Embed Size (px)
Citation preview

OR I G I N A L A R T I C L E
Noninvasive follicular neoplasm with papillary like nuclearfeatures: A comprehensive analysis with a diagnostic algorithm
Chanchal Rana1 | Shreyamsa Manjunath2 | Pooja Ramakant2 |
Kulranjan Singh2 | Suresh Babu1 | Anand Mishra2
1Department of Pathology, King George's
Medical University, Lucknow, India
2Department of Endocrine surgery, King
George's Medical University, Lucknow, India
Correspondence
Dr Chanchal Rana, Associate Professor,
Department of Pathology, King George's
Medical University, Lucknow.
Email: [email protected]
Abstract
Background: Noninvasive follicular thyroid neoplasm with papillary-like nuclear features
(NIFTP) lacks the carcinoma label, avoiding aggressive therapy, physiological, social and
financial impact of cancer diagnosis. Unfortunately, the preoperative diagnosis is still a
challenge. Varied incidence of NIFTP has been document with limited data on preopera-
tive cytological, radiological characteristics and the impact on risk of malignancy in each
category of the Bethesda system of reporting thyroid cytopathology.
Method: Retrospective analysis of 20 NIFTPs with an attempt to provide a preopera-
tive diagnostic algorithm based on the cytological and ultrasound features along with
incidence and implication on risk of malignancy in various Bethesda categories with
its impact on patient management.
Result: Incidence of NIFTP in our study was higher in comparison to that docu-
mented from other Asian countries. TIRADS 3 was the most common sonographic
diagnosis. NIFTP was commonly preceded by indeterminate or benign Bethesda cat-
egory. Major impact of excluding NIFTP form malignant category was seen on
Bethesda categories II and IV with 20% and 27% reduction in risk of malignancy,
respectively.
Conclusion: Retrospective analysis should not be confined only to follicular variant of
papillary thyroid carcinoma but cases of follicular adenoma and adenomatous colloid
nodule should always be included in review to ascertain the true incidence of NIFTP.
NIFTPs are less likely to have malignant preoperative cytology. NIFTP shares major
cytological and ultrasound features with follicular adenoma, adenomatous colloid
nodule and minimally invasive follicular papillary carcinoma. When analyzed together,
taking minor findings in consideration, can favor a diagnosis.
K E YWORD S
cytology, NIFTP, risk of malignancy, thyroid, ultrasound
1 | INTRODUCTION
The crisis in the over diagnosis and treatment of the encapsulated
papillary thyroid carcinoma, follicular variant (EFV-PTC), brought a
working group of the Endocrine Pathology Society to critically re-
examine this entity in 2016.1 As a result of this endeavor, Nikiforov
et al advocated a revision of diagnostic terminology with the funda-
mental aim of avoiding the term carcinoma, and the consequent risk
of overtreatment for noninvasive tumors that are essentially clinically
benign, with a recurrence rate < 1%.2 Hence, noninvasive follicular
thyroid neoplasm with papillary-like nuclear features (NIFTP) termi-
nology was recently introduced and incorporated in the 4th edition of
Received: 11 September 2019 Revised: 10 December 2019 Accepted: 10 December 2019
DOI: 10.1002/dc.24375
330 © 2019 Wiley Periodicals, Inc. Diagnostic Cytopathology. 2020;48:330–341.wileyonlinelibrary.com/journal/dc

the World Health Organization (WHO) Classification of Tumors of
Endocrine Organs, published in 2017, in a new chapter on borderline
tumors of follicular cell origin.3
Almost 3 years have passed since the introduction of this new
entity and experiences from different countries and institutions have
been published in an attempt to evaluate whether certain degree of
disagreement still persists or whether the new diagnostic criteria are
in complete harmony with the diagnosis and management. In spite of
Asian continent being a major contributor to worldwide prevalence of
thyroid cancer (according to GLOBOCON database; estimated 48%
new cases in 2012), the prevalence of NIFTP in Asians has not been
reported extensively as compared with the western world.4,5 There
are limited studies from Asia and even fewer form India5-10 and those
present have reported a significantly lower prevalence (0%-5%) as
compared to western data (15%-25%).2,11-14
Preoperative cytological assessment along with ultra-sonographic
evaluation of the thyroid nodule forms the basis of patient management
with thyroid nodule, hence, it becomes imperative to identify NIFTP entity
at postoperatively to prevent overtreatment and decrease morbidity in
these patients. Unfortunately, diagnostic criteria of NIFTP are primarily
based on histology and feasibility of an accurate diagnosis of NIFTP on
fine needle aspiration cytology (FNAC) and ultrasonography still remains a
controversial matter.2
Relatively questionable prognosis and nature of NIFTP has signifi-
cantly influenced The Bethesda system of reporting thyroid cytopa-
thology (TBSRTC) such that in updated 2017 guidelines, risk of
malignancy (ROM) has been calculated in two ways: when NIFTP is
not considered a malignancy, and when NIFTP is still included among
the “carcinomas.”15 The ROM decreased significantly in indeterminate
categories after removing NIFTP from tally of malignancy as early data
suggests that NIFTP constitutes a substantial proportion of the
“malignancies” hidden in these categories.16,17
Hence, this study is an attempt to comprehensively analyze
noninvasive follicular NIFPT by focusing on its prevalence in our
population, ultrasonography findings, preoperative cytological
assessment, histopathological evaluation, mutational analysis for
BRAFV600E and implication of NIFTP diagnosis on risk of malig-
nancy in various Bethesda categories along with impact on patient
management.
We also intend to propose a preoperative diagnostic algorithm
based on cytological and ultra-sonographic features for NIFTP.
2 | MATERIALS AND METHODS
2.1 | Study design and sample population
This is a retrospective cohort study, which included all the patients
with thyroid swelling visiting the department of endocrine surgery,
who underwent fine-needle aspiration and/or histopathological evalu-
ation in our unit of department of pathology, between 2016 and
2018. For each patient, demographic and clinical information were
collected from hospital database.
2.2 | Cytopathological evaluation
FNAC was performed using a 23 or 24-gauge needle attached to a
10 mL syringe. Air-dried and alcohol-fixed smears were prepared and
stained with May-Grunewald-Giemsa (MGG) and hematoxylin and
eosin (HE) stain, respectively. Final cytological diagnoses were based
on the six tier diagnostic category of TBSRTC.18 These categories
include: non-diagnostic (ND), Benign, atypia of undetermined signifi-
cance/follicular neoplasm of undetermined significance (AUS/FLUS),
follicular neoplasm/suspicious of follicular neoplasm (FN/SFN), suspi-
cious for malignancy (SM) and malignant category.
2.3 | Histopathological follow-up
Histological specimens in the form of hemi-thyroidectomy (HT)/total
thyroidectomy (TT) and/or core needle biopsies (CNB) were also
included wherever present. Histological diagnoses were classified
according to the third edition of the WHO pathology and genetics of
tumors of endocrine organs as well as being staged according to the
seventh edition of the AJCC Cancer Staging Manual. CNB for histo-
pathological follow-up has been used only in cases of anaplastic thy-
roid carcinoma (ATC) they are stage IV malignancy in which
resection is not usually advised.
2.4 | Review of potential cases of NIFTP
Considering the primary requisite of NIFTP as a well-demarcated or
encapsulated nodule, all the cases previously diagnosed as EFV-PTC,
adenomatous colloid nodule or follicular adenoma (FA) were reviewed
again for the possibility of NIFTP. All the cases of PTC without any
lymph nodes metastasis were also reviewed to rule out any possibility
of missing EFV-PTC at initial diagnosis. A consensus diagnostic crite-
rion by working group of noninvasive follicular thyroid neoplasms
with NIFTP was applied for each case and diagnosis was made accord-
ingly. The diagnostic criteria include:
1. Encapsulated or clear demarcation
2. Follicular growth pattern with
a. No papillae
b. No psammoma bodies
c. <30% solid/trabecular/insular growth pattern
3. Nuclear scores 2 to 3
4. No capsular and no vascular invasion
5. No tumor necrosis
6. No high mitosis (<3 per 10 high-power fields)
Two independent pathologists evaluated these cases as well as
their corresponding FNA smears in a blinded manner. The FNA smears
were evaluated for cellularity, architecture, presence or absence of
nuclear features of PTC for which three parameters were assessed:
Nuclear size and shape (ie, enlargement, elongation and crowding/
RANA ET AL. 331

overlapping); membrane irregularity (grooves, pseudo inclusions) and
chromatin. In cases of discrepancy, a joint decision was made.
2.5 | Radiological details
The thyroid ultrasounds were reported as per The American College of
Radiology —TIRADS reporting system and scoring performed accord-
ingly. Details were gathered retrospectively and following parameters
were assessed: size, shape (oval or round), echogenicity (hypo echoic,
hyper echoic, isoechoeic, etc.), composition (solid, predominantly solid,
mixed solid-cystic), vascularity (increased or no increase), margins
(smooth, ill-defined, irregular/lobulated, extrathyroidal extension) and
calcification (present or absent).
2.6 | Malignancy follow-up rates
The results of final histopathology diagnoses were compared to FNAC
diagnoses to find out malignancy rate of each categories of TBSRTC. In
calculating the malignancy follow-up rate for the benign category, the
total number of original FNA diagnoses was used as the denominator.
For all other diagnostic categories, malignancy follow-up rates were cal-
culated by using the number of cases with follow-up histology results.
If a patient had multiple FNA samples in the same procedure yield-
ing two different diagnoses, only the diagnosis with higher malignant
potential was used for calculating malignancy follow-up rates. Papillary
microcarcinoma (<1 cm) on resection were not considered malignant
except when the prior cytological interpretation was SM or malignant,
because the subcentimeter foci may not be targeted by the needle.
The ROM was calculated in two ways, similar to 2017 BSRTC,
one by considering NIFPT as benign neoplastic lesion and secondly
including NIFTP in tally of malignancies. The difference between both
results constituted a decrease in ROM (DROM).
2.7 | Immunohistochemistry for BRAF V600Eanalysis
Immunohistochemistry (IHC) staining was performed using a commer-
cially available BRAFV600E mutation-specific antibody. In brief, after
de-paraffinization and rehydration, paraffin-embedded tissue sections
(3 μm thick) were blocked with 3% hydrogen peroxide for 4 minutes
at room temperature. Microwave-assisted heat-induced antigen
retrieval was performed using the optimized antigen retrial condition
followed by incubation with BRAF V600E-specific monoclonal mouse
antibody (clone VE1; Abcam ab228461; dilution1: 100). A case papil-
lary thyroid carcinoma with BRAFV600E mutation, proved by molecu-
lar technique, was used as a positive control.
BRAF V600E expression within the cytoplasm was subjectively
graded as: 0, no cytoplasmic staining visualized at any magnification; 1
+, weak, requiring a ×10 or greater objective to recognize flavescent
staining on the section; 2+, moderate, easy to recognize yellow
staining with a ×10 objective; and 3+, strong brown staining with a 4×
microscopic objective.
3 | RESULTS
This study-included total of 617 FNA cases reported, according to
updated TBSRTC 2017, between 2016 and 2018. The age ranged from
2 to 85 years with mean age 39.9 years and median as 40 years. There
was a female predominance with a male: female of 1:4. During the
same period, 329 histology specimens (Hemi-, total thyroidectomy and
core needle biopsies) were received and reported. However of these
617 cytology cases, histology follow-up was available in 292 patients.
Table 1 shows the distribution of various diagnostic entities
reported in different Bethesda categories. There were 28 (4.5%) non-
diagnostic smears such that the adequacy rate was 95.5%. Majority of
TABLE 1 Distribution of various diagnostic entities and Bethesdacategories in FNA samples (n = 617)
Diagnostic categoryNo ofcases (n = 617)
%Cases
Non diagnostic 28 4.5
Benign 417 67.6
Colloid nodule 306 49.6
Goiter 80 12.9
Lymphocytic thyroiditis 25 04.1
Abscess 3 0.48
Granulomatous thyroiditis 2 0.30
Subacute thyroiditis 1 0.15
AUS/FLUS 22 3.6
FN/SFN 62 10.0
Follicular neoplasm 51 08.2
Hurthle cell neoplasm 11 01.8
SM 16 2.6
Malignant
Papillary carcinoma thyroid 72 11.7
Anaplastic carcinoma thyroid 29 04.7
Metastasis 23 03.7
Medullary carcinoma thyroid 04 0.60
Non-Hodgkin's lymphoma 05 0.80
Poorly differentiated carcinoma 04 0.60
Hurthle cell carcinoma with lymph
node
02 0.30
Metastasis
Extra medullary plasmacytoma 01 0.15
Primary undifferentiated sarcoma 01 0.15
Primary squamous cell carcinoma 01 0.15
Abbreviations: AUS, atypia of undetermined significance; FLUS, follicular
neoplasm of undetermined significance; FN, follicular neoplasm; SFN,
suspicious of follicular neoplasm; SM, suspicious for malignancy.
332 RANA ET AL.

the lesions were benign (67.6) and there were only 3.6% cases
(22 cases) of AUS. There were 72 cases of FN/SFN and among these
cases and there were four cases where the possibility of FV-PTC or
NIFTP was given. All these four cases were reported between
November 2017 and December 2018 and fortunately histology follow
up was available in all four of these cases.
3.1 | Overview of NIFT cases
On the basis of the criteria used for review (as mentioned in materials
and methods), there were 54 potential cases of NIFTP among which
15 fulfilled the diagnostic criteria and hence were labeled as NIFTP.
Apart from these 15 cases, there were five more cases with primary
diagnosis of NIFTP diagnosed during November 2017 to December
2018. Therefore, a total of 20 cases of NIFTP are included in this
study. These retrospectively diagnosed 15 cases of NIFTP were ini-
tially diagnosed as adenomatous colloid nodule (two cases), follicular
adenomas (five cases) and Follicular variant-Papillary thyroid carci-
noma (eight cases).
3.1.1 | Incidence of NIFTP
We calculated the incidence of NIFTP in three ways: incidence of
NIFTP is 5.1% when all the thyroid histopathological samples were con-
sidered, 16.2% among all neoplastic lesions (benign and malignant) and
29.6% when only PTC cases were included. Majority of these patients
were female (80%) and were ≤ 35 years (75%) of age (age range
18–70 years). All these patients were biochemically normal with the
duration of nodule being 3 months to 7 years. There was no associated
lymphadenopathy, history of rapid increase or compressive symptoms.
3.1.2 | Ultrasonography details
Ultrasonography details were available in all the cases. TIRADS score
corresponded to mildly suspicious category (score 3) in 95% cases. On
gray scale, all these nodules were well circumscribed with smooth
margins and were wider than taller. They were mostly solid/predomi-
nantly solid (95%) and hyper-echoic/predominantly hyper-echoic
(85%) Comet tail sign, calcification, lobulated margin were characteris-
tically absent. Color Doppler ultrasound demonstrated an increase in
vascularity in 60% of cases, which was more common peripherally.
However, hypoechoic halo was identified in 12 cases and nodular
background was present in 16 patients. Table 2 shows ultrasonogra-
phy details of all the cases of NIFTP.
3.1.3 | Review of preoperative cytology smears
Preoperative cytology smears were available in all the cases, among
which two had nondiagnostic cytology. A majority (55.6%; 10 cases)
of the NIFTP cases had indeterminate cytology of FN/SFN. There
were seven cases (35.3%) in benign category and only one in malig-
nant. Smears in most of these cases were moderately cellular. The
most common cytological abnormality seen was significant micro fol-
licular pattern, presence of nuclear enlargement and prominent
nuclear overlapping. Nuclear grooving was also commonly seen. Fre-
quent intra-nuclear pseudo-inclusions (>3) were not identified but
occasional pseudo inclusion1,2 could be identified in two cases only.
Psammoma bodies and papillae were typically absent and there was
either no colloid or if present were in the form of thick blotches.
3.1.4 | Histopathology of NIFTP cases
On histological evaluation, 12 cases were completed encapsulated
with a thin or thick capsule and remaining cases were well demarcated
with no or partial encapsulation. There was a background of nodular
TABLE 2 Ultrasonography details of NIFTP cases (n = 20)
Type of ultrasound Features
No of cases
(%age)
Gray scale ultrasound
Circumscription Well circumscribed 20 (100%)
Invasive 00
Shape Oval 20 (100%)
Round 00
Composition Solid 10 (50%)
Predominantly solid 09 (45%)
Mixed solid cystic 01 (05%)
Cystic 00
Echogenicity Hyper echoic or
predominantly hyper
echoic
17 (85%)
Hypo echoic 03 (15%)
Isochoric 00
Calcification Present 00
Absent 20 (100%)
Other features
Comet tail sign Present 0 (0%)
Absent 20 (100%)
Hypo echogenic
halo
Present 12(60%)
Absent 08(40%)
ACR-TIRAD SCORE 2 (Not suspicious) 1 (5%)
3 (Mildly suspicious) 19 (95%)
Color Doppler ultrasound
Vascularity Increased 12 (60%)
Not increased 08 (40%)
Pattern of increased
vascularity
Central 04 (20%)
Peripheral 08 (40%)
RANA ET AL. 333

goiter in 16 cases characterized by presence of vague nodules com-
posed of variable sized colloid filled follicles.
The nuclear score was mostly 2 (80%), with common abnormali-
ties seen in nuclear shape/size (enlarged overlapping nuclei) and chro-
matin characteristics (chromatin margination or glassy nuclei). Nuclear
membrane irregularity could also be easily appreciated in many cases
however significant nuclear grooving was not as common. These
nuclear findings were mostly patchy and not uniformly present in the
entire lesion. In the remaining four cases (20%), the nuclear score was
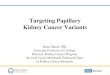
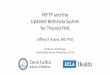
3. Figures 1 and 2 show cytological and corresponding histological
features of NIFTP observed in some of our cases with variable nuclear
score.
3.1.5 | Risk of malignancy and impact on NIFTP onpatient management
The risk of malignancy was calculated in two ways by including as well
as excluding NIFTP from the malignancy tally. There was one core
needle biopsy specimen, which was reported as inadequate and there-
fore excluded. Hence, there were a total of 289 cases where cytology
and histology could be correlated. Table 3 shows the details of ROM
along with the percentage DROM.
The major impact of including NIFTP in malignant category was
seen in Bethesda category I (nondiagnostic) and IV (FN/SFN) where
the malignancy risk decreased from 60% to 40% and 48.6% to 21.6%,
respectively. There was also a minor decrease in risk in benign cate-
gory, however, there was no difference in suspicious and malignant
categories.
3.1.6 | BRAF V600E mutation analysis by IHC
None of these 20 cases showed any cytoplasmic positivity and hence
were reported as negative for this mutation on IHC.
3.1.7 | Surgical management
The types of initial surgeries performed included 15 hemi-
thyroidectomies and five total thyroidectomies. Fortunately, major-
ity (75%) of the patients invariably underwent a proper treatment.
However, in 25% of the cases overtreatment in the form of total
thyroidectomy could have been avoided. Among these five cases,
four were reported as FV-PTC on cytology and one was
inadequate.
F IGURE 1 Case 1 (cytology andcorresponding histology) with nuclearscore of 2. A, Cytological smeardisplaying clusters of atypical cellswith overlapping round to oval nuclei(H&E, ×400). B, Correspondinghistology with enlarged roundoverlapping nuclei with chromatinclearing and margination (H&E, ×400)[Color figure can be viewed atwileyonlinelibrary.com]
F IGURE 2 Case 2 (Cytology andcorresponding histology) with nuclearscore of 3. A, Cytological smeardisplaying clusters of atypical cellswith overlapping predominantly ovalnuclei with grooving and occasionalintranuclear inclusion (H&E, ×400). B,Corresponding histology withenlarged round to oval overlappingnuclei with chromatin clearing andmargination and irregular nuclearmembrane with prominent grooving(H&E,×400) [Color figure can beviewed at wileyonlinelibrary.com]
334 RANA ET AL.

4 | DISCUSSION
NIFTP represents a group of neoplasm, which are well demarcated,
noninvasive with follicular architecture, nuclear features similar to
papillary carcinoma thyroid and negligible risk of recurrence or metas-
tasis. At molecular level, these tumors are known to show similarity to
follicular neoplasm, demonstrating high percentage of RAS and PAX8/
PPARG rearrangement, which more commonly occur in classical PTC
and invasive follicular variant of PTC. BRAFV600E mutation has not
been documented in NIFTP, but they might have BRAF-K601E muta-
tions.19-21 Presently, after ~3 years of adopting a new terminology,
NIFTP remains the topic of interest which has significantly influenced
the practice of endocrine pathology compelling the health profes-
sionals in this field to adjust current approaches and guidelines to this
new entity.
The NIFTP working group has proposed following modification in
the diagnostic criteria documented in the original publication by
Nikiforov et al22:
1. “True papillae <1%” to be replaced by “no true papillae.”
2. Examination of entire tumor, and not just capsule, with optional,
but recommended BRAF V600E analysis using immunohistochem-
istry or molecular techniques, in cases with florid nuclear features
of PTC (nuclear score 3).
During the review process in our study, we also encountered a
case with few true papillae (<1%) present at the periphery. This case
was excluded in view of modified criteria for NIFTP. However, this
patient had been in follow up for last 3 years and has not shown any
sign of malignancy till now.
The extent of all the changes related to the NIFTP reclassification
apparently depends on the incidence of NIFTP in a certain population.
Approximately, 30 studies have been conducted in America, Europe
and Asia reporting variable incidence.2,4,5,7,9,11,16,17,23-30 Bychkov
et al, in a meta-analysis, documented an average worldwide preva-
lence rate of 9.1%, with a lower rate in Asian studies (1.6%) as com-
pared with non-Asian countries (13.3%).4 This difference could be
attributed to various perceptions of histological diagnostic thresholds,
different nature of papillary thyroid carcinoma, and different
approaches in the management of thyroid nodules. However, these
rates are based on NIFTP documented among PTC cases only. In none
of these studies, cases of adenomatous colloid nodule or follicular
adenomas were reviewed. Well demarcated/-encapsulated lesions
being the first diagnostic criterion make it important to consider these
cases as well. We had two cases of adenomatous colloid and five
cases of follicular adenomas, which were reclassified as NIFTP. In our
study, we have documented the incidence in a very elaborative way,
such that the incidence was 5.1% among all thyroid lesions while it
was 16.2% among neoplastic cases and 29.6% when only PTCs were
considered. Incidence in our setting is significantly higher as compared
to those documented in studies form Asia as well as other countries
(Table 4). All these studies so far may not truly reflect the incidence
and prevalence of this entity due to wide variation in their designs,TABLE3
Summaryofmaligna
ncyrate
aswellasFNACan
dhistologicalcorrelationin
various
Bethe
sdacatego
ries
(N=230)
FNAC
Histopa
thology
diag
nosis
Riskofmalignan
cy
Diagn
ostic
catego
ry
Ben
ignne
oplastic
NIFTP
Maligna
ntROM
with
NIFTP)
ROM
(without
NIFTP)
%Dec
rease
inROM
No.o
fcases
Ben
ign
Follicu
lar
aden
oma
Hurthle
cell
aden
oma
Nond
iagn
ostic
10
31
02
4(3
anap
lasticca
and1Follicu
larcarcinoma)
60.0
40.0
20.0
Ben
ign
186
167
50
6
8(1
each
ofan
aplasticca
andno
nho
dgkin
lymph
oma(N
HL);2
offollicu
larca
and4PTC)
2.3
1.3
1.0
AUS/FLU
S09
52
00
2(2
PTC)
22.2
22.2
0.0
FN/SFN
37
96
410
8(6
Follicu
larca,1
med
ullary
thyroid
carcinoma
(MTC)a
nd1Hurtlecellcarcinoma)
48.6
21.6
27.0
SM08
10
00
7(3
Ana
plasticcarcinoma,2PTCan
d2NHL)
87.5
87.5
0.0
Maligna
nt39
00
00
39(12an
aplasticca,1
7PTC,2
Metastaticca,
3NHL,2po
orlydifferen
tiated
and1ea
chof
MTC,u
ndifferentiatedSa
rcomaan
dPrimary
squa
mous
cellcarcinoma(SCC))
100
100
0.0
Abb
reviations:A
US,
atyp
iaofun
determ
ined
sign
ifican
ce;F
LUS,
follicu
larne
oplasm
ofun
determ
ined
sign
ifican
ce;F
N,follicu
larne
oplasm;N
IFTP,n
oninvasive
follicu
larthyroid
neo
plasm
withpap
illary-like
nuclea
rfeatures;P
TC,p
apillarythyroid
carcinoma;
ROM,riskofmaligna
ncySF
N,suspicious
offollicu
larne
oplasm;S
M,suspicious
formaligna
ncy.
RANA ET AL. 335

TABLE4
Compa
rative
analysisofincide
ncea
anddistribu
tionofNIFTPin
various
Bethe
sdacatego
ries
Stud
y(yea
r)(Referen
ce)
Place
andye
arofstud
yNo.o
fNIFTPcases
Incide
nceNIFTP(%
)
DistributionofNIFTPin
various
Bethe
sdadiagn
ostic
catego
ries
BCI(Nondiag
nostic)
BCII(Ben
ign)
III(AUS/FLU
S)IV (FN/SFN)
V(SFM)
VI
(Malignan
t)
Strickland
17
USA
2015
85
28.0
1(1.2%)
13(15.3%)
17(20.0%)
7(8.2%)
39(45.9%)
8(9.4%)
Howittet
al31
German
y2015
72
—3(4.2%)
9(12.5%)
13(18%)
7(9.7%)
35(48.6%)
5(6.9%)
Fan
quin
etal16
USA
-Switzerlan
d2016
173
22.9
1(0.6%)
15(8.7%)
54(31.2%)
46(26.5)
42(24.3%)
15(8.7%)
Rosarioet
al12
Brazil2
016
126
15.0
1(0.8%)
10(8.0%)
25(20%)
53(42%)
32(25.4%)
5(4.0%)
Can
berk
etal5
Turke
y2016
94
27.6
13(13.8%)
15(15.9%)
14(14.9%)
23(24.5%)
17(18.1%)
12(12.8%)
Sing
het
al26
USA
2017
21
12.1%
—1(5%)
4(19%)
10(48%)
3(14%)
3(14%)
Hirokawaet
al7
Japa
n2017
42
—2(4.9%)
2(4.9%)
5(12.2)
1(2.4%)
4(9.8%)
27(65.9%)
Bycho
vet
al45
India
15
10.2%
00
6(40%)
9(60%)
00
Japa
n09
4.0%
2(22.2%)
1(11.1%)
04(44.4%)
111.1%)
1(11.1%)
Korea
06
3.4%
01(16.6%)
3(50%)
02(33.3%)
0
Korea
06
2.4%
00
1(16.6%)
1(16.6%)
2(33.3%)
2(33.3%)
Taiwan
11
6.1%
1(9.1%)
3(27.3%)
3(27.3%)
3(27.3%)
1(9.1%)
0
Tha
iland
2018
12
8.9%
3(25%)
6(50%)
02(16.6%)
1(8.3%)
1(8.3%)
Current
stud
yIndia
20
29.6%
2(10%)
7(35%)
010(50%)
01(5%)
Abb
reviations:A
US,
atyp
iaofun
determ
ined
sign
ifican
ce;F
LUS,
follicu
larne
oplasm
ofun
determ
ined
sign
ifican
ce;F
N,follicu
larne
oplasm;N
IFTP,n
oninvasive
follicu
larthyroid
neo
plasm
withpap
illary-like
nuclea
rfeatures;S
FN,suspicious
offollicu
larne
oplasm.
aRefersto
incide
nceofNIFTPin
patien
tsofPap
illarythyroid
carcinoma.
336 RANA ET AL.

retrospective nature and estimation of rates based on primary search
via FNA database, which implies that the accurate rate of NIFTP
worldwide still needs to be established.
Since NIFTPs or their former equivalent (EFVPTCs) typically do
not show the full range of nuclear features seen in classic type PTCs,
particularly when the atypia is subtle or focal, they are frequently
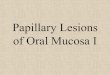
F IGURE 3 Diagnostic algorithm based on major and minor ultrasonography and cytological features
RANA ET AL. 337

assigned an indeterminate cytological diagnosis within the TBSRTC
classification system.16,21,31-33 Contrary to these findings authors like
Hirokava et al, Stickerland et al and Howitt et al have documented
>50% NIFTP cases placed in higher Bethesda categories (SFM and
malignant).7,17,31 The reason for this discrepancy is unclear but may
be due to institutional differences in the threshold of cytological inter-
pretations. Our study also placed NIFTP in SFN/FN (52.6%) followed
by benign (31.6%) and there was only one case with malignant preop-
erative cytology. These findings again signify the fact, that a substan-
tial number of cases of NIFTPs could have been diagnosed as
adenomatous nodule/goiter; therefore for true incidence of NIFTP it
is important to review these cases as well. Prospective studies in near
future may answer these debatable territories.
The current paradigm in the treatment of patients with NIFTP is
limited surgery such as lobectomy rather than subtotal/complete thy-
roidectomy or postoperative radioiodine treatment. Therefore, com-
prehensive evaluation for the diagnosis of preoperative NIFTP is
important for clinicians to achieve better decision to manage the
patients. Preoperative diagnosis is still a challenge as ultrasonography
and FNA are two main modalities for preoperative analysis in thyroid
nodule, but unfortunately there are no diagnostic criteria for NIFTP
based on them. Chandler et al reported NIFTP cases to be more likely
to have predominant micro-follicular pattern, absent intra-nuclear
inclusions (INI) and less obvious nuclear elongation and grooves than
FVPTCs.32 Some authors have, even recommended quantification of
cytological features, example a cut-off of ≥3 being considered for
pseudo-inclusions.23,32,34 However, Ng et al found as many as 22% of
their NIFTP cases to show ≥3 INI, thus, raising doubts over reliability
of this measure.35,36
There is limited literature on ultrasonography features of NIFTP,
which could help in making a definitive diagnosis.14,37,38 NIFTP, follic-
ular adenoma, adenomatous colloid nodule and minimally invasive FV
PTC share common cytomorphological (micro-follicular pattern) and
radiologically (wider than taller circumscribed lesions) features. Minor
ultrasound findings such as comet sign (common in colloid nodule),
complete hypo genic halo (common in follicular adenoma), nodular
background (not seen in follicular adenoma), lobulated margins (FV-
PTC), etc. can be very helpful in such situation. Table 6 shows a com-
parative analysis of cytology and ultrasound features in these entities.
This is the only study from India so far which has documented the
sonography characteristic in detail. Our data suggest that NIFTP nod-
ules corresponds to TIRAD score 3 and are characterized as well cir-
cumscribed, wider than taller, mostly solid and hyper echoic lesion
with smooth outlines and peripheral increase in vascularity. Figure 3
describes a diagnostic algorithm based on major and minor ultraso-
nography and cytological features to differentiate between these enti-
ties and direct the management of these patients.
Introduction of NIFTP has also created some challenges for thy-
roid FNAC: among them, its impact on the ROM in the diagnostic cat-
egories of TBSRTC and the resulting need for modification of clinical
management guidelines may be critical.39 Clinicians should always be
aware of the malignancy rate in various Bethesda categories in their
respective hospitals to improve their management decisions. FewTABLE5
Compa
risonofim
pact
ofNIFTPonrisk
ofmaligna
ncyin
various
stud
ieswithan
dwitho
utco
nsideringNIFTPas
maligna
ncy
Stud
ies
Strick
land
etal17
Faqu
inet
al16
Laye
fieldet
al42
Can
berk
etal5
Updated
TBSR
TC15
Presentstudy
Bethe
sda
catego
ries
ROM
aROM
bDROM
ROM
aROM
bDROM
ROM
aROM
bDROM
ROM
aROM
bDROM
ROM
aROM
bDROM
ROM
aROM
bDROM
Nondiagno
stic
18.9
17.0
1.9
25.3
23.9
1.4
9.5
9.5
013
6.5
6.5
5–1
05–1
00
60.0
40.0
20
Ben
ign
13.2
5.4
7.8
9.3
5.8
3.5
10.7
7.1
3.6
7.0
6.0
1.0
0–3
0–3
02.3
1.3
1.0
AUS/FLU
S39.2
21.6
17.6
31.2
17.6
13.2
17.4
15.1
2.3
45
30
15
~10-30
6-18
4–1
222.2
22.2
0
FN/SFN
45.5
37.5
8.0
33.2
18.0
15.2
22.2
19.7
2.5
30
10
20
25-40
10-40
15
48.6
21.6
27
Suspicious
of
maligna
ncy
87.2
45.7
41.5
82.6
59.2
23.4
82.8
65.8
17.0
72
48
24
50-75
45-60
15
87.5
87.5
0
Maligna
nt98.7
93.6
5.1
99.1
95.7
3.4
100
87.2
12.8
98
87
11
97-99
94-96
3100
100
0
Abb
reviations:A
US,
atyp
iaofun
determ
ined
sign
ifican
ce;D
ROM,d
ifferenc
ein
risk
ofmaligna
ncyF
LUS,
follicu
larne
oplasm
ofun
determ
ined
sign
ifican
ce;F
N,follicu
larneo
plasm
;NIFTP,n
oninvasive
follicu
lar
thyroid
neoplasm
withpa
pillary-likenu
clea
rfeatures;R
OM,riskofmaligna
ncySF
N,suspicious
offollicu
larne
oplasm.
aRiskofmaligna
ncyby
consideringNIFTPas
maligna
ncy.
bRiskofmaligna
ncyby
notco
nsideringNIFTPas
maligna
ncy.
338 RANA ET AL.

TABLE6
Compa
rative
analysisofultrasoun
dan
dcytology
find
ings
ofNIFTPwithother
differen
tialdiagno
sis3
7,38,42
Ultraso
undfind
ings
Ade
nomatous
collo
idno
dule
NIFTP
Follicu
larad
enoma
Inva
sive
FV-PTC
Compo
sition
Mixed
(solid
andcystic)
Predo
minan
tlysolid
Predo
minan
tlycysticormixed
cystican
d
solid
lesions
Predominan
tlysolid
Ech
oge
necity
Isoecho
genicto
slightlyhy
perech
oge
nic
Predo
minan
tlyhy
perech
oge
nic
Isoecho
icorpred
ominan
tlyan
echoic
Usuallyhyp
oechoge
nic
Orien
tation
Wider
than
taller
Wider
than
taller
Wider
than
taller
Tallerthan
wider
Margin
Smooth
Smooth
Smooth
Spiculated/lobulatedmargin
Calcification
Absen
tormacro
calcification
Usually
absent
ifpresen
tthan
macro
calcification
Absen
tormacro-calcification
Micro
calcifications
Halo
Absen
tMay
bein
encapsulated
one
sCompletethin
toun
even
Inco
mplete
Comet
tailartifact
Present
Absen
tAbsen
tAbsent
Vascu
larity
Predo
minan
tlype
riph
eralflow
Predo
minan
tlype
riph
eralflow
Absen
ceofinternalflow
orpred
ominan
tly
periph
eralflow
4
Marke
dintran
odular
Nodu
larity
in
remaining
thyroid
Usuallypresen
tUsually
presen
tAbsen
tUsuallypresent
Cytology
find
ings
Architecturalfeatures
•Microfollicu
larpa
ttern
•Largeno
nbran
chingcellu
larmono
laye
red
shee
tswithco
lloid
inba
ckgroun
d
•Microfollicu
larpa
ttern
•Microfollicu
larpa
ttern
•Three
dimen
siona
lmultilaye
redshee
ts
withan
dwithtrab
ecular
pattern
•Microfollicu
larpattern
•Monolaye
rbranch
ingshee
t
Nuc
lear
enlargem
ent
Absen
tPresent
Present
Present
Nuc
lear
shap
eRoun
dun
iform
Roun
dto
ovale
nlarge
dEnlarge
droun
dto
mild
anisonu
cleo
sis
Ovaltoelongateden
larged
with
moderatean
isonucleo
sis
Nuc
lear
ove
rlap
ping
Minim
alPresent
freq
uently
Minim
alPresentSign
ifican
tly
Nuc
lear
grooving
Minim
alPresent
freq
uently
Minim
alPresentSign
ifican
tly
Intranu
clea
rpseu
do
inclusion
Usuallyab
sent
Occasiona
l1,2
Usually
absent
Frequen
t(>3)
Chromatin
Den
seGroun
dglassto
vesicu
lar
Granu
lar
Groundglassto
vesicu
lar
TruePap
illae
Absen
tAbsen
tAbsen
tMay
bepresent
Psammomabo
dies
Absen
tAbsen
tAbsen
tMay
bepresent
RANA ET AL. 339

studies have shown that NIFTP has affected malignancy risk in each
category with the greatest impact being on FN/SFN and non-
diagnostic categories.40 A recent meta-analysis by Layfield et al has
shown that NIFTP remarkably affect risk of malignancy in indetermi-
nate Bethesda categories.41 In our study, similar to those by Faquin
et al16 and Canberk et al,5 the highest reduction in risk of malignancy
was in FN/SFN Bethesda category (27%) followed by non-diagnostic
category (20%). Although lesser impact is known in benign category
but special attention should be given to this subset, which may
require closer monitoring compared to non-neoplastic benign nodules.
This notion can be backed up by the fact that NIFTP is known to be a
precursor lesion and have a propensity to progress to invasive follicu-
lar variant of PTC. The international working group for NIFTP also
postulates it as an oncogene driven clonal tumor and a precursor
tumor to invasive EFVPTC. The WHO editorial committee thus
decided to incorporate a new chapter, 2-2A: other encapsulated follic-
ular patterned thyroid tumors, in which there were two sub-chapters,
UMP and NIFTP, in the fourth edition WHO classification of tumors
of endocrine organs. They were given a behavior code of 1 (borderline
or uncertain behavior) by the WHO committee.3 NIFTP is still a newly
diagnosed enitity and long term follow up will shed more light on bio-
logical behavior in coming future. There was no impact on cases with
AUS, SFM and malignant cytology. Contrary to these findings Kim
et al documented no significant decrease in risk of malignancy after
excluding NIFT from malignant lesions.39 Comparison of our findings
with some previous studies is shown in Table 5. Our study had its
shares of limitation: firstly retrospective study with lesser number of
cases in AUS/FLUS and SFM Bethesda categories; and secondly lack
any comparison with two edges like FA in benign, and IFV-PTC in
malignant edge to proof the usefulness of the algorithm.
To conclude, ultrasonography and cytology findings when put
together can be efficiently used to suggest preoperative diagnosis of
NIFTP. NIFTPs are less likely to have malignant preoperative cytology
but can be commonly preceded by benign Bethesda category. Hence,
inclusion of cases of follicular adenoma and adenomatous colloid nod-
ule is important to determine the true incidence. Countries with
higher incidence of thyroid cancers can further work up to establish
their own malignancy risk range and parameters. Future prospective
studies are required is required to validate the proposed diagnostic
algorithm.
ACKNOWLEDGEMENT
Authors acknowledge King George's Medical University Medical
Research Unit, Department of Health Research.
CONFLICT OF INTEREST
AUTHOR CONTRIBUTION
Chanchal Rana contributed to conception and design, provision of
study materials or patients, collection and assembly of data, data analy-
sis and interpretation, final approval of manuscript and manuscript writ-
ing. Shreyamsa manjunath contributed to provision of study materials
or patients, collection and assembly of data, final approval of
manuscript and manuscript writing. Suresh Babu contributed to provi-
sion of study materials or patients and collection and assembly of data.
Pooja Ramakant contributed to conception and design, provision of
study materials or patients, final approval of manuscript and manuscript
writing. Kulranjan singh contributed to provision of study materials or
patients, final approval of manuscript and manuscript writing. Anand
Mishra contributed to provision of study materials or patients, adminis-
trative support, final approval of manuscript and manuscript writing.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available on
request from the corresponding author. The data are not publicly
available due to privacy or ethical restriction.
ORCID
Chanchal Rana https://orcid.org/0000-0002-1783-7689
REFERENCES
1. Seethala RR, Baloch ZW, Barletta JA, et al. Noninvasive follicular thy-
roid neoplasm with papillary-like nuclear features: a review for pathol-
ogists. Mod Pathol. 2018;31(1):39-55.
2. Nikiforov YE, Seethala RR, Tallini G, et al. Nomenclature revision for
encapsulated follicular variant of papillary thyroid carcinoma: a para-
digm shift to reduce overtreatment of indolent tumors. JAMA Oncol.
2016;2(8):1023-1029.
3. Lloyd RV, Osamura RY, Klöppel G, eds. WHO Classification of Tumours
of Endocrine Organs. 4th ed. Lyon: IARC Press; 2017.
4. Bychkov A, Jung CK, Liu Z, Kakudo K. Non invasive follicular thyroid
neoplasm with papillary-like nuclear features in Asian practice: per-
spectives for surgical pathology and cytopathology. Endocr Pathol.
2018;29(3):276-288.
5. Canberk S, Gunes P, Onenerk M, et al. New concept of the encapsu-
lated follicular variant of papillary thyroid carcinoma and its impact on
the Bethesda system for reporting thyroid cytopathology: a single-
institute experience. Acta Cytol. 2016;60(3):198-204.
6. Hahn SY, Shin JH, Lim HK, et al. Preoperative differentiation between
noninvasive follicular thyroid neoplasm with papillary-like nuclear fea-
tures (NIFTP) and non-NIFTP. Clin Endocrinol (Oxf). 2017;86(3):444-450.
7. Hirokawa M, Higuchi M, Suzuki A, Hayashi T, Kuma S, Miyauchi A.
Non invasive follicular thyroid neoplasm with papillary-like nuclear
features: a single-institutional experience in Japan. Endocr J. 2017;64
(12):1149-1155.
8. Jeon MJ, Song DE, Jung CK, et al. Impact of reclassification on thyroid
nodules with architectural Atypia: from noninvasive encapsulated fol-
licular variant papillary thyroid carcinomas to noninvasive follicular
thyroid neoplasm with papillary-like nuclear features. PLoS One. 2016;
11(12):e0167756.
9. Lee SE, Hwang TS, Choi Y-L, et al. Molecular profiling of papillary thy-
roid carcinoma in Korea with a high prevalence of BRAFV600E muta-
tion. Thyroid. 2017;27(6):802-810.
10. Mahajan S, Agarwal S, Kocheri N, Jain D, Mathur SR, Iyer VK. Cytopa-
thology of noninvasive follicular thyroid neoplasm with papillary-like
nuclear features: a comparative study with similar patterned papillary
thyroid carcinoma variants. Cytopathol. 2018;29(3):233-240.
11. Thompson LD. Ninety-four cases of encapsulated follicular variant of
papillary thyroid carcinoma: a name change to noninvasive follicular
thyroid neoplasm with papillary-like nuclear features would help pre-
vent overtreatment. Mod Pathol. 2016;29(7):698-707.
12. Rosario PW, Mour~ao GF, Nunes MB, Nunes MS, Calsolari MR. Non
invasive follicular thyroid neoplasm with papillary-like nuclear fea-
tures. Endocr Relat Cancer. 2016;23(12):893-897.
340 RANA ET AL.

13. Paulson VA, Shivdasani P, Angell TE, et al. Non invasive follicular thy-
roid neoplasm with papillary-like nuclear features accounts for more
than half of “carcinomas” harboring RAS mutations. Thyroid. 2017;27
(4):506-511.
14. Bychkov A, Keelawat S, Agarwal S, et al. Impact of noninvasive follic-
ular thyroid neoplasm with papillary-like nuclear features on the
Bethesda system for reporting thyroid cytopathology: a multi-
institutional study in five Asian countries. Pathology (Phila). 2018 Jun;
50(4):411-417.
15. Cibas ES, Ali SZ. The 2017 Bethesda system for reporting thyroid
cytopathology. Thyroid. 2017;27(11):1341-1346.
16. Faquin WC, Wong LQ, Afrogheh AH, et al. Impact of reclassifying
noninvasive follicular variant of papillary thyroid carcinoma on the
risk of malignancy in the Bethesda system for reporting thyroid cyto-
pathology. Cancer Cytopathol. 2016;124(3):181-187.
17. Strickland KC, Howitt BE, Marqusee E, et al. The impact of noninva-
sive follicular variant of papillary thyroid carcinoma on rates of malig-
nancy for fine-needle aspiration diagnostic categories. Thyroid. 2015;
25(9):987-992.
18. Cibas ES, Ali SZ. The Bethesda system for reporting thyroid cytopa-
thology. Thyroid. 2009;19(11):1159-1165.
19. Basolo F, Macerola E, Ugolini C, Poller DN, Baloch Z. The molecular
landscape of noninvasive follicular thyroid neoplasm with papillary-
like nuclear features (NIFTP): a literature review. Adv Anat Pathol.
2017;24(5):252-258.
20. Giannini R, Ugolini C, Poma AM, et al. Identification of two distinct
molecular subtypes of noninvasive follicular neoplasm with papillary-
like nuclear features by digital RNA counting. Thyroid. 2017;27(10):
1267-1276.
21. Jiang XS, Harrison GP, Datto MB. Young investigator challenge:
molecular testing in noninvasive follicular thyroid neoplasm with
papillary-like nuclear features. Cancer Cytopathol. 2016 Dec;124(12):
893-900.
22. du Jour KP, Schmitt AC, Chen AY, Griffith CC. Application of strict
criteria for noninvasive follicular thyroid neoplasm with papillary-like
nuclear features and encapsulated follicular variant papillary thyroid
carcinoma: a retrospective study of 50 tumors previously diagnosed
as follicular variant PTC. Endocr Pathol. 2018;29(1):35-42.
23. Rosario PW. Impact of noninvasive follicular thyroid neoplasm with
papillary-like nuclear features (NIFTP) on the outcomes of lobectomy.
Ann Surg Oncol. 2018;26(1):306.
24. Cho U, Mete O, Kim M-H, Bae JS, Jung CK. Molecular correlates and
rate of lymph node metastasis of noninvasive follicular thyroid neo-
plasm with papillary-like nuclear features and invasive follicular vari-
ant papillary thyroid carcinoma: the impact of rigid criteria to
distinguish noninvasive follicular thyroid neoplasm with papillary-like
nuclear features. Mod Pathol. 2017;30(6):810-825.
25. Pusztaszeri M, Auger M. Update on the cytologic features of papillary
thyroid carcinoma variants. Diagn Cytopathol. 2017;45(8):714-730.
26. Singh R, Avila J, Jo K, et al. Patients with noninvasive follicular thyroid
neoplasm with papillary-like nuclear features are unlikely to have
malignant preoperative cytology. Ann Surg Oncol. 2017;24(11):3300-
3305.
27. Parente DN, Kluijfhout WP, Bongers PJ, et al. Clinical safety of
renaming encapsulated follicular variant of papillary thyroid carci-
noma: is NIFTP truly benign? World J Surg. 2018;42(2):321-326.
28. Jaconi M, Manzoni M, Pincelli AI, et al. The impact of the noninvasive
follicular thyroid neoplasm with papillary-like nuclear feature termi-
nology in the routine diagnosis of thyroid tumours. Cytopathol. 2017;
28(6):495-502.
29. Zhou H, Baloch ZW, Nayar R, et al. Non invasive follicular thyroid
neoplasm with papillary-like nuclear features (NIFTP): implications for
the risk of malignancy (ROM) in the Bethesda system for reporting
thyroid cytopathology (TBSRTC). Cancer Cytopathol. 2018;126(1):
20-26.
30. Kiernan CM, Weiss VL, Mehrad M, Ely K, Baregamian N,
Solórzano CC. New terminology-noninvasive follicular neoplasm with
papillary-like nuclear features (NIFTP) and its effect on the rate of
malignancy at a single institution. Surgery. 2018;163(1):55-59.
31. Howitt BE, Chang S, Eszlinger M, et al. Fine-needle aspiration diagno-
ses of noninvasive follicular variant of papillary thyroid carcinoma.
Am J Clin Pathol. 2015;144(6):850-857.
32. Chandler JB, Colunga M, Prasad ML, et al. Identification of distinct
cytomorphologic features in the diagnosis of NIFTP at the time of
preoperative FNA: implications for patient management. Cancer
Cytopathol. 2017;125(11):865-875.
33. Strickland KC, Vivero M, Jo VY, et al. Preoperative Cytologic diagnosis
of noninvasive follicular thyroid neoplasm with papillary-like nuclear
features: a prospective analysis. Thyroid. 2016;26(10):1466-1471.
34. Rosario PW. Diagnostic criterion of noninvasive follicular thyroid
neoplasm with papillary-like nuclear features (NIFTP): absence of
papillae. Hum Pathol. 2018;83:225.
35. Ng D, Can NT, Ma ZV, van Zante A, Ljung B-M, Khanafshar E.
Cytomorphologic features of noninvasive follicular thyroid neoplasm
with papillary-like nuclear features (NIFTP): a comparison with infil-
trative follicular variant of papillary thyroid carcinoma. J Basic Clin
Med. 2017;1:51-56.
36. Maletta F, Massa F, Torregrossa L, et al. Cytological features of “non-invasive follicular thyroid neoplasm with papillary-like nuclear fea-
tures” and their correlation with tumor histology. Hum Pathol. 2016;
54:134-142.
37. Rosario PW, Silva TH, de Oliveira PHL. Impact of noninvasive follicu-
lar thyroid neoplasm with papillary-like nuclear features (NIFTP) on
the risk of malignancy estimated by the ultrasonographic classifica-
tion of the American Thyroid Association (ATA) in thyroid nodules
>1 cm. Endocrine. 2018;60(3):535-536.
38. Yang GCH, Fried KO. Pathologic basis of the sonographic differences
between thyroid cancer and noninvasive follicular thyroid neoplasm with
papillary-like nuclear features. Ultrasonography. 2018;37(2):157-163.
39. Bizzarro T, Martini M, Capodimonti S, et al. Young investigator chal-
lenge: the morphologic analysis of noninvasive follicular thyroid neo-
plasm with papillary-like nuclear features on liquid-based cytology:
some insights into their identification. Cancer Cytopathol. 2016;124
(10):699-710.
40. Kim M, Kim JE, Kim HJ, Chung YR, Kwak Y, Park SY. Cytologic diag-
nosis of noninvasive follicular thyroid neoplasm with papillary-like
nuclear features and its impact on the risk of malignancy in the
Bethesda system for reporting thyroid cytopathology: an institutional
experience. J Pathol Transl Med. 2018;52(3):171-178.
41. Layfield LJ, Baloch ZW, Esebua M, Kannuswamy R, Schmidt RL.
Impact of the reclassification of the noninvasive follicular variant of
papillary carcinoma as benign on the malignancy risk of the Bethesda
system for reporting thyroid cytopathology: a meta-analysis study.
Acta Cytol. 2017;61(3):187-193.
42. Rosario PW. Ultrasonography and cytology as predictors of noninva-
sive follicular thyroid (NIFTP) neoplasm with papillary-like nuclear
features: importance of the differential diagnosis with the invasive
encapsulated follicular variant of papillary thyroid cancer. Clin
Endocrinol (Oxf). 2017;87(5):635-636.
How to cite this article: Rana C, Manjunath S, Ramakant P,
Singh K, Babu S, Mishra A. Noninvasive follicular neoplasm
with papillary like nuclear features: A comprehensive analysis
with a diagnostic algorithm. Diagnostic Cytopathology. 2020;
48:330–341. https://doi.org/10.1002/dc.24375
RANA ET AL. 341