Embed Size (px)
Citation preview

�
CLINICAL REPORT
Ocular Pterygium—Digital Keloid Dysplasia
Hugo Abarca,1y Anne E Christensen Mellgren,2,3y Milana Trubnykova,1 Olav H. Haugen,2,3Gunnar Høvding,2,3 Kare Steinar Tveit,4 Gunnar Houge,3,5 Cecilie Bredrup,2,5
and Raoul C Hennekam6*1Instituto Nacional de Salud del Nino, Lima, Peru2Department of Ophthalmology, Haukeland University Hospital, Bergen, Norway3Department of Clinical Medicine, University of Bergen, Bergen, Norway4Department of Dermatology, Haukeland University Hospital, Bergen, Norway5Center for Medical Genetics and Molecular Medicine, Haukeland University Hospital, Bergen, Norway6Department of Pediatrics, Emma Children’s Hospital and Department of Clinical Genetics, Academic Medical Center,
University of Amsterdam, Amsterdam, Netherlands
Manuscript Received: 3 March 2014; Manuscript Accepted: 3 July 2014
How to Cite this Article:Abarca H, Mellgren AEC, Trubnykova M,
Haugen OH, Høvding G, Tveit KS, Houge
G, Bredrup C, Hennekam RC. 2014. Ocular
pterygium—digital keloid dysplasia.
Am J Med Genet Part A 164A:2901–2907.
We describe an adolescent Peruvian male with marked, aggres-
sive ingrowth of conjunctiva (pterygium-like) over the cornea
associated with keloid formation on his distal limbs. He has in
addition camptodactyly of all fingers and to some extent of his
toes, and unusual skin pigmentations. He resembles an earlier
described family from Norway in which a mother and two
children showed a similar combination of signs. We present
the follow-up of the Norwegian family. The entity resembles the
Penttinen syndrome but can be differentiated due to the early
aging in the latter, which is lacking in the presently reported
entity. We suggest naming this entity ocular pterygium–digital
keloid dysplasia. The condition follows likely an autosomal
dominant pattern of inheritance. � 2014 Wiley Periodicals, Inc.
Key words: keloid; childhood ocular pterygium; camptodactyly;
autosomal dominant
Conflict of interest: NoneyHugo Abarca and Anne E Christensen Mellgren have contributed
equally to the manuscript.
Grant sponsor: Western Norway Regional Health Authority; Grant
numbers: 911466, 911688.�Correspondence to:
Dr Raoul C Hennekam, Department of Pediatrics, Room 7-236, AMC,
Meibergdreef 9, 1105AZ Amsterdam. E-mail [email protected]
Article first published online in Wiley Online Library
(wileyonlinelibrary.com): 14 August 2014
DOI 10.1002/ajmg.a.36713
INTRODUCTION
Keloid formation can be defined as increased scar tissue formation
not being in accordance to the trauma.Keloidsmay impair function
by restriction of the skin and decrease of joint mobility, can be
aesthetically disfiguring, and may cause intense symptomatic dis-
tress due to the itching and pain, which often accompanies keloids.
Keloids do not occur frequently in syndromes and if they occur
together with other manifestations, they are located at upper
thorax, shoulders and upper arms, which are also the predilection
sites of isolated keloids.
In 1998 Haugen and Bertelsen [1998] reported on a mother and
two sons with ingrowth of conjunctival tissue that gradually
covered the whole cornea and progressive keloid formation in their
hands and fingers. A single family with possibly the same entity has
been reported since [Balaji et al., 1991; Booth andHodgkins, 2006].
Here we report on a patient from a second family with very similar
findings, and provide an update on the family reported by Haugen
2014 Wiley Periodicals, Inc.
and Bertelsen. We suggest naming this entity ocular pterygium-
digital keloid dysplasia.
CLINICAL REPORT
The proband was the fifth child of nonconsanguineous Peruvian
parents. There are several persons in the familywithocular pterygia:
the parents of the proband are both construction workers. Father
developed pterygia from the age of 30 years and mother had minor
pterygia from the age of about 20 years. Neither has undergone
surgery.Mother has one brother who underwent successful surgery
for his pterygia. There are noother known eye diseases in the family,
and no one is known to have keloid formation.
Theproband is thefifth child of these parents. Their first children
were twins born at 8months weighing 2700 g. Both died in infancy,
2901

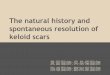
FIG. 1. Face of the proband. Note the narrow nasal bridge and
prominent nose.
2902 AMERICAN JOURNAL OF MEDICAL GENETICS PART A
one due to an infection, and the other of unknown reasons. Their
next son died in infancy because of an infection as well. Mother
subsequently gave birth to a healthy daughter who never developed
problems similar to the proband. All children were born by
caesarean section. Because of this obstetric history the pregnancy
of theprobandwas endedby caesarean at 34weeks. Birthweightwas
2500 g and lengthwas stated tohavebeennormal.He received “light
therapy” at home for 4 weeks because of prolonged hyperbiliru-
binaemia. His psychomotor development was normal; he could sit
at 6months, andwalk at 16months.His initial speech development
was somewhat slow (first words at 2 years) but subsequently his
cognitive development was completely normal.
Since childhood he complained of early fatigability, which
persisted into adulthood. Cardiac examination showed normal
cardiac anatomy and function. He was found to have ingrown
toenails which were surgically corrected, after which keloid forma-
tion started at his toes.Non-operated toes developedkeloids aswell,
which was possibly related to nail bed irritation, and he had also a
skin lesion on his right sole. The keloids increased with time, and
after a biopsy was taken rapid growth was noted. He had congenital
mildly decreasedmobility of his fingers, showing in only faint distal
flexion creases of all fingers, but initially no keloid formation at his
hands.Radiological studies failed to showbony abnormalities of the
hands. At 5 years reduced vision was first noticed. At 7 years, an
aggressive pterygium was diagnosed on the right eye, starting from
the nasal side and spreading over the cornea. A year later a similar
pterygium was noticed on the left eye. At 9 years, he underwent
pterygium excision in both eyes, in the left eye Mitomycin C was
applied, but the pterygia recurred. Repeated surgery on the right eye
was performed but without success. Subsequently, he developed a
right-sided symblepharon. At 18 years a keratoprosthesis was
implanted in the right eye, with initial success and regain of
some visual acuity, but subsequent loss of vision due to dislocation
of the keratoprosthesis to the interior of the eye. He has subse-
quently developed phthisis in the right eye, and has visual acuity of
light perception only. In the left eye visual acuity was 0.2 (Snellen)
despite recurrence of the pterygium. The temporal part of the
cornea of the left eye is still clear (Fig. 3).
The probanddeveloped around15 years of age darkly pigmented
skin lesions on trunk and limbs, which sometimes were confluent
but sometimes also disappeared. Clinically the skin changes resem-
bled brown angiokeratomas. At that time hammertoes developed,
especially of the right 2nd, 3rd, and 4th toe. The camptodactyly had
gradually increased and he developed two small keloids, both after
trauma, on a middle finger. At age 19 years he was diagnosed
with photosensitive dermatitis in his face needing treatment
(methotrexate).
On examination at age 19 years the proband was a normally
intelligent adolescent, height 167 cm(10th centile) andweight 60 kg
(30th centile), and head circumference 57.0 cm (50th centile). He
had normal hair, an irregularly formed right eyebrow and blephar-
ophimosis, interpreted to be secondary to the earlier surgery
(Fig. 1). There were tongues of conjunctival tissue invading the
cornea in both eyes, in the right eye covering the whole cornea
(Fig. 2), narrow nasal bridge, prominent nose, normal teeth,
somewhat high palate, and pits of the posterior helices. He had a
normal trunk with mildly increased fat deposits, a thoracic kypho-
sis, and normalmale genitalia. Therewasmild hyperhidrosis of face
and trunk.Mobility in shoulders and elbowswasnormal, andhands
showed camptodactyly of all fingers. There were small keloids on
the middle finger (Fig. 3a). There were only faint flexion creases
visible over the distal interphalangeal joints. Mobility in hips and
knees was normal. He had hammertoes, more marked on the right
side, shortened distal phalanges of the halluces, and bluish discol-
ored keloid tissue on the dorsum of both halluces with some
spreading to the dorsum of the feet (Fig. 3b).
UPDATE OF HAUGEN AND BERTELSEN REPORT
The family consists of an affected mother (proband) and two
affected sons. The parents of the proband had reportedly normal
eyes and no keloids. At 2 years ingrowth of scar tissue was observed
in both eyes of the proband. Despite surgery the ingrowth pro-
gressed and became confluent when she was 8 years of age. From
20 years on she developed keloid-like scars on the flexor side of the
fingers causing flexion contractures (Fig. 4a). In her sixties she quite
abruptly developed large granuloma-annulare-like eczemas on the
posterior aspect of both upper arms. In one of these lesions a
sarcoma developed that was successfully treated. The number of
cutaneous fibromas increased over the years, especially on the
central face, trunk, and extremities. At 73 years she developed an
adenocarcinoma of the endometrium, and she died at age 75 years.
The oldest son of the proband presented with progressive,
superficial grayish corneal opacities in the left eye at 1 year of
age and in the right eye at 2 years. At 3 years multiple tongue-like
ingrowths approached the center of the corneas (Fig. 4b). Surgical
interventions in the right eye were unsuccessful. In his second
decade he developed multiple broad-based fibromas on his trunk
and neck. At 21 years he developed keloids on his fingers but these
were less pronounced compared to those in hismother and brother.
At 35 years keloids developed on his halluces (Fig. 4a).
The youngest son of the probandhadnormal eyes until the age of
six when thin, grey-white tissue became apparent at the upper
temporal limbal region of the right eye. The changes progressed
slowly and at 18 years of age covered the whole cornea. The left eye

FIG. 2. Eyes of the proband at 19 year of age. Note phthisic right eye (axial length 16mm), extensive scarring due to conjunctival ingrowth
over the cornea and previous surgery. The symblepharon of the lower eyelid is secondary to surgery. The left eye (23mm) shows conjunctival
ingrowth nasally and superiorly; the temporal part is relatively spared.
FIG. 3. a. Right hand of the proband and detail of left middle finger. Note the camptodactyly and only faint distal interphalangeal flexion
creases. The left middle finger has two small keloids both as results of minor trauma. Fig. 3b. Feet of the proband. Note extensive keloid
formation. The keloids on both halluces appeared after surgery for ingrown nails. The keloids on the other toes apparently developed
spontaneously.
ABARCA ET AL. 2903

FIG. 4. a. Distal limbs of family reported by Haugen and Bertelsen [1998]. Left panel: Large keloids on the fingers of the proband (mother)
causing syndactyly and restricted movements of especially the index and middle finger, and extending from the back of the fingers to the
distal back of the hands. Middle panel: Keloids on the plantar side of the halluces of the eldest son. Right panel: Keloids on the right hand of
the youngest son, ending just proximal to the nail bed. Fig. 4b. Eyes of family members reported by Haugen and Bertelsen [1998]. Left panel:
The un-operated left eye of the eldest son, showing vascularized tissue covering the cornea completely. Right panel: The left eye of the
youngest son showing conjunctival ingrowth on the cornea resembling pterygium.
2904 AMERICAN JOURNAL OF MEDICAL GENETICS PART A
was unaffected until the age of 20, when similar changes appeared,
and in less than four years the optic axis was covered (Fig. 4b). At
15 years slowly progressive and bilaterally symmetric keloids de-
veloped on the third, fourth, and fifth fingers covering the dorsal
and lateral aspect of thedistal phalanges (Fig. 4a).At 28years keloids
arose on the plantar side of both halluces. In addition he developed
erythema in the face, and multiple fibromas in his face, neck,
shoulders, and back.
DISCUSSION
We report on a single individual who has aggressive, early ocular
pterygium-like formation with an unusual progression and lack of
response to treatment. In addition he has early onset keloid
formation on all distal limbs. These manifestations resemble the
manifestations described in the three members of a Norwegian
family to a great extent (Table I). The present proband showed
camptodactyly of hands and feet from early on. Marked campto-
dactyly of hands were seen in the proband of the Norwegian family,
but this was secondary to the extensive keloid formation on the
ventral side of her fingers. The present proband has an increased
thoracic kyphosis and truncal fat deposits, which were not evident
in the Norwegian family. As the major findings in the proband are
very similar to the findings in the family described by Haugen and
Bertelsen, it seems likely they have the same entity. We suggest
naming the entity ocular pterygium – digital keloid dysplasia, as
there are ocular pterygia, keloids on the digits, and the early onset,
the continuousprogressionduring life andhistological findingsfit a
dysplasia.
Booth and Hodgkins [2006] provided an update of a family
reported earlier on by Balaji and colleagues [1991]. In the first
report the family was reported to have Ebstein anomaly (displace-
ment of the septal and posterior tricuspid valve leaflets) and
restricted finger and toemovements [Balaji et al., 1991]. The update
described that one member had ingrowth of fibrous tissue in the
cornea on one side andmultiple keloids on trunk and limbs [Booth
and Hodgkins, 2006]. It was stated that by history several other
family members had multiple keloids as well. It remains uncertain
whether this family has ocular pterygium-digital dysplasia, due to
the presence of eye manifestations in only one of multiple affected
members, presence of keloids also on the trunk, and presence of
Ebstein anomaly.
A pterygium is a common fibrovascular dysplasia affecting the
bulbar conjunctiva, more frequently located on the nasal than
temporal limbus. In addition to discomfort it can give rise to visual
problems if it crosses the pupillary axis. In peri-equatorial countries
and in high altitude regions a high incidence of pterygia is seen.
Pterygia are assumed to be caused by high exposure to ultraviolet
light. Additional risk factors include family history, increasing age,
andmale gender. Certain groups, such as outdoor workers, have an

TABLE I. Main Characteristics in the Present Proband Compared to The Updated Findings Reported by Haugen and Bertelsen [1998]and to Penttinen Syndrome.
Proband
Haugen and Bertelsen, 1998 Penttinen syndromea
P1 (Mother) P2 (son) P3 (son) P1 P2 P3Cognition Nl Nl Nl Nl Nl Nl NlGrowth (centile) 167 cm
(P10)175 cm(P90)
170 cm(P15)
173 cm(P25)
P50–75 >3SD 3SD
Ocular pterygia bilat bilat bilat bilat � bilat bilatAge diagnosis 7yr 2yr 1yr 6yr 9yr 9yrProgression þþ þþ þþ þþ ? ?Age 1st surgery 9yr 4yr 3yr 23yr ? ?
Keloid (age) 4yr 20yr 22yr 15yr 2yr (3yr)Hands þ þþ þ þ þ þ �Feet þþ - þ þ þ þOther � right arm � � elbows, knees buttocks
Thin, translucent skin � � � � þ þ þAbnormal skin pigmentation þ � þ þ � � �Abnormal hair pigmentation � � � � þ ? ?Acro-osteolysis � � � � þ þ þShort, broad digits � � � � þ þ þCamptodactyly
Fingers þ þþ � � þþ þþ þþToes þ � � � � � �
FaceHair nl nl nl nl sparse sparse sparseNasal bridge narrow � � � broad � �(Pre)maxilla nl � � � retracted retracted retractedNose prominent � � � � � �Thin upper Vermilion � � � � þ þ þ
Hyperkyphosis þ � � � � þ þLipodystrophy (trunkal fat
deposits)� � � þ þ þ
Other � multiplefibromas
multiplefibromas
multiplefibromas
bifid uvulacorneal clouding
widefontanel
craniosynostosisEpilepsy VSD
aP1: Penttinen et al., 1997; P2 and P3: Zufferey et al., 2012.
ABARCA ET AL. 2905
increased incidence to develop pterygia [Liu et al., 2013]. The
prevalence of pterygium in Peru has been described as high as
31%. However, in less than 1% of the cases the pterygium extended
more than halfway to the center of the cornea and no patients below
20 years of age were described [Rojas and Malaga, 1986]. Since the
family of the proband has several risk factors for developing
pterygium (they live at a high altitude and are outdoor workers),
pterygium development is not unexpected in early adulthood,
which is the case in the affected familymembers except theproband.
In addition, the natural history in the other family members is as
expected for normal pterygiumdevelopment anddifferent from the
course in the proband. Therefore it is unlikely that pterygium
development in familymembers is causally related to the aggressive
conjunctival ingrowth seen in the proband. Pterygium formation in
children is rare and can in most cases be managed conservatively
[Monga et al., 2012].One family inwhich aggressive pterygiumwas
present in three second degree family members, of which two
developed ocular changes in childhood (at 6 and 4 years, respec-
tively) has been described. No extraocular signs or symptoms were
reported, in particular not with respect to the skin [Islam and
Wagoner, 2001].
Another main finding in the present patient is the keloid
formation at the distal limbs. There are only a limited number
ofMendelian entities that go along with keloid formation. Some of
the connective tissue disorders such as Ehlers-Danlos syndrome
type IV [Burk et al., 2007] and lateralmeningocele syndrome [Chen
et al., 2005] can show keloid formation. Goeminne syndrome is
characterized by a progressive torticollis, kyphosis, pectus forma-
tion, umbilical herniae, varicose veins, normal intelligence, and
keloids on trunk and limbs, including hands [Fryns and
Gevers, 2003], and this condition may in fact also be a connective
tissue disorder. One of us (RCH) has seen severalmales and females

2906 AMERICAN JOURNAL OF MEDICAL GENETICS PART A
with a phenotype that resembles frontometaphyseal dysplasia but
without detectable Filamin A mutations, who had numerous
rounded keloidswidely spreadover their body. Themost frequently
occurring syndrome that goes along with keloid formation in a
significant percentage of patients is Rubinstein-Taybi syndrome
[Hennekam, 2006]. A recent study showed that 24% of all Rubin-
stein-Taybi patients develop keloids [Van de Kar et al., in press].
Keloids in this entity are located on upper thorax, shoulders and
upper arms, and rarely elsewhere.Myhre syndrome is characterized
by intellectual disability, short stature with a stocky body build,
hearing loss, an unusual face, and keloids can occur in the upper
airways (nose; larynx) [McGowanet al., 2011]. Inoculo-ectodermal
syndrome macrocephaly, areas of aplasia cutis of the scalp, epi-
bulbar dermoids, and areas of hyperpigmentation of the skin can go
along with keloid formation as well [Evers et al., 1994]. Several
families have been described with a phenotype that resembles
Bardet-Biedl syndrome without the distal limb anomalies but
with deafness, cataract, and keloid formation as additional man-
ifestations [Boor et al., 1993]. Heyen and co-workers reported on
several individuals from a single family who had a large optic cup-
to-disc ratio, camptodactyly and keloid formation on trunk or
proximal limbs [Heyen et al., 2008]. Finally, keloid formation has
rarely been described in chromosome imbalances such as Turner
syndrome and deletions of the terminal part of chromosome 19p
[Archer et al., 2005], and in a small number of case reports [Leung
et al., 1988;Coffin, 1990;Anandan et al., 2008]. In noneof the above
entities progressive conjunctival ingrowth on the cornea was seen,
and only very infrequently keloids develop on their hands and feet.
There is a single entity in which ocular pterygia have been reported
together with keloids on the distal limbs, i.e. Penttinen syndrome
[Penttinen et al., 1997; Zufferey et al., 2012]. The three patients
reportedwith this entitymayhaveocular pterygia that arise at a very
young age as in ocular pterygium-digital keloid dysplasia, and may
also have keloid formation on the back of the hands and feet
(Table I). However, in Penttinen syndrome the affected individuals
may show somatic overgrowth, facial characteristics (sparse hair,
retracted maxilla and pre-maxilla, and thin upper vermillion), an
unusual thin and translucent skin, progressive acro-osteolysis,
progressive lipodystrophy, and short and broad digits, especially
thumbs and halluces. We concur with Zufferey and co-workers
[2013] that despite the resemblances the differences are sufficient to
discern the two entities.
We conclude that the present patient resembles the family
reported by Haugen and Bertelsen [1998] but not any other entity,
The occurrence of the syndrome in twogenerations, both sexes, and
absence of consanguinity all point to an autosomal dominant
pattern of inheritance. The cause is unknown. We have initiated
a molecular study using next generation sequencing techniques in
order to detect the gene causing this entity.
ACKNOWLEDGMENTS
We thank the family for their participation in this study. We thank
Eyvind Rødahl for useful discussions and Marte Emilie Sandvik
Haaland and Lisbet Sviland for professional assistance. This study
was supported by grants from theWesternNorwayRegionalHealth
Authority (911466 and 911688 to C.B). None of the authors have
any conflicts of interests.
REFERENCES
Anandan V, Parveen B, Prabhavathy D, Priyavarthini V. 2008. AdamsOliver syndrome—A variant. Int J Dermatol 47:1260–1262.
ArcherHL,Gupta S, Enoch S, ThompsonP,RowbottomA,Chua I,WarrenS, Johnson D, Ledbetter DH, Lese-Martin C, Williams P, Pilz DT. 2005.Distinct phenotype associated with a cryptic subtelomeric deletion of19p13.3-pter. Am J Med Genet 136A:38–44.
Balaji S,DennisNR,KeetonBR. 1991. Familial Ebstein anomaly:A reportofsix cases in two generations associated with mild skeletal abnormalities.Br Heart J 66:26–28.
BoorR,Herwig J, Schrezenmeir J, Pontz BF, SchonbergerW. 1993. Familialinsulin resistant diabetes associated with acanthosis nigricans, polycysticovaries, hypogonadism, pigmentary retinopathy, labyrinthine deafness,and mental retardation. Am J Med Genet 45:649–653.
Booth AJ, Hodgkins PR. 2006. Pseudopterygium arising in a patient withmultiple keloids. J Pediatr Ophthalmol Strabis 43:49–51.
Burk CJ, Aber C, Connelly EA. 2007. Ehlers-Danlos syndrome type IV:Keloidal plaques of the lower extremities, amniotic bands, limbdeformities, and a new mutation. J Am Acad Dermatol 56 (Suppl 2):S53–S54.
ChenKM, Bird L, Barnes P, Barth R,Hudgins L. 2005. Lateral meningocelesyndrome: Vertical transmission and expansion of the phenotype. Am JMed Genet 133A:115–121.
Coffin GS. 1990. Developmental retardation with unusual facies, arthritis,and hearing impairment. Dysmorph Clin Genet 4:103–109.
CoroneoMT, Chui JJY. 2013. Pterygium In: Holland EJ,MannisMJ, BarryLee W, Ocular surface disease:Cornea, conjuntiva and tear film. Phila-delphia: Elsevier Sauders. p. 125–144.
EversMEJW, Dijkman-Neerincx RHM,Hamel BCJ. 1994. Oculo-ectoder-mal syndrome: A new case. Am J Med Genet 53:378–379.
Fryns JP, Gevers D. 2003. Goeminne syndrome (OMIM 314300): Anothermale patient 30 years later. Genet Counsel 14:109–111.
Haugen OH, Bertelsen T. 1998. A new hereditary conjunctivo-cornealdystrophy associated with dermal keloid formation. Acta OphthalmolScand 76:461–465.
Hennekam RCM. 2006. Rubinstein-Taybi syndrome. Eur J Hum Genet14:981–985.
Heyen CA, Delk PR, Bull MJ, Weaver DD. 2008. A report of an apparentnew genetic syndrome consisting of joint contractures, keloids, largeoptic cup-to-disc ratio and renal stones. Am J Med Genet 146A:3120–3125.
Islam SI, WagonerMD. 2001. Pterygium in youngmembers of one family.Cornea 20:708–710.
Leung RSC, BeerWE, Mehta HK. 1988. Aplasia cutis congenita presentingas a familial triad of atrophic alopecia, ocular defects and a peculiarscarring tendency of the skin. Br J Dermatol 118:715–720.
Liu L, Wu J, Geng J, Yuan Z, Huang D. 2013. Geographical prevalence andrisk factors for pterygium: A systematic review and meta-analysis. BMJOpen 3:e003787.
McGowan R, Gulati R, McHenry P, Cooke A, Butler S, KengWT, MurdayV,WhitefordM,Dikkers FG, Sikkema-Raddatz B, van Essen T, Tolmie J.2011. Clinical features and respiratory complications in myhre syn-drome. Eur J Med Genet 54:553–559.

ABARCA ET AL. 2907
Monga S, Gupta A, Kekunnava R, Goyal S, Vemuganti GK, Sachdeva V.2012. Childhood pterygium; a descriptive study of 19 cases presented to atertiary eye care center. Am J Ophthalmol 154:859–864.
Penttinen M, Niemi KM, Vinkka-Puhakka H, Johansson R, Aula P. 1997.New progeroid disorder. Am J Med Genet 69:182–187.
Rojas JR, Malaga H. 1986. Pterygium in Lima, Peru. Ann Ophthalmol18:147–149.
Van de Kar A, Houge G, ShawAC, Van BelzenMJ, Peters DJM,HennekamRC. Keloids in Rubinstein-Taybi syndrome: A clinical study. Br JDermatol. In press.
Zufferey F, Hadj-Rabia S, De Sandre-Giovannoli A, Dufier JL, Leheup B,Schweitze C, Bodemer C, Cormier-Daire V, Le Merrer M. 2012. Acro-octeolysis, keloid like-lesions, distinctive facial features, and overgrowth:Two newly recognized patients with premature aging syndrome, pentti-nen type. Am J Med Genet 161A:1786–1791.