Embed Size (px)
Citation preview
Outcomes of care among patients admitted to the rehabilitation unit of a specialistthe rehabilitation unit of a specialist neuropsychiatric hospital in Nigeria
bby1Adebowale T.O., 1Onofa L.U., 1Sowunmi O.,
1Majekodunmi O.E., 2Latona O.O.Affiliation:Affiliation:1. Neuropsychiatric Hospital Aro, P. M. B. 2002, Aro, Ab k O S Ni iAbeokuta, Ogun State, Nigeria.
2. Department of Epidemiology and Medical p p gyStatistics , University of Ibadan, Ibadan, Nigeria
Presenting Author:D O f L k U kDr. Onofa Lucky UmukoroM.B; B.S, FWACP, M.SC (Epidemiology), Unit Consultant Psychiatrist (Rehabilitation)Department of Community & Rehabilitation PsychiatryNeuropsychiatric Hospital, Aro, Abeokuta,Ogun State, Nigeria.Ogun State, Nigeria.Email: [email protected]: +2348033336875Tel: +2348033336875
Being
AN ORAL PAPER PRESENTATION AN ORAL PAPER PRESENTATION
FOR DOUGLAS BENNETT PRIZE PRESENTATIONS
AT THE ANNUAL RESIDENTIAL CONFERENCE OF
THE FACULTY OF REHABILITAION & SOCIAL
PSYCHIATRYPSYCHIATRY
ROYAL COLLEGE OF PSYCHIATRISTS
21‐22 NOVEMBER, 2013
THISTLE BIRMINGHAM CITY, BIRMINGHAM
OCCUPATIONAL THERAPY DEPARTMENT , ARO PSYCHIATRIC HOSPITAL, NIGERIA
INTRODUCTIONINTRODUCTION
M l di d hi h ll i f % f hMental disorders exert a high toll, accounting for 13% of thetotal global burden of disease. In Africa, neuropsychiatricdisorders accounted for about 18% of years lived withdisorders accounted for about 18% of years lived withDisability (YLD) in 2000 (WHO, 2001).Psychiatric rehabilitation is a whole systems approach toPsychiatric rehabilitation is a whole systems approach torecovery from mental illness that maximizes an individual’squality of life and social inclusion by encouraging theirskills, promoting independence and autonomy in order togive them hope for the future and leads to successfulcommunity living through appropriate support(killapsy etcommunity living through appropriate support(killapsy etal, 2005).
INTRODUCTION CONT’D
The unmet needs of the mentally disabled have pointed theway towards longer‐term and more comprehensive in‐
i h bili i i h l di bl d i di id lpatient rehabilitation services to help disabled individualto develop the emotional, social and intellectual skillsneeded to live learn and work in the community with theneeded to live, learn and work in the community with theleast amount of professional support(Adair et al, 2005).
INTRODUCTION CONT’DINTRODUCTION CONT’D
Discharge from in‐patient rehabilitation is a measure of goodDischarge from in patient rehabilitation is a measure of goodoutcome because it marks an important stage in the individual’srecovery. The person would have gained the skills needed fordaily living self medicating engagement with communitydaily living, self medicating, engagement with communitysupport to gain help and sense of identity (Strauss, 1986).
In psychiatric practice, some mentally ill patients spend their lifein continuous hospitalization due to severe mental illness,substance dependence homelessness and abandonment by thesubstance dependence, homelessness and abandonment by thepatient’ relatives(Roger et al 2004, Rosler 2005).
INTRODUCTION CONT’D
In developing countries like Nigeria, the issue of long‐stayis intertwined with the history of orthodox psychiatric care.In the early 20th century asylums were established inIn the early 20th century, asylums were established inselected cities in the country. These were to serve as placesof confinement for psychiatric infirm. When theseof confinement for psychiatric infirm. When theseasylums were converted to full‐fledged psychiatrichospitals, most of the patients had remained in thesefacilities(Boroffka, 1995, Ekpo et al, 2000).
In view of the peculiar mental health situation in Nigeria,there has been strong recommendations for theestablishment of rehabilitation centres to cater for thisestablishment of rehabilitation centres to cater for thiscategory of long‐stay patients(Taiwo et al, 2008).
INTRODUCTION CONT’DINTRODUCTION CONT’D
Th N hi i h i l A h fThe Neuropsychiatric hospital, Aro the foremostpsychiatric hospital in Nigeria(The Mecca of Psychiatry inWest Africa) formally established Rehabilitation unit inWest Africa) formally established Rehabilitation unit in2002 and a transitional half‐way home (Hope Villa) in2009 for the effective rehabilitation and community re‐yintegration of patients.No study had been undertaken on the outcome of theservice. Knowledge of factors associated with outcome isuseful to guide treatment for patients.Thi d h f d k lThis current study was therefore undertaken to evaluatethe outcomes of care among patients admitted to therehabilitation unit of Neuropsychiatric Hospital Arorehabilitation unit of Neuropsychiatric Hospital, Aro,Abeokuta, Nigeria.
OBJECTIVES
This study sets out to determine the outcomes of careamong patients admitted to the rehabilitation unit of a
i li hi i h i l i Ni i bspecialist neuropsychiatric hospital in Nigeria byexamining socio‐demographic profiles, type of mentalillness and associated physical co‐morbidities of theillness and associated physical co‐morbidities of thepatients .The factors influencing rehabilitation outcomes among theThe factors influencing rehabilitation outcomes among thepatients were also assessed.
METHODSThe Study centre is the Neuropsychiatric Hospital Aro(WHO ll b i C f R h & T i i i(WHO collaborating Centre for Research & Training inmental health) Abeokuta, Ogun State, Nigeria.The Neuropsychiatric Hospital Aro started at the LantoroThe Neuropsychiatric Hospital Aro started at the LantoroAnnex which was a colonial local government prison until13th April, 1944 when it was transformed into an asylum for13 April, 1944 when it was transformed into an asylum forthe care of mentally ill soldiers repatriated from the SecondWorld War. This asylum was converted to NeuropsychiatricHospital (526 bed‐space) Aro in 1954 and was designated aWHO Collaborating Centre for Research and Training inMental Health in 1976 In 2002 the hospital establishedMental Health in 1976. In 2002, the hospital establishedrehabilitation wards (60 bed spaces) and later atransitional half‐way home (hope villa) for effectivey ( p )rehabilitation of disabled patients.
METHODS CONT’D
Patients were admitted to the rehabilitation unit based onfulfillment of placement criteria. The Rehabilitation unitili l idi i li h d i iutilizes a multidisciplinary team approach to administer
psycho‐pharmacological, psychosocial, vocational andother structured intervention to patients in the unitother structured intervention to patients in the unitPatients had supervised vocational engagements bothwithin and outside the hospital settingwithin and outside the hospital setting

MULTI‐DISCIPLINARY TEAM MEETING AT THE REHABILITAION UNIT
METHODS CONT’D
Following ethical approval, we conducted aretrospective review of records of all patients admittedretrospective review of records of all patients admittedto the unit over eleven (11) years period fromSeptember 2002 to August 2013.p g 3There were 62 admissions of which 6 patients’ caserecords could not be traced. Consequently, 56 caseC q y, 5records were available to analysis.Data was collected using a semi‐structured proformaData was collected using a semi structured proformaand analysis was done using SPSS version 17.
METHODS CONT’DFrequency tables and cross tabulations of relevant socio‐d hi li i l h bili i ddemographic, clinical, rehabilitation and outcomevariables were drawn up.For survival analysis the desired outcome is achievingFor survival analysis, the desired outcome is achievingdischarge from the rehabilitation unit and re‐integrationinto the community.into the community.Survival data analysis was done using Kaplan‐Meiermethod for censored data. This involved coding thegoutcome variables into 1 – discharge (the desired outcome)and 0 – other outcomes which are censored.The factors influencing discharge were evaluated usingCox’s Proportional Hazard Regression. The factors in themodel ere socio demographic ariables clinicalmodel were socio‐demographic variables, clinicaldiagnoses and rehabilitation variables.
The Chi‐square tests were used to test associationsqbetween categorical variables and Independent student – t‐test to compare the difference in the means of quantitativevariables.Hazard ratios (HRs) and their 95% confidence intervals(CI ) bt i d th f i ti(CIs) were obtained as the measure of associations.P – values of significance was set at P ≤ 0.05.
RESULTS
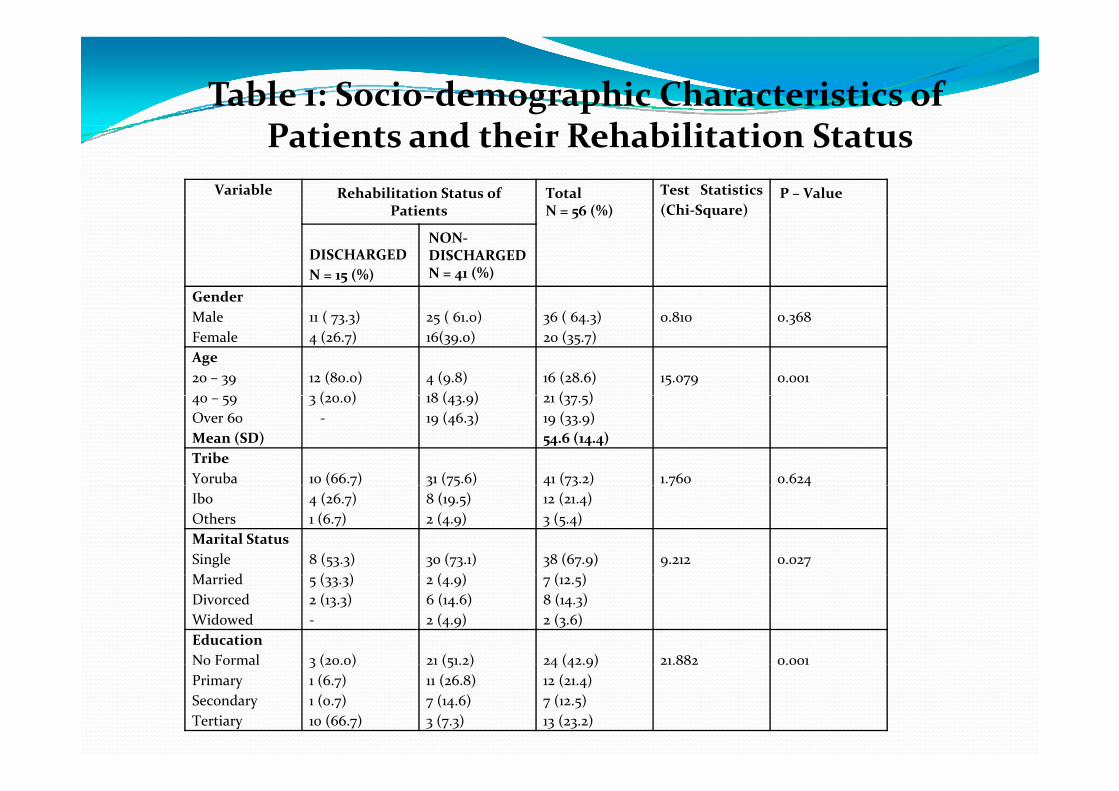
Table 1: Socio‐demographic Characteristics of P i d h i R h bili i SPatients and their Rehabilitation Status
Variable Rehabilitation Status of Patients
TotalN = 56 (%)
Test Statistics(Chi‐Square)
P – Value5 ( ) ( q )
DISCHARGEDN = 15 (%)
NON‐DISCHARGED N = 41 (%)
GenderMaleFemale
11 ( 73.3)4 (26.7)
25 ( 61.0)16(39.0)
36 ( 64.3)20 (35.7)
0.810 0.368
Age20 – 39 12 (80.0)
( )4 (9.8)8 ( )
16 (28.6)( )
15.079 0.00140 – 59Over 60Mean (SD)
3 (20.0)‐
18 (43.9)19 (46.3)
21 (37.5)19 (33.9)54.6 (14.4)
TribeYoruba 10 (66.7) 31 (75.6) 41 (73.2) 1.760 0.624IboOthers
( 7)4 (26.7)1 (6.7)
3 (75 )8 (19.5)2 (4.9)
4 (73 )12 (21.4)3 (5.4)
7 4
Marital StatusSingleM i d
8 (53.3)( )
30 (73.1)( )
38 (67.9)( )
9.212 0.027MarriedDivorcedWidowed
5 (33.3)2 (13.3)‐
2 (4.9)6 (14.6)2 (4.9)
7 (12.5)8 (14.3)2 (3.6)
EducationNo Formal 3 (20.0) 21 (51.2) 24 (42.9) 21.882 0.001o o aPrimarySecondaryTertiary
3 ( 0.0)1 (6.7)1 (0.7)10 (66.7)
(5 . )11 (26.8)7 (14.6)3 (7.3)
4 (4 .9)12 (21.4)7 (12.5)13 (23.2)
.88 0.00
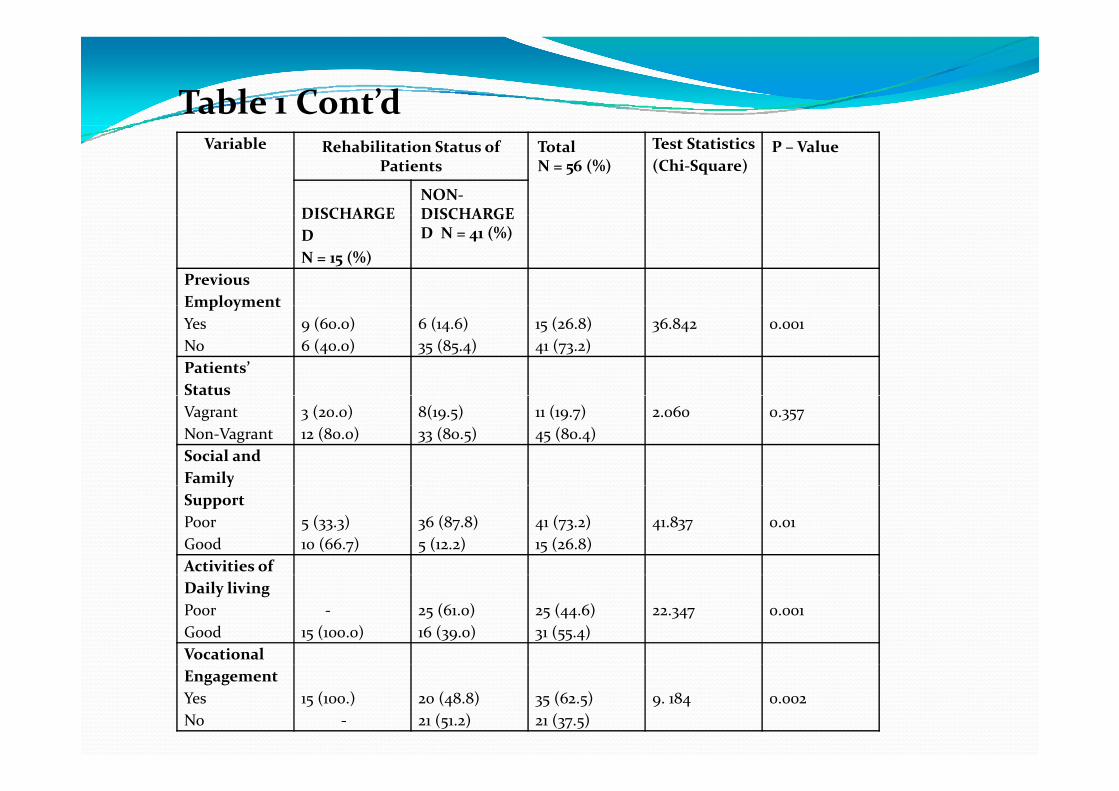
Table 1 Cont’dVariable Rehabilitation Status of
PatientsTotalN = 56 (%)
Test Statistics(Chi‐Square)
P – Value
DISCHARGENON‐DISCHARGEDISCHARGE
DN = 15 (%)
DISCHARGED N = 41 (%)
PreviousEmploymentEmploymentYesNo
9 (60.0)6 (40.0)
6 (14.6)35 (85.4)
15 (26.8)41 (73.2)
36.842 0.001
Patients’StatusVagrantNon‐Vagrant
3 (20.0)12 (80.0)
8(19.5)33 (80.5)
11 (19.7)45 (80.4)
2.060 0.357
Social andFamilyySupportPoorGood
5 (33.3)10 (66.7)
36 (87.8)5 (12.2)
41 (73.2)15 (26.8)
41.837 0.01
Activities ofDaily livingPoorGood
‐15 (100.0)
25 (61.0)16 (39.0)
25 (44.6)31 (55.4)
22.347 0.001
VocationalEngagementYesNo
15 (100.)‐
20 (48.8)21 (51.2)
35 (62.5)21 (37.5)
9. 184 0.002
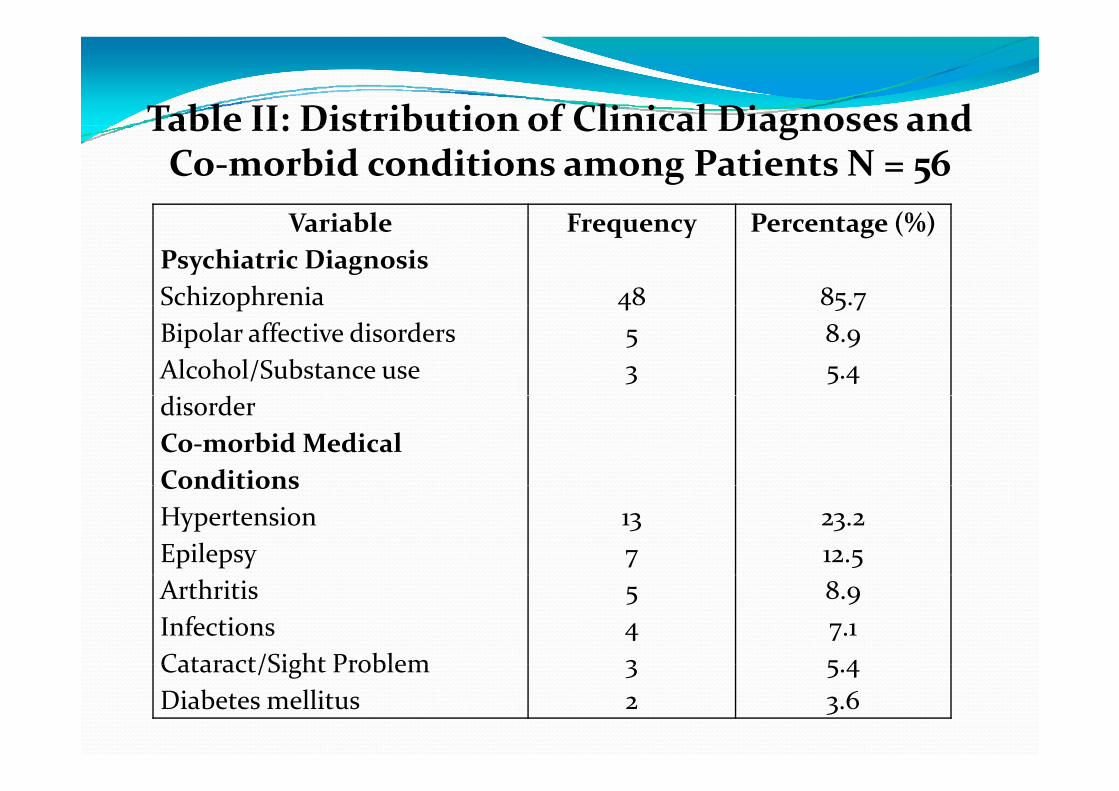
Table II: Distribution of Clinical Diagnoses and Table II: Distribution of Clinical Diagnoses and Co‐morbid conditions among Patients N = 56
V i bl F P (%)VariablePsychiatric DiagnosisSchizophrenia
Frequency
48
Percentage (%)
85.7pBipolar affective disordersAlcohol/Substance use d d
453
5 78.95.4
disorderCo‐morbid Medical ConditionsConditionsHypertensionEpilepsy
137
23.212.5
ArthritisInfectionsCataract/Sight Problem
543
8.97.15 4Cataract/Sight Problem
Diabetes mellitus32
5.43.6
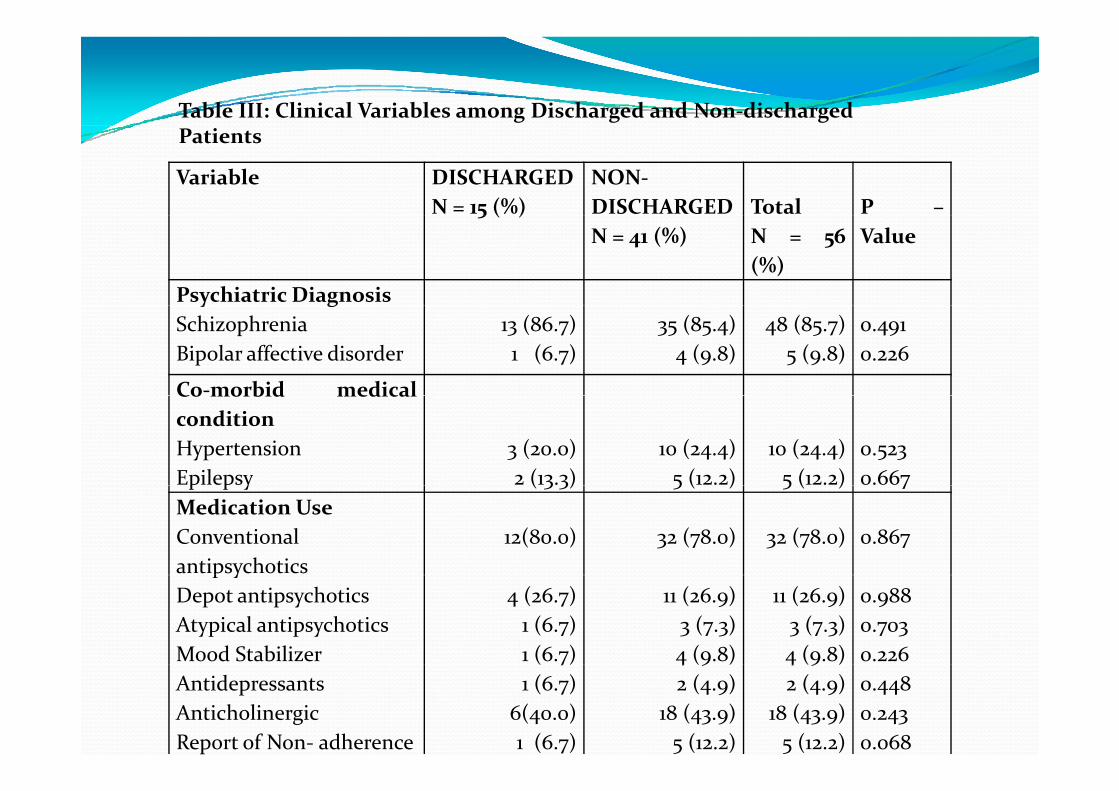
Table III: Clinical Variables among Discharged and Non‐discharged
Variable DISCHARGEDN = 15 (%)
NON‐DISCHARGED Total P –
Patients
5 ( )N = 41 (%) N = 56
(%)Value
Psychiatric Diagnosisy gSchizophreniaBipolar affective disorder
13 (86.7)1 (6.7)
35 (85.4)4 (9.8)
48 (85.7)5 (9.8)
0.4910.226
Co‐morbid medicalCo morbid medicalconditionHypertensionEpilepsy
3 (20.0)2 (13.3)
10 (24.4)5 (12.2)
10 (24.4)5 (12.2)
0.5230.667p p y ( 3 3) 5 ( ) 5 ( ) 7
Medication UseConventionalantipsychotics
12(80.0) 32 (78.0) 32 (78.0) 0.867p y
Depot antipsychoticsAtypical antipsychoticsMood Stabilizer
4 (26.7)1 (6.7)1 (6.7)
11 (26.9)3 (7.3)4 (9.8)
11 (26.9)3 (7.3)4 (9.8)
0.9880.7030.226
AntidepressantsAnticholinergicReport of Non‐ adherence
( 7)1 (6.7)
6(40.0)1 (6.7)
4 (9 )2 (4.9)
18 (43.9)5 (12.2)
4 (9 )2 (4.9)
18 (43.9)5 (12.2)
0.4480.2430.068
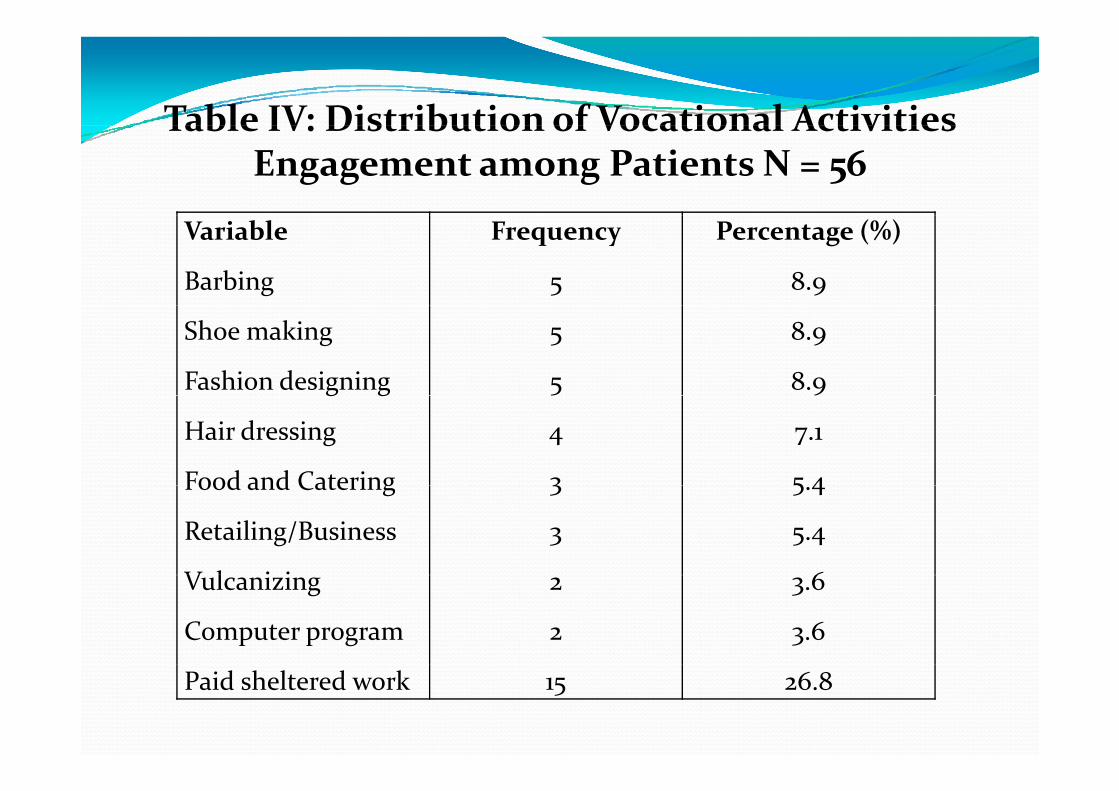
Table IV: Distribution of Vocational Activities Table IV: Distribution of Vocational Activities Engagement among Patients N = 56
Variable
Barbing
Frequency
5
Percentage (%)
8.9
Shoe making
Fashion designing
5
5
8.9
8.9g g
Hair dressing
Food and Catering
4
3
7.1
5 4Food and Catering
Retailing/Business
V l i i
3
3
5.4
5.4
6Vulcanizing
Computer program
2
2
3.6
3.6
Paid sheltered work 15 26.8
TAILORING SECTION OF OCCUPATIONAL THERAPY DEPT.
HAIRDRESSING SECTION OF OCCUPATIONAL THERAPY DEPT
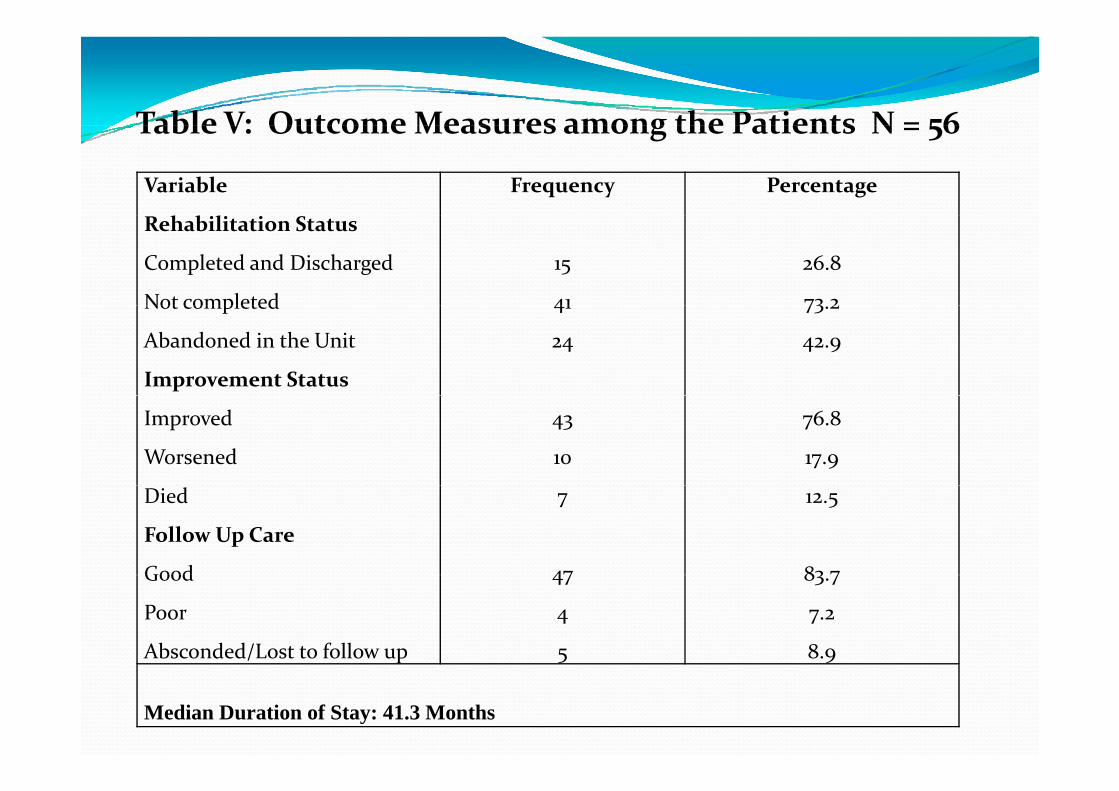
Table V: Outcome Measures among the Patients N = 56Table V: Outcome Measures among the Patients N = 56
Variable
h bili i
Frequency Percentage
Rehabilitation Status
Completed and Discharged
Not completed
15
41
26.8
73 2Not completed
Abandoned in the Unit
Improvement Status
41
24
73.2
42.9
Improved
Worsened
43
10
76.8
17.9
Died
Follow Up Care
Good
7
47
12.5
83 7Good
Poor
Absconded/Lost to follow up
47
4
5
83.7
7.2
8.9
Median Duration of Stay: 41.3 Months
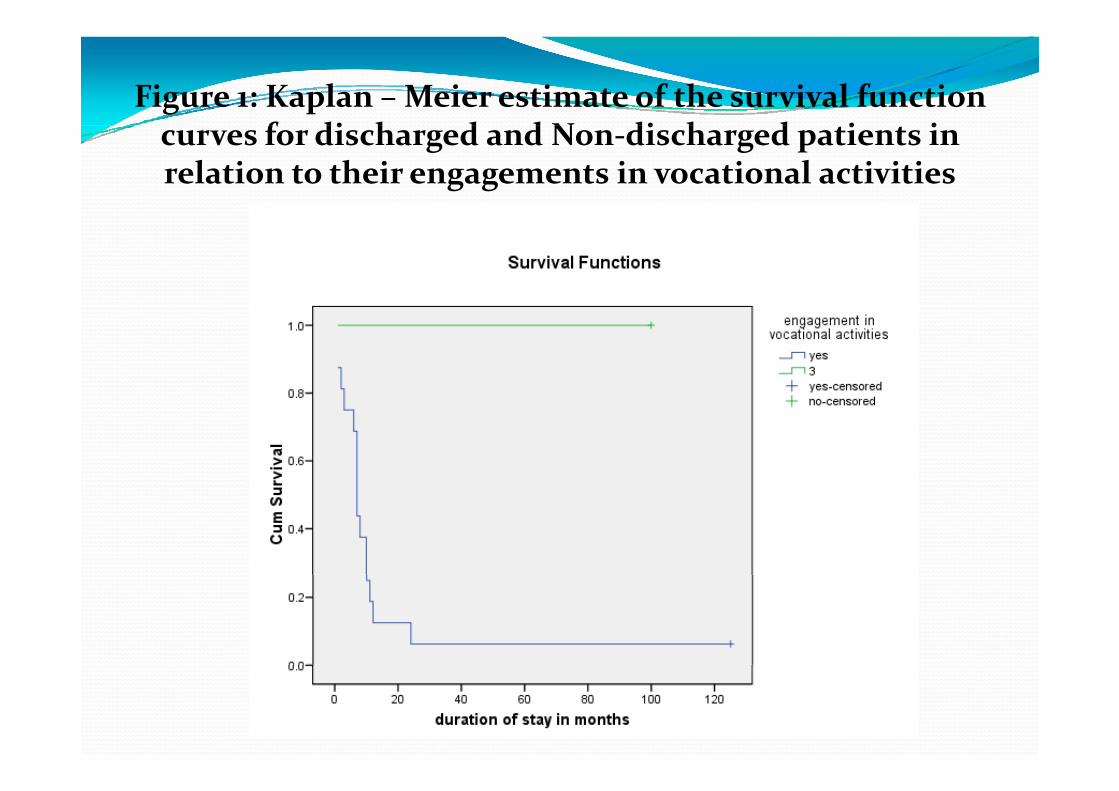
Figure 1: Kaplan – Meier estimate of the survival function f di h d d N di h d i i curves for discharged and Non‐discharged patients in
relation to their engagements in vocational activities
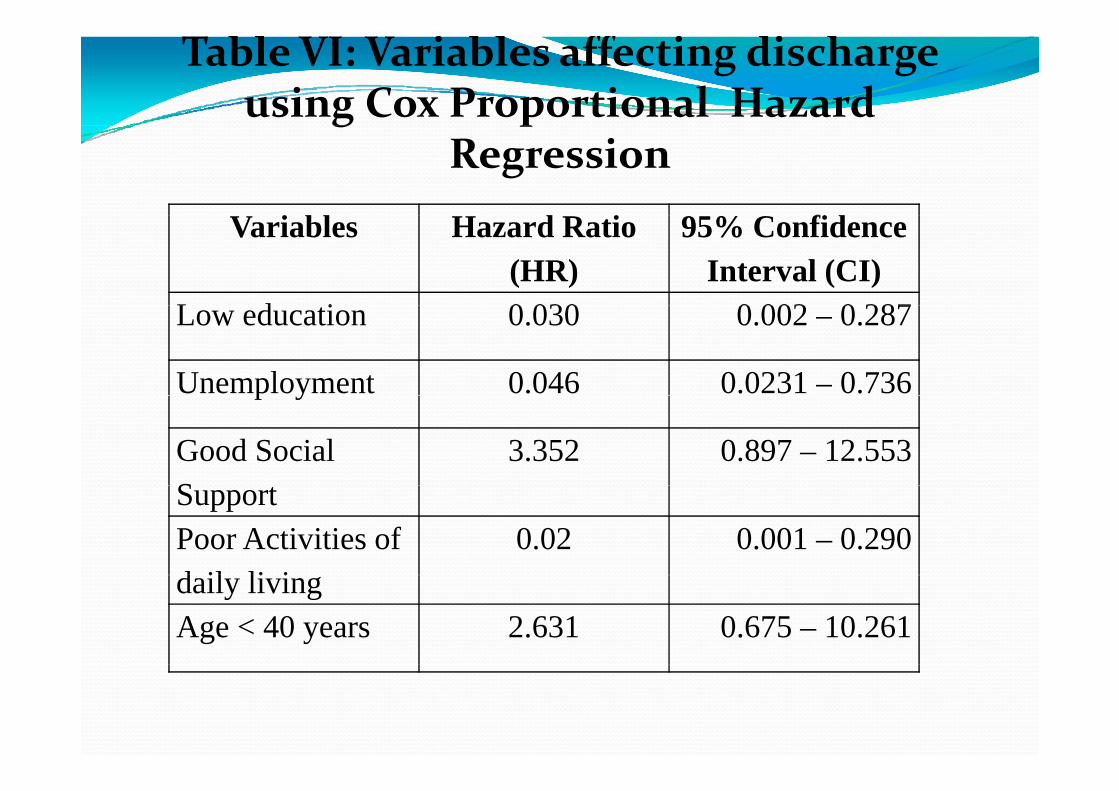
Table VI: Variables affecting discharge using Cox Proportional Hazard g p
Regression
V i bl H d R i 95% C fidVariables Hazard Ratio (HR)
95% Confidence Interval (CI)
L d i 0 030 0 002 0 287Low education 0.030 0.002 – 0.287
Unemployment 0.046 0.0231 – 0.736p y
Good Social S
3.352 0.897 – 12.553SupportPoor Activities of d il li i
0.02 0.001 – 0.290daily livingAge < 40 years 2.631 0.675 – 10.261
DISCUSSION
In our study, the socio‐demographic and rehabilitationvariables predicting good rehabilitation outcomesp g gwere high education, previous employment, youngerage, being married, having good social and familysupport, good activities of daily living and engagementin vocational activities.These findings were in variance to finding of somestudies (Strauss, 1986; Wiersma et al 1988; Wiersma et
)al, 2000; Harrison et al, 2001) that found only limitedevidence that socio‐demographic variables predict
toutcome.
DISCUSSION CONT’D
The non‐discharged group had inferior socio‐demographic profiles which could be a reflection of g p pthe severity of illness that interfered with normal role performance
LIMITATIONSAll retrospective studies have certain limitations.All retrospective studies have certain limitations.
Some patients’ case records were missing.
No baseline rating of illness severity with any standardsymptoms rating scale.y p g
For some of the patients, their ages may not be exact.p , g y
Small sample size limits generalization of resultsSmall sample size limits generalization of results
CONCLUSIONCONCLUSIONIn a sample of rehabilitation in‐service patients,we conclude that good socio demographic profileswe conclude that good socio‐demographic profilesand engagement in vocational activities weresignificantly associated with achieving dischargesignificantly associated with achieving dischargeduring the eleven year period we studied.I Ni i d h d l i i h iIn Nigeria and other developing countries, there isneed for the recognition of the role ofh bili i i dd i h drehabilitation in addressing the adverse
consequences of mental disability to thei di id l i d h iindividual, community and the nation.Future research on the dynamics and econometricsof this rehabilitation psychiatry service is highlyindicated.
Declaration of Interest –None
Acknowledgements Acknowledgements Matrons Abolaso, Adewoyin,
Multidisciplinary team members of Rehabilitation UnitMultidisciplinary team members of Rehabilitation UnitMiss Kazeem for secretarial job
Rehabilitation in Aro Psychiatric Hospital, Nigeria
The Ugly
The Bad
The Good
No Psychiatry without Rehabilitation….
References World Health Organization. Mental Health. NewgUnderstanding, New Hope, Geneva: World HealthReport 2001.
Killapsy H, Harden C, Holloway F. What do mentalhealth rehabilitation services do and what are they for?A national survey in England. Journal of mental health2005, 14: 157‐165.
Adair CE, Mc Dougall GM, Mitton CR. Continuity ofcare and health outcomes among persons with severemental illness. Psychiatric Serv, 2005; 56: 1061‐1069.
Strauss JS. Discussion: What does rehabilitationaccomplish. Schizophr Bull 1986; 12: 720‐723.
Wiersma D, Nienhuis FJ, Slooff CJ, Giel R. Naturalcourse of Schizophrenic Disorders: A 15‐year follow upf D h i id h S hi h B ll 88of a Dutch incidence cohort. Schizophr. Bull 1988; 24:
75‐85.Wi D W d li J D i k E G K Wiersma D, Wanderling J, Dragomirecka E, Ganev K,Harrison G, AnDer Heiden W et al: Social disability inSchizophrenia: Its development and prediction over 15Schizophrenia: Its development and prediction over 15years in incidence cohorts in Six European Centres.Psychol med 2000; 30: 1155‐1167Psychol med 2000; 30: 1155‐1167.
Harrison G, Hopper K, Craig T, Laska E, Siegel C,Wanderling J et al Recovery from psychotic illness: aWanderling J, et al. Recovery from psychotic illness: a15 and 25‐ year international follow‐up study. Br. J.Psychiatry 2001; 178: 506‐517.Psychiatry 2001; 178: 506 517.
Rogers ES, Anthony W, Lyass A. The nature anddimensions of social support among individuals withpp gsevere mental illnesses. Common Ment. Health J.2004; 40: 437‐450.
Rosler W. Psychiatric rehabilitation today: AnoverviewWorld Psychiatry. October 2006: 151‐157.
Boroffka A. Psychiatric Care in Nigeria.Psychopathologic Africaine 1995‐1996; XXVII; 1: 27‐36.

GOD BLESSGOD BLESS
THANKS FOR LISTENING
QUESTIONS?????QUESTIONS?????QQ