Embed Size (px)
Citation preview

i

ii
ABSTRACT
Identification of the determinants of maternal morbidity and mortality is a valid scientific
endeavour in its own right, but it is particularly relevant to any undertaking to improve maternal
health. By understanding the determinants of ill-health and their inter-relationships, it is
possible to develop treatments, seek preventative measures, target high-risk individuals and
groups, and assess the health implications of changes in the biological, physical, or social
environment. This paper provides a framework for studying the determinants of maternal
morbidity and mortality. Examples are cited from both developed and developing countries,
with an emphasis on the latter.
The term 'determinants' is defined broadly in this paper as encompassing all associations
between factors of interest and maternal health outcomes. Included within this are causes,
which primarily refer to pathogenic determinants of mortality; risk factors, which have a
biologically causal link to the outcome of interest; and risk indicators which are simply
associated with the outcome. Maternal health determinants are conceptualised as belonging to
one of three groups: determinants of pregnancy, determinants of morbidity, and determinants of
mortality. It is noted that methodological techniques for ascertaining the determinants of health
often reduce the issues under consideration to simplified, often linear, relationships between the
determinants and specific, usually negative, health outcomes. This approach is not always
appropriate since factors which are determinants from one perspective, may be outcomes from
another, and the repeat nature of pregnancy and morbidity makes the entire process a dynamic
one with many possible complex interactions. Risk indicators are often highly correlated, and
epidemiological strategies for analysis which eliminate confounders and look for single effects
are not always relevant.
Demonstrating associations requires a clear understanding of the types of health outcomes seen.
Maternal mortality, a single event occurring during pregnancy or the puerperium, is contrasted
to morbidity where four main patterns are seen including: diseases seen only during pregnancy
and the puerperium; diseases starting in pregnancy and the puerperium but continuing into the
interpartum period; diseases caused by pregnancy but not temporally located within the
pregnancy; and pre-existing diseases which are either temporarily or permanently worsened by
pregnancy.
After discussing outcome patterns, this paper describes the measurement of determinants.
Methods for obtaining information on the pathogenic causes of morbidity and mortality are
briefly summarized. The range of data sources, and measurement and analysis techniques for
identifying risk factors and indicators are discussed. Finally the study design implications of
attempting to show biologically causal relationships as opposed to associations are addressed.

iii
LIST OF CONTENTS
ABSTRACT
ii
LIST OF CONTENTS
iii
LIST OF TABLES AND FIGURES
iv
PREFACE
v
ACKNOWLEDGEMENTS
vi
1. INTRODUCTION
1
1.1 Defining ‘Outcomes’
2
1.2 Defining ‘Determinants’
5
2. CHOOSING OUTCOMES
7
2.1 Characterising and Identifying Pregnancy
7
2.2 Characterising and Identifying Maternal Morbidity
8
2.3 Characterising and Identifying Maternal Mortality
13
3. CHOOSING DETERMINANTS
15
3.1 Determinants of Pregnancy
15
3.2 Determinants of Morbidity and Mortality
17
4. DEMONSTRATION ASSOCIATIONS
20
4.1 Case Selection/Comparison Groups
20
4.2 Measures of Association
22
4.3 Conclusion
24
REFERENCES
26

iv
LIST OF TABLES AND FIGURES
Table 1 Percentage of women aged 15-49 who are pregnant at a given point in
time, for various levels of the general fertility rate
12
Table 2 List of proximate and distal determinants of fertility
16
Figure 1
Schema showing the broad categories of outcomes and determinants
related to mental health
3
Figure 2 Schema representing patterns of maternal morbidity 10
Figure 3 Diagram showing possibilities of selection bias 21

v
PREFACE
In January 1989, a new research initiative was launched by the Maternal and Child Epidemiology
Unit at the London School of Hygiene and Tropical Medicine. The primary objectives of this
programme are to evaluate existing methods for measuring maternal health in developing countries
and to develop, pilot and promote the use of new approaches. Two principal phases of activities
can be distinguished. The first comprised an eighteen month preparatory period, and the second a
three-year phase of field investigations in collaboration with six institutions in developing
countries.
The Phase I (1989-90) activities, supported by the British Overseas Development Administration
and the Ford Foundation, included:
-developing a computerized reference collection
- preparing four review papers on measuring maternal health
-conducting an illustrative analysis of survey data on maternity care in six African countries
- refining the Sisterhood Method for estimating the level of maternal mortality
-establishing formal links with other research groups working on maternal health
- hosting a Workshop to develop proposals for field activities in Phase II.
This document represents the third of the four review papers addressing methodological issues in
maternal health. The first paper sets the stage by examining definitional and conceptual issues that
underlie the measurement of maternal health. The remaining three focus on measurement-related
issues relevant to the three major purposes of information on maternal health:
- establishing levels and trends,
- identifying the determinants, and
- monitoring and evaluating programmes.
The first document, "Measuring maternal health: defining the issues", focuses on the implications
of the process of conceptualization for programmes and for measurement and considers maternal
health in the context of women's health (Graham and Campbell, 1990). The second paper,
"Measuring maternal mortality and morbidity: levels and trends", looks at the types of
methodologies, measures and sources of data available for measuring morbidity and mortality
(Campbell and Graham, 1990). This, the third, "Measuring the determinants of maternal morbidity
and mortality: defining and selecting outcomes and determinants, and demonstrating associations",
is organized around selecting morbidity and mortality outcomes and demonstrating associations
between them. The last paper, "Measuring the effectiveness of maternal health programmes",
examines the types of interventions used to improve maternal health with regard to the
methodologies available to assess impact and effectiveness (Graham and Campbell, 1991).
Phase II of the research initiative in Methodologies for Measuring Maternal Health will contribute
to strengthening the maternal health information base by identifying appropriate approaches for
meeting information needs in developing countries. For further details on this initiative, contact
the programme director, Dr Wendy Graham, at:
Maternal and Child Epidemiology Unit
London School of Hygiene and Tropical Medicine
Keppel Street, London WC1E 7HT.
vi
ACKNOWLEDGEMENTS
Preparation of this paper and three others on methodologies for measuring maternal health was
funded by a grant from the Ford Foundation. We acknowledge and appreciate the support of
three members of the Foundation in particular: Dr Marge Koblinsky, who was involved at the
initiation of the work; Mr Stuart Burden, who liaised with the project in the middle; and Dr José
Barzelatto, who enabled us to see it through to completion.
We are also indebted to our colleagues Dr Patricia Doyle, Dr Vincent Fauveau, Ms Véronique
Filippi, Ms Masuma Mamdani, Dr Melissa Parker and Dr Cleone Rooney who made several
editorial improvements to this particular paper. Our thanks are also due to Ms Lynne Davies for
her preparation of text and tables.

1
1. INTRODUCTION
Identifying the determinants of maternal morbidity and mortality is a valid scientific endeavour
in its own right, but it is particularly relevant to any undertaking to improve maternal health. By
understanding the determinants of ill-health and their inter-relationships, it is possible to
develop treatments, seek preventive measures, target high-risk individuals and groups, and
assess the health implications of changes in the biological, physical, or social environment. On
the other hand, it is also important to recognize that identifying and intervening against specific
determinants of maternal ill-health is not exclusively within the sphere of bio-medical expertise,
and that a multidisciplinary approach to studying and resolving health problems is imperative.
Recent investigations of the determinants of women's morbidity and mortality have either
adopted a condition-specific focus, such as work by Bang et al. (1989), the Reproductive
Morbidity Interdisciplinary Research Group (1991) and Wasserheit et al. (1989) seeking factors
contributing to reproductive tract infections, or have evolved around methods for operations
research in Safe Motherhood, such as the approach looking at delay factors taken by the
Prevention of Maternal Mortality Project of Columbia University (Thaddeus and Maine, 1990).
This paper is one of a series of four papers highlighting relevant methodological issues. As
with any other morbid condition, measuring the determinants of maternal ill-health requires five
steps:
1.choosing a particular outcome of interest;
2.hypothesizing an association between the outcome and a certain factor or factors;
3.measuring the outcome and factors;
4.demonstrating the association; and
5.specifying the nature of the mechanism linking the factors and the outcome.
The range of disciplines, study designs, data collection instruments, study populations, measures
of association and analysis techniques available for studying the determinants of maternal
morbidity and mortality does not differ substantially from the range available for examining the
determinants of most other health conditions. However, certain methods have special relevance
to maternal morbidity and mortality, and some pertinent measurement issues are frequently
neglected.
This paper is organized into four parts. After the introduction, which clarifies what is meant by
'outcomes' and 'determinants', the second section focuses on the patterns of maternal health
outcomes. Pregnancy and mortality are contrasted to morbidity, where four main patterns are
seen, including: (1) diseases seen only during pregnancy and the puerperium; (2) diseases
starting in pregnancy and the puerperium but continuing into the interpartum period; (3)
diseases caused by pregnancy but not temporally located within the pregnancy; and (4) pre-
existing diseases which are either temporarily or permanently aggravated by pregnancy. Section
3 presents the categories of determinants - determinants of pregnancy, mortality and morbidity -
as well as the tiers of determinants - pathogenic causes, risk factors and risk indicators. The
paper concludes by reviewing issues of study design, case selection and choice of comparison

2
groups, and measurement of exposures and outcomes which arise in the process of
demonstrating associations.
1.1Defining 'Outcomes'
Before contemplating ways of measuring the determinants of maternal health outcomes, an
understanding of the 'outcomes' under consideration is needed. Health, despite being defined as
a positive state of physical, mental and social wellbeing and not just the absence of disease
(WHO, 1948), is frequently used synonymously with ill-health; and maternal health is no
exception. The emphasis on the negative aspects of maternal health stems in part from the lack
of operational definitions and suitable indicators of both positive health and of social and mental
health, and, in part, from the view that pregnancy is pathogenic (Graham and Campbell, 1990;
Leavitt, 1988). There is a third reason for the emphasis on ill-health: analytical techniques for
ascertaining the determinants of health frequently simplify the linkages to linear relationships
between the determinants and single, usually negative, health outcomes.
This paper also concentrates on morbidity and mortality. However, even without the added
complexities of measuring positive health, the definition of outcomes remains complicated by
the relationship of maternal ill-health to pregnancy. Maternal morbidity and mortality lie at an
interface between reproduction and health, and even when a single negative outcome, such as
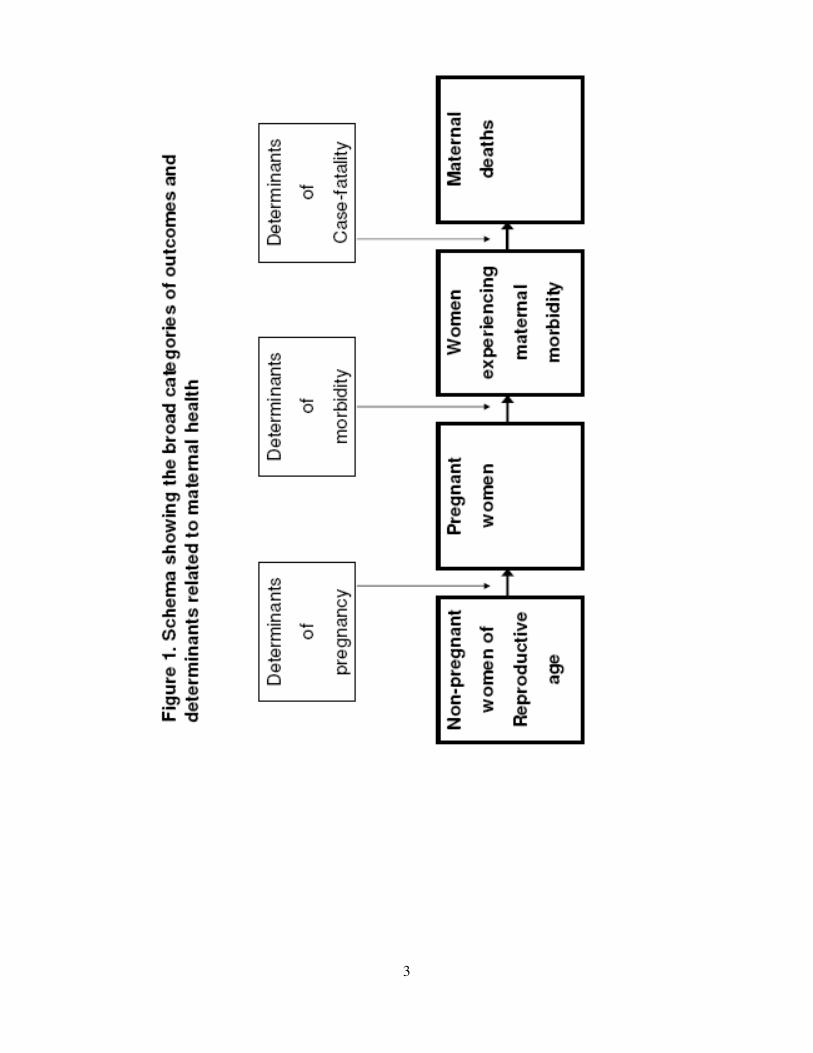
maternal death from postpartum haemorrhage, is selected for study, it must be recognized that a
woman passes through up to three stages, each conditional upon the preceding stage, in order to
become a case. For example, a woman must become pregnant, experience a problem associated
with the pregnancy (morbidity), and fail to have that problem resolved (mortality) in order to die
from pregnancy-related causes. With maternal morbidity, she must fall pregnant and experience
a problem associated with that pregnancy on a long- or short-term basis. Conceptualizing
maternal ill-health in this way with at least two stages for morbidity and three for death,
emphasizes that three relevant categories of determinants must be considered: determinants of
pregnancy, determinants of morbidity, and determinants of mortality (Figure 1).
Categories of determinants are not necessarily exclusive. While any one determinant may
appear in multiple categories, the mechanisms through which it acts, and the direction and
magnitude of its effects, will differ. A woman's age, for example, can determine her probability
of becoming pregnant, her risk of developing pregnancy-induced hypertension once pregnant,
and her probability of dying of eclampsia, given it develops. A specific determinant may also
have multiple mechanisms within a broad category. For example, age may determine mortality
either through a constitutional effect, or through its influence on a woman's ability to negotiate
needed medical care for herself.
Specific determinants which belong in several broad categories can act on maternal health in the
same, or in opposing, directions. For example, in most societies, educated women are exposed
to fewer pregnancies than uneducated women, and are more likely to seek and receive
appropriate care once they experience morbidity. In both cases, education lowers the risk of
mortality. On the other hand, women outside stable unions are less likely to be
3

4
exposed to the risk of pregnancy (Bongaarts and Potter, 1983), but in some situations are more
likely to die if they become pregnant (Kwast and Liff, 1988). Hence marriage both increases
and decreases the risk of maternal mortality and may have varying overall effects in different
countries.
Recognition of the three conditional stages of an outcome (pregnancy, morbidity, and mortality)
clarifies interpretation of the impact of determinants which may act on maternal morbidity and
mortality in opposing directions. There are, however, two obvious drawbacks to the framework
in Figure 1. Firstly, it fails to capture the dynamic nature of biological processes. Unlike the
representation in Figure 1, neither pregnancy nor morbidity are necessarily single events.
Instead, pregnancy for the individual woman comprises a pattern of childbearing including a
whole range of frequencies (gravidities) and intervals between pregnancies, while morbidity
may encompass a complex series of repeated episodes of various illnesses. This limitation is
overcome in theory for maternal mortality by indicators such as the lifetime risk which take an
aggregate perspective encompassing the entire reproductive period. The lifetime risk of
maternal mortality can be shown to be a function of the total gravidity rate, the all-cause
morbidity ratio per 100,000 pregnancies, and the case-fatality risk1.
Attempting to put the formula into practice highlights the second drawback to the framework in
Figure 1: the complexities of measuring morbidity risks, and their attendant case-fatalities, for
an entire range of morbidities make it virtually impossible to put the framework into use. This
is partly because, in contrast to pregnancy and mortality which can be expressed as binary
conditions (the woman is either pregnant or not, or dead or not), maternal morbidity is not a
single entity, and the most that can usually be said is that a woman does or does not have a
particular range of illnesses or symptoms. The nature of the specific morbidity per se, its
severity and its duration have an integral role in determining its amenability to treatment and
thus its prognosis; these factors vary widely from morbidity to morbidity. The availability and
accessibility of services are also influential in case-fatality and can be quite diverse for different
morbidities and/or settings. Consequently, there are many more biologically causal
determinants of morbidity and mortality than of fertility, and some of these are as yet
unidentified. In contrast to the models of the determinants of fertility, the difficulties of
identifying and measuring even those biologically causal determinants which are known, makes
the prospect of a testable model of the determinants of maternal mortality seem remote.
1.This is summarized as a formula which can be applied either to all-cause maternal mortality or
to cause specific lifetime risks:

5
1.2Defining 'Determinants'
Classifying determinants by the outcome they influence (pregnancy, morbidity, mortality) is not
sufficient; it is also necessary to delimit the range of determinants under consideration. Most
studies have primarily focused on causes of death and on age and parity as risk factors. An
important contribution of early work on Safe Motherhood has been to broaden perceptions of
what determines or 'causes' a maternal death. Several illustrations of the complex chain of
events leading to a maternal death, including Fatallah's 'Why did Mrs X die' (WHO, 1986) and
Kwast's case histories (WHO, 1987), have shown that although the most immediate
determinants of maternal death are medical causes, maternal health goes beyond medical issues.
Three additional categories which play an important role in determining the risk of death can be
identified: (1) health service factors, including the quality of care and the accessibility and
availability of preventative and curative health services; (2) reproductive factors, including the
woman's constitution, her parity, general health status, and age; and (3) socio-economic factors,
including urban/rural residence, education, income, status, and cultural factors.
Adopting such a broad view of determinants has several advantages: it places both outcomes
and possible interventions in their social context thereby increasing the potential for success in
various cultural settings; it suggests more potential points of intervention; and it is more likely
to lead to interventions with multiple health impacts. A broad definition is not without its
disadvantages however, since the effects of intricate relationships can be difficult to demonstrate
and successful interventions against complex situations, such as low socio-economic status, are
not easily implemented and may be perceived by decision makers to lie outside the scope of
health interventions. Furthermore, if the relationship between a determinant and the outcome is
complex, the underlying mechanism may be misinterpreted, and manipulation of some
determinants, particularly those which are not biologically causal, will not necessarily result in
the desired change. A solution which avoids the latter difficulty, without restricting the focus to
pathogenic causes, is to emulate research into the determinants of fertility and of child mortality
and consider several tiers of determinants.
In a now classic study, Davis and Blake (1956) postulated that social, economic and
environmental factors act through eleven 'intermediate fertility variables' to influence fertility.
These include: (1) factors affecting exposure to intercourse; (2) factors affecting exposure to
conception; and (3) factors affecting gestation and successful parturition. The development of
this framework, which emphasized that all changes in the outcome (fertility) must be mediated
through the eleven intermediate biological mechanisms, led to considerable progress in
understanding fertility determinants. Further developments have reduced these eleven
'proximate'2 factors to a model predicting the total fertility rate using four main variables of
interest: stable sexual union (marriage), contraception, lactation and induced abortion
(Bongaarts and Potter, 1983).
2."Proximate" and "distal" determinants are used in the demographic literature on fertility to
describe biologically causal and socioeconomic determinants, respectively.

6
The above fertility models have influenced the construction of frameworks of infant and child
health, which also emphasize that more distant socioeconomic determinants must be
behaviourally or environmentally linked to adverse health outcomes through biological
mechanisms (Mosley and Chen, 1984; van Norren and van Vianen, 1986). The implication for
maternal health is to suggest, for instance, that although low levels of female education may be
positively associated with poor maternal health outcomes, improvements in a distal determinant,
such as female education, will not necessarily reduce maternal mortality unless, for example,
they also lead to changes in fertility patterns, uptake of care, or constitutional factors. An
extreme example is seen among well educated women in the Faith Assembly of God, a
fundamentalist religious sect in the United States. These women have a maternal mortality ratio
of 872/100,000 in part because they refuse to use medical services (Kaunitz et al., 1984).
Conversely, some oil-rich Arab States have been able to reduce maternal mortality markedly
through almost universal high-quality care, without simultaneous improvements in women's
status (Rosenfield and Maine, 1987). By contrast, improvements in proximate determinants,
such as effective treatment of a potentially fatal morbidity, will necessarily decrease the lifetime
risk of maternal death, providing all other influencing factors remain constant.
Despite potential misinterpretation of the effects of distal determinants, a broad view of the
determinants of maternal morbidity and mortality is maintained in this paper. The terms
'determinants', 'risk indicators', 'risk factors', and 'causes', as well as 'antecedents', 'influences',
'covariates' and 'correlates', all of which have been used interchangeably in the health literature
to describe the associations between the outcome of interest and other factors, are defined here
in order to keep some distinctions in the layering of determinants. 'Determinants' is used as a
broad term describing all factors associated with the outcome of interest. Within 'determinants',
three tiers are defined: 'causes', which describe pathogenic (medical) causes of morbidity or
mortality; 'risk factors' which have a biologically causal link to the outcome of interest; and 'risk
indicators' which include all other determinants (Backett et al., 1984).

7
2. CHOOSING OUTCOMES
The first step in demonstrating an association is to decide the maternal health outcomes of
interest. Of the three possible stages a woman can pass through, pregnancy, morbidity, and
mortality, two -- pregnancy and mortality -- pose relatively few conceptual problems, although
both can be difficult to measure. Pregnancy and mortality each have an implicit role in the ICD-
10 definition, which states that a pregnancy-related death is the death of a woman while
pregnant or within 42 days of termination of pregnancy (WHO, 1990a). Although maternal
morbidity seems an intuitive and necessary intermediary, there is no clear-cut definition of what
constitutes a maternal morbidity (Campbell and Graham, 1990; Graham and Campbell, 1990).
At this early phase in conceptualizing and understanding the epidemiology of maternal
morbidity, it is necessary to determine which morbidities are influenced by pregnancy at all and
thus which are maternal morbidities before commencing to study their determinants. At a
minimum, conditions leading to maternal mortality should be included, but it is also known that
many serious consequences of pregnancy affect women beyond the narrow time-band when
maternal deaths can occur. A broader definition, removing the time limitation and including all
conditions directly or indirectly arising from, or aggravated by, childbearing and its
management, does not diminish the measurement difficulties (Campbell and Graham 1990;
Graham and Campbell, 1990). The next three subsections discuss ways of characterizing each
of the stages of pregnancy, morbidity and mortality.
2.1 Characterizing and Identifying Pregnancy
The state of pregnancy is conceptually simple to describe. Pregnancy occurs when the
conditions leading to conception are present and sexual intercourse takes place; these factors, or
proximate determinants, are relatively well described and quantified (Bongaarts and Potter,
1983). However, unlike fertility research which often establishes pregnancy by the ensuing
birth, research into maternal health may necessitate detecting pregnancy in its early stages. The
ease of ascertaining pregnancy depends on whether laboratory tests, clinical examinations, or
women's reports are used and on the gestational age of the pregnancy, with early pregnancies
being the most difficult to detect.
Pragmatically, studies have to rely on women's cooperation to obtain good quality information
on pregnancy, and little is gained, for example, by using assays to detect early pregnancy unless
women want their pregnancies detected. The critical factor is rarely the technical difficulty of
determining pregnancy but rather women's willingness to disclose their pregnancies to
researchers. If substantial numbers of women do not know or are unwilling to state that they are
pregnant, it becomes difficult to obtain a representative sample (Airey and Campbell, 1988;
Baretto et al., 1992; Peoples-Sheps et al., 1988). An illustration of this is provided by a drug
trial using ivermectin to cure river blindness in Liberia which went to considerable lengths to
identify and exclude pregnant women. The investigators found that, on average, their questions
had a specificity of 98% but a sensitivity of only 79% (Pacque et al., 1991). For very early
pregnancies, sensitivity was as low as 26%. That is, only 26% of the women subsequently
found to be pregnant correctly identified themselves as pregnant. Similarly, Airey and
Campbell (1988) found significant underreporting of early pregnancies in several of the
Demographic and Health Surveys.

8
2.2 Characterizing and Identifying Maternal Morbidity
In contrast to pregnancy and mortality, maternal morbidity takes many forms. It can be an acute
or a chronic condition, which is either recognized and acknowledged as an illness or is not
apparent to the respondent. The perception of symptoms of morbidity vary between cultures
and can manifest in ways that are physically apparent to all, apparent to a trained eye, or
measurable only with certain instruments. The seriousness of specific morbidities also varies:
some are instantaneously lethal, while others are potentially lethal, disabling, or simply
discomforting. Morbidity events may be single episodes which resolve spontaneously, are
treated, or have permanent incurable effects, while others may recur occasionally or frequently.
Finally, each specific morbidity may have a whole spectrum of manifestations. For example,
haemoglobin levels are normally distributed, with anaemia, which occurs at the low end of the
distribution, ranging from mild to severe. Uterine prolapse, on the other hand, may manifest
itself through several symptom complexes, appearing as pain in some women and incontinence
in others. The forms taken by a particular morbidity are partly a function of its type and partly
due to its interaction with the woman's constitution and underlying health status.
The definition of maternal health initially proposed by Graham and Campbell (1990) and
elaborated by WHO (1990b) encompasses positive and negative outcomes from any cause
related to childbearing or its management. Although nulligravid women are excluded, the scope
of the definition is only slightly narrowed since maternal morbidity can occur any time
following the first pregnancy and continuing beyond the menopause. The definition proposed
by Graham and Campbell (1990) is further sub-divided to parallel the definition of maternal
mortality: pregnancy either causes morbidity directly or it interacts with the woman's underlying
health condition to cause disease. This concept can be applied to both physical and other forms
of ill-health. For example, pregnancy can lead to eclampsia (direct physical ill-health), or it can
aggravate underlying essential hypertension (indirect physical ill-health). Alternatively, a
teenager socially well-adapted to her milieu may become outcast as an unwed mother, or a
woman with an untreated vesico-vaginal fistula may experience a combination of physical,
mental and social ill-health.
Unfortunately, the link between pregnancy and specific morbidities is not always as apparent as
the above examples. Even if morbidity coincides with pregnancy or the puerperium, it is not
necessarily maternal morbidity. A study by Datta et al., (1980) in India reports that only 30%
of morbidity during this period is related to pregnancy or the puerperium, implying that 70% of
morbidity is not pregnancy-related. By contrast, studies in developing countries have shown
that between 80 to 95% of mortality during pregnancy and the puerperium is pregnancy related
(Chen et al., 1974; Fortney et al., 1984). Furthermore, while the International Classification of
Disease lists codes falling within the maternal death definition, no such criteria are provided for
pregnancy-related morbidity (WHO, 1977). When underlying morbidity (e.g. diabetes) is
exacerbated so markedly by pregnancy that it results in death, it is uncontroversial to label the
death an indirect maternal one. If the same morbidity is only slightly aggravated, however, it
may be difficult to recognize it as an indirect maternal morbidity in the absence of detailed
knowledge of the natural history of the disease and its previous presentation in the woman.
Indeed it may only be possible to attribute risks associated with pregnancy to populations of
women rather than to individuals. Criteria for "normality" are not present in all cases. For
example, Weigel and Weigel (1988) argue that nausea and vomiting during pregnancy are signs
of good health and that women experiencing these symptoms are not ill. Unless explicit

9
definitions of maternal morbidity are made, and similar ranges of conditions included, data from
different studies will not be comparable.
Building up a picture of disease patterns in the absence of pregnancy is virtually impossible in
many settings where the majority of women will have been pregnant at least once by a certain
age. Settings where this is not the case, as for example in some developed countries, tend to
experience low rates of morbidity anyway, and women who remain nulligravid in both
developed and developing country settings are likely to differ from their gravid counterparts in
many ways, not least in their fecundability. For example, MacKie et al., (1991) studied the risks
of complications of melanoma in four groups of women: women with initial melanoma
diagnosis before first pregnancy, during pregnancy, after last pregnancy, and between
pregnancies. The investigators were unable to compare these with nulliparous women with
melanoma because none were available in the study area. Special sub-groups who voluntarily
avoid pregnancy, such as nuns, have been used to understand aspects of reproductive
epidemiology, but this approach has extremely limited potential (Nathanson, 1985).
Three further factors influence the morbidity outcome and have implications for its
identification and the ease and timing of its measurement: the availability of treatment, the
repeatable nature of pregnancy, and the possibility of health benefits arising from pregnancy.
Some treatments may completely remove all signs and symptoms of the morbidity, while others
leave physical traces which can remain constant or be exacerbated by subsequent pregnancies or
other events. In extreme cases, the damage may be so great as to prevent further pregnancy,
leading to the paradoxical result that women with fewer pregnancies may be the ones bearing
the greatest cost of pregnancy (Graham and Danso-Manu, 1988). Secondly, the effect of
repeated pregnancies on underlying health status may lead to cumulative insults to a woman's
health. This would suggest that higher parity women maybe an ideal group in which to study
maternal morbidity. However, the frequency of, and intervals between, pregnancy are highly
related to other biological factors which play a role in health, particularly age. This makes it
difficult to adjust for the effects of these events separately, since high-parity pregnancies will
almost inevitably result from shorter intervals and occur at older ages. In assessing the impact
of pregnancy on a woman who has had five pregnancies, it is unclear whether the incremental
effect on her health should be assessed by comparing her to a woman of the same age with four
pregnancies or to an older woman of the same parity. The need to control for other important
variables in addition to age and parity, such as socio-economic status, may rapidly lead to small
numbers of women under consideration in each category of a data set.
Finally, it must not be assumed that the effects of pregnancy on women's health are necessarily
negative. Studies of the long-term sequelae of pregnancy suggest that the hormonal
consequences of pregnancy may provide strong protective effects against breast and ovarian
cancer (Beral, 1985; Booth et al., 1989; Green et al., 1988), while pregnancy has been found to
have no affect on the prognosis of malignant melanoma (MacKie et al., 1991)
Morbidity Matrix. Figure 2 presents maternal morbidity in a simplified schematic form with
four dimensions. It is intended to highlight measurement-related issues encountered when

10
Figure 2. Schema representing patterns of maternal morbidity
Dimension I: Diseases observable only during pregnancy and the puerperium
(1)
(2)
(3)
Dimension II: Diseases starting during pregnancy or the puerperium, but
continuing beyond it
(4)
(5)
Dimension III: Disease associated with pregnancy but not temporally
located within it
(6)
(7)
Dimension IV: Underlying disease exacerbated by pregnancy
(8)
(9)
(10)
(11)

11
investigating maternal morbidity, including relevant study populations and feasible reference
periods. The first dimension, shown by I:1-3, illustrates diseases seen only during pregnancy,
delivery and the puerperium. Such conditions are usually recognized as being 'caused' by the
pregnancy, since they are temporally associated with it, and in many ways are the simplest
morbidities to identify as conditions or diseases of pregnancy, not least by women themselves.
Despite associating these conditions with pregnancy, women may not, however, perceive them
as problems but rather as 'normal' aspects of pregnancy. Defining and probing for symptoms is
necessary to identify problems of interest, such as nausea, which may not be perceived as, or
indeed be, maternal morbidities. On the other hand, if women's own perceptions of their health
problems are to be included, room must be left for open-ended ascertainment of problems such
as backache, haemorrhoids or spirit-possession, since these self-reported morbidities may not
correspond to medically defined symptoms or be of concern to investigators. Examples of
diseases showing the patterns of morbidity shown in Figures I:1-3 include ante- and postpartum
haemorrhage, obstructed labour, infection, hepatitis, vomiting, urinary tract infections, monilia,
gestational diabetes, cholestatic jaundice of pregnancy, pregnancy induced hypertension, and
eclampsia.
Since the morbidities in dimension I must coincide with the relatively brief 46 week period of
pregnancy and the puerperium to be considered maternal morbidities, they can be difficult to
study in the community because of the relative scarcity of pregnancy (Airey and Campbell,
1988; Filippi et al., 1990; Peoples-Sheps et al., 1988). Table 1 estimates the percentage of
reproductive age women pregnant at a given point in time. It shows that, depending on the
general fertility rate, between 3 and 20% of women of reproductive age can be expected to be
pregnant, and between 0.4 and 2% will be at a specific gestational month. This is compounded
by difficulties in ascertaining early pregnancy and the fact that not all pregnant women will have
a specific illness of interest. Morbidities also vary with gestational age of pregnancy. Unless
good, representative records are available or morbidities can be recalled over long periods,
acquiring a representative sample with sufficient women at various gestational ages to inquire
about current morbidity status or morbidity in the previous two weeks can be daunting. In other
words, even though maternal morbidity is reported to be at least 16 times more common than
maternal mortality, it can still be rare on a period basis (Datta et al., 1980).
Dimension II:4-5 in Figure 2 illustrates diseases starting during pregnancy or the puerperium
and continuing into the interpartum period. As with conditions typified by dimension I, such
diseases are frequently perceived as maternal morbidities. Because such conditions are likely to
be chronic, they can often be picked up through prevalence studies. If a condition is permanent,
its point prevalence may be high enough to ensure sufficient women are identified during cross-
sectional surveys. The chronic aspect also means, however, that such diseases may change over
time and become part of the background health status of the woman. If subsequent pregnancies
are not precluded, they may interact with, and possibly worsen the condition. The availability of
treatment can also play a role in the ease of detecting these types of morbidities. Examples of
conditions typified by dimension II: 4-5 include fistula, haemorrhoids, varicose veins, anaemia,
and possibly other nutritional deficiencies.
Dimension III:6-7 reflects diseases associated with pregnancy and the puerperium, but not
temporally located within the same time period. Because such conditions are not necessarily
associated with pregnancy by women or researchers, extensive data sets and creative analyses

12
Table 1.Percentage of women age 15-49 who are pregnant at a given moment in time, for
various levels of the general fertility rate
Country Year General
Fertility Rate
per 10001
Percentage
pregnant at given
point in time2
Percentage at
specific
gestational month
at a given point in
time
Japan 1986 45 3 0.4
Canada 1985 54 4 0.5
France 1986 58 4 0.5
USA 1985 60 5 0.5
Mauritius 1986 67 5 0.6
Thailand 1985 73 5 0.6
Ireland 1985 75 6 0.6
Brazil 1985 76 6 0.6
Mexico 1980 97 7 0.8
Costa Rica 1984 122 9 1.0
Egypt 1982 152 11 1.3
Bangladesh 1981 162 12 1.4
Honduras 1981 197 15 1.6
Pakistan 1976 206 15 1.7
Afghanistan 1979 233 17 1.9
Rwanda 1978 236 18 2.0
1.The General Fertility Rate (GFR) is the live births per 1000 women aged 15-49 Source: UN
(1989).
2.The percentage pregnant at a given point in time is roughly estimated by multiplying the GFR
by 9 months gestation.
12 months per year
This figure slightly underestimates the number of women pregnant since not all pregnancies
result in live births.
3.The percentage at any given month of gestation is calculated by dividing the GFR by 12
months per year.

13
may be required to show an association. Some studies, such as those reported by Omran and
Standley (1978, 1981), have attempted to associate parity with various gynaecological
conditions including menstrual problems, vaginal discharge, itching, prolapse, urinary problems,
nutritional status, and vaginal or cervical abnormalities. Other less obvious long-term
morbidities associated with parity include diabetes mellitus, and may include all circulatory
disease, hypertensive disease, ischaemic heart disease, and sub-arachnoid haemorrhage (Beral,
1985; Green et al., 1988).
The final representation, dimension IV:8-11, depicts situations where background disease is
either temporarily or permanently worsened by pregnancy. Following parallels with maternal
mortality, these are the 'indirect' maternal morbidities. In such cases, the subsequent pregnancy
can act in a threshold, or a continuous manner. Understanding the interaction of indirect
morbidities and pregnancy requires knowledge of the natural history of the disease, basic
information which is often lacking. For example, epidemiological studies are frequently carried
out among 'white middle class males' and extrapolated to other groups (Cotton, 1990), making it
difficult to understand how conditions are influenced by pregnancy. Indirect morbidities
known, or suspected, to be exacerbated by pregnancy include AIDS, leprosy, tuberculosis,
malaria, malnutrition, and essential hypertension.
In 1957, Jewett argued the case eloquently for expanding our definition of maternal morbidity
using poliomyelitis as an example: "This disease can kill old or young, male or female, pregnant
or non pregnant, and might on the one hand be called non-obstetric. On the other hand, since its
incidence in pregnant women is thought to be much greater than in other adults, must it not be
called obstetric?" (Jewett, 1957). Much work remains to be done on the epidemiology of
maternal morbidity, particularly with regard to indirect morbidities, outcomes not temporally
associated with pregnancy or the puerperium, conditions affecting organs or systems besides the
reproductive tract, and factors affected by the pattern of childbearing rather than by individual
pregnancies. Although the morbidities involved are not fully listed, Figure 2 suggests ways of
thinking about the variety of outcomes and the target populations needed to study them.
2.3Characterizing and Identifying Mortality
Death is the final irreversible end-point of ill-health and there is little conceptual ambiguity
about it as an outcome. Rather, problems arise in locating a representative sample of deaths in
the community, and in ascribing pathogenic causes. These measurement problems are
discussed in detail by Campbell and Graham (1990), and include inadequate vital registration
and lack of proper medical certification of death. For deaths which are not medically attended,
causes must be reconstructed using "verbal autopsies" which rely on lay sign and symptom
reporting. Lack of medical training, different concepts of illness, sensitivity of the subject,
and/or trauma of the circumstances may make precise causes difficult to elicit. For example, in
their study of maternal mortality in Addis Ababa, Kwast and Liff (1988) attribute two deaths to
"Zar", describing it as "a condition which may manifest in bizarre behaviour, convulsive
seizures and extreme apathy. Several conditions would fit this description, e.g. typhus,
eclampsia or meningitis." Respondents may not know, recall or wish to inform the interviewer
about a given maternal death. The reluctance to discuss abortion-related deaths, for example, is
documented (Baretto et al., 1992). Even within medical facilities deaths may not be ascribed a
pathogenic cause due to the limitations of medical knowledge, clinical skills, diagnostic tests,
and autopsy techniques and facilities, as well as the lack of availability or the lack of skill of
those carrying them out. Numerous studies in both developed and developing countries have

14
shown official statistics to misclassify between 2-73% of maternal deaths as non-maternal
deaths (Campbell and Graham, 1990); very little work has been done on misclassification of
cause within the overall category of maternal causes (Grubb et al., 1988).

15
3. CHOOSING DETERMINANTS
The outcome chosen for investigation depends on several criteria including the priority of the
problem, its prevalence and preventability, the context, and the investigator's interests. Once an
outcome is selected, determinants must be hypothesized, and the study design and analysis
techniques selected. Much of this choice is dictated by the type of outcome under consideration
and the categories and tiers of determinants being explored. Epidemiological techniques will
play a large role in examining risk factors, while techniques derived from sociology and other
behavioural science disciplines must be used to study socio-economic and other more distal
influences.
3.1 Pregnancy Determinants
The proximate and more distal determinants of fertility contribute to maternal morbidity and
mortality because pregnancy is a pre-condition. Models of the proximate determinants suggest
for example, that non-contracepting, non-lactating women in stable sexual unions are most
exposed to the risk of pregnancy, and that on an aggregate level, these characteristics, together
with induced abortion, primarily determine the total fertility rate (Bongaarts and Potter, 1983).
Age is another important determinant which influences both fecundability and the likelihood of
exposure to intercourse. The implications of these proximate determinants of pregnancy for
maternal health have been illustrated by Graham and Airey (1987), who among others, show
that in many settings the majority of maternal deaths come from the mid-reproductive ages
where the most women are giving birth, despite the youngest and oldest women having the
highest age-specific risks per pregnancy. Although not yet demonstrated empirically, the same
relationships are likely to hold for age and maternal morbidity.
Distal determinants of fertility are often considered at both the societal and individual level
(Cochrane 1979; Lesthaeghe et al., 1981). Social institutions, cultural norms, economic and
environmental conditions as well as women's education, status, employment, ethnicity, and
family size desires have been identified as important distal determinants. These are listed
together with the proximate determinants in Table 2. Generally, higher levels of education,
income and women's status are associated with lower levels of fertility, and it is assumed that
they have a similar association with maternal morbidity and mortality, although this is by no
means certain. Louden (1987) argues, for instance, that maternal health, as opposed to neonatal
and infant health, is resistant to socio-economic indicators and is much more a function of
medical care. Indeed, until the 1930s, women of higher social class in England and Wales had
higher rates of maternal mortality probably because they were more likely to be delivered by
doctors in hospitals and consequently develop sepsis. More recently, Presern (1991) reports that
traditional midwives refuse to deliver low-caste Nepali women who thus probably receive better
quality delivery care because they are more likely to turn to modern medical facilities.
Women's employment generally reduces fertility as well. The anticipated direction of its impact
on maternal health is difficult to assess however. Studies of child health often assume that the
autonomy and resources gained through women's employment will improve child health, but it
is uncertain whether women can or will command these resources for their own health. In some
situations, women may continue to work to the detriment of their health just to remain in
employment. This possibility, coupled with the potential for occupational health

16
Table 2. List of proximate and distal determinants of fertility
Proximate determinants proposed by Davis and Blake (1956):
I Factors affecting exposure to intercourse
A Those governing the formation and dissolution of unions in the reproductive period
1. Age of entry into sexual union
2. Permanent celibacy: proportion of women never entering into sexual union
3. Amount of reproductive period spent after or between unions
a. When unions are broken by divorce, separation or desertion
b. When unions are broken by the death of the husband
B Those governing the exposure to sexual intercourse within union
4. Voluntary abstinence
5.Involuntary abstinence (from impotence, illness, unavoidable but temporary
separations)
6. Coital frequency
II Factors affecting exposure to conception (conception variables)
7. Fecundity or infecundity, as affected by involuntary causes
8. Use or non-use of contraception
a. by mechanical or chemical means
b. by other means
9.Fecundity or infecundity as affected by voluntary causes (sterilization, sub-incision,
medical treatment)
III Factors affecting gestation and successful parturition
10. Fetal mortality from involuntary causes
11. Fetal mortality from voluntary causes
Postpartum infecundability and lactational infecundability should be added to these proximate
determinants.
Socioeconomic and environmental determinants proposed by Bulatao and Lee (1983):
Social Institutions,
cultural norms,
economic and
environmental
conditions
Socio-economic
characteristics
Reproductive history
Demand for
children
Supply of
children
Fertility
regulation
costs
Motivation
to control
fertility Fertility
regulation to
limit family
size
Fertility

17
hazards, makes it difficult to speculate on the likely impact of employment on maternal health.
It is equally difficult to anticipate the direction of an effect of ethnicity as this is likely to be
mediated through a variety of culturally influenced behaviours.
3.2 Morbidity and Mortality Determinants
Conceptualization of the determinants of maternal morbidity and mortality is in the initial stages
of development. Studies have tended to focus on biomedical determinants, variously classified
as genetic or constitutional, environmental, and behavioral risk factors. A review of over 60
studies of the determinants of maternal ill-health shows that the most commonly-stated 'causes'
are pathogenic causes, such as haemorrhage and sepsis. These, together with investigations of
age and parity as biomedical risk factors concentrating health risks among very young and very
old women and nulliparous and grand multiparous women, far outnumber studies investigating
other tiers of determinants. Research which moves away from a clinical orientation with its
underlying paradigm of biologically causal links and biochemical markers, and considers a
wider range of determinants, is rare. This may be partly because maternal health is viewed not
as a public health issue but rather as a medical problem to be handled at the individual level.
The public health relevance of such clinically-oriented epidemiological research in developing
countries is being increasingly called into question (Akin, 1991). Narrowly focused studies
such as those dominating the maternal health literature often ignore the effects of important
confounding variables. Similarly, the fact that women may change their behaviour if they
perceive threats to their health is unrecognized, or is ignored because it is considered
analytically intractable. The policy conclusions arising from such narrow studies will tend to
favour medical interventions without considering mitigating effects of socio-economic factors
on the adoption and impact of the advocated interventions (Mosley and Chen, 1984; Akin,
1991).
Ultimately of course, most morbidities are of a physical nature and so biological factors must
come into play. However, studying the bacterial pathogens present in women with puerperal
sepsis may have relatively little impact on prevention in settings where malnourished women,
delivering in unhygienic environments with untrained personnel, have all kinds of contaminants
introduced through repeated vaginal examinations and die of sepsis because they cannot
command the resources to seek effective treatment when they experience problems.
Debates on the value of considering different tiers of health determinants have a long history.
Myntti (1991) contrasts the social medicine movement of the nineteenth century, where the
suggestions for preventing typhus included unlimited democracy, education and the
disestablishment of the Catholic church, with current trends whereby physicians,
epidemiologists and public health officials recommend treatment technologies and individual
behaviour modification. Such varying perspectives on the prevention of disease are unlikely to
be reconciled easily although it is anticipated that the variety of disciplines now involved in
maternal health will enhance the scope, and hopefully the quality, of the research. For example,
Myntti (1991) describes the present day role of anthropologists as counteracting 'the willingness
of many researchers to end the analysis with a simple documentation of behaviour rather than
investigating the context in which such behaviour takes place'. For health practitioners,
however, exploring the context of morbidity and mortality can be threatening to their
professionalism as it may lead away from solutions found in single technologies or
prescriptions, and even out of the health domain altogether. Multidisciplinary studies may also

18
point to determinants of ill-health which are not amenable to intervention at all in a given
context.
An important element in understanding the determinants of morbidity and mortality involves the
relationship of morbidity to mortality. As shown in Figure 1, each stage is conditional on the
previous one, and maternal mortality is conditional on maternal morbidity. Thus pregnancy and
the characteristics of a specific morbidity, including its severity, duration and pathogenic nature,
are frequently labelled "causes" of maternal mortality. These characteristics, their interaction
with the woman and with other morbidities or risk factors for the prognosis of morbidity, and
the availability, accessibility, quality and effectiveness (including compliance) of services and
treatments are grouped as determinants of death. For clarity however, it is preferable to separate
those which are primarily determinants of morbidity or pregnancy. Similarly, one type of
morbidity may lead to another without necessarily leading to death. Uterine atony may, for
example, lead to uterine rupture. In other words, influences which are determinants in one
instance may be outcomes in another depending on the stage which is under consideration.
Tiers of Determinants. Not all determinants are known and it is impossible to describe ways of
measuring all of them. However, some common determinants are briefly discussed below
following the three tiers; pathogenic causes of mortality, biologically causal risk factors, and
risk indicators.
Pathogenic causes of maternal mortality include all fatal conditions aggravating or aggravated
by pregnancy. The complications of pregnancy, childbirth and the puerperium listed in the ICD-
9 include 40 major three-digit divisions (WHO, 1977). The most common direct causes of
death however are haemorrhage, sepsis, obstructed labour, hypertensive diseases of pregnancy
and complications of illegally induced abortion, while common indirect causes include malaria,
and hepatitis.
Reproductive factors, including the woman's constitution, her age, parity, and general health
status are the most commonly considered factors as they can be measured relatively easily in
facility-based studies. Reproductive factors are thought to play a biologically causal role
although some, such as age and parity may influence women's confidence and use of services.
Often however, studies merely demonstrate an association with age and parity and recommend
targeting of high risk women for special care without exploring the mechanisms for the
association.
Another major category of determinants are health service factors. Here it is helpful to
distinguish between curative and preventative interventions, although once again the
conditionality of the three stages means that an intervention which cures morbidity prevents
death. It is common to distinguish between interventions by modern and traditional health
practitioners as well as those carried out by women themselves. As regards risk factors, this is
perhaps less useful than distinguishing between iatrogenic or harmful practices and helpful or
beneficial ones. These can be generally grouped under the quality of care. The accessibility and
availability of preventative and curative health services also belong in the health service
category. Thaddeus and Maine (1990) have reviewed the literature on maternal health care
utilization and proposed a useful framework examining three phases of delay: (1) delay in
deciding to seek care on the part of the individual, the family or both; (2) delay in reaching an
adequate health facility; and (3) delay in receiving adequate care at the facility.

19
This final category, socio-economic factors, is extremely broad and often includes urban/rural
residence, education, income, status, and cultural factors as risk indicators. Because such
influences are not necessarily causal, it is important to elaborate on the expected direction of an
association and possible reasons behind it while recognizing the potential for confounding. For
example, the evidence on the importance of maternal education has led to several exchanges
(Harrison, 1989a, 1989b; Maine et al., 1989). Hospital studies often find that illiterate women
have higher maternal mortality ratios than more educated women, leading some to argue that
female education will reduce maternal mortality. Others counter that such an assumption
assumes a causal relationship which is not adequately demonstrated by such studies. Indeed
much of the effect of education may be due to selection bias, as in many countries illiterate
women normally deliver at home and only use hospitals for complicated deliveries, arriving late
and often moribund. If access to health services is controlled for by only considering women
booked into the health system, further insight into the effects of education can be gained. In
Zaria, Nigeria between 1976-9, women with lower educational levels had better survival than
more highly educated women (110 versus 250 maternal deaths per 100,000 live births
respectively) (Harrison, 1985). By contrast, a hospital study in Port Harcourt in 1987-9 showed
women with less than secondary school education experienced almost five times the maternal
mortality of booked women with secondary or higher education (640 versus 130 maternal
deaths per 100,000 live births respectively)(Briggs and Oruambo, 1991). Some differences may
be due to underlying health status but it is also likely that ability to pay for health services and
staff attitudes play an important role (Campbell et al., 1991; Harrison et al., 1991). Further
exploration of the reasons for such differentials may lead to remedies well within the means of
hospital staff and available resources.
Arriving at an operational measure of a proposed determinant is another important but
potentially difficult task. For instance, many studies mention status of women as an important
aggregate level determinant of maternal health. Yet to assess the impact of women's status on
maternal mortality requires an indicator of status to be identified and measured. The status of a
woman cannot, however, be determined as easily as her age. The International Women's Rights
Action Watch (Isaacs et al., 1988) lists over 170 possible indicators of women's status, some of
which are characteristics of the woman while others apply to a local community or an entire
country. Even age is not necessarily simple to measure in countries where women are not aware
of their date of birth. In addition to obtaining a date of birth from the woman or from a birth
certificate, methods used to estimate women's dates of birth include local calendars, age in years
or in age groups, age at marriage and marriage duration, and even osteological evidence.
A move beyond pathogenic causes and biomedical risk factors to multiple risk indicators also
poses analytical problems. Risk indicators emerging from a broad view of determinants are
often highly correlated, and epidemiological strategies for analysis that discuss elimination of
confounders and single effects may be inappropriate. Unfortunately, despite sophisticated
analytical techniques developed to determine the relationship between socioeconomic variables
and child mortality, such literature often gives rise to conclusions that are so sweeping (such as
the richer and more educated you are, the better your health) that they are of little use to policy
makers (Akin, 1991).
20
4. DEMONSTRATING ASSOCIATIONS
Once the outcomes and determinants have been identified, it remains to select the study
population, to measure the outcomes and determinants, and to demonstrate an association.
4.1 Case Selection/Comparison Groups
In many situations, the choice of the outcome of interest and the availability of data determines
the study population. In investigations of maternal health, this choice is complicated by the
three stages through which a woman passes and it is important to keep in mind how case or
study population selection may influence the results. Furthermore, in many study designs, but
particularly in case-control studies, selection of an inappropriate comparison group is a major
source of bias.
For example, a study following up women after delivery to assess postpartum depression may
demonstrate that very young mothers are at greatest risk of depression. However, because the
study starts with women who are pregnant, it only considers the risk of depression given a
woman is pregnant and fails to recognize that very young women are less exposed to the risk of
pregnancy. In case-control studies, this dilemma presents itself in the choice of a control. A
case-control study of the risk of ectopic pregnancy associated with contraceptive use in
developing countries which opted to use both pregnant and non pregnant controls illustrates this
point. Results showed that while tubal ligation increased the risk of ectopic pregnancy given a
woman was pregnant (Odds Ratio=10.9), it substantially decreased the risk of ectopic pregnancy
overall (Odds Ratio=0.2) (Gray and Campbell, 1985). The choice and interpretation of a
comparison group in such instances is crucial.
This issue of the three stages of pregnancy, morbidity and mortality can lead to other potential
sources of error. If for example, cases are chosen using births or pregnancies as the sampling
unit, high parity women are more likely to be represented, all else being the same. If the
comparison group is then sampled from among women at large, then the parity distribution in
the cases and comparison group will be spuriously different.
Furthermore, the question of the representativeness of the study population affects the extent to
which results can be generalized to the population at large. For example, a study of risk factors
for case fatality in hospitals may be well designed, but still have little relevance in settings
where few women have access to hospital facilities and the majority of deaths take place at
home.
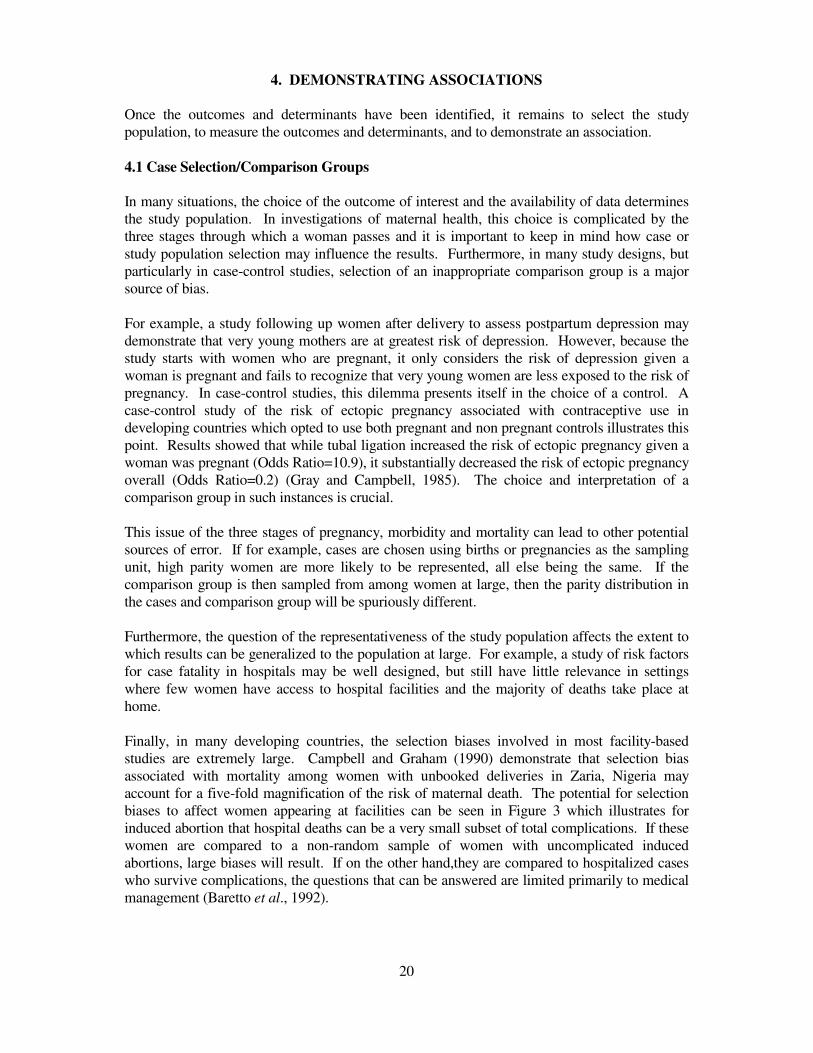
Finally, in many developing countries, the selection biases involved in most facility-based
studies are extremely large. Campbell and Graham (1990) demonstrate that selection bias
associated with mortality among women with unbooked deliveries in Zaria, Nigeria may
account for a five-fold magnification of the risk of maternal death. The potential for selection
biases to affect women appearing at facilities can be seen in Figure 3 which illustrates for
induced abortion that hospital deaths can be a very small subset of total complications. If these
women are compared to a non-random sample of women with uncomplicated induced
abortions, large biases will result. If on the other hand,they are compared to hospitalized cases
who survive complications, the questions that can be answered are limited primarily to medical
management (Baretto et al., 1992).
21
Figure 3. Diagrma showing possibilities of selection bias
Women
Sexually active
reproductive-age
women
Pregnant women
Unaccepted
pregnancy
Induced abortion
Complications
Hospitalized
Die Survive
Sexually inactive and/or
non-reproductive age
women
Non-pregnant women
Accepted pregnancy
Continued pregnancy
No complications
Not hospitalized
Die Survive

22
4.2 Measures of Association
Study designs to establish risk factors. Identification of risk factors for morbidity and
mortality involves establishing several criteria including a biological link, often assessed
through strength of the association, presence of dose response, and biological plausibility, and a
temporal sequence. The techniques for establishing risk factors are generally epidemiological
and consider individual level associations, and use prospective and retrospective rather than
cross-sectional designs. This is because while cross-sectional and ecological methods can
provide valuable clues to associations between variables, only studies incorporating a time
element can truly establish risk factors which precede disease.
Opportunities for considering maternal deaths or potentially fatal morbidities using prospective
or intervention studies are limited. In addition to ethical difficulties and the problems of loss to
follow-up, enormous numbers are needed and the time scale and cost are prohibitive unless
cohorts likely to exhibit high mortality rates are identified. For example, to answer the widest
range of questions on maternal health, a cohort of never pregnant women would need to be
identified (possibly as early as their own birth or conception) and followed through pregnancy,
morbidity and death. The problems of following such an 'average risk' group could be
circumvented by selecting a 'cohort' of unbooked hospital admissions with a high likelihood of
death. This group of women is highly selected however and more distal factors such as
accessibility to health services or risk of pregnancy could not be studied and representativeness
of the community at large would be low. For these reasons, the use of prospective studies,
especially in the community, are rare (Peoples-Sheps et al., 1988; Datta et al., 1980). Ongoing
surveillance areas such as Matlab in Bangladesh, the sites monitored by the MRC in The
Gambia or Sine Salloum in Senegal are more practical to use but such surveillance is rare and
tends to concentrate on mortality measurement. Historical cohorts can also be used but only in
settings where good records are maintained (Beral, 1985).
Given the difficulties associated with prospective studies, much of the research on risk factors
will be retrospective. As mentioned earlier, case-control studies often face difficulties selecting
the appropriate comparison group - a dead control or a living one for mortality studies; a
pregnant or non-pregnant one for morbidity and mortality studies; one suffering the same
condition for mortality studies. The problems of obtaining unbiased and comparable data for
the two groups are considerable. For example, relatives of a maternal death might simply not
know about the circumstances or might provide a different level of accuracy to the control or the
relatives of the control. Also problematic in case-control studies are the multiple layers of risk
which mean that comparison groups have to be chosen carefully. The choice of the appropriate
control becomes difficult and will heavily influence the determinants studied (Campbell, 1983).
In developing countries with limited health service coverage, behavioural and socio-economic
factors related to uptake of care are likely to introduce heavy biases.
It is imperative that case-control studies of maternal health give adequate consideration to the
exact question being asked and to the choice of comparison group. If cases are selected from
hospitals, pregnant controls should be from among women who intended to deliver in the same
place as the case did. Thus for many questions a woman who ends up as a complicated hospital
case after intending to deliver at home should have a control who delivered at home. Despite
these problems, case-control studies are a promising, but as yet underused approach. Only one
developing country case-control study of maternal mortality has been cited in the literature to

23
date (Bhatia, 1985; 1986); most case-control studies of maternal morbidity have been carried
out in developed countries. Careful case-control study designs can also be used to examine
medical practices within hospital settings. A common belief is that problems arise in getting
women to the hospital; that once women are there, medical services will help. The evidence for
this is contradictory and numerous studies have identified avoidable factors within the hospitals
(Campbell et al., 1991; Thaddeus and Maine, 1990).
The pattern of morbidity also plays a role in determining the methodology used. If the research
is concerned with rare conditions, the study must either follow high risk groups prospectively
(which limits the breadth of risk factors that can be considered) or else rely on a retrospective
design. Similarly, the location of the study -- ie community vs hospital -- is likely to be
determined by characteristics of the disease. If conditions manifest signs which can only be
detected clinically, health examinations are required and health facilities may be the only
possible venue.
Study designs to establish risk indicators. Risk indicators can be identified through a much
broader set of techniques than the search for risk factors. Many of the determinants under
consideration, such as educational level, are relatively long-term characteristics of the woman
and so establishing a temporal sequence is less problematic. Nevertheless it is important to be
aware of reverse causality. For example a woman's status may be improved by her having
children while a morbid condition such as fistula will lower a woman's status in the community.
The levels of analyses possible also vary: cross-national aggregate level assessments, secular
trends, as well as individual level analyses may be conducted.
Some of the analyses of risk indicators have used focus group or case history techniques to gain
a qualitative picture of the processes that contribute to maternal health from the perspective of
the health provider and the woman herself (Kwast, 1987). Other examinations of the broader
level factors have used standard techniques of multivariate analysis (Crook et al., 1991; Findley,
1989). Akin (1991) and Manton et al. (1991) suggest that for some types of conditions, health
measurement requires a combination of subjective, socio-anthropological techniques and
objective analytical and statistical procedures. Manton et al. (1991) have developed procedures
called the Grade of Membership, which they feel is free from restrictive assumptions, to look at
a multiplicity of variables. With this they are able to identify complex response profiles from
discrete response data.
Measures of association. The most common analytical methods for demonstrating
associations basically consist of comparing levels of morbidity or mortality among different
subgroups. This can be achieved either by comparing prevalence or by comparing incidence
rates or risks. Calculation of these measures of incidence or prevalence are discussed in depth
by Campbell and Graham (1990). Once these measures are calculated, analysis can consist of
straightforward comparisons between two groups or can involve more complex, n by n way
comparisons using cross-tabulations. For example, Fauveau et al. (1988) report that the
maternal mortality ratios for deaths from postpartum haemorrhage were 110, 90 and 230 per
100,000 live births for women aged 15-19, 20-34 and 35-44 years respectively. Alternatively,
multivariate techniques may be used to simultaneously adjust for the effects of many variables.
An alternative to directly comparing rates and risks is to calculate relative risks. This measure,
which is derived from cohort studies, involves looking at the ratio of two rates or risks, and

24
implies the relative likelihood of an outcome in a group with one characteristic compared to
another group with a different characteristic. For example, a prospective study of Navajo
women shows that women with cesarian-sections were four times more likely to develop
postpartum fever or endometritis than women having vaginal deliveries (Relative Risk=4.0)
(Slocumb and Kunitz, 1977). A third measure, the odds ratio (or relative odds), is calculated
from retrospective or cross-sectional studies. For instance, a case control study of ectopic
pregnancy found that in developing countries women who smoked were four times more likely
to have an ectopic pregnancy than non-smoking pregnant controls (OR=4.0) (Campbell and
Gray, 1987).
A fourth and final measure of association is the attributable risk. This measure is influenced by
the frequency of the determinant in the study population and describes the maximum proportion
of the disease that can be attributed to the determinant. One potential application of attributable
risk is with indirect morbidities; it should be possible to calculate the proportion of the disease
attributable to pregnancy in most settings.
4.3 Conclusion
This paper has reviewed the steps involved in measuring the determinants of maternal morbidity
and mortality. The first decision is frequently choosing the outcome and determining the
feasibility of measuring it. With maternal morbidity outcomes, this may be problematic since
these are less well-defined, infrequently studied, and require further methodological
development. The next step, choosing and measuring determinants, is simplified if the three
stages of pregnancy, morbidity, and mortality are kept in mind and it is recognized that the
overall impact of a determinant is the net effect of its influences on the risk of pregnancy,
morbidity and mortality. The distinction between causal determinants and risk indicators is
another useful step as it facilitates interpretation of results. Finally once outcomes and
determinants have been measured, it remains to demonstrate an association and thus show that a
factor is indeed a determinant of maternal morbidity or mortality. The most appropriate
methods to use depend on the type of study, the indicator and the study aims. Relative risks and
odds ratios can be derived from individual level data used to examine biologically causal
associations, while ecological methods are useful for generating hypotheses.
The sequence of steps involved in demonstrating an association presented above is an idealized
one. Often, opportunities for demonstrating associations are presented through routine data or
reanalysis of existing data. Such analyses are to be encouraged since data collection is costly
and data are frequently underutilized. Occasionally, natural experiments are created by changes
in factors which influence maternal health and these instances should also be exploited. For
example, Ekwempu et al. (1990) demonstrated the impact of structural adjustment programmes
on maternal health by looking at changes in the numbers of deliveries and complicated
deliveries after hospital charges were introduced. In other instances, study contexts limit
feasible designs and measuring and interpreting the determinants of maternal morbidity and
mortality require innovative methods.
Many authors express dissatisfaction with both the epidemiological focus and some socio-
economic approaches to studying health. The former only considers medical factors while the
latter either results in broad generalizations which act through a black box or makes very
specific observations which are only applicable in very specific contexts. It is increasingly

25
suggested that a proper understanding of health needs to harness social, economic behavioural
and cultural information and insights to address biomedical questions. Integration of socio-
economic and behavioural models with bio-medical models may be possible in looking at risk
indicators but as yet insights gained from disciplines outside epidemiology do not address
biological causality.

26
REFERENCES
AIREY, P. and CAMPBELL, O. (1988). Demographic and Health Surveys: a Critical
Assessment of the Health Component based on Six African Surveys. London School of
Hygiene and Tropical Medicine, Workshop on the Determinants of Health and Mortality in
Africa, 1 September 1988 - 26 October 1988.
AKIN, J.S. (1991). Estimating the impact of socioeconomic and biomedical factors on child
health - the Cebu study. The Health Transition: Methods and Measures. The Proceedings
of an International Workshop, London, 7-9 June 1989. Cleland J. and Hill A.G. eds.
Australian National University, Canberra.
BANG, R., BANG, A., BAITULE, M., CHOUDHARY, Y., SARMUKADDAM, S. and TALE,
O. (1989). High prevalence of gynaecological diseases in rural Indian women. Lancet i:
85-88.
BARETTO, T., CAMPBELL, O.M.R., DAVIES, J.L., FAUVEAU, V., FILIPPI, V.G.A.,
GRAHAM, W.J., MAMDANI, M., ROONEY, C.I.F. and TOUBIA, N.F. (1992).
Investigating induced abortion in developing countries: methods and problems. Submitted
to Studies in Family Planning.
BACKETT, E.M., DAVIES A.M. and PETROS-BARVAZIAN, A. (1984). The risk approach
in health care with special reference to maternal and child health, including family planning.
Public Health Papers No 76. Geneva: World Health Organization.
BERAL, V. (1985). Long term effects of childbearing on health. Journal of Epidemiological
Community Health 39: 343-346.
BHATIA, J.C. (1985). Maternal Mortality in Anantapur district India: preliminary findings of a
study. Interregional Meeting on Prevention of Maternal Mortality, Geneva, 11-17
November 1985. Document FHE/PMM/85.9.16. Geneva: World Health Organization.
BHATIA, J.C. (1986). A study of maternal mortality in Anantapur district, Andhra Pradesh,
India. (Unpublished)
BONGAARTS, J. AND POTTER, R.G. (1983). Fertility, Biology, and Behavior: An Analysis
of the Proximate Determinants. New York: Academic Press.
BOOTH, M, BERAL, V., and SMITH P.G. (1989) Risk factors for ovarian cancer- a case-
control study. British Journal of Cancer 60: 592-598.
BRIGGS, N.D. AND ORUAMABO, R.S. (1991). Technology-free obstetrics (letter). Lancet
337: 553.
BULATAO, R.A. AND LEE, R.D. (1983). An overview of fertility determinants in developing
countries. In: Determinants of Fertility in Developing Countries, eds. R.A.Bulatao and
R.D.Lee. New York: Academic Press.

27
CAMPBELL, O.M.R. (1983). Analysis of a Case Control Study of Ectopic Pregnancy:
Examination of Risk Factors, Control Selection Bias, and Diagnostic Validation. Sc.M.
thesis. Baltimore: The Johns Hopkins University.
CAMPBELL, O.M.R. and GRAHAM, W.J. (1990). Measuring maternal morbidity and
mortality: levels and trends. Maternal and Child Epidemiology Unit Research Paper No. 2.
London: London School of Hygiene and Tropical Medicine.
CAMPBELL, O.M.R. and GRAY, R.H. (1987). Smoking and Ectopic Pregnancy: A
Multinational Case-Control Study. Smoking and Reproductive Health Rosenberg M.J. ed.
Littleton: PSG Publishing Company Inc.
CAMPBELL O.M.R., ROONEY, C.I.F., FILIPPI, V.G.A. and GRAHAM, W.J. (1991).
Technology-free obstetrics (letter). Lancet, 337: 1095-1096.
CHEN, L.C., GESCHE, M.C., AHMED, S., CHOWDHURY, A.I. and MOSLEY, W.H.
(1974). Maternal mortality in rural Bangladesh. Studies in Family Planning 5(11): 334-341.
COCHRANE, S.H. (1979). Fertility and Education. What Do We Really Know? World Bank
Staff Occasional Papers, No. 26. Baltimore: Johns Hopkins University Press.
COTTON, P. (1990). Is there still too much extrapolation from data on middle-aged white
men? Journal of the American Medical Association, 263 (8): 1049-1055.
CROOK, N., RAMASUBBAN, R. and SINGH, B. (1991). A multi-dimensional approach to the
social analysis of the health transition in Bombay. The Health Transition: Methods and
Measures. The Proceedings of an International Workshop, London, 7-9 June 1989. Cleland
J. and Hill A.G. eds. Australian National University, Canberra.
DATTA, K.K., SHARMA, R.S., RAZACK, P.M.A., GHOSH, T.K. and ARORA, R.R. (1980).
Morbidity pattern amongst rural pregnant women in Alwar, Rajasthan-A cohort study.
Health and Population-Perspectives and Issues 3: 282-292.
DAVIS and BLAKE (1956). Social structure and fertility: an analytic framework. Economic
development and Cultural Change 4(4): 211-235.
FAUVEAU, V., KOENIG, M.A., CHAKRABORTY, J., and CHOWDHURY, A.I. (1988).
Causes of maternal mortality in rural Bangladesh, 1976-1985. Bulletin of the World Health
Organization. 66(5): 643-651.
FILIPPI, V.G.A, GRAHAM, W.J. and CAMPBELL, O.M.R. (1990). Utilizing Survey Data on
Maternity Care in Developing Countries: an Illustrative Study. Maternal and Child
Epidemiology Unit Research Paper No. 3. London: London School of Hygiene and Tropical
Medicine.
FINDLEY, S.E. (1989). Community, social structure and health: conceptual models of
influence. Health Transition Workshop, London, 7-9 April, 1989.
28
FORTNEY, J.A., SALEH, S., GADALLA, S. and ROGERS, S.M. (1984). Causes of death to
women of reproductive age in Egypt. Working Papers in Development No. 49, Office of
Women in International Development, Michigan State University.
GRAHAM, W.J. and AIREY, P. (1987). Measuring maternal mortality: sense and sensitivity.
Health Policy and Planning, 2(4), 323-333.
GRAHAM, W.J. and CAMPBELL, O.M.R. (1990). Measuring maternal health: defining the
issues. Maternal and Child Epidemiology Unit Research Paper No. 1. London: London
School of Hygiene and Tropical Medicine.
GRAHAM, W.J. and CAMPBELL, O.M.R. (1991) Measuring the effectiveness of maternal
health programmes. Maternal and Child Epidemiology Unit Research Paper. London:
London School of Hygiene and Tropical Medicine (forthcoming).
GRAHAM, W.J. and DANSO-MANU, M. (1988). Maternal depletion and maternal mortality:
a missing link? Paper prepared for the IUSSP African Population Conference, Dakar,
Senegal, November 7-12, 1988.
GREEN, A., BERAL, V. and MOSER, K. (1988). Mortality in women in relation to their
childbearing history. British Medical Journal 297: 391-395.
GRUBB, G.S., FORTNEY, J.A. SALEH, S., GADALLA, S., EL-BAZ, A., FELDBLUM, P.
and ROGERS, S.M. (1988). A comparison of two cause-of-death classification systems
for deaths among women of reproductive age in Menoufia, Egypt. International Journal of
Epidemiology 17: 201-207.
HARRISON, K.A. ed. (1985). Childbearing, health and social priorities: a survey of 22774
consecutive hospital births in Zaria. British Journal of Obstetrics and Gynaecology
(suppl.5).
HARRISON K.A. (1989a) Maternal mortality in developing countries. British Journal of
Obstetrics and Gynaecology 96(1): 1-3.
HARRISON K.A. (1989b). Maternal mortality in developing countries. British Journal of
Obstetrics and Gynaecology 96: 1119-1123.
HARRISON, K.A., BRIGGS, N.D., ORUAMABO, R.S. (1991). Technology-free obstetrics.
Lancet, 338: 382-383.
ISAACS, S., HOLT, R., and IRVIN, A. (1988). Assessing the status of women: A guide to
reporting using the convention on the elimination of all forms of discrimination against
women. International Women's Rights Action Watch. Columbia University, New York.
JEWETT, J.F. (1957). Changing maternal mortality in Massachusetts. New England Journal of
Medicine 256: 395-399.

29
KAUNITZ, A.M., SPENSE, C., DANIELSON, T.S., ROCHAT, R.W and GRIMES, D.A.
(1984). Perinatal and maternal mortality in a religious group avoiding obstetric care.
American Journal of Obstetrics and Gynaecology 150(7): 826-831.
KWAST, B.E. (1987). Roads to maternal death: case histories including comments on
preventative strategies. Safe Motherhood Conference. Nairobi 1987.
KWAST, B.E. AND LIFF, J.M. (1988). Factors associated with maternal mortality in Addis
Ababa, Ethiopia. International Journal of Epidemiology 17(1): 115-121.
LEAVITT, J.W. (1988). Joseph B DeLee and the practice of preventative obstetrics. American
Journal of Public Health 78(10): 1353-1360.
LESTHAEGHE, R.J., SHAH, I.H. and PAGE, H.J. (1981). Compensating changes in
intermediate fertility variables and the onset of natural fertility transition. In: Proceedings
of the IUSSP General Conference, Manila. Liège: Ordina.
LOUDEN, I. (1987). Puerperal fever, the streptococcus, and the sulphonamides, 1911-1945.
British Medical Journal 295: 485-490.
MacKIE, R.M., BUFALINO, R., MORABITO, A., SUTHERLAND, C., CASCINELLI, N.
(1991). Lack of effect of pregnancy on outcome of melanoma. Lancet 337: 653-655.
MAINE, D., WRAY, J. KAMARA, RAVAONOROMALALA, V. AND ROSENFIELD A
(1989). Maternal mortality in developing countries. British Journal of Obstetrics and
Gynaecology 96(1): 1119-1123.
MANTON, K.G., WOODBURY, M., DOWD, J.E. (1989). Methods to identify geographic and
social clustering of disability and disease burden. The Health Transition: Methods and
Measures. The Proceedings of an International Workshop, London, 7-9 June 1989. Cleland
J. and Hill A.G. eds. Australian National University, Canberra.
MOSLEY, H.W. and CHEN, L.C. (1984). An analytical framework for the study of child
survival in developing countries. In: Child Survival. Strategies for Research. H.W. Mosley
and L.C. Chen, eds. Population and Development Review. Supplement, Volume 10. New
York: Population Council.
MYNTTI, C. (1991). The anthropologist as a storyteller: picking up where others leave off in
public health research. The Health Transition: Methods and Measures. The Proceedings of
an International Workshop, London, 7-9 June 1989. Cleland J. and Hill A.G. eds.
Australian National University, Canberra.
NATHANSON, C.A. (1984). Sex differences in mortality. Annual Review of Sociology 10:
191-213.
OMRAN, A.R. and STANDLEY, C.C. (1978). Family Formation Patterns and Health.
Geneva: World Health Organization.

30
OMRAN, A.R. and STANDLEY, C.C. (1981). Family Formation Patterns and Health: Further
Studies. Geneva: World Health Organization.
PACQUE, M., MUNOZ, B., POETSCHKE, G., FOOSE, J., GYCERE, B.M. and TAYLOR,
H.R. (1991). Pregnancy outcome after inadvertent ivermectin treatment during
community-based distribution. Lancet 336: 1486-1489.
PAHO (1985). Health of Women in the Americas. Scientific publication no. 488. Pan
American Health Organization.
PEOPLES-SHEPS, M.D., KALSBEEK, W.D. and SIEGEL, E. (1988). Why we know so little
about prenatal care nationwide: an assessment of required methodology. Health Services
Research 23: 359-380.
PRESERN C. (1991). Urban basic services - a community profile. Lalitpur, Nepal.
REPRODUCTIVE MORBIDITY INTERDISCIPLINARY RESEARCH GROUP (1991).
Study on Reproductive morbidity in Rural Giza. Description of Study and Results of First
Phase of Analysis. Zurayk, H. ed.
ROSENFIELD, A. and MAINE, D. (1987). Maternal mortality - a neglected tragedy. Where is
the M in MCH? Lancet ii: 83-85.
SLOCUMB, J.C. AND KUNITZ, S.J. (1977). Factors affecting maternal mortality and
morbidity among American Indians. Public Health Reports 92(4): 349-356.
THADDEUS, S. AND MAINE, D. (1990). Too Far to Walk: Maternal Mortality in Context.
Prevention of Maternal Mortality Program, Center for Population and Family Health,
Columbia University.
VAN NORREN, B. and VAN VIANEN, H.A.W. (1986). The Malnutrition-Infections
Syndrome and its Demographic Outcome in Developing Countries. Publication Number 4.
The Hague: PCDO/Programming Committee for Demographic Research.
WASSERHEIT, J.N., HARRIS, J.R., CHAKRABORTY, J., KAY, B. and MASON, K.J.
(1989). Reproductive tract infections in a family planning population in rural Bangladesh:
an ignored opportunity to promote MCH-FP programs. Studies in Family Planning 20(2):
69-80.
WEIGEL, M.M. and WEIGEL, R.M. (1988). The association of reproductive history,
demographic factors, and alcohol and tobacco consumption with the risk of developing
nausea and vomiting in early pregnancy. American Journal of Epidemiology 127: 562-570.
WORLD HEALTH ORGANIZATION (1948). Constitution of the World Health Organization.
Geneva: World Health Organization.
WORLD HEALTH ORGANIZATION (1977). International classification of diseases. Manual
of the international statistical classification of diseases, injuries, and causes of death. Ninth
revision. Geneva: World Health Organization.

31
WORLD HEALTH ORGANIZATION (1986). Maternal mortality: helping women off the road
to death. WHO Chronicle, 40: 175-83.
WORLD HEALTH ORGANIZATION (1987). Safe Motherhood Initiative an information kit.
Geneva: World Health Organization.
WORLD HEALTH ORGANIZATION (1990a). The international conference for the tenth
revision of the International Classification of Diseases. World Health Statistics Quarterly
43: 204-245.
WORLD HEALTH ORGANIZATION (1990b). Measuring reproductive morbidity. Report of
a Technical Working Group, Geneva 30 August - 1 September 1989. Document
WHO/MCH/90.4. Geneva: World Health Organization.