Embed Size (px)
Citation preview
Overcoming TAH Challenges: Innovation in PT Practice
February 18, 2016
Property of Hu and Seidel, not to be distributed without permission. 1
Overcoming TAH Challenges: Innovation in PT Practice
Suzanne Seidel, PT, CCSVicky Hu, PT, DPT, CCS, CSCSCedars-Sinai Medical Center
APTA Combined Sections MeetingAnaheim, California
February 17-20, 2016
Disclosures• Vicky Hu – no relevant financial relationship exists• Suzanne Seidel – no relevant financial relationship exists
Learning Objectives1. Explain the indications and contraindications for use
of Total Artificial Heart (TAH)2. Describe indications and contraindications for timing
of physical therapy related to TAH3. Describe physical therapy progression and functional
outcomes for TAH patient population4. Recognize critical elements from case examples that
impact PT practice
Outline• Introduction• TAH mechanics, indications/contraindications to TAH implantation
• Pathophysiology necessitating TAH implantation• Indications/contraindications, early mobilization with TAH with physical therapy
• Research study highlighting the optimal timing of physical therapy including barriers to early mobilization
• Case examples to illustrate physical therapy intervention from TAH implant to transplantation
• Implications and strategies for optimal physical therapy practice with the TAH patient population
• Q&A
Cedars-Sinai Medical Center
• Primary service area includes 3.3 million people
• 962 beds including 24 cardiothoracic ICU, 24 step-down unit, 32 advanced heart failure unit
• 2013-2014: 241 heart transplants, 47 Total Artificial Heart implants
Introduction• Current standard of care for end-stage heart failure is cardiac transplantation
• As of 11/13/2015, approximately 4,200 people are listed with UNOS National organ transplant registry waiting for a heart transplant, 350 of those are in California (8%){ Status 1A – 479, Status 1B – 1787{ Status 2 – 958{ Status 7 – 1000
• Approximately 2,200 donor hearts are available each year in the US
• Mechanical circulatory support is increasingly being utilized to treat end-stage heart failure, as bridge to transplant
SynCardia Systems, Inc.UNOS , 2015
Copeland, Arabia, Tsau, et al 2003Copeland, Smith, Arabia, et al 2004
Overcoming TAH Challenges: Innovation in PT Practice
February 18, 2016
Property of Hu and Seidel, not to be distributed without permission. 2
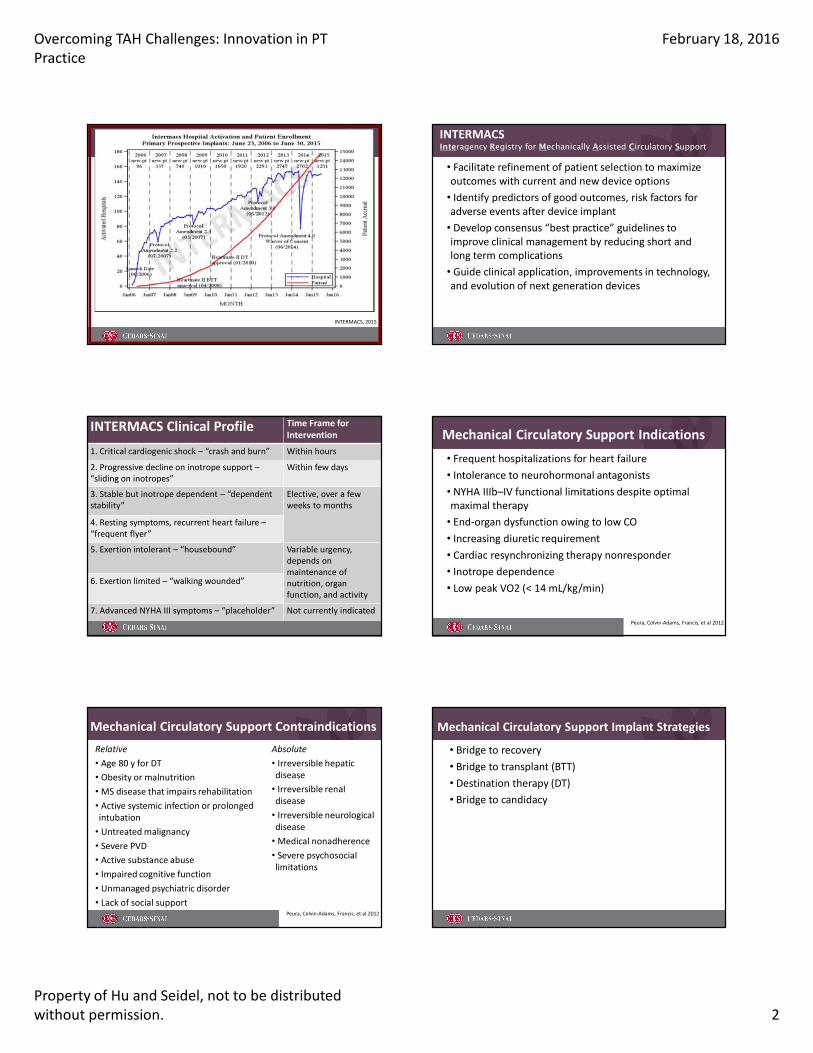
INTERMACS, 2015
INTERMACSInteragency Registry for Mechanically Assisted Circulatory Support
• Facilitate refinement of patient selection to maximize outcomes with current and new device options• Identify predictors of good outcomes, risk factors for adverse events after device implant• Develop consensus “best practice” guidelines to improve clinical management by reducing short and long term complications• Guide clinical application, improvements in technology, and evolution of next generation devices
INTERMACS Clinical Profile Time Frame for Intervention
1. Critical cardiogenic shock – “crash and burn” Within hours
2. Progressive decline on inotrope support –“sliding on inotropes”
Within few days
3. Stable but inotrope dependent – “dependent stability”
Elective, over a few weeks to months
4. Resting symptoms, recurrent heart failure –“frequent flyer”
5. Exertion intolerant – “housebound” Variable urgency,depends on maintenance of nutrition, organ function, and activity
6. Exertion limited – “walking wounded”
7. Advanced NYHA III symptoms – “placeholder” Not currently indicated
Mechanical Circulatory Support Indications• Frequent hospitalizations for heart failure• Intolerance to neurohormonal antagonists• NYHA IIIb–IV functional limitations despite optimal maximal therapy• End-organ dysfunction owing to low CO• Increasing diuretic requirement• Cardiac resynchronizing therapy nonresponder• Inotrope dependence• Low peak VO2 (< 14 mL/kg/min)
Peura, Colvin-Adams, Francis, et al 2012
Absolute
• Irreversible hepatic disease
• Irreversible renal disease
• Irreversible neurological disease
• Medical nonadherence• Severe psychosocial limitations
Mechanical Circulatory Support Contraindications
Peura, Colvin-Adams, Francis, et al 2012
Relative
• Age 80 y for DT• Obesity or malnutrition• MS disease that impairs rehabilitation• Active systemic infection or prolonged intubation
• Untreated malignancy• Severe PVD• Active substance abuse• Impaired cognitive function• Unmanaged psychiatric disorder• Lack of social support
Mechanical Circulatory Support Implant Strategies
• Bridge to recovery• Bridge to transplant (BTT)• Destination therapy (DT)• Bridge to candidacy
Overcoming TAH Challenges: Innovation in PT Practice
February 18, 2016
Property of Hu and Seidel, not to be distributed without permission. 3
Bridge to Recovery• Temporary maintenance of circulation after an acute event, during which time the heart is expected to recover, and mechanical support is then removed without need for transplant• Patients with reversible cardiac insults such as cardiogenic shock, peripartum cardiomyopathy{ Too high risk for durable implantable MCS device{ Allows stabilization, and clarification of potential cardiac recovery or reversal of other medical issues that may interfere with transplantation or durable implantable MCS device placement
Stewart and Givertz, 2012Peura, Colvin-Adams, Francis, et al 2012
Non-durable MCSTemporary/rescue devices:• Intra-aortic balloon pump• Extracorporeal membrane oxygenation• Percutaneous{ TandemHeart{ Impella 2.5
• Extracorporeal{ CentriMag{ (Thoratec pVAD)
Bridge to Transplant• Transplant candidate that would not survive, or would develop progressive end-organ dysfunction from low cardiac output before an organ becomes available{ Improve survival, functional status, quality of life –particularly for those predicted to have a long wait for an appropriate donor{ Reverse or prevent end-organ dysfunction
Stewart and Givertz, 2012Peura, Colvin-Adams, Francis, et al 2012
Destination Therapy• Not transplant candidate but need long term support• Failed to respond to optimal medical management for ≥ 45 of last 60 days, or balloon pump dependent for 7 days, or IV inotrope dependent for 14 days• EF < 25%• Demonstrates functional limitation with peak VO2 ≤ 14 mL/kg/min unless balloon pump or inotrope dependent, or physically unable to perform the test
Centers for Medicare & Medicaid Services, 2013Stewart and Givertz, 2012
Peura, Colvin-Adams, Francis, et al 2012
Bridge to Candidacy• Not currently listed for transplant• Potential for recovery unclear• No absolute or permanent contraindication to transplantation• Transplant eligibility dependent on condition after device implantation{ Development or resolution of comorbidities
Stewart and Givertz, 2012Peura, Colvin-Adams, Francis, et al 2012
Durable MCS Devices• Thoratec HeartMate II – BTT, DT• Thoratec pVAD – BTT, DT• HeartWare HVAD – BTT, (DT)• SynCardia Total Artificial Heart – BTT, (DT)
Overcoming TAH Challenges: Innovation in PT Practice
February 18, 2016
Property of Hu and Seidel, not to be distributed without permission. 4
MCS Common Components• Pump• Driveline• System controller/console• Power source
Thoratec CentriMag• External• Short term – 6 hrs, up to 30 days• Magnetically-levitated pump impeller Æcontinuous blood flow• Pump speed up to 5,500 RPM• Cardiac output up to 9.9 L/min
Reprinted with the permission of Thoratec Corporation
Thoratec pVAD• External• Rigid plastic housing, 2 chambers separated by polyurethane membrane• Pneumatic – compressor shuttles air in/out Æpulsatile• SV = 65 mL• CO up to 7.1 L/min• Auto/fixed rate up to 110 bpm
Reprinted with the permission of Thoratec Corporation
Thoratec HeartMate II• Internal pump, 10 oz – implanted beneath diaphragm, in pre-peritoneal or intra-abdominal space
• Rotor (magnet), located inside a thin-walled titanium duct 12 mm in diameter, spins on bearings –6,000-15,000 RPM (normal 8,000-10,000 RPM)
• Continuous flow, cardiac output 3-10 L/min
• Designed for several years of circulatory support – BTT, DT
Reprinted with the permission of Thoratec Corporation
• Internal pump, 160 g (5.6 oz)• Motor speed 1800-4000 RPM, recommended 2400-3200 RPM• Impeller spins blood, continuous flow Æ cardiac output up to 10 L/min{ Calculated by pump power and speed, hematocrit
HeartWare HVAD
Courtesy: HeartWare, Inc.
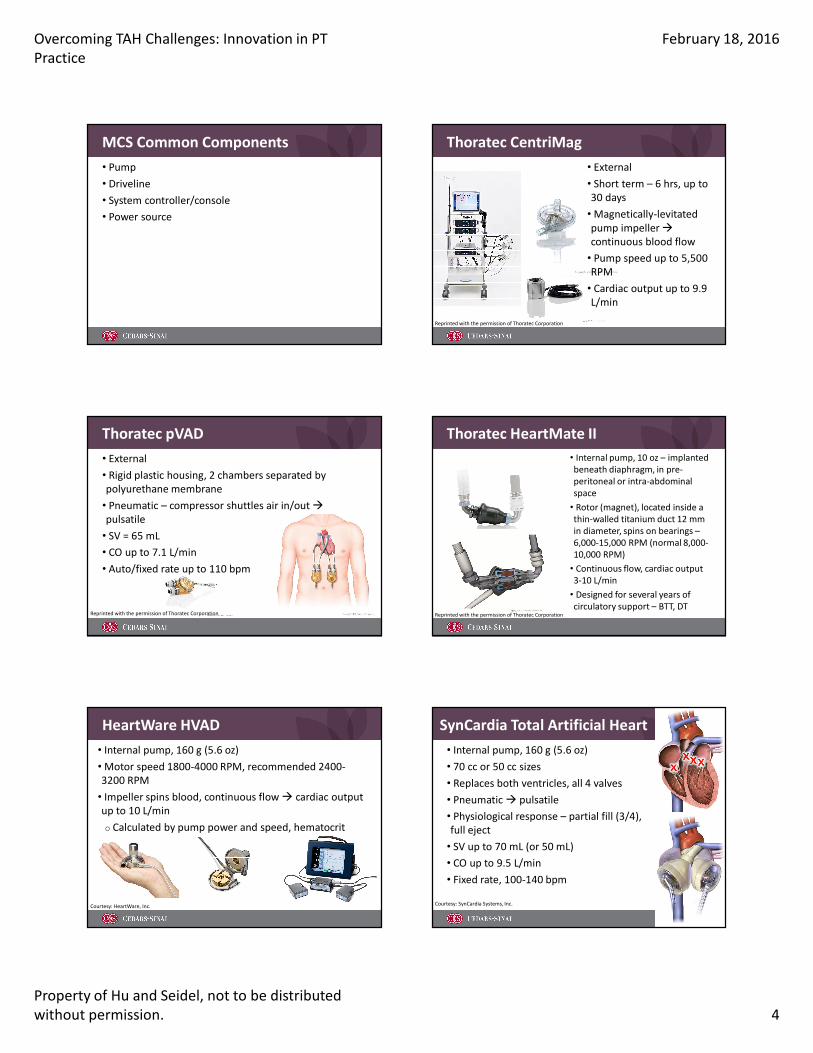
SynCardia Total Artificial Heart• Internal pump, 160 g (5.6 oz)• 70 cc or 50 cc sizes• Replaces both ventricles, all 4 valves• Pneumatic Æ pulsatile• Physiological response – partial fill (3/4), full eject• SV up to 70 mL (or 50 mL)• CO up to 9.5 L/min• Fixed rate, 100-140 bpm
Courtesy: SynCardia Systems, Inc.
Overcoming TAH Challenges: Innovation in PT Practice
February 18, 2016
Property of Hu and Seidel, not to be distributed without permission. 5
TAH Indications• Bridge to transplantation{ Transplant eligible{ At risk of imminent death from non-reversible biventricular failure
• Destination therapy (investigational){ Ineligible for cardiac transplantation{ Remote likelihood of becoming eligible for a transplant
SynCardia Systems, Inc.
TAH Contraindications• Patients who do not have sufficient space in the chest { < 10 cm distance between the sternum and T10 measured by CT scan
• Body surface area{ < 1.7 m2 for 70 cc{ > 1.85 m2 for 50 cc
• Patients who cannot be adequately anticoagulated
SynCardia Systems, Inc.
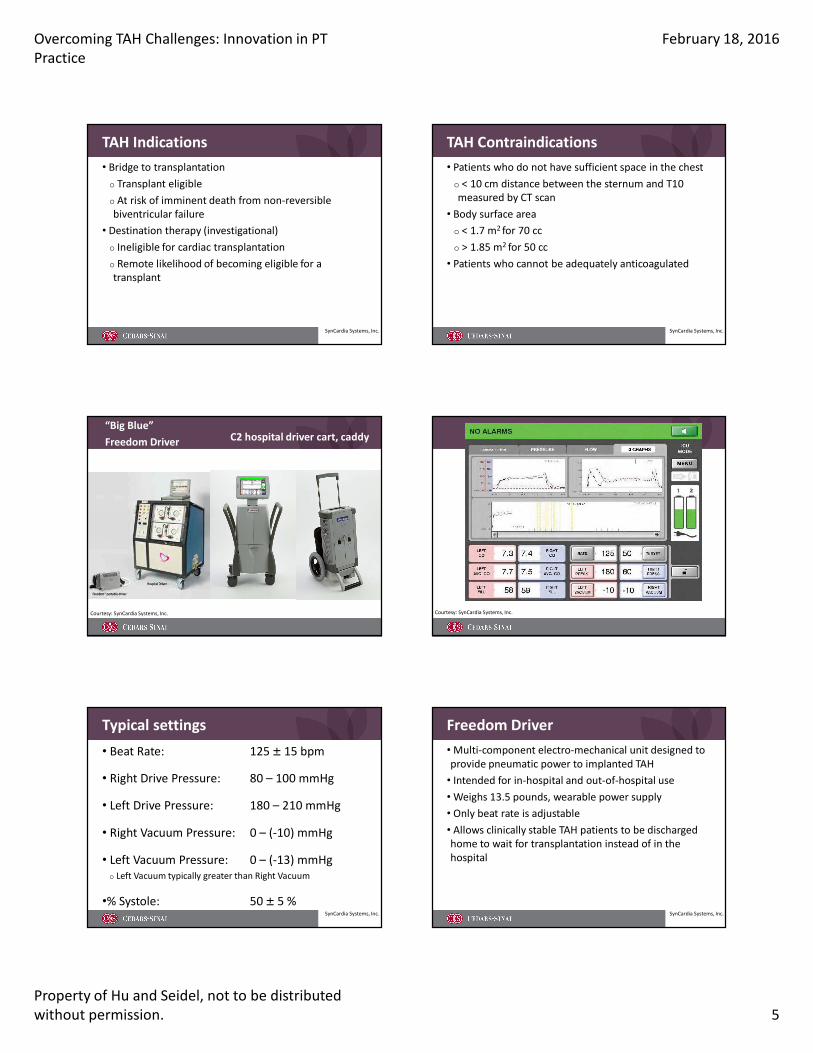
“Big Blue”Freedom Driver C2 hospital driver cart, caddy
Courtesy: SynCardia Systems, Inc. Courtesy: SynCardia Systems, Inc.
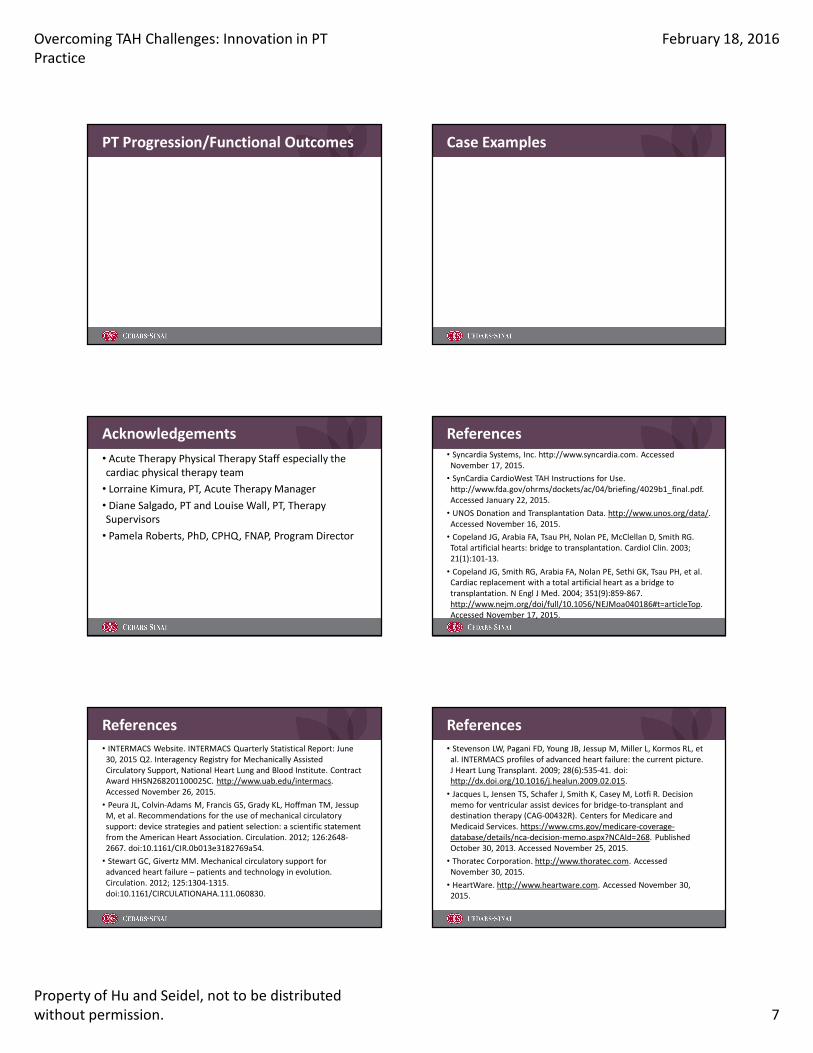
Typical settings• Beat Rate: 125 ± 15 bpm
• Right Drive Pressure: 80 – 100 mmHg
• Left Drive Pressure: 180 – 210 mmHg
• Right Vacuum Pressure: 0 – (-10) mmHg
• Left Vacuum Pressure: 0 – (-13) mmHg{ Left Vacuum typically greater than Right Vacuum
•% Systole: 50 ± 5 %SynCardia Systems, Inc.
Freedom Driver• Multi-component electro-mechanical unit designed to provide pneumatic power to implanted TAH• Intended for in-hospital and out-of-hospital use• Weighs 13.5 pounds, wearable power supply• Only beat rate is adjustable• Allows clinically stable TAH patients to be discharged home to wait for transplantation instead of in the hospital
SynCardia Systems, Inc.

Overcoming TAH Challenges: Innovation in PT Practice
February 18, 2016
Property of Hu and Seidel, not to be distributed without permission. 6
Freedom Driver
Courtesy: SynCardia Systems, Inc.
Pathophysiology Necessitating TAH• Biventricular heart failure – final common pathway of all cardiovascular disease{ Pediatric and adult congenital conditions{ Cardiomyopathy{ Persistent ventricular tachycardia{ Refractory cardiogenic shock{ Transplant rejection{ Acquired VSD{ Cardiac amyloidosis
• INTERMACS profile 1 or 2
SynCardia Systems, Inc.
Benefits of TAH• Eliminates native heart complications:{ Arrhythmias{ Failing ventricles{ Malfunctioning heart valves
• Shortest blood path of any MCS device• CO up to 9.5 L/min – speeds recovery of vital organs• Highest bridge to transplant rate – 79%• Immediately available
SynCardia Systems, Inc.Stewart and Givertz, 2012
TAH and Patient Recovery• Within 2 weeks:{ 65% of core patients were OOB by post-op day 5{ 60% of core patients were walking > 100 ft at 2 weeks after implant{ Liver function returned to normal{ Kidney function improved significantly, trending to normal
SynCardia Systems, Inc.FDA Summary of Safety and Effectiveness, 2004
TAH and Physical Therapy• Limited published research regarding PT intervention after TAH implantation
{ Comparison of BP response following TAH vs LVAD implantation
{ Single patient case studies
� Early progressive mobilization
� Utilizing previously established guidelines for patients with heart failure and MCS
Canada and Flattery, 2012Kohli, Canada, Arena, et al, 2011
Nicholson and Paz, 2010Fernandez and Ford, 2014
Indications/Contraindications to Initiating PT• Medically stable, chest closed• Able to follow simple commands• Abdominal binder to secure driveline• No telemetry monitoring necessary• Monitor signs/symptoms of exercise intolerance, orthostasis, vitals – BP, O2 sat, RR, RPE/Borg• Monitor device rate, flow, volume{ Partial fill, full eject
• Ensure power source, air tanks sufficient for duration of session
Overcoming TAH Challenges: Innovation in PT Practice
February 18, 2016
Property of Hu and Seidel, not to be distributed without permission. 7
PT Progression/Functional Outcomes Case Examples
Acknowledgements• Acute Therapy Physical Therapy Staff especially the cardiac physical therapy team • Lorraine Kimura, PT, Acute Therapy Manager• Diane Salgado, PT and Louise Wall, PT, Therapy Supervisors• Pamela Roberts, PhD, CPHQ, FNAP, Program Director
References• Syncardia Systems, Inc. http://www.syncardia.com. Accessed November 17, 2015.
• SynCardia CardioWest TAH Instructions for Use. http://www.fda.gov/ohrms/dockets/ac/04/briefing/4029b1_final.pdf. Accessed January 22, 2015.
• UNOS Donation and Transplantation Data. http://www.unos.org/data/. Accessed November 16, 2015.
• Copeland JG, Arabia FA, Tsau PH, Nolan PE, McClellan D, Smith RG. Total artificial hearts: bridge to transplantation. Cardiol Clin. 2003; 21(1):101-13.
• Copeland JG, Smith RG, Arabia FA, Nolan PE, Sethi GK, Tsau PH, et al. Cardiac replacement with a total artificial heart as a bridge to transplantation. N Engl J Med. 2004; 351(9):859-867. http://www.nejm.org/doi/full/10.1056/NEJMoa040186#t=articleTop. Accessed November 17, 2015.
References• INTERMACS Website. INTERMACS Quarterly Statistical Report: June 30, 2015 Q2. Interagency Registry for Mechanically Assisted Circulatory Support, National Heart Lung and Blood Institute. Contract Award HHSN268201100025C. http://www.uab.edu/intermacs. Accessed November 26, 2015.
• Peura JL, Colvin-Adams M, Francis GS, Grady KL, Hoffman TM, Jessup M, et al. Recommendations for the use of mechanical circulatory support: device strategies and patient selection: a scientific statement from the American Heart Association. Circulation. 2012; 126:2648-2667. doi:10.1161/CIR.0b013e3182769a54.
• Stewart GC, Givertz MM. Mechanical circulatory support for advanced heart failure – patients and technology in evolution. Circulation. 2012; 125:1304-1315. doi:10.1161/CIRCULATIONAHA.111.060830.
References• Stevenson LW, Pagani FD, Young JB, Jessup M, Miller L, Kormos RL, et al. INTERMACS profiles of advanced heart failure: the current picture. J Heart Lung Transplant. 2009; 28(6):535-41. doi: http://dx.doi.org/10.1016/j.healun.2009.02.015.
• Jacques L, Jensen TS, Schafer J, Smith K, Casey M, Lotfi R. Decision memo for ventricular assist devices for bridge-to-transplant and destination therapy (CAG-00432R). Centers for Medicare and Medicaid Services. https://www.cms.gov/medicare-coverage-database/details/nca-decision-memo.aspx?NCAId=268. Published October 30, 2013. Accessed November 25, 2015.
• Thoratec Corporation. http://www.thoratec.com. Accessed November 30, 2015.
• HeartWare. http://www.heartware.com. Accessed November 30, 2015.
Overcoming TAH Challenges: Innovation in PT Practice
February 18, 2016
Property of Hu and Seidel, not to be distributed without permission. 8
References• FDA Summary of Safety and Effectiveness Data. March 17, 2004. http://www.accessdata.fda.gov/cdrh_docs/pdf3/P030011b.pdf. Accessed November 30, 2015.
• Canada J, Flattery, M. Exercising the patient with a mechanical circulatory support device. International Society of Heart Lung Transplantation Links. 2012; 3(8). http://www.ishlt.org/ContentDocuments/2012JanLinks_Canada-Flattery.html. Accessed November 17, 2015.
• Kohli H, Canada J, Arena R, Tang D, Peberdy M, Harton S, et al. Exercise blood pressure response during assisted circulatory support: Comparison of the total artificial heart with a left ventricular assist device during rehabilitation. J Heart Lung Transplant. 2011; 30(11):1207-1213. http://www.jhltonline.org/article/S1053-2498(11)01043-6/fulltext. Accessed November 17, 2015.
References• Fernandez N, Ford K. Early progressive mobilization and physical therapy management in a patient with a total artificial heart device. Cardiopulm Phys Ther J. 2014; 25(1):23-28.
• Nicholson C, Paz J. Total artificial heart and physical therapy management. Cardiopulm Phys Ther J. 2010; 21(2):13-21. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2879422/. Accessed January 22, 2015.
• Holman WL. Interagency registry for mechanically assisted circulatory support (INTERMACS): what have we learned and what will we learn? Circulation 2012; 126:1401-1406. doi: 10.1161/CIRCULATIONAHA.112.097816.
• Jaroszewski DE, Anderson EM, Pierce CN, Arabia FA. The SynCardiafreedom driver: A portable driver for discharge home with the total artificial heart. 2011; 30(7):844-845. doi:10.1016/j.healun.2011.03.014.
References• Pierce C, Staley L, Bright H. The total artificial heart patient: building the bridge from implant to transplant. [PowerPoint Slides]. American Association of Cardiovascular and Pulmonary Rehabilitation 28th Annual Meeting. 2013. http://www.aacvpr.org/Portals/0/events_edu/annuallmeeting13/28AMSyllabus/S401_Bright,%20Pierce,%20Staley.pdf. Accessed January 22, 2015.
• Kirsch M, Mazzucotelli JP, Roussel JC, Bouchot O, N’Loga J, Leprince P, et al. Survival after biventricular mechanical circulatory support: Does the type of device matter?. J Heart Lung Transplant. 2012; 31(5):501-508. doi:10.1016/j.healun.2011.11.024.
• Barnard J, Tsui S. The total artificial heart in a cardiac replacement therapy programme. Br J Hosp Med. 2012; 73(12):634-639.
References• Shah KB, Tang DG, Cooke RH, Harton S, Flattery M, Katlaps GJ, et al. Review: Implantable mechanical circulatory support: Demystifying patients with ventricular assist devices and artificial hearts. Clinical Cardiology. 2011; 34:147-152. doi:10.1002/clc.20825.
• Johnson W. Editors’ pick: Total artificial heart transplants: Future or biding time? Royal College of Surgeons in Ireland Student Medical Journal. 2011; 35-39. http://www.rcsismj.com/4th-edition/heart-tx/. Accessed November 17, 2015.





























