Embed Size (px)
Citation preview
Objective
In Japan, laparoscopic inguinal herniorrhaphy(LH) is not popular. We performed a retrospective study to evaluate the results of LH in our hospital.
Patients
Between August 1992 and February 2008, 286 patients with 315 hernias were operated on at our department.
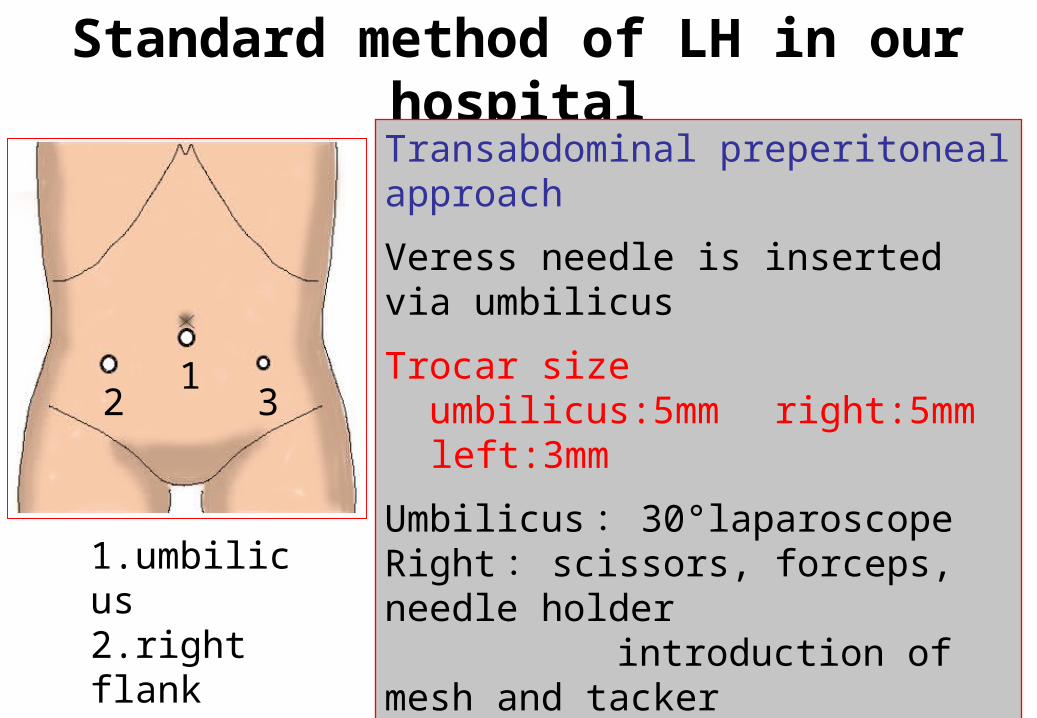
Standard method of LH in our hospitalTransabdominal preperitoneal approach
Veress needle is inserted via umbilicus
Trocar size umbilicus:5mm right:5mm left:3mm
Umbilicus : 30°laparoscopeRight : scissors, forceps, needle holder introduction of mesh and tackerLeft : forceps
Mesh : polyester or polypropylene soft ( average size:14×9cm )
1.umbilicus2.right flank3.left flank
12 3
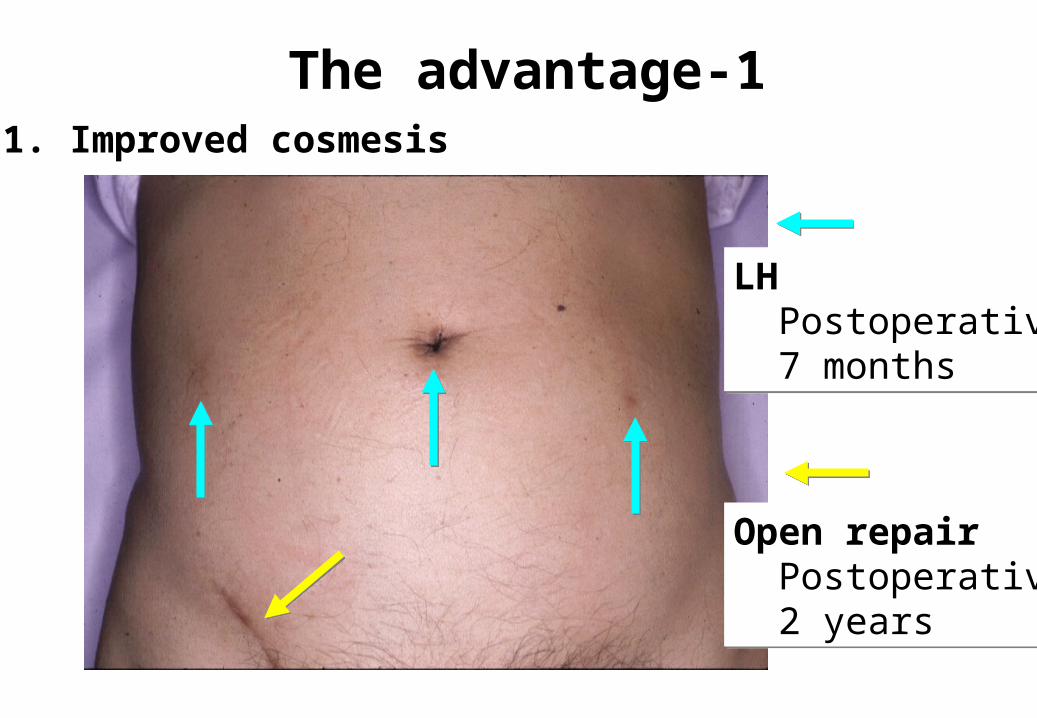
The advantage-11. Improved cosmesis
LH Postoperative 7 months
LH Postoperative 7 months
Open repair Postoperative 2 years
Open repair Postoperative 2 years
The advantage-22. Less postoperative pain Earlier return to normal activity Less chronic postoperative pain
《 meta-analysis of randomized control trial 》
・ less postoperative pain, more rapid return to normal activity The EU Hernia Trialists Collaboration: Br J Surg 87:860-867, 2000
・ less persisting pain The EU Hernia Trialists Collaboration: Ann Surg 23:322-332, 2002
・ lower incidence of chronic pain Schmedt CG, et al: Surg Endosc 19:188-199, 2005
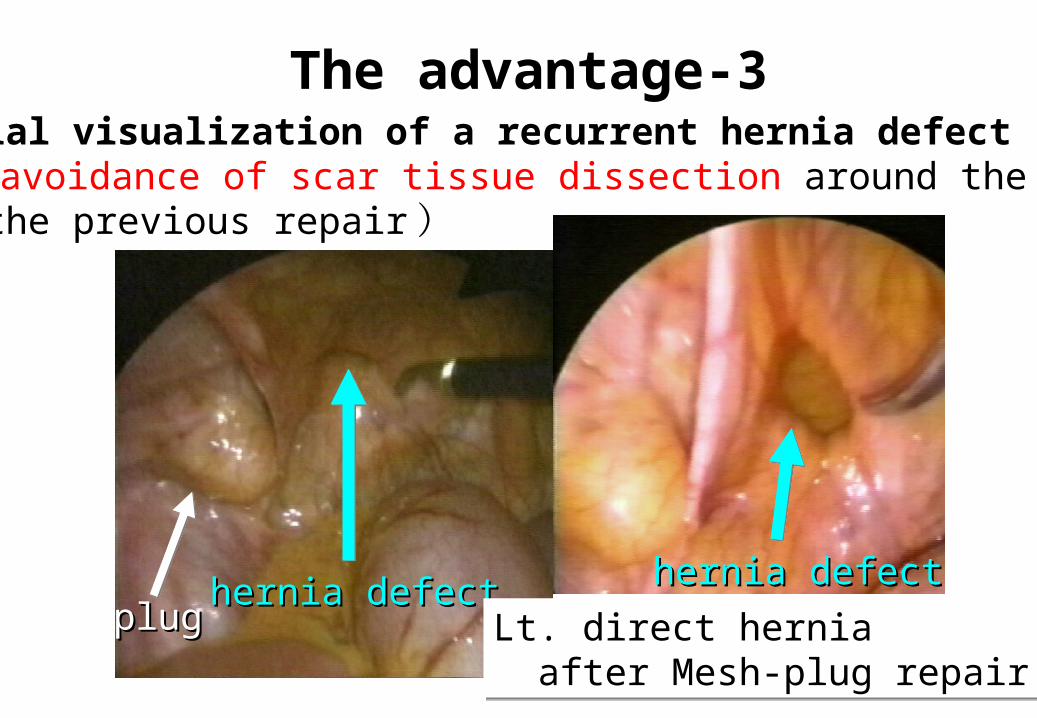
The advantage-33. Initial visualization of a recurrent hernia defect ( the avoidance of scar tissue dissection around the area of the previous repair )
plugplughernia defecthernia defect hernia defecthernia defect
Lt. direct hernia after Mesh-plug repairLt. direct hernia after Mesh-plug repair
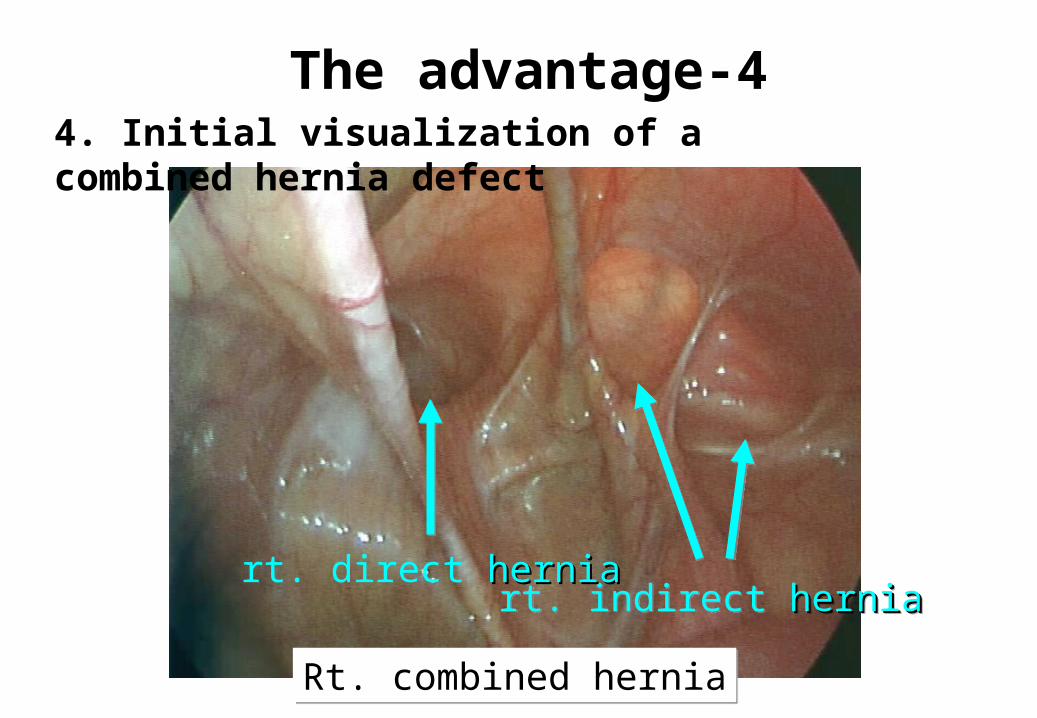
The advantage-44. Initial visualization of a combined hernia defect
Rt. combined herniaRt. combined hernia
rt. indirect herniaherniart. indirect herniaherniart. direct herniahernia
The advantage-55. No additional incision to treat bilateral hernias
《 prospective randomized controlled clinical study 》
With relation to open tension-free repair
・ higher cost
・ less postoperative pain
・ earlier return to work
Sarli L.et al.: Surg Laparosc Endosc Percutan Tech 11:262-267, 2001
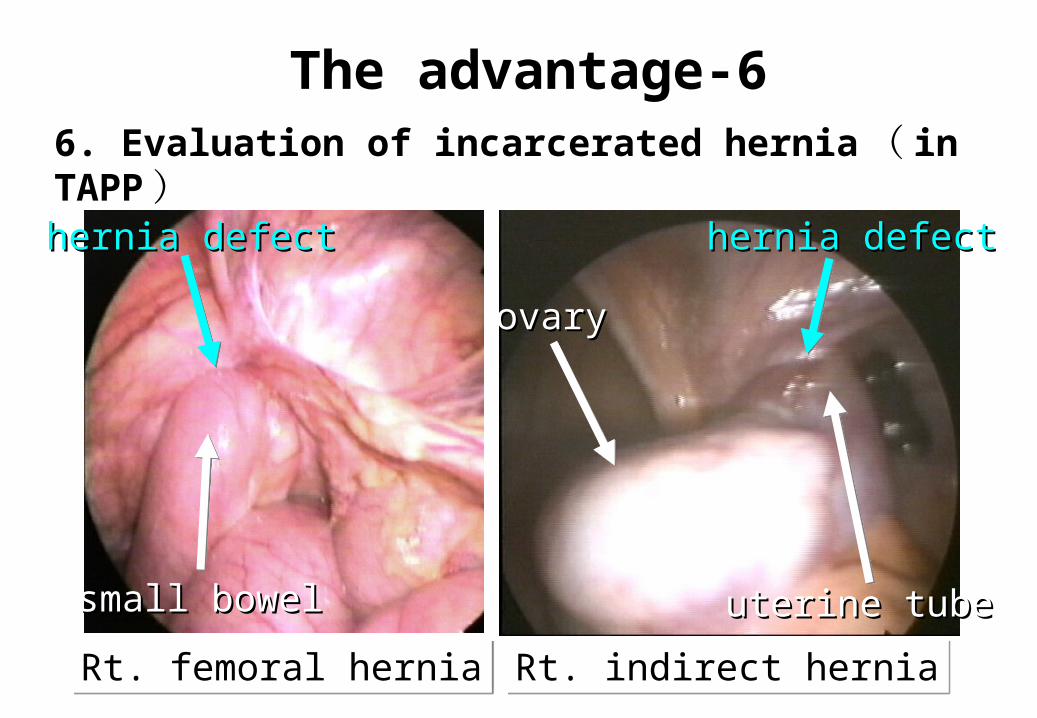
The advantage-66. Evaluation of incarcerated hernia ( in TAPP )
hernia defecthernia defect
small bowelsmall bowel
hernia defecthernia defect
uterine tubeuterine tube
ovaryovary
Rt. indirect herniaRt. indirect herniaRt. femoral herniaRt. femoral hernia
The advantage-77. Diagnosis of unsuspected contralateral hernia ( in TAPP )
※In our practice, it is 3.8% ( 11/286 ) .
・ The reported laparoscopically detected incidence of occult contralateral hernias is between 11.2% and 50%. Koehler RH.: Surg Endosc 16:512-520, 2002
The disadvantage-11. Increased operative cost ( general anesthesia, equipment )
But
・ The total cost for working patients are lower with the laparoscopic technique, when the cost of lost work days is factored into overall expense. Heikkinen T. et al: Surg Endosc 12:1199-1203, 1998
・ From a societal perspective, laparoscopic approach can be a cost-effective treatment option for inguinal hernia repair. Stylopoulos N. et al: Surg Endosc 17:180-189, 2003
The disadvantage-2
2. Specific training and long learning curve
Learning curve is
・ 30–50 cases DeTurris SV. et al: J Am Coll Surg 194:65-73,
2002
・ 40 procedures Lim M. et al: Surg Endosc 20:1453-1459, 2006
※ Some authors have quantified the LH learning curve at 30–250 hernia repairs.
The disadvantage-3
3. Major complications and recurrences during the learning curve
※We experienced two severe complications. ( one bladder injury and one trocar site hernia )
〔 Reported serious complications 〕 ・ visceral injury (bladder, intestine, etc. ) ・ vascular injury ( iliac artery, etc. ) ・ trocar site hernia ・ bowel obstruction ・ testicular ischemia ・ nerve injury ( genitofemoral nerve, etc. )
Conclusions
1. Laparoscopic herniorrhaphy has many advantages for both experienced surgeons and patients.
2. The widespread adoption of laparoscopic herniorrhaphy needs cost saving and surgeon’s technical skill.