Embed Size (px)
Citation preview

Haem Gone Bonkers
Haematology Is the study of blood, blood consists of cells, these cells are red and wh\te much 1\l<.e the American flag but that's stars and stripes and therefore doesn't really apply here. In this viscous soup
. ·there are also little pancakes called platelets. They klnda float around and just play matchmaker between the reds and the whites. Platelets are to blood what cupid Is to love, you get the picture right? Blood travels throughout the body like a river through a canyon. Much like a r\ver though \t too can run dry and when that happens you need a blood confusion, that's when some strangers blood gets dumped Into your body and In that confusion you get transfused. Blood Is pumped throughout the body by a fist ... oh no I mean an organ the size or a fist. Any case bloods real reason for existence Is that It Imports o_xygen to all your tissues and exports carbon dioxide from them. You may now be asking how this Import/export scenario occurs1 well think of It like this. Ok glad we got through that. Moving on, blood plays a critical role In clotting. Remember the time when you cut yourself and that red stuff' poured out of our body ... well after a while the flow of blood slows down and a mesh-like weave grows over your wound, that's a scab, and clotting klnda causes that. Now let's get down to the serious stuff' regarding blood. Vampires dig It and it's a turn-off to quesy-weasy people. Other than that blood Is like the fuel in your car, It's costly and when your tank runs dry you're screwed I So In conclusion, we can then summarize the following:
• Blood Is red • Blood Is of a liquid constituency • Blood Is Important • Blood Is costly • It flows like a river • And Flnally ... a blood confusion could save your life
How do I get clean oxygen blood, well that's really easy, you just open your mouth and swallow whole packets of air, air Is made up of oxygen, nitrogen and other gases. For the purposes of this summary though we shall only analyse oxygen. Oxygen Is made up an oxy and a gen, when these two combine you get a gas that Is for all Intents and purposes the most widely used and popular 9as on the planet.
Now you must be wondering how we purge ourselves of dirty carbon blood, well that's the easy part and that's why I have left It for last .. People normally slit their wrists when they want to purge themselves of dirty carbon blood but alternatively you can bleed out and cleanse yourself the urbanretro wa.y, walt for It, by snorting crack cocaine, that way it looks cool as It run.s out your nose and yo!) get the benefits or a sensational "high" but that's another summary all together and I feel we hav~_covered enough today •
. Remember: When in doubt just ooen your mouth arid swallow big packets of air, the rest will take care of Itself. And don't forget to always keep a stranger close in the event you might" need to stay alive I
By Harry Haemorrhage 16/09/2009

The Red cell
Revision:
c Jnl y source of haemopoiesis in adults "' Ceq!!]! s!ce!eton & Proximal long bones . J ux !aglomerular cells in kidney- Produce erythropoietin (EPO)- in response to !02 and fandrogens -stimulate erythropoiesis . (';~tho In gical process interferes with normal baemopoiesis =Results in extramedullary haemopoiesis "' Liver & Spleen . 1"un10vt:r: Red cell= 120 days, Pits= 7 days, Granulocytes= 7 hours
l'tJBR.EDGEW PRONJRMOBLAST- ltondensed nucleus, eventually lost • I Myeloproliferative disorders, Deficient erythropoiesi6
L LAT£ NORMOBum only in circultion in extramedullary haemopoiesis
1 . . RSTlCULOCY'fm- Remains in marrow for 1-2 days, Residwil RNA, Able to synthesize Hb, (1 = t p~ti~~ (as a result of, eg Haemorrhage/Hemolysis)
1 · I · I (! = ~ productiorr.(eg 1II0.1'1Y7W failur•J C!P.CULATION.ilLooseRNA • Bloodloss~l .. ----·· ------~~~
- i 1 MATURE- for 1-2 days
1 BR.YTHROCYT&~ 120 days
oesniucrroN- in reticuloendothelial system:~ ~·-•LEx~cess~i~ve~ha~em~o~lY51S~· .!_7~~ OLOB~HAEM':l ~-
IRON'} reutilized BILIRUBIN .l.. bind to albmnin- then to liver, etc.
• Hl'l = Haem & Globin (transport 02/C02) -Globin .. 2 alpba-&2 Beta-chains ·Synthesis occurs in mitochondria of red cell
Normal Values for adult peripheral bid Men Women
So where can a problem be? At big anows ...
Hb-(g/dL) PVC(haematocrit,UL) RCC(1012'L) MCV(fL)
~f!' 5:.f675-'l; 0.42-0.53 . 0.36-0.45 4.5-6.0 3.9-5.1
. (_ il\ 1...>:4.'NL ..-,...6"S€...=- ~u.\T;t>\e_ \0-;e\D'N'O- ~a;:_ "bNU:> p ·
-~ C..~u.A fcu..~(Pc.'?...(AD.A) MCH(pg) MCHC(g/dL} WCC(L091L) P1ts(I09/L) ESR(mmlh) Reticulocytes (% of total RCC)
Old film abnormalities:
She tlbnormalities: Variation in size
80-96 27-32 32-36 4-ll 150400-, <2~ o-.Z.:Z.tr.'o
Anisocytosis: ~lncrocytosis: Microcytosis:
Increase in diametcr(tMCV) Decrease in diameter (lMCV)
Shllpe abnormalities: Normal: Discocyte (biconcave) !'oikilocytosis: Variation in shape
CPt~ ~ ~i-Ti~
~Lt:: H:r:..v
Spherocyte: Spherical RBC {hereditary spb.erocytosis, immune haemolytic anaemia) Sickling: Crescenteric cells (sickle ceU anaemia) fl ir.atre shapes: severe uraemia & carcinomatosis Fragmented cells 1 ~crustocytes) : Elliptocyte: rarget ceU: r c:ardrop cell:
Inclusion: Nuclei: II einz bodies: I lowell-Jolly bodies: !Jn•ophilic stippling:
. . .. Split R.BC (Microangiopath.ic haemolytic anaemia, prosthetic heart valve) Oval, elongated RBC (hereditary elliptocytosis, megaloblastic anaemia) bell-shaped, looks like target on dried film (liver disease, haemoglobin S & C, thalassemia, Fe deficiency) Single pointed end, looks like a tewdrop (myelofibrosis)
Immature RBC, indicates serious medical condition (severe anaemia, leukaemia, bone marrow mets.) Denaturated haemoglobin (G6PD deficiency) Small nuclear remnant with colour of pyknotic nucleus (post splenectomy, hyposplenism, haemolytic anaemia, megaloblastic) Deep blue granulations of variable size & nwnber, pathologic aggregation of ribosomes (lead intoxication, thalassemia)
j
J
]
j
'J
I
J I
.J
J
~ J
J
J
1
.L
I _ i ___
I .l..
i I
·'-
t I
i
"'-i
J.

J
_I
NB:Pale Pt is NOT anaemic, just pale-----prove anaemia with labs! I
Anaemia- Decrease in number of circulating RBC/mm3, the~ or the volwne of packcd-cells/1 OOm1 -Nar A DIAONOSIS! -manifestation ofunderiymg disorder
Aetiology: Anaemia can result from 1 of3 basic mechanisms: APPROACH~ 1 )Blood loss (> reticulocyte.r) 2)Deficient erythropoiesis (< reticu/ocytes) 3)Excessive haemolysis (> relicu/ocyles) l)SxiSt .
l)Sx: Fatigue Breathle$sness Patpitattons )2i.Biness Tinnitus Heiidaehe J:nsamnia Angiea
Sg: PaUorof
*Skin *Mucous membranes *Palms *Col\iunctiva
Tachycardia Cardiac dilatation Systolic flow murmur
\oeaema1
2)Hx & Exam- try to find cause! Background: Mediterranean, Asian, Black (Thalassemia), Black (SickiCH:ell)
Vegan- Vit B 12 deficieocy Alcoholic -Folate deficiency
2)Hx!Exam ·• try to ID cause clinically. 3 )Bid loss first consideration (acute or chronic)
-Hx/Exam/stool test for occult bid -Transfusion needed?
4 )Bid loss 110t daectcd: •
-DoS/I: \ f\SLT bih-t- ~\~' S)Decreascd production vs ia:rcascd l.. !....;;:::_-.JF-----'-,.--1 destruction? (n:ticulocytes) -t \~ c:.u.lc:x::.t'Go .
6)Anaemia vs Pancytopenia . 7)Based onMCV· 8)Further investigation based on results
Cancer, rheumatic disorders, chronic inflam diseases - suppress bone marrow or enlarge spleen. Hx of mc:lena, menorrhagia, epistaxis, hematochezia, hematemesis Hx of weight loss -cancer Diffuse severe bone/chest pain- sickle cell disease Glove/stocking paresthesias -Vit 812/Folate deficiency Past medical Hx: past anaemias, therapies, Sx 's of rena~ liver, endocrine disturbances, AIDS or other chronic disease Fam Hx - NB in hereditary anaemia, ask· about anaemia, jaundice, gall bladder disease, SJ2Iepectomy,
Exam: Sg's PLUS Hepatomegally?, SplenomegaUy? - Tbalassaemia Haemorrhagic shock- Hypotension, Tachycardia, Tachypnoea, Confusion Pale, Jaundice & dark urine- Haemolysis? · Fever+ Murmur= IE, a possible cawe of haemolysis Peripheral neuropathy- Vit Bl2 deficiency Glossitis - B 12 deficiency/Fe dificiencx Koilonychia, brittle hair, brittle nails, angular stomatitis, atrophy of papillae of tongue, dysphagia- Fe dificiency Bone deformities - Thalassaemia Major Leg ulcers - Sickle cell disease, thalassaemia intermcdia
3)Acute or chronic bld loss is your FIRST consideration, so exclude it. Hx: melena, menorrhagia, epistaxis, hematochezia, hematemesis? Stool tc.1t for occult hlood
4)Blood loss not detected, Do the following labs: l)FBC, (OffNB importance: MCV, MCH, RDW) 2)Examination of peripheral smear (Esp. the Retlculoeytes) J )Serum Bilirubin, LDH & Haptoglobin- In ·haemo!fiis vs haemorrhage
FBC includes: -Hb
Nonno.l RDW >Anaemia of chronic disease >Thalassaemia
-RBC count ·MCV (mean corpuscular volume- a measure ofRBC size) =Micro/Normo!Macrocytic v -Hct (measure of% ofbld made up ofRBCs) ·MCH (mean corpuscular Hb- a measure of Hb in individual RBCs) = Hypochromic/Normochromic -MCHC (measure of Hb concentration in individual celb) < TRDW
>Fe deficiency >Dual deficiency
-RDW (RBC volume di;;tn'butio~ width) -pcgree of variation in RBC sizq-T~W may b~ the only indicator for a mixed deficiency, eg.llllcrocwtic + macrocytot1c <ltsorder, or m1crocytosu + rettculocytosts.
Peripheral smear: -V cry sensitive for excessive RBC production & haemolysis. -Recognize abnormal cells shape, size as descn'bed on previous page) -Reticulocyte count: ~essive production, due to· (haemorrhagclhaemolysis), J. =decrease marrow activity (marrow failure)
Dillrubin & LDH = T in haemolysis, normal in bid loss Haptoglobin (sucks up free Hb in ci.tculation) = ~ in haemolysis, normal in bid loss
>Myelodysplastic Syndrome
\
>Uver disease >Pernicious anaemia >Folate deficiency .._______,

7)~uw dus:;ify_ a~c~r~i-~!~CV -~-~~!!culocl_t':s. __ _
ttoll ,·rllntll"'"r"nce . MlCROCYTlC NORMOCYI'IC MACROCYTIC fMCV(>lOO) lnclltcot !MCV(<80) Normal MCV(80-100)
.\,lpo•r .. ncc or_ 114no ~hrr.qw
' ormoblastic J ~ --~--·· ··· · ·- - ..
fltfl'diC >Fe deficiency . yclodysplasia >Haemolytic >Alcohol >Thalasaemia : yelofibrosis >Post bld loss >Anaemia of cbro · '. plasia disease . Infiltration >Sideroblastic · leukaemia etc)
Altered Haem/Globin iynth~
.>Liverdiseaso · • >Eudocrinc
(thyroid,add.isons)
Deficient EPO or inadequare!$!011SC to it
1 lo ti~t1hcr investigations, depending on your "narrowed-down" results.
!ron deficiency Anaemia <Mlcrocvtic ClMCVl. Hypochromic l!MCHll ..
)>
)>
)>
Inadcquite Fe for Hb synthesis Hb maintained as long as possible until Fe-&tores are depleted. Causes: a)! intake
b) TabsOrption ( eg. post gastrectomy) c}f demands (growth & pregnancy} d)Bioodloss(u~,hookwo~,e~)
~ 0 ~c~~ \,jot. e. .
~ ~o~P'tio~ · :~~~~~c)~. 1'h\.,l\Q!6 .
I
C'lln Pic: I llritt!IS hair 1 nrtttle nails
Hx: Diet, NSAIDS, Bid in faeces (hacmorrhoids/CNhookworms), menorrhagia? S\I: FBC & Smear.,. microcytosis, hypocbromic, poikilocytosis, anisocytosis, target cells
Iron studies- Serum iron L
rotaiiroQ binding c~r~ t I Scmm ferritin (stot; L "&~GNOS~can also decrease in ! Koilonychia (spoon shaped)
\
·Angular Stomatitis i ·Atrophy of filliform papillae of 1 rongue
- · · · - • A & inflammation) S~luble transfer receptors J --Used to differentiate btwn Fe ~ deficiency & anaemia of chronic
disease = normal \ ·l'lummer-Vinsoa/Patterson··!Jrown-Kelly syndrome:
·, •Glossitis \.. •Dysppahgia
•Rerropharyngeal Web
Transferrin (transport) <_~9% Diff dx: Thalassacmia, Anaemia of chronic disease, Sideroblastic anaemia ( in all of the the
J.eruiii'Fenitiii=no:..~ . Mx: Fe eficiency anaemia~~ dx.---Look for cause
l}Rx. underlying cause 2)Give .!L!l!!.to correct anaemia ~errous sulphate 200ma- ts!s. best abmrbed fasting)
.--22_Ba?lcw.ctlro.n.stores (Administer long enough to replenish stores -up to 6 magqw ~ack of comoliancefcontinuing haemorrbaie/wrong dx, eg Thalassaemia
Parental Fe= ll'iUslow IV- fn GIT disease, eg crohn's
moN: Iron =Haem-iron (frm meat) better absorbed than non-haem iron (cereals)
Fe3+ =insoluble ferric fonn Fe2+ 2 Better absorbed
Absorption "'First in duodenum Inside mucosal cell, either transferred to plasma, or stored there as ferritin & lost into gut lumen when mucosa is shed (regulates Iron balance) . '.• ·.- ~ -;~ . - ~ - r~(."-\.1-'•(~ -:: i ~ .- . .
Transport= Bound to transferring (Beta-globulin synthesized by liver) Most irou bound to transferring comes fun macropbages in reticuloendothelial system (dead RBC) & not frm absorbed iron.
Iron stores= 213 of total body iron is in cin:ulatiou (Hb) Iron stored in reticuloendothelial cells, hepatocytes & skeletal muscle cells 213 stored as .ferritin (soluble). & 113 as haemosiderin !Insoluble)
J
J
J
I j_
l
! ..L.
I .L
I
J
! J.

Anaemia of Chronic disease
Pathuphys:J. Release ofjmn from marrgw · l EPO } Mediated by inflame.cytokines, cg.ll..l, lNF ! Red cell survival
>~ :> due to cwtc ipf,.,tign (TB, IE, osteomyelitis) or inflam.disease (Chron's, RA, SLE, CA) J,> S/1: erum iron J.
TIBC! ~erum f~tjp !!Jmal I
Slderoblastic Anaemia
:> :> > > > >
Causes: lnhereted -X-linked
SII:
Mx:
Accumu(atjon of Jmn jn mjtoohpndrja of erytbroblasts- disordered Hacmsynthesis forming ring of !ron around auc(a!S Hypochromic Microcytic- clue tg ineffective haem synthesis Refractory anaemia Excess iron in marrow1 & _ring sideroblasts in marrow DX: Presence of rinS sidcrobla5ts ·
Acquired -Myelodysplasia -Myolopmliferativo disorders -Myeloid leukaemia -Drugs, cg Isoniazid -Alcohol abuse -Lead toxicity . -Others: RA. CA, Megaloblastic & Haemolytic anaemias
Serum iron t · Serum TIBC ~ normal Serum ferritin T Serum soluble transfer receptors oo!ID8Vi
Withdraw alcoboV4rugs Sometimes respond to 12yridoxinc. Folic acid to Rx accompanying deficiency
The Thalassaemias
Normal= 1:1 production of Alpha & Beta chains (globin in haemoglobin) Thalassaemia = "imbalance" globin chain pmbuctiQn (too manvJtoo little alpha/beta):
!)Precipitation of globin chains in red cell precursor- pctive ezythro~iS§is · c-------}-t)Precipitation of globin in mature RBC- haemolysis ' · "' LBeta Thalassaemia0
Homozygous,. No notmal B-chains 12roduced (B,) or _very reduced (B•) Thus eltcess alpha chains--- precipitate-- ineffective erythropoiesislhaemotrsis = J.Hb A (Adult Hb)
Heterozygous = Symptomless 011crocytosis :1: mild anaemia Molecular genetics- defects mainly point mutations, ather than gene deletions as in alpha thalassaem.ia
Clinical Svndromes:
Thalassaemia 1\lfinor (trait): Common carrier (heterozygous) Asymptomatic/mild anaemia Microcytic, b.ypochromic, but normal serum ferritin & iron stores (not Fe dcficie.!!!) No Iron Rx
Thalassaemia lntermedia: Symptomati<;, moderate anaemia (7-10) Do not require regular transfusions Combined homozygous Beta & Alpha Thalassaemia Spleaomeg, bone deformities, Leg ulcers, gallstones. infections .
. Thalassaemia Major (Cooley's anaemia): Most present..:::..L.Yr .Failure to thrive;;;tcterial infections Severe anamlia
Extramedullary baemopoiesis- Hepatospleaomeg, . .
~Suppress ineffective erythropoiesis Prevent bone deformities, allow normal growth & development Folic acid supplements
. Bone expansion (Thalas$aemia facies, xray slaill = "hair on end" Xray hand=- tfiliiii"ed cortex)
Regular transfusions (Hb > 1 0). If regular transfusions needed - do splenectomy> 6 yrs of age (prophyla;ds) Iron overload due to transfusions- damage to endocrine glands,liver, pancreas, myocardium= Give _ch~lating_ agent (D:sfcrriox~e)
a-
I
1.
I
I
\ ,\lphll Tltalassaemia
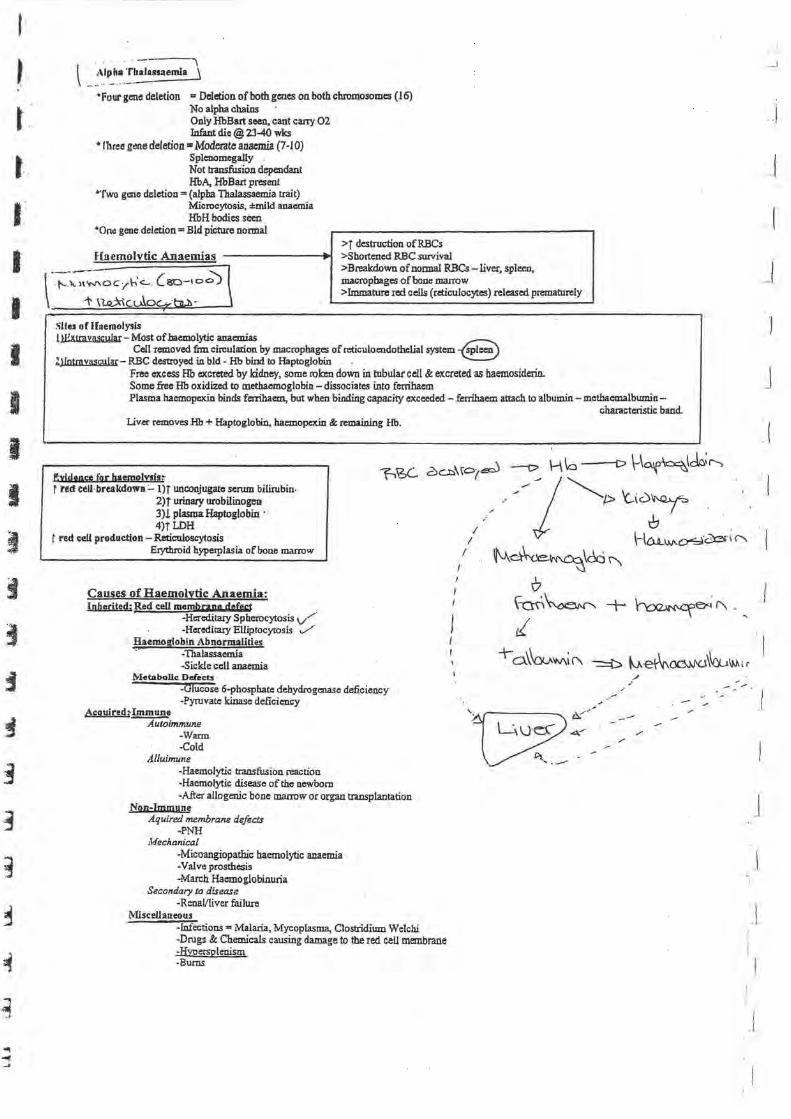
• four gene deletion = Deletion of both genes on both chromosomes { 16) No alpha chains Only HbBart seen, cant ca.ny 02 Infant die@ 23-10 wks
• lhree gene deletion • Moderate anaemia (7 -10) Splenomcga.lly Not transfusion dependant HbA, HbBart present
•Two gc:ne deletion= (alpha Thalassaemia trait) Microcytosis, :!:mild anaemia HbH bodies seen
"One gene deletion= Bid picture normal
Haemolvtic Anaemias --------l~
v;:-::~oc,h'<- L80-lO.;; I 1' \ l.Q..:X\ c. uloc:.... h..b · _1
Slles or Uoemolysis
>T destruction ofRBCs >Shortened RBC survival >Breakdown of normal RBCs -liver, spleen, macropbages of bone marrow >Immature red cells (reticulocytes) released prematurely
UHxlrnynscular- Most of haemolytic anaemias Cell removed fnn circulation by macrophages of reticuloc:ndothclial system -8
ljlotrnynscular- RBC destroyed i.o. bid- Hb bind to Haptoglobi.o. . Free excess Hb excreted by kidney, some roken down in tubular cell & excreted as baemosiderin. Some free Hb oxidized to methaemoglobi.o. -dissociates into fcrribacm Plasma hacmopcxi.o. binds fctrihaem, but when binding capacity exceeded - ferrihaem attach to albumin- mcthacmalbumin-
Liver removes Hb + Haptoglobin, hacmopcxin & remaining Hb.
fl!yipeoce for baemo!vsls; . r red eell·breakdowa:... I)T unconjugate serum bilirubin.
2)T urinary urobilinogen 3)! plasma Haptoglobin· 4)TLDH
t red cell production- Reticuloscytosis Erythroid hypetplasia of bone marrow
Causes of Haemolytic Anaemia: Inherited; Red cell membrane defcst
-Hereditaty Spherocytosis if -Hereditazy Elliptocytosis ,_/
Haemoglobin Abnormalities ·' -Thalassacmia
-sickle cell anaemia Metabolic: Defe<:ts
-Glucose 6-phospbate dehydrogenase deficiency -Pyruvate kinase deficiency
Acquired~ Immune Autoimmune
-Warm -Cold
Alluimune -Haemolytic transfusion reaction -Haemolytic disease of the newborn -After allogenic bone marrow or organ transplantation
Non-Immune Aquired membrane defects
-PNH J'v.fechanical
-Micoangiopathic haemolytic anaemia ·Valve prosthesis -March Haemoglobinuria
Secondary to disease -RenaVIiver failure
~fiscellaneous -Infections= Malaria, Mycoplasma, Clostridium Welchi -Drugs & Chemicals causing damage to the red ceU membrane -Hvoersplenism -Burns
chatacteristic band.
/ ,·
' ' •
.J
J
_j
.J
.J
- .. -""" .
J
I _ l ,,
1
_L

Red Cell Membrane Defects
Hereditary Spherocytosis (HS)
Most common inherited haemolytic anaemia 1/5000 Defect in red cell membrane= Red cell loose part of cell membrane as it pass through spleen Surface: Volwne ratio decrease= cell becomes spherocytic Spherocyte- More reg!d, thus less deformable- cant pass tf1rough splen jc mjcmcjrcu!ation- PrE
Clln pic: SII: Jaundice @ birth Mild anaemia Anaemia, Splenomegally, leg ulcers As with many haemolytic anaemias:
Bld film- spherocvtes & reticulocytey Haemolysis (increased !rilim!Lin,Jllli, decreased_ Haptoglobin) Direct antiglobulin ( coombs) negative in sobcmcytosis, ruling out autoimmune haemolytic anaemia -
Aplastic, Haemolytic, Megaloblastic Crisis may interrupt disease
Mx: Spleen (site of cell destruction) must be removed (increased bilirubin & gallstones confirms choice for removal) (splenectomy -lifelong penicillin) folate levels momtored Prophylactic folate
{. Cl' I Haemoblobin abnormalities ~· · l
d ·.,. . Globin chain production- Thalassacmia r.--Structure of Globin chain- Sickle cell Combined defect chain production & structure
Sickle cell anaemia A\o~ Q;:lo~~ c-b~ ~\~\e. = ~ ~\e;,.l 'oi\l7 Mainly in~ (25% caw the gene- Sickle cell Hb == $ingle-bl1Se mutation of adenine to ~e)
-Jiomozyanus state (sickle cell amu:mia) = Both genes are abnoqnal-!!2§§ - Severe -Hetemzygm,r; state (sickle cell tmi!) =One chromosome cany the gene- HbAS -No sx. 's
J flexibility of cells, rigid. sickle appearance . Initially reversible- repeated sickeling -loose membfcUJe flexibility- irreversibly sickled Sickeling produce: a)! RBC survival .
f )Impaired passage through microcirculation- obstruction of small vesels )> @ickeling precipitated fY: ~. :Oehydration, Col, _acidosis, HYJ!oxia
l.ln.l!.c: . ....:::::::.. fh•~ ;1'. ~~ ., e.:±,
~~1ifSJ;j\:mld feet~"~ (~~ . Long Term problems- nearly every organ affected Growth & development: ! weight & height
-Pain in bo -femur, hwnerus, vertebrae, ribs, pelvis
~~:!;!!;!!.!~~;~~~~~ rop m no.
i'vLt:
Splenic sequestration= Painfull enlarged spleen, splenic Pooling of RBCs, later- fibrotic Non-functioning spleen.
Marrow aplasia= Follow infection with Parvo B 19 --= · ::::=-=- -rrm. no rettculocytes
S/1: FBC: !Hb (6-8) T reticulocytes
Bld film: features of hypersplenism · Sickeling
Sickle solubility test Hb electropb.oresis Screen parents
>Avoid precipitant >Painfull attac!G =inpatient supportive Rx (02, fluid, Ab's, analgesia) :J"ruiaemia a Transfuse only for: Hf, stroke/TIA, A.C.S, acute splenic - sequestration, aplastic crisis
>Solenes;tomy may be lifesaving >Hydroxycarbamide - T HbF
! episodes of pain, AC.S, ne:d for bid transfusion
>Bone marrow transplantation
Delay in sexual development Bones: chr9nic io.fa.wts (due to vaso-occlusion)
A VN of hips, shoulders, compression of vcitebrac:, shortening Of bones in hands & feet p . !! ~myelitis commonest
Infections common in susceptib1e tissue (bones, lungs, kidneys) Resp: Acute sickle chest pain (up to 30%), caused by infection, fat
emboli frm necrotic bone, pulm.infarcts Pulm.HT & chronic lung disease---commonest cause of death
Leg ulcers: Spontaneous (vaso-occlusive) FoUowing trauma
Cardiac: Cardiomegally Arrhythmias Iron overload cardiomyopathy MI due to thrombi
Neurological: Cx in 25% TIA. fits, cerebral infarction, cerebral haemorrhage, coma
Cholelithiasis: Pigmented stones due to chronic haemolysis Uver: Cbronic hepatomegaUy & liver dysFx--Trapping of cells Renal: Chronic interstitial nephritis occurs Priapism: due to vaso-occlusion Eye: Retinopathy, vitrous haemorrhage, retinal detachment Pregnancy: l placental bid flow-abortion, lgrowth, pre-eclampsia
Sickle cell trait -No Sx, ,t,mless under severe anoxia (aeroplane}_£~esthesja -Protected against Plasmodium Falciparup1
-Bid count & film = normal :Dx by +ye sjckle test

I
I
I
I
I
I
I
I
I
I
I
J
I
I
I
i"letaboUc disorders of red cell
Red cdltnetnbolism; lh•d r.<•ll : ·····No nucleus, mitochondria, nlx>somes . ·•· ·Energy needed to main rain .tlcx.ibilir:y &: biconcave shape •.••• J Enzyme systems:
I) .GI):cni:Qic Emhden-Mevorhof (90% glucose metabolised)= m£ enzyme: Pyruvate kinase) l) Hexose Monophospahte pathway (10% glucose metabolised) .. NADPH (enzyme: G6PD) .1) Pappaport-Luebering shunt= 2,3 BPG .~
Glucose 6 Phosphate Dehydrogenase deficiency- Most common
}> Hexose monophosphate shunt system }> Oxidized glucose 6-phosohate to 6-phaspboglyccrate (reduction ofNADP - NADPH) ~ Common, presents with haemolytic anaemia, more common in men }> Chromosome 28 }> 400 structural subtypes > Single aminoacid substitution > 2 common variants: African {haemolysis self limiting, new cells frm marrow = normal)
Mediterranean {both young & old cells affected) > After oxidanl shock= !Hb - death
Clinical syndromes: -Acute drug induced haemolysis (dose related) ·Favism (ingestion offlava beans) .Chronic haemolytic anaemia -Neonatal jaundice ·Infections
S\[: FBC "'normal btwn attacks
Mx: Stop affecting. drug Rx infection ;.·
1\~bl-l sf\ {";j\i{v..~l(...., ..\1 '\h\\-~\d.oi\'. -to ~u.\D:j (1ll
tJ \-t~
During attack: mgwar contracted cells Bite cells Blister cells (Hb detached fnn cell membranes) Heinz bodies
Bld transfusion Splenectomy not helpful!!!!!
Reticulocytosis Hacmolysis G6PD deficiency DNA analvsis
Pyruvate kinase deficiency
)> Most common after G6PD deficiency )> ! A TP = rigid cells
S\1: Anaemia (Hb 5-10) Hacmolysis
Rx: Bid transfusion during pregnancy & infection Rx infection
Bld film: prickle cells Reticulocytosis
Splenectomy may improve condition
Autoimmune Haemolytic Anaemias > jRBC destruction due to autoantibodies l> +ve Coombs test (antiglobulin test) - detect antibodies on red cell )> Types : warm and cold Antibodies attach better to red cell ® .body temp, or~p
Warm Temp 37 c Type of ~ antibody Coombs test Strong +ve Causes 1' Idiopathic condition AutQi!Jm!une
Causes of:! c~ condition Lvmohoma~
Cold ! 37C
~..)
+vc Idiopathic Infections: EBV, Mycoplasma pneumonia
_Lymphomas
Warm: Clin pic= Anaemia@ all ages, short episode, later chronic, Jaundice + palpable spleen S\1: Haemolytic anaemia, Spherocytosis, +coombs, Autoantibodies Mx: C&.rticosteroids, Azathioprine, Splenectomy
Cold:@ ~temp S\1: Red cell agglutination, Coombs, IgG antibodies Mx: R.'t Underlying cause, if infective= corticosteroids+ splenectomy.
·l
1
J
I •. ..!.
Alloimmune haemolytic anaemias
> Antibodies produced in 1 individual react with red cell of 8Il0ther -Haemolytic disease of new bom -Haemolytic transfusion reaction -Allogenic bone marrow transplantation
Haemolytic disease of the newborn
> Fetomatemal incompatibility > IgG cross placenta (mother-fetus). Not IgM > Most common type- ABO incompatibility (mother 0, baby A) > ABO usually mild > RhD incompatibility less common- due to anti·D prophylaxis > Seositization- Due to fetal red cell to mother (Delivery/ectopic/miscarriage/bid transfusion/amniocentesis) > 1st pregnancy rarely affected
Clinpic: -Mild haemolytic anaemia -run- 18wks + -Hydrops fetalis = hepatospleo.omegally, oedema, HF -Kcmictirus due to severe jaundice in neonatal period (unconjugated bilirubin &. bile pigment deposition in basal ganglia = Brain damage, spastic, deafuess)
S\1: Routine antenatal serology- ABO & RhD determined Ultrasound- detect changes in fetal growth & CVS failure @birth of affected infant (coni bid obtained)
·anaemia ( t reticulocytes) -+veCoombs -!bilirubin
Mx: ~ . Mild= Phototherapy: Converts bilirubin to water-soluble 11:rivcrdin- exit via kidney, thus risk for Kcmictirus lBld exchange: coni Hb< 12, cord bilirubin> 60umoVL, later serum bilirubin> 300 umoVL, rapid T bilirubin.
Prevention: Anti·D given after delivery if Mother RhD -ve, Fetus RhD +ve. no maternal anti·D detectable in mothers ~erum. Anti·D = 500 iu 1M within 481us after delivery
Non immune haemolytic anaemias
Paroxysmal noct11rnal haemoglobinuria
> Rare aquired red cell defect > Clope of red cells sc:rusitive to destruction by activated compliment > Cells continuously haemolysed intravascular > Pits & granulocytes also affected·-Thrombocytopenia & neutropenia
Clin pic: Haemolysis, venous thrombosis, haemoglobinuria Precipitant"' infection, iron therapy, surgery D~ urine @ night &; early morning Some patients only anaemia & abdo pain Venous thrombi= Hepatic, mesenteric, cerebral veins
S/1: Haemolysis Anaemia Flow cytomctry Bone mam>w
Rx: Supportive (chronic) -bid traosfusion Eculizumab Anticoagulant for thrombi Bone marrow traosplant
May progress to aplastic anaemia, acute leukaemia.
Mechanical Haemolytic anaemia
Physical trauma in circulation- direct injwy • ceU lysis - resealing of cell membrane- 4istorted red cells - fagaents.
~ -Damaged heart valve; -March baemoglobinuria =damage to red cells in feet (prolonged marcb!ronning) .l\lficro Angiopathic Haemolytic anaemia (Due to abnormal microcirculation) ~.Malignant Hr, _eclampsia, HUS, m, rnculitis,
~-

I
I
• I
...
Anaemia due to Marrow failure
> Pancytopenia+ aplasia {hypocellularity) of bone manow > No leukaemia. CA cells in bld & marrow > Due to l in p\utipotential stem cells - fault in those remaining > Sometimes failure in 1 cell line .> Evaluate for Myelodysplasia, PNH, acute myeloblastic leukaemia
Causes: r: Congenital, eg. Fanconi's anaemia= autosomal recessive, skeletal, renal, c.as anonnalities. Z: Otemicals, eg.Benzene
Drugs: chemotherapy Idiosyncmtic reactions
Insectides Jnonizing mdiation Infections: Viral Hep, EBV, HIV, parvovirus, TB Pregnancy C- p)? u.:>C..
. /""'~~ / / Clin pic: Maqpw fujlurc =- Aniu:mia, bleeding, Infection
Bruisi!Jg, ~Iistm in mouth, b.lsm; ro;~: EcchymosiS, lvmphadcnopathy, h ato len m
SII : No reticulocytes Pancytopenia (death usually due to haemorrhage/infection) HYJ!Ocellular/Aplastic bone marrow
Mx: Supportive (RBCs &Pits) wbile awaiting manow tlllosplant Rx infection Marrow transplant< 40yrs + HLA identical sibling
> 40 yrs = possible host vs graft reaction Immunosuppressants
NB:[.t§O? cell aplliSia?r---@rmoma in 30% of cases 1. ________ _ Mlicr~miaS' rj}\lo@ bil-lA ~~~·~ · ) Megaloblastic Normoblastic } Appearance ofbonc marrow •
Vita~"' lhot· Folate.. t reticulocytes (haemorrhagelhaemolysis)
Liver disease
Megaloblasti~a~eibflf'
VltBll:< > > >
Delayed nne lear maturation of erhthrocytes in bene marrow Seen in l. Vit B 12, lfolate; myelodysplasia due to dyserythropoiesis Key problem: Block in DNAkkthesis owing to inability to methylate deoxyuridine monphospbatc to deoxythymidine monophosp te, which is used to build DNA
Synthesized by microorganisms: ;. Found in meat, fish, eggs &. mille, not in plants • Main fx: ~ylation ot:homol)ysteine-to methionine with demethylation of methyl THF polyglutamate to 1HF. (THF = substlllte for folate synthesis) Absocbtion: Bind in stomach to ~binder (B 12 binding protein, related to .PLasma transcob~I). fml.ll!iy,a. Bind to intrinsic. factorr Intrinsic factor= frm parietal cells ( canies vitb 12 complex to ileum). Vit B 12 enter ilia! ce~ IF remain in lumem Vit B 12 enter bone mirrow via transcoballamin II.•
Causes of L Vit B 12: Low intake (vegans) L absorbtion =stomach---Pernicious anaemia
--Gastrectomy ---Congenital deficiency in IF
=small bowel----· -lleal disease ---Bacterial overgrowth
Pancreatitis Coeliac disease Metformin
---Tropical sprue ----FISh tapeworm
____ j
J
I
1
· _ _ (
_/
I
J
J
1

.. I
rcrojcjous Anaemia
Autoim.nuule disorder A.;; b ~ Atrophic gastritis =Joss of parietal c.d§ =: ~ IF = ! B 12 absorptiQ_n
\L CJ..'D .::> •
Autoimmune gastritis = affects fundus = panetaYchief cells replaced by mucin-secreting cells= l IF secretion
( ~rticostcroids help!!! Clio pic: lemon-yellow colour (combination of pallor & mild jaundice)
:!: red, sore tongue (glossitit} ~
:!:~ar~c>~ . ~ci(,gm Y gcs =can be irreversible (megaloblastic madness.) .....Anaemia sometimes not clinically apparent ~ neuropathy- Periphetal nerves
? Symmetrical parasthcsia in fingecs & to~ (glove & stocking) ~ vibration sense & propriocqrtion Weakness & ataxia Paraplegia may result
Pallagra = dementia, dianboea, deciuatitis, periphcraliiCUl'Opathy, optic atrophy ~
S/U: Gastric biopsy if ?pernicious anaemia Hb=! Serum~=t Serum VitB12 = L Serum F~ normal or t Bone mmow =. tYPlciif1caturcs
Mx: Vit B 12: Hydroxycobalamin 1 OOOug 1M (S-6mg over 3 wks}, corticosteroids in pernicious anaemia, no transfusion.
[hue~ > Present in food as polyglutamate > Methylation of homocysteiJJ to methionine- requires mcthylcobalamin & methyl THF as co-enzymes > Green vegetable & liver/kidney ·
~s;t; ... ecoVdCJ'.; 'V0 ..._
F~ /V Poor intake (nutritional)
-old age -starvation -L SES -alcohol
Poor intake due to anorexia -GIT disease (parietal gastrectomy, celiac disease, crohn's disease) -CA
.~alasorotion -small bowel disease
Excess utilization - -physiological (pregnancy, lactation)
-pathological (Haemolysis (T RBC production), inflarn, CA with T ceU turnover) Antifolate drugs (anticonvulsants, me; · cthoprim Neural tube defects
Clin pic':" Asymptomatic._ anaemia, glossitis, NO neurogathy --SII: Serum measurements as others
Occult GIT disease?-small bowel biopsy
Mx: Transfusion not indicated Folate= S mgldal for 4 mo~~-ProphytaCtic folic .a~eid.m grcgnancy = 4QOmpy
Macrocytosis without megaloblastic changes · > Alcohol . > Liver disease > Reticulocytosis (hacmorrhagelhaemolysis) > Hypothyroidism l> Drugs: cytotoxics, cg.azathioprine
Diffdx for red tongue· >Candida >Fe deficiency > Vit B 12 deficiency >Folate deficiency

I
NnJoprollfera tive disorders .1) 'l'nlycythacmia hl Mydn!ibrosis (myelosclerosis) .:) My.:lodysplasia d) ~~~scntial thrombocythaemia "1 C :tmmic myeloid leukaemia
l'ulycythnemin
POLYCYTHAEMIA (t Bb) I l)Do Hb I True (absolute) A Relative: dehydration, bums, gaisboclc's syndrome
1 ~ r : Polycythaemia veta (myeloproliferative) I S)Bone marrow
J)EPO Inappropriate tEPO~ ~ .:,-\_,.c._~
Renal: tumours, cysts o\: ~e . Appropriate j EPO (due to chronic tissue hypoxia) I
! ~----~
liver: Hepatocellular Ca Cirrhosis
Endocrine: Adrenal tumour Other tumours: cerebellar haemangioblastoma
Massive uterine fibroma Bronchial CA
Drugs: EPO Androgens J S)CT/Socar
•r altitude •smoking (COPD) "Lung disease •cvs: R-L shunt *t02 affmity, eg.Mcthaemoglobinaemia
4)Lung Fx
PCV (Paclced eel~ volume) better indicator than Hb (Hb l in Fe deficiency)
n)Polycythaemla Vera
l> Clonal stem cell disorder, failure of apoptosis l> Usuall pt > 60 }> Tiredness, depression, vertigo, tinnitus, visual disturbances }> j B?, angina, claud:~ation, tendency to bleed
1 1 )
}> !]_Ching iftCIO hot bath] t:;.. . , l> Gout - due to increased cell tumo ver l> Cyanosis. Con_iuCtival infiltrates > ~plccn paloable in 70 n. Hgpatomegally 30% l> Cx: Thrombosis & haemorrhage
S/1: Hb & PVC = f Bone marrow- erythroid hYPerplasia
·Red cell volume = f Plasma volume • T Serum uric acid = f Leucocyte alkaline phosobatase = t VitB12 = i EPO = Nonnal or!
t WCC/Plts + Splenomegally + t PVC/Hb = PV until proven otlterwlse
lvb: Maintain normal blood count & prevent Clt
~V encsection Chemotherapy
Prognosis t~% progress to meylofibros.!J
""'- . . . ~I
HI blocker (for pruritis)
[_~~~~r_oo\w-Yth3~- Gaisbock's syndrome RCV- nonnal "-l plasma volume (thus relative polycythaemia)
.---.~)>~~.!!!!!0
> S~t.!lEes!' :r hYJ?erte~~v~ > Presents with MI/Cerebral ischaemia
Mx: Vcnesect10n & stop smoking /t;'\"-:::\it/;;\::'V\\o:\"u'\..Q~
J
1
"_I
, I
_j
I _j
I
1 ·'
b)Myelofibrosls
> Clonal proliferation of stem cells J> Fibrosis in marrow- due to hype~plasia of abnormal megakaryocytes > Myeloid dysplasia in liver & spleen
Clin pic: Very similar to CML Splenomegally iWCC Perisplenitis Z to plenic infiuct Gout, bmising, bleeding -thrombocytopenia
S\I: Anaemia Poikilocytosis (teardrop forms) jWCC/Plts Bone marrow aspiration= if.uuaw:ccssM:~lueto conditio~,
= r megajmryocytes~ Philadelphia eluomosomc absent---distinguish myelofibrosis fun CML' LAP f (leucocyte alkaline phosphatase) 1 serum urate ! serum folate
Main distinguishing feature (CML vs myelofibrosis) = appeamncc of JDIUIOW- Megalwyocytes
Diff dx: leukaemia ./ Lymphoma..,/ TB ./
Mx:
Malignancy ( r I Z) ..,/ Radiation ~
Supportive Bld tr.mstiJ.sion FoUcacid Analgesia Allapurinol Hydroxycarbamide Chemotherapy- reduce spleen size Massive spleen- splenectomy
Prognosis: mean survival= 3 yrs
c)Myelodysplasia
= absent Philadelphia chromosolllll
li> Group of acquired bone marrow disorders --defect in stem cells li> f bone marrow failure over serial measurements > Abnonnalities in all three cell lines (red/white/pits) > t morbidity & mortality > Mainly elderly
Clinp pic:(l(uacmia infection, bleeding= due to pan~o~
S\I: Pancytopenia
Different types - ring sideroblasts present in all types
MA: < 5 % blasts in marrow ·RBC/Plts transfUsion -~on-
> s % biilstSinai'iirow -~ -·~y(low dose single agent) ~C -~~Erin~Yek>b13sti~ < 60 yrs -Boiie marrow ~lant <S<J'"Yci (Hi:A matching ilonor) -~
d) Essential Thrombocythaemla
li> tP!~;> 1 000 x IO'IL > Brwsmg. b!ecdjn~ gyr li> S,p!egjc hypertrophy -~ recurrent thrombosis -- ~!enic atrophy ~ Distinguish fim Z thromf:iosis (haemorrllagc, connective tissue disorders, CA, splenectomy)
~\
I
I
I
it#
A Bit About the Spleen
largest lymphoid organ Left hypochondrium r."' Traube's space dull in enlargement 'l _. \I 'l==C "'S ~.J ·
2 anatomical co~onems: -Red pulp= sinuses .l.il.lc:d by cndoth~lial macrophages -White pulp= structure similar to lymphoid follicles Blood enters -White pulp--R~ pulp
4 majnFx's: 1} Old blood • Sequestration & phagocytosis
· Normal red ~ll is flexible. Pass through red pulp into venous system. Abnormal cell (via hypoxia, ! glucose, ! Ph} -.stuck in red puip- removed by phagocytosis. 113 of pits ~estrated in spleen.
2} New Blood .. Enramedullary haemopolesls :eluripotent stem cells proliferate during .haemolytic anaemias orThalassaemia major.
3} Blood storage-Blood ~ling. All enlarged spleen pool up to 40% of red cell mass.
4} Immunology • Immunological fx. 25% ofT lymphocytes & 1~% ofB lymphocytes are present in selecn.
$PLENOl'dEQALLY; m Is His Prlmarv Mlss!Onlf .IJLfWisiA: ·. G::-\';:::.0 .
Acute: IE, Infective moaonuclcosis, TyPhoid, septic shock \- -q: I.J , C 't--J\.. J ChroniC:" TB & brucellosiS - t Parasitic: Malana, Kila ND.r, Schistosomiasis
U1!J!.m: RA, sr:r,San:oidosis Humatolqzjslll: Haemolytic anaemia's
Haemoglobinopatbies Leukaemias,lymphomas, myeloproliferative disorders
~rtal hypertension:· Liver disease MlscellaneoiiS: Storage disease, amyloid, ncoplasias, tropical Splenomegally
~..._~~ ··--- -~- ~ ., . "E. ~SIVE SPLEEN: CML, Chronic malaria, Kala Azar, Myelofib~sis . ~
v ~ '-' ~ ....._, ......, .._,. ....... '--' '--' ~ -
Hypersplenis1Dr.f
@. o CUt.-I~AAye\b~t'oo9.s-
0 hl-6,\btk>-.
0 N--'fC..b\co..G~\. U.\l'-1'\. A0\I.J...W'
> ·>
}>
c ~At:; ~.o \ 'f\.U.~-.1\0-ean result rrm setenomegaUy rrm any cau.sc. o '(_ct \o. A -f:or Common due to haematolog.i:al causes, polt41··Hi, RA (felty's syndrome} & lymplloma It produces: Pan~oliEa.
· Ha OJ (due to sequestration ofRBCs) 1 plasma volume
Rx = depend on causft Splenectomy if severe anaemia/thrombocytopenia
SQelenectomy
Indications: Trauma ITP Haemolytic anaemias Hypersplenism
Problems after Splenectomy: Acute j in pits Thromboembolic phcmnomena r risk for infection, particularly pncwnococ
Post-splenectomy haemato/ogical features : -Thrombocytosis
Prophylaxis Post-splenectomy >Pneumococcal-< >Meningococcal >Annuallnfluen21r-> Haemopbillu.s influenze >Longterm Petr¥.500mg· ~2 hrly
-normal WCC/T lumphocytes & monocytes -abnormal red cell morphology: Howe[ Jolly bodies
Splenic Atrophy
)- In sickle cell anaemia--due to infarction > Coeliac disease· Ji' Dermatitis herpetiformis > Ulcerative colitis )- Essential thrombocytopenia·
Pappcnheimer bodies (contain sideroblastic granules) Target cells Irregular contracted RBCs
' - I
· - I
--1
!
.J
u • I
:J
J
J
l
l
I I
J..
The White Cell
,----Neutrophils Eosinopbils Basophils Lymphocytes{
Granulocytes
Neu trgohils
:> PrecUISor = Myeloblast (large nucleus, 2-S nucleoli) :> Mature neutrophil= nucleus 2-S lobes
Secondary granules -lysozyme, collagenase, lactofcnin :> Maturati011 !:ime = 10 days :> . --~~'t;.(t)ji:~ :> Infection/coticosteroids = Neutrophils released into circulation (frm marginating pool & bone marrow)
· cclls into circula ·o in ra id onse ("shift to left" on bid film) :> Fx: Ingcst&kjll bacteri!tfunsi. &:da!J!aSCdceJk -:> Ingestion--destruction: a)02 dcpcnant (hydrogen peroxide)
r-~-:--.....-:-:--.... b-"-')02'-'-<"_..-~cndcnt (lysosomal enzymes & lactofcrrin) :> LAP found in lcucocytes
tWee > 10 x 109/L in bacterial infection due to tissue dama~ Also in~. exercise, corticosteroids '-~ Any necrosis= release of soluble facton---~s~Seen u~
= release IL 1 - yrex :J :> Lcukaemoid reaction =:roduction of we-- severe infection, TB, malignancy infiltration :> I §oeryt.hCOblatic ana~-- nucleated RBe + we precursor in peripheral bld.
':" -~= Marrow infiltration, myelofibrosis, osteoperosis, myeloma, !~oma, Haemolytic anaemia, megaloblastic anaemia.
~ :> < 1,5 X 10'/L :> Absence of Ncutrophils---agranulocytosis :> Black pt's .. 1 wee :> Neutropenia =ii'jVF.tra::;-1 =m=-=o-::.st:-:c:::o:::mm=o::n:-:c::au:::s::e:-11 > Severs jQfe:ctjgp :> Administer Ab's in severe neutropenia :> Steroids in severe autoinunune neutropenia
Neutroohll Leucocvtosis (>10 x tO' ILl
Bacterial infection Tissue necrosis ( traumall'viT)
• Inflam (RA/Gout) Drugs: corticosteroids Haematological (myeloproli:f7leukaemoidl
Leucoccythroblastic) Physiological: Pregnancy, exercise Malignancy: bronchial, breast, gastric Metabolic: Renal failure, acidosis
Eosinophils
:> Larger than neutrophils > Nucleus = 2 lobes > Large cytoplasmic granules > Stain deep red
Neutropenll! (< 1.5 x 109/L)
Acquired: Vtral Severe bacterial
<Ee!ty:s ijlidrome:J Autounmune
• l'ancytopenia frm any cause White cell i!plasia
Inherited: • Ethnic (black pt' s)
Infantile agranulocytosis • Cyclical (2-3 wks)
EoslnophiUa
Allergy: . -Hayfever -Hyper.~ensitivity reaction
Pausites: -Ascaris lumbricoides< -Hookworms· :> Fx =phagocytic , involved in killing. protozoa & helminths.
:> Also involved in allergic .reactions ·• · Skin:
-Urticaria -Eczema -PemphigJJS
-Ca·· -Eosinophilic leukaemia

Ba~ouhils
}> Nucleus similar to Neutrophil
Basophilia Myeloproliferative dlsorcters:
-Polycythaemia -CML .
}> Filled with large black granules (histamine, heparin, enzymes) Inflammation:
. -Acute hypersensitivity -Inflam bQ.wl diseases
Iron deficiency ~ Physiological role unknown ;.. Binding of lgE = release histamine (bypmensitivity reaction)
Monoeytes
J>. larger than Neutrophils J>. Variable shape ~ Few granules > Precursor of macrophages
Lymphocytes
> Nearly half of circulating WC > Descent fun plutipotential stem cell > Small cells, little larger than RBC )> Dark staining central nucleus > T cells mediate cellular immunity > B ·cells mediate humoral immunity > Lifespan vazy, several days to years
Pancytopenia
./ Aplastic anaemia
./ Acute letibeuua (in subleukacmic phase)
./ Marrow infiltration: -malignant lymphoma -metastatic CA -myelofibrosis
./ H:mersplenism
./ Pernicious anaemia
./ SLE
./ Oisseminated TB
The platelet I
Remember: Haemos.tasi.:l depends upon interaction btwn: 1) Vessel wall 2) Pits 3) Clotting factors
Haemostasis • 2 nhases:
l'donocvtosu:
Infection~,~ -Bactcri~
Infiam:
~n::ti~SSU!Llli.wJ!~! - bowl diseases
Mau~ ~0 tuJDDiii})
t"J!fosytosis ection: -~ -~acteria!: Bordetella pertussis
Lymphoproliferative disease: :Qb. -.!YJEphoma
Post-splenectomy
!)~mary phase: damaged vessel constrict, pits form plua-am:st bleeding 2)Secondary phase: activation of coagulation system, with secondacy deposition oeesb to secure the platelet plug. ·
Pit= discoid, 2-4um., t'h"' 7 daysr Activated pit (via; ~~in, collagen) ~-b~ome ~phl;rical--:-extend pseudoohilia--~to subendothelium& other pits: · k>..>IS>fL ~-.u.\\.·ilo~ . Platelet binding to subendothelium =dependant on high molecular weight .von Willcb@nd tiicto~ (frm endothelial cells), which bridge platClet membrane glycoproteins &_subendothelial collagen.
Thro~ytonenla ~=J> menakacyoc:yte maturation faihuc
-l) tots consumPtion . 3) 1 segycsfratjon by spleen
Causes: ~ disorder ! productio ) HxJ?.oplasia: -~diopat ..-- :-drug induced; cvtotoxic:s~antimerabolites
b!filtrative: -Leukaemia, myeloma, CA, myelofibrosis
Thrombocytosb Pits raised most commonly in inflam process.
Cau!en Reactlvll! thi'Omoc:ytosls -cbroilic inflam disorders· -CA . -tissue damage -haemolytic anaemias -post-splenectomy -post-haemorrhage
Malignant thr.omboc:ytosls -r thrombocythaemia, myelofibrosis, CML
' I I
J
]
J
J
J
L
l l
. l
L

L
L
I
···:Osler-Weber-Rendu -Ehlers-Danlos
'P}~Je\~~.:.,ti,Q.,\11J...~td.em -ITP -TIP
~Jl~~~e . Vessel waD abnormalities ~leeding disorders: Osler-Weber-Rendu _ -HaemopliJ1ii"i\'~
1>- Hereditary baemorrbagic telangiecta/ ;, ~ · }- TeliUigtectaslll-~.~nasal passage, tongue, long & G.!T.... > Pulmonary arteriovenous malformations- hypoxia > Clm pic: Recurrent bleeding, especially epistaxis, or Fe deficiency due to GIT bleeding. > S\f!Ook t'or bleed -Gastroscopy · > Mx: Fe therapy & transfuSion
Ehlers-Danlos
> Congenital disorder of collagen synthesis > Joint hrperextensibilicy, skin elastici9', capillaries !'<1Qr1Y surm.llnlkd.~~~n l> Clin pic: ecchymoses common
Platelet function abnormaUdes 1IJ (Idiopathic thrombocytopenic p11rp11ra)
Autoantibodies directed at o1ate!et meumranc---rcsults in premature removal of platelet frm ciJculation More in females Sx\Sg ?f co~ective tissue disease ~elsuona · ormaJ bld filni, i pits, bone marrow = t mcgakarygcytcs Mx: prednisolo!!CJ ~fusions when bleeding, IgQ in life-tbmatcnjoe hac:rilorrhue
!!! c:r,:lirombotle thrombocytopenic p11rpura} NBf EXCLUDE IT WHEN RBC FRAGMENT a' PRES · ~.1\ t-. ·. · · ·- · · ~f -t:> ~ &c~~'~' ~IU-.I.V-.
> ~ve platelet aggregation- due to lame von Willebrand molcculss) 1J > Normally- von Willebrand protease (ADAMTS 13} '~" large von wille rand molecules into smaller ''strings". > In TIP, there is ! ADAMTS 13 (due to genetic abnormality in the enzyme or antibodies against it), thus .l!!fru!
mwtimers von Willcbrand--plts aggregation--platelet thrombi. > Clio pic = PENT AD: \Cl\""V=5 •
v1 )Thrombocytopenia ~Microangiopathic haemolytic anaemia (RBC fragment, a.k.a. schiztoc~es, on bld film) ~S Slt- seizures, confusion, coma (thrombi in vessels) v4)Renal Fx Abnormalities (thrombi in vessels) 0)Fever
l> Mx..:..fff.(contain ADAMTS 13) (NOT platelet transfusion!!) Corticosteroids
In HIV pt's =The pathophys differ. (HIV associated thrombotic microanglopathy) · HlV associated endothelial injury--results in t von Wilebrand production-thus Jelative deficiency in. APAMJS!3}. Mx: No studil:8". tO prove that ~rk.
Only proven therapy·~
PLEASE, NEVER MISS A TIP (RBC FRAGMENTS ON SMEAR!!), MORTALITY= 100% if not treated!!
Thrombocytopenia
> Thrombocytopenia causing bleeding= haematological emergency )> Rx: platelet transfusion -
Rx underlying cause.
The von willebrand protein (vWf), synthesized in endolth~lial cell my megak:aryocytes. 2 F:t's: !)acts as carrier ~tcGitor factor VIII. A defiCiei!Cyi~--secondary reduction in VIII.
2)form bn~ pl'Jite(;t :i su'&'iiidotbclium---allowing pits to adhere to damaged vessel.
abnormaJI~~CP.~ clinpic :~ ~ l f :"' ,-~()( ;s S/I: !vWF . \0 ' -.....--·
! vm . , -.. , ,.-3-~ ~ r in bleeding time ··- (.: ;;:), ~ \ \c'!~· \ _,, ..... ~~.;;;,.-,. Mx: DesmoprcssiqJT vWF level) ·•·.
Persistent 6feeds = fuctor VITI concentrates (contain VIII & vWF)

_H~e~op~::!J9!.9:t~~s,g~~!W > factor IX deficiency > mates:k\inked
).__ ~ cTiilicaU~ indistinwjs!Ja!lle fim haemophilia A \ ""~ Frequincy offfieeafng episodes- related to plasma level of factor IX
> Mx: Facto IX infusion ·: ii' =-
PIC (Disseminated intravascular soagulationl
Can be initiated by variety of mechanisms > > Endothelial damagc---~tissue factor expression-activation of clotting cascade (through extrinsic pathway)-
coosumptton o~ e!_ts, Factor V & vm. fibrioog_en-oOtential hacmorrbagic state (don't want to clot) SII: thrombocytopenia ....------------.
fi!rodiJ'!»iiliin time (due to factor V & fibrinogen deficiency) Causes of DIC; i -partull tfliO'mboplastin time (due to Factor V, Vill & fibrinogen deficiency) .Infections: .!. fibrinogen concentration · · ·E.coti i o:aiiiiers (cleaved fnn fibrin by plasmin, establishing evidence [email protected]!JiW -N.meoiogitidis
M-e: R.-c ~ndition. eg~s ·Strep.pocwnonia Bleeding- bid eroducts eg.FFP & pits . -Malaria Correct: acidosiS, dehydration. renal failure, hYpoxia Cancers:
Liver disease & bleedlpg = ! synthesis ofclottini factQ(S Renal disease & bleeding= severity of haemorrhagic state-proportioaal to plasma ~concenlration
The Leukaemias (this has been asked in the clinicjl( exam!) -·
-Lung, pancreas, prostate Obstetric:: -placental abruption -PET -Retailled <lead fetus -Amniotic fluid embolism
Malignant neoplastic proliferation - i number of WCs (malignant leucocytes) in bone marrow & peripheral bld :'\cute= proliferation of primitive stSm cell accumulation of~. predominantly in bone marrow--'-Causes !!lilrrRW faj!ure. ~c = malignant clone is able to differentiate--accumulation of mme mature cells. -
Four main groups (classified by clinical course, & cell of origin): a) Acute lymphoblastic leukaemia( AlL)--~~ b) Acute myeloid leukaemia (AML)------r.ougg adults c) ph!Onic myeloid leukaemia (CML)---middle-aged adults d) <;hronic lymphocytic leukaemia (CLL)---elderly
ex( Suspected when t WCCJ confr.rmed by examining the bone marrow.
Due to overgrowth of malignant cells in maaow- normal cell§ are crowded out -leads to~ thrombocytoQ!i:llia, loss of normal immune cells (Neutrophils & functional lymphocytes). Remember: the malignant circulatins wJiite cells_are abnormal, thus although the labs will show a i. wee, clinically the pt will sbow features of a ! wee.
Aetiology: Chromosomal alterations (In pt's with Downs) & external factors (ionising radiation, benzene, chemotherapy)
e..Bc-..A~CA WEC.... -~d:c\1'\ ~a -·lethargy, tiredness, malaise · }
Thrombocytgpeoia-petechla, bruising, bleeding Immunosuopression-t lnfe~tions ~ Features of MARROW FA!L1JRE (4 things)= clin pic. Cytolcines (fim abnormal cells)-low-grade fever ll.:J.. T cell turnover--Gout ---
a) Acute lvmohoblastlc leu!caernla fALLl- young children
J> Clin pic: Sg/sx of marrow failure Organ enlargement (lymph nodes, llver, spleen)-more in chronic fotm:1 Gingival enlargement less common(more in AML)
. Common infections = oral candida & herpes J> S/I: Anaemia = normal/j MCV .
PH-s- ~-P - t. . ~~5 ~~--")::-L.
c...~t-~~- .
Leucocytccount(vary: lx lll'!L-SOOX'IO~/L) ~1 Thrombocytopenia · .. . · 1 ·-\Hl~ .:::;t:Q_u..,--. GeiV . B~ in peripheral bid film-usually diagnostic - \?1 1\A Bone marrow-DIAGNOSTIC-. -hyperccllular
_,
__ I
J ~J
---~
I __ ,
J
J
)
_L
L
,_
l
;
l i.
i L
1
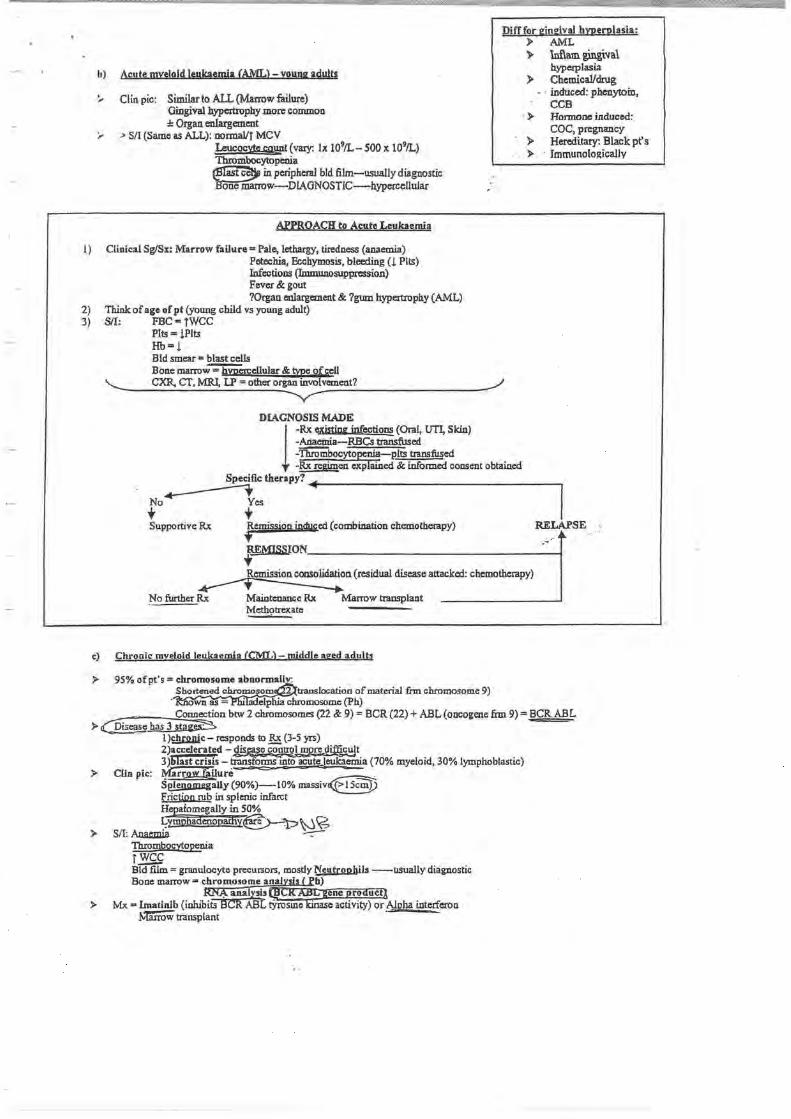
h) Acute myeloid leukaemia CAML>- young adults
:.. Clin pic: Similar to ALL (Manow failure) Gingival hypertrophy more common :1: Organ enlargement
:,. > SII (Same as ALL): nonnallt MCV Leucocvte COJWt (vary: lx 109/L- SOO x 109/L) Thrombocytopenia ~ in peripheral bid film-usually diagnostic ~w-DIAGNOSTIC-hypercellular
APPROACH to Acute Leukaemia
I) Clinical Sg/Sx: Marrow failure= Pale, lethargy, tiredness (anaemia) Petechia, Ecchymosis, bleeding (l Pits) Infections (Immunosuppression) Fevcr&gout ?Organ enlargement & ?gum hypertropb.y (AML)
2) Think of age of pt {young child VS young adult) 3) S/I: FBC= tWCC
Plts =!Pits Hb=! Bld smear= blast cells
Difffor gingival hypernlasia: )o AML > lnflam. gingiva\
hyperplasia } Chemical/drug
- · induced: phenytoin, CCB
· )o Honnone induced: COC, pregnancy
} Hereditary: Blackpt's )o · Immunolol!:ically
Bone marrow-=liiPercellular & tme ofgcll '-._ CXR, cr, MRl, LP =other organ involvement? __,I
--v-DIAGNOSIS MADE
1-Rx cxjsting infections (Oral, UTI, Skin) -A.aaemia-RBCs transfused -'fliiO'iiibocyto~-P.Its transfused -~en eitj)lliked & informed consent obtained
Specific therapy?+-------------------,
No~es I + t Supportive Rx Remission induced (combination chemotherapy) RELAPSE . .~ ~
~NQ~ION ____________________________ __,
~o. (residual disease attacked: chemotherapy)
No further Rx Maintenance Rx Marrow transplant Methotrexate
c) Chronic myeloid leukaemia CCML)- middle aged adults
.l> 95% ofpt's =chromosome abnormal! . Shortened chromosom t:r.mslocation of material frm chromosome 9)
own as = · adelphia chromosome (Ph) ~ Connection btw 2 chromosomes (22 & 9) = BCR (22) + ABL (oncogene lim 9) = BCR ABL
.l> Disease has 3 stag~ · · l)£!ww,ic- responds to !2, (3-5 yrs)
2)accelerated -~~t 3 )blast crisis - transforms mto acuteJcukacmia (70% myeloid, 30% lymphoblastic)
.l> Clin pic: ~ar~lure =- = . Se!snomcgally (90%)-10% massiv~ Frictipn rub in splenic infarct ~aiomcgally in SO% ~JUo&adcnopatfivE>-:p~ ~
;;.. SII: AD.wnia ~ Thrombocytopenia rwcc Bid fUm= granulocyte precuxsors, mostly Neutropbils --usually diagnostic Bone marrow 3 chromosome ana~~s (~h)
ltN~ anal!!ls @ci{ ~ene produffl. > Mx -Imatinib (inlubits BCR ABL t)-rosmc -~activity) or Algha interferon
M"arrow transplant ·

;
1)
2) 3) 4) 5)
d) Chronic Jvmobqcrtlc !eu!caemJa CCLIJ-----..eJderly C§S-70) median SUIVival- 6 yrs
)> Most common lc:ukacmia > B-lymphOCYtes tail to respond to antigens (transformation & antibody formation) :;;> ;; ItT mass ofimmuno-incompetent cells , 70% ofdx maae incidentally ---------;..:. Cliiipic: ~emia, infections,@"ess LYMPHADENOPAniY)nightsweats, weight loss, mild splenomegally ;. S/I: ~. ~mboeytgpeg.ia
t ~.lymphocytosis ~ticulqcvte & Coombs test ,(jf.lcmolytic ana::§ua co~~' Bone masmw . --
)> Stage A (~0%) =No anaemia. no thrombocytopenia, < 3 lymphoid enlargement, 1;1£. rx StageS (:lO%) = ~o anaemia, no thromboc~nia, > 3 lymphoid enlargement, chemothera_py Stage~ (lQ%) =Anaemia and/or thrombocytopenia, regardless ofnr of lymphoid ~ement, chemoth~
(fuultipl;-~loma / )>
)>
)>
)>
)>
)>
)>
)>
Neoplastic transfonnation of plasma 8-cells of bone marrow (plasma 8 cells produce antibodies) Rare, more common in blacks Chromosomal abnormality Plasma B cells prod igmmggglobulios--thus CltCCSS immunoglobulins in plasma & urine Usually incomplete immnoogJabdios Accumulate in tissue-amyloidosis 1n kidney e; Jones Proteins (form castsJ--renal tubular obstruction-renal-failure. Activated osteoclasiS (my malignant plasma cclls~steolytic b_9Jle
· --osteoporosis -pathological (mcturss -hypercalcaemia-renal failute
Marrow infiltration- crowding out of normal cells - anaemia, neutropenia, thrombocytopenia Increased bld viscosi~ l normal antibodies ---]'1iitCc m ecttions Clin pic: Hvueryiscosity =Retinal bleeds, bruising, CCF, cerebral ischaemia, h~is~l
Amyloid ="Panda" eYes:DCP.bmtiU:t:ndrome, c~m9l..tYJJ®lW1i~me BOnejfain &·fiitlCTrSJons ("salt & pepper" appearance on xray- punched out areas) R""enal failure = Amyloid, hypercalcaemia, Infection Spinal cord colll2ression= bony collapse, c:Jttradural mass Bids - Anaeaua, ~liibocvtoo~ PJY!Cytope!lia, rajsed ESR hypercalcaemia Iiiiiiiunogro&ilins= hYJ?oga.nunaglobulinaemia of normal immunoglob!Aw
Dx: Bid film & marrow- increase plasma cells (marrow) Anaemia, thrombocytopenia, leukopenia ~erum protein dectmphnresis paraprotein (IgG hYPetgammaglgbul jnaemia)
Overall hypogammag!obulinaemia Urine protein electrophoresis- B.eucc Jones proteins · Hypercalcaemia Renal Fx- cteat clearance, shows degree of impairment ESR-t ~keletal radiographic survey- MRI, PET,
- L.\l'"li'JL
c <;;_ e_ ~t---
Mx: Chemotherapy & symptomatic Rx (transfusion for anaemia & ! pits, rx infections) Mean sUrvival = 3 yrs
r. c\, ~\c~~\ P.:~;~~~- :~- £l~l~~~~j_c.~\~"} IF_~-:~.:_·~---~J DVT -risk of emboli!!
Virchow's triad =Blood viscosity (eg.T pits), vessell wall abnormalities, turbulent flow of bld (eg.pressure on vein: varicose \ '- ...._...) veins, pelvic tumour) Venous thrombi ~aiigis ~~e~r01
~-~~· '->"'......___."-::::.J
APPROACH; • ,.P_Mlteria:
· ·· -Active cancer (pt received R.'t in past 6 months/Currently receiving palliativ.: R't) -Paralysis, pateSis, or recent plaster immobilization of lower limbs -Recently bedridden for 3 days or morefmajor surgery in previous 12 weeks -Tenderness along distribution of deep venous system -Entire leg swoUen -Calf swe1ling @ least 3cm than other calf (1 0 em below tibial tuberosity) -Pitting confined to symptomatic leg -collate!al S\ll)erficial veins (nonvaricose) -Previously documented DVT -Altemati.ve dx @least as likely as DVT
SCORE< 2 = Dvr unlikely > 2 = Dvr likely
~1
~t
=1
=1 =1 =1 =1 =1 =-2
-· . , -------. ~) . . \ ·:::; ( u \.r::-c c : >~<"_.,~·
(:on firm dx: venous Doppler &/or venogram, CT/MRI ~~,o~~: ~BC, UCE, -~Fr· (;lot prof!Ie,D-~r~~~k_~~~p~4l!?_ . .\CL-antibodies1 AT ni ~evz.klYili~;!ltap.t !sve.~-R% :;;> •/ •/ -- ·/ . ·7 _.,.....
PrQjiiiila:ds .. - ~ ·~, · ;' ~ .· ..... ;, '·,·'
·' r ..
.J
_j
1 I
_\_
J
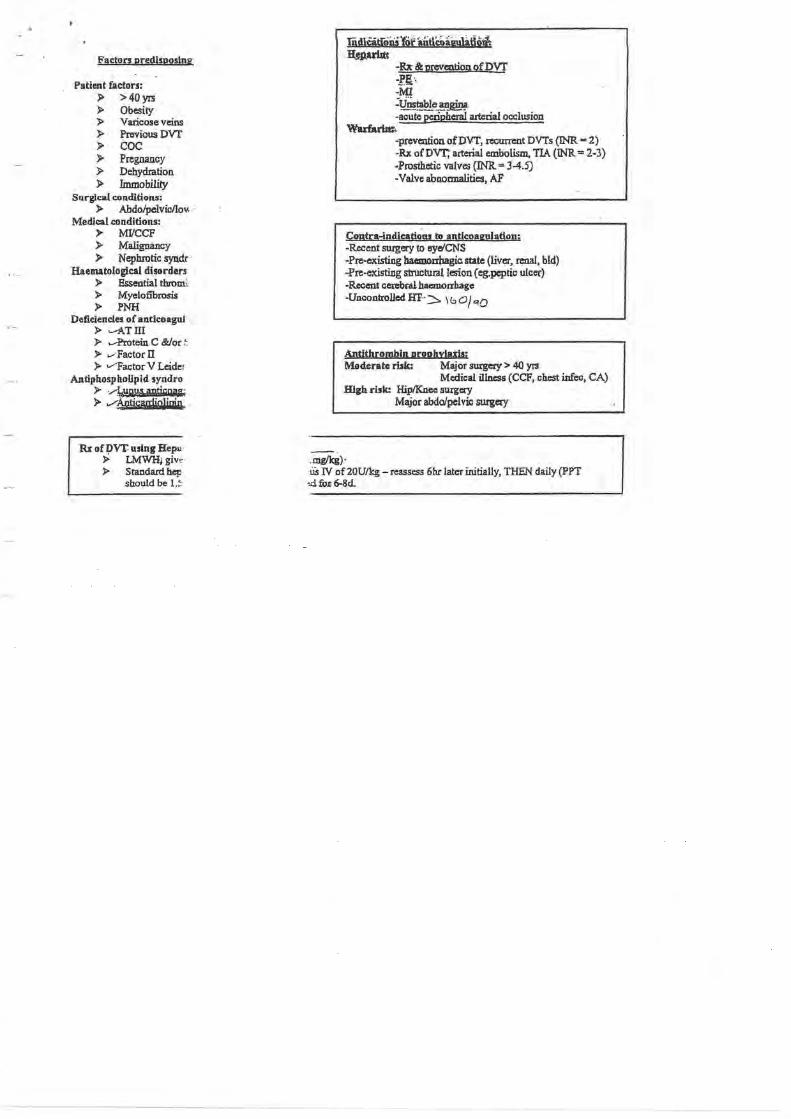
Factors predlsoos!ng
Patient factors: )> > 40yrs > Obesity > Varicose veins > Previous ovr > coc > Pregnancy > Dehydration )> Immobility
Surgical conditions: > Abdolpelvicllo\<
Medical conditions: > MI/CCF > Malignancy > Nephrotic syndr ·
Haematological disorders > Essential thromc > Myelofibrosis > PNH
Deficiencies of antlcoaguJ > ....-1\TIII > ....-Protein C &/or c > ..-Factor ll > vfactor V Leider
Antiphospholipld syndro > ·~W!§ aptjGQiJG1 > v~arrljQ)jqjg.
Rx Bf ~vr using Hepu > LMWH;giw· > Standard hep
should be 1.!
-Rx & prevention of Dvr -!'E:· -MI :q_~~~ -acute peripheral arterial occlusion
Wadari.lt:. -prevention ofDVf, recum:nt DVTs (D'ffi = 2) -Rx of DVT; arterial embolism, TIA (INR = 2-3) -Prosthetic valves (INR = 3-4.5) -Valve abnormalities, AF
Contra-indications to anticoagulation; -Recent surgery to cye/CNS -Pre-existing haemoubagic state (liver, renal, bld) -Pre-existing structural lesion ( eg.peptic ulcer) -Recent cerebra!hacmoahagc -Uncontrolled Hl'··:::::,. \ b 0 J <~O
Antithrombin proohy!atis: Moderate rbk: Major surgery> 40 yrs
Medical illness (CCF, chest infcc, CA) High rbk: Hip/Knee surgery
Major abdo/pelvic surgery
.mg/kg)· lis IV of20Uikg- reassess 6hr later initially, THEN daily (PPT
>:i fo.r 6-8d.

/.
3
3
3
Lymphoma
Definition: • Disorders caused by mrulsnant proliferation of lymphocytes
Accumulate in LN causing Lymphadenopaffiy ·
Classification: 1 •
• Hodgkin's - Cc.J-.-'\'\1'~ o Characteristic cells with mirror Image nuclei -+ Reed Sternberg cells
• Non-Hodgkln's _ ~ CovJt, 1\.\.J,ll..t- .
Hodgkin's Lymphoma
Classification: • Lymphocyte predominant .... low grade B-celi Non-Hodgkins lymphoma
Nodular sclerosing -+ young adults Mixed cellularity .... elderly
• Lymphocyte depleted
2 peaks of incidence -+ young adults and elderly
Olnlcal Features: • Painless rubbery lxmphadenopathy
o Typically cervical, auxiliary. inguinal o Can become 111attecl
• May fluctuate in size • Mediastinal node involvement may cause bronchial or SVC obstruction ~' ' : · ~xtenslon may cause pleural effusion . ' , ~ .
Spread Is contiguous and extra nodal disease Is rare ::;;= C~\ "'~ ;
Soeclal Investigations: Bloods
0 FBC +film . Normocytic normochromic anaemia if together with lymphopenia POOR
PROGNOSTIC FACTOR
ex~
• CT
0
0
0
0
ESR T. U&E must beN before Rx LDH T Is poor prognostic factor LFT
May show mediastinal mass
o Chest and abdomen for staging o (Single node> 10cmVs POOR PROGNQST!C FACTOR
• LN Biopsy o Surgical or percutaneous needle biopsy under radio guidance
l]iaCiiiia Af1n Arbor Svstem: J 't@>\r o? ~ c::::::::;= -.;:; conflned:tB"S'lnQJa EN region G2 •
• " "' 2" or> nodal areas 61! iimne side of dlaphram JU> l!:!_valvement of nOdes on bom sides of aiap'FiragiTTI _ IV. spread beyond LN ... Bone rna~ liver'
each stage subdivided in~ no syst;mic Sx and B-+ systemic Sx
(;pfb~\~ u.\) \XMi:M~ . ~ b.\cb~ 0
Locallsede~al~n- F~~~~ -
Management -r- j A Radiotherapy J- 'J:-
Stage .Ldisease Stage II A disease with 3 orless areas Involved After chemo to areas where originally bulk disease
. Lesions causing serious pressure effects
Chemotherapy ,-.,c=------::.......-""1 • All pts with B Sx \1-g, "$. -:n: /-n:t fnL • Stage II with > 3 areas Involved
Sta e disease · ombined modality Rx
Prognosis: Depends on stage and grade of disease
•
,. ~10% · ! wt in l~st q ~ofliM . Fevef > 38 (c.,O..\ c:W) Drenching nisht sweats, t-
Complication's of Rx RadloRx
o i risk for 2ndary malignancies
o IHD o Hypothyroidism o Lung fibrosis
ChemoRx o Myelosuppression o Nausea, alopecia, infection o Non-Hodgkin"s o infertility
.J
J
. 1
J
J
.1 I i
_L
I .L
1
l

® Nofl:Hodgk!n's Lymphoma r-\-_)o\ -(Qr-..,l._\1'~-""~ :J Definition; -
Monoclonal proliferation of lymphoid tissue May be B or T cell origin
Aetlo!ogv: Viruses
Late manifestation HIV Infection m.HSV-8,HTLV
Bacteria- -• Gastric lymphoma assoc with H. pylori
Genetics -Some have genetic association 1(14, 18) translocation
Immunology Congenital immune-deficiency states Immune suppression post organ transplant
Clinical Features: LN enlargement :1: systemic Sx HSM Extranodal disease more common with Involvement of bone marrow, gut, thyroid, lung, skin, testis, brain rare Bone Same staging system but NHL more likely to be S Ill or IV at presentation
• Compression syndromes-+ GIT obstruction, ascites, SVC obstruction, spinal cord compression
Special Investigations: As for Hodgkin's lymphoma PLUS Bone marrow aspiration lmmuno-phenotyping of surface antigens on lymphocytes lg detenninatlon -+ can be markers of Rx response Uric Acid -> some aggressive high grade NHL assco with iitit urate levels -. can precipitate RF HiV testing -\ N~ Risk FACTOR FOR LYMPHOMA l
Wtnagement Low Grade
• Asymptomatic pts may need no ex • I ndieations for Rx are
o Marked systemic sx o Lymohadenopathy causing discomfort or
disfigurement o Bone marrow failure o Compression syndromes
Radiotherapy o Locai·S I disease
Chemotherapy o Mainstay of Rx
Monoclonal Ab RX
Factors Determining Rx Strategy • Age • Degree of concomitant
disease • Histological grade
Staging • HIV status • Patient's vvlshes
o Used to target surface antigens and deliver cytotoxic drugs or radloRx. Stem Cell transplantation
o Improves disease free survivat but longer E/U is awaited before conclusions about cure
High Grade;, Need RX at Initial presentation
• Chemotherapy o CHOP therapy Is mainstay of Rx o Cyclophosphamide, hydroxyduanorubicln, Oncovin ®(vincristine), prednisolone
• Radiotherapy o Stage I without bulky disease o Compression syndromes o Residual localised site of bulk disease after chemoRx
• Monoclonal .Aa Rx o As above
Stem Cell Transplantation o Benefits pts at 1" relapse with cure rates of 50%
Proonosis:
o Lymphoblastic lymphoma is very aggressive type that affects young adults and should be considered as candidates
Depends on histological grade and stage at presentation ·

i i
t
r J
t
l
' I
/Nephrology
)> Acute Renal Failure )> Chronic Renal Failure )> Glomerulonephritis )> Proteinuria )> Haematuria )> Nephrotic Syndrome
I __ I
I
J
j
I .J
I · -'-.
I I _ _,___
! _I_
'! i

APPROACH TO A PATIENT WITH POSSIBLE NEPHROTIC SYNDROME
1. Introduce the patient 2. Background medical history: of importance are the following bearing In mind that the
causes of NS can be Idiopathic (in the form of different histological types of GN} or secondary to a systemic disease or drug. NB 80% due to the following types of glomeruloneptvitis: mlnlmal <:hange (In kids), FSGS & membranous (adults) as weU as membranoproUierallve.
3. Clinical problem A number of cYnical problems may be present given that nephrotic syndrome has the following consequences:
Thus the patient may present with the following combination of features: oedema (mainly dependent or affecting lower Umbs, possibly extending to ganllaUa & abdomen :1: periorbital :1: genital), without features of CHF oedema plus various possible thromboembolic phenomena {likely DVT), oedema plus features of CHD (due to atherosclerosis, such as Angina), oedema± Infection. · Furthennore: the patient may have a~ of OM, NSAlO use, HIV. ate (as above) HENCE: the most likely diagnosis for this paUent'e presentation is NEPHROTIC SYNDROME- due to the most likely cause es discussed In tabla 1 above HQwever, the roltowlng conditions must also be considered given the Oedema etc:
4. History Focus on all the causes above. Plus tnings li~e polyuria , po!ydips•a. naerr.aH.:\a, \\r.en oedema began, features of cardiac failure etc.
5. Examination General: J : think Hepatitis B&C; A: think t susceplihiiity to infx, leukaemia, malaria; Clubbing: think malignancy; 0 : assess fully; L: generalised- think HIV & Lymphoma; Face: (malar rash) eyes (xanthalesmata , arcus comeaHs), large tongue (?amyloidosis- look lor purpura around eyes). skin: (acanthosis nlgr1cans, Kaposi sarcoma, features suggestive of SLE, cellulitis), hands, feet & joints (features of RA, tendon, xanthomas, diabetic feet, digital gangrene); CVS: rule out CCF (examine JVP and sx of pulmonary oedema), consider IE; pericarditis may suggest SLEIRA, assess pulses and carotids for broils; legs (assess for DVT, claudlcallon (this wiU be suggested more on Hx)) Respiratory: extra-articular features of RA; sx of infection; Ca Lung, pleuritis {lniX,SLE, RA) Abdomen: oedema may be present (chetk sacrum as well); Assess for HSM (malaria, leukaemia, lymphoma), splenomegaly (RA, malaria, amyloidosis), hepatolmegaly (hepalltls); these pis are prone to SBP. Neurological: seizure, psychosis, myalgia (SLE) peripheral neuropathy {OM, amyloidosis), stroke Uke symptoms due to underlying atherosclerosis ± hypercoagulability
6. Speclallnvestlgatlons
7. Treatment
Urine: dipstlx (protein, glucose); MC&S (expect to see latty casts InNS; RBC and pigmented casts in glomerulonephritis) and 24hr protein excretion ~ • >3.5g /1 .73m1/day); Bence jones proteins (think.-. rule out myeloma as a cause for proteinuria/amyloidosis) Blood: FBC & dlff & ESR (lnfx, mangnancy), malaria smear, LFT, UKE, CRP, cultures, Immunoglobulins U InNS), elec:trophoresls (think myeloma) glucose± Hba1c, llpogram, disease specific serology (hepatitis, RA (RF), SLE (ANA, ANCA, anti dsONA etc)) Other: renal ultrasound; l!nal biopsy I should be done In all adults); CXR
Generat monitor UKE, BP, fluid balance and weight regularly Treat any underlying disease as per normal guidelines Restrict salt Intake and maintain a normal protein Intake Diuretic therapy: e.g. La six 6D-250mg/day po :1: spironolactone. Aim for 1 kg/day weight loss ... ACE-Is slow the progression of protelnuriaand renal fanure T reat lnfecllons Prophylactic heparin {If Immobile) e.g. enoxaperin 20mg sc daily Hypertension: aim for BP < 125n5 since proteinuria Is an Independent risk factor for CV disease. ACE-I Is first Hne HyperHpldaemia: stalin Serolds lor autoimmune causes.
8. lnfonnatlon for the patient
2

:r ..
lJ JlJ
t-- j-- )---
;"':': :-:.: : ., ., ' 0~ l· ~ ~ 't ~ f
ltJ ... lJJ 00 lltl w w liJ
Approach to a patient with Acute Renal Failure (Som~ authors refer to acute renal Injury)
1, Introduce the patient 2. Important background History
Conditions causing dehydration/fluid loss: dlarr11oea, ) vomiUng, polyuria (DM) Cond!Uons causing effective hypovolaemla: CHF, cirrhosis CondiUons requiring NSAID, ACE-II ARB - think chronic paln/arthritls/llypertenslon/CHF/ Conditions requiring calclneurln Inhibitors (c!ciosporin,tacroUmus) think IIansplantadon, myasthenia gravis etc. cirrhosis/liver failure- ?hepatorenal syndrome Uncontrolled BP or hypercllolesterolaemla (microvascular damage) } Other Hx suggestive of vascuUtis/CTD or disease assoc wkh HUSIITP (e.coU food poisoning, HIV etc) Glomerulonephritis (haematuria, backache, recent step lnfx admission to hospital for "kidney problem") Toxins: drugs, rhabdomyolysls, crush Injury, IIauma ..... suggestive of ATN ..----~ Hx suggesUve of urinary retention (e.g. prostate hypertophy/ca) 1-or trauma \Wth l oujpul or other malignancy J Neurological fallout (sc compression, paraplegia etc)
3. Clinical Problem .... un&kely to be a cBnlcal problem In itself but will be a feature of an underlying disease or pathological stale -. NB: the dx is baS!Id on acute (S 3rnonths) !in renal Fx manifested by l [Cr] and t [Urea), sometime assoc. with oigurla (< 500mUday). GFR Is< 30mVmln/1.73m2
(normal 120mVmlnl1.73m2).
..... NB: the most common cause of ARF is renal ischaemia due to Pre-renal hypovolaemlaldisorder auto-regulation which then progresses to ATN (I.e. becomes renal); -+the typical ratio of urea(mmoUL) :creatinine (IJmoVL) Is 1:20: when t[U] >» t(Cr], think pre-renal aetiolOgy (esp. dehydration & haemorrhage) .
!bus, the clinical problem mty be phrased as follows: this patient with (?underlying disease/suggestive tWrelevant clinical findings). with abnonnal urine volume (anuria, oliguria, polyuria)ls lkely to have ARF. This Is supported by (If already done} /or would be llllPPOrted by tha following additional findings -. abnonnal Uraa & Creatinine ± haematurla ±casts on urfna MC&S
4. Hlsto.y: mention important positives and negative guided by tile info above 5. Examination
.... in acute RF, the clinical picture of the underlying disorder v.illlikely dominate, So look for features ot
Dehydrallon. oedema (pulmonary/peripheral). Diabetes MeDitus. chronic liver disease (thlnk hepatorenal syndrome). heart failure, hypertenstlon, ,sepsis, haemorrhage {pallor/anaemia), vasculitis or other CT dlsese, HIV,
'-~- J- J--·
W'
)_
'\ !fn·,· :· "~ !l R" - · ~·,,1 w uu . m 1.'"·:·· · '~ ~ r· w·· ,, m !l '! ,. ~'· .-~1~''':~w"·':iu
£.._
w w w w . ·_ '.; .. ·:··' _·· ..
glomerulonephritis (esp. renal angle tenderness). trauma/crush Injury, urinary tract obstruction: Hx or sx of STI as a cause for obstruction, neurological examlnalion NB! (can result In funclional obstruction of urinary tract)
6. Speclallnvestlgatlons Blood: FBC, Urea & Cr (thlnk prerenallf Uf »Crt). electrolytes (TK due to l excretion or t tissue breakdown: ! Na If failure to excrete excess water Intake; acidosis); Ca, P04 Urine: Dipstlx. volum·e, Microscopy .... nb cests. crystals. sediment C&S Foley catheterlsatlon: exclude bladder outlet obstruction Fluid challenge (I.e. bolus to rule out prerenal causes) Imaging: abdo U/S (kidney size, hydronephrosis, post renal obstruction) Indications for biopsy: o Diagnosis unclear o Pre-renal azotaemla or ATN Is unUkely o OUguria > 4 weeks
7. Treatment 1. Preliminary measures
Pre-ranat oplimlze volume status and cardiac perfonnance Renal: exclude rev~KSible causes; discontinue offending drugs, Rx lnfactlon, opllmlze electrolytes and hold ACEIIARBs Post renat consider obstruction: physical (stones, strictures. tumour) vs. functional (neuropathy)-+ foley catheter, suprapubic calher, nephrostomy, stenllng.
2. Compllctlon Mx: Auld overload: NaCI restriction, high dose loop dlurellcs Hyperl@laemla: know !hlsUI
3. Definitive Mx -. according to the underlying cases (NB, renal transplant Is not a treatment for ARF (unlike oU1er organs e.g. Uver)
"indications for dialysis: Refractory llyperkalaemle Refractory acidosis Refractory volume overload Elevate Urea (.35 mmoVL) Pericarditis Encephalopathy Pulmonary oedema
B. lnfonnatlon for the patient
2

i_
I
t -··
j
DeflniHon:
Nephrology Chronic Renal Failure
Irreversible deterioration In renal function developing over a period of years • ESRF - death will occur without renal replacement therapy
•
Aetiology: • Congenital and Inherited
o PKD, Alpert's Syndrome • Renal artery Stenosis • Hypertension • Glomerular Diseases
o lgA Nephropathy Interstitial Diseases
• Systemic Inflammatory Diseases o SLE, vasculitis
• Diabetes Mellitus · • Unknown
Classification: STAGE GFR ml/mln per1.73m~
I > 90 with othrer evidence of renal damage II 60 - 89 with other evidence of renal damaqe Ill 30-59 with( out) evidence of renal damage IV 15- 29 with( out) evidence of renal damaqe v < 15 established renal failure
• Other Sx: protelnuna. haematurla
Clinical Features:
Clinical Abnormalities In Uremia Fluid and .Electrolyte Disturbances Neuromuscular Disturbances Dermatological Disturbances Volume expansion Fatigue
•.
Pallor "
Hyponatremia Sleep disorders Hyperplgm.entation Hyperkalemia Headache Prur{tis Hyperphosphatemla Impaired mentation Ecchymoses
' Lethargy Nephrogenic fibroslng dermopathy Eridocrlne - M~tabollc Disturbance Asterixis Uremic frost 2ndary .byperparathyrdoidlsm Muscular Irritability (Rx quinine) Ady.namic bone Peripheral neuropathy GIT Dlstrubances Vit D defident osteomalacia Restless leg syndrome (Rx ·Anorexia CHO resistance clonazepam) Nausea and vomiting Hyperuricemia Myodonus GE Hypertriglycerldemia Seizures PUD t Lipoprotiens Coma GE bleeding ~ HDL Muscle cramps Idiopathic asdtes PE malnutrition Myopathy Peritonitis Impaired growth and development lnfertllty and Sexual Oysfunctlon CVS and Pulmonary Disturbances Haematologlc and Immunologic Amenorrhoea Arterial HT Disturbances Amyloidosis CCF or Pulmon oedema Anaemia
Pericarditis Lymphocytopenia HCM or Dilated Cardiopyopathy Bleeding diathesis Uremic Lung r infections Accelerated alherosderosis Leukopenia Hypotension and Arrhythmias thrombocytopenia Vascular calcification
Other Sx: • Pallor. yellow skin pigmentation • Hlccoughs • Brown nails • Purpura, bruising, excoriation • ·; j BP, cardiomegaly, perlcardial rub • Pleural effusion, pulmonary or peripheral
oedema • Proximal myopathy • Later. arrhythmias. encephalopathy,
seizures. coma --. death
Anaemia • Normocytic. normochromic
• ~ erythropotetin, ~ production due to tox1c effects of uremia on bone marrow l red cell survival, r blood loss due to r capillary fragility and poor platelet fx t dietary Intake and absorption of Fe and other hemanitics
Renal Osteodystrophy Impaired renal function -+ t Vit D .... .1. Ca2
•
absorption -+ L plasma Ca • --. stimulation of parathyroid glands - j PTH -+ t osteoclastic activity and ~ mineralization of bone Impaired renal function - ~ P04 excretion - hyperphosphatemia

I
j
• Presents as Osteomalacia, osteitis fibrosa, osteoporosis and osteosclerosis
Myopathy · Combination of poor nutrition, hyperparathyroidism, Vit D deficiency and electrolyte disturbance
Neuropathy
cvs
.1. libido, amenorrhoea, galacorhoea Rx Bromocrlptine
• f insulin T Y1 and post receptor ~ insulin action -+ changes CHO metabolism
HT due to Na retention and activation of RAAS
Demyelination of medullated fibres Acidosis • Long fibres involved earlier • Foot drop, delayed gastric emptying,
diarrhoea and hypotension • May improve with dialysis
Endocrine Function
Metabolic acidosis • Protons buffered in bone instead of Ca -+
worse bone disease CaCO, is good agent-+ doent T Na and binds excess PO.
• Hyperprolactlnemla and hyperparathyroidism
Bleeding
Special Investigations: • Bloods
FBC, U&E (T urea, j creat), ESR, CMP: l Ca, t P04, j Alk Phos,
• Uremia impairs platelet Fx and f bleeding time
Reversible actors in CRF
HT
0
0
Urine 0 MCS, dlpstlx, 24 Hr creatinine clearance( estimation
OfGFR) .
• l Renal artery perfusion Urinary tract obstruction Infection -+ j catabolism and urea production • Renal U/S
Nephrotoxic medication o Exclude obstruction, size of kidneys • CXR
o Cardiomegaly, perfcardiaVpulmonary effusion, pulmorle'll!!'l'l!!l'l'!'!!"-._ ____________ ..
• Renal Biopsy BoneXR
o Osteodystrophy
Management: General:
Refer early to nephrologist In stage I and II > risk of CVS death than ESRF
Specific Hypertension --+ ACE-1/ARB even If BP normal can save function
•
Dialysis
o Aim c:: 130/80 If protlenurlc, < 12Sn51f > 1g/day Dysli!Jidemia -+ Statins Oedema -. Furosemide arid fluid restrictions Anaemia
o Exclude other causes, consider erythropoietin Osteodystrophy
o Treat If j PTH o Restrict dietary phosphate (milk, eggs) o Give calcichew to bind in gut and L absorption o Supplement vlt D and Ca
Diet o Na restrictions , K restrictions only if hyperK", o Moderate protein Intake o HCOJ for metabolic acidosis
Restless leg syndrome o Clonazepam 0.5 - 2mg dly
Hemodialysis at 600- 8000molll Peritoneal dialysis
Renal Transplant
Indications for Dlalvsls • H yperkalemla (refractory) • Acidosis (refractory) • Volume overload • Elevated BUN(> 35 mM) • P ericardltls
E ncephalopathy • E dema (pulmonary)
•,
__ ,
___ j
J
. -1
J
_j
j_
J
l
J

Glomerulonephritis
Oefiriltlon: Group of disorders where there Is damage to the Glomerular filtration apparatus Leakage of protein :1: blood Into urine Pts present with HT, haematurla, nephritic syndrome etc.
General Management Refer to nephrologist BP < 130/80 or< 125/75 if> 1 g protienurla/day Same as for CRF ..... oedema, lipids
FEATURES Thin Basement Autosoma~ dominant membrane Nephropathy Persistent microscopic
haematuria Rarely minor protlenuria
Minimal Change Commonest cause Glomerulonephritis nephritic syndrome In kids
Believed to be T-lymphocyte mediated Associated Hodgkin's Lymphoma, drugs Does not progress to renal lmpainnent Only small proteins leaked -+albumin
Membranous Unknown aetiology, 20-Nephropathy 30% Nephrotic syndrome
In adults Risk of renal vein throm_bosis Associated with Malignancy Drugs ..... gold, penicillamine, captoptil AI-+ SLE, RA, thyroid lnf -+ Syphillis, leprosy HBV
Focal Segmental Primary .... idiopathic Glomerulosclerosis Secondary ..... lgA
nephropathy, vasculitis, Alpert's syndrome, Heroin use, Sickle Cell disease, HIV· 50% have impaired renal Fx
lgA Nephropathy Commonest GN in the world Usually young (! with episodic macroscopic haematuria few days after pharyngitis/UTI lgA Immune complexes overproduced and deposit In messaf"lglal cells
Henoch Scholein Systemic variant of lgA Purpura Nephropathy
Small vessel vasculitis Proliferative GN Classified histologically
Most common post· streptococcal-.1 -2 weeks post infection Reaction to streptococcal antigen deposited In glomerulus
Rapily Progressive Most aggressive, can cause Glomerulonephritis ESRFindays
Causes Wegne(s Granulomatosis, Goodpasture's Syndrome, infections, SLE Present with features of renal failure :t features of systemic disease
DIAGNOSIS Renal biopsy
Selective proteinuria Renal biopsy
Renal Biopsy
Renal biopsy
Renal Biopsy
lmmun- fluorescence for lgA and C3 In skin or renal biopsy Renal biopsy Immuno-fluorescence lgG and C3 deposits Serology Antistreptolysin titre
MANAGEMENT Monitor 1 - 2 yrly Usually has benign course Small risk CRF
Remits on t dose steroids 1 mglkg prednisolone x 6 weeks May be prone to frequent relapse ..... maintenance steroids I cytotoxic Rx
Poor prognostic factors: ! renal function, ttt protnlenuria
Rx steroids, cyclophosphamide
40% spont remission
Steroids Cyclophosphamide If steroid resistant 30- 50% -+ ESRF Chance of recurrence after transplant
General measures Immune suppression If renal impairment Worse If t BP, male, proteinuria, renal failure at presentation ± 20 % ESRF over 20 yrs
As for lgA nephropathy
Supportive >95% recover renal function
Aggressive Immune suppression - ti dose steroids+ cydophosphamide, with plasma exchange to get rid of immune complexes Poor prognosis If Initial creatinine >6000moVI

Haematuria ·
Bleeding from anyv.t!ere In the renal tract
HEMAJU"R1A I I
P~endahematuria HenuJm.i1 but NORBC'son mi<:tO'lr:opy
True Hematuria • coloor:d urine but neptive dip~tic:k • diifemtiial diagnosis
• fOod (e.g. beets) ·d~ -=->'-~ ( _,.. ___ . \
• ~on e.g. u"""PUlJ
I . Nephrolag.ieal (c:asts lllldlor proteiD)
. rd . b. As..octate n·tt UrinAry Trnct Infection
Fi~·e 6. An Approach to Hemnl\uia
~· Renal:
• Neoplasia • Glomerulonephritis • Tubulointerstitlal nephitis • Polycystic kidney disease • Papillary necrosis • Infection • Trauma
Extrarenal: • Calculi
• myo8l~b111llria • hcmo ob.inurill
(due hem,olyo;j.s) Nl:l: myoglobmuna aud hcn93i<?U}uuria will rcsist.:r on dipsti..:k a~ blocd -
UrolaHical.l (no casts or pt9tcia) • think 8111110tllic:ally:
• ureter • bl....tdet •urcthn • misc:clfao<:ou1 (o.,g. TB)
Aisoci~'l'>ilh Prtminuria • think anatomically:
• glomerul.lr • fubuloint=ti.Ul
• Infection - cystitis, prostatitis, urethritis • Neoplasia - bladder, prostate, urethra • Trauma
Infective endocarditis Myoglobinuria Food dyes- beetroot Drugs .- senna, rifampicin
• Porphyria
Soeclallnvestigations: Urine
0
0
Blood · 0
AXR • Renal U/S
MCS, cytology Estimation protienurla
FBC. U&E. CRP. ESR, clotting profile
• Renal Biopsy
Hematolo~c:nl • coa11Ulopathy • Uclae hemoglobinop:~thies
I Associated \\ith Casts • sec Tabl,. 2 for 1}-pe> of
casts and their QUSCS
Interpretation of Casts • Hyaline
o Not Indicative of disease o Concentrated urine o Fever, excerclse
• RBC . o Glomerular bleeding _, GN o = active sediment
• Leucocyte o Pyelonephritis o Interstitial nephritis
• Heme-granular o ATN o Proliferative GN
• Fatty/oval fat bodies o Nephritic syndrome

~1~\:.L· ~~s~. '. ~?{S:'
m.;,"· '! ·(.'::·~. :
~-:.: .
I J
·/ .·
Proteinuria
Definition: • <150mg/d Is considered acceptable, containing< 30mg albumin. More Is considered pathological
Pro~ (determine ag dipstick aruror 24 hour urine OJllcciion)
I I Tubuloiutastitial Glom~ • usually< 2J24 hour • mixed LMW pro~
• nstJa1ly > 2i'JA hour • primarily albumin
I 7"--
Prolifemtin Nonprolifiemtjye
Figure S. An Approach to Proteinuria
Causes of Proteinuria: Physiological:
• Orthostatic • VIgorous exercise • fever
R'lnal • fBP • Diabetes mellitus • Myeloma, amyloidosis (urlriary Bence jones protien)
Extra· Renal • Pregnancy • · Vaginal mucous • Recent ejaculation
Soeclal Investigations: • BP • Urine MCS • 24 hr urine collection - creatinine clearance and total protein
Urine albumin/creatinine ratio
I
o Simpler way than 24 hr collection, reasonably accurate estimation • Renal U/S • Auto-antibodies • Renal biopsy
o If function is deteriorating
Microafbumlnurta: • Undetetecable on dfpstfx but 30- 300mg/24hrs on lab tests • Causes - DM, Minimal change GN, t BP
Management • Special investigations to Identify cause • Treat cause • Optimise co-morbidities e.g. BP
t
.1.
-..
I !._

Symptoms: l Hyperosmolar Hyperglycaemlc sj:aie)
1. Severe hy er caemia (> 33 mmoU!,.) 2. Osmolan • > 0 3. No acidosis or U • ketones 0/1+
~: ~'\!:~::and Uraemia
6. Patient Is usually an erderl~
Mx: 1. l:ialf N Saline (0.45%) used as replacement fluid if plasma Na > 145
mmollL with 1/2 Insulin dose than used in DKA (50) as patients are more sensitive to Insulin. Start Infusion @ 3mllhour.
2. NB: Nonnal plasma osmol = 280-300 mmoVL Na lev ells an indicator for osmoll Decreased consciousness = plasma osmor > 340 mmoVL 0.45% Saline used until osmolality approaches nonnal THEN use 0.9% Saline.
3. CVP to regulate replacement rate. 4. Check plasma Na regularly 5. Prophylactic Heparin - 5000U SC
~ Catecholamine metabolism:
1. 01romaffin cells in the adrenal medulla -+ epinephrine 2. tyrosine in peripheral postganglioniC sympathetic naves .... norepinephrine
Patient presents with: 1. Triad: PalpltaJ!ons, Pounding headache, diaphoresis! 2 •. Tremor, anxiety, chest or abdominarpain, nausea, vomiting 3. HALLMARK: sustained or paroxysmal hyf?!'!rtension! 4. Symptoms often predpitated b¥ stress, exertion, food!
Pathophys: • Rare tumor of the adrenal medulla! • Tumour arises from the sympathetlc chromaffin cells In the adrenal
medulla. • . • ms most commonly a single tumour of the adrenal medulla. • 10% rule: 10% fa!!!l!Jal, 10% bilateral, 10% malignant ib%
extra-adrenal. • Most common extra-adrenal site: AORTIC BIFURCATION (Organs
of Zuc:kerandl) - . • Cases sporadic or part of MEN 2a or 2b. [Multlple endocrine
neoplasm) = Part of the Heridltary cancer syndrome [MEN, Neurofibromatosis, von Hlppei-Uodau syndrome)
• Rare treamble cause of hypertension ( <0.1 %) Investigations:
1. 3 x 24 hours urine samples Increased catecholamine level 2. "Elevated plasma epinephrine that Is not suppress y onldlne (central
alpha blocker) 3. positive CflMRI findings .4. Meta- iodobenzoguanldlne (MIBG) uptake by tumour site during scan (
MIBG is a chromaffin seeking isotope scan espedally U!ieful to locate extra-adrenal tumours)
Treatment: 1. _eRE-SURGERY .t.JB!!{&equate alpha blocka@ Phenoxybenzamine po. 2. PERI-OP: Phentolamine fV
{BloCh alpha receptors before blocking beta receptors to avoid unopposed beta block!)
3. B- Blocker; PCQpanolol 4. Volume restore with vigorous salt-loading s. S.,1:!!9Ical cemo•'il gf the n 1mour 6. re-screen urine 2 weeks post-op and again after one month 7. Monitor BP (RISK of HYPOTENSION)

c_ .. Neurology M '* 8¥ ..
:> Bedside Neuropsychiatric Assessment :> Cortical Lobar Functions
-r Findings helpful for localization ~thin the nervous system )> Aphasia )> Dysarthria :> Gait disorders :> Nystagmus r Pupillary signs r Tremor r Vertigo r Moveinent disorders r Coma r Dementia }> Delirium :> Parkinson's Disease )> Epile_1:6y. )> Status Epiltpticus )> Stroke ~ Headache )> CNS infections >:· Neuro-opthalmology r Cerebellar disease :> Multiple Sclerosis )> Myasthenia Gravis )> Spine & spinal cord > Peripheral neuropathy )> Acute inflammatory polyneuropathy > Diseases of mliscle }> Neu.roecfudermal syndromes
II
I I
l 1

Tr~scortical Aphasias (Sensory, Motor, Mixed) • lesions outside perisylvian language zone • ~ep~t~~i9_n __ ~el~tively preserv~·
Anomie Aphasia • inability to generate word names in confrontational tasks and in spontaneous speech • if word-finding difficulty occurs in relative isolation, lesion can often be localized to posterior
middle temporal/inferior parietal region or subcortical white matter
• may occur with metabolic disorders or space-occupying lesions
Important Ae__~ia Points • clinical profile reflects~ebrovasclilij rather than functional anatomy
classical aphasias; typically produced by lesions in the MCA territory transcortical aphasi~; result from l~s_ions fn lhehorder -zorie between :~£A, MCA, and PCA territorie.~ __ (~ershed areas), often associate(fWithCeJ!l9.r~L{IJJ9..~~ (i.e. P9st.:MI, po_stcardiac_ ~~~~ry, carbq_n m_9_!!.<?.J{!~~ E~i!?.~~~~· ~Y.E.~ens~on)
Table 8. Com panson of Classic .t\pl1asms
Fentllrt'
Lesion Location Pluency
Repetition
Naming
Comprehension ( ~--eroal + written~
\Vl'itiog
~ssodated t·t.~rrures
!rt~i!!ht
Broca's nre1
Non tlut:rrt Eftbrcft.tl , -Tclegmpl1icf:pccch" Agranunattc.."'l
.Etlbrtilll, poor
Poor
l~rt.-served
"Poor
An'tlre of detlcit
\Vhat to tell the patient/family:
Wernicke's area
l~luent Parapha->ic errors Circum)ocutions ~eolO\!:I.'ltns l'l'essui!! of spt:ech
Poor \.
Relative s~b-ing Poor
Content abnormal
Unatvarc of de licit
_eaobal
Nontlu~nt ;\gran1matic Neologi~s lvltninlal vclume
Poor
Pour
Poor
Poor
l-Jemiokeia (right) r~ emlilrtt5Uiesm Visual tield defect (right hon:npnymous flernlanopu:)
Awnre
Conduction
Arcuate fasciculus
Fluent Paraphasic emxs
Poor to worse vs . spont<llli.'OUS Spl->t:Ch
POOl'
Preserved
Penmanship prcs~r...-cd
Mild hemipl!:!g1a
A\vare
• language deficit following acute stroke can change rapidly, especially if the initial impairment is mild
• with recovery, patient may evolve from one type of aphasia to another type • most recovery occurs in first three months after onset but continues for more than one year • conduction, transcortical, and anomie aphasias often recover completely; • global aphasias have a poor prognosis
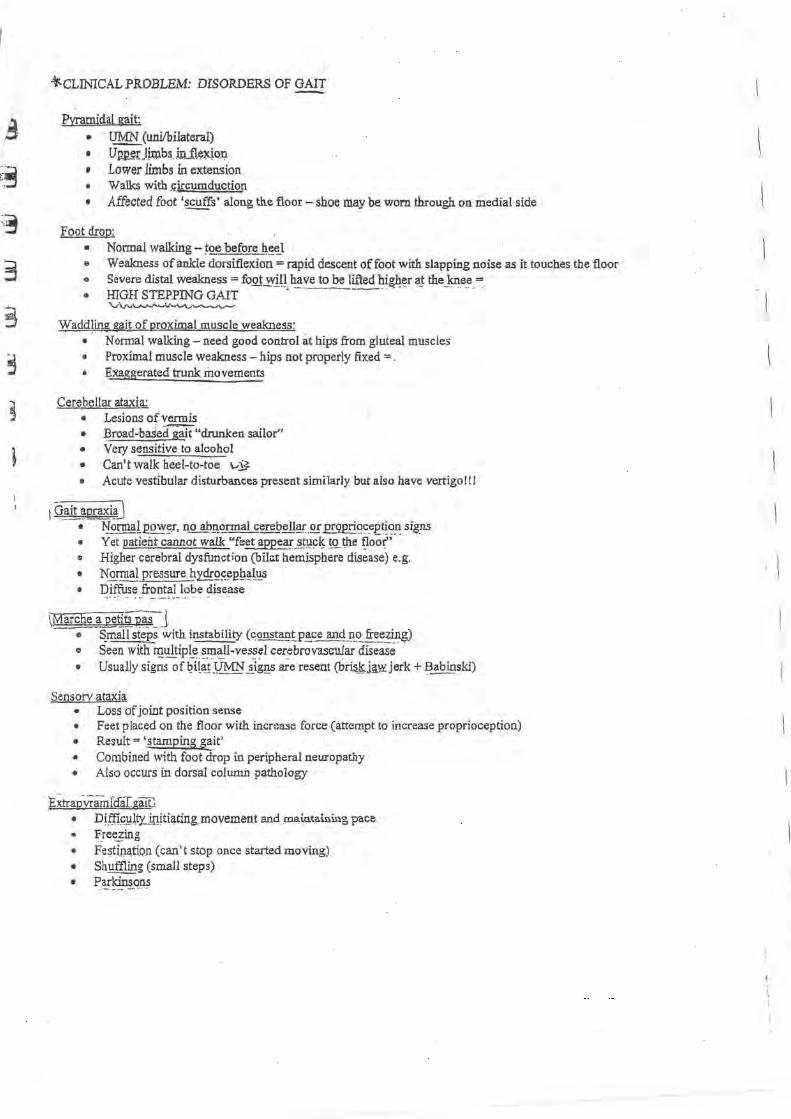
, ~CLINICAL PROBLEM: DISORDERS OF GAIT
Pyramidal gait: • ~(uni/bilateral)
• Up.~rJ®b~. mJl~~on • Lower limbs in extension • Walks with J;ircumduction • Affected foot ·~s· along th.e floor- shoe may be worn through on medial side
Foot drop: • .. .. •
Normal walking- ~Q_e befQ!e ~~~1 Weakness of ankle dorsiflexion= rapid descent of foot with slapping noise as it touches the floor Severe distal weakness= fogt~_gl have to be lifted high~r a_! the ]<nee= HIGH STEPPING GAIT ·. - -··------- -- ... ·-- . v\r..'-"-~-'-"-''-"-'--,.._.-
Wadd]ing sait of proximal muscle weakness: • N onnal walking - need good control at hips from gluteal muscles • Proximal muscle weakness- hips not properly fixed = . • Exaggerated trunk movements
Cerebellar ataxia: • Lesions of vermis • .f3road-ba$e(fg;ili"drunken sailor'' • Very sensitive to alcohol • Can't walk heel-to-toe \.-~ • Acute vestibular disturbances present similarly but also have vertigo!!!
I (}ait ~praxi~] • ~~_rmat pow~_r, no @gqnnal cerebell!!!._Q!" E!..9.E!i~~-eet~o~ si8_ns • Yet patient cannot walk "feet appe1if._S_!!l9~ !Q.. ~e tJoof o Higher cerebral dysfunction (bil<lt hemisphere disease) e.g. • 1'{<2_rp1al pressure h;-idrO~~l?Q~l'!s • Diffuse frontal lobe disease
\Marche _!\_petits P.~S:J - e ~mall st~s with instability (qg_~~tP!~c!.!!~ fr~~-~i_n~)
o Seen with ~ultiple small-vessel cerebrovascular disease • Usually signs of ~?it~i~ ii@s. are resent (bri~~i~jerk +Babinski)
Sensory ataxia • Loss of joint position sense • Feet placed on the floor with increase force (attempt to increase proprioception) • Result= 'stamping gait' • Combined with foot drop in peripheral neuropathy • Also occurs in dorsal column pathology ·
Extra0wamraaGruu • Diffi.@l!Y...initi(!.ting_movement and roa.io.ta.ining pace • f.ree_~ing
• Fe~tipa,tioJl (can't stop once started moving) • · Shuffling (small steps)
• P~r~!Q.n:S
J

CLINICAL PROBLEM: DYSARTHRIA ~· ..... ·l.'-~'l,..·~l.,..'1,. "'._ ~ ... , ...
[ say this because the patient has a dis~_E~ce of n<~~l!~ articulation or phonation, without affecting the content· of speech (language)
!'vtECHANISM OF SPEECH: ' ., •,_ ...
Cortical initiation (Broca's are~) . ; ,' ': ,·' .:\ · · · Descending tract (corticobulbar) from left hemisphere to nucleus ofCN X and xir · •
• Corpus Callosum connects motor cortex ofleft hemisphere with right hemisphere • Cortico-bulbar tract from right hemisphere to nucleus of cranial nerve X and XI£ $ CN X and XII supplies spft_plilate, p~ary:nx. larynx and ton~e
a The extrapyramidal and erebellar systems modulate the action of muscle of articulation
5TYPES
PARKINSON DYSARTHRIA
• Inability to show rapid alternating movements of muscles of speech • Addition signs present (resting_tre~or,_ ~£8:dykinesia, ~igidity etc.) • M.on().t()J;l~ speech • Hyp()ph'?.I!i~. (soft speech)
CEREELLAR DYSARTHRIA • Inability to perform rapid alternating movements of the lips, tongue and soft palate
• Associated signs of cerebellar dysfunction in the limbs and trunk • Characteristics: Atactic intonation, slurry speech, abnormal prosody, scanning speech
·~:~)·-J BULBAR DYSARTHRIA
• LMN lesion of CN X and XII • E.g. N!9., C!u~g~in Barre " Decreased volume of speech • ~asal speech, impaired lip movement
PSElJ;OBULBAR DYSARTHRIA
.. Bilat Ul\IIN paralysis of motor CN from pons to medulla (CN V, VII, X, XII) • Clinical picture resembles bulbar dysarthria • S_pe.ech is slpw and lll_?not~~e
• L~tc;h and sl~ speech
\ -··
• Muscles of speech are spastic and fast repetitive movements of the tongue and lips are jerky • Often diffuse '£!MN si~ns e.g. Babinski, jaw jerk, positive put reflex
MQTORNEURON DISEASE DYSARTHRIA
• Co:l!~iX:_~tion of UMN and LlYIN paralysis • Degeneration of the motor nuclei in the pons and medualla with a pseudobulbar clinical picture
• Tongue atrophy with fasciculations • Muscles of the face and jaw are weak • Paralysis of the soft palate

t
CLINICAL PROBLEM: APHASIA
I say this because: the patient has a ~isorde~2fl~~ge (produced by a ~r~bralJ~§.ion) characterized by err~~--~ spe«:ch production, _impaired comp_~ehension, reading, wri~~g and wor~=-"~di!~g difficulty
• aphasia is an important localizing symptom usually indicative of dominant hemispheric dysfunction
(~su,al_~ !h~lef! ~~9'!~sp~e!e) • Preassessment Information Needed:
1. handedness (writing, drawing, using toothbrush, scissors) 2. educationallevel 3. native language 4. preexisting learning difficulties
• J:.~illi\&i.Repr~s.entati0i1 in ~eft hem~_p_~ere for almost all rig_})._t~ll.at_l~ed people andm2_st _lei} }1agd~4_g~opl.~ (15%) - -~cs-n's lh.;,.\e. ..
• Neuroanatomy of Aphasia 1. R_~~tL<?!,_i~~r!orfrEI?:~l ~?-~~ ~roca's area) used for 111otor speech production 2. Wernicke's area (P.B~~~P..?~!-~~~.._i~erio~ par!e.t~l) used for
comprehension 9f spoken language and for initiation of reply or action
3. visual sttmuHreach Wernicke's area through ID.Igular gyrus which is thought to be important for co_mp_rehen~j9n pf written language -
4. these two areas connected through association bundle @_<;iiat~.fasciru.tfus) and altogether comprise the \P!-z:!.~s-y.,lv.-i_?Il-_--._1.-~i!,!ag~_ ~~~e}
• aphasias may also result from damage to areas ofthe brain outside the perisylvian language zone (transcortical aphas i~s)
lb_2sessment-o£Aph~iJ · \L) • fluency
nonfluent patients usually have damage in Broca's area fluent patients have damage in Wernicke's area
(L; • repetition used to Qi~illg_u-~h_si?.S~i~l!Lap_h~~L~ (arising from lesions in the perisylvian language zone) from the transcortical aphasias repetition d-isturbance- ciassicill aphasias: Broca's, Wernicke's, conduction aphasias, . ·- --···· ··- ·*---- . -- --....___ ... 1...-"--"'-- - · -·- ........ '-- ·" \.. -· '--·-· .. .. - - -· ·
global
• r~petition in_!act- t[~s~o .. ~!c~l- ~P.h~_ias, ~~-~!P~:~as ( -.~> • P.ara2_has1c errors f p..f;,o..c;}
incorrect substitution of words or parts of words • characteristics of aphasia (vs. dysarthria) • e.g. "sook" instead of"book", "table" instead of"chair"
(i._._. . c~.Prehension- verbal and written (~.l • naming ( t : • writing
TYPES OF APHASIA
I --'
.J
[
I . I

. Jce~ebni!m · ·---···
Brainstem) ,--- . - -
· ( ~pin~ _~<?_r.d> ; .. _.
Signs
~Q.norii.laJ.lllei1t~l §t~tu~ or cognitive impairment
Seizures
Unilateral w~algl~~sa and sensory abnon;naJJ.ties including head and limbs
Vis!llll_ ft~l4. ~q~ormalities
¥.g_vement agn,_o_~alities (e.g., diffuse incogrdin~#Qn, tremor, chorea)
Isolated <?ranial nerve agQ,grmalities (single or multiple)
"~rossed" ~-~aknessa and sensory abnormalities ofhead and limbs, e.g., wealmess of~g_ht _ face and left ~-~dJeg
Back pain or ~nde~~~~-
-I ~s - --- \--:;, M~~d_gpQer an<1: lq~er motor neuron findings
I ~~~ory lev~! ~-~~----~----~-S~p~h~in~· ~;te~r~- ~~- y~s __ fun __ c_t_io_n ______________________________________ ~ i sp~al root~) ~~dia~g_ ~~~ 2-a!.n .j' ···- --- . w_eakness6 or seJ;l~IY_~bn~~allties following root distribution (see Figs.
25-2 and 25-~)
Peripheral_ne!Y¢ ,
Neuromuscular junction
Muscle
Weakness6 or sensory abnormalities following nerve distribution (see FigS". 25-=2-and-2-s=J) · - - ----
-~ ' Stocking or glove'' distribution of sensory loss
~ilateral weakness including fa~~ ~~is, diplopia, dysphagia) and P.m~ ..
Inc.~e~ipg weakness with exertion
Sparing of sensation
Bil~~eral pro~imal or distal weakness
Sparing of sensation
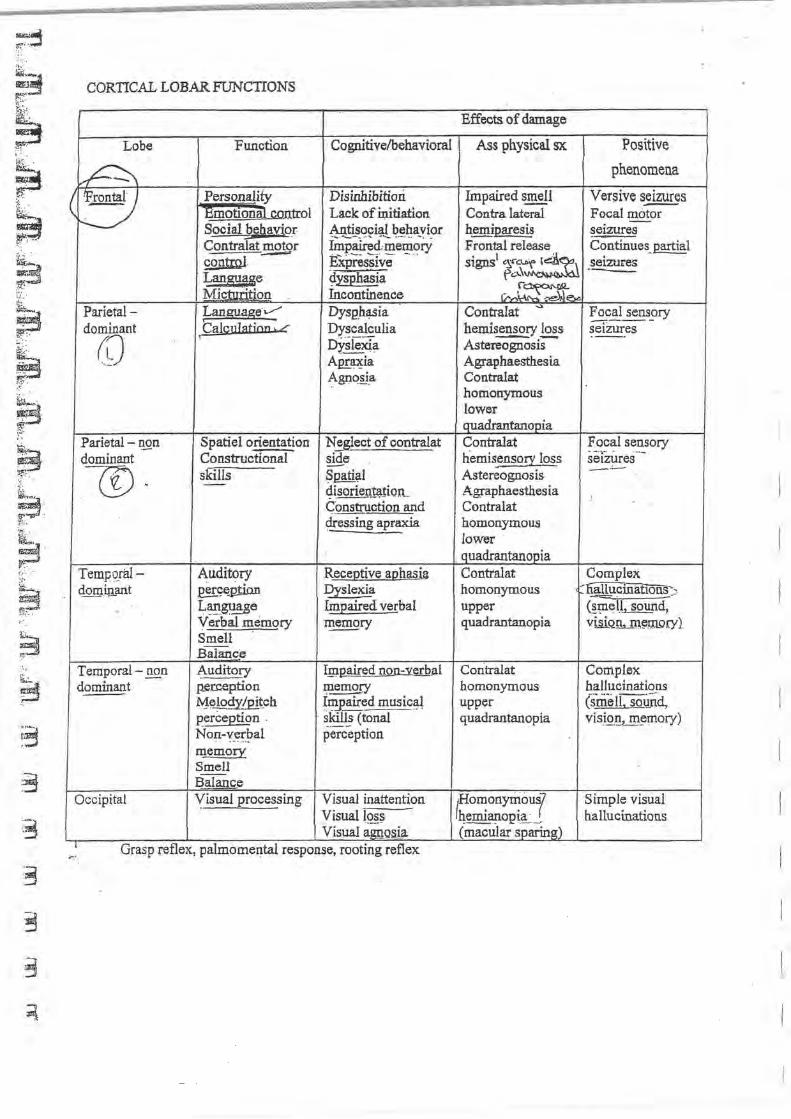
~· r L ~·. ~ ·· ··
b ~ · ~.· . ,:,.:. :·
~ ~
~ ~·3
·-
CORTICAL LOBAR FUNCTIONS
Lobe Function Cognitive/behavioral
~ (~
Personality Disinhibition ~motiona1 control Lack of ll:titiation Social b~gavior Antisocial behavior
;:;:
imp~J,'ffi~mozy Contralat motor ------ ExiJress!ve-· -... · · contm.l Lan8H_!se ~ysphasia · Micturition Incontinence
Parietal- Lang!!age ..----- Dysph~ia dominant Cal~Jllation ...c Dyscalculia
rD DY.sieXTa Am:.a:;ia ~gnQ~.a
Parietal - n._qn Spatiel orientation Neglect of contralat dominant Constructional side
.CD skills Spati~l - ·- 4isorie_n~tion_ Construction and dressing apraxia
Tempqral- Auditory ReceQtive aghasia domin_ant ~q~p!ion Dyslexia
" L~gu~_ge finEaired verbal Verbal memory ~ry
Smell Balartce
Temporal- _1!£n ~uditory I_m.pair~d noll::Y~.al
~omin~t p.erception memory M~!pitch ~~_Eaired music~l perception . · ~lrill! (tonal Non-verbal perception . ~ .... ..
memory Smell --~alanq_e
Occipital '(isual processing Visual inattention Visual iQ~~ Visual agnQsia
1 ,.., ... Grasp reflex, palmomental response, rootmg reflex
Effects. of damage
Ass physical sx Positive
phenomena
Impaired smell Versives~s Contra lateral Focal motor -hemiparesis seizures Frontal release Continues_ partial signs1 "X'~ ~~~ seizures
f'c:.~o.\~ --·~~ v----~ ~.:..11 .....
Contralat "' Focal sensory hemisensory loss
~,.-----
setzures Astereognosis
----
Agraphaesthesia Contralat homonymous lower quadrantar10pia Contralat Focal sensory tiemisensory loss
. -- ... - . . ~·-setzures
Astereognosis - -·-Agraphaesthesia Contralat homonymous I ower
. quadrantanopia .I
Contralat Complex homonymous ~cinat1ons~~ upper (~p1el.l. sound, quadrantanopia viliQ!h...m~m..ory)
Coritralat Complex homonymous hallucinations upper (smell, sotind, quadrarttanopia visi.Q.~~ m~mory)
f~e::~~uf Simple visual --··· p , ___ , hallucinations
.,
(macular sparing)
I
:...

JIEDSIDE NEUROPSYCHIATRIC ASSESSMENT .·· -~_ \.~-- --- ......... ~- ......... , . ., -· ·-.. ·-· ..... ·=:.· , · :::...:..: · _. ·-~' ...... ____ _ ._ ... _ ... I \ - I A1TENT10N AND CONCENTRATION I ~ ' ·-.-acs,dcSiiille as e.g .• awake aud co-operative' or 'co-<Jperaling but sleepy' etc.
Alphabet lest Read a random scqUdi.~otiCi.icrs wiiliih"C-iclli:rA ac<.Uffiiig more often than the olh<:rs. Patient must tap the table ev<ty time you say tbe lettec A. (almost like playing SNAP)
, 1 . i.A.Ncrui6EJ \.. .J ~pontaucous speech
Assess ~Y. prosody, ~tjty.~ etc. Llm_p~ed spout"!!cous speccb,is characteristic of ~·s dysphasia ,Paraphrase (substitUied word lltat sounds like tbe word that person wanted to usc e.g. 'sitter' instead of'sister'. Also known as phonemic parnp~ ,_. If the substituted word belongs to !he same category liS !he intended word, e.g. apple instead of peach it is known as semantic parapluasing.
Comprebo:usion Give palicnt 1 stage col1liJUilld. then IJy a 2,3,4 stage command Impairment of comprehension known as seosmy or Wernicke's dysphasia
Repetition -- · Repeat: 'no ifs ands or butS'
Indicates danlBge to arcuate fasciculus lmpainru:llt called •Co.nautMn aphliSia'
Naming · ~-...;;;.;;.,,..;;;;
Ask the patient 10 name objects e.g. pclliwatch b}' pointing atlhem lmpainnent is known as 'iiiiDiinal dysphasia' ·- · • ._,, .. ,.,.. Overlaps with 'visual object agnosl.ll
Writing Ask patient to write a short sentence (must JflBke sense, ignore spelling) lmpainuent luwwn as agtaphia
Rcadiug -Ask P!ltien! 1o read 'close yow- eyes' Patic:ut must follow lbe cow.maod to prove comprehension lmpainncnt luwwn as d.,;:Iexia or alexia
Mixed dysphasia Sc:Wom only ooo of above 6 impaired If more II1W1 I, known as mixc~g}obal d~~
/ -,: \.MEMORY ·''"""" ------~-V .---;·--rr •cult to assess, need coUateral
Alternative, hide 5 objects in consultiug room {with patient watching), after 5min ask patieDI to ,ollccl all S objects. Most people wilh 1 years of schooling will be able 10 do this
.. -~~> Ui>l@ . '-.':" -; !~~ \J!JtiJ!O.!l!M! '!'.'?!~~I!'!X'~~·.'!'s
inability to perform volunla!y motor sequences disorder of skilled movement that cannot be accounted for either by ~~~ 9!!1Xia ~~sensory loss: compr~llcosloii orai~tiOil lesion iii jiarieW. ani!/or"prcmiiior cortex constructional- inability to draw or construct (R or L) d!essing. inability to dress(R)
ideomotor - inability to carry out skilled movements (L) " ·&· """ pwitll• - -" c• '"""· --· ---• h~ !!!~~~oal- inability to sequence actions (bilateml) e.g. ask patient to pcrl'onn a seritl of movements
I J~.;:. \:AGNOSIA\ ~) -
• !mpaired higher !;lrd~¥.DSO~ pr~c~~ diSOr""der in the recognition of the significance of sensory stimuli a! !hough primary sensation and naming ability arc intact .- ·· · ·
• ~esion in parictaUoccipilal ~ uriportant to·cxatllitleSciiSorv palh~~!!!~! ~~ tactile, auditory, visual agnosia- inability to identitY objects" through a specific sensory modality (bilateral)
• tactile awosia(astcrcognosis)- inability to idcntify objects with touch {intact sensory lie) • prosopagnosia - loss of face recognition (bilateml) • an~~.! - denial of illness, specifically hemiparesis (R} • ~~i.a- inability to identify body pan • ~o!ier agnosia - loss of finger recoguiti011 {1..) • SJ!&tial ~s!!l- inability 10 recognize places (R)
,Pc:rslm2llD'f!Y11drome: ~ia ~ pnger •fi!\2!i!.o conffisiOJLif:ri@t and.wt (dominant piii'letirlo6e ies1on)
G) l~l!f~CTIONS .. \ • Seria17's or S letter word spelt backwards
Tests c:onccntrntion, working mcJliOI)' and CXC<:Utivc functioning • Red-green lest
Patient mll5t SIIY red when yoo say green and visa verna Patient must be able to inhibit incorrect resp!llse
• Month! of the year backwards/days of the week backwards • Alternating band movement$
Luria 1: both bands opened and closed llltmu~~cly Luria 2:Patient must alternate one band between flat, fist and the side of the band on a surface
• Design fiucncy The patient is asked to draw as IIWIY designs as possible, consisting offourUncs oflength, with each line touching at least one other line, in one tninute. Most individuals can gcuerale 5-7/min

LL Ll'1 _ _ ;:M: . . . ~ .AGf\. • .,_,v
Rhythmic movement of eyes <;:~mposed of a quick rod a slo~ ~~!!ei)t and may
be ro~, ~rtical or horizontaL 9~-~~-~~-~~!_:.~~~~ ~:_f"U:e~,b~ ~ir~~ti?~ of quick component. -Classification
• Eendular. • movements of equal velocity in two directions • onset usually in infancy (congenital and acquired) as a result of some
visual impairment but can occasionally be a symptom of cerebellar or brainstem .disease
• congenital nystagmus • ~~!. _fyrnti.Q_n
rapid, pendular, jerk on lateral gaze • often with head tremor • may be associated with ~K~!!i!al cataract,_ congenital macull!!: defec~
albinism • persistent throughout life ·
·~\ • -two components: a fast phase and a slow phase • ny~t!!g!J)YS.is..!lliiDCd according to. direction of_~~ f~i pJl~!!
benign jerk nystagmus, at extremes of lateral gaze IS a common finding without pathological significllilce
• two nystagmus syndromes are most conunon gaze evoked __
• occurs with gaze toward a direction • often adverse effect of sedative or anti-convulsant • can alsoresuitfrom cerebcliar or c~vestibiiiiir dysfunct~Q!!
vestibular • increases with gaze toward the fast phase .
usually associated with vertigo when lesion is in peripheral vestibular apparatus
Labyrinthine Disease • due to a left-right imbalance of stimulation from vestibular system • causes a slow drift of eyes towards side with damage/decreased stimulu~
(thus nystagmus. i.e. ~nst phase is away from_ ~~~~o!l) • physiological ·
• rotational acceleration with nystagmus pointing to direction of turning, i.e. slow phase points to visual image
• cold/hot H 2 0 instilled into ear decreased/increased relative stimulus from CN viii, resulting in nystagmus_to the oppositdsame side
• for caloric testing, remember" COWS»--- ·Co.....'• \e'L C old water resUlts in nystagmus to Opposite side
• W arm water results in nystagmus to S arne side • pathological .
• characteristically unidirectional horizontal (toward nonnal side) ur horizontal rotary .
• nystagmus towards normal side; may have torsional component • ~~o"present;~~s and_~~~:_~Ld~ft~~ss common in
Meruere's, vestibular neuritis, vascular disease
-~ '< \" ·v • in berugn positionw veitigo;-etfcit by Dix-Hallpike maneuver (see OT7) which fatigues with repetition
Cerebellar Disease • horizontal jerk nystagmus towards the side of the cerebellar lesion (opposite
to labyrinthine nystagmus)
\8iilrist"em niSease-1 . • _verticiil nysfii~us,jerk nystagmus with fast phase in direction of gaze;
vertigo m1corrunon • other signs ofbrainstem involvement present (cranial nerve. abnormalities) • pons-midbrain, medial longitudinal fasiculus (MLF)
• "ataxic nystagmus"t'intemuclear ophthalmoplegia" • note: acquired pendular nystagmus signifies MS • lower medulla
• down beating nystagmus on forward or lateral gaze can be seen in lesions around the cervicomedullary jm1ction (e.g. Chiari malformation, cerebellar degeneration)
• up beating nystagmus in primary gaze can be seen in lesions in the medulla
(e.g. MS, tumour, Wernicke's)

PUPlLLARY SIGNS
CLINICAL PROBLEM: ABNORMAL PUPILS/ PUPIL REFLEXES
3 RD nerve palsy· • Dilated pupil • Extraocular muscle palsy (eye typically 'down and out' • Complete~
Homers syndrome· a sympathetic defect causing partial ptosis, miosis, wtd anhydrosis ami apparent enopll1almos ~1ay occur anywhere along the sympathetic pathway on the affected side
1st order neuron (preganglionic): !l_ypothalamus, meduUa (brainstem stroke), spjnlll W!!!_Q!!f, t.:!S. iuira~l!!!i!!l. ll!!_n~~:Syf"fuw.Hi.Y~li.~ 2nd order neuron (preganglionic): apical lung cancer (Pancoast's tumour), paravertebral mass,carotid artel)' dissection Jrd order nellflln (postganglionic): cluster headache, migraine, cavernous sinus mass, truuma (including surgical)
clinical confinnation with cocaine test: cocaine docs not dilale a miotic Homer's pupil no test to differentiate ceut'iul from ·preganglionic lesion parcdrine (~ydroxyamphetam..i!!C?) will not dilate a post-ganglionic Homer's pupil most preganglionic Homer's are serious, whcteas m_2~~.Q.@:.ful.mers_~ benign ·
Holmes Adie syndrome {myotonic pupil)
• be.E_!ll!' conditiQn • usually occurs in woman • usually unilateral (li&>A.j • Affectcdp~pil noll_lla~~~~Y dilated witlt J?QQ!.~~_!ion !~ !!&t!.. .
Pupil i.l s!Q~!Y ~c.t!'tU9.!\C~o!lmlodation, may even constnct more tban·a normal puptl Associated with a~~t/di~~~~~ ~~e .l!'ld kn~ reflexes (Holmes Ad.ie syndrome)
A rgy II Robertson pypil: • P...!JPil is constricted and ~nrc active to light but reacts to accommodation • Iris may be patchily atrophied or depigmented
·<:"~(-" .. ?'~} ,-) _, ~eurosvP-bilis ~--...- t DiBbetes mcllitllS
(:;) ('""··""~- • ~~-a~ s~drol_!!!_: (pseudo- Argyll Robertson) .·< C, ' \' ~ · 6 ·\N:. ,.: .. - .x~c. J ' . '-- · · --~ ' ~-· -Local pupillary damage:
• Jrregular_eupils, often with associated adhesions to the lens (synechia) viuiable d-egree of reactivity
• Evidence oftmurnalinflamrnation
-- ILJ!II.,."
'· Relative afferent papillary defect (Marcu!d}un.;-) . • a failure of direct pupillary responses to light ..
a sign of <!_afi.l~~~ -~~ th~ aff~re~ ~~_n l!f~ E\!llilllliYreiii:X. arc- (C~ optic nerve (Optic neuritis, ischemia, compression) 1
optic chiasm {severe compression, e.g. pituit81)' tmnm1J:) optic tract to prctectat nu.;leus
• clinical assessment: swinging [email protected] • swing light from one eye to the other
when normal side is illuminated, both pupils constrict when damagelsldi:-iS'hi~iiiiiiect, boilfln.lpils paradoxically dilate . -···- - .... .. _ ...
l Hutchinson pu~ . .-------;-Arises om tapidly raisin~la!cml IV · •
• The~~ on the side ofilie leston first constricts and then widelY. dilates • The other pupil ilien goes iliiough the same sequence -

CLINICAL PROBLEM: TREMOR- rhythmic os~i}~~'!!Y !J!yo.!_unt!l.IY_~ov~.mef!_t about an axis
/Re~ting i'remor.7 ~~.p--:-siowCJ-7 Hz), coarse, distal
• thecharacteristic trenior of ParkinS.Q~m-• hands- pill rolling, alternating flexion/extension of fingers or hands, alternating pronation/supination of
forearms • best examined with hands resting in lap, ~an be broughl_E_!!!_~tasks of~~P.-.C?en~tion
(Postural ancfActiori-(KinetiC) Tremor/ -'-'-'~---- ra8t76:.-f2 -Hz). tiDe, usually upper limbs, head (titubation)- titubation stops when head supported! 1!
"' seen best with arms and hands outstretched • physiOi.o-gicaC- ---- - ·- -·-- · ·--- · ·· ·
always present, imperceptible to the eye o exaggerated physiological
•
•
•
anxiety, sleep depriyation, engQ_crine (thyrotoxicosis, cushings, hypqglycaemia, phaeochromocytoma, drugs (beta agonists, coc, dopamine agonists, caffeine, theophylline, lithium, epilim, tricyc!ics, phenothiazines, amphetamines),~ (lead, mercury, arsenic) and alcohol withdrawel
essential tremor AD inheritance (familial) patient complains of shaking whepp~~ !e~cup, putting a glass to the mouth, or tr.d!!g to ~ soup - · · -- --- ·- -- - - - ·-- -
affects handwriting, and voice head titubation is seen tremor diminishes with alcohol
treatment: ·_propmnoloi; ·nadolol; prhru'"d;;O.e(barbiturate) if B-b locker contraindicated (diabetes, asthma) • surgery \).A.JVv-v-0 - . ,.
postural (Holmes/rubral/peduncular)~r · - - Violent, large amplitude postural tremor that worsens as a targ~is approaced.
Originates from the S.!l~rior cerebe_~ Q.eql.l:!_l<:_~~ (site of cerebellar outflow to red nucleus) Common ·in advanced MS, very debilitating Treatment: Stereotactic thalamotomy (poor results) ·
rfntention Tremor (Cerebeflar Tremor)\ . f-.-due to·orea.Kdowrioffeedback control of targeted movements
• seen in diseases of cerebellar outflow (worsens with alcohol) ~coarse tremor -;o;_iitti~~r-ge]'lq;_ !lbsent at r~t.
mtention tremor \yo~~a.t_ ~"!!~ P?int_ !!f mover!lent may be associated with d.):'sarthria, nystagmus and ~tax~
• examination maneuvers: f~er t~!:_lesting, h~clto shin testing etc. -~- - ·-· -
Investigatiog_ of Tremor ·- • all patients< age of 4S_exhibiting ~mar should be screened for\WjlsoJ:!.'~iseaseJ~.(U~-e~~~~ copr_er
-~loplas!Ilin_J~); and havetTSH1(postural tremor) anc( C:T(MR.I}lfCerebellar Cftsease suspected) -performea

VERTIGO _ ___...,_.
CLINICAL PROBLEM: VERTIGO (defmed as an illusion of movement of self or swroundiugs (Usually .~l?!ato!Y/"Ri"!!!!!ll) often associated witlfiiiipwslon,(retlS'aiioa 'OI'iiOdypi.iJledmspiice)Oij~lilopsia ·1 (visual illusiou of moving bock and fo<lh)as well as ~~~~-~4~.!'.ru.!-li.!'g an.<! g'!\! ~ia; venigo nu.st be distinguished from other causes of dixz.iness, such as prcs~c, gait abuonnalities and psychogenic pl~e_no~··~) ·- .- ·-·--- ... __ _
l say this because:
On history; • distinguish from prcsyncopc (feeling lightheaded and faiot) ·nature ofvcnigo:-dli!iiiiU.,i'l positional? rccWTent? • audi1i_ry_ S)(l1ll!lll111S (hcariug loss and tinnitus)? • ,;~;;rolo~!~~l_~.P!O.(U~? . . • ~§.~.U~~J:!? (e.g. awinoglycostdes)
On clinical examination· • otoscopy, twtiug f01k tests for hearing • nystagmus, cranial nerves- especially 9:!.:! (including com~al reflex) • long nact signs: cerebeUar, pyflllllidal, senso'Y. • tiln__d<>!~~PY - -- -- - . . . -
Suggested spe<ial investigntioM:
• ~.lJJ!i!!!!!2!n'. £i!!.01~ ~W>g • evoked potentials,_ ~G,9J~ ·VDRL
,. ----.... Tahlc IJ. Pcrir>her-o~l vs. Centrat V.:rti~u'
F\:.ature
Calodc. Tc>l
l\ro.~in.'itcm ~1r (. 'r:miul n~·,.\.! si£nit
ll~:ui!tg lu>s.. li111UltL'\
Nuu:it.'U tuld Vomiiing Vt!rtign
Fulliu~.
\1 i.\tr~l lhativn
l~l(i7iiillt'' · .~~~~~lillll."i j,~~llll.! uwuy ~\lll klsi(lfl (.)in!''-1i'-tn u,l\:s nuc dauug< wl~u dln.:..:lion uf }:rub! d~UilJt~:i
1\bl'U.1rm;al '"' sid..: of ~~~iull
• -\b,.:nt
Vlku !:!!."''-~"
~~ dll~n n.N.atitulU~ al~u~-s: prL~·nt
(Jiicn .!all• 11.1 u..., ,;,~.: . pppu~lh!'ll\Shigmus ~h1SI pha:ic) I.C . I~·~~
(l!hihiiS 11\Sh:\!ntUS
C('nlnll
!\.fa} be llllfllll\1
(Jtlen Prt:S<:nt
t J.;uall" uhs.:m ··--( t;.u~li)' milt!, ullen Uh'l(;nt
Olkn lld!iU!l" 111"11 !lll:.:ii<k!Jl" Jesiott 1;\ul ma)~ '"~tmibl~ dtre\.'Uon
~\'\"
\·~\i.:...-1~
~Jkni!!ll po~!~9!!..~ ~~!'th~\l lru\UU.a M~ni.?.re'~ tlisa~ ~~ar u,;uronilis ~.PT!nK-cii<i\-s-· -fi!>tul:w OriiiflO:xicily AMilihE nl!ttr<'tn~ V.:':"ouhtr luop
Centrul
Hernes Zoster C§ainscy Hlliiisyndromc)
HE_P.~c.C:':\lption.<!f ~!e~ @!l.!!i!Q~Y c!,ID!Il Facial palsy +I- 'i)~fiicss, tinnitus, vertigo ~~ .............. . ·t~
&;..;;~.-.ii~1
+\.. .... \.~ ... : ..c :: .. ·C 1;0. '".;.
. ... .. - Vcltigo'(lasting >20min at a time,+/- NN) • HE;;ri;;B loss (fluctuating, sensorineuaml but may become penuancnl)
Tinnitus (or • scosc of a\UU fullnc5s)
lb:Bedrest for acute attack, C~<:, endolymphatic sack sur~
[Aiiit~e Jabaffitiiruq - ~· · ~!'!P-~~1, severe vertigo
}'{LV No deafuess or tinnitus c;.;;cs: ·vas<U!ar lesions, viral
s;w~ y~gq ~o.ve~ ~ <:I!<.Ys Complete recovery takes 3-4 ~
Rx: Reassure, sedate
r AcoustiCiictifom!f\ . · "-=. :M19iiiateiJ bcllri!!J:.!fliS, onset of vertigo only l.all:r
lpsilalcral i.nvolveme!ll of CN 5,6,9,10 and cerebellar signs Conunon in neurofibromatosis
CLINICAL PROBLEM: ASTERIXES/flapping tremor
0 /E: Ask patient to hold arms out with the hands extended at the wrists, iftitis posture is periodically the hands will transiently drop vefore the posture is taken up again.
dropped,
Pathology: Asterixes is the result of i!ltermitt~~! (aill)l'e of the l!arietal mechanis~. required to maintain a posture.
Causes:
• • e
• •
Renal failure
Liver failure
Hxpercapnia (O~·-t-Drug toxicity (e.g. P~~n~in), Acute focal parietal or t!tala:.n_:~~S~?-~S (e.g. vascular)
SII and TREATMENT according to causes.
. :.iS •;.\' . CLINICAL PROBLEM: CHOREA (jerky, involuntary, small amplitude, purp~less movements)
.;c ==::a - .
0/E: Fidgety movements of the limbs and grimacing of the face ~ , .._\, . . . - . ..·· J~'c.:>-\0 ."1....\,..uT-l
~ ,,~v ~->'• . .
Pathology: Disease in caudate nucleus (e.g I:IE!Ltin!@n's) or pxcessive activitv in the striatum due to dopaminer~ic D z . drugs used to treat Parkinsons
Causes: e
• • 0
•
•
Hereditary (Huntington's, Wilson's, Porphyria, Neuroacantocytosis, Paroxysmal choreoathetosis) Cerebral birth injury (k;ernicterus) Cerebral trauma Drugs (levodopa, dop~fne agonists, phenothiazines, tricyclics, coc)
Endocrine (pregnancy, coc, thyrotoxicosis, hypoparath.yroiclism, hypoglycaemia)
Infective/inflammatory (Post-streptococal-~ydenhams, SLE, Antiphospholipid antibody syndrome, Henoch Schonlein Purpura, CJ disease) 'St- \)-;h..~ 2-c.~.o,c.c .
Va5cular (lacunar infarct, A V}.-0
SII and TREATMENT according to causes.
CLINICAL PROBLEM: HEiVflBALLISMUS (more dramatic ballistic .movements of the limbs, usually unilat _......._......_..,._..._ ... , _ _.•- · - · ... - - '- ....... ~· -- ......... - ......... ' · · :
especially in proximal limb muscles)
• • • •
Lesion in C..Q.~tralateral subilialru;nic Dl!9l~':!:S or its neuronal projections usually self-limited, resolving in 6-8 weeks most common cause is stroke (PCA territory) neuroleptics are often effective for symptomatic treatment

3
3
3
CLINICAL PROBLEM: A,THETOSIS (stow, writhing movements of the limbs)
CL.ll-II~AL PROBLEM: DYSTONIA . c: ¥0'1
• sustained co-contraction of agonist and antagonist muscles which distort the limbs, trunk or face into cbaractel1stic postures··-- ·- · ··
• idiopathic torsion dystonia childhood onset, sporadic or dominant inheritance initially fntermittent progressing to constant disabling generalized dystonia
• abnormal movements are not present dL~g ~le~, and are enhanced J?~mo~<?_~-~l!~.s~ and y_~t!l.!~ activicy · · .. ·-··
"' Fq_cal DystgJiias: These are the most common forms of dystonia. They typically present in the fourth to sixth decades and affect women more than men. The major types are:
1. Blepharospasm: dystonic contractions of the eyelids with increased blinking that can interfere with readmg, watching TV, and driving.
2. Oromandibular dystonia (.OMD): contractions of muscles of the lower face, lips, tongue, and jaw (opening or closing). Meige's syndrome is a combination ofQMQ and blepharospas~ that predominantly affects women over the age of 60 years.
3. Spasmodic dysphonia : dystonic contractions of the vocal cords during phonation, causing impaired speech. Most caies affect the adductor muscles and cause speech to have a choking or strained quality. Less commonly, the abductors are affected, leading. to speech with a breathy or whispering quality.
4. Cervical dystonia: dystonic contractions of neck muscles, causing the head to deviate to one sid~ ( ~;cl.icoliis ),"Iii aforward direction ( anterocollis ), or in a backward direction (retrocollis) . Muscle contractions can be painfi.ii and asso"ciated with dystonic tremor 8rid""a secondary cervical rad.iculopathy.
5. Ll!!;k.1xstonias: these can be present in either arms or legs. and are often brought out by task-specific activities such as handwriting (writer's cramp), playing a musical instruglent (musician's cramp), or putting in golf(the yips). ~
• Focal dystonias can extend to involve other body regions (-30% of cases) and are frequently misdiagnosed as psychiatric or orthopedic problems. Their cause is not known, but genetic factors, autoimmunity, and repeated trauma have been implicated.
Causes: perinatal anoxia, birth trauma and kernicterus are common causes .. . ---- . ........._
Treatment often unsatisfactory anticholiriergics and botulinum toxin injection, surgery ------------· ..... . .
CLINICAL PROBLEM: MYOCLONUS (rapi~~h~1k-li.ke muscle jerks, sufficient to move a joint; often repetitive and sometimes rhythmic) - -
• generalized myoclonus widespread distribution physiologic: occurring during failing asleep or awakening (nocturnal myoclonus); and hiccups essential: benign condition, sometimes inherited, occurring in absence of other neurological symptoms epileptic: ~eizure disorder predominates symptomatic: part of another disorder- degenerative (Wilson's, Huntington's, Alzheimer's) ;
Causes: infectious (CJD disease, AIDS dementia complex, SSPE); metabolic (hepatic and renal failure)

• segmental myoclonus
_.eatment
restricted to particular part of body arise from lesions affecting_ cerebral cortex, brainstem or spinal cord
clonazepam may suppress myoclonic movements treat underlying condition (e.g. valproate)
CLINICAL PROBLEM: TIC (brief, rapid, stereotyped and irresistable actions, often resembling fragments of .rrnal behaviour) -
" wo~en with~~~~. diminish during voluntary activity or mental concentration, and disappear during sleep 1!1 most frequent forms: blinking, sniffing, throat clearing, hitching the shoulder, or throwing the head to the
side or backwards · ··· ·- - · -- ·
• simple tics (e.g. eye blinking) begin in cfuTdliOoa as nervous mannerisms and disappear spontaneously
• Gilles de Ia Tourette Syndrome multiple motor tics vocal tics: sniffing, snorting, involuntary vocalizations and the compulsive utterance of obscenities
• (coprolalia-:veryrare) cc ·\·::. ;\ ,-~r\1), ~'-"C'<-. '<' ~-)l u . may be associated with obsessive compulsive disorder, attention deficit hyperactivity disorder,or a mood disorder
reatment
I ' "'•
.· ..... ~
often familial clustering, 1:1.2:!
simple tics may respond to ~~nzod.iazepines halope~ol and pimozide are traditionanreatments usualfy 0 not treat unless marked tic or disabling
firtua.lly all movement disorders, including tremor, tics, dystonia, myoclonus, chorea, ballismus, and parkinsonism, an be psychogen"ic in origin. Tremor affecting the upper limbs is the most common psychogenic movement
disorder. Psychogenic movements can result from a _somatofonn or c.qnv~r~j9n disorder, malingeri.Qg (e.g., seeking financial gain), or a f~us disorder (e.g., seeking_Q!!YChological gain). Psychogenic movement disorders are :ornmon (estimated 2-3% of patients in a movement disorder clinic), more prominent in women, disabling for the
!atient and family, and expensive for society (estimated $20 billion annually). Clinical features suggesting a psychogenic movement disorder include an acute onset and a pattern of abnormal movement that is inconsistent .vith a known movement disorder. Diagnosis is based on the nonorganic quality of the movement, the absence of 'in dings 0 fan organic disease process, and positive features that speCifically point to a psychogenic illness such as variability and distractibility. For example, the magnitude of a psychogenic tremor is increased with attention and diminishes or even disappears when the patient is distracted by being asked to perform a different task or is unaware :hat he or she is being observed. This is the opposite of what occurs with organic movement disorders, which tend to Norsen when the patient is distracted and abate with attention. Other positive featUres that suggest a· psychogenic problem include a tremor frequency that is variable or entrains with the frequency oftapping in the contralateral limb and a positive response to placebo medication. Comorbid psychiatric problems such as. ~iety, depression, and ~motional trauma may be present but are not necessary for the diagnosis of a psychogenic movement disorder to be made. Psychogenic movement disorders can occur as an isolated entity or in association with an underlying organic problem. The diagnosis can often be made based on clinical features alone, and unnecessary tests or medications should be avoided. Underlying psychiatric problems should be identified and treated.
-----------
Definition • a state in which patients show no meaningful response to environmental stimuli • from which they" cannoi"\)e aroused . .
Pathophysiology · -----------· · · • consciousness consists o~~_£OmE9._f\~n_!S
arous~ • alertness, sleep-wake cycle ~_E!!!:_nt - responding to external stimuli i.e. seeing, feeling, hearing, speaking
• consciousness requires i!l!~g.!lQ!'l!lsi:;p_m:ces_ intact reticular activating system (RAS) in brainstem
" le~_!_Q!_lS difftlScly a.ffecgpi!j~ml¥E~.!.""-&. or directly ag~~~-~e .13-~S cause impairment of consciousness and potentially coma .
., focal hemispheric damage does not alter consciousness except b>:: mass effect or by precipitating seizures Classification --- · ----- -- -- ---- -- · ·
• structural lesions (tumour, pus, blood, CSF); (1/3 of all cases of coma) ----- - ·- - e.~pagd}.?~_:.'!-P.rate~~~'i¥.:!!1-¥~; cause~ transtent.orial. herniation, .leadi~g to brains:ern compression (and thus
·.RA'S' dysftinaloii} or maJor shift (honzontal) wtth bilateral henusphertc dysfunction posterior fossa lesion: may directly destroy the neurons of the brainstem RAS
• metabolic dlsordersidiffuseliemispheric damage (2/3 of comas) --;---ae{iCiency of_es~~ntial substrates, i.e. ~-~yge!lt ~lucose, v~tam.~n ~_!2
endogenous/exogenous toxms, i.e. drugs, _hea~etals, solvents sysTemic mefii'ifuftc diseases, I.e. ~effiia:- hepatic encepbiiQPathy, e~~~_p--~L}'!ejq~.balances
General Management: · ·-• Alrway and C-spine stabilization -../ • Breathing -../ • Circulation ,/ • Drugs · · •
o thiamine SO mg I:M (think about alcoholism/nutritional causes) \ e;e~"~f~ T ......._ tt \.i o naloxone (Narcan) 0.4 mg!ml2E.!UV (think about opiates) · . c_ __ ,, <, u.-.. • 1- \.J . o 50_ III'. 59% glucose IV "t" ·\i-,1c-~- ~ \01-i<\Q .__..-.. •.. - . :;,
Evaluate patient J.: ·
EVAL'JATrNO THE COMATOSE PATIENT
~.0' • p£eviol!slr.e~;ent head injury (hematomas)
sudden collapse (intracerebral hemorrhage (ICH, SAH) lim6 .. iwitchlng!incontinence (post-ictal state)
· sT<iwOfise.L~f SY-mptoms (mass or metabolic, bugs or drugs) ·diabetes mellitus (DM) (hypoglycemia or hyperglycemia) depre-ssion( drug overdose)
• telephone witnesses, read ambulal!c~_report, check for .l!!~~i~.:~~r! l:!_~cc:!et Physical E..X1i!nfuation · -------- -- -,, · neurological - full examination essential but concentrate o~ Gcs:• follow over time
res_Eiratio~ _ (rate and pattern) ·- ' a·pneu~~c or _ataxic (brainstem) . . : . _ Ciieyne·Stokes (cortical, brainstem or toxic/metabolic)-<-~tfJ//p-----•·~\,-..\_,.,..-pos~- -=- -· . de~o~: severe b~tateral d~mag__e at?\?ve f?idb!ain ( --.-~ '\' \;.o::-- < c.~- \~(:- < :...U dec_erebrate: damage inmlabrain, ~iencephalon ·"t""·- '< -
movement · (l ~ \j...~ce\ ~~:\IJ\Ot (-' spontaneity, symmetry and seizure activity pupils ·reactivity and symmetry (CN II, III), papillede~ (increased ICP) reflexes \ . , corneal reflex (CN:VI VII) :: .:y!5"' ''.''"'.;..:i v
gag reflex (91f~. t 'i Is: :..-:: o!_-'__.., .C i i ocuTOcephalic reflex/doll 's eye reflex (after C-spine clearance}: test for brainstem integrity oculovestibular reflex (rule out tympanic perforation and cerumen impaction first) deep tendon reflexes and tone
.. j
l

. .,
.p: .'
plant~r retlex caloric stimulation: normal response consists ofip~_ilateral stow g_az~ (brainstem mediated) and contralateral saccadic correction (cortically mediated); cannot be voluntarily resisted LP after nonnal Cf to rule out meningitis, subarachnoid hemorrhage (SAH) (increasing evidence that lumbar puncture (LP) can be done as primey investigation if no evidence of increased ICP)
• Decorticate posturing i.e. arms flexed at elbow and wrist, and legs extended at knee and ankle in response to a noxious stimulus, points to a lesion below the thalamus but above the red nucleus.
• Decerebrate posturing i.e. arms extended at elbow, pronated and flexed at wrist, and legs extended at knee and ankle, suggests a lesion below red nucleus but above vestibular nucleus.
Assessment and DDx • orderly, progressive, loss of function- expanding supratentorial lesion is likely
o hematoma, neoplasm, abscess,· irifiammation, hydrocephalus, etc. 0 massiveinfai:cffon with edeiE.~ . -~- (.;. ·-----··
• simultaneous onset of impaired consciousness, ~inpoint p!!£ils ()71~ and brains tern signs (i.e. skew deviation of eyes) suggests !]OSterio.r fossa. lesion
o brainstem infarct or hemorrhage 0 cereoellir infarct' or '&emorifiage
Note: abruptonset of vertTgo;nystagffius, vomiting, inability to stand/walk (with normal lower limb strength) with occipital headache, coma, miosis, and contralateral ocular deviation suggests c;:er~~Llar h~t:n~r:rhag_e
call Neurosurgery for surgical compression • scattered neurological dysfunction (i.e. wacioiiiliiitem with no focal signs~ suggests metabolic coma
o ~P.oxia, hypoglycemia, toxins, major organ failure o majorendocrine disturbance (i.e._m~l!_lll), major acid-base/electrolyte disturbance o ~~war~ ~~ingitis and SAH - can mimic metabolic coma!
BRAIN DEATH 1efinition
irreversiWe.loss. of prain function; vital structures ofthe brain necessary to maintain consciousness and independent vegetative survival are diU1laged beyond repair c~-~~~vascular activity may persist for as long as two weeks but usually CV collapse occurs within several days
.1A.NDATORY CRITERIA FOR DlAGNOSlS no. pQte11tially anesthetizing amounts of either toxins or drugs present (e.g. barbiturates) hypothermia below 32°C or other physiologic (metabolic, endocrine) abnormalities must be corrected irrever$ible structural disease or a known and ii:reversible endogenous metabolic cause due to organ failure must be present 12_p_q!!!:~i.9d of no cortical or brainstem functioning must have elapsed no cerebral function no bminstem-reflexes clrcuiation may be intact, purely spinal cord reflexes may be retained no seizures no p·uplfreaction to bright light in both eyes absent corneal reflexes, no vestibu!o-ocular reflex. (VOR) no eye movements when ice water slowly injected into unoccluded external auditory meatus with head raised at 30° no gag .refl~x to bronchial stimulation with suction tube no motor response in the face or muscles supplied by cranial nerves to a painful stimulus (supraorbital pain, intranasal pain) no respiratory effort when disconnected from ventilator for I 0 minutes after being hyperventilated with 6 L 0 2 /minut~ to prevent anoxia, (apn<!a test) · evaluation has to be performed by ~o specialists (e.g. neurologist, anesthetist, neurosurgeon), patient has to be evalll_ated on two separate occasions ·
P~B,~IHE.NT..VEGEIA TlYE. ST A ri;:J no evidence of behavioural response to visual, a119i_t_ory, tactile, or noxious stimuli no awareness of self or environment no language comprehension or expression due to irreversible loss of cerebral cortical function BUT with intact brainstem function and rudimentary movement patients have normal eye opening and slee~wake cycles, and may sur-Vive for years in this state (average life expectancy = 2-5 years.} EEO may be flat or nearly so
i. \ .. ". ' ...... ~; ·. ' .... -. \
\ ·._ \.: \ ('
. ---\ " . ·~ ',i ,\_I •' ' ~

( 'UNlCt\L PROBLEM: Confused, agitated patient . ------·-........- ---·•. ~ \ \, ·. \. \. ........ . , .... _,
' . . . . . l)hl~lQ.!itic Criteria DS~.{.,iv .l '- .. , . ,, .. . , _. . . . . ·- ·, , · · ·· · · . , . . '.1. -.~ · ..
r\. disturbance of consciousness (i.e. reduced clarity of awareness of the environment) with reduced ability
. ....
In i'tH.:us, sustain or shift attention ,-\ . :, : , . _ .· ., . . - . _ _. '-·: ,, .. ,,., __ .. .. '·. ,-,_ . ·. ··.·- ~· ., < . · .. \· 1 • ..•• 1 r. a change in cognition (i.e. memory deficit, disorientation, language disturbance) or development of a pcn:~ptual disturbance not better accounted for by a preexisting, established, or evolving dementia - · · · T· ... • • \ ·
C. disturbance develops over short p_eriod of time (hours-days) and tends to fluctuate over the course of the day 1 l. there is evidence from· the history, physical examination or laboratory findings that the disturbance is ·.: .. (
dlll1 to a physiological consequence of a GMC, substance intoxication/withdrawal, medication use, ttl.'< in exposure, or a combination
\- .... ' . ... •, "' ~ ·; ·. . \ - \-_· \ S·;" . . \(,:- :" .. , t\ \,; .~ • ~_,. . ..:. \ .·. \ ~ .. _::.
. ~ "\_ .. (\lJ.!J_rnon symptoms • wandering attention • dis tractable • disorientation (time, place, rarely person) • misinterpretations, illusions, hallucinations ·speech/language disturbances (dysarthria, dysnomia, dysgraphia) • affective symptoms (anxiety, fear, depression, irritability, anger, euphoria, apathy) • sh i fl:s in psychomotor activity (groping/picking at clothes, attempts to get out of bed when unsafe, sudden movements, sluggishness, lethargy)
. , ·': • • ••• ·J. ~ ·. <' \_(' ,·· .. · .._;r
• ' · .
Risk factors .. ~hospitalization (incidence!J9.:40%)) • nursing home residents (incidence 60%) • childhood (i.e. febrile illness, anticholinergic use) • old age (especially males)
t" '.'·.··." · ... ;,_'
• severe illness (i.e. cancer, AIDS) •.-. (. .
• pre-existing cognitive impairment or brain pathology • recent anesthesia • substance abusers
·,-:: ( · ·· · ·'\ .- ... \ ~ ... : .. ..... ~.--· ... • .• :'. t~ "z.r (\\.;~,
Folstein exa'm .. is helpful to assess baseline of altered mental state- i.e. score will improve as symptoms resolve
Differential for Delirium I - Infectious (encephalitis, meningitis, UTI, pneumonia) W- Withdrawal (alcohol, barbiturates, benzodiazepines) A- Acute metabolic disorder (electrolyte imbalance, hepatic or renal failure) T- Trauma (head injury, postoperative) C- CNS pathology (stroke, hemorrhage, tumour, seizure disorder, Parkinson's) H- Hypoxia (anemia, cardiac failure, pulmonary embolusya::=-
1 c..o 1~, / r·" :.__)
0- Deficiencies (vitamin B 12, folic acid, thiamine) E- Endocrinopathies (thyroid, glucose, parathyroid, adrenal) A- Acute vascular (shock, vasculitis, hypertensive encephalopathy) T ·Toxins, substance use, medication (alc;ohol, anesthetics, anticholinergics, narcotics) H ~Heavy metals (arsenic, lead, mercury) · ·
.·./ '
investigations '; r -· .·/ '· ' / , i. • ' . ' . ,. • standard: CBC + diff, lytes, calcium, phosphate, ~agne~i~, glucose, ESR, LFTs (AST, ALT, ALP,
albumin, bilirubin), RFTs (Cr, BUN), urinalysis, ECG
{ l '
• as indicated: T~H, CT head, toxicology/heavy metal screen, VDRL, LP, LE preparation, B,t2 3Jld to lie acid
\ \
I .I

.. 1 ;p
lwels, EEG (typically abnormal: generalized slowing or fast activity) Indications for radiotogical _intervention: focal neurological deficit, acute change in status, anticoagulant use, <. ' · ·\ ':. · ·· ..
. . -- · . ~ . . .. {" . \ . . \ . . ' .: · .. \ r \ early incpf!tine.nce, gait abno:mlality, history of can~er ( ' · · " \ ' ·· ·, '·' ·. '- ~ · ~._, ''· ·' · · '
~ -... , · .. l c·'·r ··\1 . \'.; ;(:~~ ..
· ... • . r:~u~enleJn , ·;·.1' ..... c ,· .. ,·· ·· r\' ... · ~- '' ·!
• identify and tn;at~deElyjng cause immediately .~ ?:;. \ 1 1:·., ( ·.:\.,· ·. l ;·,., \ ~ • stop all non-~ssential medi_'cations_ · . . ·~ .··\ ·' ':" ·
~- - - ' -"'' ' \. . .. . , (!.':-...
• maintain nutriti_<>p., hy~tion, el~c.tr.olyte balance and monitor vitals \- \)< <' \ (. .:': ....
• environment should be ~t and w~Jl:llt !-..~ .•4' .~: ' . ' ·~ ... e .. \ . \• ~·-:· ·. ·. ,. • optimize b,el!Iing and .vi?~l9.!l • room ne.'!£ nursing station for closer observation; constant care if patient jumping out of bed, pulling out
lines • famj_ly_ member present for reassurance and ~e-<!tientation . • calendar, clock for orientation cues • pharmacological - .haloperidof (fo~ E:!~e ), lora'iepam; physical restraints if patient becomes violent • up to 50% 1 year mortality rate after epiSode of delirium -·=-
T<tblc!. Companson of Dementia, Delinum and J?s.:udodementia qf~~
Onset
Duration
N1tltlru! History
Lo::~·elof Consciawmess
/\tten!i(Ul
( lrie~itation
Behaviour
Psydwmotor
Slo::l:.'p W<~ke Cydt:
Mood <llld Artcct
Cognition
Delusions
Ml!mory Loss
l.angttagc
Hal.luci nations
Quali:ry of tlallucinatious
iYkdkal Status
,;
Ol!ll\Ctlli <I
Pro~essivc Usuul~y in-e'l<-et!.ihlc
Nomml
Not initiuny ant:~:teu
ln!m:t inithlty
DL<~inhihit ion. cu!ll~tropluc r~actil1n impttim1ent in i\DL lAD l. personality change. los.~ of SOCial ~;rJCc;S .
Nom~t1l
Fragrn.;nt~d sk."\:p at night
Del--rea sed exe<.:uti ve fuucrioniug. pauciry oi thought
Com pensatmy
Recent, cventilllll)' remole
A!,'flOSit), uphu..>i:t.. ikcr~lscd
cumpreherJSion. rcpt:tition. sp~ch: e~hn!alia_ palilalia
VHriubl;:
V ~cuuu:<lblmul
Variablt!
Delirium
Ac-utt: !hours · .tays)
1-luctuuring, r.:wrsible High mor~iclity/Rrortllluy in vecy •>Ill
Flu~:tuming t.llv<::r :!<f hours) ·.\:
Dt::cru~st:<l {1\~l•ldi!ring. t.t!S,V <.listra.:tion)
hnfJ<tirl;J (usually .to time aud place), llw.:tuntes
Sev~:-r~ agilntionir·emnfution
Fluctuates bt;l'w<:-:~1 cxtr~'ITit!S
;\nx i<IIK irnntvle. llucruaring
F.luciuntiug pn:ccck:d by mood changes
Nightmarish mod puorl~ formcJ
i\ifarked ret-eut
Dy9nomin. dy !;grapniu. :_;p~c~;h : mrnbling, im:h::vant, mcoherent. subject cl~g(!!;
Visual i.'Ummon
A.:ule iiJn,s-;;. drug toxicit-y
Dem-essior\
Subacute
Varictblc
R!!<.'ln'l'ent. l~suulf)l r;!vcrsibk
Ntxmal
[rnJJ01'tuninL!. sci f-nurrn/ sui cidc .
Slowing
l:.i!rly rnQrniug """'k~ning
[),;;pressed, ~!;•hie
Ftuct.m1ting
Nihilistic. sorna.tic
~Recent \ . __ ____ ,..,..
};ot aftl:ctctl
l .ess common, uu<lit\)I'Y predoruino:tes
Sdf·d<!prl!ci.ltory

·.~ . · ...
DEMENTIA
Epidemiology pn:.valencc increases with age: I 0% in patients over 65 years; 25% in patiems over 85 pr,;valence is increased in people with Down syndrome and head trauma
• Alzheimer's dementia comprises> 50% of cases; .vascular causes comprise appm>Cimately 15% of case5
• 10% of dementia cases potentially curable DiagnoSi'Stfor Dementia of Alzheimer's Type) __ .. " "l , ''-· ··,•, - ::
development of !n.'!li.ip!i cpgiliiiv¢ deficits ma-nifested by bOth , , ._, ·-- • '.. r- " •
~t!Cll}(ll)' LmPJ!irment (impaired ability to learn new information or to recall previously learned information)
: .
one or more of the following cognitive disturbances --·c "ap"~ia (language distuabance)
ii. aPJMia (in_tpai~>! abjlity to carry ()Ut motor activities despite intact motor functiol•)
iii. a~ia (f!li!ure to rec!lgnize or identiJY objec!S despite iQ\J!Cl sense.!)' limctiot!)
iv. disturbance in executive function (i.e. PUmning, oq~aoil'ing, seq\!~_ocjng, 1 . abstract !ltink\f!g}
cognitive deficits significantly im.Q?-ir sociaVoc_c~pational fll1lctioning and are a significant decline from prior functioning .. co~rse ch~cte.rized by gr~u~fol)set 'and c9n~nuil]g ~ognitive decline cognitive deficits are not due to CNS conditions, sy~temic conditions, subslance-induced ~ondili.Q!l~ - · · . - . . . . .
deficits do not occur t:~~jusively during course of delirium disturbance is not better ac<ounted for by w10ther Axis I disorder (e.g. MOE, schizophrenia) ..
Subtypes with or withoutl>Chavioural disturbance (i.e. wandering, agitation) e~Ji-~!!iei:aiie or;;ru;~~~iiY~~- · ·-l~tc_ ~~ct: age of onsot.? Q5 y~ars·
~-~~t__<;_ommou Causes or Dementia _________ _
:·• Al~eiuterl dise~e Vnsc~!!l!" \!emeptiu Mul!!-infarct Difi\!~~- white .millltr disense (Bimwanger's) ~ '· · ... i: (. Alcoholism" P~tkii!s~·~;~ !li~~e . . • Druglmedtcatton mtoxtcano~n ______ _
Lt!ss Comwoo Causes of Dementia
Vitamin deticiencies ---~amiQ~ {_B 1) : Wemi~~·s encephalopathy'
-----.-------------il
·---
B., (pernicious anemia)" mco~i!liC a.cid (pellagra)" Endocrine and other organ failure Hypothyroidism• Adreriallnsiifficiency and Cushing's syndrome• Hypo- and _hYJ>Crparathyroidism• Renal failure' Li.v~i- fuiltire• Pulmonary failure' Ctiron"ic ififu:tions HIV N~urQn~philis• Papovavirus (progressive multifocall~oencephalopathy) \ Prign (Creutzfeldt-Jakob and GerstliiiUlii·Straus:der-Scheinker diseases) T.u~r~~:~tosjs, fungal, ~ pr!)tozoal" · · · - - · Whipple's disease• Head trauma and diffuse brain damage Dementia pu~1 ilistica Chronic subd ral hematoma• Post&llloxia Posteocep~alitis Normnl~press\are hydrocephalus• Neoplastic \ Prinuuy b~.i!'llwma? -Metasiatic braha tumor" P"&n.;,co~la:itic 11i~bic encephalitis Toxic disordQrs\ " Drug; medicatio~. and narcotic poisoning• Heavy metal into\ication" o~alysi~ d.C~e11.ti~ (l!!uiiiiilum)' . Orjlii!!!~JOt:CI!lS · \ l'~Y.\<Wlltric \_ DeP.f.~~~~on <£Seii~~-ementia)"_ j Schizop_br~pia' - .. · Conversion reaction• rieje~e~a_ii~~'dis~rilers Hwllington 's disease Pick's disease Dementia with Lewy bodies Progressive supranuclear palsy (Steel-Richardson syndrome) .Multisystem d~generat)on <~-Dntger syndrome) l!ered~~ii!S (some fo~) _. . .. _ t!_o!o.~_ne~«?n diseasc{illl)~t!ophic lateral sclerosis' (~LS); some forms) F!.C?.fl.!llt,emp~r:l\1 4elllen~~ _ · · · · · ··· ~~!li~!__b.~~~~~g_c;P.t<!Jllion IY!!l)!iP.I~ scle~().sis
~ ..... . '· ;._' . ---··· . 'v ,\ · ~ \C · v ·( "l ·... ,-~ .:: .. ~-- ...
. t <\.. -• -··--
1.,.., , ... _. -....... \, .. .:. ~ . ·~ · .. :-. . .:.
. ~ . ,: .. ._ .. \ . -. .1.... - · -~ . . .
. _.:_ - . l -...: : - -. ' . .. .
I L l '• • .
.... _
,..-- , __ _

\.
·,.._ ·
; ... .. ·.
Adult Down's syndrome with Alzheime(s ALS-Parkinson's-Demenlia complex of Guam Miscellaneous Sarco.idosisa Vasculitis• CADAS!Letc Acute intenuiuent porphyria•· Recurrent nonconvulsive.s.::iz:ures• Additional conditions in children or adolescents Hallcrvorden-Spalz disease Subacute sclerosing panencephalitis · S .. ·. ;
Metabolic disorders (e.g., Wils.nn's and !-t:!g!1's diseases, leukodystrophies, lipid storage dist;~es. mitochondrial mutations) ·
"Potentially reversible dementia.
Investigations (rule out reversible causes) • standard work-up plus • ~ i~i~a~: TSH, VDRL, B 12, folic acid, albumin, SPECT CT head in dementia • i~dications for CT ..brutd: as above in Delirium section plus: ~e<" 6o~ 'iap,if! .~nset
(unexplained decline in · . ·- ·· · -- - -- -cognition of function over l-2 months), d_~menlili ()f rela.tiv~ly_ short duration ( < 2 years), recent significant he.ad trauma. unexplaiq~d l!~!lcoJogical SY.mP.l!lf!lS (new onset of severe
~ '-' headache/seizures) Management
• treat medical problems and prevent others . ' '. ·. provide orien,atioo cues (e.g, clock, calendar)
• provide education an~ ~up~~·ror patient and family (day programs, respite care, suppon groups, home care)
• consider l011g term care plan (nursing home) and power ofartomey/living will • infonn Ministry ofTransponation about patient's i!,l!!~i!i.!}:'~~. ~~i~~-~a~y
consider pharmacologicalthempy. . . .. low-dose neuroleptics (haloperidol) and an~~ep~e.ssants (if behavioural or emotiomil symptoms promineaii); stan low and go s'low
·anti-cholinesterase inhibitors (e.g. donepezil (Aricept)) some evidence supports-~ E. NSAlDS, estrogen (controversial) reassess P~rlllacological 1herapy every ~ths
. ,., __
· .. ....
·. '
:\l_. ... .
I '-
'"\~ .,., I f.~ ,,: .
I'
; ~ ....... ;.. ' \,. ....... . .
. I !;'(
\ -·
\ .. : ·. '·
• ~~ ; , 1
: · ' It . _. , '<" ' ·::·:· :.
~. ~ I I . ,, ..
........
.. -_ ~ ...
\~ l '·- " - ~ • '\ • • : '•.

.:.)- . _, .
~~_!I~~~~.- an idiopathic. ~e~enerativc CNS disa.der
CUNlCAL PROBLEM: ~Aitli.ll'lS()NlSMS!l'ARK.JNSONS DISEASE
I s•y this becaus•: Triad ofbn!dykinesia, tremor(pill roll) and rigidity(cogweellleadpipe). +: Hx: '-- · · · - _.,__ -- -- ;,..---- ·. ·. - · ·
~l~wly pro&~i'lr:: lnsidious OllSet ~~we~ ~p.-10 yen,rs
Vascular JIU(kinson"~ ~~:M.~!!!~~: l9l4 Ou epidemic (cnc::ephatiris lctbargica .. Awatkenins5")
~boli~: Wilson's . t-.. ·•,;_
~ toss of dopamincrgic 11isrost,iatal '!~.~~in substantia.n.igra'sz.ona compacta dQ'V4minc ~~urons dcgc.ncrato, up~~~i~a !!0~ balance bctwU!' dopaminerslc inhibitlon. ~ e~ol&nergic . . ucillllion ofsuiatnl ou1pu1 (GAllA) neurons. resulls in rclalivo acetylcholine (ACh) execS! . .. '>• lossorli;,.,ron~ in multiple other sclcclod areas , . res~ It is rd»live incrca5e in OABAtfgic output from striatum ' ·..:.. "' "' ·• · L~wy ~o~!!-:1 {~~~op,hl'_ic jnli~·c'Uial inclusion granules)
• l no I spcctfic to rD Iru!msnl - · .. . . ;~ ~ p_g~;t,mine precursor (Levodopa + Carbidopalb~nscrazidc)- more cffcctivt form~"'' compared to
- aaonists. bul have more other ffi010f compltcaUons. ~Include: • MoiQr fluctul!iool wb111 !!<;cr~~d levels (mcrcase PO sympwmslfrCOZing) Dru_g induced dy•kinesias (dystonia, olcathisia, chorea, moclonus) . . NN
1 po~tu~aJ hypolenslo~ c~~ac anh~ins. cn~na (de~c~d prolactm~ mcrcased OH)~
psycluotric (vivid dreams, agtlallon, paran••a. confuston, halluctnalloll$) · - · -?!,in)r.fui.ielf!'a!fti~!llf..din!~~ "'.l!ff in~J~JGry "!OY<Ine/liS ... . ..). .
Do~ne a,aqlili!J (Pramipexolc, -!l~l!i!!l!!!W -loss cffectivclhWI above butlm motor SJE. SIB: ....__ - ""s'Dmnole:nce; slcc_p •episodes' Nom-- - · · ·
'---
OriiwstDtic hypotension, syncope Ni~~lm~es. hal~uc:inations
':. T/;uU.:. FIUn! a~1~tr ~~r .'Mn.Jfodl us~.:;> !:...~b .... .G..l.l. -:.~ ... ~ J;.....Jj:ui · lncrease release of e!!flm.t,¢.00\1$.Qa.w,rnJro.t: l~~"i) · · -Inhibition o£.~_{Entacapone)- ~C:d~~! ·~_ff-t!me" OQ l~odo~ UC3Un:nl
Inhibition of~.(Selcgilinc:. Rasagilioc)- used for~~~ SJ~omauc rcli~fpnor 10 dop.u"'.tlncta·.: R.-. -reduces •off·timc• on lc~odopa lreatmcnt
Drugs offccling ~c ch~lincrgic _system (Bcnzhexol, ~~nztropin~)- fi~ line f~~ lrt~~ng padcinsoniw uus_ed by ~scnllal antt~chohc '.rca~l!ftl
Clinical Pearl In Parkinson's disease, poJiurtl/ inJIDbility generoUy apprars later In the colllse of the disuue. If .PEt~ ~~~'.E.~~~~'l .~c~ -~'!:t:ller ~if!..er'f'l!~n:-.~~~ll!! ~~~&nMU e.g. P~r~~~~l~·-~as~tar.!'!.rki~'!.'s.
What to tell !he pa.tieo1·
~~~'[~~ o.cre arc drlW.~!i_l~le butlhese drugs ~.1.!'~'!~. ~i~~·f!'~cts . We will try to find a drug or combtnatioa of drugs that best suits you as an individual. r.!J!S!'.~I~ !!·~~~ pn the AP' of o~ I[ OY'1'Pioms •"!'l in mi~dl·J!fe. tlu: d~~ ~~!!!Jiy ~l~w.)y progressive and.6~~!y 19 '!!lort~ lifospaa because of !!<?m_plicatio.is of i<TI!i>~!>iti!Y and ~odency to full Onset after 1!!. is unlikely to shollen lifo or become severe. Family nicmlicrs should be ~y~d and.uaincd in caring for such a pe.ticnL Suppon groups are available.
\YDicUt'!'. (ps~o) p,rkjpsooism · • pa.rkinson•a-likc stat«: d~u_: ~~ .m_uJtipl~ slf~k~
imaging usually •l•J!I!'.I. I!M~I Jllll8liA iJII:IIIIGe or \llhil.~ m~r l'iwtg~ Swcnlliy occurs in e~; liOoociated with ~Y~!!!!i.!'!J. often have signs and symptoms of farlcinson's below lhe ~st (~hart stepped pit. '!)1111 hcsilalion, freezing, po•illflll i.....U.ili•y) but relative sp~.O!!.II.il!!rotlhc.~aist (oormal voice and feo>lal expression, abscnco ol resllrcmor and bradykinesio) P.OO! r05po~ !Q J.-..'!.2!!! pallenb with true PD mily abo have cc:rc~rovuo~lw di~r.ase in addition their "D
o!·:, Cf/MR.I helpful in distinguishing v.Scular park.insonsim from' bUe PO
.::rasclli i1 us" msoaQ!iRa.l • ~~~!!iv~ ~ul!..~uc;!~ ~~!Y (PSP)(Stotelc, RK:hanlsol\ Olsz.ewaki SyndrOdlc)
~c o£ onsc~ SO to 10 ycar:a •
onset eharacterized by dif!l:u!!f i~ b.'!!""""• ~ll!PI.f~ll~ •. ocular dinurbaaccs, slurred speech, d(:ijl~~a, ·~~· ~"'1n.aliry chan&cs. dop~enion, ~·~-f~_!a! ~PR>SiDf! may take years for cltaractcristic syndrome to fully develop
s~pranucl~ ophlhalmoplegia- abnormality of vertical aau (if eyet ""'fixaled 011 a taraet .. d neck is flexed and extended, full ot 8 movemants can be obtained') ~~<!_o~u_l..bf.l!:.~~ - ~spastic weakness ot Jilwynaeal museulature, ~~l"~cd '!Je'7'h. mouth held ~pea. •W!I~oll(ins ~!ff\cull!.~ ~Wra.J~d jow JC<~ !Xial dy1to~ia. ~~ 5Ji£f~ina-and extension 'otth• nee~ (conuas.t to 'o.rll;i~ll'' wl,f:~ ncok.is Qcxcd) affected neurons in t~!UUP.S~ t~....!!!:!!-us, ~so.nslia. and pui~aqucductu.l grey patltology: . .w:uiofit>tillili'Y ' IMSI<~ (like in Alzheimer's) L-dopa not "Cry effective in FSP
~~ ~thln.l-h•!"s. . may have prominent dementia or nonnal cosmlion
Multiple System Atrophy includes striatonigral degeneration, •poradic olivoponroc:..ebellar atrophy, Shy-Drager Syndrome PNkiluoni.a.n. fcatufCS carty dysautonomia (orthostatic hypotension, impotence, bladder dysfuntlion, mouled cold hands) other fcatwcs arc c:crebclla.r dyfunClion, pyramidal Uilel sisns, stimulus sensitive myoclonus of hands and feet, extreme forward ncu:k ne~iun~ inspiratory Jtfidor, dysarthria

·ILEPSY i
CLIN fCAL PROBLEM: Recurrent seizures/epilepsy (give extra detail e.g. TLE if clear from hx/examination) . ._ -· .. --·----·--" .
nv this because:
!.ffi .. . ag.e:- of onset: primary generalized seizures rarely begin <} or > 20 r.ears of age
• .pre~itlli'<ilits; sle~p. deprivation, ~g~, EtQH, TV screen, emotional upset, inf~?~ti.ons etc. • presence ofaur&: implies. focal onset • patient's responsiveness"clur1iig attack • nature of neurololtical features suggests location of focus
lllQW = 'ffi)mal lobe ~ visuall~'?.ry/gustatory halluC~JlS =!f~I!:lE<irallobe .. \
• salivation, cyanosis, tongue !>itin8, incontinence • Ja:cKsOfuan:-mru-c1i} O[l~ b~dy part is initially affected, fo~e~J:>y_ spread to other areas
(e.g. fingers to hands to arm to face) • adversive: head or eyes are turned forcibly to the contralateral frontal eye field • ~utomatisms: patE~~-o~_!'.ep~t.itiye activitie~ that look purposeful, (e.g. ch.ew~g, walking, lip-~rn.a.~~g) • temporal lobe epilepsy: unilateral posturing, behavioral disturbances, automatisms, olfacto~ gustatory
hallucinatons '-o....---v, _.,,_,_._ ··- ·,_ .. _.· - .... . _ --- · --· -- · •
• post.:ic~l1£9ms- limb pains, tongue sor~ness, head~che, drowsiness, To~cl's p_~s (hemiparesis) • duration: ic.~. i~- s~?~ (seconds- minutes), P._<?st-ictus can be long (mix)u~g.!!£>) • family history of seizures • Rast histo_ry of ne~logical insult: birth: injtJry, ht;l~d tr~uma, stroke, C~S . infection, drug use/abuse • f~.riJ: febrile seiz.m-es affec\ ~%\of children between 3 months and 5 yea~s of ag~·. • benign if brief solitary, generalized tonic clonic la:;!!E-~-~s _t~~ _ J .? minute_s and n_ot _El.Or~_ ~eq11ent than
oiic:~~4 ho_grs · . · 0/E:
• pulse (especially rhythm), BP, heat!_~~~l!~tation Co~E.~~~-,netE".I?J9gi.91!J ~Je.am~ation (CN, motor, reflexes, tone, sensory, coordination, mini mental exam)
· ab§~P..i2~ sei~res can be Erecipi!ated by hyperventilation: have patient take up to l 00 deep breaths and .. ,
watch for a brief, transient cessation of activity and tglas~y stare;• · • ..
asymmetry of fingernail, toe, and limb size (clue to early d-~~ge of contralateral hemisphere) arteriovenui malf~m~tions (AVM's) may present as focal seizures:
• auscultate for .~ (carotid, orbital, cranial, spinal), yi~u~J tields, optic fundi
• head exam for evidence of trauma (look, then feel)
• ;kir;· exam: look for characteristic lesions of neurocutaneous syndromes (neurofibromatosis (NF);· tuberous sclerosis complex, Sturge-Weber syndrom.e) ~--·-"'- \\\:y~\ \I ,, ':.:.-:~, -· c' .. \ !.<. ~
Reconunended S/I: Adjust according to most likely causes (from hx and examination) • ~: FBC, UKE, LFT, CMP • CXR. ECG • EEG( • CT!MRI (Ix: ad:~~ onset, focal (eatures, EEG shows focal origin, poor seizure control) • !:£infective/inflammatory markers, specific tests for ~yPhilis, mv, collagen diseases
. (_._\;" ~> ~ iT-l..I(-~\J-::.-__,_ Etiology:
• a_eneraliz~d · • idiq~fuiE (family history in up to 40% of cases)
diffuse cerebral damage (encephalitis, anoxia, s!.Qr~IDL-gi§~a~~s) inflammatory (MS-uncommon: st.E:.) · ·--·-metabQ!ic (hypocalcemia, hypoglycemia, hyponatremia, porphyria, hypoxia, renal failure, hepatic _failure)
l(.::..:v ·•· .:~. : .._
.,
l l i !
l ' ::

d~ (EtOH withdrawal, TCAs, MAO Is, neuroleptics, cocaine, amphetamineU_
• Antimalarials (chloroquine, mefloquine) • Radiographic contrast agents
• Antimicrobials/antivi:r.!Us • Theophylline
• -lactam and related compounds • Sedative-hypnotic drug withdrawal .. Quinolones
_: / . a Alcohol
• Acyclovir .. • Barbiturates (short-acting)
• Isoniazid • Benzodiazepines (short-acting)
• c::ianciclovir • Drugs of abuse
• Anesthetics and analgesics • Amphetamine
• Local anesthetics • Cocaine
• Dietary supplements • Phencyclidine 0 Antidepressants • Methylphenidate
• Antipsychotics • Flumazenila
• Lithium
• partial (focal) cerebral trauma birth iniWY vascular (cerebral hemorrhage, cortical infarcts, AVM, cavernoma)· ce;:eb;'l tumours infections (meningitis, encephalitis; cerebr~ abscess, subdural empyema, syphilis, TB, HIV, cys~[c~rcosi~) - ---· ·--
inflaxnmatiqn (sarcoidosis, SLE, vasculitis) Genetic: tuberous sclerosis, neurofibromatosis, von Hippel-Lindau .....--... # · ... _ - • • •
Types of seizures: . · ·- --~ -·-Tonic clonic seizures (may have aura, usually not evident from hx as LOC from generalized seizure causes
retrogr_~de amnesia for immediately preceding events. Pt becomes ~d, LOC, fal!s +/- injury, resp_ ~~sted with cya~l§. rigi_d_!_ty _I~~axt;:s, +/-_ cl9nlc js;,rks/ flaccid coma for several minutes, may have urinary inco.~t!~ence or t~ngu~~~g_. ~e~!!l.~ CO!l$1!io~e<ss~ confusion, headache, sleepy, mu~cle p~ms. etc.)
• Complex partial seizures (May have altered L09 without falling down ''blac~out''. May have automatisms eg smacking lips, picking at clothes. Usually a...;ses from t~wporal IQbe, rarely frontal lobe. R!!gain5. ·- · -consciousness feeling muddled and drowsy. Before attack patient may have alterations in mood, deja vu, jarnais vu (feeling of unreality); comph:ix.hallw::;~ati9~ ofsou~d. smt:U. taste, vision, emotional changes, visceral sensations. If these alterations occur without subsequent seizure = simple partial seizure. Complex partial seizures from ant part of frontal lobe may produce bizarre behaviour such as incoherent screaming, ill-directed motor activity, usuallyabrupt onset, short nature and occurrence during sleep may help diffrrentiate such attacks from psychogenic attacks.
• Absence seiZ!Jres (minor seizure, resembles complex partial, generalized in absence seizure of childhood"petit mjJ". Petit mal always starts in childhood and the attacks are usually briefer and very much more frequent than complex partial seizures, not associated with post-ictal confusion. Caused by generalised discharge that does not spread out of the hemispheres and so does not cause loss of posture)
• Atoni_~ (brief lqss of muse!~ tqne, heavy falls, +/- LOC, only occurs in association with other seizures. Should not be considered in the diff of collapsed pt in pt without known epilepsy.) ':'-*< ·
• Partial motor (epileptic activity arising in the pr~~~~nt;!al gyrus, affects contralateral face, arm, trunk or leg. Characterized by rhythmical jerking or sustained spasm of the affected parts. May remain localized or may spread "J~an epilepsy", lasting from a few seconds to a few hours. May get Todds p~esis.)
• ~artial sensorv (Arises in sensoiy __ ~Qj1ex- unpleasant tingling/electric sensation- Jacksonian march: spreading (in seconds) of above mentioned sensations over body)
• Versive (forced deviation of eyes/turning of head to opposite side- often becomes generalised TC) • Partial visual (occipital epileptic foci causing simple visual hallucinations e.g. balls of light/patterns of
colour) -Formal visual hallucinations of faces or scenes arise more anteriorly in the temporal lobes ...
i j
'·

ypes' of epilepsy: ·-; · Primary generalised epilepsy ( qQ.!!et. childhoodladolescenqe, no structural c~us~) • ~e~()_pq_!ry_g~~~~c!~:pgespy _(onset adulthood, structural cause) • P.~~l_epJ!e.R~Y (usually due to ~2_c~J5er~qral pathology)
Differential ~ia~osis: • (.~ sjpcope_.)
• causes: n~Lur()ge,oic..vasodepre.ssor and vasovagal reaction SYQlR~fu~ic p~()J,g~ ~y~tem (SNS) failure decre~ed cardiac output (CO) or inadequate intravasc'!~!l!: yoLu.me o~ers -(e:g. hypoXi~ anemia)
• . __ NOTE: _sll!cop~may igd~~e a seizure - this is not epilepsy o ;· j>seudosefitfre;.. .
' can be impossible to differentiate without EEG often occur in conjunction with epilepsy history of sexua~e'~-~~ patterned after witnessed seizure (i.e. health care worker, sibling or friend with seizures) see Table 5
-----:-----.. • (narcolepsy (cataplexy) • pi~ associated with_~ensory_qr:_tp.otor SY.ID.PtE_z_ns or vertebrobasilar migraine • (~ h~erventilation, panic attacks • .. BjPSI~sc~~~ attack- · • ( ~ycem.ia ) • (~~tbiomoc~~)
Table4 Se'·
C1ml'acteristic
Time of onset
Pos:iti.on
Onset
Aura
Colo~u·
Autonomic features
Duration
Urinmy incontinence
Disorientarion. ~.;;t;Ictal
~lotor m:tivil'y
Injury
Automat isms
E.EG
Seizure
Day or nig!tt
AnY ..,__
$udden or brief aura
lPoss ibi~~si.fuuwta> . ~g.rmal or (..:yano_tJc(ronic-douk)
Wnco!l~J).t()_!!_ _m.tts.ide of ictus
Brief ~>r prolopgcd
C~p..!!!Q11
Can occur with. tonic-donie. CQtl:JD~KpHrtlnt·--- --. -- - .
·.Gafl __ ~cctu•· ,
(0;_~;n· c:rq <'~!:~!'-".\\:it h. absence qr t;QmpJex P<lf.ti;-.u F teqtt~n~_abnormaL may oo.normal
S 11c e
Rare
Rare
Occasional brief tonl~ se!itrre (x donie jerk$
(R_.i;e·-..
Nt[!,G
Norma]
.<'f -

Table 5. Seizures versus Pseudoseizures (non-epileptic "seizures")
Clmracrerhiic
Trigger$ Duration
Motor acti viry
Timing
\ ' \ ...!_. ..; ...... . ...
Physii..·al iqjury
Utina1'Y lnconr1netK'e
Rcpr•odn(.'.lion of attack
EEG
Management:
Psendosei.zure
~t.'Oill!OOll in lne elderly - -- -, <.. I
~ntgtipn;,[ c(jsturfvnlee \ ;:;...; f-.:1 .. .... < '- ' -- '" '\..: ..... : _1.:
],'fay be prolonged (
Suggestion abovo;: or stimuli plus suggestion
nonnal id:·,u and post-k:tal patlem:;
E ile ic Seizure
r.~~~ Uncommon Brief
Autolnatisms. in complex Partial scizun::s. St~eot_yp.ic Synchronous mov<!rnents
Day or night
May occur.
~ -Spontaneous
Inter· ictal disduug.e~ th:quent
Table 6. fndicntions and Important Sidc~Effccts..ofMajm Antiepileptic Drugs
Drug lndiC"'..ttion
Parti,-u qr gr;m·ra!i~d I.QlllC·clQnlC SCU'lJrC:S
All :;ent~raJjzcd seizr m~s iJf purtial seizures
.. --- - ~ - -·- . __ .,.-- ... , r -i , Ab5ence sci:1.ures ~ 1-. . .,.:,;.~=~= ----·- ------ · ·
M:tjor SiJt::-Eflects _ Dpse-Rdated - luios,:ncrmic
D!pl~pia Omrnt:ss lleadaeh~ Nausea Drov .. -sint)SS Neutropt.:nia Hyponatremia
Nyst:;Jgmus :\taxta Nausea V~lm!ting, ____ ______ _
rbnngr.:a!}lyperpla.•mi--cpre~ton
Drow-;mc~s Pantdo:-:ical i in seizure:; Megaloblastic anemia
Tremor Wl;!idtt l:!'ain Dysp~ps1a Nausea Vomiting, {Alup~cia -'· -Penpt~~::ral -edema
Naw;ea Arton:~ia Vomitincr Adtatiog Dt-;owsincss Hl!aduc::he Lethargy
...... \::.. .--:.:!2:
(
I (_

• Pllarm.a~9!o.~al begin with ~me ~~jor anti~~!.lYll~!lJlt with as~pl_~_~osage schedule (see Table 6) ad)_!-!St d~~ to achieve-plasma level in low therapeutic riiiige- · ··· · · · · · if no seizure control, increase dose until maximum safe dose or side-effects become intolerable
1 if'ffo ·seizure CODtrOJ, cfuiil~~§~Con9.drug, !flen_ ~~-~_g before us.fng combinations! . c!g~~pam.: mostly used tor .r~!fE-9J9n' myoclonic seizures adjunctive therapy: gabapen~ (Neurontin), vi~batrin (Sabril),l~l!lQt;rigill§ (Lamictal) Withdrawel of drugs: C9!l.~kler.wt2.-4 yrsseizure free, slowly over 6·12 months.
• c surgi~h- . 11-.._,B - ·- ·· ·- · ·· · ---~ for ss:lected ~~~s Q(complex.p<!rtial epilepSy with an identifiable focus
-· ----· · ··- ..•. -----, ( What to teU the patient: \
··- ·- ·" -- -... .. ....... . ~ . ... ~·
• psychosoc.@l e_dl!Eate g_ati~g.ts_and family advise about_s~~jng, ~g, locked bathrooms, operating dangerous machinery, climbing heights, chewing gum pr~~Wic:Y i"s~1,es: counseling and monitoring blood levels closely, teratogenicity of antiepileptic drugs,fot~e~4:-_§_mglday for 3 months prior to conception (throughout child-bearing years)
• inform ofprohi!>ition to_~ye_~..?._ requirements to notify government .support groups,_Epilepsy Associatfoli\ follow-up visits to ensure_c;:.Qmpliance; evaluate changes in symptoms/seizure type (re-investigate) Prognosis: In_20 years: ~Q% seizure free without drugs, 20% seizure free for past 5 years but still on durgs, 30% continued seizures with optimal therapy 4Q_ fold increase 1!1 ~udd~~- l!.n.~xp_!aiz!ed death in patients with epilepsy! l!!
-- -----

---------\? -z ; STATUS EPILEPTICUS ~ r .
) •. - \ ~')... ~ .: '--·,,_·-'-~\'~ t:.:./l ·~~-.:> " ~l ~\.~ ... \.. ,; > t ;. c~-·~\,\.:. ( '-' '-' ~ · ' ,._
• life-threatening state ( 5-l OO(o ) with either a continuous sei~es lastin minutes _ · .
·ora~ occurring with,pg~ the Qatientregaining full consciousness between attacks - '"'-2. '- ·
• risks: rep~itiye grand mal seizures impair v~ntilation, resulting in anoxi~ cerebral ,- .~ . ~-
~ 1schemra
7 ;~"~nr::~==~~ :::~~ ".~,~tr·c::~,:::::d,::,~;~::~o~~·~::=: I· 1HHABCs~ ;:·') ...:...._."'-·L·~.c:.:A.\J-.'-"~) 'h_.._:..._ .. _,..\ly <·· - - ... ,·.c·rc. · 1· 1 c~-~-- -.,\,-.. t - ~\i.J:-·,, , · .,J.·r -\. < t~ \.:"•·· " · \ <..
1 - - - - : ,., .. . ., < :r . . .·:- .. .. . \; c: \. . . .... : . .\
Q move patient away from danger (fire, water, machinery, furniture) • · lateral ~emi-prone position, mandible pushed forward; o use ru:opflaryngeal/endotracheal tube with high-flow oxygen • monitor RR, HR, BP and temperature
General: • · Secure IV line • Bloods (glucose, UKE, CMP, LFT, extra sample for drug levels)
Interrupt(~~-\ • give 5_0 ml.~O.% glu_cp.se IV and thj~~ 100 mg 1M .. .... -o
•
. ' \ :'\
• .!£.uzepall}-IV 2-4 Iii~CO._OS m~g) or ~-~~~-~.9II1g:~v(pr_ (repeat once after Ijmin) set up IV infusion of phenytoin (~5~-~~~g loading dose with maintenance started 12 hour~ later); ~ (: ''-''_l.\, .. " · v,~ ... u..:·. << ·. -.. .. \,q ... . } L\.c.~ 7. <;c: ,..._.__~J~~tl _ momtor BP and ECG dunng mfus10n ---D-74...114~\-t......v ....... ~ ~~ _ •
•
• phenobarbital if no response (watch for hypotension and respiratory depression) phenobarb iv infusion 15mg/kg at lOOmg/min general anesthesia in ICU (e.g. pentothal) if no response. to phenobarbital
monitor lyteS; gluco~e, urea, creatinine, lactate, myoglobin, blood gases, ECG midazolafu\<cttf.P''(ffl IctJ) or pentobarbital "coma" . . .
"')<.:> .:.· · ~ -... : ~"- \ \;',; c t":-- .- 1,< ·'.·
Assess the Cause ofthe Status • accucheck (rule outj!iyi:?ogyceinia)_1 · • draw metab~lic and drug screen (most common (EtOH)/ ~ • measure antiConvulsant levels - -,;-- ( ':.~ .._,..:;,}0 )' -~ ·
• CXR, EEG and consider stat CT or IviRI if first seizure or i_f focal neurological deficits elicited
I ' . !
I . I
! '·

1. illense(sub-cortical)/moderate(usually cortical) ~~<:gia (i11volv~g ... leg/~f:ice) on RJL. _Is speech alfecred'l (sugg.:sling dominant vs non-domtuanl kSton), l:bcs,c fiAAI~ llllUJigg.osb.vc:
of a~l )!IIJ;1Ul.d.alsoJike4cw!<>-<>Ut m<>-fullowing :.Juain..lwuar,<SUbdllt:aL1uwnaHIJ!18e, tu:oiiiijfiSces:~.~php,/jljf,~as, 'L~t:Jis, dem)'WnatiDn, 'llli§mins-auro,,
~io, antJ.C!JliWtSitut.di~ ' • • • 2. Anato..UClllluution appears to bem the coltlcal regton m e.g. Left MCA I say this because
ru>u allccted more than leg. Options .. ,
~l \ '~ "s,.:_.:-~ "-;,\~c.:;,(:.O.::., -"'® rC"'e-r-,eb-ra}~art-c-ry-cb;-r-at-lc7b_o_cc'·l-us-:-io-n.s-·7(11S:-::.:-::ua-;U.-r'S--;;-:2\---~~...,.!'-' ' ··• 1-./~ • MCA: arm>le , ACA: le >ann
~\52_
((SP'-il~
Lacuner infarctions (usually DMihYJICt1sa~--"\/O.::: ., D.EEP C$£bral infarct, usually ~ width ~g intema\ caesulelbmwstem
• !>:ficro-MI~IjosdggsisAipohyalino•is . . . Dsnsl: motor nemtplc!l'alhemillypoaesthesla. May have dysartluia, tlomolateral ataxia with crossed arcsis
Internal carotid artery territro • Clinical picturolikc MCA. ACA, iutcrnal capsule
Lateral slriale artc.rY: hemisensocy, hemiplegia. halll0oomoll5 hemianopia Carotid TIA: usually atherolarteriosclcrosis at origin1lfiutemal wotid artery(stenosis) wilh micro-ctnl>oli. Tr~atw I , ,
V enebro-basilar area • Bilatera wealolesslclumsiness(may be unilateral or shifting) • - e111l binocular visual defects • 2 or more of:' 1/enigo, diplopi~ dysphagia, atu.ia • -siir not ~b~neficial.
), l~I.IM 1!~~1111:3'- is due to an iufaml~/bacmD!Dg_<;{llli). Motivate: dislribulion,:~evcrity etc). Mo~lty you won't be able to telL Qecreased·GCS;.Nl'l.aiuib&a!lilc!l;
r--1 - \...:'reeS\:iuiU>;c.:. :-. t-l - \--\e'O'I'-.1,-\-e.D~ ~\'"'\
$1!!J!CSI,bacmg!l!§r. -- --4. Actiological dlll.wllinpresent in this patient.. also addolhers you looked for!!!
111.\lllrilllldifiable: -Agc:~gawlerl-ifiua hx,&WII..l~l~Sldllatl.u<. , . ,
r-\ ~ 1-'rfce.:cv::::.c ¢""'' ~' \-lc,lr
H - \-CPJ s.
ModifiabJj: Hypertension, heart lesions (AF), DM, Alcohol, Smoking, coc, bypervtscustty
sylldromcs,~iucrc cd htt etc. . , , , , Conimeoto : paticnt,~nruf~~Wmk polclltial'l . .
.::; . ..;. 'l'.f'u L.•J"'\ ·\ . }\-\ c &'6 r
-c.oc..
Spcciatinv..Ugatioll·to<nntin11·dx: ~~at. MRI better but not cost cCfeclivc,
Mx:
) . \);-.;\
ABC according to A'fl-S Only lhrombolyse if SlfOke <3hours ago and nllt suggestive of baemorrage! A-Antiplatclet (Aspirin NB) A-Auticoagulaot (EBM: Avoid heparin, no dear benefit but incre~es risk for haemorrhage B-BP (only after I w""k. not in thc.aclllC ~base) .,_? '? flO'{ B-BP (very important. Treating !OOOpts for I year preveots'"'l2 strokes!) C·Carotid endarterectomy (ifindicalc:d)
0)~ ~ ~o.-'1: LS ~Wl. c\t.s...~ca...\ \7\~ ~ S\::\o\(.~
• i'lelireased-LQC,
• ·~todetioils
• -Hcmiation • Splli:ps.y
Lastly, explain this to the patient,.,
• ~lSll>S •. illlml • -~..Ilia • Qm~ ··~etc.
• Oooslipati011 • ·~PJc:W.QJI:·
S.\u.i d ~·\00-c) =:
'Ju.._\~j.t., . c.~~·~
• Y au had a stroke, to prevent further attlleks we need to treat the: abOve mentioned factors. The magnitude of the deficit will most likely improve as brain swelling recovm. May however bleed into area wid• increased deflcit (rarG), Rehabilitation is imponant to recover some indcpendcacc etc.
NB: If you get a patient witb DVf and stroke, what was frrst?'l? • DVT caused stroke (must have ASD etc,) • Slrokc caused DVT (immobiUty) • Increased tendency In clot may cause both
What if the patient is very youug'l'l • Cardiac emboli (ECHO) • Premature atherosclerosis· • Anerial dissection
C: .... Thrombophilia (protein C, S and antithrombin 3 deficiency) l. Homocystinuria ~
Antipbospbolipid';llitibody syndrome
• SLE • Vasculitis (do ESR, CRP. ANCA !_anlineutrophil sytoelasmic antibod\'.l • CADASIL (cerehral autosomal dominant arterlopaiby with subcortical infarcts and ·
lcucpcnccphalopathy) (do MRI, genetic analysis, skin biopsy) • Mitochondrial cytopatby (do s-lactatl:, muscle biopsy) • Newovasmdar syphilis • Primary iulrliCCrebral haelllOrrbago (A VM, drug misuse, coagulopathy)
Subarachnoid hlicmorthage (Berry, A VM, vertebral dissection)
·.2) _A\1\o.\o...\J.lCa \ 0,~ l A.\,.Jc\lJEoi © -..,) ')~-.d_co.,/ -=: J...V\.Sod (;I. -0 ,1,, .. ,..'. I .,_... 1- '"'""" ·~< In \- +---•• ,-' '"" \._ 1' T'J\1; ~Sj '-= 'I\-·~'-'•-'•-'·U•I\J''V\~Q_ ._),;.. \1'-y'fe.\\UUUliU"-
'-"••' ___ ..... ....... ,_.;. ... _.:...,__,_.;. __ . ........ .
f..t._.> LL-<.'c 'is.o.ctciS. / AC,.~o\'=y'. ~ c_~
t:.) a:" fC<"~'J'.O"::O.'\ i c. Soct.ci.s.. , 7) f'-'-\i'-CJt{<Y"'-0..\ S-\:o..~
~) (ju-..\:.- Lit:l'c,Y.;; AA&t<.;Cc.b ol, ~::.v_,YSI'Or\ I •

llE.-\.DACJ;U:
Classification (HJS 200!)
• ~_'.!!!:!..!: primary headaches - vast majority of headaches are of this type; tlligrllin~. tepsiontype headache, cluster headache:
• PJll1.2: _secondary headaches -the headache is a symptom of underlying disease e.g. meniiigilis, SAH, ll:mpordl arteritis, increased ICP, tumour. abscess, substanc"c wilildnlWSI, psychiatric <li:iardcr, ENT problems et~:
• Part 3: Cranial neuralgias, central and primary facial, including trigeminal neuralgia. ~timmulus headach~ optic p.cur!lis. herpes ZQat~ indu.et:d headpain etc.
• when to be concerned? o New-ouset headache o • Different or more severe than any previous headache; o the worst headache ever o Suddeu onset (maximal at onset -no increase over min.} o lleaduche associated with o • Fever o • Meningeal irritation o • Projectile vomiting o • Altered level of consciousness o • Focal neurological symptoms or signs o • Recent head injury o • Optic disc edema
MIGRAINE Diagnositc criteria;
A At least 5 attac!U rulfilling criteria B-D B. Headache attaCk lasting 4-721ml!!s (untreated or unsuccessfully treated) c. Headache has at least 2 of the following charactenstlcs
• Unilaterallocation • rutsating quality • Moderate to severe pain • Agrivation by or cau~i(lg avoidance of !;OUtinc physical activity
D. During lhe headache at least I' oflhe following: • N and or vomiting ' • Photophobia and phonophobia
E. Not attributed to onothcr disorder Types:
• two main types • migraine without aura (common migraine)- 85%
migraine with aura (classical migraine) - 15% other types: childhood periodic syndromes, ritinal migraine etc.
Epidemiology • common: 17% of adult Canadian population • F:M-= 3:1, young> old • peak age 25-34 years
\ _ .
- -· - ·-· -· • familial6u%
\~igraine without A~.:J • pulsating or throbbing • typically unilateral, can be bilateral • gradual onset, lasts 2-72 hours (if untR>Dtcd or WlSUCces.sfully treated)
• interferes with activities of daily living and ability to work associated with nausea and vomiting
• may be associated with photo/phonophobia • worse with movement, straining, coughing. bending &iter, odors • better with rest, immobility, quiet, darkness, pressure 6n scalp, cold compress • may have dilated, inflamed extn~cranial vessels . • prodrome and post-headache phast-s with changes in n\ood. activity. appetite, polyuria,
autonomic symptoms
[Migraine With A";J · . • follows pattern of migraine without aura but is preceded or accompanted by aura lasting
10-30 minutes characterized by
transient focal neurological symptoms: visual (most common), sensory, motor, language, perception visual symptoms: fortification spectn (zig :zags), scintillating scotomata (spots), teichopsia (flashing light!l) correlates with vasoconstriction of intracranial vessels
~typical MigrainD . • migraine aura without headache • basilar migraine (usually young women, occipital headache, mimics vertcbrobasilllf
insufficiency . i.e. visual field defects, diplopia, vertigo, l!laxia, alterations in consciousness) herniplcgic/hemisc:nsory migraine (deficit may persist for hours) ophthalmoplegic migraine (rare. e.g. CN m palsy; rule out aneurysm)
• retinal migraine (monocular scotoma or blindness) migraine in childhood: recurrent abdominal pains, vomiting and motion sickness; recurrent sleepwalking
\!riggeriJ. . • stress and relaxauon • fatigue, sleep excess or deprivation • weather
medications: exogenous estrogen nnd nitroglycerin • bright light
hormonal factors (menstrUation, ovulation, pregnancy, menopause) dietary factors (fasting, caffeine withdrawal; tyramine (cheeses), nitrites (bacon, !ahuni),
-

Management Strategies non-pharmacologic: education (avoid triggers, stress management), relaxation training, biofeedback, cogilitivc behavioural therapy (CBT), hypnosis, accuputure pharmacologic (symptomatic rreannenr):
analgesia: NSAIDS, acetaminophen, summatriptan (lmmitrex), ergotamine derivatives - specialist usc only (avoid consecutive days, wait 24 hours after ergotamine) NSAJDS, acetaminophen, ergotamine often combined with each other and/or caffeine others (benzodiazepines, opioids, barbiturates) antiemetics (eg. metaclopramide) NB: Beware rebound HIA caused by long·tenn use of analgesics
When to use prophylactic treatment: : • 2 or more attacks per month causing disability for 3 or more days per month
Devastatingly severe attacks Attacks accompanied by neurological fall-out Chronic headache disorders If patient requests it
prophylllctic treatments beta blockers calcium channel blockers others (TCA, SSRI, cyproheptadine, methysurgide, phenelzine, valproate, NSAIDs, riboflavin lisinopril)
homeopathic remedies: some evidence for few admit if severe headache persisiS for longer than two days
TENSION-TYPE HEADACHE Diagnostic criteria:
A. Headache occurring Q~ 15 days per month on average for 3 months ( 180 days per year) and fulfilling criteria B-D -----
B. Headache I&Sts hours or may be continuous C. Headache has at least 2 of the following characteristics
• Bilaternllocation • Pressing/tightening quality (non-pulsating) • Mild or moderate intensity • Not aggravated by routine activity
D. Both of \he following: • No more than one of photophobia, phonophobia or mild nausea • Neither moderate or severe nausea nor vomiting
E. Not attributed to another disorder Epidemiology
very common (30%) f > M; onset before 40's
.;ounst.!!"£. ~ .th r~u~-~~ and e ..... ---~~ .... n removal of precipitants . physical methods (massage, heat, biof'eedback, relalaltion) non-narcotic analgesics (NSAIDs probably more effective tllan acetaminophen) prophylaxis - TCAs (imipramine, amitryptylline) +1- psychothe!llpy
CLUSTER HEADACHE Diagnostic criteria
A. At least 5 attacks fulfilling criteria B~D
B. Severe or very severe unilateral orbital, supraorbital and or temporal pain lasting 15-180 minutes if untreated , -
C. Headache is accompanied by at least 1 of the following • Ipsilateral conjunctival injection • Ipsilateral nasal congestion or rhinorhoea • Ipsilateral eyelid <Jedema • Ipsilateral forehead and facial sweating
Ipsilateral miosis and or ptosis • Sense of restlessness or agitation
D. Attacks have a frequency of one every other day to & per day E. Not attributed to another disorder
Epidemiology: • uncorrunon • M > F; middle-age, mean age of onset is 25 years of age, rarely family history
Other signs and symptoms
• treatment
abrupt onset, ~flen in early am (waking pqtient uo from sleep) alcohol may _precipitate no nauseii/vomltlng
prophylaxis with vempamil, mcthysergide (yoljng patient), li!hlum, predmsone · ' . · acute treatment with ergottun,!g.e. tryptans +/- 0 2 inhalation
MEDICATION-INDUCED HEAPACIIE signs and symptoms
• treatment
chronic daily/ncar daily headache having characteristics of both migraine and tension-type headaches , occuning in patients whO are chronic (over) users of analgesic medieatioo: _(vicious cycle of headache-> analgesic use-> headache)
outpatient: gradual tapering of overused medicine replacing it with a long acting NSAID, or, abruptly stop overused drug, substitute a uansitional medicine and then taper the transitional drug(e.g. NSAid, Diffi, steroids, triptans)
fnpatiem: Continuous IV DHE. Sodium '1/alproare therapy and metodoprem>Jc or IV neuroleptics and or conicosteroids
TRACfiON HEADAOIE pathophysiology
caused by an intracr.mial mass lesion (e.g. nunour, blood, pus) signs and symptoms .
mild and intermittent--> more severelpersistent~ Wllike previous headaches
• diagnosis
precipitated by head-low, Valsalva, lying ~\Nil, e.xertion • Wllr.i~WII.ffi. • constant in location or diffuse
accompanied by other neurological symptoms/signs tJ...,- lll1miting, pllpilledl:llla
requires imaging contrast CT or MR1
treatment - neurosurgery
MENINGEAL IRRITATION (Meningitis. Subarachnoid Hemorrhage) any sex .. o.ny age, wiy time
• signs and symptoms . • severe, generalized hea(!ache with ·nausealvomi\ing and pllorophobta
meningitis is maximal in hours to days, SAH is mnximal in seconds to minutes SAJI may have ' sentinel bleed": severe headache may be preceded by warning headache
• physical exam . • positive K.cltlig's sign(lroee extension with hip in flexion arrested due to
• diagnosis
pain) : . positive Brodzinski's sign (gentle, passive, forward neck tlex1on >S
arrested, while other head movements are normal) llU!Uingitis presents with symptoms/Sign$ of inft:etion, SAH may have a fever
non-contrast CT lumbar puncture with CSF studies ifCT negative (CT alone does not rule out SAH) or CT unavailable LP contraindicated if decreased LOC, papilledema, or focal neu10logtcal sig1is (see LP section)
·GIANT CEU ABTERJJS • RED FLAG- untreated can lead to blindness (20-25%)
inflammation of medium- and large-sized arteries, predominantly those originating from the aortic arch and the aorta itself
:---
• tjp!".;I.(~ !Xls..:.t:l'UX' t.:~~ ... ~~}0; ~ -'·.- ........... "':
Clinical F.::arurcs oveJ" 50 yeac; of age, more cornmJn m •.>.,:uaeli
• temporal headach~ and scalp tiOIIdeme.ss due to ii\IUnL-r.:.ttor. Oli ::-"" -·;:;..;.i,~ ..-.~ ~· the temporal or occipital arteries
• sudden, painless loss of vision. diplopia andJor permanent visual loss • due to narrowing of the ophthalmic.or posterior ciliaJY arteries • tongue and jaw claudication (pain in muscles of mastication on chP.Y.ing) • polymyalgia rheumatica (proximal myalgia, constitutional symptoms, elevated ESR)
occurs in 30% of patients qonic arch syndrome; involvement of subclavian. brachial branches of aorta result in pulseless disease, aortic aneucysm +/-rupture
Diagnosis • clinical suspicion, i~~~;reased ~R.. increased CRP, teJIIPQral iU1Cry biopsy, 1111giography
Treatment high dose prednilone 1 mgllcg in divided doses until symptoms resolve ~tjtiop~ 9r ~\ht.!tr~ if refia~tocy (not provell)
• highly effective in the trc:aunent of giant cell arteritis and in the prevention of blindness and other vascular complications
MENSTRUAL ASSOOATED MIGRAINE
• Acu~ treatment: NSAIDS, DHE. Triptans • Short teuu prophylaxis: NSAIDS, Brgoblmine, Methysergide, Triptans, Magnesium
COITAL AND EXERCISE INDUCED C£1'11Al.GIA • middle aged men • develop, sudden, severe headache at the climax of seXllal intercourse • no vomiting/neclc stiffuess
duration< 10-lSmin, dull hePdache may persist for some hours
Diagnosis • Do LP, CTIMRI to exclude subarnchnoid or other headaches
Management
• Treat- simple analgesics • Ptt:veot- prop(llllll]ollindomc:tacin ·
(I!_!
, .
...:NS U•.· ~-. WNS .!.__ ____ •• .
MENTNGITIS ~~nmation oftlte rnt11ingcs
Predi~plising FacJQrs · ·-·-~ systemic {especially respirat~ty) or eneninge~! {otitis media, odontogenic, sinu_sitis)
iiil"ectlons
• he~111~ ~atomicalmenim;ejll defects
• previous l!_eurosu · edurc~
• cal)~er, alco a tsm .an r unmung<l_~f!~~ states Etiology _ "'-
• b~cterin.l ~ .. t -.-......... neonates: E. coli. Group B Streptococclls, Listtria monocytogenes
infants and children: H. inj/uenzae, S. pneumoniae, N. meningicidis \-\ "'::.. 11--..) adolescents and !!!!!J!_s: ~ pneumoniae, N. menlngitidis elderly: S. pnewt~olliae, N. meningiridis • Grarn negatives C§~. !~~: ~, G!!!!i_~e.&_~~~ _ ·-inununocom!lfomj~ed: Listeria mono~ytogenes . \ ._;;,;;
• viral ("aseptic")·- · . -; Enteroviruses, H. il!lluenzae. HIV, HSV, Adenovirus
• fung!ll -·-- - ----..... - C!YJI!OC!)SCUS
• other Tappnem_q pa/lid11m (meningeal neurosyphillis) Bprre/la burgdor(eri (Lyme disease) 11!..
Signs and Symptoms . • peo!J!ltes aod children: fever, ~omittng, ~~~~. ~ritpbili!-Y1 and ,.e..oor feedm~ • older chi!dren and a~~~: !Wr· ~~~~~$,e. ~~.~.s.~~~.:.S~· c=!,'*·-~]s.~: and
vomiting, lethargy, .. • Oierui[gCat slgm"'(i.e. Kemig's, Brudzinski's)
.. ·;
other signs include alter~d le~el of_co!.).S£~1!,~ness, ~~lml\ (septic mi_croemboli), seiz~. focal neurQ!II&Cal,SJEJk CN pa~)i'-.
Diagnosis · • fBC + differential
"uKE for SIAfm'
.~.. . .. ~ . ~
• :\t;ra~s m1;J ~~icate ijrimary inf;flilln.~j~e (CXR, sinuses, mastoid bone) CSF eofilc (see Table 20) (l[!!_m slam: Cl!l!illf
• PCR +/-serology (viral) daCT. EEQ if fnc~li!r
Treatment • initial choice of antibiotics is empirical, based upon the patient's age and predisposing
factors -c\:;. :=-c.Cx?.;:- r \~'-·'~q, \..Jo~''--\~J-~; t-\'::n__GiocbJL
Jo. \'.j<:::,ck <::.\~-QS l\.Wl.~"" ~\1\.L,\j,(J~o..l Sc\ S .
~ 'S6.c:.i..JS;e::-, ~ LOC (b.:c-c.~'-~0..\ \OJ~" t;='oc.o.\ ~\W.i._~ ·-" / r . ..
<' IS ~ -
---e . .
~--. --- __ .:·A~-- ~ ---~- ~ iieowu.:s: ame_ic:!iin T .::e~oU.}t.-:-.= (~ CSF ~£...::3".:n ~ r-;:n-$-a.'; · · infants and chlla.ren: amptcllim ..;. Silt' ~,.,.,-.a -rep· -~:! adolescen!S and adu!IS:~illin, -elderly: I!S:nicillin + ampict tp ~ CSF leak: 9Win~•~lin + R'iDta5~n C
• rcportllblc to PulJhc"Healtl\ _ .
. CiRfli..FlJ~~~i~ns \ •.. ~ .-...>-.. .• ~""::»·/ <.X·· • ~c, seizures, cerebral edema, h droce alus, SlAP .. .:A_~......> · \ • rest . u· . ne~oio~i~t 9.;A~.1Jespectally c _ ~eatb 1
! ····
• ""Mortiiilit)ranaf.1orta!ity: S. pneumoniae : about25%~. meni11gilidis : 10%; H. injluenzae: S<yo - ·.-- · ........,_. -
• worse prognosis with ex.tremes of ase; delays in dia&nosi~d rreatmcnt; ~plicating illness; • -"Stiiji(i[ or coma; seizures; focal neurological signs
Prevention· - · · . , regular childhood immunization agains~ ll irifluenzae \
• vaccinate against N. meningitidis if traveling to endemic meningitic areas • . prophylactic;I£!.a.,l!!£in for household and close contacts ~r,g: infl..JI.em~d, ~
.. •. -N.meningttldismemngitis·affectedpatients . . -~~ \ C'"\\\.,. --·------.. ·---·· · ~~~r~~~r~~~: Table 20. CSl' l'rofil~ lbr CNS lnfct~io.u
;\pp;.."UfiUI:t'
GltM.:tt&r.:(Jll!ltUI!I.)
I'Hrt..:'ill(l!''l)
l:.:UC:1KW tt\:U !flrutn ')
llrc,tuu,iuun&(.'.t-11
Pll:s.<ll\!(mmHs)
ENCEPHALITIS Pathophysiology
r
NonnuJ llul.'b:riul
l.'"--ur t-.!Mnnlld.:_~!>'
~ o.:..-......t{J u.~-114S l ,..,.., ... ~"' L;I lm:t~.utiJ "t"
'-!'"~~ ~ t!X•lUU ~~~~~,1' "'-1tiuu1Llt't -
Vinri.ISn*lli., TIIJI'unpl o\,«pplc ....... ,Jl .. ~kis
Ntona'-111~~· ..
C.: I. ...I)·
Nmn:U~ tlt.:<:n:aL....-d~ - ~~ .@) lll<rtlekl.l '1- lila-;.--...,.,"' htLh!u...:d ""
'"""'"""""""' '"'"""'-"" ~ In,.,..~~
l.z::tll·~..: l .l-'n•rlt0Cl1.:• ~ ·~
N!A ~ llh:.T\.""~~ WA
• .
• an acute m!!!P:ffiapuy rnwase O~the brain 4ue IO direct viral invasion or to hypersensUtVII)' mttlate y a viruS (foreign protein · common portals of viral entry into host include re ira to (mumps, measles. influen2ll), enteric (rabies, CMV, HIV). enito11rin tract en rovtruses). and venereal spread (HS\i,c'Mv,Iiiv)- ...
• other viruses reach CNS via peripheral nerVes (rabies, HS V)

--------------~
£1iology
• ·,viral (usual cause): ~V. ·~s. measles, rabies, arbovirus, HIV, poliovirus, CMV, vancella zoster " --- - - - . . -.---- . - -
• ~~cter}aJ, mycobacterial and spirochetal: ~yc,gema pneumoniae, syphilis, Li_steria, TB. tyj5fio1d fever VI=> - ~coo ....., .:c--
·~iiE,CJyptococcosis, histoj1lasmosis, candida, ~~is • _purasiti~: W~l)~~~is. !~~~m ~~~ ~ (cyst1cercosis)
. ockettsml: Rocl)' Mountaiil spott;;afevror wiclaSSifiea: CJD (prion) . . - -
Signs and Symptoms · acute~ illness, malaise, chills, nausea, vomit ins
• meningeul involvement: beadach;·siiffneck · • p!Uenchynlal disease: sei211res, mental status changes, focal neurological signs,
increasing ICP if a significant brain volume lsd;m;aged by the infectious process Diagnosis -
• typically is based on clinical pictUre • CSF can confmn inflammatory process
CSF profile (cell count and differential, glucose, protein), cultures, stains may help provide specitic diagnosis or limit possibilities
• serologic studies arc valuable in diagnosing encephalitis • CT/MRI!EEG to defmc anatomical substrata affected may show focus • brain tissue biopsy for cul!ur~, histolo~ical cxwuination, ultra structural study, and
iniffiunocytoehemisuy - · ··· · · · Treatment
• geneml sup£onive core plus measures directed against specific infecting agent • monitor~! trinqions carefitlly (BP, HR. respirations) • mainraiii"Outritional status (hyperalimentationlgastroscopy feeds) • reportableio Pu'biiC'n'ea'iih
Clinical Pearl • With meningitis_~~rebral ffiiictigii rema•i\1 i1iiiiijal • With encephalttiS, pahents often havet~Itetcd mental status (speech, movement).
. . . ~WF!:? r \.\,\\,\\.~1.1 (lre.~~-~~E~Iialltfs" . \ •; pailio ys1o ogy
o !!fJl!e,~fi~in~~»'j~Ui!if~ hef!Iorrhagic proces~ with lymphocrt:ic ~d priiSma ce reaclloo, uc t usulilly mvolvcs the~~
o ~il~ith ~but herpes encephalitis can also be caused by V~ricella sig~ar~;rc~~r~0s~5~e. on I {~\~"~-; ~\·e~f~E}.
0 headache, Stl nee ·1 VOmit~ heffij arEs(s anl! f0cai'07flen'era1!=?l!if Se!~~S .. 1 -· .... I • • -
o lt6fi! s•li!)'t"oTiem~orallo, ~ S target ~fu.ncl!q 1 cto a. ucma o , bcltavloral d1stur ance, co.:{ lex rt1al se1zure · · ·
0 usua y .ra 1 es . and may result in coma or death
,--
· """t . ~~.l*'e"#n• ... 11114i.>.'•, i:» *' . .;· - =e ·?;;, ... ...L..-... .: o conunon SP•-.uela.e in -·Fvfr''' 'l"-' ... - ~ - ~ .... ..rs a,r.a rr. ... TaJ~ - .. .:1 ~ .. l \'h)l!t o1 • r- .. ··-·
(teflecting limbic invo vemcnt) . o can present ~¥!pralep!I:JfW •l»'ii2Q. o may also cause ,l!.9J.jttnn;tl.\l.g~
• diagnosis o CTIMJU: medial telnporallobc necrosis o N!G: ~yJ~t ~!o..?.'!fi.li. pen0d1c discharges o ~!QQY- when diagnosis uncertain o -~fCSF for HSV DNA: for rnpid diagnosis
• treatment o JIV acyclov!~~ diagnosis .1:~~p;c~~~ \ \ ~
Arbovirus Ence balitis • ep1 emtc, sporadic, virus type by location (Eastern Equine is the worst, summer worst) • newly recognized in North America ,ws;r NUwjws • lJXsr;mgnaljt}'1~9_1;hit,lj!,V:~~g~ •.
signs and symptoms o rapid or coma with conyut;jms;jznm beydg-

·liROOPTHALMOLOGL
1 liS< >RDERS OF_LA'J:'ERAL (}AZE . • voluntary eye movements are triggered in the frontal eye fields, located anterior to the
precentral gyrus, bilaterally in frontal lobe _,;-
e each frontal eye field controls voluntary saccades to the contralateral side via connections 1o the contralateral paramedian ·pontine reticular fonnation (PPRF)
• a seizure involving a frontal eye field will cause eye deviation towards the opposite side 0 a unilateral lesion in one frontal eye field prevents voluntary saccades to the opposite
side, o eyes deviate toward the side of the lesion (may also occur with large parietal lobe lesion)
• can be overcome with doli's eye maneuver • in contrast, a unilateral lesion in the pons prevents voluntary saccades to the ipsilateral
side, -·--• eyes deviate away from the lesion (because the corticopontine pathways cross)
• cannot be overcome with doll's eye maneuver
nt il:al gaze palsy= lesi<;>ns in upper brainstem • common causes of lateral and vertical gaze palsies are brainstem i~r.~-~s, MS, tu~~~rs
·.r cmudear Opthalmoplegia (INO) . • results from a lesion in !!}~dial longitudinal fasciculus (MLF) which causes a ~sconjugate
gaze • MLF links CN VI in pons with CN.III in midbrain
• adduction of contraiateral eye is impaired but there is full excursion of abducting eye + nystagmus
• cannot be overcome by caloric testing • adducts normally with convergence
" frequently bilateral e up beating nystagmus on up gaze often present • usually indicates MS; but vascular disease, neoplasia, or Wernicke's encephalopathy may
be etiological factor · · ·
c )nt: and a Half Syndrome • lesion in MLF and PPRF • have an INO with inability to gaze toward side of lesion • ipsilateral eye immobile in horizontal plane and movement of contralateral eye restricted
to abduction

< WffC DISC OEDEMA
T;~blc ll. Causes of Optic Disc Edema
()th<:r \ ymptom:;
l'uril
hrudtL'>
Oplic Nenricis
• ~<tpidly P,r<!grC.'i:>iv.; los~ • ( entm[ VISI\ID 1<.1$$ · . / ·s .· • Acuitv aft(..'Cfcd . ,_ .. • lkcn:!'ased ~\)\nur visidh
• T e.utlcr gluhc. puinliJI <'n nwtion ··
• Artcritic (Si:l! llb'n"·ltrl1Q··a · ChaptCJ·) • Bilateral rarely in adults ~· • .Mav alternate in MS • Freqr.ieut in l..'hildre:n
• N<> aniso~.-oria • R.•\I_'f? prt.'S<!nl
• lktrohulbar • nmrmtl in 2/J. l/3 h>tre unilateral disk sm:/li.ng (plw:>ician & patients~ nothing)
• Papillitis- vtmahk -• Di.'ic swell in!!, iew flame
hcmorrlmges
• IV mcthylpn:d:ni.solmtc: (sltortcn:. tltl<ll:ks)
• Oral pn:dnison~, may • ltl1,1'Ctt~d rdapsc rmc • Section t(lr trcatmem if urtcritit: • Aisudatecl with MS in 74''"o of • femaks unJ .-;..~% cifrna~ ··
( )(her Causes of Disc Edema
• cl:!ntral retinal vein occlusion • · systemic illil.ess • HTN, vasculitis, hypercapnia e toxic/metabolic/nutritional deficiency • infiltration
• lisuallv no lo~s ofvision • Po~"ihfe trdll:;i~nt obscuration • Variablt! acllitv • Nonnal co\oui vbion
• 1-k:adm:hc. nau><:a., vomit in!! • Focal ncUrCllogkuJ c!cti ci IS·-
• N<J anisocoria • No R:\PD
• Variable disc ~'\veiling und ht:murrha!!es ..
• Absl!nl vent'!!$ ptllsativns
• T ft:<tt ~rcL~i ti!.: C'iltiSI:! uf im;r.:;a:;~d !C I'
• neoplastic: leukemia, lymphoma, glioma • non-neoplastic: sarcoidosis
• A<:ut;: ii~ld defect!; !Cl.mrrnonly altitudinal)
• lX:crt:ast.~d colour vi~iun
• :vrunartcritit; u:;ualtv no othc:r symr.toms
• TypiC3li,Y undurera[
• i\ u rut isocori:J • RAPD prt::s.:nt
• t•aie St:!!ln-:mul dis~: ~:d<:nK1 \:,·ith llnmc h...:rnorrlmgc ~;
• Consider .i\St\ tor nmNn·r.::ritic ist.:h...:mi<.: ut:uropa[b y
• pseudotumour cerebri · ·--• idiopathic sign~ and symptoms of increased ICP, with a normal CT
usually in obese young women • compressive
• meningioma, hemangioma, thyroid ophthalmopathy
I !
·-'
I J

' '""'"""'~--"-~ ;\.EBELLUM ~ J-.~S
!JNICAL PROBLEM: · Cerebellar disease (or any of the symptoms discussed below)
:; this because the patient has: (any of the following) 41 ataxia
:-a-diSturbance in the ~!ll~.o-~ p~r:f~Ili!~£e.J?f.Y.PlYPW1' motor acts • can affect gait, trunk, limbs, ~eech. e~ moyemen~ • e.g. • dysmetria (inability to control range of movement) • dys-dfadq_~ggkil!esia (inability to perform rapid alternating movements)
·inte~d-;n tremor ..... -v'-...--...........-..,.._'-""_.._~.....- .. ·• -~-_ .. _ _..__,.--
• muscle hypotonia • lnipaired check/rebound and pendular reflexes • ~ysarthria (e.g. scanning speech, telegraphic) • n~stagrnus
• f~s..t99J.n1lP.Il~I!.t~I beat is toward side of~n -- ~ tv~ • no motor weakness or sensory loss
patomy of the lesion: • ~~~ signs if unilateral lesion • BJl~ifboth sides are affected e.g. C§pilum tox, alco.hQ.~. MS, tumors, Arnold Chiari, Crebellar
degeneration (F~ie<h.'~~P.:S.~~a), SLE, etc. • paleocerebellum (s_u_p~r!orapd.m~..rlor vel-rpis)
~- coordmatestrunk and leg movement • neocex!W.~ (ctntc:,rio~JID4 .. P.9.~terior lobes)
• coordinates P~'!~PK qf..~alJ.istic and.tfu.~!y __ ~o~:~~~d_liP..~~'(~!ll.eE~upper limb • archlcerebellum (flocculog,odular lobe)
· • · i:iiallitenance of balance and eye lMvements during stance and gait ' .. A •. A •. lVt.J\..A..r'-..AN'-.. ~·· .;; ;; ... $
'irential Diagnosis:
CQUIRJ~:I?~ CEREBELLAR DlSEA..SE$4
· ·olloTic Cerebel1ar Degeneration · " midline (superiOr V'ennis)' atrophy ·
• tniiiCai and gait ~l~~ta, broad-based stance ·less frequent·;; a;:IIJ_ a~~ .nystagmU:$;<;ty;;arthria, . .Q.y].Qf9~~ and trun~al _ Lns.,~bil!_ty
• progressive, but partly reversible with abstinence • presentation may be ~e, s~e or c~oni..c • with or without previous Wernicke's enc_ephalopathy
• confusion, ataxia, opthalmoplegia (CN Vl nerve) ;meopla'St~bellar Degeneration -... •· diffuse cerebellar atrophy • rapidl).'_P._t:,<?~~ve . • gait and limb ataxia are prominent, often with ~Y..S.~la and ~yocl~n~ • associated with particular neoplasms
• s~~!l c~_ii"Sarcln,_9i!t.i..9ff!!ig. ~reast, ovary, and lymphoma
REDITARY ATAXIAS ,eancn--rs-AtaXTa ____ _ . • AR (chromosome 9) · • age of onset between 1.~~f2Q_y~ars __ • progressive gait ataxia, followed by l~m.b at~~ Fithin 2..Y.~'!rs ---
J~ ••
, .

• leg weakness, .knee and ankle areflexia, positive Babinski • ·musculoskeletal \lbnoi'I!lalities (kyphoscoliosis, pes:cavu5) • impaired j9int position sense and vibration sense in legs • cerebellar dysarthria .. degeneration of spinocerebellar, pyramida.t and large sensory fibers • death from cardiac (cardiomyopathy) or pulmonary (kyphoscoliosis} causes within 10-20 years of onset
Ataxia Telangiectasia • AR (chromosome.l1) • multisystem disorder characterized by PLQ&r.essiv~ ~reb~llar ataxia,
ocular and cutaneous telangiyctasia and immunodeficiency -- ·-- -• p~ogressive ataxia develops in infancy; telangiectasia develops later
Autosomal Dominant Cerebellar Ataxia (adult onset) • type l- ataxia, ophthalmoplegia, dementia, spasticity o type 2- ataxia, retinopathy with progressive visual loss e type 3 -ataxia alone, age of onset >50 years
NON-CEREBELLAR CAUSES TO EXCLUDE ·sensory ataxia Q_c>ss oflt;>in:t positiqn)_em;ej • pyramidal and extrapyramidal disorders which i.utez:fere.witb. controlled moveme11t NB-symptorns improve gradually with time if underlying disease does not progress
PI??{_OF ATAXLt\ Onset
Acute (minutes to hours)
Su~.:1Cl!te (hou1·s to days)
Cnronk (davs to \\leeks) . .
Episodic
TREATN£ENT
Disease Process
Cerebellar hemorrhage/inlllrction Traum.<1 ~a.~~ on gi: __ .
Posterior tbssa ttUU.Ol•rfabscess Ms-· Toxins f-{'-'dro~enh .. ·1h..t,S Cthll!:tin-!Batrt: syndrome VIral c;erebelli~is
Alcoholic cerebellar degenemlion ~af~~-~tl~ <.:erebdlifr smdrome ~i'il'atn~n.mag1wm compress1on .. Chron1c mfechon (CJU. rubdhl. pmteneephalttts} Hydrofephall!$ . · · V1tamrn E d~tictency H"\<'POthY1-okli.sm r-lert.'<lit1trl/ nraxia Idiopathic de_gt!neJ-ative ataxias
Recurrent intmdcati~>ns. JVlS TIA (ifact.'Or_npanied bv .othet· svmptoms) Dommant P-~ITtodicuta.xiu (iu ctii!dren) ·
The most important goal in management of patients with ataxia is to identify treatable disease entities. There is no
proven therapy for any of the autosomal dominant ataxias (SCAl to -28). There is preliminary evidence that
Ide ben one, a free-radical scavenger, can improve myocardial hypertrophy in patients with classic Fried reich ataxia;
there is no current evidence, however, that it improves neurologic function. Iron chelators and antioxidant drugs
are potentially harmful in-Friedreich's patients as they may increase heart muscle injury. ~ce.~azolamide can reduce
the duration of symptoms of episodic ataxia.
I
I c
) 1..

1\lULTlPL£ SCL£ROSIS (!\IS)
- a relapsin& or provessivc disease of CNS myelin clulractcriz<:d by disscmiwucd patches of demyelination of llu: brain aod spinal cord, resulting iu multiple and varied neurological symptoms and signs usually wiU• exacerbations and remissions. Lesions separated in time and space.
CLINICAL PROBLEM: MS
l say tltis because:
Hx:
OlE:
Patient may tell you if dx previously n>ade symptoms: parasthesia, gait disorder, weakness (e.g. hemiparesis, paraparesis (myelopathy)) and incoordination, visual loss (optic neuritis) and diplopia, incontinence, fatigue onset usually 20-40, but can be younger or older F:M-3:2 provwcuce in North America 1/1,000; most conunon in European racc:s aod in countries farther fiOJu the equator genetic predispusition: 3% risk for fust dcgJee relatives, 30% concordance for idcutical twins, HLA DR2 and Ow2 association
• signs: hyperrdlcxin, ataxia, nystagmus, spasticity and timb weakness ColJUuon Fearurcs
relapsing and remitting seusory symptoms subacute paioless spinal cord lesion acute brain stem syndrome subacute Joss of function of upp(r limb (dorsal column deficit) 6" CNpalsy
•. internuclear ophtbalmoplegia (lesion in MLF causing failure of adduction of the ipsilateral eye aud nystagmus of the abduaina eye ou attcmprod lateral gazo) optic ncwitis, optic atrophy - relative afferent pupil defect (Marcus Guon pupil- swing light bc:tween.pupils, affected pupil will paradoxically dilate when light is shone in it. This happens because the consensual relaxation response of lhe normal pupil will predominate as the affected eyes afferent pathway is parti aUy d11maged) Lhemutte's siW' (forward fie»: ion of the neck causes electric shock sensation dow11 the back to limbs, indicative of cciVical cord lesion) Uhlhoffs phenomenon (wors.:ning of symptoms with heat e.g. hot bath, exercise) trigeminal neuralgia in patients under SO postw"allrubt1li/Holmcs tremor rccUJTenl facial palsy
Etiololl:i • unlmown but inununological and viral theories (autoimmune attack of oligodcndrocytes)
Patho!!)gy multiple discrtte lesions of myelin destruction (plaques) common plaque sites include optic nerve, perivcntricul•r ilfcas, corpllS callosu,n, brainstem. spinal cord ·
• . Exludc! other strua...-n.:rd ~ ,~.t.::U ~( ~:-.::::.::~ rcy.:=. ! Demonslnll~ other sites of imulvcmeru (~!Rl. •".sci ct=.a ".:.:.;::; ;.:.{:::;.::...; ,
• Demonstrate inflammatory nature of lesions (CSF: o!igoclonallz ~d; L1 ~f. a , :r..::~ :.-:i concentration, mild lymphocytosis and increased protein) Exclude other conditions (CXR, s-AC£ (sarcoidosis), s-B 12, ANA (SU). Antipl>.lspbolipiJ antibody)
Management acute treallocnt
corticosteroids arc the most commonly used lnoatmcnt for acute attacks current recommendation is to trent disuhfuag attacks with SOO to !,000 mg of IV mclhylprcdnisolone for 3-S days with or witho\11 sbort orallllpcring dose ofprcdtli3one
• symptomatic tteauneot · symptowatic treatment for spasticity (baclofen ), painful symptoms gabapentin. tegretol),
bladder dysfunction (ditropan), sexual dysfunetion (Viagm). ataxia (c~am, IZN)fatiguc (aman!lldine), depression (SSRI's)
monitor closely for infection especially UTI (pconc to urinary retention) physiotherapy, speech therapy, occupational therapy. nutrition, social wad.: di!;Case suppressing agents
interferons, copolymers arc being used to suppress disease nt:tivity mechaoistn uncertain disease suppressing medications arc indie11tcd for ambulating patieuts with ficquent relapses, A2albioprine may be used ll-intcrferon (beta lb, Betascron) shown to decrease relapse rate, deer~ rogrcssion of disability
in patients with relapsing/remitting and progressive disease ll-intcrfcron (beta Ia, Avonco:) appears promising with similar efficacy w bctaseron Copolymer also decreases relapse rate in !dapsing remiUing disease and is QllJ'CI1IIy under investigation for use in secondary progressive trials un.dcr way for chronic and primarily progressive
What to tell the parient· • patieait education and counseling (disclosure, projlllosis, future expectations, support groups,
psychosocial issues: divorce, depression, suicide not uncommon
Course of Illness • 5 Types • relapsing remirting (80% present this way initially, F>M)
primary progressive (gradually progressive clinical counc li9D1 prcscuration, FGM) secondary provcssive (starts with rehtpsing remitting becomes progressive)
• clinically inactive: disease mixed paltem

\ ~YASTHENIA GRAVIS/ LAMBERT-EATON SYNDROME] F • . ~·
CLINICAL PROBLEM: MY ASTHENIA GRAVIS/ LAMBERT-EATON SYNDROME
I sav this because: o/e & h.x •.• .>·
• fluctuating course of muscle weakness, chiefly in muscles innervated by cranial nerves, causmg ptos~ ffiplopia, ~ysphagia and characteristically improved by cholinesterase-inhibiting drugs
• fatigability with use, relief with rest e remitting and exacerbating course "' fatigability is the hallmark of diseases affecting the.peuromuscgJ~f.ill£EtiOnz., e wea ess t at worsens with activity and improves with rest
Epidenriology e bimodal age of onset: 20's female'> males I 60's males> temales • !flymoma in 10% ofp~ts (more often in those aged 30-60) • associated with other autoimmune diseases: IDDM, thyroid disease, vitiligo
Pathophysiology .-• an autoimmune disease: production of antibodies to acetylcholine CAChl
receptors at nicotinic post-synaptic neuromuscular junction • decreased number of ACh receptors
Classi~__..._.._.., =• ·--
a based on distribution of weakness • g,yneralize.d; p,;:_oi<-imal~~a!}n~s-!3 (neck flexors, deltoids, hip flexors) • ocular: p~~s.L~_ffi)pl~ • bulbar: "Ctyspnagia:ctysartfllia
•"'-"•~·rz~· Diagnosis t1 §M...G ~hows ~~cle fatigabili:n' with repetitive stimulation 8 - single fiber-EMG: increased jitter (variability in the firing of individual muscle fibers of a
motor unit) e Tensilon test ( edrophonium) with transien~ reversal of weakness within 30-60 seconds • anti-acetylcholine receptor (AChR). antibodies (90% of generalized myasthenia
compared to 50% of pure ocular myasthenia have detectable serum antibodies) • thymic hypei"Elasia/thymomas visualized by CT or MRI
Treatment • anti-ACh inhibitors (increased ACh at receptor site) Mestinon, pyridostigmine • 'immunosuppressive drugs to attack underlying process:
• steroids) azathioprine e for acute crisis:
• IVIG, Rlasm~pheresis • thymectomy if indicated (after CT of chest to assess for thymoma)
Diff: Lambert-Eaton syndrome
- J
I

·. · ... · '' •. ;,
I. ' • :.A •• •.11;.~ • •• • ,
·· Ii\M BERT -EATON sXNi)Rolvm \ ~\·i ·.::: ... , ·- ·.-·• ...
.. r
• pathophysiology a myasthenic syndrome, due to l:!utoimmune._oroce.§S which targets mechanism releasing AClJ., re';ulting in inadequate release of ACh from nerve tenn.inals (antibodies to pre· synaptic ca++ channels)
• associated with small cell lung carcinoma and other malignancies ~ ...... .a..--......_.- .. .-. ............ .,.,.._-..- .... ~~....,....
• signs and symptoms ----~- - -~--- 4W'W , - -
• progressive proximal muscle weakness and fati~e but, unlike myasthenia gravis, bulbar and eye symptoms are. uncommon
• may be a temporary increase in muscle power during first few contractions • may have autonomic sympton.ls: dz:y m.Q!.!th, impotence, q_rthostatic hypotensio?,
constipation, p
difficult micturition, paresthesias, ~zyoreflexia, aching paip • diagnosis .
• EMG shows paradoxical increase in successive muscle contractions • poor response to edrophonium
• treatment • therapy of underlying neoplasm • plasma~heresis • Immune suppression o 3,4 diaminopyridine (according to Davidsons ©)
' '
"" ~ ·• :. . ·'··· ..
' . 1 . ·~. :, .. .
~~ !" . .. , ...... ~ . ...... ~" "t"- '\_ .
~ . · ~~. . ...... ' · .~ ~ _ .. ,
i ! •
\
/ r l
., I
. ·• . ,_,
\:,_" ........
'". . .,. . ~ . . ... • ·. ..,·r. •. ·~. •

\SPINE AND SPINAL CORD I CLINICAL PROBLEM: NEUROLICAL DEFICIT IN A :iEEV£ ROOT DISTRffilWGN(spinal cord lesion
([say thi3 bet:ause):
HISTORY: • Pain: Localized over spine or root distribution (may be aggravated by coughing etc.) • &nsory: Paraesthesia/numbness, spreads proximally from lower limbs to truq!s • Motor: ~ss, heaviness, stiffness. Most commonly in legs • Sphincters: U!]jenceylhesitancy, later urinary retention
OlE:
"' 0
• • ..
garaplegic/ guadriple~jc deficit corresponding to a ~sory level IT 4-nipple, T l 0-navel, L5-dorswn of foot, S !-lateral foot) bladder and bowel incontinence .!:Mtf signs~t the level/of the lesion and~ signsfi?elow the levcllofthe lesion (see Table 15) radicular symptoms ~· ~ ~atomal sen~ory .Jo~
• causes • extradural: disc, trauma, cervical spondylosis, bone, tumour (metastases), abscess • intradural, extramedullary: meningioma, neurofibroma, (lrachooid cyi!!_ • iDtradutl/.1, intramedullary: demyelination.. inflammatory (transverse myelitis) tumour. infarct, hemorrhage (A VM), or de~eration (subacute combined degeneration (SACD)), syrinx
Table 15. Comparism1 ofUMN and LMN Lesions
T0r1e
Fasc-iculation.->
\Veakucss
Upper Motor Neuron (UMN)
Nonhal (unless dislL~e)
lnct·eased (spastic:),~~~
Absent G ~~ ·
Pyram ida] patkm (.. pper .zxtremi.ry: ext<::n.<;ors wcakesl Lmver cxtremrty: tl"'~Ol':l Wl.!rtkcsr
fncre-Jsc::d +
Lower Motor N\!uron (LMl'i)
Muse!~ wastln!!·
~rea.-~ed (£bad f~\7"!>i<f.') flrest:nt
?pccitic t-c• lesicm I.e. rDot, nerve
\ Compressive · ~SPfq_2J.d~i~ Epidural, intradural, or intramedullary Y.a.s.s=.ulit!s. neoplasm 9 Infectious Epidural abscess Viral: VZV, HSV-1 and -2, CMV, HIV, Epidural hemorrhage HTL V-I, others Cervical spondylosis Bacterial and mycobacterial: Borrelia, Herniated disc Listeria, syphilis, others Posttraumatic compression by fractured. Mycoplasma pneumoniae or displaced vertebra or hemorrhage Parasitic: schistosomiasis, toxoplasmosis
LJ - • ~'-J \JVo, 0'<' ' ~ Vascular "' , ~~- . Artenovenous rna orma 10n Syringomyelia Antiphospholipid syndrome and other Meningomyelocoele hvpercoagulable states Tethered cord syndrome
9 ~ Metabolic ~ ~2 ~efl2iency (subacute combined degeneration)
. I
· •'\gjnal'cord svndrowes: difi \ . . \ c.;:,. lrown-Sequard Syndrome: lateral compression ofonebalfofspinal cord~ ~e·t-.:~o. co
• ipsilateral LMN signs at level of lesion
• ipsilateral I~_g_fyibration and proprioc-S'!!on below lesion . , . • contralateral loss ofpain and temperarure below lesion \::::o~\ 1 ~'~~\ou...~c:.. ·
• ipsilateral hemiplegia or monoplegia below lesion & UMN signs :w; • coiiL'1loncauses-,...t1fin_o!!!,radia~ pto~~+b9. : fO'I\·~· \·~W\~. ,'\c\.... .
:entral £ord Sxn&om) • • <.A\Ote).l:\of'o...
• common causes are i~~gll?.le~ and intrinsic tumours Pr~ • suspended or cape sensory oss over sh~callesion most common • dissociated senm loss .
~ss of pam and temperature sensation with spared touch. joint position and vibration • atrophMfintrinsic hand muscles (anterior hom cells), . ·
( ;ntenor gi?mal _ efr g@rt'nlfl , ., sudden para/quadriplegia; initial fiaccicti!Y and areflexia ( .. spinal shock"); -e- L ~ ~-s ·
within days develop !J!ill'l signs below lesion • preserved vibration and position sense (spared posterior columns) • due to occluded anterior s ina! arte , uSually at thoracic level
:ubacute o i D eneration o t e ma or • corticospinal and posterior columns are affected e.g. vitamin B 12 deficiency, HIV • s stem de eneration therefore no · tinct motor or se~
::onus e u aris Cauda E uina S drome · · · • hyPotonic b a der and rectal sphincters • ~in and loss of sensation in saddle distribution in perineum • _&o~ aQ§e11t ~s • causes: cord disc herniation tumour, inflammatorY
r oramen a urn o • quadripare§iS, neck/head pain, hand atrophy+/- cerebell\lf signs • cause: ~s · ·
~nsverse $d]'e'ifis I • back pam, rapid onset cord syndrome • cause: est-infections, inflammatory, demyelLrJation
t'Mural Abscess
• •
.... om o trauma. tumour • loss of all sensation and voluntary motor ti.mction below level (UMN2
SPECLA.L rNVESTIGATIONS (according to diff: l?.!22_ds,~,.,bEs etc)
~SSESSMENT -acute intervention (surgery) needed in ''}cute spinal cord s;mdrome' .. . refer to neurosurgery
TREATMENT PLAN- depends on cause. Also prevent complications (see stroke summary)
'ATIENT rNFOR.J.YfATION
Discuss the condition with the patient and the family. Explain that there are various causes which may result in the 1atients clinical picture and that the patient would need a thorough investigation before prognosis etc. will be Jiscussed. Information regarding rehab, preventing pressure sores etc. is vital. ~

i sav this because: ~ "'==>J.,o.v-\-·Hx.and OlE: .!1-t'aeth~~· ~uscle .!!~kn~~s etc. Ask about: tV E~~e. s\o.W.. • onset, progression {acute, subacute, chronic) ® d...c-.\"""'h""' • det~nnine if motor, sensory, autonomic dysfunction. ~~.7 \ , .__.. ....... ,,..,'4\Q--
• if chronic motor, see musCle atrophy and' ab~ent reflexes "S~\~ tc'\" . • ifsens_?FY• may have paresthes~as in addition to sensory Ioss~\u.?"~ -t-\-\.~ G'Selr~y ~\.ml\C)IIJ~"<>-. · ·autonomic dysfunct;on includes anhydrosi~, qr dysmptility, ori&ostatlc'hwotension, ~~ .
impotence, bladder/bowel dysfunction, impairment of pupillary responses \'J...~ ~~ :\:::)\)...\ , \-\'1.\.J 1
A\.c.c'\;;-.c, \ • mononeuropathy vs. polyneuropathy' • proximal vs. dist?l fo"'-r-- l.f.-t=> •. c~oX:.\o.h) \.l.~.c:~k.~o· l • upper vs. lower extremities. S\0~ 0\'\ ~ ~~"'o\'y_,.. • fiber :>i.~e selectivity , ~
• 1~: m..2,!~~ w~2§.s, ~orjoin~ QQ.Sl~~· vlQ.raijo~, and_!.£,ucb!p,ressw-e fAIJ:. '1> ~ • ( . ,
• s~l: ~and ~m~re~e TQ~~· autonomic dysfimc!io~ · .:t ~' ~'C.~ ~~ ~' ~ ~ • relationships to systemtc tilness (Q.~, M •. ~~9.ID. , . · a::::¢' {:0.-w. • family history, especially with unexplained polyneuropathy from childhood (hereditary); -\U\IS'-.. '<..cj later life, paraneoplastic or paraproteinemic causation is more likely \..AO~ ~
• pes cavus, thickened nerves in hereditary causes 1:::>\-s\o.\ ~ ~ e Ko.~' 1~ ~\e)()a
Assessment:
I disorders mimkkinu PNS dist::L'ic · h_:ijervcntilation - ··
• mvasthcnia gravis • spi.nal mtL'H:ular airophy
e!t."St(ation ·:
din ic::tV,lubs/ED:i" I
true PNS di:st:~
• myopntlty I foaiVrlit~ "''"""'h;.,. • psvchooenic dem:<:linatin~ . L-ervicui cord putholog_y pol}:neJ}ropatny . ·Othq - I I
mononeuropathy , mononeuropat!i~· acq1f'r.:d-unithrm ~"' h~reditary • compressjon multiple..x - injurv - isd1emic nommiJim.n
' (vasculitis) - inflammat\11')' i.e. GBS
"EDS -ek:;;lr(Jdtll~'l'JO:;tic srudies - inftltrath'c • 11un-iu flamlnntol;;
Figure 17. A<>scssmcnt of Periphcrnl Neuropathies
ditlijse disens~
I axonal
potyncurvalhy
I :t<.iyrirelj
- .<>;sremic • cfn1g~roxill$ • nutritional
r I
I I .

·-Ill V ;md antiretroviral therapy neuropathy
; (,ju: ~li~fi!.Jcr sensoo: {ataxic-neuropathies) ;· .
':liiJ•.n:n's syndrome
Vit:11nin B 12 neuropathy (from dorsal column involvement)
I h rido."<ine toxicity ._b. . .. .
I· rinln:ich's ataxia ..
j"''uall- :~nd large-fiber:. Global sensory loss
• < ·:lf'l:inomatous sensory neuropathy
I k·n.:ditary sensory neuropathies (recessive and dominant)
I I )iabctic sensory neuropathy I --1\lotor-[!redominant neuroQatbies
'
) ltnrnune neuropathies: acute (Guillain-Barre syndrome); relapsing
---
t\L'utc intennittent porphyria
I l>iphtheritic neuropathy
l.~· ad nt:uropathy ..
.l_li:_~!~ctic lumbosacralplexus neuropathy (diabetic amyotrophy)
.~~utuuomic _
;\cut~: Acute pandysautonomic neuropathy, botulism, porphyria, GBS, amiodarone, vincristine
I Cl.u'unic:. Amyloid, diabetes, Sjogren, Chagas, paraneoplastic
Otltl•r causes: chrome renal failure, SLE, RA, hypothyroidism
:C!H_!>monly used drugs associated with PN: .• • Statins
1\) . . \ .. \ 0.:3\ .c~c.:_.\ .. \'-N~t-. C)~ ':l..\'C~'il~·\0\\~ iC'"l:.
" IZN • Ethambutol • Metronidazole
Chloramphenicol • Phenytoin • Colchicine • Poison: Organophosphates ·
L<tlJ investigations (based on clinical suspicion)
1 \!\ \ ~,'( c: ,'~ \-··\\ l. \.) <~)', )~\\ i\, 'S.
-l; '?,\ '2..
~\'\\)
Lkctrodiagnostic studies (NCS, EMG, quantitative sensitivity testing) • L:untirm neuropathy and elimination of non-neuropathic disorder • ltlL:~If ization of focal lesion, prediction of pathology
NL:rvt: biopsy has limited use · v:1sctditides, sarcoid, amyloid, inherited storage disorders
. Treatment:
• Antidepressants (tricyclics, SSRI's) • Anticonvulsants (Carbamazepine, Gabapentin etc.)
• Opiods (second line) • Alternative (acupuncture etc.)
\ . <..('
\):~ ~-'~.N.::.(;e. U-~'cx:--1 ·'t(t'c\ C<S\.,:, ._, ~
- \- :( .\' "- := T c J\ (o.'""'7\ \'/( )\::~'\\..t...~~ C /J- :.. C,(._'o..'{;C:.\OC c;, :<_:k ( ·._:.:.,(____
)\I.'C\''>0'
G\(\''-'C<> ""· .. c.·, Sc 'c 'c:-..\\!'<~
·:c\i-..c': \~ :-.J.> • • \' "c')~c)-.'\c)

ACUTE INFLAMM. DEMYELINATING POLYNEUROPATHY (QUILLIAN BARRE) A:l1Cf>
CLINICAL PROBLEM: Ascending ~cle paralysis and areflexia (?GB)
I say this because: ('.16~ On hx and OfE: p\cs.\:o.\.). o-1\et 4- w~ . je~, I , :,
• Sx started 1-4 weeks after RTI/diarrhoea (70% Compylobacter) At. ""'-"' ... " .. ......_, ...._ •
• Distal paraesthesia and limb pains precede ~--- -
11 May or may not have a sensory component
Apyrexial, no sl'stemic signs _A, •\o·-lo"'"'-'c ... . c """"i'Ci:t
gapidly ascending muscle weakne~s (~er to upper lim_.bs but £F.9&Pal >severe) Facial and bulbar involvement is common __ _ ... _.,
o lt~s.P. ~~Sf~e~. involved in 20%, may need ventilation · . e ~esses for 1-3-::ks but may haEpen in a few bgurs
Pathology: Autoimmune cell mediated inflammatorx respons,e at myelin of spinal roots.. ~ripheral and extra-axial cranial nerves. Inflammatory cznokines blocks nerve conductio,n leading to complement-mediated destruction of myelin sheath+/- axon.
-- --- ~~~-- · l,b~ ... ,e.\\'4'-~\~ \ Diff: ":, l ____ .... ~ . .
• ~~}~~.g}_;:.~-~~--Y~~?}}O~~~ia, ~~~}.a andare.f1~25.~~) • Cbron:ic Inflanunatory Demyelinating Polyneurop~thy (similar with chronic nature) · • -Aiw"ay;, ~~~~l~?~·~~ut~,~;o~h~5f~~~~~~~ ..... - ·-·~~- ~~---~ ~
• • - ·- · ·.,Y') .~- ...... •• • .~ ,....,.....,,~ .}. .; :S a --~-~~~~yt},; (poJy§l!!~ti.!I~ .. l]pdq~a. sy~~_rp.ic lupys __ ery14_erp~~OS:UJi· CAwg;$ya,uss syndr.qrpe), .. t?
to~~LI,l.s (organophosphates, lead), l?Rmlis;n, di:a\l.!Qsna, 12.Clml.rt .. ria, \9 .. 1?.~H?.~4. .. sP.~!-~2!.4 2~. -..; . c~~.a.._~q~An.:~ s.~c!E,?E.l.~o '-o ~
seecmrrnve_~tfgation_~.G .. j ~ ·-@ . { ' ': ,, \-'1 J !1}1 o CS_f.p,r.qtejnJ~wr~~$-~d (but normal in first 10 days!!)
• •
•
CSF cell count normal ~- .•1 · <:-;•\ .:. :::.' , ... ,...·. \ . -~ ·---··· . .. .. ~- --- - ~ . · ... ~ . '.~ .. ....... .,..- ...... -~lectrophY.~!o~o,&y: Typical ch~~,S after L,w,eek only, cond~~t!.0!1. ~l.~,c~3 IJlU,.l~~fq~al . mo~or slow,ing_ etc. To detect the underlying cause: 9N1V, mycoplasma, compylobacter, CXR, stool culture, iiiliil~U?~Oe?Y._, ·,,,-' .. ·. <T.:. .....• ; •. ' · ··'·· .i . · .. -." ··."- ~ ,. _,. ~-·· ... : '· ··' ~-- i- 4 ' ' ;, ·· ' : '

~yq_:;c;..'\~y u~ . A~OV ( ~'\:lo\;0-J\'~/ •
~~~ E).
DISEASES OF MUSCLHI \)<O'AMc.\ ~~~ ... ~ ~~7 ~
General /\_ · ~- , ~r ~~~ • muscle disorders have features of a LMN lesion ~ 'o."t, c,,O\.c-r ~ ~ • myopathies cause ·~weakncss, usually worse in axial and proximal limb girdle muscles
• muscle disuse causes type U fiber atrophy @ \e%\ ~el:::::. .
Table 16. Comparison of MoscJe and Nerve Disorders
N~ruropathy
\Veakm:ss Bulk Reflexes Sensation EtviG
Prox.itmlt (ex¢;;pt ntyotontu) Decrea..~ (late finding)
Ncrm~ Dc~:.reased (lat~ findi-ng) Normal
Distal (except GuUlain~f3arr~) Decreased ~'leda.
Deereasedt
M usc It: enzymes MLL';cle biopsy
Myopathic; NCS normal
lno-eas.t:d Nettrdpnthie;. NCS may b~ slow US1:latlynommt.
Diffuse losSl Grtnip.·tibre ~
CLINICAL PROBLEM: OFTEN (but not always) bilat proximctl IlPlScle weakne5$without sensory falloutt
) --e.~ ~\\a.t"' ()u.~· c::: e:,l
l',QI..XMXQ~ (PMY)IP~ (DMY) "~~\~ ~ ~ . . • an inflammatory and probably autoim:mune muscle disease characterizeat"y the subacute onset ":.;.- I., '-" ' ,-,, .r \.' , .•.
(weeks to months) ofsymmetricld, prcroma1.muscleweaknC'31S of limbs and girdle • 15% have accompanying skinras.la. (dermatomyositis) • heliotrope:rasb., rash on extensOl'surface~ "shawl" sign, ectopic calcifications in subcutaneous tissue • muscles may be painful and tender • pharyngeal and lazyngeal'.muscle involvement leads to dysphcmmand dysphouim • accompanying features include Raynaud~s· phenomen&n, arthralgi._ malais114 weight loss and low-grade
fever 6u.~~o~ f\ceu\~ -epidemiology
8 per 100,000, age 30-60 10% of adults with myopathy have neoplasia, usuaHy carcinomaJ. . \ 60% of adults > 40 years with dermatomyollitis have neoplasia (\-bto.-\l..C.C~\~ ~~'\.{"-'' 15% may have symptoms and signs of a collagen vascular disease (CVIJ} ~· eo.. . \
clinical signs/symptoms ~ \\\C>\S. Q \i~' increased CPK.ib . ... 13'.--,, . -: •. ;.m':!.,. ~~><:, <::': dC-i\' may have circulating antibodres .o Rf, AN:A · . \A:).~, ~~
diagnosis
EMG' myopathi'e (myopathic motor units on EMG and spontaneous activity - fibrillation potentials, insertional activity) muscle- biopsy showing destruction of muscle fiber! with inflammatory cells
treatment • steroidS or immunosuppre~ives (prednisone 60-80 mglday, l!_nuran) . ., .Av .. ;\: ""b '\
~ ~Ca.tc".J;oN--'tCf>cl-\_y ~"~\\\\a.\ \uv~ 6tsl?~ .C A-Yl -) . Other Inflammatory MyopathieS! . /
• inclusion body myositis • infectiou:ll
viral - Enteroviruses: Coxsackievirus, Echovirus parasitic ~ toxoplasmosis, schistosomiasis
, • drug-induced ~ penicillamine, clofibrate, bezafibrate ,.:) METABOLIC MY OJ? A THIES
• correction of the endocrine disturbance results in recovery
D\~ ~l"c\ . ..\.c:eY Lc,;, \o-'\~c;---. ~s~-c:.CE:,
--r \1\..~ \o\N'- . (::> ~/ D~Y
\-U:.\J riJ'.~\.4\o~ '-l7'C2'/ ~a_>~O
a-/

• acromegaly: with proximal weakness and fatigue • thyrotoxicosis: weakness in 20%, shoulder girdle> pelvic • bypothyroidisllll pro~ weakness, pelvic girdle > shoulder, associated with • painful cramps and muscle stiffuess • hyper· or hypoadrenalism: proximal myopathy due to these conditions, • also due to steroids used to treat hypoadrenalism
-~ L!JiliE.!Dirr~fi:im~ ··:) QuchemJ.e ¥'u.~cular.D.xstrooh.'i
• epidemiology l{i&Q.Q..Iive male births, prevalence 3/100,000 ~~~.e (Xp21), dX§!fQR..hJn. ~!tr o,:_:~~i,ls.,_ap, 40% sporadic , \.J!',co}.c '.J~.o•\ 'f'-6..>1~·-0 ;.;.1 ~ c:..
• signs and symptoms progressive muscle weakness §"~~~~t, hard to climb ~tairs, Q.~e .. ~~) ~~~e~o_p_~~.Pi£~CV:s · · axia:t musCles invo ved, Te'id'S to ~!~o¥2~~ and r~!o~.~~ c~ mus;Ie involved late in Co.EfJe C o.\6io·N~ \ \},.... mean IQT$'-:W"Po~lo,;.,~ tlia7i nonnal r •J.J.:C'\ progress iv~.~.!!l .. 41ir~~d2Jesf~l'!;.,e
• investigations • . cesubstantially increased - early sign
E..W E.~- c~~~ .. l!£!i<Hl.a_R.IJ?~~and x:h~~~ , muscle .btopsy- no stammg 0 ys~oplim : .. ..A\ty.J..">J.-1.. ,··\:;d-\!:~·1' '·1 " c:.,o\et'.
Becke~ rt.;{u,~cu~ Q;¥sttoph.:i, • epidemiology ~ live male births mean age of onset I.~~~· 90% by age 20 _signs and symptoms less severe than Duchenne
... s~uscles ~£.~.~qrg,zf~~ mental ret~n rare
: .. ~~="~l~llf
same gene, different mutation
?o4xotQnic.lli:s.troph:t;.. ~ Co..'-f\...\ ~.:!C \i\J'..\.}..~\.L · • epidemiology
AD ( 19q), triplet repeat • 5/lOO,OOO,a~-~~::,.
• signs and symptoms dist~l \V~~;;s, ~~!~.faci;i Cifin, ~}!!~9J~£~J;.lW,~J~25· · pt.9.~· ~~J.!IDQD\l, masseter allii'Stemo~ei:domastm<f atropfiy) · .
ll?:i'.2t2!1~= f~~~1t~1~--~!:lt~ .. ~~~!.!~~~ IlJ.a~: _fi?J.!~l .,!:~~~ql teft~;,:_~l~ atr~J- ':' ::\ .~,_\ , .'·~- . . . multis.ystem teatures mclud111~ ~. c~~c·}7,SE_~~ll· s~~l~t,.al and e.B.~~~:~f~~211~ s,U~ht~.E~~!ru1.l~M!..) . .
' ' . '
I
i

Neuroectodermal syndromes Tissue derived frm ectodetm forms tumours & hamattomas, -with lesions in skin. eye, & CNS.
1) Neurofibromatosis 2) 'Tuberous Sclerosis (Epiloia) 3} · Sturge-Wcbcr syndrome ( encepbalofacial angiomatosis) 4) Von Hippel-Li.;ldau syndrome(Ietinoccrcbcl!::t angiomatosi!) 5) Ataxia Telangiectasia 6) Osler-Weber-Rendu syndrome (hercditaryhacmorrhagic telangiectasia)
l)Neuroflbromatosis
) Multiple skin neurofibromas (fun neurilemma sheath) & pigmentation .l> Epidemiology= 1/4000 live birtll$ .l> Autosomal dominant )> 2 types;
Type 1 (peripheral> 70%) -a.k.a. Von Rec:klinghausen's disca5(f -Chromosome 11· -Freckling: skin folds (axilla, groin, neck,
submammary--crowe's sg) -Derma/neurofibromas; gelatinous in texture,
Not painfull. -Nodular neurofinromas: arise frm verve trunks,
Finn--can give rise to paraesthesia. -Lisch nodules = hamartomas on iris,
(sproete op iris)> 2 =significant. -Dx criteria:
-Dlff o.~:
> 6 caf6-au-lait (> l5mm postpubertal) > 2 neurobibro!IIa$ Freckling in axilla Optic glioma > 2 Lisch nodules l" degree relative with NI' l" ·
McCune Albright Multiple lentigenes) Urticaria pigmentosa ·.
-C:<: (30%) ~ Learning disability =Nerve root compression = GIT: bleed, obstruction = bone: cystic lesiocs =Scoliosis =plexiform neuro-fibromas: large subcutaneous
S wel!ings----Malignancy in 5·% = optic· glioma -Nix: Multidiciplinary
Yearly assessment---cutaneous survey Removing all lesions-unrealistic
2lTuberous Sclerosis <Epiloia)
> Rare; autosomal dominanl!
> ±Retinal phakomas (glial masses) > Renal tumour.; > Glial overgrowth in brain > Gliomas-
3\Stur"'e Weber !vndrome {encephalofacial anglomatoslsf
Type 2 (central) -Rare= 1/35 000 -Chromosome 22 ·· -Ox: I)bilatetal Ve.!Jtibular schwannomas (MRI!Cf)
(acoustic neuroma)---sensorineuralllearlng loss l" sg, ±tinnitus/vertigo. Bec..ign tumours---compress On structures = i ICP)
2) 1" degree relative with NF2 and either: A)unilatctal vestibular sch.wannoma, or B)oncr of following;
-Dif£Dx: NFl
I)neurofibromao mmeningoma-· lll)glioma-.. N)schwannoma• . V)juvenile catatacr•-occurs before
other manifestations, used for screening t risk pt's.
-Cx: Schwa.onomas o!'other cranial nerves; Men.ingioma.si
-l.Vb:: Hearing tl:sal MRI foltowupo Vestibular achWllDllOIIIII$- neurosurgery (Cxed by
hearing loss/facial palsy)
)> Extensive port-wine: stain on one side of face-t- leptomeningeal angioma > Epilepsy= common;

:fW on H!opel L!nda11 svulfrome
.> Retinal/cerebellar hacmangioblastomas devclo~ J;> Renal, adtcnal &; panereatic. tumouts somctimelf
S>Ataxia te!anglestasta
J;> Progxessive ataxia )> Tela.ngic:-ectasia;;r nose. conjUIIl)tiva. caJS &:skiltcreaseiJ )> Defects in-cell-mediated' iminunit¥ at lintl1iody J)I'Odu'ctiOll )> Death in 314 decado--Infectioollymphomicula:tmalignancf'
6)05ter-Weber-Rendll:--see haematology·section

' ~ I
)> · ·Acute liver failure ~ > Abdominal mass V > Ascites )> Splenomegally > Hepatosplenomegally )> Liver Orrhosis > Portal Hypertension )> Liver neoplasms )> Viral Hepatitis
. . : ..
Abdomen
<1 -, .
• ! 1
j .,
·J ., '
' I ~
' ,; l
j
-~

APPROACH to the JAUNDICED PATIENT
1. Introduce the patient 2. Relevant Backwound history (which may Indicate the cause of jaundice}
• Recent malaria: antimalarials & malaria cause jaundice } ,..,----.....,
..
recent blood transfusions _ haemolysis
O~cupation (heahhcare worker, ~ex worker}, tattoos & pierdngs Alcohol abu::5e or Hx of cinhosls H~ of hepatitis or EBV OU1er autoimmune disease • f chance of Alllepalitls COPD: chance of a1 amlillYpsin deficiency TB: INH, rifampicin, PZA Hypercholesterolaemla: statlns cause J Mood disorders: Epl am and MAO Is cause J Recent anaesthesia: "halOUiilne hepaUUs"
hepatocellular
Abd. aminal pain: think gallstones (In CBD). pancrealltis and chol chal cyst Recent antibiotics: flucloxacillln. co-amoxyclav. nitrofurantoin ...-------,]
HX: of dark urlne & pale stools ± coUcky pain 1 Oral contraceptives I cholestasls Psychosis: Chlorpromazine L. --~---' OM: sulfonylureas RA:go~ ·
3. ~linical problem Patient has a cUnical problem of jaundice plus con1blnatlons of the loUowlng on Hx 11nd physical examination:
.• · Hx & othur sx of chronic liver disease (see notes on hepatomegaUy & HSIIA) -. •compUcatedldecompensated" cirrhosis is likely: this could be due to superimposed sepsis (UTI, pneumonia, SBP), viral hepatitis, alcohol misuse, drugs, malignancy or Gl bleuding. Features of an acute (or chronic) Infection without findings suggestive of chronic iver disease: think of viral hepalilis ( esp if classic prodrome :1: sexual or occupational exposure), autoimmune hepatitis (esp young female), malarlil or other <;<~u:;es of haemolysis (e.g. ·rrp, HUS, HIV), ;~s weu as sx of TB FeatulllS suggesUng malignancy: other malignancy (fiver mets common), weight loss, anorexia, fever, lymphadenopathy, sx of obstructive jaundice. palpable gallbladder & painless J (courvolsfer's law) Psych patient with no other significant clinical features: think meds as above Asymptomatic pt with only t unconj bilirubin: Gilberts syndrome (esp after fasUng or EtOH consumpUon.
4. History: discu55ed above.
5. Exlilmlnation (see approach to HSM as well) Must examine for :~igns of ~hronlc iver disease, hepatic encephalopathy, as well as features of contrlbutory conditions
Genarat sx of blood transfusions or IVDU, tattoos, plamar erythema. gynacomasUa, spider naevla,capul medusil, cour.teilller BaumgarteJJ syndrome. CVS: sx of CCF: Respiratory: consolidationJpneumonia/pulmonary oedema/bronchus Ca Abdo: masses, pancreas
6. Speciallnvestlgallons r---------,
/I )(
!iaemolysls 8. Ineffective erythropoesl~
(e.g. megalobla~Uc an) Do Coombs and rnaiarla smear :1: LDH, haptoglobin
Gilberts syndrome. Most common form of congentlal
URINE for bilirubin & SER.UM-bili & LFT's
& other LFf's OK: Dubln-Johnson or Rotors (very RARE)
"hepatocellular Jaundice· Drugs
nan haemolytic hyperbllfnlblnaemia Viral Alcohol Autoimmune Haemochtomatosls WUson'selc
Special Investigations: Clotting studies Hep studies Drug levels Iron studies Autoantlbodles
Biochemical chan<1es SU<i<!eslin<~ aetiology of aundlc.-Enivmo comblnaUon Dlaonostlc b'keihood Amlno-tranferases ALP . HepatoceUular (AST&ALT Jaundice >x6 <2.5 90% <x6 > 2.5 10o;. Other combinaUons No clear lle!laralion
MRCP If unDkely to need duct decompression ERCP: vice versa
Biliary ObstrucUon
10'Y• 80'Yo
t GGT may suggest alcohol abuse, but may also be caused by barbiturates. carbamazsplne, glucocortlcoids. griseofulvin, INH. Rifampicin, &. phenytQin (!lOt comprehensive) FBC: detect causes ol anaemia wee & dlff: leucocytosis may suggest dtolangilis, alcoholic hepatitis; atypical lymphocytes may suggest Infective mono (EBV)
7. Treatment: according to the underlying cause 8. Explanation to patient
Approach to a patient with ACUTE LIVER FAILURE
1. Introduce the patient
2. Relev;mt Background Hl<itory twilhout Hx of chronic liver Wseasel Drugs (70-80% _, e.g. paracetamol, halothane. antituberculous drugs, ecstasy, herbal remedies); Viral infections (5%: Hep AJB/D as well as 5%: yellow lever, EBV, CMV etc .... thus immune status and travel Hx is very NB); pregnancy (may give acute fatly liver); malignancy (liver mets, lymphoma): recent shockJcardiac failure; mushrooms (amanila phalloides); NB: sudden onset (plus ascites) in the absence o! ln!ectlons/drugs: hepatic venous oul11ow obstruction (Budd-Chiar\) /with Hx of chronic liver di§ease I.e acute-on-cbronic!: all the causes of cirrhosis and Its compUcations: alcohol, chronic viral hepatitis, hereditaJy disease (haemochromatosls, o1-antillypsln deficiency, 1' biliary cirrhosis, wilson's); autoimmune Uver disease, NASH, CHF etc Thus ask about alcohol Hx, work & social habits (health CW, IV drug abuse); diabetes
3. Clinical Problem The term acute hepatic failure refers to a syndrome of hepatic encephalopathy resuHing from a sudden Impairment or Uver!unction, characterised by mental changes progressing from confusion and stupor to coma and death. Can occur suddenly in a previously hea~hy liver (=acute liver failure) or more commonly as •acute-on-chronic" liver failure: in this case took for a precipitant .... GIT haemorrhage, hyperkalaemia, excess dietary protein, paracentesis, acidosis, trauma, Infection, colon surgefY, sedatives
!fr.i!lP.''~~~tt:~~~1&!A~~~~~~~l~i,\~~~;1!~~!,.-.;~"" - ,r· ~·;~ k" ~~- · t';;,! :l"'-~''":·~~,~-"~··•< :~~~ID.: .~~~H,. __ ... . <.o:;uc~"i-.t~ ::f.!fi~iU!l .. ~~ff...!:.,.Jn.tli .... ~~!l4l'!:.r~~ ~~ ~.lJ .~~M.f.a-..... n~r:~at{~jj't_ ~..:... ~·~ :;.Eni:ephalopa'lhy Within.? . · -_ Within 8-28 days of 9nset :· , .•. Within 5-26.weeks ' •; : : , .. ·. · ;;days of.llnliiol of jaundice · : : ,.,· ' . .. . · _':: .... . .. ··.:J ... ~~rmit.1J~Il~tm~l~n\ID.\(ij':J:Ji5::Q?.Aim~;:f~~J£-~i;i;·::J w:nwmrni?Ji~jl:~:r..~E~~£tt: ;,:comm~ly,dt~a_l'? clrugs ,and · .. -: Cryptogenic, drug~ ·.•. ·· -.'. . '. Cryptogenic, clrugs · · · . , ~:Vi~es 1 ~~~::~.: ·! :-. :;.; 1·: •• : · r~. {::·.' .: : '!· ~ , :·~ ·- ;:-:1 · ~ - , ., ·: ·. _ ,· __ . · ... ··:. .; ... ··•• ··· : ··:· ~~- .·. .
. THUS, "this patient most likely has a clinical problem of acute liver failure as thQ following features are Dres!lnl": jaundice, hepatic encephalopathy, fetor hapaticus, asterixis, constructional apraxia (cannot draw a 5-pointed star) PLUS either CO!llpatible Hx or signs of chronic liver disease {suggestive of acute-on-chronic decompensation).
/ The grade of encephalopathy Is:
t:Grade 2:-~ ;-jnerelislng·dr9W&jn'~a$;: confusion, slurred speech ·· .' :·-~· ;.: .
~'i!!}~~w.•1l!ililfl1~!\!t;~-~if~~t~lsl'!ir.cinlf9.'~(~~iC?~1r~t:d~ ~Grade4 ;;, ' eama-~ ·" :'··-:~~~-.:~ ;~- = .: .: . · ·. ... -:.·.. · ."·
The following eompti.:atlons must be born in mind: hypoglycaemla, Infection (bacteriaVfungal), renal failure, MOF (esp. hypotension and respiratory failure) The following conditions must also be considered/ruled out: sepsis, trauma, seizure activity, diabet.lc ketoacidosis ..
4. History: mention important positives and negatives.
5. Examination General: obviously JACCOL Is very nb to help suggest a cause/precipilant; fetor hepaticus; signs o! autoimmune disease; see (notes on hepalomegaly for a comprehensive review of the sx of chronic liver disease)
CVS: pulse. BP are NB (see below) Respiratory: hyperventilation due lo ICP changes or hepatopuimonary syndrome CNS: flapping tremor (asterixls); signs of l ICP: unequaVabn reacting pupils, fixed pupils, hyperten-sive episodes, bradycardia, hyperventilatlon, profuse sweating, lOcal or general myoclonus, local fils or decerebrate posturing Abdo: RUQ mass or discomfort; peripheral sx of chronic liver disease
6. Speciallnvestlgations Investigations to detennine the aetiology o FBC, LFT and UKE (Cr Is more useful since urea is synthesised In the
Hver) o Toxicology on blood and urine o lgM anti·HBc o lgM anti-HAV o Anti-HEV, HCV, CMV, HSV, EBV o Caeruloplasmin, serum copper, urinary copper, slit lamp eye exam (an for
Wilson's) · o Ferrllin/iron profile o Cultures: blood, urine, ascites fluid o Autoantibodies: ANA, Antl-SM, Anti-LKM etc o Immunoglobulins o U/S liver and Doppler of hepatic veins (asp. for ?Budd-Chlari)EEG to
rule out underlying se!lure disorder (limited value) Liver function tests o PT/INR: prolOngs as coagulation factor synthesis declines o Bilirubin o Transaminases are Initially high but fall a5 liver damage progress o Albumin Is usually normal unless prolonged course
7. Treatment Nurse with head 20" head up tn tCU. Intubate to protect airway+ NG tube (removo blood from stomach - ~ nitrogen load) Foley catheter and CVP Monitor vital, urine output and pupils hourly; dally weight Check FBC, UE, LFT & INR daily 10% dextrose IV, 1LJ12hrs to prevent hypoglycaemla Rx any known causes Dietary consultation + folate, thiamine & B 12 Haemodialysis if renal failure ensues (hepatorenal syndrome: splanchnic vasodilation causes an ARF picture) Avoid sedatives or drugs with hepatic metabolism Lorazepam lor seizures PPI prophylaxis tor stress ulceration Uaise with transplant services Complications: o Infection: ceftriaxone until sensitivities know (avoid gentamicin) o Bleeding: vii K 10mg/d for 3 days, plts/FFP/blood o Ascites: fluid restriction, tow salt diet o Hypoglycaemia: 50ml 50% dextrose if finger prick glucose <2mmotll o Encephalopathy: lactulose (30-SOmls/Shr, regular enemas to l
nitrogen forming gut bacleria, neomycin (short tenn only) o Cerebral oedema
Information for the patient
2

.,_, __
APPROACH TO A PATIENT WITH AN ABDOMINAL MASS
I. lutruduc«- tlae patic-ut
2. Rtlev:wtlla<kground Hx: l'aiuful moulh ulcclli, dianhoea, arthritis and weight loss Weight loss, fatigue, night swca~ Alcohol LlSeJabu.sc:, Dinbetes, previous hepatitis may give; cluCJ to the cause of an culargc:d liver (see hepatomegaly notes) Previous dy:icotcry: Liver ood colon nbstc.ssa ..
tlx of alcohol&. pain radiating to the back on the left (recent or remote) _, pancreatic cysts/pscudocysb. Rcunt infe<:tion e.g. vimi(EBV), pamsitic (malaria), bacterial (IB) may explain an enlarged 5plccn (sec 5ph:nomcgaly DOtes} Painless jaundice, wcightlos5, dark urine, pale stools DM, ~g""ic overuse, pallor, fatigue, yellow tinge to slcio, bone pain, dyspnoea and ankk:iwcUing--> think cluonic ccnal failure (look for signs of OM, polycystic disease, Gout, Slll, n:ual tumour, amyloidosis) NB: kidneys usually swaU but""'' be fin the conditious noted.
ABDOMINAL DISTENSION
UUQ !\-lASS ~ liver untU pronu otherwise: see notes on hepatume::aly/ HSlli
4. History Mention positive findings as well as iruportaDt negative findiags. Also 111entloo wbat WILS
looked Cor. S. Examination:
CeDcral: J: Db for suspc<:tcd liver/paru:reas/splcen pathology; A: nil .rploen & lr/Jlney; duhblas: nb mo (csp.Croho's, cirrhosis, m lympboma, bronchial ca & 111 (whlcll may }liver /spleen or CIWSc 2• GIT ca); Oedema: thlnk RI)AI Cill5CS, cardiac c~U!CS, livcrfa.ilurc, pelvic tumour, Conn's IWDOur, L: may sugg~t infective or malignant pathology. . Head: chtc:k the eyes for arcus comcalis, lUUltbomas and Sx of dlabetic:JHT retinopathy etc -+may be NB io. a paUQOI with a suspected ccoal mass; purpura 11111und the eyes loa patiten wilb an t•plecnlkidocy may bcip with a dx of a111yloidoals; lllJ•os perulo: sarcoidosis; malar rash: SLE; features ofsysiCIIIic sclerosis; moutlo & phlU"YDlr! Sl<of aptbous ulccn, candidiasis, infectious mononucleosis MSK: look for fcalllrc ofltA, gout, or other forms of artbtitis (plus aystemic manifestations thereof) CVS; pul5c nttc (taclly in infections), measure BP (T in DIOst eoal disease), munnw-a (IFJSBH) signs of bean fal)ucc, friction cub'pcricarditis, pulsus pa.radoxus; Rcspllatocy: may Sllggcst Infective or neoplastic causes of abdomloal mass; look forfeatw:es conslslcot with malignancy (e.g. bncbio.l plexus patboloCY, horner's) or TB; .keep satcOidosis in the hack of your mind.. Abdo: obviously a palpable mass in a speciftc quadrant plus any features of disease lo tbc relevant organ system Look at the sleW; collateral vessels etc for clues to uoderlyiog diseAse Neuco; Horoer'slhrachill plexus fullout (lhinkpaocoast tumour· with 2' spread to livcr)cranlal nerve fallout (CN m ulooc llliiY be consistent with OM); !lapp Inc · tremorluterixls: liver or kidney fnilurc; proximal myopltlby (thlolc DM}; porlpboral 11europatby- glove & stockiog (think DM) ; altered DlD<Idlal;ecp-wakc cycle ravena! -lhiDk bep..Uc encepbalopalhy;
7. Treatment: --> accordiDc to underlyiot: pathology 8. lllformatlon for lhe patient
2
_, .. ~ .. -- .. --c-Approach To A Patient Wit'\6~~!!':.,~1
1. Introduce the patient
2. Relevant Baekground History Known malignancy: esp. ovarian, hepatic, peritoneal Hx of chronic Hep BIC. alcohol abuse Young female with other autoimmune disease {e.g. DM, UC. glomerulonephrills, AI thyroiditis. pernicious anaemia}->? autoimmune Uver cinhosis Cardiac failure (known or suggested by PND, dyspnea, orU10pnoea, peripheral oedema, poor effort tolerance, typical drug therapy)
. K.n.?~P l!i?I ~~~!!P.!!.tla:...,. . . 'Cona1tldns assoc w1!fi !JXll,lliU,QWI0~!£118: nephnolc syndrome (see notes). PLE, malnutrition; "" Pancreatitis CTD lvascuHlis Hypothyroidism Chronic renal failure + Hx of dialysis
,..,~., .... l~-:~~~i~d~;w&litiiiWJ!!i~:~c;~~~t:.~~J~.~~~,.~,J''""'~'~.·-~ !:s~!!,iU Vllli\i' ' . · .. ~~ saii.!!H!."""""'!! . 'lilr:o'lml~~'i&Ul
,: ,~~~f~Iti~'~i;:~~s:~m~~"·lmjr 3. Clinical Problem
Thls is a patla111 with known (If a known disease present) currently presenting with asciles {-. I can reasonably suspect ascites because tile following are present: abdo distension/ flank fullness, shifting dullness to percussion, t fluid thrill: eversion of the umbUlcus. hemialstriae.tscrotal oedema,± right sided pleural effusion (hepaUc hydrothorax) all of which suggest fluid In the abomen > 1L). The aetiology of tile . ascites is mosl tikaly;
~.gn~f1finlil~iili!lm2~~1:1~~~!~~~~!:~~~~:~~~~
4. History: Mention poshive findings as well as negative findings: I.e. what was enquired about.
5. Examination Directed at fonding underlying disease:
Over cirrhosis (so examine for sx of chronic Hver disease), features of maUgnancy features of cardiac disease
• featur!l~ p!.J!'I "'ftiil~stive of autoimmune pathology
6. Speclallnvestlgatlons
Diagnosis may be made cllnlcally when lluld > 500ml Diagnostic paracentesis: (do on most paUents) o Ce I and dilf!'r at · o em g ucose U In Ca & TB). albumin. protein, amylase [> 1000u/L
~'ll.uc ascites), trlglycerldes)
o ~-u ure & §.f.l!l~lt¥.!¥,!lti!J! ~~l!l o olii'QY.tusualty pos1hve fiij)eiltoneal carcinomatosis) o ~liiiik TB
'A2h'b M":bz
Relevant 'other' bloods as dictated by suspected uonderlying pathology Imaging: U/S, abdo-XR, CT os appropriate
7. Treatment Therapeutic paracentesis (safe if albumin given concomitantly) · Medical: o NaCI restrictlon o Diuretics (splnonolactooe, furosemide) o Aim ofr 0,5 kg loss per day to l chances of precipitating ARF o 1kg loss per day if peripheral oadema present Surgical o LaVeen shunt (old),TiPSS, liver transplant
8. Information to the patient
2
~.z Tests suggesting hepatobillary disease
6.3 Miscellaneous Tests
FBC, ESR & Diff: Delccts: anaemia (macrocytic most Ulcely), sickle cdb, malaria (111ust do smears IJld serology as well}, t WCC (sllggcstivc of type of infection),? lcu.kacmiollympboma, raised ESR could Nggest TB, ulallgnancy, autoinuu\lllC: disease CRI' Blood glucose Hcpalitis acrology as dict.old by lh and findiogs konprofilc Auloimlnune marlcCD as IICCCSsary (hypcrgammaglobulillllemia, ANA, RF, anti-SM, anti-KIM); Nil: tllCSC patlc:ull way have .flt.bcly +viral serology (csp. anl.i·HCV)
z. Treatment; ,. Cinbbsb 1111d portal fiT: lifestyle cluwg .. , diet, sympto111atlc, acutc·livcr JAilun: aod TIPS Vinll bepatilis : bospllallsc if coccphalopatby, coagulup~lhy, seven: vomiting, · bypoglycacotla, otherwise: supporllve rx; ifbcpC-+INF & nbsvirln; ifHcpB .... INFa, lam.ivudinc, adefovir Autoimmune: s~Craids aod otber immUWISUppteSSanl Rx.
8, NB Erplaln the disease to the pa!lenl
•how to describe an enlarged liver. Siu: em below costal margin Surface:: smoolh or .irrcgtilor Edge: SQlOOth or mgular Coll.listcncy: sol\ or bard 7rcodell1CS$ ? pulsatile Audible bnlit
ADlliTONAL TOPICS wurtb nadia& Ia Oxford HCM Hercditary hacrnochromatosis pg 2S4 al· antitrypsio deficiency pg 256 Wib011's disease pg 257
3
... •.

PORTAL HYPERTENSION
fatbouhysiolugy Cbau<teri<ed by prolonged elevation of portal venous pressuu (ourmal: 2-5 wwll&); }'Is wita clinical features usually have portal pressure of > llmmHg rn:5S\I£C + flow X I'"C)iSlaucc Uulikdy that 1 flow 01lonc cao cause porl:d HT ( ;aUbough d~scribcd in AV fistula or tnassivc: splcoomegaly) 3 sites ofT resistance (i.e. causes):
Cl!aisal Featuru • Mainly due to ponal veoous congestion and collatcntl vessel formation.
N;;,BSPLEN~~()~Y~~.c~~!.f~~. la(pl bcwSO 100 109n) ltyPtis\c.Wiui li>a): occur: ICSWIS 1D ..,.uwuucytopaeo IS - X , ... CoUatc.ral vesscis on the utcrior alxlomioal wall: may result io Caput rucdllS;I or "CruveiUU.:rBaumgwtcu syndlowc" -a vcoous bwn over a large collateral vessel Most' clinically NB collateGJJ.oi occur iu stom•ch &. oesophagus; can cause severe bleeding. Rectal varies way be mistakcu for haemorr)loids. Fetor hcp~tit:us rc:ndts from portosy,lcmic sbunling of mctcapUJm dirctlly to lhc lWigs, Jfllvcr failwc is pn:.scut + portosys~mlc shunting -.hepatic encephalopathy cao occur.
~ompli<al!ous V ariccal blcclllng Congestive autropalhy Hypcr.iplcnism Altcites Rc:n•l failure Hepatic encephalopathy
luves!lcatlogs • Radiological and endoscopic evaluation of the uuper GITto exclude varices
Imaging (UIS) can shoiv hypcnplcnis, c:oll.otcral vessels, portal vein thrombsosi Portal vc:JlOgrapby shows tl>e site (possibly the cause) of portal venous obstructinn
~f aD2ogement • D-bloch:rs (propranolol, oadolol) and nitrates ! the risk of variceal bleeding
Shunl:i: o Goal is to 1 porto! venous pressure
o TI1W1jugular intr.lhepatic portc.systcmic shunt (l'IPS): intcrvculion radiologist creates shunt btw portal and hepatic veio via A catheter io .the liver.
o Can be used to stop acute bleeding or prevent rebleediog o Rare shuot5: portocaval and di!:tal splenorenal (Warren)

CIR.RllOSIS
Odioition: diffuse, incvcrsible fibrosis witlt hepatocellular nodular n:geocrntion. Any condition leading to pc:rsisu:ut or recurrent hepatocyte death may lead to hepatic cirrhosis.
ND: decompensation implies Ute development of ascites± t bilirubin± encephalopathy ± TINR
Palhuge-oeshj
l'olbology;
Stellate cells arc activated by cytokiru:o relcascd by other cell lyJ><'> in the liver (hepatocytes, kuppfcr cells, pits & lymphocytes) Cells then pc!peruatc their own activution by sySillhesis ofTGF p and PDGF Netttcsult is inflammation with fibrosis, widc:sprCild cell death, wilh nodules of hypcrprolifcr.oting survwg hepalocytes IL-6 & 13 =by T-lywphocytcs Wllammatianaod further fibrosis.
Changes usually affcctlbe whole liver with loss of nonnal an:bitetture and vascttlaturc, with the fonnation of portosystemic shwls. Microoodlllar type: nodules < lmmm, seen in alcobollc disease Macrooodular typc:as)'UliUCait, large fibrous scan.
Clh!lnl (eaturu; • May be asymp1oiWilic, or have isolalcd hcpalou~egaly • . J'req CODtplainiS: Weakness, fatigue, UtUSCle cnunps, weigh! losS, au.orc:xia, nausea,
votiliting, RUQ distomfort Jlepatomcg-ly (csp. early alcohol&. blll:mochrolllitosis) .Ascites Circulatol)' changes (spider naevi, cyanosis, palmat erythema) EndoeriDc Blccdin& ~ncy Portal HT Hepatic encephalopathy Clubbing Parotid colargemcnl Nail chan,gcs (l<:ucouychla, Terry's nail!)
Definitive: biswlogy on biopsy Suggestive; liver eu2)1111e5, bilirubin. INR. t gamma globulin lolbumin Imaging: ll/S, CT
Meuaee111eul Rx undcrlylog cause&. stop all alcohol Maintain adequate nutrition Jtx COIUplicatJnns
Comot!catlogs;
Hacmatolol(ical Renal Failure
PWJCytopacuia (hypcrsplc!Wlm) . Pre-renal (over diuresis) arull clotting Fx--> end result . ATN is bleeding, infx & sepsis . Hepatorenal syndrome
Hcmuooulmonarv svndrolllll . Liver cinbosis . Blood g .. abnormal . Pubn. Vasculature abo. . AU due to flli.lutc of liver to clear or prodl.ICC circulating pulmonary vasodilalory substances
Other factors : nutrition, alcohol consumption, ascites, varices, encepbalopalby, albumin, JNR, Bilirubin, creatinine
2
--VIRAL HEPATITIS
(see jauudicc notes for approach to a patient with jauudice)
Couuuun cause ofjawuJicc:- nwst Lc considered in anybody presenting with "hepa1i1ic• fcatw-cs
oulFTs (high transaminases, typically 200-2000 Ull; ALT>AS1). Viruses differ ill their teudeucy to cause acut<> vs. chronic inf<etion ( Hcp B, B+D. C, but !!Q.I.hL!D
A CUT!! INFEC110N Acli•I•GY' llcpatilis Viruses (A.B,C.D,E); Olher viruses .(EBV, CMV,lUV, heqxs, yellow fever)
1. cliu.ical f.:ah&£e5: a. non spc<:ific prodromal illness: headache, myalgia, arthr.tlgia, N& V, anorexia± dark
urine &. pale stooiJ b. prodrome precedes l.bc development of jaundice by a few days ID 2 weeks c. ,vomiting&. diarrhoea may follow . d: 'liver tender but minimally ca~argcd c .. • awld splenomegaly &cervicallympluadenopalhy in pts with EBV. f. Symptoms last3-6 weeks
2. lnvuligatiou:
~~~flW.iii~~~WDtiili'lt;W>~iit~tifil~mYi:bl'l ; . -· · · . .withlt\LT>.~:~;:::: Bilirubiai' · · :'. · ::. :·__ :';.c:s
.·1·
4. Mnagea.aenl:
Most pis don't need hospital care Avoid sedatives and narcotics-+ poor liver metabolism No •pc<:Uic dielal}' wodif"scatioos nee mary Avoid alcohol during acute illness Avoid eloctive surgery during acute illness: risk of post op liver failure
CHRONIC IIEPATJTIS llefiuitl•u:
1 transaminascs for> 6 months; requires liver biopsy to determine severity/ need for trutwcnl
Acllology: Viral (HUV B, B+D; C; not A or E); Drugs (mchyldopa, INH, amiodarone, uotrofunntoin); Autoimmune; seoetic (Wilson's, al-antitrypsis deficiency); metabolic (NASH)
CUnlcal featuces: Often asympromaric; constilulional sx.: futiguc. malaise, anorexia, weight Joss; Sx of chronic liver disease (see ootes); finn h~patomcgaly +splenomegaly; T AST, ALT.
HEPATITIS n: ..... one of the most CODUDOD cause of chronic liver disease and hepatoctllular Ca. ([or npter on HBC m Davison's v• 967-81 Hcp B virus consists of a core containing DNA and a DNA polymerase enzyme needed for vii\IS replicatioo. The core is surrounded by a surface protein. THe virus and •n ccess of the surface protein {=surface antigen) circulate iu the blood. H= ace the only soun:c of infection. Nb since both HIV and Hep B require reverse lraoscriptase to rcpliCllte, some NR Tl's are effective in both HIV and HepB (Tcnofovir, Lamivudinc end Emtricitabinc) lUnate oftraDJmlssloa.: horizontal {10% risk of chronic lnfx): !VDA, tattoos, unscrec:ncd blood, sex
Vertical (90% risk of chronic infx): HbsAg positive mother.
Prof'RosJo~aw1.s mnempalc "SECCES1'
Maa•eemeot; l.A~:uto~
supportive. l. Cbroa.k::
110 drug is able to eradicate HBV compktely. The inwcation for Rx b a high vin.lload in the ptcscnco of active hepatitis (Think+ HBcAg) and elevated serum transamlnascs. Options Include: . • a-interferon: augments native immune response. Most effective in piS with low vbatload
and aansamirlases > 2x upper level of nonnal Lamlvudinc: NRTI: inhibit DNA polymeuse and suppresses HBV-DNA levels. long tcnn therapy limited by mula lions. Adefovirffcnofovir: nucleotide analogue (ic. NtRTl). Effective In suppressing most of !he lamivudine induced DNA polymer3se mulant viruses Uvcr transplantation
2

UVER NEOPLASMS '
BENIGN --1.-Ca .. rnollS D:&!'m:Wgioma
MoSI common benign hepatic tumour due Ill malformation of angiopl;..W: fetal lissuc; Risk fac10rs: steroid lhclapy , females, cslrogell.l Clinical fooatl!'cs: usually small .&. as)'JupiOmatic; large tumours may cause painltliscowfort; ~kwilh rupture if large. Trcanncot: now:; or cxci$lou by lobectomy or enuclcatioo
1. AdeJlom" Benign &)aodular cpid:u:lial tumour Clinlcal D:aeurcs: as)'lllpiOmatic; but 2S% RUQ pain/mass Rx: stop slcroids or OCP & Excuo (due to risk ofllllligiWIC)I or spontaneous 1\aplun:lbnemonbogc
3. Focal Nodular Uyprrplasla
MAI.!GNANT
PRIMA~Y
Thougbllo he due to local ischemia wilh tissue ~egcncr.ujon Asymptolllillk, mcly grows or bleeds, no wallg,nW potcplial Tn:alm<ut: may l>c di.fficull to distinKUisll fon11 ad.cuowa: thus JCSect
U•ually hepaCoccUular calbcparoma OlbcQ include: angiosarcoma, hepatoblastoma, haemangiocndothclioma 20-25% of all carcinoPIII$ in A1iica ~k fattors: · o Chronic liver inflammations: chrllllic HBV/C, cirrhosis, bacmochromatosil, al-antillyptsiu o Mcds: OCPs, slcroids o Swokin& &. alcohol o Chc:mil:llls: aJiatOlliJI, vinyl chloride Clbllcal fclll11ra o R.UQ dlscowfort, rigbl sbouldcr pain 0 . JaWldiCC, wcalr:w:$5, filtigue, Weight loss, fever o HcpaiOIIICgaly, bnJlr, rub o Ascites wilh blood o l'anwcoplastic syndrulllCS (e.g. cushing's, bypoglycaemia o Melli: lupc, boiiC, brain, jlC{ilooeal seeding Iavesli,alia.., o · ~lllcd ALP, bilitubin,llldu-fciOproleiu{80"/.ofpaticD!s) o tvs, cr. MRI (best), angio~:IJpby o biopsy Treahacat o Cinhoois is a relative contraindication to resection due 10 i hepatic reserve o Surgical n:oa:liou or tranSphlol l'rogQosu o 70Yo have mets 10 uodcs & lung II prcsc:lllalion o Survival without treatment : 3 lllODlhs
o S yC<Il' survival: x !Wo
SECONDARY Mo.st COllllllDD hcparic: malignancy Causes: GIT (most toDUJ\OU), IWlg, breast, pancreas, ov;uy, ulcrus, kidney, gallbladder, prostate ' Rx: n:sc<:tion if co otto! of lhc primary tumour is possible, uo extrahtpaticc or Clltrapulmooaly JDCIS Prognosis: 30-40% j year survival wilh "curative• resection.

..
·)>· .SLE )> Systemic Sclerosis )> Mixed Connective Tissue disease )> Relapsing Polychondritis )> Dermatomyositis & Polymyositis )> Crystal Arthropathies
-Gout -Pseudogout -Apatite deposition disease
>RA > Sero-negative spondylarthropathies
-Ankylosing Spondylitis -Reactive arthritis . -Psoriatic arthritis
> Sjogren's syndrome
ou-lcs~~"'"'ur;d aorcJ,hcns
~ dcJ

Auto-immune Connective Tissue Diseases f: Systemic Lupus Erythematosus
Definltjon; Multi-systemic iilJto::lmmuna.dlsease wher~ @.Uto-~!1tlbodles (via B-cells) are pr9Q.!:!_ced against auto-
-~ns an<r deposited In organs- Damage · · ·~·- • · · ·- -
Pathooenesls: • Genetic predisposition _, abnormal immune response ~ auto-Ab and immune complexes - Inflammation
-Damage: o Rena failure o ·,Atheros·· erosis o - mo osis 0~-0 Damage from Rx
Clinical Features: > 4/11 =SLE S - Serotltls
o .f'..w.mti:; ..... dyspnoea +1- effusion, Pleuritic chest pain o Pericarditis-+ chest pain, ECG changes, pericardiai.Rub +/-effusion
0 ..... Oral ulcers · o Oral or nasal. Usually painless and non-errosive
A -+ Arthritis o AffeCts 90% ppl o > 2 oints 'nful. tender. swollen +1- effusion o Capsular laxity eads to reversible deforming arthropathy ..... Jaccould's Arthropathy o Aseptic bone necrosis
P --. Photosensitivity o S_un-exposed are<l$-o SUNBLOCK o May cause disease flare up
B--. Blood · o Haemolyticanaemla o Leucopenia > 2 occassions •
•
Drug Induced Lupus: INH Hydralazine Procainamide o LymghoQ~ia> occasions(< 1.9 x 10 9
)
o Platelets < ·1 00 In absence of drug effect • "'*- R .... Renal .
• •
Chlorpromazine Phenytoin Msoclated with anti-histone Ab In almost 100% of-cases
Aetiology :
o Persistent proteinuria> 0.5gld (3 +on dipstix) o Cellular casts __. red .ceiVgranular/ mixed
A-+ANA .....
o +vein> 95% I - Immunology
o Anti ds DNA-~ or Anti- Sm Ab or Anti phospholipid Ab+ based on: o t lgM or lg'tror.anticardtohptn-;s;b, +ve lupus arlllCOagulant o False +be syphlns > 6 months_, confirmed by -ve Treponema Pallidum immobilization
N _. Neurological o fvloyemend d/o or~urooathy o Seizures/ psychgsts unrelated to Drugs/ toxins/ metabolic factors
M .... Malar (butterfly) . o Fixed erythema (flat/raised) over malar eminences o ·spannt nasolabial folds · o Found hi-Y. patients
0 .-. .O!?coid Rash o Erythematous raised patches on ears, cheeks. scalp, forehead or chest o 3 stages: _erythema- pigmented hyperkeratotic o_:der:na~~~s ?~~~~~~_,atrophic lesions
Relapsing remitting course Fatigue Pyrexia In flares ! weight, alopecia Non - infective endocarditis
PLUS
o (Libman Sacks Syndrome) Migraines (40%) T CVS risk Osteoporosis Vasculitis
Auto-Immune. 0.2% population )>:d' 9:1, typically women or child bearing age Also common in Caribbean's and Asians Immunology:
Anti-phospholipid Syndrome • Ab against
Type 1: primary Type II: 2ndary, assoc with other auto-immune disease
. esp. SLE • Antl-phosphoilpld +ve = anticardiollpin + lupus
anticoagulants
Cause Fea!.\!res of; C: cc:iagulation defect- Straka, CVS, Renal L: livedo reticularis 0: obstetric ... recurrent miscarriages T: thrombocytopenia
Management: Low dose Aspirin I warfarin Advice in preqnancv
I
J
I.
' L

o > 95% ANA +ve o Os DNA almost exclusive fD SLE o Other assoc Auto-immune diseases: SjOgren's Syndrome, auto-immune thyroid disease (5 -
10%) .
Special Investigations: • Anti ds DNA ab
Complement: C3 C•l ESR Bloods
0
0
0
FBC, U&E, LFT, CRP {often Normal} Think of SLE If ESR j but CRP normal
Urine 0
BP
.6~·
If both t think of Infection, serositis, arthritis
Blood or protein
· ·.; _ i_ .. ..
,, .. · .. , , .: ,u
.· .. '
•
•
•
General Management; High dose.or~doisone =!: cyclophosphamide for severe flare-ucs e.gaemolytlc anaemia, nephritis, pericarditis, 'eNS disease Low dose steroids In chronic disease
. Hyroxvrll!gmguiA.Jn joint/ skin Sx uncontrolled by NSAIO's
0 SfE: irreversible retinopathy -+ baseline + annual F/u
Remember lmmune-suppressvle therapy makes pt more liable to Infection Lupus Nephritis:
o Steroids + cyclophosphamide o S/E: myelosuppression, alopecia, Infertility,
haemorrhagic cystitis
< ·' ··. -·

Systemic Sclerosis
Definition: • Chronic systemic disorder of unknown aetiology characterized by skin thickening (scleroderma) and
involvement of Internal organs (fibrosis)-+ Heart, lungs, GIT, Kidneys
Epidemiology; Peak age of onset 30 -50 Sex d':~ 4:1 , prevalence 10-20/100 000 Genetic association Environmental Factors:.
o Chemicals: toluene, trichloroethylene, benzene o Drugs: bleomycin. pentazocine, L-tryptophan
Pathophysiology: Genetically susceptible individual" _. initial vascular injury -+ functional & structural vascular alterations -:+ inflammation & auto--Immunity-+ Initiated and sustained fibroblast activation & differentiation _, . pathological librogenesis and Irreversible tissue damage ·
Classification: 1: Diffuse Scleroderma -+ Skin thickening of trunk, face, proximal + distal extremities
II: Limited Sclerodenna - Face, neck, distal to knee and elbow -+ CREST Syndrome
Subcutaneous calcinosis Raynaud's Phenomena Oesophageal dysmoUDty -+ hypomotile oesophagus Sclerodactyll
• Telangiectasias
Ill: Sine Scleroderma .... No skin thickening but organ Involvement, vascular, serological
IV: Overlap .... Ox of Sse + SLE/ RAJ Inflammatory muscle disease
V: Undifferentiated -> Raynaud's phenomena with clinical and lab features of Sse -+ S-anti-centromere Ab, abnormal nail folds, finger oedema, Ischemic injury ·
Clinical Differences:
Limited Sclerodenna Diffuse Scierodenna
Long duration of Raynaud's Short duration of Ravnaud's Puffy flnqers Swollen hands and feet Slow progression Rapid progression Mild constitutional Sx Many Constitutional Sx
• arthalgias • arthalgla, carpal tunnel Syndrome Most common presentation All organ Involvement . oral ulcers • pulmonary Hbrosis
• oesophageal . cardiac and renal crises (most common cause . small bowel t) • oulmonarv fibrosis
Pulmonarv HT In 10% Pulmonary HT rare Anti-centromere Ab 50-90% Antl-centrom ere Ab 5% Anti-Scl-70 Ab 10- 15% Anti-Scl-70 Ab 20- 30 % . topoisomerase I
Management: Immune-suppressants e.g. lVI cyclophosphamide-+ In organ involvement
• Joint I Tendon Involvement o Pharms:
NSAID's, analgesia, !. dose corticosteroids o Physical:
aggressive physiotherapy, flexion/extension exercises, splinting not well tolerated • GIT Involvement
o Heartburn Antacids, ClmeHdlne ,PPIIIke Ompeprazole
o Dysphagia/vomiting Reflux Rx, eat upright, proklnetlc drugs oesophageal dilation
o Nausea/vomiting/bloating Prokinetlc drugs
o Dlarrohea
.I
I

Definition:
Proklnetics, broad spectrum Ab o Bloating/pseudo-obstruction
Conservative decompression, avoid surgery Antibiotic trial, prokinetic drugs
o Constipation Stool softners, bulk to stimulate muscles
Pulmonary interstitial alveolitls o Cyclophosphamide and steroids
Renal Crisis o ACE~!
., .. -. Mixed Connective Tissue Disease
• Meets criteria for SLE, Sse and polymyositis Debate wnether this Is a distinct disease
Relapsing Polychondritis
Definition: • Affects cartilage: pinnae ()floppy ears), nasal septum +/-larynx (stridor)
Assoc: aortic valve disease, polyarthritis, vasculitis • Rx: steroids and immune-suppressants

I Dermatomyositis and Polymyositis
Definition: · Progressive-symmetrical proximal musde weakness due to striated muscle Inflammation Muscle weakness may also Include
o Dysphonia o Dysphagia o Respiratory weakness
• /" t risk of malignancy esp. Dermatomyositis
Diagnosis: • Muscle pain and proximal muscle weakness
t Creatinine kinase Abnormalities on EMG Diagnosis confirmed by muscle biopsy
• Auto-antibodies .... anti-ml2 and anti-Jo1
Non-Muscle Causes of Weakness Episodic
· l. BP, hypotonia • HypervenHiation
Hypoglycaemla • CVI
Anxiety attacks Persistent
• Anaemia Malignancy Malnutrition
• Organ failure Clinical Features Dermatomyositis skin Signs:
• Malar rash Includes nasolabial folds Metabolic -o hypophosphatemia, hyperthyroidism, hyperparathyroidism
• Heliotrope rash on eyelids ±oedema (lilac purple rash) • Chronic/ acute infection
• G~ra~~~~ · ~ Nail fold erythema (dilated capillary loops) 1 ~
o Red papules over knuckles, elbows, knees A o Pathognomlc If T CK and proximal weakness PpcD6 ·
• Subcutaneous calcifications • Mechanic's hand's
. o Painful skin cracking of tips and lateral aspects of fingers Extra-muscular Features:
o Fever, arthalgla, Raynaud's, lung fibrosis, Myocarditis
Special !nvestlgatloos: CK
• EMG Investigation Pathological Process Findings
Muscle
Heart
Lung
Skin
GIT
Auto ant1bod1es
Management:
Jo1 PM Sci nRNP
Screen for malignancy Prednisolone
Biopsy
EMG
Gallium Scan ECG, CXR Biopsy
CXR Radionucleotide Biopsy
Biopsy
X-ray
Inflammation and fibrosis -Myoffberdestructlon
Inflammation Myocarditis, Fibrosis i\/!yocardltls, Fibrosis
Inflammation and fibrosis Inflammation and fibrosis Inflammation and fibrosis
Inflammation
Inflammation and fibrosis
Polymyositis 30% 10% 10%
Mononuclear cell infiltration Low amplitude short polyphasic potentials t Uptake in affected celts LVH, arrhythmias,, myotlber size varta!lon, mononuclear cell Infiltrates Interstitial markinqs V/Q mismatch Destruction of alveolar space and fibrosis Vacuolization of basal cell layer, mononuclear cell Infiltration Reflux and unco· ordinated peristalsis
Dermatomyositis 5o/o <5% 5%
Immune-suppressant and cytotoxic Rx- resistant cases o Azothlaprine, methotrexate, cyclophosphamide, cycl.;;.osiil;p•<o.,n.,niiie,_ __________ ...,.
Monitor course of illness r o Muscle Sx o Muscle strength • o Lab studies
.. • •
Diff Ox: Carcinomatous myopalhy Inclusion body myositis Muscular dystrophy Endocrine/ metabolic myopathy Rhabdomyolysis Infection (HIV) Drugs
-
" 1 i

Approach to the Painful/Swollen Joint
., Degenerative
>50 yrs Worse with usage Improves with rest No systemic Sx Weight bearing joints
OSTEOARTHRITIS
MONOARTHRmS
I GOUT I Podagra Olecranon bursitis Tophus Finger/ ear (may be small and ulcerated} -!Temp
! Urate solubility
..
-.f0SEVDO-GOUT CHONDROCALCINOSIS (CPPD)
1 Apatite deposition I
I ~\c cl\-\AII:hs_
SYMETRICAL
l RHEUMATOID ARTHRITIS
Inflammatory
Any age group Morning stiffness Pain> 1 hr Improves with exercise Worse with lriactlvity Systemic Sx
POLY ARTHRITIS
ASYMETRICAL
1 SERO-VE SPONOYLOARTHROPATHIES
Group of disorders that share some clinical features .and genetic associations
Ankyloslng Spondylitis Reactive arthritis
• Psoriatic arthritis enteropathic arthritis Juvenile onset spondylo-arthritls

Deflnition: • Abrupt onset of aevere joint inflammation, often beginning at night
75% 111 attacks in 111 MTP joint • Usually monoartlcular, but can be polyarticular • Attacks subside In 3 - 10 days • Urate crystals present In synovial fluid • Hyperurecemla may or may not be present
Urate Svnthesls and Elimination:
Synthesis
Dietary purines
Purine Synthesis
H yperuri cem Ia: Overproduction (1 0%)
Ethanol MyelopcOiifecatjve DLO
Undarexceretlon (90%) Renal Insufficiency Drugs and toxins
o Diuretics o Ethanol o Pyrazinamide o Low dose aspirin
Clinical Picture:
Metabolism
Body Purine Nuc!leotides
Tissue Nucleic Acids
B> 1 Purines
Uric Acid
/~
~ Cb • Asymptomtlc hyperuricemia-. continues until1 st attack
§• ~ goutY aithn!ts • Interval hyperuricemia-. periods between attacks • Chronic tophus gout <9• Cx--+ kidney stones, nephropath;t
CAN BE SYMMETRICAL-+ DO NOT CONFUSE WITH RA
Diagnosis: Famll~ and history of attacks Typical clinical pic and gouty t~hi t S-Urate ..... may be N during attack Urate crystals In aspiration fluid ~ -
o punched out erosions, looks rat bitten o soft tissue swelling o sclerotic mamk!s
c c.
0 ( ' i~
Elimination
/' Internal Excretion
~ Renal Excreti\:APe 'iD~
~~· ifi -d:~~ ~· ~
ex)
i . r'\.o U<:.~v-.... . ~ ~
· ~~~ ~ -c9-cJ . -1'- "S _l.J.:<" c::>h ' \ U\ott c.~\n~ ~ kfZ-- . l o overhanging edges .........
Management; Exclude precipitants Lo~ diet and avoidance o~ .
o No foods with T purine content-. sardines, anchovies, liver, kidneys Acute Attack
o NO URIC ACID LOWERING DRUG -o ALLOPURINOL (can precipitate gout) o NSAIDS ot in kidney failure) o olchicine ~ C)o'LO-...._, 6-/or-f OlJ. of. j/">1\ 1 o \.2 -' _.) '7 v....r-c ICJ • Q Yl(' o Steroids in resistant cases q (Jnct:)n~ (Q 1Jed ~C){)ce}
.Job ret.t-1 rfbn-fir7 4 eo
_j
/ j

•
•
• 0
. 0
0
0
Pseudogout I Chondrocafcinosis
- Definition: . (E_-~~ C \P'i~U_ • CPPD -. calcium pyrophosphate deh)dfata..depaslt(o disease
Crystals seen on asplra!IOII of :synovial fluid, clinieal!y-often6foody c:~pi~ate
Clinical Features: Acute synovitis
• Chronic arthropathy Radiographic -+ chondrocalcinosis Common Sites for Deposition
o Shoulder, wrist ankle, knee, elbow, hlp
Associations: Family predisposition Ageing
• Metabolic disease } ~ o . Hyperparathyroidism :;: o Hypophosphatasla > o Hypomagnesemia ~ o Haemochromatosis ~ o · Wilson's disease g o Gout. ochronosis -o Possible associations
• .. lqjct insult. OA .-Not In RA . :---
.;·
Gout vs. Pseudogout:
Sex Ratio (cj':<j?) Peak Age Most common joint Serum Urate Radiological
• . Crystals
• . . Trjggers:
Calcifications Erosions
Type Shape Birefringence
Joint trauma ltnercurrent medical illness --. chest inf Surgery Blood transfusion Institution of thyroxine Rx Joint lavage Most cases spontaneously
Diagnosis: Synovial fluid - CPPD crystals
GOUT 2:1
40--~ ( '1' MTP ) '-~
None Characteristlr
MSUM Needle
Strong -ve
XR-+ calcifications, white LOOK FOR 1HEM!I - '
Management: Aspirate joint Symptomatic relief
-
PSEUDOGOUT 4:1
-- 6£l._ .... ,
( Knee ) NOmfal
Chondrocalclnosls Degenerative
CPPD Small rod like
Weak +ve
Apatite Deposition Disease h .• I ~ w\...tt:....~ \N'.~~ . ~>s\v 'N\ ~IJ'-J"'\N
Definition: - ~ . Uf \:::o"'-V=> ~~ · • Clinical syndromes associated wltn deposition of ~patite in and around Jomts
j/.... Subcutaneou~ Deposits: • like the calcification of hands in scleroderma
Asymptomatic chance finding Acute and chronic inflammation SKin ulceration 2ndary infection
• Pressure necrosis of surrounding tissues Mechanical Interference wltn function
..._ Periarticular Deposjts: Like calcification of supraspinatus tendon
• Asymptomatic chance finding Acute calcific periarthritis Chronic perlart/cuiar pain/ dysfunction
"'- Intra-articular Deposits: • Synovial and ~alge deposits in damaged joints • Asymptomatic chance finding
Acute synovitis Severe osteoarthrltls Destructive Arthropathies of older people
g {2,J.J~utvJAi(JtQ AI2.1Hf.2.17LS
~ All ct.doar->,...,..une.l ocrd•4'0r'.Q r>"1Dy prooerrl ;vAh da .
o {2,h<Jt,!Yl(datd N:dob 4> 8crt_Jj nJerrt; dr:;.;orrn ~-~~
r /Vl;tro/ Mt+ted
oltf1CB6 ·' Dcr:)ructf,vf:) J,~cose) 'r1Cd r><pek.nc;t/ /Jra'ye.rol'{d chseoco
(}0U1 n
OOids
..
J
\
i
1
J I
I r '·
l

• l r
Rheumatoid Arthritis
Pathogenesis: Interplay between infectious, genetic and honnonal factors Aetiology
o Mycobacterium o EBV o HLA DR4 t suscel)tlbility o Sex hormone implicated In t incidence in females
3 Stages: o Initiation of non-specific Inflammation o Amplification resulting In T-cell activation o Chronic Inflammation wfftl tissue lnfury
Diagnosis; • Early RA Sx and Signs not drar:NUc • JoinT pain and swellln with momln s • re omlnantly small joints, symmetrical
Difficulty making ftst, pain on walking, esp. on awakening Good response to NSAIDs
• Duration > 12 wks
American Rheumatoid Association Diagnostic Criteria • ~nrning stjffpess > 1 hr befor~.Jmproving for > B Wks
A-~A}:J • Arthritis of > 3 !oint 9reas Including
o . PIP, MCP, wrist, elbow, knee, elbow, MTP 5!hritis of hand join is ,Swmetdcal arthiffis
·~ Rheumatoid nodules • N +.!LS, • • Radiological appearance .
· o Erosions or periarticular osteopenla
>4=RA ~ 2 does not exclude RA
Clinical Features: Evidence of synovitis .
o J01nt tenderness, swelling/effusion, warm Systemic features:
o ~r. fatigue, L 1M Eye
o Scleritis, keratoconjunctivitis Lung
o Fibrosis, nodules Pleura
o Effusion Pericardium
o Effusion Spleen _ ____.-
o Splenomegaly Gut
o Amyloidosis Kidney
o Amyloidosis Bone Marrow
o Anemia o 'fhrombocytopenia
Musde o WasUng
Skin o Thinning, ulceration, nodules
CNS o Peripheral neuropathy, mononeuritis muliplex
. .
:!
:; ,,
,·
J .,
CharecterlsUc Hand Deformities: • Radrat devtanon 6t wrist ~ • J,Jtnar deviation Qf digits ~ V""'" Palmar subluxation of proximal phalanges (Z deformity) •1,./'S..)Van neck deformity--+ hyper-extension of PIP with cornpensat01y 1\exlon DIP • V13outonnlere-+ flexion of PIP, extension DIP · • "/Thumb-+ hyperextension of PIP, flexion of MP.:,.-.Ioss of mobility V Mallet finger · t/ Nodules ·
Characteris!lc_~etormitijf' ., Ever n of hindfoo
Planar subluxation of metatarsal heads • I§ Widening of forefoot .... • Hallux valgus
Lateral deviation and dorsal subluxaiion of toes
SpeciallnyeStlgatlons: XR . Bloods
o CRP, RF, antl-CCP - --:-- +ve In 80% , In pts prone to severe disease and will .benefit from early
aggressive RX Activity Assessment
o No of tender joints o No of swollen joints o Physical Sx · o Radiologic analysis
Morblditv In RA: ! life expectancy-+ Y.- Y. related to CVD Osteoporosis Lymphoma Infections Amylo~osls NSAID toxicity "Biologicals
· r\llanagement: General Principles:
• Pain relief L Inflammation Protect joints Maintain Fx Rx systemic Involvement
Early Rx: · Early aggressive Rx Window of opportunity first 2 yrs Combination± steroids then step down
DMARDS: Combine with low dose steroids DMARD toxicity not more than long term NSAIO use
Risk Factors for Radiologic Progression:
• Involvement of hand and foot joints • Disease > 3 months
~ 2 swollen joints • RF+ve
1 disease activity and penetration • 11 CRP
Use early to protect joints from damage-+ erosion-+ permanent damage Methotrexate
o lmhbits dihydrofolate reducta~ (purine synthesis) o Induces adenosrne release -+ anti inflammatory o Use weekly, combine with folate o Up to 20 - 25mg o Monitor for toxicity- pulmonary. Liver, bone marrow
Sulphasalazine ' .. · o Modulates 8 cell response and angiogenesis
Cl}loroquine .. · o. Modulates cytoklne secretion
TNF-<r:inhibitors o Rapid clinical response
TN F-a Inhibitors Saftey Issues: • Infection-+ common,
opportunistic • Pancytopenia, aplastic
anemia • Demyelinating D/0 • SLE like Sx • CCF • Lymphoproliferative D/0
~
~ ~~' \~
F
I •
1...
i .
i··-
i -
.I
l