Embed Size (px)
Citation preview

PART 1 Oesophagus
COPYRIG
HTED M
ATERIAL


3
Anatomy
The adult oesophagus is a muscular tube some 250 mm long, which extends from the pharynx, at the cricoid carti-lage opposite the sixth cervical vertebra, to the oesophago - gastric junction, about 25 mm to the left of the midline, opposite the tenth or eleventh thoracic vertebra. The oesophagus has longitudinal mucosal folds and, when empty, a very narrow lumen. For endoscopists, the distance from the incisor teeth to the upper end of the oesophagus is about 150 mm and to the oesophago - gastric junction about 400 mm, depending, clearly, on the height of the person. The oesophagus pierces the left crus of the dia-phragm and has an intra - abdominal portion about 15 mm in length. Its principal relations, important to the patholo-gist in assessing the local spread of cancer, are with the trachea, left main bronchus, aortic arch, descending aorta and left atrium.
The arterial supply of the oesophagus is by the inferior thyroid, bronchial, left phrenic and left gastric arteries and by small branches directly from the aorta. Its veins form a well - developed submucosal plexus draining into the thyroid, azygos, hemiazygos and left gastric veins. It, thus, provides an important link between the systemic and portal venous systems. Lymphatic channels from the phar-ynx and upper third of the oesophagus drain to the deep cervical lymph nodes, either directly or through the parat-racheal nodes, and also to the infrahyoid lymph nodes; from the lower two - thirds they drain to the posterior medi-astinal (para - oesophageal) lymph nodes and thence to the thoracic duct. From the infra - diaphragmatic portion of
the oesophagus, drainage is to the left gastric lymph nodes and to a ring of lymph nodes around the cardia. Some lymph vessels may drain directly into the thoracic duct. In its upper part the oesophagus is innervated by the glossopharyngeal nerve and, throughout its length, it is supplied by fi bres from the vagus nerve and local sympa-thetic ganglia.
The lower end of the oesophagus is anchored posteriorly to the pre - aortic fascia and is surrounded by the phreno - oesophageal ligament, which blends into the muscularis propria of the oesophagus. This arrangement allows some degree of movement and rebound. Dissection studies indicate that no discrete anatomical sphincter is present but there are differences of opinion as to whether, and if so how, the muscle at the oesophago - gastric junction is modi-fi ed. One careful anatomical study [1] has ruled out the presence of any thickening of the muscularis mucosae or of the circular muscle coat but has described the separation of obliquely arranged inner circular muscle fi bres into fas-cicles, which continue into the stomach to form the circular muscle layer. However, another equally thorough investi-gation [2] describes a defi nite thickening of the inner cir-cular muscle coat. Both studies have concluded that the arrangements that they describe might, and probably do, act as a functional sphincter.
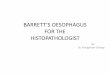
The oesophageal wall in cross - section can be divided macroscopically into stratifi ed squamous epithelium, lamina propria, muscularis mucosae, and the submucosa, muscularis propria and adventitia (Figure 1.1 ). Gross inspection of cut sections of tumours in the oesophagus generally reveals the depth of tumour invasion and this
CHAPTER 1
The n ormal o esophagus: a natomy, s pecimen d issection and h istology r elevant to p athological p ractice Kaiyo Takubo 1 and Neil A. Shepherd 2 1 Tokyo Metropolitan Institute of Gerontology and Tokyo Medical and Dental University School of Medicine, Tokyo, Japan 2 Gloucestershire Cellular Pathology Laboratory, Cheltenham, UK
Morson and Dawson’s Gastrointestinal Pathology, Fifth Edition. Edited by Neil A. Shepherd, Bryan F. Warren, Geraint T. Williams, Joel K. Greenson, Gregory Y. Lauwers and Marco R. Novelli.© 2013 Blackwell Publishing Ltd. Published 2013 by Blackwell Publishing Ltd.

4 Oesophagus
epithelium with a subjacent lamina propria resting on the underlying muscularis mucosae.
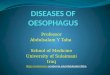
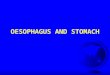
Epithelium Resection specimens usually have a thinner squamous epithelium compared with biopsy specimens because the superfi cial layers are likely to be lost during surgical han-dling. The squamous epithelium (Figure 1.2 ) has a basal zone consisting of several layers of cuboidal or rectangular basophilic cells, with dark nuclei, in which glycogen is absent. It occupies about 10 – 15% of the thickness of the normal epithelium, although it may be thicker in the last 20 mm or so of the squamous - lined oesophagus. Occasional mitoses are evident in the basal and parabasal cell layers. Above the basal zone, the epithelial cells are larger and become progressively fl attened but, even on the surface, they retain their nuclei. Keratohyaline granules are not usually present in the surface cells of the normal epithe-lium. However, glycogen is abundant. Ki - 67 (monoclonal antibody MIB - 1) immunostaining usually shows a negative reaction in the basal layer, on the basement membrane, and a positive reaction in the parabasal layers. Epithelial stem cells may be present in the basal layer. The presence of Ki - 67 - positive cells in more than three cell layers is an abnormal feature, consistent with gastro - oesophageal refl ux disease (Figure 1.3 ).
Single intra - epithelial lymphocytes ( ‘ squiggle ’ cells) lying between the squamous cells are common, particularly in the lower half of the mucosa, and in this situation their convoluted nuclei may be confused with the nuclei of neutrophils. They are a normal feature. Characterisation using monoclonal antibodies has shown them to be T lym-phocytes [3] . Langerhans ’ cells are antigen - presenting cells that are demonstrable, by electron microscopy and metal impregnation techniques, as sparsely distributed ovoid forms with radiating dendritic processes, occurring in all layers of the oesophageal epithelium [4] . They are posi-
Figure 1.1 The microanatomy of the wall of the oesophagus: in this cross - section, A is the squamous epithelium - lined mucosa and B the muscularis mucosae, which is separated from the mucous membrane by the lamina propria. C is the submucosa, which contains the oesophageal submucosal glands (D), whereas the circular and longitudinal layers of the muscularis propria are outside the submucosa.
Figure 1.2 The normal squamous epithelium of the oesophagus: this is a stratifi ed squamous epithelium with no keratinisation or a well - developed glandular layer. Note the thickness of the basal cell layer and the height of the papillae.
Figure 1.3 The normal oesophageal epithelium on Ki - 67 immunostaining: the basal cells (arrows) on the basement membrane do not stain but parabasal cells are positive for Ki - 67.
assessment of depth, through the various layers of the wall, is of critical importance for staging and prognostication.
Histology
Mucosa
The squamous - lined mucosa is about 500 – 800 μ m thick and is composed of non - keratinising stratifi ed squamous

The normal oesophagus 5
be aggregated around the ducts of the oesophageal submu-cosal glands. There are numerous vascular papillae (also known as intrapapillary vessels or intrapapillary capillary loops), associated with connective tissue, which project upwards for two - thirds of the total thickness of the epithe-lium. Changes in the vascular pattern are evident by mag-nifying endoscopy under various pathological conditions.
Relatively large vessels are observed more frequently in the lamina propria than in the submucosa in cross - sections of the lower oesophageal sphincter. These vessels are considered to be the longitudinal palisade vessels visible at endoscopy and helpful in defi ning the true oesophago - gastric junction.
Muscularis m ucosae The muscularis mucosae shows a variable pattern. In its upper part it commonly consists of isolated or irregularly arranged muscle bundles, rather than forming a continu-ous sheet, but in the middle and lower thirds it forms a continuum of longitudinal and transverse fi bres and may reach up to 300 μ m in thickness at the squamo - columnar junction. In the resected oesophagus, thick collections of fi ne irregular muscle fi bres are evident at sites of previous biopsy.
Submucosa
The submucosa contains the oesophageal submucosal glands (deep glands, oesophageal glands proper), Meiss-ner ’ s plexus and a ramifying lymphatic plexus within a loose connective tissue network, which accounts for the early and extensive submucosal spread of oesophageal car-cinoma. The oesophageal submucosal glands tend to be arranged in rows parallel to the long axis [15] and, although scattered, they are relatively concentrated at the upper and lower ends of the oesophagus. The glands are compound tubulo - alveolar in type and resemble labial salivary glands, containing both mucous and serous secretory cells and oncocytes, with surrounding myo - epithelial cells, anchor-ing them to the underlying basement membrane. The mucous cells contain sulphomucins. Many glands do not contain serous cells. From two to fi ve lobules drain into a common duct lined by a fl attened cuboidal epithelium initially, which becomes stratifi ed squamous in type, and surrounded by lymphocytes and plasma cells after passing obliquely through the muscularis mucosae (Figure 1.4 ). The presence of oesophageal submucosal glands and/or their ducts is presumptive evidence that any sampled biopsy material derives from the true anatomical oesophagus.
Muscularis p ropria
The muscularis propria consists of well - developed circular and longitudinal coats. In its upper part these are striated
tively stained with antibodies against S - 100 protein and react with monoclonal antibodies against HLA - DR (major histocompatibility complex [MHC] class II) and OKT6 (CD1). They also contain calcitonin gene - related peptide (CGRP), which may serve as an immunomodulator. The number of Langerhans ’ cells and the intensity of their immu-noreactivity for CGRP are increased in refl ux oesophagitis [5] . They contain Langerhans ’ granules (Birbeck ’ s granules), seen on electron microscopic examination.
Both melanocytes and non - melanocyte argyrophil cells are randomly distributed in the basal layer of the epithe-lium, the former usually as small groups and the latter singly [6,7] . These cell types are presumably the origin of primary malignant melanomas and small cell undifferenti-ated (oat cell) carcinomas, respectively, that occur at this site. Merkel ’ s cells are also present in the epithelium.
Transmission electron microscopy (TEM) studies of the squamous epithelium have broadened our understand-ing of the micro - anatomy [8 – 13] . Basal cells are cuboidal or columnar with large, centrally placed nuclei and rela-tively simple cytoplasm containing few organelles. They are attached to the basement membrane by frequent hemi - desmosomes. Prickle cells show numerous keratin fi la-ments, relatively abundant glycogen, a prominent Golgi apparatus and more numerous desmosomes. The squa-mous cells of the superfi cial or functional zone become increasingly fl attened towards the lumen, contain some phospholipid material and have a coating of acid mucosub-stance which is likely to have a protective function. Scan-ning electron microscopy shows a complex pattern of micro - ridges lining the lumen. Membrane - coated granules, 0.1 – 0.3 μ m in diameter, are present in the intermediate and superfi cial zones of the oesophageal epithelium. As well as being the source of mucosubstances, they also contain acid hydrolases which, when secreted into the intercellular space, may be responsible for the reduction of desmosomes exhibited by squamous cells as they approach the luminal surface.
Free - ending nerves are located in the intercellular spaces of the squamous epithelium and reach the subepithelial nerve plexus. These nerves probably mediate oesophageal pain. Cell proliferation studies have demonstrated a slower cell cycle time in basal cells overlying papillae, in compari-son with the interpapillary basal cells [14] . The turnover time of the oesophageal epithelium is about 4 – 7 days in rats and mice. The corresponding period in humans is said to be 10 days or less, although no defi nitive data are available.
Lamina p ropria The lamina propria consists of loose connective tissue con-taining a sprinkling of lymphocytes, mostly helper T cells, plasma cells, and occasional eosinophils and mast cells. Focal collections of lymphocytes and plasma cells may

6 Oesophagus
be evident and assessable (see below). The adventitia is in continuity with the adjacent mediastinal connective tissues.
Tissues a djacent to the o esophagus, i ncluding the p leura
These are of some importance because they are or may be present in resected oesophagus specimens. The proximal stomach is almost universally present in such specimens whereas pharynx and spleen are occasionally seen in speci-mens resected with the oesophagus. The trachea, bronchus, lung, diaphragm, azygos vein, thoracic duct, thymus and aorta can also be present in oesophageal resection speci-mens. Although usually termed the circumferential resection margin of the oesophagus, it is important to note that, especially on the right but also on the left, a sizable propor-tion of the circumference of oesophageal resection speci-mens is actually invested not by adventitial connective tissues, thus constituting a true surgical margin, but by pleura, which all radical oesophago - gastrectomy specimens will possess. Involvement of the circumferential margin can be infl uenced by surgical quality but a surgeon can do little about pleural involvement. We advocate accurate identifi cation of the pleura, on both sides, and painting, preferably by coloured gelatin, of only the true circum-ferential surgical margin to allow differentiation of these structures in histological sections.
Location of the o esophago - g astric j unction
Precise defi nitions of the oesophago - gastric junction are essential before an accurate diagnosis of columnar - lined oesophagus (CLO) (see Chapter 5 : Barrett ’ s oesophagus) can be made. Anatomically, the defi nition of the oesophago - gastric junction is the line between the angles of the opened oesophagus and gastric curvature. This defi nition can be used for surgically resected materials. Clinically, however, the location of the oesophago - gastric junction is controver-sial [21] . The distance between the anatomical oesophago - gastric junction and the squamo - columnar junction, on macroscopic examination of postmortem specimens, has ranged from 0 – 10 mm with a mean of 3 mm [22] to 5 − 21 mm with a mean of 11 mm [23] .
In North America and European countries, the endo-scopic defi nition of the oesophago - gastric junction is the upper limit of the gastric folds. However, this upper limit shows considerable vertical movement during endoscopy [24] . When a small volume of air is present in the oesopha-gus, or at expiration, the upper end of the mucosal folds moves rostrally. When a large volume of air is present, or in deep inspiration, the upper end of the columnar mucosal folds moves caudally. Therefore, the upper limits of the columnar mucosal folds are not in a constant position. Palisade vessels are always evident within the oesophagus
and both oxidative (fast twitch) and glycolytic (slow twitch) fi bres are present [16] . There is a gradual change to smooth muscle in the upper and middle thirds, although, in the lower third, both coats are entirely composed of smooth muscle with no clear evidence of sphincter formation. A well - defi ned myenteric nerve (Auerbach ’ s) plexus is present at all levels but there appears to be no well - formed submucosal plexus. Three types of neuron are identifi able [17,18] . One is argyrophilic, multi - axonal and, probably, sympathetic, and sends out numerous dendrites and axons to surround other neurons in the same and adjacent ganglia but does not directly supply muscle. The second type is not argyrophilic but cholinergic and probably parasympa-thetic, supplying the muscle. It is likely that the former has a coordinating function and the latter a motor function. A third type of fi bre, probably part of the communicating system, is rich in vasoactive inhibitory peptide (VIP). Such fi bres are commonly associated with sphincteric mechanisms [18] . There are also numerous intrinsic fi bres containing neuropeptide Y [19] . Ganglion cells decrease in number with age [20] but the smooth muscle does not appear to undergo corresponding atrophy.
Adventitia
The adventitia of the oesophagus is a thick layer of coarse connective tissue around the oesophagus and is seen to surround the oesophagus in resection specimens. It con-tains blood vessels, lymphatics and lymph nodes, multiple branches, anterior and posterior, of the vagus nerve and other neural structures. Its comprehensive examination is of particular importance in such resection specimens because here proximity of tumour to the circumferential surgical resection margin and the pleural surfaces will
Figure 1.4 The submucosal gland of the oesophagus: the terminal portions consist of mucous cells. A duct (D) is evident.

The normal oesophagus 7
often be found in the distal 10 mm of the oesophagus. They are observed in about half of all patients with oesophageal or gastric carcinoma.
In cardiac mucosa adjacent to the squamo - columnar junction, most of the gland cells are mucous in type and stain strongly with periodic acid – Schiff (PAS). Occasional cells near the upper ends of the glands, close to the squa-mous junction, may secrete both sialomucins and sulpho-mucins [26] . Parietal cells, morphologically identical to those in the fundic glands, are present in small numbers (oxyntocardiac glands) and occasionally chief cells are present as well. Numerous endocrine cells, some of which are argentaffi n and others argyrophil, are found in this region [27] . Lymphoid follicles are also common in the deeper part of the mucosa, or extend through the muscu-laris mucosae into the submucosa.
Pancreatic tissue (Figure 1.6 ) may be seen in the mucosa at the oesophago - gastric junction: it is recognisable by the presence of variably sized nests or lobules of acinar tissue, 0.2 – 1.6 mm in diameter, admixed with cardiac glands, and composed of cells with basally located, small, round and uniform nuclei and abundant cytoplasm. These structures appear eosinophilic and granular in the apical and middle portions and basophilic in the basal area. Some mucous cells may be intermingled [28] . As a result of their resem-blance to pancreatic exocrine cells and their immunoposi-tivity for lipase, the term ‘ pancreatic acinar metaplasia ’ has been used to describe this feature. Some have sug-gested an association with gastritis but subsequently it has been recognised as a common feature in patients attending for elective upper gastrointestinal endoscopy and is not
[25] , are observed within the lower oesophageal sphincter and can be used to defi ne the oesophago - gastric junction. So, in Japan, the oesophago - gastric junction is defi ned endoscopically as the lower limit of the palisade vessels [22] . Based on this defi nition, many cases may actually be defi ned as representing ultra - short segment columnar - lined oesophagus (see Chapter 5 section ‘ Ultra - short segment Barrett ’ s oesophagus ’ ). Pathologists should always pay attention to the true origin of any biopsy specimen from the mucosa around the oesophago - gastric junction.
Oesophageal cardiac glands (superfi cial glands, mucosal glands) are small mucous glands in the lamina propria. They are branched simple tubulo - alveolar glands, located mainly in the lower and upper oesophagus. Oesophageal cardiac glands beneath the oesophageal squamous epithe-lium at the squamo - columnar junction show continuity with the gastric cardiac mucosa and can be observed at endoscopy through the squamous epithelium in about half of all patients examined. However, cardiac glands are histologically evident at or around the oesophago - gastric junction in almost all individuals (Figure 1.5 ). The maximum overlap of the squamous epithelium and cardiac glands extending continuously from the gastric cardia, as demonstrated by histological and endoscopic examination, may be up to 15 mm. Endoscopically, oesophageal cardiac glands beneath the squamous epithelium in the oesophago - gastric junction zone usually appear yellowish in colour, and are fl at or slightly elevated. Columnar - lined islands are also observed endoscopically in squamous mucosa and are similar in colour to those of the gastric cardiac mucosa, being unstained with Lugol ’ s iodine. Columnar islands can
Figure 1.5 The oesophageal cardiac glands (also known as superfi cial or mucosal glands) beneath squamous epithelium in the oesophago - gastric junction zone. Mucous gland lobules are present. Part of a cardiac - type gland (arrow) is apparent in the squamous epithelium.
Figure 1.6 Pancreatic metaplasia and ciliated epithelium in the mucosa at the oesophago - gastric junction. Pancreatic acinar cells with eosinophilic cytoplasmic granules are present among cardiac - type glands. The ciliated epithelium is histologically similar to that of bronchial pseudo - stratifi ed columnar epithelium.

8 Oesophagus
in the submucosa, but EMRs are also employed as a ‘ big biopsy ’ , e.g. for the defi nitive diagnosis of well differentiated squamous cell carcinoma when multiple previous biopsies have been unable to fully confi rm the diagnosis. Of increasing importance is their use in the man-agement of early neoplasia complicating Barrett ’ s oesopha-gus (see Chapter 5 ).
Although somewhat dependent on the endoscopic methodology used, before fi xation they can be stretched to refl ect the size and shape as in the body and then pinned to a board with the mucosal aspect uppermost. The specimen(s) should then be immersed in a large container of formalin and fi xed for at least half a day or overnight. Either initially or after fi xation, they can be painted to demonstrate peripheral and deep margins of excision. India ink, coloured paints and coloured gelatin can be used, depending on local laboratory preferences. For speci-mens that have been resected piecemeal, pinning and fi xa-tion should be performed by an endoscopist aware of the actual confi guration of the lesion in vivo to enable more precise restructuring and assessment of ultimate (espe-cially peripheral) resection margins.
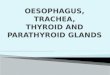
It is recommended that fi xed specimens obtained by EMR and ESD are cut into slices 2 – 3 mm thick for serial sectioning and microscopic examination. The lines of sec-tioning should be at right angles to the line forming a tangent to the resection margin close to the tumour [33] .
Surgical r esection s pecimens
Oesophagectomy and oesophago - gastrectomy operations are most commonly undertaken for carcinoma of the oesophagus. In the Far East, this is usually for squamous cell carcinoma whereas, in western countries, adenocarci-noma complicating Barrett ’ s oesophagus is now over-whelming the most common indication for these operations. Increasingly neo - adjuvant chemo(radio)therapy has been used and this may make identifi cation of the site of the tumour diffi cult and require extensive blocking of the oesophagus to ensure that the entire tumour site has been assessed histologically. This section will give guidance as to the appropriate macroscopic preparation and assessment of these specimens but the interested reader is referred to guidelines and protocols published by Japanese, UK and US authorities for a comprehensive guide to the assessment of such specimens [33 – 35] .
Surgically resected specimens should be opened lon-gitudinally in a standard way. We recommend standard opening ventrally. The part of the oesophagus containing the tumour may then be left unopened with an appropriate fi xative - soaked wick to ensure internal fi xation. Alterna-tively, that part can be opened in a standard way (ventrally) with the circumferential margin previously painted to aid accurate assessment of margins of excision. At this time, whether or not the tumour is opened, it is important for
specifi cally associated with any clinical or histological abnormalities of the oesophagus or stomach [29] . Similar foci have been described in the gastric antral and body mucosa but appear to be much less common at these sites, although they have been reported in some 3% of antral biopsies from children [30] . A pancreatic phenotype is also well recognised in Barrett ’ s metaplastic tissue in the true oesophagus (see Chapter 5 ).
Multilayered epithelium (ME) or squamous metaplasia - like change may be evident in the oesophageal cardiac glands beneath the squamous epithelium and in cardiac mucosa adjacent to it (Figure 1.6 ). There may also be a pseudo - stratifi ed (partly ciliated) columnar epithelium, often merging with the squamous metaplasia - like change [31,32] . When histological examination of a biopsy specimen reveals pancreatic acinar metaplasia, multilayered epithelium, squamous metaplasia - like change or pseudo - stratifi ed co-lumnar epithelium with occasional cilia, we fi rmly believe that the tissue can yet derive from the ‘ normal ’ mucosa of the oesophago - gastric junction zone and does not necessarily infer true glandular metaplasia of the lower oesophagus, alternatively known as Barrett ’ s oesophagus (see Chapter 5 ).
Handling of e ndoscopic and r esection o esophageal s pecimens
Endoscopic r esection s pecimens ( F igure 1.7 )
Endoscopic mucosal resection (EMR) and endoscopic sub-mucosal dissection (ESD) are relatively new techniques of increasing importance for the diagnosis and treatment of neoplasia in the oesophagus. They can be used for the removal of small benign tumorous nodules, such as granu-lar cell tumours and other small connective tissue tumours
Figure 1.7 Schema illustrating one method for sectioning endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) specimens advocated by the Japan Esophageal Society [33] . Fixed specimens that have been obtained by EMR and ESD are cut into slices 2 – 3 mm thick. (Reproduced with kind permission from Springer Science+Business Media: Esophagus, Japanese Classifi cation of Esophageal Cancer, tenth edition: part I, vol 6, 2009, p.39, Japan Esophageal Society, © 2009.)

The normal oesophagus 9
fi cial tumour is fi xed to the muscularis propria. If not fi xed, the tumour will slide over the muscularis propria when only slight force is applied to the mucosa, indicating that it is probably a superfi cial carcinoma without invasion to the muscularis propria. We recommend that, in cases of superfi cial carcinoma, the specimen is sliced parallel to the long axis of the oesophagus. Whole step sections can then be prepared [33,35] .
In more advanced carcinoma, be it squamous cell carci-noma or adenocarcinoma, it is clearly important to exten-sively sample the most deeply invasive tumour. One or more representative slices of the tumour at the site of deepest invasion, estimated by inspection and palpation, parallel and perpendicular to the oesophagus, should be blocked and submitted for histopathological examination to demonstrate the deepest aspect of the tumour and its relationship to the layers of the oesophageal wall, adventi-tial tissues and, critically, the circumferential resection margin and pleural surfaces [33 – 35] .
References 1. Jackson AJ . The spiral constrictor of the gastro - esophageal junc-
tion . Am J Anat 1978 ; 51 : 265 . 2. Liebermann - Meffert D , Allgower M , Schmid P , Blum AL . Mus-
cular equivalent of the lower esophageal sphincter . Gastroenterol-ogy 1979 ; 76 : 31 .
3. Mangano MM , Antonioli DA , Schnitt SJ , Wang HH . Nature and signifi cance of cells with irregular nuclear contours in esopha-geal mucosal biopsies . Mod Pathol 1995 ; 5 : 191 .
4. Geboes K , DeWolf - Peeters C , Rutgeerts P , et al. Lymphocytes and Langerhans cells in the human oesophageal epithelium . Virchows Arch A Pathol Anat Histopathol 1983 ; 401 : 45 .
5. Singaram C , Sengupta A , Stevens C , Spechler SJ , Goyal RK . Localization of calcitonin gene - related peptide in human esopha-geal Langerhans cells . Gastroenterology 1991 ; 100 : 560 .
6. de la Pava S , Nigogosyan G , Pickren JW , Cabrera A . Melanosis of the esophagus . Cancer 1963 ; 16 : 48 .
7. Tateishi R , Taniguchi H , Wada A , Horai T , Tanaguchi K . Argy-rophil cells and melanocytes in esophageal mucosa . Arch Pathol 1974 ; 98 : 87 .
8. Hopwood D , Logan KR , Coghill D , Bouchier IAD . Histochemi-cal studies of mucosubstances and lipids in normal human oesophageal epithelium . Histochem J 1977 ; 9 : 153 .
9. Logan KR , Hopwood D , Milne G . Ultrastructural demonstration of cell coat on the cell surface of normal human oesophageal epithelium . Histochem J 1977 ; 9 : 495 .
10. Al Yassin TM , Toner PG . Fine structure of squamous epithelium and submucosal glands of human oesophagus . J Anat 1977 ; 123 : 705 .
11. Hopwood D , Logan KR , Bouchier IAD . The electron microscopy of normal human oesophageal epithelium . Virchows Arch (B) 1978 ; 26 : 345 .
12. Hopwood D , Logan KR , Milne G . The light and electron micro-scopic distribution of acid phosphatase activity in human normal oesophageal epithelium . Histochem J 1978 ; 10 : 159 .
13. Logan KR , Hopwood D , Milne G . Cellular junctions in human oesophageal epithelium . J Pathol 1978 ; 126 : 157 .
14. Jankowski J , Austin W , Howat K , et al. Proliferating cell nuclear antigen in oesophageal mucosa: comparison with autoradiogra-phy . Eur J Gastroenterol Hepatol 1992 ; 4 : 579 .
the prosector to identify the pleural surfaces and ensure that these can be accurately differentiated, at the time of histological assessment, from the true circumferential resection margin by appropriate painting (see above). Fur-thermore, these specimens undergo dramatic shortening immediately after surgery because of contraction of the muscularis propria such that the oesophageal segment is often only half the length it was in situ . Efforts should therefore be made to ensure that these specimens are received in the laboratory as soon as possible so that they can stretched and pinned on a corkboard to refl ect the length at the time of resection.
Although some authorities recommend that oesophagec-tomy specimens should always be fi xed unopened through the tumour, we believe that there are times, especially in early cancer, multifocal dysplasia and superfi cial cancer (particularly that complicating Barrett ’ s oesophagus) and when neo - adjuvant therapy has effectively ablated the tumour, when opening the specimen is appropriate to allow accurate identifi cation of those parts of the specimen for submission for histological assessment. After neo - adjuvant therapy, only an area of superfi cial scarring of the mucosa may be seen, on opening, and this may be less easy to appreciate in transverse sections of a specimen previously left unopened. Assessment of these specimens should not be beholden to blanket national and international ‘ rules ’ but should be determined by the requirements of the indi-vidual case and local laboratory practices.
In a specimen left unopened, a large sharp knife should be used to section the entire tumour area transversely with identifi cation of the orientation achieved by differential painting or another method favoured by the laboratory. These slices can then be submitted for histology in their entirety, usually in big blocks, such that all adventitial tissues, para - oesophageal lymph nodes and pleural sur-faces can be assessed, along with the true circumferential resection margin, previously identifi ed by painting. We recommend coloured gelatin for this purpose because it adheres very effectively to the surface, is readily identifi ed in histological sections and does not run or spread like other fl uids used in laboratories for this purpose.
It is important to ensure that proximal and distal surgical resection margins are assessed histologically and separate doughnuts from these margins should always be submit-ted for histology in their entirety because oesophageal cancer, both squamous cell carcinoma and adenocarci-noma, can demonstrate discontinuous spread, often as a result of submucosal lymphovascular spread, with involve-ment of margins at some distance from the primary tumour. The proximal and distal resection margins can be assessed in sections taken parallel to the margins and/or in longitu-dinal sections perpendicular to them [33,34] .
Superfi cial carcinoma can usually be distinguished from advanced carcinoma by macroscopic observation of cut surfaces of the tumour or by determining whether a super-

10 Oesophagus
27. Krause WJ , Ivey KJ , Baskin WN , MacKercher PA . Morphological observations on the normal human cardiac glands . Anat Rec 1978 ; 192 : 59 .
28. Doglioni C , Laurino L , Dei Tos AP , et al. Pancreatic (acinar) metaplasia of the gastric mucosa: histology, ultrastructure, immunocytochemistry and clinicopathologic correlation of 101 cases . Am J Surg Pathol 1993 ; 17 : 1134 .
29. Wang HH , Zeroogian JM , Spechler SJ , Goyal RK , Antonioli DA . Prevalence and signifi cance of pancreatic acinar metaplasia at the gastroesophageal junction . Am J Surg Pathol 1996 ; 20 : 1507 .
30. Krishnamurthy S , Integlia MJ , Grand RJ , Dayal Y . Pancreatic acinar cell clusters in pediatric gastric mucosa . Am J Surg Pathol 1998 ; 22 : 100 .
31. Glickman JN , Chen Y - Y , Wang HH , et al. Phenotypic character-istics of a distinctive multilayered epithelium suggests that it is a precursor in the development of Barrett ’ s esophagus . Am J Surg Pathol 2001; 25 : 569 .
32. Takubo K , Vieth M , Honma N , et al. Ciliated surface in the esophagogastric junction zone: a precursor of Barrett ’ s mucosa or ciliated pseudostratifi ed metaplasia? Am J Surg Pathol , 2005 ; 29 : 211 .
33. Takubo K , Makuuchi H , Fujita H , et al. Japanese classifi cation of esophageal cancer. Parts I, II and III . Esophagus 2009 ; 6 : 1 .
34. Mapstone N . Dataset for the Histopathological Reporting of Oesophageal Carcinoma , 2nd edn . London : Royal College of Pathologists , 2007 . Available at: www.rcpath.org/resources/pdf/G006OesophagealdatasetFINALFeb07.pdf (accessed April 2011).
35. Washington K , Berlin J , Branton P , et al. Protocol for the examina-tion of specimens from patients with carcinoma of the esophagus . College of American Pathologists , 2011 . Available at: www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/Esophagus_11protocol.pdf (accessed April 2011).
15. Goetsch E . The structure of the mammalian esophagus . Am J Anat 1910 ; 10 : 1 .
16. Whitmore I . Oesophageal striated muscle arrangement and his-tochemical fi bre types in guinea pig, marmoset, macaque and man . J Anat 1982 ; 134 : 685 .
17. Smith B . The neurological lesion in achalasia of the cardia . Gut 1970 ; 11 : 388 .
18. Alumets J , Fahrenkrug J , Hakanson R . A rich VIP nerve supply is characteristic of sphincters . Nature 1979 ; 280 : 155 .
19. Aggestrup S , Emson P , Uddman R , et al. Distribution and content of neuropeptide Y in the human lower esophageal sphincter . Digestion 1987 ; 36 : 68 .
20. Eckardt V , Le Compte PM . Esophageal ganglia and smooth muscle in the elderly . Am J Dig Dis 1978 ; 23 : 443 .
21. American Joint Committee on Cancer . Esophagus and esoph-agogastric junction . In: AJCC Cancer Staging Manual , 7th edn . New York : Springer , 2009 : 103 .
22. Takubo K , Arai T , Sawabe M . Structures of the normal esophagus and Barrett ’ s esophagus . Esophagus 2003 ; 1 : 37 .
23. Bombeck CT , Dillard DH , Nyhus LM . Muscular anatomy of the gastroesophageal junction and role of phrenoesophageal ligament. Autopsy study of sphincter mechanism . Ann Surg 1966 ; 164 : 643 .
24. Takubo K , Vieth M , Aida J , et al. Differences in the defi nitions used for esophageal and gastric diseases in different countries. Endoscopic defi nition of the esophagogastric junction, the pre-cursor of Barrett ’ s adenocarcinoma, the defi nition of Barrett ’ s esophagus, and histologic criteria for mucosal adenocarcinoma or high - grade dysplasia . Digestion 2009 ; 80 : 248 .
25. De Carvalho CAF . Sur l ’ angio - architecture veineuse de la zone de transition oesophagogastrique et son interpretation fonction-nelle . Acta Anat 1966 ; 64 : 125 .
26. Gad A . A histochemical study of human alimentary tract muco-substances in health and disease . 1. Normal and tumours. Br J Cancer 1969 ; 23 : 52 .