Embed Size (px)
Citation preview

Outcome of patients with hematologic malignancy admitted to the ICU
Geeta Mehta MD, FRCPC
Mount Sinai Hospital
Toronto, Canada
CCCF
November 2, 2016

Disclosures

Hematologic Malignancy
• Advances in diagnostics, risk stratification and treatment regimens including hematopoietic cell transplantation (HCT)
• Aggressive treatment has been extended to higher risk candidates: older, more comorbid illness, receiving salvage chemotherapy
• More dose-intensive regimens, or novel approaches to HCT (mismatched, haploidentical, cord blood transplant )
• As a consequence, there has been an increased risk of serious complications and need for ICU care.

Complications
• Infectious
• Chemotherapy related
• HCT related
• Bleeding
• Acute respiratory failure
• GVHD
• Sinusoidal Obstructive syndrome
• etc…

ICU survival has improved
• In 1999, the American College of Critical Care Medicine stated: ‘patients with HM are poor candidates for ICU admission with a mortality rate of up to 90%. Immediate treatment limitation/refusal of ICU admission is advocated’ (Crit Care Med 1999)
• Recent reports showing improved ICU survival rates challenge this perception
• Mount Sinai Hospital
– Between 2012 and 2015, 420 patients from Princess Margaret Hospital were admitted to ICU
– ICU mortality 32%
• > 500 ICU admissions annually in Canada


We need more data
• More multi-center and population studies are needed to evaluate outcomes and predictors
• Functional outcomes
• Patient and family perspectives
• Advance Care Planning
• Clinical Practice Guidelines

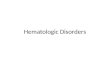
AJRCCM 2016
age > 66 yrICU LOS >2 wk

• Retrospective chart review
• 151 consecutive patients with AML and ALL admitted to Mount Sinai Hospital Medical-Surgical ICU, a 16-bed ICU affiliated with the University of Toronto
• 2009 to 2012
• Objective: to describe ICU interventions, short and long-term outcomes, and predictors of outcome

Patient Characteristics
Age, years 54 (15)
Female 76 (50%)
APACHE II 27 (22-33)
SOFA 10 (8-13)
MODS 7 (6-10)
Neutropenia (<500) 84 (74)
Thrombocytopenia (<50) 126 (86)
Admission Diagnosis
Sepsis 74 (49)
Respiratory 46 (31)
Cardiovascular Failure 14 (10)
Gastrointestinal Bleed 3 (2)
Neurological Dysfunction 8 (5)

N (%)
Leukemia Type
Acute Myeloid Leukemia
Acute Lymphoblastic Leukemia
118 (78)
33 (22)
Chemotherapy Stage
Induction
Consolidation
Intensification Phase
Reinduction for Relapse
Reinduction for Non-response
Not Provided Chemotherapy within 40 days
No Pharmacy Records
55 (36)
9 (6)
5 (3)
29 (20)
12 (8)
33 (22)
3 (2)
Leukemia Factors
CNS Infiltration
HCT before ICU
Allogeneic
Autologous
GVHD
9 (6)
20 (13)
17
3
11 (7)
Leukemia Characteristics (N=151)

Outcomes
ICU stay 4 days (2-8)
Survival
ICU 62%
30-day 49%
90-day 40%
6 months 34%
12 months 25%

Characteristics of ICU survivors and non-survivors at ICU
discharge and 1-year post ICU admission

Characteristics of ICU survivors and non-survivors at ICU
discharge and 1-year post ICU admission

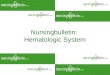
Multivariable analysis of independent predictors of
ICU mortality
VariableOdds Ratio Estimates
(95% CI)P Value
SOFA
Induction Stage at ICU admission
Relapse Stage at ICU admission
Age
Septic Shock
Invasive Ventilation
1.18 (1.01-1.38)
0.43 (0.16-1.17)
0.49 (0.14-1.66)
1.01 (0.98-1.05)
4.06 (0.97-7.50)
9.64 (3.39-27.40)
0.03
0.09
0.25
0.39
0.057
<0.001

Other Canadian studies
Study Patients N ICU
Mortality
1 year
mortality
Krajuljak AML/ALL 151 38% 75%
Cornish 2016 HM 206 45% 74%
Roze des Ordons 2010 AML 45 44% 71%
Trinkaus 2009 Auto-SCT 34 38%
Scales 2008 HCT 504 74%

Crit Care
2008
• OHIP database
• Adults (>18 years) who underwent BMT1992 to 2002


Internationally - Single center studies
Study Country Patients N ICU
Mortality
1 year
mortality
Kroschinsky 2002 Germany HCT 104 44% 71%
Massion 2002 Belgium HM 84 38 75%
Afessa 2003 US HCT 112 33
Rabbat 2005 France AML 83 34 49%
Bruennler 2007 Germany HM 94 43
Ferra 2007 Spain HM 100 49
Thakkar 2008 US AL 90 68
Silva 2013 Mexico HM 102 46
Bird 2012 UK HM 199 34
Hill 2012 UK HM 147 73
Hampshire 2014 UK – 3
centers
HM 187 49
Medic 2015 Croatia HM 170 54

Grrr-OH: Groupe de recherche respiratoire en réanimation
onco-hématologique
17 centers in France and Belgium
Study Patients N ICU Mortality Hospital
Mortality
Azoulay 2013 HM 1011 39%
Lengline 2015Allo-HCT 497 51% 90-day
Mokart 2015 Neutropenic 289 45% 75%
Lemiale 2015 HM - ARF 382 32%
Darmon 2015 HM - AKI 671 38%

Independent Predictors of Mortality
• Azoulay 2013: Poor performance status, Charlson
comorbidity index, allogeneic HSCT, organ dysfunction
score, cardiac arrest, acute respiratory failure, malignant
organ infiltration, and invasive aspergillosis
• Mokart 2015: allogeneic HCT (OR 3.83; 95 % CI 1.75–
8.35), MV (OR 6.57; 95 % CI 3.51–12.32),
microbiological documentation (OR 2.33; CI 1.27–4.26),
RRT (OR 2.77; 95 %CI 1.34–5.74)
• Lengline 2015: GVHD, MV, RRT
• Darmon 2015: AKI (OR 1.65, 95% CI 1.19-2.29)

Summary
• Patients with hematologic malignancy
– ICU mortality 40%; 1 year mortality as high as 75%
• Not possible to predict outcome with 100%
certainty
• Cannot justify denying these patients ICU
admission
• Independent predictors of mortality vary
– Pre-morbid functional status may be as
important as HM and acute illness variables

Urgently needed…
• Multicenter outcome studies on patients with HM who require ICU admission
• Population based data on survival and functional outcomes
• Comprehensive evaluation of the factors contributing to long term morbidity in patients who survive their critical illness
• Patients, families, and clinicians will benefit from knowing which patients survive, and the challenges faced by survivors and their families

JAMA 2016

COHOCritical Care Outcomes of Patients with
Hematologic Malignancy or Hematopoietic
Cell Transplant

Vision: To become a world class centre
in providing critical care services to
oncological patients
Mission: To provide the best critical care
for oncological patients by having optimal
knowledge, communication, and
research development through
collaborations of all stakeholders
Focus on:
1. Clinical Knowledge
2. Education
3. Research
4. Quality Improvement
Examples of Projects by COIN Members
AFI TOPIC
1 Acute Promyelocytic Leukemia
Outcomes Study
2 Interhospital Transfer
3 Intrahospital Transfer
4 Data Mapping
5 Medications (Tumor Lysis Mgt)
6 Education
7 Advance Care Planning
8 Blood Bank
9 Hickman Line
10 Hypoxia post BMT
Quality Improvement Initiative
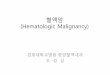
Critical Care Oncologic Investigative Network
(COIN)

Intensivists Patients
Family Members
Palliative care
Hematologists
Transplant
physicians
Rehab
specialistsDieticians
Pharmacists
Spiritual
Care