Embed Size (px)
Citation preview

Paolo Coll, M.DPaolo Coll, M.D
Benign Prostatic Benign Prostatic Hyperplasia.Hyperplasia.

ObjectivesObjectives1) To describe briefly the prostate functional 1) To describe briefly the prostate functional
anatomy. anatomy.
2) To discuss the diagnostic approach in 2) To discuss the diagnostic approach in with Lower Urinary Tract Symptoms “LUTS”.with Lower Urinary Tract Symptoms “LUTS”.
3) To review Clinical Base Evidence Data for BPH 3) To review Clinical Base Evidence Data for BPH treatment decision.treatment decision.
4) To review principles on pharmacological and non- 4) To review principles on pharmacological and non- pharmacological treatment modalities for BPH. pharmacological treatment modalities for BPH.

ProstateProstate Located between the base of the Located between the base of the
urinary bladder and the pelvic urinary bladder and the pelvic diaphragm. Surrounded by a diaphragm. Surrounded by a fibrous capsule. fibrous capsule.
Muscular and glandular organ Muscular and glandular organ about 3cm both in length and about 3cm both in length and diameter, weight is about 10-diameter, weight is about 10-20gm.20gm.
Two surfaces and five lobes, an Two surfaces and five lobes, an apex and a base.apex and a base.
Anterior and posterior surfacesAnterior and posterior surfaces
Right and Left Lateral lobesRight and Left Lateral lobes
Right and Left Posterior lobesRight and Left Posterior lobes
Median Lobe.Median Lobe. Blood and nerve supply branches Blood and nerve supply branches
of inferior vesical and middle of inferior vesical and middle rectal arteries + inferior rectal arteries + inferior hypogastric plexus.hypogastric plexus.

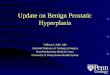
ProstateProstateQ: Area of prostate affected: inner/outer?
A: Area mostly affected in BPH is the inner or internal zone (Paraurethral glands)

ProstateProstate Are specific lobes predisposed to prostatic pathologies?Are specific lobes predisposed to prostatic pathologies?
YES,
1-Benign Prostatic Hyperplasia
2-Malignant Transformation

Introduction and Brief Introduction and Brief EpidemiologyEpidemiology
Benign prostatic hyperplasia (BPH) is a common problem among older men, and is responsible for considerable disability; however, it is an infrequent cause of death..
Is defined as a diseased process characterized
by stromal and epithelial cell hyperplasia beginning in the periurethral zone of the prostate.
Mortality rates for most developed countries in the 1980s were 0.5 to 1.5/100,000

BPHBPH PrevalencePrevalence — — The prevalence of histologically The prevalence of histologically
diagnosed prostatic hyperplasia increases from 8 percent in diagnosed prostatic hyperplasia increases from 8 percent in men aged 31 to 40, to 40 to 50 percent in men aged 51 to men aged 31 to 40, to 40 to 50 percent in men aged 51 to 60, to over 80 percent in men older than age 80 60, to over 80 percent in men older than age 80

Natural HistoryNatural History
The natural history of BPH is The natural history of BPH is becoming better understood.becoming better understood.
While prostatic mass increases with While prostatic mass increases with age, an individual man's symptoms age, an individual man's symptoms may notmay not..
Of men with moderate symptoms Of men with moderate symptoms followed for five years, about 40% followed for five years, about 40% improve, 45% remain unchanged, improve, 45% remain unchanged, and only 15% deteriorate.*and only 15% deteriorate.*
*Oesterling J. E. Benign Prostatic Hyperplasia: Medical and Minimally Invasive Treatment Options. N Engl J Med. 1995; 332: 99-109.

Natural History IINatural History II
BPH ComplicationsBPH Complications
Acute and Recurrent Urinary RetentionRecurrent InfectionsRenal InsufficiencyBladder DescompensationBladder Stones

Bladder DecompensationBladder Decompensation

Q: How often do you monitor patients Q: How often do you monitor patients with BPH for probable malignancy with BPH for probable malignancy development, though the incidence is development, though the incidence is low?low?
• A: BPH is not a known predisposition or risk factor for prostate malignancy. Consequently no guidelines exist on monitoring BPH symptomatic patients for malignancy.

““Doc I can hardly pee”Doc I can hardly pee”
A 75 y/o M comes to your office with a 6 A 75 y/o M comes to your office with a 6 month hx of nocturia, hesitancy, a slow month hx of nocturia, hesitancy, a slow flow of urine, and terminal dribbling. The flow of urine, and terminal dribbling. The symptoms have been progressing. symptoms have been progressing. Otherwise, he is well and has had no Otherwise, he is well and has had no significant medical illnesses.significant medical illnesses.
PE: Abdomen: PE: Abdomen: normal.normal.
Rectal exam: Rectal exam: enlarged prostate, smooth in contour and enlarged prostate, smooth in contour and firm and has no nodules or irregularities.firm and has no nodules or irregularities.

Initial evaluationInitial evaluation
2003 AHCPR* Updated recommendations 2003 AHCPR* Updated recommendations from previous 1994 guidelines.from previous 1994 guidelines.
Lower urinary tract pathologies in aging man Lower urinary tract pathologies in aging man produce similar, if not identical symptoms.produce similar, if not identical symptoms.
The challenge in patients with LUTS is to The challenge in patients with LUTS is to establish that the symptoms are BPH related.establish that the symptoms are BPH related.
US Agency for Health Care Policy and Research (AHCPR)*

By following the Clinical Practice By following the Clinical Practice Guidelines to exclude other diseases Guidelines to exclude other diseases and by using the AUA symptom score to and by using the AUA symptom score to evaluate severity it is possible to evaluate severity it is possible to determine which men need immediate determine which men need immediate evaluation by a urologist and which are evaluation by a urologist and which are candidates for watchful waiting or candidates for watchful waiting or medical therapy. medical therapy.

Evaluation

HistoryHistory A medical history should be taken to identify A medical history should be taken to identify
other causes of voiding dysfunction and other causes of voiding dysfunction and comorbidities that may complicate treatment.comorbidities that may complicate treatment.
Age.Sx’s frequency and volume. (Symptoms Index score)Previous surgical hx. (Hx of urethritis or urethral injury)Family Hx of BPH or prostate carcinoma.Pharmacological hx. Treatment with drugs that can impair bladder function (anticholinergic drugs) or increase outflow resistance (sympathomimetic drugs)Excessive urine production.

The chief complaint of the patient with BPHThe chief complaint of the patient with BPHis usually bothersome “LUTS” typified by: is usually bothersome “LUTS” typified by: IIrritativerritative OR OR ObstructiveObstructive Urinary frequencyUrinary frequency.. Urgency.Urgency. Urge incontinence.Urge incontinence. Nocturia.Nocturia. HesitancyHesitancy Decreased intermittent force of stream.Decreased intermittent force of stream. Sensation of incomplete bladder.Sensation of incomplete bladder. Slow termination/dribblingSlow termination/dribbling

Physical ExamPhysical Exam
A physical exam including both a DRE and A physical exam including both a DRE and a focused neurological examination, a focused neurological examination, should be performed.should be performed.
GeneralDREFocused Neurological Exam*
Ambulatory StatusLE’S Neuromuscular functionAnal sphincter tone

Rectal ExamRectal Exam Mr. x, This is not a painful maneuver ,you will feel a coldness sensation Mr. x, This is not a painful maneuver ,you will feel a coldness sensation
because of the lubricant and this will be followed by the sensation of having because of the lubricant and this will be followed by the sensation of having to move your bowels, but this will not happen. Please take a deep breath..to move your bowels, but this will not happen. Please take a deep breath..

Q: Pertinent findings to watch out for on the Q: Pertinent findings to watch out for on the digital rectal exam?digital rectal exam?
Fast & effective to r/o locally advanced prostatic carcinomaFast & effective to r/o locally advanced prostatic carcinoma

UrinalysisUrinalysis
A urinalysis should be performed by A urinalysis should be performed by dipstick testing or microscopic dipstick testing or microscopic examination of the sediment to screen examination of the sediment to screen for hematuria and evidence of an UTI.for hematuria and evidence of an UTI.
Bladder CarcinomaUrethral StricturesUrethral-Bladder StoneUTI’S
- = <

PSA TestingPSA Testing
Measurement of PSA should be done Measurement of PSA should be done in the following individuals:in the following individuals:Those with at least a 10yr-life expectancy and to whom knowledge of the presence of prostatic cancer would change management.
Those for whom the measurement of their PSA would change the management of their voiding symptoms.
*Serum PSA is one predictor of the natural Hx of BPH, higher PSA increased risk of future prostate growth and flow rate deterioration.
*Optional Test*Optional Test

Urine CytologyUrine Cytology
*Optional Test*Optional Test
Maybe considered in men with a Maybe considered in men with a predominance of irritative symptoms, predominance of irritative symptoms, specially with Hx of SMOKING to aid in the Dx specially with Hx of SMOKING to aid in the Dx of Bladder Carcinoma Insitu or Bladder of Bladder Carcinoma Insitu or Bladder carcinoma. carcinoma.

Evaluation II

The AUA Symptom Index Tool for BPH The AUA Symptom Index Tool for BPH and the Disease Specific Quality of Life and the Disease Specific Quality of Life
QuestionQuestionThe AUA Symptom score index (Identical to the IPSS) should be done in the initial assessment of each patient presenting with BPH.
Seven questions that relate to the associate symptoms.
0-7 MILD8-19 MODERATE20-35 SEVERE
*Although a Validated test , test clarity, retest, reliability, internal consistency is not a replacement for personal discussion with the patient.

Evaluation III

Optional Dx Tests IOptional Dx Tests IFollowing the initial evaluation of the patient, urinary flow rate-recording and measurement of post-void residual may be appropriate for certain cases. These tests usually are not necessary prior to the institution of watchful waiting or medical therapy.
1- Neurological disorders known to affect bladder function.
2- Prior failure BPH treatment.
3- Those desiring surgical intervention.

Post-Void Residual Urine Post-Void Residual Urine VolumeVolume
Residual urine volume can be determined by Residual urine volume can be determined by in-out catheterization, radiographic methods, in-out catheterization, radiographic methods, or USG. or USG.
12CC
200-300CC
>12 CC
200-300
350 CC
Q: Based on this information what residual volume needs invasive therapy?
A: No level of residual level in and of itself , mandate invasive therapy.

PVR “5 Facts”PVR “5 Facts” 11-As the result of large test-retest variability and lack of -As the result of large test-retest variability and lack of
appropriately designed outcome studies appropriately designed outcome studies is not feasible is not feasible to establish a PVR “cutpoint” for decision makingto establish a PVR “cutpoint” for decision making..
22-The Panel recommended the use of -The Panel recommended the use of PVR PVR measurement as optionalmeasurement as optional in men undergoing non- in men undergoing non-invasive therapy. invasive therapy. 33-Some studies have predicted high Residual -Some studies have predicted high Residual volumes with high failure rates of watchful waiting.volumes with high failure rates of watchful waiting.
44-Possible indicator of BPH, a large residual volume -Possible indicator of BPH, a large residual volume is probably associated with increased risk of is probably associated with increased risk of infection and is a precursor to bladder infection and is a precursor to bladder decompensationdecompensation..55-Although long-term controlled data are lacking -Although long-term controlled data are lacking many patient maintain fairly large Residual volumes many patient maintain fairly large Residual volumes without evidence of UTI’S, Renal insufficiency or without evidence of UTI’S, Renal insufficiency or bothersome LUTS.bothersome LUTS.

Maximal Urinary Flow Maximal Urinary Flow RateRate
Greater than 15 mL/sec are thought to exclude clinically important bladder outlet obstruction.
>15 mL/sec
Below 15 mL/sec are compatible with obstruction due to prostatic or urethral disease; however, this finding is not diagnostic since a low flow rate can also result from bladder decompensation.
< 15ml/sec
*Among men with BPH, those with maximal flow rates less than 10 mL/sec have better outcomes after surgical intervention than those with higher flow rates.
<10mL/sec

There is evidence to support that certain There is evidence to support that certain tests may be valuable in predicting the tests may be valuable in predicting the response to therapy in specific response to therapy in specific circumstances. circumstances.
Optional Dx Tests II (Invasive)Optional Dx Tests II (Invasive)
Additional tests such as pressure-flow urodynamic studies, urethrocystoscopy and USG are optional in patients choosing invasive therapies, or if prostate size and anatomical configuration are important considerations for a given treatment modality.

Patient Choosing Invasive Therapies
Pressure Flow-StudiesPressure Flow-Studies Measurement of the pressure in the Measurement of the pressure in the
bladder during voiding provides the most bladder during voiding provides the most accurate means for accurate means for determining bladder determining bladder outlet obstructionoutlet obstruction
UrethrocystoscopyUrethrocystoscopyUrethral risk factors Ej: StricturesUrethral risk factors Ej: StricturesHematuria Micro-or gross,Hematuria Micro-or gross,Endoscopic appearance may guide the Endoscopic appearance may guide the choice therapychoice therapy
USG Transrectal USG Transrectal or or TransabdominalTransabdominalSize, shape and anatomical features Size, shape and anatomical features Ej: Vesical lobes of the prostate are Ej: Vesical lobes of the prostate are of importance to select patients for of importance to select patients for Transurethral microwave heat Tx.Transurethral microwave heat Tx.TUIP v.s TURP and other Tx TUIP v.s TURP and other Tx ModalitiesModalities

General OverviewGeneral Overview
Watchful Waiting
Medical Therapies
Minimally Invasive Therapies.
Surgical Therapies

What is the evidence that What is the evidence that medical therapy helps BPHmedical therapy helps BPH??
Drugs are useful if they reduce Drugs are useful if they reduce symptoms, avoid surgery, or prevent symptoms, avoid surgery, or prevent complications.complications.
*Evidence that drugs provide anything more than symptomatic benefit is severely limited.

Initial Management and DiscussionInitial Management and Discussion of Medical treatment with the of Medical treatment with the
patient.patient.
Management of Patients with mild or moderate to
Severe BPH symptoms without Bother.
Management of patients with moderate to severe BPH symptoms with Bother.


““Doc sometimes I can’t Doc sometimes I can’t pee”pee”
A 75 y/o M comes to A 75 y/o M comes to your office with a 6 your office with a 6 month hx of nocturia, month hx of nocturia, hesitancy, a slow flow hesitancy, a slow flow of urine, and terminal of urine, and terminal dribbling. The dribbling. The symptoms have been symptoms have been progressing. Otherwise, progressing. Otherwise, he is well and has had he is well and has had no significant medical no significant medical illnesses.illnesses.
PE: Abdomen: normal.PE: Abdomen: normal. Rectal exam: Rectal exam:
enlarged prostate, enlarged prostate, smooth in contour and smooth in contour and firm and has no firm and has no nodules or nodules or irregularities.irregularities. AUA AUA
SymptoSymptom Index m Index 66
AUA AUA SymptoSymptom Index m Index 66
AUA AUA SymptoSymptom m IndexIndex>>2222
AUA AUA SymptoSymptom m IndexIndex>>2222

Mild-Moderate-Severe Symptoms Mild-Moderate-Severe Symptoms of BPH without Bother.of BPH without Bother.
Non-Bothersome Sx’s of BPH
Unaffected quality of life
Risks of Medical Therapy
Risks of medical therapy outweight the benefits of symptoms improvement.

Moderate-Severe Symptoms of Moderate-Severe Symptoms of BPH BPH With Bother.With Bother.
Alpha adrenergic Blocker TherapyAlpha adrenergic Blocker Therapy
Alfuzolin
(Uroxatral)
Tamsulosin* (Flomax)
Terazosin
(Hytrin)
Doxazosin*
(Cardura)
Clinical BPH is partlyProduced by alpha1-adrenergic-mediated contraction of smooth muscle resulting in bladder outlet obstruction.
Equal clinical effectiveness.
Different safety profiles.
2 Agents efficacy dose dependency.(Terazosin-Doxazosin)
THEORY AGENTS
PROFILE ADVERSE

Moderate-Severe Symptoms of Moderate-Severe Symptoms of BPH BPH With Bother.With Bother.
5-Alpha Reductase Inhibitor Therapy5-Alpha Reductase Inhibitor TherapyTHEORY AGENTS PROFILE ADVERSE
These drugs act by reducing the size of the prostate gland. The type 2 form of 5-alpha-reductase catalyzes the conversion of testosterone to dihydrotestosterone in prostatic and other androgen-sensitive tissues.
Finasteride
(Proscar)
Dutasteride
(Avodart)
Serum dihydrotestosterone concentrations decreased by about 70 percent.
Are not appropriate for patients with LUTS without evidence of Prostatic Enlargement.
<Risk of Acute Urinary Retention and BPH related Sx.
Is partially effective in relieving LUTS.

Moderate-Severe Symptoms of Moderate-Severe Symptoms of BPH BPH With Bother.With Bother.
Combination therapyCombination therapy
Combined finasteride-alpha adrenergic antagonist therapy for 6 to 12 months does not appear to be more effective than single-drug therapy for symptom scores and maximal urinary flow rate.
However, longer term therapy has shown a benefit from combined therapy. MTOPS trial -Combination therapy reduced the risk of clinical progression by 66 percent, significantly greater than with either drug alone.-Symptom scores improved with all therapies, but to a greater degree with combined therapy -Combination therapy or finasteride alone (but not doxazosin alone), reduced the risk of acute urinary retention and the need for invasive therapy.


HERBAL THERAPIESHERBAL THERAPIES
Saw palmetto (Serenoa Repens)
DOSAGE AND STANDARDIZATION — Oral: 160 mg twice daily, standardized to contain at least 80% to 90% fatty acids and sterols per dose.
PHARMACOLOGY — Excessive formation of dihydrotestosterone (DHT) is believed to stimulate enlargement of the prostate (hyperplasia).There are three mechanisms by which saw palmetto alters the effects of DHT.
SUMMARY — Saw palmetto is used in men to improve symptoms of benign prostatic hyperplasia (BPH). Several studies have reported that the effects of saw palmetto are comparable to symptomatic improvements which result from medications commonly used for this disorder.
Despite evidence of safety and some efficacy of these products, questions regarding their standardization remain.

INVASIVE TREATMENTINVASIVE TREATMENT
In general, men with moderate to In general, men with moderate to severe symptoms due to BPH are severe symptoms due to BPH are candidates for invasive therapies. candidates for invasive therapies.
Failure of medical treatment.Failure of medical treatment.Recurrent urinary tract infections. Recurrent urinary tract infections. Recurrent or persistent gross Recurrent or persistent gross hematuria.hematuria.Bladder stones.Bladder stones.Renal insufficiency.Renal insufficiency.Refractory urinary retention.Refractory urinary retention.

http://www.nucleusinc.com/medical-animations.php?page_no=1&show_anim=turp.movhttp://www.nucleusinc.com/medical-animations.php?page_no=1&show_anim=turp.mov

Transurethral Resection of the Transurethral Resection of the Prostate (TURP).Prostate (TURP).
Most commonly employed .Most commonly employed . Reduces symptoms in 88 percent of patients. Reduces symptoms in 88 percent of patients. The most frequent complications: Inability to void, The most frequent complications: Inability to void,
Clot retention, secondary infection and bleedingClot retention, secondary infection and bleeding Long-term complications include Long-term complications include retrograde ejaculation (70 percent of treated retrograde ejaculation (70 percent of treated
patients), impotence (14 percent; range: 3 to 32 patients), impotence (14 percent; range: 3 to 32 percent), partial incontinence (6 percent), and percent), partial incontinence (6 percent), and total incontinence (1 percent). total incontinence (1 percent).
Approximately 10 percent of patients require Approximately 10 percent of patients require retreatment within five years. retreatment within five years.

Transurethral Resection of the Transurethral Resection of the
ProstateProstate

Transurethral incision of the Transurethral incision of the prostate (TUIP)prostate (TUIP)
Is an endoscopic procedure using Is an endoscopic procedure using only one or two incisions to reduce only one or two incisions to reduce constriction of the urethra without constriction of the urethra without removing any of the prostate gland.removing any of the prostate gland.
It is generally offered as a treatment It is generally offered as a treatment option for younger patients in whom option for younger patients in whom fertility and antegrade ejaculation fertility and antegrade ejaculation are important issues. are important issues.

Transurethral Ultrasound-Transurethral Ultrasound-Guided Prostatectomy (TULIP, Guided Prostatectomy (TULIP,
(VLAP), (CLAP), (ILCP),(VLAP), (CLAP), (ILCP), Transurethral ultrasound-guided Transurethral ultrasound-guided
prostatectomy (TULIP) using a free fiber.prostatectomy (TULIP) using a free fiber. Free-fiber visually guided laser ablation of Free-fiber visually guided laser ablation of
the prostate the prostate (VLAP).(VLAP). Contact laser ablation of the prostate Contact laser ablation of the prostate
(CLAP) using visual guidance.(CLAP) using visual guidance. Interstitial laser coagulation of the Interstitial laser coagulation of the
prostate (ILCP).prostate (ILCP).

Transurethral Vaporization of the Transurethral Vaporization of the Prostate (TUVP) or Transurethral Prostate (TUVP) or Transurethral
Electrovaporization of the Prostate Electrovaporization of the Prostate (TVP)(TVP)
Is now performed using endoscopic Is now performed using endoscopic electrosurgical equipment to remove electrosurgical equipment to remove prostatic tissue with limited coagulation. prostatic tissue with limited coagulation.
The procedure provides urinary symptom The procedure provides urinary symptom reduction similar to that of TURP, with reduction similar to that of TURP, with less postoperative irritation, urinary less postoperative irritation, urinary retention, blood loss.retention, blood loss.

Transurethral Microwave Transurethral Microwave Thermotherapy (TUMT)Thermotherapy (TUMT)
Is a single-session, minimally invasive Is a single-session, minimally invasive outpatient treatment in which a microwave outpatient treatment in which a microwave antenna is placed in a urethral catheter. antenna is placed in a urethral catheter.
Microwave energy causes deep, rapid tissue Microwave energy causes deep, rapid tissue heating, while a cooling system circulates heating, while a cooling system circulates water to protect adjacent tissue.water to protect adjacent tissue.
No major complications, including No major complications, including incontinence and sexual dysfunction, have incontinence and sexual dysfunction, have been reported in patients treated with TUMT. been reported in patients treated with TUMT.

Open ProstatectomyOpen Prostatectomy Surgical removal of the inner portion of the prostate Surgical removal of the inner portion of the prostate
using a suprapubic or retropubic approach is the oldest using a suprapubic or retropubic approach is the oldest and most effective treatment for relieving the and most effective treatment for relieving the symptoms of BPH and increasing maximum urinary flow. symptoms of BPH and increasing maximum urinary flow.
Symptomatic improvement occurs in 98 percent of Symptomatic improvement occurs in 98 percent of patients who undergo this procedure, and the patients who undergo this procedure, and the retreatment rate is only 2 percent.retreatment rate is only 2 percent.
However, open prostatectomy is the most invasive However, open prostatectomy is the most invasive
treatment for BPH and is associated with the most treatment for BPH and is associated with the most morbidity. Therefore, this procedure is typically morbidity. Therefore, this procedure is typically reserved for use in patients with a very large prostate reserved for use in patients with a very large prostate gland or structural problems such as a large median gland or structural problems such as a large median lobe that protrudes into the bladder or a large bladder lobe that protrudes into the bladder or a large bladder calculus or urethral diverticulum.calculus or urethral diverticulum.

ConclusionsConclusions
Alpha-1-antagonists reduce symptoms in some patients. Their Alpha-1-antagonists reduce symptoms in some patients. Their effect is detectable within 2 weeks. If the patient experiences no effect is detectable within 2 weeks. If the patient experiences no clear benefit by 1 month, the drug should be discontinued.clear benefit by 1 month, the drug should be discontinued.
The evidence of a significant benefit to risk ratio for finasteride The evidence of a significant benefit to risk ratio for finasteride is less clear. It may be useful for men with large prostates; a is less clear. It may be useful for men with large prostates; a therapeutic trial of at least 3 months is required.therapeutic trial of at least 3 months is required.
Saw palmetto extracts cannot be recommended because Saw palmetto extracts cannot be recommended because effective doses of available preparations have not been effective doses of available preparations have not been established and evidence of safety and long term efficacy are established and evidence of safety and long term efficacy are insufficient. insufficient.
Before using any drug to treat BPH, develop a clear treatment goal Before using any drug to treat BPH, develop a clear treatment goal with the patient.with the patient.. If symptoms are not bothersome and there . If symptoms are not bothersome and there are no indications for urologic evaluation, try "watchful are no indications for urologic evaluation, try "watchful waiting" first.waiting" first.
Patients with "mild" symptoms of BPH should be reassured and do Patients with "mild" symptoms of BPH should be reassured and do not need any treatment. not need any treatment. Many patients with "moderate" to Many patients with "moderate" to "severe" symptoms will improve spontaneously."severe" symptoms will improve spontaneously.

ResourcesResources
www.jr2.ox.ac.uk/bandolierwww.jr2.ox.ac.uk/bandolier www.auanet.orgwww.auanet.org www.aafp.orgwww.aafp.org www.ti.ubc.cawww.ti.ubc.ca