Embed Size (px)
Citation preview

690
Introduction"It is the God given right of every human being to appear human". - Ernest L. DaBreo
Eye is a vital organ not only in terms of vision but also being an important component of the facial expression. Most common tumors that affect the eye, ocular cavity, or the orbital region are Basal Cell Carcinoma (BCC), Retinoblastoma (RB), malignant melanoma, squamous cell carcinoma of the conjunctiva, and rhabdo myosarcoma; that may require partial or complete resection of eyeball or eyeballs [1-4]. Removal of this organ may be also be indicated in cases of a severe trauma, congenital abnormality or disease such as an infection or untreatable painful glaucoma This results in great difficulties for post-surgical rehabilitation, aesthetical recovery, and social integration of the patient [5,6].
Surgical procedures adopted for the removal of an eye were classified by Peyman, Saunders and Goldberg into three general categories: Enucleation, evisceration and exenteration [7]. Enucleation is a surgical procedure in which the globe and the attached portion of the optic nerve are excised from the orbit. Evisceration is removal of the contents of globe while leaving the sclera and extraocular muscles intact. Exenteration is the most radical of the three procedures and involves removal of the eye, adnexa, and the part of the bony orbit [8].
Orbital rehabilitation is a complex process which requires specificity in technique according to a particular patient. An orbital prosthesis is created to restore a more normal anatomical structure and cosmetic defect created by these conditions in a person. Prosthesis is generally constructed after complete healing (usually 2 to 4 months).
A successful facial prosthesis depends on several factors like durability, biocompatibility, flexibility, weight, color, hygiene, thermal conductivity, ease of use, texture, and availability. No maxillofacial material has all of these ideal properties although several materials are available that possess most of these properties with increased tear resistance and tensile strength and significant durability [9-11]. Prosthesis for orbital defects is made from a variety of materials, such as
poly(methyl methacrylate), polyurethane elastomer, silicone elastomer or urethane backed medical grade silicone. Silicone elastomer is widely used material which is relatively color stable and can be colorized very easily. They are mainly retained using mechanical means of anatomical undercuts, spectacle frames, magnets or by the use of osseointegrated extra oral implants [8]. Present paper highlights a simple and economical technique to rehabilitate a patient with silicone orbital prosthesis.
Patient and MethodsA 61-year-old male patient had reported to the Department of Prosthodontics, All India Institute of Medical Sciences (AIIMS), with a chief complaint of missing right eye since 6 months. Surgical exenteration of the right eye was done due to fungal infection. Patient gave the history of diabetes for which the patient was put on insulin for the past seven years. Extraoral examination of the patient showed a large orbital defect on right side (Figure 1a). A definite bony undercut was found on the superior border of the orbit which eventually helped in the retention of the prosthesis.
Orbital Prosthesis: A Novel Reconstructive Approach
Bhavita Wadhwa Soni1, Nitin Soni2, Mohit Bansal3
1Senior Resident, Department of Prosthodontics, Oral Health Sciences Center, Post Graduate Institute of Medical Education and Research, Chandigarh, India. 2Reader, Department of Periodontology, Daswani Dental College, Kota Rajasthan, India. 3Senior Resident, Department of Community Dentistry, Oral Health Sciences Center, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
Abstract Rehabilitation of facial defects is a daunting task, requiring an individualized design of the technique for each patient. The disfigurement associated with the loss of an eye may result in significant physical and emotional problems. Various treatment modalities are available, one of which is the use of implants. Although implant-supported orbital prosthesis has a superior outcome, it may not be advisable in all the patients due to economic factors. The present article describes a reconstructive approach for a patient with exenterated right eye using silicone orbital prosthesis which improved his psychological, physical, social, functional, emotional and spiritual needs. Multidisciplinary management and team approach are essential in providing accurate and effective rehabilitation.
Key words: Orbital, Prosthesis, Rehabilitation, Management
Corresponding author: Dr. Mohit Bansal, Senior Resident, Department of Community Dentistry, Oral Health Sciences Center, Post Graduate Institute of Medical Education and Research, Chandigarh, India. Tel: 09855701797; e-mail: [email protected]
Figure 1a. Pre treatment photograph.
691
OHDM - Vol. 13 - No. 3 - September, 2014
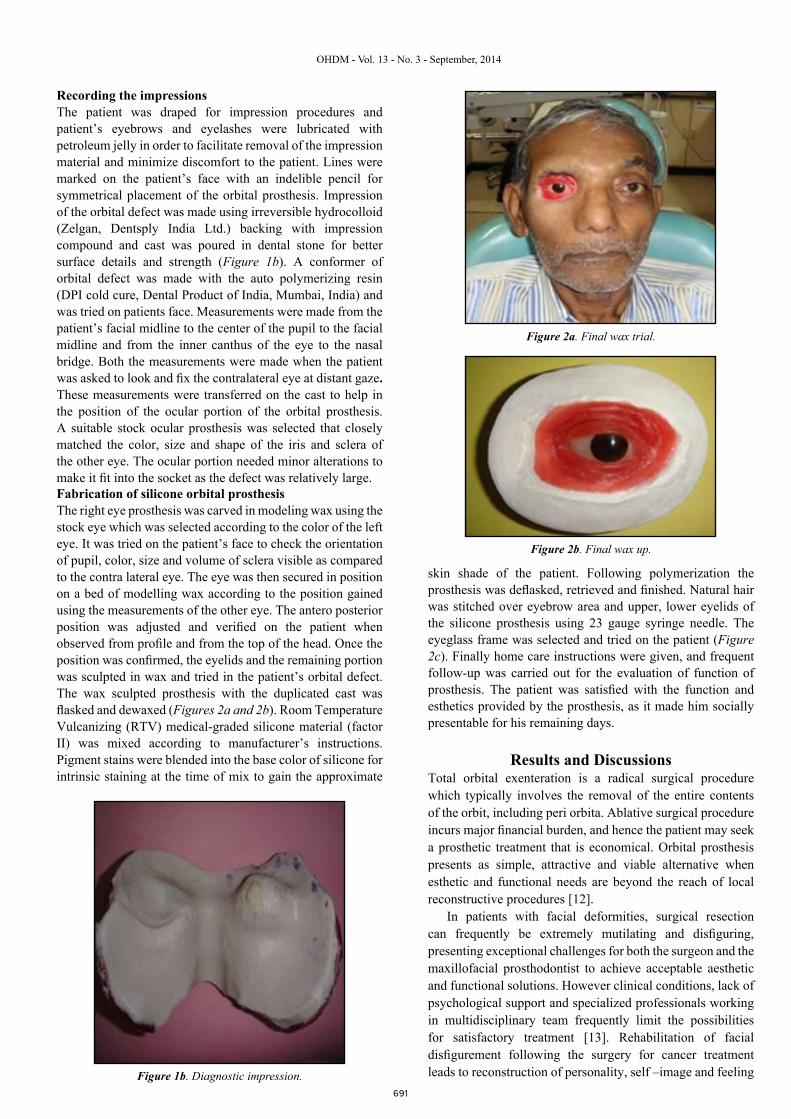
Recording the impressionsThe patient was draped for impression procedures and patient’s eyebrows and eyelashes were lubricated with petroleum jelly in order to facilitate removal of the impression material and minimize discomfort to the patient. Lines were marked on the patient’s face with an indelible pencil for symmetrical placement of the orbital prosthesis. Impression of the orbital defect was made using irreversible hydrocolloid (Zelgan, Dentsply India Ltd.) backing with impression compound and cast was poured in dental stone for better surface details and strength (Figure 1b). A conformer of orbital defect was made with the auto polymerizing resin (DPI cold cure, Dental Product of India, Mumbai, India) and was tried on patients face. Measurements were made from the patient’s facial midline to the center of the pupil to the facial midline and from the inner canthus of the eye to the nasal bridge. Both the measurements were made when the patient was asked to look and fix the contralateral eye at distant gaze. These measurements were transferred on the cast to help in the position of the ocular portion of the orbital prosthesis. A suitable stock ocular prosthesis was selected that closely matched the color, size and shape of the iris and sclera of the other eye. The ocular portion needed minor alterations to make it fit into the socket as the defect was relatively large.Fabrication of silicone orbital prosthesisThe right eye prosthesis was carved in modeling wax using the stock eye which was selected according to the color of the left eye. It was tried on the patient’s face to check the orientation of pupil, color, size and volume of sclera visible as compared to the contra lateral eye. The eye was then secured in position on a bed of modelling wax according to the position gained using the measurements of the other eye. The antero posterior position was adjusted and verified on the patient when observed from profile and from the top of the head. Once the position was confirmed, the eyelids and the remaining portion was sculpted in wax and tried in the patient’s orbital defect. The wax sculpted prosthesis with the duplicated cast was flasked and dewaxed (Figures 2a and 2b). Room Temperature Vulcanizing (RTV) medical-graded silicone material (factor II) was mixed according to manufacturer’s instructions. Pigment stains were blended into the base color of silicone for intrinsic staining at the time of mix to gain the approximate
skin shade of the patient. Following polymerization the prosthesis was deflasked, retrieved and finished. Natural hair was stitched over eyebrow area and upper, lower eyelids of the silicone prosthesis using 23 gauge syringe needle. The eyeglass frame was selected and tried on the patient (Figure 2c). Finally home care instructions were given, and frequent follow-up was carried out for the evaluation of function of prosthesis. The patient was satisfied with the function and esthetics provided by the prosthesis, as it made him socially presentable for his remaining days.
Results and DiscussionsTotal orbital exenteration is a radical surgical procedure which typically involves the removal of the entire contents of the orbit, including peri orbita. Ablative surgical procedure incurs major financial burden, and hence the patient may seek a prosthetic treatment that is economical. Orbital prosthesis presents as simple, attractive and viable alternative when esthetic and functional needs are beyond the reach of local reconstructive procedures [12].
In patients with facial deformities, surgical resection can frequently be extremely mutilating and disfiguring, presenting exceptional challenges for both the surgeon and the maxillofacial prosthodontist to achieve acceptable aesthetic and functional solutions. However clinical conditions, lack of psychological support and specialized professionals working in multidisciplinary team frequently limit the possibilities for satisfactory treatment [13]. Rehabilitation of facial disfigurement following the surgery for cancer treatment leads to reconstruction of personality, self –image and feeling Figure 1b. Diagnostic impression.
Figure 2a. Final wax trial.
Figure 2b. Final wax up.

692
OHDM - Vol. 13 - No. 3 - September, 2014
of having overcome the disease. These individual experiences are complex, challenging and have striking effects on their lives. Multidisciplinary approach should be opted for their reintegration into the society and reducing the prejudice and stigma of disease and disfigurement [14].
Present case came with an urge for cosmetic as well a social concern which was successfully treated by silicone orbital prosthesis that is practical, trouble-free and cost-effective. Selection of a reasonable maxillofacial prosthetic material and economically feasible retentive aid should be the goal of rehabilitating such pati ents. Since silicone has better marginal adaptation and lifelike appearance, it has been used for the fabrication of orbital prostheses.
Silicones have been used for over 50 years in the field of
maxillofacial prosthetics, with desirable material properties including flexibility, biocompatibility and ability to accept intrinsic and extrinsic colorants, chemical and physical inertness and mouldability [15].
The most commonly used conventional method to retain orbital prostheses is the eyeglass frames and anatomic retentive undercuts [16]. The patient treated in this report had a favourable anatomical undercuts in the defect which was used to retain the silicone orbital prosthesis. The silicone prosthesis has advantage of light weight, better esthetics with lifelike appearance than acrylic prosthesis. The thin flash of the silicone eye merged with the adjacent skin to give a lifelike appearance. Use of adhesive was minimal as prosthesis was retained by favourable anatomical undercut. So, the chance of allergic reaction caused due to the use of adhesives was reduced to minimal. Further, instead of sticking artificial eye lashes, natural hair was stitched over eyebrow area and upper, lower eyelids of the silicone prosthesis using syringe needle. This enhanced the natural touch to the artificial eye giving natural appearance.
ConclusionExenteration of the orbital contents with an ablative surgery can severely affect a person in terms of function, esthetics and psychological trauma. A well retained, user-friendly, removable maxillofacial prosthesis is the key to successful prosthetic rehabilitation in such cases. So, as a dental professional it is our duty to implement our knowledge into practicality and fabricate the prosthesis in an acceptable fashion to meet the physiologic, anatomic, functional and cosmetic requirements of the patient so as to boost ones confidence and lead a better life.
Figure 2c. Post treatment photograph.
References1. Heckmann M, Zogelmeier F, Konz B. Frequency of facial
basal cell carcinoma does not correlate with site-specific UV almol exposure. Archives of Dermatolology. 2002; 138: 1494-1497.
2. Aerts I, Rouic LL, Gauthier-Villars M, Brisse H, Doz F, Desjardins L. Retinoblastoma. Orphanet Journal of Rare Diseases. 2006; 1: 1-11
3. Bonanoni MTBC, Almeida MTA, Cristofani LM, Filho VO. Retinoblastoma: A three-year-study at a Brazilian Medical School Hospital. Clinics. 2009; 64: 427-434.
4. Chintagumpala M, Barrios CP, Paysse EA, Plon SE, Hurwitz R. Retinoblastoma: Review of current management. Oncologist. 2007; 12: 1237-1246.
5. Goel BS, Kumar D. Evaluation of ocular prosthesis. Journal of All India Ophthalmol Society. 1969; 17: 266-269.
6. Nath K, Gogi R. The orbit. Indian Journal of Ophthalmology. 1976; 24: 1-14.
7. Peyman GA, Sanders DR, Goldberg MF. Principles and Practice of Ophthalmology. 1987; 3: 2.
8. Mishra SK, Ramesh C. Reproduction of custom-made eye prosthesis manoeuvre: A case report. Journal of Dentistry and Oral Hygiene. 2009; 1: 59-63.
9. Beumer J, Ma T, Marunick M, et al. (Editors) Restoration of facial defects: Etiology, disability, and rehabilitation. Maxillofacial rehabilitation: Prosthodontic and surgical considerations. St Louis: Ishiyaku EuroAmerica; 1996; pp. 377-453.
10. Heller HL, McKinstry RE (Editors) Facial materials. Fundamentals of facial prosthetics. Arlington: ABI Professional Publications; 1995. pp. 79-97.
11. Begum Z, Kola MZ, Joshi P. Analysis of the properties of commercially available silicone elastomers for maxillofacial prostheses. International Journal of Contemporary Dentistry. 2011; 2.
12. Konstantinidis L, Scolozzi P, Hamedani M. Rehabilitation of orbital cavity after total orbital exenteration using oculofacial prostheses anchored by osseointegrated dental implants posed as a one-step surgical procedure. Klin Monbl Augenheilkd. 2006; 223: 400–404.
13. Sirianni D, Leles CR, Mendonca EF. A 12- year retrospective survey of management of patients with malignant neoplasms in the orbital cavity in a Brazilian cancer hospital. The Open Dentistry Journal. 2013; 7: 140-145.
14. Costa EF, Nogueira TE, Lima NCS, Mendonça EF, Leles CR. A qualitative study of the dimensions of patients’ perceptions of facial disfigurement after head and neck cancer surgery. Special Care Dentistry Association. 2014; 34: 114-121.
15. Jani RM, Schaaf NG. An evaluation of facial prostheses. The Journal of Prosthetic Dentistry. 1978; 39: 546-550.
16. Parel SM. Diminishing dependence on adhesives for retention of facial prosthesis. The Journal of Prosthetic Dentistry. 1980; 43: 552-560.







![INDEX [microdentsystem.com] · 2015-11-24 · INDEX PRESENTATION. INTRODUCTION MULTIPLE PROSTHESIS. REMOVABLE AND IMMEDIATE PROSTHESIS. SINGLE PROSTHESIS CEMENTED PROSTHESIS. Microdent](https://img.pdfslide.net/doc/110x75/5facd9ee77a5ed547a36b19c/index-2015-11-24-index-presentation-introduction-multiple-prosthesis-removable.jpg)