ilidity index for thetotal scale was 3.426 with only 5 items hav-ing average ratings less than 3.00, none ofwhich were less than 2.0. Before this largerfield test, a new panel of 5 experts workingin assisted living was convened to discuss theitems and suggest additional items importantto the growing assisted living industry. The re-search team drafted new items and a revisedinstrument with 41 items was used for thefield test.
The sample of facilities was solicited from2 states, Missouri and Wisconsin, as a part ofthe larger NINR-sponsfired field study.'^ Datawere collected from 216 assisted living facil-ities (198 in Missouri and 18 in Wisconsin);of these, observations from 207 different as-sisted Uving facilities were complete and us-abie for analysis. Observers were RNs whocompleted the OQI-AL after a focused 20- to30-minute walk-through of each assisted liv-ing facility. For interrater purposes, a pair ofobservers visited 73 facilities. Test-retest visitswere made to 77 facilities.
An exploratory factor analysis and the meth-ods of Classical Test Theory and Generalizabil-ity Theory were used to study the reliabilityand validity of data obtained by the observers.Item analysis and exploratory factor analysisresulted in a final instrument of 34 reliableitems with a coherent (>factor structure. The6 factors were named by the research team:Homelike, Caring, Access and Choice, Light-ing, Pets and Plains, and Outdoor Spaces.
The revised 34-item instrument wasthen analyzed for interrater and test-retest

6 JOURNAL OF NURSING CARE QuAUTY/IA aJARY-MARCH 2007
correlations. Coefificient alphas were calcu-lated for all first RN visits to all facilities in thestudy. Findings revealed acceptable interrateriuid test-retest reliability evidence in additionto strong internal consistency for the totalinstrument and all but one subscale (OutdoorSpaces). As a final step, a GenenilizabilityTheory analysis was performed to combinethe sotirces of error into a single coefficient.These results were applied to a DecisionStudy that revealed the reliability of theinstrument can be improved by increasingthe numbers of visits from 1 to 2 or byincreasing the numbers of raters from 1 to 2.This improvement may be of importance toresearchers or to consumers with sufficienttime to make 2 site visits to a facility or have afriend or family member accompany them onone site visit and each score the instrument.An important feature of tlie instrument is thatit is highly reliable when used by multipleusers or multiple times (or a combination ofthe 2).
Scoring guidelines to help those who usethe instrument interpret the results were de-veloped for each subscale and the total scoreofthe OIQ-AL. Guidelines were developed onthe basis of the distribution of scores fromall the observations in the study, as was donefor the nursing home version in the largerstudy.'^ OIQ-AL scores above the 80th per-centile were chosen as suggestive of a qualityfacility; scores below the 20th percentile wereviewed as suggestive of quality problems.
The work performed on the OIQ-AL overthe past several years and the psychomet-ric evidence from the most recent researchindicates that the OIQ-AL is a brief instru-ment that evaluates the multidimensionalconcept of quality of care in assisted liv-ing facilities in a reliable and valid manner(M. Rantz et al, unpublished data, 2006).Copies of the instrument with a user's guidecan be ordered from the Web site main-tained by the research team at the Uni-versity of Missouri; excerpts of the instru-ment and more information are available onthe Web site www.nursinghomehelp.org forproviders, consumers, and other researchers.
USING THE OIQ-Al IN QUALITYIMPROVEMENT PROGRAMS
For assisted living facilities, there are advan-Uges of routinely using the OIQ to evaluatetheir overall quality of care. On the basis ofthefindings of our most recent field testing (M.Rantz et al, unpublished data. 20(K>), we sug-gest 2 observers tour a facility on the same dayand at the same time, not discuss their obser-vations, and then each independently score aninstrument. Their scores are averaged for eachitem, and subscale scores and total scores arecalculated (directions are provided on the in-strument). Using 2 raters and averaging tlieirscores improves the reliability of the instru-ment. An alternative that also improves reli-ability is for 1 rater to tour on 2 occasions,such as touring on 1 day and scoring a firstinstrument then touring the next day or laterin the week and scoring a second instrument(not referring to the first). Then the 2 instru-ments are averaged for each item, and sub-scale scores and total scores are calculated.
Perhaps a board member, community mem-ber, or panicular staff could be asked to teamup each month to complete the instrumentsand report results to a quality improvementteam in the facility. Involving board membersor others in quality improvement can be help-ful to facility staff who may become accus-tomed to viewing things as "well it is alwaystliat way" or "gee, we always do that." Anotherplan might be to have members of a facilityquality improvement team tour and score theinstrument monthly; in this case, it would beimportant for the staff member to approachthe facility after being outside for some timeso that odors can be detected more readily.
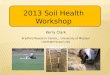
Having access to a valid and reliableinstrument that measures care quality inassisted living can be a huge help to facilitiesas they approach qualit>' improvement.Fresh perspectives and challenges to thequality improvement team are necessary tohelp them continuously identify issues toimprove and also have ways to measure theirimprovement. Displaying monthly resultsof the OIQ-AL using line graphs of results

Measuring Quality of Care in Assisted Living
100
20
•ProceM•SinjotureTotal (core
January May July Saptertibar
Figore 1. Display of monthly Observable Indicators of Quality-Assisted living Scores.
from prior months for each subscale canillustrate areas in need of attention as wellas improvements; graphs of the summativesubscales (process, structure) and the totalOIQ-AL score can illustrate overall progress.
REFERENCES
A sample of a graph illustrating the monthlysummative and overall scores for a facility ispresented in Figtire 1. We encourage assistedliving facilities to use the OIQ-AL and offeradvice to us and others about its usefulness.
1. National Center for Assisted Living. Pacts andTrends: The Assisted Living Sourcebook. Wasiiii^-lon, rH~: Naiiona! Center for Assisted Living; 2001.
2. Administration on Aging. A Profile of Older Amer-icans. 2002, Administration on Aging, US Depan-mcnt of Health and Human Scrvict^. Available at:www.aoa.gov/prof/Sutistics/proflle/l .asp. AccessedJuly 2006.
3. Rantz MJ, Hicks L, Grantio VT. et al. Nursing homequality, cost, staffing, and staff-mix. Gerontologist.2()O4;44(l):24-58.
4. Rantz M|, Zwygart-Stauffecher M. Popejoy L, t t al.Nursing home care quality: a multidimtrnsiimal theoretical model integrating the views of consumers andproviders.y Nurs Care Qual. l999;14(l):l6-.^7.
5. Rantz Ny, Mchr I>, Popejoy L, et al. Nursing homecare quality: a multidimensional thcorclical model.yNurs Care Qual. 1998;12(3):3O-46.
6. Rantz tA). Mehr DR, Conn V, et al. Assessing qualityof nursing home care: the foundation for improvingresident outcomes.^ Nurs Care Qual. 1996; 10(4): I -9.
7. Rantz f U, Mehr DR, Petroksi GF, et al. Initial field-testing of an mstrument to measure 'Ohser%^hle in-
dicators of ntirsing home care quaUty.'/ Nurs CareQua/. 2OOO;14{3):1-12.
8. Rantz MJ, Mehr DR. A quest to understand and mea-sure nursing home quality of care, long-term CareInterface. 2001;2C7):34-38.
9, Ranlz M. Jensdottir AB, Hjaltadonir I, ct ai. Interna-tional field tesr results of the observable indicatorsof nursing home care quality lastrument. Int NursRev. 2OO2;49(4):234-242.
10. Aud MA. Rantz MJ. Quality concerns in assisted livingfiadliUes.y A^wrs Care Quat. 2004; 19:8-9.
11. Aud MA. Rantz MJ, Zwygan-Stauffiichrr M, Man-ion P Developing a residential care facility versionof the observable indicators of nursing home carequality instrument./ Nurs Care Qual. 2004;19:48-57.
12. Rantz MJ. Zwygart-Staffadier M, Mehr D, Petroski G,Owen S, Madsen R. Field tetiEing, refinement and psy-chometric evaluation of a new measure of nursinghome care quality, y Nurs Meas, 2OO6;14<2):155-154.
13- Waltz CE Strickland OL. Lenz ER. Measurementin Nursing Research, 3rd ed, New Vorit: SpringerPublishing: 2004,