Embed Size (px)
Citation preview

Review
Optic ataxia as a deficit specific to the on-line control of actions
Scott Glover*
Department of Experimental Psychology, University of Oxford, South Parks Road, Oxford OX1 3UD, UK
Received 23 June 2003; revised 23 June 2003; accepted 28 June 2003
Abstract
Optic ataxia is characterized by inaccuracies in body movements under visual control, and is a common consequence of damage to the
posterior parietal lobes in humans. It is argued here that optic ataxia can be characterized as a deficit in the visual on-line guidance of actions,
with action planning remaining relatively intact. This contrasts with the common view of optic ataxia as representing a deficit in the
transformations that take place between visual inputs and motor outputs. Evidence in support of the planning-control view comes from the
pattern of spared and disrupted behaviors in patients with optic ataxia. It is shown that spared behaviors are those that emphasize planning,
whereas disrupted behaviors are those that emphasize control. In particular, recent studies have highlighted the inability of a patient with
optic ataxia to make on-line adjustments to targets that change position during the movement. Taken in sum, the data from patients with optic
ataxia is more consistent with the planning-control interpretation of optic ataxia than with the visuomotor transformation interpretation.
q 2003 Elsevier Ltd. All rights reserved.
Keywords: Optic ataxia; Planning; Control; Reaching; Grasping; Parietal lobes
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 447
2. Planning and control in action . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 448
3. Disrupted behaviors in patients with optic ataxia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 449
3.1. Pointing to targets in the periphery. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 449
3.2. Hand orientation in ‘posting’ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 449
3.3. Grasping . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 450
3.4. Manual tracking . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 450
4. Factors mediating the presence and severity of optic ataxia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 451
4.1. Fixation of the target . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 451
4.2. Practice. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 451
4.3. Familiarity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 452
4.4. Previews . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 452
4.5. Visual feedback. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 453
5. Specific dissociations of planning and on-line control in optic ataxia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 453
5.1. The Pisella et al. study. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 453
5.2. The Grea et al. study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 454
6. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 454
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 455
1. Introduction
Although Crougneau [15] was the first to describe
misreaching behavior following damage to the posterior
parietal lobes, Balint [2,35] was the first to use the term
‘optic ataxia’ as a description of the disorder. The
visuomotor basis of optic ataxia was evident in the presence
of a hand effect in Balint’s patient. In particular, when
reaching under visual guidance, the impaired hand was only
impaired in one visual field, showing that the deficit could
0149-7634/03/$ - see front matter q 2003 Elsevier Ltd. All rights reserved.
doi:10.1016/S0149-7634(03)00072-1
Neuroscience and Biobehavioral Reviews 27 (2003) 447–456
www.elsevier.com/locate/neubiorev
* Tel.: þ44-01865-271378.
E-mail address: [email protected] (S. Glover).

not be either strictly visual (i.e. which could be the case if it
affected only one visual field for both hands) or strictly
motor (i.e. affecting only one hand in both visual fields).
Further, both hands were accurate at touching body parts
with the eyes closed. Although Balint’s patient suffered
from a constellation of symptoms known today as ‘Balint’s
syndrome’ [5], optic ataxia represents a distinct disorder and
can be dissociated from elementary visuoperceptual,
proprioceptive, motor, praxic, or attentional deficits. Since
Balint’s time, the study of patients with optic ataxia has
revealed a fairly complex pattern of spared and disrupted
behaviors [23,34,49,53–55,61], and interpreting these
results has been a challenge for neuropsychologists.
In this paper, I propose a planning-control account of
optic ataxia. I argue that the brain regions commonly
damaged in patients with optic ataxia, the superior parietal
lobule (SPL) and the intraparietal sulcus (IPS), are
associated with on-line control in humans, whereas the
spared inferior parietal lobe (IPL) is associated with action
planning. Behaviorally, I argue that damage to the SPL
and/or IPS (as occurs in patients with optic ataxia) is
associated with deficits specific to the on-line control of
actions. (The consequences of damage to the IPL vis-a-vis
action planning are reviewed elsewhere [26,27] and so will
not be elaborated on in this paper). A similar characteriz-
ation of the SPL/IPS regions implicated in optic ataxia as
subserving ‘on-line control’ functions has also been
postulated by Rossetti and his colleagues [34,55,63,64].
An alternative explanation for optic ataxia is the
‘visuomotor transformation’ hypothesis [49,50,53,54]. On
this account, optic ataxia is said to represent a specific
disruption in the transformations that take place between
visuospatial input and motor output. These transformations
are thought to rely heavily on the human SPL and/or IPS.
These and other authors [4] have paralleled the performance
of patients with optic ataxia with neurophysiological studies
of monkeys. Note that the visuomotor transformation
hypothesis does not make a distinction between how
the movements are planned and how they are monitored
and adjusted on-line.
2. Planning and control in action
Woodworth [70] was the first to posit that actions are
comprised of two stages, an ‘initial impulse planning’ and a
‘current control’ stage. Since Woodworth’s time, the
properties of these two stages have become increasingly
well-understood [13,14,19,20,31,39,40,52,69,71]. Modern
views of planning and control generally agree that planning
represents a process occurring prior to the initiation of the
movement, designed to select and initiate a movement
appropriate to the goals of the action. For example, if an
actor’s goal is to grasp a book lying on a table, the planning
centers must determine a movement of the limb that will
bring the limb reasonably close to the book and shape
the hand appropriately to grasp the book. Control, on the
other hand, is thought to rely on a combination of visual and
proprioceptive feedback, in conjunction with an efference
copy of the movement plan, to monitor and adjust the
movement on-line, correcting for any spatial errors arising
from the plan itself or from outside forces (e.g. if the target
moves during the movement).
Generally speaking, the output of planning processes will
be evident early in a movement, whereas the output of
control processes will be evident late in the movement.
Apart from this temporal distinction, the planning and
control systems have been hypothesized to differ in several
ways [25,26,29]. For example, planning is argued to be a
relatively crude system that integrates a large amount of
visual and cognitive information, whereas on-line control is
a much more precise system that is focused on analyzing the
visuospatial characteristics of the target (e.g. its size, shape
and orientation). This means that the spatial parameters of a
movement will often be planned in but a crude way—the
planning system will endeavor only to bring the hand
reasonably close to the target and form it in a shape that is
reasonably close to that required. How precise the planning
of the movement is will depend on the quality and quantity
of information available to the planning system. Once the
movement is initiated, control processes will be used to
more precisely adapt the action to the spatial characteristics
of the target. The end result will be movements that may be
imperfectly planned, but nevertheless can be monitored and
adjusted on-line so as to be ultimately accurate.
Another distinction between planning and on-line control
is the speed of processing in each stage. Whereas planning is
a relatively slow and deliberate process [26,40], control tends
to be fast and automatic [14,31,71], at least for simple goal-
directed movements. This suggests that fast on-line adjust-
ments will be possible only when the control system is intact.
Slower adjustments can always be made, but these require the
relatively long process of deliberate, conscious comparison
between hand and target. For example, healthy subjects begin
to adjust to changes in target position or size within 100–
175 ms [13,52], even before they become consciously aware
of the change in the target [14], or even when a change in the
target is not consciously perceived [31,66].
Planning is hypothesized to rely to a large extent on
memories of past experience [62], whereas on-line control
tends to operate based on immediately available visual and
proprioceptive information. This predicts that planning
would benefit much more from experience and practice than
would on-line control [22,28,57,59]. Practice effects would
be evident in improved movement planning-the planning
system will generally be much more accurate for move-
ments that are well practiced than for movements under
novel circumstances. More practiced movements will tend
to require less on-line adjustment than movements under
novel circumstances.
Although the precision of both planning and on-line
control processes can also benefit from practice during
S. Glover / Neuroscience and Biobehavioral Reviews 27 (2003) 447–456448

development [68], the accurate use of on-line control seems
to be gained much earlier in the lifespan [67]. For example,
whereas infants as young as five months are able to accurately
guide their hands visually to objects in the workspace, it is
only in the third year of life that the early kinematics (i.e.
planning) of childrens’ movements reflect the stereotypical
pattern seen in adults [44]. This suggests that planning
processes rely to a much greater extent on memories of past
experiences than control; the latter appears to be a much more
innate skill requiring much less practice to master.
The neural correlates of planning and control in humans
can be gleaned from PET imaging studies [26]. In many
studies, motor behavior has been correlated with increased
activity in the IPL, SPL, and IPS [36,43,60]. However, these
studies have not specifically dissociated planning from
control. In other studies, planning and control have been
dissociated through either tasks emphasizing either the pre-
movement (planning) or execution (control) stage of action,
or scanning time devoted to one or the other stage of action.
These studies have generally found either increased activity
in the IPL associated with action planning [17,32,45,65], or
increased activity in the SPL and/or IPS associated with on-
line control [18,21,33,45].
The functional characterization of planning and control
described earlier provides a suitable framework for inter-
preting the pattern of disrupted behaviors in patients with
optic ataxia with damage to the SPL/IPS on-line control
system. In the ensuing review, it will be seen that these
patients have the largest deficits in conditions that
emphasize on-line control, and small or non-existent deficits
in conditions that emphasize planning.
3. Disrupted behaviors in patients with optic ataxia
Within the realm of visuomotor spatial behavior, patients
with optic ataxia have been found to make errors in a number
of different behaviors. This is consistent with the visuomotor
transformation hypothesis, which predicts a global deficit in
the use of vision for action. However, a careful examination
of these deficits reveals that the conditions under which these
errors occur are those that stress the on-line control system,
and that errors are more likely to occur late in the movement
(in the control stage) than early (in the planning stage).
3.1. Pointing to targets in the periphery
Patients with optic ataxia generally make large errors in
speeded pointing to targets in the visual periphery, both
using the hand [1,46,53,58,61], and foot [61]. Errors tend to
be more common in the visual field contralateral to the
lesion and tend to more often and more strongly affect the
contralateral hand [53,54].
According to the planning-control hypothesis, these
deficits result from a paucity of the visual input available
during planning and the concomitant reliance on on-line
control [55]. In particular, it is clear that peripheral vision
possesses much less spatial resolution than foveal vision
[47]. The lack of high resolution visual information for
planning the movement results in large errors. In normal
subjects, these errors can be overcome by adequate on-line
control [31,41]. In patients with optic ataxia, however, the
on-line control system is damaged and so cannot correct
these errors.
One alternative interpretation of optic ataxic perform-
ance in pointing to targets in the periphery relies on the
finding that systematic errors towards fixation occur in
many patients with optic ataxia [58]. In extreme cases, optic
ataxics may even be unable to point anywhere but towards
fixation [10–12]. This might suggest that optic ataxia can
represent a failure to enact the final stage of the visuomotor
transformation process (i.e. the transformation from retinal
to hand-centered reference frames). This hypothesis would
not predict, however, cases in which optic ataxia leads to
random errors in direction [58] unless there were also a
specific role of the IPS/SPL in the on-line correction of
random noise in the planning system.
3.2. Hand orientation in ‘posting’
Patients with optic ataxia have also been shown to have
difficulties in a ‘posting’ task [53,54]. This task uses a
circular wooden board out of which is cut a oval-shaped
hole large enough to allow a hand to pass through. The
experimenter holds up the board at arm’s length in the visual
periphery of the patient at various orientations, and the
patient is required to ‘post’ their hand through the slot.
Perenin and Vighetto [53] observed that patients with
optic ataxia were largely impaired at this task, showing
three basic kinds of deficits. First, patients often misoriented
their hand with respect to the hole. Second, patients
sometimes missed the hole or the board entirely with their
hand. Finally, patients sometimes misshaped their hands,
‘fanning’ their fingers out wide, for example, instead of
holding them tightly together in a straight line as the task
demanded. In their second study, however, Perenin and
Vighetto [54] observed that patients with optic ataxia were
largely successful at the task, although some errors did
occur. One reason for this discrepancy between studies may
be that the patients had recovered somewhat over time
(many of the same patients participated in both studies).
A planning-control interpretation of posting suggests that
it is largely controlled on-line because it represents such an
unfamiliar task. It is hard to imagine a condition in real life in
which one needs to ‘post’ their hand through a slot presented
at arm’s length in any orientation other than 0 or 908 (most
slots are oriented at one or the other of these angles). The
result of this unfamiliarity is that the planning system cannot
easily draw on a motor program from memory to do the task.
Thus, the plan cannot be easily specified and there is a
concomitant reliance on on-line control. This would predict
that performance of optic ataxics would be much improved
S. Glover / Neuroscience and Biobehavioral Reviews 27 (2003) 447–456 449

under ‘normal’ circumstances (e.g. when posting a letter in
central vision) than under these ‘clinical’ conditions. Note
however that, because they reflect errors in action, the results
of the posting task are also consistent with the visuomotor
transformation hypothesis.
3.3. Grasping
Deficits in grasping have also been commonly observed in
patients with optic ataxia [2,34,37,41,48,49,53,54,61]. These
deficits seem to be concentrated in the on-line phase of
action. For example, Jakobson et al. [37] observed that their
patient VK had difficulty in grasping objects, a deficit they
attributed to an impairment in visuomotor transformations
(i.e. planning). However, an examination of this patient’s
kinematic data suggested that her deficit was largely confined
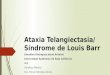
to the later stages of the movement (Fig. 1). During the early
stage of the action, the grip aperture rose in a manner very
similar to the patterns observed in a healthy subject. Indeed,
apart from a slowing in reaction time (that might reflect a
compensatory strategy in order to deal with her impairment),
the timing of VK’s early kinematic markers were quite
consistent with those of the control subjects.
It was only in the latter half of the movement that VK’s
grasping appeared to degenerate. Here, whereas the healthy
subjects smoothly finished the movement by closing their
hand around the object, VK had several secondary peaks in
the grip aperture profile. It was only after considerable time
had elapsed that VK was able to actually grasp the object.
This disruption in VK’s grasping behavior seems strongly
in favor of a planning-control distinction in optic ataxia,
despite the authors’ contention that the deficit was one of
visuomotor transformations [37]. Indeed, what might be
thought of as reflecting the ‘plan’ of the movement, indexed
in the early part of the grip aperture profile, was by all
appearances quite normal in this patient. It was only after the
movement was well underway that the grip aperture profile
became disrupted as the hand opened and closed repeatedly.
Jeannerod [41] observed a similar deficit in the parietal
patient ‘Tho’. This patient showed a difficulty in grasping
objects, but, as with VK [37], the early part of the trajectory
was largely normal. It was only after some time had elapsed
in the course of the movement that Tho’s difficulties became
apparent, as he repeatedly opened and closed his thumb-
finger aperture. Again, this is consistent with an interpret-
ation of optic ataxia as a deficit specific to the on-line control
stage of actions. Caution must be emphasized in interpreting
this result, however, as Tho. also suffered from some
impairment in somatosensory function, and thus cannot
truly be categorized as having a pure case of optic ataxia.
Binkofski et al. [6] also observed kinematic abnormal-
ities in grasping in patients with damage including the
anterior IPS. These patients were shown to have greater
disruption in the latter stages of actions, although they also
tended to have abnormalities that occurred somewhat earlier
in the trajectory than those in patient VK [37] and patient
Tho. [41], suggesting Binkofski’s patients may have had
difficulties with movement planning as well. This may have
been due to the fact that the anterior IPL was also damaged
in many of these patients.
3.4. Manual tracking
In manual tracking a moving target must be followed with
the finger, requiring continual monitoring of the relationship
between the hand and target, and continual on-line adjust-
ment of the movement in order to minimize the error. In fact,
manual tracking tasks in which the direction and velocity of
the target are unpredictable virtually eliminate the possibility
of anticipatory planning. Yet in all of the studies of patients
with optic ataxia reviewed for this paper, only one made
mention of manual tracking performance [23]. This perhaps
speaks to the relative lack of attention that has been paid to
the notion of a specific on-line control deficit in patients with
optic ataxia over the last century.
Ferro [23] examined a patient who presented with a small
lesion in the SPL of the left hemisphere. This patient initially
presented with errors in pointing with the contralesional hand
that were worse in the visual periphery. The errors were even
greater, however, if the target was moving and he had to track
it manually. Although this patient recovered quickly,
showing almost no impairment in pointing and grasping
tasks after just 10 days, the patient did retain a minor deficit in
manual tracking as judged by the examiner.
I suggest that this patient’s deficit in manual tracking was
almost indisputably related to on-line control. However,
data on manual tracking performance in patients with optic
ataxia are extremely lacking, and it is clear that more
examinations will be required if the planning-control
hypothesis is to be tested. Future tests will be able to
employ careful modern day recording techniques in order to
accurately quantify the existence and extent of the deficit.
Fig. 1. Representative traces of the grip aperture profiles of the optic ataxic
VK compared to two healthy control subjects. Grip aperture is plotted along
the y-axis, time along the x-axis. Notice that, apart from a longer reaction
time, the early portion of VK’s grip aperture profile is quite similar to that
of the control subjects. Copied with permission from Jakobsone et al.
(1991), Neuropsychologia [37].
S. Glover / Neuroscience and Biobehavioral Reviews 27 (2003) 447–456450

4. Factors mediating the presence and severity
of optic ataxia
In all of the aforementioned cases, errors in visually-
guided action have been observed in patients with optic
ataxia. Generally, these errors were consistent with both the
planning-control and visuomotor transformation hypotheses.
However, it will be seen in the ensuing section that there are
many factors that mediate the presence and severity of optic
ataxia. The ameliorating effects of these factors are
consistent with the planning-control framework inasmuch
as they can be argued to reflect conditions under which
planning processes are emphasized over control processes.
However, as the visuomotor transformation hypothesis
predicts that both planning and on-line control are disrupted
in optic ataxia, such amelioration is anomalous.
Within the planning-control framework, certain factors
would be predicted to mediate the presence and/or severity
of optic ataxia. These represent conditions in which
planning systems are given more information and are
thus able to select a more accurate action. The resulting
accuracy in planning should make on-line control much
less necessary, and deficits in on-line control much less
noticeable. The consequences are that patients with optic
ataxia should be much improved under such conditions.
This can be contrasted with the visuomotor transformation
hypothesis, that would generally argue that inaccuracy of
movements under visual guidance should generally suffer
from a deficit in visuomotor transformations that is not
subject to ameliorating factors.
4.1. Fixation of the target
Fixating a target while reaching to it can vastly improve
the performance of patients with optic ataxia [46,53,54,61].
Even briefly fixating the target then returning the eyes to a
central position before reaching has been reported to
improve performance [61]. As mentioned earlier, a reason
for this could be that fixating a target allows for a relatively
accurate estimate of its position, based on the greater spatial
resolution of central vision. This would lead to more
accurate planning, which in turn would place much less
demand on the on-line control system.
An alternative interpretation of the impairment in
pointing to targets is that it reflects a deficit in visuomotor
transformations [50,53,54]. However, this ignores the fact
that pointing to a target that is fixated is quite unimpaired in
the vast majority of these patients [1,53,55,61]; for
exceptions see Refs. [10,23,53]. It is only if one assumes
that foveal vision allows for accurate planning and less
reliance on on-line control that it becomes understandable
that pointing in central vision is generally much more
accurate in patients with optic ataxia [55].
It is interesting to note here that evidence from healthy
subjects is unclear as to whether pointing to a target in the
visual periphery is more difficult than pointing to targets in
central vision. Whereas some studies have found larger
errors when pointing to peripheral targets [7,8], others found
this only for fast movements [3], and others found no effects
at all of pointing in peripheral versus central vision [56].
Similarly, in grasping, Goodale and Murphy [30] found grip
scaling to object size preserved when grasping targets in
peripheral vision, just as is found for grasping targets in
central vision [38,39]. However, it is notable that in the
Goodale and Murphy study there were generally larger grip
apertures and scaling was less precise in peripheral than in
central vision. Taken in sum, the results from studies of
healthy subjects have been generally consistent with respect
to the planning-control hypothesis that movements directed
towards peripheral targets are more difficult to plan than
those to central targets. However, clearly more work is
needed to test this hypothesis.
4.2. Practice
Practice is another factor that leads to more accurate
planning and less reliance on on-line control. Practice
effects on planning might occur through the experience of
handling the target [24] (at least for grasping), and/or
through accumulated knowledge of errors made on previous
trials (for both grasping and pointing). As such, practice
should improve the performance of patients with optic
ataxia in both pointing and grasping tasks. Rondot et al. [61]
observed that when their patients were allowed to
continuously perform the same task of pointing to targets
in the periphery, their performance improved over a number
of trials. Here, patients presumably became aware of their
errors and were able to modify movement planning
accordingly, making on-line adjustments less necessary.
Although one cannot rule out some improvement in on-line
control mechanisms as well in these cases, it seems more
parsimonious to suggest that patients with optic ataxia show
improvements for the same reasons as healthy subjects
improve at difficult visuomotor tasks over time-practice
leads to more accurate planning [22,28,57,59].
Similar results were observed by Milner et al. [49] for
grasping wooden blocks: movements of the optic ataxic IG
became much more similar to those of healthy controls in a
second block of testing than they had been in the first block.
Such practice effects were not evident in healthy control
subjects [49] presumably because they had intact on-line
control systems that made practice unnecessary for normal
performance of the task.
Thus one can see that practice generally improves the
performance of patients with optic ataxia. Although for
grasping one could argue that practice benefits accrue
through haptic experience with the target, this argument
does not hold for pointing. In the latter case, practice can
only benefit planning due to visual knowledge of errors
being used in the planning of future trials. Such an effect is
consistent with the planning-control interpretation, but
seems much less likely for the visuomotor transformation
S. Glover / Neuroscience and Biobehavioral Reviews 27 (2003) 447–456 451

hypothesis. The former would hold that practice aids
planning in general, the latter would predict that visuomotor
transformations are impaired in optic ataxia, and that little
or no benefit of practice should accrue.
4.3. Familiarity
Related to the issue of practice is familiarity. Jeannerod
et al. [42] reported a patient (AT) with a deficit in grasping
following bilateral posterior parietal lesions. AT was
observed to have a grossly poor scaling of the grip aperture
in reaching to white cylindrical plastic ‘neutral’ objects.
Remarkably, however, AT was much better when these
‘neutral’ objects were replaced with familiar, everyday
objects, such as a lipstick or a glass. In these cases, AT’s
performance was much improved and in fact was compar-
able to that of a healthy control subject.
This dissociation is surprising if one believes that
patients with optic ataxia suffer simply from a disruption
in the transformation of visual information into motor
behavior [50]. Rather, there was clearly a benefit of having
recognized the targets as common objects and having
previously interacted with such objects. One way of
explaining this is that AT relied on a ‘perceptual’
representation in order to guide her grasping [42]. However,
a more parsimonious explanation might be that AT
benefited from her experience with familiar objects in
a more direct way, through an ability to more easily select
an appropriate action plan from a vastly greater repertoire
than was available for grasping unfamiliar objects.
4.4. Previews
Viewing a target for some time prior to directing a
movement towards it should also improve planning pro-
cesses and require less reliance on on-line control. In several
studies, Milner and his colleagues [48,49,51] have shown
that allowing patients with optic ataxia to see the target
several seconds prior to responding to it leads to a dramatic
improvement in performance as compared to conditions in
which the target had to be responded to immediately.
In one study, Milner et al. [49] observed that the optic
ataxic IG, who had suffered bilateral damage including the
SPL, IPS, and a small part of the IPL, showed improved grip
scaling when given a brief preview of the target five seconds
before having to grasp it. Similar results were found for
patient AT (see also Ref. [42]) who was much more accurate
in pointing to peripheral targets when she was allowed a
preview of them five seconds prior to moving.
Even more interesting were the effects of replacing the
target with one of a different size during the delay period
between the preview and the re-presentation of the target.
For example, Milner et al. [49] had IG and several control
subjects perform a preview grasping task. In some cases, the
target was replaced during the interval between the preview
and the grasp by a target of a different size. Although
healthy subjects reached to the ‘new’ target as normally as
before (i.e. their maximum grip apertures were not affected
by the preview of a different-sized target), IG had maximum
grip apertures that were influenced by the size of the ‘old’
target, and was only slowly able to correct her movement in
flight to the ‘new’ target (Fig. 2).
How to explain these rather surprising results? Although
Milner and his colleagues suggested that these results
implied that patients with optic ataxia can operate using a
‘perceptual’ visual representation [49] when conditions are
appropriate, the planning-control interpretation seems
equally plausible. In the latter view, previews allow for
more visual information to be processed for longer in the
planning system, and hence for the formation of a more
accurate plan. Further, in the condition in which the target
is replaced, I would argue that the original plan remains
paramount in both the optic ataxic and the healthy subjects,
but that in the latter on-line control is able to easily adapt
the plan to the changed circumstances. According to this
view, both patients with optic ataxia and controls should
show a tendency to scale their grasp according to the size
of the previewed object early in the reach; this tendency
should be eliminated by the time maximum grip aperture is
attained in the controls (i.e. at roughly two-thirds of the
duration of the movement), but not in patients with optic
ataxia.
Fig. 2. Effects of delay period in which object was replaced with a new object of a different size. Shows IG’s (left) maximum grip apertures and those of a
control subject (right) for objects of initial and/or final sizes of 2 cm or 5 cm. Copied with permission from Milner et al. (2001), Current Biology [49].
S. Glover / Neuroscience and Biobehavioral Reviews 27 (2003) 447–456452

4.5. Visual feedback
A planning-control interpretation suggests that visual
feedback should not improve the performance of patients
with optic ataxia in quickly-executed actions because the fast
on-line control system that uses visual feedback to make fast
corrections is impaired. This can be contrasted with a view of
optic ataxia in which visuomotor transformations in general
are thought to be disrupted [50,53,54]. In the latter view,
visual feedback might be thought to be of at least some
benefit to patients with optic ataxia, given the large errors that
would be assumed to occur during action planning.
Evidence to date suggests that the availability of visual
feedback has little impact on the performance of most
patients with optic ataxia [10,16,23,37,41,42,46,53]. In
many cases, the availability of visual feedback has been
inconsequential to the performance of patients with optic
ataxia [37,53], and in some cases visual feedback even
seems to make performance worse rather than better [10,
16]. When improvements are observed, these usually
correspond to the use of a deliberate strategy of slowing
the movement down so as to carefully localize the target,
perhaps with respect to proprioceptive input from the hand
[23,41,46]. This ‘slow’ use of visual feedback can be
contrasted with the typically fast and automatic on-line
corrections that are seen in healthy subjects [13,31,52,71].
5. Specific dissociations of planning and on-line control
in optic ataxia
Two recent studies have examined the performance of an
optic ataxic (IG) specifically in the planning and on-line
control stages of actions [34,55]. As described earlier, IG
suffered from a bilateral lesion of the posterior parietal
cortex, including the SPL, IPS, an area along the parieto-
occipital junction, and a small area in the IPL. Studies of
Pisella et al. and Grea et al. have convincingly demonstrated
that optic ataxia, in IG at least, can manifest itself
specifically in the on-line control phase of actions. In
contrast, there is little evidence that this patient has
difficulty in transforming visual input into the planning of
movements, as would be predicted by the visuomotor
transformation hypothesis.
5.1. The Pisella et al. study
Pisella et al. [55] studied the tendency of IG to make
‘automatic’, involuntary corrections to target jumps. IG and
several healthy controls were seated at a computer screen
with their finger situated at the bottom of the screen. The
primary task was to make fast pointing movements to a target
that appeared 25 cm vertical from the starting position. On
80% of the trials, the target remained in the same location
throughout the trial. However, on 20% of trials, the target
jumped slightly horizontally coincident with the onset of the
movement. Free eye movements were allowed.
When the target remained stationary, IG was nearly as
accurate as healthy subjects in pointing to the target. This
suggested that, as for most other patients with optic ataxia,
her planning system was able to plan accurate movements
for targets in central vision. However, when the target
jumped, IG’s performance was markedly different from the
controls. Specifically, healthy subjects easily and automati-
cally made on-line corrections to the new position of the
target, even for movements lasting only 200 ms. However,
IG was grossly impaired at making these fast on-line
corrections; more often than not she completed her move-
ment in the direction of the initial target location (Fig. 3).
Fig. 3. Percentage of pointing responses made to the new location of the target when the target changed position, for a control subject (top) and IG (bottom).
Along the x-axis is the time taken to complete the movements. Note that whereas the control subject often made on-line corrections within 150 ms, IG was only
able to make slow and deliberate corrections. IG was not, however, slower than the control subjects overall. Copied with permission from Pisella et al. (2000),
Nature Neuroscience [55].
S. Glover / Neuroscience and Biobehavioral Reviews 27 (2003) 447–456 453

5.2. The Grea et al. study
Grea et al. [34] followed up Pisella et al.’s work with IG
by examining her ability to make on-line corrections in a
grasping task, with free eye movements. As in Pisella et al.,
IG’s performance was compared to healthy subjects. In the
Grea et al. experiment, the task involved grasping a cylinder
in central vision. Again, the cylinder remained stationary on
80% of the trials, and changed position (moving either to the
left or right by use of a torque motor controlled via
computer) on the remaining 20% of trials. Similar to her
performance in the pointing task used by Pisella et al., IG
was far more impaired at the grasping task when the target
changed position. Remarkably, on these trials, the authors
reported that IG
…showed a dramatic inability to correct her ongoing
movement in response to the target jump. When the
cylinder position was modified at movement onset, IG
exhibited two distinguishable movements, a first move-
ment toward the initial position of the object and a second
movement toward the final position… (Grea et al., 2002,
p. 2476)
For both these studies, it is worth emphasizing that IG did
not suffer from any elementary perceptual or motor defects,
nor did she have any reported problems in orienting her eyes
to the changes in target position. Further, IG showed perfect
accuracy in verbally reporting the changes in a ‘perceptual’
control condition. And under normal conditions (i.e. when
the target remained stationary throughout the trial), IG was
nearly as accurate as the healthy controls. It was only when
an on-line response was required to a change in the target
that IG showed a large impairment at the task.
Some caution is necessary here because the results
obtained with changes in target position have so far only
occurred with a single subject. Thus, it is not entirely certain
that similar results would occur with other patients with
optic ataxia. Further, the damage to IG’s brain was quite
extensive and the on-line control system could not easily be
localized within the area of damage, although the fact that
the IPS and SPL were damaged in IG is consistent with the
notion that these regions are involved in the visual on-line
control of actions. Nevertheless, more studies will need to
further examine the role of on-line control in optic ataxia
under conditions that stress the on-line system.
6. Conclusions
Damage to the SPL and neighboring IPS leads to a
complex constellation of deficits in the visual control of
movement. Past studies have shown that these deficits
include errors in pointing to targets in the visual periphery
[54], in orienting the hand to post it through a slot [53], in
grasping [37,42], and in manual tracking [23]. Such deficits
can be argued to reflect a disruption in the on-line control of
actions because they occur primarily in peripheral vision (in
pointing tasks), primarily in the second half of the
movement (in grasping), in a very unfamiliar task (posting),
and during a task that specifically evokes on-line monitoring
and corrections (manual tracking).
The factors that modulate the presence or extent of optic
ataxia also seem consistent with a planning-control
interpretation. Patients with optic ataxia are often less
impaired when more information is available to the
planning system, such as when actions are allowed to take
place in central vision as opposed to peripheral vision [53];
when actions are repeatedly practiced [61]; are directed
towards familiar objects as opposed to being carried out in
unfamiliar conditions [42]; or when previews of targets are
given prior to reaching [49]. Conversely, patients with optic
ataxia are usually no less impaired when more information
is available to the on-line control system, such as when
visual feedback of the moving hand is allowed as opposed to
when it is blocked [37,53,54]. Indeed, visual feedback has
even been found to increase the errors made by some
patients with optic ataxia [10,16].
Finally, the optic ataxic IG has been shown to be nearly
as accurate as healthy subjects in directing actions towards
stationary targets, but to show a marked impairment in
performing the same tasks when the target changes position
coincident with movement initiation. These impairments in
on-line adjustments have occurred both for pointing [55]
and grasping [34].
The evidence reviewed here suggests a coincidence
between the brain regions implicated in on-line control in
healthy humans [18,21,33], and those damaged in patients
with optic ataxia [53,54]. In both cases, the SPL and IPS
have been heavily implicated in on-line control. Thus, the
planning-control distinction seems to provide a useful
framework for exploring the pattern of spared and disrupted
behaviors in patients with optic ataxia.
It is interesting that neurophysiological studies of the
macaque have also shown the importance of the parietal
lobes in visually-guided (see Ref. [9] for a review). In these
models, the argument is made that visuomotor transform-
ations take place through an interaction of frontal and
parietal structures. Thus these models are (superficially at
least) similar to the proposal of Ref. [50], inasmuch as
neither seem to consider a possible separation between
planning and on-line control. I would suggest that future
studies on the macaque might benefit from a consideration
of the planning-control distinction.
Although the evidence in favor of a planning-control
interpretation of optic ataxia is strong, there are some points
that may be challenged. For example, the errors shown by
healthy subjects when pointing to targets in the periphery
tend to be directed away from fixation [7,8], whereas those
of patients with optic ataxia tend to be directed towards
fixation [10,53]. This inconsistency begs the question as to
whether or not these errors result from similar processes in
S. Glover / Neuroscience and Biobehavioral Reviews 27 (2003) 447–456454

the two classes of subjects. Another point of contention
might be that the tasks that have been argued to most heavily
involve on-line control (e.g. manual tracking, adjustments to
a target perturbation) and in which patients with optic ataxia
have the greatest deficits, may simply be more difficult than
tasks that are argued not to rely most heavily on on-line
control (e.g. pointing to a fixated target). Whereas this
argument may be worthy of consideration, it would not
apply to other conditions in which optic ataxics are impaired
(e.g. in the latter stages of a grasping movement).
Finally, it should be noted that it still may be possible to
reconcile many of these results with a visuomotor
transformation hypothesis. For example, practice effects
that lead to improved performance in patients with optic
ataxia may reflect the accumulation of haptic experience
with the target [24], rather than affecting ‘visually-
determined’ planning per se. However, this argument can
only apply to tasks in which haptic feedback is available
(i.e. grasping), and would not apply to pointing tasks, which
also seem to benefit from practice [61]. Further, actions can
always be argued to be ‘perceptually-guided’ under
conditions such as the ‘preview’ condition or when the
target is familiar [49]. However, such an argument
potentially runs the risk of circularity—what is impaired
must of necessity be ‘action-guided’ and what isn’t impaired
must of necessity be ‘perceptually-guided’. In contrast to
such ad hoc explanations, the planning-control model makes
clear a priori predictions that rely on logical presumptions as
well as established behavioral findings.
Future studies may be oriented towards exploring the
types of clear planning-control dissociations revealed by
Pisella et al. [55] and Grea et al. [34]. In particular, more
studies will be needed to test patients with optic ataxia over
the course of the movement on tasks that specifically
emphasize planning and/or control. Examples of the former
include highly-practiced or familiar tasks carried out in
central vision with long views of the target. Examples of the
latter include reactions to target perturbations, manual
tracking, and tasks carried out in peripheral vision with brief
views of the target. Other conditions that further stress the
on-line control system, such as the wearing of light-
refracting prism goggles, could also be of interest in studies
of patients with optic ataxia. Investigations such as these
could be useful in more specifically defining the nature of
optic ataxia, and by proxy, the functions of the SPL and IPS
in the human brain.
Acknowledgements
This work was supported by the Natural Sciences and
Engineering Research Council of Canada through a fellow-
ship to the author. The author wishes to express his gratitude
to Matthew Rushworth and Umberto Castiello for insightful
comments on a draft version of this manuscript, as well as to
David Carey, Yves Rossetti, and Laure Pisella for their very
helpful reviews.
References
[1] Auerbach SH, Alexander MP. Pure agraphia and unilateral optic
ataxia associated with a left superior parietal lobule lesion. J Neurol
Neurosurg Psychiatry 1981;44:430–2.
[2] Balint R. Sellenlahmung des ‘Schauens’, optische Ataxie, raumliche
Storung der Aufmersamkeit. Monatschrift fur Psychiatrie und
Neurologie 1909;25:51–81.
[3] Bard C, Hay L, Fleury M. Role of peripheral vision in the directional
control of rapid aiming movements. Can J Psychol 1985;35:151–61.
[4] Battaglia-Mayer A, Caminiti R. Optic ataxia as a result of the
breakdown of the global tuning fields of parietal neurones. Brain
2002;125:225–37.
[5] Baylis GC, Baylis LL. Visually misguided reaching in Balint’s
syndrome. Neuropsychologia 2001;39:865–75.
[6] Binkofski F, Dohle C, Posse S, Stephan KM, Hefter H, Seitz RJ,
Freund H-J. Human anterior intraparietal area subserves prehension: a
combined lesion and functional MRI activation study. Neurology
1998;50:1253–9.
[7] Bock O. Localization of objects in the peripheral visual field. Behav
Brain Res 1993;56:77–84.
[8] Bock O. Contribution of retinal versus extraretinal signals towards
visual localization in goal-directed movements. Exp Brain Res 1986;
64:476–82.
[9] Burnod Y, Baraduc P, Battaglia-Mayer A, Guigon E, Koechline E,
Ferraina S, Lacquaniti F, Caminiti R. Parieto-frontal coding of
reaching: an integrated framework. Exp Brain Res 1999;129:325–46.
[10] Buxbaum LJ, Coslett HB. Subtypes of optic ataxia: reframing the
disconnection account. Neurocase 1997;3:159–66.
[11] Buxbaum LJ, Coslett HB. Spatio-motor representations in reaching:
evidence for subtypes of optic ataxia. Cogn Neuropsychol 1998;15:
279–312.
[12] Carey DP, Coleman RJ, Della Salla S. Magnetic misreaching. Cortex
1997;33:639–52.
[13] Castiello U, Bennett K, Stelmach G. Reach to grasp: the natural
response to perturbation of object size. Exp Brain Res 1993;94:
163–78.
[14] Castiello U, Jeannerod M. Measuring time to awareness. Neuroreport
1991;2:797–800.
[15] Crouigneau G. Etude clinique et experimentale sur la vision mentale.
These de Doctorat en Medecine. Paris: Devillaire; 1884.
[16] Damasio AR, Benton AL. Impairment of hand movements under
visual guidance. Brain 1979;29:170–8.
[17] Deiber M-P, Ibanez V, Sadato N, Hallett M. Cerebral structures
participating in motor preparation in humans: a positron emission
tomography study. J Neurophysiol 1996;75:233–47.
[18] Desmurget M, Epstein CM, Turner RS, Prablanc C, Alexander GE,
Grafton ST. Role of the posterior parietal lobe in updating reaching
movements to a visual target. Nat Neurosci 1999;2:563–7.
[19] Desmurget M, Grafton ST. Forward modeling allows feedback control
for fast reaching movements. Trends Cogn Sci 2000;4:423–31.
[20] Desmurget M, Pelisson D, Rossetti Y, Prablanc C. From eye to hand:
planning goal-directed movements. Neurosci Biobehav Rev 1998;22:
761–88.
[21] Desmurget M, Grea H, Grethe J, Prablanc C, Alexander G, Grafton
ST. Functional anatomy of nonvisual feedback loops during reaching:
a positron emission tomography study. J Neurosci 2001;21:2919–28.
[22] Elliot D, Chua R, Pollock BJ, Lyons J. Optimizing the use of vision in
manual aiming: the role of practice. Q J Exp Psychol A 1995;48:
72–83.
[23] Ferro JM. Transient inaccuracy in reaching caused by a posterior
parietal lobe lesion. J Neurol Neurosurg Psychiatry 1984;47:1016–9.
[24] Gentilucci M, Daprati E, Toni I, Chieffi S, Saetti M. Unconscious
updating of grasp motor program. Exp Brain Res 1995;105:291–303.
[25] Glover S. Visual illusions affect planning but not control. Trends
Cogn Sci 2002;6:288–92.
S. Glover / Neuroscience and Biobehavioral Reviews 27 (2003) 447–456 455

[26] Glover S. Separate visual representations in the planning and control
of action. Behav Brain Sci 2003;a. in press.
[27] Glover S, Dixon P. The role of vision in the on-line correction of
illusion effects on action. Can J Exp Psychol 2001;55:96–103.
[28] Glover S, Dixon P. Motor adaptation to an optical illusion. Exp Brain
Res 2001;137:254–8.
[29] Glover S, Dixon P. Semantics affect the planning but not control of
grasping. Exp Brain Res 2002;146:383–7.
[30] Goodale MA, Murphy KJ. Action and perception in the visual
periphery. In: Their P, Otto-Karnath H, editors. Parietal lobe
contributions to orientation in 3D space. New York: Springer; 1997,
p. 447–61.
[31] Goodale MA, Pelisson D, Prablanc C. Large adjustments in visually
guided reaching do not depend on vision of the hand or perception of
target displacement. Nature 1986;320:748–50.
[32] Grafton ST, Arbib M, Fadiga L, Rizzolatti G. Localization of grasp
representations in humans by position emission tomography. II.
Observation compared with imagination. Exp Brain Res 1996;112:
103–11.
[33] Grafton ST, Mazziotta J, Woods R, Phelps M. Human functional
anatomy of visually guided finger movements. Brain 1992;115:565–87.
[34] Grea H, Pisella L, Rossetti Y, Desmurget M, Tilikete C, Grafton ST,
Prablanc C, Vighetto A. A lesion of the posterior parietal cortex
disrupts on-line adjustments during aiming movements. Neuropsy-
chologia 2002;40:2471–80.
[35] Harvey M, Milner AD. Translation of R. Balint’s Psychic paralysis of
gaze, optic ataxia, and spatial disorder of attention. Cogn Neuropsy-
chol 1995;12:261–81. (originally appearing in Monatsschrift fur
Psychiatrie und Neurologie 1909;25:51–81).
[36] Inoue K, Kawashima R, Satoh K, Kinomura S, Goto R, Koyama M,
Sugiura M, Ito M, Fukuda H. PET study of pointing with visual
feedback of moving hands. J Neurophys 1998;79:117–25.
[37] Jakobson LS, Archibald YM, Carey DP, Goodale MA. A kinematic
analysis of reaching and grasping movements in a patient recovering
from optic ataxia. Neuropsychologia 1991;29:803–9.
[38] Jakobson LS, Goodale MA. Factors affecting higher-order movement
planning: a kinematic analysis of human prehension. Exp Brain Res
1991;86:199–208.
[39] Jeannerod M. The timing of natural prehension movements. J Mot
Behav 1984;16:235–54.
[40] Jeannerod M. The neural and behavioural organization of goal-
directed movements. Oxford: Oxford University Press; 1988.
[41] Jeannerod M. Mechanisms of visuomotor coordination: a study in
normal and brain-damaged subjects. Neuropsychologia 1986;24:
41–78.
[42] Jeannerod M, Decety J, Michel F. Impairment of grasping movements
following a bilateral posterior parietal lesion. Neuropsychologia 1994;
32:369–80.
[43] Kertzmann C, Schwarz U, Zeffiro T, Hallett M. The role of posterior
parietal cortex in visually guided reaching movements in humans. Exp
Brain Res 1997;114:170–83.
[44] Konczak J, Dichigan J. The development towards stereotypic arm
kinematics during reaching in the first three years of life. Exp Brain
Res 1997;117:346–64.
[45] Krams M, Rushworth MF, Deiber M-P, Frackowiak R, Passingham R.
The preparation, execution, and suppression of copied movements in
the human brain. Exp Brain Res 1998;120:386–98.
[46] Levine DN, Kaufman KJ, Mohr JP. Inaccurate reaching associated
with a superior parietal lobe tumor. Neurology 1978;28:556–61.
[47] Mason C, Kandel ER. Central visual pathways. In: Kandel ER,
Schwartz JH, Jessel TM, editors. Principles of neural science, 3rd ed.
Amsterdam: Elsevier; 1991.
[48] Milner AD, Dijkerman HC. Direct and indirect visual routes to action.
In: de Gelder B, de Haan EHF, Heywood CA, editors. Out of mind:
varieties of unconscious processing. Oxford: Oxford University Press;
1999.
[49] Milner AD, Dijkerman HC, Pisella L, McIntosh RD, Tilikete C,
Vighetto A, Rossetti Y. Grasping the past: delay can improve
visuomotor performance. Curr Biol 2001;11:1896–901.
[50] Milner AD, Goodale MA. The visual brain in action. Oxford: Oxford
University Press; 1995.
[51] Milner AD, Paulignan Y, Dijkerman HC, Michel F, Jeannerod M. A
paradoxical improvement of misreaching in optic ataxia: new
evidence for two separate neural systems for visual localization.
Proc R Soc Lond B 1999;266:2225–9.
[52] Paulignan Y, MacKenzie C, Marteniuk R, Jeannerod M. Selective
perturbation of visual input during prehension movements. I. The
effects of changing object position. Exp Brain Res 1991;83:502–12.
[53] Perenin M-T, Vighetto A. Optic ataxia: a specific disorder in
visuomotor coordination. In: Hein A, Jeannerod M, editors. Spatially
oriented behavior. New York: Springer; 1983. p. 305–26.
[54] Perenin M-T, Vighetto A. Optic ataxia: a specific disruption in
visuomotor mechanisms. I. Different aspects of the deficit in reaching
for objects. Brain 1988;111:643–74.
[55] Pisella L, Grea H, Tilikete C, Vighetto A, Desmurget M, Rode G,
Boisson D, Rossetti Y. An ‘automatic pilot’ for the hand in human
posterior parietal cortex: toward reinterpreting optic ataxia. Nat
Neurosci 2000;3:729–36.
[56] Prablanc C, Echallier JF, Komilis E, Jeannerod M. Optimal response
of eye and hand motor systems in pointing at a visual target. I. Spatial-
temporal characteristics of eye and hand movements and their
relationships when varying the amount of visual information. Biol
Cybern 1979;35:113–24.
[57] Proteau L, Marteniuk RG, Levesque L. A sensorimotor basis for
motor learning: evidence indicating specificity of practice. Q J Exp
Psychol A 1992;44:557–75.
[58] Ratcliff G, Davies-Jones GAB. Defective visual localization in focal
brain wounds. Brain 1972;95:49–60.
[59] Redding GM, Wallace B. Adaptive spatial alignment and strategic
perceptual-motor control. J Exp Psychol Hum Percept 1996;22:
379–94.
[60] Rizzolatti G, Fadiga L, Matelli M, Bettinardi V, Paulesu E, Perani D,
Fazio F. Localization of grasp representations in humans by PET.
I. Observation versus execution. Exp Brain Res 1996;111:246–52.
[61] Rondot P, De Recondo J, Ribadeau Dumas JL. Visuomotor ataxia.
Brain 1977;100:355–76.
[62] Rosenbaum DA, Meulenbroek RJ, Vaughan V, Jansen C. Posture-
based motion planning: applications to grasping. Psychol Rev 2001;
108:709–34.
[63] Rossetti Y, Pisella L. Several vision for action systems: a guide to
dissociating and integrating dorsal and ventral functions. In: Prinz W,
Hommel B, editors. Attention and Performance. XIX. Common
mechanisms in perception and action. ; 2002. p. 62–119.
[64] Rossetti Y, Pisella L, Vighetto A. Optic ataxia revisited: visually
guided action versus immediate visuo-motor control. Exp Brain Res
2003; in press.
[65] Rushworth MF, Ellison A, Walsh V. Complementary localization and
lateralization of orienting and motor attention. Nat Neurosci 2001;4:
656–61.
[66] Savelsbergh GJ, Whiting H, Bootsma R. Grasping tau. J Exp Psychol
Hum Percept 1991;17:315–22.
[67] von Hofsten C. Development of visually-directed reaching: the
approach phase. J Hum Mov Stud 1979;5:160–78.
[68] von Hofsten C, Fazel-Zandy S. Development of visually-guided hand
orientation in reaching. J Exp Child Psychol 1984;38:208–19.
[69] Wolpert DM, Ghahramani Z, Jordan M. An internal model for
sensorimotor integration. Science 1995;269:1880–2.
[70] Woodworth RS. The accuracy of voluntary movements. Psychol Rev
Mono 1899;Suppl 3:3.
[71] Zelaznik HN, Hawkins B, Kisselburgh L. Rapid visual feedback
processing in single-aiming movements. J Mot Behav 1983;15:
217–36.
S. Glover / Neuroscience and Biobehavioral Reviews 27 (2003) 447–456456