Embed Size (px)
Citation preview
Ovary
Dr. Raid Jastania
Ovary
• Salpingo-oophoritis
• Endometriosis
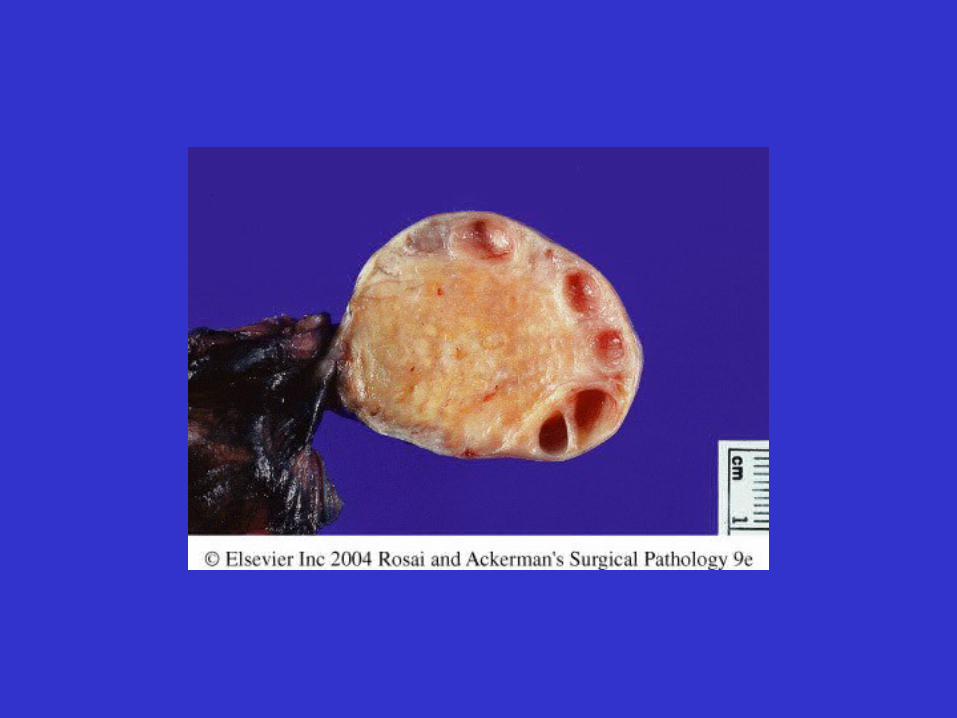
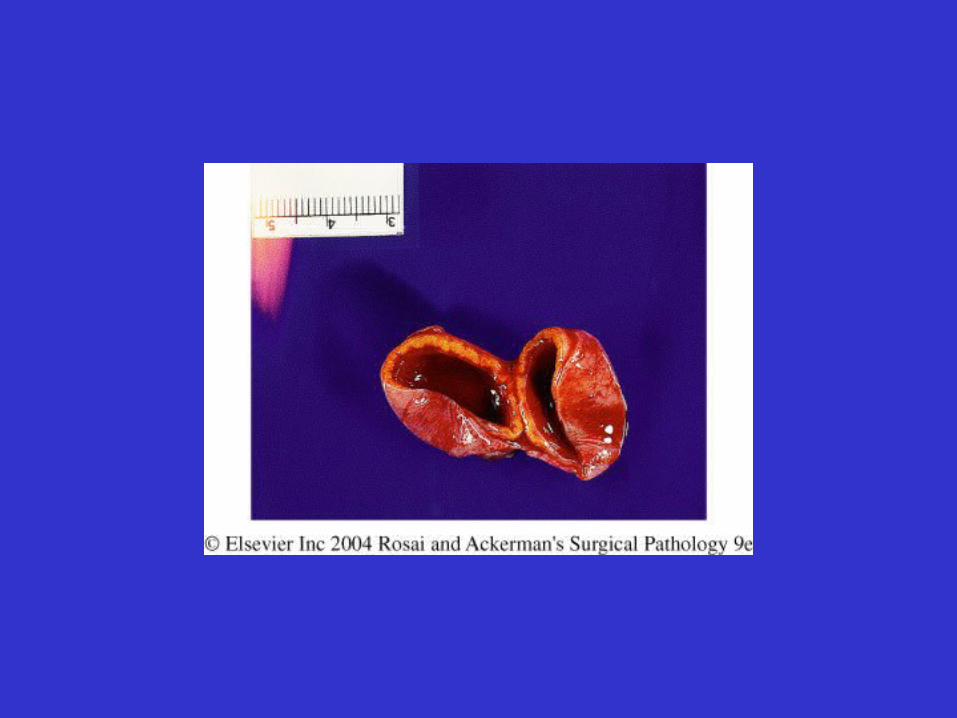
• Cysts– Follicle cyst– Luteal cyst– Common, 1-1.5 cm, clear fluid– May be palpable, cause pain or acute abdomen
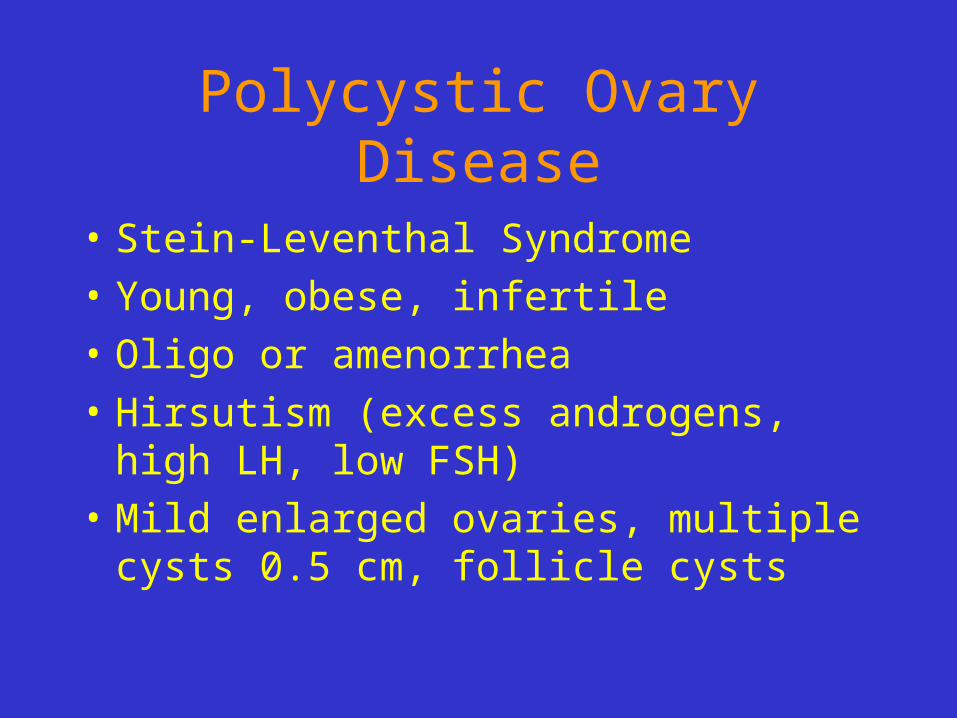
Polycystic Ovary Disease
• Stein-Leventhal Syndrome
• Young, obese, infertile
• Oligo or amenorrhea
• Hirsutism (excess androgens, high LH, low FSH)
• Mild enlarged ovaries, multiple cysts 0.5 cm, follicle cysts
Case Presentation
• 52-year-old, fit, slim former dancer goes to her internist because of vague abdominal pain and a feeling of fullness. Her medical history is noncontributory. Her gynecologic history includes: menarche, age 13; coitarche, age 18; lifetime sexual partners, 3; no IV drug use or transfusions. Her internist examines her, but can find no problems, so he sends her to a gastroenterologist. The GI specialist examines her, finds no problems, and orders upper and lower GI studies, which are negative
• The woman continues to see these physicians, with worsening symptoms, over five months; it is decided that, because no disease has been found, she needs a psychiatric consultation to aid with her developing anxiety and depression. The psychiatrist knows he needs to exclude organic disease before he treats emotional symptoms, so he performs a physical examination. He notes abdominal fullness with a fluid wave, consistent with ascites. He also performs a pelvic examination. A 10-cm left adnexal mass is easily felt.
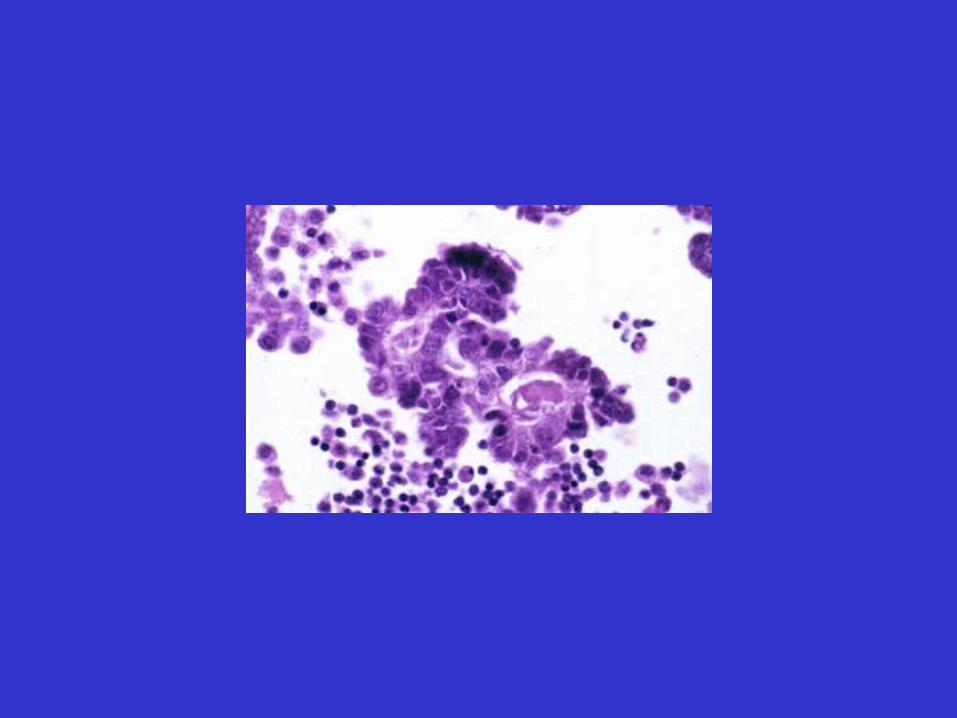
• Cytologic examination of the ascitic fluid is performed. At laparotomy, a tumor is diagnosed by the pathologist by doing a frozen section. Tumor is found to have spread to her other ovary, omentum, and numerous sites on her peritoneum. She receives chemotherapy, but dies one year after diagnosis.
Ovarian Tumors
• Ovarian carcinoma is the 5th most common cancer in US
• Classification:– Surface epithelial tumors– Germ cell tumors– Sex cord-stromal tumors
Ovarian Tumors
• Risk factors:– Nulliparity– Family history (5-10% are familial)– BRCA1, BRCA2– K-ras, P53
Ovarian tumors
• Presentation: mass, pressure, obstruction, torsion
• Pseudomysoma• Hormone production• Meigs syndrome (ovarian tumor, ascites
and hydrothorax)• Krukenberg tumor (metastatic gastric
cancer to the ovary)
Classification of Ovarian Tumors
• Surface epithelial tumors– Serous
– Mucinous
– Endometrioid
– Clear cell
– Brenner
• Sex cord tumors– Fibroma/Thecoma
– Granulosa cell tumor
– Sertoli-Leydig cell tumor
• Germ cell tumors– Dysgerminoma
– Teratoma• Mature
• Immature
– Embryonal carcinoma
– Yolk sac tumor
– choriocarinoma
• Surface epithelial-stromal tumors
• Classification : – Bening, borderline (low malignant potential),
Malignant
– Serous– Mucinous– Endometrioid– Clear cell– Brenner tumor
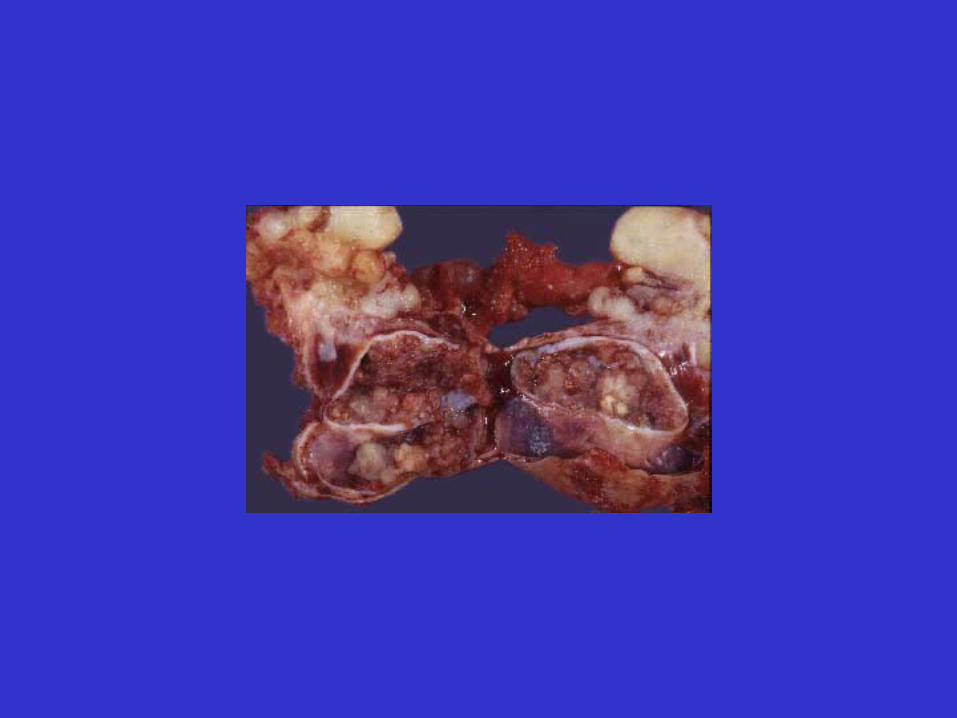
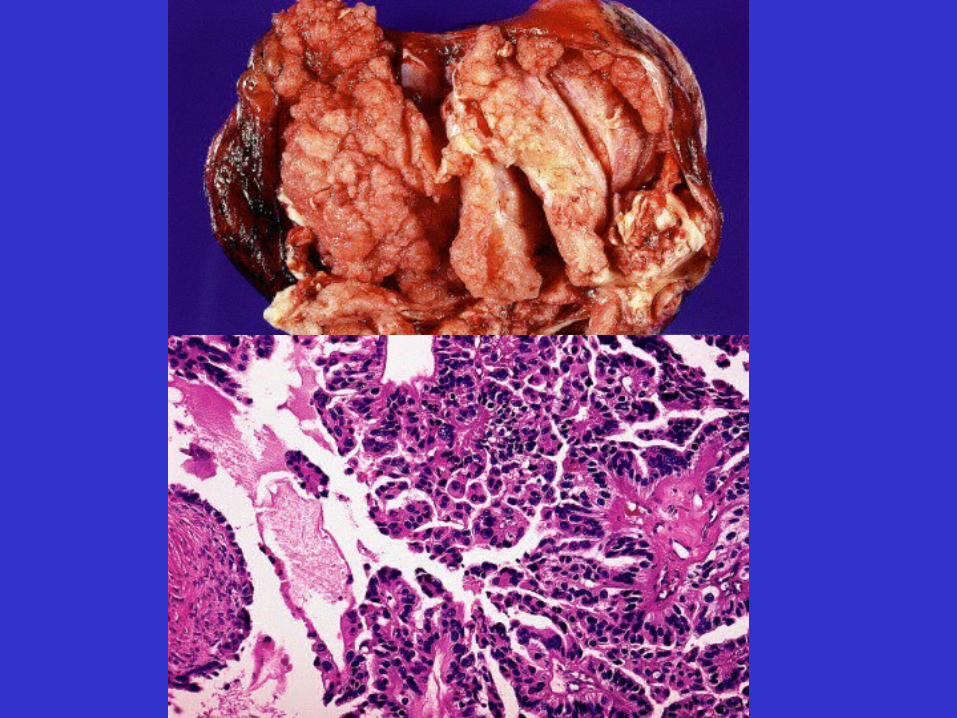
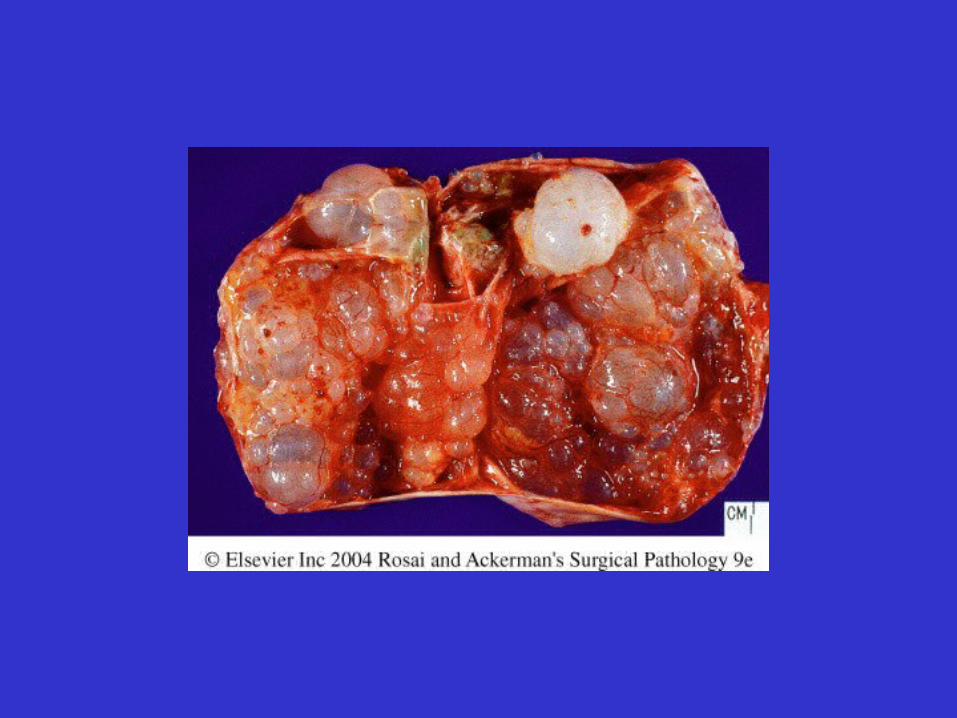
Serous tumors
• 60% benign, 15% LMP, 25% malignant
• Cystic – feature of benign (cystadenoma, cystadenofibroma
• Solid- fearture of malignant
• Papillary projections, nodular
• 25% are bilateral
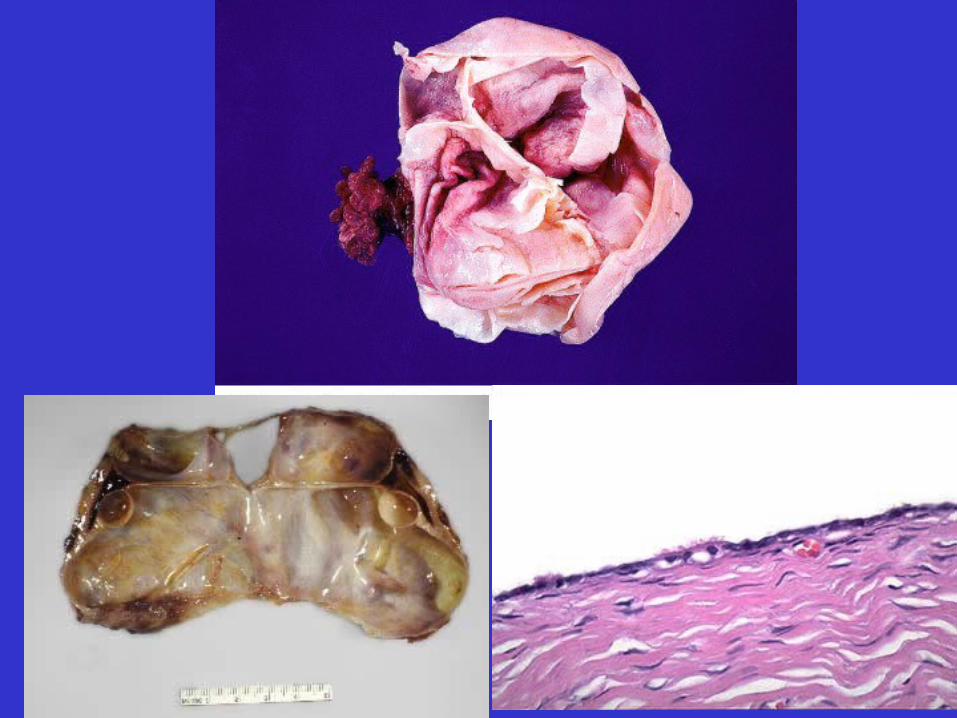
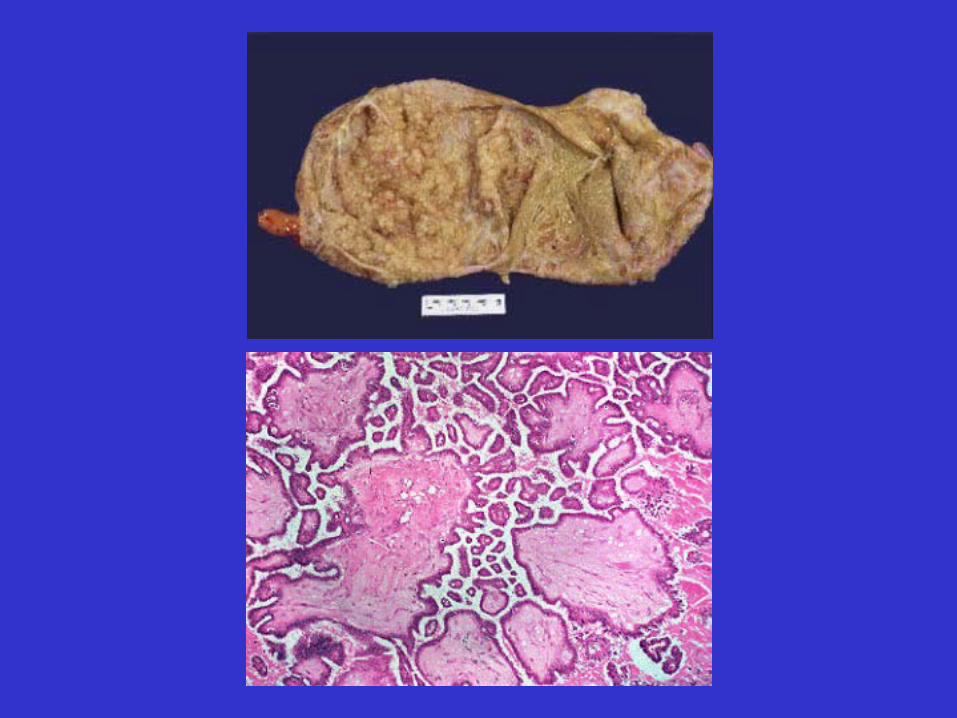
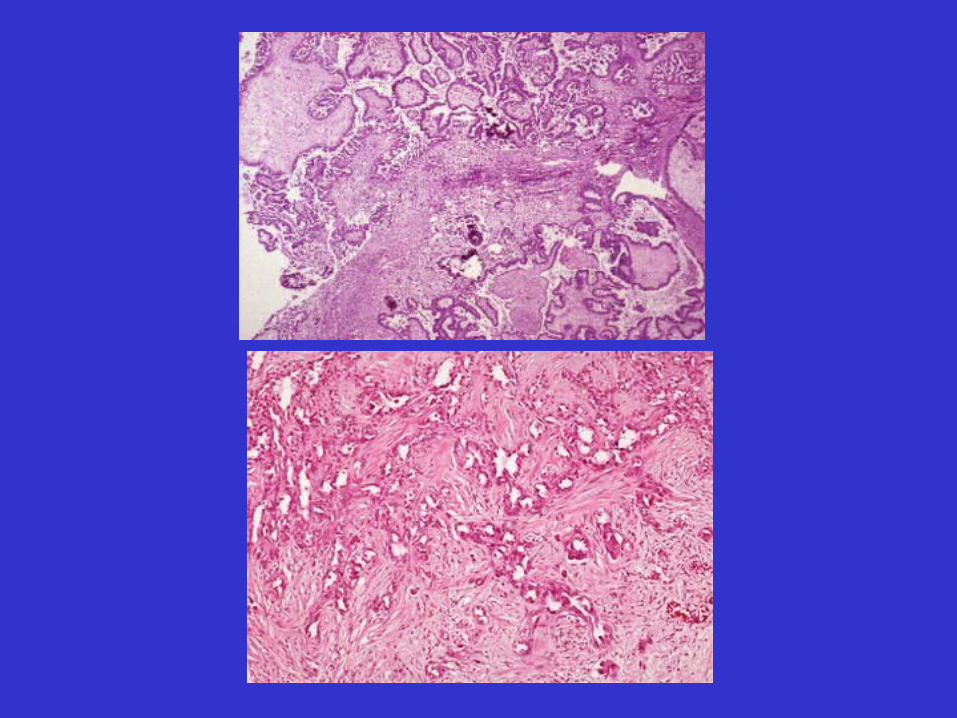
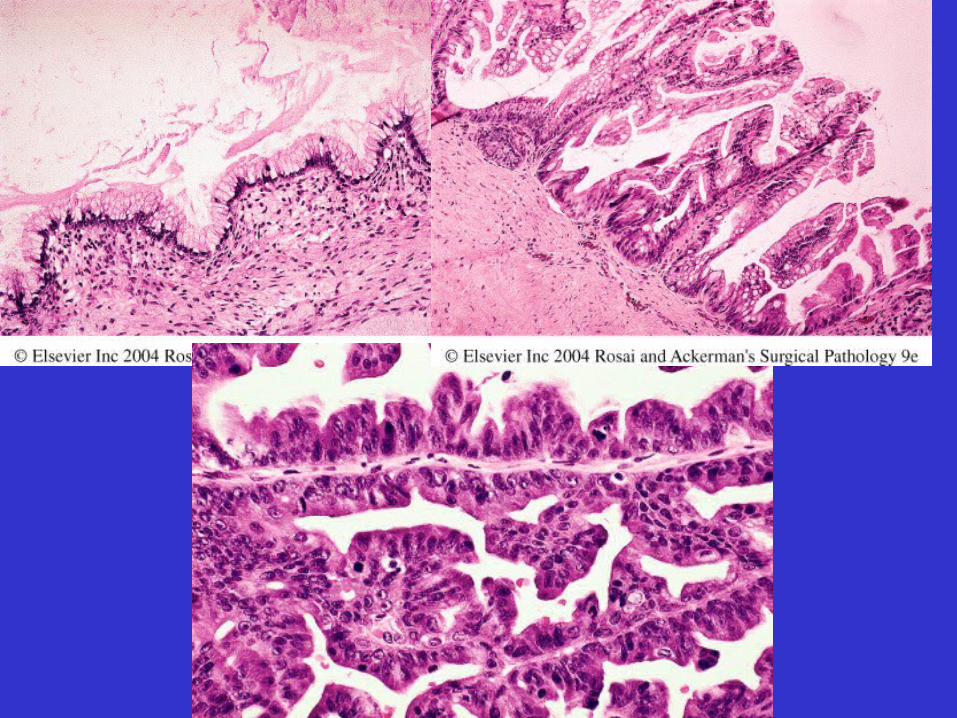
Serous tumors
• Benign- single layer of cuboidal/columnar epithelium
• LMP- papillary projections
• Carcinoma- invasion of stroma, features of malignancy
Serous tumors
• Prognosis:
LMPMalignant Carcinoma
Limited to ovary
100% 70%
Extend beyond ovary
80% 13%
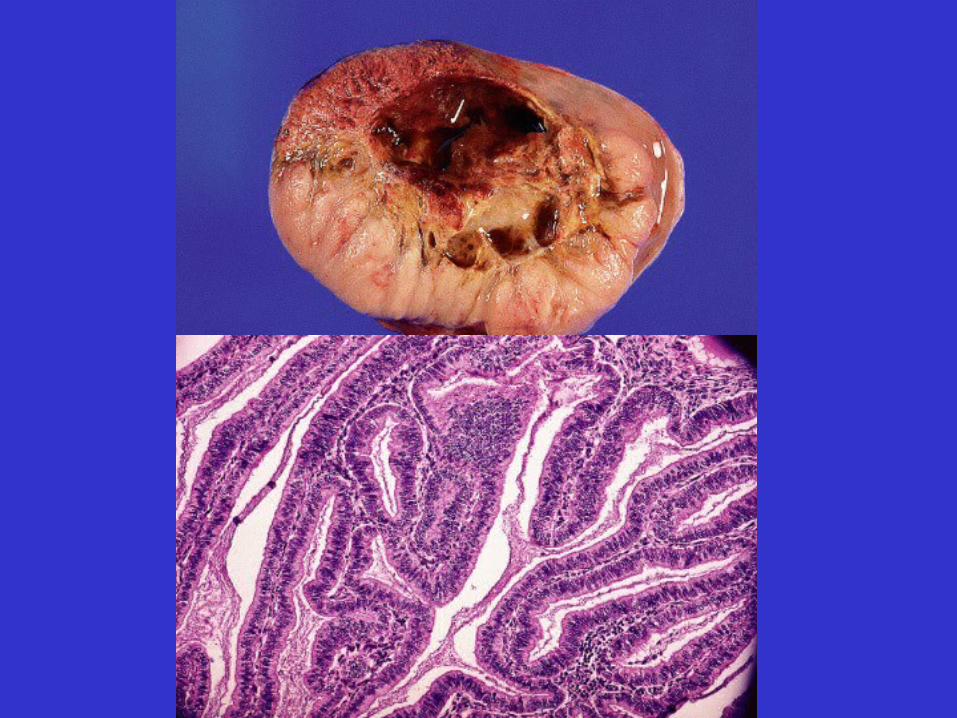
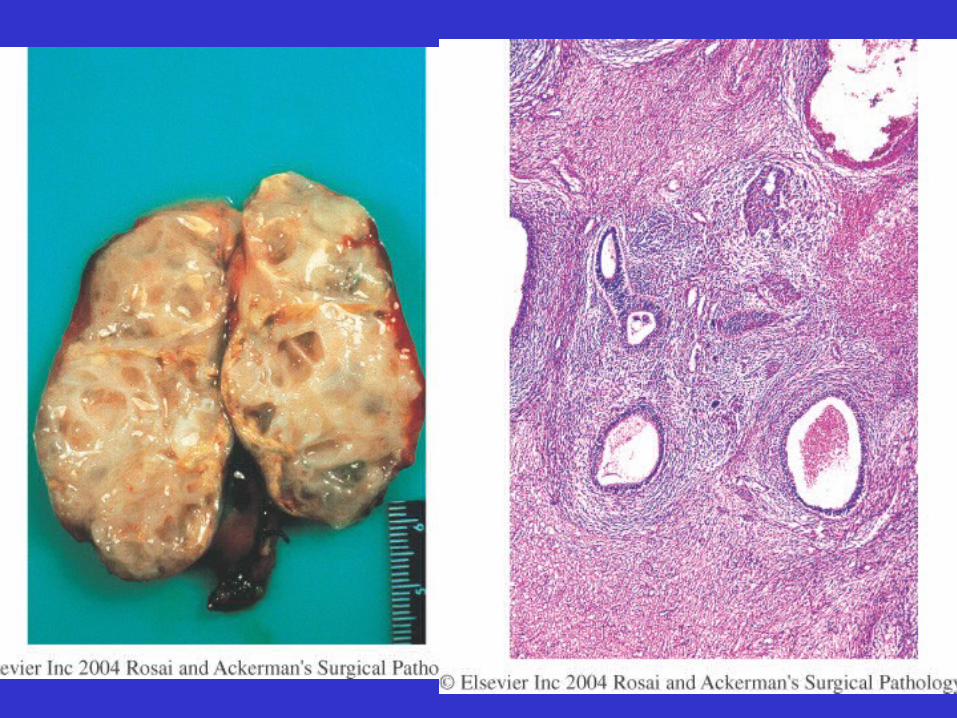
Mucinous Tumors
• Similar to serous
• Can be benign, LMP or malignant
• The lining is mucus producing epithelium
• Benign>malignant
• Usually multilocular
• May present as Pseudomyxoma peritonei
Endometrioid tumors
• Mostly malignant
• Associated with endometrial carcinoma in 15-30% of cases
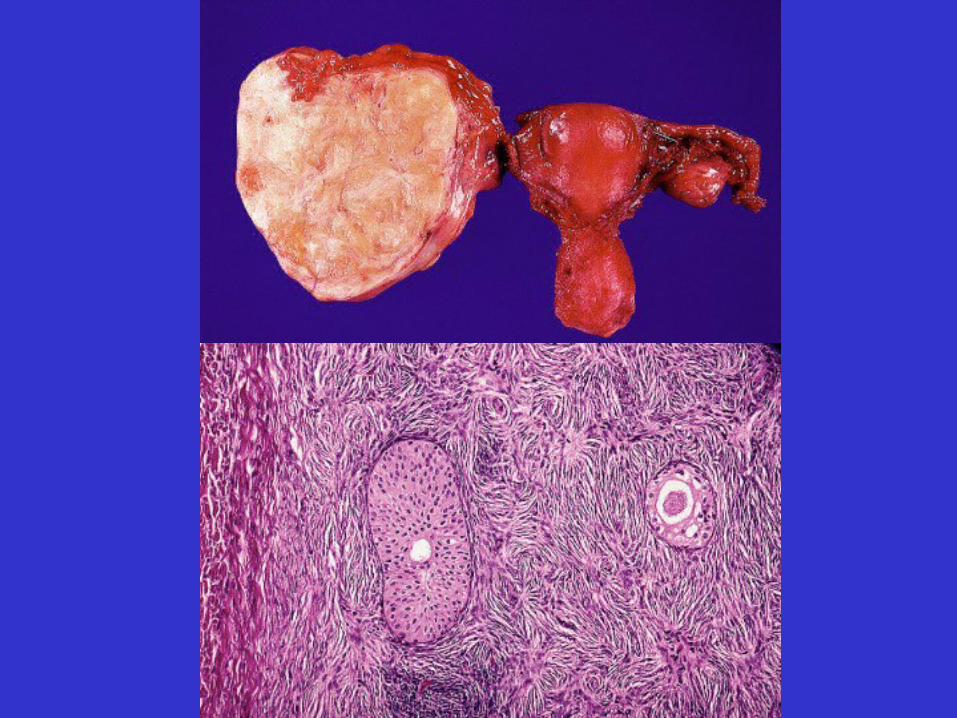
Brenner Tumor
• Small, solid
• Incidental
• Transitional epithelium
• Mostly benign
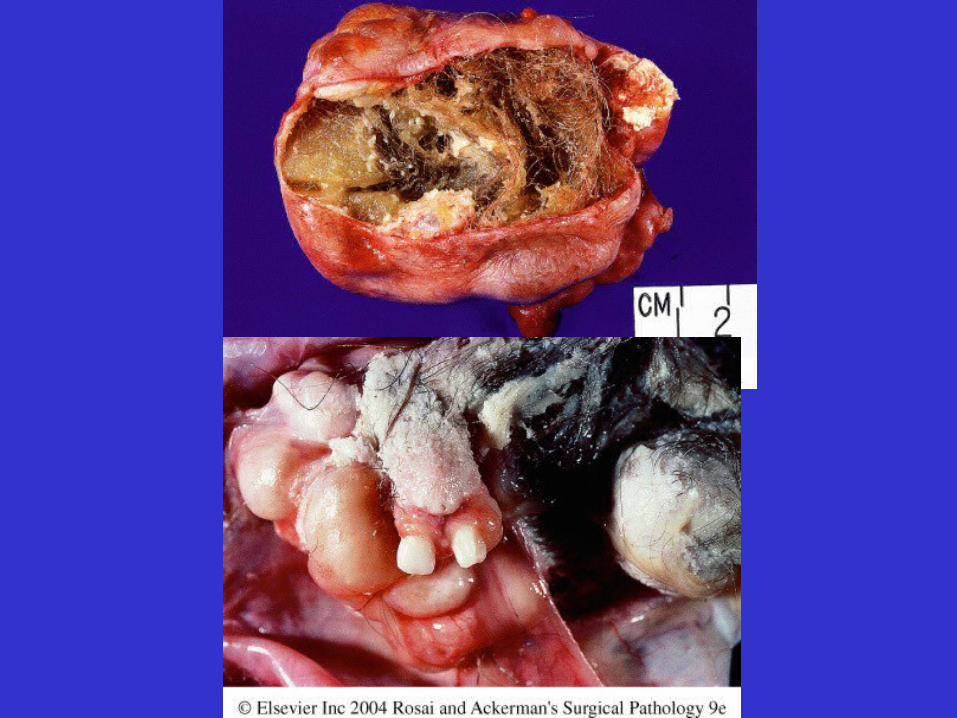
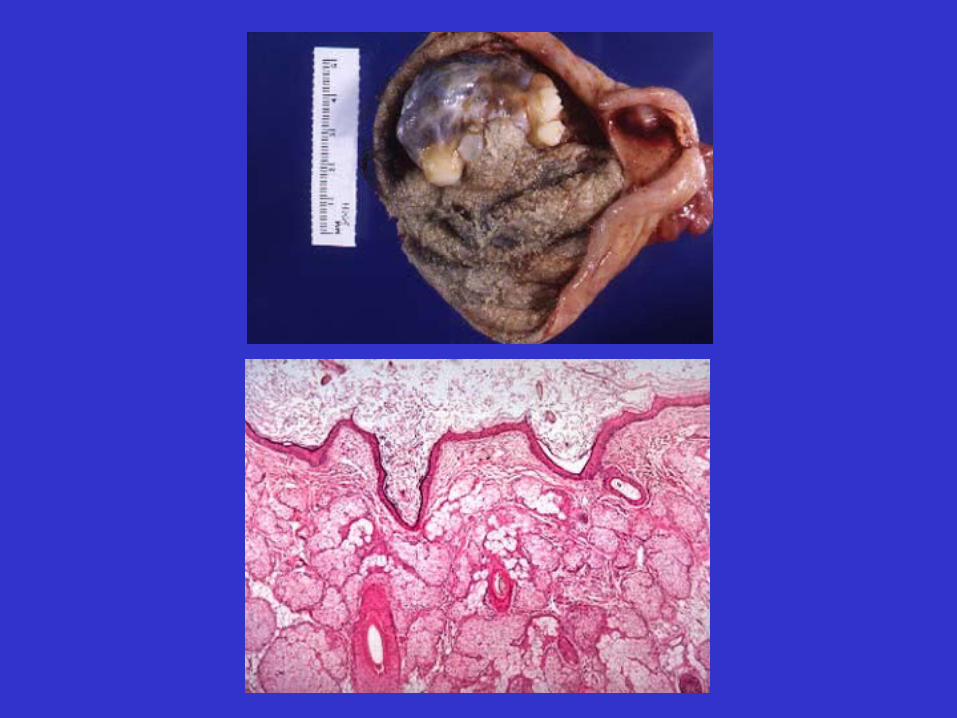
Germ Cell Tumors
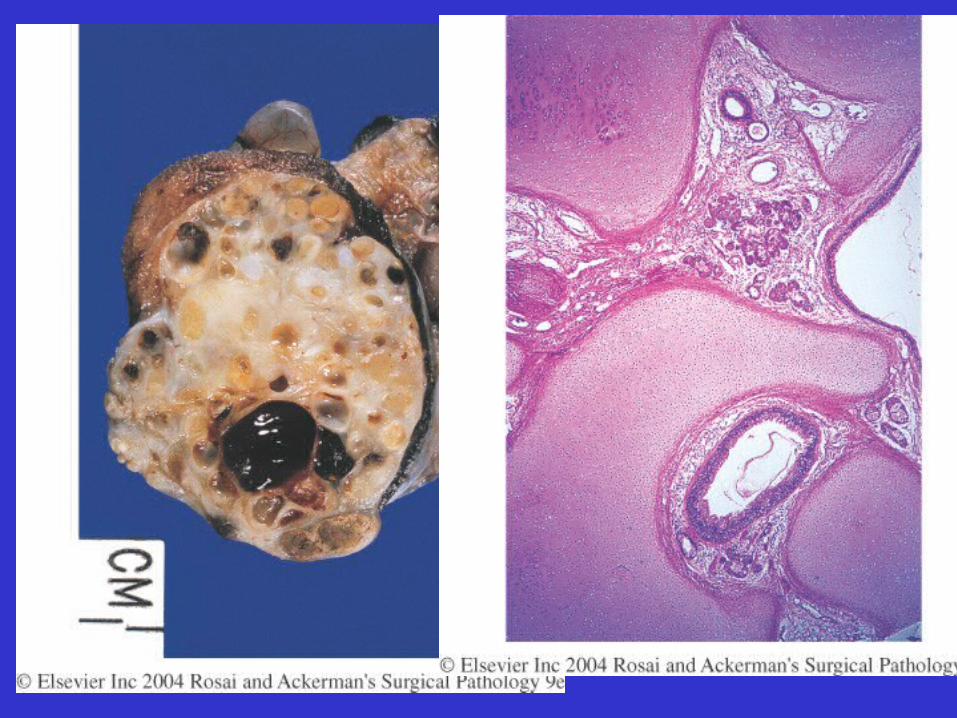
• Mature cystic teratoma (dermoid cyst)– Incidental, mass lesion, torsion, infertility– 90% unilateral– Can show all the 3 germ lines (endoderm,
ectoderm, mesoderm)• skin, appendeges, hair, sebaceous gland
• bone, cartilage, teeth, muscle
• neural tissue

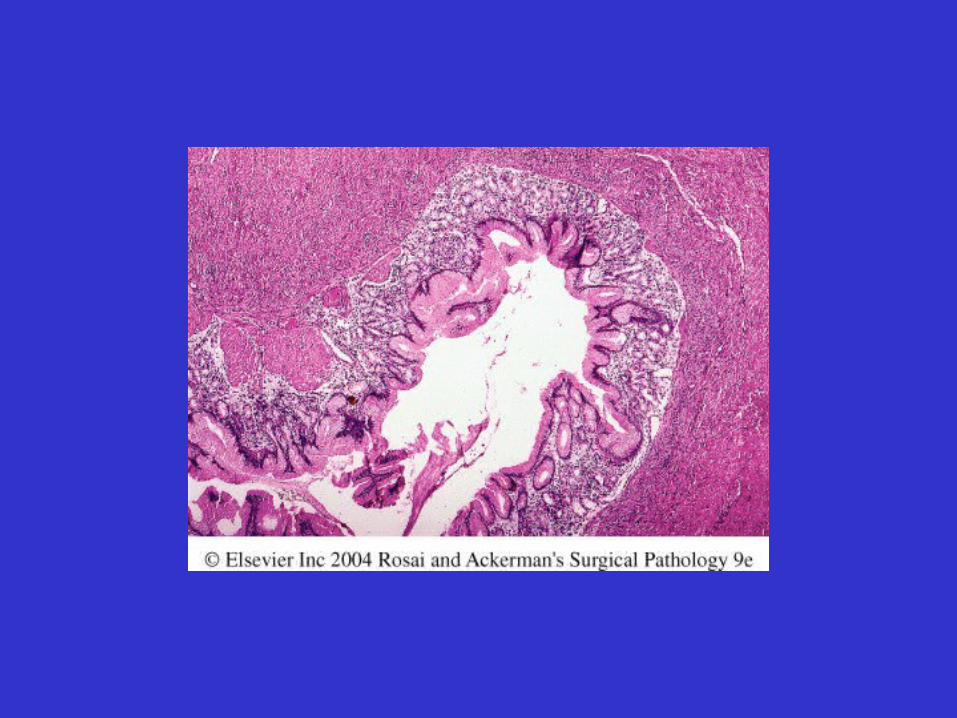
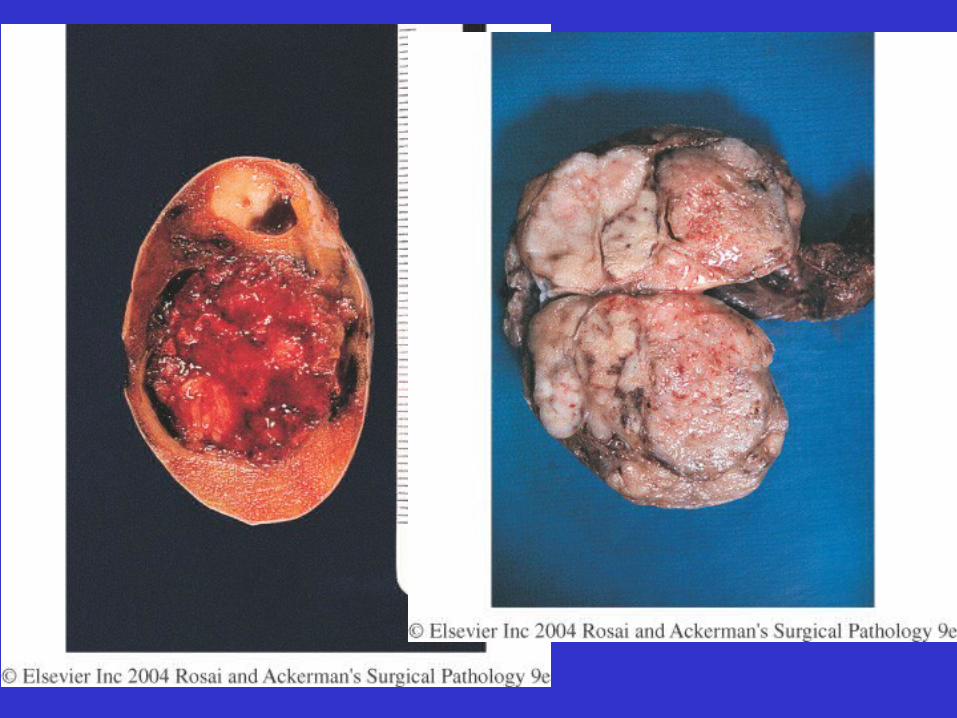
Germ Cell Tumors
• Immature Teratoma– 18 years– Bulky solid– Mostly mesoderm: cartilage, bone, muscle– Ectoderm: neural tissue
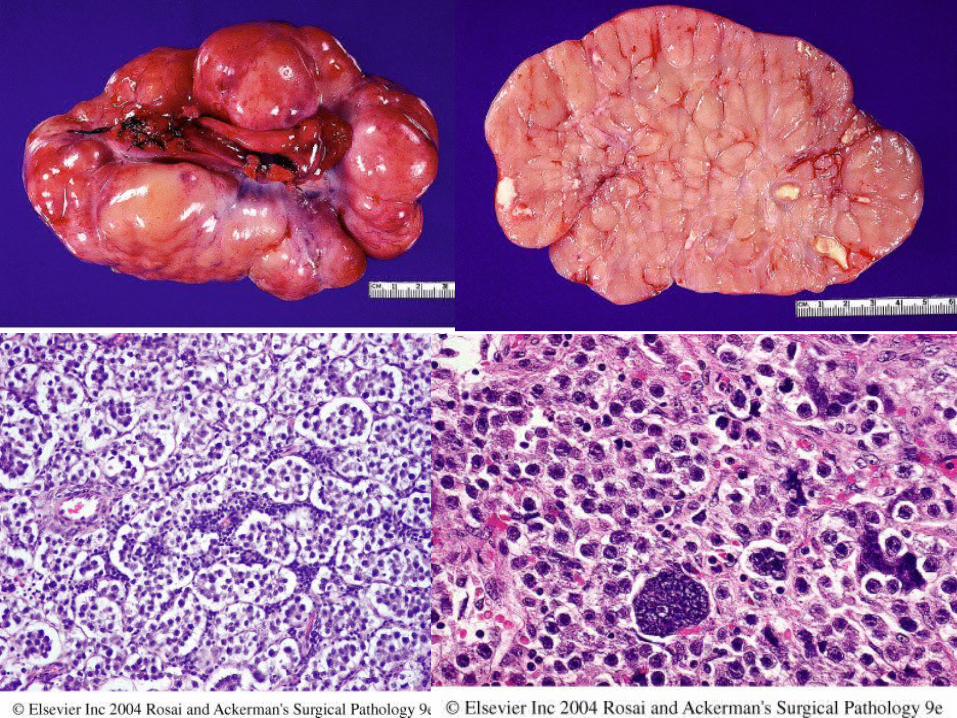
Germ Cell Tumors
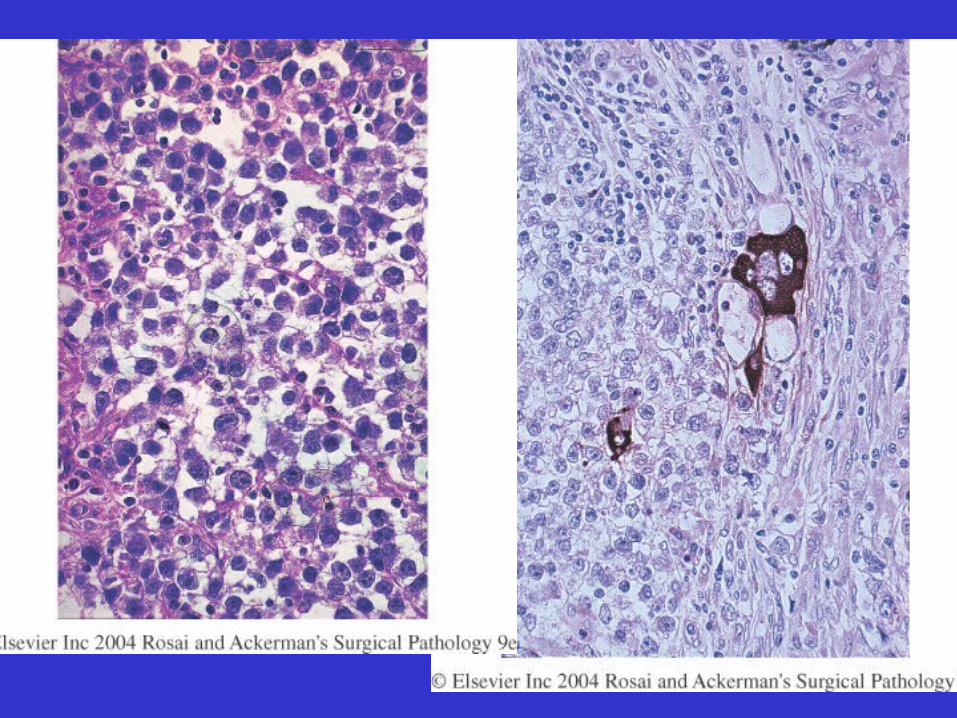
• Dysgerminoma– Malignant tumor– Similar to seminoma in males– 2nd or 3rd decade– Associated with gonadal dysgenesis– Solid large turmors– Sheets of large cells – Lymphoid component
Germ Cell Tumors
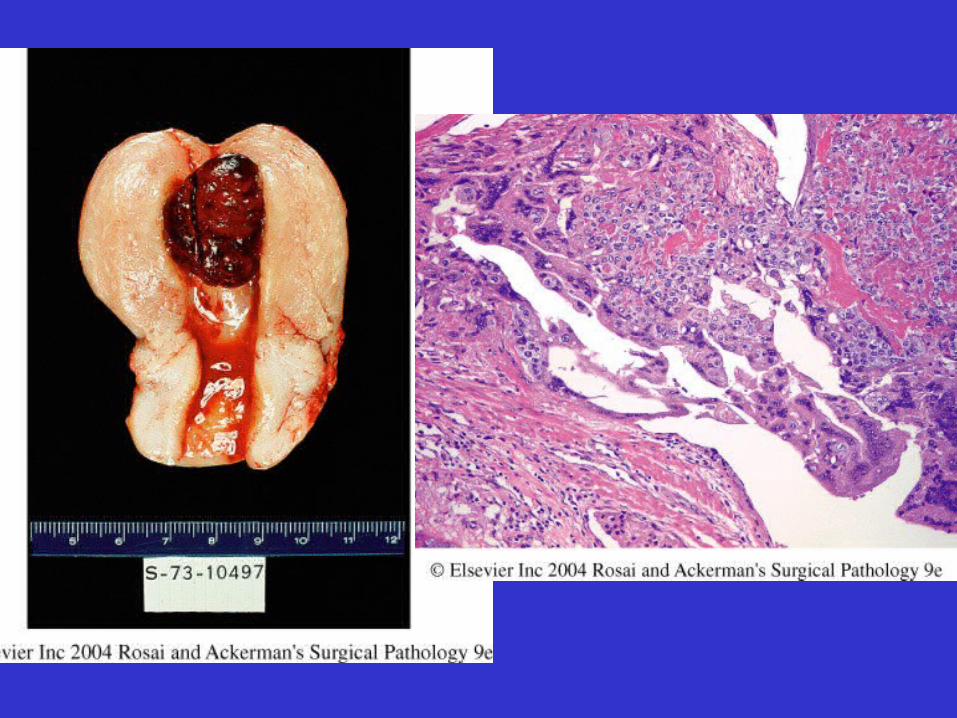
• Choriocarcinoma:– Young adults– Small hemorrahgic– Cytotrophoblast, syncytiotrophoblast– Metastasize early.
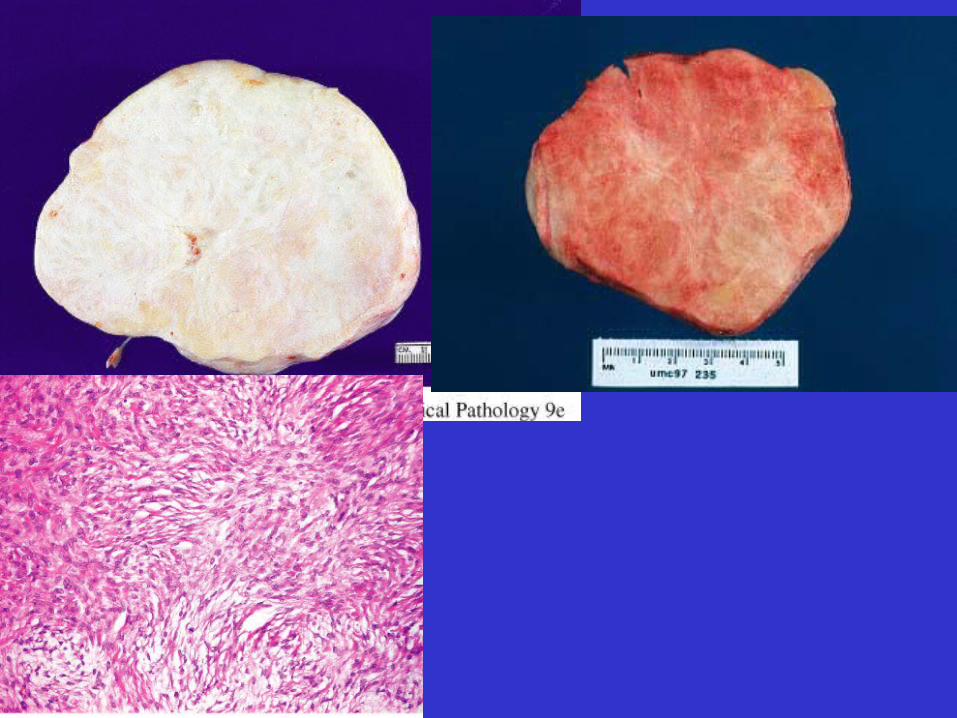
Sex cord tumors
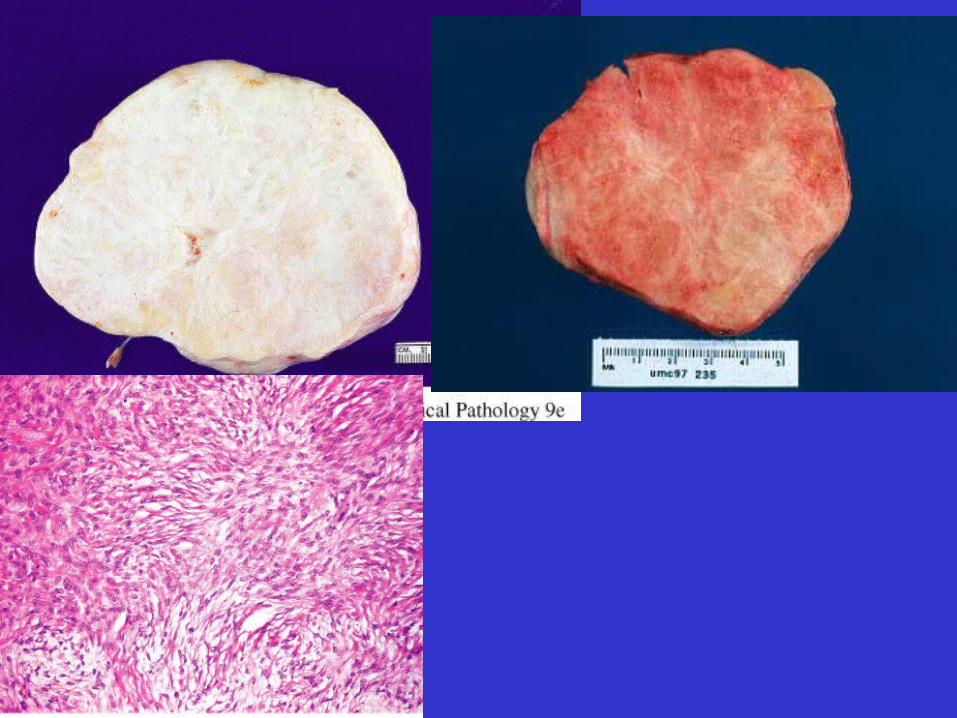
• Fibroma-thecoma– Benign– Solid gray fibrous– Can produce estrogen– Meigs syndrome (ascites and hydrothorax)– Fibrous proliferation with theca like cells
Sex cord tumors
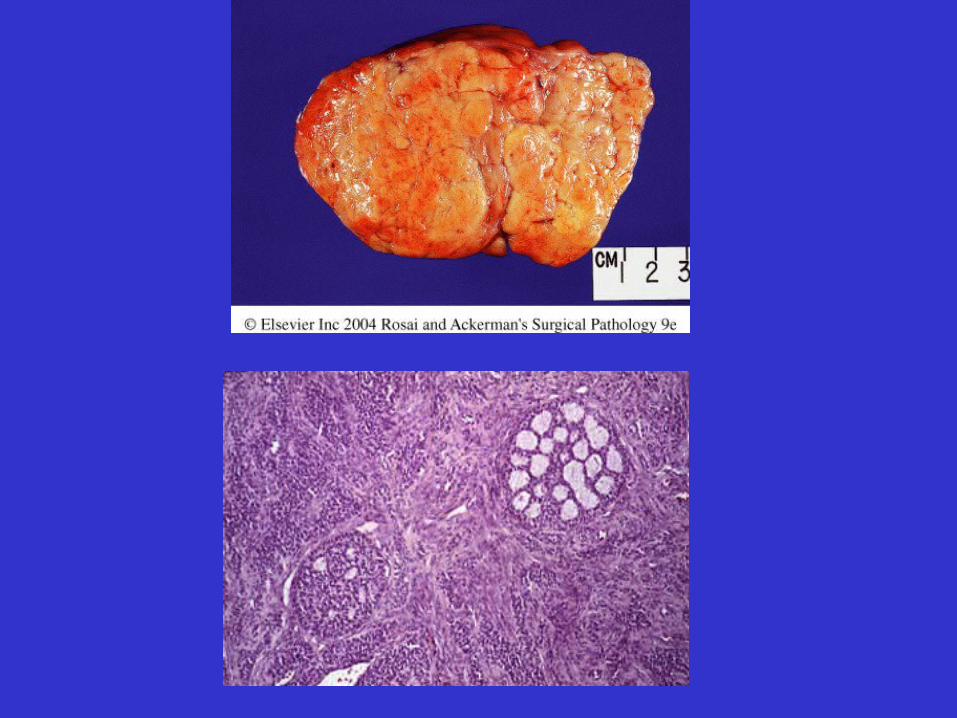
• Granulosa cell tumor– Postmenopausal– Solid mainly with small cysts– Gray yellow– Call-Exner bodies– Most produce estrogen (risk for breast and
endomertial cancer)
Sex cord tumors
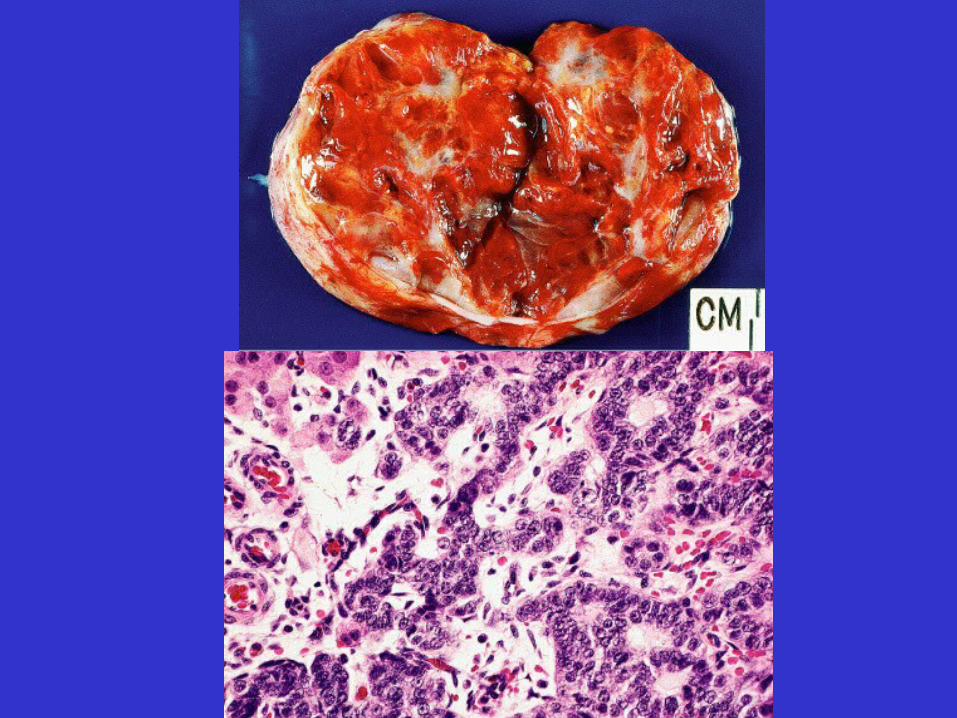
• Sertoli-Leydig cell tumor– Small yellow-orange-brown – Produce androgen
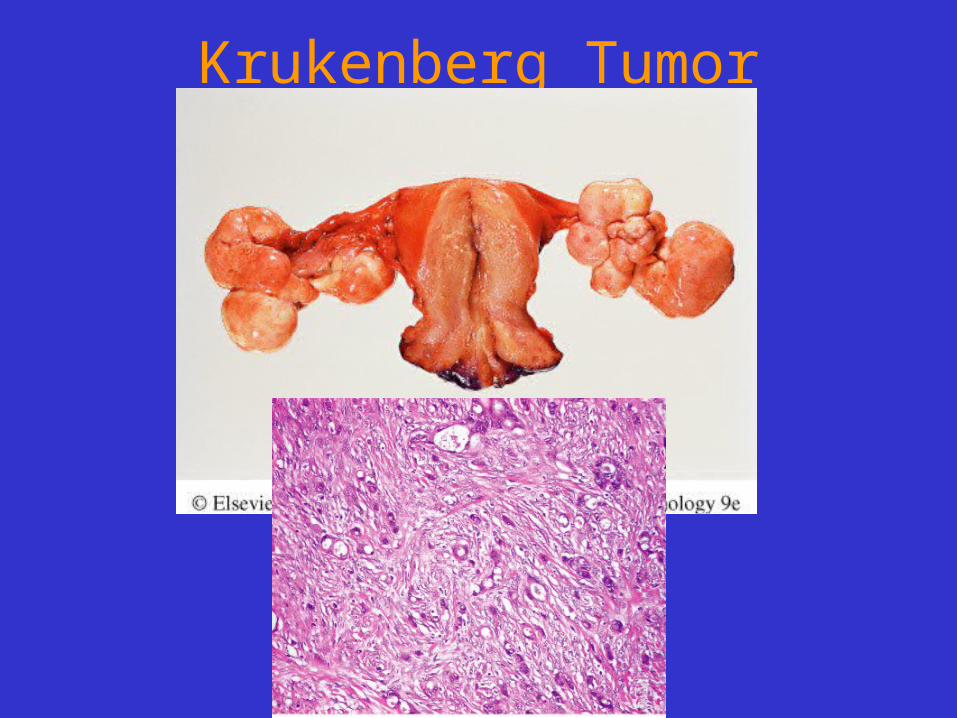
Krukenberg Tumor
Pictures
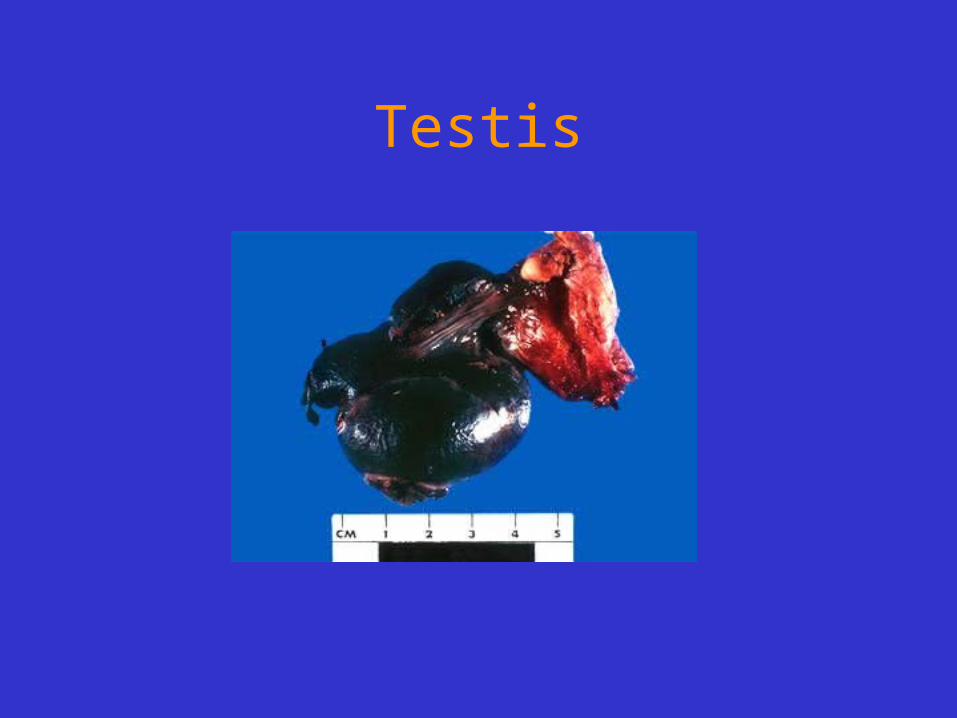
Testis
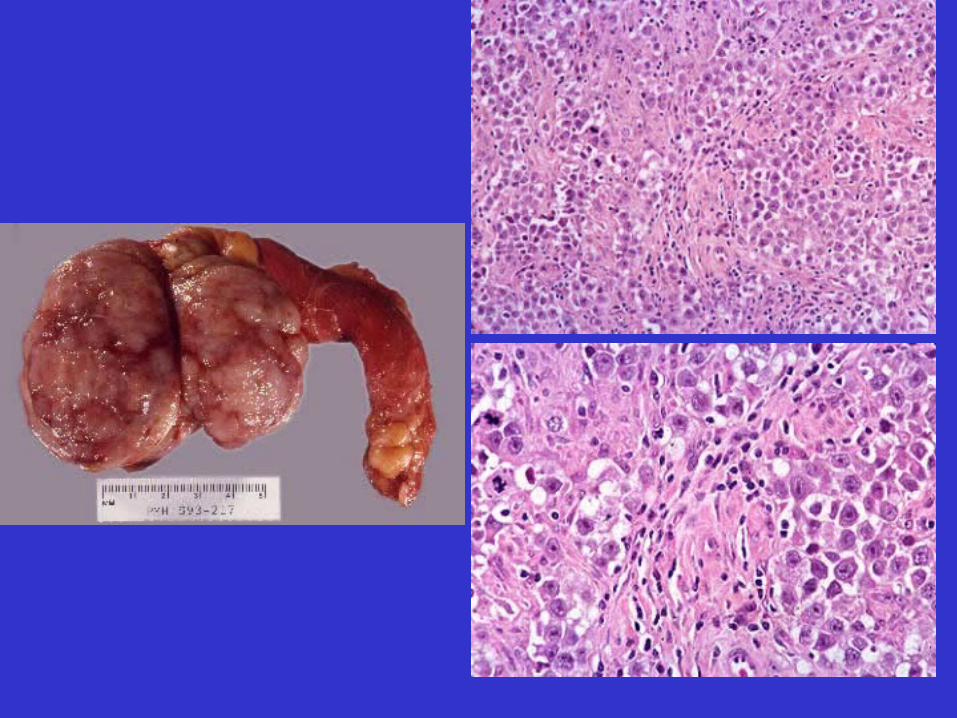

Testicular Germ cell tumors
– Seminoma Non-Seminom
1. Teratoma
2. Embryonal carcinoma
3. Yolk sac tumor
4. Choriocarcinoma
– Mixed Germ cell tumors (60%)
Classification of Ovarian Tumors
• Surface epithelial tumors– Serous
– Mucinous
– Endometrioid
– Clear cell
– Brenner
• Sex cord tumors– Fibroma/Thecoma
– Granulosa cell tumor
– Sertoli-Leydig cell tumor
• Germ cell tumors– Dysgerminoma
– Teratoma• Mature
• Immature
– Embryonal carcinoma
– Yolk sac tumor
– choriocarinoma


![UNDESCENDED OVARY PRESENTED WITH ...A].pdf272 273 274 UNDESCENDED OVARY PRESENTED WITH fPARAOVARIAN CYST Guldeniz ,Aksan DESTELI1T urk a n GURS1 ,HlimeCEVIK2lsi BuletZEYNELOL3 1 D](https://img.pdfslide.net/doc/110x75/5fc9b82ef7f5f41d2e282d63/undescended-ovary-presented-with-apdf-272-273-274-undescended-ovary-presented.jpg)