Embed Size (px)
Citation preview

HAS - Medical, Economic and Public Health Assessmen t Division 1/26
The legally binding text is the original French ver sion
TTRRAANNSSPPAARREENNCCYY CCOOMMMMIITTTTEEEE Opinion
5 November 2014
BYETTA 5 µg, solution for injection in 1.2 ml pre-f illed pen B/1 (CIP: 34009 378 092 6 9) B/3 (CIP: 34009 378 093 2 0)
BYETTA 10 µg, solution for injection in pre-filled pen B/1 (CIP: 34009 378 094 9 8) B/3 (CIP: 34009 378 095 5 9)
Applicant: ASTRAZENECA
INN Exenatide
ATC code (2013) A10BX04 (Other blood glucose lowering drugs, excluding insulins)
Reason for the request
Extension of indication
Lists concerned National Health Insurance (French Social Security Cod e L.162-17) Hospital use (French Public Health Code L.5123-2)
Indication concerned “BYETTA as adjunctive therapy to basal insulin with metformin in adults who have not achieved adequate glycaemic control wi th these agents.”

HAS - Medical, Economic and Public Health Assessmen t Division 2/26
Actual Benefit Substantial in the treatment of type 2 diabetes as adjunctive therapy to basal insulin with metformin in adults who have not achie ved adequate glycaemic control with these agents.
Improvement in Actual Benefit
In combination with basal insulin and metformin in patients with type 2 diabetes inadequately controlled by these medicin es, taking into account the data available, namely a non-inferiority study of exenatide versus insulin lispro, BYETTA does not provide any improvement in actual benefit (level V, non-existent).
Therapeutic use
The BYETTA proprietory medicinal products are a tre atment alternative to rapid-acting insulin in patients starting triple th erapy including basal insulin and metformin, whose type 2 diabetes is inadequatel y controlled by these medicines, and who cannot tolerate or have contrain dications to Sulfonylureas or where insulin/metformin/Sulfonylur ea triple therapy has failed. Appropriate titration should first be carried out w ith the aim of normalising fasting blood glucose. This use requires specialist advice justifying treatment escalation in the management of type 2 di abetes.
HAS - Medical, Economic and Public Health Assessmen t Division 3/26
01 ADMINISTRATIVE AND REGULATORY INFORMATION
Marketing Authorisation (centralised)
Date of initial Marketing Authorisation: 20 November 2006 Extension of indication: 19 March 2012 Risk management plan + national monitoring
Prescribing and dispensing conditions / special status List I
ATC Classification
2013 A Alimentary tract and metabolism A10 Drugs used in diabetes A10B Blood glucose lowering drugs, excluding insulins A10BX Other blood glucose lowering drugs, excluding insulins A10BX04 Exenatide
02 BACKGROUND
The BYETTA proprietary medicinal products are currently reimbursed in the treatment of type 2 diabetes as dual therapy (with metformin or a Sulfonylurea) or as triple therapy (with metformin and a Sulfonylurea), in patients who have not achieved adequate glycaemic control at the maximum tolerated doses of these treatments (Committee opinion of 28 February 2007, substantial actual benefit and IAB IV in patients treated with a combination of metformin and Sulfonylurea in the management of type 2 diabetes). Exenatide, the active substance in BYETTA, is a glucagon-like peptide-1 (GLP-1) receptor agonist which stimulates insulin secretion in a glucose-dependent manner, inhibits glucagon secretion, delays gastric emptying and slows the absorption of glucose by the intestines. In a letter dated 2 July 2013, the Transparency Committee informed all pharmaceutical companies marketing incretins (gliptins and GLP-1 analogues) that it intended to re-assess actual benefit, improvement in actual benefit and target population for all these proprietary medicinal products, following reports of pancreatic conditions potentially linked to these medicines. Because of this, the Committee postponed the assessment of all pending applications, including this request for the inclusion of a new indication of BYETTA. At a meeting on 12 March 2014, the Committee's Bureau decided not to proceed with the re-assessment of incretins. In fact, on the basis of current knowledge and the available data from the literature considered by the FDA, EMA and ANSM, to date there is no evidence supporting a link between incretins and an increased risk of pancreatitis and pancreatic cancer. Nonetheless, these risks should still be monitored.1 These risks will be subject to increased pharmacovigilance follow-up, through clinical trials examining morbidity/mortality and through epidemiological studies, and the Committee will keep a close eye on these. This request concerns the inclusion of BYETTA in combination with basal insulin and metformin in adults who do not have adequate glycaemic control with these medicines on the lists for National Health Insurance and hospital use. The company is not seeking inclusion in the indications in combination with basal insulin without metformin (because combining a GLP-1 agonist with basal insulin alone currently has no role in the therapeutic strategy) and in combination with basal insulin and pioglitazone (because pioglitazone is no longer marketed in France).
1 Egan AG et al. Pancreatic safety of incretin-based drugs FDA and EMA assessment. N Engl J Med 2014; 370:794-7.

HAS - Medical, Economic and Public Health Assessmen t Division 4/26
03 THERAPEUTIC INDICATIONS
“BYETTA is indicated for treatment of type 2 diabetes mellitus in combination with: - metformin - Sulfonylureas - thiazolidinediones2 - metformin and a Sulfonylurea - metformin and a thiazolidinedione2 in adults who have not achieved adequate glycaemic control on maximally tolerated doses of these oral therapies. BYETTA is also indicated as adjunctive therapy to basal insulin with or without3 metformin and/or pioglitazone2 in adults who have not achieved adequate glycaemic control with these agents .”
04 DOSAGE
“BYETTA therapy should be initiated at 5 µg exenatide per dose administered twice daily (BID) for at least one month in order to improve tolerability. The dose of exenatide can then be increased to 10 µg BID to further improve glycaemic control. Doses higher than 10 µg BID are not recommended. BYETTA is available as either a 5 µg or a 10 µg exenatide per dose pre-filled pen. BYETTA can be administered at any time within the 60-minute period before the morning and evening meal (or two main meals of the day, approximately 6 hours or more apart). BYETTA should not be administered after a meal. If an injection is missed, the treatment should be continued with the next scheduled dose. BYETTA is recommended for use in patients with type 2 diabetes mellitus who are already receiving metformin, a Sulfonylurea, pioglitazone and/or a basal insulin. One can continue to use BYETTA when a basal insulin is added to existing therapy. When BYETTA is added to existing metformin and/or pioglitazone therapy, the current dose of metformin and/or pioglitazone can be continued as no increased risk of hypoglycaemia is anticipated, compared with metformin or pioglitazone alone. When BYETTA is added to Sulfonylurea therapy, a reduction in the dose of Sulfonylurea should be considered to reduce the risk of hypoglycaemia. When BYETTA is used in combination with basal insulin, the dose of basal insulin should be evaluated. In patients at increased risk of hypoglycaemia, consider reducing the dose of basal insulin. The dose of BYETTA does not need to be adjusted on a day-by-day basis depending on self-monitored glycaemia. However, blood glucose self-monitoring may become necessary to adjust the dose of Sulfonylureas or the dose of basal insulin. Special populations Elderly BYETTA should be used with caution and dose escalation from 5 µg to 10 µg should proceed conservatively in patients > 70 years. The clinical experience in patients > 75 years is very limited.
2 Obsolete indication; pioglitazone has not been marketed in France since July 2011. 3 The company is not seeking reimbursement in combination with basal insulin without metformin.

HAS - Medical, Economic and Public Health Assessmen t Division 5/26
Patients with renal impairment No dosage adjustment of BYETTA is necessary in patients with mild renal impairment (creatinine clearance 50 – 80 ml/min). In patients with moderate renal impairment (creatinine clearance 30-50 ml/min), dose escalation from 5 µg to 10 µg should proceed conservatively. BYETTA is not recommended for use in patients with end-stage renal disease or severe renal impairment (creatinine clearance < 30 ml/min). Patients with hepatic impairment No dosage adjustment of BYETTA is necessary in patients with hepatic impairment. Paediatric population The safety and effectiveness of exenatide have not been established in patients under 18 years of age.”
05 THERAPEUTIC NEED4,5,6,7
The aim of treatment in type 2 diabetes is to reduce morbidity and mortality, particularly through good glycaemic control. The short-term objectives are to improve symptoms (thirst, polyuria, asthenia, emaciation and blurred vision) and prevent acute complications (infections and hyperosmolar coma). The longer-term objectives are to prevent chronic microvascular complications (retinopathy, nephropathy and neuropathy) and macrovascular complications (myocardial infarction, strokes and obliterative arteriopathy of the legs) and to reduce mortality. According to the HAS guidelines (2013), the glycaemic target should be individualised depending on patient profile and can therefore change over time. Diabetes is progressive and all aspects of treatment should be re-assessed regularly: lifestyle and dietary measures, health education and drug treatment. Data from the literature cannot be used to define a lower limit for the HbA1c target. Once the target is achieved, treatment will be adjusted on a case-by-case basis. For most patients with type 2 diabetes, an HbA1c target ≤ 7% is recommended . Drug treatment should be initiated or re-assessed if the HbA1c is higher than 7%. Special cases: for patients newly diagnosed with diabetes, who have a life expectancy of more than 15 years and no history of cardiovascular events, a target of ≤ 6.5% is recommended, but this should be achieved by implementing or strengthening lifestyle and dietary measures then, if these fail, through oral monotherapy. In a certain number of special cases, the glycaemic target will be less demanding: age > 75 years; history of a macrovascular complication; chronic renal failure; proven serious comorbidity; limited life expectancy (< 5 years); long duration of diabetes (> 10 years); and patients in whom a target of 7% proves difficult to achieve because increased medication risks causing severe hypoglycaemia.
4 NICE (National Institute for Health and Clinical Excellence). NICE and diabetes: a summary of relevant guidelines. November 2009. 5 SIGN (Scottish Intercollegiate Guidelines Network). Management of diabetes - A national clinical guideline. Guideline 116. March 2010. 6 ADA (American Diabetes Association) and EASD (European Association for the Study of Diabetes). Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes: a patientcentered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012;35:1364-79. 7 Stratégie médicamenteuse du contrôle glycémique du diabète de type 2 [Drug strategy for glycaemic control of type 2 diabetes]. Recommandations de bonne pratique de la HAS [HAS good practice guidelines]. January 2013.
HAS - Medical, Economic and Public Health Assessmen t Division 6/26
Implementing effective lifestyle and dietary measures is a prerequisite to drug treatment for glycaemic control. Drug strategy: According to the HAS good practice guidelines (2013), the strategy generally recommended is: - metformin monotherapy, - then dual therapy with the combination metformin + Sulfonylurea. If the glycaemic target is not reached despite dual therapy with metformin + Sulfonylurea,
� if the difference from the HbA1c target is < 1%: triple therapy with metformin + Sulfonylurea + alpha-glucosidase inhibitors or DPP-4 inhibitors;
� if the difference from the HbA1c target is > 1%: add insulin in combination with metformin + Sulfonylurea or add a GLP-1 analogue as triple therapy, if BMI is ≥ 30 kg/m2 or if weight gain on insulin gives cause for concern.
In patients with elevated HbA1c levels (> 9.0%), dual therapy from the outset or insulin therapy can be offered as 1st-line treatment. Some patients do not achieve or maintain their glycaemic targets on insulin therapy alone. Combining insulin with another antidiabetic drug is recommended in these cases. In practice, it is metformin which is widely used for combinations with insulin.8 In the rare cases where metformin is contraindicated or not tolerated, Sulfonylureas should be offered. If the targets are not achieved with these dual therapies, the doses of insulin can be increased but this dose increase is often associated with a higher risk of hypoglycaemia and weight gain. In patients whose type 2 diabetes is inadequately controlled by basal insulin, the usual treatment intensification strategy acts on post-prandial blood glucose by adding one or more injections of rapid-acting insulin. At this stage in the disease, when fasting blood glucose is well controlled by basal insulin, post-prandial blood glucose actually makes a substantial contribution to elevated total blood glucose and elevated HbA1c.9,10 However, the treatment intensification strategy using several injections of rapid-acting prandial insulin is not always well accepted because it exposes patients to a greater risk of hypoglycaemia and weight gain. Therefore, the decision to intensify treatment is often postponed. GLP-1 receptor agonists are effective on glycaemic control with no additional risk of hypoglycaemia and beneficial effects on weight, and may be an alternative for intensifying basal insulin before resorting to multiple injections of rapid-acting insulin. This treatment alternative is a new strategy for the individualised management of patients whose type 2 diabetes is inadequately controlled by basal insulin alone. It is recognised in the most recent European and American guidelines, which state that the therapeutic strategy combining insulin with drugs that act on the incretin system, in particular combining insulin with a GLP-1 receptor agonist, can help some patients to achieve their target. These combinations are recommended before insulin regimens comprising several injections, which are considered to be more complex. In its guidelines, HAS states that combining a GLP-1 analogue with insulin requires specialist advice.
8 Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyperglycaemia in type 2 diabetes mellitus: a consensus algorithm for the initiation and adjustment of therapy: A consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 2009;52:17-30. 9 Riddle M. et al. Contributions of Basal and Postprandial Hyperglycemia Over a Wide Range of A1c Levels Before and After Treatment Intensification in Type 2 Diabetes. Diabetes Care 34:2508–2514, 2011 10 Monnier L. et al. Postprandial and Basal Glucose in Type 2 Diabetes: Assessment and Respective Impacts. Diabetes Technology & Therapeutics 2011; 13, Supplement 1: S25-S32
HAS - Medical, Economic and Public Health Assessmen t Division 7/26
Among the GLP-1 analogues, lixisenatide (LYXUMIA) is indicated in combination with insulin (under assessment by the Transparency Committee). As regards gliptins, linagliptin or sitagliptin are treatment options that can be added to the insulin + metformin combination in patients who do not achieve or maintain glycaemic targets on combined insulin and metformin.11,12 The role of saxagliptin in triple therapy, due to its poor efficacy and doubts over its safety profile, had not been defined by the Committee pending the re-assessment of all gliptins.13 Dapagliflozin, the 1st drug from the therapeutic category of sodium-glucose co-transporter 2 (SGLT2) inhibitors, is an additional treatment resource as triple therapy with insulin and metformin.14 Canagliflozin and empagliflozin are under assessment by the Committee.
11 Transparency Committee opinion for TRAJENTA 5 mg. 20 March 2013. Substantial actual benefit as triple therapy. 12 Transparency Committee opinion for JANUVIA 100 mg and JANUMET 50 mg/1,000 mg. 18 July 2012. Substantial actual benefit as triple therapy. 13 Transparency Committee opinion for ONGLYZA 5 mg. 15 May 2013 Low actual benefit as triple therapy. 14 Transparency Committee opinion for FORXIGA 10 mg. 23 April 2014. Moderate actual benefit as triple therapy.

HAS - Medical, Economic and Public Health Assessmen t Division 8/26
06 CLINICALLY RELEVANT COMPARATORS
06.1 Medicinal products
In patients whose type 2 diabetes is inadequately controlled by basal insulin, the usual treatment intensification strategy involves acting on post-prandial blood glucose by adding one or more injections of rapid-acting insulin to basal insulin. Medicines other than Sulfonylureas which are indicated in combination with insulin and metformin, when these together with diet and exercise do not provide adequate glycaemic control, are also given in the table below.
NAME (INN)
Company
Same TC* Yes / No Indications in combination with insulin and metform in** Date of
opinion AB IAB (Wording)
Reimbursed Yes/No
GLP-1 agonist LYXUMIA 10 µg, 20 µg, 10 µg/20 µg Solution for injection Lixisenatide Sanofi Aventis
Yes Treatment of adults with type 2 diabetes mellitus to achieve glycaemic control in combination with oral glucose-lowering medicinal products and/or basal insulin when these, together with diet and exercise, do not provide adequate glycaemic control.
Under assessment
- - No
DPP-4 inhibitors TRAJENTA 5 mg Film-coated tab. Linagliptin*** Boehringer Ingelheim
No In combination with insulin with or without metformin, when this regimen alone, with diet and exercise, does not provide adequate glycaemic control. 20/03/2013
Insufficient as dual therapy (+ insulin) Substantial as triple therapy (+ insulin + metformin)
V in treatment No
ONGLYZA 5 mg Film-coated tab. Saxagliptin*** AstraZeneca
No As combination therapy with insulin (with or without metformin), when this regimen alone, with diet and exercise, does not provide adequate glycaemic control.
15/05/2013
Insufficient as dual therapy (+ insulin) Low as triple therapy (+ insulin + metformin)
V in treatment Yes
JANUVIA/XELEVIA 25 mg, 50 mg Film-coated tab. Sitagliptin*** MSD
No As add-on to insulin (with or without metformin) when diet and exercise plus a stable dose of insulin do not provide adequate glycaemic control.
19/09/2012 Moderate as dual therapy (+ insulin) Insufficient in comb. with metformin
V in treatment
50 mg: yes
25 mg: no

HAS - Medical, Economic and Public Health Assessmen t Division 9/26
NAME (INN)
Company
Same TC* Yes / No Indications in combination with insulin and metform in** Date of
opinion AB IAB (Wording)
Reimbursed Yes/No
JANUVIA/XELEVIA 100 mg Film-coated tab. Sitagliptin*** MSD
No
As add-on to insulin (with or without metformin) when diet and exercise plus a stable dose of insulin do not provide adequate glycaemic control.
18/07/2012 Insufficient as dual therapy (+ insulin) Substantial as triple therapy (+ insulin + metformin)
- V in treatment
Yes
GALVUS/EUCREAS 50 mg, Tablet Vildagliptin*** Novartis
No In combination with insulin (with or without metformin) when diet and exercise plus a stable dose of insulin do not provide adequate glycaemic control.
Under assessment - - No in this
indication
VIPIDIA 6.25 mg, 12.5 mg, 25 mg, Film-coated tab. Alogliptin Takeda
No In combination with other glucose lowering medicinal products including insulin, when these, together with diet and exercise, do not provide adequate glycaemic control. 01/10/2014
Insufficient as dual therapy (+ insulin) Moderate as triple therapy (+ insulin + metformin)
-
V in treatment
No
Sodium -glucose co -transporter 2 (SGLT2) inhibitors FORXIGA 10 mg Film-coated tab. Dapagliflozin AstraZeneca
No In combination with other glucose-lowering medicinal products including insulin, when these, together with diet and exercise, do not provide adequate glycaemic control.
23/04/2014
Insufficient as dual therapy in addition to insulin Moderate as triple therapy (+ insulin + metformin)
- V in treatment No INVOKANA 100 mg,
300 mg, Film-coated tab. Canagliflozin Janssen
No Add-on therapy with other glucose-lowering medicinal products including insulin, when these, together with diet and exercise, do not provide adequate glycaemic control. 05/11/2014
JARDIANCE 10 mg Film-coated tab. Empagliflozin Boehringer Ingelheim
No In combination with other glucose-lowering medicinal products including insulin, when these, together with diet and exercise, do not provide adequate glycaemic control.
Under assessment
- - No
* Therapeutic category ** For other indications, see the SPC for the proprietary medicinal product *** Available as a fixed-dose combination with metformin
HAS - Medical, Economic and Public Health Assessmen t Division 10/26
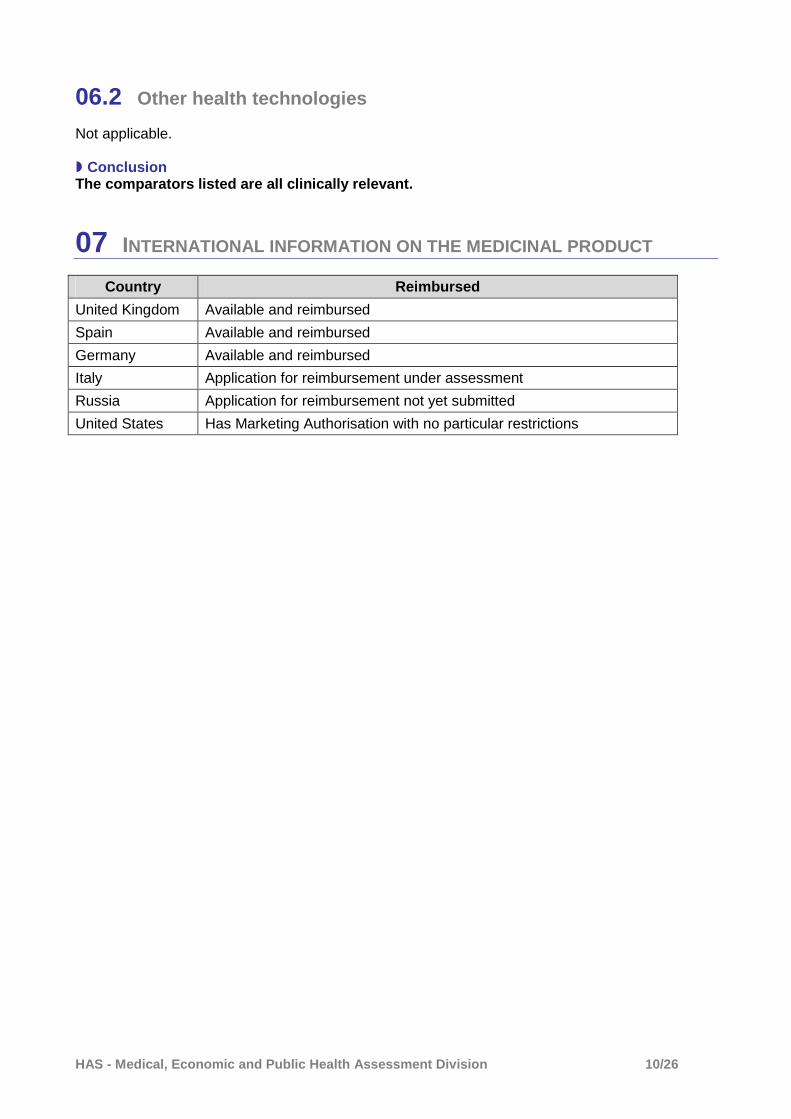
06.2 Other health technologies
Not applicable. � Conclusion The comparators listed are all clinically relevant.
07 INTERNATIONAL INFORMATION ON THE MEDICINAL PRODUCT
Country Reimbursed
United Kingdom Available and reimbursed
Spain Available and reimbursed
Germany Available and reimbursed
Italy Application for reimbursement under assessment
Russia Application for reimbursement not yet submitted
United States Has Marketing Authorisation with no particular restrictions

HAS - Medical, Economic and Public Health Assessmen t Division 11/26
08 SUMMARY OF PREVIOUS ASSESSMENTS
Date of opinion 28 February 2007 (inclusion)
Indication BYETTA is indicated for treatment of type 2 diabetes mellitus in combination with metformin and/or a Sulfonylurea in patients who have not achieved adequate glycaemic control on maximally tolerated doses of these oral therapies.
Actual benefit Type 2 diabetes is a chronic disease with potentially serious complications. BYETTA is used in the context of treatment for hyperglycaemia. The efficacy/adverse effects ratio for BYETTA is high. There are treatment alternatives to this proprietary medicinal product. BYETTA is an additional treatment resource for the management of type 2 diabetes patients. The actual benefit is substantial .
IAB
BYETTA provides a minor improvement in actual benefit (IAB IV) in the management of type 2 diabetes in patients treated with a combination of metformin and Sulfonylurea who have not achieved adequate blood glucose control at the highest tolerated doses of these treatments.
Studies requested The Transparency Committee requests that a study be set up on a representative sample of French type 2 diabetes patients treated with BYETTA. The aim of this study will be to describe the following aspects under actual treatment conditions: • the characteristics of the patients treated (including age, BMI and baseline HbA1c value) • the conditions for use of this proprietary medicinal product (indication, dosage and dose adaptations, concomitant treatments, blood glucose monitoring procedures, etc.) • the treatment maintenance rate • the frequency of discontinuations and the reasons for them • the change in HbA1c and weight, and the occurrence of hypoglycaemic episodes, in the long term (2 years). The duration of the study, to be determined by a scientific committee, should be duly justified, and it should be sufficient to answer the Transparency Committee's questions. If scheduled or ongoing studies, in particular within the scope of the European Risk Management plan, do not answer all the questions raised by the Transparency Committee, a specific study must be conducted.
HAS - Medical, Economic and Public Health Assessmen t Division 12/26
09 ANALYSIS OF AVAILABLE DATA
The company provided the results of: - a randomised, double-blind, parallel-group, placebo-controlled study15 aiming to evaluate
the efficacy and safety of exenatide as dual therapy (in combination with basal insulin) or as triple therapy (in combination with basal insulin and an oral antidiabetic drug: metformin or pioglitazone), in patients with type 2 diabetes inadequately controlled by basal insulin or by basal insulin in combination with an oral antidiabetic drug;
- an open-label, randomised, non-inferiority study16 versus insulin lispro, in patients with uncontrolled diabetes on insulin glargine + metformin.
The company also provided safety data from a non-inferiority study comparing the addition of insulin lispro protamine to the addition of insulin glargine in terms of glycaemic control in patients with type 2 diabetes poorly controlled by exenatide and OADs (metformin, metformin + Sulfonylurea or pioglitazone). As this study did not aim to evaluate exenatide, its results are not presented in this opinion.
09.1 Efficacy
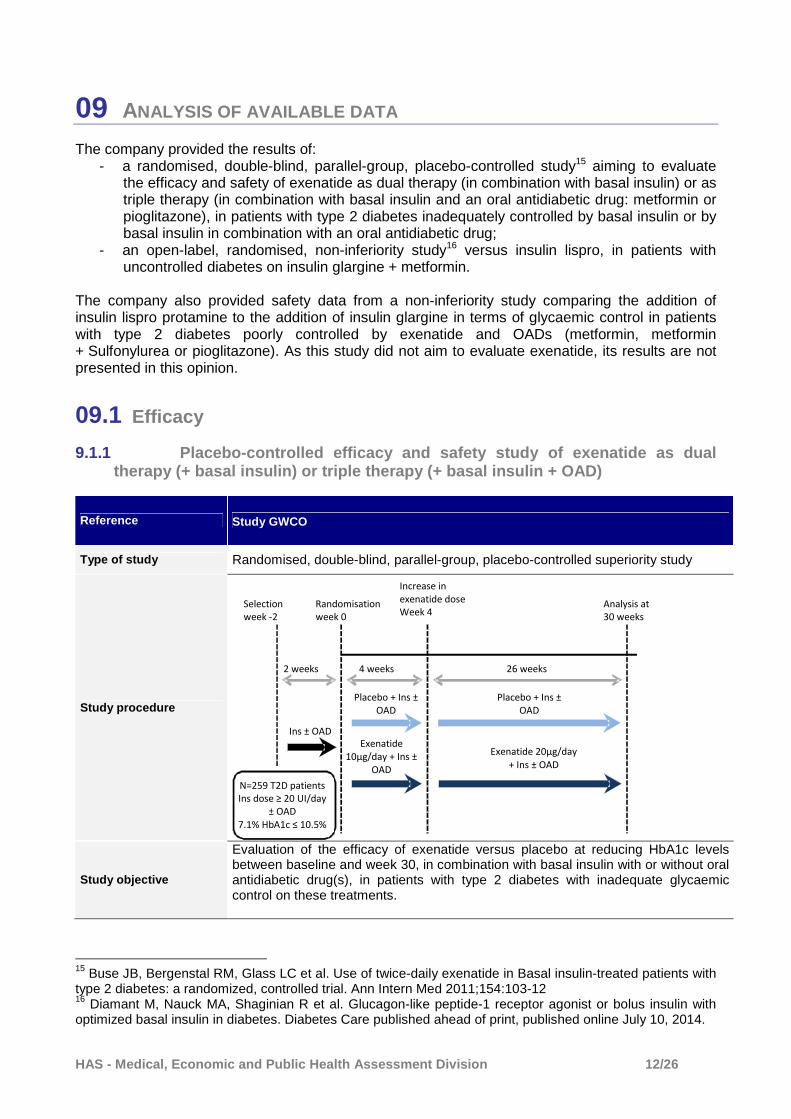
9.1.1 Placebo-controlled efficacy and safety study of exe natide as dual therapy (+ basal insulin) or triple therapy (+ basa l insulin + OAD)
Reference Study GWCO
Type of study Randomised, double-blind, parallel-group, placebo-controlled superiority study
Study procedure
Study objective
Evaluation of the efficacy of exenatide versus placebo at reducing HbA1c levels between baseline and week 30, in combination with basal insulin with or without oral antidiabetic drug(s), in patients with type 2 diabetes with inadequate glycaemic control on these treatments.
15 Buse JB, Bergenstal RM, Glass LC et al. Use of twice-daily exenatide in Basal insulin-treated patients with type 2 diabetes: a randomized, controlled trial. Ann Intern Med 2011;154:103-12 16 Diamant M, Nauck MA, Shaginian R et al. Glucagon-like peptide-1 receptor agonist or bolus insulin with optimized basal insulin in diabetes. Diabetes Care published ahead of print, published online July 10, 2014.
Analysis at
30 weeks
2 weeks 4 weeks 26 weeks
Placebo + Ins ±
OAD
Exenatide
10μg/day + Ins ±
OAD
Ins ± OAD
Randomisation
week 0
N=259 T2D patients
Ins dose ≥ 20 UI/day
± OAD
7.1% HbA1c ≤ 10.5%
Placebo + Ins ±
OAD
Selection
week -2
Exenatide 20μg/day
+ Ins ± OAD
Increase in
exenatide dose
Week 4
HAS - Medical, Economic and Public Health Assessmen t Division 13/26
METHOD
Main inclusion criteria
- Type 2 diabetes - Age ≥ 18 years - Stable weight for at least 3 months before inclusion and BMI ≤ 45 kg/m² - Poorly controlled diabetes, indicated by an HbA1c level ≥ 7.1% and ≤ 10.5% - Treatment with insulin glargine (≥ 20 IU/day) alone or in combination with an OAD
at a stable dose (metformin ≥ 500 mg/day, pioglitazone ≥ 15 mg/day or metformin + pioglitazone ≥ 500 mg/day and ≥ 15 mg/day respectively) for at least 6 weeks before inclusion)
Main non-inclusion criteria
Patients who received an OAD or insulin unauthorised in the study or a weight loss medicine for longer than one week in the 3 months prior to inclusion or for any duration in the month prior to inclusion. History of at least one major hypoglycaemic episode in the 6 months prior to starting treatment.
Study size and sites 59 centres in 6 countries (USA, Greece, Israel, Mexico, Puerto Rico, UK)
Products studied
1:1 randomisation to one of 2 groups, stratified by HbA1c level: ≤ 8.0% or ≥ 8.1%: - Exenatide: 5 µg x 2/day, then in week 4: 10 µg x 2/day. - Placebo administered subcutaneously
Patients continued to receive their metformin and/or pioglitazone treatment at the same doses as those administered before starting the study.
Primary efficacy endpoint Change in HbA1c level from baseline to week 30
Main secondary endpoints
- Proportion of patients achieving an HbA1c level ≤ 7% at 30 weeks - Analysis of change in blood glucose measured by the patient at 7 different times
during the day (7-point blood glucose) and in mean daily blood glucose based on these 7 measurements
- Change from baseline to week 30 in: o fasting blood glucose o weight o waist size o mean daily dose of insulin administered
Sample size
Based on an estimated lost to follow-up rate of 20%, to demonstrate a difference in HbA1c of 0.5% (standard deviation 1.1%) between the 2 groups in terms of change from baseline to week 30, with a threshold of 5% and a power of 90%, 260 randomised patients were required.
Results analysis method
All randomised patients who took the treatment at least once (modified ITT population). The main data analyses were performed using a mixed model for repeated measures. The LOCF17 method was used for secondary analyses. Seven analyses of change in HbA1c in subgroups of patients (defined by whether metformin treatment was combined with insulin, baseline HbA1c value, BMI, duration of diabetes, etc.), specified in the protocol, were performed. As no adjustment method was applied to take account of multiple comparisons, the possibility of an overestimation of the effect cannot be ruled out. Consequently, no conclusions can be drawn from these exploratory analyses, and they are therefore not presented.
Results A total of 261 patients were randomised (138 in the exenatide group and 123 in the placebo group). In each group, one patient left the study before receiving the treatment. Consequently, the analysis population consisted of 259 patients: 137 in the exenatide group and 122 in the placebo group. At 30 weeks, the study withdrawal rate was comparable in both groups (18.8% (n=26/138) in the exenatide group and 17.9% (n=22/123) in the placebo group). The most common reason was the occurrence of an adverse event in the exenatide group (9.4% of patients versus 0.8% in the
17 LOCF: Last observation carried forward

HAS - Medical, Economic and Public Health Assessmen t Division 14/26
placebo group) and the patient’s decision to stop treatment in the placebo group (8.9% of patients versus 5.1% in the exenatide group). On inclusion, patient characteristics were comparable in both groups, with the exception of sex, with significantly more women in the exenatide group, and the distribution of OAD treatments (metformin and/or pioglitazone), which differed between the two groups (Table 1). The mean patient age was 59 years. Table 1: Patient characteristics on inclusion
Exenatide (N=137)
Placebo (N=122)
Age (years) mean (SD) ≤ 65 years > 65 years
58.7 (8.9)
73.0% 27.0%
59.4 (10.0)
68.9% 31.1%
Sex, n (%)* Male Female
70 (51.1) 67 (48.9)
78 (63.9) 44 (36.1)
Weight (kg) mean (SD)
95.4 (20.4)
93.4 (21.2)
BMI (kg/m2) mean (SD)
33.8 (5.8)
33.1 (6.2)
Duration of diabetes (years) mean (SD) < 10 years ≥ 10 years
12.3 (6.9) 36.5% 63.5%
12.4 (7.1) 38.5% 61.5%
HbA1c (%) mean (SD) HbA1c ≤ 8% HbA1c > 8%
8.32 (0.85)
43.8% 56.2%
8.50 (0.96)
35.2% 64.8%
Fasting blood glucose (mmol/l) mean (SD) 7.28 (2.58) 7.49 (2.64) Mean daily dose of insulin (IU) mean (SD)
49.46 (29.88)
47.43 (25.38)
OAD treatment , n (%)* Metformin Metformin + pioglitazone Pioglitazone No OAD
91 (66.4) 23 (16.8) 21 (15.3)
2 (1.5)
91 (74.6) 8 (6.6)
17 (13.9) 6 (4.9)
* Significant difference between groups on inclusion
� Results for the primary efficacy endpoint: change in HbA1c at 30 weeks After 30 weeks of treatment, a greater reduction from baseline HbA1c levels was observed in the exenatide group than the placebo group: -1.71% versus -1.00% (mean difference between groups: -0.71%, 95% CI [-0.95; -0.47], p<0.001).

HAS - Medical, Economic and Public Health Assessmen t Division 15/26
Table 2: Change in HBA1c level (%) at 30 weeks
Exenatide Placebo
n/N 112/137 100/122
Baseline mean (SEM18) 8.33 (0.08) 8.54 (0.09)
Mean at week 30 (SEM) 6.70 (0.09) 7.41 (0.09)
Change from baseline, mean (SEM) -1.71 (0.09) -1.00 (0.09) Difference between treatments 95% CI p
-0.71 [-0.95; -0.47]
< 0.001 The results for change in HbA1c in the subgroup of patients treated with basal insulin and metformin cannot be used as they are based on an analysis which was not pre-specified in the protocol. Furthermore, the numbers in this subgroup are very low (75 patients in the exenatide group and 74 patients in the placebo group).
� Results for secondary endpoints at 30 weeks � Proportion of patients achieving HbA1c level ≤ 7%
After 30 weeks of treatment, a difference favouring exenatide over placebo was observed in the percentage of patients who achieved an HbA1c level ≤ 7% (67.6% vs 34.0%, p<0.001). Table 3: Proportion of patients with HbA1c ≤ 7% at 30 weeks
Exenatide Placebo
n/N 108/137 94/122
Patients with HbA1c ≤ 7%, n (%) 73 (67.6) 32 (34.0)
p < 0.001 � Change in fasting blood glucose
After 30 weeks of treatment, no difference between the 2 groups was demonstrated in change in fasting blood glucose. Table 4: Change in fasting blood glucose
Exenatide Placebo
Fasting blood glucose (mmol/l) , n/N 111/137 98/122
Baseline mean (SEM) 7.42 (0.2) 7.43 (0.2)
Mean at week 30 (SEM) 6.13 (0.2) 6.54 (0.2)
Change from baseline, mean (SEM) p
-1.28 (0.2) < 0.001
-0.87 (0.2) < 0.001
Difference between treatments 95% CI p
-0.41 [-0.99; 0.18]
0.174
18 Standard error of the mean

HAS - Medical, Economic and Public Health Assessmen t Division 16/26
� Analysis of change in 7-point self-monitored blood glucose Blood glucose was measured at 7 points during the day (before and after breakfast, lunch and dinner and once at 3 am). At 30 weeks, a difference favouring exenatide over placebo was observed in the reduction in blood glucose since starting treatment at 6 of the 7 points measured. No difference between the 2 groups was demonstrated in change in morning pre-prandial blood glucose. � Change in mean daily blood glucose
A difference favouring exenatide over placebo was observed in the change in mean daily blood glucose (measured at 7 points during the day) (mean difference between groups: -1.08 mmol/l, 95% CI [-1.55; -0.61]; p<0.001). � Change in weight
At 30 weeks, a difference favouring exenatide over placebo was observed in terms of weight loss (mean difference between groups: -2.74 kg, 95% CI [-3.74; -1.74]; p<0.001). � Change in waist size
After 30 weeks of treatment, no difference in reduction in waist size (LOCF) was demonstrated between the 2 groups (mean difference between the groups: -0.83 cm, NS). � Change in daily dose of insulin administered
After 30 weeks of treatment, no difference was found between the 2 groups in change from baseline daily dose of insulin administered, related to weight (mean difference between the groups: -0.05 IU/kg, 95% CI [-0.10; 0.00]; NS).
9.1.2 Non-inferiority study versus insulin lispro
Reference Study versus insulin lispro
Type of study Randomised, controlled, open-label non-inferiority study versus insulin lispro
Study procedure
Study with a duration of 44 weeks: - 2-week selection phase during which antidiabetic treatment was continued. - 12-week titration phase with daily fasting blood glucose measurements used
to adjust the insulin glargine dose (≥ 20 IU/day) and with Sulfonylurea treatments stopped.
- Patients with an HbA1c level > 7% during the 2 weeks preceding week 0 were randomised and entered the 30-week treatment phase.
Study objective
Comparison of change in HbA1c level from baseline to 30 weeks, on exenatide + basal insulin + metformin versus insulin lispro + basal insulin + metformin in type 2 diabetes patients with inadequate glycaemic control on basal insulin + metformin ± Sulfonylurea.
METHOD
Main inclusion criteria
- Type 2 diabetes - Age ≥ 18 years - BMI between 25.0 and 45 kg/m² - Poorly controlled diabetes, indicated by an HbA1c level ≥ 7.0% and ≤ 10.0% - Treatment with insulin glargine (≥ 20 IU/day) for at least 3 months combined with
metformin (minimum dose 500 mg/day) ± Sulfonylurea at a stable dose
Main non-inclusion criteria
Patients who have received an OAD or an insulin not authorised in the study Any medical history or concomitant treatment likely to interfere with the results
Study size and sites 108 centres in 17 countries including France (n=64 patients)
Products studied 1:1 randomisation to one of 2 groups, stratified by country and Sulfonylurea use: - Exenatide: 5 µg x 2/day, then in week 4: 10 µg x 2/day. Insulin glargine was
HAS - Medical, Economic and Public Health Assessmen t Division 17/26
reduced by 10% or more in patients with HbA1c ≤ 8.0%. - Insulin lispro 5 or 10 µg/day as 3 injections before meals. Insulin glargine
was reduced by 30% or 50% at the investigator’s discretion. The Sulfonylurea treatment was stopped on entering the titration phase. The metformin treatment was continued.
Primary efficacy endpoint Change in HbA1c level from baseline to week 30
Main secondary endpoints
- Proportion of patients achieving an HbA1c level ≤ 7% at 30 weeks - Proportion of patients achieving an HbA1c level ≤ 6.5% at 30 weeks - Proportion of patients achieving an HbA1c level ≤ 7% at 30 weeks with minimal
weight gain (≤ 1 kg) - Proportion of patients achieving an HbA1c level ≤ 6.5% at 30 weeks with minimal
weight gain (≤ 1 kg) - Change in weight from baseline to 30 weeks
Sample size
Based on an estimated lost to follow-up rate of 20%, a sample of 506 patients could demonstrate non-inferiority with a power of 96% (or 80%) and a non-inferiority margin of 0.4% (or 0.3%). Non-inferiority was demonstrated if the upper limit of the 95% confidence interval was below the non-inferiority margin, defined as 0.4% (or 0.3%).
Results analysis method The non-inferiority margin for HbA1c was 0.4%. If non-inferiority was demonstrated, a non-inferiority margin of 0.3% was tested. If non-inferiority was demonstrated, superiority was tested in the intention-to-treat population.
Results Out of 1,036 patients selected, 917 patients were included in the 12-week titration phase and 637 were randomised. A total of 627 patients received at least one dose of the study treatment (315 in the exenatide group and 312 in the insulin lispro group) (intention-to-treat population). The per-protocol population consisted of 510 patients (i.e. 80.1% of patients randomised): 247 patients (78.2%) in the exenatide group and 263 (81.9%) in the insulin lispro group. In total, 52 patients (16.5%) in the exenatide group stopped treatment versus 46 patients (14.3%) in the insulin lispro group. The most common reasons were the patient’s decision (5.7% in the exenatide group versus 9.0% in the insulin lispro group) or the occurrence of an adverse event (5.4% in the exenatide group versus 2.5% in the insulin lispro group). Table 5: Patient characteristics on inclusion (PP population)
Exenatide (N=247)
Insulin Lispro (N=263)
Age (years) mean (SD) 59.5 (9.6) 59.4 (9.3)
Sex, n (%)* Male
128 (52%) 133 (51%)
Weight (kg) mean (SD)
91.1 (16.6) 89.4 (17.0)
BMI (kg/m2) mean (SD) 32.7 (4.7) 32.3 (4.7)
Duration of diabetes (years) mean (SD)
12 (8-17) 11 (8-15)
HbA1c (%) mean (SD)
8.3 (0.98) 8.2 (0.87)
Fasting blood glucose (mmol/l) mean (SD)
7.1 (2.3) 7.1 (2.5)
Daily dose of insulin (IU), mean (SD) 61.5 (30.9) 61.1 (35.2) OAD treatment , n (%)* Metformin dose in mg/day Patients previously on a Sulfonylurea
2038 (633) 85 (34%)
1998 (648) 99 (38%)
� Results for the primary endpoint
At week 30, the change in HbA1c level from randomisation was -1.13 [-1.24,

HAS - Medical, Economic and Public Health Assessmen t Division 18/26
-1.03] in the exenatide group and -1.10 [-1.20, -1.00] in the insulin lispro group. Non-inferiority between exenatide and insulin glargine was demonstrated in the per-protocol population, in terms of change in HbA1c level from baseline, since the upper limit of the confidence interval was below the set margin of 0.4% or 0.3% with a difference of -0.04% [-0.18; 0.11] (NS). The results in the intention-to-treat population confirmed this finding. The superiority of exenatide to insulin lispro was not demonstrated, since the confidence interval included 0. At 30 weeks, the insulin glargine dose was 56.9 IU/day in the exenatide group and 93.7 IU/day in the insulin lispro group.
� Secondary endpoint results Exenatide
(N=247) Insulin Lispro
(N=263) HbA1c ≤ 7% HbA1c ≤ 6.5%
49.6% 26.2%
49.0% 25.5%
HbA1c ≤ 7% and weight gain ≤ 1 kg HbA1c ≤ 6.5% and weight gain ≤ 1 kg
44.6 [37.4, 50.2] 23.1 [17.6, 28.4]
22.9 [17.9, 28.4] 14.5 [10.4, 19.3]
Change in weight (kg) -2.5 (0.3) 2.1 (0.2)
09.2 Safety/Adverse effects
9.2.1 Data from the placebo-controlled clinical trial of the efficacy and safety of exenatide as dual therapy (+ basal insuli n) or triple therapy (+ basal insulin + OAD)
During the 30 weeks of the study, the mean exposure to the treatments was comparable between the two groups (183.2 ± 60.4 days in the exenatide group and 189.4 ± 52.7 days in the placebo group). The proportions of patients who had at least one adverse event (AE) were 79.6% in the exenatide group and 70.5% in the placebo group (Table 6). 5.8% of patients in the exenatide group versus 9.0% in the placebo group had at least one serious adverse event (SAE). A higher proportion of patients in the exenatide group:
- stopped treatment following an AE (8.0% versus 1.6%) - had an AE deemed by the investigator to be treatment-related (50.4% versus 20.5%) - had an AE deemed by the investigator to be related to type 2 diabetes (22.6% versus
10.7%). The majority of AEs were of mild to moderate intensity. No deaths were reported in the exenatide group, versus one death (myocardial infarction) in the placebo group.

HAS - Medical, Economic and Public Health Assessmen t Division 19/26
Table 6: General safety
Patients with at least one AE, n (%) Exenatide (N=137)
Placebo (N=122)
Total Treatment-related (evaluated by the investigator) Related to type 2 diabetes (evaluated by the investigator) Withdrawals due to AEs
109 (79.6) 59 (50.4) 31 (22.6)
11 (8.0)
86 (70.5) 25 (20.5) 13 (10.7)
2 (1.6)
Patients with at least one SAE, n (%) 8 (5.8) 11 (9.0)
Deaths 0 1 (0.8%)
Gastrointestinal events (nausea, vomiting and diarrhoea), headaches and dyspepsia were the most common AEs deemed to be treatment-related (> 5%) in patients on exenatide. Twelve patients in the exenatide group stopped treatment due to AEs (6 cases of nausea, 4 of vomiting, 1 of diarrhoea and 1 of headache) versus 2 patients in the placebo group (1 case of joint swelling and 1 of myocardial infarction). All other AEs had a comparable frequency in both treatment groups. Table 7: Distribution of AEs deemed to be treatment-related (> 5% in either group) – Number of patients (%)
Exenatide (N=137)
Placebo (N=122)
Nausea Vomiting Diarrhoea Dyspepsia Headache
47 (34.3) 21 (15.3) 15 (10.9)
7 (5.1) 9 (6.6)
9 (7.4) 2 (1.6) 3 (2.5) 2 (1.6)
0 Specific safety � Hypoglycaemia
“Minor hypoglycaemia” (reflecting symptoms of hypoglycaemia treated by patients themselves or resolving without action, associated with blood glucose < 3.0 mmol/l): 24.8% (n=34, 92 episodes) in the exenatide group and 28.7% (n=35, 82 episodes) in the placebo group. “Hypoglycaemic symptoms” (reflecting symptoms of hypoglycaemia not confirmed with a blood glucose measurement): 56.9% (n=23) in the exenatide group and 58.2% (n=22) in the placebo group. No cases of major hypoglycaemia (hypoglycaemic symptoms with loss of consciousness or seizure resolving rapidly after sugar or glucagon intake, documented hypoglycaemia [< 3.0 mmol/l] requiring intervention from a third party) were observed in the exenatide group, versus 1 patient (2 episodes) in the placebo group. � Abdominal pain
Fourteen AEs relating to abdominal pain (distension, discomfort, pain) were observed in the exenatide group and 10 in the placebo group. � Injection site events
Three AEs at the injection site (haematoma, irritation, local reaction) (2.2%) were reported in one patient from the exenatide group. � Oedema
Six cases of peripheral oedema were reported: 2 in the exenatide group and 4 in the placebo group. � Cancer
One patient (0.3%) in the placebo group had prostate cancer, not deemed by the investigator to be treatment-related.
HAS - Medical, Economic and Public Health Assessmen t Division 20/26
� Pancreatitis and acute renal failure
No cases were reported in this study.
9.2.2 Non-inferiority study versus insulin lispro
The proportion of patients with a treatment-related adverse event was higher in the exenatide group (72.4%, n=228) than in the insulin lispro group (56.1%, n=175). Gastrointestinal AEs (nausea, vomiting, diarrhoea) were more common in the exenatide group at 47% versus 13% in the insulin lispro group. Hypoglycaemia was less common in the exenatide group (29.5% versus 41.7% of patients), as was confirmed diurnal hypoglycaemia (15.2% versus 33.7%). The nocturnal hypoglycaemia rate was comparable (24.8% versus 26.6%). The serious adverse event rate was 5.7% in the exenatide group and 7.4% in the insulin lispro group. The rate of AEs resulting in treatment discontinuation was 5.4% (n=17) in the exenatide group and 2.6% (n=8) in the insulin lispro group. In the exenatide group, these were mostly nausea (2.9%, n=9) and vertigo (0.6%, n=2). 22.2% of patients (n=70) in the exenatide group had anti-exenatide antibodies (versus 2.6%, n=8 in the insulin lispro group).
9.2.3 PSUR data
� Summary of pharmacovigilance observations from the last available PSUR, covering the period from 1 April to 30 September 2012 (PSUR 15)
During the reporting period for this most recent PSUR, exposure to BYETTA was estimated at 133,500 patient-years, and exposure to exenatide (administered daily or weekly) at 160,300 patient-years. Overall exposure to BYETTA since it was first marketed was estimated at 2,267,000 patient-years, and exposure to exenatide (administered daily or weekly) at 2,300,300 patient-years. During the reporting period for this PSUR, a total of 1,573 notifications were received, including 283 considered to be serious. No changes regarding BYETTA’s safety were made to the SPC during the reporting period covered by this PSUR. No new pharmacovigilance signals were identified, particularly as regards events that are subject to special monitoring (see section 9.2.4 Risk management plan).
� Safety data from the cumulative analysis on 30 Sept ember 2012 regarding identified and potential risks that are subject to special mon itoring as part of the European RMP:
- Pancreatitis
The notification rate for cases of pancreatitis on exenatide, in any form, was 0.91 per 1,000 patient-years. In France, no cases of severe pancreatitis (necrotising, haemorrhagic or fatal) were reported during the period in question. A mechanistic study (H8O-EW-GWDP) aiming to explore the effects of exenatide on gallbladder motility and sphincter of Oddi tone did not demonstrate any significant difference versus placebo.
- Acute renal failure The notification rate for cases of acute renal failure on exenatide, in any form, was 0.32 per 1,000 patient-years. No new renal risks have emerged.
- Rapid weight loss (defined as weight loss greater than 1.5 kg in one week)

HAS - Medical, Economic and Public Health Assessmen t Division 21/26
A cumulative review of notified cases on BYETTA in the post-marketing period up until 31 March 2010 identified 17,632 cases of weight loss, of which 2% to 3% correspond to rapid weight loss.19 Following this observation, the safety data were updated in 2010 to emphasise this risk of rapid weight loss.
- Hypersensitivity reactions A relationship between the presence of antibodies, potentially linked to exenatide’s immunogenic nature, and injection site reactions is expected. A cumulative review of notified cases on BYETTA in the post-marketing period up until 31 March 2010 found a notification rate for cases of anaphylactic shock and/or reactions of 0.37 per 10,000 patient-years, confirming that such reactions are rare. None of the reactions reported were fatal or led to significant complications.
- Cardiovascular events Two cumulative analyses of cardiac events occurring on BYETTA, undertaken for PSURs (up to 30 September 2007 and up to 31 March 2009), did not show any increased incidence in these events in patients treated with exenatide compared with other treatment groups or to the general type 2 diabetes population, based on epidemiological data. The most commonly reported cardiovascular events are known complications of diabetes and probably relate to the natural progression of type 2 diabetes. Most fatal cases occurred in patients with a history of heart disease and/or significant risk factors. There are no significant worrying signals in the data available to date.
- Pancreatic cancer and thyroid tumours The notification rate for cases of pancreatic cancer was 0.09 per 1,000 patient-years and the rate for thyroid tumours was 0.03 per 1,000 patient-years. No new clinically significant information on these risks has emerged.
9.2.4 SPC data
According to the SPC, “The most frequent adverse reactions were mainly gastrointestinal related (nausea, vomiting and diarrhoea). The most frequently reported single adverse reaction was nausea which was associated with the initiation of treatment and decreased over time. Patients may experience hypoglycaemia when BYETTA is used with a Sulfonylurea. Most adverse reactions associated with BYETTA were mild to moderate in intensity. Acute pancreatitis and acute renal failure have been reported rarely since exenatide twice daily has been marketed.”
9.2.5 Risk management plan
The European RMP includes: - identified risks: pancreatitis, acute renal failure and rapid weight loss (> 1.5 kg per week); - potential risks: risks associated with the development of anti-exenatide antibodies (more
specifically anaphylactic reactions), cardiovascular events, pancreatic cancer, thyroid tumours, and malignant tumours following concomitant use of an insulin;
- missing information: adolescents, pregnancy, very elderly patients (≥ 75 years), combination with other antidiabetic drugs (insulins).
9.2.6 National monitoring
In France, as an extension to the European RMP, the French National Agency for Medicines and Health Products Safety (ANSM) has set up a national monitoring programme for incretin mimetics.
19 RMP version 20
HAS - Medical, Economic and Public Health Assessmen t Division 22/26
In this context, the Pharmacovigilance Technical Committee20 (TC) has reiterated that “Diabetes is a disease with an increased risk of pancreatitis or pancreatic cancer. Following the publication by Butler et al.21 in March 2013, which demonstrates, in a very limited series of autopsies, pancreatic alpha-cell and beta-cell hyperplasia with cellular proliferation in the pancreases of diabetic patients treated with incretins versus non-diabetic subjects or patients treated with other drugs, an arbitration procedure in accordance with article 5.3 was initiated at European level in order to assess all preclinical, clinical trial and pharmacovigilance data on the risk of pancreatitis and pancreatic cancer. Regarding the risk of pancreatic cancer, as there was no sufficiently robust scientific evidence, the addition of the word “cancer” to the SPC was not accepted by the members of the Technical Committee. We are awaiting morbidity, mortality and cardiovascular safety results from long-term studies, and comprehensive pancreatic safety data must be added to this.”
09.3 Usage/prescription data
For information, according to the IMS panel (moving annual total, spring 2014), 45,753 prescriptions were issued for the proprietary medicinal product BYETTA (exenatide administered twice daily), including:
- 76% in combination with a biguanide, - 46% in combination with a Sulfonylurea, - 27% in combination with an insulin and slow-acting analogue, - 18% in combination with an insulin and rapid-acting analogue.
09.4 Summary & discussion
In the indication as triple therapy in combination with insulin and metformin (for which the company is seeking inclusion), the available data come from 2 studies: - A randomised, placebo-controlled, double-blind, parallel-group study which evaluated the efficacy and safety of exenatide as dual therapy (in combination with basal insulin) or as triple therapy (in combination with basal insulin and an oral antidiabetic drug, either metformin or pioglitazone), in patients with type 2 diabetes inadequately controlled by basal insulin (± an oral antidiabetic drug). This study included 137 patients in the exenatide group and 122 in the placebo group. The Committee is astounded by the low numbers of type 2 diabetes patients included in this multicentre study. Because of this, only 91 patients included in each group (66.4% in the exenatide group and 74.6% in the placebo group) had inadequately controlled diabetes on metformin and insulin. It should be noted that 16.8% of patients in the exenatide group received combined pioglitazone + metformin (versus 6.6% in the placebo group), a non-recommended quadruple therapy. 15.3% of patients in the exenatide group (versus 13.9% in the placebo group) took pioglitazone together with insulin (a non-recommended combination). Therefore, the population included in this study was heterogeneous in terms of treatment received, making the results difficult to interpret. The Committee notes that in this study there were substantial differences between the numbers of patients included, and the numbers from which the primary efficacy and secondary endpoint results were calculated. After 30 weeks of treatment, in the overall study population (patients on dual therapy and triple therapy), a reduction in HbA1c levels from baseline was observed in both groups and was
20 ANSM. Réunion du Comité technique de pharmacovigilance [Meeting of the Pharmacovigilance Technical Committee] – CT012013043. 18 June 2013. 21 Marked Expansion of Exocrine Pancreas with Incretin Therapy in Humans with Increased Exocrine Pancreas Dysplasia and the Potential for Glucagon-Producing Neuroendocrine Tumors. Diabetes. March 2013.

HAS - Medical, Economic and Public Health Assessmen t Division 23/26
significantly greater in the exenatide group (mean difference between the groups: -0.71%, 95% CI [-0.95; -0.47], p<0.001). No solid conclusions can be drawn from the change in HbA1c levels in the subgroup of patients treated with basal insulin and metformin in this study, because these results come from an analysis that was not pre-specified in the protocol and involve a small number of patients. At 30 weeks, the study withdrawal rate was comparable in both groups. The most common reason was the occurrence of an adverse event in the exenatide group (9.4% of patients versus 0.8% in the placebo group) and the patient’s decision to stop treatment in the placebo group (8.9% versus 5.1% in the exenatide group). This reason, “the patient’s decision”, is vague. The proportions of patients who had at least one adverse event (AE) were 79.6% in the exenatide group and 70.5% in the placebo group. 5.8% of patients in the exenatide group versus 9.0% in the placebo group had at least one serious adverse event (SAE). A higher proportion of patients in the exenatide group:
- stopped treatment following an AE (8.0% versus 1.6%) - had an AE judged by the investigator to be treatment-related (50.4% versus 20.5%) - had an AE judged by the investigator to be related to type 2 diabetes (22.6% versus
10.7%). The majority of AEs were of mild to moderate intensity. Gastrointestinal events (nausea, vomiting and diarrhoea), headaches and dyspepsia were the most common AEs deemed to be treatment-related (> 5%) in patients on exenatide. - An open-label, randomised, non-inferiority study of exenatide versus insulin lispro which included patients with type 2 diabetes treated with insulin glargine and metformin (with or without a Sulfonylurea) with an HbA1c between 7% and 10%. After a 2-week selection phase, patients entered a 12-week titration phase and were then randomised between the exenatide and insulin lispro groups. A total of 637 patients were randomised. The per-protocol population consisted of 510 patients (i.e. 80.1% of patients randomised): 247 patients in the exenatide group and 263 in the insulin lispro group. Patients had had diabetes for more than 10 years. The HbA1c was 8.3% in the exenatide group and 8.2% in the insulin lispro group. On inclusion, the mean daily doses of insulin glargine were 61.5 IU/day in the exenatide group and 61.1 IU/day in the insulin lispro group. At 30 weeks, the insulin glargine dose was 56.9 IU/day in the exenatide group and 93.7 IU/day in the insulin lispro group. The mean metformin dose was 2 g/day in each group. Non-inferiority between the insulin glargine/metformin/exenatide combination and the insulin glargine/metformin/insulin lispro combination was demonstrated at 30 weeks in the per-protocol population, in terms of change in HbA1c level from baseline, since the upper limit of the confidence interval was below the set margin of 0.4% or 0.3% with a difference of -0.04% [-0.18; 0.11]. These results were confirmed in the intention-to-treat population. The patients included had type 2 diabetes that was not controlled by dual therapy with insulin glargine (high dose) and metformin (2 g/day mean dose), i.e. a treatment intensification strategy for insulin therapy. More than 30% of patients were also treated with a Sulfonylurea, which was stopped on starting the titration phase. Patients in the exenatide group lost weight, whereas patients in the insulin lispro group gained weight (a secondary endpoint). The proportion of patients with a treatment-related adverse event was higher in the exenatide group (72.4%, n=228) than in the insulin lispro group (56.1%, n=175). Gastrointestinal AEs (nausea, vomiting, diarrhoea) were more common in the exenatide group (47% versus 13%). Hypoglycaemia was less common in the exenatide group (29.5% versus 41.7% of patients), as was confirmed diurnal hypoglycaemia (15.2% versus 33.7%). The nocturnal hypoglycaemia rate was comparable (24.8% versus 26.6%). 22.2% of patients (n=70) in the exenatide group had anti-exenatide antibodies (versus 2.6%, n=8 in the insulin lispro group).

HAS - Medical, Economic and Public Health Assessmen t Division 24/26
No morbidity/mortality data are available.
09.5 Planned studies
The studies currently taking place, included in the RMP,Erreur ! Signet non défini. are: - A pharmacoepidemiological study (H8O-MC-B015) in the United States, to evaluate the
relative/absolute risk of pancreatic/thyroid cancer in patients with type 2 diabetes starting treatment with exenatide administered twice daily, in comparison with other antidiabetic treatments (including insulin).
- An efficacy and safety study (GWBQ) in adolescents with type 2 diabetes (ongoing study-final report expected in 2017).
During its assessment of the application for inclusion, the Committee requested that a study be set up on a representative sample of French type 2 diabetes patients treated with BYETTA. This study would aim to describe, in the current clinical context: - the characteristics of the patients treated (including age, BMI and HbA1c value on starting treatment); - the conditions under which this proprietary medicinal product is used (indication, dosage and dose adjustments, concomitant treatments, methods used to monitor blood glucose, etc.); - the treatment maintenance rate; - the treatment discontinuation rate and reasons; - changes to HbA1c and weight, as well as the long-term (2-year) incidence of hypoglycaemia. The final report from this study has been submitted and will be examined by the Transparency Committee during the renewal of inclusion for the BYETTA proprietary medicinal products.

HAS - Medical, Economic and Public Health Assessmen t Division 25/26
010 THERAPEUTIC USE
The BYETTA proprietary medicinal products are a treatment alternative to rapid-acting insulin in patients starting triple therapy including basal insulin and metformin, whose type 2 diabetes is inadequately controlled by these medicines, and who cannot tolerate or have contraindications to Sulfonylureas or where insulin/metformin/Sulfonylurea triple therapy has failed. Appropriate titration should first be carried out with the aim of normalising fasting blood glucose. This use requires specialist advice justifying treatment escalation in the management of type 2 diabetes.
011 TRANSPARENCY COMMITTEE CONCLUSIONS
In view of all the above information, and following the debate and vote, the Committee’s opinion is as follows:
011.1 Actual benefit
� In triple therapy in combination with insulin and m etformin
� Type 2 diabetes is a chronic disease with potentially serious complications, particularly cardiovascular complications. � BYETTA is used in the context of treatment for hyperglycaemia. � The efficacy/adverse effects ratio for BYETTA, in triple therapy in combination with insulin and metformin, is high. � The BYETTA medicinal products are a treatment alternative to rapid-acting insulin in patients starting triple therapy including basal insulin and metformin, whose type 2 diabetes is inadequately controlled by these medicines, and who cannot tolerate or have contraindications to Sulfonylureas or where insulin/metformin/Sulfonylurea triple therapy has failed. � There are treatment alternatives to this proprietary medicinal product.
� Public health benefit: The public health burden of type 2 diabetes is substantial because of its high prevalence, which is constantly increasing, and the associated microvascular and macrovascular complications. The public health burden in the subpopulation of patients for whom BYETTA is indicated as triple therapy in combination with insulin and metformin is considered to be moderate. Improving the therapeutic management of type 2 diabetes patients is a public health need which is an established priority. The proprietary medicinal product BYETTA is unlikely to benefit public health in this extension of indication as triple therapy in combination with insulin and metformin, as there is no additional impact on public health criteria (morbidity/mortality data, improved quality of life) compared with the current treatment of type 2 diabetes. Consequently, BYETTA is not expected to have any impact on public health.
Consequently, the Committee considers that the actu al benefit of BYETTA in combination with basal insulin and metformin, in adults who do not have adequate glycaemic control on these medicines, is substantial.

HAS - Medical, Economic and Public Health Assessmen t Division 26/26
The Committee recommends inclusion on the list of m edicines refundable by National Health Insurance and on the list of medicines appro ved for hospital use in this extension of the indication and at the dosages in the Marketing Authorisation. � Proposed reimbursement rate: 65%
011.2 Improvement in actual benefit (IAB)
In combination with basal insulin and metformin in patients with type 2 diabetes inadequately controlled by these medicines, taking into account the data available, namely a non-inferiority study of exenatide versus insulin lispro, BYETTA does not provide any improvement in actual benefit (level V, non-existen t).
011.3 Target population
The target population for BYETTA in its extension of indication consists of patients with type 2 diabetes inadequately controlled by basal insulin and metformin at optimal doses, who cannot tolerate or have contraindications to Sulfonylureas or where insulin/metformin/Sulfonylurea triple therapy has failed. The most recent French epidemiological data, from the “Diabetes Atlas” report published by the International Diabetes Federation and from National Health Insurance data, estimate the prevalence of diabetes at 3.5 million people in France, of whom 2.9 million are treated pharmacologically (4.4% of the general population in 2009). With an estimated annual growth rate of 4.7% in the population with treated diabetes (general scheme only), 3.33 million people would be affected in 2012. Furthermore, data extracted from the ENTRED 2007-2010 study show that type 2 diabetes is the most common form and accounts for 91.9% of patients with diabetes (i.e. 3.06 million people treated for type 2 diabetes). The ENTRED study showed that about 17% of patients treated for type 2 diabetes took insulin. Furthermore, the ECODIA 2 study showed that 61% of patients on insulin therapy were treated with a combination of insulin + OAD and that 40% of these patients were inadequately controlled. Table 8: Summary of epidemiological data used to assess the target population for BYETTA
Population considered Number Source
Patients with diabetes 3.50 million International Diabetes Federation
Patients with treated diabetes 3.33 million National Health Insurance
Patients with type 2 diabetes 3.06 million ENTRED
Patients treated with basal insulin therapy (17% of type 2 diabetics) 520,200 ENTRED
Patients treated with insulin + OAD (61%) 317,322 ECODIA 2 study
Subpopulation inadequately controlled (HbA1c > 8%) by basal insulin + OAD treatment (40%) 126,929
Estimate For this extension of indication, the target popula tion for BYETTA falls within a population of about 127,000 patients with type 2 diabetes inad equately controlled by treatment with basal insulin and an oral antidiabetic drug.


![Bericht zu PM10-Tagesmittelwerten und Überschreitungen …...28.04.2011 PM10 [µg/m³] 1 58 05.11.2011 PM10 [µg/m³] 5 62 12.11.2011 PM10 [µg/m³] 3 102 23.11.2011 PM10 [µg/m³]](https://img.pdfslide.net/doc/110x75/5feb2fd0c3ceb232dc68d90f/bericht-zu-pm10-tagesmittelwerten-und-oeberschreitungen-28042011-pm10-gm.jpg)





![[Product Monograph Template - Standard] - Novartis...Page 1 of 60 PRODUCT MONOGRAPH PrSANDOSTATIN® (Octreotide acetate Injection) 50 µg/ mL, 100 µg/ mL, 200 µg/ mL, 500 µg/ mL](https://img.pdfslide.net/doc/110x75/5ea993fd17e967737b0c06c0/product-monograph-template-standard-novartis-page-1-of-60-product-monograph.jpg)




















