Embed Size (px)
Citation preview

Opioid Stewardship Committee: A Multimodal ApproachKYLE E ICHELBERGER, PHARMD, BCPS
LAWRENCE MEMORIAL HOSPITAL
LAWRENCE, KANSAS A partner for lifelong health
1

Objectives:Identify leading strategies for developing an opioid stewardship committee
Review opioid stewardship goals and recommendations
Establish and evaluate metrics to measure opioid stewardship
Share LMH Health’s opioid stewardship committee initiatives
Review of use of multimodal pain management
Discuss factors that help/hinder an Opioid Stewardship Program
2

Opioid Stewardship Program Overview:•March 2018: LMH joined Vizient’s Opioid Stewardship Collaborative
•May 2018: Attended Mid-America Improvement Leader Network in St. Louis
•May 2018: Created Opioid Stewardship Committee
•Resources:◦ Joint Commission Standards◦ National Quality Partners Playbook: Opioid
Stewardship◦ CDC Opioid Prescribing Guidelines
3

LMH Opioid Stewardship Goals•Optimize pain management pharmacotherapy
•Minimize opioid associated adverse events and cost
•Promote education on safe opioid prescribing, administration, and patient monitoring
•Develop opioid stewardship metrics for assessment
•Enhance patient experience regarding opioid utilization and understanding
4

NQP Opioid Stewardship PlaybookFundamental Actions:
1. Leadership Commitment and Culture2. Organizational Policies3. Clinical Knowledge, Expertise, and Practice4. Patient and Family Caregiver Education and
Engagement5. Tracking, Monitoring, and Reporting6. Accountability7. Community Collaboration
5

Vizient Collaborative Project Focus Distribution
Source: Lichauer, Jim. Implementation of an Opioid Stewardship Program Collaborative Knowledge Transfer Webinar. Presented March 4, 2019. https://amc.vizientinc.com/pages/35362. Accessed on April 24, 2019.
6

1. Leadership Commitment and Culture
Create the infrastructure for formal opioid stewardship program
Receive buy-in from the board of directors
Include opioid stewardship in the annual operating plan
Integrate opioid stewardship into organizational patient safety plan
Establish new ways to assess and treat pain
Disconnect opioid prescribing and patient satisfaction
Destigmatize substance abuse disorder
ACTION Established Opioid Stewardship Committee Executive sponsor Chair members Physician champions
Reported OSC projects to administration and board members
Devoted time and resources to OSC goals IT/Data Analyst New technology/tools Physician representation
RECOMMENDATIONS
7

Opioid Stewardship Committee Composition
•Pharmacy
•Orthopedic Physician
•Pain Management Physician
•Primary Care Physician
•Anesthesiologist
•Hospitalist
•Pelvic Health Specialist
•Emergency Medicine Physician
•Emergency Department Director
•Data Analytics
•Pain Team Chair/OB Clinical Coordinator
•Executive Representative: Clinical Excellence Vice President
•Clinical Excellence Manager
•Application Integration Director (IT)
•Integration Engineering Manager (IT )
•Pain Clinic Nurse
•Pain/Palliative Care Nurse Practitioner
•Risk Management
•Director of Primary Care
•Care Coordination Director
•Outpatient Social Worker
•Director of Integrated Crisis Team
•PACU Director
•PACU Nursing Manager
•Operational Excellence
•Primary Care Nurse Practitioner
8

2. Organizational PoliciesRECOMMENDATIONS
Promote current pain management services
Implement a functional pain scale and opioid risk tools
Standardize the use of the state’s PDMP
Implement naloxone dispensing policy targeting specific patient populations
Establish a formal partnership with local treatment facilities for MAT
ACTION
ED Opioid Prescribing Policy New Opioid Risk Tool (ORT) New Pain Assessment CAPA replaced Numeric Pain Scale
Utilizing Cerner’s Opioid Toolkit Tracking Recommendations
Pain Management Services Drug Take-back options Naloxone Recommendations
9

3. Clinical Knowledge, Expertise, and Practice
Implement inpatient pain orders for opioid naive pain and opioid tolerant patients Expand non-pharmacologic pain management modalities Develop core competencies for pain management Standardize pain assessment tools Develop a pain comfort menu Implement a respiratory suppression scale Create alerts to identify high-risk patients, identify high-dose prescribing and high-risk combinations
Create a tiered-system guideline of discharge opioid prescriptions
Educate prescribers about multimodal analgesia
Support consistent use of PDMP for all prescribers
Develop standardized risk assessment tool and referral network for OUD
Establish a standardized naloxone program for high risk patients
10

3. Clinical Knowledge, Expertise, and Practice
Multimodal Pain Management Total Joint Replacement Hysterectomy C-sections Spinal fusions Laminectomies ALTO in ED Universal Multimodal order-set
Integration of PDMP (KTRACs) in EHR
Screening and referral for OUD
Naloxone recommendation
Clinical Training/Education: Opioid stewardship Pain Management Communication techniques Tapering Psychosocial aspects of pain (stress, anxiety,
depression)
11

Medical Staff Education•Provided information about UDS drug screens available at LMH and send-out options for pain agreement patients
•Developed computer-based learning program for physicians using CDC guidelines
•Palliative care and pain specialist helping to developing CME lecture
•Wrote MedStaff Newsletter detailing recent restrictions to opioid prescribing• Including Medicaid, Wal-Mart, BCBS,
UnitedHealthCare
12

Multimodal Pain Management: Purpose
To examine the safety and efficacy of a multimodal pain
management strategy for total joint replacement
patients
13

Multimodal Pain Management: Background•With current opioid epidemic, providers and healthcare agencies have searched for alternatives to opioids to manage pain and reduce patient harm
•2012 ASIPP:• Opioid use accompanied by increasing fatalities and
adverse consequences, and a lack of evidence regarding effectiveness and safety
•2016 American Pain Society:• recommend acetaminophen and/or NSAIDs as part
of multimodal analgesia for management of postoperative pain
• recommend use of gabapentin or pregabalin as a component of multimodal analgesia
•2018 AANA:• Pre-medicating patients with acetaminophen,
gabapentinoids, NSAIDs, and corticosteroids decreased postoperative pain, length of stay, and opioid use
14

Multimodal Pain Management: Objectives◦ Primary Outcome:
◦ Measure morphine milligram equivalent (opioid use) use at 12hr, 24hr, 48hr
◦ Secondary Outcomes:◦ Incidence of intolerable pain at 12hr, 24hr, 48hr◦ Opioid adverse effects:
◦ Nausea◦ Constipation◦ Itching◦ Overdose
15

Multimodal Pain Management: MethodsPre-operative Medications
Intra-operativeMedications
Post-Operative Medications
Pre-Multimodal(Control Group)
None Interarticular Joint Compound: • Ropivacaine• Epinephrine• Clonidine• Ketorolac
• Mild: APAP 650mg q4hr PRN• Moderate: hydrocodone/APAP 7.5/325mg q4hr PRN• Moderate 2nd: ketorolac 30mg q6hr PRN x 2 doses• Severe: Oxycodone 10mg q4hr PRN• Severe 2nd: Morphine IV 2mg q2hr PRN
Post-Multimodal (Multimodal Group)
• Gabapentin 600mg x 1 dose
• Celecoxib 400mg x 1 dose
• Acetaminophen 1000mg PO x 1 dose
Interarticular Joint Compound: • Ropivacaine• Epinephrine• Clonidine• Ketorolac
Scheduled APAP 1000mg three times dailyScheduled celecoxib 200mg twice dailyModerate: Oxycodone 5mg q4hr PRN Severe: Oxycodone 10mg q4hr PRNSevere 2nd: Ketorolac 15mg PRN x 1 doseSevere 3rd: Morphine IV 2mg q2hr PRN
16

Multimodal Pain Management: DemographicsParameter Pre-MM Post-MM P ValueAge: Avg (range) 63.3 (47-87) 64.6 (41-86) 0.304145Sex:Male: n (%) 12 (40%) 20 (45%) 0.641925Female: n (%) 18 (60%) 24 (55%)LOS in days: Avg (range) 2.7 (1-4) 2.15 (1-6) 0.062251BMI: Avg (range) 30.9 (22.2-40.4) 29.8 (19.4-39.4) 0.254934Surgery:Knee: n (%) 12 (40%) 20 (45%) 0.641925Hip: n (%) 18 (60%) 24 (55%)
17

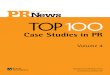
Multimodal Pain Management: Results
PRIMARY OUTCOME: Measure and compare cumulative morphine milligram equivalent between pre-implementation and post-implementation of a multimodal pain management strategy at 12 hours, 24 hours, and 48 hours postoperatively.
12 H Post-op Cumulative 24 H Post-op Cumulative 48 H Post-opPre-Multimodal 65.38 111.25 172.67Post-Multimodal 55.39 93.44 131.13
65.38
111.25
172.67
55.39
93.44
131.13
0.0020.0040.0060.0080.00
100.00120.00140.00160.00180.00200.00
MM
E
Average Morphine Milligram Equivant Use
18

Multimodal Pain Management: Results
SECONDARY OUTCOME: Measure and compare the incidence of patients not reporting intolerable pain (NPS ≥7 or CAPA=intolerable) between pre-implementation and post-implementation of a multimodal pain management strategy at 12 hours, 24 hours, and 48 hours postoperatively.
No Intolerable Pain at 12 H No Intolerable Pain at 24 H No Intolerable Pain at 48 HPre-Multimodal 30.0% 23.3% 20.0%Post-Multimodal 52.3% 47.7% 45.5%
30.0%23.3% 20.0%
52.3%47.7% 45.5%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
Patie
nts
Number of patients not reporting intolerable pain
19

Multimodal Pain Management: Results
SECONDARY OUTCOME: Measure and compare incidence of nausea, constipation, itching and overdose between pre-implementation and post-implementation of a multimodal pain management strategy.
50%
30%
3%
0
31%
16%
4%
0
0% 10% 20% 30% 40% 50% 60%
Nausea
Constipation
Itching
Overdose
Nausea Constipation Itching OverdosePost-MM 31% 16% 4% 0Pre-MM 50% 30% 3% 0
Side Effect Profile
20

Multimodal Pain Management: DiscussionPrimary Outcome:
•Opioid use• Trend toward reduced opioid use
• Particularly at 48 hours post-operatively
Secondary Outcomes:•Incidence of intolerable pain
• Significant reduction of intolerable pain at 24 and 48 hours after surgery
•Side effect profile• Trend toward reduced incidence of nausea and
constipation
Limitations:
•Retrospective
•Pre-Implementation sample size
•Allergies/Intolerances/Age/Renal function limited use of celecoxib and gabapentin
•Pain Assessment Challenges• NPS vs. CAPA• Subjectivity of pain assessment
•Assessment of medication use for nausea, constipation, itching
21

Multimodal Pain Management: Conclusion
Use of a multimodal pain management strategy, that
incorporates use of preoperative gabapentin, scheduled
acetaminophen and scheduled celecoxib, appears to reduce opioid
use, incidence of intolerable pain and common opioid side effects.
22

4. Patient and Family Caregiver Education and Engagement
Utilize Cerner’s opioid use agreement forms
Nonpharmacologic Options LMH Comfort Menu
Limit risk of opioid abuse: Limit prescribed quantity at discharge Utilize ORT Naloxone co-prescribing criteria
Update Opioid Discharge Education Drug interactions Side effects (withdrawal and overdose) Safe drug storage/disposal Risk of dependence Naloxone availability and use Tapering
23

Pain Management Agreement•Standardized Pain Management Agreement document
•Work with IT, HIMS and physicians to utilize Cerner’s Closed-looped Opioid Treatment Agreement Program• Alerts a provider who begins to order an opioid if the
patient is part of an Opioid Treatment Agreement with another provider
• Notifying the primary prescriber of an expiring agreement 30 days prior to the expiration
24

5. Tracking, Monitoring, and Reporting: Data Sources/Metrics LMH Discharge Opioid Data Douglas County Health Dept. Overdose Data Cerner’s Lights-On Data CollectionMedicare Opioid Prescribing Data Great Plains QIN Prescribing Data
Handouts
ICD 10 Codes for Opioid Poisoning and Non-Poisoning for inpatient and outpatient (Vizient Data) Inpatient naloxone use
25

Opioid Data Collection•Working with IT to develop a report to collect data on discharge opioid prescriptions throughout health system
1. Percentage of patients discharged from the hospital with opioid discharge prescription
2. Percentage of opioid discharge prescriptions exceeding 7 days
3. Use of multimodal order-set 4. Percentage of patients from the ER
discharged with opioid prescriptions
5. Percentage of patients discharged on opioids who receive discharge education on opioids
•Future Goal:• Inpatient MMED (available and
administered)• Comparable data to support
outpatient prescriptions• Establish clinic opioid data collection
26

Douglas County Health Department CollaborationDee Vernberg, PhD, MPH
Syndromic Surveillance◦ Analysis platform developed by Johns Hopkins
that uses EMR data to detect outbreaks
Opioid project goals ◦ To validate an opioid overdose syndrome query ◦ To develop relationships with other community
partners for prevention and treatment of overdoses
◦ To enhance opioid overdose preparedness efforts in Douglas County and develop public health’s role in this effort
27

Monthly LMH Overdose 2016-2019
28

Weekly LMH Overdose: 2017-2018
29

Douglas County Opioid Prescribing (Medicare Data)
0
20
40
60
80
100
120
140
160
180
PRAT
T
TREG
O
GRAH
AM
MO
NTG
OM
ERY
BOU
RBO
N
NES
S
SEW
ARD
REN
O
ELLI
S
GREE
LEY
CRAW
FORD
COW
LEY
SCO
TT
STAN
TON
NO
RTO
N
THO
MAS
SHER
MAN
MCP
HERS
ON
LAN
E
LYO
N
FORD
ELLS
WO
RTH
SUM
NER
RILE
Y
DOU
GLAS
GEAR
Y
BRO
WN
JACK
SON
NEO
SHO
MIA
MI
KEAR
NY
RICE
HAM
ILTO
N
MAR
SHAL
L
NEM
AHA
GRAY
LIN
N
BARB
ER
PHIL
LIPS
REPU
BLIC
HASK
ELL
DICK
INSO
N
SHER
IDAN
MEA
DE
CLAR
K
OTT
AWA
HODG
EMAN
COM
ANCH
E
LIN
COLN
KANSAS COUNTIES
2017 OPIOID PRESCRIBING RATE PER 100
30

LMH Health Opioid Prescribing Rate
31

6. AccountabilityEstablished Opioid Stewardship CommitteeAddressing community pain management needs
by adding new Pain ClinicMeeting Joint Commission StandardsEstablishing a Diversion CommitteeReviewing policy/procedures surround controlled
substance waste Share prescribing data so providers can see how
they compare with their peers
32

Diversion CommitteeCreate a Diversion Oversight Committee
Create a Diversion Response Team
Update Policies and Procedures
Improve tracking and reporting
Develop Diversion Risk Rounds to identify potential areas of diversion
Educate staff on proper disposal and identifying potential diversion
33

7. Community Collaboration Douglas County Health Department Data Drug Take-Back Programs
Public messaging about pain management strategies and opioid use: Radio Newspaper
Public Library Pain Management Education
Bert Nash Community Mental Health Center
34

Drug Take-Back Options: Deterra™ •Safely dispose of unused medications at home with the Deterra™ Drug Deactivation System
•The only patented technology that deactivates prescription drugs, rendering them ineffective for abuse and safe for the environment.• Free of charge • Simple 3-step process• Works with pills, liquids and patches
•Provided by Douglas County Health Department/DCCCA Grant
35

Drug Take-Back Options: MedSafe™ •Drop off unused controlled substances at Lawrence Pain Specialist Clinic
•MedSafe is an ultimate-user medication collection and disposal solution• Easy-to-operate system accepts controlled (Schedules II-V), non-
controlled, and over-the-counter medicines• Cost-effective and easy-to-manage system that meets DEA
regulations• Inner liners transferred by a common carrier• Controlled drugs destroyed using incineration, meeting the DEA's
destruction standard of non-retrievability
•Provided by Douglas County Health Department/DCCCA Grant
36

Opioid Stewardship FactorsHELPED
Prioritization as a community crisis
Hospital and medical staff leadership support
A strong committee with a charter
Organizational patient safety goals for opioid stewardship
Inclusion of opioid stewardship as part of the annual operating plan
Taking advantage of current climate and regulatory standards Structure and support
IT support and dedicated time
Protected time for patient care providers to attend meetings
HINDERED
Agreeing on appropriate and meaningful metrics
Obtaining and identifying necessary data
Competing time commitments and not having dedicated personnel
Communicating with key stakeholders, structural and cultural barriers
Sharing provider prescribing data and the potential repercussions of sharing un-blinded data
Lacking a good process to disseminate important information/education
Lacking pain management clinicians in the acute care setting
37

Current Opioid Stewardship InitiativesCompleted In Process Planned
• Physician UDS Education (7/15/18)• Med Staff Newsletter detailing
insurance/pharmacy opioid restrictions (7/20/19)
• Deterra Controlled Substance Disposal Bags Available (9/19/18)
• C-Section and Hysterectomy Multimodal Orders (11/16/18)
• Stull’s Total Shoulder Multimodal Orders (10/2/18)
• Multi-Modal Pain Management in Total Joint Replacements and data collection (11/22/18)
• ED Opioid Policy (12/6/18)• Create Diversion Committee and policy
(12/2018)• Update Discharge Opioid Education (3/2019)• Health Dept: Overdose Data Collection
(4/2019)• LMH Prescribing Data from KFMC (5/2019)• Discharge Opioid Data Collection (5/2019)
• Pain Agreement Notification-Janelle/Cerner/Dr.Harper/Pain clinic
• Universal multimodal orders• Update opioid prescription
sentences to reflect <50MMED/7 day supply
• Double Opioid Sentences to reduce amount filled.
• Community Opioid Disposal Program at the hospital
• Provider use of KTRACS Data• Inpatient Opioid Data Collection• Multimodal Orders for Spine Surgery• Hospital Controlled Substance
Disposal Dropbox• Addition and documentation of non-
pharmaceutical options• Community Collaborative- Public
Education- Newspaper/Radio
• Opioid Tapering• Opioid + Benzo Warning• High Dose Opiates Warning (>90MMED)• Naloxone Prescribing Guideline• Hospital Opioid Policy- include methadone
policy• Improve treatment access to
buprenorphine for OUD• HealthTracksRX (deferred until 2019)• Opioid Stewardship Newsletter• ED ALTO orderset- Dr. Dahl
38

Collaborative: Key LearningCreate a formal and embedded infrastructure for the opioid stewardship program A leader or leadership team is required by Joint Commission Develop charter
Develop a simple and balanced set of metrics, covering the domains of opioid stewardship Track a short list of meaningful measures to monitor the impact of opioid stewardship and pain management
initiatives
Establish a formal communication process to relay performance and policy updates to practitioners and front-line workforce Formalized way to communicate measures and changes in policies, guideline and regulations. Establish criteria for reporting data
Realize that opioid stewardship is one step on the path to improve the patient’s pain management Joint Commission states that hospitals must assess and manage the patient’s pain and minimize risks
associated with treatments
39

Opioid Stewardship Committee: Future• Reevaluate committee involvement using TJC Standards and CDC Recommendations
• Solidify Data Collection/Analysis Process
• Physician Involvement
• Implement Cerner Opioid Toolkit update• Morphine Milligram Equivalent Tracking
• Implement multimodal pain management and ERAS
• Update surgical and ED order sets
• Expand Community Collaboration
• Controlled Substance Disposal Program
• Expand treatment options for Opioid Use Disorder
40

References:1. Mikosz C, Conlon P, et al. National Quality Partners Playbook: Opioid Stewardship. National
Quality Forum 2018.
2. Williams SN, Wolford ML, Bercovitz A. Hospitalization for total knee replacement among inpatients aged 45 and over: United States, 2000–2010. NCHS data brief, no 210. Hyattsville, MD: National Center for Health Statistics. 2015
3. Chou R, Gordon DB, Leon-Casasola OA, et al. Management of postoperative pain: A clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, executive committee, and administrative council. J Pain. 2016;17(2):131-157.
4. Oseka L, Pecka, S. Anesthetic Management in Early Recovery After Surgery Protocols for Total Knee and Total Hip Arthroplasty. American Association of Nurse Anesthetists Journal. 2018;86:32
5. Clarke H, Pereira S, Kennedy D, et al. Gabapentin decreases morphine consumption and improves functional recovery following total knee arthroplasty. Pain Res Manag. 2009;14(3):217-212.
41

Opioid Stewardship Committee: A Multimodal ApproachKYLE EICHELBERGER, PHARMD, BCPS
[email protected] A partner for lifelong health
42