-
Management of Childhood Onset Nephrotic Syndrome
abstractThe therapeutic approach to childhood nephrotic syndrome
is basedon a series of studies that began with an international
collaborativeeffort sponsored by the International Study of Kidney
Disease in Chil-dren in 1967. The characteristics of children
presenting with nephroticsyndrome have changed over recent decades
with greater frequencyof the challenging condition focal segmental
glomerulosclerosis and agreater prevalence of obesity and diabetes
mellitus, which may beresistant to glucocorticoids in the former
and exacerbated by long-term glucocorticoid therapy in the latter 2
conditions. The ChildrensNephrotic Syndrome Consensus Conference
was formed to systemati-cally review the published literature and
generate a childrens primarynephrotic syndrome guideline for use in
educational, therapeutic, andresearch venues. Pediatrics
2009;124:747757
Idiopathic nephrotic syndrome affects 16 in 100 000 children,
makingthis condition one of the more common childhood kidney
diseases. Thetherapeutic approach to childhood nephrotic syndrome
is based onstudies that began with the International Study of
Kidney Disease inChildren (ISKDC). Between 1967 and 1974, 521
children with nephroticsyndrome entered into this study with a
histologic classification ofminimal change (MCNS) (77.1%), focal
segmental glomerulosclerosis(FSGS) (7.9%), membranoproliferative
glomerulonephritis (6.2%), andothers (8.8%).1,2 Normalization of
urine protein levels with 8 weeks ofglucocorticoid therapy was
predictive of MCNS with a sensitivity of93.1% and specificity of
72.2%.2 Consequently, pediatricians began us-ing therapeutic
response to glucocorticoids for evaluation and therapyfor incident
patients.
The sentinel work of the ISKDC followed by a series of studies
by theArbeitsgemeinschaft fur Padiatrische Nephrologie (APN) formed
thefoundation for management of children with nephrotic
syndrome.35
The characteristics of children presenting with nephrotic
syndromehave changed over recent decades. Contemporary literature
has doc-umented an increasing incidence of FSGS-induced nephrotic
syndromein the 1990s compared with that of the 1970s.6 FSGS is less
responsiveto glucocorticoids and has greater risk for progressive
kidney failurecompared with the MCNS that dominated the ISKDC
cohort.2,7 Fur-thermore, children in the United States have a
greater prevalence ofobesity and diabetes mellitus compared with
children of previous de-cades, which may be exacerbated by
long-term glucocorticoid thera-py.8,9 The Childrens Nephrotic
Syndrome Consensus Conference wasformed to assess current
evaluation and management practices forchildren with nephrotic
syndrome among North American Pediatric
CONTRIBUTORS: Debbie S. Gipson, MD, MS,a Susan F.
Massengill,MD,b Lynne Yao, MD,c Shashi Nagaraj, MD,d William E.
Smoyer,MD,e,f John D. Mahan, MD,f Delbert Wigfall, MD,g Paul Miles,
MD,h
Leslie Powell, RN, CPNP,a Jen-Jar Lin, MD, PhD,d,i
HowardTrachtman, MD,j and Larry A. Greenbaum, MD, PhDk
aDivision of Nephrology and Hypertension, Department ofMedicine
and Pediatrics, University of North Carolina, ChapelHill, North
Carolina; bPediatric Nephrology, Levine ChildrensHospital at
Carolinas Medical Center, Charlotte, North Carolina;cDepartment of
Pediatric Nephrology, Inova Fairfax Hospital forChildren, Falls
Church, Virginia; dDepartment of PediatricNephrology, Wake Forest
University Medical Center, Winston-Salem, North Carolina;
eDepartment of Pediatric Nephrology,University of Michigan, Ann
Arbor, Michigan; fDepartment ofPediatric Nephrology, Nationwide
Childrens Hospital, Columbus,Ohio; gDivision of Nephrology,
Department of Pediatrics, DukeUniversity Medical Center, Durham,
North Carolina; hAmericanBoard of Pediatrics, Chapel Hill, North
Carolina; iDepartment ofPediatric Nephrology, East Carolina
University, Greenville, NorthCarolina; jDepartment of Pediatric
Nephrology, SchneiderChildrens Hospital, New Hyde Park, New York;
and kDepartmentof Pediatric Nephrology, Emory University and
ChildrensHealthcare of Atlanta, Atlanta, Georgia
KEY WORDSproteinuria, pediatric, nephrosis, kidney disease
ABBREVIATIONSISKDCInternational Study of Kidney Disease in
ChildrenMCNSminimal-change nephrotic syndromeFSGSfocal segmental
glomerulosclerosisUp/curine protein/creatinine ratioBIDtwice
dailyACE-Iangiotensin-converting enzyme inhibitorARBangiotensin
receptor blockerHMG-CoA3-hydroxy-3-methylglutaryl coenzyme A
www.pediatrics.org/cgi/doi/10.1542/peds.2008-1559
doi:10.1542/peds.2008-1559
Accepted for publication Nov 26, 2008
Address correspondence to Debbie S. Gipson, MD, MS, Universityof
North Carolina, Division of Nephrology and Hypertension,
7012Burnett Womack Building, CB 7155, Chapel Hill, NC
27599-7155.E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,
1098-4275).
Copyright 2009 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno
financial relationships relevant to this article to disclose.
SPECIAL ARTICLES
PEDIATRICS Volume 124, Number 2, August 2009 747 at
Indonesia:AAP Sponsored on February 7,
2015pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
Nephrologists,10 systematically reviewthe published literature,
and generatea childrens primary nephrotic syn-drome guideline for
use in educa-tional, therapeutic, and researchvenues.
METHODS
Participating sites were gatheredfrom the Southeast and Midwest
Pedi-atric Nephrology study groups. Onerepresentative from each
center wasasked to represent the institution forthe consensus
conference and subse-quent meetings by conference call.Participants
(along with their institu-tions) are listed as authors.
A literature search was conducted byusing the PubMed search
engine.English-language literature generatedfrom North America,
Europe, and Asiawas identified by using the key wordsnephrotic
syndrome, proteinuria,and child. A total of 709 articles
wereidentified. Simultaneously, membersof the consensus group were
asked tosubmit a list of key articles relevant tothe topic of
childhood nephrotic syn-drome that were used to validate andaugment
the PubMed search. Articleswith original scientific
investigation,clinical trials, cohorts, and case-control studies
were retained for a to-tal of 344 articles.
The consensus study group was di-vided into working groups to
reviewthe literature and present guidelinerecommendations to the
full studygroup for discussion at the June 21,2007, Childrens
Nephrotic SyndromeStudy Group Consensus Conferenceheld in Chapel
Hill, North Carolina, andduring subsequent conference callsthrough
July 30, 2007. The charge tothe consensus participants was to
cre-ate a consensus document and educa-tional module for childhood
nephroticsyndrome on the basis of literaturewhen available andwith
expert opinion
when the literature was insufficient.All recommendations were
generatedby the physician participants and werenot subject to
previous review by thefunding agency.
This document was designed for physi-cians who manage children 1
to 18years old with:
a urine protein/creatinine ratio(Up/c) of 211; and
a serum albumin level of 2.5mg/dL.
On presentation, the evaluation of achild with proteinuria
includes a thor-ough review for signs and symptomsthat may suggest
that the nephroticsyndrome is a secondary condition.Malar rash,
adenopathy, arthritis, fe-vers and weight loss may be signs
ofsystemic lupus erythematosus, anddiffuse lymphadenopathy and
hepato-splenomegaly may suggest lymphoma.These disorders require a
differentevaluation andmanagement approachand will not be
considered within thisdocument.
EVALUATION OF CHILDREN WITHNEPHROTIC SYNDROME
Recommendations for initial evalua-tion include:
urinalysis;
first morning Up/c;
serum electrolytes, serum urea ni-trogen, creatinine, and
glucose;
cholesterol level;
serum albumin level;
complement 3 level;
antinuclear antibody level (forchildren aged 10 years or withany
other signs of systemic lupuserythematosus);
hepatitis B, hepatitis C, and HIV se-rology in high-risk
populations;
purified protein derivative level; and
kidney biopsy for children aged12 years.
A urinalysis with microscopy is recom-mended for identifying
hematuria, cellu-lar casts, or other evidence of nephritis,which
should precipitate evaluation forglomerulonephritis rather than
primarynephrotic syndrome. First morning Up/cwill establish the
degree of proteinuriawithout the contribution of benign
ortho-static increases in urinary protein excre-tion. Complement 3
and antinuclear anti-body screen for proteinuric diseasesassociated
with hypocomplementemia,including membranoproliferative
glo-merulonephritis and systemic lupus ery-thematosus, which
require additional in-vestigation with laboratory tests andkidney
biopsy.
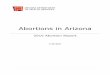
A kidney biopsy for children over theage of 12 is recommended
because ofthe frequency of diagnoses other thanminimal-change
disease. Figure 1 pre-sents a summary of 223 kidney biop-sies
obtained between 2001 and 2006from a southeast regional
referralcenter showing that FSGS accounts forthe majority of kidney
diseases in chil-dren undergoing biopsy for protein-uria in this
region.
DEFINITIONS
The following are terms commonly usedfor nephrotic
syndromemanagement.Remission: Up/c 0.2 or Albustix-negative
(Albustix, Miles, Inc, Diagnos-tics Division, Elkhart, IN) or trace
for3 days.Relapse: After remission, an increasein the first morning
Up/c to 2 or Al-bustix reading of 2 for 3 of 5 consec-utive
days.Frequently relapsing: 2 or more re-lapses within 6 months
after initialtherapy or 4 relapses in any 12-month period.Steroid
dependent: Relapse duringtaper or within 2 weeks of
discontinu-ation of steroid therapy.Steroid resistant: Inability to
induce aremission with 4 weeks of daily steroidtherapy.
748 GIPSON et al at Indonesia:AAP Sponsored on February 7,
2015pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
Discrepancies in the definition ofsteroid-resistant nephrotic
syndromecreate difficulties for comparing out-comes for reported
treatment strate-gies.2,12,13 On the basis of the ISKDCstudy, 95%
of children with steroid-responsive nephrotic syndrome
willdemonstrate resolution of proteinuriawith 4 weeks of daily
glucocorticoidtherapy and 100% after an additional 3weeks of
alternate-day therapy.2 Thisconsensus guideline uses a 4-weekoral
glucocorticoid limit to define ste-roid resistance; however,
therapy maybe continued during the subsequentevaluation for
steroid-resistant ne-phrotic syndrome, allowing the cap-ture of
late responders. Glucocorticoiddosing is presented as mg/kg and
mg/m2. Published studies in childhood ne-phrotic syndrome have
included glu-cocorticoid dosing with either mg/kgor mg/m2 regimens.
Actual prescribeddose will vary on the basis of the stan-dard used,
especially at the extremesof weight, but no literature exists
toprove that 1 scheme is more effectivethan the other.
THERAPY
Initial Therapy for ChildhoodNephrotic Syndrome
prednisone 2 mg/kg per day for 6weeks (maximum: 60 mg);
thenprednisone1.5mg/kgonalternatedays for 6weeks (maximum:
40mg);
no steroid taper is required at theconclusion of this initial
therapy.5
The initial therapy for nephrotic syndromeinchildren
isbasedonthestudiessumma-
rized in Fig 2. This series of studies evalu-ated initial
prednisone exposure rangingfrom 4 to 28 weeks.25,14,15 The
12-weektreatment regimen including 6 weeksof prednisone at 60 mg/m2
per day (2mg/kg per day) plus 6 weeks at 40mg/m2 (1.5mg/kg) on
alternate days isrecommended by this consensuspanel because of
maximum effect andminimization of glucocorticoid-relatedadverse
effects.5,1518 Results of severalstudies in India, Europe, and
Japanhave challenged this course of therapywith a long treatment
taper, additionof cyclosporine, and lower initial dailyprednisone
doses of 40 mg/m2 per daybut have not demonstrated
significantimprovements in sustained remissionover the traditional
12-week regi-men.14,16,18,19 Cessation of prednisone
after12weekswithout a taperhasnodisadvan-tage and may limit the
negative effects ofprolonged courses of prednisone. A 24-month
sustained remission rate of 49%and frequent-relapse rate of 29% is
ex-pectedwith this regimen.
Initial or Infrequent-RelapseTherapy
prednisone 2 mg/kg per day untilurine protein test results are
nega-tive or trace for 3 consecutive days;
then prednisone 1.5 mg/kg on alter-nate days for 4 weeks.
FIGURE 1Kidney biopsy results from 223 children with proteinuria
referred for diagnostic kidney biopsy (Glo-merular Disease
Collaborative Network, J. Charles Jennette, MD, Hyunsook Chin, MS,
and D. S. Gipson,2007). n number of patients. MPGN indicates
membranoproliferative glomerulonephritis; C1Q,nephropathy.
FIGURE 2Summary of early published trials of initial therapy
studies for primary nephrotic syndrome inchildren. APN indicates
Arbeitsgemeinschaft fur Padiatrische. CyA indicates cyclosporine A
and Predindicates prednisone.
SPECIAL ARTICLES
PEDIATRICS Volume 124, Number 2, August 2009 749 at
Indonesia:AAP Sponsored on February 7,
2015pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
Treatment of the nephrotic syndromeinitial or infrequent relapse
requiresconsiderably less glucocorticoids thaninitial therapy.
Glucocorticoids (2 mg/kgper day prednisone equivalent)
continueuntil urine protein levels normalize for 3days. The dose is
then reduced to alter-nate days for 4 weeks.20
Frequently Relapsing NephroticSyndrome Therapy Options
prednisone 2 mg/kg per day untilproteinuria normalizes for 3
days,1.5 mg/kg on alternate days for 4weeks, and then taper over
2months by 0.5 mg/kg on alternatedays (total: 34 months);
oral cyclophosphamide 2 mg/kg perday for 12 weeks (cumulative
dose:168 mg/kg) based on ideal bodyweight started during
prednisone(2 mg/kg per day) induced remis-sion, decrease prednisone
dose to1.5 mg/kg on alternate days for 4weeks, and then taper over
4 weeks;
mycophenolate mofetil 25 to 36 mg/kgper day (maximum: 2 g/day)
dividedtwice daily (BID) for 1 to 2 years with atapering dose of
prednisone; and
cyclosporine A 3 to 5 mg/kg per day di-vided BID for an average
of 2 to 5 years.
Patients with frequently relapsing ne-phrotic syndrome have
treatment op-tions that include extended dosing ofglucocorticoids,
cytotoxic agents, myco-phenolate mofetil, or calcineurin
inhibi-tors. When glucocorticoids have not pro-duced signs of
toxicity, this therapy maybe continued with an extended
dosingregimen. Clear data regarding the opti-mal extended course of
prednisone or,indeed, any other of the therapeutic op-tions for
frequently relapsing nephroticsyndrome have not been published;
con-sequently, these recommendations arelargely based on
opinion.
Cytotoxic agents, including cyclophos-phamide or chlorambucil,
used in com-bination with glucocorticoids have beendemonstrated to
induce a sustained
remission of 72% at 2 years and 36% at5 years in frequently
relapsingnephroticsyndrome.21 On the basis of a meta-analysis from
pediatric nephrotic syn-drome studies, cytotoxic agents have
asignificant toxicity profile including 1%fatality, 1.5% severe
bacterial infections,and 0.2% to 0.6% late malignancy. Up to3% of
patients receiving chlorambucilhave reported seizures. Reduced
fertilityafter cytotoxic therapy has been de-scribed. Compared with
cyclophospha-mide, chlorambucil is associated with aslightly
greater toxicity profileandno im-provement in efficacy.21
A 6-month course of mycophenolatemofetil with a tapering dose of
alternate-day prednisone induced remission in75% of 33 patients
during therapy andmaintained in 25%after therapywasdis-continued.22
The relapse rate in thesepa-tients improved from 1 episode every
2monthsbeforemycophenolatemofetil to1 every 14.7 months during
therapy.22
Cyclosporine for 2 to 5 years has re-sulted in60%remissionduring
the initialyear of therapy.23,24 Remissionwasmain-tained in only
28% of children duringthe second year of cyclosporine.25 Up to40%
of patients may need additionalalternate-day prednisone to
maintainremission. There is a high rate of re-lapse after
cyclosporine withdrawal.25
The nephrotoxic effects of cyclosporinewarrant careful
monitoring of kidneyfunction and blood drug levels. Tacro-limus, an
alternative calcineurin in-hibitor, provides no advantage
re-garding nephrotoxicity profile. The riskfor nephrotoxicity
attributable to cal-cineurin inhibitors makes this a third-line
option for frequently relapsing ne-phrotic syndrome.23,25,26
Steroid-Dependent NephroticSyndrome Therapy
glucocorticoids are preferred in the ab-sence of significant
steroid toxicity;
secondary alternatives should be cho-sen on the basis of
risk/benefit ratio;
cyclosporine A 3 to 5 mg/kg per daydivided BID;
tacrolimus 0.05 to 0.1mg/kg per daydivided BID; and
mycophenolate mofetil 24 to 36mg/kg per day or 1200 mg/m2 perday
divided BID (maximum: 2 g/day).
Steroid-dependent nephrotic syndromeoccurs in 24% of children
with ne-phrotic syndrome.27 Some childrencan maintain a remission
with low-dose glucocorticoids given daily or onalternate days, but
many continue torelapse. Steroid-induced adverse ef-fects, such as
obesity, hypertension, andcataracts, develop in a significant
pro-portionofpatientsandpromptcliniciansto search for
steroid-sparing therapies.
There have been no randomized, con-trolled trials reported in
the English-language literature that addresssteroid-free protocols
for steroid-dependent nephrotic syndrome. For 1European study an
improved outcome-with the glucocorticoid deflazacortcompared with
prednisone in 40 chil-dren was reported.28 Deflazacort is
notavailable in the United States. Use ofcyclosporine, levamisole,
mycopheno-latemofetil,mizoribine(notavailable in theUnited States),
cyclophosphamide, orchlorambucil may reduce the risk of re-lapses
without glucocorticoids.21,2932
Oralcyclophosphamide2to3mg/kgperdayfor8 to 12 weeks in
steroid-dependent chil-dren induces remission in 40% at 2 years,24%
at 5 years, and 17% in long-termfollow-up.21,32 Given the severity
ofcyclophosphamide-associated adverse ev-ents, cytotoxic agents are
considered athird-line choice for steroid-dependent ne-phrotic
syndrome therapy.
Steroid-Resistant NephroticSyndrome Management
kidney biopsy;
tailor therapeutic regimen accord-ing to kidney histology;
and
provide optimal supportive therapy.
750 GIPSON et al at Indonesia:AAP Sponsored on February 7,
2015pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
Steroid resistance places a patient at in-creased risk for both
the development ofcomplications of nephrotic syndromeand
progression to end-stage kidney dis-ease.33,34 The goal of therapy
for steroid-resistant nephrotic syndrome is com-plete resolution of
proteinuria andpreservation of kidney function. How-ever, pediatric
and adult studies havedocumented an improved kidney sur-vival rate
for patients with a partial re-mission, defined as 50% reduction
inproteinuria from baseline, comparedwith those without control of
protein-uria.33,34 Because of this risk for end-stage kidney
disease and the potentialutility of histology for
therapeuticdecision-making, nephrologists performa kidney biopsy
before initiation of ther-apy for patients with steroid
resistance.
The optimal therapy for steroid-resistant nephrotic syndrome
remainspoorly defined but requires a completeunderstandingof
thearmamentariumoftherapeutic options and a fully engagedpediatric
nephrologist to promote an op-timal outcome. Clear
evidence-basedguidelines for the treatment of steroid-resistant
nephrotic syndrome are notpossible on the basis of a lack of
suffi-cient randomized, controlled trials.
There are 3 major categories of ther-apy for steroid-resistant
nephroticsyndrome: (1) immunosuppressive;(2) immunostimulatory; and
(3) non-immunosuppressive. The more com-monly used
immunosuppressive ther-apies include calcineurin
inhibitors,mycophenolate mofetil, pulse intrave-nous
methylprednisolone, and cyto-toxic agents.3541 Other less
commonlyused or controversial treatments in-clude plasma exchange
and immuno-absorption.42 Novel agents are underinvestigation, but
their safety and effi-cacy have not yet been determined.4345
The only reported immunostimulatoryagent in use is levamisole.
However,this agent is not universally available.Last,
nonimmunosuppressive treat-
ments are commonly considered to beconservative therapy and
includeangiotensin-converting enzyme inhibi-tors (ACE-Is),
angiotensin receptorblockers (ARBs), and vitamin E.33,46
Disease-based therapeutic recommen-dations are beyond the scope
of theseguidelines.
ACE-I and ARB Therapy
ACE-I or ARB therapy is recom-mended for steroid-resistant
ne-phrotic syndrome;
consider use of ACE-Is or ARBs withsteroid-dependent or
frequently re-lapsing nephrotic syndrome; and
counsel regarding contraindications ofACE-I or ARB therapy
during pregnancy.
Blockade of the renin-angiotensin sys-tem has been shown to
blunt the evo-lution of kidney disease, especiallythose associated
with marked protein-uria.4749 Several studies have demon-strated a
reduction in proteinuria withACE-I or ARB therapy.33,4850 These
drugsare generally well tolerated but alsohave documented adverse
effects in-cluding hyperkalemia, angioedema,cough (ACE-Is), and,
rarely, acute renalfailure. Combination therapy withACE-Is plus
ARBs may simultaneouslyincrease efficacy and
adverse-effectpotential.51,52 Women of childbearingage must be
counseled regarding theteratogenic effects of ACE-I and
ARBtherapy.53
Hypertension Management
control blood pressure to 90thpercentile of normal54;
recommend low-salt diet, exercise,and weight reduction if
obesity ispresent; and
ACE-Is and/or ARBs for chronicpharmacologic management.
Hypertension is present in 13% to51% of children with nephrotic
syn-drome.55,56 Blood pressure generallyimproves with remission of
nephrotic
syndrome.56 When antihypertensivetherapy is indicated, the
expected re-duction in proteinuria and blood pres-sure with ACE-I
or ARB agents makethem first-line agents.57
Edema Management
counsel caregivers regarding po-tential complications of edema;
and
consider treatment with low-sodiumdiet, modest fluid
restriction, diuretics,and albumin infusions.
Edema is one of the cardinal symp-toms of nephrotic syndrome.
Immedi-ate physician involvement is war-ranted if the patient
developsrespiratory distress, which may besecondary to pleural
effusions or pul-monary edema. Sodium restriction toa level of 1500
to 2000 mg daily is com-monly recommended. Severe edemaassociated
with weeping tissuesshould be monitored for secondary in-fection.
Severe edema may requirepharmacologic intervention includingloop
diuretics, thiazide diuretics, and25%albumin infusion. At a high
dose orwith chronic administration, diureticsmay cause hypokalemia,
exacerbatehyponatremia, cause intravascularvolume depletion, and
increase therisk for acute renal failure. Althoughonly a
temporizing measure, treat-ment with 25% albumin infusions
anddiuretics may be prescribed for chil-dren with severe edema.
Albumin infu-sion may produce acute expansion ofintravascular
volume leading to hyper-tension, pulmonary edema, and con-gestive
heart failure.58
COMPLICATIONS
The complications of childhood ne-phrotic syndrome are
associated withdisease activity and therapy. Active ne-phrotic
syndrome increases the riskfor therapy-associated growth
compli-cations, dyslipidemia, infections, andthromboembolism.
SPECIAL ARTICLES
PEDIATRICS Volume 124, Number 2, August 2009 751 at
Indonesia:AAP Sponsored on February 7,
2015pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
Obesity and Growth
monitor BMI and linear growth;
provide counseling on weight con-trol; and
consider glucocorticoid alterna-tives when short stature or
obesityis present.
Glucocorticoids may impair growthand increase BMI, with these
effectsproportional to dose and duration ofthe disease and
therapy.5963 Steroid-sparing treatment strategies may im-prove
linear growth.59,64,65 Glucocorti-coid therapy may increase
BMI.59,66,67
Children who are overweight at initia-tion of steroid therapy
are more likelyto remain overweight after treatmentfor nephrotic
syndrome.62,67 Steroid-sparing strategies have been associ-ated
with a lower BMI.59,65 Anticipatorydietary counseling is
recommendedfor children with nephrotic syndrome.
Dyslipidemia
low-fat diet;
consider low-density lipoproteincholesterol-lowering drug
therapywhen fasting low-density lipopro-tein cholesterol levels are
persis-tently 160 to 190 mg/dL; and
counsel regarding contraindica-tions of
3-hydroxy-3-methylglutarylcoenzyme A (HMG-CoA) reductaseinhibitors
during pregnancy.
Dyslipidemia is an expected finding inchildren with nephrotic
syndrome andmay resolve when patients are in re-mission. Children
who have refractorynephrosis often have persistent dyslip-idemia.
In adult studies, persistent ne-phrotic syndrome is associated
withatherosclerosis and an increased riskof coronary artery
disease. One retro-spective study, however, suggestedthat relapsing
nephrotic syndrome inchildhooddoes not lead to increase in riskfor
cardiovascular disease.68 Treatmentincludes dietary counseling to
limit di-etary fat to 30% of calories, satu-
rated fat to 10% of calories, and300 mg/day dietary
cholesterol.
Treatment with HMG-CoA reductaseinhibitors in adults with
nephroticsyndrome have demonstrated a ben-eficial effect on
dyslipidemia andmay impact the progression ofchronic kidney
disease.69,70 Treat-ment of children with steroid-resistant
nephrotic syndrome andpersistent dyslipidemia with HMG-CoA
reductase inhibitors has beenproposed in childhood dyslipidemiacare
guidelines, but randomizedstudies are lacking.71
Infection
counsel regarding signs and symp-toms of infections such as
cellulitis,peritonitis, and bacteremia; and
provide empiric therapy for peritonitisuntil culture results are
available.
Infection is a common complication inchildren with nephrotic
syndrome andan important cause of mortality.72
Edema associated with weeping tis-sues should bemonitored
carefully fordevelopment of secondary infectiouscomplications
including cellulitis.Spontaneous bacterial peritonitis, pre-senting
with fever, severe abdominalpain, peritoneal signs, and,
occasion-ally, signs of sepsis, is a well-describedcomplication
associated with morbid-ity and mortality.7375 The predisposi-tion
to peritonitis is felt to be multifac-torial, including the
presence of lowserum albumin, ascites, and an im-paired immune
system.74,76 Definitivediagnosis of peritonitis requires cul-ture
of peritoneal fluid. A Gram-stainand cell count should also be
obtained.Bacteremia may be concurrent.
Although Streptococcus pneumoniae isthemost common organism that
causesperitonitis in childhood nephrotic syn-drome, Gram-negative
organisms causea significant percentage of spontaneousbacterial
peritonitis cases.72,73,75,77 Thereare no data supporting the
efficacy of
prophylactic penicillin in preventingperitonitis in childhood
nephrotic syn-drome.78 The potential benefit must bebalanced
against the risk of allergicreactions and the development of
re-sistant organisms.77 Administration of23-valent and heptavalent
conjugatedpneumococcal vaccines is recom-mended to provide immunity
against abroad range of pneumococcal strains.
Thromboembolism
evaluate children with a thrombo-embolism for an underlying
hyper-coagulopathy; and
provide anticoagulation therapy forchildren with nephrotic
syndromeand thromboembolism.
Two percent to 5% of children with ne-phrotic syndrome develop
thrombo-embolism.7981 The risk seems higherin children with
steroid-resistant com-pared with steroid-sensitive disease.81
Potential sites for thromboembolisminclude deep vein, central
sinus, andrenal vein thrombosis, pulmonary em-bolism, and arterial
sites.
Multiple factors are postulated tocause the increased risk of
thrombo-embolism in nephrotic syndrome.There are urinary losses of
factorsthat inhibit clot formation (eg, anti-thrombin III) and
increased levels offactors that promote clot formation(eg,
fibrinogen).80 Thrombocytosis andplatelet hyperaggregability are
com-mon with nephrotic syndrome.82 More-over, volume depletion
caused by dehy-dration or diuretic therapy mayincrease the risk of
clot formation.81
Although there have been no placebo-controlled studies,
anticoagulationseems to be effective in childrenwith ne-phrotic
syndrome. Heparin, low molecu-larweight heparin, andoral
anticoagula-tion with warfarin are therapeuticoptions.81,8385
Fibrinolytic therapy hasbeen effectively used in some children,but
its use must be balanced by the in-creased risk of
complications.81,86,87
752 GIPSON et al at Indonesia:AAP Sponsored on February 7,
2015pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
During periods of disease activity andincreased thromboembolic
risk, chil-dren should be encouraged to continuephysical activity
and avoid prolongedbed rest. The role of prophylactic
antico-agulation medication such as low-doseaspirin isunclear.
Prophylacticanticoag-ulation may be indicated in the settingof
thromboembolism history, an under-lying hypercoagulable condition
beyondnephrotic syndrome, steroid-resistantnephrotic syndrome, and
the presenceof a central venous catheter.88 Thepoten-tial benefits
and risks of such therapymust be evaluated individually.
Vaccinations
immunize with the 23-valent andheptavalent conjugated
pneumo-coccal vaccines;
immunize the immunosuppressedor actively nephrotic patient
andhousehold contacts with inactivatedinfluenza vaccine yearly;
defer immunization with livevaccines:
until prednisone dose is 2 mg/kgper day (maximum: 20mg);
for 3 months from completion oftherapy with cytotoxic agents;
or
for 1 month from completion ofother daily immunosuppression;
provide varicella immunization ifnonimmune, on the basis of
immu-nization history, disease history, orserologic evaluation;
provide postexposure immunoglob-ulin for nonimmune
immunocom-promised patients; and
consider intravenous acyclovir forimmunosuppressed children at
theonset of chicken pox lesions.
Vaccination is especially important forchildren with nephrotic
syndrome. Theyare at risk formore severe infections be-cause of the
impact of nephrotic syn-drome and the effects of
immunosup-pression.89 Moreover, children withnephrotic syndrome are
especially sus-ceptible to pneumococcal disease.75
Varicella infection may lead to life-threatening disease in
children receiv-ing immunosuppressive medications.89
Varicella vaccination, proven to be safeand effective in
children with nephroticsyndrome, should be administered onthe basis
of the recommended guide-lines for live vaccines.9093
Monitoring
Table 1 sets forth a summary of moni-toring recommendations
accordingto nephrotic syndrome severity andtreatment regimen.
CONCLUSIONS
Childhood nephrotic syndrome is achronic health condition that,
opti-mally, is managed by a team preparedto provide ongoing care.
Pediatric pa-tients and their caregivers require ed-ucation
regarding the complex treat-ment of this chronic
condition,including proper administration ofmedications, adherence
to dietary re-strictions, and necessity for medicalmonitoring. An
initial 12-week glu-cocorticoid therapeutic regimen hasbeen shown
to decrease subsequentnephrotic syndrome relapse rates
insteroid-responsive children.2,3 How-ever, to avoid many of the
adverse ef-fects associated with this treatmentcourse, careful
anticipatory guidanceand support of families should be pro-vided by
a multidisciplinary team.
Complications of nephrotic
syndromethatariseduringdiseaseactivityaswell asthe treatment itself
also require an antici-patory approach. Commonly
occurringcomplications related to chronic steroidadministration
include hypertension, obe-sity, and linear growth retardation.
Abnor-malities in bone density may also develop.Steroid-sparing
regimens warrant agent-specific monitoring. Adverse effects
arevaried and range from hypertension andacute renal failure with
calcineurin inhibi-
TABLE 1 Monitoring Recommendations for Children With Nephrotic
Syndrome
HomeUrineProtein
Weight,Growth,BMI
BloodPressure
Creatinine Electrolytes SerumGlucose
CBC LipidProfile
DrugLevels
LiverFunction
Urinalysis CPK
DiseaseMild (steroid responsive) Moderate (frequentrelapsing,
steroiddependent)
Severe (steroid resistant) TherapyCorticosteroids
Cyclophosphamide Mycophenolate mofetil Calcineurin inhibitors
ACE-Is/ARBs HMG-CoA reductaseinhibitors
CBC indicates complete blood count; CPK, creatine kinase.
SPECIAL ARTICLES
PEDIATRICS Volume 124, Number 2, August 2009 753 at
Indonesia:AAP Sponsored on February 7,
2015pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
tors to infertility and potential for futuremalignancywith
cytotoxic agents.
Patients with steroid-resistant ne-phrotic syndrome are at
greatest riskfor progressive kidney injury, compli-cations of
chronic nephrotic syn-drome, and complications associatedwith
pharmaceutical therapy. An indi-vidualized treatment plan based
onkidney histology and response will re-quire the involvement of a
pediatric
nephrologist to optimize control of ne-phrotic syndrome and
minimize mor-bidity and mortality rates.
These guidelines are based on the bestsummary of available
published dataand opinion when data were insuffi-cient. In addition
to the development ofthese guidelines, the panel has identi-fied
opportunities for validation andimprovement of this consensus
docu-ment through collaborative research.
ACKNOWLEDGMENTSThis research was supported in partby the
University of North CarolinaCenter for Education and Research
onTherapeutics (Alan Stiles, MD, princi-pal investigator), funded
by the Agencyfor Healthcare Research and Quality,award 2
U18HS10397-08.
We thank Sara Massie, Sue Tolleson-Rinehart, Jackie MacHardy,
and MollieColeman.
REFERENCES
1. Churg J, Habib R, White RH. Pathology of the nephrotic
syndrome in children: a report for theInternational Study of Kidney
Disease in Children. Lancet. 1970;760(1):12991302
2. The primary nephrotic syndrome in children: identification of
patients with minimal changenephrotic syndrome from initial
response to prednisonea report of the International Study ofKidney
Disease in Children. J Pediatr. 1981;98(4):561564
3. Alternate-day versus intermittent prednisone in frequently
relapsing nephrotic syndrome: a re-port of Arbeitsgemeinschaft fur
Padiatrische Nephrologie. Lancet. 1979;1(8113):401403
4. Short versus standard prednisone therapy for initial
treatment of idiopathic nephrotic syndromein children.
Arbeitsgemeinschaft fur Padiatrische Nephrologie. Lancet.
1988;1(8582):380383
5. Ehrich JH, Brodehl J. Long versus standard prednisone therapy
for initial treatment of idiopathicnephrotic syndrome in children.
Arbeitsgemeinschaft fur Padiatrische Nephrologie. Eur J
Pediatr.1993;152(4):357361
6. Srivastava T, Simon SD, Alon US. High incidence of focal
segmental glomerulosclerosis in ne-phrotic syndrome of childhood.
Pediatr Nephrol. 1999;13(1):1318
7. Lichtig C, Ben-Izhak O, On A, Levy J, Allon U.
Childhoodminimal change disease and focal
segmentalglomerulosclerosis: a continuous spectrum of disease?
Pathologic study of 33 cases with long-term follow-up. Am J
Nephrol. 1991;11(4):325331
8. Harris KM, Gordon-Larsen P, Chantala K, Udry JR. Longitudinal
trends in race/ethnic disparities inleading health indicators from
adolescence to young adulthood. Arch Pediatr Adolesc Med.
2006;160(1):7481
9. Fagot-Campagna A, Pettitt DJ, EngelgauMM, et al. Type 2
diabetes among North American childrenand adolescents: an
epidemiologic review and a public health perspective. J Pediatr.
2000;136(5):664672
10. Gipson DS, MacHardy N, Massengill S, et al. Variability in
childhood onset nephrotic syndromemanagement in North America. 2009
In press
11. Hogg RJ, Furth S, Lemley KV, et al. National Kidney
Foundations Kidney Disease Outcomes QualityInitiative clinical
practice guidelines for chronic kidney disease in children and
adolescents:evaluation, classification, and stratification.
Pediatrics. 2003;111(6 pt 1):14161421
12. Clarkson MR, Meara YM, Murphy B, Rennke HG, Brady HR.
Collapsing glomerulopathy: recurrencein a renal allograft. Nephrol
Dial Transplant. 1998;13(2):503506
13. Niaudet P, GagnadouxMF, BroyerM. Treatment of childhood
steroid-resistant idiopathic nephroticsyndrome. Adv Nephrol Necker
Hosp. 1998;28:4361
14. Bagga A, Hari P, Srivastava RN. Prolonged versus standard
prednisolone therapy for initial epi-sode of nephrotic syndrome.
Pediatr Nephrol. 1999;13(9):824827
15. Hodson EM, Knight JF, Willis NS, Craig JC. Corticosteroid
therapy for nephrotic syndrome inchildren. Cochrane Database Syst
Rev. 2005;(1):CD001533
16. Hiraoka M, Tsukahara H, Matsubara K, et al. A randomized
study of two long-course prednisoloneregimens for nephrotic
syndrome in children. Am J Kidney Dis. 2003;41(6):11551162
17. Ksiazek J, Wyszynska T. Short versus long initial prednisone
treatment in steroid-sensitive ne-phrotic syndrome in children.
Acta Paediatr. 1995;84(8):889893
18. Hoyer PF, Brodehl J. Initial treatment of idiopathic
nephrotic syndrome in children: prednisoneversus prednisone plus
cyclosporine Aa prospective, randomized trial. J Am Soc
Nephrol.2006;17(4):11511157
754 GIPSON et al at Indonesia:AAP Sponsored on February 7,
2015pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
19. Hiraoka M, Tsukahara H, Haruki S, et al. Older boys benefit
from higher initial prednisolonetherapy for nephrotic syndrome.
Kidney Int. 2000;58(3):12471252
20. Nephrotic syndrome in children: a randomized trial comparing
two prednisone regimens insteroid-responsive patients who relapse
earlyreport of the international study of kidney dis-ease in
children. J Pediatr. 1979;95(2):239243
21. Latta K, von S, Ehrich JH. A meta-analysis of cytotoxic
treatment for frequently relapsing nephroticsyndrome in children.
Pediatr Nephrol. 2001;16(3):271282
22. Hogg RJ, Fitzgibbons L, Bruick J, et al. Mycophenolate
mofetil in children with frequently relapsingnephrotic syndrome: a
report from the Southwest Pediatric Nephrology Study Group. Clin J
AmSoc Nephrol. 2006;1(6):11731178
23. Gregory MJ, Smoyer WE, Sedman A, et al. Long-term
cyclosporine therapy for pediatric nephroticsyndrome: a clinical
and histologic analysis. J Am Soc Nephrol. 1996;7(4):543549
24. Kitano Y, Yoshikawa N, Tanaka R, Nakamura H, NinomiyaM, Ito
H. Ciclosporin treatment in childrenwith steroid-dependent
nephrotic syndrome. Pediatr Nephrol. 1990;4(5):474477
25. Abeyagunawardena AS, Dillon MJ, Rees L, vant Hoff W,
Trompeter RS. The use of steroid-sparingagents in steroid-sensitive
nephrotic syndrome. Pediatr Nephrol. 2003;18(9):919924
26. Hulton SA, Jadresic L, Shah V, Trompeter RS, Dillon MJ,
Barratt TM. Effect of cyclosporin A onglomerular filtration rate in
children with minimal change nephrotic syndrome. Pediatr
Nephrol.1994;8(4):404407
27. Wong W. Idiopathic nephrotic syndrome in New Zealand
children, demographic, clinical features,initial management and
outcome after twelve-month follow-up: results of a three-year
nationalsurveillance study. J Paediatr Child Health.
2007;43(5):337341
28. Broyer M, Terzi F, Lehnert A, Gagnadoux MF, Guest G, Niaudet
P. A controlled study of deflazacort inthe treatment of idiopathic
nephrotic syndrome. Pediatr Nephrol. 1997;11(4):418422
29. Fujieda M, Ishihara M, Morita T, et al. Effect of oral
mizoribine pulse therapy for frequentlyrelapsing steroid-dependent
nephrotic syndrome. Clin Nephrol. 2008;69(3):179184
30. Niaudet P. Treatment of childhood steroid-resistant
idiopathic nephrosis with a combination ofcyclosporine and
prednisone. French Society of Pediatric Nephrology. J Pediatr.
1994;125(6 pt 1):981986
31. Gellermann J, Querfeld U. Frequently relapsing nephrotic
syndrome: treatment with mycopheno-late mofetil. Pediatr Nephrol.
2004;19(1):101104
32. Vester U, Kranz B, Zimmermann S, Hoyer PF. Cyclophosphamide
in steroid-sensitive nephroticsyndrome: outcome and outlook.
Pediatr Nephrol. 2003;18(7):661664
33. Gipson DS, Chin H, Presler TP, et al. Differential risk of
remission and ESRD in childhood FSGS.Pediatr Nephrol.
2006;21(3):344349
34. Troyanov S, Wall CA, Miller JA, Scholey JW, Cattran DC.
Focal and segmental glomerulosclerosis:definition and relevance of
a partial remission. J Am Soc Nephrol. 2005;16(4):10611068
35. Prospective, controlled trial of cyclophosphamide therapy in
children with nephrotic syndrome.Report of the International study
of Kidney Disease in Children. Lancet. 1974;2(7878):423427
36. Garin EH, Orak JK, Hiott KL, Sutherland SE. Cyclosporine
therapy for steroid-resistant nephroticsyndrome: a controlled
study. Am J Dis Child. 1988;142(9):985988
37. Hymes LC. Steroid-resistant, cyclosporine-responsive,
relapsing nephrotic syndrome. PediatrNephrol. 1995;9(2):137139
38. Lieberman KV, Tejani A. A randomized double-blind
placebo-controlled trial of cyclosporine insteroid-resistant
idiopathic focal segmental glomerulosclerosis in children. J Am Soc
Nephrol.1996;7(1):5663
39. Ponticelli C, Rizzoni G, Edefonti A, et al. A randomized
trial of cyclosporine in steroid-resistantidiopathic nephrotic
syndrome. Kidney Int. 1993;43(6):13771384
40. Elhence R, Gulati S, Kher V, Gupta A, Sharma RK. Intravenous
pulse cyclophosphamide: a newregime for steroid-resistant minimal
change nephrotic syndrome. Pediatr Nephrol. 1994;8(1):13
41. Tarshish P, Tobin JN, Bernstein J, Edelmann CM.
Cyclophosphamide does not benefit patients withfocal segmental
glomerulosclerosis: a report of the International Study of Kidney
Disease inChildren. Pediatr Nephrol. 1996;10(5):590593
42. Feld SM, Figueroa P, Savin V, et al. Plasmapheresis in the
treatment of steroid-resistant focalsegmental glomerulosclerosis in
native kidneys. Am J Kidney Dis. 1998;32(2):230237
43. Cho ME, Smith DC, Branton MH, Penzak SR, Kopp JB.
Pirfenidone slows renal function decline inpatients with focal
segmental glomerulosclerosis. Clin J Am Soc Nephrol.
2007;2(5):906913
44. Letavernier E, Bruneval P, Mandet C, et al. High sirolimus
levels may induce focal segmentalglomerulosclerosis de novo. Clin J
Am Soc Nephrol. 2007;2(2):326333
SPECIAL ARTICLES
PEDIATRICS Volume 124, Number 2, August 2009 755 at
Indonesia:AAP Sponsored on February 7,
2015pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
45. NakayamaM, Kamei K, Nozu K, et al. Rituximab for refractory
focal segmental glomerulosclerosis.Pediatr Nephrol.
2008;23(3):481485
46. Tahzib M, Frank R, Gauthier B, Valderrama E, Trachtman H.
Vitamin E treatment of focal segmentalglomerulosclerosis: results
of an open-label study. Pediatr Nephrol. 1999;13(8):649652
47. Gansevoort RT, Sluiter WJ, Hemmelder MH, de Zeeuw D, de Jong
PE. Antiproteinuric effect ofblood-pressure-lowering agents: a
meta-analysis of comparative trials. Nephrol Dial
Transplant.1995;10(11):19631974
48. Ellis D, Vats A, Moritz ML, Reitz S, Grosso MJ, Janosky JE.
Long-term antiproteinuric and renopro-tective efficacy and safety
of losartan in children with proteinuria. J Pediatr.
2003;143(1):8997
49. Bagga A, Mudigoudar BD, Hari P, Vasudev V. Enalapril dosage
in steroid-resistant nephroticsyndrome. Pediatr Nephrol.
2004;19(1):4550
50. Yi Z, Li Z, Wu XC, He QN, Dang XQ, He XJ. Effect of
fosinopril in children with steroid-resistantidiopathic nephrotic
syndrome. Pediatr Nephrol. 2006;21(7):967972
51. Wolf G, Ritz E. Combination therapy with ACE inhibitors and
angiotensin II receptor blockers to haltprogression of chronic
renal disease: pathophysiology and indications. Kidney Int.
2005;67(3):799812
52. Hanevold CD. Acute renal failure during lisinopril and
losartan therapy for proteinuria. Pharma-cotherapy.
2006;26(9):13481351
53. Cooper WO, Hernandez-Diaz S, Arbogast PG, et al. Major
congenital malformations after first-trimester exposure to ACE
inhibitors. N Engl J Med. 2006;354(23):24432451
54. National High Blood Pressure Education Program Working Group
on High Blood Pressure inChildren and Adolescents. The fourth
report on the diagnosis, evaluation, and treatment of highblood
pressure in children and adolescents. Pediatrics. 2004;114(2 suppl
4th report):555576
55. Nephrotic syndrome in children: prediction of histopathology
from clinical and laboratory char-acteristics at time of diagnosis:
a report of the International Study of Kidney Disease in
Children.Kidney Int. 1978;13(2):159165
56. Kuster S, Mehls O, Seidel C, Ritz E. Blood pressure in
minimal change and other types of nephroticsyndrome. Am J Nephrol.
1990;10(suppl 1):7680
57. Chiurchiu C, Remuzzi G, Ruggenenti P. Angiotensin-converting
enzyme inhibition and renal protec-tion in nondiabetic patients:
the data of the meta-analyses. J Am Soc Nephrol. 2005;16(suppl
1):S58S63
58. Haws RM, BaumM. Efficacy of albumin and diuretic therapy in
children with nephrotic syndrome.Pediatrics.
1993;91(6):11421146
59. Tanaka R, Yoshikawa N, Kitano Y, Ito H, Nakamura H.
Long-term ciclosporin treatment in childrenwith steroid-dependent
nephrotic syndrome. Pediatr Nephrol. 1993;7(3):249252
60. Donatti TL, Koch VH, Fujimura MD, Okay Y. Growth in
steroid-responsive nephrotic syndrome: astudy of 85 pediatric
patients. Pediatr Nephrol. 2003;18(8):789795
61. Emma F, Sesto A, Rizzoni G. Long-term linear growth of
children with severe steroid-responsivenephrotic syndrome. Pediatr
Nephrol. 2003;18(8):783788
62. Hegarty J, Mughal MZ, Adams J, Webb NJ. Reduced bone mineral
density in adults treated withhigh-dose corticosteroids for
childhood nephrotic syndrome. Kidney Int. 2005;68(5):23042309
63. Ruth EM, KemperMJ, Leumann EP, Laube GF, Neuhaus TJ.
Childrenwith steroid-sensitive nephroticsyndrome come of age:
long-term outcome. J Pediatr. 2005;147(2):202207
64. Berns JS, Gaudio KM, Krassner LS, et al. Steroid-responsive
nephrotic syndrome of childhood: along-term study of clinical
course, histopathology, efficacy of cyclophosphamide therapy,
andeffects on growth. Am J Kidney Dis. 1987;9(2):108114
65. Elzouki AY, Jaiswal OP. Long-term, small dose prednisone
therapy in frequently relapsing ne-phrotic syndrome of childhood:
effect on remission, statural growth, obesity, and infection
rate.Clin Pediatr (Phila). 1988;27(8):387392
66. Foster BJ, Shults J, Zemel BS, Leonard MB. Risk factors for
glucocorticoid-induced obesity inchildren with steroid-sensitive
nephrotic syndrome. Pediatr Nephrol. 2006;21(7):973980
67. Merritt RJ, Hack SL, Kalsch M, Olson D. Corticosteroid
therapy-induced obesity in children. ClinPediatr (Phila).
1986;25(3):149152
68. Lechner BL, Bockenhauer D, Iragorri S, Kennedy TL, Siegel
NJ. The risk of cardiovascular diseasein adults who have had
childhood nephrotic syndrome. Pediatr Nephrol.
2004;19(7):744748
69. Olbricht CJ, Wanner C, Thiery J, Basten A. Simvastatin in
nephrotic syndrome. Simvastatin inNephrotic Syndrome Study Group.
Kidney Int Suppl. 1999;71:S113S116
70. Valdivielso P, Moliz M, Valera A, Corrales MA,
Sanchez-Chaparro MA, Gonzalez-Santos P. Atorvasta-tin in
dyslipidaemia of the nephrotic syndrome. Nephrology (Carlton).
2003;8(2):6164
756 GIPSON et al at Indonesia:AAP Sponsored on February 7,
2015pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
71. Holmes KW, Kwiterovich PO Jr. Treatment of dyslipidemia in
children and adolescents. CurrCardiol Rep. 2005;7(6):445456
72. Tain YL, Lin G, Cher TW. Microbiological spectrum of
septicemia and peritonitis in nephroticchildren. Pediatr Nephrol.
1999;13(9):835837
73. Krensky AM, Ingelfinger JR, Grupe WE. Peritonitis in
childhood nephrotic syndrome: 19701980.Am J Dis Child.
1982;136(8):732736
74. Hingorani SR, Weiss NS, Watkins SL. Predictors of
peritonitis in children with nephrotic syndrome.Pediatr Nephrol.
2002;17(8):678682
75. Gorensek MJ, Lebel MH, Nelson JD. Peritonitis in children
with nephrotic syndrome. Pediatrics.1988;81(6):849856
76. Matsell DG, Wyatt RJ. The role of I and B in peritonitis
associated with the nephrotic syndrome ofchildhood. Pediatr Res.
1993;34(1):8488
77. Milner LS, Berkowitz FE, Ngwenya E, Kala U, Jacobs D.
Penicillin resistant pneumococcal peritonitisin nephrotic syndrome.
Arch Dis Child. 1987;62(9):964965
78. McIntyre P, Craig JC. Prevention of serious bacterial
infection in children with nephrotic syn-drome. J Paediatr Child
Health. 1998;34(4):314317
79. Mehls O, Andrassy K, Koderisch J, Herzog U, Ritz E.
Hemostasis and thromboembolism in childrenwith nephrotic syndrome:
differences from adults. J Pediatr. 1987;110(6):862867
80. Citak A, Emre S, Sairin A, Bilge I, Nayir A. Hemostatic
problems and thromboembolic complicationsin nephrotic children.
Pediatr Nephrol. 2000;14(2):138142
81. Lilova MI, Velkovski IG, Topalov IB. Thromboembolic
complications in children with nephroticsyndrome in Bulgaria
(19741996). Pediatr Nephrol. 2000;15(12):7478
82. Zwaginga JJ, Koomans HA, Sixma JJ, Rabelink TJ. Thrombus
formation and platelet-vessel wallinteraction in the nephrotic
syndrome under flow conditions. J Clin Invest.
1994;93(1):204211
83. Deshpande PV, Griffiths M. Pulmonary thrombosis in
steroid-sensitive nephrotic syndrome.Pediatr Nephrol.
2005;20(5):665669
84. Gangakhedkar A, Wong W, Pitcher LA. Cerebral thrombosis in
childhood nephrosis. J PaediatrChild Health. 2005;41(4):221224
85. Papachristou FT, Petridou SH, Printza NG, Zafeiriou DI,
Gompakis NP. Superior sagittal sinusthrombosis in steroid-resistant
nephrotic syndrome. Pediatr Neurol. 2005;32(4):282284
86. Jones CL, Hebert D. Pulmonary thrombo-embolism in the
nephrotic syndrome. Pediatr Nephrol.1991;5(1):5658
87. Share A, Uzun O, Blackburn ME, Gibbs JL. Prolonged local
infusion of streptokinase in pulmonaryartery thrombosis with
nephrotic syndrome. Pediatr Nephrol. 1996;10(6):734736
88. AndrewM, Michelson AD, Bovill E, Leaker M, Massicotte MP.
Guidelines for antithrombotic therapyin pediatric patients. J
Pediatr. 1998;132(4):575588
89. Dowell SF, Bresee JS. Severe varicella associated with
steroid use. Pediatrics. 1993;92(2):223228
90. Quien RM, Kaiser BA, Deforest A, Polinsky MS, Fisher M,
Baluarte HJ. Response to the varicellavaccine in children with
nephrotic syndrome. J Pediatr. 1997;131(5):688690
91. Alpay H, Yildiz N, Onar A, Temizer H, Ozcay S. Varicella
vaccination in children with steroid-sensitivenephrotic syndrome.
Pediatr Nephrol. 2002;17(3):181183
92. Furth SL, Arbus GS, Hogg R, Tarver J, Chan C, Fivush BA.
Varicella vaccination in children withnephrotic syndrome: a report
of the Southwest Pediatric Nephrology Study Group. J
Pediatr.2003;142(2):145148
93. American Academy of Pediatrics. Active and passive
immunization. In: Pickering LK, Baker CJ,Long SS, McMillan JA, eds.
Red Book. 27th ed. Elk Grove Village: American Academy of
Pediatrics.2006:940
SPECIAL ARTICLES
PEDIATRICS Volume 124, Number 2, August 2009 757 at
Indonesia:AAP Sponsored on February 7,
2015pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
DOI: 10.1542/peds.2008-1559; originally published online July
27, 2009; 2009;124;747Pediatrics
Howard Trachtman and Larry A. GreenbaumSmoyer, John D. Mahan,
Delbert Wigfall, Paul Miles, Leslie Powell, Jen-Jar Lin, Debbie S.
Gipson, Susan F. Massengill, Lynne Yao, Shashi Nagaraj, William
E.
Management of Childhood Onset Nephrotic Syndrome
ServicesUpdated Information &
mlhttp://pediatrics.aappublications.org/content/124/2/747.full.htincluding
high resolution figures, can be found at:
References
ml#ref-list-1http://pediatrics.aappublications.org/content/124/2/747.full.htat:This
article cites 91 articles, 17 of which can be accessed free
Citations
ml#related-urlshttp://pediatrics.aappublications.org/content/124/2/747.full.htThis
article has been cited by 13 HighWire-hosted articles:
Subspecialty Collections
ary_disorders_subhttp://pediatrics.aappublications.org/cgi/collection/genitourinGenitourinary
Disorders
bhttp://pediatrics.aappublications.org/cgi/collection/urology_suUrology
y_subhttp://pediatrics.aappublications.org/cgi/collection/nephrologNephrologythe
following collection(s):This article, along with others on similar
topics, appears in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables)
or in its entirety can be found online at: Information about
reproducing this article in parts (figures,
Reprints
http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN:
1098-4275.Grove Village, Illinois, 60007. Copyright 2009 by the
American Academy of Pediatrics. All and trademarked by the American
Academy of Pediatrics, 141 Northwest Point Boulevard,
Elkpublication, it has been published continuously since 1948.
PEDIATRICS is owned, published, PEDIATRICS is the official journal
of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on February 7,
2015pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/content/124/2/747.full.htmlhttp://pediatrics.aappublications.org/content/124/2/747.full.htmlhttp://pediatrics.aappublications.org/content/124/2/747.full.html#ref-list-1http://pediatrics.aappublications.org/content/124/2/747.full.html#ref-list-1http://pediatrics.aappublications.org/content/124/2/747.full.html#related-urlshttp://pediatrics.aappublications.org/content/124/2/747.full.html#related-urlshttp://pediatrics.aappublications.org/cgi/collection/nephrology_subhttp://pediatrics.aappublications.org/cgi/collection/nephrology_subhttp://pediatrics.aappublications.org/cgi/collection/urology_subhttp://pediatrics.aappublications.org/cgi/collection/urology_subhttp://pediatrics.aappublications.org/cgi/collection/genitourinary_disorders_subhttp://pediatrics.aappublications.org/cgi/collection/genitourinary_disorders_subhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/
-
DOI: 10.1542/peds.2008-1559; originally published online July
27, 2009; 2009;124;747Pediatrics
Howard Trachtman and Larry A. GreenbaumSmoyer, John D. Mahan,
Delbert Wigfall, Paul Miles, Leslie Powell, Jen-Jar Lin, Debbie S.
Gipson, Susan F. Massengill, Lynne Yao, Shashi Nagaraj, William
E.
Management of Childhood Onset Nephrotic Syndrome
http://pediatrics.aappublications.org/content/124/2/747.full.html
located on the World Wide Web at: The online version of this
article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005.
Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois,
60007. Copyright 2009 by the American Academy published, and
trademarked by the American Academy of Pediatrics, 141 Northwest
Pointpublication, it has been published continuously since 1948.
PEDIATRICS is owned, PEDIATRICS is the official journal of the
American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on February 7,
2015pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/content/124/2/747.full.htmlhttp://pediatrics.aappublications.org/