Embed Size (px)
Citation preview
Archives of Disease in Childhood, 1970, 45, 656.
Outbreak of Infantile Gastro-enteritis Caused byEscherichia coli 0114
S. I. JACOBS, A. HOLZEL, B. WOLMAN, J. H. KEEN, V. MILLER, JOAN TAYLOR, andR. J. GROSS
From the Departments of Pathology and Paediatrics, Booth Hall Children's Hospital, Manchester; and the SalmonellaReference Laboratory, Central Public Health Laboratory, London
Jacobs, S. I., Holzel, A., Wolman, B., Keen, J. H., Miller, V., Taylor, J., andGross, R. J. (1970). Archives of Disease in Childhood, 45, 656. An outbreak ofinfantile gastro-enteritis caused by Escherichia coli 0114. An outbreak ofinfantile gastro-enteritis occurred at Booth Hall Children's Hospital as part of a generalincident in north-western England, caused by Esch. coli 01 14K9OH2.The organism, which could not be identified with routinely used antisera, caused
an unusually prolonged illness after an insidious onset, and was characterized bysevere vomiting, together with the passage of very watery stools which became mucus-like and which had a distinctive smell. 29 children were affected and 20 requiredintravenous feeding for a mean period of 10 days. 7 children died late in theillness, but all were young and debilitated by other acquired or congenital anomalies.Sugar intolerance was prominent, and there was difficulty in returning the children totheir routine formulae. Gentamicin and colistin sulphate may have had some effectin reducing the mortality caused by the illness.
Liver function abnormality was common, suggesting that Esch. coli 0114 might haveproduced a substance with widespread visceral effects.
In December 1968 an unusual form of infantilegastro-enteritis was first seen in the Manchester area(Lancet, 1969) and continued into the spring of 1969.The illness was very severe, had a prolonged course,and was associated with a high mortality. It wascaused by Escherichia coli 01 14K9OH2 (Jacobs,1969).
Esch. coli 01 14K9OH2 was previously implicatedas a cause of infantile gastro-enteritis in Birminghamfrom December 1951 to January 1954 (Rogers andCracknell, 1956) and the same Esch. coli serotypewas responsible for another outbreak in the Municharea in 1958 (Linzenmeier, 1960). Four cases ofinfantile diarrhoea due to Esch. coli 0114 were notedin London between 1954 and 1956, but all theseorganisms possessed flagellar antigens differentfrom the one found in the present outbreak (Charter,1956). Two strains of Esch. coli 01 14K9OH32 hadbeen isolated from calves with scours in 1950, aserotype grown from the sporadic cases of humanillness examined by Charter.Though some of the patients seen in Birmingham
Received 14 April 1970.
were severely ill and required intravenous therapy,none died, nor was their disease pattern unusual.Similarly, babies suffering from gastro-enteritiscaused by Esch. coli 0114 were treated in London inmid-1968 and early 1969 (British Medical Journal,1969; Valman and Wilmers, 1969), but there is noindication that their illness took a distinctive clinicalcourse.
Clinical Features of Disease During Man-chester Outbreak
Gastro-enteritis caused by Esch. coli. 0114 differedfrom the commonly encountered pattern of diseasein several of its manifestations.
Severity of illness and age incidence. Esch.coli 0114 was isolated from 29 patients under the ageof 2 years, and 21 required intravenous fluidtreatment. 3 patients were symptomless excretorsof the organism. The illness was most serious invery young children: all the 15 children under theage of 2 months required intravenous therapy, and6 of the 7 deaths occurred in this age-group. The
656
on May 3, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.45.243.656 on 1 O
ctober 1970. Dow
nloaded from
Outbreak of Infantile Gastro-enteritis Caused by Escherichia coli 0114
170-
,60
150 -
1-
140-E
130*
120-
110
Sodium
0
0@
a t0* -010-
E. co/i0114G.E.
0
0@
* -
* 0
.
0
0
0
otherG.E.
crLU
E
145
135-
125-
115-
105-
95.
85
Chloride
0
0*:00:0
g**.0
00
0
Ecoli0114G.E.
0
0
*-S
S.
otherG.E.
240-
200
E 60-
8i::: 120
E
80
40'
0
U rea
0
000
0
0
Ecoli0114G.E.
0
0
0
other
G.E.
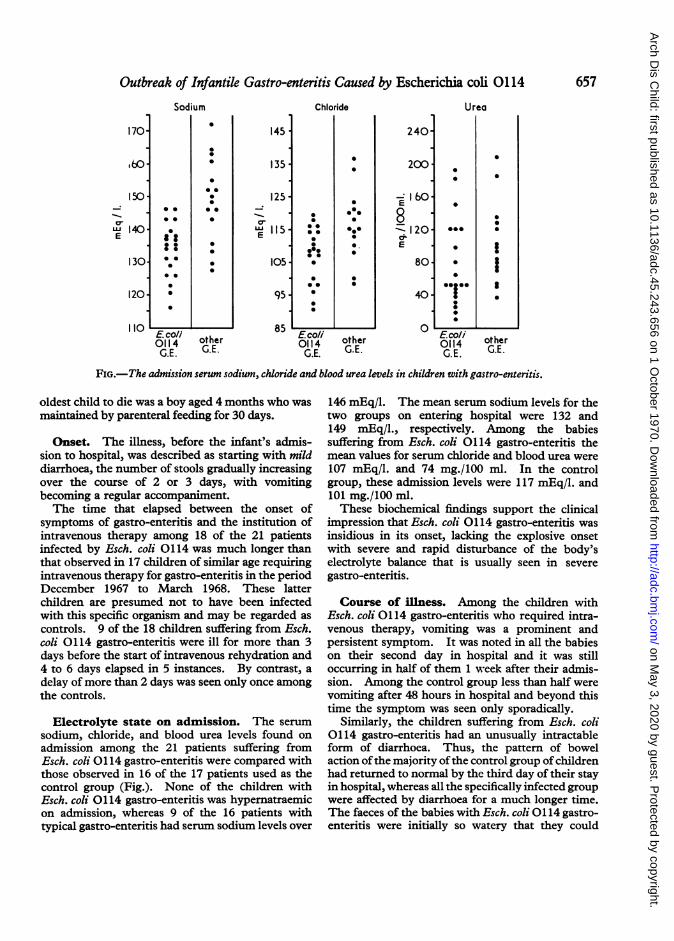
FIG.- The admission serum sodium, chloride and blood urea levels in children with gastro-enteritis.
oldest child to die was a boy aged 4 months who wasmaintained by parenteral feeding for 30 days.
Onset. The illness, before the infant's admis-sion to hospital, was described as starting with milddiarrhoea, the number of stools gradually increasingover the course of 2 or 3 days, with vomitingbecoming a regular accompaniment.The time that elapsed between the onset of
symptoms of gastro-enteritis and the institution ofintravenous therapy among 18 of the 21 patientsinfected by Esch. coli 0114 was much longer thanthat observed in 17 children of similar age requiringintravenous therapy for gastro-enteritis in the periodDecember 1967 to March 1968. These latterchildren are presumed not to have been infectedwith this specific organism and may be regarded as
controls. 9 of the 18 children suffering from Esch.coli 0114 gastro-enteritis were ill for more than 3days before the start of intravenous rehydration and4 to 6 days elapsed in 5 instances. By contrast, a
delay of more than 2 days was seen only once amongthe controls.
Electrolyte state on admission. The serum
sodium, chloride, and blood urea levels found on
admission among the 21 patients suffering fromEsch. coli 0114 gastro-enteritis were compared withthose observed in 16 of the 17 patients used as thecontrol group (Fig.). None of the children withEsch. coli 0114 gastro-enteritis was hypernatraemicon admission, whereas 9 of the 16 patients withtypical gastro-enteritis had serum sodium levels over
146 mEq/l. The mean serum sodium levels for thetwo groups on entering hospital were 132 and149 mEq/l., respectively. Among the babiessuffering from Esch. coli 0114 gastro-enteritis themean values for serum chloride and blood urea were
107 mEq/l. and 74 mg./100 ml. In the controlgroup, these admission levels were 117 mEq/l. and101 mg./100 ml.These biochemical findings support the clinical
impression that Esch. coli 0114 gastro-enteritis was
insidious in its onset, lacking the explosive onsetwith severe and rapid disturbance of the body'selectrolyte balance that is usually seen in severe
gastro-enteritis.
Course of illness. Among the children withEsch. coli 0114 gastro-enteritis who required intra-venous therapy, vomiting was a prominent andpersistent symptom. It was noted in all the babieson their second day in hospital and it was stilloccurring in half of them 1 week after their admis-sion. Among the control group less than half werevomiting after 48 hours in hospital and beyond thistime the symptom was seen only sporadically.
Similarly, the children suffering from Esch. coli0114 gastro-enteritis had an unusually intractableform of diarrhoea. Thus, the pattern of bowelaction ofthe majority ofthe control group ofchildrenhad returned to normal by the third day of their stayin hospital, whereas all the specifically infected groupwere affected by diarrhoea for a much longer time.The faeces of the babies with Esch. coli 0114 gastro-enteritis were initially so watery that they could
657
on May 3, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.45.243.656 on 1 O
ctober 1970. Dow
nloaded from
Jacobs, Holzel, Wolman, Keen, Miller, Taylor, and Grossscarcely be distinguished from urine. Later theyconsisted entirely of mucus and had a characteristicfoetid smell unlike anything previously associatedwith infantile diarrhoea, and which pervaded theentire cubicle.
Feeding difficulties. In babies suffering fromEsch. coli 0114 gastro-enteritis it was necessary tomaintain the children by parenteral feeding forprolonged periods, because any attempt to givenourishment by mouth precipitated a rapid returnof diarrhoea and vomiting, or severely exacerbatedthese symptoms.None of the 21 children who developed Esch. coli
0114 gastro-enteritis and required intravenoussupport was treated in this way for less than 3 daysand only 8 could dispense with this form of therapyin under 1 week. The mean length of timeparenteral alimentation was maintained was 10-2days and the maximum period was 30 days. Whendeath occurred, this was a late event and supervened,on average, 14-4 days after the beginning of intra-venous feeding. These findings contrast markedlywith those observed in the control group of 17children who required intravenous therapy, amongstwhom the infusion was never maintained for morethan 3 days (mean 1 6 days) with 4 of the 5 deathsoccurring during the child's first day of hospitaltreatment.Though a child with Esch. coli 0114 gastro-
enteritis frequently required prolonged intravenoustherapy, there was little difficulty in maintainingnormal electrolyte and urea levels in the blood even
in those cases which finally proved fatal.
Prognosis. A bad prognosis was indicated bythe development of any of three signs-gastro-
intestinal haemorrhage, jaundice, and anasarca andeffusions in the serous cavities.Four of the 7 patients who died, vomited fresh
blood or passed melaena stools before death, andevidence of alimentary tract bleeding was found intwo others at necropsy. Amongst these childrenwith ante-mortem haemorrhage, the bleeding beganto occur 6, 4, 3, and 2 days, respectively, beforedeath. The blood coagulation system was normalin 2 of these infants as measured by the plasmaclotting time, the prothrombin time, the kaolincephalin time, the thrombin calcium time, and thefibrinogen titre. No haemorrhage was observedin any child with Esch. coli 0114 gastro-enteritis whosurvived.
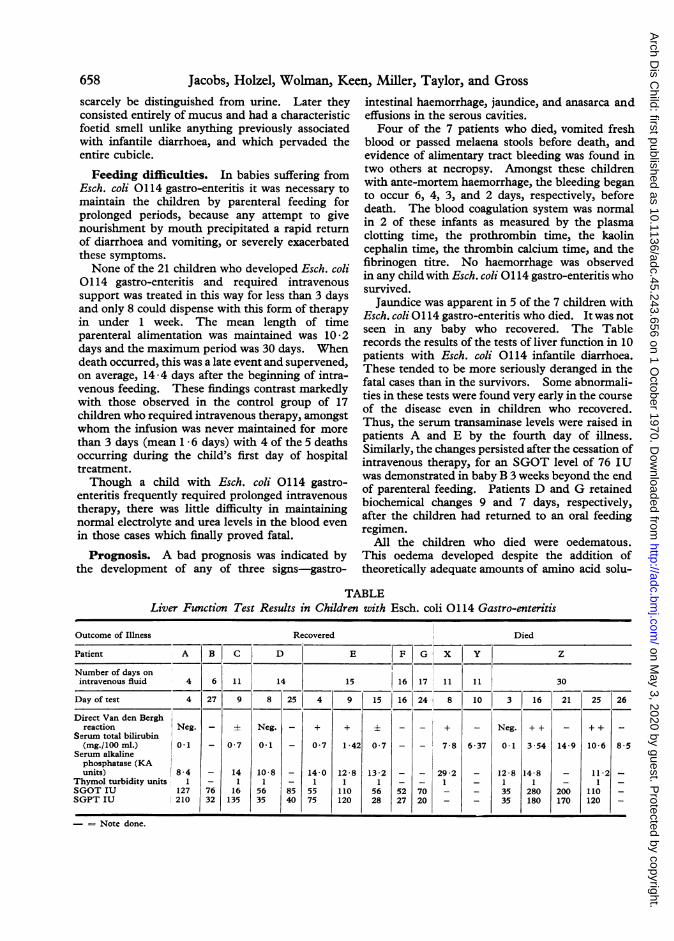
Jaundice was apparent in 5 of the 7 children withEsch. coli 0114 gastro-enteritis who died. It was notseen in any baby who recovered. The Tablerecords the results of the tests of liver function in 10patients with Esch. coli 0114 infantile diarrhoea.These tended to be more seriously deranged in thefatal cases than in the survivors. Some abnormali-ties in these tests were found very early in the courseof the disease even in children who recovered.Thus, the serum transaminase levels were raised inpatients A and E by the fourth day of illness.Similarly, the changes persisted after the cessation ofintravenous therapy, for an SGOT level of 76 IUwas demonstrated in baby B 3 weeks beyond the endof parenteral feeding. Patients D and G retainedbiochemical changes 9 and 7 days, respectively,after the children had returned to an oral feedingregimen.
All the children who died were oedematous.This oedema developed despite the addition oftheoretically adequate amounts of amino acid solu-
TABLELiver Function Test Results in Children with Esch. coli 0114 Gastro-enteritis
Outcome of Illness Recovered Died
Patient A B C D E F G X Y Z
Number of days onintravenous fluid 4 6 11 14 15 16 17 11 11 30
Day of test 4 927 8 25 4 9 15 16 24 8 10 3 16 21 25 26
Direct Van den Berghreaction Neg. - ± Neg. - + + ± _ _ + - Neg. + + - + + -
Serum total bilirubin(mg./100ml.) 0-1 - 0 7 0-1 - 0 7 1 42 0 7 _ 7 8 6 37 0 1 3 54 14-9 10-6 8-5
Serum alkalinephosphatase (KAunits) 8-4 - 14 10-8 - 14-0 12-8 13-2 _ 292 _ 12 8 148 _ 11-2
Thymol turbidity units 1 - 1 1 - 1 1 1 - 1 _ 1 1 _ 1 _SGOT IU 127 76 16 56 85 55 110 56 52 70 - - 35 280 200 110 _SGPT IU 210 32 135 35 40 75 120 28 27 20 - _ 35 180 170 120 _
- = Note done.
658
on May 3, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.45.243.656 on 1 O
ctober 1970. Dow
nloaded from

Outbreak of Infantile Gastro-enteritis Caused by Escherichia coli 0114tions and multivitamin preparations to their intra-venous infusions. Plasma was also given to restorethe depleted protein stores. At his death baby Zwas found to have a total serum protein level of5*25 g./100 ml. of which 3 5 g. was albumin.Despite these normal protein values, at necropsy165 ml. clear yellow fluid was found in his seroussacs, the majority being contained in the peritonealcavity.
Antibiotic treatment. 12 of the 14 childrentreated with either gentamicin or colistin sulphatesurvived, but, in contrast, only 2 of the 7 infantswho did not receive these antibiotics recovered.
However, it must be noted that these findings arenot necessarily proof ofthe value of these antibiotics,for a number of the fatal cases occurred early in theoutbreak, while many of the recoveries tended to bepatients seen later in the year. Further, some ofthe treated infants received gentamicin and colistinduring the course of their illness and not ab initio.Hence, they could partially consist of a self-selectinggroup who would have recovered even if these drugshad not been given.
Management of oral feeding. In the treat-ment of this prolonged illness the clinical impressionwas formed that the most successful means ofreintroducing the children to oral feeding afterintravenous infusion was 5% fructose in N/5saline.
This carbohydrate could be tolerated when othermono- and disaccharide and amino acid solutionsprovoked a rapid return of vomiting and diarrhoea.Lactose-containing preparations were particularlyprone to cause an exacerbation of the child'ssymptoms and the apparent intolerance to thissubstance persisted for the longest period.Attempts were made to perform lactose tolerance
tests on 3 children who had seemingly recovered.Two vomited the loading dose of carbohydrateimmediately and the tests were abandoned. Thethird child collapsed with profuse diarrhoea andvomiting during the test, and feeding by the intra-venous route had to be restarted. Chromatographicexamination of the faeces showed the presence ofsugar, but the significance of this was doubtfulbecause all the babies were subject to considerableintestinal hurry.
Post-mortem FindingsA post-mortem examination was performed on all
the patients who died, and viable Esch. coli 0114was recovered from the bowel of 6 of the 7 children
at this time, even though they had been ill for aconsiderable period before their death.The babies were anaemic and very oedematous.
Clear yellow or orange fluid was found in everypatient in all the serous cavities, being mostcopious in the peritoneum, where it ranged inamount from 15-125 ml. The pleural cavitiescontained about 10 ml. each and there was a similarquantity in the pericardium.
Large quantities of altered blood were found in6 of the 7 cases along the entire length of thealimentary tract. This had originated from super-ficial gastric erosions. The mucosal pattern of thestomach was flattened as were the circular folds ofthe small intestine. The mucosa of the bowel wasoedematous but no significant ulceration was found.
Jaundice was present in 5 of the 7 children, theliver being enlarged in all 7. Despite the generallywasted condition of the child, the liver weight wasabout twice that expected for the child's age. Onmicroscopy, the liver was congested, infiltrated withfat and showed patchy necrosis.The thymus never weighed more than one-fifth
of the value accepted as normal. It, and the otherreticulo-endothelial organs microscopically showedsevere lymphoid depletion. The kidneys of thechildren were congested and on histologicalexamination showed severe tubular cell swelling.Major congenital anomalies were found in 2
children (spina bifida; repaired oesophageal atresia);one child had Down's syndrome (21-22/13-15chromosomal translocation); and other infectivecomplications were seen in 3 of the 4 remainingchildren (monilial pyelonephritis; staphylococcalsepticaemia; bronchopneumonia) . Thus, the speci-fic infection can only be said to have played somepart in causing the death of a group of debilitatedchildren, and its exact role in this respect isproblematic.
Microbiological FindingsA routine admission screening programme of
faecal specimens was in operation before the out-break began in order to discover patients carryingthe common enteropathogenic Esch. coli serotypes,Salmonella and Shigella species and viruses. InJanuary 1969 routine examination of throat swabsto isolate Mycoplasma sp. was instituted to eliminatethe possibility that very young babies were reactingclinically in a bizarre manner to such organisms,for 2 older children had presented with primaryatypical pneumonia.The basis of the methods used to isolate these
micro-organisms was as follows.
659
on May 3, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.45.243.656 on 1 O
ctober 1970. Dow
nloaded from
Jacobs, Holzel, Wolman, Keen, Miller, Taylor, and GrossEnteropathogenic Esch. coli: Plating onto McConkey
and horse blood agar and examination of the Esch. coligrowth with antisera prepared against the 9 mostcommonly encountered enteropathogenic serotypes,namely Esch. coli 026, 055, 086, 0111, 0119, 0125,0126, 0127, and 0128.None of these antisera would identify Esch. coli 0114
or assist in differentiating it from normal non-entero-pathogenic serotypes, but the techniques used wereclearly satisfactory, for in 1969 this hospital reported tothe Central Epidemiological Research Laboratory theisolation of 84 strains of enteropathogenic Esch. coliexcluding type 0114. The total of such organismsnotified throughout England and Wales in 1969 was5,147 (British Medical Journal, 1970). Therefore, thisgeneral children's hospital, with its daily average bedoccupancy of 68 babies under 2 years old, contributed1 * 5% of the entire national analysable total.
Salmonella and Shigella sp: Primary plating ontodesoxycholate citrate agar, enrichment in selenite Fbroth and replating on to desoxycholate citrate agar.
Viruses: Routine inoculation of either or both HeLaor Hep 2 cell lines, rhesus or cynomolgus monkey kidneycells, and the WI 38 line.Mycoplasma sp: Inoculation of throat swabs on to a
slightly modified enriched selective PPLO formula,described by Cruickshank (1965), and into a modificationof Kraybill and Crawford's (1965) medium with sub-sequent plating on to Cruickshank's PPLO agar. Serumcold agglutinins were sought by the method recommend-ed by Cruickshank (1965).
In order to determine whether a single Esch. coliserotype was common to a number of babies, faeces werecollected from 3 infants with enteritis who had not beenill for more than 2 days and who had not receivedantibiotic therapy. No pathogen identifiable by thecurrent regimen had been isolated from these specimens.Five representative colonies were selected from eachMcConkey plate for more detailed study by the Salmon-ella Reference Laboratory.The Esch. coli serotypes found in these specimens
were as follows:Patient A: Esch. coli 015K?H1 and 0114K9OH2.Patient B: Esch. coli 044K?H18 and 0114K9OH2.Patient C: Esch. coli 04K12H2 and 044K?H18.Both Esch. coli 044 and 0114 have been isolated from
outbreaks of infantile enteritis, and it was not untilcultures from further patients were examined that itbecame clear that Esch. coli 0114 was the importantcausal agent in this outbreak and was grown from themajority of patients.
Sensitivity tests on the organism were carried out usingthe disc diffusion method on nutrient agar, apart fromthose in which the effects ofsulphonamides and trimetho-prim were being examined. In these instances lysedblood agar was employed together with a light inoculum.All the antibiotic discs were manufactured by MastLaboratories apart from trimethoprim and sulphameth-oxazole, alone and in combination, which were obtainedfrom Oxoid Ltd.
The organism was found to be resistant to ampicillin(25tg.), carbenicillin (100 ,ug.), cephaloridine (25 jig.),streptomycin (25 ,&g.), neomycin (10 ug.), kanamycin(30 ,ug.), chloramphenicol (25 ,ug.), and tetracycline(25 ,ug.). It was sensitive to colistin sulphate (200 jug.)and gentamicin (10 jug.). It was also sensitive totrimethoprim (1 *25 ,ug.) though it was completelyresistant to both sulphadimidine (200 jug.) andsulphamethoxazole (23-75 pg.). However, there wassome in vitro synergistic effect between trimethoprimand sulphamethoxazole. The average zone diameteraround a disc containing only trimethoprim was23 -1 mm., but for a combination of the anti-bacterialsubstances the inhibition area was always larger, withan average diameter of 27 mm.
History of OutbreakWhen only limited general epidemiological
information is available there is considerabledifficulty in associating an uncommon enteropatho-genic serotype of Esch. coli with an outbreak ofinfantile gastro-enteritis, despite thorough localroutine laboratory investigations and the use ofcentral specialist diagnostic facilities.The present outbreak began at the end of
December 1968. Because Esch. coli 0114 producedsuch a readily identifiable illness a retrospectivesurvey suggests that by 31 March 1969, 36 childrenhad been affected, but the organism was isolatedfrom only 20 of these. It was cultured from afurther 9 infants up to 31 July 1969. The firstisolation of the organism was from a specimen offaeces dated 14 February 1969.During December 1968 and January 1969, 11
children are considered to have been infected by theorganism, which was probably brought into thehospital on 4 separate occasions. It is likely thatin 3 of these instances the disease was introducedfrom the general community in Greater Manchester.The fourth infected child, suffering from intractablediarrhoea, was transferred from a neighbouringhospital to Booth Hall Hospital for specialistgastro-enterological care.Many of the 7 remaining children were suffering
initially from respiratory tract infections, but theirillnesses gradually changed to the insidious,chronic gastro-enteritis characteristically producedby Esch. coli 0114 in this outbreak. Thus, at thistime, a respiratory pathogen was primarily sought.Further, a viral influenza epidemic was expected,while an infection with Mycoplasma pneumoniae hadbeen diagnosed in 2 older children. 'The specificcases occurred sporadically over 6 weeks, andinvolved 3 separate infant medical wards. Incontrast, there was no cross-infection with Sh.sonnei or other recognized enteropathogenic Esch.
660
on May 3, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.45.243.656 on 1 O
ctober 1970. Dow
nloaded from

Outbreak of Infantile Gastro-enteritis Caused by Escherichia coli 0114coli serotypes among babies who were being nursedconcurrently in the same cubicalized buildings.
In February, 8 cases of Esch. coli 0114 gastro-enteritis occurred in two waves, five days apart, on a
previously unaffected special surgical unit housingvery debilitated neonates. Hence, specimens ofEsch. coli were at once sent to the SalmonellaReference Laboratory who identified inter alia bothEsch. coli 0114 and 044 (see above). No conclusionscould, therefore, be drawn, for while either mighthave been a pathogen, they could equally haverepresented part of the indigenous bland hospitalflora. None the less, all the involved wards were
closed for new patients and for disinfection.At the end of March before any fresh infant
medical cases had been accepted by the hospital,3 patients were readmitted. All were well at thetime of their initial discharge, but on their return
they were suffering from infantile diarrhoea.Cultures submitted to the Salmonella ReferenceLaboratory yielded a pure growth of Esch. coli 0114from 2 of these children. It was concluded, there-fore, that this organism was the probable cause ofthe peculiar gastro-enteritis, but no deductionscould be made whether it was confined to thehospital or was more widespread in the community.
Early in April it was unofficially learnt that otherhospitals in Greater Manchester were encounteringgastro-enteritis of similar type. Their patientshad no connexion with Booth Hall. Cultures were
sent from some of these children to the SalmonellaReference Laboratory which confirmed the presence
of Esch. coli 0114 Between April and July 1969,91 of the 124 cases of Esch. coli 0114 infantile gastro-enteritis reported to the Epidemiological ReferenceLaboratory of the Public Health Laboratory Serviceoriginated in north-western England. Thus, theBooth Hall outbreak consisted merely of part of a
wide community experience.Between the beginning of May and the end of
July 1969, Esch. coli 0114 was brought into hospitalby 9 patients with gastro-enteritis.At the close of the study cases were still being
admitted from domiciliary practice and from otherinstitutions, but the recognition of the aetiologicalrole of Esch. coli 0114 and the concomitant ability ofthe local laboratory to identify this serotype, both incases and in carriers, successfully reduced the rateof cross-infection within the hospital.
DiscussionThe disease we observed was unusual in its
severity, and its course was reminiscent of theAberdeen epidemic of 1947 caused by Esch. coli 0 11
(Smith, 1955).
In recent years such outbreaks have been un-common in this country and gastro-enteritis is seenas a rapidly developing illness which may requireurgent supportive measures to readjust the patient'swater and electrolyte balance. These correctionscan usually be performed without difficulty, andthe baby is able to return quickly, by way ofregrading of feeds, to his routine formula. Paripassu, there is an abatement in the child's symptoms.In a few fatal cases death occurs while the infant ison his way to hospital or in the immediate resuscita-tive stages.
In contrast, our data show that the infantilediarrhoea caused by Esch. coli 0114 was moreinsidious in starting, had a prolonged course, and ahigh mortality that occurred late in the illness.This was associated with gastro-intestinal haemor-rhage, jaundice, and oedema. The presence ofother congenital and acquired debilitating condi-tions, however, predisposed to a fatal outcome.On admission to hospital, children suffering from
Esch. coli 0114 gastro-enteritis showed less disturb-ance of their electrolyte balance than infants withmore typical forms of the disease. None the less,these children were severely ill, suggesting that theconventional blood chemistry parameters were notmeasuring the extent of the baby's cellular meta-bolic inbalance, either on admission or during theirillness. Support for the hypothesis that there waswidespread derangement of function was theevidence of parenchymal liver damage seen early inthe disease. Simple calorie starvation could notaccount for this if water and electrolyte balance wasrestored. Our children with Esch. coli 0114 gastro-enteritis were receiving a carefully calculated andadequate diet throughout their illness. Septicaemiawas never shown.
It seemed, therefore, that Esch. coli 0114 may haveproduced some toxic product with a widespreadbodily effect.The primary site of action of Esch. coli 0114 could
be the intracellular carbohydrate-splitting enzymesof the small intestinal mucosa, or the transportmechanism involved in carrying sugars and aminoacids across cell membranes, for at first the childrenappeared to be intolerant of any carbohydrate.Amino acid solutions, however, were equally badlytolerated, but the earliest sign of recovery was theacceptance of these together with fructose. Lactosewas especially difficult to assimilate and low lactoseformulae had to be continued for long periods. Inthe recovery stages our attempts to perform lactosetolerance tests were unsuccessful.
Gentamicin and colistin sulphate appeared tohave some effect in reducing the mortality, but no
661
on May 3, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.45.243.656 on 1 O
ctober 1970. Dow
nloaded from
Jacobs, Holzel, Wolman, Keen, Miller, Taylor, and Grosscontrolled trial was undertaken. Valman andWilmers (1969), who also used gentamicin, onlyreported one death, but their outbreak of gastro-enteritis caused by Esch. coli 0114 took place in thesummer. In our experience, infantile gastro-enter-itis, in general, is exacerbated by respiratory illness,and such diseases were widespread in the communityduring the winter months when we experienced ourlow recovery rate. In the late spring and summerwe had only a single fatality.
Complete information is not available about theeffect of antibiotics on the carriage of Esch. coli 0114,but several patients remained excretors after pro-longed courses of both gentamicin and colistinsulphate, singly and in combination. Our observa-tions, therefore, differ from those of Valman andWilmers who infer that gentamicin alone preventedthe emergence of the carrier state. However, theseworkers gave their gentamicin orally, whereas wegave it intramuscularly. The colistin sulphate wasusually given orally. Several children remainedexcretors even though they were prescribed bothantibiotics directly after the isolation of Esch. coli0114 from their admission faecal sample. Hence,the failure of specific treatment in preventing faecalcarriage in these cases was not due to delay in givingthe drugs. It is possible, however, that the pre-scription of antibiotics to which the organism wasresistant was harmful. Thus, a child was dis-charged home as a carrier of Esch. coli 0114 after along illness during which he had been treated, interalia, with specific antibiotics and freeze-driedplasma infusions: 61 days after the child was givenhis last blood-product unit he returned to hospitalwith a severe attack of hepatitis and lapsed intocoma. The serum was positive for Au-SH antigen.Esch. coli 0114 was not isolated from the child'sstools on admission or on several subsequentoccasions. He was given neomycin (to which Esch.coli 0114 is resistant), steroids, and a high caloriediet and his level of consciousness became normal.However, the child collapsed suddenly in a state ofprofound shock and died. The liver disease wasconfirmed at necropsy, but in addition the entirelength of the child's bowel was grossly distendedwith watery fluid, which on aerobic culture yieldeda pure growth of Esch. coli 0114. Cross-infectionwith the organism is unlikely in this instance, and itis suggested that the neomycin might have greatlyreduced the normal flora in the child's bowel andleft an ecological vacuum. In this, any smallnumbers of resistant Esch. coli 0114 that remainedfrom the baby's previous illness could multiply andcause very acute disease. Thus, the widespreaduse of antibiotics in infantile gastro-enteritis, where
the sensitivity and identity of the causative organismis not known, may have occasional serious con-sequences, in addition to encouraging the generalemergence of antibiotic-resistant bacteria.
Unfortunately, accepted pathogenic bacteria areisolated from only a minority of all children sufferingfrom infantile diarrhoea, though in the severestcases a recognized agent is frequently found. AtBooth Hall Hospital in 1968 only 82 such organismswere isolated from 250 children with gastro-enteritis.The yield of viruses has also been small, for in theperiod 1962-64 only 15 viruses were grown from399 children in this hospital suffering from thedisease (Holzel et al., 1965). Therefore, abouttwo-thirds of the children admitted with gastro-enteritis are discharged without any microbial causefor their illness being discovered.The children from whom no recognized patho-
genic organisms are isolated are a major hazard tobabies nearby. If another child acquires theirpathogen and develops disease there is no routinemethod of determining the origin of the infection ordefining its nature. Hence, no rational control ortreatment measures can be instituted. In thepresent outbreak it was only the unusual course ofthe disease that began to suggest that it was causedby a single distinctive agent. Among the 17 child-ren who were affected by Esch. coli 0114 on the 3medical wards as a result of probable cross-infectionbetween December 1968 and March 1969, 8 werefound while they were still in-patients, but the other9 became ill with gastro-enteritis after they had beendischarged on the completion of treatment for theirprimary disease. These data suggest that any childwho develops gastro-enteritis during his stay inhospital or shortly after his discharge from anyinstitution should be completely investigated todetermine the bacteriological aetiology ofhis disease.Such investigations may show the beginnings of anoutbreak caused by a little known pathogen thatpossesses the power of spreading.
Likewise, if no pathogenic organism is isolated byroutine methods from a child dying or seriously illwith gastro-enteritis, then here too an additional fullmicrobiological search should be made for lesscommonly accepted causes.The significance of these less commonly isolated
pathogenic organisms is often very difficult toevaluate and a knowledge of the indigenous wardflora is vital in interpreting the possibility of cross-infection. If it is reasonably certainly established,however, that such an agent has been identified,then this information should be immediately notifiedto the central and local public health authorities,
662
on May 3, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.45.243.656 on 1 O
ctober 1970. Dow
nloaded from

Outbreak of Infantile Gastro-enteritis Caused by Escherichia coli 0114 663who should be responsible for disseminating thefindings to all the appropriate agencies in the field.
We would like to thank Dr. D. I. K. Evans and Dr.G. C. Turner for their help in investigating the bloodcoagulation and the Au-SH antigen problems of someof these children. We are grateful to the Epidemiolo-gical Research Laboratory of the Public Health Labora-tory Service for access to their records.
REFERENcEs
British Medical Journal (1969). Acute infective gastroenteritis.(Leading article), 2, 263.(1970). Gastroenteritis in children. (Note.) 2, 58.
Charter, R. E. (1956). Escherichia coli type 0.114 isolated frominfantile diarrhoea and calf scours. J'ournal of Pathology andBacteriology, 72, 33.
Cruickshank, R. (1965). Medical Microbiology, 11th ed., p. 497 and912. Livingstone, Edinburgh.
Holzel, A., Parker, L., Patterson, W. H., Cartmel, D., White,L. L. R., Purdy, R., Thompson, K. M., and Tobin, J. O'H.(1965). Virus isolations from throats of children admitted to
hospital with respiratory and other diseases, Manchester, 1962-4. British Medical Journal, 1, 614.
Jacobs, S. I. (1969). In Report on Gastroenteritis, p. 25. Ed. byF. N. Marshall. Department of Health and Social Security,London.
Kraybill, W. H., and Crawford, Y. E. (1965). A selective mediumand color test for Mycoplasma pneumoniae. Proceedings of theSociety for Experimental Biology and Medicine, 118, 965.
Lancet (1969). Gastroenteritis at Booth Hall Children's Hospital,Manchester. (Note.) 1, 843.
Linzenmeier, G. (1960). Zur Diagnostik von E. coli 114 ausStiihlen dyspepsiekranker Sauglinge. Zentralblattfur Bakterio-logie, Parasitenkunde, Infektionskrankheiten und Hygiene. 1.Abteil Originale, 177, 435.
Rogers, K. B., and Cracknell, V. M. (1956). Epidemic infantilegastroenteritis due to Escherichia coli type 0114. Journal ofPathology and Bacteriology, 72, 27.
Smith, J. (1955). The Aetiology of Epidemic Infantile Gastroenteritis.Royal College of Physicians, Edinburgh.
Valman, H. B., and Wilmers, M. J. (1969). Use of antibiotics inacute gastroenteritis among infants in hospital. Lancet, 1, 1122.
Correspondence to Dr. S. I. Jacobs, Department ofPathology, St. James's Hospital, Leeds, LS9 7TF.
on May 3, 2020 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.45.243.656 on 1 O
ctober 1970. Dow
nloaded from